Back To Chiropractic Continuing Education Seminars
|
|
|
- Marilynn Reynolds
- 5 years ago
- Views:
Transcription
1 Welcome: Back To Chiropractic Continuing Education Seminars Basic AMA Impairment Ratings for Chiropractors: ~ 6 Hours This course counts as 6 Hours of CE for the Chiropractic Board of Examiners for the state of California. There is no time element to this course, take it at your leisure. If you read slow or fast or if you read it all at once or a little at a time it does not matter.
2 GLENN CRAFTS, B.S., D.C., Q.M.E. UTILIZATION REVIEW DIRECTOR PRIVATE PRACTICE Copyright -ALL RIGHTS RESERVED Do Not Duplicate or Distribute without written permission
3 Disclaimer The following course material contains the opinions of the author and does not reflect the opinions of the Division of Workers Compensation, or associated entities. This course is intended to be used as a reference tool in assisting QMEs, and is not to be relied on as legal advice.

4 Remember, the guide is a guide
5 Combine or Add Impairments? California DWC requires use of the AMA Guides to Impairment, 5 th Edition Use of the Combined Value Chart to determine impairment Combine all impairment ratings from one body part/region with other body part(s) Exceptions to combining = impairment for a single joint (i.e. thumb or elbow)
6 Chapters 15, 16 & 17 Chapter 15: The Spine Chapter 16: The Upper Extremities Chapter 17: The Lower Extremities
7 Chapters 15 The Spine Determine if you will use Diagnosis Related Estimate (DRE) vs. Range of Motion (ROM) method to calculate the spinal impairment present. Section 15.2 Determine the appropriate method Section 15.3 DREs (Diagnosis Related Estimates) Section 15.4 Page 384; Lumbar Spine DRE Section 15.5 Page 389; Thoracic Spine DRE Section 15.6 Page 392; Cervical Spine DRE

8 DRE vs. ROM AMA Guides, Pg. 379


9 DRE vs. ROM AMA Guides, Pg. 379


10 DRE vs. ROM AMA Guides, Pg. 380


11 DRE vs. ROM AMA Guides, Pg. 381
12 Section 15.2 Determining the Appropriate Method Takeaways Always review available medical records, take a careful and thorough history, AND examination to elucidate presence of structural abnormalities, neurological deficitsand loss of motion segmental integrity. Only evaluate impairments that are permanent (i.e. will not change over the next 12 moths with treatment). Identify the injured worker s most severe OBJECTIVE findings. Determine if there is MULTI-LEVEL involvement within the SAME region.
13 Section 15.2 Determining the Appropriate Method Takeaways Use ROM if: 1. There are fracturesat more than one level within the same spinal region (i.e. compression Fx at L2 & L4) 2. Radiculopathybilaterally OR- multiple levels within the same spinal region. 3. Multi-Level motion segmental alterationwithin the same spinal region (i.e. fusion L3-5) 4. Recurrent disc herniation OR-stenosis with radiculopathyat the same or different level within the same spinal region.
14 Section 15.2 Determining the Appropriate Method Takeaways Using DRE: Determine which category best fits the injured worker Most ratings are between category I-III Corticospinal tract injuries use Section 15.7 for spinal cord damage (Table 15-6) If residual symptoms impact the ability to perform ADLs (despite treatment), then assign the higher category percentage (i.e. Use 8% for a lumbar DRE category II; 5-8%) Combine DRE ratings from different regions of the spine (i.e. cervical & lumbar) using the Combine Values Chart.
15 Section 15.2 Determining the Appropriate Method Takeaways Using DRE: There are 5 DRE categoriesfor each spinal region (cervical, thoracic & lumbar) Categories are chosen based on 2 scenarios: 1. Signs, symptoms & diagnostic test results 2. Presence of fractures/dislocations with or without symptoms Altered motion segmental integrity qualifies for categories IV-V
16 To determine impairment evaluation process DRE vs. ROM
17
18 Choosing DRE Method The previous slide (figure 15.4) helps the QME/evaluator decide if DRE method should be used based on the following: 1. First, ensure the injured worker is now P&S (Permanent & Stationary) in order to determine any impairment. 2. Ensure there was in injury and that the injury applies to a single level (i.e. single vertebral level; L4-5 disc) 3. ROM would be used instead of DRE if there is multi-level involvement to the same spinal region (i.e. multiple fractures or multiple disc lesions at different levels; L2-3 & L4-5) 4. Read through the 5 categories (I-V) and place the injured worker into the most appropriate category based on their condition.

19 Place patient into appropriate category


20
21 Lumbar DRE Example
22 Section 15.4 Lumbar Spine DRE Read through the 5 categories of DRE (page 384 next slide) related to the lumbarspine to identify which category most appropriately describes the patient. Example: 40 year old male injured his lower back after lifting a heavy box at work. He is now P&S and suffers the following residuals: Physical Exam: Moderate palpable hypertonicityover the B/L lumbar paraspinals and right QL (quadratus lumborum). Diminished lumbar ROM with left lateral bending of 15/25 degrees. Patient complains of right leg pain into the hamstrings, but not verified as a true radiculopathy with diagnostic studies such as MRI/CT or electrodiagnostic studies. Diagnosis: Lumbar sprain/strain



23
24 Section 15.4 Lumbar Spine DRE The injured worker is best described as: DRE Lumbar Category II Rates between 5-8% Impairment of the Whole Person (WPI) Category II is most appropriate because the injured worker has: 1) a specific lifting injury 2) muscle spasm at time of the examination 3) asymmetric loss of range of motion 4) non-verifiable radicular complaint.
25 Section 15.4 Lumbar Spine DRE Q. How do we determine what WPI percentage to use for Category II (5-8%)? A. Determining which percentage of WPI is up to the QME/evaluator, but requires some form of substantiation. In this case, it would be medically appropriate to rate the injured worker towards the lower end, or 5%. The injured worker did not have objective medical evidence outside of the physical exam and subjective factor to support their complaint of LBP with concomitant radiculopathy (i.e. no MRI or EDS supporting discogenic lesion, or peripheral nerve entrapment was pathologically present). WPI = 5% per Lumbar Spine Category II
26 Section 15.4 Lumbar Spine DRE NOTE: If this case presented with more severe subjective factors and better objective support, then a higher rating more towards 8% could be justified.
27 Section 15.4 Lumbar Spine DRE Lumbar DRE Category III (10-13%) Impairment Requires significant signs of radiculopathy & confirmed by positive diagnostic study Surgical intervention for diagnosed radiculopathy (resolved or unresolved) Presence of compression fracture 25-50% of the vertebral body
28 Section 15.4 Lumbar Spine DRE Lumbar DRE Category IV (20-23%) Impairment Loss of motion segmental integrity (i.e. flexion/extension radiographs >4.5 mm Compression fracture that exceeds 50% of vertebral body without neuro compromise
29 Section 15.4 Lumbar Spine DRE Lumbar DRE Category V (25-28%) Impairment Meets criteria of BOTH categories III & IV Compression fracture that exceeds 50% of vertebral body with neurological compromise
30 Thoracic DRE Example
31 Section 15.5 Thoracic Spine DRE Section 15.5 Page 389 Read through the 5 categories of DRE (page 389 next slide) related to the thoracicspine to identify which category most appropriately describes the patient. Example: 32 year old male injured his mid back after falling off of a fork lift resulting in a compression fracture at the T11 vertebra. ADLs not inhibited much by this injury. Injured worker reports pain with heavy lifting and paresthesia into the right lower extremity. Physical Exam: Inconsistent decreased pinwheel sensation over the right LE. 4/5 muscle testing with right quads. X-Ray: compression fracture of T11 with 45% body height loss




32
33 Section 15.5 Thoracic Spine DRE This injured worker is best categorized in DRE III 15-18% impairment of the whole person Patient falls within the 25-50% compression fracture of one (1) vertebral body (T11 = 45% compression Fx) Patient also has residual neurological complaint of right LE paresthesia/weakness (4/5) that was documented by X-Ray and is an ongoing neurological impairment of the lower extremity. Diagnosis: T11 compression fracture Impairment: 18% since the compression fracture is nearly 50% of the vertebral body coupled with ongoing neurological findings.
34 Section 15.5 Thoracic Spine DRE Thoracic spine DRE category IV would be appropriate if the compression fracture was > 50% of the T11 vertebral body WITHOUT neural compromise. DRE IV would also be appropriate if there was alteration of motion segment integrity ORbilateral/multi-level radiculopathy (i.e. requires flexion/extension x-ray views; > 2.5 mm)
35 Section 15.5 Thoracic Spine DRE Thoracic spine DRE category V would be appropriate if the compression fracture was > 50% of the T11 vertebral body WITH neural compromise. DRE Vwould also be appropriate if there was impairment of the lower extremity defined by category III AND-loss of structural integrity defined by category IV.
36 Cervical DRE Example
37 Section 15.6 Cervical Spine DRE Section 15.6 Page 392 Read through the 5 categories of DRE (page 392 next slide) related to the cervicalspine to identify which category most appropriately describes the patient. Example: 39 year old female injured her neck from slip and fall at work onto a cement floor in a warehouse. She developed neck pain that radiates into her right digits 1-2. Conservative therapies and medications failed to ameliorate her pain. MRI revealed a herniated disc at C6-7. She had surgery to remove the C6-7 disc and fuse the two vertebra. Currently, she has residual neck pain. Right upper extremity neurological deficits resolved after surgery. Physical Exam: Decreased ROM Neurological exam unremarkable Positive shoulder depressor test for hypertonic upper traps B/L




38
39 Section 15.6 Cervical Spine DRE This injured worker is best categorized in DRE IV 25-28% impairment of the whole person DRE category IV is appropriate because of the alteration of motion segment integrity (fusion) Diagnosis: Disc herniation at C6-7 Impairment: 28% since the injured worker underwent surgical intervention to remove the C6-7 disc and fuse two vertebrae. Segmental motion at C6-7 is lost permanently with the fusion procedure.
40 Section 15.6 Cervical Spine DRE Cervical spine DRE category V would be appropriate IF there was significant upper extremity impairment/total neurologic loss at a single level ORsevere multi-level neurologic dysfunction. Since this patient did not have any residual extremity pain, category V would be inappropriate. DRE V would be appropriate if there were fractures, structural compromise of the spinal canal with severe upper extremity motor & sensory deficits (without lower extremity involvement)


41
42 Switching Gears Let s use the ROM Method

43
44 ROM Method - Spine Section 15.8 Page 398 Things to remember: Use ROM method of rating if the injury applies to more than a single level (i.e. L2, L3 & L5) Cannot rate if acuteor not P&S ROM method is based on: 1. Diagnosis 2. Measuring the ROMs 3. Neurologic Deficit Combining 1-3 (above) using the Combined Values Chart
45 ROM Method Spine Section 15.8 Page 398 Things to remember: 1. Warm-up first 2. Obtain at least 3 consecutive measurements 3. Calculate the mean (average) of the three. 4. The mean is calculated by adding the highest and lowest value and dividing by two. 5. If the average is < 50 degrees, the 3 consecutive measurements should fall within 5 degrees of the mean. 6. If the average is > 50 degrees, the 3 consecutive measurements must fall within 10% of the mean. 7. ROM testing may be repeated up to 6 times. 8. If after 6 attempts this criteria is not met, the results are considered INVALID!
46 ROM Method Spine Table 15-7 = Used to determine the Diagnosis based impairment with ROM method. If there are >2 diagnoses within the same spinal region, then choose the most significant DDX. This percentage will be combined with the impaired ROM AND- neurologic deficit.


