ROTATIONAL & ANGULAR VARIATIONS IN CHILDREN:
|
|
|
- Darren Powers
- 5 years ago
- Views:
Transcription

1 ROTATIONAL & ANGULAR VARIATIONS IN CHILDREN: IN-TOEING, OUT-TOEING, BOWED LEGS, AND KNOCK-KNEES Leigh Ann Lather MD FAAP 29 September, 2018 MSK Bootcamp

2 I have no relevant financial relationships with the manufacturers of any commercial products and/or providers of commercial services discussed in this CME activity. I do not intend to discuss an unapproved or investigative use of a commercial product or device in my presentation.
3 LEARNING OBJECTIVES ROTATIONAL VARIATIONS ARE THE MOST COMMON REASON FOR REFERRAL TO PEDIATRIC ORTHOPAEDICS. 1. Be able to confidently reassure parents through education about physiologic in-toeing, out-toeing, genu varum (bowed legs), and genu valgum (knock-knees). 2. Recognize red flags: indications for radiographs, laboratory testing, and/or referral to a pediatric orthopedist or other pediatric specialist.
4 CASES 1. A 2 year-old boy with bowed legs, in-toeing, who is constantly tripping over his own feet. 2. An 18 month-old NICU grad with severe out-toeing. 3. A 10 year-old girl with knock-knees, flat feet, and knee pain who runs funny and would like to be excused from PE due to knee pain and bullying by her peers and her PE teacher. 4. A 21-month obese African-American girl with severe bowed legs and falling. 5. An 11 year old girl with flat feet, and pain in both knees.
5 CASE #1 A 2 YEAR-OLD BOY WITH BOWED LEGS, IN-TOEING, AND CONSTANTLY TRIPPING OVER HIS OWN FEET. Family noted bilateral leg bowing during infancy. The bowing seemed worse when he started walking at 16 months. His in-toeing is now so bad that he trips over his own feet and falls constantly. Earlier this week he fell and got a huge knot on his forehead and the parents rushed him to the ED. They are worried that he is going to hurt himself seriously and they are going to be accused of child abuse. Also, father wore braces because of in-toeing and the braces helped him. 1. Are you worried about 2 year olds and falling? 2. Are you worried about in-toeing in a 2 year old? What is the most likely cause? 3. Is bowed legs at age 2 normal? What else do you want to know? 4. What are the most important exam skills to focus on? 5. Likely to need referral? Not likely to need referral?


6 CASE #1 2 YEAR OLD: BOWED LEGS, IN-TOEING, AND TRIPPING 1 st : Do you think the bowing of the legs is improving? Do you think one side is worse than the other? Does either knee ever appear to give out or bow out to the side with walking or running? Was he born at term or premature? Breast or bottle fed? Does he drink milk and eat dairy foods? What does his growth chart for height look like? Is he obese? Is there a family hx of bowed legs and was treatment required? Is a referral warranted?


7 DIFFERENTIAL: BOWED LEGS Refer: Ortho, Genetics, NSGY




8 1 yr 2 yr 3-4 yr 7-8 yr Normal physiologic development

9 CASE #1 A 2 YEAR-OLD BOY WITH BOWED LEGS, IN-TOEING, AND CONSTANTLY TRIPPING OVER HIS OWN FEET. 1. Are you worried about 2 year olds and falling? 2. Are you worried about in-toeing in a 2 year old? What is the most likely cause? 3. What are the possible causes and how will you explain them?

 University of Virginia")
10 In-toeing: physiologic Age at presentation Infant Likely diagnosis Metatarsus adductus Toddler Internal tibial torsion School age Femoral anteversion (most common) University of Virginia Orthopaedic Surgery






11 4-part rotational profile exam* 1. Foot shape 2. TFA= Thigh Foot Angle. Tibial torsion 3. IR/ER Internal and External rotation= Femoral version University of Virginia 4. FPA Foot Progression Angle Sum of the Parts *record the data for follow up Quick and powerful way to sort out & explain in-toeing Orthopaedic Surgery
![Thigh-Foot Angle [TFA] Adult Normal = +5-30⁰ Most](/docs-images/87/96769487/images/12-2.jpg "are Neutral: by age 7 Not all outgrow it by age")

12 Thigh-Foot Angle [TFA] Adult Normal = +5-30⁰ Most are Neutral: by age 7 Not all outgrow it by age 2-3 University of Virginia Orthopaedic Surgery Internal torsion gets better External torsion can increase
 Mild 70-80 Moderate 80-90 Severe 90 Total arc IR+ER= ~90 degrees")

13 Exam: IR/ER hip Prone on firm surface, hips extended pelvis level (use hand on sacrum) Mild Moderate Severe 90 Total arc IR+ER= ~90 degrees While prone: *Note also if there is -Internal torsion -Metatarsus adductus Remember that FPA is The Sum of the parts University of Virginia Orthopaedic Surgery


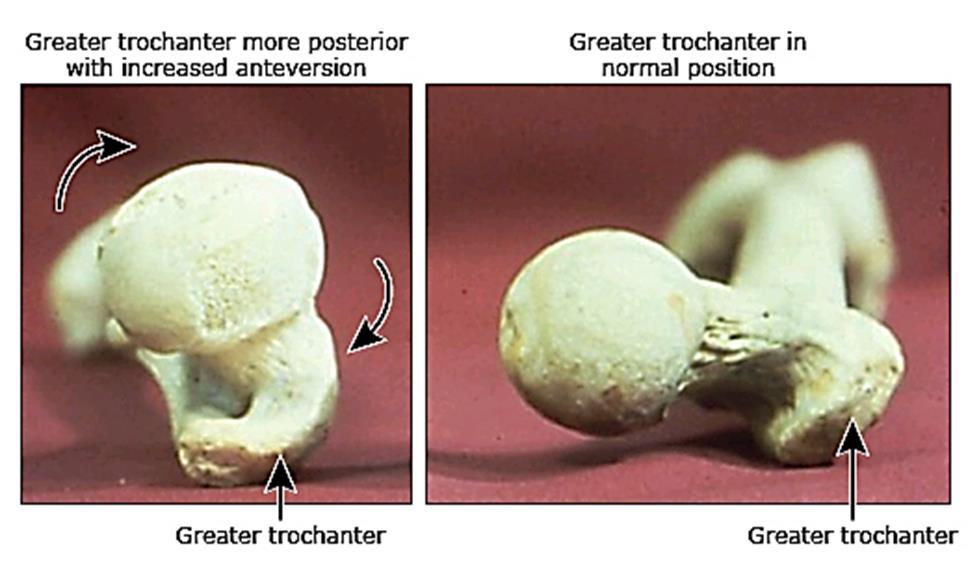

14 Anatomy University of Virginia Orthopaedic Surgery



15 Anatomy - functional Why do they in-toe? Intoeing is a natural adaptation provides a Mechanical advantage during gait -Lengthens the gluteal muscles To stabilize the pelvis University of Virginia Orthopaedic Surgery


16 End Case #1 Age at presentation Infant Likely diagnosis Metatarsus adductus Toddler Internal tibial torsion Our Patient School age Femoral anteversion (most common) To refer, or not to refer University of Virginia Orthopaedic Surgery

17 CASE #1 2 YEAR OLD: BOWED LEGS, IN-TOEING, AND TRIPPING Tripping and falling? Normal. Reassure re: normal development and NAT Bowed legs? Parents think it is improving Still obvious at 2 but symmetric, improving 1. Measure and see back in 3 mos. 2. AP standing bilateral legs Advantage of imaging: easily helps sort out the differential dx In-toeing? Internal tibial torsion and femoral anteversion are normal variants Both will improve but it may take several years. Referral? Possibly for the bowing, esp. if parent very anxious. OR, schedule a follow up in 3 months for reassurance.
18 CASE #2 AN 18 MONTH-OLD NICU GRAD WITH SEVERE OUT-TOEING. 18 month-old male presents for his WCC. He has just started walking and his physical therapist is concerned about his degree of out-toeing and suggested that there might be a problem with the hips and bracing might be indicated. Born at 36 weeks, breech, LGA, IDM, transferred to NICU in the first 24 hours of life for respiratory distress, developed pulmonary HTN, treated with ECMO. Other complications include NEC, need for TPN, tracheostomy and G-tube placement, feeding difficulties. After many months, he was finally discharged and has made rapid developmental progress at home- walking, speaking a few words, eating, scheduled for trach and G-tube removal. They feel he is a miracle baby and now they have adjusted their developmental hopes and expectations, but they are worried that he may have hip problem that was missed or that his abnormal walking is a consequence of all that happened to him. They want to know if he will always be slew-footed.

