pthaigastro.org Caustic injury The 5 th Pediatric GI Days Pediatric GI & Liver Emergency : Current Practical Management
|
|
|
- Albert Kelley
- 5 years ago
- Views:
Transcription
1 The 5 th Pediatric GI Days Pediatric GI & Liver Emergency : Current Practical Management Caustic injury Phisek Yimyaem Pediatric Department, Khon Kaen Regional Hospital 18 July 2013
2 Outlines Introduction Type & mechanism Clinical manifestations Management & complications Severe corrosive ingestion in KKH Prevention Summary
3 Introduction Pediatric GI emergency Most often in first 3 years of life Most ingestions by children are accidental 75% of accidental ingestion: 2 nd containers Adolescents & young adult: related to attempted suicide ( more severe)
4 Corrosive ingestion : In KKH N = 5 ( M 2, F3 ) Mean age = 4 4 ingested acid ( HCl, 2 sulfuric acid, formic acid ) 1 ingesed weak base All from secondary container 4/5 EGD : abnormal 2 cases, normal 2 cases




5 Mechanisms of damage to UGI tract Strong alkaline: liquify tissue by dissolving & saponifying lipid producing liquefactive necrosis damages varies from minor erythema to deep ulceration or perforation Drain cleaner Oven cleaner Detergent Hair relaxer


6 .o r g Mechanisms of damage to UGI tract ro Strong acid: ig a st coagulate proteins inhibit deeper damage pt ha Toilet cleaner Lead acid battery producing coagulative necrosis Eschar formation



7 Mechanisms of damage to UGI tract Medication in pill : pill esophagitis Solid foreign bodies : perforation,pressure necrosis Pill esophagitis
8 Clinical manifestations Dysphagia Drooling Oropharygeal burn Retrosternal &Abdominal pain & vomiting Hematemesis Features suggesting upper airway injury (stridor, hoarseness, nasal flaring,retractions) ARDS
9 Clinical signs Drooling mucosal injury (Erythema,swelling, ulcer) Lack of visible damage in the mouth dose not preclude damage in lower in gut
10 Principle of management Stabilize ABCs, appropriate treatment of airway injury and hypotension Intubation may be necessary in respiratory distress External decontamination by copious irrigation with water min. History should focus on agent involved - amount, time of ingestion - intention ( severe) - child abuse (very small children & infants)
11 General management Do not induce emesis No gastric lavage or activated charcoal Neutralization should be avoid Dilution with water or milk may be useful ( intermediate ) NPO Intravenous fluid Chest X-ray Emergency endoscopy
12 Objective for Endoscopy Categorize the extend and grade of injury visible damage circumferential ulceration (grade 2b or greater) organs are involved Guided for treatment and indicated prognosis
13 When Endoscopy Endoscope if indicated warning sign Favor Early endoscopy > late endoscope Within 24 hours if possible Appropriate to identify the full extent of injury Should be avoid during 5 15 days post ingestion None of warning sign : watch and observe
14 Warning signs Drooling Dysphagia Abdominal pain & vomiting Visible mouth lesions Airway embarrassment Intentional ingestion
15 Zargar s classification of caustic injury Grade Visible appearance Clinical significance 0 Hx+ve, no symptom&visible damage Able to take fluids immediately 1 Edema, loss of normal vv pattern, hyperremia, no transmucosal injury 2a 2b 3a Transmucosal injury, friability, hemorrhage, blistering, exudate, scattered superficial ulceration 2a plus deep discrete ulceration and/or circumferential ulceration Scattered deep ulceration with necrosis of tissue Temporary dysphagia, able to swallow within 0-2 days, no long term sequalae Scarring, no stenosis, no long term sequalae Small risk of perforation,scarring may result in later stenosis Risk of perforation, high risk of later stenosis 3b Extensive necrotic tissue High risk of perforation and death, high risk of stenosis (1991)
16 Management of grade 2a or less Adequate nutrition (by mouth if possible) Repeat endoscopy at 2-3 wk (optional )
17 Management of grade 2 or higher ICU care Nutritional supplement : TPN Maintain acid reduction therapy (PPI twice daily) until completed healing Considered long term prophylaxis acid-suppressing Rx ATB; grade 2b or greater or fever Retained NG tube for feeding & stent
18 Corticosteroids : friend or foe? Still controversy in prevention of stricture May have use in the second or third degree injury Prednisolone 1-2 mg/kg/day to a maximum of 60 mg/day, tapered over a -3- week course Only a single controlled trial: Dexamethasone 1MKD may be benefit ( Bautista et al,eur Pediatr Surg 1996: ) High dose steroids for several weeks: increase complication
19 Corticosteroids (2) Systematic review, 6 studies in Europe ( 2=steroid,2= no steroid,2 compared with and without steroid) (steroid x 8 days) Pts with 2 nd and 3 rd degree burns (N=572) 305 pts ( 35.1%) with steroid VS 267 pts ( 33.3%) without steroid developed stricture Steroids do not prevent the development of strictures and may lead to the development of serious adverse effects (Peldova et al, Toxicol Rev,2005:125-9)
20 Complications Lip, mouth, oropharygeal burn Airway obstruction Esophageal & gastric perforation Mediastinitis Tracheoesophageal fistula Stricture formation Pyloric stenosis Late development of carcinoma
21 Follow up Grade 2 or greater : esophagogram (3 wk after ingestion) If present stricture, started dilatation Application of Mitomycin C or other agent (halofunginone) Other modality: laser or surgery Monitor other late complication Sliding hiatus hernia & GERD Motility disorder Pulmonary aspiration & chronic pulmonary disease Esophageal cancer
22 Severe corrosive ingestion : experience in KKH
23 In KKH : case 1 A 3 - yr old girl Accidentally ingested formic acid in secondary container Exfoliative skin and swelling of upper and lower lips Erythema of oral mucosa Stridor due to UAO


24 Case 1 : EGD esophagus stomach
