Laryngotracheal stenosis in children
|
|
|
- Terence Fisher
- 5 years ago
- Views:
Transcription
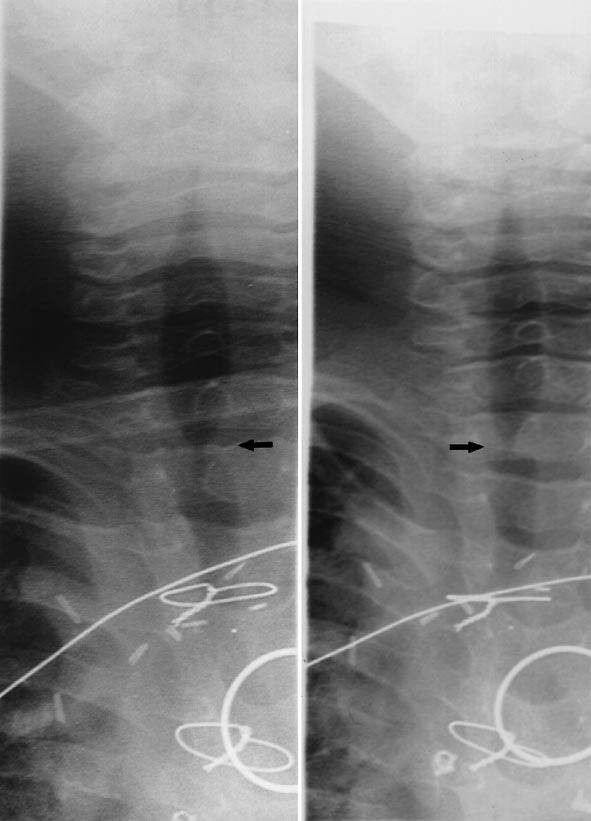
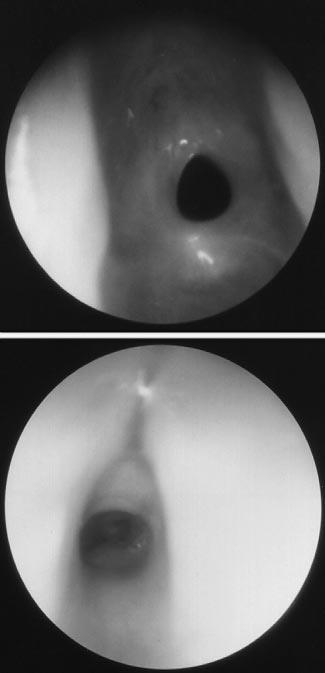
1 Eur Arch Otorhinolaryngol (1998) 255 : Springer-Verlag 1998 LARYNGOLOGY M. M. Lesperance G. H. Zalzal Laryngotracheal stenosis in children Received: 8 March 1977 / Accepted: 31 July 1997 Abstract The diagnosis of laryngotracheal stenosis should be suspected in children with stridor, feeding difficulties, or atypical croup. Only half of the children with congenital laryngotracheal stenosis require tracheotomy, and many of these children can be decannulated following uncomplicated surgical therapy. In contrast, tracheotomy-dependent patients with acquired laryngotracheal stenosis require more extensive surgical intervention, which should be carried out as early as possible to provide the best opportunity for developing normal oral communication. Key words Laryngotracheal stenosis Intubation Tracheotomy Airway obstruction Management Introduction Laryngotracheal stenosis is a congenital or acquired narrowing of the airway, representing a continuum of disease that may affect the glottis, subglottis, and/or trachea. Previously, the term subglottic stenosis was often used (inaccurately) as an umbrella term to describe stenosis occurring anywhere in the airway because the subglottis was the most frequent site of stenosis. Currently, rod lens telescopes are available, allowing the experienced endoscopist to describe precisely the site and type of airway pathology. This review will address the etiology, diagnosis, and management of laryngotracheal stenosis. M.M. Lesperance ( ) Division of Pediatric Otolaryngology, Department of Otolaryngology Head and Neck Surgery, University of Michigan Medical Center, Ann Arbor, MI , USA G. H. Zalzal Department of Otolaryngology Head and Neck Surgery, Children s National Medical Center, Washington, DC , USA Diagnosis Diagnosis entails a complete history and physical examination, radiologic evaluation, and endoscopy. Presenting symptoms of laryngotracheal stenosis include stridor, restlessness, irritability, dyspnea, tachypnea, apnea, and cyanosis. Glottic stenosis may affect vocal cord mobility and present clinically as a weak, hoarse cry, aphonia, or aspiration with recurrent pneumonia. Respiratory distress with feeding may result in failure to thrive. Permanent pectus excavatum may result from long-standing increased negative pleural pressures during inspiration coupled with the increased compliance of the chest wall of the young child. The diagnosis may be confounded by concurrent pulmonary, cardiac, or neurologic disease. Mild to moderate laryngotracheal stenosis may be occult until the child is 1 3 months of age, when the infant becomes capable of greater physical activity that requires increased ventilation [7]. In the majority of cases, the child with laryngotracheal stenosis will present with croup. Atypical croup refers to (1) multiple episodes of croup in the first year of life; (2) multiple hospital admissions for croup; (3) failure of prompt response to appropriate med- Fig. 1 Anteroposterior radiograph of airway demonstrating moderate subglottic stenosis with (arrow) absence of normal subglottic shouldering in a 22-month-old girl Fig. 2 a, b Airway fluoroscopy of a 4-year-old boy with congenital heart disease and tracheal stenosis involving (arrow) limited segment of thoracic trachea. a Inspiratory view; b dynamic component evident on expiratory view Fig. 3 Radiograph obtained immediately after birth of male infant demonstrating laryngeal atresia with tracheoesophageal fistula. Note endotracheal tube tip (black arrow) contacting atresia plate with upper esophagus (white arrows) distended by air Fig. 4 Acquired circumferential laryngotracheal stenosis of moderate severity. The scar in this patient was mainly a soft (membranous) stenosis Fig.5 Congenital laryngotracheal stenosis. The stenosis is usually anterior, involving the immediate subglottic area

2 a 2b
3 14 ical management; and (4) croup requiring endotracheal intubation. Children with severe laryngotracheal stenosis have significant respiratory distress that persists in the absence of upper respiratory tract infection. Severe congenital laryngotracheal stenosis may be symptomatic at birth. The latent period for acquired laryngotracheal stenosis is generally 2 4 weeks from the time of airway injury, and the degree of respiratory distress is often progressive over time. High kilovoltage anteroposterior and lateral airway radiographs (Fig. 1) should be obtained unless the severity of respiratory distress precludes radiologic evaluation. If true inspiratory and expiratory views are difficult to obtain, airway fluoroscopy may be useful (Fig. 2). Although barium esophagram may be indicated to assess feeding problems, it rarely rules out external compression of the trachea. Computed tomography may be useful in assessing the length of the stenotic segment. However, as sedation is contraindicated in the child with a compromised airway, this latter study may be difficult to obtain. Preoperative voice analysis and pulmonary function tests are useful in older children [23]. Flexible fiberoptic endoscopy is performed to assess supraglottic and glottic pathology. On occasion, the subglottis can be visualized with flexible endoscopic examination. Congenital laryngeal webs may be partial or complete (laryngeal atresia) and are characterized by a firm fibrous membrane connecting the vocal cords (Fig. 3). An immobile vocal cord may be evidence of posterior glottic stenosis with cricoarytenoid joint fixation [1], and laryngeal electromyography should be performed to assess vocal cord innervation. At present, the standard for diagnosis is direct laryngoscopy and bronchoscopy under general anesthesia. The outer diameter of the largest bronchoscope that can pass through the stenosis should be noted. Congenital subglottic stenosis is defined as a subglottic diameter of 4 mm or less in a full-term neonate, or a diameter less than 3.5 mm in a premature neonate [21]. The length and location of the stenotic segment are noted. The use of the rod lens telescope without the bronchoscope allows dynamic assessment of the cartilaginous support. Membranous subglottic stenosis (sometimes called soft tissue stenosis ) may be due to submucosal fibrosis, submucous gland hyperplasia, or granulation tissue. Most commonly, the stenosis is circumferential and symmetric, with the smallest diameter 2 3 mm below the vocal cords (Fig. 4). Frequently, posterior glottic stenosis is continuous with stenosis of the posterior subglottis [12]. Cartilaginous stenosis presents as a deformity of the cricoid cartilage projecting into the airway lumen from the posterior, anterior, or lateral walls [13]. A small cricoid of otherwise normal shape will present as a symmetric stenosis. Causes of asymmetric congenital cricoid narrowing include an elliptical or oval-shaped cricoid, isolated enlargement of either the anterior or posterior cricoid lamina, or incomplete laryngeal cleft. A trapped first tracheal ring is a type of cartilaginous stenosis characterized by a nondistensible, complete tracheal ring [8]. Etiology and pathophysiology Laryngotracheal stenosis is considered congenital when there is no previous documentation of a normal airway, and risk factors for acquired stenosis are absent (Fig. 5). The most common cause of acquired stenosis is endotracheal intubation, accounting for approximately 90% of mature laryngotracheal stenoses [12]. Histopathologic studies of the airway have shown that even brief periods of endotracheal intubation can cause damage to the thin respiratory epithelium of the subglottis [11]. The subglottis is the narrowest region of the airway in children, and the cricoid cartilage is the only complete circumferential cartilaginous ring in the airway. The loose areolar tissue of the submucosa readily develops edema, which extends inward at the expense of the airway lumen. Endotracheal intubation causes mucosal compression when the pressure from the tube exceeds the capillary pressure of the mucosa [10, 12]. Mucosal edema, ischemia, and ulceration lead to perichondritis and chondritis. Healing occurs by secondary intention with granulation tissue proliferation and deposition of fibrous tissue. A weakened cartilage framework and a firm scar narrowing the lumen of the airway result. External compression may contribute to the loss of cartilage support, which often persists long after surgical relief of the compression. The differential diagnosis includes vascular anomalies, such as innominate artery compression or double aortic arch, and congenital masses, such as bronchogenic cyst, duplication cyst, teratoma, cystic hygroma, and hemangioma. Systemic illnesses such as sepsis, dehydration, anemia, avitaminosis, hypoxia, neutropenia, and immunosuppression also influence the development of laryngotracheal stenosis through alteration of perfusion, nutrition, and resistance to infection. The most important risk factor for the development of laryngotracheal stenosis is the duration of intubation. Although 5 10 days of intubation are generally considered to be an acceptable length of time for intubation in adults, there is no definite safe period in children. In general, premature infants may be intubated for longer periods, since airway cartilages in the neonate are more yielding and pliable [10]. The size of the tube should allow an air leak at an inspiratory pressure of 20 cm H 2 O. The rate of laryngotracheal stenosis has been reported as very low when small (2.5 mm) endotracheal tubes are used in infants weighing less than 2500 g [4]. However, because of the intensive nursing care required to keep the tubes patent, larger tubes are often used in North America. The type of endotracheal tube is rarely debated, now that Silastic and polyvinyl chloride tubes without cuffs are used almost uniformly. Laryngotracheal stenosis may result from external or surgical trauma through a similar mechanism of edema, granulation, and fibrosis. Severe glottic stenosis may result from blunt laryngeal trauma, particularly when the injury is not repaired promptly, and the stenosis often extends to the supraglottis and subglottis. Caustic ingestion
 used to reconstruct anterior laryngotracheal stenosis and thermal burns can cause severe mucosal damage that results in stenosis.")
