Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth. Objectives 11/7/2017
|
|
|
- Reginald Patrick
- 6 years ago
- Views:
Transcription

1 Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth Objectives 1. Be able to discuss brain anatomy and physiology as it applies to traumatic brain injury 2. Be able to discuss different types of injuries to the brain 3. Be able to discuss different surgical interventions to treat brain injuries 4. Be able to discuss various medical interventions to treat brain injuries 1
 Guidelines for the Management of Severe Traumatic Brain Injury 3 rd Edition (2007) Evidence Based treatments Class I Evidence: Good")

2 Resources Guidelines for the Acute Medical Management of Severe Traumatic Brain Injury in Infants, Children, and Adolescents Second Edition (2012) Guidelines for the Management of Severe Traumatic Brain Injury 3 rd Edition (2007) Evidence Based treatments Class I Evidence: Good quality Prospective Randomized Controlled Trial (RCT) Class II Evidence: Moderate or poor quality RCT or Good-Quality cohort or goodquality Case control Class III Evidence: Moderate or poor-quality RCT or cohort; Moderate or poor-quality case-control; case series, databases, registries, expert opinion 2
3 Modified Monro-Kellie hypothesis The sum of the intracranial volumes of blood, brain, and CSF and other components (ie blood clot, tumor) is constant and that an increase in any one of these must be offset by an equal decrease in another, or else the pressure in the closed inelastic cranium will rise and pressure is distributed evenly throughout the intracranial cavity. Glasgow Coma Scale (GCS) Points Best eye Best verbal Best motor obeys 5 - oriented localizes 4 spontaneous confused Withdraws to pain 3 To speech inappropriate Flexor (decorticate) 2 To pain incomprehensibl e 1 none none none Extensor (decerebrate) 3
4 Head injury severity Mild: GCS Moderate: GCS 9-13 Severe: GCS 3-8 Initial assessment of TBI 1. ABCs (hypoxia, airway, hypotension, anemia, etc) 2. Seizures 3. Infection? 4. Spine injury 4
5 ICP management principles and considerations 1. HOB 30 degrees, head midline 2. Temperature (level II evidence moderate hypothermia degree C (89-91 degrees F) 3. Mass lesion (ie hematoma), consider decompressive craniectomy 4. Hyperventilation: level III evidence, not below PCO2 30 mm Hg, avoid elevated pco2 5. Mannitol/hypertonic saline 3% 6. Ventriculostomy/lumbar drainage/csf drainage 7. Consider seizures as cause, consider seizure prophylaxis 8. Sedation and neuromuscular blockade; no propofol on infants and children 9. Barbiturates an option to consider, level III evidence 10. CPP = MAP ICP, minimum 40 mm Hg in children 11. Treat ICP greater than 20 mm Hg Neurological exam 1. visual exam: external trauma, scalp, ears, raccoon s eyes, facial fractures 2. carotid and orbital auscultation 3. cranial nerve exam 4. level of consciousness, communication, orientation 5. motor exam 6. sensory exam 7. Reflexes Definitions: Concussion Contusion (cerebral) Contrecoup injury Diffuse axonal injury (DAI) Basilar skull fracture Subdural hematoma Epidural hematoma Traumatic intracerebral hemorrhage 5

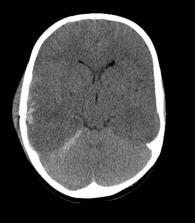
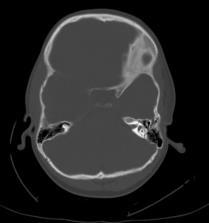
6 6/28 3 ½ year old boy fell from barn loft ladder onto concrete. LOC at scene. Brief CPR from bystanders at the scene. He was hemodynamically stable at scene and en route to hospital. Best neurological exam before sedation/paralysis was described as posturing type movement. Head CT performed Right temporal and frontal skull fracture and underlying acute subdural hematoma 6


7 7

8 8


9 1. Left frontal twist drill and placement of ventricular drain. 2. Right frontotemperoparietal craniectomy and evacuation of subdural hematoma 3. Bone flap left off and placed in right abdominal wall subcutaneous pocket 9


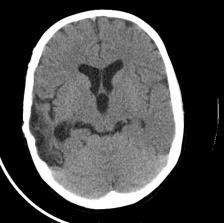
10 Remained intubated To PICU Sedated, neuromuscular blockade Head CT post-op day 1 10

11 Post-op day 1 ICPs overnight EVD 15 cc/hr of CSF Versed, Norcuron, Fentanyl drips Post-op day 2 Tmax up to 102, very bad ICPs up mm Hg Coughing and moving with stimulation CPP = MAP ICP Goal CPP of 40, so goal MAP of 70 Augment BP Add prn Mannitol CT head with open cisterns, collapsed ventricular system Bronchoscopy for mucous plug and atelectasis 11
12 Post-op day 7 Transitioned from mannitol prn to 3%NaCl drip around POD 4. ICPs 20 Serum Na stable at 148 Tolerating feedings, transpyloric Stopped Neuromuscular blocker and weaning sedation Post-op day 9 Opens eyes, moving some MRI for prognostic purposes Slowly raising EVD to wean off 12

13 Post-op day EVD removed Sitting up, purposeful movement, eyes open Progressed to some PO intake Post-op day Fitted with helmet Eating Talking Left leg drags a little with walking Needs significant assistance to walk Home at request of parents with outpatient therapies 13

14 Electively re-admitted about one month post injury for replacement of bone flap Discharged on postop day 2 Will continue helmet for 8 more weeks 14

15 15

16 Returned for office follow-up two months after bone flap replacement with increased fluid under scalp and mobile bone flap Horsing around with brothers and sisters Return to OR with repair of dura and revision of cranial flap 16

17 At 3 months, 4 months, and 7 months post-op office visits his scalp and bone flap have healed Now out of helmet CT showed good healing Now just over 5 years old Swings left leg slightly but doing well 17
8/29/2011. Brain Injury Incidence: 200/100,000. Prehospital Brain Injury Mortality Incidence: 20/100,000
 Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
PRACTICE GUIDELINE. DEFINITIONS: Mild head injury: Glasgow Coma Scale* (GCS) score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8
 score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8") PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
HEAD INJURY. Dept Neurosurgery
 HEAD INJURY Dept Neurosurgery INTRODUCTION PATHOPHYSIOLOGY CLINICAL CLASSIFICATION MANAGEMENT - INVESTIGATIONS - TREATMENT INTRODUCTION Most head injuries are due to an impact between the head and another
HEAD INJURY Dept Neurosurgery INTRODUCTION PATHOPHYSIOLOGY CLINICAL CLASSIFICATION MANAGEMENT - INVESTIGATIONS - TREATMENT INTRODUCTION Most head injuries are due to an impact between the head and another
Traumatic Brain Injuries
 Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
Traumatic Brain Injury:
 Traumatic Brain Injury: Changes in Management Across the Spectrum of Age and Time Omaha 2018 Trauma Symposium June 15, 2018 Gail T. Tominaga, M.D., F.A.C.S. Scripps Memorial Hospital La Jolla Outline Background
