Evaluation and Management of Pediatric Stridor
|
|
|
- Shona Verity McDowell
- 5 years ago
- Views:
Transcription






1 Evaluation and Management of Pediatric Stridor Pamela Nicklaus, MD FACS Associate Professor Fellowship Director Pediatric Otolaryngology Children s Mercy Hospital and Clinics 2013 Children's 2013 Mercy Children's Hospitals Mercy and Hospitals Clinics. All and Rights Clinics. Reserved. All Rights 03/13 Reserved. 03/13
2 Overview Definitions Case presentations of stridor by location Evaluation Treatment 2

3 Anatomy review: 3

4 Anatomy review: real time Video: Behold, the human larynx! 4

5 Child vs. adult airway 1. A child s larynx is located HIGHER in the neck than the adult 5
")
6 Child vs. adult airway 2. A child s airway is narrower and more conical Cricoid (subglottis) considered narrowest portion of child s larynx 6






7 Remember college Physics? Poiseuille s (pwaa-zuhee) Law: Resistance inversely proportional to radius to 4 th power Bernoulli s Law: Pressure decreases as velocity increases, causing tendency to collapse Resistance 16x 3x 2013 Children's Mercy Hospitals and Clinics. All Rights Reserved. 01/13 03/13
8 Child vs. adult airway 3. A child s laryngeal and tracheal cartilages are softer, more dynamic, cause of malacia Over time, both growth and mineralization of the cartilages make these structures more rigid On the plus side, laryngeal fractures are less common in children. 8

 2013 Children's Mercy Hospitals and Clinics. All Rights Reserved.")
9 Stridor: Definitions Stridor: Harsh, high-pitched, musical sound produced by turbulent airflow through partially obstructed airway Inspiratory Expiratory Biphasic Stertor: Low-pitched inspiratory sound from nose/pharynx (like snoring) 2013 Children's Mercy Hospitals and Clinics. All Rights Reserved. 01/13 03/13

10 This 2 month old patient presents to your office Video: 10
11 Assessment: Localization of stridor Inspiratory stridor (high-pitched)- Supraglottic 2013 Children's Mercy Hospitals and Clinics. All Rights Reserved. 01/13 03/13
12 Assessment strategies 1. Assess acuity! Is this evolving rapidly? Fever Drooling (new onset) Rapid change in cry or voice New food aversion New retractions/nasal flaring Body position (arching) Fatigue 12
13 Assessment strategies 2. Obtain Airway History/chronicity Acute? Progressive? Prior respiratory problems? ALTEs aspiration pneumonias croup like episodes History of prematurity History of intubation Difficult intubation? #? Length of time intubated? 13
14 Assessment strategies 3. Review associated symptoms Feeding adequacy and diet Failure to thrive Choking episodes Consistency of food? Liquids vs. solids? Frequent spitting up/reflux history Apneas Perioral cyanosis or blue spells 14
15 Assessment strategies 4. Exam Vitals with continuous pulse oximetry Assess work of breathing Accessory muscle use, retractions Quality of stridor Describe Pitch, intensity Inspiratory/biphasic/expiratory Improve with prone or side positioning? Worsen with crying/agitation/feeding? 15


16 Laryngomalacia Video: Laryngeal collapse during breathing 16

17 LARYNGOMALACIA- common Most common cause of inspiratory stridor in the newborn Typically begins after several weeks of life Increases with feeding, exertion Feeding problems common GERD common due to negative intrathoracic pressures required for breathing Respiratory distress, apnea, and cyanosis may occur 2013 Children's Mercy Hospitals and Clinics. All Rights Reserved. 01/13 03/13




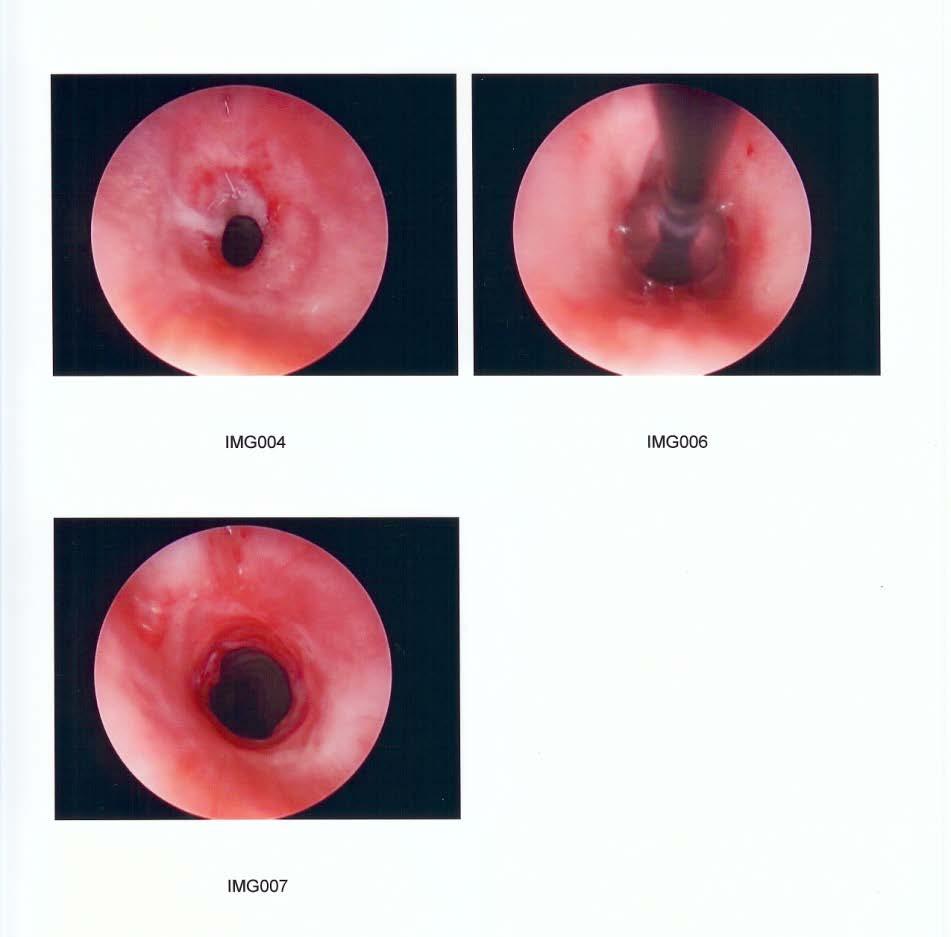
18 Laryngopharyngeal reflux : signs Erythema Cobblestoning Pretreatment Severe Edema Edema + Erythema Normal After 6 months PPI Image from


19 LARYNGOMALACIA Self limited disorder- parents can be counseled that 90% of cases resolve by age 2. Lots of assurance Reflux therapy Supraglottoplasty or temporary tracheostomy required in ~10% Indicated for failure to thrive, prolonged feeding, recurrent ER visits, or cyanosis/severe apnea, and rarely parental anxiety Children's Mercy Hospitals and Clinics. All Rights Reserved. 01/13 03/13

20 This 2 month old patient presents to your office Video: Note: Biphasic stridor with lower pitch Difficulty feeding 20
21 Assessment: Localization of stridor Biphasic stridor: intermediate pitch Fixed lesion Glottis & Subglottis Extrathoracic (proximal) trachea 2013 Children's Mercy Hospitals and Clinics. All Rights Reserved. 01/13 03/13
 22")
22 Tracheomalacia Primary Congenitally weak/insufficient tracheal cartilage Secondary Tracheal compression or weakening caused by Esophageal atresia Vascular rings/slings External Mass lesions Prior surgery (tracheostomy, TEF repair) 22
23 Management of tracheomalacia Primary: Similar to laryngomalacia will generally improve with time. Often associated with concurrent laryngomalacia Positive pressure ventilation/cpap Severe malacia may require temporary tracheostomy Secondary: depending on etiology may improve or worsen with time. Removal of mass lesions Vascular surgery Resection and reanastomosis of weak segment if isolated. (I.e. esophageal atresia site) 23
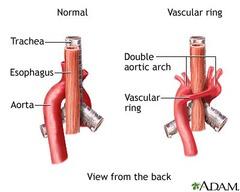

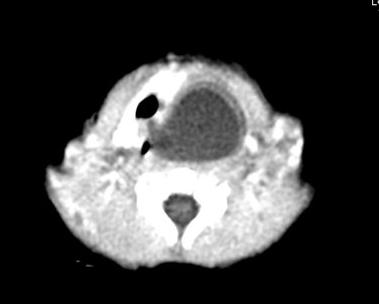
24 Tracheal compression 24

25 This infant presents to your office with recurrent croup, but no other URI symptoms: Video: recurrent croup patient 25