4 Fig. 6 Anterior cricoid split procedure. Note the endotracheal tube in the subglottic lumen and the distraction of the segments of the cricoid cartilage after the anterior split Fig. 7 Anterior costal cartilage graft (modified boat shape) used to reconstruct anterior laryngotracheal stenosis and thermal burns can cause severe mucosal damage that results in stenosis. Glottic and subglottic stenosis may result from a high tracheotomy, cricothyrotomy, or endoscopic laser procedures [12, 17]. Anterior glottic stenosis is most commonly a consequence of endoscopic procedures involving both true vocal cords at one session [17]. A 20% incidence of subglottic stenosis has reported following laser treatment of subglottic hemangioma [15]. Although many patients with laryngotracheal stenosis have demonstrable physiologic gastroesophageal reflux (GER), there are no accepted clinical criteria to confirm the presence of pathologic GER or reflux disease. A prospective study of patients undergoing laryngotracheal reconstruction revealed no differences in outcome whether or not patients underwent preoperative testing for GER, had evidence of GER, or were treated for GER [25]. Surgical technique (discussed below) rather than the presence or treatment of GER is likely the most important factor in successful treatment of laryngotracheal stenosis. Excessive suctioning, multiple intubations, and tube changes should be avoided in order to minimize trauma to the airway mucosa. A child with a history of laryngotracheal stenosis may sustain significant re-injury to the airway while undergoing a brief general anesthetic if the anesthesiologist is not informed of the need to use a smaller tube. Adequate sedation of the intubated patient will reduce the shearing action of the tube caused by swallowing or volitional motion of the patient. Meticulous hygiene is critical, as secondary bacterial infection increases inflammation and the deposition of scar tissue [14]. Concomitant use of a nasogastric tube increases the risk of secondary infection because of local reaction to the foreign body and increased stasis of secretions. The reported incidence of laryngotracheal stenosis in intubated patients is approximately 1 5% [6, 10]. In the 1960s, prolonged endotracheal intubation of neonates became widely accepted as an alternative to tracheotomy [Brandstater 1962, unpublished work]. During this time, the incidence of laryngotracheal stenosis was 12 20% [9]. The reduction in the incidence over the last years is likely due to improved education of health care personnel leading to increased awareness of the factors discussed above. However, the exact incidence rate of laryngotracheal stenosis is unknown. Many children are initially asymptomatic and will not be diagnosed until they are referred for rigid endoscopy much later in life. In addition, severely ill children may die of their primary illness before laryngotracheal stenosis is recognized. Finally, although staging systems for laryngotracheal stenosis have been described, none are universally applicable and useful. The Cotton staging system is useful for mature, firm, circumferential stenosis confined to the subglottis [7]. Management Unlike acquired stenoses, congenital subglottic stenoses carry an excellent prognosis. Respiratory distress associated with upper respiratory tract infections can be treated with aggressive medical management. In mild cases, the airway will increase in diameter as the child grows, and surgery will not be necessary. Tracheotomy is required to relieve airway obstruction in less than 50% of cases of congenital laryngotracheal stenosis. If reconstructive surgery is postponed or declined, most patients remain tracheotomy-dependent for 2 5 years [12]. Cases of increased severity require surgical intervention. In our experience, the majority of patients with acquired laryngotracheal stenosis or severe congenital stenosis require tracheotomy. Given that the mortality of tracheotomy is still 2 5% per child per year, there is no role for wait-and-see management in acquired or severe laryngotracheal stenosis. In general, the mortality of tra-
5 16 cheotomy is particularly related to the status of the residual airway above the tracheotomy tube. However, surgical correction of the airway is contraindicated in the patient who would still require a tracheotomy for mechanical ventilation, supplemental oxygen, or management of other pulmonary or neurologic disease. Subglottic cysts and very thin, limited regions of stenosis may be amenable to endoscopic resection with the carbon dioxide laser [16]. However, stenosis may become dramatically worse after laser therapy. Circumferential laser treatment will often lead to cicatricial contracture of the airway lumen. We believe that the failure of laser therapy should not be considered a prerequisite for laryngotracheal reconstruction, as many stenoses will not be amenable to such treatment at any time. Anterior cricoid split was first described by Cotton and Seid [8] for the treatment of acquired subglottic stenosis. The indications were expanded to include patients with congenital subglottic stenosis that would otherwise require tracheotomy or endotracheal intubation [9]. Anterior cricoid split is indicated in children with a small, normally shaped cricoid ring, extensive submucosal fibrosis, or for decompression of subglottic cysts. After induction of general anesthesia with endotracheal intubation, the laryngotracheal complex is exposed through a cervical incision. The cricoid cartilage and the first and second tracheal rings are split in the midline anteriorly to allow expansion of the cricoid ring (Fig. 6). The endotracheal tube is replaced as a stent for 7 days. Severe congenital stenosis, marked deformity of the cricoid cartilage, or failure of the anterior cricoid split procedure are indications for tracheotomy and laryngotracheal expansion surgery. The concept of laryngotracheal expansion surgery is to divide an existing scar and distract the edges of a stenotic site with an interposed graft to widen the airway lumen [7, 12]. The scar is not resected, since creating a surface denuded of mucosa will inevitably heal with recurrent formation of scar. The operation is customized for each patient, involving choices regarding the graft (anterior, posterior, or both), the stent (discussed below), the type of cricoid incision (anterior, posterior, or four-quadrant split), and the need for laryngofissure. The autogenous costal cartilage graft is the most useful for laryngotracheal reconstruction [5]. The advantages of cartilage include less resorption than bone grafts, viability without a vascular pedicle, and ease of carving. Donor site morbidity is minimal. Unlike bone grafts, cartilage grafts will maintain their bulk despite a lack of functional stress. The graft is harvested with the inner perichondrium in situ and placed with the perichondrium facing the lumen as a barrier to infection [22]. The boat-shaped graft used for posterior grafts is modified for anterior grafts (Fig. 7) to include outer flanges in order to prevent prolapse into the lumen, gain more distraction, and avoid the need to bevel the graft. Stents are used to restore distorted anatomy, maintain a lumen, counteract keloid formation, and create a stable framework in the absence of cartilage support. The choice of stent and duration of stenting depends on the purpose of the stent. If the stent is placed only to keep repaired areas in place (i.e., a posterior costal cartilage graft), only a short duration of stenting is required. Conversely, months of stenting are required if the function of the stent is to counteract scar formation. Stent materials include Teflon (Aboulker), Silastic (Montgomery stent and Swiss roll stent), polyvinyl chloride (endotracheal tube), and a finger cot stent. Rubber stents should not be used. The Aboulker stent is most commonly used, as Teflon is the least reactive stent material. Oral antibiotics are administered while the stent is in place to prevent infection and colonization of the granulation tissue. The long Aboulker stent extends inferiorly from the tip of the tracheotomy tube to the arytenoid cartilages superiorly [19]. Since the long stent is wired to the tracheotomy tube, the outer cannula of the tracheotomy tube cannot be changed for the duration of stenting. The short Aboulker stent is used if the stenosis is confined to the glottis and if the duration of stenting will be short (4 5 weeks). The short stent is secured with a suture, since the inferior aspect of the short stent is above the tracheotomy tube. The disadvantage of the short stent is the potential for granulation tissue formation between the stent and the tracheotomy tube. The average time to decannulation after stent removal is 4 weeks. The position of the stent is monitored with flexible laryngoscopy for stent displacement or granulation tissue. Glottic stenosis may recur if the stent does not extend superiorly enough to distract the vocal cords. Complications of stenting include granulation tissue with subsequent stenosis, wound infection, stent breakage, and stent migration. Anterior cricoid split with anterior costal cartilage grafting is indicated for anterior tracheal wall collapse or isolated anterior subglottic stenosis. The anterior costal cartilage graft is placed such that it extends inferiorly to repair the previous tracheotomy site. One-stage laryngotracheoplasty refers to procedures performed on these relatively mild cases of laryngotracheal stenosis that do not require stenting for longer than 1 week. Indications for posterior costal cartilage grafting include posterior glottic and subglottic stenosis, complete or circumferential stenosis, vocal cord fixation, and bilateral subglottic shelves. In order to place posterior grafts, the cricoid must be split in the midline both anteriorly and posteriorly; therefore, a rigid posterior cricoid lamina must be present. Laryngofissure may be necessary in the presence of posterior glottic stenosis in order to visualize the superior extent of the stenosis. An anterior graft is used in addition to the posterior graft if the anterior cricoid cannot be closed around the stent. The indications for a four-quadrant cricoid split without grafting are continuous, complete scarring from glottis to trachea, severe distortion of the anatomy, or the absence of a stable cartilage framework. The cricoid cartilage is split anteriorly, posteriorly, and laterally on both sides. A long duration (i.e., 6 months) of stenting is required. Resection of the stenotic segment with primary end-toend anastomosis is indicated for isolated subglottic or up-
