Research Article Ultrasonographic Validation of Anatomical Landmarks for Localization of the Tendon of the Long Head of Biceps Brachii
|
|
|
- Byron Sutton
- 5 years ago
- Views:
Transcription
1 Hindawi BioMed Research International Volume 2017, Article ID , 5 pages Research Article Ultrasonographic Validation of Anatomical Landmarks for Localization of the Tendon of the Long Head of Biceps Brachii Saiyun Hou, 1 John Harrell, 1 and Sheng Li 2 1 Department of Physical Medicine and Rehabilitation, Baylor College of Medicine, Houston, TX, USA 2 Department of Physical Medicine and Rehabilitation, University of Texas Health Science Center-Houston, Houston, TX, USA Correspondence should be addressed to Sheng Li; sheng.li@uth.tmc.edu Received 15 October 2016; Accepted 19 January 2017; Published 12 February 2017 AcademicEditor:JohnT.W.Yeow Copyright 2017 Saiyun Hou et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Objectives. To establish anatomical landmarks for biceps tendon groove localization based on intrinsic anatomical relations and to validate the localization with ultrasonographic measurement. Design. Perspective, observational, single-blinded pilot study. Participants. 25 healthy male and female volunteers ages years. Methods. We used two anatomical landmarks, the medial epicondyle vertical line related landmark and the coracoid process landmark. The distance from the groove skin mark to the medial epicondyle vertical line and the coracoid process was measured horizontally and was measured at 0 and 45 of shoulder external rotation, respectively. Results. Medial epicondyle vertical lines were 9.3 mm/21.5 mm medial to the groove at 0 /45 of shoulder external rotation, respectively. Correlation coefficients were 0.04/0.10, 0.32/0.42, and 0.26/0.37 for weight, height, and BMI in 0 /45 of shoulder external rotation, respectively. The distance between the coracoid process and the groove was 44.0 mm/62.2 mm in 0 /45 of shoulder external rotation, respectively. Correlation coefficients were 0.36/0.41, 0.36/0.54, and 0.18/0.12 for weight, height, and BMI in 0 /45 of shoulder external rotation, respectively. Conclusions. The medial epicondyle vertical line and the coracoid process landmark are both useful anatomical landmarks to localize the biceps groove. The anatomical landmark based localization is essentially not correlated with subject s weight, height, or BMI. 1. Introduction The long biceps tendon arises mainly from the supraglenoid tubercle and partly from the superior glenoid labrum, passes through the glenohumeral joint, and enters the intertubercular groove. Its intra-articular and extra-articular portions are stabilized by a series of soft-tissue restraints arising from the coracohumeral ligament, superior glenohumeral ligament, and supraspinatus and subscapularis tendons [1]. Pathologies of the long head of the biceps tendon (LHBT) present an important source of shoulder pain, often causing significant losses in this joint flexion. Isolated disorders of LHBT include tendinopathy, dislocation, and partial or complete tears. LHBT tendinopathy is generally due to inflammatory, traumatic, and degenerative causes related to overuse, becoming chronic in most cases [2]. Also it is commonly accompanied by shoulder pathology such as rotator cuff dysfunction, scapular dyskinesis, adhesive capsulitis, glenohumeral joint arthritis, SLAP (superior labrum anterior to posterior) lesions, or supraspinatus tendinosis [3 5]. A few studies [6 9] have found a close relationship between rotator cuff tears and associated injuries produced in LHBT. Disorders of the LHBT areassociatedwithrotatorcufftearinupto90%ofcases [6, 8]. Physical examination is unreliable in the diagnosis of LHBT pathology. Local anesthetic or steroid injection into the biceps long head tendon sheath is commonly used for diagnosis and treatment. Ultrasonography is preferred for visualizing the LHBT. However, it has a disadvantage of machine use and being time consuming. Long head of bicepspalpationattheleveloftheintertuberculargroove not only plays a central role in the physical examination of patients who present with anterior shoulder pain but is also the primary means of localization for biceps tendon sheath injections. Unfortunately, only approximately 5.3% overall accurate rate of long head of biceps groove palpation was reported in 25 examiners including attending physicians, fellows, and residents [10]. In this study we developed two anatomical landmarks, medial related vertical line, and
 was marked under ultrasound guidance (c). coracoid related landmarks which are based on intrinsic anatomical relations.")


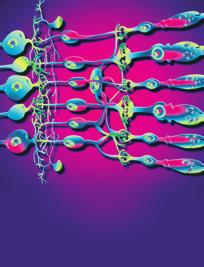
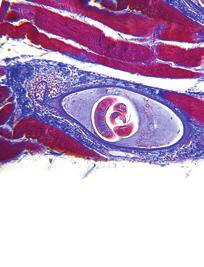
2 2 BioMed Research International (a) (b) (c) Figure 1: Biceps long head tendon groove (arrow) in the neutral position (a) and 45 of shoulder external rotation (b) was marked under ultrasound guidance. Coracoid process (arrowhead) was marked under ultrasound guidance (c). coracoid related landmarks which are based on intrinsic anatomical relations. The relationship between those two landmarks and LHBT is consistent and reliable. The purpose of the present study was to introduce these two anatomical landmarks for localization of biceps tendon groove and to validate the localization with ultrasonographic measurement. 2. Methods 2.1. Design. The perspective, observational study was completed in a tertiary care center at an academic institution. All of participants were blinded to study. Two anatomical landmarks were developed to localize LHBT groove and localization was validated with ultrasonographic measurement Participants. Participants were recruited on a volunteer basis through word of mouth and posters. Participants were included if they are healthy adults between 18 and 64 years old. Exclusion criteria were those who (1) had a history of shoulder pain or injury and those of shoulder surgical intervention; of biceps tendinitis or injury; or of shoulder joint chronic pathology, including but not limited to such issues as osteoarthritis, Rheumatologic, or autoimmune disorders and (2) were pregnant or lactating. Each participant s height, weight,andcalculatedbmiwererecorded Ethic Statement. The study protocol (H36580) was approved by the local Institutional Review Board and was conductedatasingle-siterehabilitationcenterinanurban tertiary academic medical center. Written informed consent was obtained from all patients before enrollment into the study Equipment. All ultrasound scans were performed on a Philips iu22 ultrasound machine with a 12 5 MHz linear array transducer (Philips Ultrasound Systems, Bothell, WA). The measurement was performed with an electronic digital caliber (NEIKO TOOLS, Gardena, CA). A 90 angle rule was usedtomarkthesiteofmedialepicondyleverticallineat intertubercular groove for each participant Procedures. Left shoulder was used to complete the study to standardize the procedure. After obtaining informed consent, age, weight, and height of the subject were recorded by a study coinvestigator. Two anatomical landmarks were used to localize the LHBT. (1) Medial Epicondyle Vertical Line Related Landmark. Participants stood upright with the shoulder in the neutral position (0 ), the elbow at 90 of flexion, and the forearm in the neutral position between pronation and supination. Firstly the biceps long head tendon groove was marked under ultrasound guidance (Figure 1(a)). Then a vertical line was drawn to pass through medial epicondyle of humerus and perpendicular to the ground with a 90 angle rule (Figure 2). The line to where the vertical line passed through anterior shoulder at the biceps groove level was marked. The distance from biceps long head tendon groove to the vertical line was measured horizontally with a digital caliper. Then participants changed their shoulder position to 45 of shoulder external rotation. The above procedure was repeated and the distance from biceps long head groove to the vertical line was measured again horizontally with a digital caliper (Figure 1(b)). (2) Coracoid Process Landmark. Participantsstoodupright with the shoulder in the neutral position (0 ), the elbow at 90 of flexion, and the forearm in the neutral position between pronation and supination. The coracoid process and biceps long head tendon groove were marked under ultrasound guidance (Figure 1(c)). The distance of the coracoid process
and 45 of shoulder external rotation (c).")
 Coracoid process (A), intertubercular groove in 0 (B), and 45 (C) of shoulder external rotation were marked with ultrasound.")
.")

