Management of knee flexion contractures in patients with Cerebral Palsy
|
|
|
- Kathleen Goodwin
- 5 years ago
- Views:
Transcription


1 Management of knee flexion contractures in patients with Cerebral Palsy Emmanouil Morakis Orthopaedic Consultant Royal Manchester Children s Hospital
2 1. Introduction 2. Natural history 3. Pathophysiology 4. Gait 5. Treatment 6. Non-operative 7. Surgical 8. Guided- growth 9. Examples Outline
3 Introduction UK incidence rate - 1 in 400 births 1,800 children diagnosed every year 30,000 children with CP in the UK 1 : 3 children with CP unable to walk
4 Brain injury Primary Effects Secondary Effects Tertiary Effects Loss of selective muscle control Abnormal muscle tone and strength Impaired sensation & balance Abnormal muscle & bone growth Adaptive mechanisms

5 KNEE most common problem - contracture of the hamstring muscles progression to fixed knee flexion contractures directly related: spasticity relative decreased growth rate of the length of the muscle fibers

6 Natural History early childhood Hamstring contractures - in early childhood Sitting children : the inability to sit for long periods Walking children : toe walkers with relatively extended knees in the jump gait pattern
 Fixed flexion")
7 Natural History late childhood Sitting more difficult except when the knees are flexed to 90 or more. Gait pattern - develop more knee flexion, walking on the toes (often with ankle equinus) Fixed flexion contractures develop
 Fixed knee")

8 Natural History adolescence Crouched gait pattern develops ( knees more flexion, feet collapse, hip flexion) Fixed knee flexion contractures deteriorate Tend to be worse in children who do no stand and spend all day sitting in a wheelchair (GMFCS 4 & 5)

9 Pathophysiology Most knee flexor muscles are two-joint muscles
10 Pathophysiology Spasticity abnormal stretch & inhibits growth Leads to muscle contractures Biarticular muscles more affected Main flexors affected: semitendinosus, semimembranosus and long head of the biceps femoris Secondary : gracilis, gastrocnemius

11 Pathophysiology Semitendinosus and semimembranosus have different configuration and fiber lengths. Allows the motor control system to use a wider length tension curve
12 Primary Pathology Decreased motor control & spasticity increases stiffness shortens the joint ROM over which there is active control Semitendinosus (shorter fiber lengths) - the most contracted muscle Then semimembranosus and biceps
13 Secondary Pathology Hamstring develop contractures prevent full extension Fixed flexion contracture develop ( contracture of the posterior knee capsule) Children always lie in bed or sit in a chair with the knees flexed or stand in a knee-flexed position capsule does not stretch


14 Tertiary Pathology Severe contractures (more than 30 ) - secondary changes can develop in the knee joint with flattening of the femoral condyles. tibia to start to hinge against the condyles rather than rotating around the arc of the condyles
 Difference of 15-20 - real difference between different")
15 Evaluation Monitoring - popliteal angle used to measure hamstring contracture Normal popliteal angles - increase with age (less than ) Difference of real difference between different examinations.

16 Evaluation Fixed knee flexion contracture - greater accuracy (within 5 ) with the goniometer Examination under anesthesia differentiate spasticity and contracture

17 Evaluation Ambulatory patients Instrumented Gait Analysis Hamstring spasticity and contracture measured with popliteal angle Popliteal angle - little correlation with knee flexion during gait
18 Normal Gait
19 Normal Gait


20 Gait Prerequisites of normal gait: 1. stance phase stability 2. swing phase clearance 3. foot preposition in terminal swing 4. adequate step length 5. energy conservation Primary function of the knee allow limb length adjustment provide stability in stance phase

21 Gait Hamstrings spasticity and knee flexion contractures knee stiffness excessive knee flexion Gait inefficient posterior pelvic tilt short step length poor knee extension in late swing crouch gait

22 Initial Contact Knee flexed shock absorption
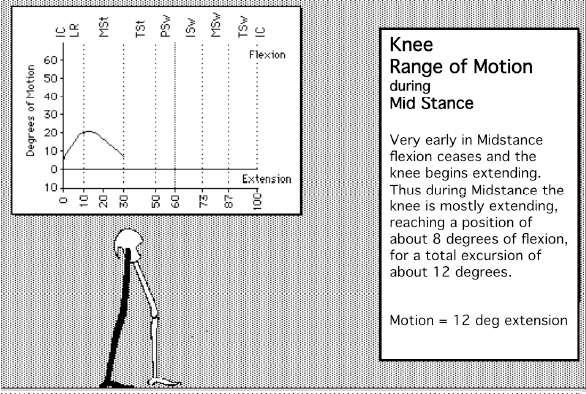
23 Mid-stance Knee starts extending

24 Terminal swing knee extending in preparation for initial contact
25 Example 11 y/o boy, spastic diplegia, GMFCS I Tight hamstrings Knee Extension Flexion Popliteal angle Uni Bilateral Functional angle 35 Patella alta Yes/No no no

26 Video
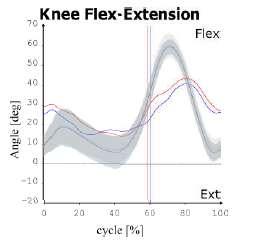
27 Kinematics
28 Indications of treatment Non-Walking patients 1. Prevent development of fixed contractures 2. Reduction of Pain 3. Improve sitting position 4. Allow standing transfers 5. Facilitate hygiene and care
29 Indications of treatment Ambulatory patients 1. Prevent development of fixed contractures 2. Reduce Pain 3. Maintain/Improve gait efficiency & physical function 4. Improve gait appearance
30 Goals of treatment ambulatory patients 1. Improve Mobility: Walk longer distances 2. More physically active 3. Participation in sports/recreational activity 4. Improve the appearance of gait 5. Improve fitness & endurance: Less tired 6. Better stability / Less tripping / Fewer falls


31 Treatment Orthopaedic Physiotherapy Surgery Orthotics Spasticity Management


32 Non-operative Physiotherapy Orthotics Spasticity Management (Botulinum toxin, SDR)
33 Surgical Management Ambulatory vs Non-Ambulatory Treatment Goals Age Severity of contractures Appropriate surgical dose

34 Distal Hamstring Lengthening Medial Hamstrings Rare lateral Fractional lengthening preferred Do not over-lengthen! Caution may cause or exacerbate anterior pelvic tilt recurvatum (back-kneeing)

35 Example Hamstring lengthening alone The knee more extended in stance but less flexion in swing (stiff knee gait)

")
36 Semitendinosus Transfer to the Adductor Tubercle Knee flexion in stance Contracture (5-20 degrees) GMFCS III - IV


37 Posterior knee capsulotomy Mild contractures Always with hamstrings and medial head gastrocnemius lengthening




38 Supracondylar Extension Osteotomy and Patellar Tendon Shortening Severe contractures Severe crouch gait with patella alta

39 Guided Growth Temporary & reversible epiphysiodesis allowing differential growth Extra-periosteal, non-locking plate, serves as a tension band
40 Guided Growth Indications: Fixed knee flexion deformity (> 10 degrees) 24 months or more predicted growth remaining The plates are applied outside the periosteum and the effects are reversible once removed Once the corrected - remove the proximal screw if the patient has growth remaining so reapplied if necessary in the future
 in order to avoid irritation of the")
41 The plates - medial and lateral to the sulcus (intracapsular, but not articular) in order to avoid irritation of the patella

42 Problems No long term studies Prominent (local bursitis) dystonic or mixed movement disorder These symptoms abate as the legs gradually straighten Caution patients crawl on knees
43 Advantages Early and full weight bearing Rapid return of knee motion Minimally invasive Advancement of the patellar tendon is usually not required

44 Surgical Technique

45 Surgical Technique

46 Example 1 13 y/o boy with spastic diplegia and knee flexion contractures

47


48
49

50
51 Example 2 14 y/o boy with spastic diplegia GMFCS II and stiff knee gait, frequent tripping
52 Pre-op Gait Analysis
53 Example 2 Underwent SEMLS Bilateral femoral derotation osteotomies Bilateral patella pull downs Medial hamstrings releases Rectus femoris release Bilateral gastro soleus recessions

