|
|
|
- Lauren Quinn
- 5 years ago
- Views:
Transcription
1
2
3

4

5

6
7
8

9

10

11
12
13
14
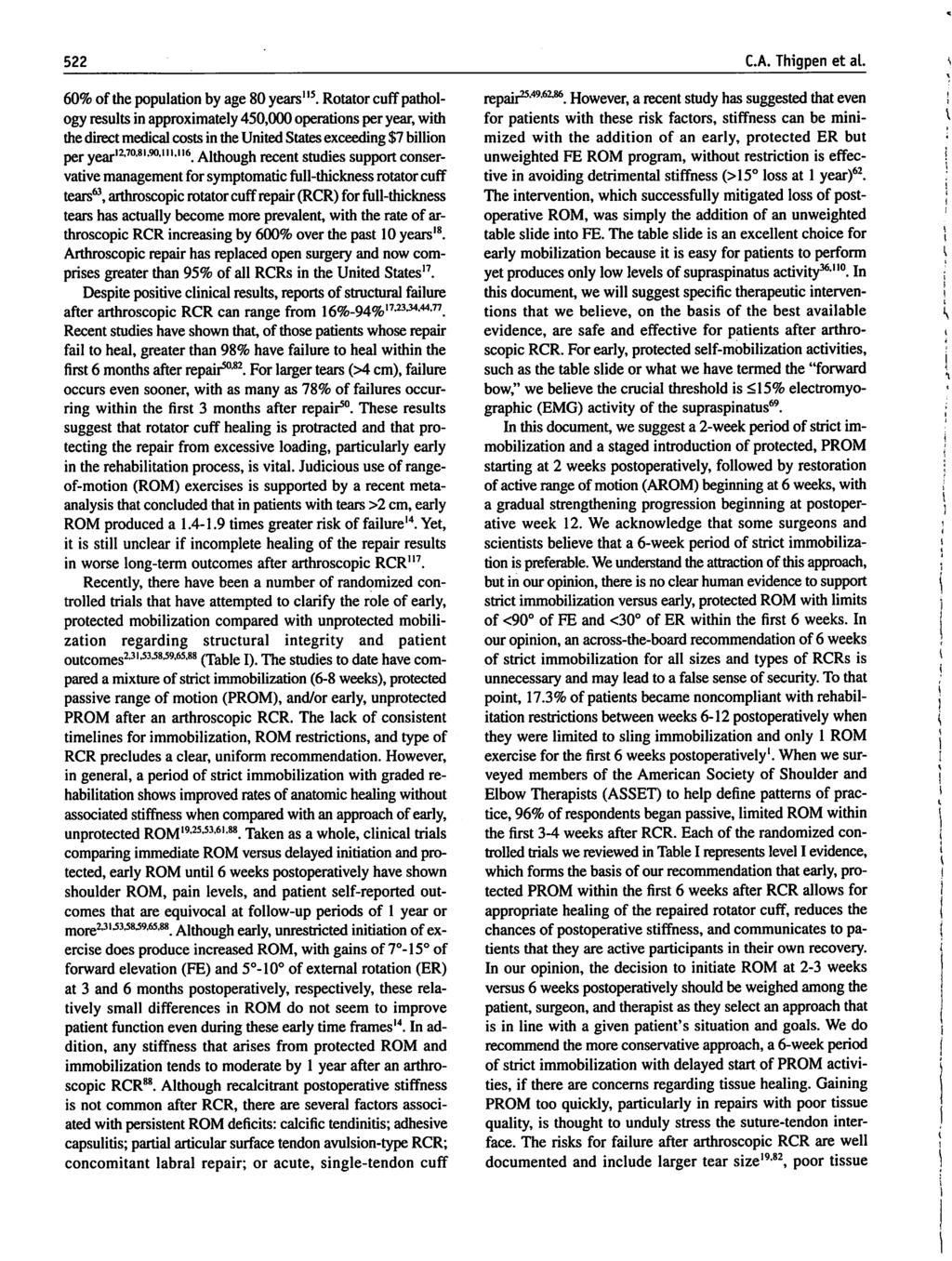
15 Appendix A: The American Society Of Shoulder And Elbow Therapists Arthroscopic Rotator Cuff Repair Rehabilitation Guide Phase 1 (POD 1 to ~ POW 6) GOALS: Maintain integrity of repair Minimize pain and inflammation Achieve staged range of motion (ROM) goals Educate the patient including postoperative precautions, modification of ADL s, and activity progression. Normalize scapula position and mobility INTERVENTIONS TO AVOID WITH INVOLVED SHOULDER: No active range of motion (AROM) of shoulder No lifting of objects No excessive stretching or sudden movements No supporting of body weight by hands No aggressive or provocative passive range of motion (PROM) exercises SPECIFIC INTERVENTIONS: Activities of primary importance: 1. Patient education (see patient education section below) 2. Protection of repair (see above interventions to avoid) 3. Achieve staged ROM goals utilizing ROM activities demonstrating an EMG activity level <15% 4. Minimize inflammation 5. Control pain with cryotherapy, prescribed medications, modalities Activities of secondary importance: 1. Normalize scapular position and mobility 2. ROM of the elbow, wrist, hand and cervical spine Immobilization: (Timeframe adjusted based on size of tear, tissue integrity, and surgeon preference) Sling immobilization is typically 4-6 weeks, followed by a gradual weaning from the sling in controlled environments for an additional 2 weeks with goal of being out of the sling by POW 6-8. Patient Education: Explain nature of the surgery Clarify interventions to avoid (listed above) Explain that lack of pain does not necessarily mean lack of stress on the repair Discuss precautions specific to the nature of the patient s surgical repair Emphasize importance of meeting but not greatly exceeding staged ROM goals Disclose importance of tissue healing 1
16 Exhibit proper sling use Limit use of upper extremity for activities of daily living (ADLs) Pain Management: Activity modification/restriction Proper use of sling Cryotherapy Gentle exercise intensity Modalities (TENS/ electrical stimulation) PRN Prescribed or over the counter medications per surgeon PROM / Flexibility: The start of shoulder PROM may be delayed up to 6 weeks post operatively based on surgeon preference, large or massive tear size, and/or poor tissue quality. POD 1-10 Patient education Pendulum (small circle or hangs) Elbow, wrist, and hand AROM, no weights o Only PROM of the elbow may be specified if concomitant biceps tenodesis/tenotomy performed. POW 1-3 Continue with above Passive forward elevation (PFE) in the plane of scapula using only exercises with < 15% EMG activity level o Forward bow o Therapist assisted PFE (seated / supine) o CPM in PFE o Patient self-assisted supine PFE using opposite hand Passive external rotation (PER) in approximately 20 abduction o All PER exercises studied have demonstrated <15% EMG activity level for the supraspinatus. o Note that the subscapularis has not been evaluated. POW 3-6 Progress PFE and PER within staged ROM goals using only activities with < 15% EMG activity level May begin joint mobilizations grade I & II for pain relief / relaxation as indicated for all shoulder girdle joints (GH, SC, AC, ST) May allow slow speed aquatic therapy for improving PROM, no swimming strokes May progress elbow, wrist, and finger AROM to light strengthening (delay to six weeks post op if with concomitant biceps tenodesis /tenotomy) MILESTONES (TESTING CRITERIA) TO PROGRESS TO PHASE II 2
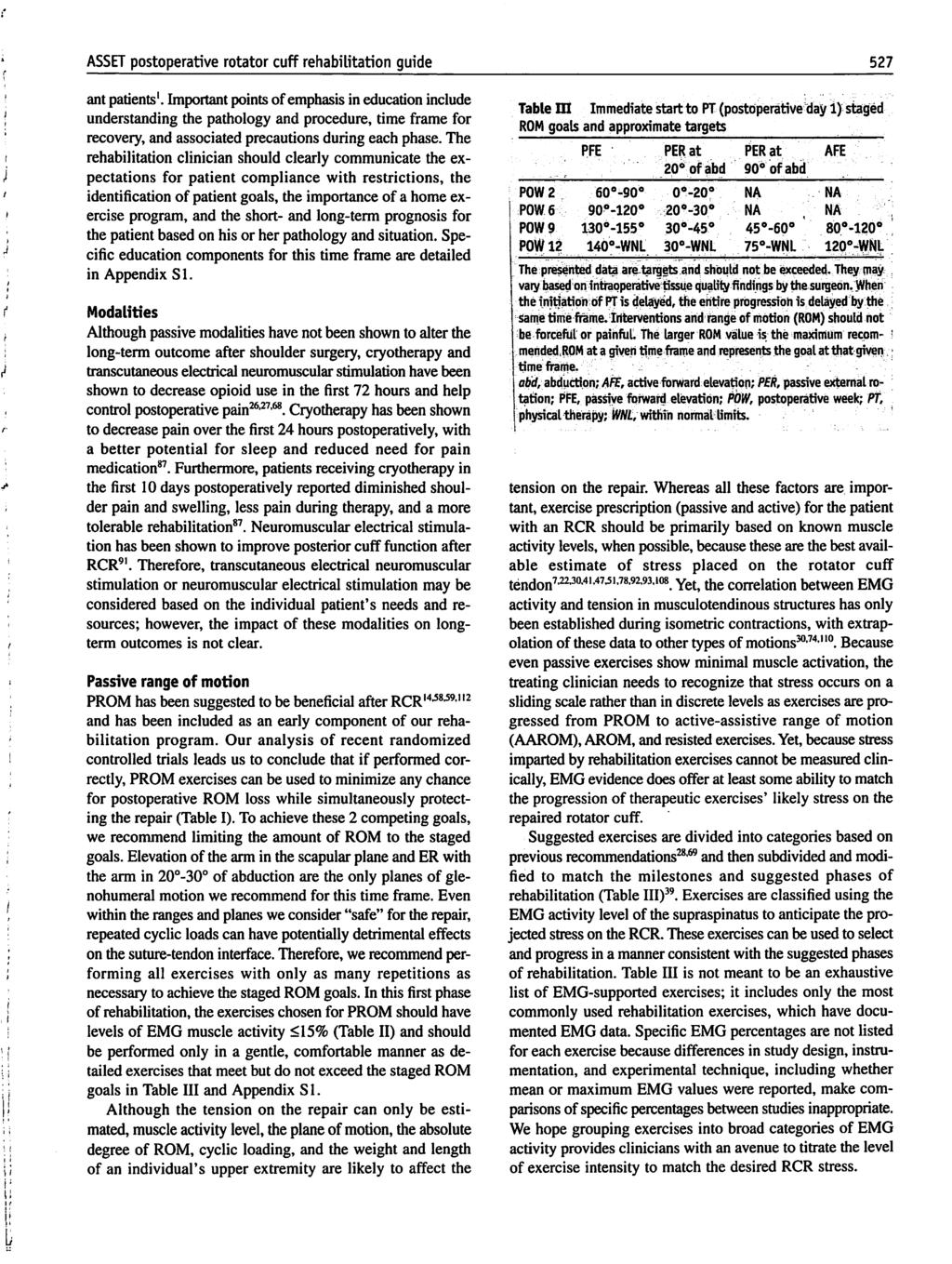
17 Appropriate healing of the surgical repair by adhering to the precautions, exercise, and immobilization guidelines. Staged ROM goals achieved, but not significantly exceeded Minimal to no pain (NPRS: 0 3/10) with ROM Phase 2 (~POW 6 to ~ POW 12) GOALS: Promote healing of soft tissue, extra care is needed to not overstress Achieve staged ROM goals Minimal pain and inflammation Initiate light muscle performance activities Perform light, non-repetitive ADL s at chest level and below INTERVENTIONS TO AVOID WITH INVOLVED SHOULDER: No active lifting or ADL s that require ROM beyond staged goals No supporting of body weight by hands No excessive behind the back movements No sudden jerking motions ROM / stretching significantly beyond staged goals Scaption with internal rotation (empty can) at any stage of rehabilitation due to impingement and stress on the cuff repair Exercises with EMG activity level > 30% (Table 2) which generally includes rotator cuff strengthening exercises with > 2 lbs resistance. SPECIFIC INTERVENTIONS: Activities of primary importance: 1. Continue patient education 2. Expand PROM/stretching 3. Achieve staged ROM goals 4. Initiate AAROM to AROM activities to establish basic rotator cuff and scapula neuromuscular control within allowed ROM Activities of secondary importance: 1. Introduction of light non-repetitive waist and chest level functional activities 2. Light resisted exercises within pain free ROM, emphasizing proper mechanics and avoiding fatigue related loss of form Immobilization: (timeframes adjusted based on size of tear, integrity of tissue and repair, and surgeon preference) Typically, gradual weaning from sling from POW 6-8 Patient Education: Continue education regarding avoiding heavy lifting or quick sudden movements. 3
