Head injuries in children. Dr Jason Hort Paediatrician Paediatric Emergency Physician, June 2017 Children s Hospital Westmead
|
|
|
- Candice Campbell
- 5 years ago
- Views:
Transcription
1
2 Head injuries in children Dr Jason Hort Paediatrician Paediatric Emergency Physician, June 2017 Children s Hospital Westmead
3 Objectives Approach to minor head injury Child protection issues Concussion
4 Perspective Tertiary children s hospital Neurosurgical service 24 hr paediatric medical and nursing service Referral patterns biased to severity Generally good access to ct scan
")
5 Wentworth Falls ( most of the time)

6 Sometimes it pours
7 Anyone involved in the management of major head injury?

8

9

10

11

12

13
14
15 Assessment A with c spine B C D- AVPU then modified GCS and pupils Don t ever forget glucose E- Secondary survey
16
17 Modified GCS Modified Glasgow Coma Scale Use for young children and infants who have limited receptive and expressive language abilities Has amendments for the assessment of verbal response
18 Eye opening Spontaneous To voice To pain None Verbal response Appropriate words or social smile, fixes and follows Cries, but is consolable Persistently irritable Restless, agitated None Movement/motor response Spontaneous movement (<1yr) Obeys command (>1yr) Localises to pain Flexion- withdrawal to pain Flexion-abnormal Extension None Score
19 GCS Has prognostic value in trauma patients GCS 3-5 = severe HI, significant likelihood of permanent impairment GCS 6-8 = moderately severe HI, needs ICU, may have permanent impairment GCS >8 = more likely to have good outcome
20 Assessment of HI severity Mild moderate severe Use of modified gcs For mild head injury, gcs >13 Development of different guidelines address first hours after injury up to 24 hours Age, mechanism, symptoms and signs are all part of these guidelines
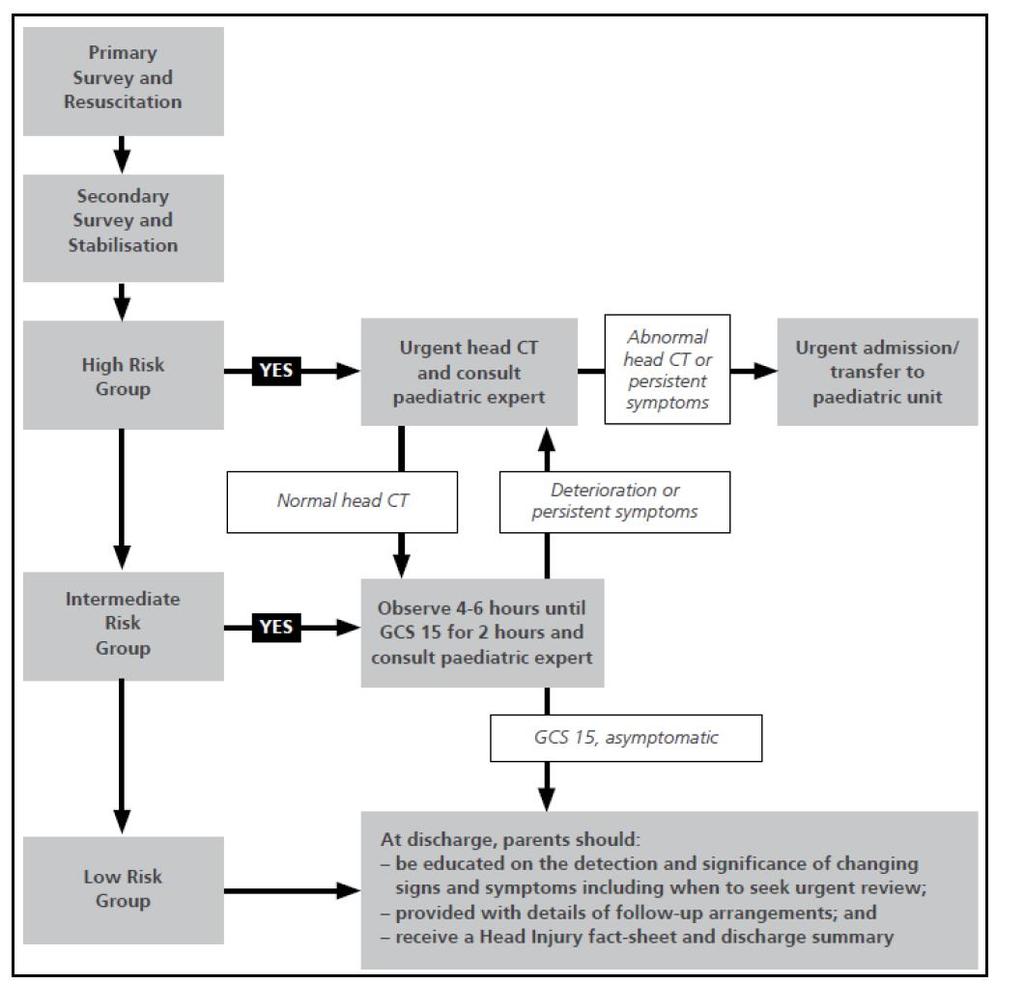
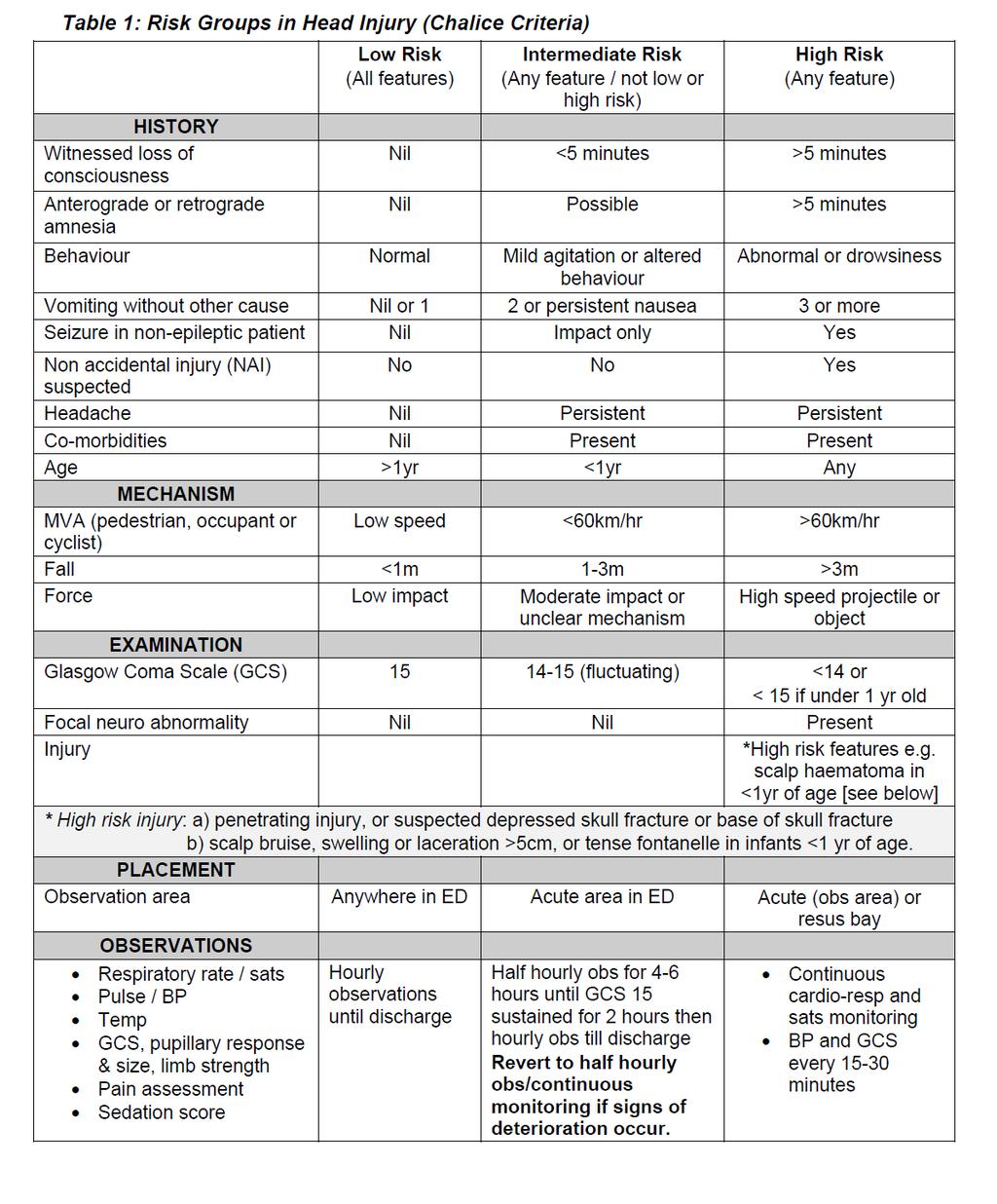
21 Risk stratification from the guidelines

22 Three Cases
23
24 History Mechanism examination
25 3yo Rear seat passenger, restrained, Truck hits car Mod GCS 6 E=1, V=1 M=4 Pupil left large and unreactive Helicopter retrieval Intubated on scene, 500ml crystalloid,

26
27 Guidelines Ministry of health Head injury guidelines or rules Based on chalice study Also Catch and Pecarn studies Recent Predict study paediatric research in emergency depts. International collaborative Comparing these in children in aust+nz
28 Chalice Study Group UK Chalice Children s head injury algorithm for the prediction of important clinical events A prospective multicentre diagnostic cohort study to provide a rule for selection of high-risk children with head injuries for CT scanning The first head injury decision rule for children Misses 5% of significant injury
