|
|
|
- Fay Cordelia Thornton
- 5 years ago
- Views:
Transcription

1 Acute anterior dislocation of the shoulder
2 Anatomy Stability: - ball & socket = compression in concavity effect Bone - big head small cup = unstable Menisci - labium = depth of cup by 20% Ligaments - glenohumeral & capsule Muscles - rotator cuff & biceps = holds ball in cup Primary Movers - Deltoid, Pec. major & Lat. Dorsy = subluxing forces Dynamic - proprioceptive feedback
3 Pathophysiology (Lazarus 1996) Chondro-labral defect causes a 65% reduction in stability in the direction of the defect Deficiency of the ant. inf. capsulolabral complex Fracture of ant. lip of glenoid = 15% Detachment of labarum/capsule = 15% Tear of glenohumeral ligaments = 54% Avulsion of subscapularis and ligs of humerus (HAGL) To prevent the persistence of the defect it needs to be repaired Arthroscopically Open
4 Acute Injury Something breaks or tears and therefore can be repaired. Repair is better than reconstruct Repair is easier than reconstruct Chronic Instability has additional plastic deformation of the capsule and glenohumeral ligaments therefore needs to be shortened Restoring the normal functional anatomy is impossible
5 Conservative Treatment Rowe JBJS, young patient with ant. dislocations 94% had recurrence if < 20 years old 62% had recurrence if < 30 years old 14% had recurrence if > 40 years old Burkhead & Rockwood (text book) 40 patients with acute dislocation & vigorous rehabilitation Only 16% had good or excellent result (1 in 6) Deny & Drew Injury, November % of all patients presenting with shoulder dislocation had previous dislocation in 1 year 43% in patients years had re-dislocations
6 Non operative treatment of shoulder dislocation in young athletes 1. Arciera J Arthroscopy, De Beardino J South Orthopaedic Ass, Haelen J Arch Orthopaedic Trauma Surgery, Hovelius J Orthopaedic Science, Wheeler J Arthroscopy, Kirkby J Arthroscopy, 1999 all over 80% recurrence rate Non operative treatment is unacceptable
7 Prospective Randomised Study Bottani etc. Military Personnel Medicine Vol 30 No First Time Acute Traumatic Shoulder Dislocation Stabilisation V s Non Operative: Follow up in 36 months 24 patients aged 18-26y. 14 Non Operative rehab immobilised 4 weeks 9 of 12 non operative had instability (75%) (6 open Bankart repair) 10 ASC Bankart repair with bioabsorbable tack <10 days 1 of 9 operated patients had instability (11%)
8 Chronic anterior instability Comparison of Arthroscopic & Open Stabilisation Sample Size Follow Up Recurrence ASC Open ASC Open ASC Open Steinbeck Field Cole Hayes etc Conclusion Arthroscopic repair for chronic instability is inferior to open repair? Due to plastic deformation
9 Arthroscopic Techniques for Primary Dislocations 1982 Johusa with staples 1987 Morgen & Badenstab transglenoid sutures 1991 Caspari -Cannulated bio-absorbable tacks 1993 Wolf & Snyder suture anchors = difficult 1989 Wheller - ASC staple 1993 Gohlke - Suture anchors 1994 Arciera - ASC transglenoid 1996 Speer - Bio-absorbable tack 1999 Wintzell - ASC lavage 2000 Introduction of a multitude of new gadgets & anchors
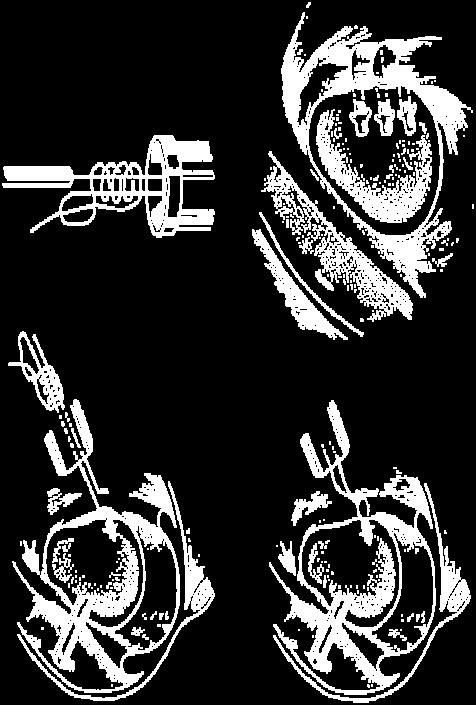
10 Arthroscopic Repairs, 1984 Knee Club Described Arthroscopic transglenoid sutures using: K wire with eye (ACL) introduced via anterior portal Sucking tube Sutures tied over infraspinatus fascia or spine of scapula Results 4 out 5 patients returned to the same level of sport with no re-dislocations

11 Arthroscopic Repair
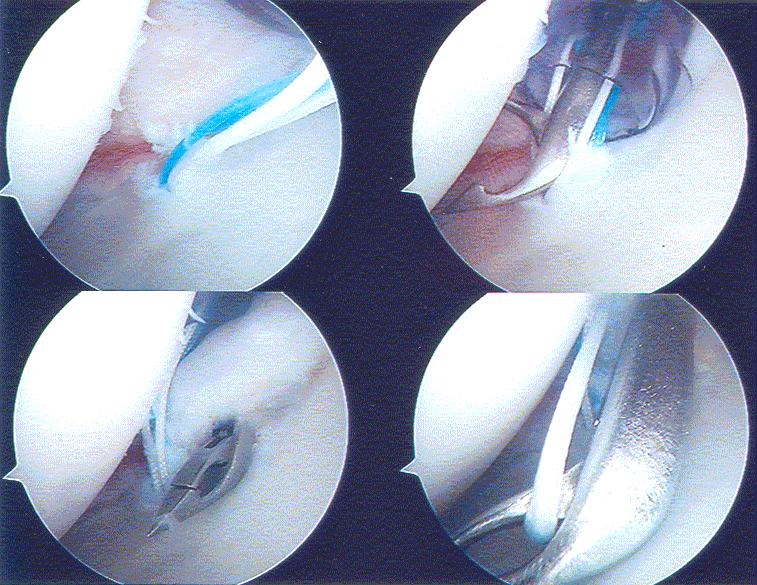
12
13
14 Boszotta & Helperstorfer Arthroscopy, July 2000 Transglenoid suture repair for initial Ant. dislocation 72 patients ( ) Aged % = Bankart lesion (6 with bone) 66% = Avulsion of capsulolabral complex Results 7% = Redislocation all due to trauma (severe in 2 out of 5) 85% = Returned to unrestricted pre injury sporting activities
15 Randomised Studies Asc. Stabilisation V s Non Operative Arciera et. al. A.J. Sports Med., military men with acute 1 st up dislocation, Average of 32 months follow up 15 patients non operative 80% redislocated 21 patients transglenoid suture 14% redislocated Bottony & Wilkings etc. A.J. Sports Medicine 2000 Patients with acute traumatic first time shoulder dislocation 14 young patients non op, 75% redislocation 10 young patients Asc. Bankart repair, 10% redislocation
16 Asc. stabilisation Dara & Gerber Journal of Shoulder & Elbow, shoulders Av 3 year follow up Recurrences occurred in patients who were chronic dislocators i.e. <30% Therefore now do open surgery for recurrent dislocations Asc. surgery for acute dislocations De Beardino et al An J. Sports Med., st up acute post traumatic Shoulders dislocation Average 37 months follow up Tack anchor. 6 Patients re-dislocated (13%) +4 had open surgery
17 Bozzotta & Helpastorger (Austria) J. Arthroscopy, 2000 Arthroscopic Transglenoid Suture Repair for Initial Ant. Shoulder Dislocation 72 Patients Sporting ambitious patients 25 Patients Bankart lesion (6 with bone) 43 Patients Capsulolabral avulsion Results 5 patients Re dislocated 2 had significant trauma 3 had insignificant trauma = 4% Therefore results of primary repair are better than surgery for recurrent dislocation But transgleniod repairs are obsolete
18 Against Arthroscopic Repair Roberts, Taylor, Brown, Hayes, Saies (Adelaide) Journal of Shoulder & Elbow, September acute 1 st up shoulder dislocations 2½ year post operative and return to Australian Rules Football Operations: Asc. suture repair 70% recurrence Asc. Bankart repair with tack 38% recurrence,.. Open repair & copsular shift 30% recurrence Therefore Asc. treatment alone not good enough
19 Cole & Warner Clinical Sports Medicine 2000 Arthroscopic V s Open Bankart Repair For Traumatic Anterior Shoulder Instability % Asc. treatment modalities are increasing due to: 1. Better understanding of the pathophysiology 2. Better pre operative evaluation of the injury (i.e. patient selection) 3. New surgical techniques 4. Better instrumentation 5. Better anchors