47 ROM Method Diagnosis Based Impairment Table 15-7; Page 404


48 ROM Method Diagnosis Based Impairment Table 15-7; Page 404



49 ROM Method Diagnosis Based Impairment Table 15-7; Page 404
50 ROM Method Diagnosis Based Impairment Table 15-7; Page 404 Section I Use for diagnosis of fractures Choose spinal region (cervical, thoracic, lumbar) Apply WPI %
51 ROM Method Diagnosis Based Impairment Table 15-7; Page 404 Section II Use for diagnosis of disc herniations Choose spinal region (cervical, thoracic, lumbar) Apply WPI % Add 1% (per spinal level) if multiple levels with/without residual signs & symptoms Add 2% if multiple operations with/without residual signs & symptoms Includes 2 nd operation Add 1% (per operation) with 3 or more operations
52 ROM Method Diagnosis Based Impairment Table 15-7; Page 404 Section III Use for diagnosis of spondylosis & spondylolisthesis (NOT operated on) Choose appropriate grade of spondy and apply WPI%
53 ROM Method Diagnosis Based Impairment Table 15-7; Page 404 Section IV Use for diagnosis of spinal stenosis, segmental instability, spondylolisthesis, fracture or dislocation(operated on) Add 1%per level if multiple levels (operated on) WITH residual signs & symptoms Add 2% (if 2 nd operation) and with multiple levels (operated on) WITHresidual and medically documented pain/rigidity Add 1% (per operation) that is 3 or more operations.
54 ROM Range of Motion Method (Inclinometry)
55 Measure the ROM Page 403 Use dual inclinometers for spinal measurements Calculate the average of each set of 3 Determine if the 3 measurements fall within 5 degrees OR-10% of the mean, whichever is larger 6 attempts are allowed before the measurements are invalid Use the maximum motion to determine any impairment rating If there are impairments due to loss of motion in more than one plane within the same spinal region, then ADD the impairments to determine TOTAL Impairment of that spinal region.
56 Examples of when to use ROM Method: DRE method does not apply; patient cannot be categorized If there is multi-level involvement in the same spinal region (i.e. Fx at multiple levels, disc herniations or stenosis with radiculopathy at multiple levels or bilaterally
57 Dual Inclinometers Where do I put them?


58

59
60 Section 15.9 Lumbar Spine ROM Use Figure 15-8 & 15-9; page 405 & 408 for inclinometer placement Use Table 15-8; page 407 lumbar flexion/extension impairment Use Table 15-9; page 409 lumbar lateral bending impairment Example: 44 year old male injured his lower back after carrying a box and tripping over an open drawer. He is P&S and suffers the following residuals: ROM vs DRE -Spine Example: DDX: Lumbar Disc Protrusion (L5-S1) (MRI Verified) = 7% using Table 15-7 II. c. Paresthesia along right lateral calf decreased light touch minimally Decreased AROMs Range of Motion (ROM) method to be used with lumbar spine. DRE not to be used for lumbar spine rating when multiple levels are identified objectively through MRI and clinical findings on exam.
61 Section 15.9 Lumbar Spine ROM Physical Exam: Lumbar Spine Normal (Degrees ) Exam Exam (Mean) Maximum Angle (WPI%) Flexion 60 20, 25, % Extension 25 10, 10, % (L) Lateral Flexion 25 12, 12, % (R) Lateral Flexion 25 15, 15, % Diagnosis: M54.5
62 Determine Neurologic Deficits Table (Sensory) & Table (motor) Use Table = Sensory neurologic deficits Use Table = Motor neurologic deficits Use Table = Upper Extremitynerve roots Use Table = Lower Extremitynerve roots



63
64 Determine Neurologic Deficits Table (Sensory) Use Table = Sensory neurologic deficits Choose the appropriate Grade between 0-5 Choose the appropriate % sensory deficit Step 1. Identify the area of nerve deficit using the dermatome charts (Figure 15-1 & Figure 15-2) NOTE: Right lateral calf paresthesia is identified on physical exam (L5)

65 Determine Neurologic Deficits Lower Extremities
66 Determine Neurologic Deficits Upper Extremities
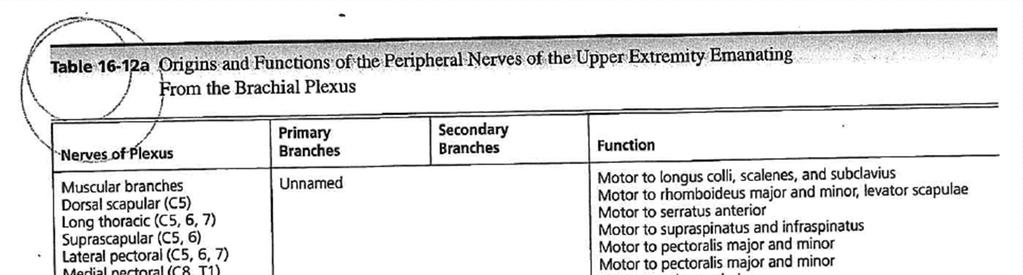
67 Determine Neurologic Deficits Table & Figure (Upper Extremity) Step 2. Identify the nerve(s) that innervate the area(s) (Table & Figure 16-48) L5 = Involves the lateral calf region




68

69

70

71 Determine Neurologic Deficits Step 3. Grade the severity of the SENSORYdeficit or pain according to the classification in Table section a(grade 0-5).
72 Determine Neurologic Deficits Step 3. Grade the severity of the SENSORYdeficit or pain according to the classification in Table section a(grade 0-5). Injured worker has distorted superficial tactile sensibility (i.e. decreased light touch) with or without minimal abnormal sensations or pain, that is forgotten during activity. This equates to a Grade 4, and range between 1-25 % sensory deficit.
73 Determine Neurologic Deficits Step 4. Find the MAXIMUM Impairment of the extremity(ies) due to SENSORY deficit or pain for EACH spinal nerve (Table 15-18) & brachial plexus (Table 16-14) Example: DDX: Lumbar Disc Protrusion (L5-S1) (MRI Verified) Paresthesia along right lateral calf Decreased light touch Decreased AROMs
 due to SENSORY deficit or pain for EACH spinal nerve (Table 15-18) L5")
74 Determine Neurologic Deficits Step 4. Find the MAXIMUM Impairment of the extremity(ies) due to SENSORY deficit or pain for EACH spinal nerve (Table 15-18) L5 is the involved nerve root in this example L5 represents a 5% maximum sensory deficit
75 Determine Neurologic Deficits Step 5. Severity of Sensory Deficit (Table 15-15) x Maximum Impairment Value (Table 15-18) = Extremity Impairment for each Spinal Nerve Grade 4 (10% is chosen) since persistent mild right calf paresthesia. Maximum sensory deficit for L5 is 5% 10% x 5% = 1% Extremity Impairment for L5
76 Determine Neurologic Deficits Step 5. NOTE: A similar process is performed for strength (MOTOR)involvement using Table and Table The example with this injured worker did not reveal any motor loss, so Table & Table will not be used for impairment rating.
77 Calculating the Final Impairment ROM Method Use Table to calculate the final WPI with the ROM method using all 3 categories below with this example: 1. Diagnosis (7%) 2. Measuring the ROMs (13%) 3. Neurologic Deficit (1%) Combine the above impairments using the Combined Value Charton page 604.




78
79 Calculating the Final Impairment Combined 1. To use the Combined Value Chart, take the highest impairment % and find the corresponding # on the extreme left of the chart (vertical/y-axis). 2. Then locate the next highest impairment % on the extreme bottom of the chart (horizontal/x-axis). 3. Where these two numbers intersectwill represent the impairment. 4. If you have multiple numbers to combine, then repeat these steps until you arrive at a final total WPI (Whole Person Impairment). 5. The number found in step 3 (above) is then found in the extreme left column and combined with the next highest number at the very bottom. Reapply these steps until all ratings have been combined to a single final Impairment rating.



80 13% combined with 7% = 19% Impairment


81 19% combined with 1% = 20% Impairment
82 Calculating the Final Impairment ROM Method 1. Diagnosis (7%) 2. Measuring the ROMs (13%) 3. Neurologic Deficit (1%) 13% combined with 7% = 19% 19% combined with 1% = 20% Total WPI = 20%

83



84

85 Cervical Spine ROM Example
86 Cervical Spine ROM Example Spinal Measurements: Table 15-12; Page 418; (Cervical Flexion/Extension) Chapter 15 Table 15-13; Page 420; (Cervical Lateral Flexion) Chapter 15 Table 15-14; Page 421; (Cervical Rotation) Chapter 15
87 Cervical Spine ROM Example Cervical Spine Normal (Degrees ) Exam Flexion 50 52, 52, 50 Extension 60 60, 62, 65 Exam (Mean) Maximum Angle (WPI%) Right Rotation 80 65, 68, 68 Left Rotation 80 65, 70, 68 Right Lateral Flexion 45 30, 30, 32 Left Lateral Flexion 45 37, 40, 38
88 Cervical Spine ROM Example Figure 15-18; Page 422; (Cervical Range of Motion (ROM)*) Chapter 15 Use tables below to determine the WPI for the cervical spine based on the measurements in the previous slide. No Neurologic Deficit reported/documented No Diagnosis Based Impairment to apply (Table 15-7) TOTAL Cervical ROM Impairment=???%


89 Dual Inclinometers Where do I put them?




90


91




92
93 AMA Guides to the Evaluation of Permanent Impairment (5th Edition) Cervical Spine Normal (Degrees ) Exam Exam (Mean) Maximum Angle (WPI%) Flexion 50 52, 52, Extension 60 60, 62, Right Rotation 80 65, 68, Left Rotation 80 65, 70, Right Lateral Flexion 45 30, 30, Left Lateral Flexion 45 37, 40, Add up the individual WPI per cervical ROM to total = 4% Cervical WPI (ROM)