26 Subglottic hemangioma biphasic stridor Looks, sounds, and acts like croup. Progressive symptoms starting in first few weeks of life. Often responds to nebulized epinephrine and oral/iv steroids Higher likelihood in patients with cutaneous hemangiomas but not always! Esp beard distribution hemangiomas 26

27 Subglottic Hemangioma: management Capillary proliferate rapidly then involute around age 5 Medical management: Propranolol (oral) New gold standard, typically begins working within days. Corticosteroids useful if propranolol contraindicated or in acute situations Surgical management: Intubation and/or tracheostomy may be required in severe cases. Intralesional injections of steroid Endoscopic or open Excision becoming less common 27

28 Same Patient History of prematurity and intubation History of intubation and RSV History of cardiac surgery and prolonged intubation Even have a history of no intubation Flexible endoscopy and see nothing 28

")
29 Subglottic stenosis biphasic stridor Congenital ( shelves / elliptical cricoid ) Acquired 29

30 Subglottic stenosis Cotton Myer Grading system: based on percentage luminal obstruction Grade I % Grade II % Grade III % Grade IV - 100% 30
31 Subglottic Stenosis: Management Depends on type of stricture and location Membranous (thin) acquired strictures Dilation CO2 laser or sharp excision + dilation Thick strictures, +/- cartilaginous component Bypass: Tracheostomy (bypass obstruction) Resect: Cricotracheal resection with primary anastomosis Augment: Laryngotracheal reconstruction with cartilage grafting 31

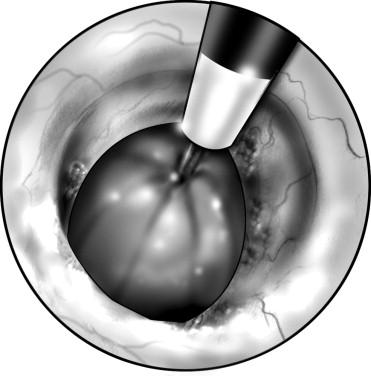
32 Balloon dilation 32

33 Open Surgical Management Augmentation 33

34 Open Surgical Management Bypass Resect 34

35 Other Causes of Biphasic Stridor 2013 Children's Mercy Hospitals and Clinics. All Rights Reserved. 03/13
36 Bilateral Vocal Fold Paralysis biphasic stridor Unilateral vocal fold paralysis does not commonly cause stridor evaluate for other causes! Bilateral vocal fold paralysis: progressive stridor as vocal cords migrate to a paramedian position Causes: Idiopathic, birth trauma, neurologic, hypoxemia at birth, iatrogenic Rule out arnold chiari malformation and hydrocephalus with MRI 36

37 Laryngeal Web biphasic stridor Rare Associated w/ Chromosome 22q11 deletion in 50% Often discovered or lysed with intubation. Thin webs : endoscopic repair Thicker webs: open surgery 37


38 Recurrent Respiratory Papillomatosis biphasic stridor 38


39 Other acquired lesions: biphasic stridor Laryngeal granuloma Subglottic cysts 39
40 1 year old presents with a funny wheeze Mom state that he is just not right Growing well Eats just fine On exam he appears healthy He has no inspiratory stridor He does have an expiratory noise, not quite a wheeze When he gets a cold it seems his mucous gets stuck and he can t cough it out 40
41 Assessment: Localization of stridor Expiratory stridor Lower pitched (wheeze or rattle) Intrathoracic trachea/bronchi 2013 Children's Mercy Hospitals and Clinics. All Rights Reserved. 01/13 03/13


42 Tracheal Stenosis Congenital Acquired High morbidity and mortality Conservative Resection vs. augmentation 2013 Children's Mercy Hospitals and Clinics. All Rights Reserved. 03/13


43 Other causes of expiratory stridor Foreign Body Distal tracheomalacia Bronchomalacia 43

44 2 year old present to the ED with stridor and barky cough and looks like this Note features: Biphasic stridor Often louder with inspiratory phase barky cough Viral Croup Video 44


45 Viral Croup (laryngotracheobronchitis) Most common cause of stridor after neonatal period Most affected are children 6 mo.- 3 y.o Peak incidence 1-2 yrs. of age Narrowest part of airway is at cricoid cartilage In children 1 mm of airway edema may crosssectional area 50-60% Most cases occur late fall or early winter Para influenza 2013 Children's Mercy Hospitals and Clinics. All Rights Reserved. 01/13 03/13



46 VIRAL CROUP Diagnosis- typically made clinically X-rays: If atypical or prolonged cases Obtain lateral neck films and PA CXR PA CXR in croup steeple sign 2013 Children's Mercy Hospitals and Clinics. All Rights Reserved. 01/13 03/13

47 Management: Isolated Croup Typically supportive Oral/IV Corticosteroids and nebulized epinephrine can be helpful for severe symptoms 2013 Children's Mercy Hospitals and Clinics. All Rights Reserved. 01/13 03/13

48 2 year old present to ED with croup symptoms for several days, but now with high fever, listless, elevated heart and respiratory rate Parents say that he scared them when he was trying to cough and could not seem to breath at all Bacterial tracheitis Often Staph superimposed after viral infection Humidification and antibiotics May need bronch,debridement and intubation especially younger children 48
49 More about recurrent croup. My child gets croup every time he gets a cold! Suspect Structural or functional ENT abnormality Subglottic lesion or stenosis Intubation history Hemangioma, foreign body, tumor Chronic laryngopharyngeal reflux Chronic aspiration- laryngeal cleft, vocal fold weakness Allergic/Spasmodic Research says everyone should be bronched and other saying only high risk need bronch 49

50 Child with one day history of sore throat, decreased oral intake, difficulty breathing, listless, fever, elevated heart rate. Video: Note: child looks very ill. stridor is variable; may be absent. Expiratory noises due to difficulty controlling secretions. 50

51 Epiglottitis/Supraglottitis Clinical Picture Less likely in infants, more common in older children and adults Decreased incidence in children secondary to HIB vaccine Onset rapid, patients look toxic Patients prefer to sit upright muffled voice, dysphagia, drooling, restlessness 2013 Children's Mercy Hospitals and Clinics. All Rights Reserved. 03/13

52 EPIGLOTTITIS: lateral neck film Normal Epiglottis 2013 Children's Mercy Hospitals and Clinics. All Rights Reserved. 03/13 Epiglottitis: thumb sign

53 Management of supraglottitis If losing airway, prepare for intubation Choose ETT one size smaller than usual Otherwise, start O2, obtain detailed history, IV access. Do not try to examine or anesthetize the nose or throat in patient with symptomatic stridor as this may induce panic, laryngospasm and total airway obstruction 53
54 Stridor by location: Supraglottic Inspiratory stridor High pitched typically increases with exertion. (bernoulli s law) Differential laryngomalacia or supraglottic lesion Infectious- supraglotitis 54
55 Biphasic stridor Stridor by location: Glottic/Subglottic typically increases with exertion. Ddx: Child Foreign body obstruction Vocal fold paralysis Subglottic/glottic stenosis Cyst or granuloma Tracheomalacia Tumors: papilloma, hemangioma Infectious - croup 55
56 Low biphasic or expiratory stridor Stridor by location: typically increases with exertion. Ddx: Tracheomalacia Vascular ring Tracheal stricture Complete tracheal rings Foreign body Trachea 56
57 Key points Paying attention to quality of stridor can help point to the source Most common cause of stridor in infants is laryngomalacia but few will require surgery Flexible fiberoptic scope exam can help determine etiology from level of vocal cords and up. 57