29 The CATCH rule The Canadian Assessment of Tomography for Childhood Head injury Prospective cohort study patients 15% scan rate
30 PECARN Pediatric emergency care applied research network More who not to scan, Up to 50% of head injured children would get a scan
31 Australian review- lancet april children 23% admitted Clinically significant head injury Ct rate of 10.5% 83 <1% neurosurgery 15 died
32 Statistics Head injuries 1-2% of visits to ED Classification according to GCS Mild HI GCS = 97% Moderate GCS 9-13 =0.5% Severe GCS 8 or less = 0.6%
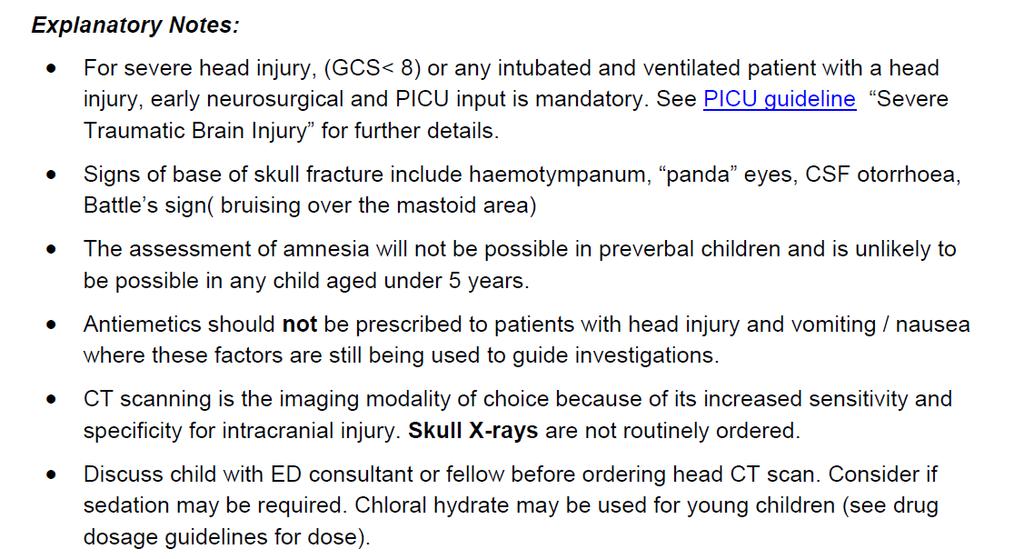
33 CT scan Ct scan radiation risk 1/1000 brain tumours from ct scan Under 4 yo may need sedation May be more helpful to say For observation, may need a scan
34 CT scan Earn your ct scan Document reasons and criteria they meet for ct scan Observation as an alternative 4hrs post injury 6 hrs post injury overnight
35 10 yo playing golf Hit in the left head by a golf club Initial loc 1-2 mins A little confused, Went home Subsequently a little more sleepy Presents to small country hospital
36 Abc intact pr 90,bp 110/60 Gcs 14, perl, e=3,v=5, m=5 Swelling to left side of head 10 pm at night, No scanner, What to do?
37

38
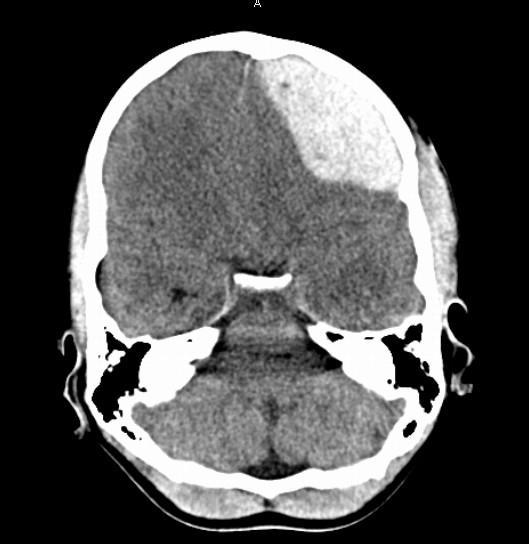
39 11 month old 11 mth old, visiting grandfather at private hospital, fell out of pram, after standing up, On tiles, Took a deep breath and cried, Consolable, Remained irritable, Kept vomiting
40 Presents 18 hours later With Mother and grandmother Mother with plaster cast on leg Irritable, Temp 36.5, pr 140,well perfused RR 24, sats 97% room air Pupils 2+ equal
41 Crying, Moving all limbs, Briefly consolable, fixes and follows, Fontanelle full, Boggy swelling right occipitalparietal region No other injury,
42 When not crying quiet, responds to pain Modified gcs E2, V4, M4 =10 Quiet enough to CT scan without sedation
43

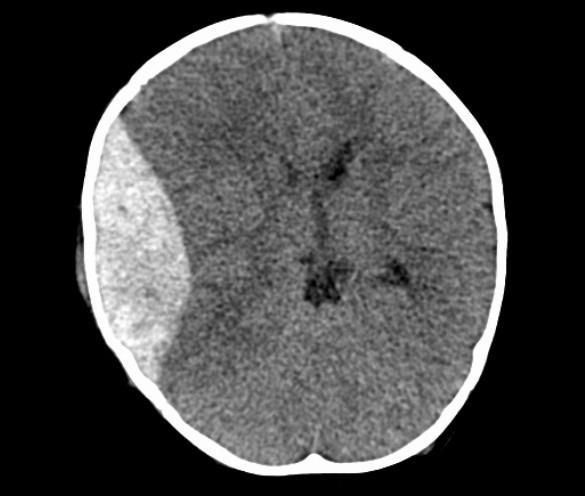
44 Middle meningeal artery
45 Large right extradural with mass effect Right parietal skull fracture Urgent theatre I am not a bad mother
46 Good response Discharged after one week Rehab team involved Child Protection team involved, DOCs previously involved, No siblings, lives with GM An accidental injury
47 Child protection Screening Delay in presentation Story not consistent/compatible Other injuries Previous history
48 Discharge
49 Discharge

50
51
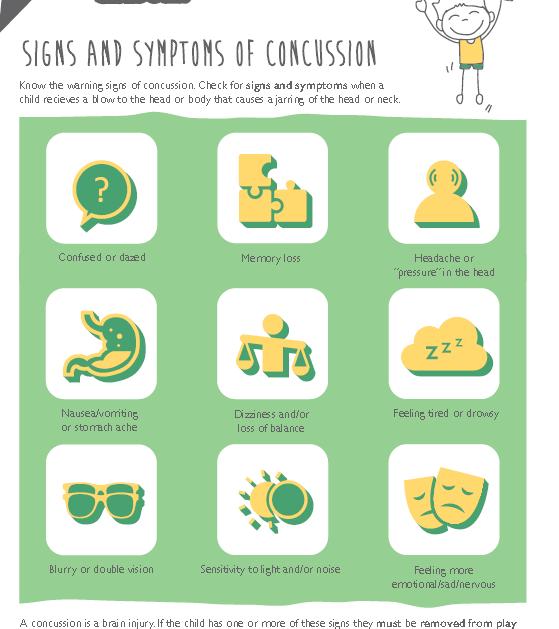
52 Concussion A concussion is an injury to the brain caused by sudden strong movement of the brain against the skull. A child does not need to be knocked out (lose consciousness) to have concussion. it is important to be on the lookout for warning signs which could appear immediately after a bump to the head or body, or over the following hours and days.
