Avoidable Imaging Learning Collaborative: 2008 Mild Traumatic Brain Injury Clinical Policy Success Story BWH Head and PE CTs with Clinical Decision
|
|
|
- Laura Hill
- 5 years ago
- Views:
Transcription

1 Avoidable Imaging Learning Collaborative: 2008 Mild Traumatic Brain Injury Clinical Policy Success Story BWH Head and PE CTs with Clinical Decision Support Using the Canadian CT Head Rule to Reduce Unnecessary Imaging



2 Presenters Michael D. Brown, MD, MSc Ali S. Raja, MD, MBA, MPH Ian Stiell, MD, MSc, FRCPC


3 Michael D Brown, MD, MSc Chair, ACEP Clinical Policies Committee
4 Provide historical context Developed by ACEP in collaboration with CDC Search and grading conducted 10 years ago Critical Question 1 most relevant to avoidable imaging Who needs head CT? Critical Q 2 & 3 address roles of MRI and biomarkers Lack of evidence for Level A or Level B recommendations Critical Q 4 addresses disposition following negative CT Yes, may be discharged.except inadequate data for bleeding disorders, anticoagulation, antiplatelets, previous neurosurgery
5 Guideline intended for adults with blunt head trauma Present to ED within 24 hours of injury GCS 14 or years or older Exclusions Penetrating trauma Multisystem trauma Age < 16 GCS < 14 Primary outcome: acute traumatic intracranial lesion on CT
6 Head CT indicated with LOC or amnesia only if one or more of the following is present: Headache Vomiting Age > 60 years Drug or alcohol intoxication Deficits in short-term memory Trauma above the clavicle Post-traumatic seizure GCS < 15 Focal neurologic deficit Coagulopathy
7 Head CT should be considered with no LOC or amnesia if any of the following: Focal neurologic deficit Vomiting Severe headache Age > 65 years Signs of basilar skull fracture GCS < 15 Coagulopathy Dangerous mechanism of injury*
 Sp = 3% (1 to 5%) LR+ = 1; LR- = 0.3 Canadian Rule adapted Se = 85% (81 to 89%) Sp = 40% (37 to 42%) LR+ = 1.4 LR- = 0.4 JAMA.")
8 GCS or 15 with a risk factor N = 3,181 in Netherlands Primary outcome: any traumatic finding on CT New Orleans Criteria adapted Se = 99% (98 to 100%) Sp = 3% (1 to 5%) LR+ = 1; LR- = 0.3 Canadian Rule adapted Se = 85% (81 to 89%) Sp = 40% (37 to 42%) LR+ = 1.4 LR- = 0.4 JAMA. 2005;294(12)
 Secondary outcome: clinically important injury New Orleans")
 LR+ = 1.7 LR - = 0.")
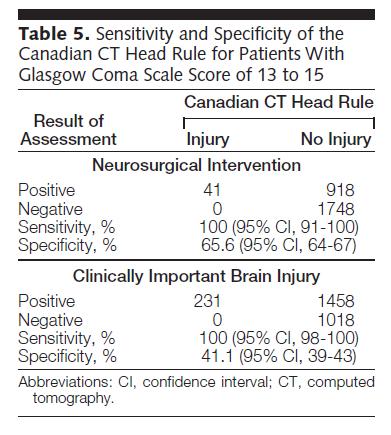
9 Enrolled 2,707 with GCS Subgroup analysis with GCS = 15 (n = 1822) Secondary outcome: clinically important injury New Orleans Se = 100%; Sp = 13% (11 to 14%) LR+ = 1 LR - = 0.1 Canadian Rule Se = 100%; Sp = 51% (48 to 53%) LR+ = 1.7 LR - = 0.3 JAMA. 2005;294(12)
10 Success Story BWH Head and PE CTs with Clinical Decision Support Ali S. Raja, MD, MBA, MPH Vice Chairman Department of Emergency Medicine, Massachusetts General Hospital Senior Faculty Brigham and Women s Hospital Center for Evidence Based Imaging Associate Professor of Emergency Medicine and Radiology Harvard Medical School Executive Director, Harvard Medical School Library of
11 Financial Conflicts of Interest: None
12 Head CT ordering rates: BWH ED in % 60% 2016 implications: Cost? Radiation exposure? 50% 40% 30% 20% 10% 0% Crude Head CT Ordering Rates Adjusted Head CT Ordering Rates 3-fold inter-physician variation (21.2%-60.1%) remained after multivariable adjustment Prevedello L, et al. Am J Med Apr;125(4):
13
14 Clinical Decision Support for Adaptive Data Collection
15
16 Lesson One One Specialty Cannot Implement Imaging CDS Alone
17 The CT-PE Problem Life-threatening diagnosis + Low-threshold for missed diagnosis + Readily available definitive diagnostic test + No physician consequences for over-testing = Rapidly increasing PE-protocol CT ordering
18 Incidence and mortality of pulmonary embolism in the United States, Wiener,. Schwartz, Woloshin. Arch Intern Med May 9; 171(9):
19 Solutions? Emergency Medicine Interventions: - Failed - Not integrated into imaging requests - Education only, Not point-of-care Radiology Interventions: - Failed - Presented novel information at the point-of care, halting flow - No internal champions
20
21
22
23

24 Inpatient CTPA USE Dunne R, et al. Radiology. February No significant increase or decrease in CTPA use trends, p=0.52 Month per 1000 admissions Month per 1000 admissions Relative reduction 12.8% p=0.008
25 Impact of effective CDS on Choosing Wisely Initiatives CT for suspected pulmonary embolism: (ACEP) ED use 20%; yield up 69% over 2 years Inpatient use 13% over one month, then stable MRI for low back pain: (ACP) Outpatients: MRI use 30% on day of PCP visit; 12.3% within 30 days of index PCP visit CT for minor traumatic brain injury (ACEP) 13.4% in use of CT in ED All above now published or in press in peer reviewed journals
26 Lesson Two CDS Must be Based on High Quality Evidence

27
28 CMS Medicare Imaging Demonstration (MID: 11/2011-9/2013) Designed as an alternate to preauthorization, MID assessed impact of CDS based on a broad set of professional society guidelines Evidence was limited to ONLY these MID guidelines BWH used same syringe as used in prior CDS
29 MID: BWH Convenership 83,064 orders in the intervention period Alert/Behavior Control Intervention P value Actionable alerts 7.9% 5.7% <0.001 Alerts ignored 98.9% (n=82,188) N/A Exams modified 1.07% (n=903) N/A Exams cancelled 0.03% (n=23) N/A
30 Protecting Access to Medicare Act (2014) Ordering professionals advanced imaging services must be exposed to evidence-based Appropriate Use Criteria (AUC) via CDS Consequence for failure imaging provider will not be paid
31 PAMA rules: Key provisions Specified AUC will be developed and published by qualified provider-led entities qple must have rigorous processes to assess and grade the evidence using a multidisciplinary team, and then publish evidence-based criteria online Implementation date initially January 2017, now delayed
32 Lesson Two CDS Must be Based on High Quality Evidence