58 2013 Children's Mercy Hospitals and Clinics. All Rights Reserved. 01/13 03/13
Disclosure Statement The Squeaky Baby
 Disclosure Statement The Squeaky Baby A Pediatric Provider s Guide to Stridor in the Young Child I have no actual or potential conflict of interest in relation to this program. Daniel Jensen, MD Assistant
Disclosure Statement The Squeaky Baby A Pediatric Provider s Guide to Stridor in the Young Child I have no actual or potential conflict of interest in relation to this program. Daniel Jensen, MD Assistant
Stridor, Stertor, and Snoring: Pediatric Upper Airway Obstruction. Nathan Page, MD Pediatrics in the Red Rocks June?
 Stridor, Stertor, and Snoring: Pediatric Upper Airway Obstruction Nathan Page, MD Pediatrics in the Red Rocks June? I have no disclosures I do not plan to discuss unapproved or off label use of products
Stridor, Stertor, and Snoring: Pediatric Upper Airway Obstruction Nathan Page, MD Pediatrics in the Red Rocks June? I have no disclosures I do not plan to discuss unapproved or off label use of products
IAEM Clinical Guideline 9 Laryngomalacia. Version 1 September, Author: Dr Farah Mustafa
 IAEM Clinical Guideline 9 Laryngomalacia Version 1 September, 2016 Author: Dr Farah Mustafa Guideline lead: Dr Áine Mitchell, in collaboration with IAEM Clinical Guideline committee and Our Lady s Children
IAEM Clinical Guideline 9 Laryngomalacia Version 1 September, 2016 Author: Dr Farah Mustafa Guideline lead: Dr Áine Mitchell, in collaboration with IAEM Clinical Guideline committee and Our Lady s Children
STRIDOR. Respiratory system. Lecture
 STRIDOR Stridor is a continuous inspiratory harsh sound produced by partial obstruction in the region of the larynx or trachea. Total obstruction cyanosis & death. Etiology Acute stridor Infectious croup
STRIDOR Stridor is a continuous inspiratory harsh sound produced by partial obstruction in the region of the larynx or trachea. Total obstruction cyanosis & death. Etiology Acute stridor Infectious croup
Neonatal Airway Disorders, Treatments, and Outcomes. Steven Goudy, MD Pediatric Otolaryngology Emory University Medical Center
 Neonatal Airway Disorders, Treatments, and Outcomes Steven Goudy, MD Pediatric Otolaryngology Emory University Medical Center Disclosure I have nothing to disclose Neonatal and Pediatric Tracheostomy Tracheostomy
Neonatal Airway Disorders, Treatments, and Outcomes Steven Goudy, MD Pediatric Otolaryngology Emory University Medical Center Disclosure I have nothing to disclose Neonatal and Pediatric Tracheostomy Tracheostomy
Epiglottitis. Bronchitis. Bronchiolitis. Pneumonia. Croup syndrome. Miss. kamlah 2
 Miss. kamlah 1 Epiglottitis. Bronchitis. Bronchiolitis. Pneumonia. Croup syndrome. Miss. kamlah 2 Acute Epiglottitis Is an infection of the epiglottis, the long narrow structure that closes off the glottis
Miss. kamlah 1 Epiglottitis. Bronchitis. Bronchiolitis. Pneumonia. Croup syndrome. Miss. kamlah 2 Acute Epiglottitis Is an infection of the epiglottis, the long narrow structure that closes off the glottis
Upper Airway Obstruction
 Upper Airway Obstruction Adriaan Pentz Division of Otorhinolaryngology University of Stellenbosch and Tygerberg Hospital Stridor/Stertor Auditory manifestations of disordered respiratory function ie noisy
Upper Airway Obstruction Adriaan Pentz Division of Otorhinolaryngology University of Stellenbosch and Tygerberg Hospital Stridor/Stertor Auditory manifestations of disordered respiratory function ie noisy
Multilevel airway obstruction including rare tongue base mass presenting as severe croup in an infant. Tara Brennan, MD 2,3
 Multilevel airway obstruction including rare tongue base mass presenting as severe croup in an infant Tara Brennan, MD 2,3 Jeffrey C. Rastatter, MD, FAAP 1,2 1 Department of Otolaryngology, Northwestern
Multilevel airway obstruction including rare tongue base mass presenting as severe croup in an infant Tara Brennan, MD 2,3 Jeffrey C. Rastatter, MD, FAAP 1,2 1 Department of Otolaryngology, Northwestern
PedsCases Podcast Scripts
 PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Chronic Stridor in Children These podcasts are designed to give medical students an overview of key topics in pediatrics.
PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Chronic Stridor in Children These podcasts are designed to give medical students an overview of key topics in pediatrics.
Complex Airway problems - Paediatric Perspective
 Complex Airway problems - Paediatric Perspective Dave Albert BACO Liverpool 2009 www.albert.uk.com Complex Ξ not simple, multiple parts Multiple problems with airway Combined Web/stenosis/multiple levels
Complex Airway problems - Paediatric Perspective Dave Albert BACO Liverpool 2009 www.albert.uk.com Complex Ξ not simple, multiple parts Multiple problems with airway Combined Web/stenosis/multiple levels
Pediatric Airway Disorders Speaker Disclosure Outline
 Pediatric Airway Disorders G. Paul Digoy, M.D. Director of Pediatric Otolaryngology OU Health Sciences Center Paul-Digoy@ouhsc.edu Office: 405 271-5504 Speaker Disclosure Speakers, moderators, or panelists
Pediatric Airway Disorders G. Paul Digoy, M.D. Director of Pediatric Otolaryngology OU Health Sciences Center Paul-Digoy@ouhsc.edu Office: 405 271-5504 Speaker Disclosure Speakers, moderators, or panelists
4. Neoplastic: benign & malignant. 5. Allergic rhinitis & nasal polyp. 6. hypertrophied tonsils or adenoids. L 5
 L 5 Stertor& Stridor Stertor& stridor are both auditory manifestation of disordered respiratory function. Stertor: Is a low pitched snoring or snuffly sound caused by obstruction of the airway above the
L 5 Stertor& Stridor Stertor& stridor are both auditory manifestation of disordered respiratory function. Stertor: Is a low pitched snoring or snuffly sound caused by obstruction of the airway above the
Airway Endoscopy The Basics Neonatal Progressive Acute Quiz
 Endoscopy of the Airway Dave Albert Airway Endoscopy The Basics Neonatal Progressive Acute Quiz The laws of Poiseuille and Bernoulli French physician,physicist mathemetician and Dutch Swiss mathemetician
Endoscopy of the Airway Dave Albert Airway Endoscopy The Basics Neonatal Progressive Acute Quiz The laws of Poiseuille and Bernoulli French physician,physicist mathemetician and Dutch Swiss mathemetician
Unilateral Supraglottoplasty for Severe Laryngomalacia in Children. Nasser A Fageeh, MD, FRCSC, FACS*
 Bahrain Medical Bulletin, Vol. 37, No. 1, March 2015 Unilateral Supraglottoplasty for Severe Laryngomalacia in Children Nasser A Fageeh, MD, FRCSC, FACS* Objective: To study the efficacy of Unilateral
Bahrain Medical Bulletin, Vol. 37, No. 1, March 2015 Unilateral Supraglottoplasty for Severe Laryngomalacia in Children Nasser A Fageeh, MD, FRCSC, FACS* Objective: To study the efficacy of Unilateral
McHenry Western Lake County EMS System Optional CE for Paramedics, EMT-B and PHRN s Croup vs. Epiglottitis. Optional #2 2017
 McHenry Western Lake County EMS System Optional CE for Paramedics, EMT-B and PHRN s Croup vs. Epiglottitis Optional #2 2017 The tones go out at 3 am for a child with difficulty breathing. As it is a kid
McHenry Western Lake County EMS System Optional CE for Paramedics, EMT-B and PHRN s Croup vs. Epiglottitis Optional #2 2017 The tones go out at 3 am for a child with difficulty breathing. As it is a kid
Wheeze. Dr Jo Harrison
 Wheeze Dr Jo Harrison 9.9.14 Wheeze - Physiology a continuous musical sound that lasts longer than 250 msec. can be high-pitched or low-pitched, consist of single or multiple notes, and occur during inspiration
Wheeze Dr Jo Harrison 9.9.14 Wheeze - Physiology a continuous musical sound that lasts longer than 250 msec. can be high-pitched or low-pitched, consist of single or multiple notes, and occur during inspiration
Pediatrics Grand Rounds 25 October University of Texas Health Science Center at San Antonio, Texas
 PEDIATRIC ENT & YOU A PATIENT CARE PARTNERSHIP Disclosure Timothy McEvoy, MD has no relevant relationships with commercial interests to disclose. Timothy McEvoy, MD UTHSCSA Department of Otolaryngology-