19 CASE #2 During the history you observe him walking independently a few steps at a time - with short steps, a wide-based gait that appears symmetric, but his feet turn out to almost 180 degrees. You think, It is a wonder he doesn t fall on his face. 1. Does he have gross motor delay? 2. Is the out-toeing concerning to you? 3. Would you get radiographs? What would you order? 4. Is this CP? Does he need a brain MRI? 5. Would bracing be helpful? What about special shoes? 6. Will this get better? 7. Is a referral indicated? If so, to which specialty?


20 CASE #2 THEY ARE WORRIED THAT HE MAY HAVE HIP PROBLEM THAT WAS MISSED OR THAT HIS ABNORMAL WALKING IS A CONSEQUENCE OF ALL THAT HAPPENED TO HIM. THEY WANT TO KNOW IF HE WILL ALWAYS BE SLEW-FOOTED Rotational profile: Hips IR/ER = 10/80+ bilateral TFA R/L = 0/0 Foot shape = straight, normal structure FPA= variable degrees external All LE joints are supple with FROM, mild hypermobility Neuro: good eye contact, follows simple commands, no spasticity in legs, downgoing toes. 2. Is the out-toeing concerning to you? 3. Would you get radiographs? What would you order? 4. Is this CP? Does he need a brain MRI? 5. Would bracing be helpful? What about special shoes? 6. Will this get better? What is the diagnosis? 7. Is a referral indicated? If so, to which specialty? EXTERNAL ROTATION CONTRACTURES OF THE HIPS - PHYSIOLOGIC





21 CASE #3 A 10 YEAR-OLD GIRL WITH KNOCK-KNEES, FLAT FEET, AND KNEE PAIN WHO RUNS FUNNY AND WOULD LIKE TO BE EXCUSED FROM PE DUE TO KNEE PAIN AND BULLYING BY HER PEERS AND HER PE TEACHER. Rotational profile: Hip IR/ER = 85/10 TFA R/L = +45/+35 Foot- straight (but w/ Flexible pes planus) FPA = near neutral walking But looks awkward Normal neurologic exam Diagnosis? Malicious Malalignment Syndrome
22 CASE #3 A 10 YEAR-OLD GIRL WITH KNOCK-KNEES, FLAT FEET, AND KNEE PAIN WHO RUNS FUNNY AND WOULD LIKE TO BE EXCUSED FROM PE DUE TO KNEE PAIN AND BULLYING BY HER PEERS AND HER PE TEACHER. MALICIOUS MALALIGNMENT SYNDROME What can you offer to help with her pain? Refer to physical therapy strength, neuromuscular control Recommend good supportive shoes, possible cushioned OTC arch supports in shoes that need them for her flexible flat feet. What would you advise for PE? Needs to stay in PE Write a doctor s note allowing self-modification of running if there is knee pain. Talk to principal /guidance counselor /PE teacher. Does she need an Orthopaedic referral? YES. (If you don t offer, they will probably ask) Some risk for patellofemoral arthritis, and the cosmetics are unacceptable to some May be a candidate for surgery: rotational osteotomy (distal tibia, prox.femur, both?) Outcomes: improved cosmesis, decreased pain. Functional change is variable.


23 CASE #4 A 21-MONTH OBESE AFRICAN-AMERICAN GIRL WITH SEVERE BOWED LEGS AND FALLING. Uncomplicated pregnancy and delivery, full-term, SVD. Bottle fed, grew well and gained weight rapidly. Height curve looks normal. Development has been normal. Walked at 10 months. Bowed legs noticed then and the bowing is getting worse. They think it might be more severe on the left. Recently they have noticed her left knee giving out to the side and sometimes this seems to make her fall. She does not complain of pain. Their pediatrician is concerned about her weight but everyone in their family is big so they feel her weight is normal. She is drinking a bottle of sweet tea. What is the differential diagnosis? Should you get an x ray? What kind? Should you order any labs? Is her weight a problem? Advice? Should you refer to a specialist? What kind? Differentia l Diagnosis of Bowed Legs Physiologic Blount disease Metabolic bone disease Skeletal dysplasia Neoplastic disease Lateral thrust of knee Confirmed on exam Observe gait in hallway






24 CASE #4- INFANTILE BLOUNT DISEASE A 21-MONTH OBESE AFRICAN-AMERICAN GIRL WITH SEVERE BOWED LEGS AND FALLING. Should you get an x ray? What kind? Should you order any labs? Is her weight a problem? Advice? Should you refer to a specialist? What kind? Bracing - KAFO Under age 3 years Stage 1 or 2 disease Blount- Risk factors Early walker Dark skin obesity



25 CASE #5 AN 11- YEAR OLD GIRL WITH FLAT FEET, AND PAIN IN BOTH KNEES. Increasing frequency of complaints of knee pain over the past year. Now that it is summer and she is barefoot, her foster mom noticed she appears to have flat feet. They have tried some arch support shoe inserts but there has been no improvement in the knee pain. Not much of her history is known. They had also noticed she was knock-kneed but the patient remembers being told she would grow out of it. Is this physiologic knock knee? What could cause this? What is on the differential? What else do you want to ask the patient? What would you do next? Does she need a referral? b Intermalleolar distance <9 cm or


 intermalleolar Metabolic bone disease Post-traumatic")

26 CASE #5 AN 11- YEAR OLD GIRL WITH FLAT FEET, AND PAIN IN BOTH KNEES What could cause this? What is on the differential? What else do you want to ask the patient? What would you do next? Does she need a referral? Pathologic genu valgum Genu valgum past age 8 : >9 cm (3.5 ) intermalleolar Metabolic bone disease Post-traumatic Skeletal dysplasias inc. MPS Neoplastic- HMO, fibrocartilaginous dysplasia Zone 1: no intervention Zone 2: consider intervention, esp w/pain Zone 3: surgery indicated







27 CASE #5 AN 11- YEAR OLD GIRL WITH FLAT FEET, AND PAIN IN BOTH KNEES. Most flat feet are benign and painless. Think outside the feet...
28 SUMMARY WHAT CAN YOU DO TODAY? 1. Use the rotational profile including gait assessment in the hallway, to help sort out and explain in-toeing and out-toeing. 2. Know/review normal physiologic development for LE rotation, genu varum and valgum. 3. Have a lower threshold for imaging (AP standing bilateral legs) bowed legs and knock knees that seem worse than usual. 4. Most of these patients have normal variants and it can be tempting to dismiss them too quickly- remember to ask, What are you most worried about? (and make sure you answer that )