54 Post-op Gait Analysis
55
56 Example 3 13 y/o boy with spastic diplegia GMFCS II with severe crouch
57 Pre-op Gait Analysis
58 Underwent SEMLS Bilateral distal femoral extension - derotation osteotomies Bilateral patellar advancement Bilateral supramalleolar derotation osteotomies


59 Post-op x-rays
60 Post-op Gait Aanalysis

61 Post-op Gait Analysis
62 Summary Surgical treatment for knee flexion contractures requires: 1. Thorough pre-op evaluation & planning 2. Realistic goals and expectations 3. Team approach 4. Appropriate timing of surgery 5. POST-OP REHAB 6. Post-op evaluation of outcomes meaningful to patients and family


63 Thank You

64
65 References Cerebral Palsy, F. Miller, Springer-Verlag, 2005 The Identification and Treatment of Gait Problems in Cerebral Palsy, J.Gage, Mac Keith Press, 2009 Pediatric Lower Limb Deformities, S. Sabharwal, Springer, 2016 Lovell and Winter's Pediatric Orthopaedics, S. Weinstein, LWW, 2013
אתגרים ופתרונות ניתוחיים סביב מפרק הברך בילדי CP ד"ר טלי בקר לאורטופדית ילדים,מרכז שניידר לרפואת ילדים
 אתגרים ופתרונות ניתוחיים סביב מפרק הברך בילדי CP היח' ד"ר טלי בקר לאורטופדית ילדים,מרכז שניידר לרפואת ילדים 1 CP- Spectrum of pathology 2 Lower Limb problems in CP Spastic Quadriplegia- Hip,Pelvis, Spine
אתגרים ופתרונות ניתוחיים סביב מפרק הברך בילדי CP היח' ד"ר טלי בקר לאורטופדית ילדים,מרכז שניידר לרפואת ילדים 1 CP- Spectrum of pathology 2 Lower Limb problems in CP Spastic Quadriplegia- Hip,Pelvis, Spine
10/26/2017. Comprehensive & Coordinated Orthopaedic Management of Children with CP. Objectives. It s all about function. Robert Bruce, MD Sayan De, MD
 Comprehensive & Coordinated Orthopaedic Management of Children with CP Robert Bruce, MD Sayan De, MD Objectives Understand varying levels of intervention are available to optimize function of children
Comprehensive & Coordinated Orthopaedic Management of Children with CP Robert Bruce, MD Sayan De, MD Objectives Understand varying levels of intervention are available to optimize function of children
AACPDM IC#21 DFEO+PTA 1
 Roles of Distal Femoral Extension Osteotomy and Patellar Tendon Advancement in the Treatment of Severe Persistent Crouch Gait in Adolescents and Young Adults with Cerebral Palsy Instructional Course #21
Roles of Distal Femoral Extension Osteotomy and Patellar Tendon Advancement in the Treatment of Severe Persistent Crouch Gait in Adolescents and Young Adults with Cerebral Palsy Instructional Course #21
ASSESSING GAIT IN CHILDREN WITH CP: WHAT TO DO WHEN YOU CAN T USE A GAIT LAB
 ASSESSING GAIT IN CHILDREN WITH CP: WHAT TO DO WHEN YOU CAN T USE A GAIT LAB Robert M. Kay, MD Vice Chief, Children s Orthopaedic Center Children s Hospital Los Angeles Professor of Orthopaedic Surgery
ASSESSING GAIT IN CHILDREN WITH CP: WHAT TO DO WHEN YOU CAN T USE A GAIT LAB Robert M. Kay, MD Vice Chief, Children s Orthopaedic Center Children s Hospital Los Angeles Professor of Orthopaedic Surgery
Muscle Testing of Knee Extensors. Yasser Moh. Aneis, PhD, MSc., PT. Lecturer of Physical Therapy Basic Sciences Department
 Muscle Testing of Knee Extensors Yasser Moh. Aneis, PhD, MSc., PT. Lecturer of Physical Therapy Basic Sciences Department Muscle Testing of Knee Extensors othe Primary muscle Quadriceps Femoris -Rectus
Muscle Testing of Knee Extensors Yasser Moh. Aneis, PhD, MSc., PT. Lecturer of Physical Therapy Basic Sciences Department Muscle Testing of Knee Extensors othe Primary muscle Quadriceps Femoris -Rectus
Lower Extremity Orthopedic Surgery in Cerebral Palsy
 Lower Extremity Orthopedic Surgery in Cerebral Palsy Hank Chambers, MD San Diego Children s Hospital San Diego, California Indications Fixed contracture Joint dislocations Shoe wear problems Pain Perineal
Lower Extremity Orthopedic Surgery in Cerebral Palsy Hank Chambers, MD San Diego Children s Hospital San Diego, California Indications Fixed contracture Joint dislocations Shoe wear problems Pain Perineal
Toe walking gives rise to parental concern. Therefore, toe-walkers are often referred at the 3 years of age.
 IDIOPATHIC TOE WALKING Toe walking is a common feature in immature gait and is considered normal up to 3 years of age. As walking ability improves, initial contact is made with the heel. Toe walking gives
IDIOPATHIC TOE WALKING Toe walking is a common feature in immature gait and is considered normal up to 3 years of age. As walking ability improves, initial contact is made with the heel. Toe walking gives
RN(EC) ENC(C) GNC(C) MN ACNP *** MECHANISM OF INJURY.. MOST IMPORTANT *** - Useful in determining mechanism of injury / overuse
 ENC(C) GNC(C) MN ACNP *** MECHANISM OF INJURY.. MOST IMPORTANT *** - Useful in determining mechanism of injury / overuse") HISTORY *** MECHANISM OF INJURY.. MOST IMPORTANT *** Age of patient Sport / Occupation - Certain conditions are more prevalent in particular age groups (Osgood Schlaters in youth / Degenerative Joint Disease
HISTORY *** MECHANISM OF INJURY.. MOST IMPORTANT *** Age of patient Sport / Occupation - Certain conditions are more prevalent in particular age groups (Osgood Schlaters in youth / Degenerative Joint Disease
Why Would Your Child Need to See Me?
 Why Would Your Child Need to See Me? Deborah M Eastwood Great Ormond St Hospital for Children, London The Royal National Orthopaedic Hospital, UK Disclosures I am an orthopaedic surgeon and I do operate
Why Would Your Child Need to See Me? Deborah M Eastwood Great Ormond St Hospital for Children, London The Royal National Orthopaedic Hospital, UK Disclosures I am an orthopaedic surgeon and I do operate
Case Study: Christopher
 Case Study: Christopher Conditions Treated Anterior Knee Pain, Severe Crouch Gait, & Hip Flexion Contracture Age Range During Treatment 23 Years to 24 Years David S. Feldman, MD Chief of Pediatric Orthopedic
Case Study: Christopher Conditions Treated Anterior Knee Pain, Severe Crouch Gait, & Hip Flexion Contracture Age Range During Treatment 23 Years to 24 Years David S. Feldman, MD Chief of Pediatric Orthopedic
Selective Motor Control Assessment of the Lower Extremity in Patients with Spastic Cerebral Palsy
 Overview Selective Motor Control Assessment of the Lower Extremity in Patients with Spastic Cerebral Palsy Marcia Greenberg MS, PT* Loretta Staudt MS, PT* Eileen Fowler PT, PhD Selective Motor Control
Overview Selective Motor Control Assessment of the Lower Extremity in Patients with Spastic Cerebral Palsy Marcia Greenberg MS, PT* Loretta Staudt MS, PT* Eileen Fowler PT, PhD Selective Motor Control
Theuseofgaitanalysisin orthopaedic surgical treatment in children with cerebral palsy
 Theuseofgaitanalysisin orthopaedic surgical treatment in children with cerebral palsy Aim of treatment Correction of functional disorder Requires analysis of function Basis for decision making Basis for
Theuseofgaitanalysisin orthopaedic surgical treatment in children with cerebral palsy Aim of treatment Correction of functional disorder Requires analysis of function Basis for decision making Basis for
Lever system. Rigid bar. Fulcrum. Force (effort) Resistance (load)