Traumatic Brain Injury: Changes in Management Across the Spectrum of Age and Time Omaha 2018 Trauma Symposium June 15, 2018 Gail T. Tominaga, M.D., F.A.C.S. Scripps Memorial Hospital La Jolla Outline Background
Case 1. Case 5/30/2013. Traumatic Brain Injury : Review, Update, and Controversies
 Case 1 Traumatic Brain Injury : Review, Update, and Controversies Shirley I. Stiver MD, PhD 32 year old male s/p high speed MVA Difficult extrication Intubated at scene Case BP 75 systolic / palp GCS 3
Case 1 Traumatic Brain Injury : Review, Update, and Controversies Shirley I. Stiver MD, PhD 32 year old male s/p high speed MVA Difficult extrication Intubated at scene Case BP 75 systolic / palp GCS 3
Traumatic Brain Injury
 Traumatic Brain Injury Mark J. Harris M.D. Associate Professor University of Utah Salt Lake City USA Overview In US HI responsible for 33% trauma deaths. Closed HI 80% Missile / Penetrating HI 20% Glasgow
Traumatic Brain Injury Mark J. Harris M.D. Associate Professor University of Utah Salt Lake City USA Overview In US HI responsible for 33% trauma deaths. Closed HI 80% Missile / Penetrating HI 20% Glasgow
Introduction to Neurosurgical Subspecialties:
 Introduction to Neurosurgical Subspecialties: Trauma and Critical Care Neurosurgery Brian L. Hoh, MD 1, Gregory J. Zipfel, MD 2 and Stacey Q. Wolfe, MD 3 1 University of Florida, 2 Washington University,
Introduction to Neurosurgical Subspecialties: Trauma and Critical Care Neurosurgery Brian L. Hoh, MD 1, Gregory J. Zipfel, MD 2 and Stacey Q. Wolfe, MD 3 1 University of Florida, 2 Washington University,
Standardize comprehensive care of the patient with severe traumatic brain injury
 Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Pre-hospital Response to Trauma and Brain Injury. Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center
 Pre-hospital Response to Trauma and Brain Injury Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center Traumatic Brain Injury is Common 235,000 Americans hospitalized for non-fatal TBI
Pre-hospital Response to Trauma and Brain Injury Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center Traumatic Brain Injury is Common 235,000 Americans hospitalized for non-fatal TBI
Pediatric Head Trauma August 2016
 PEDIATRIC HEAD TRAUMA AUGUST 2016 Pediatric Head Trauma August 2016 EDUCATION COMMITTEE PEER EDUCATION Quick Review of Pathophysiology of TBI Nuggets of knowledge to keep in mind with TBI Intracranial
PEDIATRIC HEAD TRAUMA AUGUST 2016 Pediatric Head Trauma August 2016 EDUCATION COMMITTEE PEER EDUCATION Quick Review of Pathophysiology of TBI Nuggets of knowledge to keep in mind with TBI Intracranial
8th Annual NKY TBI Conference 3/28/2014
 Closed Head Injury: Headache to Herniation A N T H O N Y T. K R A M E R U N I V E R S I T Y O F C I N C I N N A T I B L U E A S H E M S T E C H N O L O G Y P R O G R A M Objectives Describe the pathological
Closed Head Injury: Headache to Herniation A N T H O N Y T. K R A M E R U N I V E R S I T Y O F C I N C I N N A T I B L U E A S H E M S T E C H N O L O G Y P R O G R A M Objectives Describe the pathological
10/6/2017. Notice. Traumatic Brain Injury & Head Trauma
 Notice All EMS Live@Nite presentations will be recorded (both audio and video) and available for public viewing online. By participating in EMS Live@Nite, you consent to audio and video recording and its/their
Notice All EMS Live@Nite presentations will be recorded (both audio and video) and available for public viewing online. By participating in EMS Live@Nite, you consent to audio and video recording and its/their
TBI are twice as common in males High potential for poor outcome Deaths occur at three points in time after injury
 Head Injury Any trauma to (closed vs. open) Skull Scalp Brain Traumatic brain injury (TBI) High incidence Most common causes Falls Motor vehicle accidents Other causes Firearm- related injuries Assaults
Head Injury Any trauma to (closed vs. open) Skull Scalp Brain Traumatic brain injury (TBI) High incidence Most common causes Falls Motor vehicle accidents Other causes Firearm- related injuries Assaults
Neuroprotective Effects for TBI. Craig Williamson, MD
 Neuroprotective Effects for TBI Craig Williamson, MD Neuroprotection in Traumatic Brain Injury Craig Williamson Clinical Assistant Professor Neurocritical Care Fellowship Director Disclosures I will discuss
Neuroprotective Effects for TBI Craig Williamson, MD Neuroprotection in Traumatic Brain Injury Craig Williamson Clinical Assistant Professor Neurocritical Care Fellowship Director Disclosures I will discuss
Head injuries. Severity of head injuries
 Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
Pediatric Trauma Initial Evaluation and management
 Pediatric Trauma Initial Evaluation and management Head Injury Closed head injury Penetrating head injury Closed Head Injury without Fractures Head injury is the most common cause of death and disability
Pediatric Trauma Initial Evaluation and management Head Injury Closed head injury Penetrating head injury Closed Head Injury without Fractures Head injury is the most common cause of death and disability
SUBJECT: Clinical Practice Guideline for the Management of Severe Traumatic Brain Injury
 ASPIRUS WAUSAU HOSPITAL, INC. Passion for excellence. Compassion for people. Effective Date: December 1, 2005 Proposed By: Samuel Picone III, MD, Trauma Medical Director Approval and Dates: Dr. Bunch,
ASPIRUS WAUSAU HOSPITAL, INC. Passion for excellence. Compassion for people. Effective Date: December 1, 2005 Proposed By: Samuel Picone III, MD, Trauma Medical Director Approval and Dates: Dr. Bunch,
Traumatic Brain Injury
 General Information Traumatic Brain Injury What you need to know Complicated condition with high variability in etiology, severity, distribution of injury, and pattern of functional impairment (Klyce,
General Information Traumatic Brain Injury What you need to know Complicated condition with high variability in etiology, severity, distribution of injury, and pattern of functional impairment (Klyce,
Neurocritical Care Basics. Tapan Kavi, MD Christina Fox, RN
 Neurocritical Care Basics Tapan Kavi, MD Christina Fox, RN GOAL 1: DON T LET THE PATIENT DIE Not unique ACLS, ATLS, ENLS, other strategies common to all emergency medical care ABCs MORE not less important
Neurocritical Care Basics Tapan Kavi, MD Christina Fox, RN GOAL 1: DON T LET THE PATIENT DIE Not unique ACLS, ATLS, ENLS, other strategies common to all emergency medical care ABCs MORE not less important
9/19/2011. Damien Beilman, RRT Adult Clinical Specialist Wesley Medical Center. Epidural Hematoma: Lens Shaped.