18 Guide the patient through using the upper extremity for appropriate ADL s in pain free ROM; starting with waist level activities, progressing to shoulder level activities, in some cases limited overhead activities. Pain Management: Continue cryotherapy Ensure appropriate use of upper extremity during ADL s Ensure appropriate level of therapeutic exercises Wean from medications Electrical and thermal modalities as needed PROM / Flexibility: Progress PFE and PER ROM within staged goals Continue phase 1 exercises especially if PROM is behind staged ROM goals Progress to flexibility exercises that demonstrate an EMG activity level >15% such as the pulley if they can be performed comfortably with correct mechanics Begin PROM exercises in other planes if significant ROM limitations are present due to stiffness (be careful due to direct passive tension on the repair) ER at multiple angles of abduction (45, 75, 90 ) Horizontal adduction IR Functional behind the back IR If capsular restrictions are present, progress as indicated to grades III & IV joint mobilizations for all shoulder girdle joints (GH, SC, AC, ST) Address scapulothoracic and trunk mobility limitations. Ensure normal cervical spine ROM and thoracic spine extension to facilitate full upper extremity ROM. AAROM and AROM Progressing to Muscle Performance and Strengthening Progress exercises as they are performed pain free with good shoulder girdle mechanics Begin with AAROM or AROM exercises demonstrated to have < 15% EMG activity level that utilize gravity minimized positions and/or short lever arms Towel slide / horizontal dusting AAROM supine wash cloth press-up progressing to AROM supine press-up Side-lying supported active elevation AROM reclined wedge press-up Slow speed aquatic exercises Supine elastic band FE > 90 Progress to elevation exercises demonstrated to have 16-29% EMG activity level. The patient is generally in the upright position moving the upper limb with support or assistance progressing to unsupported elevation. AAROM pulley Incline board dusting Ball roll on wall 4
19 Upright wall slide Upright wand AAROM into FE Upright wand AAROM concentric, independent active lowering Upright unsupported active FE (no external resistance) Initiate an AROM progressing to light below chest level strengthening program for the deltoid, rotator cuff, and scapula musculature Do not initiate until overall pain level is appropriately low (0-2/10 NPRS), ROM has achieved staged goals for this phase, and patient can tolerate light ADL s at waist level. Emphasize ER, IR, scapula retraction, and short lever forward elevation EMG evidence suggest that typical activity level for these exercises range from the 16-29% category to the > 50% category based on level of resistance and exercise technique Pain free isotonic, elastic resistance, or closed chain exercises in the 16-29% EMG activity range appear appropriate during phase 2 Isotonic exercises in the 16-29% EMG activity level utilize gravity for resistance to no more than 1-2 lbs Elastic resistance exercises in the 16-29% EMG activity level provide no more than 2-3 lbs of resistance by utilizing very light levels of resistance, minimal to no pre-tension, and less than 75% elongation of the band compared to the starting position Closed chain exercises in the 16-29% EMG activity level include the quadruped and triped positions Address abnormal scapular mobility as indicated Improve pectoralis minor flexibility if limited Motor learning drills through auditory, visual, or tactile cues Limb supported AROM activities Strengthen scapular retractors and upward rotators Light manual resistance in supported positions Strength/Endurance: Scapula and core strengthening Address core stability deficits as indicated MILESTONES (TESTING CRITERIA) TO PROGRESS TO PHASE III: Staged ROM goals achieved with minimal to no pain (NPRS 0-2/10) and without substitution patterns. Strengthening activities completed with minimal to no pain (NPRS 0-2/10) Appropriate scapular posture statically and dynamically during ROM /functional activities Goals: Phase 3 (~POM 3 to ~ POM 5) 5
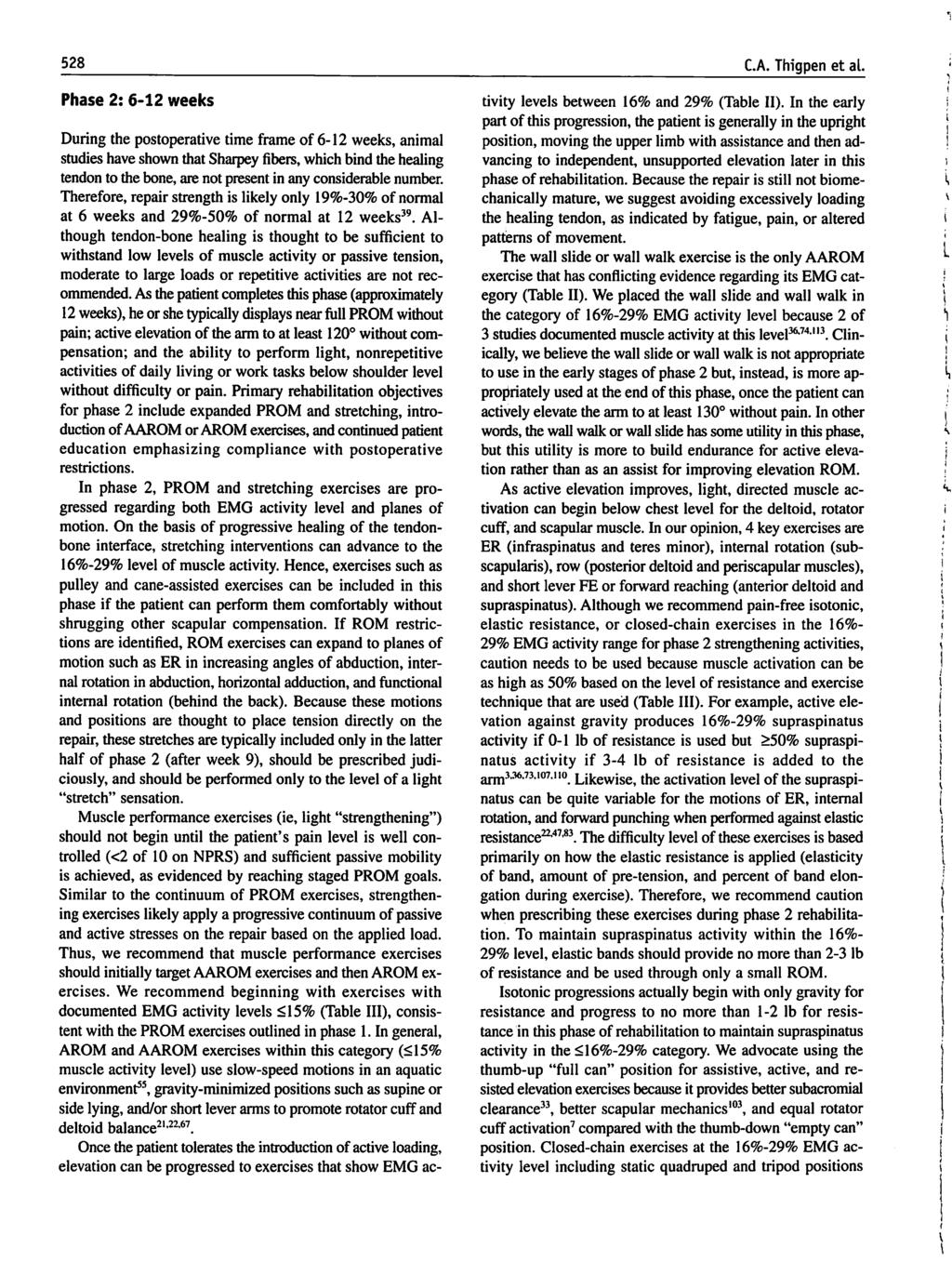