3 BioMed Research International 3 (a) (b) (c) Figure 2: (a) Black line represents a vertical line passing through the medial epicondyle of humerus and perpendicular to ground. Black dot represents the intertubercular groove. Medial epicondyle related landmark was marked with a 90 anglerulerintheneutralposition(b)and 45 of shoulder external rotation (c). (a) (b) Figure 3: (a) Black line represents the distance between the coracoid process and the intertubercular groove. (b) Coracoid process (A), intertubercular groove in 0 (B), and 45 (C) of shoulder external rotation were marked with ultrasound. The distance of the coracoid process and the biceps long head tendon groove was measured horizontally between A and B or C at the coracoid level. and the biceps long head tendon groove was measured horizontally with a digital caliper at the coracoid level (Figure 3). The above procedure was repeated when participant s arm waskeptat45 of shoulder external rotation. The distance of thecoracoidprocessandthebicepslongheadtendongroove was measured with a digital caliper at 45 of shoulder external rotation Data Analysis. Mean and 95% confidence interval (CI) of the distance measured at 0 and 45 of shoulder external rotation were calculated for those two anatomical landmarks, respectively. Also correlation coefficients between height, weight, and body mass index (BMI) and those two anatomical landmarks related measurement were calculated. 3. Results 25 healthy volunteers (16 female and 9 male; years of age; mean, 29.5 ± 5.4 years) had body mass index (BMI) of (mean, 23.2 ± 3.7). According to American CDC BMIclassificationcriteria,thissampleincluded19normal weight subjects (BMI ), 1 underweight subjects (BMI < 18.5), and 5 overweight subjects (BMI ). All anatomic landmarks were identified under ultrasound guidance in all subjects. All medial epicondyle vertical lines were medial to the biceps groove at both 0 and 45 of shoulder external rotation. The horizontal distance between the biceps groove and medial epicondyle vertical line was found to be 9.3 mm (95% CI, 6.8 to 11.8) and 21.5 mm (95% CI, 18.9 to 24.1) in 0 and 45 of shoulder external rotation, respectively. Correlation coefficients were 0.04/0.10, 0.32/0.42, and 0.26/0.37 for weight, height, and BMI in 0 /45 of shoulder external rotation, respectively (Table 1). The horizontal distance between the coracoid process and the biceps tendon groove was found to be 44.0 mm (95% CI, 41.5 to 46.5) and 62.2 mm (95% CI, 59.2 to 65.2) in 0 and 45 of shoulder external rotation, respectively. Correlation coefficients were 0.36, 0.36, and 0.18 for weight, height, and
4 4 BioMed Research International Table 1: Medial epicondyle vertical line related landmark: average distance between the biceps groove and medial epicondyle vertical line were measured at 0 and 45 external rotation. Correlation coefficients between the distance and weight, height, and BMI were calculated at 0 and 45 of shoulder external rotation. CC: correlation coefficients. BMI: body mass index. Average distance (95% CI) and weight and height and BMI 0 neural position 9.3 mm ( ) external rotation 21.5 mm ( ) Table 2: Coracoid process landmark: average distance between biceps groove and coracoid process were measured at 0 and 45 external rotation. Correlation coefficients between the distance and weight, height, and BMI were calculated at 0 and 45 external rotation. CC: correlation coefficients. BMI: body mass index. Average distance (95% CI) and weight and height and BMI 0 neural position 44.0 mm ( ) external rotation 62.2 mm ( ) BMI in 0 neutral position, respectively. At 45 of shoulder external rotation, correlation coefficients were 0.41, 0.54, and 0.12 for weight, height, and BMI, respectively (Table 2). Collectively, the results support the intrinsic anatomical relations between these landmarks and the LHBT groove. 4. Discussion The long head of the biceps tendon (LHBT) can be a source of pain or shoulder dysfunction [11]. Local anesthetic or steroid injection into the biceps long head tendon sheath is commonly used for diagnosis and treatment. Identifying the biceps tendon as a pain generator in patients presenting with shoulder pain syndromes has significant and diagnostic and therapeutic implications. An accurate and complete diagnosis facilitates optimal treatment [12]. Inthestudydescribedherein,twoanatomiclandmarks for biceps tendon identification were used and their relationships to LHBT within the intertubercular groove were evaluated. The medial epicondyle vertical line lies approximately 1 centimeter medial to the biceps groove when the shoulder is in the neutral position and about 2 centimeters when shoulder is at 45 of external rotation. The coracoid process landmark lies approximately 4.4 centimeters when the shoulder is in the neutral position, about 6.2 centimeters when the shoulder is at 45 of external rotation. Therefore, these two anatomical landmarks are effective for LHBT identification and can be performed easily in an outpatient setting. The relationship between the observed landmarks and the LHBT is rooted in intrinsic anatomical relations among them. The medial epicondyle of the humerus is a bony protrusion located on the medial side of distal humerus (Figure 2). The relationship among them is consistent and reliable. Given this intrinsic relation, this anatomical landmark based localization is not correlated with subject s weight, height, or BMI. The coracoid process is a small hook-like structure on the lateral edge of the superior anterior portion of the scapula. It is localized in the deltopectoral groove between thedeltoidandpectoralismajormuscles.thereiscertain intrinsic relation between coracoid process and intertubercular groove. Glenohumeral joint subluxation, dislocation, or effusion may change this relationship. Physician should be aware of it when patient has the comorbidity of GH joint pathology. Given this intrinsic relation, coracoid related landmark is not correlated with subject s weight or BMI. The heighthasthemoderatecorrelationtothedistancemeasured in 45 of shoulder external rotation, but no correlation in 0 of shoulder external rotation. Therefore we recommend that physicians localize the LHBT in the neutral position of shoulder when measuring with coracoid process related landmark. The two anatomical landmarks introduced in this study were developed to identify the localization of LHBT within theintertuberculargroove.thelocalizationwasvalidated with ultrasonographic measurement. Correlation between the distance and weight, height, and BMI increased when shoulder externally rotated to 45 degree compared with the neutral position for these two landmarks. We recommend that the neutral position of shoulder is a better way to localize the LHBT. 5. Limitations Firstly, although 25 subjects were conducted for this pilot study, further study including increased sample size could help improve the accuracy of the measurements and increase its generalisability. Secondly, this measurement is reliable only if the coracoid process, LHBT, and medial epicondyle of humerus and LHBT are intact as was the case in our subjects. If the coracoid process and medial epicondyle of humerus arefracturedorthelhbtisdislocated,thesemeasurements cannotprovideguidanceaboutwherethelhbtmaybe found. Thirdly, intraobserver and interobserver error were not included because all measurements were made by one author.
5 BioMed Research International 5 6. Conclusion We used two new anatomical landmarks for biceps tendon groovelocalization.themedialepicondyleverticallineisa useful anatomical landmark to localize the biceps groove. It lies approximately 1 centimeter medial to the biceps groove when the shoulder is in the neutral position and about 2 centimeters when shoulder is at 45 degrees of external rotation. This anatomical landmark based localization is not correlated with subject s weight, height, or BMI. The coracoid process landmark is also a useful anatomical landmark to localize the biceps groove. It lies approximately 4.4 centimeters when the shoulder is in the neutral position, about 6.2 centimeters when the shoulder is at 45 degree of external rotation. No correlation exists between the distance to the biceps groove and weight, height, or BMI in 0 of shoulder external rotation, whereas a moderate correlation with height exists in 45 of shoulder external rotation. Those two anatomical landmarks allow for efficient and safe identification of the tendon of the long head of biceps brachii when examining or injection. Abbreviations BMI: Bone mass index CI: Confidence interval LHBT: Long head of the biceps tendon GH: Glenohumeral joint SLAP: Superior labrum anterior to posterior. Competing Interests The authors declare that they have no competing interests. [6]D.P.Beall,E.E.Williamson,J.Q.Lyetal., Associationof biceps tendon tears with rotator cuff abnormalities: degree of correlation with tears of the anterior and superior portions of the rotator cuff, AmericanJournalofRoentgenology,vol.180, no. 3, pp , [7] C.-H. Chen, K.-Y. Hsu, W.-J. Chen, and C.-H. Shih, Incidence and severity of biceps long head tendon lesion in patients with complete rotator cuff tears, JournalofTrauma Injury, Infection and Critical Care,vol.58,no.6,pp ,2005. [8] A. M. Murthi, C. L. Vosburgh, and T. J. Neviaser, The incidence of pathologic changes of the long head of the biceps tendon, Shoulder and Elbow Surgery,vol.9,no.5,pp , [9] C.D.Peltz,J.E.Hsu,M.H.Zgonis,N.A.Trasolini,D.L.Glaser, and L. J. Soslowsky, The effect of altered loading following rotator cuff tears in a rat model on the regional mechanical properties of the long head of the biceps tendon, Biomechanics,vol.43,no.15,pp ,2010. [10] G. P. Gazzillo, J. T. Finnoff, M. M. Hall, Y. A. Sayeed, and J. Smith, Accuracy of palpating the long head of the biceps tendon: an ultrasonographic study, PM&R, vol. 3, no. 11, pp , [11] F. Elser, S. Braun, C. B. Dewing, J. E. Giphart, and P. J. Millett, Anatomy, function, injuries, and treatment of the long head of the biceps brachii tendon, Arthroscopy Arthroscopic and Related Surgery,vol.27,no.4,pp ,2011. [12] M. Zanetti, D. Weishaupt, C. Gerber, and J. Hodler, Tendinopathy and rupture of the tendon of the long head of the biceps brachii muscle: evaluation with MR arthrography, American Roentgenology,vol.170,no.6,pp ,1998. Acknowledgments This study was supported in part by NIH NICHD/NCMRR 1R21HD References [1] P.Habermeyer,P.Magosch,M.Pritsch,M.T.Scheibel,andS. Lichtenberg, Anterosuperior impingement of the shoulder as a result of pulley lesions: A Prospective Arthroscopic Study, Shoulder and Elbow Surgery, vol.13,no.1,pp.5 12, [2] U.G.Longo,M.Loppini,G.Marineo,W.S.Khan,N.Maffulli, and V. Denaro, Tendinopathy of the tendon of the long head of the biceps, Sports Medicine and Arthroscopy Review, vol. 19,no. 4, pp , [3] M. Khazzam, M. S. George, R. S. Churchill, and J. E. Kuhn, Disorders of the long head of biceps tendon, Shoulder and Elbow Surgery,vol.21,no.1,pp ,2012. [4]M.I.HarwoodandC.T.Smith, Superiorlabrum,anteriorposterior lesions and biceps injuries: diagnostic and treatment considerations, Primary Care: Clinics in Office Practice,vol.31, no.4,pp ,2004. [5] C.D.Peltz,S.M.Perry,C.L.Getz,andL.J.Soslowsky, Mechanical properties of the long-head of the biceps tendon are altered in the presence of rotator cuff tears in a rat model, Orthopaedic Research, vol. 27, no. 3, pp , 2009.