20 Protocol for Acute Repair 1. Mature & active person to 50 years old 3. First episode of glenohumeral dislocation Reduced on field, first aid, club Dr or DEM 4. Examination & X-ray 5. Informed consent time off work - outcome 6. Examination under GA 7. ASC of glenohumeral joint, check rotator cuff as well 8. Acute repair of all demonstrable tears or fractures restore normal anatomy 11. Rehab activity collar & cuff, physiotherapy 12. Avoid ext. rotation and abduction for 6 weeks 13. Return to contact sport in 12 weeks
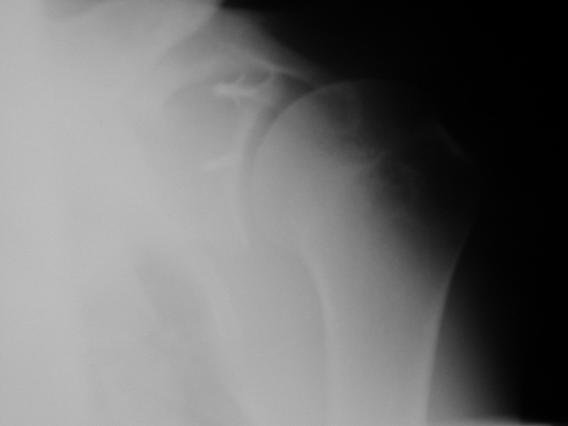
21 Investigations 1. Plain x-rays 2. CT scans if complicated associated feature 3. MRI rarely get more information from Asc. 4. Examination Under GA Supine load shift test with arm at 80 abducted compared with normal shoulder 1+ ball to rim 2+ ball riding over rim with spontaneous reduction 3+ ball stays dislocated 5. Arthroscopy
22 Arthroscopic Repair Procedure Patient Position General Anaesthetic Beach Chair with arm held by assistant Lateral position with arm in traction & shoulder abducted Shoulder examined, degree & direction of instability noted Portals = 2 or 3 Posterior portal Ant. sup portal Ant inf portal (occasionally) Injury assessed & debrided Repair method selected
23 Rehabilitation 1. Minimal in first 4 weeks No ext rotation Abduction less than 45 Pendulum exercises Isometric resistance exercises 2. Graduated in 4 8 weeks ROM Graduated weight training 3. Return to sport Non contact = 6 weeks contact = 12 weeks
24 Arthroscopic V s Open Bankart Repair Advantages Accurate diagnosis of all structures Less morbidity/pain Small scars Faster recovery Sooner return to activities Less restriction of movement Disadvantages Need all the equipment Technically demanding Long learning curve Lack of versatility Higher failure rate arthroscopic = up to 33% - open = less than 10%
25 Stern Jozrawi Rastolazzi Arthroscopy Oct Advantages V s Disadvantages of Asc. Repair Advantages cosmesis morbidity stiffness Easy revision Disadvantages 1) Reluctance to refer patient immediately 2) Difficult operation 3) Expensive instrumentation 4) Biological healing time is not accelerated 5) Same post operative restrictions
26 Problems 1. Difficulty convincing Club Trainers, Physicians, sporting club Doctors & DEM staff to refer the young athlete within 2-3 days. 2. Time consuming discussions convincing patient to have the operation rather than early return to sport. No problem advising a recurrent dislocators to have a stabilisation procedure at the end of a sporting season. 3. Mostly after hours surgery with staff who are not familiar with the operation and instrumentation.
27 Arthroscopy of Shoulder 1935 Japanese Surgeons arthroscoped, shoulders 1960s Curiosity activity in the western world 1970s Diagnostic Asc. examination open surgery 1980s Simple Asc. techniques for simple problems 1990s Instrumentation & tacks more tried it. 2000s Techniques & anchors Can be done by any surgeon skilled in arthroscopic techniques
28 Shoulder reduced on field, first aid room or DEM then referred 1970s s s - Treatment History Conservative for all 1 st up unless fractures with Bristows or Bankart repair for recurrences Asc. transglenoid sutures tied over spine of scapula or muscle fascia patient in lateral position with arm in traction or patient in Beach chair position multiple, tacks and sutures surtac screw tack anchors etc better anchors and sutures have made the procedure available for all surgeons experienced in arthroscopic technique

29 Acute Labral Tear

30 Acute Repair of Anterior Labral Tear
31 Conclusion Asc. repair of the Capsulo-ligamentous injury to the shoulder is a simple procedure for a surgeon skilled in arthroscopic technique Chronic instabilities have associated plastic deformity of the tissues that need to be addressed and this makes the result of a simple procedure unpredictable. An active young person with a first traumatic dislocation of the shoulder should have the damage repaired arthroscopically within 10 days of the injury
SHOULDER INSTABILITY
 SHOULDER INSTABILITY Dr.KN Subramanian M.Ch Orth., FRCS (Tr & Orth), CCT Orth(UK) Consultant Orthopaedic Surgeon, Special interest: Orthopaedic Sports Injury, Shoulder and Knee Surgery, SPARSH Hospital
SHOULDER INSTABILITY Dr.KN Subramanian M.Ch Orth., FRCS (Tr & Orth), CCT Orth(UK) Consultant Orthopaedic Surgeon, Special interest: Orthopaedic Sports Injury, Shoulder and Knee Surgery, SPARSH Hospital
Orthopaedic and Spine Institute 21 Spurs Lane, Suite 245, San Antonio, TX Tel#
 Orthopaedic and Spine Institute 21 Spurs Lane, Suite 245, San Antonio, TX 78240 www.saspine.com Tel# 210-487-7463 PATIENT GUIDE TO SHOULDER INSTABILITY LABRAL (BANKART) REPAIR / CAPSULAR SHIFT WHAT IS
Orthopaedic and Spine Institute 21 Spurs Lane, Suite 245, San Antonio, TX 78240 www.saspine.com Tel# 210-487-7463 PATIENT GUIDE TO SHOULDER INSTABILITY LABRAL (BANKART) REPAIR / CAPSULAR SHIFT WHAT IS
Patient ID. Case Conference. Physical Examination. Image examination. Treatment 2011/6/16
 Patient ID Case Conference R3 高逢駿 VS 徐郭堯 55 y/o female C.C.: recurrent right shoulder dislocation noted since falling down injury 2 years ago Came to ER because of dislocation for many times due to minor
Patient ID Case Conference R3 高逢駿 VS 徐郭堯 55 y/o female C.C.: recurrent right shoulder dislocation noted since falling down injury 2 years ago Came to ER because of dislocation for many times due to minor
The suction cup mechanism is enhanced by the slightly negative intra articular pressure within the joint.
 SHOULDER INSTABILITY Stability A. The stability of the shoulder is improved by depth of the glenoid. This is determined by: 1. Osseous glenoid, 2. Articular cartilage of the glenoid, which is thicker at
SHOULDER INSTABILITY Stability A. The stability of the shoulder is improved by depth of the glenoid. This is determined by: 1. Osseous glenoid, 2. Articular cartilage of the glenoid, which is thicker at
Recurrent Shoulder Dislocation.