20 Full P/AROM Optimize neuromuscular control Gradually restore of shoulder strength, power, and endurance Return to ADL s, work, and recreational activities that do not require heavy lifting, powerful movements, or repetitive overhead activities INTERVENTIONS TO AVOID: No lifting of objects heavier than lbs. No sudden lifting, jerking, or pushing activities No uncontrolled movements SPECIFIC INTERVENTIONS: Activities of primary importance: Normalize AROM Progressive shoulder girdle strengthening and endurance Progressive neuromuscular control exercises Activities of secondary importance: Minimize or eliminate end range glenohumeral joint stiffness Eliminate deficits in core and scapular performance Patient Education: Counsel in importance of gradually increasing stress to the shoulder while returning to ADL s, work, and recreational activities Education in interventions to avoid (listed above) Pain Management: Continue cryotherapy post activity as needed Extend modalities as needed Ensure appropriate use of upper extremity during ADL s Establish appropriate level of therapeutic exercises PROM / Flexibility: Continue stretching and passive ROM exercises as needed per patient impairments AROM, Strength, Endurance, and/or Power: Continue the phase 2 progressions for below chest level strengthening gradually progressing resistance to be complimentary with the 30-49% EMG activity level. Complete the phase 2 elevation progression of gravity minimized elevation to upright supported/assisted elevation to upright unsupported elevation as patients may not have completed this at the beginning of phase 3 Once phase 2 elevation progression is complete, initiate resisted elevation Ensure that unsupported AROM elevation is pain free and performed without substitution 6
21 Initially performed in a position of comfort with low stress to the surgical repair (e.g. Full Can in the plane of the scapula) Exercises should be progressive in terms of muscle demand / intensity (short lever exercises initially with progression of lever length as appropriate) Exercises should also be progressive in terms of shoulder elevation range Program should focus on relatively low resistance (.5-2 lbs) to keep EMG activity level below 50%. Progressive resisted exercises are matched to the patient s functional demands Nearly full elevation in the scapula plane should be achieved before elevation in other planes Consider other strengthening exercises in the 30-49% EMG activity level based on patient s functional demands and occasionally progressing select patients to exercises below with no weight or very light weight after post-operative month 4 External rotation (ER)/Internal rotation (IR) at various angles of abd Prone Rowing Prone Horizontal Abduction Prone Extension Neuromuscular Re-education: Dynamic stabilization exercises Light PNF for cuff /deltoid/scapula (rhythmic stabilization or slow reversal hold) Open chain kinesthetic awareness drills (ROM replication, etc.) Closed chain activity progression For most patients following arthroscopic rotator cuff repair, Phase 3 concludes their supervised rehabilitation MILESTONES (TESTING CRITERIA) TO PROGRESS TO PHASE 4: MMT at least 4+/5 Pain free with basic ADLs and phase 3 strengthening Patient work demands or goals for recreational activities requires progressive loads or positions not reached during phase 3 exercises Demonstrates adequate shoulder girdle dynamic stability for progression to higher demanding work/sport specific activities. Surgeon approval Phase 4 (~POM 5 to ~ POM 6+) Goals: Maintain full non-painful AROM Normalize muscular strength, power, and endurance Return to demanding functional activities Complete return to sport training 7
22 INTERVENTIONS TO AVOID: Painful activities Activities that result in substitution patterns Exercises significantly more stressful / demanding than functional demands Exercises that provide a large increase in load compared to previous exercises SPECIFIC INTERVENTIONS: Activities of primary importance: Progressive neuromuscular control exercises Progressive strengthening and endurance exercises Exercises that progressively replicate speed and power demands Activity specific progression to sport, work, and hobbies Patient Education: Counsel on importance of gradually increasing stress to the shoulder while returning to normal ADL s, work, and recreational activities. Educate on specific technique and modifications for weight lifting and overhead activities. Pain Management: Cryotherapy PRN Ensure appropriate use, rest/ recovery time of upper extremity during work, recreational hobbies Provide appropriate level of therapeutic exercises PROM/Flexibility: Continue stretching and passive ROM exercises as needed per patient impairments Neuromuscular Re-education: Address any remaining deficits of rotator cuff, scapula, or trunk Advance proprioceptive, neuromuscular activities Strength/ Endurance/ Power: Continue progression of phase 3 strengthening, increasing use of 50% or greater EMG activity exercises and transition to general upper extremity maintenance program such as the Throwers Ten Program Develop an activity specific advanced strengthening progression utilizing the following principles as a guide o Integrate activity specific functional movement patterns (i.e. throwing or work specific) o Decrease amount of external stabilization provided to shoulder girdle (i.e. unsupported IR and ER in elevated positions) o Increase speed of movements 8