PEDIATRIC ENT & YOU A PATIENT CARE PARTNERSHIP Disclosure Timothy McEvoy, MD has no relevant relationships with commercial interests to disclose. Timothy McEvoy, MD UTHSCSA Department of Otolaryngology-
Dundee Focused FRCS ENT Viva Course
 Dundee Focused FRCS ENT Viva Course Choanal atresia Nasal masses Craniofacial Micrognathia Glossomegaly IM Retropharyngeal abscess Caustics Vascular compression FB Bacterial tracheitis TOF Bronchiolitis
Dundee Focused FRCS ENT Viva Course Choanal atresia Nasal masses Craniofacial Micrognathia Glossomegaly IM Retropharyngeal abscess Caustics Vascular compression FB Bacterial tracheitis TOF Bronchiolitis
Basic Science Review Wound Healing
 Subglottic Stenosis Deborah P. Wilson, M.D. Faculty Advisor: Norman Friedman, M.D. The University of Texas Medical Branch Department of Otolaryngology Grand Rounds Presentation April 14, 1999 Basic Science
Subglottic Stenosis Deborah P. Wilson, M.D. Faculty Advisor: Norman Friedman, M.D. The University of Texas Medical Branch Department of Otolaryngology Grand Rounds Presentation April 14, 1999 Basic Science
Neonatal Stridor. Neonatology Roy Rajan, MD. Assistant Professor, Pediatric Otolaryngology Emory University
 Neonatal Stridor Neonatology 2015 Roy Rajan, MD Assistant Professor, Pediatric Otolaryngology Emory University Disclosures None 2 Goals/Objectives Describe embryology related to laryngeal development Define
Neonatal Stridor Neonatology 2015 Roy Rajan, MD Assistant Professor, Pediatric Otolaryngology Emory University Disclosures None 2 Goals/Objectives Describe embryology related to laryngeal development Define
Section 4.1 Paediatric Tracheostomy Introduction
 Bite- sized training from the GTC Section 4.1 Paediatric Tracheostomy Introduction This is one of a series of bite- sized chunks of educational material developed by the Global Tracheostomy Collaborative.
Bite- sized training from the GTC Section 4.1 Paediatric Tracheostomy Introduction This is one of a series of bite- sized chunks of educational material developed by the Global Tracheostomy Collaborative.
Stridor in Children. Agrício Nubiato Crespo and Rodrigo Cesar e Silva
 Stridor in Children Agrício Nubiato Crespo and Rodrigo Cesar e Silva Introduction Stridor can be defined as the audible sign produced by the turbulent air flow through a narrow segment of the respiratory
Stridor in Children Agrício Nubiato Crespo and Rodrigo Cesar e Silva Introduction Stridor can be defined as the audible sign produced by the turbulent air flow through a narrow segment of the respiratory
Airway Concerns. Trouble Breathing. Anywhere from nose to lungs. Neonates are obligate nasal breathers. Nasal symptoms:
 Pediatric Airway Naren Venkatesan, MD Mentor: Harold Pine, MD The University of Texas Medical Branch (UTMB Health) Department of Otolaryngology Head & Neck Surgery Grand Rounds Presentation April 26, 2013
Pediatric Airway Naren Venkatesan, MD Mentor: Harold Pine, MD The University of Texas Medical Branch (UTMB Health) Department of Otolaryngology Head & Neck Surgery Grand Rounds Presentation April 26, 2013
Tracheoesophageal Fistula and Esophageal Atresia
 Patient and Family Education Tracheoesophageal Fistula and Esophageal Atresia What is tracheoesophageal fistula? The word fistula means abnormal connection. Tracheoesophageal fistula (TEF) is a condition
Patient and Family Education Tracheoesophageal Fistula and Esophageal Atresia What is tracheoesophageal fistula? The word fistula means abnormal connection. Tracheoesophageal fistula (TEF) is a condition
CONGENITAL TRACHEAL STENOSIS PRESENTING IN THE NEONATAL PERIOD
 CONGENITAL TRACHEAL STENOSIS PRESENTING IN THE NEONATAL PERIOD J Reiter, C Springer, E Erez Israel Society of Pediatric Pulmonolgy Jerusalem, September 2 nd, 2015 Topics Case Presentation Surgical Intervention
CONGENITAL TRACHEAL STENOSIS PRESENTING IN THE NEONATAL PERIOD J Reiter, C Springer, E Erez Israel Society of Pediatric Pulmonolgy Jerusalem, September 2 nd, 2015 Topics Case Presentation Surgical Intervention
Society of Rural Physicians of Canada 26TH ANNUAL RURAL AND REMOTE MEDICINE COURSE ST. JOHN'S NEWFOUNDLAND AND LABRADOR APRIL 12-14, 2018
 Society of Rural Physicians of Canada 26TH ANNUAL RURAL AND REMOTE MEDICINE COURSE ST. JOHN'S NEWFOUNDLAND AND LABRADOR APRIL 12-14, 2018 Dr. Andrea Losier OTTAWA ON 332 PEDS ER CASES Pediatric ED Cases
Society of Rural Physicians of Canada 26TH ANNUAL RURAL AND REMOTE MEDICINE COURSE ST. JOHN'S NEWFOUNDLAND AND LABRADOR APRIL 12-14, 2018 Dr. Andrea Losier OTTAWA ON 332 PEDS ER CASES Pediatric ED Cases
Subject Index. Bacterial infection, see Suppurative lung disease, Tuberculosis
 Subject Index Abscess, virtual 107 Adenoidal hypertrophy, features 123 Airway bleeding, technique 49, 50 Airway stenosis, see Stenosis, airway Anaesthesia biopsy 47 complications 27, 28 flexible 23 26
Subject Index Abscess, virtual 107 Adenoidal hypertrophy, features 123 Airway bleeding, technique 49, 50 Airway stenosis, see Stenosis, airway Anaesthesia biopsy 47 complications 27, 28 flexible 23 26
Acute Laryngitis in Childhood
 Acute Laryngitis in Childhood Hany Simon Junior Viral croup Definition The term croup syndrome characterizes a group of diseases with variable anatomic involvement and etiology, and is clinically manifested
Acute Laryngitis in Childhood Hany Simon Junior Viral croup Definition The term croup syndrome characterizes a group of diseases with variable anatomic involvement and etiology, and is clinically manifested
Objectives. Case Presentation. Respiratory Emergencies
 Respiratory Emergencies Objectives Describe how to assess airway and breathing, including interpreting information from the PAT and ABCDEs. Differentiate between respiratory distress, respiratory failure,
Respiratory Emergencies Objectives Describe how to assess airway and breathing, including interpreting information from the PAT and ABCDEs. Differentiate between respiratory distress, respiratory failure,
Participant Objectives. Airway Anatomy. Airway Anatomy. Airway Anatomy: Pediatric Considerations. Airway Anatomy: Pediatric Considerations
 Common Pediatric Respiratory Emergencies NAPNAP Chicago Session 314 Wednesday, March 21, 2018 Participant Objectives Discuss upper airway illness in the pediatric population Discuss lower airway illness
Common Pediatric Respiratory Emergencies NAPNAP Chicago Session 314 Wednesday, March 21, 2018 Participant Objectives Discuss upper airway illness in the pediatric population Discuss lower airway illness
Review of literature suggests that there are three basic theories that attempt to explain the development of laryngomalacia.
 TITLE: Current Concepts in Diagnosis and Management of Laryngomalacia SOURCE: Grand Rounds Presentation, UTMB, Dept. of Otolaryngology DATE: March 31, 2009 FACULTY PHYSICIANS: Shraddha Mukerji, MD and
TITLE: Current Concepts in Diagnosis and Management of Laryngomalacia SOURCE: Grand Rounds Presentation, UTMB, Dept. of Otolaryngology DATE: March 31, 2009 FACULTY PHYSICIANS: Shraddha Mukerji, MD and
Unconscious exchange of air between lungs and the external environment Breathing
 Respiration Unconscious exchange of air between lungs and the external environment Breathing Two types External Exchange of carbon dioxide and oxygen between the environment and the organism Internal Exchange
Respiration Unconscious exchange of air between lungs and the external environment Breathing Two types External Exchange of carbon dioxide and oxygen between the environment and the organism Internal Exchange
RESPIRATORY FAILURE. Michael Kelly, MD Division of Pediatric Critical Care Dept. of Pediatrics
 RESPIRATORY FAILURE Michael Kelly, MD Division of Pediatric Critical Care Dept. of Pediatrics What talk is he giving? DO2= CO * CaO2 CO = HR * SV CaO2 = (Hgb* SaO2 * 1.34) + (PaO2 * 0.003) Sound familiar??
RESPIRATORY FAILURE Michael Kelly, MD Division of Pediatric Critical Care Dept. of Pediatrics What talk is he giving? DO2= CO * CaO2 CO = HR * SV CaO2 = (Hgb* SaO2 * 1.34) + (PaO2 * 0.003) Sound familiar??
Aetiology. Poor tube management. Small cricoid (acquired on congenital) Reflux Poor general status. Size of tube (leak) Duration of intubation