 Recurrent Shoulder Dislocation www.fisiokinesiterapia.biz Anatomy of the Shoulder Shoulder Dislocations Case Study Rehabilitation Pick List Anatomy of the Shoulder Articulations Sternoclavicular Acromioclavicular
Recurrent Shoulder Dislocation www.fisiokinesiterapia.biz Anatomy of the Shoulder Shoulder Dislocations Case Study Rehabilitation Pick List Anatomy of the Shoulder Articulations Sternoclavicular Acromioclavicular
Shoulder Instability
 J F de Beer, K van Rooyen, D Bhatia Shoulder Instability INSTABILITY means that the shoulder dislocates completely (dislocation) or partially (subluxation). Anatomy The shoulder consists of a ball (humeral
J F de Beer, K van Rooyen, D Bhatia Shoulder Instability INSTABILITY means that the shoulder dislocates completely (dislocation) or partially (subluxation). Anatomy The shoulder consists of a ball (humeral
SHOULDER PROBLEMS & ARTHROSCOPIC MANAGEMENT
 SHOULDER PROBLEMS & ARTHROSCOPIC MANAGEMENT DR.SHEKHAR SRIVASTAV Sr. Consultant-KNEE & SHOULDER Arthroscopy Sant Parmanand Hospital,Delhi Peculiarities of Shoulder Elegant piece of machinery It has the
SHOULDER PROBLEMS & ARTHROSCOPIC MANAGEMENT DR.SHEKHAR SRIVASTAV Sr. Consultant-KNEE & SHOULDER Arthroscopy Sant Parmanand Hospital,Delhi Peculiarities of Shoulder Elegant piece of machinery It has the
SHOULDER INSTABILITY
 SHOULDER INSTABILITY Your shoulder is the most flexible joint in your body, allowing you to throw fastballs, lift a heavy suitcase, scratch your back, and reach in almost any direction. Your shoulder joint
SHOULDER INSTABILITY Your shoulder is the most flexible joint in your body, allowing you to throw fastballs, lift a heavy suitcase, scratch your back, and reach in almost any direction. Your shoulder joint
OBJECTIVES. Therapists Management of Shoulder Instability SHOULDER STABILITY SHOULDER STABILITY WHAT IS SHOULDER INSTABILITY? SHOULDER INSTABILITY
 Therapists Management of Shoulder Instability Brian G. Leggin, PT, DPT, OCS Lead Therapist, Penn Therapy and Fitness at Valley Forge Adjunct Assistant Professor, Department of Orthopaedics, University
Therapists Management of Shoulder Instability Brian G. Leggin, PT, DPT, OCS Lead Therapist, Penn Therapy and Fitness at Valley Forge Adjunct Assistant Professor, Department of Orthopaedics, University
My shoulder popped out what now?
 My shoulder popped out what now? Richard Dallalana Epworth Shoulder Symposium June 2017 Shoulder Dislocation First event Best approach? Manual Reduction Should it be put back on field? - YES Prone lying
My shoulder popped out what now? Richard Dallalana Epworth Shoulder Symposium June 2017 Shoulder Dislocation First event Best approach? Manual Reduction Should it be put back on field? - YES Prone lying
First-Time Anterior Shoulder Dislocation: Is it time to take a stand?
 Evaluation and Treatment of the Injured Athlete Martha s Vineyard July 22nd, 2018 First-Time Anterior Shoulder Dislocation: Is it time to take a stand? Robert A. Arciero, MD Professor, Orthopaedics University
Evaluation and Treatment of the Injured Athlete Martha s Vineyard July 22nd, 2018 First-Time Anterior Shoulder Dislocation: Is it time to take a stand? Robert A. Arciero, MD Professor, Orthopaedics University
Management of Anterior Shoulder Instability
 Management of Anterior Shoulder Instability Angelo J. Colosimo, MD Head Orthopaedic Surgeon University of Cincinnati Athletics Director of Sports Medicine University of Cincinnati Medical Center Associate
Management of Anterior Shoulder Instability Angelo J. Colosimo, MD Head Orthopaedic Surgeon University of Cincinnati Athletics Director of Sports Medicine University of Cincinnati Medical Center Associate
Anatomy GH Joint. Glenohumeral Instability. Components of Stability. Components of Stability 7/7/2017. AllinaHealthSystem
 Glenohumeral Instability Dr. John Steubs Allina Sports Medicine Conference July 7, 2017 Anatomy GH Joint Teardrop or oval shape Inherently unstable Golf ball and tee analogy Stabilizers Static Dynamic
Glenohumeral Instability Dr. John Steubs Allina Sports Medicine Conference July 7, 2017 Anatomy GH Joint Teardrop or oval shape Inherently unstable Golf ball and tee analogy Stabilizers Static Dynamic
P.O. Box Sierra Park Road Mammoth Lakes, CA Orthopedic Surgery & Sports Medicine
 P.O. Box 660 85 Sierra Park Road Mammoth Lakes, CA 93546 SHOULDER: Instability Dislocation Labral Tears The shoulder is the most mobile joint in the body, but to have this amount of motion, it is also
P.O. Box 660 85 Sierra Park Road Mammoth Lakes, CA 93546 SHOULDER: Instability Dislocation Labral Tears The shoulder is the most mobile joint in the body, but to have this amount of motion, it is also
SLAP Lesions Assessment & Treatment
 SLAP Lesions Assessment & Treatment Kevin E. Wilk,, PT, DPT Glenoid Labral Lesions Introduction Common injury - difficult to diagnose May occur in isolation or in combination SLAP lesions: Snyder: Arthroscopy
SLAP Lesions Assessment & Treatment Kevin E. Wilk,, PT, DPT Glenoid Labral Lesions Introduction Common injury - difficult to diagnose May occur in isolation or in combination SLAP lesions: Snyder: Arthroscopy
RECURRENT SHOULDER DISLOCATIONS WITH ABSENT LABRUM
 RECURRENT SHOULDER DISLOCATIONS WITH ABSENT LABRUM D R. A M R I S H K R. J H A M S ( O R T H O ) A S S I S T A N T P R O F E S S O R M E D I C A L C O L L E G E, K O L K A T A LABRUM Function as a chock-block,
RECURRENT SHOULDER DISLOCATIONS WITH ABSENT LABRUM D R. A M R I S H K R. J H A M S ( O R T H O ) A S S I S T A N T P R O F E S S O R M E D I C A L C O L L E G E, K O L K A T A LABRUM Function as a chock-block,
Rehabilitation Guidelines for Labral/Bankert Repair
 Rehabilitation Guidelines for Labral/Bankert Repair The true shoulder joint is called the glenohumeral joint and consists humeral head and the glenoid. It is a ball and socket joint. Anatomy of the Shoulder
Rehabilitation Guidelines for Labral/Bankert Repair The true shoulder joint is called the glenohumeral joint and consists humeral head and the glenoid. It is a ball and socket joint. Anatomy of the Shoulder
Shoulder Instability and Tendon Injuries
 Shoulder Instability and Tendon Injuries Shoulder Update Spire Hospital Leeds November 2017 Simon Boyle Consultant Shoulder and Elbow Surgeon Simon Boyle York and Leeds Nuffield Trained in Yorkshire, Annecy,
Shoulder Instability and Tendon Injuries Shoulder Update Spire Hospital Leeds November 2017 Simon Boyle Consultant Shoulder and Elbow Surgeon Simon Boyle York and Leeds Nuffield Trained in Yorkshire, Annecy,
Shoulder Instability. Fig 1: Intact labrum and biceps tendon
 Shoulder Instability What is it? The shoulder joint is a ball and socket joint, with the humeral head (upper arm bone) as the ball and the glenoid as the socket. The glenoid (socket) is a shallow bone
Shoulder Instability What is it? The shoulder joint is a ball and socket joint, with the humeral head (upper arm bone) as the ball and the glenoid as the socket. The glenoid (socket) is a shallow bone
Shoulder Injuries: Treatments that Work, Do Not Work, and When ENOUGH is Enough? Mark Ganjianpour, M.D. Beverly Hills, CA April 20, 2012
 Shoulder Injuries: Treatments that Work, Do Not Work, and When ENOUGH is Enough? Mark Ganjianpour, M.D. Beverly Hills, CA April 20, 2012 Multiaxial ball and socket Little Inherent Instability Glenohumeral
Shoulder Injuries: Treatments that Work, Do Not Work, and When ENOUGH is Enough? Mark Ganjianpour, M.D. Beverly Hills, CA April 20, 2012 Multiaxial ball and socket Little Inherent Instability Glenohumeral
Page 1. Shoulder Injuries in Sports.
