SUMPh N. Testemitanu Radiology and Medical imaging department PEDIATRIC IMAGING. M. Crivceanschii, assistant professor
|
|
|
- Amelia Haynes
- 5 years ago
- Views:
Transcription

1 SUMPh N. Testemitanu Radiology and Medical imaging department PEDIATRIC IMAGING M. Crivceanschii, assistant professor

2 GOALS AND OBJECTIVES to be aware of the role of modern diagnostic imaging modalities and use proper sequences in pediatric imaging to be familiar with radiological findings in common pediatric pathologic conditions tips and tricks in pediatric imaging that every student should now


3 IMAGING MODALITIES


4 IMAGING MODALITIES Conventional Radiography Computed Tomography Magnetic Resonance Imaging Ultrasonography Angiography Scintigraphy, Positron Emission Tomography, PET/CT
5 COMMON PEDIATRIC CONDITIONS 1. Newborn respiratory distress 2. Childhood lung disease 3. Soft tissues of the neck 4. Other diseases
6 NEWBORN RESPIRATORY DISTRESS 1. Transient tachypnea of the newborn 2. Neonatal respiratory distress syndrome (hyaline membrane disease) 3. Meconium aspiration syndrome 4. Bronchopulmonary dysplasia

7 TRANSIENT TACHYPNEA OF THE NEWBORN Most common cause of respiratory distress in the newborn. Result of delay in the resorption of fetal lung fluid. Clinically: immediate onset of tachypnea, typically improve over several hours with oxygen and supportive therapy and completely recover by 48 hours. Imaging findings: hyperinflation, streaky perihilar linear densities, fluid in the fissures and/or laminar pleural effusions.


8 TRANSIENT TACHYPNEA OF THE NEWBORN All images Learning Radiology. Recognizing the basics. 3 rd edition.


9 RESPIRATORY DISTRESS SYNDROME OF THE NEWBORN (HYALINE MEMBRANE DISEASE) Is a disease of premature infants The major cause of this disorder is surfactant deficiency. Clinically: cyanosis, grunting, nasal flaring, intercostal and subcostal retractions, and tachypnea. Imaging findings: diffuse ground-glass or finely granular appearance to the lungs in a bilateral and symmetric distribution; air bronchograms; hypoaeration; air leak - a complication of positive pressure ventilation.



10 RESPIRATORY DISTRESS SYNDROME OF THE NEWBORN All images Learning Radiology. Recognizing the basics. 3 rd edition.
11 MECONIUM ASPIRATION SYNDROME Is the most common cause of neonatal respiratory distress in postmature infants. Clinically: severe respiratory distress almost immediately; tachypnea, hypoxia, and hypercapnia. Imaging findings: The lungs are hyperinflated with diffuse ropey densities (similar in appearance, but not in timing, to bronchopulmonary dysplasia). There may be patchy areas of atelectasis and emphysema from air trapping. Spontaneous pneumothorax and pneumomediastinum occur in 25%.There may be an associated pneumonia.



12 MECONIUM ASPIRATION SYNDROME All images Learning Radiology. Recognizing the basics. 3 rd edition.

13 MECONIUM ASPIRATION SYNDROME All images Learning Radiology. Recognizing the basics. 3 rd edition.


14 BRONCHOPULMONARY DYSPLASIA Is a consequence of early, acute lung disease, frequently respiratory distress syndrome. Is defined as oxygen dependence at 28 days of life to maintain arterial oxygen tensions >50 mm Hg accompanied by abnormal chest radiographs. Clinically: oxygen dependence, hypercapnia, and a compensatory metabolic alkalosis. Imaging findings: hyperaerated lungs, coarse, irregular, ropelike, linear densities, representing atelectasis or, later, fibrosis; air trapping.

15 BRONCHOPULMONARY DYSPLASIA All images Learning Radiology. Recognizing the basics. 3 rd edition.

16 CHILDHOOD LUNG DISEASE 1. Reactive airways disease/bronchiolitis 2. Asthma 3. Pneumonia



17 REACTIVE AIRWAYS DISEASE/BRONCHIOLITIS Group of diseases in the pediatric population featuring wheezing, shortness of breath, and coughing. Unlike asthma, which is chronic, reactive airways disease is usually transient, although it can progress over time to asthma. Clinically: tachypnea, retractions, cough, fever, and rhinorrhea. Imaging findings: peribronchial thickening, hyperinflation of the lungs, atelectasis from mucus plugging may be present.


18 REACTIVE AIRWAYS DISEASE/BRONCHIOLITIS All images Learning Radiology. Recognizing the basics. 3 rd edition.

19 ASTHMA Asthma is a clinical, not a radiologic, diagnosis. Complications include atelectasis secondary to plugging by mucus, pneumothorax, and pneumomediastinum. During or after an acute attack, the lungs may be overaerated with flattening of the diaphragm. There may be peribronchial thickening.


20 ASTHMA All images Learning Radiology. Recognizing the basics. 3 rd edition.

21 PNEUMONIA Age is a determining factor in both the causes and clinical presentation of childhood pneumonia. Clinically: fever, chills, tachypnea, cough, pleuritic chest pain, and shortness of breath. Imaging findings: - Bacterial pneumonia - characteristically produces lobar consolidation, or around pneumonia, with pleural effusion in 10% to 30% of cases. - Viral pneumonia - characteristically shows interstitial infiltrates or patchy areas of consolidation suggestive of bronchopneumonia.

22 PNEUMONIA All images Learning Radiology. Recognizing the basics. 3 rd edition.

")
23 SOFT TISSUES OF THE NECK 1. Enlarged tonsils and adenoids 2. Epiglottitis 3. Croup (laryngotracheobronchitis) 4. Ingested foreign bodies
24 ENLARGED TONSILS AND ADENOIDS Newborns do not have visible adenoids. Not visible radiographically until 3 to 6 months. Clinically: nasal congestion, mouthbreathing, chronic or recurrent otitis media as a result of their proximity to the Eustachian tubes, painful swallowing, and sleep apnea. Imaging findings: look for marked narrowing or obliteration of the nasopharyngeal airway.
25 ENLARGED TONSILS AND ADENOIDS All images Learning Radiology. Recognizing the basics. 3 rd edition.

26 EPIGLOTTITIS Life-threatening medical emergency. Peak incidence from about 3 to 6 years of age. Clinically: resembles croup, classical triad of epiglottitis is drooling, severe dysphagia, and respiratory distress with inspiratory stridor. Imaging findings: enlargement of the epiglottis, thickening of the aryepiglottic folds, narrowing of the subglottic portion of the trachea.

27 EPIGLOTTITIS E All images Learning Radiology. Recognizing the basics. 3 rd edition.
28 CROUP (LARYNGOTRACHEOBRONCHITIS) It typically occurs from age 6 months to 3 years. It frequently follows a common cold. Clinically: harsh cough described as barking or brassy, associated with hoarseness, inspiratory stridor, lowgrade fever, and respiratory distress. Imaging findings: distension of the hypopharynx, distension of the laryngeal ventricle, and haziness and/or narrowing of the subglottic trachea.

29 CROUP (LARYNGOTRACHEOBRONCHITIS) E All images Learning Radiology. Recognizing the basics. 3 rd edition.
 at the aortic arch (20%), or at the")

30 INGESTED FOREIGN BODIES Majority occur between 6 months and 6 years. 80% pass spontaneously. Often, they impact just below the cricopharyngeus at the level of C5-C6 (70%) at the aortic arch (20%), or at the level of the esophagogastric junction (10%). Major complications of ingested foreign bodies are perforation, obstruction, or stricture formation. Clinically: dysphagia and odynophagia. Imaging findings: depend on whether the foreign body is opaque or not.


31 INGESTED FOREIGN BODIES All images Learning Radiology. Recognizing the basics. 3 rd edition.
32 OTHER DISEASES 1. Cardiomegaly in infants 2. Salter-Harris epiphyseal plate fractures 3. Child abuse 4. Necrotizing enterocolitis 5. Esophageal atresia with/without tracheoesophageal fistula
.")
33 CARDIOMEGALY IN INFANTS Cardiothoracic ratio may reach up to 65% in infants. Any assessment of cardiac enlargement in an infant should take into account other factors such as the appearance of the pulmonary vasculature, and any associated (e.g., a murmur, tachycardia, or cyanosis). Thymus gland may overlap portions of the heart and sometimes mimic cardiomegaly.