25 Case 1 : hospital course Tracheostomy UGI study 1 mo after : no stricture

26 Case 1 : hospital course 3 mo after develops dysphagia and drooling : esophageal stricture Perform esophageal dilatation
 in secondary container V/ S : stable Erythema in oral")
27 In KKH : case 2 A 2 -yr - old boy Accidentally ingested toilet cleaner ( VIM,hydrochloric acid 13% w/w ) in secondary container V/ S : stable Erythema in oral cavity No stridor





28 EG junction pt ha ig a esophagus st ro.o r g Case 2 : EGD body antrum
29 Case 2 : hospital course 1 mo after : develops frequent vomiting UGI study : gastric outlet obstruction Perform gastro-jejunostomy
30 In KKH : case 3 4 yr-old boy Accidentally ingested of glass cleaners in secondary container ( Isopropyl alcohol,na lauryl ether sulfate,ethylene glycol N-Butyl ether ) Drooling,abdominal pain and vomiting 3 hours after,dysnea : on ETT No endoscopy


31 Case 3 : Chemical pneumonitis D1 Day 1 D3
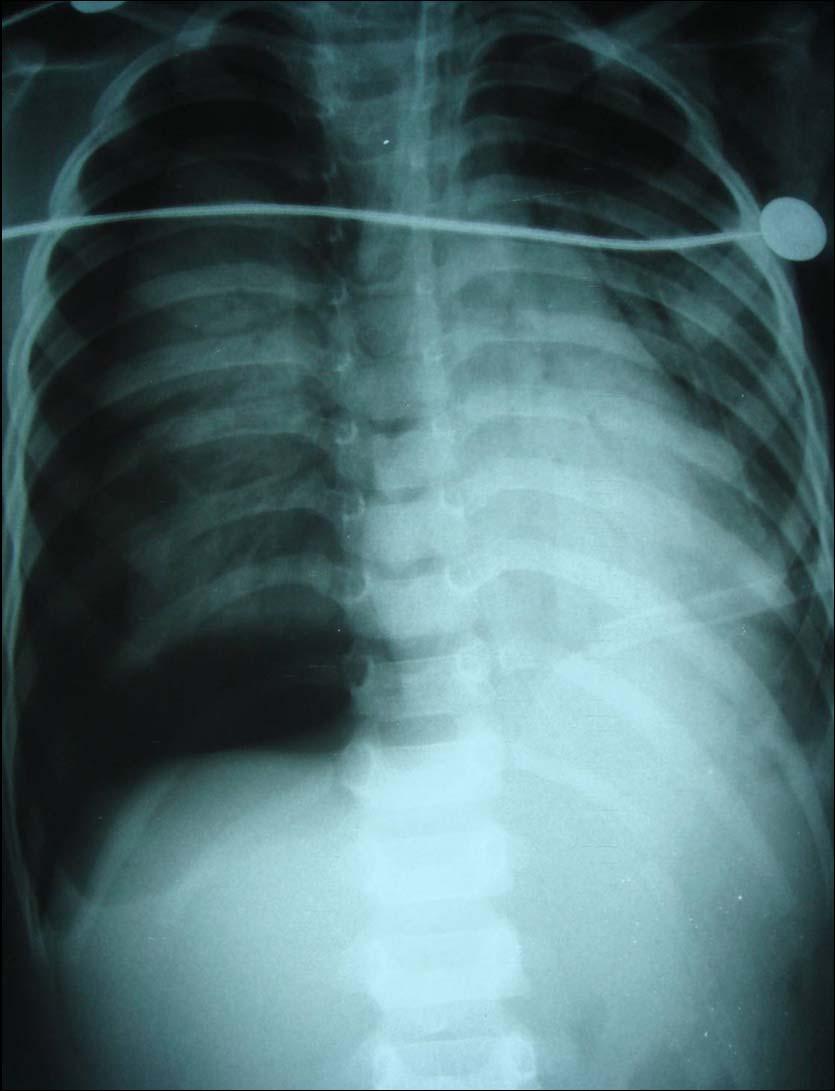

32 Case 3 : pneumothorax D 4 D 4 Day 3
33 Prevention Banned sale of granular and concentrated household cleaners Child-safe containers with warning signs Sale of secondary containers should be banned Safe storage Warnings on disk battery or toys packages Fluid before pill medication and upright position

34 Prevention : secondary containers

35 pt ha ig a st ro.o r g Prevention : childproof cap


36 pt ha ig a st ro.o r g Prevention : warning sign
37 Do not induce emesis, lavage, neutralization, NPO, IV fluid Consider EGD within 12 hr after congestion Grade 0-1 Grade 2 Grade 3 Supportive Rx start oral feeding D/C with education Summary : Acute abdomen series if suspected perforation NG placement after EGD consider steroid &ATB& PPI & NPO1wk Esophageal stricture Esophageal dilatation NG placement after EGD consider steroid &ATB& PPI NPO1wk,start TPN Esophagogram 3 wk after ingestion No stricture D/C & F/U injury prevention & education


38
Esophageal injuries. 新光急診張志華醫師 Facebook.com/jack119
 Esophageal injuries 新光急診張志華醫師 Facebook.com/jack119 Pre-test 1 What is the most common cause of esophageal injuries? A. Traffic accidents B. Gunshot wounds C. Iatrogenic Pre-test 2 Which contrast agent
Esophageal injuries 新光急診張志華醫師 Facebook.com/jack119 Pre-test 1 What is the most common cause of esophageal injuries? A. Traffic accidents B. Gunshot wounds C. Iatrogenic Pre-test 2 Which contrast agent
Caustic Esophageal Injury. Aliu Sanni, MD SUNY Downstate Medical Center March 21, 2013
 Caustic Esophageal Injury Aliu Sanni, MD SUNY Downstate Medical Center March 21, 2013 Case presentation 3F with no PMH presented to outside facility after drinking unmarked bottle containing oven cleaner
Caustic Esophageal Injury Aliu Sanni, MD SUNY Downstate Medical Center March 21, 2013 Case presentation 3F with no PMH presented to outside facility after drinking unmarked bottle containing oven cleaner
Esophageal injuries. Pre-test /11/10. 新光急診張志華醫師 Facebook.com/jack119. O What is the most common cause of esophageal injuries?
 Esophageal injuries 新光急診張志華醫師 Facebook.com/jack119 Pre-test 1 O What is the most common cause of esophageal injuries? A. Traffic accidents B. Gunshot wounds C. Iatrogenic 1 Pre-test 2 O Which contrast
Esophageal injuries 新光急診張志華醫師 Facebook.com/jack119 Pre-test 1 O What is the most common cause of esophageal injuries? A. Traffic accidents B. Gunshot wounds C. Iatrogenic 1 Pre-test 2 O Which contrast
Suspected Foreign Body Ingestion
 Teresa Liang Suspected Foreign Body Ingestion 1. General Presentation Background: Of more than 100,000 cases of foreign body ingestion reported each year in the United States, 80% occur in children, with
Teresa Liang Suspected Foreign Body Ingestion 1. General Presentation Background: Of more than 100,000 cases of foreign body ingestion reported each year in the United States, 80% occur in children, with
Pediatric Ingestion Injuries: Assessment & Treatment
 Pediatric Ingestion Injuries: Assessment & Treatment Benjamin L. Eithun, MSN, CRNP, RN, CPNP-AC, CCRN, TCRN Andrea L. Williams, PhD, RN UW Health & AFCH Case #1 Presentation Dispatched to Sandstone Ridge
Pediatric Ingestion Injuries: Assessment & Treatment Benjamin L. Eithun, MSN, CRNP, RN, CPNP-AC, CCRN, TCRN Andrea L. Williams, PhD, RN UW Health & AFCH Case #1 Presentation Dispatched to Sandstone Ridge
Chapter 153 Caustics. Episode Overview: Wisecracks. Key Points: Rosen s in Perspective
 Chapter 153 Caustics Episode Overview: 1) Compare acid and alkali caustic burns 2) Describe clinical features of significant airway and esophageal injury by caustics 3) What are indications for endoscopy
Chapter 153 Caustics Episode Overview: 1) Compare acid and alkali caustic burns 2) Describe clinical features of significant airway and esophageal injury by caustics 3) What are indications for endoscopy
Down the Tube: Caustic Ingestions. Significance & Management in the ED. Laura Chng PGY-3
 Down the Tube: Caustic Ingestions Significance & Management in the ED Laura Chng PGY-3 Caustic Ingestions Not common but you ll see them Controversial You drank WHAT? ED management can change outcome Who
Down the Tube: Caustic Ingestions Significance & Management in the ED Laura Chng PGY-3 Caustic Ingestions Not common but you ll see them Controversial You drank WHAT? ED management can change outcome Who
Acquired pediatric esophageal diseases Imaging approaches and findings. M. Mearadji International Foundation for Pediatric Imaging Aid
 Acquired pediatric esophageal diseases Imaging approaches and findings M. Mearadji International Foundation for Pediatric Imaging Aid Acquired pediatric esophageal diseases The clinical signs of acquired
Acquired pediatric esophageal diseases Imaging approaches and findings M. Mearadji International Foundation for Pediatric Imaging Aid Acquired pediatric esophageal diseases The clinical signs of acquired
KIDS PUT THINGS IN THE CRAZIEST PLACES...