94
95 Play Role in Impairment




96
97 Pain Add On Pain Add On -Example: Body Parts Chapter Number Table/Figure Number Pain Related Impairment(Slight) 18-Page 574 Figure 18-1 Page 5 of the AMA Guides indicates The Guidesrefers to common ADLs, as listed in Table 1-2. The ADLs listed in this table correspond to the activities that physicians should consider when establishing a permanent impairment rating. A physician can often assess a person s ability to perform ADLs based on knowledge of the patient s medical condition and clinical judgment. A 3% whole person impairment for pain may be assigned. Please review figure 18-1, page 574 of the AMA Guides and also 18.3d part C on page 573. Step three states If pain-related impairment appears to increase the burden of the individual s condition slightly, the examiner can increase the percentage found in step 1 by up to 3%. No formal assessment of pain-related impairment is required.
98 Upper Extremity AMA Rating


99 Goniometer
100 Upper Extremity Step 1: Hand

 and enter the values on the Upper")
101 Upper Extremity Steps to Evaluating Impairment Section 16.9 Page 511: (Hand): Determine impairment (if applicable) and enter the values on the Upper Extremity Evaluation Record (Figure 16-1a); Part 1
: Determine impairment (if applicable) and enter the values on the")
102 Upper Extremity Steps to Evaluating Impairment Section 16.9 Page 511: (Wrist, Elbow & Shoulder): Determine impairment (if applicable) and enter the values on the Upper Extremity Evaluation Record (Figure 16-1b); Part 2
.")
103 Upper Extremity Steps to Evaluating Impairment Determine any HAND impairment using Figure 16-1a Upper Extremity Impairment Evaluation Record (Part 1). Convert the Thumb Impairment to Hand Impairment using (Table 16-1)


104 Upper Extremity Steps to Evaluating Impairment Convert the Total Hand Impairment to Upper Extremity Impairment using (Table 16-2)


105 Upper Extremity Steps to Evaluating Impairment Convert the Total Upper Extremity Impairment to a final whole Person Impairment using (Table 16-3)
106 Upper Extremity Step 2: Wrist, Elbow, Shoulder
107 Upper Extremity Steps to Evaluating Impairment Determine any WRIST, ELBOW, SHOULDER impairment using Figure 16-1b Upper Extremity Impairment Evaluation Record (Part 2). WRIST: Determine the impairments due to loss of motion (AROM) (section 16.4g) Determine the impairment due to other disorders (i.e. tenosynovitis) (section 16.7) Combine the values to determine the Upper Extremity Impairment related to the WRIST. Enter this impairment on Line 2 (Figure 16-1b) ELBOW: Determine Upper Extremity Impairments due to loss of motion (AROM) (section 16.4h) Determine the impairment due to other disorders (section 16.7) Combine the values to determine the Upper Extremity Impairment related to the ELBOW. Enter this impairment on Line 2 (Figure 16-1b) SHOULDER: Determine Upper Extremity Impairments due to loss of motion (AROM) (section 16.4i) Determine the impairment due to other disorders (section 16.7) Combine the values to determine the Upper Extremity Impairment related to the SHOULDER. Enter this impairment on Line 2 (Figure 16-1b)
108 Upper Extremity Steps to Evaluating Impairment Determine the TOTAL UPPER EXTREMITY IMPAIRMENT by combining parts I-IV in Figure 16-1b (below) NOTE: Some part(s) may not apply (i.e. no amputation, etc.)
 using Table")
109 Upper Extremity Steps to Evaluating Impairment Determine the TOTAL UPPER EXTREMITY IMPAIRMENT Enter on the bottom of part 2 Convert the TOTAL Upper Extremity Impairment to a WHOLE PERSON IMPAIRMENT (WPI) using Table 16-3
110 Upper Extremity Example
111 Upper Extremity Example Extremity Impairment - Example: DDX: (R) Elbow-Lateral Epicondylitis & (R) wrist strain Figure 16-34; Page 472; (Pie Chart Elbow Flexion/Extension) Chapter 16 Figure 16-37; Page 474; (Pie Chart Elbow Supination/Pronation) Chapter 16 Right Elbow Normal (Degrees ) Exam Exam (Mean) Maximum Angle (WPI%) Flexion , 125, % Extension 0 0, 0, 0 0 0% Supination 80 65, 65, % Pronation 80 70, 72, %
112 Upper Extremity Impairment Example Find elbow measurement on corresponding arc Supination = top of arc Pronation = bottom of arc Example: 30 degrees of supination represents 2% impairment
 wrist strain Figure 16-34; Page 472; (Pie Chart Elbow Flexion/Extension)")
113 Upper Extremity Impairment Example Extremity Impairment - Example: DDX: (R) Elbow-Lateral Epicondylitis & (R) wrist strain Figure 16-34; Page 472; (Pie Chart Elbow Flexion/Extension) Chapter 16
 wrist strain Figure 16-37; Page 474; (Pie Chart Elbow Supination/Pronation)")
114 Upper Extremity Impairment Example Extremity Impairment - Example: DDX: (R) Elbow-Lateral Epicondylitis & (R) wrist strain Figure 16-37; Page 474; (Pie Chart Elbow Supination/Pronation) Chapter 16
115 Upper Extremity Impairment Example Extremity Impairment - Example: DDX: (R) Elbow-Lateral Epicondylitis & (R) wrist strain Figure 16-31; Page 469; (Pie Chart Wrist Radial/Ulnar Deviation) Chapter 16
116 Upper Extremity Impairment Example Extremity Impairment - Example: DDX: (R) Elbow-Lateral Epicondylitis & (R) wrist strain Figure 16-28; Page 467; (Pie Chart Wrist Flexion/Extension) Chapter 16
117 Upper Extremity Impairment Example Extremity Impairment - Example: DDX: (R) Elbow-Lateral Epicondylitis & (R) wrist strain Figure 16-28; Page 467; (Pie Chart Wrist Flexion/Extension) Chapter 16 Figure 16-31; Page 469; (Pie Chart Wrist Radial/Ulnar Deviation) Chapter 16 Right Wrist Normal (Degrees ) Exam Exam (Mean) Maximum Angle (WPI%) Flexion 60 45, 44, % Extension 60 47, 46, % Radial Deviation 20 12, 14, % Ulnar Deviation 30 17, 16, %
118 Extremity Impairment - Example: Upper Extremity Impairment Example DDX: (R) Elbow-Lateral Epicondylitis & (R) wrist strain The following tables/figures are necessary to determine a rating for the upper extremities: Figure 16-1b; Page 437; Upper Extremity Impairment Evaluation Record (Wrist, Elbow, Shoulder); Chapter 16 (Right Upper Extremity) Figure 16-1b yielded: 10% (Wrist) and 3% (Elbow) which combines to 13% Table 16-3 (Pg 439) was used to convert the Total Upper Extremity Impairment (13%) to Impairment of the Whole Person (8%) (Right Upper Extremity) Impairment of the Whole Person = 8%
119 Upper Extremity Shoulder Measurements


120 Upper Extremity Shoulder Measurements


121 Upper Extremity Shoulder Measurements


122 Upper Extremity Shoulder Measurements


123 Still Awake?
124 Resources State of California Dept. of Insurance UR and Causation section of FAQs: Division of Workers Compensation Dept. of Industrial Relations - URAC MTUS Regulations: ACOEM-Occupational Medicine Practice Guidelines 2 nd Edition 2004 CWCI LexisNexis ICD-10 CM PMIC 2015 CPT Plus PMIC AMA Guides, 5 th Edition 2005