 Resistance (load)") Lever system lever is any elongated, rigid (bar) object that move or rotates around a fixed point called the fulcrum when force is applied to overcome resistance. Force (effort) Resistance (load) R Rigid
Lever system lever is any elongated, rigid (bar) object that move or rotates around a fixed point called the fulcrum when force is applied to overcome resistance. Force (effort) Resistance (load) R Rigid
MANUAL PRODUCT 3 RD EDITION. Pediatric Ankle Joint P: F: BeckerOrthopedic.com.
 PRODUCT MANUAL 3 RD EDITION P: 800-521-2192 248-588-7480 F: 800-923-2537 248-588-2960 BeckerOrthopedic.com Patent Pending 2018 Becker Orthopedic Appliance Co. All rights reserved. TRIPLE ACTION DIFFERENCE
PRODUCT MANUAL 3 RD EDITION P: 800-521-2192 248-588-7480 F: 800-923-2537 248-588-2960 BeckerOrthopedic.com Patent Pending 2018 Becker Orthopedic Appliance Co. All rights reserved. TRIPLE ACTION DIFFERENCE
Gait analysis and medical treatment strategy
 Gait analysis and medical treatment strategy Sylvain Brochard Olivier Rémy-néris, Mathieu Lempereur CHU and Pediatric Rehabilitation Centre Brest Course for European PRM trainees Mulhouse, October 22,
Gait analysis and medical treatment strategy Sylvain Brochard Olivier Rémy-néris, Mathieu Lempereur CHU and Pediatric Rehabilitation Centre Brest Course for European PRM trainees Mulhouse, October 22,
Changes in lower limb rotation after soft tissue surgery in spastic diplegia
 Acta Orthopaedica 2010; 81 (2): 245 249 245 Changes in lower limb rotation after soft tissue surgery in spastic diplegia 3-dimensional gait analysis in 28 children Bjørn Lofterød 1 and Terje Terjesen 2
Acta Orthopaedica 2010; 81 (2): 245 249 245 Changes in lower limb rotation after soft tissue surgery in spastic diplegia 3-dimensional gait analysis in 28 children Bjørn Lofterød 1 and Terje Terjesen 2
RN(EC) ENC(C) GNC(C) MN ACNP *** MECHANISM OF INJURY.. MOST IMPORTANT ***
 ENC(C) GNC(C) MN ACNP *** MECHANISM OF INJURY.. MOST IMPORTANT ***") HISTORY *** MECHANISM OF INJURY.. MOST IMPORTANT *** Age of patient - Certain conditions are more prevalent in particular age groups (Hip pain in children may refer to the knee from Legg-Calve-Perthes
HISTORY *** MECHANISM OF INJURY.. MOST IMPORTANT *** Age of patient - Certain conditions are more prevalent in particular age groups (Hip pain in children may refer to the knee from Legg-Calve-Perthes
Methods Patients A retrospective review of gait studies was conducted for all participants presented to the Motion Analysis
 58 Original article Predictors of outcome of distal rectus femoris transfer surgery in ambulatory children with cerebral palsy Susan A. Rethlefsen a, Galen Kam d, Tishya A.L. Wren a,b,c and Robert M. Kay
58 Original article Predictors of outcome of distal rectus femoris transfer surgery in ambulatory children with cerebral palsy Susan A. Rethlefsen a, Galen Kam d, Tishya A.L. Wren a,b,c and Robert M. Kay
Ankle Valgus in Cerebral Palsy
 Ankle Valgus in Cerebral Palsy Freeman Miller Contents Introduction... 2 Natural History... 2 Treatment... 3 Diagnostic Evaluations... 3 Indications for Intervention... 3 Outcome of Treatment... 5 Complications
Ankle Valgus in Cerebral Palsy Freeman Miller Contents Introduction... 2 Natural History... 2 Treatment... 3 Diagnostic Evaluations... 3 Indications for Intervention... 3 Outcome of Treatment... 5 Complications
Influence of surgery involving tendons around the knee joint on ankle motion during gait in patients with cerebral palsy
 Influence of surgery involving tendons around the knee joint on ankle motion during gait in patients with cerebral palsy Seung Yeol Lee, M.D., Ph.D. 1, Kyoung Min Lee, M.D., Ph.D. 2 Soon-Sun Kwon, Ph.D.
Influence of surgery involving tendons around the knee joint on ankle motion during gait in patients with cerebral palsy Seung Yeol Lee, M.D., Ph.D. 1, Kyoung Min Lee, M.D., Ph.D. 2 Soon-Sun Kwon, Ph.D.
CHAPTER 8: THE BIOMECHANICS OF THE HUMAN LOWER EXTREMITY
 CHAPTER 8: THE BIOMECHANICS OF THE HUMAN LOWER EXTREMITY _ 1. The hip joint is the articulation between the and the. A. femur, acetabulum B. femur, spine C. femur, tibia _ 2. Which of the following is
CHAPTER 8: THE BIOMECHANICS OF THE HUMAN LOWER EXTREMITY _ 1. The hip joint is the articulation between the and the. A. femur, acetabulum B. femur, spine C. femur, tibia _ 2. Which of the following is
FACTS 1. Most need only Gastro aponeurotic release [in positive Silverskiold test]
![FACTS 1. Most need only Gastro aponeurotic release [in positive Silverskiold test]](/thumbs/83/88335212.jpg "FACTS 1. Most need only Gastro aponeurotic release [in positive Silverskiold test]") FOOT IN CEREBRAL PALSY GAIT IN CEREBRAL PALSY I True Equinus II Jump gait III Apparent Equinus IV Crouch gait Group I True Equinus Extended hip and knee Equinus at ankle II Jump Gait [commonest] Equinus
FOOT IN CEREBRAL PALSY GAIT IN CEREBRAL PALSY I True Equinus II Jump gait III Apparent Equinus IV Crouch gait Group I True Equinus Extended hip and knee Equinus at ankle II Jump Gait [commonest] Equinus
Second Course Motion Analysis and clinics: why set up a Motion Analysis Lab?? TRAMA Project. January th Clinical case presentation
 Second Course Motion Analysis and clinics: why set up a Motion Analysis Lab?? - Clinical cases presentation - TRAMA Project January 14-17 th 2008 Iván Carlos Uribe Prada Instituto de Ortopedia Infantil
Second Course Motion Analysis and clinics: why set up a Motion Analysis Lab?? - Clinical cases presentation - TRAMA Project January 14-17 th 2008 Iván Carlos Uribe Prada Instituto de Ortopedia Infantil
DEFICIENCE MOTRICE CEREBRALE: INTERVENTIONS EN ORTHOPEDIE PEDIATRIQUE CAROLINE FORSYTHE MD, FRCSC RESUME SURVEILLANCE DES HANCHES
 DEFICIENCE MOTRICE CEREBRALE: INTERVENTIONS EN ORTHOPEDIE PEDIATRIQUE CAROLINE FORSYTHE MD, FRCSC RESUME SURVEILLANCE DES HANCHES TRAITMENTS NONCHIRURGICALES BOTOX PLATRES D INHIBITION APPROCHE CHIRURGICALE
DEFICIENCE MOTRICE CEREBRALE: INTERVENTIONS EN ORTHOPEDIE PEDIATRIQUE CAROLINE FORSYTHE MD, FRCSC RESUME SURVEILLANCE DES HANCHES TRAITMENTS NONCHIRURGICALES BOTOX PLATRES D INHIBITION APPROCHE CHIRURGICALE
Myology of the Knee. PTA 105 Kinesiology
 Myology of the Knee PTA 105 Kinesiology Objectives Describe the planes of motion and axes of rotation of the knee joint Visualize the origins and insertions of the muscles about the knee List the innervations
Myology of the Knee PTA 105 Kinesiology Objectives Describe the planes of motion and axes of rotation of the knee joint Visualize the origins and insertions of the muscles about the knee List the innervations
Prevention and Treatment of Injuries. Anatomy. Anatomy. Chapter 20 The Knee Westfield High School Houston, Texas
 Prevention and Treatment of Injuries Chapter 20 The Knee Westfield High School Houston, Texas Anatomy MCL, Medial Collateral Ligament LCL, Lateral Collateral Ligament PCL, Posterior Cruciate Ligament ACL,
Prevention and Treatment of Injuries Chapter 20 The Knee Westfield High School Houston, Texas Anatomy MCL, Medial Collateral Ligament LCL, Lateral Collateral Ligament PCL, Posterior Cruciate Ligament ACL,
Muscles of the Thigh. 6.1 Identify, describe the attachments of and deduce the actions of the muscles of the thigh: Anterior group