 KIDS PUT THINGS IN THE CRAZIEST PLACES... YOU CAN T MAKE ME EAT MY DINNER! 2 year old observed to stuff corn up right nostril Judith Klein, MD FACEP Assistant Professor of Emergency Medicine UCSF-SFGH
KIDS PUT THINGS IN THE CRAZIEST PLACES... YOU CAN T MAKE ME EAT MY DINNER! 2 year old observed to stuff corn up right nostril Judith Klein, MD FACEP Assistant Professor of Emergency Medicine UCSF-SFGH
ESOPHAGEAL CANCER AND GERD. Prof Salman Guraya FRCS, Masters MedEd
 ESOPHAGEAL CANCER AND GERD Prof Salman Guraya FRCS, Masters MedEd Learning objectives Esophagus anatomy and physiology Esophageal cancer Causes, presentations of esophageal cancer Diagnosis and management
ESOPHAGEAL CANCER AND GERD Prof Salman Guraya FRCS, Masters MedEd Learning objectives Esophagus anatomy and physiology Esophageal cancer Causes, presentations of esophageal cancer Diagnosis and management
Update on the Diagnosis and Treatment of Caustic Ingestion
 The Ochsner Journal 9:54 59, 2009 f Academic Division of Ochsner Clinic Foundation Update on the Diagnosis and Treatment of Caustic Ingestion Michael Lupa, MD,* Jacqueline Magne,{ J. Lindhe Guarisco, MD,
The Ochsner Journal 9:54 59, 2009 f Academic Division of Ochsner Clinic Foundation Update on the Diagnosis and Treatment of Caustic Ingestion Michael Lupa, MD,* Jacqueline Magne,{ J. Lindhe Guarisco, MD,
DR. SAAD AL-MUHAYAWI, M.D., FRCSC. ORL Head & Neck Surgery
 TRAUMA IN ORL DR. SAAD AL-MUHAYAWI, M.D., FRCSC Associate Professor & Consultant ORL Head & Neck Surgery TYPES OF TRAUMA EAR & TEMPORAL BONE TRAUMA NOSE & FACIAL BONES TRAUMA LARYNGEAL TRAUMA NECK TRAUMA
TRAUMA IN ORL DR. SAAD AL-MUHAYAWI, M.D., FRCSC Associate Professor & Consultant ORL Head & Neck Surgery TYPES OF TRAUMA EAR & TEMPORAL BONE TRAUMA NOSE & FACIAL BONES TRAUMA LARYNGEAL TRAUMA NECK TRAUMA
Inflammation of the Esophagus (Esophagitis) Basics
 Basics") Inflammation of the Esophagus (Esophagitis) Basics OVERVIEW Inflammation of the esophagus typically involves the tubular area of the esophagus itself (known as the esophageal body ) and the muscular area
Inflammation of the Esophagus (Esophagitis) Basics OVERVIEW Inflammation of the esophagus typically involves the tubular area of the esophagus itself (known as the esophageal body ) and the muscular area
Foreign Body Management
 Foreign Body Management NYSGE Fellows Summer Course Susana Gonzalez, MD Assistant Professor of Medicine 1 Objectives Timing of endoscopy When? Anatomic location Where? High risk objects What? Choosing
Foreign Body Management NYSGE Fellows Summer Course Susana Gonzalez, MD Assistant Professor of Medicine 1 Objectives Timing of endoscopy When? Anatomic location Where? High risk objects What? Choosing
Back to Basics: What Imaging Test should I order? Jeanne G. Hill, M.D. Pediatric Radiology Medical University of South Carolina
 Back to Basics: What Imaging Test should I order? Jeanne G. Hill, M.D. Pediatric Radiology Medical University of South Carolina Disclosure Neither I nor any member of my immediate family has a relevant
Back to Basics: What Imaging Test should I order? Jeanne G. Hill, M.D. Pediatric Radiology Medical University of South Carolina Disclosure Neither I nor any member of my immediate family has a relevant
Oesophageal Disorders
 Oesophageal Disorders Anatomy Upper sphincter Oesophageal body Diaphragm Lower sphincter Gastric Cardia Symptoms Of Oesophageal Disorders Dysphagia Odynophagia Heartburn Atypical Chest Pain Regurgitation
Oesophageal Disorders Anatomy Upper sphincter Oesophageal body Diaphragm Lower sphincter Gastric Cardia Symptoms Of Oesophageal Disorders Dysphagia Odynophagia Heartburn Atypical Chest Pain Regurgitation
INTRODUCTION TO UPPER ENDOSCOPY
 INTRODUCTION TO UPPER ENDOSCOPY Satish Nagula, MD Associate Professor of Medicine Icahn School of Medicine at Mount Sinai NYSGE First Year Fellows Course July 14, 2018 Early endoscopes 1805: Bozzini Lichtleiter
INTRODUCTION TO UPPER ENDOSCOPY Satish Nagula, MD Associate Professor of Medicine Icahn School of Medicine at Mount Sinai NYSGE First Year Fellows Course July 14, 2018 Early endoscopes 1805: Bozzini Lichtleiter
Gastroesophageal Reflux Disease in Infants and Children
 Gastroesophageal Reflux Disease in Infants and Children 4 Marzo 2017 Drssa Chiara Leoni Drssa Valentina Giorgio pediatriagastro@gmail.com valentinagiorgio1@gmail.com Definitions: GER GER is the passage
Gastroesophageal Reflux Disease in Infants and Children 4 Marzo 2017 Drssa Chiara Leoni Drssa Valentina Giorgio pediatriagastro@gmail.com valentinagiorgio1@gmail.com Definitions: GER GER is the passage
 P R E S E N T S Dr. Mufa T. Ghadiali is skilled in all aspects of General Surgery. His General Surgery Services include: General Surgery Advanced Laparoscopic Surgery Surgical Oncology Gastrointestinal
P R E S E N T S Dr. Mufa T. Ghadiali is skilled in all aspects of General Surgery. His General Surgery Services include: General Surgery Advanced Laparoscopic Surgery Surgical Oncology Gastrointestinal
The Foreign Body. Neil H. Stollman, MD, FACG
 The Foreign Body Neil H. Stollman, MD, FACG Associate Clinical Professor of Medicine University of California San Francisco Chief, Division of Gastroenterology Alta Bates Summit Medical Center, Oakland,
The Foreign Body Neil H. Stollman, MD, FACG Associate Clinical Professor of Medicine University of California San Francisco Chief, Division of Gastroenterology Alta Bates Summit Medical Center, Oakland,
Poison (Toxicant): any substance or agent capable of producing a deleterious response in a biological system or living organism.
: any substance or agent capable of producing a deleterious response in a biological system or living organism.") Poison (Toxicant): any substance or agent capable of producing a deleterious response in a biological system or living organism. Poisoning= overdose toxicity intoxication= toxicity due to foreign substance
Poison (Toxicant): any substance or agent capable of producing a deleterious response in a biological system or living organism. Poisoning= overdose toxicity intoxication= toxicity due to foreign substance
AGA SECTION. Gastroenterology 2016;150:
 Gastroenterology 2016;150:1026 1030 April 2016 AGA Section 1027 Procedural intervention (3) Upper endoscopy indications 3 6 Non-response of symptoms to a 4 8 week empiric trial of twice-daily PPI Troublesome
Gastroenterology 2016;150:1026 1030 April 2016 AGA Section 1027 Procedural intervention (3) Upper endoscopy indications 3 6 Non-response of symptoms to a 4 8 week empiric trial of twice-daily PPI Troublesome
Faculty Disclosure. Objectives. State of the Art #3: Referrals for Gastroscopy (focus on common esophagus problems) 24/11/2014
 24/11/2014") State of the Art #3: Referrals for Gastroscopy (focus on common esophagus problems) Dr. Amy Morse November 2014 Faculty: Amy Morse Faculty Disclosure Relationships with commercial interests: Grants/Research
State of the Art #3: Referrals for Gastroscopy (focus on common esophagus problems) Dr. Amy Morse November 2014 Faculty: Amy Morse Faculty Disclosure Relationships with commercial interests: Grants/Research
Eosinophilic Esophagitis. Another Reason Not to Swallow
 Eosinophilic Esophagitis Another Reason Not to Swallow Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or
Eosinophilic Esophagitis Another Reason Not to Swallow Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or
PYLORIC STENOSIS: AN UNUSUAL COMPLICATION OF ALKALINE CORROSIVE POISONING*
 NOVEMBER, 1968 PYLORIC STENOSIS: AN UNUSUAL COMPLICATION OF ALKALINE CORROSIVE POISONING* By VIVIAN J. HARRIS, M.D.t COLUMBUS, T HE swallowing of an alkaline corrosive, such as sodium hydroxide (lye),
NOVEMBER, 1968 PYLORIC STENOSIS: AN UNUSUAL COMPLICATION OF ALKALINE CORROSIVE POISONING* By VIVIAN J. HARRIS, M.D.t COLUMBUS, T HE swallowing of an alkaline corrosive, such as sodium hydroxide (lye),
Formaldehyde (HCHO) C 1
 C 1") BASF Chemical Emergency Medical Guidelines Formaldehyde (HCHO) C 1 Information and recommendations for doctors at hospitals/emergency departments Patients exposed only to formaldehyde gas or vapor do not
BASF Chemical Emergency Medical Guidelines Formaldehyde (HCHO) C 1 Information and recommendations for doctors at hospitals/emergency departments Patients exposed only to formaldehyde gas or vapor do not
Endoscopic Treatment of Luminal Perforations and Leaks
 Endoscopic Treatment of Luminal Perforations and Leaks Ali A. Siddiqui, MD Professor of Medicine Director of Interventional Endoscopy Jefferson Medical College Philadelphia, PA When Do You Suspect a Luminal
Endoscopic Treatment of Luminal Perforations and Leaks Ali A. Siddiqui, MD Professor of Medicine Director of Interventional Endoscopy Jefferson Medical College Philadelphia, PA When Do You Suspect a Luminal
Disclosures. Repaired Esophageal Atresia and Tracheoesophageal Fistula and Chronic Dysphagia. Case Presentation. Case Presentation.