125 Thanks So Much For Being Here Today! Hope To See You Soon Back To Chiropractic CE Seminars! backtochiropractic.net 125
QME AMA Impairment Ratings (6hrs) ~ Glenn Crafts, DC ~ Back to Chiropractic CE Seminars
 ~ Glenn Crafts, DC ~ Back to Chiropractic CE Seminars") QME AMA Impairment Ratings (6hrs) ~ Glenn Crafts, DC ~ Back to Chiropractic CE Seminars Instructions: Answer all questions and email answers to: marcusstrutzdc@gmail.com Please DO NOT scan tests or test
QME AMA Impairment Ratings (6hrs) ~ Glenn Crafts, DC ~ Back to Chiropractic CE Seminars Instructions: Answer all questions and email answers to: marcusstrutzdc@gmail.com Please DO NOT scan tests or test
Basic AMA Impairment Ratings for Chiropractors CE Exam 6 Hours ~ Back to Chiropractic CE Seminars
 Basic AMA Impairment Ratings for Chiropractors CE Exam 6 Hours ~ Back to Chiropractic CE Seminars Simply list your answers (write down letter choice only: in a NUMBERED vertical column and email to: marcusstrutzdc@gmail.com
Basic AMA Impairment Ratings for Chiropractors CE Exam 6 Hours ~ Back to Chiropractic CE Seminars Simply list your answers (write down letter choice only: in a NUMBERED vertical column and email to: marcusstrutzdc@gmail.com
RECIPES FOR RATINGS !!! A. FIBROMYALGIA: 0% WPI P. 569 B. THORACIC OUTLET SYNDROME 0% WPI P. 569 C. MYOFASCIAL PAIN SYNDROME 0% WPI P.
 RECIPES FOR RATINGS 1. THE "0% WPI" RATINGS A. FIBROMYALGIA: 0% WPI P. 569 B. THORACIC OUTLET SYNDROME 0% WPI P. 569 C. MYOFASCIAL PAIN SYNDROME 0% WPI P. 569 D. TENDINITIS OF UPPER EXTREMITY 0% WPI P.
RECIPES FOR RATINGS 1. THE "0% WPI" RATINGS A. FIBROMYALGIA: 0% WPI P. 569 B. THORACIC OUTLET SYNDROME 0% WPI P. 569 C. MYOFASCIAL PAIN SYNDROME 0% WPI P. 569 D. TENDINITIS OF UPPER EXTREMITY 0% WPI P.
THE SPINE AMA GUIDES CHAPTER 15
 THE SPINE AMA GUIDES CHAPTER 15 Tim Mussack Marlene Phillips Bradford & Barthel, LLP AMA Analysis and Ratings Division HOUSEKEEPING ITEMS To control background noise, all attendees will be muted. Access
THE SPINE AMA GUIDES CHAPTER 15 Tim Mussack Marlene Phillips Bradford & Barthel, LLP AMA Analysis and Ratings Division HOUSEKEEPING ITEMS To control background noise, all attendees will be muted. Access
4/28/2015 DR. TRACY W. PRICE, D.C. PPI due to injury or illness AMA GUIDES TO THE EVALUATION OF PERMANENT IMPAIRMENT 5 TH EDITION
 DR. TRACY W. PRICE, D.C CHAPEL HILL CHIROPRACTIC CENTER, INC. 1520 HOME AVE. AKRON, OH 44310 PH.330.630.1500: FAX.330.630.9303 EMAIL: DOCKTRACY@AOL.COM WEB: AKRONCHHIRO.COM AMA GUIDES TO THE EVALUATION
DR. TRACY W. PRICE, D.C CHAPEL HILL CHIROPRACTIC CENTER, INC. 1520 HOME AVE. AKRON, OH 44310 PH.330.630.1500: FAX.330.630.9303 EMAIL: DOCKTRACY@AOL.COM WEB: AKRONCHHIRO.COM AMA GUIDES TO THE EVALUATION
IMPAIRMENT RATING 5 TH EDITION MODULE III THE UPPER EXTREMITIES AND PAIN
 IMPAIRMENT RATING 5 TH EDITION MODULE III THE UPPER EXTREMITIES AND PAIN PRESENTED BY: RONALD J. WELLIKOFF, D.C., FACC, FICC In conjuction with: The physical examination is the determining factor of a
IMPAIRMENT RATING 5 TH EDITION MODULE III THE UPPER EXTREMITIES AND PAIN PRESENTED BY: RONALD J. WELLIKOFF, D.C., FACC, FICC In conjuction with: The physical examination is the determining factor of a
EVALUATING AMA IMPAIRMENT IN CALIFORNIA. Report Writing Mark Evans, DWC Rater
 EVALUATING AMA IMPAIRMENT IN CALIFORNIA Report Writing Mark Evans, DWC Rater What Makes a Good Report? Identifiers Patient name Claim number Date of injury Date of birth Occupation/duties Introduction/purpose
EVALUATING AMA IMPAIRMENT IN CALIFORNIA Report Writing Mark Evans, DWC Rater What Makes a Good Report? Identifiers Patient name Claim number Date of injury Date of birth Occupation/duties Introduction/purpose
Steven Feinberg MD Andrew Sew Hoy MD
 Steven Feinberg MD Andrew Sew Hoy MD COA Conference April 17 th 2010 September 3 rd 2009 PD Rating rebuttable may use any method within the Guides of the Evaluation of Permanent Impairment 5 th Edition
Steven Feinberg MD Andrew Sew Hoy MD COA Conference April 17 th 2010 September 3 rd 2009 PD Rating rebuttable may use any method within the Guides of the Evaluation of Permanent Impairment 5 th Edition
Case Studies, Impairment of the Spine in Washington State
 Case Studies, Impairment of the Spine in Washington State NAOEM at Skamania, 2015 25 Sep, 2015 Tim Gilmore, MD Several Slides from this Presentation Borrowed with permission from the Washington State Department
Case Studies, Impairment of the Spine in Washington State NAOEM at Skamania, 2015 25 Sep, 2015 Tim Gilmore, MD Several Slides from this Presentation Borrowed with permission from the Washington State Department
Regional Review of Musculoskeletal System: Head, Neck, and Cervical Spine Presented by Michael L. Fink, PT, DSc, SCS, OCS Pre- Chapter Case Study
 Regional Review of Musculoskeletal System: Presented by Michael L. Fink, PT, DSc, SCS, OCS (20 minutes CEU Time) Subjective A 43-year-old male, reported a sudden onset of left-sided neck and upper extremity
Regional Review of Musculoskeletal System: Presented by Michael L. Fink, PT, DSc, SCS, OCS (20 minutes CEU Time) Subjective A 43-year-old male, reported a sudden onset of left-sided neck and upper extremity
WORKPLACE SAFETY AND INSURANCE APPEALS TRIBUNAL DECISION NO. 2192/16
 WORKPLACE SAFETY AND INSURANCE APPEALS TRIBUNAL DECISION NO. 2192/16 BEFORE: E. Kosmidis: Vice-Chair HEARING: August 30, 2016 at Toronto Written DATE OF DECISION: October 25, 2016 NEUTRAL CITATION: 2016
WORKPLACE SAFETY AND INSURANCE APPEALS TRIBUNAL DECISION NO. 2192/16 BEFORE: E. Kosmidis: Vice-Chair HEARING: August 30, 2016 at Toronto Written DATE OF DECISION: October 25, 2016 NEUTRAL CITATION: 2016
Cervical Spine in Baseball
 Cervical Spine in Baseball Robert G Watkins, IV, MD Co-Director, Marina Spine Center Marina del Rey, CA Vice Chief of Staff Cedars-Marina del Rey Hospital Disclosures n Pioneer / RTI Consulting, Royalties
Cervical Spine in Baseball Robert G Watkins, IV, MD Co-Director, Marina Spine Center Marina del Rey, CA Vice Chief of Staff Cedars-Marina del Rey Hospital Disclosures n Pioneer / RTI Consulting, Royalties
Case Report: CASE REPORT OF FACET ARTHROPATHY INDUCED NERVE ROOT COMPRESSION RESULTING IN MOTOR WEAKNESS AND PAIN
 Cox Technic Case Report #100 published at www.coxtechnic.com (sent October 2011 on 10/11/11 ) 1 Case Report: CASE REPORT OF FACET ARTHROPATHY INDUCED NERVE ROOT COMPRESSION RESULTING IN MOTOR WEAKNESS
Cox Technic Case Report #100 published at www.coxtechnic.com (sent October 2011 on 10/11/11 ) 1 Case Report: CASE REPORT OF FACET ARTHROPATHY INDUCED NERVE ROOT COMPRESSION RESULTING IN MOTOR WEAKNESS
Comprehension of the common spine disorder.
 Objectives Comprehension of the common spine disorder. Disc degeneration/hernia. Spinal stenosis. Common spinal deformity (Spondylolisthesis, Scoliosis). Osteoporotic fracture. Anatomy Anatomy Anatomy
Objectives Comprehension of the common spine disorder. Disc degeneration/hernia. Spinal stenosis. Common spinal deformity (Spondylolisthesis, Scoliosis). Osteoporotic fracture. Anatomy Anatomy Anatomy
Cox Technic Case Report #169 published at (sent 5/9/17) 1
 1") Cox Technic Case Report #169 published at www.coxtechnic.com (sent 5/9/17) 1 Management of Lumbar Radiculopathy Associated with an Extruded L4 L5 disc and concurrent L5 S1 Spondylolytic Spondylolisthesis
Cox Technic Case Report #169 published at www.coxtechnic.com (sent 5/9/17) 1 Management of Lumbar Radiculopathy Associated with an Extruded L4 L5 disc and concurrent L5 S1 Spondylolytic Spondylolisthesis
RADICULOPATHY AN INTRODUCTION TO
 AN INTRODUCTION TO RADICULOPATHY This booklet provides general information on radiculopathy. It is not meant to replace any personal conversations that you might wish to have with your physician or other
AN INTRODUCTION TO RADICULOPATHY This booklet provides general information on radiculopathy. It is not meant to replace any personal conversations that you might wish to have with your physician or other
WORKPLACE SAFETY AND INSURANCE APPEALS TRIBUNAL DECISION NO. 111/15
 WORKPLACE SAFETY AND INSURANCE APPEALS TRIBUNAL DECISION NO. 111/15 BEFORE: V. Marafioti: Vice-Chair HEARING: January 14, 2015 at Toronto Written Post-hearing activity completed on April 30, 2015 DATE
WORKPLACE SAFETY AND INSURANCE APPEALS TRIBUNAL DECISION NO. 111/15 BEFORE: V. Marafioti: Vice-Chair HEARING: January 14, 2015 at Toronto Written Post-hearing activity completed on April 30, 2015 DATE
Common Thoraco- Lumbar Problems in the Mature Athlete
 Common Thoraco- Lumbar Problems in the Mature Athlete Diana Heiman, MD Associate Professor, Family Medicine Residency Director East Tennessee State University Objectives Review the pathophysiology of the
Common Thoraco- Lumbar Problems in the Mature Athlete Diana Heiman, MD Associate Professor, Family Medicine Residency Director East Tennessee State University Objectives Review the pathophysiology of the
HISTORY AND CHIEF COMPLAINT:
 submitted by Keith M. Bartley, D.C. Jasper, IN 07/21/11 presented at Cox Seminar in Nashville, TN, on October 8 9, 2011 HISTORY AND CHIEF COMPLAINT: 01/21/11 55 year old male press operator for Jasper
submitted by Keith M. Bartley, D.C. Jasper, IN 07/21/11 presented at Cox Seminar in Nashville, TN, on October 8 9, 2011 HISTORY AND CHIEF COMPLAINT: 01/21/11 55 year old male press operator for Jasper
PREPARED FOR. Marsha Eichhorn DATE OF INJURY : N/A DATE OF ANALYSIS : 12/14/2016 DATE OF IMAGES : 12/8/2016. REFERRING DOCTOR : Dr.
 Accent on Health Chiropractic 405 Firemans Ave PREPARED FOR Marsha Eichhorn DATE OF INJURY : N/A DATE OF ANALYSIS : 12/14/2016 DATE OF IMAGES : 12/8/2016 REFERRING DOCTOR : Dr. David Bohn This report contains