6 MEDIATORS of INFLAMMATION The Scientific World Journal Gastroenterology Research and Practice Diabetes Research International Endocrinology Immunology Research Disease Markers Submit your manuscripts at BioMed Research International PPAR Research Obesity Ophthalmology Evidence-Based Complementary and Alternative Medicine Stem Cells International Oncology Parkinson s Disease Computational and Mathematical Methods in Medicine AIDS Behavioural Neurology Research and Treatment Oxidative Medicine and Cellular Longevity
Case Report Intra-Articular Entrapment of the Medial Epicondyle following a Traumatic Fracture Dislocation of the Elbow in an Adult
 Hindawi Case Reports in Orthopedics Volume 2018, Article ID 5401634, 6 pages https://doi.org/10.1155/2018/5401634 Case Report Intra-Articular Entrapment of the Medial Epicondyle following a Traumatic Fracture
Hindawi Case Reports in Orthopedics Volume 2018, Article ID 5401634, 6 pages https://doi.org/10.1155/2018/5401634 Case Report Intra-Articular Entrapment of the Medial Epicondyle following a Traumatic Fracture
Shoulder Joint Examination. Shoulder Joint Examination. Inspection. Inspection Palpation Movement. Look Feel Move
 Shoulder Joint Examination History Cuff Examination Instability Examination AC Joint Examination Biceps Tendon Examination Superior Labrum Examination Shoulder Joint Examination Inspection Palpation Movement
Shoulder Joint Examination History Cuff Examination Instability Examination AC Joint Examination Biceps Tendon Examination Superior Labrum Examination Shoulder Joint Examination Inspection Palpation Movement
Case Report Medial Radial Head Dislocation Associated with a Proximal Olecranon Fracture: A Bado Type V?
 Case Reports in Surgery, Article ID 723756, 4 pages http://dx.doi.org/10.1155/2014/723756 Case Report Medial Radial Head Dislocation Associated with a Proximal Olecranon Fracture: A Bado Type V? Neil Segaren,
Case Reports in Surgery, Article ID 723756, 4 pages http://dx.doi.org/10.1155/2014/723756 Case Report Medial Radial Head Dislocation Associated with a Proximal Olecranon Fracture: A Bado Type V? Neil Segaren,
Arthroscopic Evaluation of Subluxation of the Long Head of the Biceps Tendon and Its Relationship with Subscapularis Tears
 Original Article Clinics in Orthopedic Surgery 2017;9:332-339 https://doi.org/10.4055/cios.2017.9.3.332 Arthroscopic Evaluation of Subluxation of the Long Head of the Biceps Tendon and Its Relationship
Original Article Clinics in Orthopedic Surgery 2017;9:332-339 https://doi.org/10.4055/cios.2017.9.3.332 Arthroscopic Evaluation of Subluxation of the Long Head of the Biceps Tendon and Its Relationship
Case Report Bilateral Congenital Agenesis of the Long Head of the Biceps Tendon: The Beginning
 Case Reports in Radiology Volume 2016, Article ID 4309213, 5 pages http://dx.doi.org/10.1155/2016/4309213 Case Report Bilateral Congenital Agenesis of the Long Head of the Biceps Tendon: The Beginning
Case Reports in Radiology Volume 2016, Article ID 4309213, 5 pages http://dx.doi.org/10.1155/2016/4309213 Case Report Bilateral Congenital Agenesis of the Long Head of the Biceps Tendon: The Beginning
Evidence Based Approach to Shoulder Injections
 Evidence Based Approach to Shoulder Injections Bradley Sandella, DO Christiana Care Sports Medicine Joseph Straight, MD First State Orthopaedics Objectives Relevant Anatomy Indications for injections Injection
Evidence Based Approach to Shoulder Injections Bradley Sandella, DO Christiana Care Sports Medicine Joseph Straight, MD First State Orthopaedics Objectives Relevant Anatomy Indications for injections Injection
The Shoulder. Anatomy and Injuries PSK 4U Unit 3, Day 4
 The Shoulder Anatomy and Injuries PSK 4U Unit 3, Day 4 Shoulder Girdle Shoulder Complex is the most mobile joint in the body. Scapula Clavicle Sternum Humerus Rib cage/thorax Shoulder Girdle It also includes
The Shoulder Anatomy and Injuries PSK 4U Unit 3, Day 4 Shoulder Girdle Shoulder Complex is the most mobile joint in the body. Scapula Clavicle Sternum Humerus Rib cage/thorax Shoulder Girdle It also includes
Case Report Successful Closed Reduction of a Lateral Elbow Dislocation
 Case Reports in Orthopedics Volume 2016, Article ID 5934281, 5 pages http://dx.doi.org/10.1155/2016/5934281 Case Report Successful Closed Reduction of a Lateral Elbow Dislocation Kenya Watanabe, Takuma
Case Reports in Orthopedics Volume 2016, Article ID 5934281, 5 pages http://dx.doi.org/10.1155/2016/5934281 Case Report Successful Closed Reduction of a Lateral Elbow Dislocation Kenya Watanabe, Takuma
FUNCTIONAL ANATOMY OF SHOULDER JOINT
 FUNCTIONAL ANATOMY OF SHOULDER JOINT ARTICULATION Articulation is between: The rounded head of the Glenoid cavity humerus and The shallow, pear-shaped glenoid cavity of the scapula. 2 The articular surfaces
FUNCTIONAL ANATOMY OF SHOULDER JOINT ARTICULATION Articulation is between: The rounded head of the Glenoid cavity humerus and The shallow, pear-shaped glenoid cavity of the scapula. 2 The articular surfaces
Shoulder Instability. Fig 1: Intact labrum and biceps tendon
 Shoulder Instability What is it? The shoulder joint is a ball and socket joint, with the humeral head (upper arm bone) as the ball and the glenoid as the socket. The glenoid (socket) is a shallow bone
Shoulder Instability What is it? The shoulder joint is a ball and socket joint, with the humeral head (upper arm bone) as the ball and the glenoid as the socket. The glenoid (socket) is a shallow bone
Practical 2 Worksheet
 Practical 2 Worksheet Upper Extremity BONES 1. Which end of the clavicle is on the lateral side (acromial or sternal)? 2. Describe the difference in the appearance of the acromial and sternal ends of the
Practical 2 Worksheet Upper Extremity BONES 1. Which end of the clavicle is on the lateral side (acromial or sternal)? 2. Describe the difference in the appearance of the acromial and sternal ends of the
Ultrasound of the Shoulder
 Ultrasound of the Shoulder Patrick Battaglia, DC, DACBR Logan University, Department of Radiology Outline Review ultrasound appearance of NMSK tissues Present indications for ultrasound of the shoulder.
Ultrasound of the Shoulder Patrick Battaglia, DC, DACBR Logan University, Department of Radiology Outline Review ultrasound appearance of NMSK tissues Present indications for ultrasound of the shoulder.
MUSCLES OF SHOULDER REGION
 Dr Jamila EL Medany OBJECTIVES At the end of the lecture, students should: List the name of muscles of the shoulder region. Describe the anatomy of muscles of shoulder region regarding: attachments of
Dr Jamila EL Medany OBJECTIVES At the end of the lecture, students should: List the name of muscles of the shoulder region. Describe the anatomy of muscles of shoulder region regarding: attachments of
SHOULDER JOINT ANATOMY AND KINESIOLOGY
 SHOULDER JOINT ANATOMY AND KINESIOLOGY SHOULDER JOINT ANATOMY AND KINESIOLOGY The shoulder joint, also called the glenohumeral joint, consists of the scapula and humerus. The motions of the shoulder joint
SHOULDER JOINT ANATOMY AND KINESIOLOGY SHOULDER JOINT ANATOMY AND KINESIOLOGY The shoulder joint, also called the glenohumeral joint, consists of the scapula and humerus. The motions of the shoulder joint
1. The coordinated action of a scapular upward rotation and humeral abduction is known as the:
 1 1. The coordinated action of a scapular upward rotation and humeral abduction is known as the: a. Carrying angle of the arm b. Scapulohumeral rhythm c. Glenohumeral capsular pattern d. Abduction resistance
1 1. The coordinated action of a scapular upward rotation and humeral abduction is known as the: a. Carrying angle of the arm b. Scapulohumeral rhythm c. Glenohumeral capsular pattern d. Abduction resistance
Anatomical Considerations/ Pathophysiology The shoulder is the most mobile joint in the body. : Three bones:
 Introduction Musculoskeletal training is generally underrepresented in medical training and residency curriculums. There is a general deficit in musculoskeletal knowledge amongst current medical students,
Introduction Musculoskeletal training is generally underrepresented in medical training and residency curriculums. There is a general deficit in musculoskeletal knowledge amongst current medical students,
11/15/2017. Biceps Lesions. Highgate Private Hospital (Whittington Health NHS Trust) E: LHB Anatomy.