 Damien Beilman, RRT Adult Clinical Specialist Wesley Medical Center Epidural Hematoma: Lens Shaped. 1 Epidural Hematoma Subdural Hematoma: Crescent-shaped Subdural Hematoma 2 Cerebral Contusion Cause of
Damien Beilman, RRT Adult Clinical Specialist Wesley Medical Center Epidural Hematoma: Lens Shaped. 1 Epidural Hematoma Subdural Hematoma: Crescent-shaped Subdural Hematoma 2 Cerebral Contusion Cause of
Disclosure Statement. Dr. Kadish has no relevant financial relationships with any commercial interests mentioned in this talk.
 Disclosure Statement Dr. Kadish has no relevant financial relationships with any commercial interests mentioned in this talk. Head Trauma Evaluation Primary and secondary injury Disposition Sports related
Disclosure Statement Dr. Kadish has no relevant financial relationships with any commercial interests mentioned in this talk. Head Trauma Evaluation Primary and secondary injury Disposition Sports related
Michael Avant, M.D. The Children s Hospital of GHS
 Michael Avant, M.D. The Children s Hospital of GHS OVERVIEW ER to ICU Transition Early Management Priorities the First 48 hours Organ System Support Complications THE FIRST 48 HOURS Communication Damage
Michael Avant, M.D. The Children s Hospital of GHS OVERVIEW ER to ICU Transition Early Management Priorities the First 48 hours Organ System Support Complications THE FIRST 48 HOURS Communication Damage
Neurosurgery Review. Mudit Sharma, MD May 16 th, 2008
 Neurosurgery Review Mudit Sharma, MD May 16 th, 2008 Dr. Mudit Sharma, Neurosurgeon Manassas, Fredericksburg, Virginia http://www.virginiaspinespecialists.com Phone: 1-855-SPINE FIX (774-6334) Fundamentals
Neurosurgery Review Mudit Sharma, MD May 16 th, 2008 Dr. Mudit Sharma, Neurosurgeon Manassas, Fredericksburg, Virginia http://www.virginiaspinespecialists.com Phone: 1-855-SPINE FIX (774-6334) Fundamentals
Moron General Hospital Ciego de Avila Cuba. Department of Neurological Surgery
 Moron General Hospital Ciego de Avila Cuba Department of Neurological Surgery Early decompressive craniectomy in severe head injury with intracranial hypertension Angel J. Lacerda MD PhD, Daisy Abreu MD,
Moron General Hospital Ciego de Avila Cuba Department of Neurological Surgery Early decompressive craniectomy in severe head injury with intracranial hypertension Angel J. Lacerda MD PhD, Daisy Abreu MD,
Index. Note: Page numbers of article titles are in bold face type.
 Neurosurg Clin N Am 13 (2002) 259 264 Index Note: Page numbers of article titles are in bold face type. A Abdominal injuries, in child abuse, 150, 159 Abrasions, in child abuse, 157 Abuse, child. See Child
Neurosurg Clin N Am 13 (2002) 259 264 Index Note: Page numbers of article titles are in bold face type. A Abdominal injuries, in child abuse, 150, 159 Abrasions, in child abuse, 157 Abuse, child. See Child
Introduction to Emergency Medical Care 1
 Introduction to Emergency Medical Care 1 OBJECTIVES 31.1 Define key terms introduced in this chapter. Slides 13 15, 17, 19, 28 31.2 Describe the components and function of the nervous system and the anatomy
Introduction to Emergency Medical Care 1 OBJECTIVES 31.1 Define key terms introduced in this chapter. Slides 13 15, 17, 19, 28 31.2 Describe the components and function of the nervous system and the anatomy
Head Trauma Inservice (October)
") John Tramell - Head Trauma Inservice, October 2005.doc Page 1 Head Trauma Inservice (October) Head trauma is the leading cause of death in trauma patients. Having a basic understanding of the anatomy and
John Tramell - Head Trauma Inservice, October 2005.doc Page 1 Head Trauma Inservice (October) Head trauma is the leading cause of death in trauma patients. Having a basic understanding of the anatomy and
North Oaks Trauma Symposium Friday, November 3, 2017
 Traumatic Intracranial Hemorrhage Aaron C. Sigler, DO, MS Neurosurgery Tulane Neurosciences None Disclosures Overview Anatomy Epidural hematoma Subdural hematoma Cerebral contusions Outline Traumatic ICH
Traumatic Intracranial Hemorrhage Aaron C. Sigler, DO, MS Neurosurgery Tulane Neurosciences None Disclosures Overview Anatomy Epidural hematoma Subdural hematoma Cerebral contusions Outline Traumatic ICH
North Oaks Trauma Symposium Friday, November 3, 2017
 + Evaluation and Management of Facial Trauma D Antoni Dennis, MD North Oaks ENT an Allergy November 3, 2017 + Financial Disclosure I do not have any conflicts of interest or financial interest to disclose
+ Evaluation and Management of Facial Trauma D Antoni Dennis, MD North Oaks ENT an Allergy November 3, 2017 + Financial Disclosure I do not have any conflicts of interest or financial interest to disclose
Chapter 26 Head and Spine Trauma The Nervous System The nervous system controls virtually all of our body activities including reflex, voluntary and
 1 2 3 4 5 Chapter 26 Head and Spine Trauma The Nervous System The nervous system controls virtually all of our body activities including reflex, voluntary and involuntary activities Voluntary activities
1 2 3 4 5 Chapter 26 Head and Spine Trauma The Nervous System The nervous system controls virtually all of our body activities including reflex, voluntary and involuntary activities Voluntary activities
Traumatic Brain Injury Pathways for Adult ED Patients Being Admitted to Trauma Service
 tic Brain Injury Pathways for Adult ED Patients Being Admitted to Service Revision Team Tyler W. Barrett, MD, MSCI Elizabeth S. Compton, NP Bradley M. Dennis, MD Oscar D. Guillamondegui, MD, MPH Michael
tic Brain Injury Pathways for Adult ED Patients Being Admitted to Service Revision Team Tyler W. Barrett, MD, MSCI Elizabeth S. Compton, NP Bradley M. Dennis, MD Oscar D. Guillamondegui, MD, MPH Michael
Mild Traumatic Brain Injury