34 CARDIOMEGALY IN INFANTS All images Learning Radiology. Recognizing the basics. 3 rd edition.
 is most vulnerable to injury. Account for as many as 30% of childhood fractures.")

35 SALTER-HARRIS EPIPHYSEAL PLATE FRACTURES In growing bone, the hypertrophic zone in the growth plate (epiphyseal plate or physis) is most vulnerable to injury. Account for as many as 30% of childhood fractures. The Salter-Harris classification of epiphyseal plate injuries is a commonly used method of describing such injuries that helps identify the type of treatment required and predicts the likelihood of complications based on the type of fracture.

36 SALTER-HARRIS EPIPHYSEAL PLATE FRACTURES Radiologyassistant.nl image



37 SALTER-HARRIS EPIPHYSEAL PLATE FRACTURES TYPE I All images Learning Radiology. Recognizing the basics. 3 rd edition.

38 SALTER-HARRIS EPIPHYSEAL PLATE FRACTURES TYPE II All images Learning Radiology. Recognizing the basics. 3 rd edition.


39 SALTER-HARRIS EPIPHYSEAL PLATE FRACTURES TYPE III All images Learning Radiology. Recognizing the basics. 3 rd edition.


40 SALTER-HARRIS EPIPHYSEAL PLATE FRACTURES TYPE IV All images Learning Radiology. Recognizing the basics. 3 rd edition.


41 SALTER-HARRIS EPIPHYSEAL PLATE FRACTURES TYPE V All images Learning Radiology. Recognizing the basics. 3 rd edition.


42 CHILD ABUSE There are several fracture sites and characteristics that should raise the suspicion for child abuse: 1. metaphyseal corner fracturesparallel the metaphysis and can have a buckethandle appearance 2. rib fractures - especially multiple fractures, and/or fractures of the posterior ribs 3. head injuries - subdural and subarachnoid hemorrhage and cerebral contusions; skull fractures


43 CHILD ABUSE All images Learning Radiology. Recognizing the basics. 3 rd edition.

44 CHILD ABUSE All images Learning Radiology. Recognizing the basics. 3 rd edition.


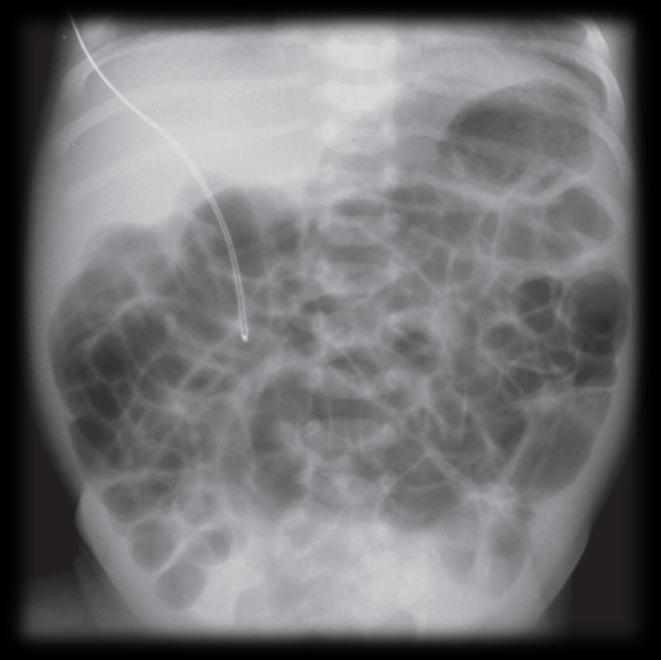
45 NECROTIZING ENTEROCOLITIS Most common gastrointestinal medical and/or surgical emergency occurring in neonates. More common in premature infants but can also be seen in term babies. Clinical findings may be subtle and can include feeding intolerance, delayed gastric emptying, abdominal distention, and/or tenderness, and decreased bowel sounds. Imaging findings - most commonly affects the terminal ileum, distended loops of bowel, pneumatosis intestinalis, abdominal free air.
46 NORMAL INFANT ABDOMEN All images Learning Radiology. Recognizing the basics. 3 rd edition.


47 NECROTIZING ENTEROCOLITIS All images Learning Radiology. Recognizing the basics. 3 rd edition.
, with a fistulous connection between the")


48 ESOPHAGEAL ATRESIA WITH/WITHOUT TRACHEOESOPHAGEAL FISTULA The most common form is a blind-ending esophagus (esophageal atresia), with a fistulous connection between the trachea and the distal esophageal remnant. Clinical findings choking, drooling, difficulty handling secretions, regurgitation, aspiration, and respiratory distress. Imaging findings - with esophageal atresia and no fistula - no air enters the GI tract, so the abdomen is airless. With a distal fistula - gas in the bowel that has entered via the trachea.



49 ESOPHAGEAL ATRESIA WITH TRACHEOESOPHAGEAL FISTULA All images Learning Radiology. Recognizing the basics. 3 rd edition.