23 o Decrease rest time to improve endurance o Suggested Exercises T-band standing PNF patterns T-band 90/90 ER/ IR w/ or w/out arm support T-band batting, golf, or tennis forehand / backhand simulation Progressive return to weight lifting program emphasizing larger, primary upper extremity muscles Start with relatively light weight and high repetitions (15-25) Gradually increase weight over the course of 6-12 weeks May initiate interval sport program after successful 3-6 week period of plyometric program, if appropriate. MILESTONES (TESTING CRITERIA) TO RETURN TO WORK, HOBBIES, SPORT: Clearance from surgeon Adequate strength and endurance of rotator cuff and scapular muscles to perform activities with minimal to no pain (NPRS 0-2/10) or difficulty Complete functional progression 9
24 Appendix B: Decision Making Algorithm for the treatment of a Patient following Arthroscopic Rotator Cuff Repair. Please see separate document. Post- Op Rehabilitation Initiated ü ü ü ü Education Topics - Early Post-Op Visit(s) Nature of surgery Use of sling Limiting use of arm Passive support while sitting/sleeping Criteria Which Will Determine Frequency of Follow Up Visits ü Comprehension- patient can - recall precautions - demonstrate sling use - perform HEP ü Pain- well controlled via - cryotherapy - pain control modalities - medications ü ROM- within staged goals
25 Appendix B: Decision Making Algorithm for the treatment of a Patient following Arthroscopic Rotator Cuff Repair. Please see separate document. Passive ROM Deficit If passive ROM measures lag behind staged ROM goals, the clinician needs to determine if pain or stiffness is the primary barrier and modify interventions accordingly. Pain Predominates - Notify MD - Review early education topics - Pain control modalities - Pendulums only (small arc) - Manual therapy to cervical, thoracic, periscapular areas as needed - Recheck in 1 week - Continue until pain controlled Stiffness Predominates - HEP at least 3x/day - Additional/ alternate PROM exercises - Glenohumeral Joint Mobs - Increase end range time to sec/ repetition - Therapist PROM in clinic 2-3x/week - Continue until ROM goals are met
26 Appendix B: Decision Making Algorithm for the treatment of a Patient following Arthroscopic Rotator Cuff Repair. Please see separate document. Active ROM Deficit If the patient is meeting PROM goals, but is unable to achieve staged AROM goals, the clinician needs to determine if continued weakness of the RC is the limitation or if the deficit is neuromuscular coordination. Rotator cuff function should be tested. The presence of lag signs raises the concern of lack of integrity of the rotator cuff repair. Weakness Without Lag - Consider motor control strategies such as manual PNF, mirror feedback, and positional strengthening - Differentiate rotator cuff vs. scapular muscle deficits - Utilize gravity eliminated or minimized positions - Consider NMES to improve volitional contraction - Supervised visits 1-3x/week until AROM goals met Weakness With Lag - Notify surgeon re: concerns about repair integrity - Modified external rotation exercises within available ROM and/ or multiposition ER isometrics - Subscapularis exercises such as belly press, low forward punches, etc - Progressive, assisted elevation program beginning in gravity eliminated/ minimized positions - Consider NMES to improve volitional contraction - Supervised visits 2-3x/week until RC integrity has been determined and AROM goals have been met Glenohumeral Stiffness Although PROM goals are being met, persistent stiffness at end ranges can perpetuate compensations of NM planning or stresses on incompletely healed RC. These concerns must be balanced against repetitive cyclic stresses at end ranges. - Continue previous focus on passive ROM program - Continue joint mobs/ therapist PROM to improve joint mobility - Educate pt. regarding goals and dosing of ROM program - Judicious volume of AROM exercises - Advise pt. to limit use of shoulder at end ranges, loading in end range positions should be avoided
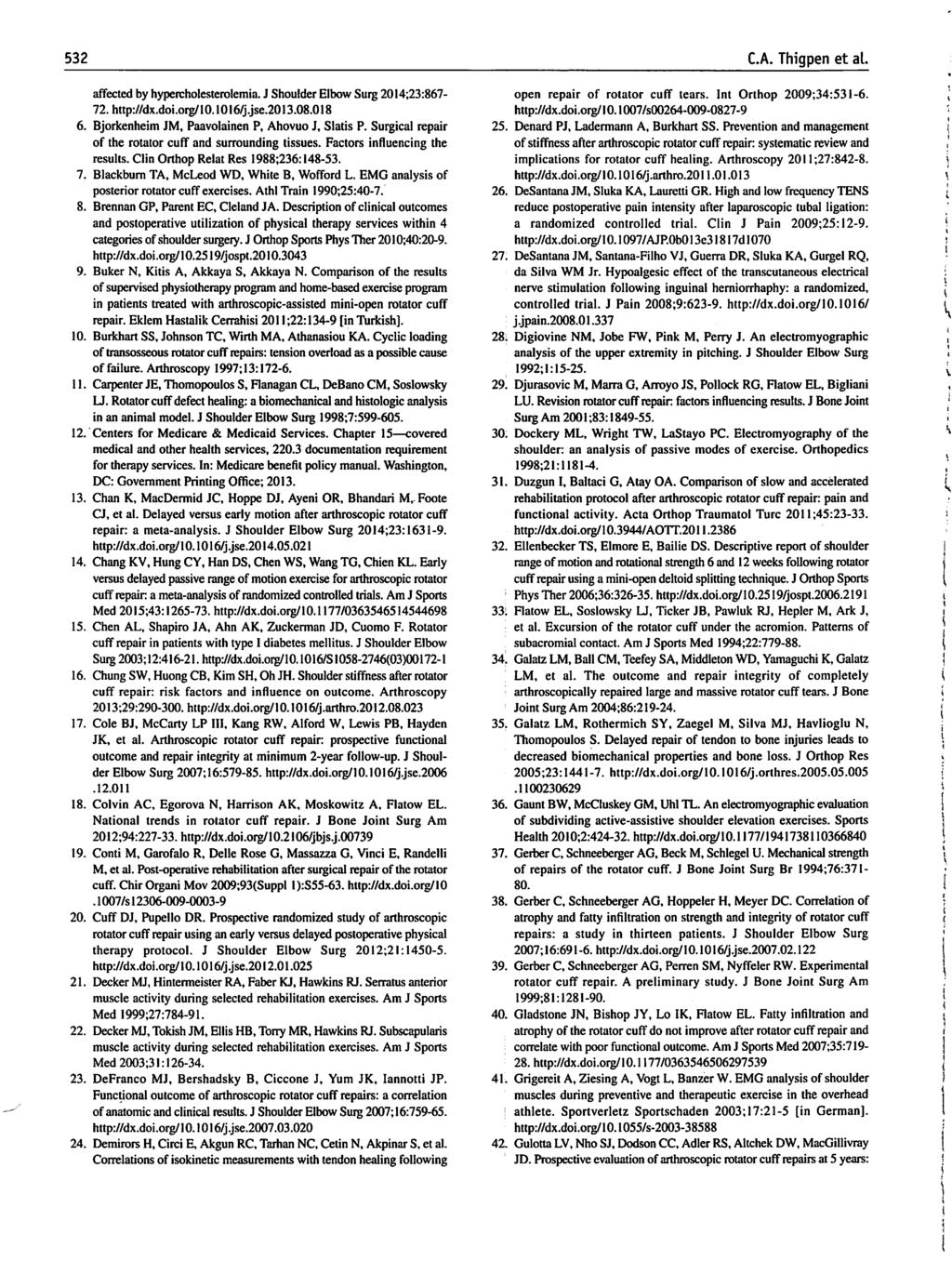