 Reflux Poor general status. Size of tube (leak) Duration of intubation") Aetiology Poor tube management Size of tube (leak) Duration of intubation Small cricoid (acquired on congenital) Reflux Poor general status Prevention Laryngeal Rest Medical Tubes Cricoid split Developing
Aetiology Poor tube management Size of tube (leak) Duration of intubation Small cricoid (acquired on congenital) Reflux Poor general status Prevention Laryngeal Rest Medical Tubes Cricoid split Developing
Management of Pediatric Tracheostomy
 Management of Pediatric Tracheostomy Deepak Mehta Associate Professor Of Otolaryngology Director Pediatric Aerodigestive Center Definitions Tracheotomy: The making of an incision in the trachea The name
Management of Pediatric Tracheostomy Deepak Mehta Associate Professor Of Otolaryngology Director Pediatric Aerodigestive Center Definitions Tracheotomy: The making of an incision in the trachea The name
Pediatric Airway and Respiratory Emergencies. Objectives 30/01/2009
 Objectives Pediatric Airway and Respiratory Emergencies Patrick Mahar, MD Review the anatomical differences between adult and pediatric airways Recognize different causes of respiratory comprise in pediatric
Objectives Pediatric Airway and Respiratory Emergencies Patrick Mahar, MD Review the anatomical differences between adult and pediatric airways Recognize different causes of respiratory comprise in pediatric
Simulation 01: Two Year-Old Child in Respiratory Distress (Croup)
") Simulation 01: Two Year-Old Child in Respiratory Distress (Croup) Flow Chart Opening Scenario 2 year-old child in respiratory distress - assess Section 1 Type: IG audible stridor with insp + exp wheezing;
Simulation 01: Two Year-Old Child in Respiratory Distress (Croup) Flow Chart Opening Scenario 2 year-old child in respiratory distress - assess Section 1 Type: IG audible stridor with insp + exp wheezing;
Congenital Laryngeal Anomalies
 Congenital Laryngeal Anomalies Prof. Hesham Abd Al-Fattah Alexandria - Egypt Embryology Resp primordium 3 rd wk Resp primordium separated by tracheoesophageal folds Fuse to form septum (4-5 wks) Larynx
Congenital Laryngeal Anomalies Prof. Hesham Abd Al-Fattah Alexandria - Egypt Embryology Resp primordium 3 rd wk Resp primordium separated by tracheoesophageal folds Fuse to form septum (4-5 wks) Larynx
Congenital Laryngeal Anomalies November 2005
 TITLE: Congenital Laryngeal Anomalies SOURCE: Grand Rounds Presentation, UTMB, Dept. of Otolaryngology DATE: November 2, 2005 RESIDENT PHYSICIAN: Jean P. Font M.D. FACULTY: ADVISOR: Seckin Ulualp, M.D.
TITLE: Congenital Laryngeal Anomalies SOURCE: Grand Rounds Presentation, UTMB, Dept. of Otolaryngology DATE: November 2, 2005 RESIDENT PHYSICIAN: Jean P. Font M.D. FACULTY: ADVISOR: Seckin Ulualp, M.D.
RESPIRATORY EMERGENCIES. Michael Waters MD April 2004
 RESPIRATORY EMERGENCIES Michael Waters MD April 2004 ASTHMA Asthma is a chronic inflammatory disease of the airways with variable or reversible airway obstruction Characterized by increased sensitivity
RESPIRATORY EMERGENCIES Michael Waters MD April 2004 ASTHMA Asthma is a chronic inflammatory disease of the airways with variable or reversible airway obstruction Characterized by increased sensitivity
THE DIFFICULT PEDIATRIC AIRWAY. Learning Objectives. The Pediatric Airway 6/7/18. Jason W. Gatling, MD Department of Anesthesiology June 7, 2018
 THE DIFFICULT PEDIATRIC AIRWAY Jason W. Gatling, MD Department of Anesthesiology June 7, 2018 Learning Objectives At the conclusion of this activity, the participants should be able to: 1. Describe what
THE DIFFICULT PEDIATRIC AIRWAY Jason W. Gatling, MD Department of Anesthesiology June 7, 2018 Learning Objectives At the conclusion of this activity, the participants should be able to: 1. Describe what
Eosinophilic Esophagitis: Extraesophageal Manifestations
 Eosinophilic Esophagitis: Extraesophageal Manifestations Karen B. Zur, MD Director, Pediatric Voice Program Associate Director, Center for Pediatric Airway Disorders The Children s Hospital of Philadelphia
Eosinophilic Esophagitis: Extraesophageal Manifestations Karen B. Zur, MD Director, Pediatric Voice Program Associate Director, Center for Pediatric Airway Disorders The Children s Hospital of Philadelphia
Upper Airway Emergencies
 Upper Airway Emergencies Selena Hariharan, M.D. Assistant Professor of Pediatrics Division of Pediatric Emergency Medicine Cincinnati Children s Hospital Medical Center CASE # 1 A 9 year old boy, previously
Upper Airway Emergencies Selena Hariharan, M.D. Assistant Professor of Pediatrics Division of Pediatric Emergency Medicine Cincinnati Children s Hospital Medical Center CASE # 1 A 9 year old boy, previously
Simulation 1: Two Year-Old Child in Respiratory Distress
 Simulation 1: Two Year-Old Child in Respiratory Distress Opening Scenario (Links to Section 1) You are the respiratory therapist in a 300 bed community hospital working the evening shift. At 8:30 PM you
Simulation 1: Two Year-Old Child in Respiratory Distress Opening Scenario (Links to Section 1) You are the respiratory therapist in a 300 bed community hospital working the evening shift. At 8:30 PM you
PEDIATRIC EMERGENCIES Sandra Horning, MD Sacred Heart Medical Center Emergency Department
 PEDIATRIC EMERGENCIES Sandra Horning, MD Sacred Heart Medical Center Emergency Department Overview Roles of the EMS in Pediatric Care Growth and Development Assessment Airway Adjuncts and Intravenous Access
PEDIATRIC EMERGENCIES Sandra Horning, MD Sacred Heart Medical Center Emergency Department Overview Roles of the EMS in Pediatric Care Growth and Development Assessment Airway Adjuncts and Intravenous Access
PEDIATRIC RESPIRATORY ILLNESS MADE SIMPLE
 Copyright 2012 Joel Berezow, MD and The Pediatrics for Emergency Physicians Network All rights reserved. Duplication in whole or in part, or electronic transmission in any form, is prohibited THE PEDIATRICS
Copyright 2012 Joel Berezow, MD and The Pediatrics for Emergency Physicians Network All rights reserved. Duplication in whole or in part, or electronic transmission in any form, is prohibited THE PEDIATRICS
Role of flexible bronchoscopy in diagnosis and treatment in children
 Role of flexible bronchoscopy in diagnosis and treatment in children Ernst Eber, MD Respiratory and Allergic Disease Division, Paediatric Department, Medical University of Graz, Austria Bronchoscopy 1897
Role of flexible bronchoscopy in diagnosis and treatment in children Ernst Eber, MD Respiratory and Allergic Disease Division, Paediatric Department, Medical University of Graz, Austria Bronchoscopy 1897
5/26/10. Upper Airway Emergencies Identify life threatening upper airway infections Recognize and treat anaphylaxis and airway burns in children
 Andi Marmor, MD Assistant Clinical Professor, Pediatrics University of California, San Francisco Upper Airway Emergencies Identify life threatening upper airway infections Recognize and treat anaphylaxis
Andi Marmor, MD Assistant Clinical Professor, Pediatrics University of California, San Francisco Upper Airway Emergencies Identify life threatening upper airway infections Recognize and treat anaphylaxis
Infectious Upper Airway Obstruction
 Infectious Upper Airway Obstruction Prof. Muhi K. Al-Janabi MRCPCH; DCH; FICMS Consultant Pediatric Pulmonologist Objectives Viral croup Objectives 1. Know and understand the aetiology and natural history
Infectious Upper Airway Obstruction Prof. Muhi K. Al-Janabi MRCPCH; DCH; FICMS Consultant Pediatric Pulmonologist Objectives Viral croup Objectives 1. Know and understand the aetiology and natural history
Chapter 124: Congenital Disorders of the Trachea. Bruce Benjamin
 Chapter 124: Congenital Disorders of the Trachea Bruce Benjamin Investigation of the larynx and pharynx may be incomplete in infants and children with congenital abnormalities without investigation of
Chapter 124: Congenital Disorders of the Trachea Bruce Benjamin Investigation of the larynx and pharynx may be incomplete in infants and children with congenital abnormalities without investigation of
ORIGINAL ARTICLE. Synchronous Airway Lesions and Outcomes in Infants With Severe Laryngomalacia Requiring Supraglottoplasty