 -Hereditary Multiple")
")
")
29 Not Ducks: -X-linked Hypophosphatemic Rickets -CP -Duchenne s MD -Post.fossa tumor -Blount disease -Skew foot -CMT -Leukemia (ALL) -Hereditary Multiple Osteochondromas -Multiple Epiphyseal Dysplasia (MED) -SCFE -Post-traumatic genu valgum (tibia physeal fx) -Tethered cord
In-toeing, Out-toeing, Growing Pains, Bowlegs, Knock-Knees and Flat Feet
 Jeffrey B. Neustadt, M.D. Scott W. Beck, M.D. Gregory V. Hahn, M.D. Drew E. Warnick, M.D. Paul L. Benfanti, M.D. Lee G. Phillips, M.D. Daniel C. Bland, M.D. Common Benign Orthopaedic Conditions In-toeing,
Jeffrey B. Neustadt, M.D. Scott W. Beck, M.D. Gregory V. Hahn, M.D. Drew E. Warnick, M.D. Paul L. Benfanti, M.D. Lee G. Phillips, M.D. Daniel C. Bland, M.D. Common Benign Orthopaedic Conditions In-toeing,
Lower Extremity Malalignment: When to Refer and When to Reassure?
 Lower Extremity Malalignment: When to Refer and When to Reassure? Mary Aschenbrener, PA-C Minnesota Academy of Physician Assistants 03/18/16 Cary H. Mielke, MD Chief of Staff Orthopaedic Burn Spinal cord
Lower Extremity Malalignment: When to Refer and When to Reassure? Mary Aschenbrener, PA-C Minnesota Academy of Physician Assistants 03/18/16 Cary H. Mielke, MD Chief of Staff Orthopaedic Burn Spinal cord
Intoeing: When to Worry? Sukhdeep K. Dulai SPORC 2018
 Intoeing: When to Worry? Sukhdeep K. Dulai SPORC 2018 What is it? Intoeing: When to worry? Why isn t it always cause for worry? What are the benign causes of intoeing? What are the pathologic causes of
Intoeing: When to Worry? Sukhdeep K. Dulai SPORC 2018 What is it? Intoeing: When to worry? Why isn t it always cause for worry? What are the benign causes of intoeing? What are the pathologic causes of
PAEDIATRIC ORTHOPAEDICS BRENT WEATHERHEAD, MD, FRCSC PAEDIATRIC ORTHOPAEDIC SURGEON MEDICAL DIRECTOR, REBALANCE
 PAEDIATRIC ORTHOPAEDICS BRENT WEATHERHEAD, MD, FRCSC PAEDIATRIC ORTHOPAEDIC SURGEON MEDICAL DIRECTOR, REBALANCE DISCLOSURES I HAVE NO INDUSTRY CONFLICTS TO DECLARE I AM AN ORTHOPAEDIC SURGEON TRAINED IN
PAEDIATRIC ORTHOPAEDICS BRENT WEATHERHEAD, MD, FRCSC PAEDIATRIC ORTHOPAEDIC SURGEON MEDICAL DIRECTOR, REBALANCE DISCLOSURES I HAVE NO INDUSTRY CONFLICTS TO DECLARE I AM AN ORTHOPAEDIC SURGEON TRAINED IN
Pediatric Orthopedics: ``To Refer or Not to Refer``
 Pediatric Orthopedics: ``To Refer or Not to Refer`` Thierry E. Benaroch, MD, FRCS(C) McGill University Health Centre Intoeing Knock knees Bowlegs Flatfeet Toe walking Knee pain Hip click Intoeing Objectives
Pediatric Orthopedics: ``To Refer or Not to Refer`` Thierry E. Benaroch, MD, FRCS(C) McGill University Health Centre Intoeing Knock knees Bowlegs Flatfeet Toe walking Knee pain Hip click Intoeing Objectives
A Patient s Guide to Rotational Deformities in Children
 A Patient s Guide to Rotational Deformities in Children 2350 Royal Boulevard Suite 200 Elgin, IL 60123 Phone: 847.931.5300 Fax: 847.931.9072 DISCLAIMER: The information in this booklet is compiled from
A Patient s Guide to Rotational Deformities in Children 2350 Royal Boulevard Suite 200 Elgin, IL 60123 Phone: 847.931.5300 Fax: 847.931.9072 DISCLAIMER: The information in this booklet is compiled from
, MD. physiologic. tibia varum. in utero (in. Disease in. variation. positioning. back and legs. instead of. Blount's. Infant with bowing in both legs
 North Jersey Orthopaedic Institute Rutgers, The Statee University of New Jersey 140 Bergen Street, D1610 Newark, NJ 07101 973-972-2150 South Orange Ambulatory Center Hackensack Medical Plaza Overlook Medical
North Jersey Orthopaedic Institute Rutgers, The Statee University of New Jersey 140 Bergen Street, D1610 Newark, NJ 07101 973-972-2150 South Orange Ambulatory Center Hackensack Medical Plaza Overlook Medical
In-toeing and Out-toeing
 In-toeing and Out-toeing What is all the fuss about? Natalie Stork, MD Assistant Professor University of Missouri-Kansas City School of Medicine, Department of Orthopaedic Surgery and Department of Pediatrics
In-toeing and Out-toeing What is all the fuss about? Natalie Stork, MD Assistant Professor University of Missouri-Kansas City School of Medicine, Department of Orthopaedic Surgery and Department of Pediatrics
Normal lower limb variants in children
 Link to this article online for CPD/CME credits The Royal London & Barts and The London Children s Hospitals, Barts Health NHS Trust, London E1 1BB, UK Correspondence to: A Yeo andreayeo@doctors.org.uk
Link to this article online for CPD/CME credits The Royal London & Barts and The London Children s Hospitals, Barts Health NHS Trust, London E1 1BB, UK Correspondence to: A Yeo andreayeo@doctors.org.uk
Leg Posture in Children
 Leg Posture in Children Exceptional healthcare, personally delivered Leg Posture in Children A guide for parents This leaflet has been produced to provide information on the normal postural variation of
Leg Posture in Children Exceptional healthcare, personally delivered Leg Posture in Children A guide for parents This leaflet has been produced to provide information on the normal postural variation of
Orthopedics. 1. GOAL: Understand the pediatrician's role in preventing and screening for
 The University of Arizona Pediatric Residency Program Primary Goals for Rotation Orthopedics 1. GOAL: Understand the pediatrician's role in preventing and screening for orthopedic injury, disease and dysfunction.
The University of Arizona Pediatric Residency Program Primary Goals for Rotation Orthopedics 1. GOAL: Understand the pediatrician's role in preventing and screening for orthopedic injury, disease and dysfunction.
Instructional Course Lecture 2011
 Instructional Course Lecture 2011 Yoon Hae Kwak Dept. of Orthopaedic Surgery Hallym University Sacred Heart Hospital Hallym University Medical Center Rotational and Angular variations of the lower extremities
Instructional Course Lecture 2011 Yoon Hae Kwak Dept. of Orthopaedic Surgery Hallym University Sacred Heart Hospital Hallym University Medical Center Rotational and Angular variations of the lower extremities
Lower Extremity Alignment: Genu Varum / Valgum
 Lower Extremity Alignment: Genu Varum / Valgum Arthur B Meyers, MD Nemours Children s Hospital & Health System Associate Professor of Radiology, University of Central Florida Clinical Associate Professor
Lower Extremity Alignment: Genu Varum / Valgum Arthur B Meyers, MD Nemours Children s Hospital & Health System Associate Professor of Radiology, University of Central Florida Clinical Associate Professor
Clinical Practice & Referral Guideline - Developmental Dysplasia of the Hip
 Clinical Practice & Referral Guideline - Developmental Dysplasia of the Hip *This guideline was developed from the American Academy of Pediatrics Clinical Practice Guideline: Early Detection of Developmental
Clinical Practice & Referral Guideline - Developmental Dysplasia of the Hip *This guideline was developed from the American Academy of Pediatrics Clinical Practice Guideline: Early Detection of Developmental
Other Congenital & Developmental Knee & Leg Disease. Jong Sup Shim,M.D. Department of Orthopedic Surgery Samsung Medical Center
 Other Congenital & Developmental Knee & Leg Disease Jong Sup Shim,M.D. Department of Orthopedic Surgery Samsung Medical Center Sungkyunkwan University School of Medicine Rotational Deformity Intoeing Outtoeing
Other Congenital & Developmental Knee & Leg Disease Jong Sup Shim,M.D. Department of Orthopedic Surgery Samsung Medical Center Sungkyunkwan University School of Medicine Rotational Deformity Intoeing Outtoeing
1. Discuss some common pediatric problems seen in the clinic. Diagnosis Clinical examination (at birth and subsequent well-baby examinations)
") 1 Pediatric Orthopaedics for Primary Care Providers 2 Disclosure Statement No conflicts related to this presentation 3 4 Goals 1. Discuss some common pediatric problems seen in the clinic 2. Examination