33
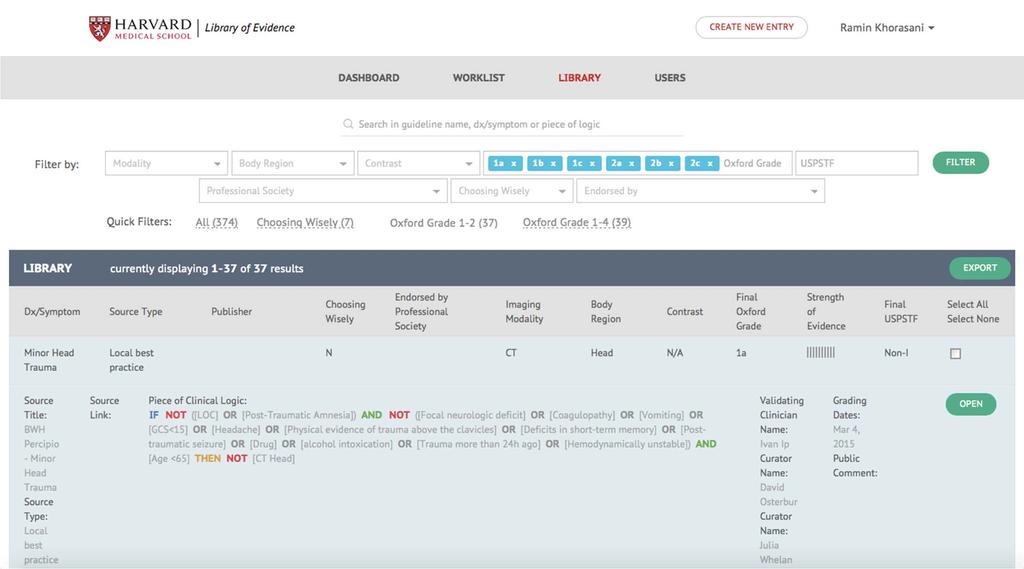
34 Harvard Medical School Library of Evidence A national public domain repository of objectively scored, health IT consumable evidence from any source designed to Accelerate adoption of CDS for imaging Highlight high priority clinical conditions where strong evidence is lacking to stimulate discovery
35
36
37 Lesson Three CDS is only the First Step
38
39
40
41
42
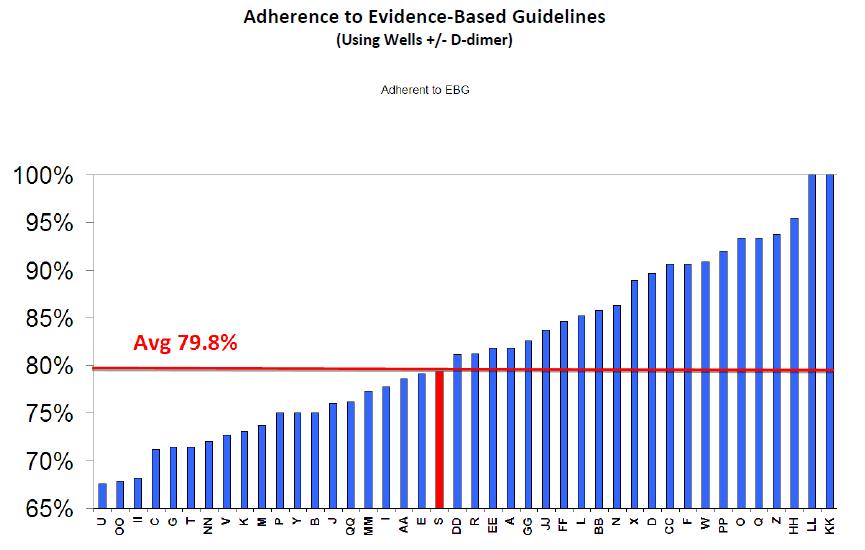
43 Impact of CDS-enabled Interventions on Documented Adherence to Evidence Imaging/ Condition Reference Type Control Intervention P value Head CT/ ED minor trauma (ACEP) Chest CT/ED PE (NQF) Gupta JAMIA 2014 Raja Acad Rad 2014 Education only 49% 76% < Education only 57% 76% <0.01 Chest CT/ED PE (NQF) Raja AJR 2015 Add MD feedback 78% 85% <0.05 LS MRI/ ambulatory (ACP) Ip American JMed 2013 Add peer to peer, MD feedback 78% 96% <0.005
44 Lessons Learned 1 One Specialty Cannot Implement Imaging CDS Alone 2 CDS Must be Based on High Quality Evidence 3 CDS is only the First Step

45 Success Story BWH Head and PE CTs with Clinical Decision Support Ali S. Raja, MD, MBA, MPH Vice Chairman Department of Emergency Medicine, Massachusetts General Hospital Senior Faculty Brigham and Women s Hospital Center for Evidence Based Imaging Associate Professor of Emergency Medicine and Radiology Harvard Medical School Executive Director, Harvard Medical School Library of

46 Using the Canadian CT Head Rule to Reduce Unnecessary Imaging

47 Ian Stiell MD MSc FRCPC Professor, Dept of Emergency Medicine, U of Ottawa Distinguished Professor and Clinical Research Chair, U of Ottawa Senior Scientist, Ottawa Hospital Research Institute Disclosures: none
48 Canadian CT Head Rule: Learning Objectives To understand the evidence behind the Canadian CT Head Rule To review how to use the CCHR on your patients


49 Minor Head Injury: The Clinical Problem 6,000,000 head injury cases / year in Canadian and U.S. EDs Classic minor head injury: Transient neurological impairment GCS <1% risk of epidural hematoma and need for intervention Yield of CT very low in North America
50 Minor Head Injury: Case Study #1 45 y.o. male knocked out x 1 minute with baseball bat headache, no amnesia, no vomiting Pmh = 0; Meds = 0 Alert, contusion forehead, GCS=15, neuro = N What do you do? CT head Observe Discharge with no imaging
51 Minor Head Injury: Case Study #2 75 y.o. female walked into door, no loss of consciousness Laceration eyebrow, no amnesia, no vomiting Pmh = HTN; Meds = diuretic Alert, 2 cm laceration eyebrow, GCS=15, neuro = N What do you do? CT head Observe Discharge with no imaging
 JAMA 2005 Implementation (N=4,531) CMAJ")
52 Canadian CT Head Rule Variation (N=1,699) Annals EM 1997 Derivation (N=3,121) The Lancet 2001 Validation (N=2,707) JAMA 2005 Implementation (N=4,531) CMAJ 2010

53 4,531 patients in 12 EDs Found barriers to KT JAMA 2005
54 JAMA 2005
55 JAMA 2005

56 4,531 patients in 12 EDs No missed injuries Barriers to KT

57 Conclusions: Canadian CT Head Rule Accurate and reliable for CT imaging in minor head injury patients Could safely limit use of imaging Also ensures that patients at risk receive CT in a timely manner


58 How to Use the Canadian CT Head Rule
59 The Canadian CT Head Rule Should Only be Used for these Patients: Minor head injury with one of: Witnessed loss of consciousness Amnesia for the injury Confusion after the injury GCS on ED arrival Injury < 24 hours
60 The Canadian CT Head Rule Should Not be Used for these Patients: < 16 years of age Minimal head injury without: Loss of consciousness Amnesia Confusion GCS < 13 Major trauma (head, chest, abdomen, # femur, hypotension) Oral anticoagulants
61 High Risk (for Neurological Intervention) 1. GCS score < 15 at 2 hrs after injury 2. Suspected open skull fracture 3. Any sign of basal skull fracture 4. Vomiting 2 episodes 5. Age 65 years Medium Risk (for Brain Injury on CT) 6. Amnesia before impact 30 min 7. Dangerous mechanism (pedestrian, occupant ejected, fall from elevation)

62 Dangerous Mechanism of Injury 1. Pedestrian struck by a vehicle 2. Occupant ejected from motor vehicle 3. Fall from elevation 3 feet or 5 stairs


63 Minor Head Injury: Case Study #1 45 y.o. male knocked out x 1 minute with baseball bat headache, no amnesia, no vomiting Pmh = 0; Meds = 0 Alert, contusion forehead, GCS=15, neuro = N What do you do? Discharge with no imaging

64 Minor Head Injury: Case Study #2 75 y.o. female walked into door, no loss of consciousness Laceration eyebrow, no amnesia, no vomiting Pmh = HTN; Meds = diuretic Alert, 2 cm laceration eyebrow, GCS=15, neuro = N What do you do? Discharge with no imaging
65 The Canadian CT Head Rule: Tips and Precautions The Rule can be safely used for patients who have been drinking if they are cooperative Patients without a history of loss of consciousness, amnesia, or confusion rarely need a CT scan Patients >65 do not need a scan just based on their age if they do not have this history

66 The Canadian CT Head Rule: Learning Aids

67 The Canadian CT Head Rule: Learning Aids
 6. Amnesia before impact 30 min 7.")
68 High Risk (for Neurological Intervention) 1. GCS score < 15 at 2 hrs after injury 2. Suspected open skull fracture 3. Any sign of basal skull fracture 4. Vomiting 2 episodes 5. Age 65 years Medium Risk (for Brain Injury on CT) 6. Amnesia before impact 30 min 7. Dangerous mechanism (pedestrian, occupant ejected, fall from elevation)
69 Emergency Medicine Research: Good Patient Care Requires Good Evidence
70