 www.schulterteam.ch Shoulder Injuries in Sports Matthias A Zumstein Shoulder, Elbow and Orthopaedic Sports Medicine Department of Orthopedic Surgery and Traumatology University of Berne, Switzerland matthias.zumstein@insel.ch
www.schulterteam.ch Shoulder Injuries in Sports Matthias A Zumstein Shoulder, Elbow and Orthopaedic Sports Medicine Department of Orthopedic Surgery and Traumatology University of Berne, Switzerland matthias.zumstein@insel.ch
Instability of the shoulder Orthopaedic Department Patient Information Leaflet. Under review. Page 1
 Instability of the shoulder Orthopaedic Department Patient Information Leaflet Page 1 Shoulder instability There is a balance between movements in the shoulder whilst maintaining stability. When the shoulder
Instability of the shoulder Orthopaedic Department Patient Information Leaflet Page 1 Shoulder instability There is a balance between movements in the shoulder whilst maintaining stability. When the shoulder
Shoulder Injuries. Glenoid labrum injuries. SLAP Lesions
 Shoulder Injuries functional anatomy clinical perspective impingement rotator cuff injuries glenoid labrum injuries dislocation Glenoid labrum injuries SLAP lesions stable or unstable traction/compression
Shoulder Injuries functional anatomy clinical perspective impingement rotator cuff injuries glenoid labrum injuries dislocation Glenoid labrum injuries SLAP lesions stable or unstable traction/compression
POSTERIOR INSTABILITY OF THE SHOULDER Vasu Pai
 POSTERIOR INSTABILITY OF THE SHOULDER Vasu Pai Posterior instability is less common among cases of shoulder instability, accounting for 2% to 10% of all cases of instability. More common in sporting groups:
POSTERIOR INSTABILITY OF THE SHOULDER Vasu Pai Posterior instability is less common among cases of shoulder instability, accounting for 2% to 10% of all cases of instability. More common in sporting groups:
Posterior Shoulder Instability
 Posterior Shoulder Instability Robert A. Arciero, MD Professor of Orthopaedics University of Connecticut USA Classification of Posterior Instability Dislocation -acute -chronic- fixed or locked Subluxation
Posterior Shoulder Instability Robert A. Arciero, MD Professor of Orthopaedics University of Connecticut USA Classification of Posterior Instability Dislocation -acute -chronic- fixed or locked Subluxation
Strategies for Failed Instability Repair
 Strategies for Failed Instability Repair Robert E Hunter MD Director, Orthopedic Sports Medicine Center HRRMC Salida, Colorado CU Sports Medicine Course Sept 28, 2012 Conflict of Interest Paid Consultant:
Strategies for Failed Instability Repair Robert E Hunter MD Director, Orthopedic Sports Medicine Center HRRMC Salida, Colorado CU Sports Medicine Course Sept 28, 2012 Conflict of Interest Paid Consultant:
Rehabilitation Protocol: Arthroscopic Anterior Capsulolabral Repair of the Shoulder - Bankart Repair Rehabilitation Guidelines
 Rehabilitation Protocol: Arthroscopic Anterior Capsulolabral Repair of the Shoulder - Bankart Repair Rehabilitation Guidelines Department of Orthopaedic Surgery Lahey Hospital & Medical Center, Burlington
Rehabilitation Protocol: Arthroscopic Anterior Capsulolabral Repair of the Shoulder - Bankart Repair Rehabilitation Guidelines Department of Orthopaedic Surgery Lahey Hospital & Medical Center, Burlington
Acute Orthopaedic Injuries Developing a Diagnostic Approach to the Shoulder
 Acute Orthopaedic Injuries Developing a Diagnostic Approach to the Shoulder WWW.FISIOKINESITERAPIA.BIZ Overview To be able to quickly categorize shoulder injuries To take appropriate history and conduct
Acute Orthopaedic Injuries Developing a Diagnostic Approach to the Shoulder WWW.FISIOKINESITERAPIA.BIZ Overview To be able to quickly categorize shoulder injuries To take appropriate history and conduct
Common Surgical Shoulder Injury Repairs
 Common Surgical Shoulder Injury Repairs Mr Ilia Elkinson BHB, MBChB, FRACS (Ortho), FNZOA Orthopaedic and Upper Limb Surgeon Bowen Hospital Wellington Hospital Objectives Review pertinent anatomy of the
Common Surgical Shoulder Injury Repairs Mr Ilia Elkinson BHB, MBChB, FRACS (Ortho), FNZOA Orthopaedic and Upper Limb Surgeon Bowen Hospital Wellington Hospital Objectives Review pertinent anatomy of the
Body Planes. (A) Transverse Superior Inferior (B) Sagittal Medial Lateral (C) Coronal Anterior Posterior Extremity Proximal Distal
 Transverse Superior Inferior (B) Sagittal Medial Lateral (C) Coronal Anterior Posterior Extremity Proximal Distal") Body Planes (A) Transverse Superior Inferior (B) Sagittal Medial Lateral (C) Coronal Anterior Posterior Extremity Proximal Distal C B A Range of Motion Flexion Extension ADDUCTION ABDUCTION Range of Motion
Body Planes (A) Transverse Superior Inferior (B) Sagittal Medial Lateral (C) Coronal Anterior Posterior Extremity Proximal Distal C B A Range of Motion Flexion Extension ADDUCTION ABDUCTION Range of Motion
Traumatic shoulder dislocation in the adolescent athlete: advances in surgical treatment Christopher R. Good and John D.
 Traumatic shoulder dislocation in the adolescent athlete: advances in surgical treatment Christopher R. Good and John D. MacGillivray Purpose of review The shoulder joint has the greatest range of motion
Traumatic shoulder dislocation in the adolescent athlete: advances in surgical treatment Christopher R. Good and John D. MacGillivray Purpose of review The shoulder joint has the greatest range of motion
The Management of Shoulder Instability. By Debbie Prince Clinical Shoulder Specialist
 The Management of Shoulder Instability By Debbie Prince Clinical Shoulder Specialist Shoulder Dislocation The most common joint dislocation Traumatic Instability, highest incidence in males aged 21 to
The Management of Shoulder Instability By Debbie Prince Clinical Shoulder Specialist Shoulder Dislocation The most common joint dislocation Traumatic Instability, highest incidence in males aged 21 to
Rehabilitation Guidelines for Anterior Shoulder Reconstruction with Arthroscopic Bankart Repair
 UW HEALTH SPORTS REHABILITATION Rehabilitation Guidelines for Anterior Shoulder Reconstruction with Arthroscopic Bankart Repair The anatomic configuration of the shoulder joint (glenohumeral joint) is
UW HEALTH SPORTS REHABILITATION Rehabilitation Guidelines for Anterior Shoulder Reconstruction with Arthroscopic Bankart Repair The anatomic configuration of the shoulder joint (glenohumeral joint) is
 Specialists in Joint Replacement, Spinal Surgery, Orthopaedics and Sport Injuries The Latarjet Procedure (coracoid transfer) Shoulder Stabilisation Surgery Ms. Ruth Delaney Consultant Orthopaedic Surgeon
Specialists in Joint Replacement, Spinal Surgery, Orthopaedics and Sport Injuries The Latarjet Procedure (coracoid transfer) Shoulder Stabilisation Surgery Ms. Ruth Delaney Consultant Orthopaedic Surgeon
Management of Humeral Bone Loss in Anterior Shoulder Instability. Scott D. Mair, MD University of Kentucky Sports Medicine
 Management of Humeral Bone Loss in Anterior Shoulder Instability Scott D. Mair, MD University of Kentucky Sports Medicine Disclosure Smith and Nephew Endoscopy fellowship support Importance Bone loss (glenoid
Management of Humeral Bone Loss in Anterior Shoulder Instability Scott D. Mair, MD University of Kentucky Sports Medicine Disclosure Smith and Nephew Endoscopy fellowship support Importance Bone loss (glenoid
Rehabilitation Guidelines for Arthroscopic Capsular Shift
 UW HEALTH SPORTS REHABILITATION Rehabilitation Guidelines for Arthroscopic Capsular Shift The anatomic configuration of the shoulder joint (glenohumeral joint) is often compared to a golf ball on a tee.
UW HEALTH SPORTS REHABILITATION Rehabilitation Guidelines for Arthroscopic Capsular Shift The anatomic configuration of the shoulder joint (glenohumeral joint) is often compared to a golf ball on a tee.