Accent on Health Chiropractic 405 Firemans Ave PREPARED FOR Marsha Eichhorn DATE OF INJURY : N/A DATE OF ANALYSIS : 12/14/2016 DATE OF IMAGES : 12/8/2016 REFERRING DOCTOR : Dr. David Bohn This report contains
[7] 5-214F - 5 = 06%
![[7] 5-214F - 5 = 06%](/thumbs/86/93472785.jpg "[7] 5-214F - 5 = 06%") Craig Andrew Lange craig@pdratings.com Our Document # 1201Taffy (PTP Rating) Impairment & Disability Rating Specialists http://www.pdratings.com/ Voice: (415) 861-4040 / Fax: (415) 276-3741 Luis Pérez-Cordero
Craig Andrew Lange craig@pdratings.com Our Document # 1201Taffy (PTP Rating) Impairment & Disability Rating Specialists http://www.pdratings.com/ Voice: (415) 861-4040 / Fax: (415) 276-3741 Luis Pérez-Cordero
Objectives. Comprehension of the common spine disorder
 Objectives Comprehension of the common spine disorder Disc degeneration/hernia Spinal stenosis Common spinal deformity (Spondylolisthesis, Scoliosis) Osteoporotic fracture Destructive spinal lesions Anatomy
Objectives Comprehension of the common spine disorder Disc degeneration/hernia Spinal stenosis Common spinal deformity (Spondylolisthesis, Scoliosis) Osteoporotic fracture Destructive spinal lesions Anatomy
Medical Affairs Policy
 Medical Affairs Policy Service: Back Pain Procedures-Epidural Injection (Caudal Epidural, Selective Nerve Root Block, Interlaminar, Transforaminal, Translaminar Epidural Injection) PUM 250-0015-1706 Medical
Medical Affairs Policy Service: Back Pain Procedures-Epidural Injection (Caudal Epidural, Selective Nerve Root Block, Interlaminar, Transforaminal, Translaminar Epidural Injection) PUM 250-0015-1706 Medical
eck and Low ack pain: ddressing he Surgical valuation
 eck and Low ack pain: ddressing he Surgical valuation KI FOX, DO T WORTH BRAIN & SPINE Goals Review anatomy Identify sources of pain Imaging: the good, the bad, and the ugly PE: findings to determine source
eck and Low ack pain: ddressing he Surgical valuation KI FOX, DO T WORTH BRAIN & SPINE Goals Review anatomy Identify sources of pain Imaging: the good, the bad, and the ugly PE: findings to determine source
WORKPLACE SAFETY AND INSURANCE APPEALS TRIBUNAL DECISION NO. 147/15
 WORKPLACE SAFETY AND INSURANCE APPEALS TRIBUNAL DECISION NO. 147/15 BEFORE: B. Goldberg: Vice-Chair HEARING: January 20, 2015 at Toronto Written DATE OF DECISION: January 27, 2015 NEUTRAL CITATION: 2015
WORKPLACE SAFETY AND INSURANCE APPEALS TRIBUNAL DECISION NO. 147/15 BEFORE: B. Goldberg: Vice-Chair HEARING: January 20, 2015 at Toronto Written DATE OF DECISION: January 27, 2015 NEUTRAL CITATION: 2015
EVALUATION AND MANAGEMENT OF CERVICAL SPINE DISORDERS
 CERVICAL SPINE EVALUATION AND MANAGEMENT OF CERVICAL SPINE DISORDERS Gregory M Yoshida MD Supports the skull Allows movement of the head Houses the spinal cord CERVICAL SPINE Unique anatomy Upper C spine
CERVICAL SPINE EVALUATION AND MANAGEMENT OF CERVICAL SPINE DISORDERS Gregory M Yoshida MD Supports the skull Allows movement of the head Houses the spinal cord CERVICAL SPINE Unique anatomy Upper C spine
ESI - Utilization Review Case Presentation
 ESI - Utilization Review Case Presentation Request for ESI Hx & PE 31 y/o F parts warehouse stocker DOI: 2008 MOI: felt tightness in legs and shoulders reaching into a shelf to move a product from one
ESI - Utilization Review Case Presentation Request for ESI Hx & PE 31 y/o F parts warehouse stocker DOI: 2008 MOI: felt tightness in legs and shoulders reaching into a shelf to move a product from one
* WORKPLACE SAFETY AND INSURANCE APPEALS TRIBUNAL DECISION NO. 84/07
 * WORKPLACE SAFETY AND INSURANCE APPEALS TRIBUNAL DECISION NO. 84/07 BEFORE: A. Suissa: Vice-Chair HEARING: January 12, 2007 at Toronto Written DATE OF DECISION: January 12, 2007 NEUTRAL CITATION: 2007
* WORKPLACE SAFETY AND INSURANCE APPEALS TRIBUNAL DECISION NO. 84/07 BEFORE: A. Suissa: Vice-Chair HEARING: January 12, 2007 at Toronto Written DATE OF DECISION: January 12, 2007 NEUTRAL CITATION: 2007
Evaluation of Tingling and Numbness in the Upper Extremities
 Evaluation of Tingling and Numbness in the Upper Extremities DR. W. ANTHONY FRISELLA M.D. ADVANCED BONE & JOINT, ST CHARLES MO MONA 2018 Overview Polyneuropathy Compressive nerve lesions Carpal tunnel
Evaluation of Tingling and Numbness in the Upper Extremities DR. W. ANTHONY FRISELLA M.D. ADVANCED BONE & JOINT, ST CHARLES MO MONA 2018 Overview Polyneuropathy Compressive nerve lesions Carpal tunnel
Original Date: October 2015 LUMBAR SPINAL FUSION FOR
 National Imaging Associates, Inc. Clinical guidelines Original Date: October 2015 LUMBAR SPINAL FUSION FOR Page 1 of 9 INSTABILITY AND DEGENERATIVE DISC CONDITIONS FOR CMS (MEDICARE) MEMBERS ONLY CPT4
National Imaging Associates, Inc. Clinical guidelines Original Date: October 2015 LUMBAR SPINAL FUSION FOR Page 1 of 9 INSTABILITY AND DEGENERATIVE DISC CONDITIONS FOR CMS (MEDICARE) MEMBERS ONLY CPT4
Common neuromusculoskeletal disorders in the workplace W. Shane Journeay, PhD, MD, MPH, FRCPC, BC-OEM
 Common neuromusculoskeletal disorders in the workplace W. Shane Journeay, PhD, MD, MPH, FRCPC, BC-OEM OEMAC Calgary September 23, 2018 OBJECTIVES 1. To name key diagnoses of neuromusculoskeletal conditions
Common neuromusculoskeletal disorders in the workplace W. Shane Journeay, PhD, MD, MPH, FRCPC, BC-OEM OEMAC Calgary September 23, 2018 OBJECTIVES 1. To name key diagnoses of neuromusculoskeletal conditions
Velez v Wys 2017 NY Slip Op 30766(U) March 29, 2017 Supreme Court, Bronx County Docket Number: /2013 Judge: Howard H. Sherman Cases posted with
 March 29, 2017 Supreme Court, Bronx County Docket Number: /2013 Judge: Howard H. Sherman Cases posted with") Velez v Wys 2017 NY Slip Op 30766(U) March 29, 2017 Supreme Court, Bronx County Docket Number: 304278/2013 Judge: Howard H. Sherman Cases posted with a "30000" identifier, i.e., 2013 NY Slip Op 30001(U),
Velez v Wys 2017 NY Slip Op 30766(U) March 29, 2017 Supreme Court, Bronx County Docket Number: 304278/2013 Judge: Howard H. Sherman Cases posted with a "30000" identifier, i.e., 2013 NY Slip Op 30001(U),
Gillian Wooldridge, DO Houston Methodist Willowbrook Hospital Primary Care Sports Medicine Fellowship May 3, 2018
 Gillian Wooldridge, DO Houston Methodist Willowbrook Hospital Primary Care Sports Medicine Fellowship May 3, 2018 Disclosures Neither I nor any family members have financial disclosures Special thanks
Gillian Wooldridge, DO Houston Methodist Willowbrook Hospital Primary Care Sports Medicine Fellowship May 3, 2018 Disclosures Neither I nor any family members have financial disclosures Special thanks
BEFORE THE ARKANSAS WORKERS' COMPENSATION COMMISSION CLAIM NO. F ROSA CORTEZ CLAIMANT BRIGHTON HOUSE CARE CENTER OPINION FILED MAY 28, 2004
 BEFORE THE ARKANSAS WORKERS' COMPENSATION COMMISSION CLAIM NO. F309834 ROSA CORTEZ CLAIMANT BRIGHTON HOUSE CARE CENTER ARKANSAS SELF INSURED INSURANCE CARRIER RESPONDENT RESPONDENT OPINION FILED MAY 28,
BEFORE THE ARKANSAS WORKERS' COMPENSATION COMMISSION CLAIM NO. F309834 ROSA CORTEZ CLAIMANT BRIGHTON HOUSE CARE CENTER ARKANSAS SELF INSURED INSURANCE CARRIER RESPONDENT RESPONDENT OPINION FILED MAY 28,
Stand-Alone Technology. Reginald Davis, M.D., FAANS, FACS Director of Clinical Research
 Stand-Alone Technology Reginald Davis, M.D., FAANS, FACS Director of Clinical Research Disclosures Stand-Alone Devices Optio-C Stalif C Coalition Prevail ROI-C Technology Descriptions Optio-C A no profile,
Stand-Alone Technology Reginald Davis, M.D., FAANS, FACS Director of Clinical Research Disclosures Stand-Alone Devices Optio-C Stalif C Coalition Prevail ROI-C Technology Descriptions Optio-C A no profile,
LUMBAR SPINE CASE 3. Property of VOMPTI, LLC. For Use of Participants Only. No Use or Reproduction Without Consent 1. L4-5, 5-S1 disc, facet (somatic)
") LUMBAR SPINE CASE 3 A.J. Lievre, PT, DPT, OCS, CMPT Aaron Hartstein, PT, DPT, OCS, FAAOMPT Orthopaedic Manual Physical Therapy Series Richmond 2018-2019 L4-5, 5-S1 disc, facet (somatic) L5/S1 Radiculopathy
LUMBAR SPINE CASE 3 A.J. Lievre, PT, DPT, OCS, CMPT Aaron Hartstein, PT, DPT, OCS, FAAOMPT Orthopaedic Manual Physical Therapy Series Richmond 2018-2019 L4-5, 5-S1 disc, facet (somatic) L5/S1 Radiculopathy
WORKPLACE SAFETY AND INSURANCE APPEALS TRIBUNAL DECISION NO. 346/14
 WORKPLACE SAFETY AND INSURANCE APPEALS TRIBUNAL DECISION NO. 346/14 BEFORE: J.E. Smith: Vice-Chair HEARING: February 25, 2014 at Toronto Written DATE OF DECISION: March 13, 2014 NEUTRAL CITATION: 2014
WORKPLACE SAFETY AND INSURANCE APPEALS TRIBUNAL DECISION NO. 346/14 BEFORE: J.E. Smith: Vice-Chair HEARING: February 25, 2014 at Toronto Written DATE OF DECISION: March 13, 2014 NEUTRAL CITATION: 2014
A.J. Lievre, PT, DPT, OCS, CMPT Aaron Hartstein, PT, DPT, OCS, FAAOMPT
 LUMBAR SPINE CASE #3 A.J. Lievre, PT, DPT, OCS, CMPT Aaron Hartstein, PT, DPT, OCS, FAAOMPT Orthopaedic Manual Physical Therapy Series Charlottesville 2017-2018 L4-5, 5-S1 disc, facet (somatic) L5/S1 Radiculopathy
LUMBAR SPINE CASE #3 A.J. Lievre, PT, DPT, OCS, CMPT Aaron Hartstein, PT, DPT, OCS, FAAOMPT Orthopaedic Manual Physical Therapy Series Charlottesville 2017-2018 L4-5, 5-S1 disc, facet (somatic) L5/S1 Radiculopathy
Lumbar Disc Herniation with Radiculopathy treated successfully with Cox Technic. presented by Dr. Steven J. Garber
 Lumbar Disc Herniation with Radiculopathy treated successfully with Cox Technic presented by Dr. Steven J. Garber 2011 Part III Cox Certification Seminar The Gaylord Opryland Hotel Nashville TN 1 Patient
Lumbar Disc Herniation with Radiculopathy treated successfully with Cox Technic presented by Dr. Steven J. Garber 2011 Part III Cox Certification Seminar The Gaylord Opryland Hotel Nashville TN 1 Patient
Diagnosis of Neck & Upper Extremity Pain