1 Pediatric Orthopaedics for Primary Care Providers 2 Disclosure Statement No conflicts related to this presentation 3 4 Goals 1. Discuss some common pediatric problems seen in the clinic 2. Examination
BIOMECHANICAL EXAMINATION OF THE PEDIATRIC LOWER EXTREMITY
 BIOMECHANICAL EXAMINATION OF THE PEDIATRIC LOWER EXTREMITY B.Resseque, D.P.M. ARCH HEIGHT OFF WEIGHTBEARING Evaluate arch height by placing a ruler from the heel to the first metatarsal head Compare arch
BIOMECHANICAL EXAMINATION OF THE PEDIATRIC LOWER EXTREMITY B.Resseque, D.P.M. ARCH HEIGHT OFF WEIGHTBEARING Evaluate arch height by placing a ruler from the heel to the first metatarsal head Compare arch
Club Feet, Flat Feet, Bow Legs, and Knock-Knees
 Club Feet, Flat Feet, Bow Legs, and Knock-Knees CHAPTER 11 113 WHAT IS A DEFORMITY AND WHAT IS? Sometimes parents worry because they think a part of their child s body is abnormal or deformed. But in small
Club Feet, Flat Feet, Bow Legs, and Knock-Knees CHAPTER 11 113 WHAT IS A DEFORMITY AND WHAT IS? Sometimes parents worry because they think a part of their child s body is abnormal or deformed. But in small
University of South Florida
 University of South Florida Pediatric Orthopaedics PGY 4 Competency Based Goals & Objectives Competency 1- Patient Care: Provide family centered patient care that is developmentally and age appropriate,
University of South Florida Pediatric Orthopaedics PGY 4 Competency Based Goals & Objectives Competency 1- Patient Care: Provide family centered patient care that is developmentally and age appropriate,
BIOMECHANICAL EXAMINATION OF THE PEDIATRIC LOWER EXTREMITY 2017
 BIOMECHANICAL EXAMINATION OF THE PEDIATRIC LOWER EXTREMITY 2017 B. RESSEQUE, D.P.M., D.A.B.P.O. Professor, N.Y. College of Podiatric Medicine ARCH HEIGHT OFF WEIGHTBEARING Evaluate arch height by placing
BIOMECHANICAL EXAMINATION OF THE PEDIATRIC LOWER EXTREMITY 2017 B. RESSEQUE, D.P.M., D.A.B.P.O. Professor, N.Y. College of Podiatric Medicine ARCH HEIGHT OFF WEIGHTBEARING Evaluate arch height by placing
LIMB LENGTH DISCREPANCIES
 LIMB LENGTH DISCREPANCIES Jill C Flanagan, MD OBJECTIVES Evaluate the patient with a possible limb length difference (LLD) Understand general treatment principles when managing limb length differences
LIMB LENGTH DISCREPANCIES Jill C Flanagan, MD OBJECTIVES Evaluate the patient with a possible limb length difference (LLD) Understand general treatment principles when managing limb length differences
BOW LEGS (GENU VARUM)
") BOW LEGS (GENU VARUM) By Dr John Ebnezar INTRODUCTION Have you noticed how your knees look like? If you observe carefully you will see that both your knees are not parallel but deviated slightly outwards
BOW LEGS (GENU VARUM) By Dr John Ebnezar INTRODUCTION Have you noticed how your knees look like? If you observe carefully you will see that both your knees are not parallel but deviated slightly outwards
Lower Extremity Disorders in Children and Adolescents Brian G. Smith. DOI: /pir
 Lower Extremity Disorders in Children and Adolescents Brian G. Smith Pediatrics in Review 2009;30;287 DOI: 10.1542/pir.30-8-287 The online version of this article, along with updated information and services,
Lower Extremity Disorders in Children and Adolescents Brian G. Smith Pediatrics in Review 2009;30;287 DOI: 10.1542/pir.30-8-287 The online version of this article, along with updated information and services,
Pediatric Orthopaedic Surgery and the HMSNs
 Reviewed and accepted by the 2011-2012 Neuromuscular Committee of the American Association of Neuromuscular & Electrodiagnostic Medicine Certified for CME credit 10/2011 05/2020 Reviewed 10/2017 by the
Reviewed and accepted by the 2011-2012 Neuromuscular Committee of the American Association of Neuromuscular & Electrodiagnostic Medicine Certified for CME credit 10/2011 05/2020 Reviewed 10/2017 by the
Topics and Cases in Pediatric Orthopaedics (Tuesday 6:30am 4 th Floor Orthopaedic Conference Room at Hamot)
") 2015-2016 Topics and Cases in Pediatric Orthopaedics (Tuesday 6:30am 4 th Floor Orthopaedic Conference Room at Hamot) 1. Considerations in the Management of Pediatric Patients Kerry Armet 7 July 2015 Fluid
2015-2016 Topics and Cases in Pediatric Orthopaedics (Tuesday 6:30am 4 th Floor Orthopaedic Conference Room at Hamot) 1. Considerations in the Management of Pediatric Patients Kerry Armet 7 July 2015 Fluid
Other Congenital & Developmental Knee & Leg Disease. Jong Sup Shim,M.D. Department of Orthopedic Surgery Samsung Medical Center
 Other Congenital & Developmental Knee & Leg Disease Jong Sup Shim,M.D. Department of Orthopedic Surgery Samsung Medical Center Sungkyunkwan University School of Medicine Torsional Deformity (Rotational
Other Congenital & Developmental Knee & Leg Disease Jong Sup Shim,M.D. Department of Orthopedic Surgery Samsung Medical Center Sungkyunkwan University School of Medicine Torsional Deformity (Rotational
LECTURE 8: DEVELOPMENTAL ORTHOPAEDICS. Paediatric MS History o Reason for referral o Past history
 LECTURE 8: DEVELOPMENTAL ORTHOPAEDICS Paediatric MS History o Reason for referral o Past history Antenatal history Birth history (term? Premmy? Breech? Complications?). Medical history/investigations/tests
LECTURE 8: DEVELOPMENTAL ORTHOPAEDICS Paediatric MS History o Reason for referral o Past history Antenatal history Birth history (term? Premmy? Breech? Complications?). Medical history/investigations/tests
Podo-Pediatrics in Private Practice. Elisabeth Hibbert B.Sc. D.Ch. November 11, 2016
 Podo-Pediatrics in Private Practice Elisabeth Hibbert B.Sc. D.Ch. November 11, 2016 My background Private Practice since 1998 Began promoting children s foot care in 2007 In 2016-35% of new patients are
Podo-Pediatrics in Private Practice Elisabeth Hibbert B.Sc. D.Ch. November 11, 2016 My background Private Practice since 1998 Began promoting children s foot care in 2007 In 2016-35% of new patients are
COMMON MUSCULOSKELETAL PROBLEMS GROWTH AND DEVELOPMENT PATHOLOGIC VS. NORMAL
 COMMON MUSCULOSKELETAL PROBLEMS GROWTH AND DEVELOPMENT PATHOLOGIC VS. NORMAL Clifford L. Craig, M.D. M2 Musculoskeletal Fall 2008 I. ANGULAR AND TORSIONAL DEFORMITIES OF THE LOWER LIMBS Examination Relaxed,
COMMON MUSCULOSKELETAL PROBLEMS GROWTH AND DEVELOPMENT PATHOLOGIC VS. NORMAL Clifford L. Craig, M.D. M2 Musculoskeletal Fall 2008 I. ANGULAR AND TORSIONAL DEFORMITIES OF THE LOWER LIMBS Examination Relaxed,
Learn the steps to identify pediatric muscle weakness and signs of neuromuscular disease.
 Learn the steps to identify pediatric muscle weakness and signs of neuromuscular disease. Listen Observe Evaluate Test Refer Guide for primary care providers includes: Surveillance Aid: Assessing Weakness
Learn the steps to identify pediatric muscle weakness and signs of neuromuscular disease. Listen Observe Evaluate Test Refer Guide for primary care providers includes: Surveillance Aid: Assessing Weakness
Finding New Friends Down Syndrome. Pedicases
 Finding New Friends Down Syndrome Pedicases Objectives List the diagnostic features of Down syndrome and its associated complications. Describe the role of the clinician in management of Down syndrome,
Finding New Friends Down Syndrome Pedicases Objectives List the diagnostic features of Down syndrome and its associated complications. Describe the role of the clinician in management of Down syndrome,
The Child With a Limp
 KID WITH A LIMP Common in ED, common in Exams Differential diagnosis is very wide Most causes benign, but mustn't miss Septic arthritis Osteomyelitis Fractures / NAI SUFE (older, heavier children) The
KID WITH A LIMP Common in ED, common in Exams Differential diagnosis is very wide Most causes benign, but mustn't miss Septic arthritis Osteomyelitis Fractures / NAI SUFE (older, heavier children) The
AAP Boot Camp KNEE AND ANKLE EXAM
 AAP Boot Camp KNEE AND ANKLE EXAM Disclosures I have no relevant financial relationships with the manufacturers of any commercial products and or providers of commercial services discussed in this CME