71
72 Avoidable Imaging Webinar: Thursday, September 15 1:00pm 2:00pmEST ACEP E QUAL Network Resources and More Information: Contact Nalani Tarrant (Project Manager): ntarrant@acep.org
Clinical Decision Support Technologies for Oncologic Imaging
 Clinical Decision Support Technologies for Oncologic Imaging Ramin Khorasani, MD, MPH Professor of Radiology Harvard Medical School Distinguished Chair, Medical Informatics Vice Chair, Department of Radiology
Clinical Decision Support Technologies for Oncologic Imaging Ramin Khorasani, MD, MPH Professor of Radiology Harvard Medical School Distinguished Chair, Medical Informatics Vice Chair, Department of Radiology
2016 PQRS OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS, REGISTRY
 Measure #416: Emergency Medicine: Emergency Department Utilization of CT for Minor Blunt Head Trauma for Patients Aged 2 through 17 Years - National Quality Strategy Domain: Efficiency and Cost Reduction
Measure #416: Emergency Medicine: Emergency Department Utilization of CT for Minor Blunt Head Trauma for Patients Aged 2 through 17 Years - National Quality Strategy Domain: Efficiency and Cost Reduction
2017 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY. MEASURE TYPE: Efficiency
 Measure #416: Emergency Medicine: Emergency Department Utilization of CT for Minor Blunt Head Trauma for Patients Aged 2 Through 17 Years - National Quality Strategy Domain: Efficiency and Cost Reduction
Measure #416: Emergency Medicine: Emergency Department Utilization of CT for Minor Blunt Head Trauma for Patients Aged 2 Through 17 Years - National Quality Strategy Domain: Efficiency and Cost Reduction
Head injury in children
 Head injury in children Michael Kim, MD Department of Emergency Medicine University of Wisconsin- Madison #1 cause of death and disability Bimodal distribution 62,000 hospitalization 564,000 ED visits
Head injury in children Michael Kim, MD Department of Emergency Medicine University of Wisconsin- Madison #1 cause of death and disability Bimodal distribution 62,000 hospitalization 564,000 ED visits
emeasure Title Emergency Medicine: Emergency Department Utilization of CT for Minor Blunt Head Trauma for Patients Aged 18 Years and Older
 emeasure Title Emergency Medicine: Emergency Department Utilization of CT for Minor Blunt Head Trauma for Patients Aged 18 Years and Older emeasure Identifier (Measure Authoring Tool) NQF Number Measurement
emeasure Title Emergency Medicine: Emergency Department Utilization of CT for Minor Blunt Head Trauma for Patients Aged 18 Years and Older emeasure Identifier (Measure Authoring Tool) NQF Number Measurement
Implementing Clinical Decision Support. C Craig Blackmore, MD, MPH, FASER Center for Health Care Improvement Science
 Implementing Clinical Decision Support C Craig Blackmore, MD, MPH, FASER Center for Health Care Improvement Science Objectives What is imaging clinical decision support? Does it work? How should it be
Implementing Clinical Decision Support C Craig Blackmore, MD, MPH, FASER Center for Health Care Improvement Science Objectives What is imaging clinical decision support? Does it work? How should it be
Disclosure Statement. Dr. Kadish has no relevant financial relationships with any commercial interests mentioned in this talk.
 Disclosure Statement Dr. Kadish has no relevant financial relationships with any commercial interests mentioned in this talk. Head Trauma Evaluation Primary and secondary injury Disposition Sports related
Disclosure Statement Dr. Kadish has no relevant financial relationships with any commercial interests mentioned in this talk. Head Trauma Evaluation Primary and secondary injury Disposition Sports related
USASOC Neurocognitive Testing and Post Injury Evaluation and Treatment Clinical Practice Guideline (CPG)
") USASOC Neurocognitive Testing and Post Injury Evaluation and Treatment Clinical Practice Guideline (CPG) Note: The intent of this CPG is to serve as general guidance for medics and medical officers. It
USASOC Neurocognitive Testing and Post Injury Evaluation and Treatment Clinical Practice Guideline (CPG) Note: The intent of this CPG is to serve as general guidance for medics and medical officers. It
Avoidable Imaging Initiative
 Avoidable Imaging Initiative Head CT decision rules and liability Does ordering more CTs protect you? Medical liability and avoidable imaging Tribe mentality- Anthropology of over ordering Presenters Dr.
Avoidable Imaging Initiative Head CT decision rules and liability Does ordering more CTs protect you? Medical liability and avoidable imaging Tribe mentality- Anthropology of over ordering Presenters Dr.
Kristin s Head Trauma Board Questions 11/07/14
 Kristin s Head Trauma Board Questions { 11/07/14 A healthy 15 y/o boy was playing football at a park near his home with a group of friends when he tripped over a friend s leg while trying to catch a pass.
Kristin s Head Trauma Board Questions { 11/07/14 A healthy 15 y/o boy was playing football at a park near his home with a group of friends when he tripped over a friend s leg while trying to catch a pass.
September 6, Dear Centers for Medicare & Medicaid Services,
 September 6, 2016 Centers for Medicare & Medicaid Services Department of Health and Human Services Attention: CMS-1631-P Mail Stop C4-26-05 7500 Security Boulevard Baltimore, MD 21244-1850 Re: Revisions
September 6, 2016 Centers for Medicare & Medicaid Services Department of Health and Human Services Attention: CMS-1631-P Mail Stop C4-26-05 7500 Security Boulevard Baltimore, MD 21244-1850 Re: Revisions
Management of Severe Traumatic Brain Injury
 Guideline for North Bristol Trust Management of Severe Traumatic Brain Injury This guideline describes the following: Initial assessment and management of the patient with head injury Indications for CT
Guideline for North Bristol Trust Management of Severe Traumatic Brain Injury This guideline describes the following: Initial assessment and management of the patient with head injury Indications for CT
Use of CT in minor traumatic brain injury. Lisa Ayoub-Rodriguez, MD Bert Johansson, MD Michael Lee, MD
 Use of CT in minor traumatic brain injury Lisa Ayoub-Rodriguez, MD Bert Johansson, MD Michael Lee, MD No financial or other conflicts of interest Epidemiology of traumatic brain injury (TBI) Risks associated
Use of CT in minor traumatic brain injury Lisa Ayoub-Rodriguez, MD Bert Johansson, MD Michael Lee, MD No financial or other conflicts of interest Epidemiology of traumatic brain injury (TBI) Risks associated
Pre-hospital Response to Trauma and Brain Injury. Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center
 Pre-hospital Response to Trauma and Brain Injury Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center Traumatic Brain Injury is Common 235,000 Americans hospitalized for non-fatal TBI
Pre-hospital Response to Trauma and Brain Injury Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center Traumatic Brain Injury is Common 235,000 Americans hospitalized for non-fatal TBI
Hit head, on blood thinner-wife wants CT. Will Davies June 2014
 Hit head, on blood thinner-wife wants CT Will Davies June 2014 Selection of Adults with Head Injury for CT Scan Early management of head injury: summary of updated NICE guidance. Hodgkinson S, Pollit V,
Hit head, on blood thinner-wife wants CT Will Davies June 2014 Selection of Adults with Head Injury for CT Scan Early management of head injury: summary of updated NICE guidance. Hodgkinson S, Pollit V,
Mild Traumatic Brain Injury. Timothy Johnson, MD, FACEP, FAAEM Fairview Southdale Emergency Department
 Mild Traumatic Brain Injury Timothy Johnson, MD, FACEP, FAAEM Fairview Southdale Emergency Department Objectives Review the epidemiology of mild TBI. Learn to appreciate the risks and benefits of CT imaging