 Mild Traumatic Brain Injury Concussions This presentation is for information purposes only, not for any commercial purpose, and may not be sold or redistributed. David Wesley, M.D. Outline Epidemiology
Mild Traumatic Brain Injury Concussions This presentation is for information purposes only, not for any commercial purpose, and may not be sold or redistributed. David Wesley, M.D. Outline Epidemiology
Update on Guidelines for Traumatic Brain Injury
 Update on Guidelines for Traumatic Brain Injury Current TBI Guidelines Shirley I. Stiver MD, PhD Department of Neurosurgery Guidelines for the management of traumatic brain injury Journal of Neurotrauma
Update on Guidelines for Traumatic Brain Injury Current TBI Guidelines Shirley I. Stiver MD, PhD Department of Neurosurgery Guidelines for the management of traumatic brain injury Journal of Neurotrauma
Traumatic brain Injury- An open eye approach
 Traumatic brain Injury- An open eye approach Dr. Sunit Dr Sunit, Apollo children's hospital Blah blah Lots of head injury Lot of ill children Various methods of injury Various mechanisms of brain damage
Traumatic brain Injury- An open eye approach Dr. Sunit Dr Sunit, Apollo children's hospital Blah blah Lots of head injury Lot of ill children Various methods of injury Various mechanisms of brain damage
LOSS OF CONSCIOUSNESS & ASSESSMENT. Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT
 LOSS OF CONSCIOUSNESS & ASSESSMENT Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT OUTLINE Causes Head Injury Clinical Features Complications Rapid Assessment Glasgow Coma Scale Classification
LOSS OF CONSCIOUSNESS & ASSESSMENT Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT OUTLINE Causes Head Injury Clinical Features Complications Rapid Assessment Glasgow Coma Scale Classification
Chapter 31. Objectives. Objectives 01/09/2013. Head Trauma
 Chapter 31 Head Trauma Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1. Define key terms introduced
Chapter 31 Head Trauma Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1. Define key terms introduced
ICP. A Stepwise Approach. Stephan A. Mayer, MD Professor, Neurology & Neurosurgery Director, Neurocritical Care, Mount Sinai Health System
 ICP A Stepwise Approach Stephan A. Mayer, MD Professor, Neurology & Neurosurgery Director, Neurocritical Care, Mount Sinai Health System ICP: Basic Concepts Monroe-Kellie doctrine: skull = fixed volume
ICP A Stepwise Approach Stephan A. Mayer, MD Professor, Neurology & Neurosurgery Director, Neurocritical Care, Mount Sinai Health System ICP: Basic Concepts Monroe-Kellie doctrine: skull = fixed volume
Trauma is the leading cause of death in the first four decades of life, with head injury being
 Correspondence to: Mr PJ Hutchinson, Academic Department of Neurosurgery, University of Cambridge, Box 167, Addenbrooke s Hospital, Cambridge CB2 2QQ, UK: p.hutch@which.net ACUTE HEAD INJURY FOR THE NEUROLOGIST
Correspondence to: Mr PJ Hutchinson, Academic Department of Neurosurgery, University of Cambridge, Box 167, Addenbrooke s Hospital, Cambridge CB2 2QQ, UK: p.hutch@which.net ACUTE HEAD INJURY FOR THE NEUROLOGIST
TRAUMATIC BRAIN INJURY. Moderate and Severe Brain Injury
 TRAUMATIC BRAIN INJURY Moderate and Severe Brain Injury Disclosures Funded research: 1. NIH: RO1 Physiology of concussion 2016-2021, Co-PI, $2,000,000 2. American Medical Society of Sports Medicine: RCT
TRAUMATIC BRAIN INJURY Moderate and Severe Brain Injury Disclosures Funded research: 1. NIH: RO1 Physiology of concussion 2016-2021, Co-PI, $2,000,000 2. American Medical Society of Sports Medicine: RCT
Head injury in children
 Head injury in children Michael Kim, MD Department of Emergency Medicine University of Wisconsin- Madison #1 cause of death and disability Bimodal distribution 62,000 hospitalization 564,000 ED visits
Head injury in children Michael Kim, MD Department of Emergency Medicine University of Wisconsin- Madison #1 cause of death and disability Bimodal distribution 62,000 hospitalization 564,000 ED visits
Injuries to the head and spine
 Injuries to the head and spine Aaron J. Katz, AEMT-P, CIC www.es26medic.net 2013 Nervous System Two sub-systems Central Nervous System ( CNS ) Brain and spinal cord Peripheral Nervous System 12 cranial
Injuries to the head and spine Aaron J. Katz, AEMT-P, CIC www.es26medic.net 2013 Nervous System Two sub-systems Central Nervous System ( CNS ) Brain and spinal cord Peripheral Nervous System 12 cranial
Update sulle lesioni emorragiche posttraumatiche
 Update sulle lesioni emorragiche posttraumatiche Corrado Iaccarino Neurochirurgia-Neurotraumatologia AOU Parma Neurochirurgia d'urgenza IRCCS ASMN Reggio Emilia LAW UPDATING This document provides recommendations
Update sulle lesioni emorragiche posttraumatiche Corrado Iaccarino Neurochirurgia-Neurotraumatologia AOU Parma Neurochirurgia d'urgenza IRCCS ASMN Reggio Emilia LAW UPDATING This document provides recommendations
Traumatic Brain Injury Pathway, GCS 15 Closed head injury
 Traumatic Brain Injury Pathway, GCS 15 Closed head injury Plus Any One of the Following Mild TBI 2010 Consensus Definition of TBI from CDC, NINDS, NIDDR, VA, DVBIC, DCoE Plus Any One of the Following New
Traumatic Brain Injury Pathway, GCS 15 Closed head injury Plus Any One of the Following Mild TBI 2010 Consensus Definition of TBI from CDC, NINDS, NIDDR, VA, DVBIC, DCoE Plus Any One of the Following New
Most hypertensive: headache, vomiting, seizures, changes in mental status, fever, changes EKG
 Wk 2. Management of Clients with Stroke 1. Stroke neurologic changes by interruption in blood supply to brain 1) Etiology Ischemia: thrombosis or embolism thrombotic strokes > embolic strokes (1) Thrombosis
Wk 2. Management of Clients with Stroke 1. Stroke neurologic changes by interruption in blood supply to brain 1) Etiology Ischemia: thrombosis or embolism thrombotic strokes > embolic strokes (1) Thrombosis
INTRACRANIAL PRESSURE -!!