 E: LHB Anatomy.") Biceps Lesions Mr Omar Haddo (Consultant Orthopaedic Surgeon MBBS, BmedSci, FRCS(Orth) ) Highgate Private Hospital (Whittington Health NHS Trust) E: admin@denovomedic.co.uk LHB Anatomy Arise from superior
Biceps Lesions Mr Omar Haddo (Consultant Orthopaedic Surgeon MBBS, BmedSci, FRCS(Orth) ) Highgate Private Hospital (Whittington Health NHS Trust) E: admin@denovomedic.co.uk LHB Anatomy Arise from superior
Case Report Reverse Segond Fracture Associated with Anteromedial Tibial Rim and Tibial Attachment of Anterior Cruciate Ligament Avulsion Fractures
 Hindawi Case Reports in Orthopedics Volume 2017, Article ID 9637153, 4 pages https://doi.org/10.1155/2017/9637153 Case Report Reverse Segond Fracture Associated with Anteromedial Tibial Rim and Tibial
Hindawi Case Reports in Orthopedics Volume 2017, Article ID 9637153, 4 pages https://doi.org/10.1155/2017/9637153 Case Report Reverse Segond Fracture Associated with Anteromedial Tibial Rim and Tibial
THE SHOULDER JOINT T H E G L E N O H U M E R A L ( G H ) J O I N T
 J O I N T") THE SHOULDER JOINT T H E G L E N O H U M E R A L ( G H ) J O I N T CLARIFICATION OF TERMS Shoulder girdle = scapula and clavicle Shoulder joint (glenohumeral joint) = scapula and humerus Lippert, p115
THE SHOULDER JOINT T H E G L E N O H U M E R A L ( G H ) J O I N T CLARIFICATION OF TERMS Shoulder girdle = scapula and clavicle Shoulder joint (glenohumeral joint) = scapula and humerus Lippert, p115
The Upper Limb II. Anatomy RHS 241 Lecture 11 Dr. Einas Al-Eisa
 The Upper Limb II Anatomy RHS 241 Lecture 11 Dr. Einas Al-Eisa Sternoclavicular joint Double joint.? Each side separated by intercalating articular disc Grasp the mid-portion of your clavicle on one side
The Upper Limb II Anatomy RHS 241 Lecture 11 Dr. Einas Al-Eisa Sternoclavicular joint Double joint.? Each side separated by intercalating articular disc Grasp the mid-portion of your clavicle on one side
Case Report Calcific Tendonitis of the Rotator Cuff: An Unusual Case
 Case Reports in Orthopedics Volume 2012, Article ID 806769, 4 pages doi:10.1155/2012/806769 Case Report Calcific Tendonitis of the Rotator Cuff: An Unusual Case Yasuhiro Mitsui, 1 Masafumi Gotoh, 1 Ryo
Case Reports in Orthopedics Volume 2012, Article ID 806769, 4 pages doi:10.1155/2012/806769 Case Report Calcific Tendonitis of the Rotator Cuff: An Unusual Case Yasuhiro Mitsui, 1 Masafumi Gotoh, 1 Ryo
7/31/2012 THE SHOULDER JOINT CLARIFICATION OF TERMS OSTEOLOGY OF THE GH JOINT(BONES)
") THE SHOULDER JOINT T H E G L E N O H U M E R AL ( G H ) J O I N T CLARIFICATION OF TERMS Shoulder girdle = scapula and clavicle Shoulder joint (glenohumerual joint) = scapula and Lippert, p115 OSTEOLOGY
THE SHOULDER JOINT T H E G L E N O H U M E R AL ( G H ) J O I N T CLARIFICATION OF TERMS Shoulder girdle = scapula and clavicle Shoulder joint (glenohumerual joint) = scapula and Lippert, p115 OSTEOLOGY
Labral Tears. Fig 1: Intact labrum and biceps tendon
 Labral Tears What is it? The shoulder joint is a ball and socket joint, with the humeral head (upper arm bone) as the ball and the glenoid as the socket. The glenoid (socket) is a shallow bone that is
Labral Tears What is it? The shoulder joint is a ball and socket joint, with the humeral head (upper arm bone) as the ball and the glenoid as the socket. The glenoid (socket) is a shallow bone that is
SHOULDER INSTABILITY
 SHOULDER INSTABILITY Dr.KN Subramanian M.Ch Orth., FRCS (Tr & Orth), CCT Orth(UK) Consultant Orthopaedic Surgeon, Special interest: Orthopaedic Sports Injury, Shoulder and Knee Surgery, SPARSH Hospital
SHOULDER INSTABILITY Dr.KN Subramanian M.Ch Orth., FRCS (Tr & Orth), CCT Orth(UK) Consultant Orthopaedic Surgeon, Special interest: Orthopaedic Sports Injury, Shoulder and Knee Surgery, SPARSH Hospital
4/12/2016. Goals. Anatomy. Basic Anatomy. Biomechanics. Function. Traumatic Rupture of Proximal Biceps: In-season Rehabilitation and Management
 Goals Traumatic Rupture of Proximal Biceps: In-season Rehabilitation and Management Thomas F. LaPorta, MD To understand the anatomy of the biceps at the shoulder To present the mechanism, signs and symptoms,
Goals Traumatic Rupture of Proximal Biceps: In-season Rehabilitation and Management Thomas F. LaPorta, MD To understand the anatomy of the biceps at the shoulder To present the mechanism, signs and symptoms,
Incorporating OMM to Enhance Your Clinical Practice Osteopathic diagnosis and approach to the upper extremity
 Incorporating OMM to Enhance Your Clinical Practice Osteopathic diagnosis and approach to the upper extremity Sheldon C. Yao, D.O. Acting Department Chair March 1, 2013 Clinical significance Upper extremity
Incorporating OMM to Enhance Your Clinical Practice Osteopathic diagnosis and approach to the upper extremity Sheldon C. Yao, D.O. Acting Department Chair March 1, 2013 Clinical significance Upper extremity
Fumiaki Takase, Atsuyuki Inui, Yutaka Mifune, Tomoyuki Muto, Yoshifumi Harada, Takeshi Kokubu, and Masahiro Kurosaka
 Case Reports in Orthopedics, Article ID 312968, 4 pages http://dx.doi.org/10.1155/2014/312968 Case Report Concurrent Rotator Cuff Tear and Axillary Nerve Palsy Associated with Anterior Dislocation of the
Case Reports in Orthopedics, Article ID 312968, 4 pages http://dx.doi.org/10.1155/2014/312968 Case Report Concurrent Rotator Cuff Tear and Axillary Nerve Palsy Associated with Anterior Dislocation of the
Proximal Biceps Tendon and Rotator Cuff Tears
 Proximal Biceps Tendon and Rotator Cuff Tears Mandeep S. Virk, MD a, Brian J. Cole, MD, MBA b, * KEYWORDS Biceps tenotomy Biceps tenodesis Rotator cuff tears KEY POINTS Long head of the biceps is commonly
Proximal Biceps Tendon and Rotator Cuff Tears Mandeep S. Virk, MD a, Brian J. Cole, MD, MBA b, * KEYWORDS Biceps tenotomy Biceps tenodesis Rotator cuff tears KEY POINTS Long head of the biceps is commonly
APPROPRIATE USE GUIDELINES
 APPROPRIATE USE GUIDELINES Appropriateness of Advanced Imaging Procedures (MRI, CT, Bone Scan/PET) in Patients with Shoulder Pain CDI QUALITY INSTITUTE: PROVIDER LED ENTITY (PLE) Compiled by Rob Liddell,
APPROPRIATE USE GUIDELINES Appropriateness of Advanced Imaging Procedures (MRI, CT, Bone Scan/PET) in Patients with Shoulder Pain CDI QUALITY INSTITUTE: PROVIDER LED ENTITY (PLE) Compiled by Rob Liddell,
Rotator Cuff and Biceps Pathology
 Rotator Cuff and Biceps Pathology Jon A. Jacobson, M.D. Professor of Radiology Director, Division of Musculoskeletal Radiology University of Michigan Disclosures: Consultant: Bioclinica Advisory Board:
Rotator Cuff and Biceps Pathology Jon A. Jacobson, M.D. Professor of Radiology Director, Division of Musculoskeletal Radiology University of Michigan Disclosures: Consultant: Bioclinica Advisory Board:
SHOULDER ANATOMY Karl Wieser, MD Department of Orthopedics, University of Zurich, Balgrist, Switzerland
 20th Course in Shoulder Surgery Balgrist SHOULDER ANATOMY Karl Wieser, MD Department of Orthopedics, University of Zurich, Balgrist, Switzerland www.balgrist.ch ANATOMY OVERVIEW courtesy of Georg Lajtai
20th Course in Shoulder Surgery Balgrist SHOULDER ANATOMY Karl Wieser, MD Department of Orthopedics, University of Zurich, Balgrist, Switzerland www.balgrist.ch ANATOMY OVERVIEW courtesy of Georg Lajtai
Musculoskeletal Ultrasound. Technical Guidelines SHOULDER
 Musculoskeletal Ultrasound Technical Guidelines SHOULDER 1 Although patient s positioning for shoulder US varies widely across different Countries and Institutions reflecting multifaceted opinions and
Musculoskeletal Ultrasound Technical Guidelines SHOULDER 1 Although patient s positioning for shoulder US varies widely across different Countries and Institutions reflecting multifaceted opinions and
I (and/or my co-authors) have something to disclose.
 have something to disclose.") Shoulder Anatomy And Biomechanics Nikhil N Verma, MD Director of Sports Medicine Professor, Department of Orthopedics Rush University Team Physician, Chicago White Sox and Bulls I (and/or my co-authors)
Shoulder Anatomy And Biomechanics Nikhil N Verma, MD Director of Sports Medicine Professor, Department of Orthopedics Rush University Team Physician, Chicago White Sox and Bulls I (and/or my co-authors)
Ultrasound-Guided Shoulder Injections 인제대학교일산백병원 재활의학과 임길병
 Ultrasound-Guided Shoulder Injections 인제대학교일산백병원 재활의학과 임길병 How to improve needle visibility Advantages of Ultrasound in Procedures Real-time imaging Avoids radiation exposure But, interventions without
Ultrasound-Guided Shoulder Injections 인제대학교일산백병원 재활의학과 임길병 How to improve needle visibility Advantages of Ultrasound in Procedures Real-time imaging Avoids radiation exposure But, interventions without
MRI of the long head of the biceps tendon: a pictorial review.