 ORIGINAL ARTICLE Synchronous Airway Lesions and Outcomes in Infants With Severe Laryngomalacia Requiring Supraglottoplasty James W. Schroeder Jr, MD; Naveen D. Bhandarkar, MD; Lauren D. Holinger, MD Objective:
ORIGINAL ARTICLE Synchronous Airway Lesions and Outcomes in Infants With Severe Laryngomalacia Requiring Supraglottoplasty James W. Schroeder Jr, MD; Naveen D. Bhandarkar, MD; Lauren D. Holinger, MD Objective:
DIFFICULT ASTHMA. Dr. Prathyusha Dr. S.Balasubramanian KKCTH
 DIFFICULT ASTHMA Dr. Prathyusha Dr. S.Balasubramanian KKCTH CASE SUMMARY 11 yr old girl, Neyveli Treated as moderate persistent asthma x 5 years On Seroflo [ LABA + steroid ] 250 2 puffs BD and intermittent
DIFFICULT ASTHMA Dr. Prathyusha Dr. S.Balasubramanian KKCTH CASE SUMMARY 11 yr old girl, Neyveli Treated as moderate persistent asthma x 5 years On Seroflo [ LABA + steroid ] 250 2 puffs BD and intermittent
PedsCases Podcast Scripts
 PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Evaluation of Stridor. These podcasts are designed to give medical students an overview of key topics in pediatrics.
PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Evaluation of Stridor. These podcasts are designed to give medical students an overview of key topics in pediatrics.
Case Report Long-Term Outcomes of Balloon Dilation for Acquired Subglottic Stenosis in Children
 Case Reports in Otolaryngology, Article ID 304593, 4 pages http://dx.doi.org/10.1155/2014/304593 Case Report Long-Term Outcomes of Balloon Dilation for Acquired Subglottic Stenosis in Children Aliye Filiz
Case Reports in Otolaryngology, Article ID 304593, 4 pages http://dx.doi.org/10.1155/2014/304593 Case Report Long-Term Outcomes of Balloon Dilation for Acquired Subglottic Stenosis in Children Aliye Filiz
Day 2 Pulmonary Breakout Interventional Pulmonology
 Day 2 Pulmonary Breakout Interventional Pulmonology R. Paul Boesch, DO, MS Assistant Professor, Pulmonary Medicine Mayo Clinic Children s Center Interventional Pediatric Pulmonology or Pulm/ENT airway
Day 2 Pulmonary Breakout Interventional Pulmonology R. Paul Boesch, DO, MS Assistant Professor, Pulmonary Medicine Mayo Clinic Children s Center Interventional Pediatric Pulmonology or Pulm/ENT airway
A study on paediatric stridor causes and management: case series
 International Journal of Otorhinolaryngology and Head and Neck Surgery Selvam DK et al. Int J Otorhinolaryngol Head Neck Surg. 2017 Oct;3(4):1031-1035 http://www.ijorl.com pissn 2454-5929 eissn 2454-5937
International Journal of Otorhinolaryngology and Head and Neck Surgery Selvam DK et al. Int J Otorhinolaryngol Head Neck Surg. 2017 Oct;3(4):1031-1035 http://www.ijorl.com pissn 2454-5929 eissn 2454-5937
Pediatric Airway Emergencies
 Pediatric Airway Emergencies The University of Texas Medical Branch Department of Otolaryngology, Grand Rounds Presentation November 23, 2005 Steven T. Wright, M.D. Faculty Advisor: Seckin Ulualp, M.D.
Pediatric Airway Emergencies The University of Texas Medical Branch Department of Otolaryngology, Grand Rounds Presentation November 23, 2005 Steven T. Wright, M.D. Faculty Advisor: Seckin Ulualp, M.D.
Sohit Paul Kanotra M.D. Director, Pediatric Aerodigestive Center
 Sohit Paul Kanotra M.D. Director, Pediatric Aerodigestive Center Children s Hospital of New Orleans Assistant Professor, Otolaryngology-Head & Neck Surgery, Louisiana State University. I do not have any
Sohit Paul Kanotra M.D. Director, Pediatric Aerodigestive Center Children s Hospital of New Orleans Assistant Professor, Otolaryngology-Head & Neck Surgery, Louisiana State University. I do not have any
Dr. (Kate) Katherine Miller GUELPH ON 121 RESPIRATORY DISTRESS IN THE NEWBORN
 Katherine Miller GUELPH ON 121 RESPIRATORY DISTRESS IN THE NEWBORN") Society of Rural Physicians of Canada 26TH ANNUAL RURAL AND REMOTE MEDICINE COURSE ST. JOHN'S NEWFOUNDLAND AND LABRADOR APRIL 12-14, 2018 Dr. (Kate) Katherine Miller GUELPH ON 121 RESPIRATORY DISTRESS
Society of Rural Physicians of Canada 26TH ANNUAL RURAL AND REMOTE MEDICINE COURSE ST. JOHN'S NEWFOUNDLAND AND LABRADOR APRIL 12-14, 2018 Dr. (Kate) Katherine Miller GUELPH ON 121 RESPIRATORY DISTRESS
Review Article Laryngomalacia: Disease Presentation, Spectrum, and Management
 International Pediatrics Volume 2012, Article ID 753526, 6 pages doi:10.1155/2012/753526 Review Article Laryngomalacia: Disease Presentation, Spectrum, and Management April M. Landry 1 and Dana M. Thompson
International Pediatrics Volume 2012, Article ID 753526, 6 pages doi:10.1155/2012/753526 Review Article Laryngomalacia: Disease Presentation, Spectrum, and Management April M. Landry 1 and Dana M. Thompson
Croup (Laryngo-tracheo-bronchitis)
") Croup (Laryngo-tracheo-bronchitis) 1a 2a 2b Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Contact Name and Job Title (author) Directorate & Speciality Date of
Croup (Laryngo-tracheo-bronchitis) 1a 2a 2b Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Contact Name and Job Title (author) Directorate & Speciality Date of
Respiratory Management in Pediatrics
 Respiratory Management in Pediatrics Children s Hospital Omaha Critical Care Transport Sue Holmer RN, C-NPT Objectives Examine the differences between the pediatric and adults airways. Recognize respiratory
Respiratory Management in Pediatrics Children s Hospital Omaha Critical Care Transport Sue Holmer RN, C-NPT Objectives Examine the differences between the pediatric and adults airways. Recognize respiratory
Common Pediatric Respiratory Illness and Emergencies
 Common Pediatric Respiratory Illness and Emergencies Rob Cloutier, MD Assistant Professor Emergency Medicine & Pediatrics Oregon Health & Science University Overview Review key differences between pediatric
Common Pediatric Respiratory Illness and Emergencies Rob Cloutier, MD Assistant Professor Emergency Medicine & Pediatrics Oregon Health & Science University Overview Review key differences between pediatric
Contents. Part A Clinical Evaluation of Laryngeal Disorders. 3 Videostroboscopy and Dynamic Voice Evaluation with Flexible Laryngoscopy...
 Contents Part A Clinical Evaluation of Laryngeal Disorders 1 Anatomy and Physiology of the Larynx....... 3 1.1 Anatomy.................................. 3 1.1.1 Laryngeal Cartilages........................
Contents Part A Clinical Evaluation of Laryngeal Disorders 1 Anatomy and Physiology of the Larynx....... 3 1.1 Anatomy.................................. 3 1.1.1 Laryngeal Cartilages........................
Respiratory system. Applied Anatomy &Physiology
 Respiratory system Applied Anatomy &Physiology Anatomy The respiratory system consists of 1)The Upper airway : Nose, mouth and larynx 2)The Lower airways Trachea and the two lungs. Within the lungs,
Respiratory system Applied Anatomy &Physiology Anatomy The respiratory system consists of 1)The Upper airway : Nose, mouth and larynx 2)The Lower airways Trachea and the two lungs. Within the lungs,
CHAPTER 7.1 STRUCTURES OF THE RESPIRATORY SYSTEM
 CHAPTER 7.1 STRUCTURES OF THE RESPIRATORY SYSTEM Pages 244-247 DO NOW What structures, do you think, are active participating in the breathing process? 2 WHAT ARE WE DOING IN TODAY S CLASS Finishing Digestion
CHAPTER 7.1 STRUCTURES OF THE RESPIRATORY SYSTEM Pages 244-247 DO NOW What structures, do you think, are active participating in the breathing process? 2 WHAT ARE WE DOING IN TODAY S CLASS Finishing Digestion
Chapter 19 - Respiratory_Emergencies
 Introduction to Emergency Medical Care 1 OBJECTIVES 19.1 Define key terms introduced in this chapter. Slides 14 15, 41, 54 19.2 Describe the anatomy and physiology of respiration. Slides 13 15 19.3 Differentiate
Introduction to Emergency Medical Care 1 OBJECTIVES 19.1 Define key terms introduced in this chapter. Slides 14 15, 41, 54 19.2 Describe the anatomy and physiology of respiration. Slides 13 15 19.3 Differentiate
Why Can t I breathe? Asthma vs. Vocal Cord Dysfunction (VCD) Lindsey Frohn, M.S., CCC-SLP Madonna Rehabilitation Hospital (Lincoln, NE)
 Lindsey Frohn, M.S., CCC-SLP Madonna Rehabilitation Hospital (Lincoln, NE)") Why Can t I breathe? Asthma vs. Vocal Cord Dysfunction (VCD) Lindsey Frohn, M.S., CCC-SLP Madonna Rehabilitation Hospital (Lincoln, NE) Objectives Examine Vocal Cord Dysfunction Examine Exercise Induced