Mild Traumatic Brain Injury Timothy Johnson, MD, FACEP, FAAEM Fairview Southdale Emergency Department Objectives Review the epidemiology of mild TBI. Learn to appreciate the risks and benefits of CT imaging
PEDIATRIC MILD TRAUMATIC HEAD INJURY
 PEDIATRIC MILD TRAUMATIC HEAD INJURY October 2011 Quality Improvement Resources Illinois Emergency Medical Services for Children is a collaborative program between the Illinois Department of Public Health
PEDIATRIC MILD TRAUMATIC HEAD INJURY October 2011 Quality Improvement Resources Illinois Emergency Medical Services for Children is a collaborative program between the Illinois Department of Public Health
A bout million patients present to UK hospitals
 420 ORIGINAL ARTICLE Application of the Canadian CT head rules in managing minor head injuries in a UK emergency department: implications for the implementation of the NICE guidelines H Y Sultan, A Boyle,
420 ORIGINAL ARTICLE Application of the Canadian CT head rules in managing minor head injuries in a UK emergency department: implications for the implementation of the NICE guidelines H Y Sultan, A Boyle,
UHSM ED Pathway ELDERLY FALL / COLLAPSE
 UHSM ED Pathway ELDERLY FALL / COLLAPSE Patient name / Pathway for patients who require assessment in ED after a fall or collapse Note: - It can be used if the patient has also sustained a minor head injury
UHSM ED Pathway ELDERLY FALL / COLLAPSE Patient name / Pathway for patients who require assessment in ED after a fall or collapse Note: - It can be used if the patient has also sustained a minor head injury
R-SCAN: Engaging Clinicians in Value-based Care
 R-SCAN: Engaging Clinicians in Value-based Care Nancy Fredericks, MBA R-SCAN Director rscan.org What is R-SCAN? A collaborative between referring clinicians and radiologists to improve patient care R-SCAN
R-SCAN: Engaging Clinicians in Value-based Care Nancy Fredericks, MBA R-SCAN Director rscan.org What is R-SCAN? A collaborative between referring clinicians and radiologists to improve patient care R-SCAN
Failure to Obtain Computed Tomography Imaging in Head Trauma: A Review of Relevant Case Law
 ORIGINAL CONTRIBUTION Failure to Obtain Computed Tomography Imaging in Head Trauma: A Review of Relevant Case Law Rachel A. Lindor, MD, JD, Eric T. Boie, MD, Ronna L. Campbell, MD, PhD, Erik P. Hess, MD,
ORIGINAL CONTRIBUTION Failure to Obtain Computed Tomography Imaging in Head Trauma: A Review of Relevant Case Law Rachel A. Lindor, MD, JD, Eric T. Boie, MD, Ronna L. Campbell, MD, PhD, Erik P. Hess, MD,
TALK TRAUMA Clearing the C-Spine. David Ouellette
 TALK TRAUMA 2011 Clearing the C-Spine David Ouellette Case #1 - Mother / Daughter MVC 34 y/o female Dangerous mechanism CHI Mumbling incoherently Femur # - distracting injury ETOH - 22 9 y/o female Dangerous
TALK TRAUMA 2011 Clearing the C-Spine David Ouellette Case #1 - Mother / Daughter MVC 34 y/o female Dangerous mechanism CHI Mumbling incoherently Femur # - distracting injury ETOH - 22 9 y/o female Dangerous
Managing the U+liza+on of CT and MR Studies in an Era of Precer+fica+on
 Managing the U+liza+on of CT and MR Studies in an Era of Precer+fica+on Steven E. Seltzer, M.D. Department of Radiology Brigham and Women s Hospital Harvard Medical School Boston, MA COI Disclosure - Partners
Managing the U+liza+on of CT and MR Studies in an Era of Precer+fica+on Steven E. Seltzer, M.D. Department of Radiology Brigham and Women s Hospital Harvard Medical School Boston, MA COI Disclosure - Partners
The United States and its health care system are in a financial
 Overuse CT Overuse for Mild Traumatic Brain Injury Edward R. Melnick, MD; Christopher M. Szlezak, MD; Suzanne K. Bentley, MD; James D. Dziura, PhD; Simon Kotlyar, MD, MSc; Lori A. Post, PhD The United
Overuse CT Overuse for Mild Traumatic Brain Injury Edward R. Melnick, MD; Christopher M. Szlezak, MD; Suzanne K. Bentley, MD; James D. Dziura, PhD; Simon Kotlyar, MD, MSc; Lori A. Post, PhD The United
Evidence Based Trauma Radiology
 Evidence Based Trauma Radiology C. Craig Blackmore, MD, MPH Department of Radiology Scientific Director, Center for Healthcare Solutions Virginia Mason Medical Center Disclosure: Book Royalties, Springer-Verlag
Evidence Based Trauma Radiology C. Craig Blackmore, MD, MPH Department of Radiology Scientific Director, Center for Healthcare Solutions Virginia Mason Medical Center Disclosure: Book Royalties, Springer-Verlag
Reviewing the recent literature to answer clinical questions: Should I change my practice?
 Reviewing the recent literature to answer clinical questions: Should I change my practice? JILL MILLER, MD PEM ATTENDING CHKD ASSISTANT PROFESSOR PEDIATRICS, EVMS Objectives Review the literature to answer
Reviewing the recent literature to answer clinical questions: Should I change my practice? JILL MILLER, MD PEM ATTENDING CHKD ASSISTANT PROFESSOR PEDIATRICS, EVMS Objectives Review the literature to answer
Referral Criteria for Medical CT Radiation Exposures. Neuro Referrals
 Referral Criteria for Medical CT Radiation Exposures Neuro Referrals CHH & HRI The Ionising Radiation (Medical Exposure) Regulations 2017 Document Control Reference No: 3.2 First published: 2016 Version:
Referral Criteria for Medical CT Radiation Exposures Neuro Referrals CHH & HRI The Ionising Radiation (Medical Exposure) Regulations 2017 Document Control Reference No: 3.2 First published: 2016 Version:
Evaluation and Stabilization of the Athlete with Possible Spine Injury
 Evaluation and Stabilization of the Athlete with Possible Spine Injury Jeffrey H. Bohmer, MD, FACEP Emergency Physician Northwestern Medicine Central DuPage Hospital June 12, 2015 Introduction Goals: 1.
Evaluation and Stabilization of the Athlete with Possible Spine Injury Jeffrey H. Bohmer, MD, FACEP Emergency Physician Northwestern Medicine Central DuPage Hospital June 12, 2015 Introduction Goals: 1.
LOSS OF CONSCIOUSNESS & ASSESSMENT. Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT
 LOSS OF CONSCIOUSNESS & ASSESSMENT Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT OUTLINE Causes Head Injury Clinical Features Complications Rapid Assessment Glasgow Coma Scale Classification
LOSS OF CONSCIOUSNESS & ASSESSMENT Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT OUTLINE Causes Head Injury Clinical Features Complications Rapid Assessment Glasgow Coma Scale Classification
Head injuries. Severity of head injuries
 Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
The AHEAD Study: Managing anticoagulatedpatients who suffer head injury
 AHEAD Study The AHEAD Study: Managing anticoagulatedpatients who suffer head injury Suzanne Mason 1,2, Maxine Kuczawski 1, Matthew Stevenson 1, Dawn Teare 1, Michael Holmes 1, ShammiRamlakhan 1, Steve
AHEAD Study The AHEAD Study: Managing anticoagulatedpatients who suffer head injury Suzanne Mason 1,2, Maxine Kuczawski 1, Matthew Stevenson 1, Dawn Teare 1, Michael Holmes 1, ShammiRamlakhan 1, Steve
Time Equals Neurons - Spinal Cord Injury Management in the first 4 Hours
 Time Equals Neurons - Spinal Cord Injury Management in the first 4 Hours William D. Whetstone M.D. Clinical Professor UCSF Department of Emergency Medicine SFGH ED Center for Neuro-Critical Emergencies
Time Equals Neurons - Spinal Cord Injury Management in the first 4 Hours William D. Whetstone M.D. Clinical Professor UCSF Department of Emergency Medicine SFGH ED Center for Neuro-Critical Emergencies
Pediatric head trauma: the evidence regarding indications for emergent neuroimaging
 DOI 10.1007/s00247-008-0996-5 ALARA: BUILDING BRIDGES BETWEEN RADIOLOGY AND EMERGENCY MEDICINE Pediatric head trauma: the evidence regarding indications for emergent neuroimaging Nathan Kuppermann Received:
DOI 10.1007/s00247-008-0996-5 ALARA: BUILDING BRIDGES BETWEEN RADIOLOGY AND EMERGENCY MEDICINE Pediatric head trauma: the evidence regarding indications for emergent neuroimaging Nathan Kuppermann Received:
:: Closed Head Injury in Adults
 ADULT TRAUMA CLINICAL PRACTICE GUIDELINES Initial Management of :: Closed Head Injury in Adults Suggested citation: Dr Duncan Reed 2007, Adult Trauma Clinical Practice Guidelines, Initial Management of
ADULT TRAUMA CLINICAL PRACTICE GUIDELINES Initial Management of :: Closed Head Injury in Adults Suggested citation: Dr Duncan Reed 2007, Adult Trauma Clinical Practice Guidelines, Initial Management of
USE OF CT SCAN IN A CHILD WITH MTBI
 TO SCAN OR NOT TO SCAN USE OF CT SCAN IN A CHILD WITH MTBI LISA AYOUB-RODRIGUEZ MD PEDIATRIC HOSPITALIST MIKE LEE MD PEDIATRIC RESIDENT BERT JOHANSSON MD PEDIATRIC HOSPITALIST DISCLOSURES I M NOT A SURGEON
TO SCAN OR NOT TO SCAN USE OF CT SCAN IN A CHILD WITH MTBI LISA AYOUB-RODRIGUEZ MD PEDIATRIC HOSPITALIST MIKE LEE MD PEDIATRIC RESIDENT BERT JOHANSSON MD PEDIATRIC HOSPITALIST DISCLOSURES I M NOT A SURGEON
Traumatic Brain Injury Pathway, GCS 15 Closed head injury
 Traumatic Brain Injury Pathway, GCS 15 Closed head injury Plus Any One of the Following Mild TBI 2010 Consensus Definition of TBI from CDC, NINDS, NIDDR, VA, DVBIC, DCoE Plus Any One of the Following New
Traumatic Brain Injury Pathway, GCS 15 Closed head injury Plus Any One of the Following Mild TBI 2010 Consensus Definition of TBI from CDC, NINDS, NIDDR, VA, DVBIC, DCoE Plus Any One of the Following New
8/29/2011. Brain Injury Incidence: 200/100,000. Prehospital Brain Injury Mortality Incidence: 20/100,000
 Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
DIAGNOSTIC PROCEDURES IN MILD TRAUMATIC BRAIN INJURY: RESULTS OF THE WHO COLLABORATING CENTRE TASK FORCE ON MILD TRAUMATIC BRAIN INJURY
 J Rehabil Med 2004; Suppl. 43: 61 75 DIAGNOSTIC PROCEDURES IN MILD TRAUMATIC BRAIN INJURY: RESULTS OF THE WHO COLLABORATING CENTRE TASK FORCE ON MILD TRAUMATIC BRAIN INJURY Jörgen Borg, 1 Lena Holm, 2
J Rehabil Med 2004; Suppl. 43: 61 75 DIAGNOSTIC PROCEDURES IN MILD TRAUMATIC BRAIN INJURY: RESULTS OF THE WHO COLLABORATING CENTRE TASK FORCE ON MILD TRAUMATIC BRAIN INJURY Jörgen Borg, 1 Lena Holm, 2
PRACTICE GUIDELINE. DEFINITIONS: Mild head injury: Glasgow Coma Scale* (GCS) score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8
 score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8") PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
Emergency Medicine Research: Creating Evidence to Improve Safety and Effectiveness of ED Patient Care
 Emergency Medicine Research: Creating Evidence to Improve Safety and Effectiveness of ED Patient Care Dr Eric Clark MD, FRCPC Department of Emergency Medicine University of Ottawa Canada No Conflicts of
Emergency Medicine Research: Creating Evidence to Improve Safety and Effectiveness of ED Patient Care Dr Eric Clark MD, FRCPC Department of Emergency Medicine University of Ottawa Canada No Conflicts of
Restore adequate respiratory and circulatory conditions. Reduce pain
 Pre-hospital management of the trauma patient is best performed by an integrated team focused on minimizing the time from injury to definitive care at an appropriate trauma center. Dispatchers, first responders,
Pre-hospital management of the trauma patient is best performed by an integrated team focused on minimizing the time from injury to definitive care at an appropriate trauma center. Dispatchers, first responders,
The research questions are presented in priority order, and are further elaborated with lay summaries and three-part questions where applicable.
 Top 30 Emergency Medicine Research Priorities 23 January 2017 The rankings were established by consensus at the final prioritisation workshop run by the James Lind Alliance Emergency Medicine Priority
Top 30 Emergency Medicine Research Priorities 23 January 2017 The rankings were established by consensus at the final prioritisation workshop run by the James Lind Alliance Emergency Medicine Priority
Imaging in the Trauma Patient
 Imaging in the Trauma Patient David A. Spain, MD Department of Surgery Stanford University Pan Scan Instead of Clinical Exam? 1 Granted, some patients don t need CT scan Platinum Package Stanford Special
Imaging in the Trauma Patient David A. Spain, MD Department of Surgery Stanford University Pan Scan Instead of Clinical Exam? 1 Granted, some patients don t need CT scan Platinum Package Stanford Special
Andrzej Żyluk 1, Agnieszka Mazur 1, Bernard Piotuch 1, Krzysztof Safranow 2
 POLSKI PRZEGLĄD CHIRURGICZNY 2013, 85, 12, 699 705 10.2478/pjs-2013-0107 Analysis of the reliability of clinical examination in predicting traumatic cerebral lesions and skull fractures in patients with
POLSKI PRZEGLĄD CHIRURGICZNY 2013, 85, 12, 699 705 10.2478/pjs-2013-0107 Analysis of the reliability of clinical examination in predicting traumatic cerebral lesions and skull fractures in patients with
Spine MRI and Spine CT Test Request Tip Sheet
 Spine MRI and Spine CT With/Without Contrast CT, MRI The study considered best for a specific clinical scenario should be ordered. The second study should be done ONLY if the first study does not provide
Spine MRI and Spine CT With/Without Contrast CT, MRI The study considered best for a specific clinical scenario should be ordered. The second study should be done ONLY if the first study does not provide
Imaging Biomarkers Significance S100B NSE. Admitted within 6 hours of injury and CT scan occurred after initial examination. N = 1,064 CT+ N = 50 4.
 Concussion Guidelines Step 1: Systematic Review of Prevalent Indicators Supplemental Content 7 Evidence Table. Included Studies For Key Question 4 Imaging and Biomarker Publications Medium Potential for
Concussion Guidelines Step 1: Systematic Review of Prevalent Indicators Supplemental Content 7 Evidence Table. Included Studies For Key Question 4 Imaging and Biomarker Publications Medium Potential for
Anticoagulants and Head Injuries. Asaad Shujaa,MD,FRCPC,FAAEM Assistant Professor,weill Corneal Medicne Senior Consultant,HMC Qatar
 Anticoagulants and Head Injuries Asaad Shujaa,MD,FRCPC,FAAEM Assistant Professor,weill Corneal Medicne Senior Consultant,HMC Qatar Common Anticoagulants and Indications Coumadin (warfarin) indicated for
Anticoagulants and Head Injuries Asaad Shujaa,MD,FRCPC,FAAEM Assistant Professor,weill Corneal Medicne Senior Consultant,HMC Qatar Common Anticoagulants and Indications Coumadin (warfarin) indicated for
Chest Pain Wave I Webinar. May, 30 th 2017
 Chest Pain Wave I Webinar May, 30 th 2017 Disclaimer The project described is supported by Funding Opportunity Number CMS-1L1-15-002 from the U.S. Department of Health & Human Services, Centers for Medicare
Chest Pain Wave I Webinar May, 30 th 2017 Disclaimer The project described is supported by Funding Opportunity Number CMS-1L1-15-002 from the U.S. Department of Health & Human Services, Centers for Medicare
Spine MRI and Spine CT Test Request Tip Sheet
 Spine MRI and Spine CT With/Without Contrast CT, MRI The study considered best for a specific clinical scenario should be ordered. The second study should be done ONLY if the first study does not provide
Spine MRI and Spine CT With/Without Contrast CT, MRI The study considered best for a specific clinical scenario should be ordered. The second study should be done ONLY if the first study does not provide
HEAD INJURY MODULE ASSESSMENT OF HEAD INJURY
 HEAD INJURY MODULE Introduction Head injury is common in both adult and paediatric populations. In all-comers with head injury, () 90% present with normal or near-normal consciousness, and mortality is
HEAD INJURY MODULE Introduction Head injury is common in both adult and paediatric populations. In all-comers with head injury, () 90% present with normal or near-normal consciousness, and mortality is
Selective Spinal Immobilization