 INTRACRANIAL PRESSURE - Significance raised ICP main cause of death in severe head injury main cause of morbidity in moderate and mild head injury main target and prognostic indicator in the ITU setting
INTRACRANIAL PRESSURE - Significance raised ICP main cause of death in severe head injury main cause of morbidity in moderate and mild head injury main target and prognostic indicator in the ITU setting
Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University
 Dr Mubarak Abdelrahman Assistant Professor Jazan University") Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University SHOCK Definition: Shock is a syndrome = inability to provide sufficient oxygenated blood to tissues. Oxygen
Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University SHOCK Definition: Shock is a syndrome = inability to provide sufficient oxygenated blood to tissues. Oxygen
Head injuries in children. Dr Jason Hort Paediatrician Paediatric Emergency Physician, June 2017 Children s Hospital Westmead
 Head injuries in children Dr Jason Hort Paediatrician Paediatric Emergency Physician, June 2017 Children s Hospital Westmead Objectives Approach to minor head injury Child protection issues Concussion
Head injuries in children Dr Jason Hort Paediatrician Paediatric Emergency Physician, June 2017 Children s Hospital Westmead Objectives Approach to minor head injury Child protection issues Concussion
Head & Brain Trauma. Presented By: Steven Jones, NREMT-P
 Head & Brain Trauma Presented By: Steven Jones, NREMT-P Head & Brain Trauma ~ 4 million head injuries in US per year ~ 450,000 require hospitalization Most are minor injuries Major head injury most common
Head & Brain Trauma Presented By: Steven Jones, NREMT-P Head & Brain Trauma ~ 4 million head injuries in US per year ~ 450,000 require hospitalization Most are minor injuries Major head injury most common
Traumatic Brain Injury (1.2.3) Management of severe TBI ( ) Learning Objectives
 Management of severe TBI ( ) Learning Objectives") Traumatic Brain Injury (1.2.3) 1.2.3.1 Management of severe TBI 1.2.3.2 Management of concussions 1.2.3.3 Sideline management for team medics/physicians 1.4.2.3.10 Controlled hyperventilation for management
Traumatic Brain Injury (1.2.3) 1.2.3.1 Management of severe TBI 1.2.3.2 Management of concussions 1.2.3.3 Sideline management for team medics/physicians 1.4.2.3.10 Controlled hyperventilation for management
INCREASED INTRACRANIAL PRESSURE
 INCREASED INTRACRANIAL PRESSURE Sheba Medical Center, Acute Medicine Department Irene Frantzis P-Year student SGUL 2013 Normal Values Normal intracranial volume: 1700 ml Volume of brain: 1200-1400 ml CSF:
INCREASED INTRACRANIAL PRESSURE Sheba Medical Center, Acute Medicine Department Irene Frantzis P-Year student SGUL 2013 Normal Values Normal intracranial volume: 1700 ml Volume of brain: 1200-1400 ml CSF:
Correlation of D-Dimer level with outcome in traumatic brain injury
 2014; 17 (1) Original Article Correlation of D-Dimer level with outcome in traumatic brain injury Pradip Prasad Subedi 1, Sushil Krishna Shilpakar 2 Email: Abstract Introduction immense. The major determinant
2014; 17 (1) Original Article Correlation of D-Dimer level with outcome in traumatic brain injury Pradip Prasad Subedi 1, Sushil Krishna Shilpakar 2 Email: Abstract Introduction immense. The major determinant
Severe traumatic brain injury. Fellowship Training Intensive Care Radboud University Nijmegen Medical Centre
 Severe traumatic brain injury Fellowship Training Intensive Care Radboud University Nijmegen Medical Centre Primary focus of care Prevent ischemia, hypoxia and hypoglycemia Nutrient & oxygen supply Limited
Severe traumatic brain injury Fellowship Training Intensive Care Radboud University Nijmegen Medical Centre Primary focus of care Prevent ischemia, hypoxia and hypoglycemia Nutrient & oxygen supply Limited
10. Severe traumatic brain injury also see flow chart Appendix 5
 10. Severe traumatic brain injury also see flow chart Appendix 5 Introduction Severe traumatic brain injury (TBI) is the leading cause of death in children in the UK, accounting for 15% of deaths in 1-15
10. Severe traumatic brain injury also see flow chart Appendix 5 Introduction Severe traumatic brain injury (TBI) is the leading cause of death in children in the UK, accounting for 15% of deaths in 1-15
H Alex Choi, MD MSc Assistant Professor of Neurology and Neurosurgery The University of Texas Health Science Center Mischer Neuroscience Institute
 H Alex Choi, MD MSc Assistant Professor of Neurology and Neurosurgery The University of Texas Health Science Center Mischer Neuroscience Institute Memorial Hermann- Texas Medical Center Learning Objectives
H Alex Choi, MD MSc Assistant Professor of Neurology and Neurosurgery The University of Texas Health Science Center Mischer Neuroscience Institute Memorial Hermann- Texas Medical Center Learning Objectives
Head Injury כל הזכויות שמורות למד"א מרחב ירושלים. Dan Drory, EMT-P, Instructor
 Head Injury Dan Drory, EMT-P, Instructor Anatomy on a fingertip The brain is a soft and gentle tissue. The brain is the most important organ. כל הזכויות שמורות למד"א מרחב ירושלים Protective layers of the
Head Injury Dan Drory, EMT-P, Instructor Anatomy on a fingertip The brain is a soft and gentle tissue. The brain is the most important organ. כל הזכויות שמורות למד"א מרחב ירושלים Protective layers of the
Chapter 57: Nursing Management: Acute Intracranial Problems
 Chapter 57: Nursing Management: Acute Intracranial Problems NORMAL INTRACRANIAL PRESSURE Intracranial pressure (ICP) is the hydrostatic force measured in the brain CSF compartment. Normal ICP is the total
Chapter 57: Nursing Management: Acute Intracranial Problems NORMAL INTRACRANIAL PRESSURE Intracranial pressure (ICP) is the hydrostatic force measured in the brain CSF compartment. Normal ICP is the total
Supplementary Online Content
 Supplementary Online Content Cooper DJ, Nichol A, Bailey M, et al. Effect of early sustained prophylactic hypothermia on neurologic outcomes among patients with severe traumatic brain injury: the POLAR
Supplementary Online Content Cooper DJ, Nichol A, Bailey M, et al. Effect of early sustained prophylactic hypothermia on neurologic outcomes among patients with severe traumatic brain injury: the POLAR
D is for Disability Altered Mental Status in Children
 D is for Disability Altered Mental Status in Children Joshua Ross, MD, FAAP Pediatric Emergency Medicine Emergency Care and Trauma Symposium June 22, 2015 Objectives Describe a basic approach to evaluating
D is for Disability Altered Mental Status in Children Joshua Ross, MD, FAAP Pediatric Emergency Medicine Emergency Care and Trauma Symposium June 22, 2015 Objectives Describe a basic approach to evaluating
Measuring severity of TBI. Traumatic Brain injury: TBI. Glasgow Coma Scale & score. Glasgow coma scale/score. Glasgow coma scale with score (GCS)
") Measuring severity of TBI Glasgow coma scale with score (GCS) ก กก functional outcome Post traumatic Amnesia (PTA) cognitive & functional deficit Assist. Prof.Savai Norasan First National Neuroscience
Measuring severity of TBI Glasgow coma scale with score (GCS) ก กก functional outcome Post traumatic Amnesia (PTA) cognitive & functional deficit Assist. Prof.Savai Norasan First National Neuroscience
The Child with Alterations in Cerebral Function
 The Child with Alterations in Cerebral Function Neurologic Assessment VS HR, BP, Respirations, Temperature LOC Orientation Pediatric Glasgow Coma Scale Eyes Pupillary response and movement, extraoccular
The Child with Alterations in Cerebral Function Neurologic Assessment VS HR, BP, Respirations, Temperature LOC Orientation Pediatric Glasgow Coma Scale Eyes Pupillary response and movement, extraoccular
Kristin s Head Trauma Board Questions 11/07/14
 Kristin s Head Trauma Board Questions { 11/07/14 A healthy 15 y/o boy was playing football at a park near his home with a group of friends when he tripped over a friend s leg while trying to catch a pass.