Anterior Shoulder Instability
 Anterior Shoulder Instability Anterior shoulder instability typically results from a dislocation injury to the shoulder joint when the humeral head (ball) of the humerus (upper arm bone) is displaced from
Anterior Shoulder Instability Anterior shoulder instability typically results from a dislocation injury to the shoulder joint when the humeral head (ball) of the humerus (upper arm bone) is displaced from
Rotator Cuff Repair TRENDS OF REPAIRS. Evolution of Arthroscopic Repair. Shoulder Girdle. Rotator Cuff Repair 8/29/2013
 Rotator Cuff Repair Indications, Patient Selection, Outcomes James C. Vailas, M.D. New Hampshire Orthopaedic Center September 14, 2013 New Hampshire Musculoskeletal Institute 20 th Annual Symposium Evolution
Rotator Cuff Repair Indications, Patient Selection, Outcomes James C. Vailas, M.D. New Hampshire Orthopaedic Center September 14, 2013 New Hampshire Musculoskeletal Institute 20 th Annual Symposium Evolution
Sports Medicine: Shoulder Arthrography. Christine B. Chung, M.D. Professor of Radiology Musculoskeletal Division UCSD and VA Healthcare System
 Sports Medicine: Shoulder Arthrography Christine B. Chung, M.D. Professor of Radiology Musculoskeletal Division UCSD and VA Healthcare System Disclosure Off-label use for gadolinium Pediatric Sports Injuries
Sports Medicine: Shoulder Arthrography Christine B. Chung, M.D. Professor of Radiology Musculoskeletal Division UCSD and VA Healthcare System Disclosure Off-label use for gadolinium Pediatric Sports Injuries
Rehabilitation Guidelines for Anterior Shoulder Reconstruction with Open Bankart Repair
 UW HEALTH SPORTS REHABILITATION Rehabilitation Guidelines for Anterior Shoulder Reconstruction with Open Bankart Repair The anatomic configuration of the shoulder joint (glenohumeral joint) is often compared
UW HEALTH SPORTS REHABILITATION Rehabilitation Guidelines for Anterior Shoulder Reconstruction with Open Bankart Repair The anatomic configuration of the shoulder joint (glenohumeral joint) is often compared
SHOULDER ARTHROSCOPY
 SHOULDER ARTHROSCOPY PATIENT HANDBOOK Physical/Occupational Therapy 3755 Orange Place, Suite 101 Beachwood, OH 44122 216-312-6045 Therapist: Post-Op Visit: Anatomy and Function of the Shoulder The shoulder
SHOULDER ARTHROSCOPY PATIENT HANDBOOK Physical/Occupational Therapy 3755 Orange Place, Suite 101 Beachwood, OH 44122 216-312-6045 Therapist: Post-Op Visit: Anatomy and Function of the Shoulder The shoulder
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abduction pillow, ultrasling, 880, 881, 882, 883 Adolescents, shoulder instability in. See Shoulder, instability of, pediatric and adolescent.
Index Note: Page numbers of article titles are in boldface type. A Abduction pillow, ultrasling, 880, 881, 882, 883 Adolescents, shoulder instability in. See Shoulder, instability of, pediatric and adolescent.
Review shoulder anatomy Review the physical exam of the shoulder Discuss some common causes of acute shoulder pain Discuss some common causes of
 Review shoulder anatomy Review the physical exam of the shoulder Discuss some common causes of acute shoulder pain Discuss some common causes of chronic shoulder pain Review with some case questions Bones:
Review shoulder anatomy Review the physical exam of the shoulder Discuss some common causes of acute shoulder pain Discuss some common causes of chronic shoulder pain Review with some case questions Bones:
Football and netball season A review of the apophysis and the acute shoulder: assessment. Simon Locke Sport and Exercise Physician
 Football and netball season A review of the apophysis and the acute shoulder: assessment Simon Locke Sport and Exercise Physician Apophyseal injuries; How to diagnose and manage? Goals for tonight Recognise
Football and netball season A review of the apophysis and the acute shoulder: assessment Simon Locke Sport and Exercise Physician Apophyseal injuries; How to diagnose and manage? Goals for tonight Recognise
The Athlete s Shoulder
 The Athlete s Shoulder Lennard Funk lenfunk@shoulderdoc.co.uk Decision Making NORMATIVE evidence base COGNITIVE environmental PSYCHOLOGICAL individual needs, bias, preferences, values Three P s 1. Major
The Athlete s Shoulder Lennard Funk lenfunk@shoulderdoc.co.uk Decision Making NORMATIVE evidence base COGNITIVE environmental PSYCHOLOGICAL individual needs, bias, preferences, values Three P s 1. Major
Types of shoulder Dislocation: Shoulder dislocation. 1. Anterior 2. Posterior 3. Luxatio erecta (inferior dislocation)
") Types of shoulder Dislocation: Shoulder dislocation 1. Anterior 2. Posterior 3. Luxatio erecta (inferior dislocation) Anterior Dislocation: head is dislocated anterior to the glenoid Most common among
Types of shoulder Dislocation: Shoulder dislocation 1. Anterior 2. Posterior 3. Luxatio erecta (inferior dislocation) Anterior Dislocation: head is dislocated anterior to the glenoid Most common among
This presentation is the intellectual property of the author. Contact them at for permission to reprint and/or distribute.
 January 19, 2012 John W. Hinchey, MD Dept of Orthopaedic Surgery Shoulder & Elbow Service This live activity is designated for a maximum of 1 AMA PRA Category 1 Credit tm. Physicians should claim only
January 19, 2012 John W. Hinchey, MD Dept of Orthopaedic Surgery Shoulder & Elbow Service This live activity is designated for a maximum of 1 AMA PRA Category 1 Credit tm. Physicians should claim only
A Patient s Guide to Labral Tears
 A Patient s Guide to Labral Tears 20295 NE 29th Place, Ste 300 Aventura, FL 33180 Phone: (786) 629-0910 Fax: (786) 629-0920 admin@instituteofsports.com DISCLAIMER: The information in this booklet is compiled
A Patient s Guide to Labral Tears 20295 NE 29th Place, Ste 300 Aventura, FL 33180 Phone: (786) 629-0910 Fax: (786) 629-0920 admin@instituteofsports.com DISCLAIMER: The information in this booklet is compiled
Thinking About Shoulder Instability Surgery (a.k.a Why do we do what we do?)
") Thinking About Shoulder Instability Surgery (a.k.a Why do we do what we do?) Thomas J. Gill Chief, MGH Sports Medicine Dept. of Orthopedic Surgery Massachusetts General Hospital Boston, MA Look, just do
Thinking About Shoulder Instability Surgery (a.k.a Why do we do what we do?) Thomas J. Gill Chief, MGH Sports Medicine Dept. of Orthopedic Surgery Massachusetts General Hospital Boston, MA Look, just do
Shoulder Instability and Stabilisation
 Shoulder Instability and Stabilisation The benefit of the huge range of movements at the shoulder is that we are able to position the hand as required, the cost is that the shoulder is more likely to dislocate
Shoulder Instability and Stabilisation The benefit of the huge range of movements at the shoulder is that we are able to position the hand as required, the cost is that the shoulder is more likely to dislocate
Case Report Arthroscopic Bony Bankart Repair Using Double-Threaded Headless Screw: A Case Report
 Case Reports in Orthopedics Volume 2012, Article ID 789418, 4 pages doi:10.1155/2012/789418 Case Report Arthroscopic Bony Bankart Repair Using Double-Threaded Headless Screw: A Case Report Takeshi Kokubu,
Case Reports in Orthopedics Volume 2012, Article ID 789418, 4 pages doi:10.1155/2012/789418 Case Report Arthroscopic Bony Bankart Repair Using Double-Threaded Headless Screw: A Case Report Takeshi Kokubu,
The Spectrum of Lesions and Clinical Results of Arthroscopic Stabilization of Acute Anterior Shoulder Instability