 Muscles of the Thigh 6.1 Identify, describe the attachments of and deduce the actions of the muscles of the thigh: Anterior group Sartorius: This is a long strap like muscle with flattened tendons at each
Muscles of the Thigh 6.1 Identify, describe the attachments of and deduce the actions of the muscles of the thigh: Anterior group Sartorius: This is a long strap like muscle with flattened tendons at each
Running Injuries in Children and Adolescents
 Running Injuries in Children and Adolescents Cook Children s SPORTS Symposium July 2, 2014 Running Injuries Overuse injuries Acute injuries Anatomic conditions 1 Overuse Injuries Pain that cannot be tied
Running Injuries in Children and Adolescents Cook Children s SPORTS Symposium July 2, 2014 Running Injuries Overuse injuries Acute injuries Anatomic conditions 1 Overuse Injuries Pain that cannot be tied
Muscles of the Hip 1. Tensor Fasciae Latae O: iliac crest I: lateral femoral condyle Action: abducts the thigh Nerve: gluteal nerve
 Muscles of the Hip 1. Tensor Fasciae Latae O: iliac crest I: lateral femoral condyle Action: abducts the thigh Nerve: gluteal nerve 2. Gluteus Maximus O: ilium I: femur Action: abduct the thigh Nerve:
Muscles of the Hip 1. Tensor Fasciae Latae O: iliac crest I: lateral femoral condyle Action: abducts the thigh Nerve: gluteal nerve 2. Gluteus Maximus O: ilium I: femur Action: abduct the thigh Nerve:
Total Hip Replacement Rehabilitation: Progression and Restrictions
 Total Hip Replacement Rehabilitation: Progression and Restrictions The success of total hip replacement (THR) is a result of predictable pain relief, improvements in quality of life, and restoration of
Total Hip Replacement Rehabilitation: Progression and Restrictions The success of total hip replacement (THR) is a result of predictable pain relief, improvements in quality of life, and restoration of
Cerebral palsy (CP) is the most common motor disability
 is the most common motor disability") CLINICAL Single- Event Multilevel Surgery to Correct Movement Disorders in Children With Cerebral Palsy Jane M. Wick, BSN, RN; Jing Feng, PhD; Ellen Raney, MD; Michael Aiona, MD ABSTRACT Cerebral palsy
CLINICAL Single- Event Multilevel Surgery to Correct Movement Disorders in Children With Cerebral Palsy Jane M. Wick, BSN, RN; Jing Feng, PhD; Ellen Raney, MD; Michael Aiona, MD ABSTRACT Cerebral palsy
SWASH CERTIFICATION EXAM
 SWASH CERTIFICATION EXAM Sitting Walking And Standing Hip Orthosis Today s Date: Location: Name: License #: Employer: Address: Ste/Apt #: City: State: Zip: Email Address: 1) Which of the following are
SWASH CERTIFICATION EXAM Sitting Walking And Standing Hip Orthosis Today s Date: Location: Name: License #: Employer: Address: Ste/Apt #: City: State: Zip: Email Address: 1) Which of the following are
Toe-Walking. Benign Variant or Scourge of Bipedal Locomotion? Definition. Physical Exam. Absent Heel Strike 2/28/2011
 Toe-Walking Benign Variant or Scourge of Bipedal Locomotion? Definition Absent Heel Strike +/- Equinus Thoughout Gait Cycle +/- Knee Hyperextension +/- Hip Flexion Physical Exam +/- Equinus Contracture
Toe-Walking Benign Variant or Scourge of Bipedal Locomotion? Definition Absent Heel Strike +/- Equinus Thoughout Gait Cycle +/- Knee Hyperextension +/- Hip Flexion Physical Exam +/- Equinus Contracture
Anatomy & Physiology. Muscles of the Lower Limbs.
 Anatomy & Physiology Muscles of the Lower Limbs http://www.ishapeup.com/musclecharts.html Muscles of the Lower Limbs Among the strongest muscles in the body. Because pelvic girdle is composed of heavy,
Anatomy & Physiology Muscles of the Lower Limbs http://www.ishapeup.com/musclecharts.html Muscles of the Lower Limbs Among the strongest muscles in the body. Because pelvic girdle is composed of heavy,
Gait Analysis: Qualitative vs Quantitative What are the advantages and disadvantages of qualitative and quantitative gait analyses?
 Gait Analysis: Qualitative vs Quantitative What are the advantages and disadvantages of qualitative and quantitative gait analyses? Basics of Gait Analysis Gait cycle: heel strike to subsequent heel strike,
Gait Analysis: Qualitative vs Quantitative What are the advantages and disadvantages of qualitative and quantitative gait analyses? Basics of Gait Analysis Gait cycle: heel strike to subsequent heel strike,
The Effects of Botulinum Toxin Type-A on Spasticity and Motor Function in Children with Cerebral Palsy
 Pacific University CommonKnowledge PT Critically Appraised Topics School of Physical Therapy 2014 The Effects of Botulinum Toxin Type-A on Spasticity and Motor Function in Children with Cerebral Palsy
Pacific University CommonKnowledge PT Critically Appraised Topics School of Physical Therapy 2014 The Effects of Botulinum Toxin Type-A on Spasticity and Motor Function in Children with Cerebral Palsy
Polio - A Model for Overuse and Aging. Acute Poliomyelitis. Acute Infection of Anterior Horn Motor Cells: Acute Polio Infection
 Polio - A Model for Overuse and Aging Mary Ann Keenan, M.D. Chief, Neuro-Orthopaedics Program Professor, Orthopaedic Surgery University of Pennsylvania Philadelphia, PA, USA Acute Poliomyelitis Acute viral
Polio - A Model for Overuse and Aging Mary Ann Keenan, M.D. Chief, Neuro-Orthopaedics Program Professor, Orthopaedic Surgery University of Pennsylvania Philadelphia, PA, USA Acute Poliomyelitis Acute viral
Surgical release of neurological hip luxation in children H. Klima Ostschweizer Kinderspital St. Gallen Abteilung für Kinderorthopädie
 Surgical release of neurological hip luxation in children H. Klima Ostschweizer Kinderspital St. Gallen Abteilung für Kinderorthopädie Development of hip luxation At birth these hips are normal developed,
Surgical release of neurological hip luxation in children H. Klima Ostschweizer Kinderspital St. Gallen Abteilung für Kinderorthopädie Development of hip luxation At birth these hips are normal developed,
Intoeing: When to Worry? Sukhdeep K. Dulai SPORC 2018
 Intoeing: When to Worry? Sukhdeep K. Dulai SPORC 2018 What is it? Intoeing: When to worry? Why isn t it always cause for worry? What are the benign causes of intoeing? What are the pathologic causes of
Intoeing: When to Worry? Sukhdeep K. Dulai SPORC 2018 What is it? Intoeing: When to worry? Why isn t it always cause for worry? What are the benign causes of intoeing? What are the pathologic causes of
Orthotic Management for Children with Cerebral Palsy
 Orthotic Management for Children with Cerebral Palsy Brian Emling, MSPO, CPO, LPO Brian.emling@choa.org Karl Barner, CPO, LPO karl.barner@choa.org Learning Objectives Inform audience of the general services
Orthotic Management for Children with Cerebral Palsy Brian Emling, MSPO, CPO, LPO Brian.emling@choa.org Karl Barner, CPO, LPO karl.barner@choa.org Learning Objectives Inform audience of the general services
HIP CASESTUDY 3. Body Chart-Initial Hypothesis: Property of VOMPTI, LLC. For Use of Participants Only. No Use or Reproduction Without Consent 1
 Body Chart-Initial Hypothesis: HIP CASESTUDY 3 Orthopaedic Manual Physical Therapy Series Charlottesville 2017-2018 Eric Magrum DPT OCS FAAOMPT Hamstring Strain HS Tendinopathy Lumbar Radiculopathy Lumbar