53

54
55
56
57
58
59
60
61 Concussion Know the signs and symptoms of concussion; and if you suspect a concussion, remove the child from play immediately. Physical activity is essential to the healthy development of children and young people and should be encouraged. It is important however, to be aware of the risk of sports concussion so that children may be given the best care when needed. A concussion is an injury to the brain caused by sudden strong movement of the brain against the skull. This is caused by a collision with another person or object. A child does not need to be knocked out (lose consciousness) to have concussion. Most concussion injuries do not involve any loss of consciousness, so it is important to be on the lookout for warning signs which could appear immediately after a bump to the head or body, or over the following hours and days.
62
63
64
65
66
67
68 Herniation Extensor posturing or hemiparesis Hypertension, bradycardia, irregular respirations Pupillary signs sluggish reaction, unilateral or bilateral dilation

69
70 Why children Large head to body ratio, high centre of gravity skull thinner and plastic transmits rather than attenuates impact skull fractures more common
71 Adults who suffered severe brain injuries as preschoolers only ¼ work full time and independently
72 GCS of 3-4 at 24 hours is BAD Severe TBI persistent multiple deficits Mild or moderate- recover verbal and non verbal skills and achieve IQ scores in the normal range. Young children with severe TBI flattest recovery
73 Who gets a CT scan?
74 Head Injury descriptors Extra axial = outside the brain Intra axial = inside the brain Extra axial- skull, extradural (epidural), subdural subarachnoid and intraventricular Intra axial - contusion, laceration, haemorrhage and DAI (= diffuse axonal injury) from rotational and shearing forces,
75 TBI leading cause of morbidity and mortality in paediatric trauma Most common cause is falls, Then MVA s
76 Chalice Study Group UK Inclusion criteria - any pt < 16 yrs with a history or signs of injury to the head. LOC and amnesia was not a requirement children presenting to the ED of 10 hospitals in 2 ½ yrs
77 Chalice Study Group UK Results 774 children had a CT head 281 (1.2%) patients showed an abnormality on CT 137 (0.6%) patients required neurosurgical intervention 15 patients died
78 CT Yes: History Witnessed LOC of > 5 min duration History of amnesia (antegrade or retrograde) of > 5 min Abnormal drowsiness 3 vomits after head injury Suspicion of NAI Seizure after head injury in a pt with no history of epilepsy
79 Examination GCS < 14, or GCS < 15 if < 1 year old Suspicion of penetrating or depressed skull injury or tense fontanelle Signs of basal skull # Positive focal neurology Presence of bruise, swelling or laceration > 5 cm if < 1 year old
80 Mechanism High speed RTA either as pedestrian, cyclist or occupant ( > 40 m /h) Fall of > 3 m in height High-speed injury from a projectile or an object
81 Four high-risk factors GCS < 15 within 2 hrs, suspected open skull #, worsening headache, irritability High-risk factors 100% sensitive for predicting need for neurosurgical intervention
82 3 Medium risk factors large boggy scalp haematoma, signs of basal skull #, dangerous mechanism of injury Medium-risk factors 98.3% sensitive
83 Management Observation Until well, 4 hours post HI Discharge with RESPONSIBLE ADULT Clear instructions Head injury advice- written
84 Prevention Helmets On the golf course In the pram In the shopping trolley In the playground
85 Surgery Options Decompressive craniectomy ICP refractory to other treatments Patients who deteriorate after admission NAI
2016 PQRS OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS, REGISTRY
 Measure #416: Emergency Medicine: Emergency Department Utilization of CT for Minor Blunt Head Trauma for Patients Aged 2 through 17 Years - National Quality Strategy Domain: Efficiency and Cost Reduction
Measure #416: Emergency Medicine: Emergency Department Utilization of CT for Minor Blunt Head Trauma for Patients Aged 2 through 17 Years - National Quality Strategy Domain: Efficiency and Cost Reduction
2017 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY. MEASURE TYPE: Efficiency
 Measure #416: Emergency Medicine: Emergency Department Utilization of CT for Minor Blunt Head Trauma for Patients Aged 2 Through 17 Years - National Quality Strategy Domain: Efficiency and Cost Reduction
Measure #416: Emergency Medicine: Emergency Department Utilization of CT for Minor Blunt Head Trauma for Patients Aged 2 Through 17 Years - National Quality Strategy Domain: Efficiency and Cost Reduction
Pre-hospital Response to Trauma and Brain Injury. Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center
 Pre-hospital Response to Trauma and Brain Injury Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center Traumatic Brain Injury is Common 235,000 Americans hospitalized for non-fatal TBI
Pre-hospital Response to Trauma and Brain Injury Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center Traumatic Brain Injury is Common 235,000 Americans hospitalized for non-fatal TBI
LOSS OF CONSCIOUSNESS & ASSESSMENT. Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT
 LOSS OF CONSCIOUSNESS & ASSESSMENT Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT OUTLINE Causes Head Injury Clinical Features Complications Rapid Assessment Glasgow Coma Scale Classification
LOSS OF CONSCIOUSNESS & ASSESSMENT Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT OUTLINE Causes Head Injury Clinical Features Complications Rapid Assessment Glasgow Coma Scale Classification
Head injury in children
 Head injury in children Michael Kim, MD Department of Emergency Medicine University of Wisconsin- Madison #1 cause of death and disability Bimodal distribution 62,000 hospitalization 564,000 ED visits
Head injury in children Michael Kim, MD Department of Emergency Medicine University of Wisconsin- Madison #1 cause of death and disability Bimodal distribution 62,000 hospitalization 564,000 ED visits
Disclosure Statement. Dr. Kadish has no relevant financial relationships with any commercial interests mentioned in this talk.
 Disclosure Statement Dr. Kadish has no relevant financial relationships with any commercial interests mentioned in this talk. Head Trauma Evaluation Primary and secondary injury Disposition Sports related
Disclosure Statement Dr. Kadish has no relevant financial relationships with any commercial interests mentioned in this talk. Head Trauma Evaluation Primary and secondary injury Disposition Sports related
8/29/2011. Brain Injury Incidence: 200/100,000. Prehospital Brain Injury Mortality Incidence: 20/100,000
 Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
Management of Severe Traumatic Brain Injury
 Guideline for North Bristol Trust Management of Severe Traumatic Brain Injury This guideline describes the following: Initial assessment and management of the patient with head injury Indications for CT
Guideline for North Bristol Trust Management of Severe Traumatic Brain Injury This guideline describes the following: Initial assessment and management of the patient with head injury Indications for CT
Brain Injuries. Presented By Dr. Said Said Elshama
 Brain Injuries Presented By Dr. Said Said Elshama Types of head injuries 1- Scalp injuries 2- Skull injuries 3- Intra Cranial injuries ( Brain ) Anatomical structure of meninges Intra- Cranial Injuries
Brain Injuries Presented By Dr. Said Said Elshama Types of head injuries 1- Scalp injuries 2- Skull injuries 3- Intra Cranial injuries ( Brain ) Anatomical structure of meninges Intra- Cranial Injuries
spontaneous localises pain withdraws to pain abnormal flexion abnormal extension none > 5 years 2 5 years 0 2 years
 APPENDIX. GLASGOW COMA SCALES (GCS) For Adults Alert patients have a total score of 5 Eye Opening: to voice to pain Verbal Score: 5 oriented confused but answers questions inappropriate words: recognises
APPENDIX. GLASGOW COMA SCALES (GCS) For Adults Alert patients have a total score of 5 Eye Opening: to voice to pain Verbal Score: 5 oriented confused but answers questions inappropriate words: recognises
PRACTICE GUIDELINE. DEFINITIONS: Mild head injury: Glasgow Coma Scale* (GCS) score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8
 score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8") PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
Introduction to Neurosurgical Subspecialties:
 Introduction to Neurosurgical Subspecialties: Trauma and Critical Care Neurosurgery Brian L. Hoh, MD 1, Gregory J. Zipfel, MD 2 and Stacey Q. Wolfe, MD 3 1 University of Florida, 2 Washington University,
Introduction to Neurosurgical Subspecialties: Trauma and Critical Care Neurosurgery Brian L. Hoh, MD 1, Gregory J. Zipfel, MD 2 and Stacey Q. Wolfe, MD 3 1 University of Florida, 2 Washington University,
Kristin s Head Trauma Board Questions 11/07/14
 Kristin s Head Trauma Board Questions { 11/07/14 A healthy 15 y/o boy was playing football at a park near his home with a group of friends when he tripped over a friend s leg while trying to catch a pass.
Kristin s Head Trauma Board Questions { 11/07/14 A healthy 15 y/o boy was playing football at a park near his home with a group of friends when he tripped over a friend s leg while trying to catch a pass.