27 Appendix B: Decision Making Algorithm for the treatment of a Patient following Arthroscopic Rotator Cuff Repair. Please see separate document. Advanced Strengthening Is the patient an athlete, laborer or have high demand recreational hobbies? ü ü ü These strengthening exercises may be added at any time post-16 weeks: -Biceps -Triceps -Rows -Lat pull downs -Wrist/ forearm strengthening YES Does the patient have: 4+/5 manual muscle testing? Full AROM for elevation? Tolerance for exercises, ADL s? NO -Supervised rehabilitation ends -Patient should continue a maintenance program several times per week at least through 6 months post-op -Program should include at minimum: -ROM/stretching (PRN) -Short lever arm elevation -Resisted external rotation -Resisted rowing -Biceps strengthening -Triceps strengthening YES NO - Continue ROM as needed - Continue previous strengthening prn - Consider alternate forms of strengthening MREs/isometrics, etc - Modify ADL performance patterns - Recheck ROM/ MMT every 2 weeks Open Kinetic Chain Focus ## Add (on progressive basis, ~ 1 new exercise/ week): -Full can with additional resistance -Resisted diagonal patterns -Resisted IR/ER 90 -Prone horizontal abduction (PHA) -Prone series -Chest press -Military press Is the patient an overhead athlete? ##- Exercises can be combined from open and closed chain boxes to target certain muscles/ movement patterns for creation of a complete treatment program Closed Kinetic Chain Focus ## Add (in progressive order): -Wall push-ups -Table push-ups -Planks -Floor push-ups -Push-ups on unstable surface -Plyometrics (bilateral) -Rhythmic stabilization (bilateral) YES Add: -Plyometrics -Body Blade/Rhythmic Stab. -Eccentrics for rotator cuff NO -Supervised rehabilitation ends -Maintenance program several times per week YES Return to throwing Is the patient a thrower? NO -Supervised rehabilitation ends RETURN TO WORK/SPORT/ HIGH DEMAND HOBBY REQUIREMENTS 1. Clearance from surgeon 2. Adequate strength and endurance of the shoulder girdle to perform activities with minimal to no pain (0-2 out of 10 NPRS) or difficulty 3. Complete functional progression
Rotator Cuff Repair Therapy Protocol
 Bart Eastwood D.O. 825 Davis st Blacksburg, VA 24060 540-951-6000 All information contained in this protocol is to be used as general guidelines only. Specific variations may be appropriate for each patient
Bart Eastwood D.O. 825 Davis st Blacksburg, VA 24060 540-951-6000 All information contained in this protocol is to be used as general guidelines only. Specific variations may be appropriate for each patient
Anterior Stabilization of the Shoulder: Distal Tibial Allograft
 Anterior Stabilization of the Shoulder: Distal Tibial Allograft Name: Diagnosis: Date: Date of Surgery: Phase I Immediate Post Surgical Phase (approximately Weeks 1-3) Minimize shoulder pain and inflammatory
Anterior Stabilization of the Shoulder: Distal Tibial Allograft Name: Diagnosis: Date: Date of Surgery: Phase I Immediate Post Surgical Phase (approximately Weeks 1-3) Minimize shoulder pain and inflammatory
Anterior Stabilization of the Shoulder: Latarjet Protocol
 Robert K. Fullick, MD 6400 Fannin Street, Suite 1700 Houston, Texas 77030 Ph.: 713-486-7543 / Fx.: 713-486-5549 Anterior Stabilization of the Shoulder: Latarjet Protocol The intent of this protocol is
Robert K. Fullick, MD 6400 Fannin Street, Suite 1700 Houston, Texas 77030 Ph.: 713-486-7543 / Fx.: 713-486-5549 Anterior Stabilization of the Shoulder: Latarjet Protocol The intent of this protocol is
Biceps Tenotomy Protocol
 Biceps Tenotomy Protocol A biceps tenotomy procedure involves cutting of the long head of the biceps just prior to its insertion on the superior labrum. A biceps tenotomy is typically done when there is
Biceps Tenotomy Protocol A biceps tenotomy procedure involves cutting of the long head of the biceps just prior to its insertion on the superior labrum. A biceps tenotomy is typically done when there is
Ms. Ruth A. Delaney, MB BCh BAO, MMedSc, MRCS
 Ms. Ruth A. Delaney, MB BCh BAO, MMedSc, MRCS Consultant Orthopaedic Surgeon, Shoulder Specialist. +353 1 5262335 ruthdelaney@sportssurgeryclinic.com Modified from the protocol developed at Boston Shoulder
Ms. Ruth A. Delaney, MB BCh BAO, MMedSc, MRCS Consultant Orthopaedic Surgeon, Shoulder Specialist. +353 1 5262335 ruthdelaney@sportssurgeryclinic.com Modified from the protocol developed at Boston Shoulder
Biceps Tenodesis Protocol
 Biceps Tenodesis Protocol A biceps tenodesis procedure involves cutting of the long head of the biceps just prior to its insertion on the superior labrum and then anchoring the tendon along its anatomical
Biceps Tenodesis Protocol A biceps tenodesis procedure involves cutting of the long head of the biceps just prior to its insertion on the superior labrum and then anchoring the tendon along its anatomical
Ms. Ruth A. Delaney, MB BCh BAO, MMedSc, MRCS
 Ms. Ruth A. Delaney, MB BCh BAO, MMedSc, MRCS Consultant Orthopaedic Surgeon, Shoulder Specialist. +353 1 5262335 ruthdelaney@sportssurgeryclinic.com Modified from the protocol developed at Boston Shoulder
Ms. Ruth A. Delaney, MB BCh BAO, MMedSc, MRCS Consultant Orthopaedic Surgeon, Shoulder Specialist. +353 1 5262335 ruthdelaney@sportssurgeryclinic.com Modified from the protocol developed at Boston Shoulder
Bradley C. Carofino, M.D. Shoulder Specialist 230 Clearfield Avenue, Suite 124 Virginia Beach, Virginia Phone