 Diagnosis of Neck & Upper Extremity Pain David B. Bumpass, MD Assistant Professor, Spine Surgery UAMS Depts. of Orthopaedic Surgery & Neurosurgery May 12, 2018 Disclosures Medtronic Spine speaking fees
Diagnosis of Neck & Upper Extremity Pain David B. Bumpass, MD Assistant Professor, Spine Surgery UAMS Depts. of Orthopaedic Surgery & Neurosurgery May 12, 2018 Disclosures Medtronic Spine speaking fees
Restraints to Movement... 4 Restraints to flexion... 4 Primary restraint into Extension... 4
 CERVICAL SPINE... 4 Neck Pain Categories... 4 Kinematics... Error! Bookmark not defined. Ranges of Motion C2-7... 4 Coupled Movements... 4 Ranges of Motion C0-2... 4 Coupled Movements... 4 Restraints to
CERVICAL SPINE... 4 Neck Pain Categories... 4 Kinematics... Error! Bookmark not defined. Ranges of Motion C2-7... 4 Coupled Movements... 4 Ranges of Motion C0-2... 4 Coupled Movements... 4 Restraints to
SpineFAQs. Neck Pain Diagnosis and Treatment
 SpineFAQs Neck Pain Diagnosis and Treatment Neck pain is a common reason people visit their doctor. Neck pain typically doesn't start from a single injury. Instead, the problem usually develops over time
SpineFAQs Neck Pain Diagnosis and Treatment Neck pain is a common reason people visit their doctor. Neck pain typically doesn't start from a single injury. Instead, the problem usually develops over time
Chapter 2 Diagnostic Algorithms. 4 Traumatic Neck Pain Algorithm
 Chapter 2 Diagnostic Algorithms 4 Traumatic Neck Pain Algorithm Patient presents with a traumatic onset of neck pain. In general, radiographs should be ordered with a history of recent, significant trauma.
Chapter 2 Diagnostic Algorithms 4 Traumatic Neck Pain Algorithm Patient presents with a traumatic onset of neck pain. In general, radiographs should be ordered with a history of recent, significant trauma.
MORE FOR BACKS PROGRAM. User guide for chiropractors and chiropractic code list (ICD-10-AM codes)
") MORE FOR BACKS PROGRAM User guide for chiropractors and chiropractic code list (ICD-10-AM codes) APRIL 2017 WELCOME TO THE MORE FOR BACKS PROGRAM This program reimburses 100% of the agreed charge for an
MORE FOR BACKS PROGRAM User guide for chiropractors and chiropractic code list (ICD-10-AM codes) APRIL 2017 WELCOME TO THE MORE FOR BACKS PROGRAM This program reimburses 100% of the agreed charge for an
IAIABC 2003 Upper Extremity Impairment Guides Part 3 of the Supplemental Impairment Rating Guides
 IAIABC 2003 Upper Extremity Impairment Guides Part 3 of the Supplemental Impairment Rating Guides Draft 11-03 IAIABC Executive Office 5610 Medical Circle, Suite 14 Madison, WI 53719 Phone: (608) 663-6355
IAIABC 2003 Upper Extremity Impairment Guides Part 3 of the Supplemental Impairment Rating Guides Draft 11-03 IAIABC Executive Office 5610 Medical Circle, Suite 14 Madison, WI 53719 Phone: (608) 663-6355
WORKPLACE SAFETY AND INSURANCE APPEALS TRIBUNAL DECISION NO. 584/08
 WORKPLACE SAFETY AND INSURANCE APPEALS TRIBUNAL DECISION NO. 584/08 BEFORE: R. McClellan : Vice-Chair HEARING: March 7, 2008 at Toronto Written No Post hearing activity DATE OF DECISION: March 12, 2008
WORKPLACE SAFETY AND INSURANCE APPEALS TRIBUNAL DECISION NO. 584/08 BEFORE: R. McClellan : Vice-Chair HEARING: March 7, 2008 at Toronto Written No Post hearing activity DATE OF DECISION: March 12, 2008
Patient Information MIS LLIF. Lateral Lumbar Interbody Fusion Using Minimally Invasive Surgical Techniques
 Patient Information MIS LLIF Lateral Lumbar Interbody Fusion Using Minimally Invasive Surgical Techniques Table of Contents Anatomy of Spine....2 General Conditions of the Spine....4 What is Spondylolisthesis....5
Patient Information MIS LLIF Lateral Lumbar Interbody Fusion Using Minimally Invasive Surgical Techniques Table of Contents Anatomy of Spine....2 General Conditions of the Spine....4 What is Spondylolisthesis....5
Spinal canal stenosis Degenerative diseases F 06
 What is spinal canal stenosis? The condition known as spinal canal stenosis is a narrowing (stenosis) of the spinal canal that in most cases develops due to the degenerative (wear-induced) deformation
What is spinal canal stenosis? The condition known as spinal canal stenosis is a narrowing (stenosis) of the spinal canal that in most cases develops due to the degenerative (wear-induced) deformation
Thoracic Spine Applied Anatomy. Jason Zafereo, PT, OCS, FAAOMPT
 Thoracic Spine Applied Anatomy Jason Zafereo, PT, OCS, FAAOMPT Clinical i l Orthopedic Rehabilitation ti Education Objectives Discuss concepts relevant to thoracic pain of red flag origin Discuss concepts
Thoracic Spine Applied Anatomy Jason Zafereo, PT, OCS, FAAOMPT Clinical i l Orthopedic Rehabilitation ti Education Objectives Discuss concepts relevant to thoracic pain of red flag origin Discuss concepts
Cox Technic Case Report #124 published at ( sent October 2013 ) 1
 1") Cox Technic Case Report #124 published at www.coxtechnic.com ( sent October 2013 ) 1 5 th Lumbar Disc Herniation with Spondylolisthesis Treated with Cox Technic Flexion Distraction by Travis Cross BS,
Cox Technic Case Report #124 published at www.coxtechnic.com ( sent October 2013 ) 1 5 th Lumbar Disc Herniation with Spondylolisthesis Treated with Cox Technic Flexion Distraction by Travis Cross BS,
Diagnostic Imaging Exams
 Guide for Chiropractors Diagnostic Imaging Exams CREATED FOR OUR CHIROPRACTIC PARTNERS This document has been prepared by the specialized, board-certified radiologists who interpret patient exams for Center
Guide for Chiropractors Diagnostic Imaging Exams CREATED FOR OUR CHIROPRACTIC PARTNERS This document has been prepared by the specialized, board-certified radiologists who interpret patient exams for Center
MORE FOR BACKS PROGRAM. User guide for chiropractors and chiropractic code list (ICD-10-AM codes)
") MORE FOR BACKS PROGRAM User guide for chiropractors and chiropractic code list (ICD-10-AM codes) MAY 2018 WELCOME TO THE MORE FOR BACKS PROGRAM This program reimburses 100% of the agreed charge for an
MORE FOR BACKS PROGRAM User guide for chiropractors and chiropractic code list (ICD-10-AM codes) MAY 2018 WELCOME TO THE MORE FOR BACKS PROGRAM This program reimburses 100% of the agreed charge for an
Common fracture & dislocation of the cervical spine. Theerachai Apivatthakakul Department of Orthopaedic Chiangmai University
 Common fracture & dislocation of the cervical spine Theerachai Apivatthakakul Department of Orthopaedic Chiangmai University Objective Anatomy Mechanism and type of injury PE.and radiographic evaluation
Common fracture & dislocation of the cervical spine Theerachai Apivatthakakul Department of Orthopaedic Chiangmai University Objective Anatomy Mechanism and type of injury PE.and radiographic evaluation
Outline. Introduction / Epidemiology. Anatomy / Pain generators. Diagnosis. Treatment. Most Important lecture!!
 Acute Low Back Pain Outline Introduction / Epidemiology. Most Important lecture!! Anatomy / Pain generators Diagnosis Treatment Course Objectives Know the RED FLAGS in history taking. Know the Pain Generators
Acute Low Back Pain Outline Introduction / Epidemiology. Most Important lecture!! Anatomy / Pain generators Diagnosis Treatment Course Objectives Know the RED FLAGS in history taking. Know the Pain Generators
POSTERIOR CERVICAL FUSION
 AN INTRODUCTION TO PCF POSTERIOR CERVICAL FUSION This booklet provides general information on the Posterior Cervical Fusion (PCF) surgical procedure for you to discuss with your physician. It is not meant
AN INTRODUCTION TO PCF POSTERIOR CERVICAL FUSION This booklet provides general information on the Posterior Cervical Fusion (PCF) surgical procedure for you to discuss with your physician. It is not meant
Epidemiology of Low back pain
 Low Back Pain Definition Pain felt in your lower back may come from the spine, muscles, nerves, or other structures in that region. It may also radiate from other areas like the mid or upper back, a inguinal
Low Back Pain Definition Pain felt in your lower back may come from the spine, muscles, nerves, or other structures in that region. It may also radiate from other areas like the mid or upper back, a inguinal
WORKPLACE SAFETY AND INSURANCE APPEALS TRIBUNAL DECISION NO. 111/07
 WORKPLACE SAFETY AND INSURANCE APPEALS TRIBUNAL DECISION NO. 111/07 BEFORE: S. Ryan: Vice-Chair HEARING: January 15, 2007 at Toronto Written DATE OF DECISION: January 17, 2007 NEUTRAL CITATION: 2007 ONWSIAT
WORKPLACE SAFETY AND INSURANCE APPEALS TRIBUNAL DECISION NO. 111/07 BEFORE: S. Ryan: Vice-Chair HEARING: January 15, 2007 at Toronto Written DATE OF DECISION: January 17, 2007 NEUTRAL CITATION: 2007 ONWSIAT
Spinal Fusion. North American Spine Society Public Education Series
 Spinal Fusion North American Spine Society Public Education Series What Is Spinal Fusion? The spine is made up of a series of bones called vertebrae ; between each vertebra are strong connective tissues
Spinal Fusion North American Spine Society Public Education Series What Is Spinal Fusion? The spine is made up of a series of bones called vertebrae ; between each vertebra are strong connective tissues
National Imaging Associates, Inc. Clinical guidelines CHIROPRACTIC SERVICES. Original Date: Page 1 of FOR CMS (MEDICARE) MEMBERS ONLY
 MEMBERS ONLY") National Imaging Associates, Inc. Clinical guidelines CHIROPRACTIC SERVICES CPT4 Codes: Please refer to pages 2-10 LCD ID Number: L35424 Novitas: J-H: DC, DE, MD, NJ, PA J-L: AR, CO, LA, MS, NM, OK, TX
National Imaging Associates, Inc. Clinical guidelines CHIROPRACTIC SERVICES CPT4 Codes: Please refer to pages 2-10 LCD ID Number: L35424 Novitas: J-H: DC, DE, MD, NJ, PA J-L: AR, CO, LA, MS, NM, OK, TX
Anatomy of the Musculoskeletal System