 Selective Spinal Immobilization Objectives Understand the background of spinal immobilization. Understand the rationale for developing a current selective spinal immobilization protocol. Review the data
Selective Spinal Immobilization Objectives Understand the background of spinal immobilization. Understand the rationale for developing a current selective spinal immobilization protocol. Review the data
EMS System for Metropolitan Oklahoma City and Tulsa 2018 Medical Control Board Treatment Protocols
 EMERGENCY MEDICAL RESPONDER EMT EMT-INTERMEDIATE 85 ADVANCED EMT PARAMEDIC 14G PATIENT PRIORITIZATION While each patient will receive the best possible EMS care in a humane and ethical manner, proper patient
EMERGENCY MEDICAL RESPONDER EMT EMT-INTERMEDIATE 85 ADVANCED EMT PARAMEDIC 14G PATIENT PRIORITIZATION While each patient will receive the best possible EMS care in a humane and ethical manner, proper patient
GUIDELINES FOR THE MANAGEMENT OF HEAD INJURIES IN REMOTE AND RURAL ALASKA
 GUIDELINES FOR THE MANAGEMENT OF HEAD INJURIES IN REMOTE AND RURAL ALASKA Approximately 800 patients with head injuries die or are hospitalized in the state of Alaska each year 1. In addition, thousands
GUIDELINES FOR THE MANAGEMENT OF HEAD INJURIES IN REMOTE AND RURAL ALASKA Approximately 800 patients with head injuries die or are hospitalized in the state of Alaska each year 1. In addition, thousands
Concussion Update and Case Presentations
 Concussion Update and Case Presentations Cayce Onks, DO, MS, ATC Associate Professor Primary Care Sports Medicine Penn State Concussion Program Departments of Family Medicine and Orthopaedics I have no
Concussion Update and Case Presentations Cayce Onks, DO, MS, ATC Associate Professor Primary Care Sports Medicine Penn State Concussion Program Departments of Family Medicine and Orthopaedics I have no
Sasha Dubrovsky, MSc MD FRCPC Pediatric Emergency Medicine Montreal Children s Hospital - MUHC October 2010
 Sasha Dubrovsky, MSc MD FRCPC Pediatric Emergency Medicine Montreal Children s Hospital - MUHC October 2010 Learning objectives 1. Discuss diagnostic goals in pediatric trauma Diagnose All vs. Severe Injuries
Sasha Dubrovsky, MSc MD FRCPC Pediatric Emergency Medicine Montreal Children s Hospital - MUHC October 2010 Learning objectives 1. Discuss diagnostic goals in pediatric trauma Diagnose All vs. Severe Injuries
Measuring Overuse and Underuse of Brain CTs in Pediatric Patients with mtbi in Two Canadian Emergency Departments
 Measuring Overuse and Underuse of Brain CTs in Pediatric Patients with mtbi in Two Canadian Emergency Departments Martin Gariépy, PhD Dr Patrick Archambault Dr Jocelyn Gravel 2017 Quebec City, Quebec,
Measuring Overuse and Underuse of Brain CTs in Pediatric Patients with mtbi in Two Canadian Emergency Departments Martin Gariépy, PhD Dr Patrick Archambault Dr Jocelyn Gravel 2017 Quebec City, Quebec,
Shenandoah Co. Fire & Rescue. Injuries to. and Spine. December EMS Training Bill Streett Training Section Chief
 Shenandoah Co. Fire & Rescue Injuries to the Head and Spine December EMS Training Bill Streett Training Section Chief C.E. Card Information BLS Providers 2 Cards / Provider Category 1 Course # Blank Topic#
Shenandoah Co. Fire & Rescue Injuries to the Head and Spine December EMS Training Bill Streett Training Section Chief C.E. Card Information BLS Providers 2 Cards / Provider Category 1 Course # Blank Topic#
Continuing Medical Education Activity in Academic Emergency Medicine
 CONTINUING MEDICAL EDUCATION Continuing Medical Education Activity in Academic Emergency Medicine CME Editor: Hal Thomas, MD Authors: Joshua S. Easter, MD, Jason S. Haukoos, MD, MSc, Jonathan Claud, MD,
CONTINUING MEDICAL EDUCATION Continuing Medical Education Activity in Academic Emergency Medicine CME Editor: Hal Thomas, MD Authors: Joshua S. Easter, MD, Jason S. Haukoos, MD, MSc, Jonathan Claud, MD,
Chapter 31. Objectives. Objectives 01/09/2013. Head Trauma
 Chapter 31 Head Trauma Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1. Define key terms introduced
Chapter 31 Head Trauma Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1. Define key terms introduced
Spine MRI and Spine CT Test Request Tip Sheet
 Spine MRI and Spine CT With/Without Contrast CT, MRI Studies should NOT be ordered simultaneously as dual studies (i.e., with and without contrast). Radiation exposure is doubled and both views are rarely
Spine MRI and Spine CT With/Without Contrast CT, MRI Studies should NOT be ordered simultaneously as dual studies (i.e., with and without contrast). Radiation exposure is doubled and both views are rarely
Instructional Course #34. Review of Neuropharmacology in Pediatric Brain Injury. John Pelegano MD Jilda Vargus-Adams MD, MSc Micah Baird MD
 Instructional Course #34 Review of Neuropharmacology in Pediatric Brain Injury John Pelegano MD Jilda Vargus-Adams MD, MSc Micah Baird MD Outline of Course 1. Introduction John Pelegano MD 2. Neuropharmocologic
Instructional Course #34 Review of Neuropharmacology in Pediatric Brain Injury John Pelegano MD Jilda Vargus-Adams MD, MSc Micah Baird MD Outline of Course 1. Introduction John Pelegano MD 2. Neuropharmocologic
Radiology Update: Balancing Diagnostic Needs with Cost Effectiveness
 Radiology Update: Balancing Diagnostic Needs with Cost Effectiveness October 2018 Ramin Khorasani, MD, MPH Professor of Radiology, Harvard Medical School Director, Center for Evidence-Based Imaging Vice
Radiology Update: Balancing Diagnostic Needs with Cost Effectiveness October 2018 Ramin Khorasani, MD, MPH Professor of Radiology, Harvard Medical School Director, Center for Evidence-Based Imaging Vice
TRAUMATIC CAROTID &VERTEBRAL ARTERY INJURIES
 TRAUMATIC CAROTID &VERTEBRAL ARTERY INJURIES ALBERTO MAUD, MD ASSOCIATE PROFESSOR TEXAS TECH UNIVERSITY HEALTH SCIENCES CENTER EL PASO PAUL L. FOSTER SCHOOL OF MEDICINE 18TH ANNUAL RIO GRANDE TRAUMA 2017
TRAUMATIC CAROTID &VERTEBRAL ARTERY INJURIES ALBERTO MAUD, MD ASSOCIATE PROFESSOR TEXAS TECH UNIVERSITY HEALTH SCIENCES CENTER EL PASO PAUL L. FOSTER SCHOOL OF MEDICINE 18TH ANNUAL RIO GRANDE TRAUMA 2017
The Yield of Head CT in Syncope: A Pilot Study
 The Yield of Head CT in Syncope: A Pilot Study The Harvard community has made this article openly available. Please share how this access benefits you. Your story matters. Citation Published Version Accessed
The Yield of Head CT in Syncope: A Pilot Study The Harvard community has made this article openly available. Please share how this access benefits you. Your story matters. Citation Published Version Accessed
Canadian CT head rule and New Orleans Criteria in mild traumatic brain injury: comparison at a tertiary referral hospital in Japan
 DOI 10.1186/s40064-016-1781-9 RESEARCH Open Access Canadian CT head rule and New Orleans Criteria in mild traumatic brain injury: comparison at a tertiary referral hospital in Japan Daddy Mata Mbemba 1,2,
DOI 10.1186/s40064-016-1781-9 RESEARCH Open Access Canadian CT head rule and New Orleans Criteria in mild traumatic brain injury: comparison at a tertiary referral hospital in Japan Daddy Mata Mbemba 1,2,
Spine MRI and Spine CT Test Request Tip Sheet
 Spine MRI and Spine CT MRI is almost always preferred over CT scan; if ordering CT, CLEARLY document why MRI is not appropriate. In cases of back pain without red flags, six weeks of multimodality supervised
Spine MRI and Spine CT MRI is almost always preferred over CT scan; if ordering CT, CLEARLY document why MRI is not appropriate. In cases of back pain without red flags, six weeks of multimodality supervised
High Risk + Challenging Trauma Cases. Hawaii. Topics 1/27/2014. David Thompson, MD, MPH. Head injury in the anticoagulated patient.