6 per tracheal stenosis, provided that a normal lumen extends at least 10 mm below the glottis. The vertical length of the stenosis must be such that after resection, the cricoid and tracheal ends can be approximated without tension. Laryngeal release will provide an extra 1 3 cm of mobilization. Stenting is not required, and the tracheotomy tube usually can be removed by 4 weeks postoperatively. Partial cardiopulmonary bypass may be necessary to accomplish the repair. Outcome of treatment The ultimate goal of laryngotracheal reconstruction is decannulation. Restoration of the normal functions of the airway at the earliest possible age will allow optimal development of speech and articulation. Success rates of 80 90% have been reported [20]. Although a functional voice can be restored in most patients, persistent voice disorders are common [3]. The postoperative voice is characterized by lower than optimal pitch and a restricted pitch range [24]. As surgical management must be individualized, comparison of results requires consideration of (1) the etiology of stenosis; (2) the number of previous (failed) endoscopic procedures; (3) the location and extent of scar and the degree of anatomic disruption in the entire airway, including the glottis; (4) the mobility of the vocal cords; (5) the stability of the laryngotracheal framework and the integrity of cartilaginous support; and (6) the patient s general medical condition. References 1. Bogdasarian RS, Olson NR (1980) Posterior glottic laryngeal stenosis. Otolaryngol Head Neck Surg 88: Reference deleted 3. Clary RA, Pengilly A, Bailey M, Jones N, Albert D, Comins J, Appleton J (1996) Analysis of voice outcomes in pediatric patients following surgical procedures for laryngotracheal stenosis. Arch Otolaryngol Head Neck Surg 122: Cotencin P, Narcy P (1993) Size of endotracheal tube and neonatal acquired subglottic stenosis. Arch Otolaryngol Head Neck Surg 119: Cotton RT (1984) Pediatric laryngotracheal stenosis. J Pediatr Surg 19: Cotton RT (1985) Prevention and management of laryngeal stenosis in infants and children. J Pediatr Surg 20: Cotton RT, Richardson MA (1981) Congenital laryngeal anomalies. Otolaryngol Clin North Am 14: Cotton RT, Seid AB (1980) Management of the extubation problem in the premature child: anterior cricoid split as an alternative to tracheotomy. Ann Otol Rhinol Laryngol 89 : Fearon B, MacDonald RE, Smith C, Mitchell D (1966) Airway problems in children following endotracheal intubation. Ann Otol Rhinol Laryngol 75: Hawkins DB (1978) Hyaline membrane disease of the neonate prolonged intubation in management: effects on the larynx. Laryngoscope 88: Hilding AC, Hilding JA (1962) Tolerance of the respiratory mucous membrane to trauma: surgical swabs and intratracheal tubes. Ann Otol Rhinol Laryngol 71: Holinger PH, Kutnick SL, Schild J, Holinger LD (1976) Subglottic stenosis in infants and children. Ann Otol Rhinol Laryngol 85: McMillan WG, Duvall AJ (1968) Congenital subglottic stenosis. Arch Otolaryngol 8: Sasaki CT, Horiuchi M, Koss N (1979) Tracheostomy-related subglottic stenosis: bacteriologic pathogenesis. Laryngoscope 89: Sie KCY, McGill T, Healy GB (1994) Subglottic hemangioma: ten years experience with the carbon dioxide laser. Ann Otol Rhinol Laryngol 103: Simpson GT, Strong MS, Healy GC, Shapshay SM, Vaughan CW (1982) Predictive factors of success or failure in the endoscopic management of laryngeal and tracheal stenosis. Ann Otol Rhinol Laryngol 91: Strong MS, Vaughan CW, Healy GB, Cooperband SR, Clemente MACP (1976) Recurrent respiratory papillomatosis: management with the CO 2 laser. Ann Otol Rhinol Laryngol 85 : Tucker GF, Ossoff RH, Newman AN, Holinger LD (1979) Histopathology of congenital subglottic stenosis. Laryngoscope 89: Zalzal GH (1988) Use of stents in laryngotracheal reconstruction in children: indications, technical considerations, and complications. Laryngoscope 98: Zalzal GH (1993) Treatment of laryngotracheal stenosis with anterior and posterior cartilage grafts. A report of 41 children. Arch Otolaryngol Head Neck Surg 119: Zalzal GH, Cotton RT (1993) Glottic and subglottic stenosis. In: Cummings CW, Fredrickson JM, Harker LA, Krause CJ, Schuller DE (eds) Otolaryngology-head and neck surgery, 2nd edn. Mosby-Year Book, St. Louis, pp Zalzal GH, Cotton RT, McAdams AJ (1986) Cartilage grafts present status. Head Neck Surg 8: Zalzal GH, Thomsen JR, Chaney HR, Derkay C (1990) Pulmonary parameters after laryngotracheal reconstruction in children. Ann Otol Rhinol Laryngol 99: Zalzal GH, Loomis SR, Derkay CS, Murray SL, Thomsen J (1991) Vocal quality of decannulated children following laryngeal reconstruction. Laryngoscope 101: Zalzal GH, Choi SS, Patel KM (1996) The effect of gastroesophageal reflux on laryngotracheal reconstruction. Arch Otolaryngol Head Neck Surg 122:
Neonatal Airway Disorders, Treatments, and Outcomes. Steven Goudy, MD Pediatric Otolaryngology Emory University Medical Center
 Neonatal Airway Disorders, Treatments, and Outcomes Steven Goudy, MD Pediatric Otolaryngology Emory University Medical Center Disclosure I have nothing to disclose Neonatal and Pediatric Tracheostomy Tracheostomy
Neonatal Airway Disorders, Treatments, and Outcomes Steven Goudy, MD Pediatric Otolaryngology Emory University Medical Center Disclosure I have nothing to disclose Neonatal and Pediatric Tracheostomy Tracheostomy
Basic Science Review Wound Healing
 Subglottic Stenosis Deborah P. Wilson, M.D. Faculty Advisor: Norman Friedman, M.D. The University of Texas Medical Branch Department of Otolaryngology Grand Rounds Presentation April 14, 1999 Basic Science
Subglottic Stenosis Deborah P. Wilson, M.D. Faculty Advisor: Norman Friedman, M.D. The University of Texas Medical Branch Department of Otolaryngology Grand Rounds Presentation April 14, 1999 Basic Science
Complex Airway problems - Paediatric Perspective
 Complex Airway problems - Paediatric Perspective Dave Albert BACO Liverpool 2009 www.albert.uk.com Complex Ξ not simple, multiple parts Multiple problems with airway Combined Web/stenosis/multiple levels
Complex Airway problems - Paediatric Perspective Dave Albert BACO Liverpool 2009 www.albert.uk.com Complex Ξ not simple, multiple parts Multiple problems with airway Combined Web/stenosis/multiple levels
Chapter 34: Stenosis of the larynx. J. N. G. Evans
 Chapter 34: Stenosis of the larynx J. N. G. Evans Stenosis of the larynx is more frequent than tracheal stenosis; in a review of 752 cases of stridor seen at The Hospital for Sick Children, Great Ormond
Chapter 34: Stenosis of the larynx J. N. G. Evans Stenosis of the larynx is more frequent than tracheal stenosis; in a review of 752 cases of stridor seen at The Hospital for Sick Children, Great Ormond
Unilateral Supraglottoplasty for Severe Laryngomalacia in Children. Nasser A Fageeh, MD, FRCSC, FACS*
 Bahrain Medical Bulletin, Vol. 37, No. 1, March 2015 Unilateral Supraglottoplasty for Severe Laryngomalacia in Children Nasser A Fageeh, MD, FRCSC, FACS* Objective: To study the efficacy of Unilateral
Bahrain Medical Bulletin, Vol. 37, No. 1, March 2015 Unilateral Supraglottoplasty for Severe Laryngomalacia in Children Nasser A Fageeh, MD, FRCSC, FACS* Objective: To study the efficacy of Unilateral
TRACHEOSTOMY. Tracheostomy means creation an artificial opening in the trachea with tracheostomy tube insertion
 TRACHEOSTOMY Definition Tracheostomy means creation an artificial opening in the trachea with tracheostomy tube insertion Indications for tracheostomy 1-upper airway obstruction with stridor, air hunger,
TRACHEOSTOMY Definition Tracheostomy means creation an artificial opening in the trachea with tracheostomy tube insertion Indications for tracheostomy 1-upper airway obstruction with stridor, air hunger,
Pediatric partial cricotracheal resection: A new technique for the posterior cricoid anastomosis
 Otolaryngology Head and Neck Surgery (2006) 135, 318-322 ORIGINAL RESEARCH Pediatric partial cricotracheal resection: A new technique for the posterior cricoid anastomosis Mark E. Boseley, MD, and Christopher
Otolaryngology Head and Neck Surgery (2006) 135, 318-322 ORIGINAL RESEARCH Pediatric partial cricotracheal resection: A new technique for the posterior cricoid anastomosis Mark E. Boseley, MD, and Christopher
College Hospital, London, over the last five years.