Body Chart-Initial Hypothesis: HIP CASESTUDY 3 Orthopaedic Manual Physical Therapy Series Charlottesville 2017-2018 Eric Magrum DPT OCS FAAOMPT Hamstring Strain HS Tendinopathy Lumbar Radiculopathy Lumbar
Human anatomy reference:
 Human anatomy reference: Weak Glut Activation Weak gluteal activation comes from poor biomechanics, poor awareness when training or prolonged exposure in deactivated positions such as sitting. Weak Glut
Human anatomy reference: Weak Glut Activation Weak gluteal activation comes from poor biomechanics, poor awareness when training or prolonged exposure in deactivated positions such as sitting. Weak Glut
Patellofemoral Instability
 Disclaimer This movie is an educational resource only and should not be used to manage Patellofemoral Instability. All decisions about the management of Patellofemoral Instability must be made in conjunction
Disclaimer This movie is an educational resource only and should not be used to manage Patellofemoral Instability. All decisions about the management of Patellofemoral Instability must be made in conjunction
Practical 1 Worksheet
 Practical 1 Worksheet ANATOMICAL TERMS 1. Use the word bank to fill in the missing words. reference side stand body arms palms anatomical forward All anatomical terms have a(n) point which is called the
Practical 1 Worksheet ANATOMICAL TERMS 1. Use the word bank to fill in the missing words. reference side stand body arms palms anatomical forward All anatomical terms have a(n) point which is called the
Clinical Evaluation and Imaging of the Patellofemoral Joint Common clinical syndromes
 Clinical Evaluation and Imaging of the Patellofemoral Joint Common clinical syndromes A. Panagopoulos Lecturer in Orthopaedics Medical School, Patras University Objectives Anatomy of patellofemoral joint
Clinical Evaluation and Imaging of the Patellofemoral Joint Common clinical syndromes A. Panagopoulos Lecturer in Orthopaedics Medical School, Patras University Objectives Anatomy of patellofemoral joint
Muscles to know. Lab 21. Muscles of the Pelvis and Lower Limbs. Muscles that Position the Lower Limbs. Generally. Muscles that Move the Thigh
 Muscles to know Lab 21 Muscles of the Pelvis, Leg and Foot psoas major iliacus gluteus maximus gluteus medius sartorius quadriceps femoris (4) gracilus adductor longus biceps femoris semitendinosis semimembranosus
Muscles to know Lab 21 Muscles of the Pelvis, Leg and Foot psoas major iliacus gluteus maximus gluteus medius sartorius quadriceps femoris (4) gracilus adductor longus biceps femoris semitendinosis semimembranosus
The Knee. Prof. Oluwadiya Kehinde
 The Knee Prof. Oluwadiya Kehinde www.oluwadiya.sitesled.com The Knee: Introduction 3 bones: femur, tibia and patella 2 separate joints: tibiofemoral and patellofemoral. Function: i. Primarily a hinge joint,
The Knee Prof. Oluwadiya Kehinde www.oluwadiya.sitesled.com The Knee: Introduction 3 bones: femur, tibia and patella 2 separate joints: tibiofemoral and patellofemoral. Function: i. Primarily a hinge joint,
Joints of the Lower Limb II
 Joints of the Lower Limb II Lecture Objectives Describe the components of the knee and ankle joint. List the ligaments associated with these joints and their attachments. List the muscles acting on these
Joints of the Lower Limb II Lecture Objectives Describe the components of the knee and ankle joint. List the ligaments associated with these joints and their attachments. List the muscles acting on these
PediLoc Extension Osteotomy Plate (PLEO)
") PediLoc Extension Osteotomy Plate (PLEO) Left PLEO Plates Sizes: 6, 8 and 10 hole plates Right PLEO Plates Sizes: 6, 8 and 10 hole plates PediLoc Extension Osteotomy Plate The technique description herein
PediLoc Extension Osteotomy Plate (PLEO) Left PLEO Plates Sizes: 6, 8 and 10 hole plates Right PLEO Plates Sizes: 6, 8 and 10 hole plates PediLoc Extension Osteotomy Plate The technique description herein
Metadata of the chapter that will be visualized online
 Metadata of the chapter that will be visualized online Chapter Title Copyright Year 2013 Copyright Holder The Knee in Cerebral Palsy Springer-Verlag Berlin Heidelberg Corresponding Author Family Name Strobl
Metadata of the chapter that will be visualized online Chapter Title Copyright Year 2013 Copyright Holder The Knee in Cerebral Palsy Springer-Verlag Berlin Heidelberg Corresponding Author Family Name Strobl
DR. (PROF.) ANIL ARORA MS
 ANIL ARORA MS") Hip Examination DR. (PROF.) ANIL ARORA MS (Ortho) DNB (Ortho) Dip SIROT (USA) FAPOA (Korea), FIGOF (Germany), FJOA (Japan) Commonwealth Fellow Joint Replacement (Royal National Orthopaedic Hospital, London,
Hip Examination DR. (PROF.) ANIL ARORA MS (Ortho) DNB (Ortho) Dip SIROT (USA) FAPOA (Korea), FIGOF (Germany), FJOA (Japan) Commonwealth Fellow Joint Replacement (Royal National Orthopaedic Hospital, London,
Patellofemoral Pain Syndrome
 43 Thames Street, St Albans, Christchurch 8013 Phone: (03) 356 1353. Website: philip-bayliss.com Patellofemoral Pain Syndrome Patellofemoral pain syndrome can be defined as a Retro-patellar (behind the
43 Thames Street, St Albans, Christchurch 8013 Phone: (03) 356 1353. Website: philip-bayliss.com Patellofemoral Pain Syndrome Patellofemoral pain syndrome can be defined as a Retro-patellar (behind the
Knee Joint Assessment and General View
 Knee Joint Assessment and General View Done by; Mshari S. Alghadier BSc Physical Therapy RHPT 366 m.alghadier@sau.edu.sa http://faculty.sau.edu.sa/m.alghadier/ Functional anatomy The knee is the largest
Knee Joint Assessment and General View Done by; Mshari S. Alghadier BSc Physical Therapy RHPT 366 m.alghadier@sau.edu.sa http://faculty.sau.edu.sa/m.alghadier/ Functional anatomy The knee is the largest
1-Apley scratch test.
 1-Apley scratch test. The patient attempts to touch the opposite scapula to test range of motion of the shoulder. 1-Testing abduction and external rotation( +ve sign touch the opposite scapula, -ve sign
1-Apley scratch test. The patient attempts to touch the opposite scapula to test range of motion of the shoulder. 1-Testing abduction and external rotation( +ve sign touch the opposite scapula, -ve sign
Modern Rx of Polio. with Ilizarov & new techniques
 Modern Rx of Polio with Ilizarov & new techniques Poliomyelitis Best Teacher of Orthopaedics Teaches Thorough clinical examination Muscle charting Gait Analysis Analysis of Joint Instability Precision
Modern Rx of Polio with Ilizarov & new techniques Poliomyelitis Best Teacher of Orthopaedics Teaches Thorough clinical examination Muscle charting Gait Analysis Analysis of Joint Instability Precision
UNIT 7 JOINTS. Knee and Ankle Joints DR. ABDEL-MONEM A. HEGAZY
 UNIT 7 JOINTS Knee and Ankle Joints BY DR. ABDEL-MONEM A. HEGAZY (Degree in Bachelor of Medicine and Surgery with honor 1983, Dipl."Gynaecology and Obstetrics "1989, Master "Anatomy and Embryology "1994,
UNIT 7 JOINTS Knee and Ankle Joints BY DR. ABDEL-MONEM A. HEGAZY (Degree in Bachelor of Medicine and Surgery with honor 1983, Dipl."Gynaecology and Obstetrics "1989, Master "Anatomy and Embryology "1994,