 High Risk + Challenging Trauma Cases David Thompson, MD, MPH Hawaii Topics Head injury in the anticoagulated patient Shock recognition Case 1: Head injury HPI: 57 yo male w/ PMH atrial fibrillation, on
High Risk + Challenging Trauma Cases David Thompson, MD, MPH Hawaii Topics Head injury in the anticoagulated patient Shock recognition Case 1: Head injury HPI: 57 yo male w/ PMH atrial fibrillation, on
Introduction. Objectives C-Spine: Where Are We Now? NAEMSP Medical Director Course 1/9/2013
 NAEMSP Medical Director Course 1/9/2013 Objectives C-Spine: Where Are We Now? Robert M. Domeier, MD EMS Medical Director Washtenaw/Livingston Medical Control Authority Department of Emergency Medicine
NAEMSP Medical Director Course 1/9/2013 Objectives C-Spine: Where Are We Now? Robert M. Domeier, MD EMS Medical Director Washtenaw/Livingston Medical Control Authority Department of Emergency Medicine
Just Clear Them The Approach to Medical Clearance
 Just Clear Them The Approach to Medical Clearance Dr. Nalin Ahluwalia MD CCFP(EM) Associate Chief of Staff Emergency Physician Oakville Trafalgar Memorial Hospital My Disclosures None! Exemplary patient
Just Clear Them The Approach to Medical Clearance Dr. Nalin Ahluwalia MD CCFP(EM) Associate Chief of Staff Emergency Physician Oakville Trafalgar Memorial Hospital My Disclosures None! Exemplary patient
Form 1 ED Data Blunt Traumatic Brain Injury (TBI)
") Complete this form * Prior to reviewing CT or skull xray (if obtained) Data Source faculty physician, fellow or resident physician, NP or PA with faculty oversight Patient Study ID Number Faculty physician,
Complete this form * Prior to reviewing CT or skull xray (if obtained) Data Source faculty physician, fellow or resident physician, NP or PA with faculty oversight Patient Study ID Number Faculty physician,
Research Article Analysis of Repeated CT Scan Need in Blunt Head Trauma
 Hindawi Publishing Corporation Emergency Medicine International Volume 2013, Article ID 916253, 5 pages http://dx.doi.org/10.1155/2013/916253 Research Article Analysis of Repeated CT Scan Need in Blunt
Hindawi Publishing Corporation Emergency Medicine International Volume 2013, Article ID 916253, 5 pages http://dx.doi.org/10.1155/2013/916253 Research Article Analysis of Repeated CT Scan Need in Blunt
Traumatic Brain Injuries
 Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
Introduction to Neurosurgical Subspecialties:
 Introduction to Neurosurgical Subspecialties: Trauma and Critical Care Neurosurgery Brian L. Hoh, MD 1, Gregory J. Zipfel, MD 2 and Stacey Q. Wolfe, MD 3 1 University of Florida, 2 Washington University,
Introduction to Neurosurgical Subspecialties: Trauma and Critical Care Neurosurgery Brian L. Hoh, MD 1, Gregory J. Zipfel, MD 2 and Stacey Q. Wolfe, MD 3 1 University of Florida, 2 Washington University,
PedsCases Podcast Scripts
 PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on the Approach to Pediatric Head Injury. These podcasts are designed to give medical students an overview of key topics
PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on the Approach to Pediatric Head Injury. These podcasts are designed to give medical students an overview of key topics
Conceptualization of Functional Outcomes Following TBI. Ryan Stork, MD
 Conceptualization of Functional Outcomes Following TBI Ryan Stork, MD Conceptualization of Functional Outcomes Following Traumatic Brain Injury Ryan Stork, MD Clinical Lecturer Brain Injury Medicine &
Conceptualization of Functional Outcomes Following TBI Ryan Stork, MD Conceptualization of Functional Outcomes Following Traumatic Brain Injury Ryan Stork, MD Clinical Lecturer Brain Injury Medicine &
Expert Group Meeting-Trauma
 Why was Trauma Summit needed? There are no clear guidelines/algorithms to assist acute management of trauma patients in the Indian setting. One of our visions is to assist young doctors in acute care medicine
Why was Trauma Summit needed? There are no clear guidelines/algorithms to assist acute management of trauma patients in the Indian setting. One of our visions is to assist young doctors in acute care medicine
Head, Face, Eyes, Ears, Nose and Throat. Neurological Exam. Eye Function 12/11/2017. Oak Ridge High School Conroe, Texas
 Head, Face, Eyes, Ears, Nose and Throat Oak Ridge High School Conroe, Texas Neurological Exam Consists of Five Major Areas: 1. cerebral testing cognitive functioning 2. Cranial nerve testing 3. Cerebellar
Head, Face, Eyes, Ears, Nose and Throat Oak Ridge High School Conroe, Texas Neurological Exam Consists of Five Major Areas: 1. cerebral testing cognitive functioning 2. Cranial nerve testing 3. Cerebellar
EMS System for Metropolitan Oklahoma City and Tulsa 2019 Medical Control Board Treatment Protocols
 EMERGENCY MEDICAL RESPONDER EMT EMT-INTERMEDIATE 85 ADVANCED EMT PARAMEDIC 14G PATIENT PRIORITIZATION While each patient will receive the best possible EMS care in a humane and ethical manner, proper patient
EMERGENCY MEDICAL RESPONDER EMT EMT-INTERMEDIATE 85 ADVANCED EMT PARAMEDIC 14G PATIENT PRIORITIZATION While each patient will receive the best possible EMS care in a humane and ethical manner, proper patient
Stroke Update. Lacunar 19% Thromboembolic 6% SAH 13% ICH 13% Unknown 32% Hemorrhagic 26% Ischemic 71% Other 3% Cardioembolic 14%
 Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
Child Neurology Elective PL1 Rotation
 PL1 Rotation The neurology elective is available to first year residents in either a 2 or 4 week block rotation. The experience will include performing inpatient consultations, attending outpatient clinics
PL1 Rotation The neurology elective is available to first year residents in either a 2 or 4 week block rotation. The experience will include performing inpatient consultations, attending outpatient clinics
Annually in the United States, 1 million patients will require
 ORIGINAL RESEARCH SPINE Screening Cervical Spine CT in the Emergency Department, Phase 2: A Prospective Assessment of Use B. Griffith, M. Kelly, P. Vallee, M. Slezak, J. Nagarwala, S. Krupp, C.P. Loeckner,
ORIGINAL RESEARCH SPINE Screening Cervical Spine CT in the Emergency Department, Phase 2: A Prospective Assessment of Use B. Griffith, M. Kelly, P. Vallee, M. Slezak, J. Nagarwala, S. Krupp, C.P. Loeckner,
Avoidable Imaging Initiative
 Avoidable Imaging Initiative Traumatic Brain Injury CT Prediction Rules in Children Optimizing Uptake of Clinical Decision Support in the Electronic Health Record Data Collection- CEDR and Quality/Performance
Avoidable Imaging Initiative Traumatic Brain Injury CT Prediction Rules in Children Optimizing Uptake of Clinical Decision Support in the Electronic Health Record Data Collection- CEDR and Quality/Performance
NEUROSURGICAL EMERGENCY GUIDELINE DEVELOPMENT GROUP P3 NEURO CENTER OF NEUROSCIENCE RESEARCH AND SERVICE USM
 NEUROSURGICAL EMERGENCY GUIDELINE DEVELOPMENT GROUP P3 NEURO CENTER OF NEUROSCIENCE RESEARCH AND SERVICE USM Chairperson Professor Dr Zamzuri Idris Head of Department Members Associate Professor Dato Dr
NEUROSURGICAL EMERGENCY GUIDELINE DEVELOPMENT GROUP P3 NEURO CENTER OF NEUROSCIENCE RESEARCH AND SERVICE USM Chairperson Professor Dr Zamzuri Idris Head of Department Members Associate Professor Dato Dr
Critically Appraising Geriatric ED Screening Instruments Opening Pandora s Box to Futility or Identifying Novel Opportunities?
 Critically Appraising Geriatric ED Screening Instruments Opening Pandora s Box to Futility or Identifying Novel Opportunities? Christopher R. Carpenter, MD, MSc, FACEP, AGSF June 2, 2015 Disclosure of
Critically Appraising Geriatric ED Screening Instruments Opening Pandora s Box to Futility or Identifying Novel Opportunities? Christopher R. Carpenter, MD, MSc, FACEP, AGSF June 2, 2015 Disclosure of
Concussion Assessment and Management Update. Oluseun Olufade, MD and Lee Kneer, MD 1/12/19