Kristin s Head Trauma Board Questions { 11/07/14 A healthy 15 y/o boy was playing football at a park near his home with a group of friends when he tripped over a friend s leg while trying to catch a pass.
Introduction and Overview of Pediatric Traumatic Brain Injury: Current status and future directions. Kids are Different. Primary Injury 3/12/2012
 Pediatric Traumatic Brain Injury Numbers Introduction and Overview of Pediatric Traumatic Brain Injury: Current status and future directions Richard A. Falcone, Jr, MD, MPH Director, Trauma Services Co-director,
Pediatric Traumatic Brain Injury Numbers Introduction and Overview of Pediatric Traumatic Brain Injury: Current status and future directions Richard A. Falcone, Jr, MD, MPH Director, Trauma Services Co-director,
European Resuscitation Council
 European Resuscitation Council Incidence of Trauma in Childhood Leading cause of death and disability in children older than one year all over the world Structured approach Primary survey and resuscitation
European Resuscitation Council Incidence of Trauma in Childhood Leading cause of death and disability in children older than one year all over the world Structured approach Primary survey and resuscitation
PEDIATRIC MILD TRAUMATIC HEAD INJURY
 PEDIATRIC MILD TRAUMATIC HEAD INJURY October 2011 Quality Improvement Resources Illinois Emergency Medical Services for Children is a collaborative program between the Illinois Department of Public Health
PEDIATRIC MILD TRAUMATIC HEAD INJURY October 2011 Quality Improvement Resources Illinois Emergency Medical Services for Children is a collaborative program between the Illinois Department of Public Health
Paediatric Neurosurgical Emergencies. Kate Parkins Consultant Paediatric Intensivist Alder Hey
 Paediatric Neurosurgical Emergencies Kate Parkins Consultant Paediatric Intensivist Alder Hey Level of consciousness AVPU GCS D Neurological Assessment Pupillary reaction to light Limb movements History
Paediatric Neurosurgical Emergencies Kate Parkins Consultant Paediatric Intensivist Alder Hey Level of consciousness AVPU GCS D Neurological Assessment Pupillary reaction to light Limb movements History
Traumatic brain injuries are caused by external mechanical forces such as: - Falls - Transport-related accidents - Assault
 PP2231 Brain injury Cerebrum consists of frontal, parietal, occipital and temporal lobes Diencephalon consists of thalamus, hypothalamus Cerbellum Brain stem consists of midbrain, pons, medulla Central
PP2231 Brain injury Cerebrum consists of frontal, parietal, occipital and temporal lobes Diencephalon consists of thalamus, hypothalamus Cerbellum Brain stem consists of midbrain, pons, medulla Central
Anesthetic Management of a Patient with Traumatic Brain Injury
 Anesthetic Management of a Patient with Traumatic Brain Injury Arne O. Budde, MD, DEAA Associate Professor of Anesthesiology Director, Division of Neuroanesthesia Department of Anesthesiology Milton S
Anesthetic Management of a Patient with Traumatic Brain Injury Arne O. Budde, MD, DEAA Associate Professor of Anesthesiology Director, Division of Neuroanesthesia Department of Anesthesiology Milton S
BATLS Battlefield Advanced Trauma Life Support
 J R Army Med Corps 2002; 148: 151-158 BATLS Battlefield Advanced Trauma Life Support CHAPTER 8 HEAD INJURIES Aim 0801. On successfully completing this topic you will be able to: Discuss general management
J R Army Med Corps 2002; 148: 151-158 BATLS Battlefield Advanced Trauma Life Support CHAPTER 8 HEAD INJURIES Aim 0801. On successfully completing this topic you will be able to: Discuss general management
Strong, flexible mass of: Skin Fascia tissue Highly provides insulation
 1 Chapter 23 Head, Facial, & Neck Trauma 2 Introduction to Head, Facial, & Neck Injuries Common major trauma 4 million people experience head trauma annually Severe injury is most frequent cause of trauma
1 Chapter 23 Head, Facial, & Neck Trauma 2 Introduction to Head, Facial, & Neck Injuries Common major trauma 4 million people experience head trauma annually Severe injury is most frequent cause of trauma
Perioperative Management Of Extra-Ventricular Drains (EVD)
") Perioperative Management Of Extra-Ventricular Drains (EVD) Dr. Vijay Tarnal MBBS, FRCA Clinical Assistant Professor Division of Neuroanesthesiology Division of Head & Neck Anesthesiology Michigan Medicine
Perioperative Management Of Extra-Ventricular Drains (EVD) Dr. Vijay Tarnal MBBS, FRCA Clinical Assistant Professor Division of Neuroanesthesiology Division of Head & Neck Anesthesiology Michigan Medicine
Rhonda Dixon, DVM Section Head, Emergency and Critical Care Sugar Land Veterinary Specialty and Emergency
 Rhonda Dixon, DVM Section Head, Emergency and Critical Care Sugar Land Veterinary Specialty and Emergency Traumatic Brain Injury Causes Pathophysiology Neurologic assessment Therapeutic Approach Status
Rhonda Dixon, DVM Section Head, Emergency and Critical Care Sugar Land Veterinary Specialty and Emergency Traumatic Brain Injury Causes Pathophysiology Neurologic assessment Therapeutic Approach Status
Severe Traumatic Brain Injury Protocol
 Severe Traumatic Brain Injury Protocol PROTOCOL I. Objective II. Definition of Severe TBI III. Patient Care: Parameters IV. Patient Care: Management Timeline (First 7 days of TBI) V. Nursing Care: Communication
Severe Traumatic Brain Injury Protocol PROTOCOL I. Objective II. Definition of Severe TBI III. Patient Care: Parameters IV. Patient Care: Management Timeline (First 7 days of TBI) V. Nursing Care: Communication
BRAIN TRAUMA THERAPEUTIC RECOMMENDATIONS
 1 BRAIN TRAUMA THERAPEUTIC RECOMMENDATIONS Richard A. LeCouteur, BVSc, PhD, Dip ACVIM (Neurology), Dip ECVN Professor Emeritus, University of California, Davis, California, USA Definitions Hemorrhage:
1 BRAIN TRAUMA THERAPEUTIC RECOMMENDATIONS Richard A. LeCouteur, BVSc, PhD, Dip ACVIM (Neurology), Dip ECVN Professor Emeritus, University of California, Davis, California, USA Definitions Hemorrhage:
Traumatic Head Injury
 Traumatic Head Injury Liu Yi, MD. PhD, associate professor Dept. Neurosurgery Conception Any injury to the skull, or brain, caused by external physical forces, in stead of degenerative or congenital nature
Traumatic Head Injury Liu Yi, MD. PhD, associate professor Dept. Neurosurgery Conception Any injury to the skull, or brain, caused by external physical forces, in stead of degenerative or congenital nature
Virtual Mentor American Medical Association Journal of Ethics August 2008, Volume 10, Number 8:
 Virtual Mentor American Medical Association Journal of Ethics August 2008, Volume 10, Number 8: 516-520. CLINICAL PEARL The Hazards of Stopping a Brain in Motion: Evaluation and Classification of Traumatic