Why Can t I breathe? Asthma vs. Vocal Cord Dysfunction (VCD) Lindsey Frohn, M.S., CCC-SLP Madonna Rehabilitation Hospital (Lincoln, NE) Objectives Examine Vocal Cord Dysfunction Examine Exercise Induced
Author(s): Matt Dawson & Zach Sturges (University of Utah) 2008
: Matt Dawson & Zach Sturges (University of Utah) 2008") Project: Ghana Emergency Medicine Collaborative Document Title: ENT Case Files (2008) Author(s): Matt Dawson & Zach Sturges (University of Utah) 2008 License: Unless otherwise noted, this material is made
Project: Ghana Emergency Medicine Collaborative Document Title: ENT Case Files (2008) Author(s): Matt Dawson & Zach Sturges (University of Utah) 2008 License: Unless otherwise noted, this material is made
Laryngoscopy Examinations
 Laryngoscopy Examinations Laryngoscopy is a visual examination of the back of the throat where the voice box (larynx) and vocal cords are located. The procedure is done by using hand mirrors and a light
Laryngoscopy Examinations Laryngoscopy is a visual examination of the back of the throat where the voice box (larynx) and vocal cords are located. The procedure is done by using hand mirrors and a light
Hoarseness. Common referral Hoarseness reflects any abnormality of normal phonation
 Hoarseness Kevin Katzenmeyer, MD Faculty Advisor: Byron J Bailey, MD The University of Texas Medical Branch Department of Otolaryngology Grand Rounds Presentation October 24, 2001 Hoarseness Common referral
Hoarseness Kevin Katzenmeyer, MD Faculty Advisor: Byron J Bailey, MD The University of Texas Medical Branch Department of Otolaryngology Grand Rounds Presentation October 24, 2001 Hoarseness Common referral
BJ Coopes, MD Medical Director, Pediatric Critical Care, Inpatient Pediatrics
 BJ Coopes, MD Medical Director, Pediatric Critical Care, Inpatient Pediatrics The BIG Question: Sick or Not Sick? Signs of Respiratory Distress Tachypnea Tachycardia Retractions Accessory muscles Head
BJ Coopes, MD Medical Director, Pediatric Critical Care, Inpatient Pediatrics The BIG Question: Sick or Not Sick? Signs of Respiratory Distress Tachypnea Tachycardia Retractions Accessory muscles Head
Department of Pediatric Otolarygnology. ENT Specialty Programs
 Department of Pediatric Otolarygnology ENT Specialty Programs Staffed by fellowship-trained otolaryngologists, assisted by pediatric nurse practitioners, ENT (Otolaryngology) at Nationwide Children s Hospital
Department of Pediatric Otolarygnology ENT Specialty Programs Staffed by fellowship-trained otolaryngologists, assisted by pediatric nurse practitioners, ENT (Otolaryngology) at Nationwide Children s Hospital
An Overview of Bronchopulmonary Dysplasia and Chronic Lung Disease in Infancy
 An Overview of Bronchopulmonary Dysplasia and Chronic Lung Disease in Infancy Housekeeping: I have no financial disclosures Learning objectives: Develop an understanding of bronchopulmonary dysplasia (BPD)
An Overview of Bronchopulmonary Dysplasia and Chronic Lung Disease in Infancy Housekeeping: I have no financial disclosures Learning objectives: Develop an understanding of bronchopulmonary dysplasia (BPD)
The Pediatric Patient. Morgen Bernius, MD NCEMS Conference February 24, 2007
 The Pediatric Patient Morgen Bernius, MD NCEMS Conference February 24, 2007 Rule #1: Everyone Loves the Pediatric Patient Pediatrics in EMS Approximately 10% of all EMS treatment is for children younger
The Pediatric Patient Morgen Bernius, MD NCEMS Conference February 24, 2007 Rule #1: Everyone Loves the Pediatric Patient Pediatrics in EMS Approximately 10% of all EMS treatment is for children younger
BRONCHIOLITIS PEDIATRIC
 DEFINITION Bronchiolitis is typically defined as the first episode of wheezing in infants < 24 months of age. It is a viral illness of the lower respiratory tract that causes tachypnea, bronchospasm, and
DEFINITION Bronchiolitis is typically defined as the first episode of wheezing in infants < 24 months of age. It is a viral illness of the lower respiratory tract that causes tachypnea, bronchospasm, and
Research Article Balloon Dilatation of Pediatric Subglottic Laryngeal Stenosis during the Artificial Apneic Pause: Experience in 5 Children
 BioMed Research International, Article ID 397295, 4 pages http://dx.doi.org/10.1155/2014/397295 Research Article Balloon Dilatation of Pediatric Subglottic Laryngeal Stenosis during the Artificial Apneic
BioMed Research International, Article ID 397295, 4 pages http://dx.doi.org/10.1155/2014/397295 Research Article Balloon Dilatation of Pediatric Subglottic Laryngeal Stenosis during the Artificial Apneic
1/3/2008. Karen Burke Priscilla LeMone Elaine Mohn-Brown. Medical-Surgical Nursing Care, 2e Karen Burke, Priscilla LeMone, and Elaine Mohn-Brown
 Medical-Surgical Nursing Care Second Edition Karen Burke Priscilla LeMone Elaine Mohn-Brown Chapter 23 Caring for Clients with Upper Respiratory Disorders Rhinitis Inflammation of Nasal Cavities Types
Medical-Surgical Nursing Care Second Edition Karen Burke Priscilla LeMone Elaine Mohn-Brown Chapter 23 Caring for Clients with Upper Respiratory Disorders Rhinitis Inflammation of Nasal Cavities Types
CRACKCast E168 Pediatric Respiratory Emergencies: Upper Airway Obstruction and Infections
 CRACKCast E168 Pediatric Respiratory Emergencies: Upper Airway Obstruction and Infections Key concepts Respiratory arrest precedes most pediatric cardiac arrests. You better recognize any airway problem
CRACKCast E168 Pediatric Respiratory Emergencies: Upper Airway Obstruction and Infections Key concepts Respiratory arrest precedes most pediatric cardiac arrests. You better recognize any airway problem
A case of a neonate with a congenital laryngeal web: management of a difficult airway and intra-operative complications
 A case of a neonate with a congenital laryngeal web: management of a difficult airway and intra-operative complications Moderators: Marcellene Franzen, MD Fellow in Pediatric Anesthesiology Medical College
A case of a neonate with a congenital laryngeal web: management of a difficult airway and intra-operative complications Moderators: Marcellene Franzen, MD Fellow in Pediatric Anesthesiology Medical College
trust clinical guideline
 CG26 VERSION 1.0 1/8 Guideline ID CG26 Version 1.0 Title Approved by Management of Croup Clinical Effectiveness Group Date Issued 01/10/2014 Review Date 31/09/2017 Directorate Authorised Staff Medical
CG26 VERSION 1.0 1/8 Guideline ID CG26 Version 1.0 Title Approved by Management of Croup Clinical Effectiveness Group Date Issued 01/10/2014 Review Date 31/09/2017 Directorate Authorised Staff Medical
Disclosures. Repaired Esophageal Atresia and Tracheoesophageal Fistula and Chronic Dysphagia. Case Presentation. Case Presentation.
 Disclosures Repaired Esophageal Atresia and Tracheoesophageal Fistula and Chronic Dysphagia Dr. DeBoer is funded by Colorado Clinical and Translational Science Institute KL2 TR001080 Emily DeBoer MD Assistant
Disclosures Repaired Esophageal Atresia and Tracheoesophageal Fistula and Chronic Dysphagia Dr. DeBoer is funded by Colorado Clinical and Translational Science Institute KL2 TR001080 Emily DeBoer MD Assistant
Physical Exam. Vitals stable on room air Abdomen soft, non-distented Normal external genitalia Patent anus No limb anomalies
 Case Presentation 1 day-old full-term baby girl noted to have drooling of saliva and increased secretions at birth Fetal US @32wks had shown polyhydramnios Birth weight 3515g Apgar 7@1min and 8@5min Unable
Case Presentation 1 day-old full-term baby girl noted to have drooling of saliva and increased secretions at birth Fetal US @32wks had shown polyhydramnios Birth weight 3515g Apgar 7@1min and 8@5min Unable
3/10/15. Summary. Anatomy Larynx. Anatomy Trachea
 Summary Anatomy Brachycephalic Airway Syndrome (BCAS) Crisis Anatomy Larynx Anatomy Trachea Tracheal rings are incomplete, C-shaped cartilage with the dorsal membrane being completed by tracheal muscle