 Disclosures Repaired Esophageal Atresia and Tracheoesophageal Fistula and Chronic Dysphagia Dr. DeBoer is funded by Colorado Clinical and Translational Science Institute KL2 TR001080 Emily DeBoer MD Assistant
Disclosures Repaired Esophageal Atresia and Tracheoesophageal Fistula and Chronic Dysphagia Dr. DeBoer is funded by Colorado Clinical and Translational Science Institute KL2 TR001080 Emily DeBoer MD Assistant
Aliu Sanni MD SUNY Downstate Medical Center August 16, 2012
 Aliu Sanni MD SUNY Downstate Medical Center August 16, 2012 Case Presentation 60yr old AAF with PMH of CAD s/p PCI 1983, CVA, GERD, HTN presented with retrosternal chest pain on 06/12 Associated dysphagia
Aliu Sanni MD SUNY Downstate Medical Center August 16, 2012 Case Presentation 60yr old AAF with PMH of CAD s/p PCI 1983, CVA, GERD, HTN presented with retrosternal chest pain on 06/12 Associated dysphagia
GIT RADIOLOGY. Water-soluble contrast media (e.g. gastrograffin) are the other available agents.which doesn t cause inflammatory peritonitis..
 are the other available agents.which doesn t cause inflammatory peritonitis..") GIT RADIOLOGY Imaging techniques-general principles: Contrast examinations: Barium sulphate is the best contrast for GIT (with good mucosal coating & excellent opacification & being inert); but is contraindicated
GIT RADIOLOGY Imaging techniques-general principles: Contrast examinations: Barium sulphate is the best contrast for GIT (with good mucosal coating & excellent opacification & being inert); but is contraindicated
EGD Data Collection Form
 Sociodemographic Information Type Zip Code Gender Height (in inches) Race Ethnicity Inpatient Outpatient Male Female Birth Date Weight (in pounds) American Indian (Native American) or Alaska Native Asian
Sociodemographic Information Type Zip Code Gender Height (in inches) Race Ethnicity Inpatient Outpatient Male Female Birth Date Weight (in pounds) American Indian (Native American) or Alaska Native Asian
Eosinophilic Esophagitis (EoE)
") Eosinophilic Esophagitis (EoE) 01.06.2016 EoE: immune-mediated disorder food or environmental antigens => Th2 inflammatory response. Key cytokines: IL-4, IL-5, and IL-13 stimulate the production of eotaxin-3
Eosinophilic Esophagitis (EoE) 01.06.2016 EoE: immune-mediated disorder food or environmental antigens => Th2 inflammatory response. Key cytokines: IL-4, IL-5, and IL-13 stimulate the production of eotaxin-3
Nicholas J. Shaheen, MD. MPH Center for Esophageal Diseases and Swallowing University of North Carolina SOM
 Eosinophilic Esophagitis: Are We There Yet? Nicholas J. Shaheen, MD. MPH Center for Esophageal Diseases and Swallowing University of North Carolina SOM Learning Objectives Understand current definition
Eosinophilic Esophagitis: Are We There Yet? Nicholas J. Shaheen, MD. MPH Center for Esophageal Diseases and Swallowing University of North Carolina SOM Learning Objectives Understand current definition
Target Audience: Emergency Medicine Residents (junior and senior level postgraduate learners), Medical Students
, Medical Students") Caustic Ingestion Authors: Bailey M. Roche, Jonathan B. Ford, MD Reviewers: Miriam T. Davis, MD; Jennifer Hannum, MD Target Audience: Emergency Medicine Residents (junior and senior level postgraduate
Caustic Ingestion Authors: Bailey M. Roche, Jonathan B. Ford, MD Reviewers: Miriam T. Davis, MD; Jennifer Hannum, MD Target Audience: Emergency Medicine Residents (junior and senior level postgraduate
Swallowed Foreign Body
 Swallowed Foreign Body Page 1 of 5 INTRODUCTION Swallowed foreign bodies can be divided into five distinct groups: 1 Small blunt objects 2 Large blunt objects 3 Potentially poisonous objects 4 Sharp objects
Swallowed Foreign Body Page 1 of 5 INTRODUCTION Swallowed foreign bodies can be divided into five distinct groups: 1 Small blunt objects 2 Large blunt objects 3 Potentially poisonous objects 4 Sharp objects
GPS* Safety Summary for Sodium Hydroxide
 GPS* Safety Summary for Sodium Hydroxide Select a Topic: Names Product Overview Manufacture of Product Product Description Product Uses Exposure Potential Health Information Environmental Information Physical
GPS* Safety Summary for Sodium Hydroxide Select a Topic: Names Product Overview Manufacture of Product Product Description Product Uses Exposure Potential Health Information Environmental Information Physical
Managing Foreign Objects in the GI Tract Tips & Tricks
 Managing Foreign Objects in the GI Tract Tips & Tricks STEPHEN LANDRENEAU, MD Take home o Perform emergent endoscopy in cases of: Esophageal obstruction due to food bolus impaction or foreign object. Disk
Managing Foreign Objects in the GI Tract Tips & Tricks STEPHEN LANDRENEAU, MD Take home o Perform emergent endoscopy in cases of: Esophageal obstruction due to food bolus impaction or foreign object. Disk
Chapter 14: Training in Radiology. DDSEP Chapter 1: Question 12
 DDSEP Chapter 1: Question 12 A 52-year-old white male presents for evaluation of sudden onset of abdominal pain and shoulder pain. His past medical history is notable for a history of coronary artery disease,
DDSEP Chapter 1: Question 12 A 52-year-old white male presents for evaluation of sudden onset of abdominal pain and shoulder pain. His past medical history is notable for a history of coronary artery disease,
Module 2 Heartburn Glossary
 Absorption Antacids Antibiotic Module 2 Heartburn Glossary Barrett s oesophagus Bloating Body mass index Burping Chief cells Colon Digestion Endoscopy Enteroendocrine cells Epiglottis Epithelium Absorption
Absorption Antacids Antibiotic Module 2 Heartburn Glossary Barrett s oesophagus Bloating Body mass index Burping Chief cells Colon Digestion Endoscopy Enteroendocrine cells Epiglottis Epithelium Absorption
A Case of Severe Neonatal Dysphagia: Experience and Reason
 A Case of Severe Neonatal Dysphagia: Experience and Reason The Contemporary Management of Aerodigestive Disease in Children 2 nd Aerodigestive Meeting Vanderbilt University, Nashville, TN Friday, November
A Case of Severe Neonatal Dysphagia: Experience and Reason The Contemporary Management of Aerodigestive Disease in Children 2 nd Aerodigestive Meeting Vanderbilt University, Nashville, TN Friday, November
01/26/2010 GENERAL SURGERY ABSITE ANATOMY ANATOMY. Yvonne M. Carter, MD Georgetown University Medical Center. Layers. mucosa. squamous epithelium
 GENERAL SURGERY ABSITE REVIEW: ESOPHAGUS Yvonne M. Carter, MD Georgetown University Medical Center ANATOMY Layers mucosa muscle squamous epithelium columnar epithelium (distal 2cm) inner = circular outer
GENERAL SURGERY ABSITE REVIEW: ESOPHAGUS Yvonne M. Carter, MD Georgetown University Medical Center ANATOMY Layers mucosa muscle squamous epithelium columnar epithelium (distal 2cm) inner = circular outer
Disclosure. Learning Objectives 4/25/2014. I have no disclosures
 Alka Goyal MD Division of Pediatric Gastroenterology Hepatology and Nutrition Children s Hospital of Pittsburgh of UPMC Disclosure I have no disclosures Learning Objectives Diagnosis of Eosinophilic Esophagitis
Alka Goyal MD Division of Pediatric Gastroenterology Hepatology and Nutrition Children s Hospital of Pittsburgh of UPMC Disclosure I have no disclosures Learning Objectives Diagnosis of Eosinophilic Esophagitis
Chapter 9. An Unusual Case of Gastric Outlet Obstruction in a Ghanaian Woman. 2 Top 25 Clinical Case Reports
 Chapter 9 An Unusual Case of Gastric Outlet Obstruction in a Ghanaian Woman Joachim Amoako, Henry Obaka, Nelson Affram, Wordui Theodore and Faizal Z Asumda* Department of Surgery, Korle Bu Teaching Hospital,
Chapter 9 An Unusual Case of Gastric Outlet Obstruction in a Ghanaian Woman Joachim Amoako, Henry Obaka, Nelson Affram, Wordui Theodore and Faizal Z Asumda* Department of Surgery, Korle Bu Teaching Hospital,
The Management of Esophageal Strictures in Children
 Akram J. Jawad, FRCS(Ed); Asal Izzidien Al-Samarrai, FRCS,FACS; Abdullah Al-Rabeeah, MS,FRCS(C); Rashed Al-Rashed, FRCP(C) From the Divisions of Pediatric Surgery (Drs. Jawad, Al-Samarrai, Al-Rabeeah)
Akram J. Jawad, FRCS(Ed); Asal Izzidien Al-Samarrai, FRCS,FACS; Abdullah Al-Rabeeah, MS,FRCS(C); Rashed Al-Rashed, FRCP(C) From the Divisions of Pediatric Surgery (Drs. Jawad, Al-Samarrai, Al-Rabeeah)
A Multidisciplinary Approach to Esophageal Dysphagia: Role of the SLP. Darlene Graner, M.A., CCC-SLP, BRS-S Sharon Burton, M.D.