 Archives of Disease in Childhood, 1986, 61, 686-690 Management of subglottic stenosis: two centres experience from R E QUINEY, M G SPENCER, C M BAILEY, J N G EVANS, AND J M GRAHAM Royal Ear Hospital, University
Archives of Disease in Childhood, 1986, 61, 686-690 Management of subglottic stenosis: two centres experience from R E QUINEY, M G SPENCER, C M BAILEY, J N G EVANS, AND J M GRAHAM Royal Ear Hospital, University
Aetiology. Poor tube management. Small cricoid (acquired on congenital) Reflux Poor general status. Size of tube (leak) Duration of intubation
 Reflux Poor general status. Size of tube (leak) Duration of intubation") Aetiology Poor tube management Size of tube (leak) Duration of intubation Small cricoid (acquired on congenital) Reflux Poor general status Prevention Laryngeal Rest Medical Tubes Cricoid split Developing
Aetiology Poor tube management Size of tube (leak) Duration of intubation Small cricoid (acquired on congenital) Reflux Poor general status Prevention Laryngeal Rest Medical Tubes Cricoid split Developing
External trauma (MVA, surf board, assault, etc.) Internal trauma (Endotracheal intubation, tracheostomy) Other
 Internal trauma (Endotracheal intubation, tracheostomy) Other") Etiology External trauma (MVA, surf board, assault, etc.) Internal trauma (Endotracheal intubation, tracheostomy) Other Systemic diseases (vasculitis, etc.) Chemo/XRT Idiopathic Trans nasal Esophagoscope
Etiology External trauma (MVA, surf board, assault, etc.) Internal trauma (Endotracheal intubation, tracheostomy) Other Systemic diseases (vasculitis, etc.) Chemo/XRT Idiopathic Trans nasal Esophagoscope
Multilevel airway obstruction including rare tongue base mass presenting as severe croup in an infant. Tara Brennan, MD 2,3
 Multilevel airway obstruction including rare tongue base mass presenting as severe croup in an infant Tara Brennan, MD 2,3 Jeffrey C. Rastatter, MD, FAAP 1,2 1 Department of Otolaryngology, Northwestern
Multilevel airway obstruction including rare tongue base mass presenting as severe croup in an infant Tara Brennan, MD 2,3 Jeffrey C. Rastatter, MD, FAAP 1,2 1 Department of Otolaryngology, Northwestern
Subject Index. Bacterial infection, see Suppurative lung disease, Tuberculosis
 Subject Index Abscess, virtual 107 Adenoidal hypertrophy, features 123 Airway bleeding, technique 49, 50 Airway stenosis, see Stenosis, airway Anaesthesia biopsy 47 complications 27, 28 flexible 23 26
Subject Index Abscess, virtual 107 Adenoidal hypertrophy, features 123 Airway bleeding, technique 49, 50 Airway stenosis, see Stenosis, airway Anaesthesia biopsy 47 complications 27, 28 flexible 23 26
ORIGINAL ARTICLE. Open Excision of Subglottic Hemangiomas to Avoid Tracheostomy
 ORIGINAL ARTICLE Open Excision of Subglottic Hemangiomas to Avoid Tracheostomy Shyan Vijayasekaran, FRACS; David R. White, MD; Benjamin E. J. Hartley, FRCS(ORL); Michael J. Rutter, FRACS; Ravindhra G.
ORIGINAL ARTICLE Open Excision of Subglottic Hemangiomas to Avoid Tracheostomy Shyan Vijayasekaran, FRACS; David R. White, MD; Benjamin E. J. Hartley, FRCS(ORL); Michael J. Rutter, FRACS; Ravindhra G.
Endoscopic Posterior Cricoid Split with Costal Cartilage Graft: A Fifteen Year Experience
 1 Endoscopic Posterior Cricoid Split with Costal Cartilage Graft: A Fifteen Year Experience John P. Dahl, MD, PhD, MBA 1,2, *, Patricia L. Purcell, MD 1, MPH, Sanjay R. Parikh, MD, FACS 1, and Andrew F.
1 Endoscopic Posterior Cricoid Split with Costal Cartilage Graft: A Fifteen Year Experience John P. Dahl, MD, PhD, MBA 1,2, *, Patricia L. Purcell, MD 1, MPH, Sanjay R. Parikh, MD, FACS 1, and Andrew F.
Subglottic Stenosis November 2002
 TITLE: Subglottic Stenosis SOURCE: Grand Rounds Presentation, UTMB, Dept. of Otolaryngology DATE: November 13, 2002 RESIDENT PHYSICIAN: Christopher D. Muller, M.D. FACULTY PHYSICIAN: Anna M. Pou, M.D.
TITLE: Subglottic Stenosis SOURCE: Grand Rounds Presentation, UTMB, Dept. of Otolaryngology DATE: November 13, 2002 RESIDENT PHYSICIAN: Christopher D. Muller, M.D. FACULTY PHYSICIAN: Anna M. Pou, M.D.
Pediatric Endoscopic Airway Management With Posterior Cricoid Rib Grafting
 The Laryngoscope VC 2011 The American Laryngological, Rhinological and Otological Society, Inc. Pediatric Endoscopic Airway Management With Posterior Cricoid Rib Grafting Matthew J. Provenzano, MD; Stephanie
The Laryngoscope VC 2011 The American Laryngological, Rhinological and Otological Society, Inc. Pediatric Endoscopic Airway Management With Posterior Cricoid Rib Grafting Matthew J. Provenzano, MD; Stephanie
ORIGINAL ARTICLE. Posterior Cricoidotomy Lumen Augmentation for Treatment of Subglottic Stenosis in Children
 Posterior Cricoidotomy Lumen Augmentation for Treatment of Subglottic Stenosis in Children Robert Thomé, PhD; Daniela Curti Thomé, MD ORIGINAL ARTICLE Objectives: To determine the results of posterior
Posterior Cricoidotomy Lumen Augmentation for Treatment of Subglottic Stenosis in Children Robert Thomé, PhD; Daniela Curti Thomé, MD ORIGINAL ARTICLE Objectives: To determine the results of posterior
ORIGINAL ARTICLE. Synchronous Airway Lesions and Outcomes in Infants With Severe Laryngomalacia Requiring Supraglottoplasty
 ORIGINAL ARTICLE Synchronous Airway Lesions and Outcomes in Infants With Severe Laryngomalacia Requiring Supraglottoplasty James W. Schroeder Jr, MD; Naveen D. Bhandarkar, MD; Lauren D. Holinger, MD Objective:
ORIGINAL ARTICLE Synchronous Airway Lesions and Outcomes in Infants With Severe Laryngomalacia Requiring Supraglottoplasty James W. Schroeder Jr, MD; Naveen D. Bhandarkar, MD; Lauren D. Holinger, MD Objective:
Tracheal stenosis in infants and children is typically characterized
 Slide Tracheoplasty for Congenital Tracheal Stenosis Peter B. Manning, MD Tracheal stenosis in infants and children is typically characterized by the presence of complete cartilaginous tracheal rings and
Slide Tracheoplasty for Congenital Tracheal Stenosis Peter B. Manning, MD Tracheal stenosis in infants and children is typically characterized by the presence of complete cartilaginous tracheal rings and
Tracheal Stenosis Following Cuffed Tube Tracheostomy
 Tracheal Stenosis Following Cuffed Tube Tracheostomy Anatomical Variation and Selected Treatment Armand A. Lefemine, M.D., Kenneth MacDonnell, M.D., and Hyung S. Moon, M.D. ABSTRACT Tracheal stenosis resulting
Tracheal Stenosis Following Cuffed Tube Tracheostomy Anatomical Variation and Selected Treatment Armand A. Lefemine, M.D., Kenneth MacDonnell, M.D., and Hyung S. Moon, M.D. ABSTRACT Tracheal stenosis resulting
SURGERY FOR PEDIATRIC SUBGLOTTIC STENOSIS: DISEASE-SPECIFIC OUTCOMES
 Ann Otol Rhinol Laryngol 110:2001 Ann Otol Rhinol Laryngol 110:2001 REPRINTED FROM ANNALS OF OTOLOGY, RHINOLOGY & LARYNGOLOGY December 2001 Volume 110 Number 12 COPYRIGHT 2001, ANNALS PUBLISHING COMPANY
Ann Otol Rhinol Laryngol 110:2001 Ann Otol Rhinol Laryngol 110:2001 REPRINTED FROM ANNALS OF OTOLOGY, RHINOLOGY & LARYNGOLOGY December 2001 Volume 110 Number 12 COPYRIGHT 2001, ANNALS PUBLISHING COMPANY
OTOLARYNGOLOGIC CLINICS ISSUE: PAEDIATRIC LARYNGOTRACHEAL RECONSTRUCTION. Edited by Dr Peter Koltai
 OTOLARYNGOLOGIC CLINICS ISSUE: PAEDIATRIC LARYNGOTRACHEAL RECONSTRUCTION Edited by Dr Peter Koltai Single and Multi Stage Pediatric Laryngotracheal Reconstruction Simone J Boardman, David M Albert Great
OTOLARYNGOLOGIC CLINICS ISSUE: PAEDIATRIC LARYNGOTRACHEAL RECONSTRUCTION Edited by Dr Peter Koltai Single and Multi Stage Pediatric Laryngotracheal Reconstruction Simone J Boardman, David M Albert Great
Chapter 124: Congenital Disorders of the Trachea. Bruce Benjamin
 Chapter 124: Congenital Disorders of the Trachea Bruce Benjamin Investigation of the larynx and pharynx may be incomplete in infants and children with congenital abnormalities without investigation of
Chapter 124: Congenital Disorders of the Trachea Bruce Benjamin Investigation of the larynx and pharynx may be incomplete in infants and children with congenital abnormalities without investigation of
Review of literature suggests that there are three basic theories that attempt to explain the development of laryngomalacia.
 TITLE: Current Concepts in Diagnosis and Management of Laryngomalacia SOURCE: Grand Rounds Presentation, UTMB, Dept. of Otolaryngology DATE: March 31, 2009 FACULTY PHYSICIANS: Shraddha Mukerji, MD and
TITLE: Current Concepts in Diagnosis and Management of Laryngomalacia SOURCE: Grand Rounds Presentation, UTMB, Dept. of Otolaryngology DATE: March 31, 2009 FACULTY PHYSICIANS: Shraddha Mukerji, MD and
IAEM Clinical Guideline 9 Laryngomalacia. Version 1 September, Author: Dr Farah Mustafa
 IAEM Clinical Guideline 9 Laryngomalacia Version 1 September, 2016 Author: Dr Farah Mustafa Guideline lead: Dr Áine Mitchell, in collaboration with IAEM Clinical Guideline committee and Our Lady s Children
IAEM Clinical Guideline 9 Laryngomalacia Version 1 September, 2016 Author: Dr Farah Mustafa Guideline lead: Dr Áine Mitchell, in collaboration with IAEM Clinical Guideline committee and Our Lady s Children
Airway Management in the ICU
 Airway Management in the ICU New developments in management of epistaxis. April 28, 2008 Methods of airway control Non surgical BIPAP CPAP Mask ventilation Laryngeal Mask Intubation Surgical Cricothyrotomy
Airway Management in the ICU New developments in management of epistaxis. April 28, 2008 Methods of airway control Non surgical BIPAP CPAP Mask ventilation Laryngeal Mask Intubation Surgical Cricothyrotomy
The surgical management of subglottic stenosis (SGS)
") Original Research Pediatric Otolaryngology Short- versus Long-term Stenting in Children with Subglottic Stenosis Undergoing Laryngotracheal Reconstruction Otolaryngology Head and Neck Surgery 2018, Vol.