 Subpectoral Bicep Tenodesis Protocol (Spreadsheet) Weeks 1-2 Modalities Treatment Restrictions Goals No active elbow flexion (6weeks) Full PROM shoulder and elbow PROM: Shoulder, elbow, forearm No active
Subpectoral Bicep Tenodesis Protocol (Spreadsheet) Weeks 1-2 Modalities Treatment Restrictions Goals No active elbow flexion (6weeks) Full PROM shoulder and elbow PROM: Shoulder, elbow, forearm No active
Arthroscopic Anterior Capsulolabral Repair Protocol
 PHASE I: POST-OP WEEKS 0-6 Goals: Arthroscopic Anterior Capsulolabral Repair Protocol Bart Eastwood D.O. 250 South Main St. Suite 224A Blacksburg, VA 24060 540-552-7133 Maximally protect the surgical repair
PHASE I: POST-OP WEEKS 0-6 Goals: Arthroscopic Anterior Capsulolabral Repair Protocol Bart Eastwood D.O. 250 South Main St. Suite 224A Blacksburg, VA 24060 540-552-7133 Maximally protect the surgical repair
Progression to the next phase based on Clinic Criteria and or Time Frames as Appropriate
 Bicep Tenodesis D. WATTS, M.D. Progression to the next phase based on Clinic Criteria and or Time Frames as Appropriate PHASE I PASSIVE RANG OF MOTION PHASE (STARTS APPROXIMATELY POST OP WEEKS 1-2) Minimize
Bicep Tenodesis D. WATTS, M.D. Progression to the next phase based on Clinic Criteria and or Time Frames as Appropriate PHASE I PASSIVE RANG OF MOTION PHASE (STARTS APPROXIMATELY POST OP WEEKS 1-2) Minimize
Limited Goals Program (Examples Include: Cuff Tear Arthropathy, Massive Irrepairable Rotator Cuff Tear, Selected Revision Surgeries)
") Limited Goals Program (Examples Include: Cuff Tear Arthropathy, Massive Irrepairable Rotator Cuff Tear, Selected Revision Surgeries) All information contained in this protocol is to be used as general
Limited Goals Program (Examples Include: Cuff Tear Arthropathy, Massive Irrepairable Rotator Cuff Tear, Selected Revision Surgeries) All information contained in this protocol is to be used as general
Rehab protocol. Phase I: Immediate Post-Surgical Phase: Typically 0-4 weeks; 2 PT visits. Goals:
 Reverse Total shoulder arthroplasty Rehab protocol Phase I: Immediate Post-Surgical Phase: Typically 0-4 weeks; 2 PT visits Allow healing of soft tissue Maintain integrity of replaced joint Gradually increase
Reverse Total shoulder arthroplasty Rehab protocol Phase I: Immediate Post-Surgical Phase: Typically 0-4 weeks; 2 PT visits Allow healing of soft tissue Maintain integrity of replaced joint Gradually increase
Total Shoulder Rehab Protocol Dr. Payne
 Total Shoulder Rehab Protocol Dr. Payne Phase I Immediate Post Surgical Phase (0-4 weeks): Allow healing of soft tissue Maintain integrity of replaced joint Gradually increase passive range of motion (PROM)
Total Shoulder Rehab Protocol Dr. Payne Phase I Immediate Post Surgical Phase (0-4 weeks): Allow healing of soft tissue Maintain integrity of replaced joint Gradually increase passive range of motion (PROM)
AC reconstruction Protocol: Dr. Rolf
 AC reconstruction Protocol: Dr. Rolf The intent of this protocol is to provide the clinician with a guideline of the post-operative rehabilitation course of a patient that has undergone a AC reconstruction
AC reconstruction Protocol: Dr. Rolf The intent of this protocol is to provide the clinician with a guideline of the post-operative rehabilitation course of a patient that has undergone a AC reconstruction
Biceps Tenotomy Protocol
 Department of Rehabilitation Services Physical Therapy The intent of this protocol is to provide the clinician with a guideline of the postoperative rehabilitation course of a patient that has undergone
Department of Rehabilitation Services Physical Therapy The intent of this protocol is to provide the clinician with a guideline of the postoperative rehabilitation course of a patient that has undergone
Post-Operative Instructions Glenoid Reconstruction using Fresh Distal Tibial Allograft
 Day of Surgery Post-Operative Instructions Glenoid Reconstruction using Fresh Distal Tibial Allograft A. Relax. Diet as tolerated. B. Icing is important for the first 5-7 days post-op. While the post-op
Day of Surgery Post-Operative Instructions Glenoid Reconstruction using Fresh Distal Tibial Allograft A. Relax. Diet as tolerated. B. Icing is important for the first 5-7 days post-op. While the post-op
Arthroscopic Rotator Cuff Repair Protocol:
 Arthroscopic Rotator Cuff Repair Protocol: The intent of this protocol is to provide the therapist and patient with guidelines for the post-operative rehabilitation course after arthroscopic SLAP repair.
Arthroscopic Rotator Cuff Repair Protocol: The intent of this protocol is to provide the therapist and patient with guidelines for the post-operative rehabilitation course after arthroscopic SLAP repair.
PROM is not stretching!
 Dx: o Right o Left Shoulder Replacement/Hemiarthroplasty Rehab Date of Surgery: Patient Name: PT/OT: Please evaluate and treat. Follow attached protocol. 2-3 x per week x 6 weeks. Signature/Date: The intent