 A Multidisciplinary Approach to Esophageal Dysphagia: Role of the SLP Darlene Graner, M.A., CCC-SLP, BRS-S Sharon Burton, M.D. What is the role of the SLP? Historically SLPs the preferred providers for
A Multidisciplinary Approach to Esophageal Dysphagia: Role of the SLP Darlene Graner, M.A., CCC-SLP, BRS-S Sharon Burton, M.D. What is the role of the SLP? Historically SLPs the preferred providers for
Esophageal Eosinophilia and Eosinophilic Esophagitis. Bible Class 09. Mai 2018
 Esophageal Eosinophilia and Eosinophilic Esophagitis Bible Class 09. Mai 2018 61 yo male No upper-gi symptoms Gastroscopy vor bariatric Operation Lesion: Papilloma Histology of the surrounding mucosa:
Esophageal Eosinophilia and Eosinophilic Esophagitis Bible Class 09. Mai 2018 61 yo male No upper-gi symptoms Gastroscopy vor bariatric Operation Lesion: Papilloma Histology of the surrounding mucosa:
EGD. John M. Wo, M.D. University of Louisville July 3, 2008
 EGD John M. Wo, M.D. University of Louisville July 3, 2008 Different Ways to do an EGD Which scope? Pediatric, regular, jumbo EGD endoscope or pediatric colonoscope Transnasal vs. transoral insertion Sedation
EGD John M. Wo, M.D. University of Louisville July 3, 2008 Different Ways to do an EGD Which scope? Pediatric, regular, jumbo EGD endoscope or pediatric colonoscope Transnasal vs. transoral insertion Sedation
SARCINA VENTICULARI IS A POSSIBLE CAUSATIVE MICROORGANISM OTHER THAN H.PYLORI IN GASTRIC OUTLET OBSTRUCTION PATHOGENESIS
 SARCINA VENTICULARI IS A POSSIBLE CAUSATIVE MICROORGANISM OTHER THAN H.PYLORI IN GASTRIC OUTLET OBSTRUCTION PATHOGENESIS 55 years old male, Farm worker, married, from Ibb Heavy Smoker, Khat chewer non-alcohol
SARCINA VENTICULARI IS A POSSIBLE CAUSATIVE MICROORGANISM OTHER THAN H.PYLORI IN GASTRIC OUTLET OBSTRUCTION PATHOGENESIS 55 years old male, Farm worker, married, from Ibb Heavy Smoker, Khat chewer non-alcohol
Dysphagia. A Problem Swallowing Foods or Liquids
 Dysphagia A Problem Swallowing Foods or Liquids What Is Dysphagia? If you have a problem swallowing foods or liquids, you may have dysphagia. It has a number of causes. Your doctor can find out what is
Dysphagia A Problem Swallowing Foods or Liquids What Is Dysphagia? If you have a problem swallowing foods or liquids, you may have dysphagia. It has a number of causes. Your doctor can find out what is
Clinical Case Presentation. Jared B. Smith, M.D. Surgical Grand Rounds, August 21, 2006
 Clinical Case Presentation Jared B. Smith, M.D. Surgical Grand Rounds, August 21, 2006 Clinical History CC: Can t swallow anything HPI: 50 y.o. male from western Colorado, greater than 2 years of emesis
Clinical Case Presentation Jared B. Smith, M.D. Surgical Grand Rounds, August 21, 2006 Clinical History CC: Can t swallow anything HPI: 50 y.o. male from western Colorado, greater than 2 years of emesis
SUMPh N. Testemitanu Radiology and Medical imaging department PEDIATRIC IMAGING. M. Crivceanschii, assistant professor
 SUMPh N. Testemitanu Radiology and Medical imaging department PEDIATRIC IMAGING M. Crivceanschii, assistant professor GOALS AND OBJECTIVES to be aware of the role of modern diagnostic imaging modalities
SUMPh N. Testemitanu Radiology and Medical imaging department PEDIATRIC IMAGING M. Crivceanschii, assistant professor GOALS AND OBJECTIVES to be aware of the role of modern diagnostic imaging modalities
Caustic materials are useful but constitute a potential. Predictors of Esophageal Stricture in Children with Unintentional Ingestion of Caustic Agents
 Original Article 233 Predictors of Esophageal Stricture in hildren with Unintentional Ingestion of austic Agents Tsung-Yi hen, MD; Sheung-Fat Ko 1, MD; Jiin-Haur huang 2, MD; Hsin-Wei Kuo 3, MD; Mao-Meng
Original Article 233 Predictors of Esophageal Stricture in hildren with Unintentional Ingestion of austic Agents Tsung-Yi hen, MD; Sheung-Fat Ko 1, MD; Jiin-Haur huang 2, MD; Hsin-Wei Kuo 3, MD; Mao-Meng
13 patients within 24 hours of hospital admission
 Corrosive acid ingestion in man endoscopic study a clinical and J B DILAWARI, SURJIT SINGH, P N RAO, AND B S ANAND Gut, 1984, 25, 183-187 From the Departments of Gastroenterology and Internal Medicine,
Corrosive acid ingestion in man endoscopic study a clinical and J B DILAWARI, SURJIT SINGH, P N RAO, AND B S ANAND Gut, 1984, 25, 183-187 From the Departments of Gastroenterology and Internal Medicine,
Various Upper Endoscopic Findings of Acute Esophageal Thermal Injury Induced by Diverse Food: A Case Series
 CSE REPORT Clin Endosc 2014;47:447-451 Print ISSN 2234-2400 / On-line ISSN 2234-2443 http://dx.doi.org/10.5946/ce.2014.47.5.447 Open ccess Various Upper Endoscopic Findings of cute Esophageal Thermal Injury
CSE REPORT Clin Endosc 2014;47:447-451 Print ISSN 2234-2400 / On-line ISSN 2234-2443 http://dx.doi.org/10.5946/ce.2014.47.5.447 Open ccess Various Upper Endoscopic Findings of cute Esophageal Thermal Injury
ESOPHAGEAL PERFORATION. Anju Sidhu MD University of Louisville Gastroenterology, Hepatology, and Nutrition January 24, 2013
 ESOPHAGEAL PERFORATION Anju Sidhu MD University of Louisville Gastroenterology, Hepatology, and Nutrition January 24, 2013 OUTLINE Risk factors Diagnosis Management GOALS Make sure you don t miss it If
ESOPHAGEAL PERFORATION Anju Sidhu MD University of Louisville Gastroenterology, Hepatology, and Nutrition January 24, 2013 OUTLINE Risk factors Diagnosis Management GOALS Make sure you don t miss it If
Gastroduodenal Stress Ulceration. Bryan Woolridge POS Rounds 29 October 2003
 Gastroduodenal Stress Ulceration Bryan Woolridge POS Rounds 29 October 2003 Objectives Define entity Etiology Differentiation of UGI ulcers Pathophysiology Identify population at risk/risk factors Clinical
Gastroduodenal Stress Ulceration Bryan Woolridge POS Rounds 29 October 2003 Objectives Define entity Etiology Differentiation of UGI ulcers Pathophysiology Identify population at risk/risk factors Clinical
Anatomy: From cricoid cartilage to diaphragm 25 Cms. 4 portions: Cervical 5 cms. Thoracic 25 cms. Abdominal 2 cms. Blood supply Lymphatic spread