Virtual Mentor American Medical Association Journal of Ethics August 2008, Volume 10, Number 8: 516-520. CLINICAL PEARL The Hazards of Stopping a Brain in Motion: Evaluation and Classification of Traumatic
Post-Cardiac Arrest Syndrome. MICU Lecture Series
 Post-Cardiac Arrest Syndrome MICU Lecture Series Case 58 y/o female collapses at home, family attempts CPR, EMS arrives and notes VF, defibrillation x 3 with return of spontaneous circulation, brought
Post-Cardiac Arrest Syndrome MICU Lecture Series Case 58 y/o female collapses at home, family attempts CPR, EMS arrives and notes VF, defibrillation x 3 with return of spontaneous circulation, brought
Medical Management of Intracranial Hypertension. Joao A. Gomes, MD FAHA Head, Neurointensive Care Unit Cerebrovascular Center
 Medical Management of Intracranial Hypertension Joao A. Gomes, MD FAHA Head, Neurointensive Care Unit Cerebrovascular Center Anatomic and Physiologic Principles Intracranial compartments Brain 80% (1,400
Medical Management of Intracranial Hypertension Joao A. Gomes, MD FAHA Head, Neurointensive Care Unit Cerebrovascular Center Anatomic and Physiologic Principles Intracranial compartments Brain 80% (1,400
Mini Research Paper: Traumatic Brain Injury. Allison M McGee. Salt Lake Community College
 Running Head: Mini Research Paper: Traumatic Brain Injury Mini Research Paper: Traumatic Brain Injury Allison M McGee Salt Lake Community College Abstract A Traumatic Brain Injury (also known as a TBI)
Running Head: Mini Research Paper: Traumatic Brain Injury Mini Research Paper: Traumatic Brain Injury Allison M McGee Salt Lake Community College Abstract A Traumatic Brain Injury (also known as a TBI)
Management of Severe Traumatic Brain Injury
 Guideline for North Bristol Trust Management of Severe Traumatic Brain Injury This guideline describes the following: Initial assessment and management of the patient with head injury Indications for CT
Guideline for North Bristol Trust Management of Severe Traumatic Brain Injury This guideline describes the following: Initial assessment and management of the patient with head injury Indications for CT
11/27/2017. Stroke Management in the Neurocritical Care Unit. Conflict of interest. Karel Fuentes MD Medical Director of Neurocritical Care
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Sanders: Mosby's Paramedic Textbook, Revised 3 rd Edition PowerPoint Lecture Notes Chapter 24: Head and Facial Traumas
 Sanders: Mosby's Paramedic Textbook, Revised 3 rd Edition PowerPoint Lecture Notes Chapter 24: Head and Facial Traumas Chapter 24 Head and Facial Trauma Objectives Describe mechanism of injury, assessment,
Sanders: Mosby's Paramedic Textbook, Revised 3 rd Edition PowerPoint Lecture Notes Chapter 24: Head and Facial Traumas Chapter 24 Head and Facial Trauma Objectives Describe mechanism of injury, assessment,
Any closer to evidence based practice? Asma Salloo Chris Hani Baragwantah Academic Hospital University of Witwatersrand
 Any closer to evidence based practice? Asma Salloo Chris Hani Baragwantah Academic Hospital University of Witwatersrand Evidence Pathophysiology Why? Management Non-degenerative, Non-congenital insult
Any closer to evidence based practice? Asma Salloo Chris Hani Baragwantah Academic Hospital University of Witwatersrand Evidence Pathophysiology Why? Management Non-degenerative, Non-congenital insult
Assessment and Scoring Tools
 Assessment and Scoring Tools 2013 APGAR Scale 0 points 1 point 2 points Heart Rate Absent 100 Respiratory Rate Absent Slow, irregular Good, drying Irritability Flaccid Some flexion Active motion
Assessment and Scoring Tools 2013 APGAR Scale 0 points 1 point 2 points Heart Rate Absent 100 Respiratory Rate Absent Slow, irregular Good, drying Irritability Flaccid Some flexion Active motion
Stroke - Intracranial hemorrhage. Dr. Amitesh Aggarwal Associate Professor Department of Medicine
 Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
Pediatric Head Injury:
 Pediatric Head Injury: Part I Basic Principles Jogi V. Pattisapu, MD FAAP FACS Emeritus Medical Director Arnold Palmer Medical Center College of Medicine University of Central Florida Orlando FL USA JogiP@mail.UCF.edu
Pediatric Head Injury: Part I Basic Principles Jogi V. Pattisapu, MD FAAP FACS Emeritus Medical Director Arnold Palmer Medical Center College of Medicine University of Central Florida Orlando FL USA JogiP@mail.UCF.edu
Traumatic Brain Injury (1.2.3) Management of severe TBI ( ) Learning Objectives
 Management of severe TBI ( ) Learning Objectives") Traumatic Brain Injury (1.2.3) 1.2.3.1 Management of severe TBI 1.2.3.2 Management of concussions 1.2.3.3 Sideline management for team medics/physicians 1.4.2.3.10 Controlled hyperventilation for management
Traumatic Brain Injury (1.2.3) 1.2.3.1 Management of severe TBI 1.2.3.2 Management of concussions 1.2.3.3 Sideline management for team medics/physicians 1.4.2.3.10 Controlled hyperventilation for management
V. CENTRAL NERVOUS SYSTEM TRAUMA
 V. CENTRAL NERVOUS SYSTEM TRAUMA I. Concussion - Is a clinical syndrome of altered consiousness secondary to head injury - Brought by a change in the momentum of the head when a moving head suddenly arrested
V. CENTRAL NERVOUS SYSTEM TRAUMA I. Concussion - Is a clinical syndrome of altered consiousness secondary to head injury - Brought by a change in the momentum of the head when a moving head suddenly arrested
To date, head injury remains the leading cause of. Outcome in patients with blunt head trauma and a Glasgow Coma Scale score of 3 at presentation
 J Neurosurg 111:683 687, 2009 Outcome in patients with blunt head trauma and a Glasgow Coma Scale score of 3 at presentation Clinical article Ro u k o z B. Ch a m o u n, M.D., Cl a u d i a S. Ro b e r
J Neurosurg 111:683 687, 2009 Outcome in patients with blunt head trauma and a Glasgow Coma Scale score of 3 at presentation Clinical article Ro u k o z B. Ch a m o u n, M.D., Cl a u d i a S. Ro b e r
Traumatic Brain Injury TBI Presented by Bill Masten
 1 2 Cerebrum two hemispheres and four lobes. Cerebellum (little brain) coordinates the back and forth ballet of motion. It judges the timing of every movement precisely. Brainstem coordinates the bodies
1 2 Cerebrum two hemispheres and four lobes. Cerebellum (little brain) coordinates the back and forth ballet of motion. It judges the timing of every movement precisely. Brainstem coordinates the bodies
11/23/2015. Disclosures. Stroke Management in the Neurocritical Care Unit. Karel Fuentes MD Medical Director of Neurocritical Care.