50
Chest X rays and Case Studies. No disclosures. Outline 5/31/2018. Carlo Manalo, M.D. Department of Radiology Loma Linda University Children s Hospital
 Chest X rays and Case Studies Carlo Manalo, M.D. Department of Radiology Loma Linda University Children s Hospital No disclosures. Outline Importance of history Densities delineated on radiography An approach
Chest X rays and Case Studies Carlo Manalo, M.D. Department of Radiology Loma Linda University Children s Hospital No disclosures. Outline Importance of history Densities delineated on radiography An approach
Shedding Light on Neonatal X-rays. Objectives. Indications for X-Rays 5/14/2018
 Shedding Light on Neonatal X-rays Barbara C. Mordue, MSN, NNP-BC Neonatal Nurse Practitioner LLUH Children s Hospital, NICU Objectives Utilize a systematic approach to neonatal x-ray interpretation Identify
Shedding Light on Neonatal X-rays Barbara C. Mordue, MSN, NNP-BC Neonatal Nurse Practitioner LLUH Children s Hospital, NICU Objectives Utilize a systematic approach to neonatal x-ray interpretation Identify
Review of Neonatal Respiratory Problems
 Review of Neonatal Respiratory Problems Respiratory Distress Occurs in about 7% of infants Clinical presentation includes: Apnea Cyanosis Grunting Inspiratory stridor Nasal flaring Poor feeding Tachypnea
Review of Neonatal Respiratory Problems Respiratory Distress Occurs in about 7% of infants Clinical presentation includes: Apnea Cyanosis Grunting Inspiratory stridor Nasal flaring Poor feeding Tachypnea
Epiglottitis. Bronchitis. Bronchiolitis. Pneumonia. Croup syndrome. Miss. kamlah 2
 Miss. kamlah 1 Epiglottitis. Bronchitis. Bronchiolitis. Pneumonia. Croup syndrome. Miss. kamlah 2 Acute Epiglottitis Is an infection of the epiglottis, the long narrow structure that closes off the glottis
Miss. kamlah 1 Epiglottitis. Bronchitis. Bronchiolitis. Pneumonia. Croup syndrome. Miss. kamlah 2 Acute Epiglottitis Is an infection of the epiglottis, the long narrow structure that closes off the glottis
Respiratory Management in Pediatrics
 Respiratory Management in Pediatrics Children s Hospital Omaha Critical Care Transport Sue Holmer RN, C-NPT Objectives Examine the differences between the pediatric and adults airways. Recognize respiratory
Respiratory Management in Pediatrics Children s Hospital Omaha Critical Care Transport Sue Holmer RN, C-NPT Objectives Examine the differences between the pediatric and adults airways. Recognize respiratory
Radiological evaluation of neonatal lesions in 118 neonates
 Original Research Article ISSN: 394-006 (P) Radiological evaluation of neonatal thoracic lesions in 8 neonates Konark Sarvaiya *, Himanshu Singla, Nirav Patel, Jai Inder Dhillon, Babubhai Patel 3 nd year
Original Research Article ISSN: 394-006 (P) Radiological evaluation of neonatal thoracic lesions in 8 neonates Konark Sarvaiya *, Himanshu Singla, Nirav Patel, Jai Inder Dhillon, Babubhai Patel 3 nd year
Acquired pediatric esophageal diseases Imaging approaches and findings. M. Mearadji International Foundation for Pediatric Imaging Aid
 Acquired pediatric esophageal diseases Imaging approaches and findings M. Mearadji International Foundation for Pediatric Imaging Aid Acquired pediatric esophageal diseases The clinical signs of acquired
Acquired pediatric esophageal diseases Imaging approaches and findings M. Mearadji International Foundation for Pediatric Imaging Aid Acquired pediatric esophageal diseases The clinical signs of acquired
Objectives. Case Presentation. Respiratory Emergencies
 Respiratory Emergencies Objectives Describe how to assess airway and breathing, including interpreting information from the PAT and ABCDEs. Differentiate between respiratory distress, respiratory failure,
Respiratory Emergencies Objectives Describe how to assess airway and breathing, including interpreting information from the PAT and ABCDEs. Differentiate between respiratory distress, respiratory failure,
Interpreting thoracic x-ray of the supine immobile patient: Syllabus
 Interpreting thoracic x-ray of the supine immobile patient: Syllabus Johannes Godt Dep. of Radiology and Nuclear Medicine Oslo University Hospital Ullevål NORDTER 2017, Helsinki Content - Why bedside chest
Interpreting thoracic x-ray of the supine immobile patient: Syllabus Johannes Godt Dep. of Radiology and Nuclear Medicine Oslo University Hospital Ullevål NORDTER 2017, Helsinki Content - Why bedside chest
FOREIGN BODY ASPIRATION in children. Dr. Xayyavong Bouathongthip, M.D Emergency department, children s hospital
 FOREIGN BODY ASPIRATION in children Dr. Xayyavong Bouathongthip, M.D Emergency department, children s hospital How common is choking? About 3,000 people die/year from choking Figure remained unchanged
FOREIGN BODY ASPIRATION in children Dr. Xayyavong Bouathongthip, M.D Emergency department, children s hospital How common is choking? About 3,000 people die/year from choking Figure remained unchanged
4/16/2017. Learning Objectives. Interpretation of the Chest Radiograph. Components. Production of the Radiograph. Density & Appearance
 Interpretation of the Arthur Jones, EdD, RRT Learning Objectives Identify technical defects in chest radiographs Identify common radiographic abnormalities This Presentation is Approved for 1 CRCE Credit
Interpretation of the Arthur Jones, EdD, RRT Learning Objectives Identify technical defects in chest radiographs Identify common radiographic abnormalities This Presentation is Approved for 1 CRCE Credit
Semiology of respiratory system in children Simple choice 1. Mark the intrauterine age of lung development onset from the gut: a) 1 week b) 24 days
 1 week b) 24 days") Semiology of respiratory system in children Simple choice 1. Mark the intrauterine age of lung development onset from the gut: a) 1 week b) 24 days c) 6 weeks d) 12 weeks e) 35 weeks 2. Stridor is not
Semiology of respiratory system in children Simple choice 1. Mark the intrauterine age of lung development onset from the gut: a) 1 week b) 24 days c) 6 weeks d) 12 weeks e) 35 weeks 2. Stridor is not
Learning Radiology: Recognizing the Basics. Text with Student Consult Online Access Code
 Learning Radiology: Recognizing the Basics. Text with Student Consult Online Access Code Herring, W ISBN-13: 9780323074445 Table of Contents 1. Recognizing Anything The "colorful" world of radiology A
Learning Radiology: Recognizing the Basics. Text with Student Consult Online Access Code Herring, W ISBN-13: 9780323074445 Table of Contents 1. Recognizing Anything The "colorful" world of radiology A
Lung- and airway emergencies
 Lung- and airway emergencies Charlotte de Lange,MD,PhD Pediatric Radiology unit, Oslo University Hospital, Norway 5th Nordic course - Emergency Radiology Oslo 18-21.5.2015 clange@ous-hf.no How come pediatric
Lung- and airway emergencies Charlotte de Lange,MD,PhD Pediatric Radiology unit, Oslo University Hospital, Norway 5th Nordic course - Emergency Radiology Oslo 18-21.5.2015 clange@ous-hf.no How come pediatric
Auscultation of the lung
 Auscultation of the lung Auscultation of the lung by the stethoscope. *Compositions of the stethoscope: 1-chest piece 2-Ear piece 3-Rubber tubs *Auscultation area of the lung(triangle of auscultation).
Auscultation of the lung Auscultation of the lung by the stethoscope. *Compositions of the stethoscope: 1-chest piece 2-Ear piece 3-Rubber tubs *Auscultation area of the lung(triangle of auscultation).
Upper Airway Obstruction
 Upper Airway Obstruction Adriaan Pentz Division of Otorhinolaryngology University of Stellenbosch and Tygerberg Hospital Stridor/Stertor Auditory manifestations of disordered respiratory function ie noisy
Upper Airway Obstruction Adriaan Pentz Division of Otorhinolaryngology University of Stellenbosch and Tygerberg Hospital Stridor/Stertor Auditory manifestations of disordered respiratory function ie noisy
ACUTE PULMNARY INFECTIONS: UNDERSTANDING THE CHEST RADIOGRAPH. Leonard E. Swischuk, M.D. University of Texas Medical Branch
 ACUTE PULMNARY INFECTIONS: UNDERSTANDING THE CHEST RADIOGRAPH Leonard E. Swischuk, M.D. University of Texas Medical Branch AUTHOR HAS NOTHING TO DECLARE LEARNING OBJETIVES Understand the pathophysiology