 MRI of the long head of the biceps tendon: a pictorial review. Poster No.: C-1861 Congress: ECR 2014 Type: Educational Exhibit Authors: P. Dewachter, L. Dewachter, A. P. Parkar ; Lier/BE, Bergen/ NO Keywords:
MRI of the long head of the biceps tendon: a pictorial review. Poster No.: C-1861 Congress: ECR 2014 Type: Educational Exhibit Authors: P. Dewachter, L. Dewachter, A. P. Parkar ; Lier/BE, Bergen/ NO Keywords:
Shoulder Arthroscopy Portals
 Shoulder Arthroscopy Portals Alper Deveci and Metin Dogan 7 7.1 Bony Landmarks Before starting shoulder arthroscopy, the patient must be positioned and draping applied. Then the bony landmarks are identified
Shoulder Arthroscopy Portals Alper Deveci and Metin Dogan 7 7.1 Bony Landmarks Before starting shoulder arthroscopy, the patient must be positioned and draping applied. Then the bony landmarks are identified
Research Article Relationship between Pain and Medial Meniscal Extrusion in Knee Osteoarthritis
 Advances in Orthopedics Volume 2015, Article ID 210972, 4 pages http://dx.doi.org/10.1155/2015/210972 Research Article Relationship between Pain and Medial Meniscal Extrusion in Knee Osteoarthritis Hiroaki
Advances in Orthopedics Volume 2015, Article ID 210972, 4 pages http://dx.doi.org/10.1155/2015/210972 Research Article Relationship between Pain and Medial Meniscal Extrusion in Knee Osteoarthritis Hiroaki
Structure and Function of the Bones and Joints of the Shoulder Girdle
 Structure and Function of the Bones and Joints of the Shoulder Girdle LEARNING OBJECTIVES: At the end of this laboratory exercise the student will be able to: Palpate the important skeletal landmarks of
Structure and Function of the Bones and Joints of the Shoulder Girdle LEARNING OBJECTIVES: At the end of this laboratory exercise the student will be able to: Palpate the important skeletal landmarks of
MRI of the Shoulder What to look for and how to find it? Dr. Eric Handley Musculoskeletal Radiologist Cherry Creek Imaging
 MRI of the Shoulder What to look for and how to find it? Dr. Eric Handley Musculoskeletal Radiologist Cherry Creek Imaging MRI of the Shoulder Benefits of Ultrasound: * Dynamic * Interactive real time
MRI of the Shoulder What to look for and how to find it? Dr. Eric Handley Musculoskeletal Radiologist Cherry Creek Imaging MRI of the Shoulder Benefits of Ultrasound: * Dynamic * Interactive real time
Shoulder Injuries. Glenoid labrum injuries. SLAP Lesions
 Shoulder Injuries functional anatomy clinical perspective impingement rotator cuff injuries glenoid labrum injuries dislocation Glenoid labrum injuries SLAP lesions stable or unstable traction/compression
Shoulder Injuries functional anatomy clinical perspective impingement rotator cuff injuries glenoid labrum injuries dislocation Glenoid labrum injuries SLAP lesions stable or unstable traction/compression
Scapular and Deltoid Regions
 M1 Gross and Developmental Anatomy Scapular and Deltoid Regions Dr. Peters 1 Outline I. Skeleton of the Shoulder and Attachment of the Upper Extremity to Trunk II. Positions and Movements of the Scapula
M1 Gross and Developmental Anatomy Scapular and Deltoid Regions Dr. Peters 1 Outline I. Skeleton of the Shoulder and Attachment of the Upper Extremity to Trunk II. Positions and Movements of the Scapula
Superior Labrum Anterior Posterior lesions: ultrasound evaluation
 Superior Labrum Anterior Posterior lesions: ultrasound evaluation Poster No.: C-0472 Congress: ECR 2017 Type: Scientific Exhibit Authors: D. Belyaev; Yaroslavl/RU Keywords: Trauma, Arthrography, Ultrasound,
Superior Labrum Anterior Posterior lesions: ultrasound evaluation Poster No.: C-0472 Congress: ECR 2017 Type: Scientific Exhibit Authors: D. Belyaev; Yaroslavl/RU Keywords: Trauma, Arthrography, Ultrasound,
DK7215-Levine-ch12_R2_211106
 12 Arthroscopic Rotator Interval Closure Andreas H. Gomoll Department of Orthopedic Surgery, Brigham and Women s Hospital, Harvard Medical School, Boston, Massachusetts, U.S.A. Brian J. Cole Departments
12 Arthroscopic Rotator Interval Closure Andreas H. Gomoll Department of Orthopedic Surgery, Brigham and Women s Hospital, Harvard Medical School, Boston, Massachusetts, U.S.A. Brian J. Cole Departments
Shoulder and Elbow ORTHOPAEDIC SYPMPOSIUM APRIL 8, 2017 DANIEL DOTY MD
 Shoulder and Elbow ORTHOPAEDIC SYPMPOSIUM APRIL 8, 2017 DANIEL DOTY MD Shoulder Articulations Glenohumeral Joint 2/3 total arc of motion Shallow Ball and Socket Joint Allows for excellent ROM Requires
Shoulder and Elbow ORTHOPAEDIC SYPMPOSIUM APRIL 8, 2017 DANIEL DOTY MD Shoulder Articulations Glenohumeral Joint 2/3 total arc of motion Shallow Ball and Socket Joint Allows for excellent ROM Requires
The Shoulder. By Patrick Ryan, Bobby Law, Jack Beaty, Alex Newhouse and Chuck Nelson
 The Shoulder By Patrick Ryan, Bobby Law, Jack Beaty, Alex Newhouse and Chuck Nelson Learning Objectives/Agenda Review the anatomy of the shoulder Describe the main diseases of the shoulder Describe the
The Shoulder By Patrick Ryan, Bobby Law, Jack Beaty, Alex Newhouse and Chuck Nelson Learning Objectives/Agenda Review the anatomy of the shoulder Describe the main diseases of the shoulder Describe the
Joint G*H. Joint S*C. Joint A*C. Labrum. Humerus. Sternum. Scapula. Clavicle. Thorax. Articulation. Scapulo- Thoracic
 A*C Joint Scapulo- Thoracic Articulation Thorax Sternum Clavicle Scapula Humerus S*C Joint G*H Joint Labrum AC Ligaments SC Ligaments SC JOINT AC Coracoacromial GH GH Ligament Complex Coracoclavicular
A*C Joint Scapulo- Thoracic Articulation Thorax Sternum Clavicle Scapula Humerus S*C Joint G*H Joint Labrum AC Ligaments SC Ligaments SC JOINT AC Coracoacromial GH GH Ligament Complex Coracoclavicular
The suction cup mechanism is enhanced by the slightly negative intra articular pressure within the joint.