PedsCases Podcast Scripts
 PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on the Approach to Pediatric Head Injury. These podcasts are designed to give medical students an overview of key topics
PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on the Approach to Pediatric Head Injury. These podcasts are designed to give medical students an overview of key topics
Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth. Objectives 11/7/2017
 Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth Objectives 1. Be able to discuss brain anatomy and physiology as it applies to
Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth Objectives 1. Be able to discuss brain anatomy and physiology as it applies to
HEAD INJURY. Dept Neurosurgery
 HEAD INJURY Dept Neurosurgery INTRODUCTION PATHOPHYSIOLOGY CLINICAL CLASSIFICATION MANAGEMENT - INVESTIGATIONS - TREATMENT INTRODUCTION Most head injuries are due to an impact between the head and another
HEAD INJURY Dept Neurosurgery INTRODUCTION PATHOPHYSIOLOGY CLINICAL CLASSIFICATION MANAGEMENT - INVESTIGATIONS - TREATMENT INTRODUCTION Most head injuries are due to an impact between the head and another
10/6/2017. Notice. Traumatic Brain Injury & Head Trauma
 Notice All EMS Live@Nite presentations will be recorded (both audio and video) and available for public viewing online. By participating in EMS Live@Nite, you consent to audio and video recording and its/their
Notice All EMS Live@Nite presentations will be recorded (both audio and video) and available for public viewing online. By participating in EMS Live@Nite, you consent to audio and video recording and its/their
Head injuries. Severity of head injuries
 Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
Traumatic brain injuries are caused by external mechanical forces such as: - Falls - Transport-related accidents - Assault
 PP2231 Brain injury Cerebrum consists of frontal, parietal, occipital and temporal lobes Diencephalon consists of thalamus, hypothalamus Cerbellum Brain stem consists of midbrain, pons, medulla Central
PP2231 Brain injury Cerebrum consists of frontal, parietal, occipital and temporal lobes Diencephalon consists of thalamus, hypothalamus Cerbellum Brain stem consists of midbrain, pons, medulla Central
USE OF CT SCAN IN A CHILD WITH MTBI
 TO SCAN OR NOT TO SCAN USE OF CT SCAN IN A CHILD WITH MTBI LISA AYOUB-RODRIGUEZ MD PEDIATRIC HOSPITALIST MIKE LEE MD PEDIATRIC RESIDENT BERT JOHANSSON MD PEDIATRIC HOSPITALIST DISCLOSURES I M NOT A SURGEON
TO SCAN OR NOT TO SCAN USE OF CT SCAN IN A CHILD WITH MTBI LISA AYOUB-RODRIGUEZ MD PEDIATRIC HOSPITALIST MIKE LEE MD PEDIATRIC RESIDENT BERT JOHANSSON MD PEDIATRIC HOSPITALIST DISCLOSURES I M NOT A SURGEON
Use of CT in minor traumatic brain injury. Lisa Ayoub-Rodriguez, MD Bert Johansson, MD Michael Lee, MD
 Use of CT in minor traumatic brain injury Lisa Ayoub-Rodriguez, MD Bert Johansson, MD Michael Lee, MD No financial or other conflicts of interest Epidemiology of traumatic brain injury (TBI) Risks associated
Use of CT in minor traumatic brain injury Lisa Ayoub-Rodriguez, MD Bert Johansson, MD Michael Lee, MD No financial or other conflicts of interest Epidemiology of traumatic brain injury (TBI) Risks associated
HEAD INJURY MODULE ASSESSMENT OF HEAD INJURY
 HEAD INJURY MODULE Introduction Head injury is common in both adult and paediatric populations. In all-comers with head injury, () 90% present with normal or near-normal consciousness, and mortality is
HEAD INJURY MODULE Introduction Head injury is common in both adult and paediatric populations. In all-comers with head injury, () 90% present with normal or near-normal consciousness, and mortality is
Referral Criteria for Medical CT Radiation Exposures. Neuro Referrals
 Referral Criteria for Medical CT Radiation Exposures Neuro Referrals CHH & HRI The Ionising Radiation (Medical Exposure) Regulations 2017 Document Control Reference No: 3.2 First published: 2016 Version:
Referral Criteria for Medical CT Radiation Exposures Neuro Referrals CHH & HRI The Ionising Radiation (Medical Exposure) Regulations 2017 Document Control Reference No: 3.2 First published: 2016 Version:
TBI are twice as common in males High potential for poor outcome Deaths occur at three points in time after injury
 Head Injury Any trauma to (closed vs. open) Skull Scalp Brain Traumatic brain injury (TBI) High incidence Most common causes Falls Motor vehicle accidents Other causes Firearm- related injuries Assaults
Head Injury Any trauma to (closed vs. open) Skull Scalp Brain Traumatic brain injury (TBI) High incidence Most common causes Falls Motor vehicle accidents Other causes Firearm- related injuries Assaults
Mild Traumatic Brain Injury
 Mild Traumatic Brain Injury Concussions This presentation is for information purposes only, not for any commercial purpose, and may not be sold or redistributed. David Wesley, M.D. Outline Epidemiology
Mild Traumatic Brain Injury Concussions This presentation is for information purposes only, not for any commercial purpose, and may not be sold or redistributed. David Wesley, M.D. Outline Epidemiology
:: Closed Head Injury in Adults
 ADULT TRAUMA CLINICAL PRACTICE GUIDELINES Initial Management of :: Closed Head Injury in Adults Suggested citation: Dr Duncan Reed 2007, Adult Trauma Clinical Practice Guidelines, Initial Management of
ADULT TRAUMA CLINICAL PRACTICE GUIDELINES Initial Management of :: Closed Head Injury in Adults Suggested citation: Dr Duncan Reed 2007, Adult Trauma Clinical Practice Guidelines, Initial Management of
BATLS Battlefield Advanced Trauma Life Support
 J R Army Med Corps 2002; 148: 151-158 BATLS Battlefield Advanced Trauma Life Support CHAPTER 8 HEAD INJURIES Aim 0801. On successfully completing this topic you will be able to: Discuss general management
J R Army Med Corps 2002; 148: 151-158 BATLS Battlefield Advanced Trauma Life Support CHAPTER 8 HEAD INJURIES Aim 0801. On successfully completing this topic you will be able to: Discuss general management
PEDIATRIC MILD TRAUMATIC HEAD INJURY
 PEDIATRIC MILD TRAUMATIC HEAD INJURY October 2011 Quality Improvement Resources Illinois Emergency Medical Services for Children is a collaborative program between the Illinois Department of Public Health
PEDIATRIC MILD TRAUMATIC HEAD INJURY October 2011 Quality Improvement Resources Illinois Emergency Medical Services for Children is a collaborative program between the Illinois Department of Public Health
European Resuscitation Council
 European Resuscitation Council Incidence of Trauma in Childhood Leading cause of death and disability in children older than one year all over the world Structured approach Primary survey and resuscitation
European Resuscitation Council Incidence of Trauma in Childhood Leading cause of death and disability in children older than one year all over the world Structured approach Primary survey and resuscitation
Can we abolish skull x-rays for head injury?