ACUTE PULMNARY INFECTIONS: UNDERSTANDING THE CHEST RADIOGRAPH Leonard E. Swischuk, M.D. University of Texas Medical Branch AUTHOR HAS NOTHING TO DECLARE LEARNING OBJETIVES Understand the pathophysiology
STRIDOR. Respiratory system. Lecture
 STRIDOR Stridor is a continuous inspiratory harsh sound produced by partial obstruction in the region of the larynx or trachea. Total obstruction cyanosis & death. Etiology Acute stridor Infectious croup
STRIDOR Stridor is a continuous inspiratory harsh sound produced by partial obstruction in the region of the larynx or trachea. Total obstruction cyanosis & death. Etiology Acute stridor Infectious croup
Suspected Foreign Body Ingestion
 Teresa Liang Suspected Foreign Body Ingestion 1. General Presentation Background: Of more than 100,000 cases of foreign body ingestion reported each year in the United States, 80% occur in children, with
Teresa Liang Suspected Foreign Body Ingestion 1. General Presentation Background: Of more than 100,000 cases of foreign body ingestion reported each year in the United States, 80% occur in children, with
PULMONARY TUBERCULOSIS RADIOLOGY
 PULMONARY TUBERCULOSIS RADIOLOGY RADIOLOGICAL MODALITIES Medical radiophotography Radiography Fluoroscopy Linear (conventional) tomography Computed tomography Pulmonary angiography, bronchography Ultrasonography,
PULMONARY TUBERCULOSIS RADIOLOGY RADIOLOGICAL MODALITIES Medical radiophotography Radiography Fluoroscopy Linear (conventional) tomography Computed tomography Pulmonary angiography, bronchography Ultrasonography,
Pediatric Shock. Hypovolemia. Sepsis. Most common cause of pediatric shock Small blood volumes (80cc/kg)
") Critical Concepts: Shock Inadequate peripheral perfusion where oxygen delivery does not meet metabolic demand Adult vs Pediatric Shock - Same causes/different frequencies Pediatric Shock Hypovolemia Most
Critical Concepts: Shock Inadequate peripheral perfusion where oxygen delivery does not meet metabolic demand Adult vs Pediatric Shock - Same causes/different frequencies Pediatric Shock Hypovolemia Most
Neonatal Chest X-Ray Interpretation
 CHAPTER 7 Neonatal Chest X-Ray Interpretation Prof. Praveen Kumar Neonatal unit, Department of Pediatrics, PGIMER, Chandigarh Learning Objectives At the end of this session, you should be able to: 1. Schematically
CHAPTER 7 Neonatal Chest X-Ray Interpretation Prof. Praveen Kumar Neonatal unit, Department of Pediatrics, PGIMER, Chandigarh Learning Objectives At the end of this session, you should be able to: 1. Schematically
PATIENT DATA EVALUATION AND RECOMMENDATION: IMAGING STUDIES
 PATIENT DATA EVALUATION AND RECOMMENDATION: IMAGING STUDIES Robert Harwood, MSA, RRT-NPS Objectives At the end of this presentation the student should be able to: Describe the indications of a chest radiograph.
PATIENT DATA EVALUATION AND RECOMMENDATION: IMAGING STUDIES Robert Harwood, MSA, RRT-NPS Objectives At the end of this presentation the student should be able to: Describe the indications of a chest radiograph.
Respiratory Disorders in the Newborn: Identification and Diagnosis Hany Aly. DOI: /pir
 Respiratory Disorders in the Newborn: Identification and Diagnosis Hany Aly Pediatr. Rev. 2004;25;201-208 DOI: 10.1542/pir.25-6-201 The online version of this article, along with updated information and
Respiratory Disorders in the Newborn: Identification and Diagnosis Hany Aly Pediatr. Rev. 2004;25;201-208 DOI: 10.1542/pir.25-6-201 The online version of this article, along with updated information and
Pitfalls of the Pediatric Chest and Abdomen SPR 2017
 Pitfalls of the Pediatric Chest and Abdomen SPR 2017 Richard I. Markowitz, MD, FACR Children s Hospital of Philadelphia Perelman School of Medicine University of Pennsylvania No Disclosures Cognitive Perceptual
Pitfalls of the Pediatric Chest and Abdomen SPR 2017 Richard I. Markowitz, MD, FACR Children s Hospital of Philadelphia Perelman School of Medicine University of Pennsylvania No Disclosures Cognitive Perceptual
Case 1. Case Discussion. History. Present Illness. Impression. Physical Examination
 Case 1 Case Discussion R1 林吉倡 2013 / 01 / 02 13-yo Male BW: 45 kg DAY1 16:35 pm C/C: Epigastric pain since this morning TPR: 36.5/94/18 BP:133/83 SpO2: 100% GCS: 15 Triage: 2 Present Illness Sudden-onset
Case 1 Case Discussion R1 林吉倡 2013 / 01 / 02 13-yo Male BW: 45 kg DAY1 16:35 pm C/C: Epigastric pain since this morning TPR: 36.5/94/18 BP:133/83 SpO2: 100% GCS: 15 Triage: 2 Present Illness Sudden-onset
BPD. Neonatal/Pediatric Cardiopulmonary Care. Disease. Bronchopulmonary Dysplasia. Baby Jane
 1 Neonatal/Pediatric Cardiopulmonary Care Disease 2 Bronchopulmonary Dysplasia 3 is a 33-day-old prematurely born girl who weighs 1420 g. At birth, her estimated gestational age was 28 weeks. Her initial
1 Neonatal/Pediatric Cardiopulmonary Care Disease 2 Bronchopulmonary Dysplasia 3 is a 33-day-old prematurely born girl who weighs 1420 g. At birth, her estimated gestational age was 28 weeks. Her initial
Respiratory Diseases and Disorders
 Chapter 9 Respiratory Diseases and Disorders Anatomy and Physiology Chest, lungs, and conducting airways Two parts: Upper respiratory system consists of nose, mouth, sinuses, pharynx, and larynx Lower
Chapter 9 Respiratory Diseases and Disorders Anatomy and Physiology Chest, lungs, and conducting airways Two parts: Upper respiratory system consists of nose, mouth, sinuses, pharynx, and larynx Lower
IAEM Clinical Guideline 9 Laryngomalacia. Version 1 September, Author: Dr Farah Mustafa
 IAEM Clinical Guideline 9 Laryngomalacia Version 1 September, 2016 Author: Dr Farah Mustafa Guideline lead: Dr Áine Mitchell, in collaboration with IAEM Clinical Guideline committee and Our Lady s Children
IAEM Clinical Guideline 9 Laryngomalacia Version 1 September, 2016 Author: Dr Farah Mustafa Guideline lead: Dr Áine Mitchell, in collaboration with IAEM Clinical Guideline committee and Our Lady s Children
Lecture Notes. Chapter 3: Asthma
 Lecture Notes Chapter 3: Asthma Objectives Define asthma and status asthmaticus List the potential causes of asthma attacks Describe the effect of asthma attacks on lung function List the clinical features
Lecture Notes Chapter 3: Asthma Objectives Define asthma and status asthmaticus List the potential causes of asthma attacks Describe the effect of asthma attacks on lung function List the clinical features
A radiological perspective of assessing neonatal respiratory distress syndrome
 Original Research Article A radiological perspective of assessing neonatal respiratory distress syndrome Jayesh Shah 1, Nikhil Parvatkar 2*, C. Raychaudhuri 3 1 Associate Professor, 2 1 st Year Resident,
Original Research Article A radiological perspective of assessing neonatal respiratory distress syndrome Jayesh Shah 1, Nikhil Parvatkar 2*, C. Raychaudhuri 3 1 Associate Professor, 2 1 st Year Resident,
Chronic lung diseases in children Simple choice 1. Finger clubbing is not characteristic for: a) Diffuse bronchiectasis b) Cystic fibrosis c)
 Diffuse bronchiectasis b) Cystic fibrosis c)") Chronic lung diseases in children Simple choice 1. Finger clubbing is not characteristic for: a) Diffuse bronchiectasis b) Cystic fibrosis c) Bronchiolitis obliterans d) Complicated acute pneumonia e)
Chronic lung diseases in children Simple choice 1. Finger clubbing is not characteristic for: a) Diffuse bronchiectasis b) Cystic fibrosis c) Bronchiolitis obliterans d) Complicated acute pneumonia e)
GOALS AND INSTRUCTIONAL OBJECTIVES
 October 4-7, 2004 Respiratory GOALS: GOALS AND INSTRUCTIONAL OBJECTIVES By the end of the week, the first quarter student will have an in-depth understanding of the diagnoses listed under Primary Diagnoses
October 4-7, 2004 Respiratory GOALS: GOALS AND INSTRUCTIONAL OBJECTIVES By the end of the week, the first quarter student will have an in-depth understanding of the diagnoses listed under Primary Diagnoses
Hyaline membrane disease. By : Dr. Ch Sarishma Peadiatric Pg