AAP Boot Camp KNEE AND ANKLE EXAM Disclosures I have no relevant financial relationships with the manufacturers of any commercial products and or providers of commercial services discussed in this CME
BORGinsole Measurement devices
 BORGinsole Measurement devices BORGinsole Angle-Finder Dorsal Flexion of the first Metatarsophalangeal joint - P. is sitting up on the examination table, with legs straight. - T. is sitting at the end
BORGinsole Measurement devices BORGinsole Angle-Finder Dorsal Flexion of the first Metatarsophalangeal joint - P. is sitting up on the examination table, with legs straight. - T. is sitting at the end
RUNNING MECHANICS AND INJURIES AN OVERVIEW DR. DAVID O BRIAN
 RUNNING MECHANICS AND INJURIES AN OVERVIEW DR. DAVID O BRIAN THIS IS REALLY ABOUT BIOMECHANICS OR THE MECHANICS OF OUR MUSCLES, JOINTS AND TENDONS THAT ENABLE US TO MOVE. BAD MECHANICS LEAD TO INEFFICIENCY
RUNNING MECHANICS AND INJURIES AN OVERVIEW DR. DAVID O BRIAN THIS IS REALLY ABOUT BIOMECHANICS OR THE MECHANICS OF OUR MUSCLES, JOINTS AND TENDONS THAT ENABLE US TO MOVE. BAD MECHANICS LEAD TO INEFFICIENCY
Gentle Guided Growth to Correct Knock Knees and Bowed Legs in Children
 PATIENT INFORMATION Gentle Guided Growth to Correct Knock Knees and Bowed Legs in Children The Guided Growth System eight-plate quad-plate INTRODUCTION Children need gentle guidance and correction in many
PATIENT INFORMATION Gentle Guided Growth to Correct Knock Knees and Bowed Legs in Children The Guided Growth System eight-plate quad-plate INTRODUCTION Children need gentle guidance and correction in many
6/23/2017. What do you see? skull fracture
 What do you see? skull fracture 1 Head CT On soft tissue windows, posterior soft tissues swelling and hemorrhage, no definite evidence of fracture Head CT On bone windows, fracture now seen subjacent to
What do you see? skull fracture 1 Head CT On soft tissue windows, posterior soft tissues swelling and hemorrhage, no definite evidence of fracture Head CT On bone windows, fracture now seen subjacent to
Second Course Motion Analysis and clinics: why set up a Motion Analysis Lab?? TRAMA Project. January th Clinical case presentation
 Second Course Motion Analysis and clinics: why set up a Motion Analysis Lab?? - Clinical cases presentation - TRAMA Project January 14-17 th 2008 Iván Carlos Uribe Prada Instituto de Ortopedia Infantil
Second Course Motion Analysis and clinics: why set up a Motion Analysis Lab?? - Clinical cases presentation - TRAMA Project January 14-17 th 2008 Iván Carlos Uribe Prada Instituto de Ortopedia Infantil
Imaging assessment of Unicomp candidates!
 7th Advanced Course on Knee Surgery - 2018: Imaging assessment of Unicomp candidates! Presenter: Anders Troelsen, MD, ph.d., dr.med., Professor Distribution of the basic primary OA patterns Medial FT:
7th Advanced Course on Knee Surgery - 2018: Imaging assessment of Unicomp candidates! Presenter: Anders Troelsen, MD, ph.d., dr.med., Professor Distribution of the basic primary OA patterns Medial FT:
Anterior knee pain.
 Anterior knee pain What are the symptoms? Anterior knee pain is very common amongst active adolescents and athletes participating in contact sports. It is one of the most common problems/injuries seen
Anterior knee pain What are the symptoms? Anterior knee pain is very common amongst active adolescents and athletes participating in contact sports. It is one of the most common problems/injuries seen
Patellofemoral Joint. Question? ANATOMY
 Doug Elenz is a paid Consultant/Advisor for the Biomet Manufacturing Corporation. Doug Elenz, MD Team Orthopaedic Surgeon The University of Texas Men s Athletic Department Question? Patellofemoral Joint
Doug Elenz is a paid Consultant/Advisor for the Biomet Manufacturing Corporation. Doug Elenz, MD Team Orthopaedic Surgeon The University of Texas Men s Athletic Department Question? Patellofemoral Joint
Hip Dysplasia David S. Feldman, MD
 Hip Dysplasia David S. Feldman, MD Chief of Pediatric Orthopedic Surgery Professor of Orthopedic Surgery & Pediatrics NYU Langone Medical Center & NYU Hospital for Joint Diseases Overview Hip dysplasia
Hip Dysplasia David S. Feldman, MD Chief of Pediatric Orthopedic Surgery Professor of Orthopedic Surgery & Pediatrics NYU Langone Medical Center & NYU Hospital for Joint Diseases Overview Hip dysplasia
Pediatric Orthopedics in Your Office. Laurel Saliman, MD Pediatric Orthopedic Surgeon Swedish Pediatric Specialty Care
 Pediatric Orthopedics in Your Office Laurel Saliman, MD Pediatric Orthopedic Surgeon Swedish Pediatric Specialty Care Overview for 20 minute whirlwind Clavicle Distal radius fractures Finger fractures
Pediatric Orthopedics in Your Office Laurel Saliman, MD Pediatric Orthopedic Surgeon Swedish Pediatric Specialty Care Overview for 20 minute whirlwind Clavicle Distal radius fractures Finger fractures
Orthotic Correction of Blount's Disease
 Orthotic Correction of Blount's Disease by Terry J. Supan, C.P.O. John M. Mazur, M.D. INTRODUCTION Infantile tibia vara is the result of abnormal growth in the proximal tibial epiphyseal late of the tibial
Orthotic Correction of Blount's Disease by Terry J. Supan, C.P.O. John M. Mazur, M.D. INTRODUCTION Infantile tibia vara is the result of abnormal growth in the proximal tibial epiphyseal late of the tibial
Bow legs in young children can be a
 ONLINE EXCLUSIVE ORIGINAL RESEARCH Management of bow legs in children: A primary care protocol This protocol, which is designed to coincide with wellchild visits, distinguishes between normal physiologic
ONLINE EXCLUSIVE ORIGINAL RESEARCH Management of bow legs in children: A primary care protocol This protocol, which is designed to coincide with wellchild visits, distinguishes between normal physiologic
Hip Dysplasia for the Primary Care Physician George Gantsoudes, MD. November 4, 2017
 Hip Dysplasia for the Primary Care Physician George Gantsoudes, MD November 4, 2017 Introduction Developmental Dysplasia of the Hip DDH - preferred term Teratologic hips Subluxation Dislocation-usually
Hip Dysplasia for the Primary Care Physician George Gantsoudes, MD November 4, 2017 Introduction Developmental Dysplasia of the Hip DDH - preferred term Teratologic hips Subluxation Dislocation-usually
The Surgical Management of Rickets & Osteogenesis Imperfecta
 The Surgical Management of Rickets & Osteogenesis Imperfecta Dr Greg Firth Chris Hani Baragwanath Academic Hospital Department of Orthopaedics University of the Witwatersrand Rickets Inadequate mineralization
The Surgical Management of Rickets & Osteogenesis Imperfecta Dr Greg Firth Chris Hani Baragwanath Academic Hospital Department of Orthopaedics University of the Witwatersrand Rickets Inadequate mineralization
A Patient s Guide to Osgood-Schlatter Lesion of the Knee
 A Patient s Guide to Osgood-Schlatter Lesion of the Knee Anatomy What part of the knee is affected? Introduction An Osgood-Schlatter lesion involves pain and swelling in the small bump of bone on the front
A Patient s Guide to Osgood-Schlatter Lesion of the Knee Anatomy What part of the knee is affected? Introduction An Osgood-Schlatter lesion involves pain and swelling in the small bump of bone on the front
New Patient Information Form
 New Patient Information Form Patient Identification Prenatal Alcohol & Drug Exposure Clinic FASD CLINIC Patient s OHIP N. Female Male Race Patient s Name Birth Date Age First Middle Last Patient s Address
New Patient Information Form Patient Identification Prenatal Alcohol & Drug Exposure Clinic FASD CLINIC Patient s OHIP N. Female Male Race Patient s Name Birth Date Age First Middle Last Patient s Address
LEG LENGTH INEQUALITY: Sports Medicine Perspective
 LEG LENGTH INEQUALITY: Sports Medicine Perspective Debra A. Zillmer, M.D. M&M Orthopaedics, Ltd 18 Year Old Experienced Cross Country Runner: Sept Sr Year Pain in left lower leg with running Pain now prevents