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Classical CNS Disease Patterns
 Classical CNS Disease Patterns Inflammatory Traumatic In response to the trauma of having his head bashed in GM would have experienced some of these features. NOT TWO LITTLE PEENY WEENY I CM LACERATIONS.
Classical CNS Disease Patterns Inflammatory Traumatic In response to the trauma of having his head bashed in GM would have experienced some of these features. NOT TWO LITTLE PEENY WEENY I CM LACERATIONS.
Chapter 8: Cerebral protection Stephen Lo
 Chapter 8: Cerebral protection Stephen Lo Introduction There will be a variety of neurological pathologies that you will see within the intensive care. The purpose of this chapter is not to cover all neurological
Chapter 8: Cerebral protection Stephen Lo Introduction There will be a variety of neurological pathologies that you will see within the intensive care. The purpose of this chapter is not to cover all neurological
PROTECT - ION 11/26/2014. Traumatic Brain Injury. Pathophysiology and Management. Disclosures. Neuro PROTECTion in Severe Traumatic Brain Injury
 Disclosures Neuro PROTECTion in Severe Traumatic Brain Injury Presented by: Mary Kay Bader RN, MSN CCNS, CNRN, CCRN, SCRN, FAHA, FNCS Neuro/Critical Care CNS Mission Hospital Badermk@aol.com Bader Honorarium
Disclosures Neuro PROTECTion in Severe Traumatic Brain Injury Presented by: Mary Kay Bader RN, MSN CCNS, CNRN, CCRN, SCRN, FAHA, FNCS Neuro/Critical Care CNS Mission Hospital Badermk@aol.com Bader Honorarium
Management of pediatric head injury
 IJCCM October-December 2003 Vol 7 Issue 4 Indian J Crit Care Med April-June 2004 Vol 8 Issue 2 Pediatric Section Management of pediatric head injury Praveen Khilnani Introduction Exact incidence of head
IJCCM October-December 2003 Vol 7 Issue 4 Indian J Crit Care Med April-June 2004 Vol 8 Issue 2 Pediatric Section Management of pediatric head injury Praveen Khilnani Introduction Exact incidence of head
Author Manuscript. Received Date : 27-Oct Revised Date : 09-Jan-2017 Accepted Date : 31-Jan-2017
 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 Received Date : 27-Oct-2016 Revised Date : 09-Jan-2017 Accepted Date : 31-Jan-2017 Article type ABSTRACT : Original Contribution
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 Received Date : 27-Oct-2016 Revised Date : 09-Jan-2017 Accepted Date : 31-Jan-2017 Article type ABSTRACT : Original Contribution
UHSM ED Pathway ELDERLY FALL / COLLAPSE
 UHSM ED Pathway ELDERLY FALL / COLLAPSE Patient name / Pathway for patients who require assessment in ED after a fall or collapse Note: - It can be used if the patient has also sustained a minor head injury
UHSM ED Pathway ELDERLY FALL / COLLAPSE Patient name / Pathway for patients who require assessment in ED after a fall or collapse Note: - It can be used if the patient has also sustained a minor head injury
Management of Traumatic Brain Injury. Olaide O. Ajayi, MD
 Management of Traumatic Brain Injury Olaide O. Ajayi, MD Traumatic Brain Injury (TBI) A bump, blow or jolt to the head that disrupts the normal function of the brain 1 Mild: Brief change in mental status
Management of Traumatic Brain Injury Olaide O. Ajayi, MD Traumatic Brain Injury (TBI) A bump, blow or jolt to the head that disrupts the normal function of the brain 1 Mild: Brief change in mental status
Tony L Smith DNP RN ACNP CCRN CFRN EMT-IV Vanderbilt LifeFlight
 Treatment of a Stroke patient: A look at how to care for the Stroke patient in the aeromedical setting Tony L Smith DNP RN ACNP CCRN CFRN EMT-IV Vanderbilt LifeFlight Objectives 1. Discuss the assessment
Treatment of a Stroke patient: A look at how to care for the Stroke patient in the aeromedical setting Tony L Smith DNP RN ACNP CCRN CFRN EMT-IV Vanderbilt LifeFlight Objectives 1. Discuss the assessment
UAMS MEDICAL CENTER TRAUMA and CRITICAL CARE SERVICES MANUAL. SUPERSEDES: New PAGE: 1 of 5. RECOMMENDATION(S): Drs. Bill Beck/J.R.
: Drs. Bill Beck/J.R.") SUPERSEDES: New PAGE: 1 of 5 Purpose: To provide recommendations for the treatment and management of patients with traumatic brain injury. Definitions: Severe TBI - Glasgow Coma Scale (GCS) of 3 to 8 without
SUPERSEDES: New PAGE: 1 of 5 Purpose: To provide recommendations for the treatment and management of patients with traumatic brain injury. Definitions: Severe TBI - Glasgow Coma Scale (GCS) of 3 to 8 without