 Original Article DOI 10.3349/ymj.2010.51.3.421 pissn: 0513-5796, eissn: 1976-2437 Yonsei Med J 51(3): 421-426, 2010 The Spectrum of Lesions and Clinical Results of Arthroscopic Stabilization of Acute Anterior
Original Article DOI 10.3349/ymj.2010.51.3.421 pissn: 0513-5796, eissn: 1976-2437 Yonsei Med J 51(3): 421-426, 2010 The Spectrum of Lesions and Clinical Results of Arthroscopic Stabilization of Acute Anterior
Chronic Shoulder Instability
 Chronic Shoulder Instability The shoulder is the most moveable joint in your body. It helps you to lift your arm, to rotate it, and to reach up over your head. It is able to turn in many directions. This
Chronic Shoulder Instability The shoulder is the most moveable joint in your body. It helps you to lift your arm, to rotate it, and to reach up over your head. It is able to turn in many directions. This
Christopher A Brown, MD Sports Medicine Orthopedist. Duke Orthopedic Residency Sports Medicine Fellowship Stanford
 Christopher A Brown, MD Sports Medicine Orthopedist Duke Orthopedic Residency Sports Medicine Fellowship Stanford Office Geneva Newark Opening Canandaigua and Penfield Topics Of Discussion Shoulder dislocation
Christopher A Brown, MD Sports Medicine Orthopedist Duke Orthopedic Residency Sports Medicine Fellowship Stanford Office Geneva Newark Opening Canandaigua and Penfield Topics Of Discussion Shoulder dislocation
GOAL. Open Bankart: Why and How? 2/16/2017. Richard J. Hawkins, MD. Convince You That Open Bankart should be in our toolbox
 Current Solutions in Shoulder & Elbow Surgery Tampa, Florida February 9 12, 2017 Open Bankart: Why and How? Richard J. Hawkins, MD Steadman Hawkins Clinic of the Carolinas Hawkins Foundation Greenville,
Current Solutions in Shoulder & Elbow Surgery Tampa, Florida February 9 12, 2017 Open Bankart: Why and How? Richard J. Hawkins, MD Steadman Hawkins Clinic of the Carolinas Hawkins Foundation Greenville,
Shoulder Arthroscopy. Dr. J.J.A.M. van Raaij. NOV Jaarvergadering Den Bosch 25 jan 2018
 Shoulder Arthroscopy Dr. J.J.A.M. van Raaij NOV Jaarvergadering Den Bosch 25 jan 2018 No disclosures Disclosure Shoulder Instability Traumatic anterior Traumatic posterior Acquired atraumatic Multidirectional
Shoulder Arthroscopy Dr. J.J.A.M. van Raaij NOV Jaarvergadering Den Bosch 25 jan 2018 No disclosures Disclosure Shoulder Instability Traumatic anterior Traumatic posterior Acquired atraumatic Multidirectional
A Patient s Guide to Shoulder Dislocations
 A Patient s Guide to Shoulder Dislocations 20295 NE 29th Place, Ste 300 Aventura, FL 33180 Phone: (786) 629-0910 Fax: (786) 629-0920 admin@instituteofsports.com DISCLAIMER: The information in this booklet
A Patient s Guide to Shoulder Dislocations 20295 NE 29th Place, Ste 300 Aventura, FL 33180 Phone: (786) 629-0910 Fax: (786) 629-0920 admin@instituteofsports.com DISCLAIMER: The information in this booklet
Conflict of Interest. New Strategies in Rotator Cuff Repair. Objectives. Learner Outcome
 Conflict of Interest New Strategies in Rotator Cuff Repair Sheri Lankford, BSN, CNOR I hereby certify that, to the best of my knowledge, no aspect of my current personal or professional situation might
Conflict of Interest New Strategies in Rotator Cuff Repair Sheri Lankford, BSN, CNOR I hereby certify that, to the best of my knowledge, no aspect of my current personal or professional situation might
External Rotation Brace Combined with a Physiotherapy Program for First Time Anterior Shoulder Dislocators; a 2 Year Follow Up
 External Rotation Brace Combined with a Physiotherapy Program for First Time Anterior Shoulder Dislocators; a 2 Year Follow Up 2010 Bi-Annual SESA Closed Conference DISCLAIMER None of the authors have
External Rotation Brace Combined with a Physiotherapy Program for First Time Anterior Shoulder Dislocators; a 2 Year Follow Up 2010 Bi-Annual SESA Closed Conference DISCLAIMER None of the authors have
Surgical versus conservative treatment for acute first-time anterior shoulder dislocation: the evidence
 J Orthopaed Traumatol (2007) 8:207 213 DOI 10.1007/s10195-007-0095-7 EVIDENCE-BASED MEDICINE SECTION R. Padua R. Bondì L. Bondì A. Campi Surgical versus conservative treatment for acute first-time anterior
J Orthopaed Traumatol (2007) 8:207 213 DOI 10.1007/s10195-007-0095-7 EVIDENCE-BASED MEDICINE SECTION R. Padua R. Bondì L. Bondì A. Campi Surgical versus conservative treatment for acute first-time anterior
ANTERIOR SHOULDER STABILIZATION CLINICAL PRACTICE GUIDELINE
 ANTERIOR SHOULDER STABILIZATION CLINICAL PRACTICE GUIDELINE Background Ohio State s Anterior Shoulder Stabilization Rehabilitation Guideline is to be utilized following open or arthroscopic anterior shoulder
ANTERIOR SHOULDER STABILIZATION CLINICAL PRACTICE GUIDELINE Background Ohio State s Anterior Shoulder Stabilization Rehabilitation Guideline is to be utilized following open or arthroscopic anterior shoulder
Double bucket handle tears of the superior labrum
 Case Report http://dx.doi.org/10.14517/aosm13013 pissn 2289-005X eissn 2289-0068 Double bucket handle tears of the superior labrum Dong-Soo Kim, Kyoung-Jin Park, Yong-Min Kim, Eui-Sung Choi, Hyun-Chul
Case Report http://dx.doi.org/10.14517/aosm13013 pissn 2289-005X eissn 2289-0068 Double bucket handle tears of the superior labrum Dong-Soo Kim, Kyoung-Jin Park, Yong-Min Kim, Eui-Sung Choi, Hyun-Chul
SHOULDER DISLOCATION & INSTABILITY Rehabilitation Considerations
 SHOULDER DISLOCATION & INSTABILITY Rehabilitation Considerations Meagan Pehnke, MS, OTR/L, CHT, CLT March 1 st, 2019 Philadelphia Surgery & Rehabilitation of the Hand: Pediatric Pre-course OUTLINE Discuss
SHOULDER DISLOCATION & INSTABILITY Rehabilitation Considerations Meagan Pehnke, MS, OTR/L, CHT, CLT March 1 st, 2019 Philadelphia Surgery & Rehabilitation of the Hand: Pediatric Pre-course OUTLINE Discuss
Biceps Tenodesis Protocol
 Biceps Tenodesis Protocol A biceps tenodesis procedure involves cutting of the long head of the biceps just prior to its insertion on the superior labrum and then anchoring the tendon along its anatomical
Biceps Tenodesis Protocol A biceps tenodesis procedure involves cutting of the long head of the biceps just prior to its insertion on the superior labrum and then anchoring the tendon along its anatomical
Disclosure. Traumatic Anterior Shoulder Instability 7/23/2018. Orthopaedics for the Primary Care Practitioner & Rehabilitation Therapist
 Orthopaedics for the Primary Care Practitioner & Rehabilitation Therapist Christopher E. Baker M.D. Sports Medicine Shoulder Reconstruction Traumatic Anterior Shoulder Instability Disclosure Speaking/Consulting
Orthopaedics for the Primary Care Practitioner & Rehabilitation Therapist Christopher E. Baker M.D. Sports Medicine Shoulder Reconstruction Traumatic Anterior Shoulder Instability Disclosure Speaking/Consulting
Glenohumeral Joint Instability. Static Stabilizers of the GHJ. Static Stabilizers of the GHJ. Static Stabilizers of the GHJ
 1 Glenohumeral Joint Instability GHJ Joint Stability: Or Lack Thereof! Christine B. Chung, M.D. Assistant Professor of Radiology Musculoskeletal Division UCSD and VA Healthcare System Static Stabilizers
1 Glenohumeral Joint Instability GHJ Joint Stability: Or Lack Thereof! Christine B. Chung, M.D. Assistant Professor of Radiology Musculoskeletal Division UCSD and VA Healthcare System Static Stabilizers
Shoulder Injury Evaluation.