LEG LENGTH INEQUALITY: Sports Medicine Perspective Debra A. Zillmer, M.D. M&M Orthopaedics, Ltd 18 Year Old Experienced Cross Country Runner: Sept Sr Year Pain in left lower leg with running Pain now prevents
Preliminary Outcome Using a New Free Motion Offloading KAFO for Postoperative Management of Hemiepiphysiodesis in Adolescent Tibia Vara
 Preliminary Outcome Using a New Free Motion Offloading KAFO for Postoperative Management of Hemiepiphysiodesis in Adolescent Tibia Vara Joseph W. Whiteside CO/LO 1399 E. Western Reserve Road, Poland, OH
Preliminary Outcome Using a New Free Motion Offloading KAFO for Postoperative Management of Hemiepiphysiodesis in Adolescent Tibia Vara Joseph W. Whiteside CO/LO 1399 E. Western Reserve Road, Poland, OH
CONNECTICUT CHILDREN S MEDICAL CENTER. Gait Analysis
 CONNECTICUT CHILDREN S MEDICAL CENTER Gait Analysis Why do Gait Analysis? Analyzing how someone walks can be difficult from observation and clinical examination alone. Gait analysis provides objective
CONNECTICUT CHILDREN S MEDICAL CENTER Gait Analysis Why do Gait Analysis? Analyzing how someone walks can be difficult from observation and clinical examination alone. Gait analysis provides objective
SCRIPT: Module 3. Interpreting the WHO Growth Charts for Canada SLIDE NUMBER SLIDE SCRIPT
 SCRIPT: Module 3 Interpreting the WHO Growth Charts for Canada 1 Welcome Welcome to Module 3 - Interpreting the WHO Growth Charts for Canada. Each of the modules in this training package has been designed
SCRIPT: Module 3 Interpreting the WHO Growth Charts for Canada 1 Welcome Welcome to Module 3 - Interpreting the WHO Growth Charts for Canada. Each of the modules in this training package has been designed
Evaluation of Gait Mechanics Using Computerized Plantar Surface Pressure Analysis and it s Relation to Common Musculoskeletal Problems
 Evaluation of Gait Mechanics Using Computerized Plantar Surface Pressure Analysis and it s Relation to Common Musculoskeletal Problems Laws of Physics effecting gait Ground Reaction Forces Friction Stored
Evaluation of Gait Mechanics Using Computerized Plantar Surface Pressure Analysis and it s Relation to Common Musculoskeletal Problems Laws of Physics effecting gait Ground Reaction Forces Friction Stored
EASING BACK PAIN DURING SEX
 EASING BACK PAIN DURING SEX Finding Comfortable Positions Sex and Back Pain When your back hurts, simple actions such as getting undressed or giving a hug may cause pain. If just the thought of having
EASING BACK PAIN DURING SEX Finding Comfortable Positions Sex and Back Pain When your back hurts, simple actions such as getting undressed or giving a hug may cause pain. If just the thought of having
Early Onset Scoliosis
 Early Onset Scoliosis GSF-0616-326 Created in collaboration with: Growing Spine Foundation 555 East Wells Street, Suite 1100 Milwaukee, WI 53202 USA P: (414) 276-6445 F: (414) 276-3349 info@growingspine.org
Early Onset Scoliosis GSF-0616-326 Created in collaboration with: Growing Spine Foundation 555 East Wells Street, Suite 1100 Milwaukee, WI 53202 USA P: (414) 276-6445 F: (414) 276-3349 info@growingspine.org
Toe-Walking. Benign Variant or Scourge of Bipedal Locomotion? Definition. Physical Exam. Absent Heel Strike 2/28/2011
 Toe-Walking Benign Variant or Scourge of Bipedal Locomotion? Definition Absent Heel Strike +/- Equinus Thoughout Gait Cycle +/- Knee Hyperextension +/- Hip Flexion Physical Exam +/- Equinus Contracture
Toe-Walking Benign Variant or Scourge of Bipedal Locomotion? Definition Absent Heel Strike +/- Equinus Thoughout Gait Cycle +/- Knee Hyperextension +/- Hip Flexion Physical Exam +/- Equinus Contracture
The best way to deal with back pain
 The best way to deal with back pain The best way to deal with back pain Back pain is common and can be very painful but, serious or permanent damage is rare. The Facts Most back pain is not due to any
The best way to deal with back pain The best way to deal with back pain Back pain is common and can be very painful but, serious or permanent damage is rare. The Facts Most back pain is not due to any
Plantar fasciitis occurs when the strong band of tissue that supports the arch of your foot becomes irritated and inflamed.
 Plantar Fasciitis and Bone Spurs Plantar fasciitis (fashee-eye-tiss) is the most common cause of pain on the bottom of the heel. Approximately 2 million patients are treated for this condition every year.
Plantar Fasciitis and Bone Spurs Plantar fasciitis (fashee-eye-tiss) is the most common cause of pain on the bottom of the heel. Approximately 2 million patients are treated for this condition every year.
Normal Values of Tibio-Femoral Angle in Nigerian Adolescents
 ISPUB.COM The Internet Journal of Orthopedic Surgery Volume 17 Number 1 Normal Values of Tibio-Femoral Angle in Nigerian Adolescents T BA, A AO, O AB Citation T BA, A AO, O AB.. The Internet Journal of
ISPUB.COM The Internet Journal of Orthopedic Surgery Volume 17 Number 1 Normal Values of Tibio-Femoral Angle in Nigerian Adolescents T BA, A AO, O AB Citation T BA, A AO, O AB.. The Internet Journal of
RN(EC) ENC(C) GNC(C) MN ACNP *** MECHANISM OF INJURY.. MOST IMPORTANT ***
 ENC(C) GNC(C) MN ACNP *** MECHANISM OF INJURY.. MOST IMPORTANT ***") HISTORY *** MECHANISM OF INJURY.. MOST IMPORTANT *** Age of patient - Certain conditions are more prevalent in particular age groups (Hip pain in children may refer to the knee from Legg-Calve-Perthes
HISTORY *** MECHANISM OF INJURY.. MOST IMPORTANT *** Age of patient - Certain conditions are more prevalent in particular age groups (Hip pain in children may refer to the knee from Legg-Calve-Perthes
Screening in well baby clinic
 Screening in well baby clinic Dr. Abdulmoein Al-Agha, Ass. Professor & Consultant Pediatrician, KAUH & Erfan Hospital, Jeddah Well baby clinic IS Not only for vaccinations and check up for fever & URTI!!!
Screening in well baby clinic Dr. Abdulmoein Al-Agha, Ass. Professor & Consultant Pediatrician, KAUH & Erfan Hospital, Jeddah Well baby clinic IS Not only for vaccinations and check up for fever & URTI!!!
SWASH CERTIFICATION EXAM
 SWASH CERTIFICATION EXAM Sitting Walking And Standing Hip Orthosis Today s Date: Location: Name: License #: Employer: Address: Ste/Apt #: City: State: Zip: Email Address: 1) Which of the following are
SWASH CERTIFICATION EXAM Sitting Walking And Standing Hip Orthosis Today s Date: Location: Name: License #: Employer: Address: Ste/Apt #: City: State: Zip: Email Address: 1) Which of the following are
Considerations in the selection of patients for Selective Dorsal Rhizotomy
 Considerations in the selection of patients for Selective Dorsal Rhizotomy The best and the worst surgery I have ever been associated with. A therapist's perspective Dean Morgan, PT Disclosure Statement
Considerations in the selection of patients for Selective Dorsal Rhizotomy The best and the worst surgery I have ever been associated with. A therapist's perspective Dean Morgan, PT Disclosure Statement
This article is also available in Spanish: Fascitis plantar y protuberancias óseas (topic.cfm?topic=a00702).
.") 1 of 5 17 Oct 2015 11:04 AM This article is also available in Spanish: Fascitis plantar y protuberancias óseas (topic.cfm?topic=a00702). Plantar fasciitis (fashee-eye-tiss) is the most common cause of
1 of 5 17 Oct 2015 11:04 AM This article is also available in Spanish: Fascitis plantar y protuberancias óseas (topic.cfm?topic=a00702). Plantar fasciitis (fashee-eye-tiss) is the most common cause of
Introduction. Anatomy
 the patella is called the quadriceps mechanism. Though we think of it as a single device, the quadriceps mechanism has two separate tendons, the quadriceps tendon on top of the patella and the patellar
the patella is called the quadriceps mechanism. Though we think of it as a single device, the quadriceps mechanism has two separate tendons, the quadriceps tendon on top of the patella and the patellar
Bow legs and knock knees: is it physiological or pathological?