 Esophagus Anatomy: From cricoid cartilage to diaphragm 25 Cms. 4 portions: Cervical 5 cms. Thoracic 25 cms. Abdominal 2 cms. Blood supply Lymphatic spread Upper 2/3 Cephalad Lower 1/3 Caudad Physiology:
Esophagus Anatomy: From cricoid cartilage to diaphragm 25 Cms. 4 portions: Cervical 5 cms. Thoracic 25 cms. Abdominal 2 cms. Blood supply Lymphatic spread Upper 2/3 Cephalad Lower 1/3 Caudad Physiology:
Understanding GERD. & Stretta Therapy. GERD (gĕrd): Gastroesophageal Reflux Disease
: Gastroesophageal Reflux Disease") Understanding GERD & Stretta Therapy GERD (gĕrd): Gastroesophageal Reflux Disease What is GERD? When the muscle between your stomach and esophagus is weak, stomach contents like acid or bile can reflux
Understanding GERD & Stretta Therapy GERD (gĕrd): Gastroesophageal Reflux Disease What is GERD? When the muscle between your stomach and esophagus is weak, stomach contents like acid or bile can reflux
A 16 yr old boy with aggressive ca esophagus. DR Ayunga A.O Physician-Garisa PGH Associate Faculty Lecturer-UON Afya Bora Fellow in Global Health
 A 16 yr old boy with aggressive ca esophagus DR Ayunga A.O Physician-Garisa PGH Associate Faculty Lecturer-UON Afya Bora Fellow in Global Health Cancer of esophagus in a 16yr old Y.N 16 yr old boy unwell
A 16 yr old boy with aggressive ca esophagus DR Ayunga A.O Physician-Garisa PGH Associate Faculty Lecturer-UON Afya Bora Fellow in Global Health Cancer of esophagus in a 16yr old Y.N 16 yr old boy unwell
Accidental Concentrated Hydrogen Peroxide Ingestion Associated with Portal Venous Gas
 Accidental Concentrated Hydrogen Peroxide Ingestion Associated with Portal Venous Gas Eslam W Youssef 1,2*, Victor S Chukwueke 3, Lina Elsamaloty 3, Sherif Moawad 1,2, Haitham Elsamaloty 1 1. Department
Accidental Concentrated Hydrogen Peroxide Ingestion Associated with Portal Venous Gas Eslam W Youssef 1,2*, Victor S Chukwueke 3, Lina Elsamaloty 3, Sherif Moawad 1,2, Haitham Elsamaloty 1 1. Department
An Overview on Pediatric Esophageal Disorders. Annamaria Staiano Department of Translational Medical Sciences University of Naples Federico II
 An Overview on Pediatric Esophageal Disorders Annamaria Staiano Department of Translational Medical Sciences University of Naples Federico II Case report F.C. 3 year old boy Preterm born from emergency
An Overview on Pediatric Esophageal Disorders Annamaria Staiano Department of Translational Medical Sciences University of Naples Federico II Case report F.C. 3 year old boy Preterm born from emergency
A Complicated Hospitalization Following Dilute Ammonium Chloride Ingestion
 A Complicated Hospitalization Following Dilute Ammonium Chloride Ingestion Toxicology Observations Kendra Hammond, MD a, Tiffany Graybill, DO a, Susannah E. Spiess, MD b,c, Jenny Lu, MD d, Jerrold B. Leikin,
A Complicated Hospitalization Following Dilute Ammonium Chloride Ingestion Toxicology Observations Kendra Hammond, MD a, Tiffany Graybill, DO a, Susannah E. Spiess, MD b,c, Jenny Lu, MD d, Jerrold B. Leikin,
Definition of GERD American College of Gastroenterology
 Definition of GERD American College of Gastroenterology GERD is defined as chronic symptoms or mucosal damage produced by the abnormal reflux of gastric contents into the esophagus DeVault et al. Am J
Definition of GERD American College of Gastroenterology GERD is defined as chronic symptoms or mucosal damage produced by the abnormal reflux of gastric contents into the esophagus DeVault et al. Am J
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS GASTROINTESTINAL (GI) PATHOLOGY LAB #1. January 06, 2012
 PATHOLOGY LAB #1. January 06, 2012") MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS GASTROINTESTINAL (GI) PATHOLOGY LAB #1 GOAL: January 06, 2012 Faculty Copy 1. Describe the basis morphologic and pathophysiologic changes which occur in
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS GASTROINTESTINAL (GI) PATHOLOGY LAB #1 GOAL: January 06, 2012 Faculty Copy 1. Describe the basis morphologic and pathophysiologic changes which occur in
Foreign Body Ingested
 Princess Margaret Hospital for Children PAEDIATRIC ACUTE CARE GUIDELINE Foreign Body Ingested Scope (Staff): Scope (Area): All Emergency Department Clinicians Emergency Department This document should
Princess Margaret Hospital for Children PAEDIATRIC ACUTE CARE GUIDELINE Foreign Body Ingested Scope (Staff): Scope (Area): All Emergency Department Clinicians Emergency Department This document should
Sodium Hydroxide (NaOH) CAS ; UN 1823 (solid); UN 1824 (solution)
 CAS ; UN 1823 (solid); UN 1824 (solution)") Sodium Hydroxide (NaOH) CAS 1310-73-2; UN 1823 (solid); UN 1824 (solution) Synonyms include caustic soda, lye, soda lye, and sodium hydrate. C Persons whose clothing or skin is contaminated with solid
Sodium Hydroxide (NaOH) CAS 1310-73-2; UN 1823 (solid); UN 1824 (solution) Synonyms include caustic soda, lye, soda lye, and sodium hydrate. C Persons whose clothing or skin is contaminated with solid
Peptic ulcer disease Disorders of the esophagus
 Peptic ulcer disease Disorders of the esophagus Peptic ulcer disease Burning epigastric pain Exacerbated by fasting Improved with meals Ulcer: disruption of mucosal integrity >5 mm in size, with depth
Peptic ulcer disease Disorders of the esophagus Peptic ulcer disease Burning epigastric pain Exacerbated by fasting Improved with meals Ulcer: disruption of mucosal integrity >5 mm in size, with depth
Sept 13: Aerodigestive Foreign Bodies (updated 08/06) Preceptor: Gereau; Vacation; David & Josh
 Preceptor: Gereau; Vacation; David & Josh") Sept 13: Aerodigestive Foreign Bodies (updated 08/06) Preceptor: Gereau; Vacation; David & Josh 1. (dara) Tell us about different Acids vs. Bases and types of injuries they cause in caustic ingestion.
Sept 13: Aerodigestive Foreign Bodies (updated 08/06) Preceptor: Gereau; Vacation; David & Josh 1. (dara) Tell us about different Acids vs. Bases and types of injuries they cause in caustic ingestion.