Dx: o Right o Left Shoulder Replacement/Hemiarthroplasty Rehab Date of Surgery: Patient Name: PT/OT: Please evaluate and treat. Follow attached protocol. 2-3 x per week x 6 weeks. Signature/Date: The intent
TOTAL SHOULDER ARTHROPLASTY / HEMIARTHROPLASTY
 Teodoro P. Nissen, M.D., Q.M.E. Fellowship Trained Board Certified Joseph M. Centeno, M.D. Fellowship Trained Board Certified TOTAL SHOULDER ARTHROPLASTY / HEMIARTHROPLASTY Protocol: The intent of this
Teodoro P. Nissen, M.D., Q.M.E. Fellowship Trained Board Certified Joseph M. Centeno, M.D. Fellowship Trained Board Certified TOTAL SHOULDER ARTHROPLASTY / HEMIARTHROPLASTY Protocol: The intent of this
Christopher K. Jones, MD Colorado Springs Orthopaedic Group
 Christopher K. Jones, MD Colorado Springs Orthopaedic Group 719-632-7669 Total Shoulder Replacement You have undergone a shoulder replacement procedure. The performance of the procedure is complete, but
Christopher K. Jones, MD Colorado Springs Orthopaedic Group 719-632-7669 Total Shoulder Replacement You have undergone a shoulder replacement procedure. The performance of the procedure is complete, but
Total Shoulder Arthroplasty / Hemiarthroplasty Protocol
 Adam N. Whatley, M.D. 6550 Main St., STE. 2300 Zachary, LA 70791 Phone(225)658-1808 Fax(225)658-5299 Total Shoulder Arthroplasty / Hemiarthroplasty Protocol The intent of this protocol is to provide the
Adam N. Whatley, M.D. 6550 Main St., STE. 2300 Zachary, LA 70791 Phone(225)658-1808 Fax(225)658-5299 Total Shoulder Arthroplasty / Hemiarthroplasty Protocol The intent of this protocol is to provide the
Latarjet Repair Rehabilitation Protocol
 General Notes: As tolerated should be understood to include with safety for the reconstruction/repair; a sudden increase in pain, swelling, or other undesirable factors are indicators that you are doing
General Notes: As tolerated should be understood to include with safety for the reconstruction/repair; a sudden increase in pain, swelling, or other undesirable factors are indicators that you are doing
Total Shoulder Arthroplasty / Hemiarthroplasty Therapy Protocol
 Total Shoulder Arthroplasty / Hemiarthroplasty Therapy Protocol The intent of this protocol is to provide the therapist with a guideline of the postoperative rehabilitation course of a patient that has
Total Shoulder Arthroplasty / Hemiarthroplasty Therapy Protocol The intent of this protocol is to provide the therapist with a guideline of the postoperative rehabilitation course of a patient that has
Rehabilitation Guidelines for Total Shoulder Arthroplasty and Hemi-arthroplasty
 Rehabilitation Guidelines for Total Shoulder Arthroplasty and Hemi-arthroplasty Josef K. Eichinger, MD General Information Total Recovery time is between 4-6 months depending on factors such as injury
Rehabilitation Guidelines for Total Shoulder Arthroplasty and Hemi-arthroplasty Josef K. Eichinger, MD General Information Total Recovery time is between 4-6 months depending on factors such as injury
Orthopedic Surgery and Sports Medicine FL License:
 Reverse Shoulder Arthroplasty Protocol: The intent of this protocol is to provide the therapist with a guideline for the post-operative rehabilitation course of a patient that has undergone a Reverse Shoulder
Reverse Shoulder Arthroplasty Protocol: The intent of this protocol is to provide the therapist with a guideline for the post-operative rehabilitation course of a patient that has undergone a Reverse Shoulder
Biceps Tenodesis Protocol
 Robert K. Fullick, MD 6400 Fannin Street, Suite 1700 Houston, Texas 77030 Ph.: 713-486-7543 / Fx.: 713-486-5549 Biceps Tenodesis Protocol The intent of this protocol is to provide the clinician with a
Robert K. Fullick, MD 6400 Fannin Street, Suite 1700 Houston, Texas 77030 Ph.: 713-486-7543 / Fx.: 713-486-5549 Biceps Tenodesis Protocol The intent of this protocol is to provide the clinician with a
Ms. Ruth A. Delaney, MB BCh BAO, MMedSc, MRCS
 Ms. Ruth A. Delaney, MB BCh BAO, MMedSc, MRCS Consultant Orthopaedic Surgeon, Shoulder Specialist. +353 1 5262335 ruthdelaney@sportssurgeryclinic.com Modified from the protocol developed at Boston Shoulder
Ms. Ruth A. Delaney, MB BCh BAO, MMedSc, MRCS Consultant Orthopaedic Surgeon, Shoulder Specialist. +353 1 5262335 ruthdelaney@sportssurgeryclinic.com Modified from the protocol developed at Boston Shoulder
Rotator Cuff Repair Protocol for tear involving Subscapularis Tendon with or without Pectoralis Major Tendon Transfer
 Rotator Cuff Repair Protocol for tear involving Subscapularis Tendon with or without Pectoralis Major Tendon Transfer D. WATTS, MD Precautions: BASIS Tendon healing back to bone is a slow process that
Rotator Cuff Repair Protocol for tear involving Subscapularis Tendon with or without Pectoralis Major Tendon Transfer D. WATTS, MD Precautions: BASIS Tendon healing back to bone is a slow process that
Type II SLAP lesions are created when the biceps anchor has pulled away from the glenoid attachment.