 ADC Online First, published on April 25, 2005 as 10.1136/adc.2004.053603 Can we abolish skull x-rays for head injury? Matthew J Reed, Jen G Browning, A. Graham Wilkinson & Tom Beattie Corresponding author:
ADC Online First, published on April 25, 2005 as 10.1136/adc.2004.053603 Can we abolish skull x-rays for head injury? Matthew J Reed, Jen G Browning, A. Graham Wilkinson & Tom Beattie Corresponding author:
A SERIES OF PAEDIATRIC TOPICS DR DANIEL WATSON
 A SERIES OF PAEDIATRIC TOPICS DR DANIEL WATSON March 2014 Who am I? MBChB Otago 1996 FACEM 2004 Staff specialist Wellington ED 2004- ~ 55k presentations PA ~ 20% paediatric APLS instructor Locum work NT
A SERIES OF PAEDIATRIC TOPICS DR DANIEL WATSON March 2014 Who am I? MBChB Otago 1996 FACEM 2004 Staff specialist Wellington ED 2004- ~ 55k presentations PA ~ 20% paediatric APLS instructor Locum work NT
Pediatric Abusive Head Trauma
 Pediatric Abusive Head Trauma Rebecca Girardet Associate Professor of Pediatrics Director, Division of Child Protection Pediatrics McGovern Medical School at The University of Texas Health Science Center
Pediatric Abusive Head Trauma Rebecca Girardet Associate Professor of Pediatrics Director, Division of Child Protection Pediatrics McGovern Medical School at The University of Texas Health Science Center
School of Hard Knocks! Richard Beebe MS RN NRP MedicThink LLC
 School of Hard Knocks! Richard Beebe MS RN NRP MedicThink LLC Fall of a Teton How Bad is He Hurt? What REALLY happened inside Johnny s head? How common are these types of injuries? PONDER THIS What part
School of Hard Knocks! Richard Beebe MS RN NRP MedicThink LLC Fall of a Teton How Bad is He Hurt? What REALLY happened inside Johnny s head? How common are these types of injuries? PONDER THIS What part
Case 1. Case 5/30/2013. Traumatic Brain Injury : Review, Update, and Controversies
 Case 1 Traumatic Brain Injury : Review, Update, and Controversies Shirley I. Stiver MD, PhD 32 year old male s/p high speed MVA Difficult extrication Intubated at scene Case BP 75 systolic / palp GCS 3
Case 1 Traumatic Brain Injury : Review, Update, and Controversies Shirley I. Stiver MD, PhD 32 year old male s/p high speed MVA Difficult extrication Intubated at scene Case BP 75 systolic / palp GCS 3
Traumatic brain Injury- An open eye approach
 Traumatic brain Injury- An open eye approach Dr. Sunit Dr Sunit, Apollo children's hospital Blah blah Lots of head injury Lot of ill children Various methods of injury Various mechanisms of brain damage
Traumatic brain Injury- An open eye approach Dr. Sunit Dr Sunit, Apollo children's hospital Blah blah Lots of head injury Lot of ill children Various methods of injury Various mechanisms of brain damage
8th Annual NKY TBI Conference 3/28/2014
 Closed Head Injury: Headache to Herniation A N T H O N Y T. K R A M E R U N I V E R S I T Y O F C I N C I N N A T I B L U E A S H E M S T E C H N O L O G Y P R O G R A M Objectives Describe the pathological
Closed Head Injury: Headache to Herniation A N T H O N Y T. K R A M E R U N I V E R S I T Y O F C I N C I N N A T I B L U E A S H E M S T E C H N O L O G Y P R O G R A M Objectives Describe the pathological
INTRACRANIAL PRESSURE -!!
 INTRACRANIAL PRESSURE - Significance raised ICP main cause of death in severe head injury main cause of morbidity in moderate and mild head injury main target and prognostic indicator in the ITU setting
INTRACRANIAL PRESSURE - Significance raised ICP main cause of death in severe head injury main cause of morbidity in moderate and mild head injury main target and prognostic indicator in the ITU setting
Injuries to the head and spine
 Injuries to the head and spine Aaron J. Katz, AEMT-P, CIC www.es26medic.net 2013 Nervous System Two sub-systems Central Nervous System ( CNS ) Brain and spinal cord Peripheral Nervous System 12 cranial
Injuries to the head and spine Aaron J. Katz, AEMT-P, CIC www.es26medic.net 2013 Nervous System Two sub-systems Central Nervous System ( CNS ) Brain and spinal cord Peripheral Nervous System 12 cranial
Instructional Course #34. Review of Neuropharmacology in Pediatric Brain Injury. John Pelegano MD Jilda Vargus-Adams MD, MSc Micah Baird MD
 Instructional Course #34 Review of Neuropharmacology in Pediatric Brain Injury John Pelegano MD Jilda Vargus-Adams MD, MSc Micah Baird MD Outline of Course 1. Introduction John Pelegano MD 2. Neuropharmocologic
Instructional Course #34 Review of Neuropharmacology in Pediatric Brain Injury John Pelegano MD Jilda Vargus-Adams MD, MSc Micah Baird MD Outline of Course 1. Introduction John Pelegano MD 2. Neuropharmocologic
O ne million patients are treated annually in United
 859 ORIGIAL ARTICLE Can we abolish skull x rays for head injury? M J Reed, J G Browning, A G Wilkinson, T Beattie... See end of article for authors affiliations... Correspondence to: Matthew J Reed, Accident
859 ORIGIAL ARTICLE Can we abolish skull x rays for head injury? M J Reed, J G Browning, A G Wilkinson, T Beattie... See end of article for authors affiliations... Correspondence to: Matthew J Reed, Accident
Traumatic Brain Injury
 Traumatic Brain Injury Mark J. Harris M.D. Associate Professor University of Utah Salt Lake City USA Overview In US HI responsible for 33% trauma deaths. Closed HI 80% Missile / Penetrating HI 20% Glasgow
Traumatic Brain Injury Mark J. Harris M.D. Associate Professor University of Utah Salt Lake City USA Overview In US HI responsible for 33% trauma deaths. Closed HI 80% Missile / Penetrating HI 20% Glasgow
Chapter 31. Objectives. Objectives 01/09/2013. Head Trauma
 Chapter 31 Head Trauma Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1. Define key terms introduced
Chapter 31 Head Trauma Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1. Define key terms introduced
SUDANESE JOURNAL OF PAEDIATRICS 2014; Vol 14, Issue No. 1
 Education and Practice Case Report and Literature Review Managing traumatic brain injury in children: When do we need a computed tomography of the head? Mohammed A Kambal (1), Manal E Abou (2), Iman Al
Education and Practice Case Report and Literature Review Managing traumatic brain injury in children: When do we need a computed tomography of the head? Mohammed A Kambal (1), Manal E Abou (2), Iman Al
Conceptualization of Functional Outcomes Following TBI. Ryan Stork, MD
 Conceptualization of Functional Outcomes Following TBI Ryan Stork, MD Conceptualization of Functional Outcomes Following Traumatic Brain Injury Ryan Stork, MD Clinical Lecturer Brain Injury Medicine &
Conceptualization of Functional Outcomes Following TBI Ryan Stork, MD Conceptualization of Functional Outcomes Following Traumatic Brain Injury Ryan Stork, MD Clinical Lecturer Brain Injury Medicine &
Best-evidence Review of Acute Care for Moderate to Severe Traumatic Brain Injury
 Pragmatic Evidence-based Review Best-evidence Review of Acute Care for Moderate to Severe Traumatic Brain Injury Reviewer Mark Ayson MBChB DPH Date Report Completed August 2011 Important Note: It is not
Pragmatic Evidence-based Review Best-evidence Review of Acute Care for Moderate to Severe Traumatic Brain Injury Reviewer Mark Ayson MBChB DPH Date Report Completed August 2011 Important Note: It is not
Acute Neurosurgical Emergency Transfer [see also CATS SOP neurosurgical]
![Acute Neurosurgical Emergency Transfer [see also CATS SOP neurosurgical]](/thumbs/87/96512765.jpg "Acute Neurosurgical Emergency Transfer [see also CATS SOP neurosurgical]") Children s Acute Transport Service Clinical Guidelines Acute Neurosurgical Emergency Transfer [see also CATS SOP neurosurgical] Document Control Information Author D Lutman Author Position Head of Clinical
Children s Acute Transport Service Clinical Guidelines Acute Neurosurgical Emergency Transfer [see also CATS SOP neurosurgical] Document Control Information Author D Lutman Author Position Head of Clinical
UHSM ED Pathway ELDERLY FALL / COLLAPSE
 UHSM ED Pathway ELDERLY FALL / COLLAPSE Patient name / Pathway for patients who require assessment in ED after a fall or collapse Note: - It can be used if the patient has also sustained a minor head injury
UHSM ED Pathway ELDERLY FALL / COLLAPSE Patient name / Pathway for patients who require assessment in ED after a fall or collapse Note: - It can be used if the patient has also sustained a minor head injury