Original Research Pediatric Otolaryngology Short- versus Long-term Stenting in Children with Subglottic Stenosis Undergoing Laryngotracheal Reconstruction Otolaryngology Head and Neck Surgery 2018, Vol.
Idiopathic laryngotracheal stenosis
 Surgical Technique Idiopathic laryngotracheal stenosis Christina L. Costantino, Douglas J. Mathisen Massachusetts General Hospital, Boston, MA 02114, USA Correspondence to: Douglas J. Mathisen, MD. Massachusetts
Surgical Technique Idiopathic laryngotracheal stenosis Christina L. Costantino, Douglas J. Mathisen Massachusetts General Hospital, Boston, MA 02114, USA Correspondence to: Douglas J. Mathisen, MD. Massachusetts
Slide thyrocricotracheoplasty for the treatment of high-grade subglottic stenosis in children
 Journal of Pediatric Surgery (2010) 45, 2317 2321 www.elsevier.com/locate/jpedsurg Slide thyrocricotracheoplasty for the treatment of high-grade subglottic stenosis in children Seong Min Kim a, Jae Ho
Journal of Pediatric Surgery (2010) 45, 2317 2321 www.elsevier.com/locate/jpedsurg Slide thyrocricotracheoplasty for the treatment of high-grade subglottic stenosis in children Seong Min Kim a, Jae Ho
Use of the Silicone T-tube to Treat Tracheal Stenosis or Tracheal Injury
 Use of the Silicone T-tube to Treat Stenosis or Injury Chang-Jer Huang MD Backgound: stenosis or tracheal is a troublesome disease. Traditional temporary tracheostomy and reconstruction can resolve some
Use of the Silicone T-tube to Treat Stenosis or Injury Chang-Jer Huang MD Backgound: stenosis or tracheal is a troublesome disease. Traditional temporary tracheostomy and reconstruction can resolve some
Section 4.1 Paediatric Tracheostomy Introduction
 Bite- sized training from the GTC Section 4.1 Paediatric Tracheostomy Introduction This is one of a series of bite- sized chunks of educational material developed by the Global Tracheostomy Collaborative.
Bite- sized training from the GTC Section 4.1 Paediatric Tracheostomy Introduction This is one of a series of bite- sized chunks of educational material developed by the Global Tracheostomy Collaborative.
4/24/2017. Tracheal Stenosis. Tracheal Stenosis. Tracheal Stenosis. Tracheal Stenosis. Tracheal Stenosis Endoscopic & Surgical Management
 Endoscopic & Surgical Management Pressure ulceration Healing: granulation cicatrization contraction Ann Surg 1969;169:334-348 Gary Schwartz, MD Department of Thoracic Surgery and Lung Transplantation Baylor
Endoscopic & Surgical Management Pressure ulceration Healing: granulation cicatrization contraction Ann Surg 1969;169:334-348 Gary Schwartz, MD Department of Thoracic Surgery and Lung Transplantation Baylor
Preliminary Results of Intraoperative Mitomycin-C in the Treatment and Prevention of Glottic and Subglottic Stenosis
 Journal of Voice Vol. 14, No. 2, pp. 282-286 2000 Singular Publishing Group Preliminary Results of Intraoperative Mitomycin-C in the Treatment and Prevention of Glottic and Subglottic Stenosis *Reza Rahbar,
Journal of Voice Vol. 14, No. 2, pp. 282-286 2000 Singular Publishing Group Preliminary Results of Intraoperative Mitomycin-C in the Treatment and Prevention of Glottic and Subglottic Stenosis *Reza Rahbar,
Case Report Long-Term Outcomes of Balloon Dilation for Acquired Subglottic Stenosis in Children
 Case Reports in Otolaryngology, Article ID 304593, 4 pages http://dx.doi.org/10.1155/2014/304593 Case Report Long-Term Outcomes of Balloon Dilation for Acquired Subglottic Stenosis in Children Aliye Filiz
Case Reports in Otolaryngology, Article ID 304593, 4 pages http://dx.doi.org/10.1155/2014/304593 Case Report Long-Term Outcomes of Balloon Dilation for Acquired Subglottic Stenosis in Children Aliye Filiz
Congenital Laryngeal Anomalies November 2002
 TITLE: Congenital Laryngeal Anomalies SOURCE: Grand Rounds Presentation, UTMB, Dept. of Otolaryngology DATE: November 20, 2002 RESIDENT PHYSICIAN: Russell D. Briggs, M.D. FACULTY ADVISOR: Ronald W. Deskin,
TITLE: Congenital Laryngeal Anomalies SOURCE: Grand Rounds Presentation, UTMB, Dept. of Otolaryngology DATE: November 20, 2002 RESIDENT PHYSICIAN: Russell D. Briggs, M.D. FACULTY ADVISOR: Ronald W. Deskin,
ORIGINAL ARTICLE. Factors Associated With Staged Reconstruction and Successful Stoma Closure in Tracheal Resection and End-to-End Anastomosis
 ORIGINAL ARTICLE Factors Associated With Staged Reconstruction and Successful Stoma Closure in Tracheal Resection and End-to-End Anastomosis Soon-Hyun Ahn, MD; Myung-Whun Sung, MD; Kwang Hyun Kim, MD Background:
ORIGINAL ARTICLE Factors Associated With Staged Reconstruction and Successful Stoma Closure in Tracheal Resection and End-to-End Anastomosis Soon-Hyun Ahn, MD; Myung-Whun Sung, MD; Kwang Hyun Kim, MD Background:
Surgical Management of Advanced and Recurrent Subglottic Stenosis October 2011
 TITLE: Surgical Management of Advanced and Recurrent Subglottic Stenosis SOURCE: Grand Rounds Presentation, University of Texas Medical Branch (UTMB Health), Department of Otolaryngology DATE: October
TITLE: Surgical Management of Advanced and Recurrent Subglottic Stenosis SOURCE: Grand Rounds Presentation, University of Texas Medical Branch (UTMB Health), Department of Otolaryngology DATE: October
Management Of Acquired Laryngotracheal Stenosis Our Experience.
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 15, Issue 2 Ver. XII (Feb. 2016), PP 32-36 www.iosrjournals.org Management Of Acquired Laryngotracheal
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 15, Issue 2 Ver. XII (Feb. 2016), PP 32-36 www.iosrjournals.org Management Of Acquired Laryngotracheal
Subglottic stenosis, with involvement of the lower larynx
 Laryngotracheal Resection and Reconstruction John D. Mitchell, MD n, Subglottic stenosis is being recognized with increasing frequency in adults, and may be the most frequent indication for airway intervention
Laryngotracheal Resection and Reconstruction John D. Mitchell, MD n, Subglottic stenosis is being recognized with increasing frequency in adults, and may be the most frequent indication for airway intervention
Subglottic stenosis in infants and children
 Original Article Singapore Med J 010; 51(1 1) : 88 Subglottic stenosis in infants and children Choo K K M, Tan H K K, Balakrishnan A Yong Loo Lin School of Medicine, National University of Singapore, 10
Original Article Singapore Med J 010; 51(1 1) : 88 Subglottic stenosis in infants and children Choo K K M, Tan H K K, Balakrishnan A Yong Loo Lin School of Medicine, National University of Singapore, 10
I enjoy open airway surgery In 2010: LTRs 28 CTRs 6 Clefts 4 Slides 20
 Michael J. Rutter, FRACS Department of Pediatric Otolaryngology- Head & Neck Surgery Aerodigestive and Esophageal Center Cincinnati Children s Hospital Medical Center Cincinnati, Ohio IPSA Denver, CO June
Michael J. Rutter, FRACS Department of Pediatric Otolaryngology- Head & Neck Surgery Aerodigestive and Esophageal Center Cincinnati Children s Hospital Medical Center Cincinnati, Ohio IPSA Denver, CO June
Contents. Part A Clinical Evaluation of Laryngeal Disorders. 3 Videostroboscopy and Dynamic Voice Evaluation with Flexible Laryngoscopy...
 Contents Part A Clinical Evaluation of Laryngeal Disorders 1 Anatomy and Physiology of the Larynx....... 3 1.1 Anatomy.................................. 3 1.1.1 Laryngeal Cartilages........................
Contents Part A Clinical Evaluation of Laryngeal Disorders 1 Anatomy and Physiology of the Larynx....... 3 1.1 Anatomy.................................. 3 1.1.1 Laryngeal Cartilages........................
FOREIGN BODY ASPIRATION in children. Dr. Xayyavong Bouathongthip, M.D Emergency department, children s hospital
 FOREIGN BODY ASPIRATION in children Dr. Xayyavong Bouathongthip, M.D Emergency department, children s hospital How common is choking? About 3,000 people die/year from choking Figure remained unchanged
FOREIGN BODY ASPIRATION in children Dr. Xayyavong Bouathongthip, M.D Emergency department, children s hospital How common is choking? About 3,000 people die/year from choking Figure remained unchanged
OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY
 OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY VERTICAL PARTIAL LARYNGECTOMY Management of small tumours involving the true vocal folds can be contentious. Tumour control is achieved
OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY VERTICAL PARTIAL LARYNGECTOMY Management of small tumours involving the true vocal folds can be contentious. Tumour control is achieved
Surgical treatment for patients with tracheal and subgllotic stenosis
 Original Research Medical Journal of the Islamic Republic of Iran.Vol. 23, No. 3, November, 2009. pp. 132-138 Surgical treatment for patients with tracheal and subgllotic stenosis Mohammad Naeimi, MD.