 Concussion Assessment and Management Update Oluseun Olufade, MD and Lee Kneer, MD 1/12/19 OBJECTIVES When to refer to a physician? When to sent to the ER? When to image? Update on sports related concussion
Concussion Assessment and Management Update Oluseun Olufade, MD and Lee Kneer, MD 1/12/19 OBJECTIVES When to refer to a physician? When to sent to the ER? When to image? Update on sports related concussion
CLINICAL MANUAL. Trauma System Activation Trauma Code Criteria
 CLINICAL MANUAL Policy Number: CM T-28 Approved by: Nursing Congress, Management Forum Issue Date: 09/1999 Applies to: Downtown Value(s): Respect, Integrity, Innovation Page(s): 1 of 4 Trauma System Activation
CLINICAL MANUAL Policy Number: CM T-28 Approved by: Nursing Congress, Management Forum Issue Date: 09/1999 Applies to: Downtown Value(s): Respect, Integrity, Innovation Page(s): 1 of 4 Trauma System Activation
Modern Management of ICH
 Modern Management of ICH Bradley A. Gross, MD Assistant Professor, Dept of Neurosurgery, University of Pittsburgh October 2018 ICH Background Assessment & Diagnosis Medical Management Surgical Management
Modern Management of ICH Bradley A. Gross, MD Assistant Professor, Dept of Neurosurgery, University of Pittsburgh October 2018 ICH Background Assessment & Diagnosis Medical Management Surgical Management
In pursuit of high value practice: Designing a strategic plan to reduce unnecessary imaging in an academic radiology department.
 In pursuit of high value practice: Designing a strategic plan to reduce unnecessary imaging in an academic radiology department April 17, 2017 1 Authors and Disclosure Matthew D. Alvin, MD, MBA, MS, MA
In pursuit of high value practice: Designing a strategic plan to reduce unnecessary imaging in an academic radiology department April 17, 2017 1 Authors and Disclosure Matthew D. Alvin, MD, MBA, MS, MA
JUSTIFICATION PROTOCOLS FOR CT SCANNING ALBURY WODONGA HEALTH WODONGA CAMPUS
 JUSTIFICATION PROTOCOLS FOR CT SCANNING ALBURY WODONGA HEALTH WODONGA CAMPUS JUSTIFICATION PROTOCOLS FOR CT SCANNING INTRODUCTION: In accordance with the Victorian Radiation Act 2005 Wodonga Medical Imaging,
JUSTIFICATION PROTOCOLS FOR CT SCANNING ALBURY WODONGA HEALTH WODONGA CAMPUS JUSTIFICATION PROTOCOLS FOR CT SCANNING INTRODUCTION: In accordance with the Victorian Radiation Act 2005 Wodonga Medical Imaging,
TURN IT UP TO 11: LP IN THE DIAGNOSIS OF SAH. Matt Greer February 10 th, 2015
 TURN IT UP TO 11: LP IN THE DIAGNOSIS OF SAH Matt Greer February 10 th, 2015 IN CASE YOU MISSED THE REFERENCE HEADACHES IN THE ED Account for approximately 2% of ED visits 1% of these are due to SAH Approximately
TURN IT UP TO 11: LP IN THE DIAGNOSIS OF SAH Matt Greer February 10 th, 2015 IN CASE YOU MISSED THE REFERENCE HEADACHES IN THE ED Account for approximately 2% of ED visits 1% of these are due to SAH Approximately
Evidence-based Evaluation of Children with Blunt Head Trauma in the Emergency Department
 Evidence-based Evaluation of Children with Blunt Head Trauma in the Emergency Department Nathan Kuppermann, MD, MPH University of California, Davis School of Medicine Departments of Emergency Medicine
Evidence-based Evaluation of Children with Blunt Head Trauma in the Emergency Department Nathan Kuppermann, MD, MPH University of California, Davis School of Medicine Departments of Emergency Medicine
Heidi Lako-Adamson, MD, NRP, FAEMS FM Ambulance and Sanford EMS Education Medical Director
 Heidi Lako-Adamson, MD, NRP, FAEMS FM Ambulance and Sanford EMS Education Medical Director Spinal cord injury statistics. Definition of spinal motion restriction. Difference between spinal motion restriction
Heidi Lako-Adamson, MD, NRP, FAEMS FM Ambulance and Sanford EMS Education Medical Director Spinal cord injury statistics. Definition of spinal motion restriction. Difference between spinal motion restriction
Children diagnosed with skull fractures are often. Transfer of children with isolated linear skull fractures: is it worth the cost?
 clinical article J Neurosurg Pediatr 17:602 606, 2016 Transfer of children with isolated linear skull fractures: is it worth the cost? Ian K. White, MD, 1 Ecaterina Pestereva, BS, 1 Kashif A. Shaikh, MD,
clinical article J Neurosurg Pediatr 17:602 606, 2016 Transfer of children with isolated linear skull fractures: is it worth the cost? Ian K. White, MD, 1 Ecaterina Pestereva, BS, 1 Kashif A. Shaikh, MD,
Trauma Registry Documentation December 16, 2014
 Trauma Registry Documentation December 16, 2014 The State of Florida now requires ALL Acute Care hospitals to submit data to the statetrauma Registry. Although Baptist Health hospitals are NOT Trauma Centers
Trauma Registry Documentation December 16, 2014 The State of Florida now requires ALL Acute Care hospitals to submit data to the statetrauma Registry. Although Baptist Health hospitals are NOT Trauma Centers
The Prehospital Validation of the Canadian C-Spine Rule by Paramedics
 The Prehospital Validation of the Canadian C-Spine Rule by Paramedics CAEP, Victoria 2007 Study Coordinating Center: C Vaillancourt MD IG Stiell MD GA Wells PhD Ottawa Health Research Institute University
The Prehospital Validation of the Canadian C-Spine Rule by Paramedics CAEP, Victoria 2007 Study Coordinating Center: C Vaillancourt MD IG Stiell MD GA Wells PhD Ottawa Health Research Institute University
Multidisciplinary Geriatric Trauma Care Guideline
 Multidisciplinary Geriatric Trauma Care Background Traumatic injury in the geriatric population is increasing in prevalence and is associated with higher mortality and complication rates comparted to younger
Multidisciplinary Geriatric Trauma Care Background Traumatic injury in the geriatric population is increasing in prevalence and is associated with higher mortality and complication rates comparted to younger
10/6/2017. Notice. Traumatic Brain Injury & Head Trauma
 Notice All EMS Live@Nite presentations will be recorded (both audio and video) and available for public viewing online. By participating in EMS Live@Nite, you consent to audio and video recording and its/their
Notice All EMS Live@Nite presentations will be recorded (both audio and video) and available for public viewing online. By participating in EMS Live@Nite, you consent to audio and video recording and its/their
Neurological examination of the neurosurgical patient. Dániel Bereczki SU Department of Neurology
 Neurological examination of the neurosurgical patient Dániel Bereczki SU Department of Neurology E-learning Indivudual study Interactive learning Self assessment at the end of chapters E-learning Indivudual
Neurological examination of the neurosurgical patient Dániel Bereczki SU Department of Neurology E-learning Indivudual study Interactive learning Self assessment at the end of chapters E-learning Indivudual
The New England Journal of Medicine A POPULATION-BASED STUDY OF SEIZURES AFTER TRAUMATIC BRAIN INJURIES
 A POPULATION-BASED STUDY OF SEIZURES AFTER TRAUMATIC BRAIN INJURIES JOHN F. ANNEGERS, PH.D., W. ALLEN HAUSER, M.D., SHARON P. COAN, M.S., AND WALTER A. ROCCA, M.D., M.P.H. ABSTRACT Background The risk
A POPULATION-BASED STUDY OF SEIZURES AFTER TRAUMATIC BRAIN INJURIES JOHN F. ANNEGERS, PH.D., W. ALLEN HAUSER, M.D., SHARON P. COAN, M.S., AND WALTER A. ROCCA, M.D., M.P.H. ABSTRACT Background The risk
Adherence to Head Computed Tomography Guidelines for Mild Traumatic Brain Injury
 Original Research Adherence to Head Computed Tomography Guidelines for Mild Traumatic Brain Injury Landon A. Jones, MD* Eric J. Morley, MD, MS William D. Grant, EdD* Susan M. Wojcik, PhD* William F. Paolo,
Original Research Adherence to Head Computed Tomography Guidelines for Mild Traumatic Brain Injury Landon A. Jones, MD* Eric J. Morley, MD, MS William D. Grant, EdD* Susan M. Wojcik, PhD* William F. Paolo,