D is for Disability Altered Mental Status in Children
 D is for Disability Altered Mental Status in Children Joshua Ross, MD, FAAP Pediatric Emergency Medicine Emergency Care and Trauma Symposium June 22, 2015 Objectives Describe a basic approach to evaluating
D is for Disability Altered Mental Status in Children Joshua Ross, MD, FAAP Pediatric Emergency Medicine Emergency Care and Trauma Symposium June 22, 2015 Objectives Describe a basic approach to evaluating
Traumatic Brain Injuries
 Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
POST CONCUSSION SYMPTOM SCALE
 CONCUSSION INITIAL VISIT FORM Demographics Patient Name: Date of Consultation: DOB: Sex: Age: Who referred you to our clinic? Primary Care Physician: Pharmacy Name/Address: Your E-mail Address: Preferred
CONCUSSION INITIAL VISIT FORM Demographics Patient Name: Date of Consultation: DOB: Sex: Age: Who referred you to our clinic? Primary Care Physician: Pharmacy Name/Address: Your E-mail Address: Preferred
Standardize comprehensive care of the patient with severe traumatic brain injury
 Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
A bout million patients present to UK hospitals
 420 ORIGINAL ARTICLE Application of the Canadian CT head rules in managing minor head injuries in a UK emergency department: implications for the implementation of the NICE guidelines H Y Sultan, A Boyle,
420 ORIGINAL ARTICLE Application of the Canadian CT head rules in managing minor head injuries in a UK emergency department: implications for the implementation of the NICE guidelines H Y Sultan, A Boyle,
USASOC Neurocognitive Testing and Post Injury Evaluation and Treatment Clinical Practice Guideline (CPG)
") USASOC Neurocognitive Testing and Post Injury Evaluation and Treatment Clinical Practice Guideline (CPG) Note: The intent of this CPG is to serve as general guidance for medics and medical officers. It
USASOC Neurocognitive Testing and Post Injury Evaluation and Treatment Clinical Practice Guideline (CPG) Note: The intent of this CPG is to serve as general guidance for medics and medical officers. It
Hit head, on blood thinner-wife wants CT. Will Davies June 2014
 Hit head, on blood thinner-wife wants CT Will Davies June 2014 Selection of Adults with Head Injury for CT Scan Early management of head injury: summary of updated NICE guidance. Hodgkinson S, Pollit V,
Hit head, on blood thinner-wife wants CT Will Davies June 2014 Selection of Adults with Head Injury for CT Scan Early management of head injury: summary of updated NICE guidance. Hodgkinson S, Pollit V,
TRAUMATIC BRAIN INJURY
 Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences TRAUMATIC BRAIN INJURY GARY STOBBE, MD UNIVERSITY OF WASHINGTON GENERAL DISCLOSURES The University of Washington
Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences TRAUMATIC BRAIN INJURY GARY STOBBE, MD UNIVERSITY OF WASHINGTON GENERAL DISCLOSURES The University of Washington
Avoidable Imaging Learning Collaborative: 2008 Mild Traumatic Brain Injury Clinical Policy Success Story BWH Head and PE CTs with Clinical Decision
 Avoidable Imaging Learning Collaborative: 2008 Mild Traumatic Brain Injury Clinical Policy Success Story BWH Head and PE CTs with Clinical Decision Support Using the Canadian CT Head Rule to Reduce Unnecessary
Avoidable Imaging Learning Collaborative: 2008 Mild Traumatic Brain Injury Clinical Policy Success Story BWH Head and PE CTs with Clinical Decision Support Using the Canadian CT Head Rule to Reduce Unnecessary
Gilbert Public Schools (High School) Athletic Department Protocol and Procedures for Management of Sports-Related Concussion
 Athletic Department Protocol and Procedures for Management of Sports-Related Concussion") Gilbert Public Schools (High School) Athletic Department Protocol and Procedures for Management of Sports-Related Concussion Medical management of sports-related concussion is evolving. In recent years,
Gilbert Public Schools (High School) Athletic Department Protocol and Procedures for Management of Sports-Related Concussion Medical management of sports-related concussion is evolving. In recent years,
Traumatic Brain Injury TBI Presented by Bill Masten
 1 2 Cerebrum two hemispheres and four lobes. Cerebellum (little brain) coordinates the back and forth ballet of motion. It judges the timing of every movement precisely. Brainstem coordinates the bodies
1 2 Cerebrum two hemispheres and four lobes. Cerebellum (little brain) coordinates the back and forth ballet of motion. It judges the timing of every movement precisely. Brainstem coordinates the bodies
Author Manuscript. Received Date : 27-Oct Revised Date : 09-Jan-2017 Accepted Date : 31-Jan-2017
 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 Received Date : 27-Oct-2016 Revised Date : 09-Jan-2017 Accepted Date : 31-Jan-2017 Article type ABSTRACT : Original Contribution
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 Received Date : 27-Oct-2016 Revised Date : 09-Jan-2017 Accepted Date : 31-Jan-2017 Article type ABSTRACT : Original Contribution
Paediatric Neurosurgical Emergencies. Kate Parkins Consultant Paediatric Intensivist Alder Hey
 Paediatric Neurosurgical Emergencies Kate Parkins Consultant Paediatric Intensivist Alder Hey Level of consciousness AVPU GCS D Neurological Assessment Pupillary reaction to light Limb movements History
Paediatric Neurosurgical Emergencies Kate Parkins Consultant Paediatric Intensivist Alder Hey Level of consciousness AVPU GCS D Neurological Assessment Pupillary reaction to light Limb movements History
Signs and Symptoms of Concussion
 Signs and Symptoms of Concussion These signs and symptoms following a witnessed or suspected blow to the head or body are indicative of probable concussion. Signs (observed by others) Appears dazed or
Signs and Symptoms of Concussion These signs and symptoms following a witnessed or suspected blow to the head or body are indicative of probable concussion. Signs (observed by others) Appears dazed or
Caring for Children with Concussion
 Caring for Children with Concussion Peter Ferraano, MD Associate Professor of Pediatrics Division of Pediatric Critical Care Medicine University of Wisconsin School of Medicine and Public Health Director,
Caring for Children with Concussion Peter Ferraano, MD Associate Professor of Pediatrics Division of Pediatric Critical Care Medicine University of Wisconsin School of Medicine and Public Health Director,
Introduction to Emergency Medical Care 1
 Introduction to Emergency Medical Care 1 OBJECTIVES 31.1 Define key terms introduced in this chapter. Slides 13 15, 17, 19, 28 31.2 Describe the components and function of the nervous system and the anatomy
Introduction to Emergency Medical Care 1 OBJECTIVES 31.1 Define key terms introduced in this chapter. Slides 13 15, 17, 19, 28 31.2 Describe the components and function of the nervous system and the anatomy
Children and Infants - Acute Management of Head Injury
 Policy Directive Ministry of Health, NSW 73 Miller Street North Sydney NSW 2060 Locked Mail Bag 961 North Sydney NSW 2059 Telephone (02) 9391 9000 Fax (02) 9391 9101 http://www.health.nsw.gov.au/policies/
Policy Directive Ministry of Health, NSW 73 Miller Street North Sydney NSW 2060 Locked Mail Bag 961 North Sydney NSW 2059 Telephone (02) 9391 9000 Fax (02) 9391 9101 http://www.health.nsw.gov.au/policies/
The Child with Alterations in Cerebral Function
 The Child with Alterations in Cerebral Function Neurologic Assessment VS HR, BP, Respirations, Temperature LOC Orientation Pediatric Glasgow Coma Scale Eyes Pupillary response and movement, extraoccular
The Child with Alterations in Cerebral Function Neurologic Assessment VS HR, BP, Respirations, Temperature LOC Orientation Pediatric Glasgow Coma Scale Eyes Pupillary response and movement, extraoccular
PAEDIATRIC ACUTE CARE GUIDELINE. Resuscitation Coma
 Princess Margaret Hospital for Children PAEDIATRIC ACUTE CARE GUIDELINE Resuscitation Coma Scope (Staff): Scope (Area): All Emergency Department Clinicians Emergency Department This document should be