Original Research Medical Journal of the Islamic Republic of Iran.Vol. 23, No. 3, November, 2009. pp. 132-138 Surgical treatment for patients with tracheal and subgllotic stenosis Mohammad Naeimi, MD.
ORIGINAL ARTICLE. Unilateral vs Bilateral Supraglottoplasty for Severe Laryngomalacia in Children
 Unilateral vs Bilateral Supraglottoplasty for Severe Laryngomalacia in Children Deepkaran K. Reddy, MD; Bruce H. Matt, MD, MS, FAAP ORIGINAL ARTICLE Objectives: To study the efficacy of unilateral supraglottoplasty
Unilateral vs Bilateral Supraglottoplasty for Severe Laryngomalacia in Children Deepkaran K. Reddy, MD; Bruce H. Matt, MD, MS, FAAP ORIGINAL ARTICLE Objectives: To study the efficacy of unilateral supraglottoplasty
Proceedings of the World Small Animal Veterinary Association Mexico City, Mexico 2005
 Close this window to return to IVIS Proceedings of the World Small Animal Veterinary Association Mexico City, Mexico 2005 Hosted by: Reprinted in the IVIS website with the permission of the WSAVA Surgery
Close this window to return to IVIS Proceedings of the World Small Animal Veterinary Association Mexico City, Mexico 2005 Hosted by: Reprinted in the IVIS website with the permission of the WSAVA Surgery
Management of Pediatric Tracheostomy
 Management of Pediatric Tracheostomy Deepak Mehta Associate Professor Of Otolaryngology Director Pediatric Aerodigestive Center Definitions Tracheotomy: The making of an incision in the trachea The name
Management of Pediatric Tracheostomy Deepak Mehta Associate Professor Of Otolaryngology Director Pediatric Aerodigestive Center Definitions Tracheotomy: The making of an incision in the trachea The name
Stridor, Stertor, and Snoring: Pediatric Upper Airway Obstruction. Nathan Page, MD Pediatrics in the Red Rocks June?
 Stridor, Stertor, and Snoring: Pediatric Upper Airway Obstruction Nathan Page, MD Pediatrics in the Red Rocks June? I have no disclosures I do not plan to discuss unapproved or off label use of products
Stridor, Stertor, and Snoring: Pediatric Upper Airway Obstruction Nathan Page, MD Pediatrics in the Red Rocks June? I have no disclosures I do not plan to discuss unapproved or off label use of products
Surgical Management of Subglottic Stenosis
 Surgical Management of Subglottic Stenosis Cameron D. Wright, MD ubglottic stenosis is usually due to either endotracheal S tube ischemic necrosis or idiopathic larygotracheal stenosis. The ischemic area
Surgical Management of Subglottic Stenosis Cameron D. Wright, MD ubglottic stenosis is usually due to either endotracheal S tube ischemic necrosis or idiopathic larygotracheal stenosis. The ischemic area
Laryngeal split and rib cartilage interpositional grafting: Treatment option for glottic/subglottic stenosis in adults
 General Thoracic Surgery Terra et al Laryngeal split and rib cartilage interpositional grafting: Treatment option for glottic/subglottic stenosis in adults Ricardo Mingarini Terra, MD, Hélio Minamoto,
General Thoracic Surgery Terra et al Laryngeal split and rib cartilage interpositional grafting: Treatment option for glottic/subglottic stenosis in adults Ricardo Mingarini Terra, MD, Hélio Minamoto,
PANELISTS. Controversial Issues In Common Interventions In ORL 4/10/2014
 Controversial Issues In Common Interventions In ORL Mohamed Hesham,MD Alexandria Faculty of Medicine PANELISTS Prof. Ahmed Eldaly Prof. Hamdy EL-Hakim Prof. Hossam Thabet Prof. Maged El-Shenawy Prof. Prince
Controversial Issues In Common Interventions In ORL Mohamed Hesham,MD Alexandria Faculty of Medicine PANELISTS Prof. Ahmed Eldaly Prof. Hamdy EL-Hakim Prof. Hossam Thabet Prof. Maged El-Shenawy Prof. Prince
Evaluation and Management of Pediatric Stridor
 Evaluation and Management of Pediatric Stridor Pamela Nicklaus, MD FACS Associate Professor Fellowship Director Pediatric Otolaryngology Children s Mercy Hospital and Clinics 2013 Children's 2013 Mercy
Evaluation and Management of Pediatric Stridor Pamela Nicklaus, MD FACS Associate Professor Fellowship Director Pediatric Otolaryngology Children s Mercy Hospital and Clinics 2013 Children's 2013 Mercy
Research Article Balloon Dilatation of Pediatric Subglottic Laryngeal Stenosis during the Artificial Apneic Pause: Experience in 5 Children
 BioMed Research International, Article ID 397295, 4 pages http://dx.doi.org/10.1155/2014/397295 Research Article Balloon Dilatation of Pediatric Subglottic Laryngeal Stenosis during the Artificial Apneic
BioMed Research International, Article ID 397295, 4 pages http://dx.doi.org/10.1155/2014/397295 Research Article Balloon Dilatation of Pediatric Subglottic Laryngeal Stenosis during the Artificial Apneic
All bedside percutaneously placed tracheostomies
 Page 1 of 5 Scope: All bedside percutaneously placed tracheostomies Population: All ICU personnel Outcomes: To standardize and outline the steps necessary to safely perform a percutaneous tracheostomy
Page 1 of 5 Scope: All bedside percutaneously placed tracheostomies Population: All ICU personnel Outcomes: To standardize and outline the steps necessary to safely perform a percutaneous tracheostomy
Tracheal T-Tube Stent for Laryngotracheal Stenosis: Ten Year Experience
 Original Article Iranian Journal of Otorhinolaryngology, Vol.26(1), Serial No.74, Jan 2014 Abstract Tracheal T-Tube Stent for Laryngotracheal Stenosis: Ten Year Experience * Arjun Dass 1, Nitin M Nagarkar
Original Article Iranian Journal of Otorhinolaryngology, Vol.26(1), Serial No.74, Jan 2014 Abstract Tracheal T-Tube Stent for Laryngotracheal Stenosis: Ten Year Experience * Arjun Dass 1, Nitin M Nagarkar
Ovid: Van Den Abbeele: Laryngoscope, Volume 109(8).August
.August") Full Text The American Laryngological, Rhinological & Otalogical Society, Inc. Volume 109(8), August 1999, pp 1281-1286 Surgical Removal of Subglottic Hemangiomas in Children [Independent Papers] Van Den
Full Text The American Laryngological, Rhinological & Otalogical Society, Inc. Volume 109(8), August 1999, pp 1281-1286 Surgical Removal of Subglottic Hemangiomas in Children [Independent Papers] Van Den
Subglottic Tracheal Resection
 Subglottic Tracheal Resection Douglas J. Mathisen The most common indication for tracheal resection is stenosis secondary to cuff injury from either tracheostomy tube or endotracheal tube or tracheostomy
Subglottic Tracheal Resection Douglas J. Mathisen The most common indication for tracheal resection is stenosis secondary to cuff injury from either tracheostomy tube or endotracheal tube or tracheostomy
Audra Fuller MD, Mark Sigler MD, Shrinivas Kambali MD, Raed Alalawi MD
 Clinical Series Successful treatment of post-intubation tracheal stenosis with balloon dilation, argon plasma coagulation, electrocautery and application of mitomycin C Audra Fuller MD, Mark Sigler MD,
Clinical Series Successful treatment of post-intubation tracheal stenosis with balloon dilation, argon plasma coagulation, electrocautery and application of mitomycin C Audra Fuller MD, Mark Sigler MD,
Laser Cordectomy. Glottic Carcinoma
 Laser Cordectomy in Glottic Carcinoma Department of Otolaryngology gy Head & Neck Surgery Alexandria University Historical Review Endolaryngeal extirpation of vocal cord cancers is a controversial o issue
Laser Cordectomy in Glottic Carcinoma Department of Otolaryngology gy Head & Neck Surgery Alexandria University Historical Review Endolaryngeal extirpation of vocal cord cancers is a controversial o issue
Wheeze. Dr Jo Harrison
 Wheeze Dr Jo Harrison 9.9.14 Wheeze - Physiology a continuous musical sound that lasts longer than 250 msec. can be high-pitched or low-pitched, consist of single or multiple notes, and occur during inspiration
Wheeze Dr Jo Harrison 9.9.14 Wheeze - Physiology a continuous musical sound that lasts longer than 250 msec. can be high-pitched or low-pitched, consist of single or multiple notes, and occur during inspiration
Congenital Laryngeal Anomalies
 Congenital Laryngeal Anomalies Prof. Hesham Abd Al-Fattah Alexandria - Egypt Embryology Resp primordium 3 rd wk Resp primordium separated by tracheoesophageal folds Fuse to form septum (4-5 wks) Larynx
Congenital Laryngeal Anomalies Prof. Hesham Abd Al-Fattah Alexandria - Egypt Embryology Resp primordium 3 rd wk Resp primordium separated by tracheoesophageal folds Fuse to form septum (4-5 wks) Larynx
Rota-Trach Double Lumen Tracheostomy Tube VITALTEC
 Rota-Trach Double Lumen Tracheostomy Tube VITALTEC Contents INTRODUCTION HISTORY REVIEW ANATOMY & PHYSIOLOGY OPERATIVE PROCEDURE THE RANGE OF TRACHEOSTOMY TUBES ROTA-TRACH TRACHEOSTOMY TUBE INTRODUCTION
Rota-Trach Double Lumen Tracheostomy Tube VITALTEC Contents INTRODUCTION HISTORY REVIEW ANATOMY & PHYSIOLOGY OPERATIVE PROCEDURE THE RANGE OF TRACHEOSTOMY TUBES ROTA-TRACH TRACHEOSTOMY TUBE INTRODUCTION
Anatomy of the Airway
 Anatomy of the Airway Nagelhout, 5 th edition, Chapter 26 Morgan & Mikhail, 5 th edition, Chapter 23 Mary Karlet, CRNA, PhD Airway Anatomy The airway consists of the nose, pharynx, larynx, trachea, and
Anatomy of the Airway Nagelhout, 5 th edition, Chapter 26 Morgan & Mikhail, 5 th edition, Chapter 23 Mary Karlet, CRNA, PhD Airway Anatomy The airway consists of the nose, pharynx, larynx, trachea, and
-Discussed in the Ebers Papyrus and the Rig Veda BC
 Tracheotomy History -Discussed in the Ebers Papyrus and the Rig Veda -1500 BC History -Treatment obstructive diseases (Antyllus, 2 nd century AD) -Discussed in the writings of Braassarolo (1546) -Considered
Tracheotomy History -Discussed in the Ebers Papyrus and the Rig Veda -1500 BC History -Treatment obstructive diseases (Antyllus, 2 nd century AD) -Discussed in the writings of Braassarolo (1546) -Considered
Adult Subglottic Stenosis: Management With Laser Incisions and Mitomycin-C
 The Laryngoscope Lippincott Williams & Wilkins 2008 The American Laryngological, Rhinological and Otological Society, Inc. Adult Subglottic Stenosis: Management With Laser Incisions and Mitomycin-C Frederick
The Laryngoscope Lippincott Williams & Wilkins 2008 The American Laryngological, Rhinological and Otological Society, Inc. Adult Subglottic Stenosis: Management With Laser Incisions and Mitomycin-C Frederick
ORIGINAL ARTICLE. Office-Based Lower Airway Endoscopy in Pediatric Patients. airway symptoms is an integral part of the otolaryngology practice.