 SHOULDER INSTABILITY Stability A. The stability of the shoulder is improved by depth of the glenoid. This is determined by: 1. Osseous glenoid, 2. Articular cartilage of the glenoid, which is thicker at
SHOULDER INSTABILITY Stability A. The stability of the shoulder is improved by depth of the glenoid. This is determined by: 1. Osseous glenoid, 2. Articular cartilage of the glenoid, which is thicker at
Stefan C Muzin, MD PM&R Attending Physician, Beth Israel Deaconess Medical Center, Harvard Medical School Onsite Physiatrist, GE Aviation, Lynn, MA
 Stefan C Muzin, MD PM&R Attending Physician, Beth Israel Deaconess Medical Center, Harvard Medical School Onsite Physiatrist, GE Aviation, Lynn, MA Consultant, OEHN (Occupational and Environmental Network)
Stefan C Muzin, MD PM&R Attending Physician, Beth Israel Deaconess Medical Center, Harvard Medical School Onsite Physiatrist, GE Aviation, Lynn, MA Consultant, OEHN (Occupational and Environmental Network)
Chronic Shoulder Disorders
 Chronic Shoulder Disorders Dr. Mustafa Elsingergy Consultant orthopedic surgeon Dallah Hospita Prof. Mamoun Kremli Almaarefa Medical College Contents INTRINSIC Shoulder Pain Due to causes in the shoulder
Chronic Shoulder Disorders Dr. Mustafa Elsingergy Consultant orthopedic surgeon Dallah Hospita Prof. Mamoun Kremli Almaarefa Medical College Contents INTRINSIC Shoulder Pain Due to causes in the shoulder
ORTHOPAEDIC INJECTION AND ASPIRATION TECHNIQUES
 ORTHOPAEDIC INJECTION AND ASPIRATION TECHNIQUES OAAPN October 20, 2016 David H. Sohn, JD MD Chief, Shoulder and Sports Medicine University of Toledo Medical Center When to aspirate? To rule out infection
ORTHOPAEDIC INJECTION AND ASPIRATION TECHNIQUES OAAPN October 20, 2016 David H. Sohn, JD MD Chief, Shoulder and Sports Medicine University of Toledo Medical Center When to aspirate? To rule out infection
Rotator Cuff Repair TRENDS OF REPAIRS. Evolution of Arthroscopic Repair. Shoulder Girdle. Rotator Cuff Repair 8/29/2013
 Rotator Cuff Repair Indications, Patient Selection, Outcomes James C. Vailas, M.D. New Hampshire Orthopaedic Center September 14, 2013 New Hampshire Musculoskeletal Institute 20 th Annual Symposium Evolution
Rotator Cuff Repair Indications, Patient Selection, Outcomes James C. Vailas, M.D. New Hampshire Orthopaedic Center September 14, 2013 New Hampshire Musculoskeletal Institute 20 th Annual Symposium Evolution
Case Report An Undescribed Monteggia Type 3 Equivalent Lesion: Lateral Dislocation of Radial Head with Both-Bone Forearm Fracture
 Case Reports in Orthopedics Volume 2016, Article ID 8598139, 5 pages http://dx.doi.org/10.1155/2016/8598139 Case Report An Undescribed Monteggia Type 3 Equivalent Lesion: Lateral Dislocation of Radial
Case Reports in Orthopedics Volume 2016, Article ID 8598139, 5 pages http://dx.doi.org/10.1155/2016/8598139 Case Report An Undescribed Monteggia Type 3 Equivalent Lesion: Lateral Dislocation of Radial
SHOULDER PAIN. A Real Pain in the Neck. Michael Wolk, MD Northeastern Rehabilitation Associates October 31, 2017
 SHOULDER PAIN A Real Pain in the Neck Michael Wolk, MD Northeastern Rehabilitation Associates October 31, 2017 THE SHOULDER JOINT (S) 1. glenohumeral 2. suprahumeral 3. acromioclavicular 4. scapulocostal
SHOULDER PAIN A Real Pain in the Neck Michael Wolk, MD Northeastern Rehabilitation Associates October 31, 2017 THE SHOULDER JOINT (S) 1. glenohumeral 2. suprahumeral 3. acromioclavicular 4. scapulocostal
CLINICAL EXAMINATION OF THE SHOULDER JOINT 대한신경근골격연구회 분당제생병원재활의학과 박준성
 CLINICAL EXAMINATION OF THE SHOULDER JOINT 대한신경근골격연구회 분당제생병원재활의학과 박준성 Clinical Examination of the Shoulder Good history, full clinical examination Detailed knowledge of the anatomy solve the majority of
CLINICAL EXAMINATION OF THE SHOULDER JOINT 대한신경근골격연구회 분당제생병원재활의학과 박준성 Clinical Examination of the Shoulder Good history, full clinical examination Detailed knowledge of the anatomy solve the majority of
US finding of the shoulder (with live demonstration) 인제의대상계백병원 안재기
 인제의대상계백병원 안재기") US finding of the shoulder (with live demonstration) 인제의대상계백병원 안재기 Shoulder US Biceps tendon & Rotator Cuff Long Head of Biceps Tendon Subscapularis tendon Supraspinatus tendon Infraspinatus tendon Teres
US finding of the shoulder (with live demonstration) 인제의대상계백병원 안재기 Shoulder US Biceps tendon & Rotator Cuff Long Head of Biceps Tendon Subscapularis tendon Supraspinatus tendon Infraspinatus tendon Teres
Anatomy of the Shoulder Girdle. Prof Oluwadiya Kehinde FMCS (Orthop)
") Anatomy of the Shoulder Girdle Prof Oluwadiya Kehinde FMCS (Orthop) www.oluwadiya.com Bony Anatomy Shoulder Complex: Sternum(manubrium) Clavicle Scapula Proximal humerus Manubrium Sterni Upper part of
Anatomy of the Shoulder Girdle Prof Oluwadiya Kehinde FMCS (Orthop) www.oluwadiya.com Bony Anatomy Shoulder Complex: Sternum(manubrium) Clavicle Scapula Proximal humerus Manubrium Sterni Upper part of
Osteology of the Elbow and Forearm Complex. The ability to perform many activities of daily living (ADL) depends upon the elbow.
 depends upon the elbow.") Osteology of the Elbow and Forearm Complex The ability to perform many activities of daily living (ADL) depends upon the elbow. Activities of Daily Living (ADL) Can you think of anything that you do to
Osteology of the Elbow and Forearm Complex The ability to perform many activities of daily living (ADL) depends upon the elbow. Activities of Daily Living (ADL) Can you think of anything that you do to
Anatomy and Physiology II. Review Shoulder Girdle New Material Upper Extremities - Bones
 Anatomy and Physiology II Review Shoulder Girdle New Material Upper Extremities - Bones Anatomy and Physiology II Shoulder Girdle Review Questions From Last Lecture Can you identify the following muscles?
Anatomy and Physiology II Review Shoulder Girdle New Material Upper Extremities - Bones Anatomy and Physiology II Shoulder Girdle Review Questions From Last Lecture Can you identify the following muscles?
Glenohumeral Joint. Glenohumeral Joint. Glenohumeral Joint. Glenohumeral Joint. Glenohumeral Joint. Glenohumeral Joint
 The Shoulder Joint Chapter 5 The Shoulder Joint Manual of Structural Kinesiology R.T. Floyd, EdD, ATC, CSCS McGraw-Hill Higher Education. All rights reserved. 5-1 Shoulder joint is attached to axial skeleton
The Shoulder Joint Chapter 5 The Shoulder Joint Manual of Structural Kinesiology R.T. Floyd, EdD, ATC, CSCS McGraw-Hill Higher Education. All rights reserved. 5-1 Shoulder joint is attached to axial skeleton
Shoulder Biomechanics
 Shoulder Biomechanics Lecture originally developed by Bryan Morrison, Ph.D. candidate Arizona State University Fall 2000 1 Outline Anatomy Biomechanics Problems 2 Shoulder Complex Greatest Greatest Predisposition
Shoulder Biomechanics Lecture originally developed by Bryan Morrison, Ph.D. candidate Arizona State University Fall 2000 1 Outline Anatomy Biomechanics Problems 2 Shoulder Complex Greatest Greatest Predisposition
Case Report Successful Outcome of Triangle Tilt as Revision Surgery in a Pediatric Obstetric Brachial Plexus Patient with Multiple Previous Operations
 Case Reports in Surgery, Article ID 715389, 4 pages http://dx.doi.org/10.1155/2014/715389 Case Report Successful Outcome of Triangle Tilt as Revision Surgery in a Pediatric Obstetric Brachial Plexus Patient
Case Reports in Surgery, Article ID 715389, 4 pages http://dx.doi.org/10.1155/2014/715389 Case Report Successful Outcome of Triangle Tilt as Revision Surgery in a Pediatric Obstetric Brachial Plexus Patient
Ultrasound-Guided Biceps Peritendinous Injections in the Absence of a Distended Tendon Sheath
 TECHNICAL INNOVATION Ultrasound-Guided Biceps Peritendinous Injections in the Absence of a Distended Tendon Sheath A Novel Rotator Interval Approach Taylor J. Stone, MD, Ronald S. Adler, MD, PhD This retrospective
TECHNICAL INNOVATION Ultrasound-Guided Biceps Peritendinous Injections in the Absence of a Distended Tendon Sheath A Novel Rotator Interval Approach Taylor J. Stone, MD, Ronald S. Adler, MD, PhD This retrospective
Case Report Arthroscopic Bony Bankart Repair Using Double-Threaded Headless Screw: A Case Report
 Case Reports in Orthopedics Volume 2012, Article ID 789418, 4 pages doi:10.1155/2012/789418 Case Report Arthroscopic Bony Bankart Repair Using Double-Threaded Headless Screw: A Case Report Takeshi Kokubu,
Case Reports in Orthopedics Volume 2012, Article ID 789418, 4 pages doi:10.1155/2012/789418 Case Report Arthroscopic Bony Bankart Repair Using Double-Threaded Headless Screw: A Case Report Takeshi Kokubu,
Connects arm to thorax 3 joints. Glenohumeral joint Acromioclavicular joint Sternoclavicular joint
 Connects arm to thorax 3 joints Glenohumeral joint Acromioclavicular joint Sternoclavicular joint Scapula Elevation Depression Protraction (abduction) Retraction (adduction) Downward Rotation Upward Rotation
Connects arm to thorax 3 joints Glenohumeral joint Acromioclavicular joint Sternoclavicular joint Scapula Elevation Depression Protraction (abduction) Retraction (adduction) Downward Rotation Upward Rotation
MR measurements of subcoracoid impingement using a new method and its relationship to rotator cuff pathology at MR arthrography
 MR measurements of subcoracoid impingement using a new method and its relationship to rotator cuff pathology at MR arthrography Poster No.: P-0055 Congress: ESSR 2014 Type: Authors: Keywords: DOI: Scientific
MR measurements of subcoracoid impingement using a new method and its relationship to rotator cuff pathology at MR arthrography Poster No.: P-0055 Congress: ESSR 2014 Type: Authors: Keywords: DOI: Scientific
region of the upper limb between the shoulder and the elbow Superiorly communicates with the axilla.