Princess Margaret Hospital for Children PAEDIATRIC ACUTE CARE GUIDELINE Resuscitation Coma Scope (Staff): Scope (Area): All Emergency Department Clinicians Emergency Department This document should be
A Healthy Brain. An Injured Brain
 A Healthy Brain Before we can understand what happens when a brain is injured, we must realize what a healthy brain is made of and what it does. The brain is enclosed inside the skull. The skull acts as
A Healthy Brain Before we can understand what happens when a brain is injured, we must realize what a healthy brain is made of and what it does. The brain is enclosed inside the skull. The skull acts as
INCREASED INTRACRANIAL PRESSURE
 INCREASED INTRACRANIAL PRESSURE Sheba Medical Center, Acute Medicine Department Irene Frantzis P-Year student SGUL 2013 Normal Values Normal intracranial volume: 1700 ml Volume of brain: 1200-1400 ml CSF:
INCREASED INTRACRANIAL PRESSURE Sheba Medical Center, Acute Medicine Department Irene Frantzis P-Year student SGUL 2013 Normal Values Normal intracranial volume: 1700 ml Volume of brain: 1200-1400 ml CSF:
Objectives. Incidence TBI: Leading cause of death & disability due to trauma. 9th Annual NKY TBI Conference 3/27/2015
 Mild Traumatic Brain Injury & Symptom Assessment in Children Becky Cook, DNP, APRN Trauma Nurse Practitioner Objectives Discuss the incidence and mechanisms of injury of mild traumatic brain injury (mtbi)
Mild Traumatic Brain Injury & Symptom Assessment in Children Becky Cook, DNP, APRN Trauma Nurse Practitioner Objectives Discuss the incidence and mechanisms of injury of mild traumatic brain injury (mtbi)
Mini Research Paper: Traumatic Brain Injury. Allison M McGee. Salt Lake Community College
 Running Head: Mini Research Paper: Traumatic Brain Injury Mini Research Paper: Traumatic Brain Injury Allison M McGee Salt Lake Community College Abstract A Traumatic Brain Injury (also known as a TBI)
Running Head: Mini Research Paper: Traumatic Brain Injury Mini Research Paper: Traumatic Brain Injury Allison M McGee Salt Lake Community College Abstract A Traumatic Brain Injury (also known as a TBI)
Pediatric Advanced Life Support
 Pediatric Advanced Life Support Pediatric Chain of Survival Berg M D et al. Circulation 2010;122:S862-S875 Prevention Early cardiopulmonary resuscitation (CPR) Prompt access to the emergency response system
Pediatric Advanced Life Support Pediatric Chain of Survival Berg M D et al. Circulation 2010;122:S862-S875 Prevention Early cardiopulmonary resuscitation (CPR) Prompt access to the emergency response system
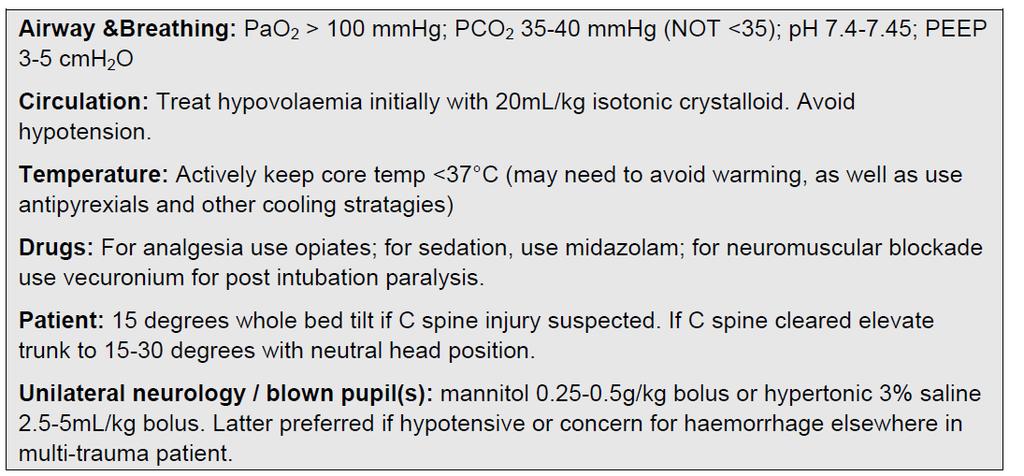
10. Severe traumatic brain injury also see flow chart Appendix 5
 10. Severe traumatic brain injury also see flow chart Appendix 5 Introduction Severe traumatic brain injury (TBI) is the leading cause of death in children in the UK, accounting for 15% of deaths in 1-15
10. Severe traumatic brain injury also see flow chart Appendix 5 Introduction Severe traumatic brain injury (TBI) is the leading cause of death in children in the UK, accounting for 15% of deaths in 1-15
TRAUMATIC BRAIN INJURY. Moderate and Severe Brain Injury
 TRAUMATIC BRAIN INJURY Moderate and Severe Brain Injury Disclosures Funded research: 1. NIH: RO1 Physiology of concussion 2016-2021, Co-PI, $2,000,000 2. American Medical Society of Sports Medicine: RCT
TRAUMATIC BRAIN INJURY Moderate and Severe Brain Injury Disclosures Funded research: 1. NIH: RO1 Physiology of concussion 2016-2021, Co-PI, $2,000,000 2. American Medical Society of Sports Medicine: RCT
Head Injury: Classification Most Severe to Least Severe
 Head Injury: Classification Most Severe to Least Severe Douglas I. Katz, MD Professor, Dept. Neurology, Boston University School of Medicine, Boston MA Medical Director Brain Injury Program, HealthSouth
Head Injury: Classification Most Severe to Least Severe Douglas I. Katz, MD Professor, Dept. Neurology, Boston University School of Medicine, Boston MA Medical Director Brain Injury Program, HealthSouth
Definition and causes:
 Up2Date September 2014 Concussion by Wendy Quick Definition and causes: A concussion is not just a "bump on the head." It is a traumatic brain injury that needs proper treatment whether it is mild or severe.
Up2Date September 2014 Concussion by Wendy Quick Definition and causes: A concussion is not just a "bump on the head." It is a traumatic brain injury that needs proper treatment whether it is mild or severe.
Daniel A. Beals MD, FACS, FAAP Pediatric Surgery and Urology Community Medical Center Associate Professor of Surgery and Pediatrics University of
 Daniel A. Beals MD, FACS, FAAP Pediatric Surgery and Urology Community Medical Center Associate Professor of Surgery and Pediatrics University of Washington Seattle Children s Hospital Objectives Define
Daniel A. Beals MD, FACS, FAAP Pediatric Surgery and Urology Community Medical Center Associate Professor of Surgery and Pediatrics University of Washington Seattle Children s Hospital Objectives Define
Pediatric Trauma Initial Evaluation and management
 Pediatric Trauma Initial Evaluation and management Head Injury Closed head injury Penetrating head injury Closed Head Injury without Fractures Head injury is the most common cause of death and disability
Pediatric Trauma Initial Evaluation and management Head Injury Closed head injury Penetrating head injury Closed Head Injury without Fractures Head injury is the most common cause of death and disability
Surgical Care at the District Hospital. EMERGENCY & ESSENTIAL SURGICAL CARE
 Surgical Care at the District Hospital 1 17 Orthopedic Techniques Key Points 2 17.1 Traction Use an appropriate method of traction to treat fractures of the extremities and cervical spine Apply extremity
Surgical Care at the District Hospital 1 17 Orthopedic Techniques Key Points 2 17.1 Traction Use an appropriate method of traction to treat fractures of the extremities and cervical spine Apply extremity
Sign up to receive ATOTW weekly
 MANAGEMENT OF PAEDIATRIC TRAUMATIC BRAIN INJURY ANAESTHESIA TUTORIAL OF THE WEEK 127 30 TH MARCH 2009 Kavitha Raghavan, King s College Hospital, London Richard Waddington, Kingston Hospital, Surrey Correspondence
MANAGEMENT OF PAEDIATRIC TRAUMATIC BRAIN INJURY ANAESTHESIA TUTORIAL OF THE WEEK 127 30 TH MARCH 2009 Kavitha Raghavan, King s College Hospital, London Richard Waddington, Kingston Hospital, Surrey Correspondence
of Trauma Assembly 27 th Page 1
 Eastern Association for the Surgery of Trauma 27 th Annual Scientific Assembly Sunrise Session 08 To Scan or Not To Scan Thatt is the Question January 16, 2014 Waldorf Astoria Naples Naples, Floridaa Page
Eastern Association for the Surgery of Trauma 27 th Annual Scientific Assembly Sunrise Session 08 To Scan or Not To Scan Thatt is the Question January 16, 2014 Waldorf Astoria Naples Naples, Floridaa Page
 PARENT & ATHLETE CONCUSSION INFORMATION SHEET WHAT IS A CONCUSSION? A concussion is a type of traumatic brain injury that changes the way the brain normally works. A concussion is caused by a bump, blow,
PARENT & ATHLETE CONCUSSION INFORMATION SHEET WHAT IS A CONCUSSION? A concussion is a type of traumatic brain injury that changes the way the brain normally works. A concussion is caused by a bump, blow,
Derivation of the children s head injury algorithm for the prediction of important clinical events decision rule for head injury in children
 885 ORIGINAL ARTICLE Derivation of the children s head injury algorithm for the prediction of important clinical events decision rule for head injury in children J Dunning, J Patrick Daly, J-P Lomas, F
885 ORIGINAL ARTICLE Derivation of the children s head injury algorithm for the prediction of important clinical events decision rule for head injury in children J Dunning, J Patrick Daly, J-P Lomas, F
Mild TBI (Concussion) Not Just Less Severe But Different
 Not Just Less Severe But Different") Mild TBI (Concussion) Not Just Less Severe But Different Disclosures Funded research: 1. NIH: RO1 Physiology of concussion 2016-2021, Co-PI, $2,000,000 2. American Medical Society of Sports Medicine: RCT
Mild TBI (Concussion) Not Just Less Severe But Different Disclosures Funded research: 1. NIH: RO1 Physiology of concussion 2016-2021, Co-PI, $2,000,000 2. American Medical Society of Sports Medicine: RCT