 Anatomy of the Musculoskeletal System Kyle E. Rarey, Ph.D. Department of Anatomy & Cell Biology and Otolaryngology University of Florida College of Medicine Outline of Presentation Vertebral Column Upper
Anatomy of the Musculoskeletal System Kyle E. Rarey, Ph.D. Department of Anatomy & Cell Biology and Otolaryngology University of Florida College of Medicine Outline of Presentation Vertebral Column Upper
3/3/2016. International Standards for the Neurologic Classification of Spinal Cord Injury (ISNCSCI)
") International Standards for the Neurologic Classification of Spinal Cord Injury (ISNCSCI) American Spinal Injury Association International Spinal Cord Society Presented by Adam Stein, MD Chairman and Professor
International Standards for the Neurologic Classification of Spinal Cord Injury (ISNCSCI) American Spinal Injury Association International Spinal Cord Society Presented by Adam Stein, MD Chairman and Professor
L5 S1 Extruded Disc Relieved with Cox Technic Decompression Spinal Adjusting
 1 L5 S1 Extruded Disc Relieved with Cox Technic Decompression Spinal Adjusting submitted by Joseph d'angiolillo DC 11 Clyde Road, Suite 103 Somerset, NJ 08873 (732) 873 2222 This is a case study of a patient
1 L5 S1 Extruded Disc Relieved with Cox Technic Decompression Spinal Adjusting submitted by Joseph d'angiolillo DC 11 Clyde Road, Suite 103 Somerset, NJ 08873 (732) 873 2222 This is a case study of a patient
Chapter 32. Objectives. Objectives 01/09/2013. Spinal Column and Spinal Cord Trauma
 Chapter 32 Spinal Column and Spinal Cord Trauma Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1.
Chapter 32 Spinal Column and Spinal Cord Trauma Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1.
How to Determine the Severity of a Spinal Sprain Outline
 Spinal Trauma How to Determine the Severity of a Spinal Sprain Outline Instructor: Dr. Jeffrey A. Cronk, DC, CICE Director of Education, Spinal Kinetics. CICE, American Board of Independent Medical Examiners.
Spinal Trauma How to Determine the Severity of a Spinal Sprain Outline Instructor: Dr. Jeffrey A. Cronk, DC, CICE Director of Education, Spinal Kinetics. CICE, American Board of Independent Medical Examiners.
Am I eligible for the TOPS study? Possibly, if you suffer from one or more of the following conditions:
 Am I eligible for the TOPS study? Possibly, if you suffer from one or more of the following conditions: Radiating leg pain Greater leg / buttock pain than back pain Severe pain sets in when walking as
Am I eligible for the TOPS study? Possibly, if you suffer from one or more of the following conditions: Radiating leg pain Greater leg / buttock pain than back pain Severe pain sets in when walking as
CERVICAL SPINE TIPS A
 CERVICAL SPINE TIPS A Musculoskeletal Approach to managing Neck Pain An ALGORITHM, as a management guide Rick Bernau & Ian Wallbridge June 2010 THE PROCESS An interactive approach to the management of
CERVICAL SPINE TIPS A Musculoskeletal Approach to managing Neck Pain An ALGORITHM, as a management guide Rick Bernau & Ian Wallbridge June 2010 THE PROCESS An interactive approach to the management of
CERVICAL SPINE EVALUATION MARK FIGUEROA PHYSICAL THERAPIST
 CERVICAL SPINE EVALUATION MARK FIGUEROA PHYSICAL THERAPIST OVERVIEW OF CLINICAL REASONING Stage of disorder Pathoanatomical diagnosis Signs and symptoms Consideration of the evidence gathered Common sense
CERVICAL SPINE EVALUATION MARK FIGUEROA PHYSICAL THERAPIST OVERVIEW OF CLINICAL REASONING Stage of disorder Pathoanatomical diagnosis Signs and symptoms Consideration of the evidence gathered Common sense
Medicare Regulations for Chiropractors. Presented by Clinic Pro Software Inc. Marilyn K. Gard. CEO, MBA
 Medicare Regulations for Chiropractors Presented by Clinic Pro Software Inc. Marilyn K. Gard. CEO, MBA Use AT modifier which means active treatment. Claims submitted for Chiropractic manipulative treatment
Medicare Regulations for Chiropractors Presented by Clinic Pro Software Inc. Marilyn K. Gard. CEO, MBA Use AT modifier which means active treatment. Claims submitted for Chiropractic manipulative treatment
STRUCTURAL BASIS OF MEDICAL PRACTICE EXAMINATION 5. September 30, 2011
 STRUCTURAL BASIS OF MEDICAL PRACTICE EXAMINATION 5 September 30, 2011 PART l. Answer in the space provided. (12 pts) 1. Identify the structures. (2 pts) EXAM NUMBER A. Suprascapular nerve B. Axillary nerve
STRUCTURAL BASIS OF MEDICAL PRACTICE EXAMINATION 5 September 30, 2011 PART l. Answer in the space provided. (12 pts) 1. Identify the structures. (2 pts) EXAM NUMBER A. Suprascapular nerve B. Axillary nerve
Patient Information ACDF. Anterior Cervical Discectomy and Fusion
 Patient Information ACDF Anterior Cervical Discectomy and Fusion Table of Contents Anatomy of the Spine...2-3 General Conditions of the Cervical Spine...4 5 What is an ACDF?...6 How is an ACDF performed?...7
Patient Information ACDF Anterior Cervical Discectomy and Fusion Table of Contents Anatomy of the Spine...2-3 General Conditions of the Cervical Spine...4 5 What is an ACDF?...6 How is an ACDF performed?...7
WORKPLACE SAFETY AND INSURANCE APPEALS TRIBUNAL DECISION NO. 1144/15
 WORKPLACE SAFETY AND INSURANCE APPEALS TRIBUNAL DECISION NO. 1144/15 BEFORE: N. Perryman: Vice-Chair HEARING: May 20, 2015 at Toronto Written DATE OF DECISION: June 29, 2015 NEUTRAL CITATION: 2015 ONWSIAT
WORKPLACE SAFETY AND INSURANCE APPEALS TRIBUNAL DECISION NO. 1144/15 BEFORE: N. Perryman: Vice-Chair HEARING: May 20, 2015 at Toronto Written DATE OF DECISION: June 29, 2015 NEUTRAL CITATION: 2015 ONWSIAT
ICD Months In Are You Doing it Right?
 ICD-10--3 Months In Are You Doing it Right? Presented by: Kathy Mills Chang, MCS-P, CCPC What Now? Most commonly asked questions Based on hundreds of questions to the Help Desk and at seminars Proactively
ICD-10--3 Months In Are You Doing it Right? Presented by: Kathy Mills Chang, MCS-P, CCPC What Now? Most commonly asked questions Based on hundreds of questions to the Help Desk and at seminars Proactively
WORKPLACE SAFETY AND INSURANCE APPEALS TRIBUNAL DECISION NO. 2307/06
 WORKPLACE SAFETY AND INSURANCE APPEALS TRIBUNAL DECISION NO. 2307/06 BEFORE: J.P. Moore : Vice-Chair HEARING: November 14, 2006 at Thunder Bay Oral Post-hearing activity completed on March 9, 2007 DATE
WORKPLACE SAFETY AND INSURANCE APPEALS TRIBUNAL DECISION NO. 2307/06 BEFORE: J.P. Moore : Vice-Chair HEARING: November 14, 2006 at Thunder Bay Oral Post-hearing activity completed on March 9, 2007 DATE
DR. X MEDICAL GROUP BROOKSHIRE AVENUE, SUITE 111 DOWNEY, CALIFORNIA (562) FAX: (562)
 FAX: (562)") DR. X MEDICAL GROUP 11111 BROOKSHIRE AVENUE, SUITE 111 DOWNEY, CALIFORNIA 90241 (562) 904-7345 FAX: (562) 904.7345 December 6, 2011 Ally McBeal, Esquire Forever insurance 10000 Hollywood Blvd, Suite 100
DR. X MEDICAL GROUP 11111 BROOKSHIRE AVENUE, SUITE 111 DOWNEY, CALIFORNIA 90241 (562) 904-7345 FAX: (562) 904.7345 December 6, 2011 Ally McBeal, Esquire Forever insurance 10000 Hollywood Blvd, Suite 100
Patient Information MIS TLIF. Transforaminal Lumbar Interbody Fusion Using Minimally Invasive Surgical Techniques
 Patient Information MIS TLIF Transforaminal Lumbar Interbody Fusion Using Minimally Invasive Surgical Techniques MIS TLIF Table of Contents Anatomy of Spine...2 General Conditions of the Spine...4 6 MIS-TLIF
Patient Information MIS TLIF Transforaminal Lumbar Interbody Fusion Using Minimally Invasive Surgical Techniques MIS TLIF Table of Contents Anatomy of Spine...2 General Conditions of the Spine...4 6 MIS-TLIF
Copyright 2017 Dr. David Hendrickson Discover Life Chiroprac c 5015 Tacoma Mall Blvd Ste E102 Tacoma, WA Phone #: (253)
") Copyright 2017 Dr. David Hendrickson Discover Life Chiroprac c 5015 Tacoma Mall Blvd Ste E102 Tacoma, WA 98409 Phone #: (253) 472 4400 www.discoverlifechiro.com Chiropractic and Sciatica Sciatica is a
Copyright 2017 Dr. David Hendrickson Discover Life Chiroprac c 5015 Tacoma Mall Blvd Ste E102 Tacoma, WA 98409 Phone #: (253) 472 4400 www.discoverlifechiro.com Chiropractic and Sciatica Sciatica is a
PARADIGM SPINE. Patient Information. Treatment of a Narrow Lumbar Spinal Canal
 PARADIGM SPINE Patient Information Treatment of a Narrow Lumbar Spinal Canal Dear Patient, This brochure is intended to inform you of a possible treatment option for narrowing of the spinal canal, often
PARADIGM SPINE Patient Information Treatment of a Narrow Lumbar Spinal Canal Dear Patient, This brochure is intended to inform you of a possible treatment option for narrowing of the spinal canal, often
Spine Pain Management Program
 Spine Pain Management Program Please complete the following information: Patient Name: Patient ID Number: Patient DOB: The procedure being requested is: Please check the indication (reason) for this procedure
Spine Pain Management Program Please complete the following information: Patient Name: Patient ID Number: Patient DOB: The procedure being requested is: Please check the indication (reason) for this procedure
Documentation for Chiropractic Evaluations (DeskBook Chapter 4.2)
") Documentation for Chiropractic Evaluations (DeskBook Chapter 4.2) Presented by Evan M. Gwilliam, DC MBA BS CPC CCPC QCC CPC-I MCS-P CPMA CMHP Vice President 1 Dr. Evan Gwilliam Education Bachelor s of
Documentation for Chiropractic Evaluations (DeskBook Chapter 4.2) Presented by Evan M. Gwilliam, DC MBA BS CPC CCPC QCC CPC-I MCS-P CPMA CMHP Vice President 1 Dr. Evan Gwilliam Education Bachelor s of
Cox Technic Case Report #126 published at (sent December 2013 ) 1
 1") Cox Technic Case Report #126 published at www.coxtechnic.com (sent December 2013 ) 1 Cox Technic Decompression Spinal Manipulation Resolves Symptoms Associated with Disc Protrusion and S1 Radiculopathy,