 Hyaline membrane disease By : Dr. Ch Sarishma Peadiatric Pg Also called Respiratory distress syndrome. It occurs primarily in premature infants; its incidence is inversely related to gestational age and
Hyaline membrane disease By : Dr. Ch Sarishma Peadiatric Pg Also called Respiratory distress syndrome. It occurs primarily in premature infants; its incidence is inversely related to gestational age and
Airway Foreign Body in Children
 Joseph E. Dohar, M.D., M.S. Dr. Dohar Financial Disclosures Alcon consultant Incusmed consultant Otonomy consultant OrbiMed consultant Learning Objectives Identify clinical situations that may require
Joseph E. Dohar, M.D., M.S. Dr. Dohar Financial Disclosures Alcon consultant Incusmed consultant Otonomy consultant OrbiMed consultant Learning Objectives Identify clinical situations that may require
There are four general types of congenital lung disorders:
 Pediatric Pulmonology Conditions Evaluated and Treated As a parent, watching a child suffer from a respiratory disorder can be frightening and worrisome. Our respiratory specialists provide compassionate
Pediatric Pulmonology Conditions Evaluated and Treated As a parent, watching a child suffer from a respiratory disorder can be frightening and worrisome. Our respiratory specialists provide compassionate
Shifting Atelectasis: A sign of foreign body aspiration in a pediatric patient
 Shifting Atelectasis: A sign of foreign body aspiration in a pediatric patient Diana L Mark, RRT Pediatric Clinical Specialist Respiratory Care Wesley Children s Hospital Discuss when foreign body aspiration
Shifting Atelectasis: A sign of foreign body aspiration in a pediatric patient Diana L Mark, RRT Pediatric Clinical Specialist Respiratory Care Wesley Children s Hospital Discuss when foreign body aspiration
Stridor, Stertor, and Snoring: Pediatric Upper Airway Obstruction. Nathan Page, MD Pediatrics in the Red Rocks June?
 Stridor, Stertor, and Snoring: Pediatric Upper Airway Obstruction Nathan Page, MD Pediatrics in the Red Rocks June? I have no disclosures I do not plan to discuss unapproved or off label use of products
Stridor, Stertor, and Snoring: Pediatric Upper Airway Obstruction Nathan Page, MD Pediatrics in the Red Rocks June? I have no disclosures I do not plan to discuss unapproved or off label use of products
Definitions and diagnostic implications of terms used in the chest radiograph and lung ultrasound diagnoses of pneumonia.
 Supplementary 1 Definitions and diagnostic implications of terms used in the chest radiograph and lung ultrasound diagnoses of pneumonia. Imaging finding Definition Implication CR Consolidation Interstitial
Supplementary 1 Definitions and diagnostic implications of terms used in the chest radiograph and lung ultrasound diagnoses of pneumonia. Imaging finding Definition Implication CR Consolidation Interstitial
Back to Basics: What Imaging Test should I order? Jeanne G. Hill, M.D. Pediatric Radiology Medical University of South Carolina
 Back to Basics: What Imaging Test should I order? Jeanne G. Hill, M.D. Pediatric Radiology Medical University of South Carolina Disclosure Neither I nor any member of my immediate family has a relevant
Back to Basics: What Imaging Test should I order? Jeanne G. Hill, M.D. Pediatric Radiology Medical University of South Carolina Disclosure Neither I nor any member of my immediate family has a relevant
The Respiratory System
 The Respiratory System Respiratory Anatomy Upper respiratory tract Nose Nasal passages Pharynx Larynx Respiratory Anatomy Functions of the upper respiratory tract: Provide entry for inhaled air Respiratory
The Respiratory System Respiratory Anatomy Upper respiratory tract Nose Nasal passages Pharynx Larynx Respiratory Anatomy Functions of the upper respiratory tract: Provide entry for inhaled air Respiratory
October Paediatric Respiratory Workbook APCP RESPIRATORY COMMITTEE
 October 2017 Paediatric Respiratory Workbook APCP RESPIRATORY COMMITTEE This workbook is designed to introduce to you the difference between paediatric and adult anatomy and physiology. It will also give
October 2017 Paediatric Respiratory Workbook APCP RESPIRATORY COMMITTEE This workbook is designed to introduce to you the difference between paediatric and adult anatomy and physiology. It will also give
Airway and Breathing
 Airway and Breathing ETAT Module 2 Adapted from Emergency Triage Assessment and Treatment (ETAT): Manual for Participants, World Health Organization, 2005 Learning Objectives Accurately determine whether
Airway and Breathing ETAT Module 2 Adapted from Emergency Triage Assessment and Treatment (ETAT): Manual for Participants, World Health Organization, 2005 Learning Objectives Accurately determine whether
Unit II Problem 2 Pathology: Pneumonia
 Unit II Problem 2 Pathology: Pneumonia - Definition: pneumonia is the infection of lung parenchyma which occurs especially when normal defenses are impaired such as: Cough reflex. Damage of cilia in respiratory
Unit II Problem 2 Pathology: Pneumonia - Definition: pneumonia is the infection of lung parenchyma which occurs especially when normal defenses are impaired such as: Cough reflex. Damage of cilia in respiratory
Respiratory system. Applied Anatomy &Physiology
 Respiratory system Applied Anatomy &Physiology Anatomy The respiratory system consists of 1)The Upper airway : Nose, mouth and larynx 2)The Lower airways Trachea and the two lungs. Within the lungs,
Respiratory system Applied Anatomy &Physiology Anatomy The respiratory system consists of 1)The Upper airway : Nose, mouth and larynx 2)The Lower airways Trachea and the two lungs. Within the lungs,
The University of Arizona Pediatric Residency Program. Primary Goals for Rotation. Pulmonary
 The University of Arizona Pediatric Residency Program Primary Goals for Rotation Pulmonary 1. GOAL: Diagnose and manage patients with asthma. 2. GOAL: Understand the role of the pediatrician in preventing
The University of Arizona Pediatric Residency Program Primary Goals for Rotation Pulmonary 1. GOAL: Diagnose and manage patients with asthma. 2. GOAL: Understand the role of the pediatrician in preventing
Anatomy & Physiology 2 Canale. Respiratory System: Exchange of Gases
 Anatomy & Physiology 2 Canale Respiratory System: Exchange of Gases Why is it so hard to hold your breath for Discuss! : ) a long time? Every year carbon monoxide poisoning kills 500 people and sends another
Anatomy & Physiology 2 Canale Respiratory System: Exchange of Gases Why is it so hard to hold your breath for Discuss! : ) a long time? Every year carbon monoxide poisoning kills 500 people and sends another
Pulmonary Problems of the Neonate. Jon Palmer, VMD, DACVIM Chief, Neonatal Intensive Care Service New Bolton Center, University of Pennsylvania, USA
 Pulmonary Problems of the Neonate Jon Palmer, VMD, DACVIM Chief, Neonatal Intensive Care Service New Bolton Center, University of Pennsylvania, USA Lower Respiratory Diseases Ventilation/Perfusion Abnormalities
Pulmonary Problems of the Neonate Jon Palmer, VMD, DACVIM Chief, Neonatal Intensive Care Service New Bolton Center, University of Pennsylvania, USA Lower Respiratory Diseases Ventilation/Perfusion Abnormalities
An Overview of Bronchopulmonary Dysplasia and Chronic Lung Disease in Infancy
 An Overview of Bronchopulmonary Dysplasia and Chronic Lung Disease in Infancy Housekeeping: I have no financial disclosures Learning objectives: Develop an understanding of bronchopulmonary dysplasia (BPD)
An Overview of Bronchopulmonary Dysplasia and Chronic Lung Disease in Infancy Housekeeping: I have no financial disclosures Learning objectives: Develop an understanding of bronchopulmonary dysplasia (BPD)
PEDIATRIC EMERGENCIES Sandra Horning, MD Sacred Heart Medical Center Emergency Department
 PEDIATRIC EMERGENCIES Sandra Horning, MD Sacred Heart Medical Center Emergency Department Overview Roles of the EMS in Pediatric Care Growth and Development Assessment Airway Adjuncts and Intravenous Access
PEDIATRIC EMERGENCIES Sandra Horning, MD Sacred Heart Medical Center Emergency Department Overview Roles of the EMS in Pediatric Care Growth and Development Assessment Airway Adjuncts and Intravenous Access