Physical Examination of the Knee
 History: Pain Traumatic vs. atraumatic Acute vs Chronic Mechanism of injury Swelling, catching, instability Previous evaluation and treatment General Setup Examine standing, sitting and supine Evaluate
History: Pain Traumatic vs. atraumatic Acute vs Chronic Mechanism of injury Swelling, catching, instability Previous evaluation and treatment General Setup Examine standing, sitting and supine Evaluate
Role Of The Fitness Professional. Causes of Fitness Related Injuries. The Assessments. Screening & Assessing: A Holistic Approach 2/9/2016
 Screening & Assessing: A Holistic Approach Role Of The Fitness Professional Fitness professionals must assess clientele, but need to understand the difference between medical diagnosis vs fitness limitations.
Screening & Assessing: A Holistic Approach Role Of The Fitness Professional Fitness professionals must assess clientele, but need to understand the difference between medical diagnosis vs fitness limitations.
The psoas minor is medial to the psoas major. The iliacus is a fan-shaped muscle that when contracted helps bring the swinging leg forward in walking
 1 p.177 2 3 The psoas minor is medial to the psoas major. The iliacus is a fan-shaped muscle that when contracted helps bring the swinging leg forward in walking and running. The iliopsoas and adductor
1 p.177 2 3 The psoas minor is medial to the psoas major. The iliacus is a fan-shaped muscle that when contracted helps bring the swinging leg forward in walking and running. The iliopsoas and adductor
Understanding and treating gait abnormality in Dravet syndrome
 Understanding and treating gait abnormality in Dravet syndrome Anne Stratton, MD, FAAP, FAAPMR Biennial Dravet Syndrome Foundation Family and Professional Conference July 19-22, 2018 Disclosures I have
Understanding and treating gait abnormality in Dravet syndrome Anne Stratton, MD, FAAP, FAAPMR Biennial Dravet Syndrome Foundation Family and Professional Conference July 19-22, 2018 Disclosures I have
From Childhood to Adulthood OMT for LOWER EXTREMITY Hip, Knee, Ankle, Foot. Objectives
 From Childhood to Adulthood OMT for LOWER EXTREMITY Hip, Knee, Ankle, Foot Jan Hendryx, DO, FAAO Peek n Peak CME March 1, 2019 Objectives 1. Demonstrate knowledge of the anatomy of the lower extremity-
From Childhood to Adulthood OMT for LOWER EXTREMITY Hip, Knee, Ankle, Foot Jan Hendryx, DO, FAAO Peek n Peak CME March 1, 2019 Objectives 1. Demonstrate knowledge of the anatomy of the lower extremity-
ANKLE PLANTAR FLEXION
 ANKLE PLANTAR FLEXION Evaluation and Measurements By Isabelle Devreux 1 Ankle Plantar Flexion: Gastrocnemius and Soleus ROM: 0 to 40-45 A. Soleus: Origin: Posterior of head of fibula and proximal1/3 of
ANKLE PLANTAR FLEXION Evaluation and Measurements By Isabelle Devreux 1 Ankle Plantar Flexion: Gastrocnemius and Soleus ROM: 0 to 40-45 A. Soleus: Origin: Posterior of head of fibula and proximal1/3 of
Arthritic history is similar to that of the hip. Add history of give way and locking, swelling
 KNEE VASU PAI Arthritic history is similar to that of the hip. Add history of give way and locking, swelling INJURY MECHANISM When How Sequence Progress Disability IKDC Activity I - Strenuous activity
KNEE VASU PAI Arthritic history is similar to that of the hip. Add history of give way and locking, swelling INJURY MECHANISM When How Sequence Progress Disability IKDC Activity I - Strenuous activity
Multiapical Deformities p. 97 Osteotomy Concepts and Frontal Plane Realignment p. 99 Angulation Correction Axis (ACA) p. 99 Bisector Lines p.
 p. 99 Bisector Lines p.") Normal Lower Limb Alignment and Joint Orientation p. 1 Mechanical and Anatomic Bone Axes p. 1 Joint Center Points p. 5 Joint Orientation Lines p. 5 Ankle p. 5 Knee p. 5 Hip p. 8 Joint Orientation Angles
Normal Lower Limb Alignment and Joint Orientation p. 1 Mechanical and Anatomic Bone Axes p. 1 Joint Center Points p. 5 Joint Orientation Lines p. 5 Ankle p. 5 Knee p. 5 Hip p. 8 Joint Orientation Angles
Apply this knowledge into proper management strategies and referrals
 1 2 3 Lower Extremity Injuries Jason Kennedy, M.D. Disclosures I have no financial/ industry disclosures. Objectives Identify common lower extremity injury patterns in the child and adolescent Apply this
1 2 3 Lower Extremity Injuries Jason Kennedy, M.D. Disclosures I have no financial/ industry disclosures. Objectives Identify common lower extremity injury patterns in the child and adolescent Apply this
5/14/2013. Acute vs Chronic Mechanism of Injury:
 Third Annual Young Athlete Conference: The Lower Extremity February 22, 2013 Audrey Lewis, DPT Acute vs Chronic Mechanism of Injury: I. Direct: blow to the patella II. Indirect: planted foot with a valgus
Third Annual Young Athlete Conference: The Lower Extremity February 22, 2013 Audrey Lewis, DPT Acute vs Chronic Mechanism of Injury: I. Direct: blow to the patella II. Indirect: planted foot with a valgus
Anterior knee pain.
 Anterior knee pain What are the symptoms? Anterior knee pain is very common amongst active adolescents and athletes participating in contact sports. It is one of the most common problems/injuries seen
Anterior knee pain What are the symptoms? Anterior knee pain is very common amongst active adolescents and athletes participating in contact sports. It is one of the most common problems/injuries seen
Changes in Sagittal Plane Kinematics and Kinetics after Distal Release of Medial Hamstrings in Cerebral Palsy
 J. Funct. Morphol. Kinesiol. 2016, 1, 6-15; doi:10.3390/jfmk1010006 Article Journal of Functional Morphology and Kinesiology ISSN 2411-5142 www.mdpi.com/journal/jfmk Changes in Sagittal Plane Kinematics
J. Funct. Morphol. Kinesiol. 2016, 1, 6-15; doi:10.3390/jfmk1010006 Article Journal of Functional Morphology and Kinesiology ISSN 2411-5142 www.mdpi.com/journal/jfmk Changes in Sagittal Plane Kinematics
DON T JUST PROVIDE A BAND-AID ELIZABETH COLE, MSPT, ATP U.S. Rehab / VGM
 DON T JUST PROVIDE A BAND-AID ELIZABETH COLE, MSPT, ATP U.S. Rehab / VGM Selecting the most appropriate product solutions for specific postural problems should be a thoughtful exercise in analyzing the
DON T JUST PROVIDE A BAND-AID ELIZABETH COLE, MSPT, ATP U.S. Rehab / VGM Selecting the most appropriate product solutions for specific postural problems should be a thoughtful exercise in analyzing the
Stretching Exercises for the Lower Body
 Stretching Exercises for the Lower Body Leg Muscles The leg has many muscles that allow us to walk, jump, run, and move. The main muscle groups are: Remember to: Warm-up your muscles first before stretching
Stretching Exercises for the Lower Body Leg Muscles The leg has many muscles that allow us to walk, jump, run, and move. The main muscle groups are: Remember to: Warm-up your muscles first before stretching
USE OF GAIT ANALYSIS IN SURGICAL TREATMENT PLANNING FOR PATIENTS WITH CEREBRAL PALSY
 USE OF GAIT ANALYSIS IN SURGICAL TREATMENT PLANNING FOR PATIENTS WITH CEREBRAL PALSY Robert M. Kay, M.D. Vice Chief, Children s Orthopaedic Center Children s Hospital Los Angeles Professor, Department