 ORIGINAL ARTICLE Office-Based Lower Airway Endoscopy in Pediatric Patients D. Richard Lindstrom III, MD; David T. Book, MD; Stephen F. Conley, MD; Valerie A. Flanary, MD; Joseph E. Kerschner, MD Background:
ORIGINAL ARTICLE Office-Based Lower Airway Endoscopy in Pediatric Patients D. Richard Lindstrom III, MD; David T. Book, MD; Stephen F. Conley, MD; Valerie A. Flanary, MD; Joseph E. Kerschner, MD Background:
3/10/15. Summary. Anatomy Larynx. Anatomy Trachea
 Summary Anatomy Brachycephalic Airway Syndrome (BCAS) Crisis Anatomy Larynx Anatomy Trachea Tracheal rings are incomplete, C-shaped cartilage with the dorsal membrane being completed by tracheal muscle
Summary Anatomy Brachycephalic Airway Syndrome (BCAS) Crisis Anatomy Larynx Anatomy Trachea Tracheal rings are incomplete, C-shaped cartilage with the dorsal membrane being completed by tracheal muscle
Day 2 Pulmonary Breakout Interventional Pulmonology
 Day 2 Pulmonary Breakout Interventional Pulmonology R. Paul Boesch, DO, MS Assistant Professor, Pulmonary Medicine Mayo Clinic Children s Center Interventional Pediatric Pulmonology or Pulm/ENT airway
Day 2 Pulmonary Breakout Interventional Pulmonology R. Paul Boesch, DO, MS Assistant Professor, Pulmonary Medicine Mayo Clinic Children s Center Interventional Pediatric Pulmonology or Pulm/ENT airway
Partial cricotracheal resection for pediatric subglottic stenosis: Long-term outcome in 57 patients
 General Thoracic Surgery Partial cricotracheal resection for pediatric subglottic stenosis: Long-term outcome in 57 patients Yves Jaquet, MD, Florian Lang, MD, Raphaelle Pilloud, MD, Marcel Savary, MD,
General Thoracic Surgery Partial cricotracheal resection for pediatric subglottic stenosis: Long-term outcome in 57 patients Yves Jaquet, MD, Florian Lang, MD, Raphaelle Pilloud, MD, Marcel Savary, MD,
PEMSS PROTOCOLS INVASIVE PROCEDURES
 PEMSS PROTOCOLS INVASIVE PROCEDURES Panhandle Emergency Medical Services System SURGICAL AND NEEDLE CRICOTHYROTOMY Inability to intubate is the primary indication for creating an artificial airway. Care
PEMSS PROTOCOLS INVASIVE PROCEDURES Panhandle Emergency Medical Services System SURGICAL AND NEEDLE CRICOTHYROTOMY Inability to intubate is the primary indication for creating an artificial airway. Care
90 th Annual Meeting The American Association for Thoracic Surgery May 1, 2010 Toronto, Ontario, Canada. Slide Tracheoplasty
 90 th Annual Meeting The American Association for Thoracic Surgery May 1, 2010 Toronto, Ontario, Canada Congenital Skills Course Slide Tracheoplasty Carl Lewis Backer, MD A.C. Buehler Professor of Surgery
90 th Annual Meeting The American Association for Thoracic Surgery May 1, 2010 Toronto, Ontario, Canada Congenital Skills Course Slide Tracheoplasty Carl Lewis Backer, MD A.C. Buehler Professor of Surgery
Laryngomalacia, laryngeal cleft and congenital unilateral vocal cord palsy: A unique case treated endoscopically without intubation or tracheostomy
 Case Report Brunei Int Med J. 2014; 10 (1): 55-59 Laryngomalacia, laryngeal cleft and congenital unilateral vocal cord palsy: A unique case treated endoscopically without intubation or tracheostomy Zara
Case Report Brunei Int Med J. 2014; 10 (1): 55-59 Laryngomalacia, laryngeal cleft and congenital unilateral vocal cord palsy: A unique case treated endoscopically without intubation or tracheostomy Zara
BILATERAL ABDUCTOR VOCAL CORD PALSY. Dr NITYA G Final year PG KIMS
 BILATERAL ABDUCTOR VOCAL CORD PALSY Dr NITYA G Final year PG KIMS INTRODUCTION Vocal cord paralysis is a sign of a disease It results from dysfunction of Recurrent laryngeal nerves on both sides Paralysis
BILATERAL ABDUCTOR VOCAL CORD PALSY Dr NITYA G Final year PG KIMS INTRODUCTION Vocal cord paralysis is a sign of a disease It results from dysfunction of Recurrent laryngeal nerves on both sides Paralysis
Laryngo-tracheal stenosis is a congenital or. A Multi-Modality Surgical Management in Laryngeal Stenosis. Case Series
 Case Series A Multi-Modality Surgical Management in Laryngeal Stenosis Ashfaque Ansari, 1 Annju Thomas 1 ABSTRACT Introduction Postintubation laryngo-tracheal stenosis requires a precise diagnosis and
Case Series A Multi-Modality Surgical Management in Laryngeal Stenosis Ashfaque Ansari, 1 Annju Thomas 1 ABSTRACT Introduction Postintubation laryngo-tracheal stenosis requires a precise diagnosis and
Laryngomalacia: patient outcomes following aryepiglottoplasty at a tertiary care center
 The Turkish Journal of Pediatrics 2013; 55: 524-528 Original Laryngomalacia: patient outcomes following aryepiglottoplasty at a tertiary care center A. Erim Pamuk, Nilda Süslü, R. Önder Günaydın, Gamze
The Turkish Journal of Pediatrics 2013; 55: 524-528 Original Laryngomalacia: patient outcomes following aryepiglottoplasty at a tertiary care center A. Erim Pamuk, Nilda Süslü, R. Önder Günaydın, Gamze
Boston. Medical Products. laryngeal and esophageal products
 Boston Medical Products laryngeal and Innovation, quality and service that define today s Gold Standards. The Montgomery Laryngeal Stent is a molded silicone prosthesis designed to conform to the normal
Boston Medical Products laryngeal and Innovation, quality and service that define today s Gold Standards. The Montgomery Laryngeal Stent is a molded silicone prosthesis designed to conform to the normal
A Randomized Study of Suprastomal Stents in Laryngotracheoplasty Surgery for Grade III Subglottic Stenosis in Children
 The Laryngoscope VC 2013 The American Laryngological, Rhinological and Otological Society, Inc. TRIOLOGICAL SOCIETY CANDIDATE THESIS A Randomized Study of Suprastomal Stents in Laryngotracheoplasty Surgery
The Laryngoscope VC 2013 The American Laryngological, Rhinological and Otological Society, Inc. TRIOLOGICAL SOCIETY CANDIDATE THESIS A Randomized Study of Suprastomal Stents in Laryngotracheoplasty Surgery
Surgical Repair of Iatrogenic Cervical Tracheal Stenosis
 Surgical Repair of Iatrogenic Cervical Tracheal Stenosis Nirmal K. Veeramachaneni, MD, and Bryan F. Meyers, MD, MPH he advent of intensive care unit management has increased the potential opportunities
Surgical Repair of Iatrogenic Cervical Tracheal Stenosis Nirmal K. Veeramachaneni, MD, and Bryan F. Meyers, MD, MPH he advent of intensive care unit management has increased the potential opportunities
CONGENITAL TRACHEAL STENOSIS PRESENTING IN THE NEONATAL PERIOD
 CONGENITAL TRACHEAL STENOSIS PRESENTING IN THE NEONATAL PERIOD J Reiter, C Springer, E Erez Israel Society of Pediatric Pulmonolgy Jerusalem, September 2 nd, 2015 Topics Case Presentation Surgical Intervention
CONGENITAL TRACHEAL STENOSIS PRESENTING IN THE NEONATAL PERIOD J Reiter, C Springer, E Erez Israel Society of Pediatric Pulmonolgy Jerusalem, September 2 nd, 2015 Topics Case Presentation Surgical Intervention
The use of metallic expandable tracheal stents in the management of inoperable malignant tracheal obstruction
 The use of metallic expandable tracheal stents in the management of inoperable malignant tracheal obstruction Alaa Gaafar-MD, Ahmed Youssef-MD, Mohamed Elhadidi-MD A l e x a n d r i a F a c u l t y o f
The use of metallic expandable tracheal stents in the management of inoperable malignant tracheal obstruction Alaa Gaafar-MD, Ahmed Youssef-MD, Mohamed Elhadidi-MD A l e x a n d r i a F a c u l t y o f
Outcomes of Endoscopic Balloon Dilatation for acquired laryngotracheal stenosis in Pediatric Patients: UKMMC Early Experience.