Subject Index. Bacterial infection, see Suppurative lung disease, Tuberculosis
 Subject Index Abscess, virtual 107 Adenoidal hypertrophy, features 123 Airway bleeding, technique 49, 50 Airway stenosis, see Stenosis, airway Anaesthesia biopsy 47 complications 27, 28 flexible 23 26
Subject Index Abscess, virtual 107 Adenoidal hypertrophy, features 123 Airway bleeding, technique 49, 50 Airway stenosis, see Stenosis, airway Anaesthesia biopsy 47 complications 27, 28 flexible 23 26
The Respiratory System Structures of the Respiratory System Structures of the Respiratory System Structures of the Respiratory System Nose Sinuses
 CH 14 D.E. Human Biology The Respiratory System The Respiratory System OUTLINE: Mechanism of Breathing Transport of Gases between the Lungs and the Cells Respiratory Centers in the Brain Function Provides
CH 14 D.E. Human Biology The Respiratory System The Respiratory System OUTLINE: Mechanism of Breathing Transport of Gases between the Lungs and the Cells Respiratory Centers in the Brain Function Provides
Gastroesophageal Reflux Disease in Infants and Children
 Gastroesophageal Reflux Disease in Infants and Children 4 Marzo 2017 Drssa Chiara Leoni Drssa Valentina Giorgio pediatriagastro@gmail.com valentinagiorgio1@gmail.com Definitions: GER GER is the passage
Gastroesophageal Reflux Disease in Infants and Children 4 Marzo 2017 Drssa Chiara Leoni Drssa Valentina Giorgio pediatriagastro@gmail.com valentinagiorgio1@gmail.com Definitions: GER GER is the passage
Phases of Respiration. Chapter 18: The Respiratory System. Structures of the Respiratory System. Structures of the Respiratory System
 Phases of Respiration Chapter 18: The Respiratory System Respiration Process of obtaining oxygen from environment and delivering it to cells Phases of Respiration 1. Pulmonary ventilation between air and
Phases of Respiration Chapter 18: The Respiratory System Respiration Process of obtaining oxygen from environment and delivering it to cells Phases of Respiration 1. Pulmonary ventilation between air and
Pediatric Learning Solutions course alignment with the Neonatal/Pediatric Specialty Examination Detailed Content Outline.
 Pediatric Learning Solutions course alignment with the Neonatal/Pediatric Specialty Examination Detailed Content Outline. The following Pediatric Learning Solutions courses align to focus areas of the
Pediatric Learning Solutions course alignment with the Neonatal/Pediatric Specialty Examination Detailed Content Outline. The following Pediatric Learning Solutions courses align to focus areas of the
!"#$%&'%()'*+,-%&&.'+('*/%)+%,#+0' 12/.,'3%)+"4#%52.
'*+,-%&&.'+('*/%)+%,#+0' 12/.,'3%)+4#%52.") !"#$%&'%()'*+,-%&&.'+('*/%)+%,#+0' 12/.,'3%)+"4#%52.!"#$%&'()$*+&,--#&$.//,0'1232'!-#0'45 *6 '7849!!"#$%&'"(&)*+),$-.*/*01) 2$34/&1)*+)5"-.3.(") 6%.(3")*+)7*(08/$)9(.:"%;.&1)) )?
!"#$%&'%()'*+,-%&&.'+('*/%)+%,#+0' 12/.,'3%)+"4#%52.!"#$%&'()$*+&,--#&$.//,0'1232'!-#0'45 *6 '7849!!"#$%&'"(&)*+),$-.*/*01) 2$34/&1)*+)5"-.3.(") 6%.(3")*+)7*(08/$)9(.:"%;.&1)) )?
Common Pediatric Respiratory Illness and Emergencies
 Common Pediatric Respiratory Illness and Emergencies Rob Cloutier, MD Assistant Professor Emergency Medicine & Pediatrics Oregon Health & Science University Overview Review key differences between pediatric
Common Pediatric Respiratory Illness and Emergencies Rob Cloutier, MD Assistant Professor Emergency Medicine & Pediatrics Oregon Health & Science University Overview Review key differences between pediatric
The Respiratory System
 The Respiratory System By Mr. Danilo Villar Rogayan Jr. Instructor I, Department of Natural Sciences RMTU San Marcelino Introduction Function Move air in an out of lungs (ventilation) Delivers oxygen (O
The Respiratory System By Mr. Danilo Villar Rogayan Jr. Instructor I, Department of Natural Sciences RMTU San Marcelino Introduction Function Move air in an out of lungs (ventilation) Delivers oxygen (O
Respiratory Disease. Dr Amal Damrah consultant Neonatologist and Paediatrician
 Respiratory Disease Dr Amal Damrah consultant Neonatologist and Paediatrician Signs and Symptoms of Respiratory Diseases Cardinal Symptoms Cough Sputum Hemoptysis Dyspnea Wheezes Chest pain Signs and Symptoms
Respiratory Disease Dr Amal Damrah consultant Neonatologist and Paediatrician Signs and Symptoms of Respiratory Diseases Cardinal Symptoms Cough Sputum Hemoptysis Dyspnea Wheezes Chest pain Signs and Symptoms
Simulation 1: Two Year-Old Child in Respiratory Distress
 Simulation 1: Two Year-Old Child in Respiratory Distress Opening Scenario (Links to Section 1) You are the respiratory therapist in a 300 bed community hospital working the evening shift. At 8:30 PM you
Simulation 1: Two Year-Old Child in Respiratory Distress Opening Scenario (Links to Section 1) You are the respiratory therapist in a 300 bed community hospital working the evening shift. At 8:30 PM you
UERMMMC Department of Radiology. Basic Chest Radiology
 UERMMMC Department of Radiology Basic Chest Radiology PHYSICS DENSITIES BONE SOFT TISSUES WATER FAT AIR TELEROENTGENOGRAM Criteria for an Ideal Chest Radiograph 1. Upright 2. Posteroanterior View 3. Full
UERMMMC Department of Radiology Basic Chest Radiology PHYSICS DENSITIES BONE SOFT TISSUES WATER FAT AIR TELEROENTGENOGRAM Criteria for an Ideal Chest Radiograph 1. Upright 2. Posteroanterior View 3. Full
Alyssa Brzenski MD May 2, 2012
 Alyssa Brzenski MD May 2, 2012 Overview Background Pre repair bronchoscopy Thorascopic repair To extubate or not? Esophageal atresia treatment of long gap esophageal atresia Complications following TEF/EA
Alyssa Brzenski MD May 2, 2012 Overview Background Pre repair bronchoscopy Thorascopic repair To extubate or not? Esophageal atresia treatment of long gap esophageal atresia Complications following TEF/EA
Chest X-ray Interpretation
 Chest X-ray Interpretation Introduction Routinely obtained Pulmonary specialist consultation Inherent physical exam limitations Chest x-ray limitations Physical exam and chest x-ray provide compliment
Chest X-ray Interpretation Introduction Routinely obtained Pulmonary specialist consultation Inherent physical exam limitations Chest x-ray limitations Physical exam and chest x-ray provide compliment
Pulmonary Emergencies. Lower Airway Structures Trachea Bronchial tree Primary bronchi Secondary bronchi Bronchioles Alveoli Lungs
 Pulmonary Emergencies Lower Airway Structures Trachea Bronchial tree Primary bronchi Secondary bronchi Bronchioles Alveoli Lungs Pulmonary Surfactant Thin film that coats alveoli Prevents alveoli from
Pulmonary Emergencies Lower Airway Structures Trachea Bronchial tree Primary bronchi Secondary bronchi Bronchioles Alveoli Lungs Pulmonary Surfactant Thin film that coats alveoli Prevents alveoli from
Lecture Notes. Chapter 16: Bacterial Pneumonia
 Lecture Notes Chapter 16: Bacterial Pneumonia Objectives Explain the epidemiology Identify the common causes Explain the pathological changes in the lung Identify clinical features Explain the treatment
Lecture Notes Chapter 16: Bacterial Pneumonia Objectives Explain the epidemiology Identify the common causes Explain the pathological changes in the lung Identify clinical features Explain the treatment
Case 1. A 35-year-old male presented with fever, cough, and purulent sputum for one week. This was his CXR (Fig. 1.1). What is the diagnosis?
. What is the diagnosis?") 1 Interpreting Chest X-Rays CASE 1 Fig. 1.1 Case 1. A 35-year-old male presented with fever, cough, and purulent sputum for one week. This was his CXR (Fig. 1.1). What is the diagnosis? CASE 1 Interpreting
1 Interpreting Chest X-Rays CASE 1 Fig. 1.1 Case 1. A 35-year-old male presented with fever, cough, and purulent sputum for one week. This was his CXR (Fig. 1.1). What is the diagnosis? CASE 1 Interpreting
TB Intensive Houston, Texas
 TB Intensive Houston, Texas October 15-17, 17 2013 Diagnosis of TB: Radiology Rosa M Estrada-Y-Martin, MD MSc FCCP October 16, 2013 Rosa M Estrada-Y-Martin, MD MSc FCCP, has the following disclosures to