 International Journal of Contemporary Pediatrics Ganavi R. Int J Contemp Pediatr. 2016 May;3(2):687691 http://www.ijpediatrics.com pissn 23493283 eissn 23493291 Clinical Perspective DOI: http://dx.doi.org/10.18203/23493291.ijcp20161068
International Journal of Contemporary Pediatrics Ganavi R. Int J Contemp Pediatr. 2016 May;3(2):687691 http://www.ijpediatrics.com pissn 23493283 eissn 23493291 Clinical Perspective DOI: http://dx.doi.org/10.18203/23493291.ijcp20161068
You may have heard different things from your friends or from family members about arthritis.
 A Publication of the National Center for Farmworker Health Let s Talk About Arthritis You may have heard different things from your friends or from family members about arthritis. For example, you may
A Publication of the National Center for Farmworker Health Let s Talk About Arthritis You may have heard different things from your friends or from family members about arthritis. For example, you may
Plantar Fasciitis and Heel Pain
 PATIENT INFORMATION Plantar Fasciitis and Heel Pain What is plantar fasciitis? Heel pain and plantar fasciitis Plantar fasciitis causes pain under your heel. It usually goes in time. Treatment may speed
PATIENT INFORMATION Plantar Fasciitis and Heel Pain What is plantar fasciitis? Heel pain and plantar fasciitis Plantar fasciitis causes pain under your heel. It usually goes in time. Treatment may speed
Overview. Acceptance criteria for all protocols
 X-Ray protocol Overview The Smith & Nephew VISIONAIRE X-Ray protocol is essentially an AP leg length image. The images are preferred to be done erect, but can be done supine if necessary due to the type
X-Ray protocol Overview The Smith & Nephew VISIONAIRE X-Ray protocol is essentially an AP leg length image. The images are preferred to be done erect, but can be done supine if necessary due to the type
UNIVERSITY OF WASHINGTON
 UNIVERSITY OF WASHINGTON THE FETAL ALCOHOL SYNDROME DIAGNOSTIC AND PREVENTION NETWORK (FAS DPN) Center for Human Development and Disability Dear Sir or Madam, Thank you very much for your request for an
UNIVERSITY OF WASHINGTON THE FETAL ALCOHOL SYNDROME DIAGNOSTIC AND PREVENTION NETWORK (FAS DPN) Center for Human Development and Disability Dear Sir or Madam, Thank you very much for your request for an
SCOLIOSIS SCHOOL SCREENING
 SCOLIOSIS SCHOOL SCREENING WE VE GOT YOUR BACK Leigh Ann Lather MD FAAP Associate Professor Orthopaedics and Pediatrics MSK Bootcamp 2018 UVA ORTHOPAEDICS UVA ORTHOPAEDICS 13y4m BA = 12 13y10m Cobb>20
SCOLIOSIS SCHOOL SCREENING WE VE GOT YOUR BACK Leigh Ann Lather MD FAAP Associate Professor Orthopaedics and Pediatrics MSK Bootcamp 2018 UVA ORTHOPAEDICS UVA ORTHOPAEDICS 13y4m BA = 12 13y10m Cobb>20
HIP DYSPLASIA AND HYPOTONIA CAN STANDING IN ABDUCTION HELP?
 HIP DYSPLASIA AND HYPOTONIA CAN STANDING IN ABDUCTION HELP? Written by: MARY MILES, PT, DPT, ATP THIS CASE STUDY IS SPONSORED BY ALTIMATE MEDICAL Standing with hips in abduction has evolved as the new
HIP DYSPLASIA AND HYPOTONIA CAN STANDING IN ABDUCTION HELP? Written by: MARY MILES, PT, DPT, ATP THIS CASE STUDY IS SPONSORED BY ALTIMATE MEDICAL Standing with hips in abduction has evolved as the new
Hyperpronation of the foot causes many different
 IMMEDIATE CHANGES IN THE QUADRICEPS FEMORIS ANGLE AFTER INSERTION OF AN ORTHOTIC DEVICE D. Robert Kuhn, DC, a Terry R. Yochum, DC, b Anton R. Cherry, c and Sean S. Rodgers c ABSTRACT Objective: To measure
IMMEDIATE CHANGES IN THE QUADRICEPS FEMORIS ANGLE AFTER INSERTION OF AN ORTHOTIC DEVICE D. Robert Kuhn, DC, a Terry R. Yochum, DC, b Anton R. Cherry, c and Sean S. Rodgers c ABSTRACT Objective: To measure
ASSESSING GAIT IN CHILDREN WITH CP: WHAT TO DO WHEN YOU CAN T USE A GAIT LAB
 ASSESSING GAIT IN CHILDREN WITH CP: WHAT TO DO WHEN YOU CAN T USE A GAIT LAB Robert M. Kay, MD Vice Chief, Children s Orthopaedic Center Children s Hospital Los Angeles Professor of Orthopaedic Surgery
ASSESSING GAIT IN CHILDREN WITH CP: WHAT TO DO WHEN YOU CAN T USE A GAIT LAB Robert M. Kay, MD Vice Chief, Children s Orthopaedic Center Children s Hospital Los Angeles Professor of Orthopaedic Surgery
1/10/2017 PEDIATRIC LIMP: BOARD REVIEW GOALS & OBJECTIVES RELEVANCE DAVID POHL, D.O. PGY-3 ST. JOHN MACOMB-OAKLAND JANUARY 21, 2017
 PEDIATRIC LIMP: BOARD REVIEW DAVID POHL, D.O. PGY-3 ST. JOHN MACOMB-OAKLAND JANUARY 21, 2017 RELEVANCE AOBFP EXAM BLUEPRINT: ORTHO 5% PEDS 4% ADOLESCENTS 4% SPORTS 3 % http://static3.businessinsider.com/image/52545f89eab8ea62534aa515-1200-375/brain%20golfing.jpg
PEDIATRIC LIMP: BOARD REVIEW DAVID POHL, D.O. PGY-3 ST. JOHN MACOMB-OAKLAND JANUARY 21, 2017 RELEVANCE AOBFP EXAM BLUEPRINT: ORTHO 5% PEDS 4% ADOLESCENTS 4% SPORTS 3 % http://static3.businessinsider.com/image/52545f89eab8ea62534aa515-1200-375/brain%20golfing.jpg
Preserve or improve gait efficiency Early identification and stabilization or correction of lower extremity deformities
 ORTHOPEDICS Primary Outcomes Maintenance of a stable and balanced spine. Optimize pulmonary function. Avoid restrictive pulmonary disease. Optimize spinal growth. Avoid or facilitate healing of sacral/ischial
ORTHOPEDICS Primary Outcomes Maintenance of a stable and balanced spine. Optimize pulmonary function. Avoid restrictive pulmonary disease. Optimize spinal growth. Avoid or facilitate healing of sacral/ischial
Adolescent Hip Dysplasia
 Adolescent Hip Dysplasia The hip is a "ball-and-socket" joint. In a normal hip, the ball at the upper end of the femur (thighbone) fits firmly into the socket, which is a curved portion of the pelvis called
Adolescent Hip Dysplasia The hip is a "ball-and-socket" joint. In a normal hip, the ball at the upper end of the femur (thighbone) fits firmly into the socket, which is a curved portion of the pelvis called
QuickTime and a decompressor are needed to see this picture. QuickTime and a decompressor are needed to see this picture.
 The Hip Andrew Pearse Consultant Trauma and Orthopaedics Worcestershire Acute Hospitals NHS Trust Introduction Brief anatomy and topography History & examination Osteoarthritis Investigations Referral
The Hip Andrew Pearse Consultant Trauma and Orthopaedics Worcestershire Acute Hospitals NHS Trust Introduction Brief anatomy and topography History & examination Osteoarthritis Investigations Referral
Effects of Immobilization. N24 Pedi Musculoskeletal Spring 2012, Week 14. Cabrillo ADN/C. Madsen RN, MSN 1. Physical effects on other systems
 Common Orthopedic Problems of Children Congenital Acquired Bones Neuromuscular Physical effects on other systems Pulmonary Cardiac Skin integrity Elimination GI GU 1 4 General Nursing Considerations any
Common Orthopedic Problems of Children Congenital Acquired Bones Neuromuscular Physical effects on other systems Pulmonary Cardiac Skin integrity Elimination GI GU 1 4 General Nursing Considerations any
WHY BASIC HIP FLEXOR STRETCHES DON'T ALWAYS WORK
 WHY BASIC HIP FLEXOR STRETCHES DON'T ALWAYS WORK Do you do a daily stretching routine only to find that your muscles tighten back up throughout the day? Do you continue to stretch your hamstrings but still
WHY BASIC HIP FLEXOR STRETCHES DON'T ALWAYS WORK Do you do a daily stretching routine only to find that your muscles tighten back up throughout the day? Do you continue to stretch your hamstrings but still
ChiroCredit.com Presents Biomechanics: Focus on
 ChiroCredit.com Presents Biomechanics: Focus on the Knee Presented by: Ivo Waerlop, DC Shawn Allen, DC 1 Focus on The Knee 2 Pertinent Anatomy Femur Tibia Fibula Patella Prepatellar bursa Infrapatellar
ChiroCredit.com Presents Biomechanics: Focus on the Knee Presented by: Ivo Waerlop, DC Shawn Allen, DC 1 Focus on The Knee 2 Pertinent Anatomy Femur Tibia Fibula Patella Prepatellar bursa Infrapatellar
Valgus Knee Deformities in Children with Juvenile Chronic Polyarthritis Treated by Epiphysial Stapling
 Archives of Disease in Childhood, 1970, 45, 388. Valgus Knee Deformities in Children with Juvenile Chronic Polyarthritis Treated by Epiphysial Stapling B. M. ANSELL, G. P. ARDEN, and I. McLENNAN* From