 1 region of the upper limb between the shoulder and the elbow Superiorly communicates with the axilla. Inferiorly, a number of important structures pass between arm & forearm through cubital fossa. 2 medial
1 region of the upper limb between the shoulder and the elbow Superiorly communicates with the axilla. Inferiorly, a number of important structures pass between arm & forearm through cubital fossa. 2 medial
Research Article Comparison of Colour Duplex Ultrasound with Computed Tomography to Measure the Maximum Abdominal Aortic Aneurysmal Diameter
 International Vascular Medicine, Article ID 574762, 4 pages http://dx.doi.org/10.1155/2014/574762 Research Article Comparison of Colour Duplex Ultrasound with Computed Tomography to Measure the Maximum
International Vascular Medicine, Article ID 574762, 4 pages http://dx.doi.org/10.1155/2014/574762 Research Article Comparison of Colour Duplex Ultrasound with Computed Tomography to Measure the Maximum
Patient ID. Case Conference. Physical Examination. Image examination. Treatment 2011/6/16
 Patient ID Case Conference R3 高逢駿 VS 徐郭堯 55 y/o female C.C.: recurrent right shoulder dislocation noted since falling down injury 2 years ago Came to ER because of dislocation for many times due to minor
Patient ID Case Conference R3 高逢駿 VS 徐郭堯 55 y/o female C.C.: recurrent right shoulder dislocation noted since falling down injury 2 years ago Came to ER because of dislocation for many times due to minor
WEEKEND 2 Shoulder. Shoulder Active Range of Motion Assessment
 Virginia Orthopedic Manual Physical Therapy Institute - 2016 Technique Manual WEEKEND 2 Shoulder Shoulder Active Range of Motion Assessment - Patient Positioning: Standing, appropriately undressed so that
Virginia Orthopedic Manual Physical Therapy Institute - 2016 Technique Manual WEEKEND 2 Shoulder Shoulder Active Range of Motion Assessment - Patient Positioning: Standing, appropriately undressed so that
Muscular Nomenclature and Kinesiology - One
 Chapter 16 Muscular Nomenclature and Kinesiology - One Lessons 1-3 (with lesson 4) 1 Introduction 122 major muscles covered in this chapter Chapter divided into nine lessons Kinesiology study of human
Chapter 16 Muscular Nomenclature and Kinesiology - One Lessons 1-3 (with lesson 4) 1 Introduction 122 major muscles covered in this chapter Chapter divided into nine lessons Kinesiology study of human
Case Report Rotator Interval Lesion and Damaged Subscapularis Tendon Repair in a High School Baseball Player
 Case Reports in Orthopedics Volume 2015, Article ID 890721, 4 pages http://dx.doi.org/10.1155/2015/890721 Case Report Rotator Interval Lesion and Damaged Subscapularis Tendon Repair in a High School Baseball
Case Reports in Orthopedics Volume 2015, Article ID 890721, 4 pages http://dx.doi.org/10.1155/2015/890721 Case Report Rotator Interval Lesion and Damaged Subscapularis Tendon Repair in a High School Baseball
Clinical Study Rate of Improvement following Volar Plate Open Reduction and Internal Fixation of Distal Radius Fractures
 SAGE-Hindawi Access to Research Advances in Orthopedics Volume 2011, Article ID 565642, 4 pages doi:10.4061/2011/565642 Clinical Study Rate of Improvement following Volar Plate Open Reduction and Internal
SAGE-Hindawi Access to Research Advances in Orthopedics Volume 2011, Article ID 565642, 4 pages doi:10.4061/2011/565642 Clinical Study Rate of Improvement following Volar Plate Open Reduction and Internal
Ultrasound assessment of most frequent shoulder disorders
 Ultrasound assessment of most frequent shoulder disorders Poster No.: C-2026 Congress: ECR 2014 Type: Educational Exhibit Authors: S. P. Ivanoski; Ohrid/MK Keywords: Trauma, Athletic injuries, Arthritides,
Ultrasound assessment of most frequent shoulder disorders Poster No.: C-2026 Congress: ECR 2014 Type: Educational Exhibit Authors: S. P. Ivanoski; Ohrid/MK Keywords: Trauma, Athletic injuries, Arthritides,
Anatomy Workshop Upper Extremity David Ebaugh, PT, PhD Workshop Leader. Lab Leaders: STATION I BRACHIAL PLEXUS
 Anatomy Workshop Upper Extremity David Ebaugh, PT, PhD Workshop Leader Lab Leaders: STATION I BRACHIAL PLEXUS A. Posterior cervical triangle and axilla B. Formation of plexus 1. Ventral rami C5-T1 2. Trunks
Anatomy Workshop Upper Extremity David Ebaugh, PT, PhD Workshop Leader Lab Leaders: STATION I BRACHIAL PLEXUS A. Posterior cervical triangle and axilla B. Formation of plexus 1. Ventral rami C5-T1 2. Trunks
Mastering the Musculoskeletal Exam UCSF Essentials of Women s Health July 7, 2016 Carlin Senter, M.D. Henry Crevensten, M.D.
 Mastering the Musculoskeletal Exam UCSF Essentials of Women s Health July 7, 2016 Carlin Senter, M.D. Henry Crevensten, M.D. I have nothing to disclose Outline Knee exam Shoulder exam Knee Anatomy The
Mastering the Musculoskeletal Exam UCSF Essentials of Women s Health July 7, 2016 Carlin Senter, M.D. Henry Crevensten, M.D. I have nothing to disclose Outline Knee exam Shoulder exam Knee Anatomy The
R. Frank Henn III, MD. Associate Professor Chief of Sports Medicine Residency Program Director
 R. Frank Henn III, MD Associate Professor Chief of Sports Medicine Residency Program Director Disclosures No financial relationships to disclose 1. Labral anatomy 2. Adaptations of the throwing shoulder
R. Frank Henn III, MD Associate Professor Chief of Sports Medicine Residency Program Director Disclosures No financial relationships to disclose 1. Labral anatomy 2. Adaptations of the throwing shoulder
Elbow. Chapter 2 LISTEN. Mechanism of Injury (If Applicable) Pain
 Pain") Chapter 2 Elbow LISTEN Mechanism of Injury (If Applicable) Patient usually remembers their position at the time of injury Certain mechanisms of injury result in characteristic patterns Fall on outstretched
Chapter 2 Elbow LISTEN Mechanism of Injury (If Applicable) Patient usually remembers their position at the time of injury Certain mechanisms of injury result in characteristic patterns Fall on outstretched
MRI SHOULDER WHAT TO SEE
 MRI SHOULDER WHAT TO SEE DR SHEKHAR SRIVASTAV Sr. Consultant- Knee & Shoulder Arthroscopy Sant Parmanand Hospital Normal Anatomy Normal Shoulder MRI Coronal Oblique Sagital Oblique Axial Cuts Normal Coronal
MRI SHOULDER WHAT TO SEE DR SHEKHAR SRIVASTAV Sr. Consultant- Knee & Shoulder Arthroscopy Sant Parmanand Hospital Normal Anatomy Normal Shoulder MRI Coronal Oblique Sagital Oblique Axial Cuts Normal Coronal
Ultrasound Guided Therapeutic Injections in the Treatment of Shoulder Pain: A Multimedia Review
 Ultrasound Guided Therapeutic Injections in the Treatment of Shoulder Pain: A Multimedia Review Poster No.: P-0127 Congress: ESSR 2015 Type: Educational Poster Authors: A. Karsandas, J. Tuckett, R. Sinha,
Ultrasound Guided Therapeutic Injections in the Treatment of Shoulder Pain: A Multimedia Review Poster No.: P-0127 Congress: ESSR 2015 Type: Educational Poster Authors: A. Karsandas, J. Tuckett, R. Sinha,
Tendinosis & Subacromial Impingement Syndrome. Gene Desepoli, LMT, D.C.