TB Intensive Houston, Texas October 15-17, 17 2013 Diagnosis of TB: Radiology Rosa M Estrada-Y-Martin, MD MSc FCCP October 16, 2013 Rosa M Estrada-Y-Martin, MD MSc FCCP, has the following disclosures to
Video Cases in Pediatrics. Ran Goldman, MD BC Children s Hospital University of British
 Video Cases in Pediatrics Ran Goldman, MD BC Children s Hospital University of British Columbia @Dr_R_Goldman Bronchiolitis Viral infection of the lower respiratory tract characterized by acute inflammation,
Video Cases in Pediatrics Ran Goldman, MD BC Children s Hospital University of British Columbia @Dr_R_Goldman Bronchiolitis Viral infection of the lower respiratory tract characterized by acute inflammation,
Phases of Respiration
 Phases of Respiration We get oxygen from the environment and it goes to our cells, there. Pulmonary ventilation External exchange of gases Internal exchange of gases Overview of respiration. In ventilation,
Phases of Respiration We get oxygen from the environment and it goes to our cells, there. Pulmonary ventilation External exchange of gases Internal exchange of gases Overview of respiration. In ventilation,
After the Chest X-Ray:
 After the Chest X-Ray: What To Do Next Alan S. Brody Professor of Radiology and Pediatrics Chief of Thoracic Imaging Cincinnati Children s Hospital Cincinnati, Ohio USA What Should We Do Next? CT scan?
After the Chest X-Ray: What To Do Next Alan S. Brody Professor of Radiology and Pediatrics Chief of Thoracic Imaging Cincinnati Children s Hospital Cincinnati, Ohio USA What Should We Do Next? CT scan?
RESPIRATORY FAILURE. Michael Kelly, MD Division of Pediatric Critical Care Dept. of Pediatrics
 RESPIRATORY FAILURE Michael Kelly, MD Division of Pediatric Critical Care Dept. of Pediatrics What talk is he giving? DO2= CO * CaO2 CO = HR * SV CaO2 = (Hgb* SaO2 * 1.34) + (PaO2 * 0.003) Sound familiar??
RESPIRATORY FAILURE Michael Kelly, MD Division of Pediatric Critical Care Dept. of Pediatrics What talk is he giving? DO2= CO * CaO2 CO = HR * SV CaO2 = (Hgb* SaO2 * 1.34) + (PaO2 * 0.003) Sound familiar??
Arabian Gulf University Kingdom of Bahrain Year 5 Pediatrics 3 rd Week Discussion with Dr. Muna Al-Jufairi (Part 2)
") Arabian Gulf University Kingdom of Bahrain Year 5 Pediatrics 3 rd Week Discussion with Dr. Muna Al-Jufairi (Part 2) - Case 1: a 32 weeks preterm developed RDS 4 hours after delivery. Chest X-ray shows:
Arabian Gulf University Kingdom of Bahrain Year 5 Pediatrics 3 rd Week Discussion with Dr. Muna Al-Jufairi (Part 2) - Case 1: a 32 weeks preterm developed RDS 4 hours after delivery. Chest X-ray shows:
Presented By : Kamlah Olaimat
 Presented By : Kamlah Olaimat 18\7\2010 Transient Tachpnea of the Definition:- newborn (TTN) TTN is a benign disease of near term or term infant who display respiratory distress shortly after delivery.
Presented By : Kamlah Olaimat 18\7\2010 Transient Tachpnea of the Definition:- newborn (TTN) TTN is a benign disease of near term or term infant who display respiratory distress shortly after delivery.
Objectives. Pulmonary Assessment 12/13/2017
 Pulmonary Assessment Reid Blackwelder, MD, FAAFP Professor and Chair, Family Medicine Quillen Colege of Medicine, ETSU Objectives Understand anatomy and physiology of pulmonary assessment techniques Remember
Pulmonary Assessment Reid Blackwelder, MD, FAAFP Professor and Chair, Family Medicine Quillen Colege of Medicine, ETSU Objectives Understand anatomy and physiology of pulmonary assessment techniques Remember
Foreign Body Management
 Foreign Body Management NYSGE Fellows Summer Course Susana Gonzalez, MD Assistant Professor of Medicine 1 Objectives Timing of endoscopy When? Anatomic location Where? High risk objects What? Choosing
Foreign Body Management NYSGE Fellows Summer Course Susana Gonzalez, MD Assistant Professor of Medicine 1 Objectives Timing of endoscopy When? Anatomic location Where? High risk objects What? Choosing
5/5/2013. The Respiratory System. Chapter 16 Notes. The Respiratory System. Nasal Cavity. Sinuses
 The Respiratory System Chapter 16 Notes The Respiratory System Objectives List the general functions of the respiratory system. Identify the organs of the respiratory system. Describe the functions of
The Respiratory System Chapter 16 Notes The Respiratory System Objectives List the general functions of the respiratory system. Identify the organs of the respiratory system. Describe the functions of
Chapter 10. The Respiratory System Exchange of Gases. Copyright 2009 Pearson Education, Inc.
 Chapter 10 The Respiratory System Exchange of Gases http://www.encognitive.com/images/respiratory-system.jpg Human Respiratory System UPPER RESPIRATORY TRACT LOWER RESPIRATORY TRACT Nose Passageway for
Chapter 10 The Respiratory System Exchange of Gases http://www.encognitive.com/images/respiratory-system.jpg Human Respiratory System UPPER RESPIRATORY TRACT LOWER RESPIRATORY TRACT Nose Passageway for
Multilevel airway obstruction including rare tongue base mass presenting as severe croup in an infant. Tara Brennan, MD 2,3
 Multilevel airway obstruction including rare tongue base mass presenting as severe croup in an infant Tara Brennan, MD 2,3 Jeffrey C. Rastatter, MD, FAAP 1,2 1 Department of Otolaryngology, Northwestern
Multilevel airway obstruction including rare tongue base mass presenting as severe croup in an infant Tara Brennan, MD 2,3 Jeffrey C. Rastatter, MD, FAAP 1,2 1 Department of Otolaryngology, Northwestern
Tubes and lines in neonatal chest radiograph
 Tubes and lines in neonatal chest radiograph Poster No.: C-1008 Congress: ECR 2014 Type: Educational Exhibit Authors: R. TUMMA, N. AHMED, V. Prasad ; Hyderabad/IN, 1 2 1 1 2 HYDERABAD, ANDHRA PRADESH/IN
Tubes and lines in neonatal chest radiograph Poster No.: C-1008 Congress: ECR 2014 Type: Educational Exhibit Authors: R. TUMMA, N. AHMED, V. Prasad ; Hyderabad/IN, 1 2 1 1 2 HYDERABAD, ANDHRA PRADESH/IN
Imaging of Thoracic Trauma: Tips and Traps. Arun C. Nachiappan, MD Associate Professor of Clinical Radiology University of Pennsylvania
 Imaging of Thoracic Trauma: Tips and Traps Arun C. Nachiappan, MD Associate Professor of Clinical Radiology University of Pennsylvania None Disclosures Objectives Describe blunt and penetrating traumatic
Imaging of Thoracic Trauma: Tips and Traps Arun C. Nachiappan, MD Associate Professor of Clinical Radiology University of Pennsylvania None Disclosures Objectives Describe blunt and penetrating traumatic
Chapter 124: Congenital Disorders of the Trachea. Bruce Benjamin
 Chapter 124: Congenital Disorders of the Trachea Bruce Benjamin Investigation of the larynx and pharynx may be incomplete in infants and children with congenital abnormalities without investigation of
Chapter 124: Congenital Disorders of the Trachea Bruce Benjamin Investigation of the larynx and pharynx may be incomplete in infants and children with congenital abnormalities without investigation of
RSV infection and lung ultrasound
 RSV infection and lung ultrasound Neonatology Clinic, University Hospital, Krakow Joanna Hurkała Joanna Pietras Agnieszka Ochoda-Mazur Poznań, 28.09.2018 1 Disclosure In relations to this presentation,
RSV infection and lung ultrasound Neonatology Clinic, University Hospital, Krakow Joanna Hurkała Joanna Pietras Agnieszka Ochoda-Mazur Poznań, 28.09.2018 1 Disclosure In relations to this presentation,
Physical Exam. Vitals stable on room air Abdomen soft, non-distented Normal external genitalia Patent anus No limb anomalies
 Case Presentation 1 day-old full-term baby girl noted to have drooling of saliva and increased secretions at birth Fetal US @32wks had shown polyhydramnios Birth weight 3515g Apgar 7@1min and 8@5min Unable
Case Presentation 1 day-old full-term baby girl noted to have drooling of saliva and increased secretions at birth Fetal US @32wks had shown polyhydramnios Birth weight 3515g Apgar 7@1min and 8@5min Unable
Basic mechanisms disturbing lung function and gas exchange
 Basic mechanisms disturbing lung function and gas exchange Blagoi Marinov, MD, PhD Pathophysiology Department, Medical University of Plovdiv Respiratory system 1 Control of breathing Structure of the lungs