National guidelines CSSL / Head injury. Guidelines on the management of a patient with a head injury
 Guidelines on the management of a patient with a head injury College of Surgeons of Sri Lanka 2007 1 Authors Dr. Prasanna Gunasena Consultant Neurosurgeon Teaching Hospital Anuradhapura (Group Coordinator)
Guidelines on the management of a patient with a head injury College of Surgeons of Sri Lanka 2007 1 Authors Dr. Prasanna Gunasena Consultant Neurosurgeon Teaching Hospital Anuradhapura (Group Coordinator)
Traumatic Brain Injury
 General Information Traumatic Brain Injury What you need to know Complicated condition with high variability in etiology, severity, distribution of injury, and pattern of functional impairment (Klyce,
General Information Traumatic Brain Injury What you need to know Complicated condition with high variability in etiology, severity, distribution of injury, and pattern of functional impairment (Klyce,
Traumatic Brain Injury (1.2.3) Management of severe TBI ( ) Learning Objectives
 Management of severe TBI ( ) Learning Objectives") Traumatic Brain Injury (1.2.3) 1.2.3.1 Management of severe TBI 1.2.3.2 Management of concussions 1.2.3.3 Sideline management for team medics/physicians 1.4.2.3.10 Controlled hyperventilation for management
Traumatic Brain Injury (1.2.3) 1.2.3.1 Management of severe TBI 1.2.3.2 Management of concussions 1.2.3.3 Sideline management for team medics/physicians 1.4.2.3.10 Controlled hyperventilation for management
Shenandoah Co. Fire & Rescue. Injuries to. and Spine. December EMS Training Bill Streett Training Section Chief
 Shenandoah Co. Fire & Rescue Injuries to the Head and Spine December EMS Training Bill Streett Training Section Chief C.E. Card Information BLS Providers 2 Cards / Provider Category 1 Course # Blank Topic#
Shenandoah Co. Fire & Rescue Injuries to the Head and Spine December EMS Training Bill Streett Training Section Chief C.E. Card Information BLS Providers 2 Cards / Provider Category 1 Course # Blank Topic#
Pediatric Head Injury:
 Pediatric Head Injury: Part I Basic Principles Jogi V. Pattisapu, MD FAAP FACS Emeritus Medical Director Arnold Palmer Medical Center College of Medicine University of Central Florida Orlando FL USA JogiP@mail.UCF.edu
Pediatric Head Injury: Part I Basic Principles Jogi V. Pattisapu, MD FAAP FACS Emeritus Medical Director Arnold Palmer Medical Center College of Medicine University of Central Florida Orlando FL USA JogiP@mail.UCF.edu
Coastal Carolina University Athletic Training Department Policy and Procedure Manual Concussion Management Revised/Reviewed 6/2012
 Coastal Carolina University Athletic Training Department Policy and Procedure Manual Concussion Management Revised/Reviewed 6/2012 INTRODUCTION: Concussion classification, management, and protocols have
Coastal Carolina University Athletic Training Department Policy and Procedure Manual Concussion Management Revised/Reviewed 6/2012 INTRODUCTION: Concussion classification, management, and protocols have
Chapter 57: Nursing Management: Acute Intracranial Problems
 Chapter 57: Nursing Management: Acute Intracranial Problems NORMAL INTRACRANIAL PRESSURE Intracranial pressure (ICP) is the hydrostatic force measured in the brain CSF compartment. Normal ICP is the total
Chapter 57: Nursing Management: Acute Intracranial Problems NORMAL INTRACRANIAL PRESSURE Intracranial pressure (ICP) is the hydrostatic force measured in the brain CSF compartment. Normal ICP is the total
Time Equals Neurons - Spinal Cord Injury Management in the first 4 Hours
 Time Equals Neurons - Spinal Cord Injury Management in the first 4 Hours William D. Whetstone M.D. Clinical Professor UCSF Department of Emergency Medicine SFGH ED Center for Neuro-Critical Emergencies
Time Equals Neurons - Spinal Cord Injury Management in the first 4 Hours William D. Whetstone M.D. Clinical Professor UCSF Department of Emergency Medicine SFGH ED Center for Neuro-Critical Emergencies
Head & Brain Trauma. Presented By: Steven Jones, NREMT-P
 Head & Brain Trauma Presented By: Steven Jones, NREMT-P Head & Brain Trauma ~ 4 million head injuries in US per year ~ 450,000 require hospitalization Most are minor injuries Major head injury most common
Head & Brain Trauma Presented By: Steven Jones, NREMT-P Head & Brain Trauma ~ 4 million head injuries in US per year ~ 450,000 require hospitalization Most are minor injuries Major head injury most common
Traumatic Brain Injury Pathway, GCS 15 Closed head injury
 Traumatic Brain Injury Pathway, GCS 15 Closed head injury Plus Any One of the Following Mild TBI 2010 Consensus Definition of TBI from CDC, NINDS, NIDDR, VA, DVBIC, DCoE Plus Any One of the Following New
Traumatic Brain Injury Pathway, GCS 15 Closed head injury Plus Any One of the Following Mild TBI 2010 Consensus Definition of TBI from CDC, NINDS, NIDDR, VA, DVBIC, DCoE Plus Any One of the Following New
Restore adequate respiratory and circulatory conditions. Reduce pain
 Pre-hospital management of the trauma patient is best performed by an integrated team focused on minimizing the time from injury to definitive care at an appropriate trauma center. Dispatchers, first responders,
Pre-hospital management of the trauma patient is best performed by an integrated team focused on minimizing the time from injury to definitive care at an appropriate trauma center. Dispatchers, first responders,
Pediatric head trauma: the evidence regarding indications for emergent neuroimaging
 DOI 10.1007/s00247-008-0996-5 ALARA: BUILDING BRIDGES BETWEEN RADIOLOGY AND EMERGENCY MEDICINE Pediatric head trauma: the evidence regarding indications for emergent neuroimaging Nathan Kuppermann Received:
DOI 10.1007/s00247-008-0996-5 ALARA: BUILDING BRIDGES BETWEEN RADIOLOGY AND EMERGENCY MEDICINE Pediatric head trauma: the evidence regarding indications for emergent neuroimaging Nathan Kuppermann Received:
Correlation of D-Dimer level with outcome in traumatic brain injury
 2014; 17 (1) Original Article Correlation of D-Dimer level with outcome in traumatic brain injury Pradip Prasad Subedi 1, Sushil Krishna Shilpakar 2 Email: Abstract Introduction immense. The major determinant
2014; 17 (1) Original Article Correlation of D-Dimer level with outcome in traumatic brain injury Pradip Prasad Subedi 1, Sushil Krishna Shilpakar 2 Email: Abstract Introduction immense. The major determinant
Evaluation and Stabilization of the Athlete with Possible Spine Injury
 Evaluation and Stabilization of the Athlete with Possible Spine Injury Jeffrey H. Bohmer, MD, FACEP Emergency Physician Northwestern Medicine Central DuPage Hospital June 12, 2015 Introduction Goals: 1.
Evaluation and Stabilization of the Athlete with Possible Spine Injury Jeffrey H. Bohmer, MD, FACEP Emergency Physician Northwestern Medicine Central DuPage Hospital June 12, 2015 Introduction Goals: 1.
Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University
 Dr Mubarak Abdelrahman Assistant Professor Jazan University") Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University SHOCK Definition: Shock is a syndrome = inability to provide sufficient oxygenated blood to tissues. Oxygen
Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University SHOCK Definition: Shock is a syndrome = inability to provide sufficient oxygenated blood to tissues. Oxygen
Coliseum SC Concussion Protocol Signs and Symptoms
 Coliseum SC Concussion Protocol Signs and Symptoms Athletes who experience one or more of the signs or symptoms listed below after a bump, blow, or jolt to the head or body may have a concussion. SIGNS
Coliseum SC Concussion Protocol Signs and Symptoms Athletes who experience one or more of the signs or symptoms listed below after a bump, blow, or jolt to the head or body may have a concussion. SIGNS
Sports Related Concussion. Joshua T. Williams, PT, DPT, OCS, SCS, CSCS
 Sports Related Concussion Joshua T. Williams, PT, DPT, OCS, SCS, CSCS Concussion & Traumatic Brain Injury Glasgow Coma Scale Minimal Mild Mod Severe? Sports concussion Severe GCS 8 Moderate GCS 9-12 Mild
Sports Related Concussion Joshua T. Williams, PT, DPT, OCS, SCS, CSCS Concussion & Traumatic Brain Injury Glasgow Coma Scale Minimal Mild Mod Severe? Sports concussion Severe GCS 8 Moderate GCS 9-12 Mild