Archives of Disease in Childhood, 1970, 45, 388. Valgus Knee Deformities in Children with Juvenile Chronic Polyarthritis Treated by Epiphysial Stapling B. M. ANSELL, G. P. ARDEN, and I. McLENNAN* From
The Hip from Cradle to Grave. Haemish Crawford Ascot Hospital Starship Children s Hospital
 The Hip from Cradle to Grave Haemish Crawford Ascot Hospital Starship Children s Hospital Developmental dysplasia hip DDH Irritable vs. septic hip Perthes disease Slipped Upper Femoral Epiphysis (SUFE)
The Hip from Cradle to Grave Haemish Crawford Ascot Hospital Starship Children s Hospital Developmental dysplasia hip DDH Irritable vs. septic hip Perthes disease Slipped Upper Femoral Epiphysis (SUFE)
Management of knee flexion contractures in patients with Cerebral Palsy
 Management of knee flexion contractures in patients with Cerebral Palsy Emmanouil Morakis Orthopaedic Consultant Royal Manchester Children s Hospital 1. Introduction 2. Natural history 3. Pathophysiology
Management of knee flexion contractures in patients with Cerebral Palsy Emmanouil Morakis Orthopaedic Consultant Royal Manchester Children s Hospital 1. Introduction 2. Natural history 3. Pathophysiology
Welcome to Pediatric Occupational Therapy
 Occupational Therapy General Intake Form 5/2014 1 Welcome to Pediatric Occupational Therapy Please fill out this form as thoroughly as possible. Should you have any questions or do not understand a statement
Occupational Therapy General Intake Form 5/2014 1 Welcome to Pediatric Occupational Therapy Please fill out this form as thoroughly as possible. Should you have any questions or do not understand a statement
Patella Instability in Children and Adolescents
 Patella Instability in Children and Adolescents Description Patella Instability is an injury to the kneecap (patella) affecting the joint it forms with the thigh bone (femur) Patella Instability can occur
Patella Instability in Children and Adolescents Description Patella Instability is an injury to the kneecap (patella) affecting the joint it forms with the thigh bone (femur) Patella Instability can occur
History. History and Physical Exam of the Pediatric Patient. History of Present Illness. Chief Complaint. Past Medical History. Past Medical History
 History History and Physical Exam of the Pediatric Patient Colleen A. Kraft, M.D., FAAP Richmond Pediatric Associates, Inc. Source Who is giving the history? Is this the patient s primary caretaker? 1
History History and Physical Exam of the Pediatric Patient Colleen A. Kraft, M.D., FAAP Richmond Pediatric Associates, Inc. Source Who is giving the history? Is this the patient s primary caretaker? 1
The Limping Child. Todd Milbrandt, MD Division Chair Pediatric Orthopaedics Mayo Clinic Rochester
 The Limping Child Todd Milbrandt, MD Division Chair Pediatric Orthopaedics Mayo Clinic Rochester Faculty Disclosure No disclosures relevant to this talk Practice Gap Primary Care Providers are faced with
The Limping Child Todd Milbrandt, MD Division Chair Pediatric Orthopaedics Mayo Clinic Rochester Faculty Disclosure No disclosures relevant to this talk Practice Gap Primary Care Providers are faced with
1. Review specialty services and programs available through Shriners Hospitals for Children
 Outreach Clinics: Creating Accessibility to Specialty Healthcare for Rural Families Presented By: Erin Jurkovich Director of Professional Relations Shriners Hospitals for Children Twin Cities June 15,
Outreach Clinics: Creating Accessibility to Specialty Healthcare for Rural Families Presented By: Erin Jurkovich Director of Professional Relations Shriners Hospitals for Children Twin Cities June 15,
Balanced Body Movement Principles
 Balanced Body Movement Principles How the Body Works and How to Train it. Module 3: Lower Body Strength and Power Developing Strength, Endurance and Power The lower body is our primary source of strength,
Balanced Body Movement Principles How the Body Works and How to Train it. Module 3: Lower Body Strength and Power Developing Strength, Endurance and Power The lower body is our primary source of strength,
Knee arthroscopy surgery
 Patient information Knee arthroscopy surgery i Important information for all orthopaedic patients undergoing knee arthroscopy surgery. Golden Jubilee National Hospital Agamemnon Street Clydebank, G81 4DY
Patient information Knee arthroscopy surgery i Important information for all orthopaedic patients undergoing knee arthroscopy surgery. Golden Jubilee National Hospital Agamemnon Street Clydebank, G81 4DY
8/9/2017. Case Based: Beyond Medial Patellofemoral Ligament. Editorial Board AJSM Social Media. Consultant. Not talking about PF pain/chondrosis Rehab
 Case Based: Beyond Medial Patellofemoral Ligament Dr Alan Getgood MD FRCS(Tr&Orth) DipSEM Assistant Professor Orthopaedic Sport Medicine Fellowship Director The Fowler Kennedy Sport Medicine Clinic University
Case Based: Beyond Medial Patellofemoral Ligament Dr Alan Getgood MD FRCS(Tr&Orth) DipSEM Assistant Professor Orthopaedic Sport Medicine Fellowship Director The Fowler Kennedy Sport Medicine Clinic University
Physical Examination of the Knee
 History: Pain Traumatic vs. atraumatic Acute vs Chronic Mechanism of injury Swelling, catching, instability Previous evaluation and treatment General Setup Examine standing, sitting and supine Evaluate
History: Pain Traumatic vs. atraumatic Acute vs Chronic Mechanism of injury Swelling, catching, instability Previous evaluation and treatment General Setup Examine standing, sitting and supine Evaluate
Mr. Siva Chandrasekaran Orthopaedic Surgeon MBBS MSpMed MPhil (surg) FRACS
 FRACS") Bunion Surgery Most people with bunions find pain relief with simple treatments to reduce pressure on the big toe, such as wearing wider shoes or using pads in their shoes. However, if these measures do
Bunion Surgery Most people with bunions find pain relief with simple treatments to reduce pressure on the big toe, such as wearing wider shoes or using pads in their shoes. However, if these measures do
PLANTAR FASCIITIS - Advice & Rehabilitation Leaflet
 Dr Patrick Wheeler Consultant in Sport and Exercise Medicine Leicester General Hospital Gwendolen Road, Leicester, LE5 4PW Telephone: 0116 258 4365 Patient information and rehabilitation leaflet Plantar
Dr Patrick Wheeler Consultant in Sport and Exercise Medicine Leicester General Hospital Gwendolen Road, Leicester, LE5 4PW Telephone: 0116 258 4365 Patient information and rehabilitation leaflet Plantar
Adult Hip Dysplasia David S. Feldman, MD
 Adult Hip Dysplasia David S. Feldman, MD Chief of Pediatric Orthopedic Surgery Professor of Orthopedic Surgery & Pediatrics NYU Langone Medical Center & NYU Hospital for Joint Diseases Overview Adult hip
Adult Hip Dysplasia David S. Feldman, MD Chief of Pediatric Orthopedic Surgery Professor of Orthopedic Surgery & Pediatrics NYU Langone Medical Center & NYU Hospital for Joint Diseases Overview Adult hip
Scoliosis. About idiopathic scoliosis and its treatment. Patient and Family Education. What types of scoliosis are there?
 Patient and Family Education Scoliosis About idiopathic scoliosis and its treatment This handout covers the most common type of scoliosis, adolescent idiopathic scoliosis. Other types of scoliosis may
Patient and Family Education Scoliosis About idiopathic scoliosis and its treatment This handout covers the most common type of scoliosis, adolescent idiopathic scoliosis. Other types of scoliosis may
Cartilage Repair Center
 Cartilage Repair Center Tom Minas, MD, MS 901 45 th Street, Kimmel Bldg. Director West Palm Beach, FL 33407 www.cartilagerepaircenter.org P: 844-714-5293 561-844-5255 F: 561-844-5245 Jennifer Andersen,
Cartilage Repair Center Tom Minas, MD, MS 901 45 th Street, Kimmel Bldg. Director West Palm Beach, FL 33407 www.cartilagerepaircenter.org P: 844-714-5293 561-844-5255 F: 561-844-5245 Jennifer Andersen,