Summary Anatomy Brachycephalic Airway Syndrome (BCAS) Crisis Anatomy Larynx Anatomy Trachea Tracheal rings are incomplete, C-shaped cartilage with the dorsal membrane being completed by tracheal muscle
Management of Respiratory Issues in the School Setting. Pediatric Indicators of High Risk 8/7/2015. Facts about Pediatric Respiratory Failure
 Management of Respiratory Issues in the School Setting Toni B. Vento, MS, RN, NCSN Supervisor of Health Services Medford Public Schools Pediatric Indicators of High Risk Anatomic features of the immature
Management of Respiratory Issues in the School Setting Toni B. Vento, MS, RN, NCSN Supervisor of Health Services Medford Public Schools Pediatric Indicators of High Risk Anatomic features of the immature
Congenital Laryngeal Anomalies November 2002
 TITLE: Congenital Laryngeal Anomalies SOURCE: Grand Rounds Presentation, UTMB, Dept. of Otolaryngology DATE: November 20, 2002 RESIDENT PHYSICIAN: Russell D. Briggs, M.D. FACULTY ADVISOR: Ronald W. Deskin,
TITLE: Congenital Laryngeal Anomalies SOURCE: Grand Rounds Presentation, UTMB, Dept. of Otolaryngology DATE: November 20, 2002 RESIDENT PHYSICIAN: Russell D. Briggs, M.D. FACULTY ADVISOR: Ronald W. Deskin,
ORIGINAL ARTICLE. Office-Based Lower Airway Endoscopy in Pediatric Patients. airway symptoms is an integral part of the otolaryngology practice.
 ORIGINAL ARTICLE Office-Based Lower Airway Endoscopy in Pediatric Patients D. Richard Lindstrom III, MD; David T. Book, MD; Stephen F. Conley, MD; Valerie A. Flanary, MD; Joseph E. Kerschner, MD Background:
ORIGINAL ARTICLE Office-Based Lower Airway Endoscopy in Pediatric Patients D. Richard Lindstrom III, MD; David T. Book, MD; Stephen F. Conley, MD; Valerie A. Flanary, MD; Joseph E. Kerschner, MD Background:
Pediatric Shock. Hypovolemia. Sepsis. Most common cause of pediatric shock Small blood volumes (80cc/kg)
") Critical Concepts: Shock Inadequate peripheral perfusion where oxygen delivery does not meet metabolic demand Adult vs Pediatric Shock - Same causes/different frequencies Pediatric Shock Hypovolemia Most
Critical Concepts: Shock Inadequate peripheral perfusion where oxygen delivery does not meet metabolic demand Adult vs Pediatric Shock - Same causes/different frequencies Pediatric Shock Hypovolemia Most
Respiratory Compromise and Swallowing
 Speech Pathology and Respiratory Care April 11, 2013 By Angela Parcaro-Tucker, MA, CCC-SLP, LSVT How can Speech Therapy help? 1 Respiratory Compromise and Swallowing Swallowing is a complex sequence of
Speech Pathology and Respiratory Care April 11, 2013 By Angela Parcaro-Tucker, MA, CCC-SLP, LSVT How can Speech Therapy help? 1 Respiratory Compromise and Swallowing Swallowing is a complex sequence of
FOREIGN BODY ASPIRATION in children. Dr. Xayyavong Bouathongthip, M.D Emergency department, children s hospital
 FOREIGN BODY ASPIRATION in children Dr. Xayyavong Bouathongthip, M.D Emergency department, children s hospital How common is choking? About 3,000 people die/year from choking Figure remained unchanged
FOREIGN BODY ASPIRATION in children Dr. Xayyavong Bouathongthip, M.D Emergency department, children s hospital How common is choking? About 3,000 people die/year from choking Figure remained unchanged
Surgical Diseases of the Upper Airways. Michael Huber DVM, MS Diplomate American College of Veterinary Surgeons
 Surgical Diseases of the Upper Airways Michael Huber DVM, MS Diplomate American College of Veterinary Surgeons Surgical Diseases of the Upper Airways General Considerations Brachycephalic Syndrome Laryngeal
Surgical Diseases of the Upper Airways Michael Huber DVM, MS Diplomate American College of Veterinary Surgeons Surgical Diseases of the Upper Airways General Considerations Brachycephalic Syndrome Laryngeal
Tracheostomy and Ventilator Education Program Module 2: Respiratory Anatomy
 Tracheostomy and Ventilator Education Program Module 2: Respiratory Anatomy Disclaimer This material is intended for use by trained family members and caregivers of children with tracheostomies who are
Tracheostomy and Ventilator Education Program Module 2: Respiratory Anatomy Disclaimer This material is intended for use by trained family members and caregivers of children with tracheostomies who are
Steroid Therapy for Tracheal Stenosis in Children
 Steroid Therapy for Tracheal Stenosis in Children Clinical Experience in 4 Children with Severe Strictures H. Biemann Othersen, Jr., M.D. ABSTRACT Recently a refinement in the treatment of tracheal stenosis
Steroid Therapy for Tracheal Stenosis in Children Clinical Experience in 4 Children with Severe Strictures H. Biemann Othersen, Jr., M.D. ABSTRACT Recently a refinement in the treatment of tracheal stenosis
Laryngomalacia, laryngeal cleft and congenital unilateral vocal cord palsy: A unique case treated endoscopically without intubation or tracheostomy
 Case Report Brunei Int Med J. 2014; 10 (1): 55-59 Laryngomalacia, laryngeal cleft and congenital unilateral vocal cord palsy: A unique case treated endoscopically without intubation or tracheostomy Zara
Case Report Brunei Int Med J. 2014; 10 (1): 55-59 Laryngomalacia, laryngeal cleft and congenital unilateral vocal cord palsy: A unique case treated endoscopically without intubation or tracheostomy Zara
Conflict of Interest: none. Neonatal Airway Masses. Neonatal Respiratory Papillomatosis. Paul J. Samuels, MD
 Paul J. Samuels, MD Professor of Anesthesiology and Pediatrics Director of Education Cincinnati Children s Hospital Cincinnati, Ohio Conflict of Interest: none Neonatal Respiratory Papillomatosis Caused
Paul J. Samuels, MD Professor of Anesthesiology and Pediatrics Director of Education Cincinnati Children s Hospital Cincinnati, Ohio Conflict of Interest: none Neonatal Respiratory Papillomatosis Caused
Subspecialty Rotation: Otolaryngology
 Subspecialty Rotation: Otolaryngology Faculty: Evelyn Kluka, M.D. GOAL: Hearing Loss. Understand the morbidity of hearing loss, intervention strategies, and the pediatrician's and other specialists' roles
Subspecialty Rotation: Otolaryngology Faculty: Evelyn Kluka, M.D. GOAL: Hearing Loss. Understand the morbidity of hearing loss, intervention strategies, and the pediatrician's and other specialists' roles
Respiratory Diseases and Disorders
 Chapter 9 Respiratory Diseases and Disorders Anatomy and Physiology Chest, lungs, and conducting airways Two parts: Upper respiratory system consists of nose, mouth, sinuses, pharynx, and larynx Lower
Chapter 9 Respiratory Diseases and Disorders Anatomy and Physiology Chest, lungs, and conducting airways Two parts: Upper respiratory system consists of nose, mouth, sinuses, pharynx, and larynx Lower
PAEDIATRIC ACUTE CARE GUIDELINE. Croup. This document should be read in conjunction with this DISCLAIMER
 Princess Margaret Hospital for Children PAEDIATRIC ACUTE CARE GUIDELINE Croup Scope (Staff): Scope (Area): All Emergency Department Clinicians Emergency Department This document should be read in conjunction
Princess Margaret Hospital for Children PAEDIATRIC ACUTE CARE GUIDELINE Croup Scope (Staff): Scope (Area): All Emergency Department Clinicians Emergency Department This document should be read in conjunction
Acquired pediatric esophageal diseases Imaging approaches and findings. M. Mearadji International Foundation for Pediatric Imaging Aid
 Acquired pediatric esophageal diseases Imaging approaches and findings M. Mearadji International Foundation for Pediatric Imaging Aid Acquired pediatric esophageal diseases The clinical signs of acquired
Acquired pediatric esophageal diseases Imaging approaches and findings M. Mearadji International Foundation for Pediatric Imaging Aid Acquired pediatric esophageal diseases The clinical signs of acquired
Overview. The Respiratory System. Chapter 18. Respiratory Emergencies 9/11/2012
 Chapter 18 Respiratory Emergencies Slide 1 Overview Respiratory System Review Anatomy Physiology Breathing Assessment Adequate Breathing Breathing Difficulty Focused History and Physical Examination Emergency
Chapter 18 Respiratory Emergencies Slide 1 Overview Respiratory System Review Anatomy Physiology Breathing Assessment Adequate Breathing Breathing Difficulty Focused History and Physical Examination Emergency