Perforated peptic ulcer
 Perforated peptic ulcer - Despite the widespread use of gastric anti-secretory agents and eradication therapy, the incidence of perforated peptic ulcer has changed little, age limits increase NSAIDs elderly
Perforated peptic ulcer - Despite the widespread use of gastric anti-secretory agents and eradication therapy, the incidence of perforated peptic ulcer has changed little, age limits increase NSAIDs elderly
Pediatric Foreign Body Ingestion/Aspiration/Removal
 Pediatric Foreign Body Ingestion/Aspiration/Removal Guideline developed by Jonathan W. Orsborn, MD, in collaboration with the ANGELS team. Last revised by Jonathan W. Orsborn, MD June 3, 2016. Foreign
Pediatric Foreign Body Ingestion/Aspiration/Removal Guideline developed by Jonathan W. Orsborn, MD, in collaboration with the ANGELS team. Last revised by Jonathan W. Orsborn, MD June 3, 2016. Foreign
Surgical aspects of dysphagia
 Dysphagia Why is dysphagia important? Surgery Surgical aspects of dysphagia Adrian P. Ireland aireland@eircom.net Academic RCSI Department of Surgery, Beaumont Hospital Why important Definitons Swallowing
Dysphagia Why is dysphagia important? Surgery Surgical aspects of dysphagia Adrian P. Ireland aireland@eircom.net Academic RCSI Department of Surgery, Beaumont Hospital Why important Definitons Swallowing
Use of Magill Forceps to Remove Foreign Bodies in Children
 THIEME Original Article e91 Use of Magill Forceps to Remove Foreign Bodies in Children Murat Oncel, MD 1 Guven Sadi Sunam, MD 1 Cagdas Elsurer, MD 2 Huseyin Yildiran, MD 1 1 Department of Thoracic Surgery,
THIEME Original Article e91 Use of Magill Forceps to Remove Foreign Bodies in Children Murat Oncel, MD 1 Guven Sadi Sunam, MD 1 Cagdas Elsurer, MD 2 Huseyin Yildiran, MD 1 1 Department of Thoracic Surgery,
Hiatal Hernias and Barrett s esophagus. Dr Sajida Ahad Mercy General Surgery
 Hiatal Hernias and Barrett s esophagus Dr Sajida Ahad Mercy General Surgery Objectives Identify the use of different diagnostic modalities for hiatal hernias List the different types of hiatal hernias
Hiatal Hernias and Barrett s esophagus Dr Sajida Ahad Mercy General Surgery Objectives Identify the use of different diagnostic modalities for hiatal hernias List the different types of hiatal hernias
Tools of the Gastroenterologist: Introduction to GI Endoscopy
 Tools of the Gastroenterologist: Introduction to GI Endoscopy Objectives Endoscopy Upper endoscopy Colonoscopy Endoscopic retrograde cholangiopancreatography (ERCP) Endoscopic ultrasound (EUS) Endoscopic
Tools of the Gastroenterologist: Introduction to GI Endoscopy Objectives Endoscopy Upper endoscopy Colonoscopy Endoscopic retrograde cholangiopancreatography (ERCP) Endoscopic ultrasound (EUS) Endoscopic
Investigation of Mortality after Corrosive Ingestion: A Prospective Study
 ORIGINAL REPORT Investigation of Mortality after Corrosive Ingestion: A Prospective Study Roohollah Yeganeh 1*, Hasan Peyvandi 1, Mohammad Mohajeri 2, Reza Bashtar 2, Mohammad Bashashati 2, and Mina Ahmadi
ORIGINAL REPORT Investigation of Mortality after Corrosive Ingestion: A Prospective Study Roohollah Yeganeh 1*, Hasan Peyvandi 1, Mohammad Mohajeri 2, Reza Bashtar 2, Mohammad Bashashati 2, and Mina Ahmadi
Esophageal Perforation
 Esophageal Perforation Dr. Carmine Simone Thoracic Surgeon, Division of General Surgery Head, Division of Critical Care May 15, 2006 Overview Case presentation Radiology Pre-operative management Operative
Esophageal Perforation Dr. Carmine Simone Thoracic Surgeon, Division of General Surgery Head, Division of Critical Care May 15, 2006 Overview Case presentation Radiology Pre-operative management Operative
Endoscopic Management of Perforations
 Endoscopic Management of Perforations Gregory G. Ginsberg, MD Professor of Medicine University of Pennsylvania Perelman School of Medicine Gastroenterology Division Executive Director of Endoscopic Services
Endoscopic Management of Perforations Gregory G. Ginsberg, MD Professor of Medicine University of Pennsylvania Perelman School of Medicine Gastroenterology Division Executive Director of Endoscopic Services
ENDOLUMINAL THERAPIES FOR GERD. University of Colorado Department of Surgery Grand Rounds March 31st, 2008
 ENDOLUMINAL THERAPIES FOR GERD University of Colorado Department of Surgery Grand Rounds March 31st, 2008 Overview GERD Healthcare significance Definitions Treatment objectives Endoscopic options Plication
ENDOLUMINAL THERAPIES FOR GERD University of Colorado Department of Surgery Grand Rounds March 31st, 2008 Overview GERD Healthcare significance Definitions Treatment objectives Endoscopic options Plication
Long Term Follow-up. 6 Month 1 Year Annual enter year #: What is the assessment date: / / Unknown. Is the patient alive? Yes No
 Long Term Follow-up 6 Month 1 Year Annual enter year #: What is the assessment date: / / Unknown Is the patient alive? Yes No Was an exam performed by a bariatric physician or PA/NP? Yes No Was the patient
Long Term Follow-up 6 Month 1 Year Annual enter year #: What is the assessment date: / / Unknown Is the patient alive? Yes No Was an exam performed by a bariatric physician or PA/NP? Yes No Was the patient
Double-Contrast Barium Swallow Guide
 Fluoroscopy Double-Contrast Barium Swallow Guide Version 3 Marie L. Duan Meservy & Samuel Q. Armstrong 2-26-2018 Special thanks to: Chandler D. Connell, RT Crista S. Cimis, RT Judith Austin-Strohbehn,
Fluoroscopy Double-Contrast Barium Swallow Guide Version 3 Marie L. Duan Meservy & Samuel Q. Armstrong 2-26-2018 Special thanks to: Chandler D. Connell, RT Crista S. Cimis, RT Judith Austin-Strohbehn,
STRIDOR. Respiratory system. Lecture
 STRIDOR Stridor is a continuous inspiratory harsh sound produced by partial obstruction in the region of the larynx or trachea. Total obstruction cyanosis & death. Etiology Acute stridor Infectious croup
STRIDOR Stridor is a continuous inspiratory harsh sound produced by partial obstruction in the region of the larynx or trachea. Total obstruction cyanosis & death. Etiology Acute stridor Infectious croup
GASTRO-OESOPHAGEAL REFLUX DR RONALDA DELACY
 GASTRO-OESOPHAGEAL REFLUX DR RONALDA DELACY DEFINITIONS GERD -Involuntary, effortless passage of gastric contents into the oesophagus +/-ejected from the mouth resulting in troublesome symptoms or complications
GASTRO-OESOPHAGEAL REFLUX DR RONALDA DELACY DEFINITIONS GERD -Involuntary, effortless passage of gastric contents into the oesophagus +/-ejected from the mouth resulting in troublesome symptoms or complications
REMOVAL OF IMPACTED DENTURES WITH POLYPECTOMY SNARE
 JMBR: A Peer-review Journal of Biomedical Sciences June 2012, Vol. 11 No.1 pp 14-19 REMOVAL OF IMPACTED DENTURES WITH POLYPECTOMY SNARE *OKUGBO SU, **OKORO E, ***KESIEME E ABSTRACT Impacted dentures have
JMBR: A Peer-review Journal of Biomedical Sciences June 2012, Vol. 11 No.1 pp 14-19 REMOVAL OF IMPACTED DENTURES WITH POLYPECTOMY SNARE *OKUGBO SU, **OKORO E, ***KESIEME E ABSTRACT Impacted dentures have
GERD: A linical Clinical Clinical Update Objectives
 GERD: A Clinical Update Jeff Gilbert, M.D. University i of Kentucky Gastroenterology 11/6/08 Objectives To review the basic pathophysiology underlying gastroesophageal reflux disease To highlight current
GERD: A Clinical Update Jeff Gilbert, M.D. University i of Kentucky Gastroenterology 11/6/08 Objectives To review the basic pathophysiology underlying gastroesophageal reflux disease To highlight current