Basic mechanisms disturbing lung function and gas exchange Blagoi Marinov, MD, PhD Pathophysiology Department, Medical University of Plovdiv Respiratory system 1 Control of breathing Structure of the lungs
Lecture 3. Inflammatory Processes
 Lecture 3 Inflammatory Processes Process: Increased vascular permeability Water and cellular infiltrations Results: Abscess, ulceration, cavitation Penetration, perforation and fistula formation Scarring,
Lecture 3 Inflammatory Processes Process: Increased vascular permeability Water and cellular infiltrations Results: Abscess, ulceration, cavitation Penetration, perforation and fistula formation Scarring,
An Image Repository for Chest CT
 An Image Repository for Chest CT Francesco Frajoli for the Chest CT in Antibody Deficiency Group An Image Repository for Chest CT he Chest CT in Antibody Deficiency Group is an international and interdisciplinary
An Image Repository for Chest CT Francesco Frajoli for the Chest CT in Antibody Deficiency Group An Image Repository for Chest CT he Chest CT in Antibody Deficiency Group is an international and interdisciplinary
Review. 1. How does a child s anatomy differ from an adult s anatomy?
 Chapter 32 Review Review 1. How does a child s anatomy differ from an adult s anatomy? A. The child s trachea is more rigid B. The tongue is proportionately smaller C. The epiglottis is less floppy in
Chapter 32 Review Review 1. How does a child s anatomy differ from an adult s anatomy? A. The child s trachea is more rigid B. The tongue is proportionately smaller C. The epiglottis is less floppy in
Handling Common Problems & Pitfalls During. Oxygen desaturation in patients receiving mechanical ventilation ACUTE SEVERE RESPIRATORY FAILURE
 Handling Common Problems & Pitfalls During ACUTE SEVERE RESPIRATORY FAILURE Pravit Jetanachai, MD QSNICH Oxygen desaturation in patients receiving mechanical ventilation Causes of oxygen desaturation 1.
Handling Common Problems & Pitfalls During ACUTE SEVERE RESPIRATORY FAILURE Pravit Jetanachai, MD QSNICH Oxygen desaturation in patients receiving mechanical ventilation Causes of oxygen desaturation 1.
Understanding Cough, Wheezing and Noisy Breathing in Children. Introduction
 Understanding Cough, Wheezing and Noisy Breathing in Children Introduction Symptoms such as cough, wheezing or noisy breathing can be caused by a number of conditions. When these occur, it is natural for
Understanding Cough, Wheezing and Noisy Breathing in Children Introduction Symptoms such as cough, wheezing or noisy breathing can be caused by a number of conditions. When these occur, it is natural for
Karen Corlett, RN, MSN, CPNP-AC/PC Pediatric Nurse Practitioner Congenital Heart Surgery Unit Pediatric Cardiac Intensivists of North Texas Medical
 Karen Corlett, RN, MSN, CPNP-AC/PC Pediatric Nurse Practitioner Congenital Heart Surgery Unit Pediatric Cardiac Intensivists of North Texas Medical City Children s Hospital, Dallas Hypoxia Shortage of
Karen Corlett, RN, MSN, CPNP-AC/PC Pediatric Nurse Practitioner Congenital Heart Surgery Unit Pediatric Cardiac Intensivists of North Texas Medical City Children s Hospital, Dallas Hypoxia Shortage of
INTRODUCTION The effect of CPAP works on lung mechanics to improve oxygenation (PaO 2
 2 Effects of CPAP INTRODUCTION The effect of CPAP works on lung mechanics to improve oxygenation (PaO 2 ). The effect on CO 2 is only secondary to the primary process of improvement in lung volume and
2 Effects of CPAP INTRODUCTION The effect of CPAP works on lung mechanics to improve oxygenation (PaO 2 ). The effect on CO 2 is only secondary to the primary process of improvement in lung volume and
Equipment: NRP algorithm, MRSOPA table, medication chart, SpO 2 table Warm
 NRP Skills Stations Performance Skills Station OR Integrated Skills Station STATION: Assisting with and insertion of endotracheal tube (ETT) Equipment: NRP algorithm, MRSOPA table, medication chart, SpO
NRP Skills Stations Performance Skills Station OR Integrated Skills Station STATION: Assisting with and insertion of endotracheal tube (ETT) Equipment: NRP algorithm, MRSOPA table, medication chart, SpO
NON INVASIVE LIFE SAVERS. Non Invasive Ventilation (NIV)
") Table 1. NIV: Mechanisms Of Action Decreases work of breathing Increases functional residual capacity Recruits collapsed alveoli Improves respiratory gas exchange Reverses hypoventilation Maintains upper
Table 1. NIV: Mechanisms Of Action Decreases work of breathing Increases functional residual capacity Recruits collapsed alveoli Improves respiratory gas exchange Reverses hypoventilation Maintains upper
Development of Respiratory System. Dr. Sanaa Alshaarawy& Dr. Saeed Vohra
 Development of Respiratory System Dr. Sanaa Alshaarawy& Dr. Saeed Vohra OBJECTIVES At the end of the lecture the students should be able to: Identify the development of the laryngeotracheal (respiratory)
Development of Respiratory System Dr. Sanaa Alshaarawy& Dr. Saeed Vohra OBJECTIVES At the end of the lecture the students should be able to: Identify the development of the laryngeotracheal (respiratory)
Firefighter Pre-Hospital Care Program Recruit Presentation. Respiratory Emergencies
 Firefighter Pre-Hospital Care Program Recruit Presentation Respiratory Emergencies The Respiratory System Anatomy Pharynx Nasopharynx Oropharynx Epiglottis Larynx Trachea Right main bronchus Left main
Firefighter Pre-Hospital Care Program Recruit Presentation Respiratory Emergencies The Respiratory System Anatomy Pharynx Nasopharynx Oropharynx Epiglottis Larynx Trachea Right main bronchus Left main
Chapter 10 The Respiratory System
 Chapter 10 The Respiratory System Biology 2201 Why do we breathe? Cells carry out the reactions of cellular respiration in order to produce ATP. ATP is used by the cells for energy. All organisms need
Chapter 10 The Respiratory System Biology 2201 Why do we breathe? Cells carry out the reactions of cellular respiration in order to produce ATP. ATP is used by the cells for energy. All organisms need
Pediatric Bronchiolitis. Janie Robles, PharmD, AE-C Assistant Professor of Pharmacy Practice Pediatrics School of Pharmacy TTUHSC Lubbock, Texas
 This PowerPoint file is a supplement to the video presentation. Some of the educational content of this program is not available solely through the PowerPoint file. Participants should use all materials
This PowerPoint file is a supplement to the video presentation. Some of the educational content of this program is not available solely through the PowerPoint file. Participants should use all materials
Chapter 13. Respiratory Emergencies
 Chapter 13 Respiratory Emergencies Introduction Patients often complain about dyspnea. Shortness of breath Symptom of many different conditions Cause can be difficult to determine. Even for physician in
Chapter 13 Respiratory Emergencies Introduction Patients often complain about dyspnea. Shortness of breath Symptom of many different conditions Cause can be difficult to determine. Even for physician in
Tracheoesophageal Fistula and Esophageal Atresia
 Patient and Family Education Tracheoesophageal Fistula and Esophageal Atresia What is tracheoesophageal fistula? The word fistula means abnormal connection. Tracheoesophageal fistula (TEF) is a condition
Patient and Family Education Tracheoesophageal Fistula and Esophageal Atresia What is tracheoesophageal fistula? The word fistula means abnormal connection. Tracheoesophageal fistula (TEF) is a condition
Children are not small adults Children are Not Small Adults Anatomic considerations Pliable bony & cartilagenous structures - Significant thoracic inj
 PEDIATRIC CHEST TRAUMA Children are not small adults Role of imaging Spectrum of injury Children are not small adults Children are Not Small Adults Anatomic considerations Pliable bony & cartilagenous
PEDIATRIC CHEST TRAUMA Children are not small adults Role of imaging Spectrum of injury Children are not small adults Children are Not Small Adults Anatomic considerations Pliable bony & cartilagenous