USE OF GAIT ANALYSIS IN SURGICAL TREATMENT PLANNING FOR PATIENTS WITH CEREBRAL PALSY Robert M. Kay, M.D. Vice Chief, Children s Orthopaedic Center Children s Hospital Los Angeles Professor, Department
Sports Rehabilitation & Performance Center Medial Patellofemoral Ligament Reconstruction Guidelines * Follow physician s modifications as prescribed
 The following MPFL guidelines were developed by the Sports Rehabilitation and Performance Center team at Hospital for Special Surgery. Progression is based on healing constraints, functional progression
The following MPFL guidelines were developed by the Sports Rehabilitation and Performance Center team at Hospital for Special Surgery. Progression is based on healing constraints, functional progression
A Patient s Guide to Rotational Deformities in Children
 A Patient s Guide to Rotational Deformities in Children 2350 Royal Boulevard Suite 200 Elgin, IL 60123 Phone: 847.931.5300 Fax: 847.931.9072 DISCLAIMER: The information in this booklet is compiled from
A Patient s Guide to Rotational Deformities in Children 2350 Royal Boulevard Suite 200 Elgin, IL 60123 Phone: 847.931.5300 Fax: 847.931.9072 DISCLAIMER: The information in this booklet is compiled from
Distal or supracondylar femoral osteotomy was first
 ORIGINAL ARTICLE Distal Femoral Osteotomy Using the LCP Pediatric Condylar 90-Degree Plate in Patients With Neuromuscular Disorders Erich Rutz, MD,*w Mark S. Gaston, MD, PhD,* Carlo Camathias, MD,* and
ORIGINAL ARTICLE Distal Femoral Osteotomy Using the LCP Pediatric Condylar 90-Degree Plate in Patients With Neuromuscular Disorders Erich Rutz, MD,*w Mark S. Gaston, MD, PhD,* Carlo Camathias, MD,* and
7/20/14. Patella Instability. Alignment. PF contact areas. Tissue Restraints. Pain. Acute Blunt force trauma Disorders of the Patellafemoral Joint
 Patella Instability Acute Blunt force trauma Disorders of the Patellafemoral Joint Evan G. Meeks, M.D. Orthopaedic Surgery Sports Medicine The University of Texas - Houston Pivoting action Large effusion
Patella Instability Acute Blunt force trauma Disorders of the Patellafemoral Joint Evan G. Meeks, M.D. Orthopaedic Surgery Sports Medicine The University of Texas - Houston Pivoting action Large effusion
MUSCLES OF THE LOWER LIMBS
 MUSCLES OF THE LOWER LIMBS Naming, location and general function Dr. Nabil khouri ROLES THAT SHOULD NOT BE FORGOTTEN Most anterior compartment muscles of the hip and thigh Flexor of the femur at the hip
MUSCLES OF THE LOWER LIMBS Naming, location and general function Dr. Nabil khouri ROLES THAT SHOULD NOT BE FORGOTTEN Most anterior compartment muscles of the hip and thigh Flexor of the femur at the hip
DOES RECTUS FEMORIS TRANSFER INCREASE KNEE FLEXION DURING STANCE PHASE IN CEREBRAL PALSY?
 DOI: http://dx.doi.org/10.1590/1413-785220162401145765 Original Article DOES RECTUS FEMORIS TRANSFER INCREASE KNEE FLEXION DURING STANCE PHASE IN CEREBRAL PALSY? Mauro César de Morais Filho 1,2,3, Francesco
DOI: http://dx.doi.org/10.1590/1413-785220162401145765 Original Article DOES RECTUS FEMORIS TRANSFER INCREASE KNEE FLEXION DURING STANCE PHASE IN CEREBRAL PALSY? Mauro César de Morais Filho 1,2,3, Francesco
Pilates for the Endurance Runner With Special Focus on the Hip Joint
 Pilates for the Endurance Runner With Special Focus on the Hip Joint Kellie McGeoy April 11 th, 2014 Aptos, CA 2013 1 Abstract: Endurance running is defined as any distance over 5 kilometers (3.1 miles)
Pilates for the Endurance Runner With Special Focus on the Hip Joint Kellie McGeoy April 11 th, 2014 Aptos, CA 2013 1 Abstract: Endurance running is defined as any distance over 5 kilometers (3.1 miles)
Medial Patellofemoral Ligament Reconstruction Guidelines Brian Grawe Protocol
 Medial Patellofemoral Ligament Reconstruction Guidelines Brian Grawe Protocol Progression is based on healing constraints, functional progression specific to the patient. Phases and time frames are designed
Medial Patellofemoral Ligament Reconstruction Guidelines Brian Grawe Protocol Progression is based on healing constraints, functional progression specific to the patient. Phases and time frames are designed
Physical Examination of the Knee
 History: Pain Traumatic vs. atraumatic? Acute vs Chronic Previous procedures done on the knee? Swelling, catching, instability General Setup Examine standing, sitting and supine Evaluate gait Examine hip
History: Pain Traumatic vs. atraumatic? Acute vs Chronic Previous procedures done on the knee? Swelling, catching, instability General Setup Examine standing, sitting and supine Evaluate gait Examine hip
Balanced Body Movement Principles
 Balanced Body Movement Principles How the Body Works and How to Train it. Module 3: Lower Body Strength and Power Developing Strength, Endurance and Power The lower body is our primary source of strength,
Balanced Body Movement Principles How the Body Works and How to Train it. Module 3: Lower Body Strength and Power Developing Strength, Endurance and Power The lower body is our primary source of strength,
Plaster-Wedging Technique:
 Plaster-Wedging Technique: An Appropriate, Safe, Quick, & Economical Method To Stretch Soft Tissue Contractures Of The Knee H.M. Steenbeek General Information. In the field of physical rehabilitation of
Plaster-Wedging Technique: An Appropriate, Safe, Quick, & Economical Method To Stretch Soft Tissue Contractures Of The Knee H.M. Steenbeek General Information. In the field of physical rehabilitation of
Jennifer L. Cook, MD
 Jennifer L. Cook, MD Florida Joint Replacement and Sports Medicine Center 5243 Hanff Lane New Port Richey, FL 34652 Phone: (727)848-4249 Fax: (727) 841-8934 ANTERIOR CRUCIATE LIGAMENT RECONSTRUCTION POST-OPERATIVE
Jennifer L. Cook, MD Florida Joint Replacement and Sports Medicine Center 5243 Hanff Lane New Port Richey, FL 34652 Phone: (727)848-4249 Fax: (727) 841-8934 ANTERIOR CRUCIATE LIGAMENT RECONSTRUCTION POST-OPERATIVE
WHY BASIC HIP FLEXOR STRETCHES DON'T ALWAYS WORK
 WHY BASIC HIP FLEXOR STRETCHES DON'T ALWAYS WORK Do you do a daily stretching routine only to find that your muscles tighten back up throughout the day? Do you continue to stretch your hamstrings but still
WHY BASIC HIP FLEXOR STRETCHES DON'T ALWAYS WORK Do you do a daily stretching routine only to find that your muscles tighten back up throughout the day? Do you continue to stretch your hamstrings but still
Does tendon lengthening surgery affect muscle tone in children with Cerebral Palsy?
 Acta Orthop. Belg., 2009, 75, 808-814 ORIGINAL STUDY Does tendon lengthening surgery affect muscle tone in children with Cerebral Palsy? Maria VLACHOU, Rosemary PIERCE, Rita Miranda DAVIS, Michael SUSSMAN
Acta Orthop. Belg., 2009, 75, 808-814 ORIGINAL STUDY Does tendon lengthening surgery affect muscle tone in children with Cerebral Palsy? Maria VLACHOU, Rosemary PIERCE, Rita Miranda DAVIS, Michael SUSSMAN
The Valgus Foot in Cerebral Palsy Equinovalgus not Plano-Valgus. Alfred D. Grant, M.D. David Feldman, M.D.
 The Valgus Foot in Cerebral Palsy Equinovalgus not Plano-Valgus Alfred D. Grant, M.D. David Feldman, M.D. Norman Otsuka, MD M.D. THE PURPOSE OF THIS PRESENTATION IS TO STATE CLEARLY THAT THE VALGUS FOOT