Gastrointestinal Obstruction
 Customer Name, Street Address, City, State, Zip code Phone number, Alt. phone number, Fax number, e-mail address, web site Gastrointestinal Obstruction (Blockage of the Gastrointestinal Tract) Basics OVERVIEW
Customer Name, Street Address, City, State, Zip code Phone number, Alt. phone number, Fax number, e-mail address, web site Gastrointestinal Obstruction (Blockage of the Gastrointestinal Tract) Basics OVERVIEW
THORACIC SURGERY: Dysphagia. Dr. Robert Zeldin Dr. John Dickie Dr. Carmine Simone. Thoracic Surgery Toronto East General Hospital
 THORACIC SURGERY: Dysphagia Dr. Robert Zeldin Dr. John Dickie Dr. Carmine Simone Thoracic Surgery Toronto East General Hospital Objectives Definitions Common causes Investigations Treatment options Anatomy
THORACIC SURGERY: Dysphagia Dr. Robert Zeldin Dr. John Dickie Dr. Carmine Simone Thoracic Surgery Toronto East General Hospital Objectives Definitions Common causes Investigations Treatment options Anatomy
Brachycephalic Airway Syndrome (Upper Airway Problems Seen in Short-Nosed Breeds) Basics
 Basics") Brachycephalic Airway Syndrome (Upper Airway Problems Seen in Short-Nosed Breeds) Basics OVERVIEW Partial upper airway obstruction in short-nosed, flat-faced (brachycephalic) breeds of dogs and cats caused
Brachycephalic Airway Syndrome (Upper Airway Problems Seen in Short-Nosed Breeds) Basics OVERVIEW Partial upper airway obstruction in short-nosed, flat-faced (brachycephalic) breeds of dogs and cats caused
Emergency Surgery Course Graz, March UPPER GI BLEEDING. Carlos Mesquita Coimbra
 UPPER GI BLEEDING Carlos Mesquita Coimbra Aim Causes Management Problem Above angle of Treitz Common emergency 1-2/1000 pts 10% rebleeed 1% angioembolization 20% over 60
UPPER GI BLEEDING Carlos Mesquita Coimbra Aim Causes Management Problem Above angle of Treitz Common emergency 1-2/1000 pts 10% rebleeed 1% angioembolization 20% over 60
WHAT IS GASTROESOPHAGEAL REFLUX DISEASE (GERD)?
?") WHAT IS GASTROESOPHAGEAL REFLUX DISEASE (GERD)? The term gastroesophageal reflux describes the movement (or reflux) of stomach contents back up into the esophagus, the muscular tube that extends from the
WHAT IS GASTROESOPHAGEAL REFLUX DISEASE (GERD)? The term gastroesophageal reflux describes the movement (or reflux) of stomach contents back up into the esophagus, the muscular tube that extends from the
Management of Foreign Body Ingestions
 Management of Foreign Body Ingestions Gregory P. Conners, MD, MPH, MBA, FAAP, FACEP Chief, Division of Emergency Medical Services Vice Chair of Pediatrics, Emergency and Urgent Care Children s Mercy Hospitals
Management of Foreign Body Ingestions Gregory P. Conners, MD, MPH, MBA, FAAP, FACEP Chief, Division of Emergency Medical Services Vice Chair of Pediatrics, Emergency and Urgent Care Children s Mercy Hospitals
Boric Acid. Boric acid had significant medical uses in the past as a topical antiseptic and irrigant.
 Boric Acid Boric acid had significant medical uses in the past as a topical antiseptic and irrigant. At one time it was mixed with honey and glycerine and sold to treat topical mucosal sores in children.
Boric Acid Boric acid had significant medical uses in the past as a topical antiseptic and irrigant. At one time it was mixed with honey and glycerine and sold to treat topical mucosal sores in children.
Epiglottitis. Bronchitis. Bronchiolitis. Pneumonia. Croup syndrome. Miss. kamlah 2
 Miss. kamlah 1 Epiglottitis. Bronchitis. Bronchiolitis. Pneumonia. Croup syndrome. Miss. kamlah 2 Acute Epiglottitis Is an infection of the epiglottis, the long narrow structure that closes off the glottis
Miss. kamlah 1 Epiglottitis. Bronchitis. Bronchiolitis. Pneumonia. Croup syndrome. Miss. kamlah 2 Acute Epiglottitis Is an infection of the epiglottis, the long narrow structure that closes off the glottis
There are many different symptoms of GER. Your child may only have a few of these symptoms. The most common symptoms include:
 This document is a short Overview of Pediatric Acid Reflux and GERD from www.reflux.org web site. Dozens of other documents about Pediatric GERD can be found in the Reading Room section of this web site.
This document is a short Overview of Pediatric Acid Reflux and GERD from www.reflux.org web site. Dozens of other documents about Pediatric GERD can be found in the Reading Room section of this web site.
Dysphagia. Conflicts of Interest
 Dysphagia Bob Kizer MD Assistant Professor of Medicine Creighton University School of Medicine August 25, 2018 Conflicts of Interest None 1 Which patient does not need an EGD as the first test? 1. 50 year
Dysphagia Bob Kizer MD Assistant Professor of Medicine Creighton University School of Medicine August 25, 2018 Conflicts of Interest None 1 Which patient does not need an EGD as the first test? 1. 50 year
Ammonia (NH 3 ) B 1. Information and recommendations for paramedics and doctors at the site. BASF Chemical Emergency Medical Guidelines
 B 1. Information and recommendations for paramedics and doctors at the site. BASF Chemical Emergency Medical Guidelines") BASF Chemical Emergency Medical Guidelines Ammonia (NH 3 ) B 1 Information and recommendations for paramedics and doctors at the site Before approaching the patient the paramedics and doctors at the site
BASF Chemical Emergency Medical Guidelines Ammonia (NH 3 ) B 1 Information and recommendations for paramedics and doctors at the site Before approaching the patient the paramedics and doctors at the site
PEDIATRIC EMERGENCIES Sandra Horning, MD Sacred Heart Medical Center Emergency Department
 PEDIATRIC EMERGENCIES Sandra Horning, MD Sacred Heart Medical Center Emergency Department Overview Roles of the EMS in Pediatric Care Growth and Development Assessment Airway Adjuncts and Intravenous Access
PEDIATRIC EMERGENCIES Sandra Horning, MD Sacred Heart Medical Center Emergency Department Overview Roles of the EMS in Pediatric Care Growth and Development Assessment Airway Adjuncts and Intravenous Access
Surgical Management of IBD. Val Jefford Grand Rounds October 14, 2003
 Surgical Management of IBD Val Jefford Grand Rounds October 14, 2003 Introduction Important Features Clinical Presentation Evaluation Medical Treatment Surgical Treatment Cases Overview Introduction Two
Surgical Management of IBD Val Jefford Grand Rounds October 14, 2003 Introduction Important Features Clinical Presentation Evaluation Medical Treatment Surgical Treatment Cases Overview Introduction Two
Foreign body ingestions occur
 Navid Dehghani, MD, FRCRC, Jeffrey P. Ludemann, MDCM, FRCSC Ingested foreign bodies in children: BC Children s Hospital emergency room protocol Clinicians should be aware of the dangers presented by disc
Navid Dehghani, MD, FRCRC, Jeffrey P. Ludemann, MDCM, FRCSC Ingested foreign bodies in children: BC Children s Hospital emergency room protocol Clinicians should be aware of the dangers presented by disc
Early View Article: Online published version of an accepted article before publication in the final form.
 : Online published version of an accepted article before publication in the final form. Journal Name: Journal of Case Reports and Images in Surgery Type of Article: Case Report Title: What is the treatment
: Online published version of an accepted article before publication in the final form. Journal Name: Journal of Case Reports and Images in Surgery Type of Article: Case Report Title: What is the treatment