Cox Technic Case Report #126 published at www.coxtechnic.com (sent December 2013 ) 1 Cox Technic Decompression Spinal Manipulation Resolves Symptoms Associated with Disc Protrusion and S1 Radiculopathy,
Cervical and Thoracic Spinal Conditions Chapter 11
 Cervical and Thoracic Spinal Conditions Chapter 11 Anatomy Spinal column Vertebrae Cervical (7) convex anteriorly Thoracic (12) concave anteriorly Lumbar (5) convex anteriorly Sacral (5 fused) concave
Cervical and Thoracic Spinal Conditions Chapter 11 Anatomy Spinal column Vertebrae Cervical (7) convex anteriorly Thoracic (12) concave anteriorly Lumbar (5) convex anteriorly Sacral (5 fused) concave
Spinal Column. Anatomy Of The Spine
 Anatomy Of The Spine The spine is a flexible column, composed of a stack of individual bones. Each bone is called a vertebra. There are seven vertebrae in the neck (cervical vertebrae) twelve in the thoracic
Anatomy Of The Spine The spine is a flexible column, composed of a stack of individual bones. Each bone is called a vertebra. There are seven vertebrae in the neck (cervical vertebrae) twelve in the thoracic
WORKPLACE SAFETY AND INSURANCE APPEALS TRIBUNAL DECISION NO. 1041/16
 WORKPLACE SAFETY AND INSURANCE APPEALS TRIBUNAL DECISION NO. 1041/16 BEFORE: K. Iima: Vice-Chair HEARING: April 20, 2016 at Toronto Written DATE OF DECISION: July 8, 2016 NEUTRAL CITATION: 2016 ONWSIAT
WORKPLACE SAFETY AND INSURANCE APPEALS TRIBUNAL DECISION NO. 1041/16 BEFORE: K. Iima: Vice-Chair HEARING: April 20, 2016 at Toronto Written DATE OF DECISION: July 8, 2016 NEUTRAL CITATION: 2016 ONWSIAT
Spine Pain Management Program
 Spine Pain Management Program Please complete the following information: Patient Name: Patient ID Number: Patient DOB: The procedure being requested: Epidural Injection Please check the indication (reason)
Spine Pain Management Program Please complete the following information: Patient Name: Patient ID Number: Patient DOB: The procedure being requested: Epidural Injection Please check the indication (reason)
Diagnostic and Treatment Approach to the Active Patient with Complex Spine Pathology
 Physical Therapy Diagnostic and Treatment Approach to the Active Patient with Complex Spine Pathology Scott Behjani, DPT, OCS Introduction Prevalence 1-year incidence of first-episode LBP ranges from
Physical Therapy Diagnostic and Treatment Approach to the Active Patient with Complex Spine Pathology Scott Behjani, DPT, OCS Introduction Prevalence 1-year incidence of first-episode LBP ranges from
FILED: RICHMOND COUNTY CLERK 01/17/ :45 PM INDEX NO /2015 NYSCEF DOC. NO. 65 RECEIVED NYSCEF: 01/17/2019
 BROOKLYN, N.Y. 11234 Kalant & Roytblat, PLLC January 3, 2019 9131 Queens Blyd., Ste. 313 Elmhurst, NY 11373 Attention: Alexander Roytblat, Esq. Re: Eran Taussi Date of Accident: January 30, 2014 Dear Mr.
BROOKLYN, N.Y. 11234 Kalant & Roytblat, PLLC January 3, 2019 9131 Queens Blyd., Ste. 313 Elmhurst, NY 11373 Attention: Alexander Roytblat, Esq. Re: Eran Taussi Date of Accident: January 30, 2014 Dear Mr.
Subaxial Cervical Spine Trauma Dr Hesarikia BUMS
 Subaxial Cervical Spine Trauma Dr. Hesarikia BUMS Subaxial Cervical Spine From C3-C7 ROM Majority of cervical flexion Lateral bending Approximately 50% rotation Ligamentous Anatomy Anterior ALL, PLL, intervertebral
Subaxial Cervical Spine Trauma Dr. Hesarikia BUMS Subaxial Cervical Spine From C3-C7 ROM Majority of cervical flexion Lateral bending Approximately 50% rotation Ligamentous Anatomy Anterior ALL, PLL, intervertebral
Low back dural tension
 Low back dural tension The Borg System is 100 % Low back dural tension Call 1.800.430.5485 or Email: slipgriproducts@earthlink.net Low back dural tension. Number: 0016. Policy. Aetna considers any of the
Low back dural tension The Borg System is 100 % Low back dural tension Call 1.800.430.5485 or Email: slipgriproducts@earthlink.net Low back dural tension. Number: 0016. Policy. Aetna considers any of the
Francine M. Pulver, MD, Clinical Assistant Professor Department of Physical Medicine & Rehabilitation Ohio State University Medical Center
 Oh My Aching Back! Francine M. Pulver, MD, Clinical Assistant Professor Department of Physical Medicine & Rehabilitation Ohio State University Medical Center Epidemiology 90% of episodes of LBP resolves
Oh My Aching Back! Francine M. Pulver, MD, Clinical Assistant Professor Department of Physical Medicine & Rehabilitation Ohio State University Medical Center Epidemiology 90% of episodes of LBP resolves
18 The Independent Orthopaedic Medical Examination
 18 The Independent Orthopaedic Medical Examination Noubar Didizian, M.D. and Samuel D. Hodge, Jr., Esq. INTRODUCTION Orthopaedic surgery is that discipline of medicine that deals with the musculoskeletal
18 The Independent Orthopaedic Medical Examination Noubar Didizian, M.D. and Samuel D. Hodge, Jr., Esq. INTRODUCTION Orthopaedic surgery is that discipline of medicine that deals with the musculoskeletal
Apportionment. APPORTIONMENT Page 1 of 5. Adopted: 1/10
 WSCC Clinics Protocol Adopted: 1/10 Apportionment Apportionment can have a variety of meanings in a variety of settings. For the purpose of this protocol, apportionment will apply to a process performed
WSCC Clinics Protocol Adopted: 1/10 Apportionment Apportionment can have a variety of meanings in a variety of settings. For the purpose of this protocol, apportionment will apply to a process performed
Mechanism of Injury, Trauma, Subluxation and Instability Outline
 Spinal Trauma Instructor: Dr. Jeffrey A. Cronk, DC, CICE Director of Education, Spinal Kinetics. CICE, American Board of Independent Medical Examiners. Mechanism of Injury is just something that you must
Spinal Trauma Instructor: Dr. Jeffrey A. Cronk, DC, CICE Director of Education, Spinal Kinetics. CICE, American Board of Independent Medical Examiners. Mechanism of Injury is just something that you must
Alan H Daniels, MD. Spine Division, Department of Orthopaedics Warren Alpert School of Medicine of Brown University
 Spinal and Orthopaedic Surgery in the Elderly Alan H Daniels, MD Spine Division, Department of Orthopaedics Warren Alpert School of Medicine of Brown University As the population ages, and patients remain
Spinal and Orthopaedic Surgery in the Elderly Alan H Daniels, MD Spine Division, Department of Orthopaedics Warren Alpert School of Medicine of Brown University As the population ages, and patients remain
Ultimate Spinal Analysis PA USA-XRAY ( )
") Page: 1 Spine Atlas Angle 7.24 S Atlas Angle 21.67 S The Atlas Angle is a measurement of the stability of the Atlas. The Atlas Plane Line is compared to true horizontal. Any increase or decrease of this
Page: 1 Spine Atlas Angle 7.24 S Atlas Angle 21.67 S The Atlas Angle is a measurement of the stability of the Atlas. The Atlas Plane Line is compared to true horizontal. Any increase or decrease of this
DEGENERATIVE SPINAL DISEASE PRABIN SHRESTHA ANISH M SINGH B&B HOSPITAL
 SPINAL CHAPTER, NESON DEGENERATIVE SPINAL DISEASE PRABIN SHRESTHA ANISH M SINGH B&B HOSPITAL INTRODUCTION DEGENERATIVE SPINAL DISEASE Gradual loss of normal structure and function of spine with time Also
SPINAL CHAPTER, NESON DEGENERATIVE SPINAL DISEASE PRABIN SHRESTHA ANISH M SINGH B&B HOSPITAL INTRODUCTION DEGENERATIVE SPINAL DISEASE Gradual loss of normal structure and function of spine with time Also
Regional Pain Syndromes: Neck and Low Back
 Regional Pain Syndromes: Neck and Low Back Srinivas Nalamachu, MD Disclosures Consultant/Independent Contractor/Honoraria: Ferring 1 Learning Objectives Identify the most common painful conditions in the
Regional Pain Syndromes: Neck and Low Back Srinivas Nalamachu, MD Disclosures Consultant/Independent Contractor/Honoraria: Ferring 1 Learning Objectives Identify the most common painful conditions in the
Patient Information MIS TLIF. Transforaminal Lumbar Interbody Fusion Using Minimally Invasive Surgical Techniques
 Patient Information MIS TLIF Transforaminal Lumbar Interbody Fusion Using Minimally Invasive Surgical Techniques MIS TLIF Table of Contents Anatomy of Spine..............................................
Patient Information MIS TLIF Transforaminal Lumbar Interbody Fusion Using Minimally Invasive Surgical Techniques MIS TLIF Table of Contents Anatomy of Spine..............................................
Gary Rea MD PhD Medical Director OSU Comprehensive Spine Center
 Gary Rea MD PhD Medical Director OSU Comprehensive Spine Center 1. The less specific the patient is about symptoms and pain, the less likely a specific diagnosis will be made and the less likely the patient
Gary Rea MD PhD Medical Director OSU Comprehensive Spine Center 1. The less specific the patient is about symptoms and pain, the less likely a specific diagnosis will be made and the less likely the patient
THE LUMBAR SPINE (BACK)
") THE LUMBAR SPINE (BACK) At a glance Chronic back pain, especially in the area of the lumbar spine (lower back), is a widespread condition. It can be assumed that 75 % of all people have it sometimes or
THE LUMBAR SPINE (BACK) At a glance Chronic back pain, especially in the area of the lumbar spine (lower back), is a widespread condition. It can be assumed that 75 % of all people have it sometimes or
DOCTOR DISCUSSION GUIDE
 DOCTOR DISCUSSION GUIDE BE PREPARED For the best outcome from a visit with your doctor, it s important to be prepared. The more completely and clearly you describe the pain you re experiencing, the easier
DOCTOR DISCUSSION GUIDE BE PREPARED For the best outcome from a visit with your doctor, it s important to be prepared. The more completely and clearly you describe the pain you re experiencing, the easier