 Tendinosis & Subacromial Impingement Syndrome Gene Desepoli, LMT, D.C. What is the shoulder joint? Shoulder joint or shoulder region? There is an interrelatedness of all moving parts of the shoulder and
Tendinosis & Subacromial Impingement Syndrome Gene Desepoli, LMT, D.C. What is the shoulder joint? Shoulder joint or shoulder region? There is an interrelatedness of all moving parts of the shoulder and
UPPER EXTREMITY INJURIES. Recognizing common injuries to the upper extremity
 UPPER EXTREMITY INJURIES Recognizing common injuries to the upper extremity ANATOMY BONES Clavicle Scapula Spine of the scapula Acromion process Glenoid fossa/cavity Humerus Epicondyles ANATOMY BONES Ulna
UPPER EXTREMITY INJURIES Recognizing common injuries to the upper extremity ANATOMY BONES Clavicle Scapula Spine of the scapula Acromion process Glenoid fossa/cavity Humerus Epicondyles ANATOMY BONES Ulna
Review shoulder anatomy Review the physical exam of the shoulder Discuss some common causes of acute shoulder pain Discuss some common causes of
 Review shoulder anatomy Review the physical exam of the shoulder Discuss some common causes of acute shoulder pain Discuss some common causes of chronic shoulder pain Review with some case questions Bones:
Review shoulder anatomy Review the physical exam of the shoulder Discuss some common causes of acute shoulder pain Discuss some common causes of chronic shoulder pain Review with some case questions Bones:
MUSCLES. Anconeus Muscle
 LAB 7 UPPER LIMBS MUSCLES Anconeus Muscle anconeus origin: distal end of dorsal surface of humerus insertion: lateral surface of ulna from distal margin of the semilunar notch to proximal end of the olecranon
LAB 7 UPPER LIMBS MUSCLES Anconeus Muscle anconeus origin: distal end of dorsal surface of humerus insertion: lateral surface of ulna from distal margin of the semilunar notch to proximal end of the olecranon
Chapter 8. The Pectoral Girdle & Upper Limb
 Chapter 8 The Pectoral Girdle & Upper Limb Pectoral Girdle pectoral girdle (shoulder girdle) supports the arm consists of two on each side of the body // clavicle (collarbone) and scapula (shoulder blade)
Chapter 8 The Pectoral Girdle & Upper Limb Pectoral Girdle pectoral girdle (shoulder girdle) supports the arm consists of two on each side of the body // clavicle (collarbone) and scapula (shoulder blade)
The Shoulder. Jill Inouye Primary Care Sports Medicine Family Medicine Resident School February 26, 2014
 The Shoulder Jill Inouye Primary Care Sports Medicine Family Medicine Resident School February 26, 2014 Objectives Review shoulder anatomy Explain and demonstrate shoulder physical exam Diagnosis and management
The Shoulder Jill Inouye Primary Care Sports Medicine Family Medicine Resident School February 26, 2014 Objectives Review shoulder anatomy Explain and demonstrate shoulder physical exam Diagnosis and management
SHOULDER PROBLEMS & ARTHROSCOPIC MANAGEMENT
 SHOULDER PROBLEMS & ARTHROSCOPIC MANAGEMENT DR.SHEKHAR SRIVASTAV Sr. Consultant-KNEE & SHOULDER Arthroscopy Sant Parmanand Hospital,Delhi Peculiarities of Shoulder Elegant piece of machinery It has the
SHOULDER PROBLEMS & ARTHROSCOPIC MANAGEMENT DR.SHEKHAR SRIVASTAV Sr. Consultant-KNEE & SHOULDER Arthroscopy Sant Parmanand Hospital,Delhi Peculiarities of Shoulder Elegant piece of machinery It has the
Returning the Shoulder Back to Optimal Function. Scapula. Clavicle. Humerus. Bones of the Shoulder (Osteology) Joints of the Shoulder (Arthrology)
 Joints of the Shoulder (Arthrology)") Returning the Shoulder Back to Optimal Function Sternum Clavicle Ribs Scapula Humerus Bones of the Shoulder (Osteology) By Rick Kaselj Clavicle Scapula Medial Left Anterior Clavicle Inferior View 20 degree
Returning the Shoulder Back to Optimal Function Sternum Clavicle Ribs Scapula Humerus Bones of the Shoulder (Osteology) By Rick Kaselj Clavicle Scapula Medial Left Anterior Clavicle Inferior View 20 degree
SHOULDER IMPINGEMENT / ROTATOR CUFF TENDONITIS / SUBACROMIAL BURSITIS
 SHOULDER IMPINGEMENT / ROTATOR CUFF TENDONITIS / SUBACROMIAL BURSITIS The terms impingement, rotator cuff tendonitis, and subacromial bursitis, all refer to a spectrum of the same condition. Anatomy The
SHOULDER IMPINGEMENT / ROTATOR CUFF TENDONITIS / SUBACROMIAL BURSITIS The terms impingement, rotator cuff tendonitis, and subacromial bursitis, all refer to a spectrum of the same condition. Anatomy The
WEEKEND THREE HOMEWORK
 WEEKEND THREE HOMEWORK READING ASSIGNMENTS Salvo Massage Therapy Principles and Practice 4 th Edition Muscolino The Muscular System Manual Muscolino The Muscle and Bone Palpation Manual Ch. 19 Skeletal
WEEKEND THREE HOMEWORK READING ASSIGNMENTS Salvo Massage Therapy Principles and Practice 4 th Edition Muscolino The Muscular System Manual Muscolino The Muscle and Bone Palpation Manual Ch. 19 Skeletal
The shoulder that won t get better.
 The shoulder that won t get better. www.fisiokinesiterapia.biz Shoulder Injuries Acute Chronic Acute shoulder injuries Instability Labral pathology (SLAP lesions) Fractures (clavicle, scapula, humerus)
The shoulder that won t get better. www.fisiokinesiterapia.biz Shoulder Injuries Acute Chronic Acute shoulder injuries Instability Labral pathology (SLAP lesions) Fractures (clavicle, scapula, humerus)
Soft Tissue Rheumatism. Elinor Mody, MD Chief, Division of Rheumatology Reliant Medical Group
 Soft Tissue Rheumatism Elinor Mody, MD Chief, Division of Rheumatology Reliant Medical Group Some problems are difficult, but diagnosing and treating most causes of joint pain are not! Common areas of
Soft Tissue Rheumatism Elinor Mody, MD Chief, Division of Rheumatology Reliant Medical Group Some problems are difficult, but diagnosing and treating most causes of joint pain are not! Common areas of
Case Report Elastic Intramedullary Nailing of a Medial Clavicle Fracture in a Pediatric Patient
 Hindawi Case Reports in Orthopedics Volume 2017, Article ID 6354284, 4 pages https://doi.org/10.1155/2017/6354284 Case Report Elastic Intramedullary Nailing of a Medial Clavicle Fracture in a Pediatric
Hindawi Case Reports in Orthopedics Volume 2017, Article ID 6354284, 4 pages https://doi.org/10.1155/2017/6354284 Case Report Elastic Intramedullary Nailing of a Medial Clavicle Fracture in a Pediatric
Vol 3, 2008 CEC ARTICLE: Special Medical Conditions Part 2: Shoulder Maintenance and Rehab C. Eggers
 Vol 3, 2008 CEC ARTICLE: Special Medical Conditions Part 2: Shoulder Maintenance and Rehab C. Eggers SHOULDER GIRDLE STABILIZATION Knowledge of the anatomy and biomechanics of the shoulder girdle is essential
Vol 3, 2008 CEC ARTICLE: Special Medical Conditions Part 2: Shoulder Maintenance and Rehab C. Eggers SHOULDER GIRDLE STABILIZATION Knowledge of the anatomy and biomechanics of the shoulder girdle is essential
Case study # 6 Sharon P
 Patient is a morbidly obese 70 year old female presenting with left shoulder pain after a severe fall. Patient is in moderate to severe pain with extremely limited range of motion due to extensive shoulder
Patient is a morbidly obese 70 year old female presenting with left shoulder pain after a severe fall. Patient is in moderate to severe pain with extremely limited range of motion due to extensive shoulder
Case Report A Thickened Coracohumeral Ligament and Superomedial Capsule Limit Internal Rotation of the Shoulder Joint: Report of Three Cases
 Hindawi Publishing Corporation Case Reports in Orthopedics Volume 2016, Article ID 9384974, 5 pages http://dx.doi.org/10.1155/2016/9384974 Case Report A Thickened Coracohumeral Ligament and Superomedial
Hindawi Publishing Corporation Case Reports in Orthopedics Volume 2016, Article ID 9384974, 5 pages http://dx.doi.org/10.1155/2016/9384974 Case Report A Thickened Coracohumeral Ligament and Superomedial
Sports Medicine: Shoulder Arthrography. Christine B. Chung, M.D. Professor of Radiology Musculoskeletal Division UCSD and VA Healthcare System
 Sports Medicine: Shoulder Arthrography Christine B. Chung, M.D. Professor of Radiology Musculoskeletal Division UCSD and VA Healthcare System Disclosure Off-label use for gadolinium Pediatric Sports Injuries
Sports Medicine: Shoulder Arthrography Christine B. Chung, M.D. Professor of Radiology Musculoskeletal Division UCSD and VA Healthcare System Disclosure Off-label use for gadolinium Pediatric Sports Injuries
Lawrence Gulotta Gillian Lieberman, MD October Gillian Lieberman, MD. Shoulder Imaging. Lawrence V. Gulotta, HMS IV 10/16/02
 October 2002 Shoulder Imaging Lawrence V. Gulotta, HMS IV 10/16/02 Goals Review Anatomy of the Shoulder -Dynamic Stabilizers -> Rotator Cuff -Static Stabilizers -> Labrum and Capsule Systematic Approach
October 2002 Shoulder Imaging Lawrence V. Gulotta, HMS IV 10/16/02 Goals Review Anatomy of the Shoulder -Dynamic Stabilizers -> Rotator Cuff -Static Stabilizers -> Labrum and Capsule Systematic Approach