The Valgus Foot in Cerebral Palsy Equinovalgus not Plano-Valgus Alfred D. Grant, M.D. David Feldman, M.D. Norman Otsuka, MD M.D. THE PURPOSE OF THIS PRESENTATION IS TO STATE CLEARLY THAT THE VALGUS FOOT
Spasticity of muscles acting across joints in children
 ORIGINAL ARTICLE Static and Dynamic Gait Parameters Before and After Multilevel Soft Tissue Surgery in Ambulating Children With Cerebral Palsy Nicholas M. Bernthal, MD,* Seth C. Gamradt, MD,* Robert M.
ORIGINAL ARTICLE Static and Dynamic Gait Parameters Before and After Multilevel Soft Tissue Surgery in Ambulating Children With Cerebral Palsy Nicholas M. Bernthal, MD,* Seth C. Gamradt, MD,* Robert M.
In the name of god. Knee. By: Tofigh Bahraminia Graduate Student of the Pathology Sports and corrective actions. Heat: Dr. Babakhani. Nov.
 In the name of god Knee By: Tofigh Bahraminia Graduate Student of the Pathology Sports and corrective actions Heat: Dr. Babakhani Nov. 2014 1 Anatomy-Bones Bones Femur Medial/lateral femoral condyles articulate
In the name of god Knee By: Tofigh Bahraminia Graduate Student of the Pathology Sports and corrective actions Heat: Dr. Babakhani Nov. 2014 1 Anatomy-Bones Bones Femur Medial/lateral femoral condyles articulate
Knee Conditioning Program
 Prepared for: Prepared by: Purpose of Program After an injury or surgery, an exercise conditioning program will help you return to daily activities and enjoy a more active, healthy lifestyle. Following
Prepared for: Prepared by: Purpose of Program After an injury or surgery, an exercise conditioning program will help you return to daily activities and enjoy a more active, healthy lifestyle. Following
Ligamentous and Meniscal Injuries: Diagnosis and Management
 Ligamentous and Meniscal Injuries: Diagnosis and Management Daniel K Williams, MD Franciscan Physician Network Orthopedic Specialists September 29, 2017 No Financial Disclosures INTRODUCTION Overview of
Ligamentous and Meniscal Injuries: Diagnosis and Management Daniel K Williams, MD Franciscan Physician Network Orthopedic Specialists September 29, 2017 No Financial Disclosures INTRODUCTION Overview of
Orthopedic Issues in Children with Special Healthcare Needs
 Orthopedic Issues in Children with Special Healthcare Needs Kathryn A Keeler, MD Assistant Professor University of Missouri-Kansas City School of Medicine, Department of Orthopaedic Surgery and Department
Orthopedic Issues in Children with Special Healthcare Needs Kathryn A Keeler, MD Assistant Professor University of Missouri-Kansas City School of Medicine, Department of Orthopaedic Surgery and Department
1-Muscles: 2-Blood supply: Branches of the profunda femoris artery. 3-Nerve supply: Sciatic nerve
 1-Muscles: B i c e p s f e m o r i s S e m i t e n d i n o s u s S e m i m e m b r a n o s u s a small part of the adductor magnus (h a m s t r i n g p a r t o r i s c h i a l p a r t ) 2-Blood supply:
1-Muscles: B i c e p s f e m o r i s S e m i t e n d i n o s u s S e m i m e m b r a n o s u s a small part of the adductor magnus (h a m s t r i n g p a r t o r i s c h i a l p a r t ) 2-Blood supply:
Maximal isokinetic and isometric muscle strength of major muscle groups related to age, body weight, height, and sex in 178 healthy subjects
 Maximal isokinetic and isometric muscle strength of major muscle groups related to age, body weight, height, and sex in 178 healthy subjects Test protocol Muscle test procedures. Prior to each test participants
Maximal isokinetic and isometric muscle strength of major muscle groups related to age, body weight, height, and sex in 178 healthy subjects Test protocol Muscle test procedures. Prior to each test participants
Long-term results after single event multilevel surgery for the correction of gait disorders in spastic diplegic cerebral palsy. Dr.
 Long-term results after single event multilevel surgery for the correction of gait disorders in spastic diplegic cerebral palsy PhD dissertation Dr. Dóra Végvári Semmelweis University Clinical Medicine
Long-term results after single event multilevel surgery for the correction of gait disorders in spastic diplegic cerebral palsy PhD dissertation Dr. Dóra Végvári Semmelweis University Clinical Medicine
HUMAN BODY COURSE LOWER LIMB NERVES AND VESSELS
 HUMAN BODY COURSE LOWER LIMB NERVES AND VESSELS October 22, 2010 D. LOWER LIMB MUSCLES 2. Lower limb compartments ANTERIOR THIGH COMPARTMENT General lfunction: Hip flexion, knee extension, other motions
HUMAN BODY COURSE LOWER LIMB NERVES AND VESSELS October 22, 2010 D. LOWER LIMB MUSCLES 2. Lower limb compartments ANTERIOR THIGH COMPARTMENT General lfunction: Hip flexion, knee extension, other motions
Hamstring Strain. 43 Thames Street, St Albans, Christchurch 8013 Phone: (03) Website: philip-bayliss.com.
 Website: philip-bayliss.com.") 43 Thames Street, St Albans, Christchurch 8013 Phone: (03) 356 1353. Website: philip-bayliss.com Hamstring Strain The hamstring muscles are very susceptible to tears, strains and other common sporting
43 Thames Street, St Albans, Christchurch 8013 Phone: (03) 356 1353. Website: philip-bayliss.com Hamstring Strain The hamstring muscles are very susceptible to tears, strains and other common sporting
Recognizing common injuries to the lower extremity
 Recognizing common injuries to the lower extremity Bones Femur Patella Tibia Tibial Tuberosity Medial Malleolus Fibula Lateral Malleolus Bones Tarsals Talus Calcaneus Metatarsals Phalanges Joints - Knee
Recognizing common injuries to the lower extremity Bones Femur Patella Tibia Tibial Tuberosity Medial Malleolus Fibula Lateral Malleolus Bones Tarsals Talus Calcaneus Metatarsals Phalanges Joints - Knee
Do the hamstrings operate at increased muscle tendon lengths and velocities after surgical lengthening?
 Journal of Biomechanics 39 (2006) 1498 1506 2004 ASB Clinical Biomechanics Award Do the hamstrings operate at increased muscle tendon lengths and velocities after surgical lengthening? Allison S. Arnold
Journal of Biomechanics 39 (2006) 1498 1506 2004 ASB Clinical Biomechanics Award Do the hamstrings operate at increased muscle tendon lengths and velocities after surgical lengthening? Allison S. Arnold
A Single-Bar Above-Knee Orthosis
 A Single-Bar Above-Knee Orthosis Robert O. Nitschke,* C.P.O. I would like to present a different approach to the design of aboveknee, or "long leg", orthoses. When weight-bearing is not necessary, I have
A Single-Bar Above-Knee Orthosis Robert O. Nitschke,* C.P.O. I would like to present a different approach to the design of aboveknee, or "long leg", orthoses. When weight-bearing is not necessary, I have
A Patient s Guide to Knee Anatomy. Stephanie E. Siegrist, MD, LLC
 A Patient s Guide to Knee Anatomy Hands, shoulders, knees and toes (and elbows and ankles, too!) Most bone and joint conditions have several treatment options. The best treatment for you is based on your
A Patient s Guide to Knee Anatomy Hands, shoulders, knees and toes (and elbows and ankles, too!) Most bone and joint conditions have several treatment options. The best treatment for you is based on your