 Shoulder Injury Evaluation www.fisiokinesiterapia.biz Basic Anatomy & Kinesiology 3 Bone Structures Clavicle Scapula Humerus Evaluation Principles Always follow a standard progression Determine the target
Shoulder Injury Evaluation www.fisiokinesiterapia.biz Basic Anatomy & Kinesiology 3 Bone Structures Clavicle Scapula Humerus Evaluation Principles Always follow a standard progression Determine the target
A Patient s Guide to Labral Tears
 A Patient s Guide to Labral Tears Sports-related injuries require specialized care to promote optimum healing. Whether you are a weekend jogger or tennis player, a professional soccer player or marathon
A Patient s Guide to Labral Tears Sports-related injuries require specialized care to promote optimum healing. Whether you are a weekend jogger or tennis player, a professional soccer player or marathon
ANATOMY / BIOMECHANICS LONG HEAD OF BICEPS ATTACHES AT THE SUPERIOR GLENOIDAL TUBERCLE WITH THE LABRUM FIBROCARTILAGINOUS TISSUE IF THERE IS A TORN SU
 SLAP LESIONS Management Of Glenoid Labrum Injuries INTRODUCTION First described by Andrews AJSM 85 Throwers 60% Normal Variants Sublabral Foramen Buford Complex Meniscoid Snyder Arth. 1990 termed SLAP
SLAP LESIONS Management Of Glenoid Labrum Injuries INTRODUCTION First described by Andrews AJSM 85 Throwers 60% Normal Variants Sublabral Foramen Buford Complex Meniscoid Snyder Arth. 1990 termed SLAP
The Cryo/Cuff provides two functions: 1. Compression - to keep swelling down. 2. Ice Therapy - to keep swelling down and to help minimize pain. Patien
 The Cryo/Cuff provides two functions: 1. Compression - to keep swelling down. 2. Ice Therapy - to keep swelling down and to help minimize pain. Patients, for the most part, experience less pain and/or
The Cryo/Cuff provides two functions: 1. Compression - to keep swelling down. 2. Ice Therapy - to keep swelling down and to help minimize pain. Patients, for the most part, experience less pain and/or
Shoulder and Elbow ORTHOPAEDIC SYPMPOSIUM APRIL 8, 2017 DANIEL DOTY MD
 Shoulder and Elbow ORTHOPAEDIC SYPMPOSIUM APRIL 8, 2017 DANIEL DOTY MD Shoulder Articulations Glenohumeral Joint 2/3 total arc of motion Shallow Ball and Socket Joint Allows for excellent ROM Requires
Shoulder and Elbow ORTHOPAEDIC SYPMPOSIUM APRIL 8, 2017 DANIEL DOTY MD Shoulder Articulations Glenohumeral Joint 2/3 total arc of motion Shallow Ball and Socket Joint Allows for excellent ROM Requires
Arthroscopic Preparation of the Posterior and Posteroinferior Glenoid Labrum
 Arthroscopic Preparation of the Posterior and Posteroinferior Glenoid Labrum By Matthew T. Provencher, MD, LCDR, MC, USNR; Anthony A. Romeo, MD; Daniel J. Solomon, MD, CDR, MC, USN; Bernard R. Bach, Jr.,
Arthroscopic Preparation of the Posterior and Posteroinferior Glenoid Labrum By Matthew T. Provencher, MD, LCDR, MC, USNR; Anthony A. Romeo, MD; Daniel J. Solomon, MD, CDR, MC, USN; Bernard R. Bach, Jr.,
ANTERIOR SHOULDER INSTABILITY which operation is best? Dr Jerome Goldberg Shoulder Surgery
 ANTERIOR SHOULDER INSTABILITY which operation is best? DISCLOSURE Arthrex fund POW Shoulder fellowship Co Director of POW Orthopaedic Research Laboratory MAC of Device Technologies Chairman AusBio Board
ANTERIOR SHOULDER INSTABILITY which operation is best? DISCLOSURE Arthrex fund POW Shoulder fellowship Co Director of POW Orthopaedic Research Laboratory MAC of Device Technologies Chairman AusBio Board
Rehabilitation Guidelines for Large Rotator Cuff Repair
 Rehabilitation Guidelines for Large Rotator Cuff Repair The true shoulder joint is called the glenohumeral joint and consists humeral head and the glenoid. It is a ball and socket joint. Anatomy of the
Rehabilitation Guidelines for Large Rotator Cuff Repair The true shoulder joint is called the glenohumeral joint and consists humeral head and the glenoid. It is a ball and socket joint. Anatomy of the
 www.fisiokinesiterapia.biz Shoulder Problems Fractures Instability Impingement Miscellaneous Anatomy Bones Joints / Ligaments Muscles Neurovascular Anatomy Anatomy Supraspinatus Anterior Posterior Anatomy
www.fisiokinesiterapia.biz Shoulder Problems Fractures Instability Impingement Miscellaneous Anatomy Bones Joints / Ligaments Muscles Neurovascular Anatomy Anatomy Supraspinatus Anterior Posterior Anatomy
HAGL lesion of the shoulder
 HAGL lesion of the shoulder A 24 year old rugby player presented to an orthopaedic surgeon with a history of dislocation of the left shoulder. It reduced spontaneously and again later during the same match.
HAGL lesion of the shoulder A 24 year old rugby player presented to an orthopaedic surgeon with a history of dislocation of the left shoulder. It reduced spontaneously and again later during the same match.
Chronic Shoulder Disorders
 Chronic Shoulder Disorders Dr. Mustafa Elsingergy Consultant orthopedic surgeon Dallah Hospita Prof. Mamoun Kremli Almaarefa Medical College Contents INTRINSIC Shoulder Pain Due to causes in the shoulder
Chronic Shoulder Disorders Dr. Mustafa Elsingergy Consultant orthopedic surgeon Dallah Hospita Prof. Mamoun Kremli Almaarefa Medical College Contents INTRINSIC Shoulder Pain Due to causes in the shoulder
Glenohumeral Joint Instability: An Athlete s Perspective
 Anatomic Considerations Glenohumeral Joint Instability: An Athlete s Perspective Michael D. Loeb, MD Texas Orthopedics, Sports Medicine, and Rehabilitation Associates Austin, Texas Static Stabilizers Osseous
Anatomic Considerations Glenohumeral Joint Instability: An Athlete s Perspective Michael D. Loeb, MD Texas Orthopedics, Sports Medicine, and Rehabilitation Associates Austin, Texas Static Stabilizers Osseous
Curative effects of under-arthroscopic anchor implantation fixation to martial arts player s shoulder joint injury.
 Biomedical Research 2017; 28 (19): 8295-8299 ISSN 0970-938X www.biomedres.info Curative effects of under-arthroscopic anchor implantation fixation to martial arts player s shoulder joint injury. Zonghao
Biomedical Research 2017; 28 (19): 8295-8299 ISSN 0970-938X www.biomedres.info Curative effects of under-arthroscopic anchor implantation fixation to martial arts player s shoulder joint injury. Zonghao
ROTATOR CUFF DISORDERS/IMPINGEMENT
 ROTATOR CUFF DISORDERS/IMPINGEMENT Dr.KN Subramanian M.Ch Orth., FRCS (Tr & Orth), CCT Orth(UK) Consultant Orthopaedic Surgeon, Special interest: Orthopaedic Sports Injury, Shoulder and Knee Surgery, SPARSH
ROTATOR CUFF DISORDERS/IMPINGEMENT Dr.KN Subramanian M.Ch Orth., FRCS (Tr & Orth), CCT Orth(UK) Consultant Orthopaedic Surgeon, Special interest: Orthopaedic Sports Injury, Shoulder and Knee Surgery, SPARSH
Biceps Tenotomy Protocol
 Biceps Tenotomy Protocol A biceps tenotomy procedure involves cutting of the long head of the biceps just prior to its insertion on the superior labrum. A biceps tenotomy is typically done when there is
Biceps Tenotomy Protocol A biceps tenotomy procedure involves cutting of the long head of the biceps just prior to its insertion on the superior labrum. A biceps tenotomy is typically done when there is
11/15/2017. Biceps Lesions. Highgate Private Hospital (Whittington Health NHS Trust) E: LHB Anatomy.