 Case Report Brunei Int Med J. 2017; 13 (1): 36-40 Outcomes of Endoscopic Balloon Dilatation for acquired laryngotracheal stenosis in Pediatric Patients: UKMMC Early Experience. M.Y Soo, B.S Goh, M. Azman
Case Report Brunei Int Med J. 2017; 13 (1): 36-40 Outcomes of Endoscopic Balloon Dilatation for acquired laryngotracheal stenosis in Pediatric Patients: UKMMC Early Experience. M.Y Soo, B.S Goh, M. Azman
Stridor in Children. Agrício Nubiato Crespo and Rodrigo Cesar e Silva
 Stridor in Children Agrício Nubiato Crespo and Rodrigo Cesar e Silva Introduction Stridor can be defined as the audible sign produced by the turbulent air flow through a narrow segment of the respiratory
Stridor in Children Agrício Nubiato Crespo and Rodrigo Cesar e Silva Introduction Stridor can be defined as the audible sign produced by the turbulent air flow through a narrow segment of the respiratory
Organ preservation in laryngeal cancer
 Organ preservation in laryngeal cancer Wojciech Golusiński Department of Head and Neck Surgery The Great Poland Cancer Centre, Poznan, Poland Poznan University of Medical Sciences, Poznan, Poland Silver
Organ preservation in laryngeal cancer Wojciech Golusiński Department of Head and Neck Surgery The Great Poland Cancer Centre, Poznan, Poland Poznan University of Medical Sciences, Poznan, Poland Silver
Congenital Laryngeal Anomalies November 2005
 TITLE: Congenital Laryngeal Anomalies SOURCE: Grand Rounds Presentation, UTMB, Dept. of Otolaryngology DATE: November 2, 2005 RESIDENT PHYSICIAN: Jean P. Font M.D. FACULTY: ADVISOR: Seckin Ulualp, M.D.
TITLE: Congenital Laryngeal Anomalies SOURCE: Grand Rounds Presentation, UTMB, Dept. of Otolaryngology DATE: November 2, 2005 RESIDENT PHYSICIAN: Jean P. Font M.D. FACULTY: ADVISOR: Seckin Ulualp, M.D.
October Paediatric Respiratory Workbook APCP RESPIRATORY COMMITTEE
 October 2017 Paediatric Respiratory Workbook APCP RESPIRATORY COMMITTEE This workbook is designed to introduce to you the difference between paediatric and adult anatomy and physiology. It will also give
October 2017 Paediatric Respiratory Workbook APCP RESPIRATORY COMMITTEE This workbook is designed to introduce to you the difference between paediatric and adult anatomy and physiology. It will also give
Subglottic stenosis in paediatric patients
 Pediatr Pol 2018; 93 (1): 80 85 DOI: https://doi.org/10.5114/polp.2018.74772 Submitted: 4.10.2017, Accepted: 15.11.2017, Published: 28.02.2018 PEDIATRIA Polska PISMO POLSKIEGO TOWARZYSTWA PEDIATRYCZNEGO
Pediatr Pol 2018; 93 (1): 80 85 DOI: https://doi.org/10.5114/polp.2018.74772 Submitted: 4.10.2017, Accepted: 15.11.2017, Published: 28.02.2018 PEDIATRIA Polska PISMO POLSKIEGO TOWARZYSTWA PEDIATRYCZNEGO
Laryngotracheal/Pulmonary Problems and the Mechanically Ventilated Patient: Pediatric Lung Transplantation
 Laryngotracheal/Pulmonary Problems and the Mechanically Ventilated Patient: Pediatric Lung Transplantation G. Kurland, MD Children s Hospital of Pittsburgh Geoffrey.kurland@chp.edu 11/2014 Objectives Discuss
Laryngotracheal/Pulmonary Problems and the Mechanically Ventilated Patient: Pediatric Lung Transplantation G. Kurland, MD Children s Hospital of Pittsburgh Geoffrey.kurland@chp.edu 11/2014 Objectives Discuss
Dundee Focused FRCS ENT Viva Course
 Dundee Focused FRCS ENT Viva Course Choanal atresia Nasal masses Craniofacial Micrognathia Glossomegaly IM Retropharyngeal abscess Caustics Vascular compression FB Bacterial tracheitis TOF Bronchiolitis
Dundee Focused FRCS ENT Viva Course Choanal atresia Nasal masses Craniofacial Micrognathia Glossomegaly IM Retropharyngeal abscess Caustics Vascular compression FB Bacterial tracheitis TOF Bronchiolitis
Tracheal Trauma: Management and Treatment. Kosmas Iliadis, MD, PhD, FECTS
 Tracheal Trauma: Management and Treatment Kosmas Iliadis, MD, PhD, FECTS Thoracic Surgeon Director of Thoracic Surgery Department Hygeia Hospital, Athens INTRODUCTION Heterogeneous group of injuries mechanism
Tracheal Trauma: Management and Treatment Kosmas Iliadis, MD, PhD, FECTS Thoracic Surgeon Director of Thoracic Surgery Department Hygeia Hospital, Athens INTRODUCTION Heterogeneous group of injuries mechanism
Therapeutic Bronchoscopy Etiology - Benign Stenosis Post - intubation Trauma Post - operative Inflammatory Idiopathic
 Endobronchial Palliation of Airway Disease Douglas E. Wood, MD Professor and Chief Division of Cardiothoracic Surgery Vice-Chair, Department of Surgery Endowed Chair in Lung Cancer Research University
Endobronchial Palliation of Airway Disease Douglas E. Wood, MD Professor and Chief Division of Cardiothoracic Surgery Vice-Chair, Department of Surgery Endowed Chair in Lung Cancer Research University
Steroid Therapy for Tracheal Stenosis in Children
 Steroid Therapy for Tracheal Stenosis in Children Clinical Experience in 4 Children with Severe Strictures H. Biemann Othersen, Jr., M.D. ABSTRACT Recently a refinement in the treatment of tracheal stenosis
Steroid Therapy for Tracheal Stenosis in Children Clinical Experience in 4 Children with Severe Strictures H. Biemann Othersen, Jr., M.D. ABSTRACT Recently a refinement in the treatment of tracheal stenosis
CHAPTER 7 Procedures on Respiratory System
 CHAPTER 7 Propunere noua clasificare proceduri folosind codificarea ICD-10-AM versiunea 3, 30 martie 2004 Procedures on Respiratory System BLOCK 520 Examination procedures on larynx 41764-03 Fibreoptic
CHAPTER 7 Propunere noua clasificare proceduri folosind codificarea ICD-10-AM versiunea 3, 30 martie 2004 Procedures on Respiratory System BLOCK 520 Examination procedures on larynx 41764-03 Fibreoptic
A case of a neonate with a congenital laryngeal web: management of a difficult airway and intra-operative complications
 A case of a neonate with a congenital laryngeal web: management of a difficult airway and intra-operative complications Moderators: Marcellene Franzen, MD Fellow in Pediatric Anesthesiology Medical College
A case of a neonate with a congenital laryngeal web: management of a difficult airway and intra-operative complications Moderators: Marcellene Franzen, MD Fellow in Pediatric Anesthesiology Medical College
DR. SAAD AL-MUHAYAWI, M.D., FRCSC. ORL Head & Neck Surgery
 TRAUMA IN ORL DR. SAAD AL-MUHAYAWI, M.D., FRCSC Associate Professor & Consultant ORL Head & Neck Surgery TYPES OF TRAUMA EAR & TEMPORAL BONE TRAUMA NOSE & FACIAL BONES TRAUMA LARYNGEAL TRAUMA NECK TRAUMA
TRAUMA IN ORL DR. SAAD AL-MUHAYAWI, M.D., FRCSC Associate Professor & Consultant ORL Head & Neck Surgery TYPES OF TRAUMA EAR & TEMPORAL BONE TRAUMA NOSE & FACIAL BONES TRAUMA LARYNGEAL TRAUMA NECK TRAUMA
Early management of laryngeal injuries'
 656 Journal of the Royal Society of Medicine Volume 74 September 1981 Early management of laryngeal injuries' A G D Maran MD FRCS Department of Otolaryngology, P M Stell chm FRCS Department of Otolaryngology,
656 Journal of the Royal Society of Medicine Volume 74 September 1981 Early management of laryngeal injuries' A G D Maran MD FRCS Department of Otolaryngology, P M Stell chm FRCS Department of Otolaryngology,
International Journal of Health Sciences and Research ISSN:
 International Journal of Health Sciences and Research www.ijhsr.org ISSN: 2249-9571 Case Report Varied Presentation and Management of Tracheal Polyps in Children Vinod M Raj 1, Varun Hathiramani 2, Swathi
International Journal of Health Sciences and Research www.ijhsr.org ISSN: 2249-9571 Case Report Varied Presentation and Management of Tracheal Polyps in Children Vinod M Raj 1, Varun Hathiramani 2, Swathi
A study on paediatric stridor causes and management: case series
 International Journal of Otorhinolaryngology and Head and Neck Surgery Selvam DK et al. Int J Otorhinolaryngol Head Neck Surg. 2017 Oct;3(4):1031-1035 http://www.ijorl.com pissn 2454-5929 eissn 2454-5937
International Journal of Otorhinolaryngology and Head and Neck Surgery Selvam DK et al. Int J Otorhinolaryngol Head Neck Surg. 2017 Oct;3(4):1031-1035 http://www.ijorl.com pissn 2454-5929 eissn 2454-5937
Discussing feline tracheal disease
 Vet Times The website for the veterinary profession https://www.vettimes.co.uk Discussing feline tracheal disease Author : ANDREW SPARKES Categories : Vets Date : March 24, 2008 ANDREW SPARKES aims to
Vet Times The website for the veterinary profession https://www.vettimes.co.uk Discussing feline tracheal disease Author : ANDREW SPARKES Categories : Vets Date : March 24, 2008 ANDREW SPARKES aims to