 E: LHB Anatomy.") Biceps Lesions Mr Omar Haddo (Consultant Orthopaedic Surgeon MBBS, BmedSci, FRCS(Orth) ) Highgate Private Hospital (Whittington Health NHS Trust) E: admin@denovomedic.co.uk LHB Anatomy Arise from superior
Biceps Lesions Mr Omar Haddo (Consultant Orthopaedic Surgeon MBBS, BmedSci, FRCS(Orth) ) Highgate Private Hospital (Whittington Health NHS Trust) E: admin@denovomedic.co.uk LHB Anatomy Arise from superior
MRI SHOULDER WHAT TO SEE
 MRI SHOULDER WHAT TO SEE DR SHEKHAR SRIVASTAV Sr. Consultant- Knee & Shoulder Arthroscopy Sant Parmanand Hospital Normal Anatomy Normal Shoulder MRI Coronal Oblique Sagital Oblique Axial Cuts Normal Coronal
MRI SHOULDER WHAT TO SEE DR SHEKHAR SRIVASTAV Sr. Consultant- Knee & Shoulder Arthroscopy Sant Parmanand Hospital Normal Anatomy Normal Shoulder MRI Coronal Oblique Sagital Oblique Axial Cuts Normal Coronal
The ball-and-socket articulation at the glenohumeral joint is between the convex
 SLAP Lesion Repair Emily Cotey, Emily Hurysz, and Patrick Schroeder Abstract SLAP lesion, which stands for Superior Labrum Anterior and Posterior, is a detachment tear of the superior labrum that originates
SLAP Lesion Repair Emily Cotey, Emily Hurysz, and Patrick Schroeder Abstract SLAP lesion, which stands for Superior Labrum Anterior and Posterior, is a detachment tear of the superior labrum that originates
Rehabilitation Guidelines for Open Latarjet Anterior Shoulder Stabilization
 UW HEALTH SPORTS REHABILITATION Rehabilitation Guidelines for Open Latarjet Anterior Shoulder Stabilization The anatomic configuration of the shoulder joint (glenohumeral joint) is often compared to a
UW HEALTH SPORTS REHABILITATION Rehabilitation Guidelines for Open Latarjet Anterior Shoulder Stabilization The anatomic configuration of the shoulder joint (glenohumeral joint) is often compared to a
Arthroscopic procedures for the treatment of anterior shoulder instability: local experiences!"#$%&'()*+,-%&./0123
*+,-%&./0123") ST Choi PYT Tse ORIGINAL ARTICLE Arthroscopic procedures for the treatment of anterior shoulder instability: local experiences!"#$%&'()*+,-%&./03 Objective. To review the outcomes of arthroscopic stabilisation
ST Choi PYT Tse ORIGINAL ARTICLE Arthroscopic procedures for the treatment of anterior shoulder instability: local experiences!"#$%&'()*+,-%&./03 Objective. To review the outcomes of arthroscopic stabilisation
The Shoulder. By Patrick Ryan, Bobby Law, Jack Beaty, Alex Newhouse and Chuck Nelson
 The Shoulder By Patrick Ryan, Bobby Law, Jack Beaty, Alex Newhouse and Chuck Nelson Learning Objectives/Agenda Review the anatomy of the shoulder Describe the main diseases of the shoulder Describe the
The Shoulder By Patrick Ryan, Bobby Law, Jack Beaty, Alex Newhouse and Chuck Nelson Learning Objectives/Agenda Review the anatomy of the shoulder Describe the main diseases of the shoulder Describe the
R. Frank Henn III, MD. Associate Professor Chief of Sports Medicine Residency Program Director
 R. Frank Henn III, MD Associate Professor Chief of Sports Medicine Residency Program Director Disclosures No financial relationships to disclose 1. Labral anatomy 2. Adaptations of the throwing shoulder
R. Frank Henn III, MD Associate Professor Chief of Sports Medicine Residency Program Director Disclosures No financial relationships to disclose 1. Labral anatomy 2. Adaptations of the throwing shoulder
Massive Rotator Cuff Tears. Rafael M. Williams, MD
 Massive Rotator Cuff Tears Rafael M. Williams, MD Rotator Cuff MRI MRI Small / Partial Thickness Medium Tear Arthroscopic View Massive Tear Fatty Atrophy Arthroscopic View MassiveTears Tear is > 5cm
Massive Rotator Cuff Tears Rafael M. Williams, MD Rotator Cuff MRI MRI Small / Partial Thickness Medium Tear Arthroscopic View Massive Tear Fatty Atrophy Arthroscopic View MassiveTears Tear is > 5cm
Arthroscopic Treatment of the First Anterior Shoulder Dislocation in Young Skiers
 Journal of ASTM International, March 2006, Vol. 3, No. 3 Paper ID JAI14199 Available online at www.astm.org Christos K. Yiannakopoulos, 1 Athanassios N. Zacharopoulos, 2 and Emmanuel Antonogiannakis 1
Journal of ASTM International, March 2006, Vol. 3, No. 3 Paper ID JAI14199 Available online at www.astm.org Christos K. Yiannakopoulos, 1 Athanassios N. Zacharopoulos, 2 and Emmanuel Antonogiannakis 1
Biceps Tenodesis Protocol
 Robert K. Fullick, MD 6400 Fannin Street, Suite 1700 Houston, Texas 77030 Ph.: 713-486-7543 / Fx.: 713-486-5549 Biceps Tenodesis Protocol The intent of this protocol is to provide the clinician with a
Robert K. Fullick, MD 6400 Fannin Street, Suite 1700 Houston, Texas 77030 Ph.: 713-486-7543 / Fx.: 713-486-5549 Biceps Tenodesis Protocol The intent of this protocol is to provide the clinician with a
Ms. Ruth A. Delaney, MB BCh BAO, MMedSc, MRCS
 Ms. Ruth A. Delaney, MB BCh BAO, MMedSc, MRCS Consultant Orthopaedic Surgeon, Shoulder Specialist. +353 1 5262335 ruthdelaney@sportssurgeryclinic.com Modified from the protocol developed at Boston Shoulder
Ms. Ruth A. Delaney, MB BCh BAO, MMedSc, MRCS Consultant Orthopaedic Surgeon, Shoulder Specialist. +353 1 5262335 ruthdelaney@sportssurgeryclinic.com Modified from the protocol developed at Boston Shoulder
From the Sports Medicine Section, Orthopaedic Surgery Service, Tripler Army Medical Center, Honolulu, Hawaii
 0363-5465/102/3030-0576$02.00/0 THE AMERICAN JOURNAL OF SPORTS MEDICINE, Vol. 30, No. 4 A Prospective, Randomized Evaluation of Arthroscopic Stabilization Versus Nonoperative Treatment in Patients with
0363-5465/102/3030-0576$02.00/0 THE AMERICAN JOURNAL OF SPORTS MEDICINE, Vol. 30, No. 4 A Prospective, Randomized Evaluation of Arthroscopic Stabilization Versus Nonoperative Treatment in Patients with
Introduction & Question 1
 Page 1 of 7 www.medscape.com To Print: Click your browser's PRINT button. NOTE: To view the article with Web enhancements, go to: http://www.medscape.com/viewarticle/424981 Case Q & A Shoulder Pain, Part
Page 1 of 7 www.medscape.com To Print: Click your browser's PRINT button. NOTE: To view the article with Web enhancements, go to: http://www.medscape.com/viewarticle/424981 Case Q & A Shoulder Pain, Part
Shoulder Trauma (Fractures and Dislocations)
") Shoulder Trauma (Fractures and Dislocations) Trauma to the shoulder is common. Injuries range from a separated shoulder resulting from a fall onto the shoulder to a high-speed car accident that fractures
Shoulder Trauma (Fractures and Dislocations) Trauma to the shoulder is common. Injuries range from a separated shoulder resulting from a fall onto the shoulder to a high-speed car accident that fractures
Anterior Stabilization of the Shoulder: Latarjet Protocol
 Anterior Stabilization of the Shoulder: Latarjet Protocol Dr. Abigail R. Hamilton, M.D. Shoulder instability may be caused from congenital deformity, recurrent overuse activity, and/or traumatic dislocation.
Anterior Stabilization of the Shoulder: Latarjet Protocol Dr. Abigail R. Hamilton, M.D. Shoulder instability may be caused from congenital deformity, recurrent overuse activity, and/or traumatic dislocation.
Upper Extremity Injuries in Youth Baseball: Causes and Prevention
 Upper Extremity Injuries in Youth Baseball: Causes and Prevention Biomechanics Throwing a baseball is an unnatural movement Excessively high forces are generated at the elbow and shoulder Throwing requires
Upper Extremity Injuries in Youth Baseball: Causes and Prevention Biomechanics Throwing a baseball is an unnatural movement Excessively high forces are generated at the elbow and shoulder Throwing requires
Personal BACKGROUND 09/03/2018. L.Lafosse Alps Surgery Institute Annecy FRANCE. L.Lafosse : LATARJET GOUTALLIER
 L.Lafosse Alps Surgery Institute Annecy FRANCE L.Lafosse Alps Surgery Institute Annecy FRANCE Personal BACKGROUND 1982 83 : LATARJET Resident @ GOUTALLIER 1984 : BANKART Resident @ DUPARC 1985 : ALLOGRAFT
L.Lafosse Alps Surgery Institute Annecy FRANCE L.Lafosse Alps Surgery Institute Annecy FRANCE Personal BACKGROUND 1982 83 : LATARJET Resident @ GOUTALLIER 1984 : BANKART Resident @ DUPARC 1985 : ALLOGRAFT
A Patient s Guide to Shoulder Instability
 A Patient s Guide to Shoulder Instability 2350 Royal Boulevard Suite 200 Elgin, IL 60123 Phone: 847.931.5300 Fax: 847.931.9072 DISCLAIMER: The information in this booklet is compiled from a variety of
A Patient s Guide to Shoulder Instability 2350 Royal Boulevard Suite 200 Elgin, IL 60123 Phone: 847.931.5300 Fax: 847.931.9072 DISCLAIMER: The information in this booklet is compiled from a variety of
Arthroscopic Findings After Traumatic Shoulder Instability in Patients Older Than 35 Years
 Arthroscopic Findings After Traumatic Shoulder Instability in Patients Older Than 35 Years Elisabeth C. Robinson,* MD, Vijay B. Thangamani, MD, Michael A. Kuhn, MD, and Glen Ross, MD Investigation performed
Arthroscopic Findings After Traumatic Shoulder Instability in Patients Older Than 35 Years Elisabeth C. Robinson,* MD, Vijay B. Thangamani, MD, Michael A. Kuhn, MD, and Glen Ross, MD Investigation performed