 Arthroscopic Superior Labral (SLAP) Repair Protocol-Type II, IV, and Complex Tears The intent of this protocol is to provide the clinician with a guideline of the post-operative rehabilitation course of
Arthroscopic Superior Labral (SLAP) Repair Protocol-Type II, IV, and Complex Tears The intent of this protocol is to provide the clinician with a guideline of the post-operative rehabilitation course of
Bradley C. Carofino, M.D. Shoulder Specialist 230 Clearfield Avenue, Suite 124 Virginia Beach, Virginia Phone
 Rehabilitation following Arthroscopic Rotator Cuff Repair: Medium Tears Phase I: Immediate Postsurgical Phase (Days 10-14) Precautions: No lifting of objects; No excessive arm motions; No excessive external
Rehabilitation following Arthroscopic Rotator Cuff Repair: Medium Tears Phase I: Immediate Postsurgical Phase (Days 10-14) Precautions: No lifting of objects; No excessive arm motions; No excessive external
Arthroscopic Labral Repair Protocol-Type II, IV, and Complex Tears:
 Arthroscopic Labral Repair Protocol-Type II, IV, and Complex Tears: The intent of this protocol is to provide the clinician with a guideline of the postoperative rehabilitation course of a patient that
Arthroscopic Labral Repair Protocol-Type II, IV, and Complex Tears: The intent of this protocol is to provide the clinician with a guideline of the postoperative rehabilitation course of a patient that
Shoulder Arthroscopy with Posterior Labral Repair Rehabilitation Protocol
 General Notes: As tolerated should be understood to include with safety for the surgical procedure; a sudden increase in pain, swelling, or other undesirable factors are indicators that you are doing too
General Notes: As tolerated should be understood to include with safety for the surgical procedure; a sudden increase in pain, swelling, or other undesirable factors are indicators that you are doing too
ARTHROSCOPIC SLAP LESION REPAIR (TYPE II) WITH THERMAL CAPSULAR SHRINKAGE
 WITH THERMAL CAPSULAR SHRINKAGE") ARTHROSCOPIC SLAP LESION REPAIR (TYPE II) WITH THERMAL CAPSULAR SHRINKAGE I. Phase I Immediate Postoperative Phase Restrictive Motion (Day 1 to Week 6) Goals: Protect the anatomic repair Prevent negative
ARTHROSCOPIC SLAP LESION REPAIR (TYPE II) WITH THERMAL CAPSULAR SHRINKAGE I. Phase I Immediate Postoperative Phase Restrictive Motion (Day 1 to Week 6) Goals: Protect the anatomic repair Prevent negative
Large/Massive Rotator Cuff Repair
 Large/Massive Rotator Cuff Repair 1. Defined a. Suturing of tears within the rotator cuff (most commonly supraspinatus muscle). Massive RCR usually involve more than the supraspinatus. b. May be done arthroscopically
Large/Massive Rotator Cuff Repair 1. Defined a. Suturing of tears within the rotator cuff (most commonly supraspinatus muscle). Massive RCR usually involve more than the supraspinatus. b. May be done arthroscopically
REHABILITATION GUIDELINES FOR ROTATOR CUFF REPAIR FOR TYPE II TEARS (MASSIVE)(+/- SUBACROMIAL DECOMPRESSION)
(+/- SUBACROMIAL DECOMPRESSION)") REHABILITATION GUIDELINES FOR ROTATOR CUFF REPAIR FOR TYPE II TEARS (MASSIVE)(+/- SUBACROMIAL DECOMPRESSION) The rehabilitation guidelines are presented in a criterion based progression. General time frames
REHABILITATION GUIDELINES FOR ROTATOR CUFF REPAIR FOR TYPE II TEARS (MASSIVE)(+/- SUBACROMIAL DECOMPRESSION) The rehabilitation guidelines are presented in a criterion based progression. General time frames
Shoulder Arthroscopy with Rotator Cuff Repair Rehabilitation Protocol
 General Notes: As tolerated should be understood to include with safety for the surgical procedure; a sudden increase in pain, swelling, or other undesirable factors are indicators that you are doing too
General Notes: As tolerated should be understood to include with safety for the surgical procedure; a sudden increase in pain, swelling, or other undesirable factors are indicators that you are doing too
Small Rotator Cuff Repair
 Small Rotator Cuff Repair 1. Defined a. Surgical repair of the rotator cuff (most commonly supraspinatus muscle) utilizing sutures b. May be done arthroscopically or open. c. May be done in conjunction
Small Rotator Cuff Repair 1. Defined a. Surgical repair of the rotator cuff (most commonly supraspinatus muscle) utilizing sutures b. May be done arthroscopically or open. c. May be done in conjunction
WILLIAM M. ISBELL, MD Jeremy R. Stinson PA-C
 WILLIAM M. ISBELL, MD Jeremy R. Stinson PA-C Post-Operative Rehabilitation Guidelines for Total Shoulder Arthroplasty (TSA) The intent of this protocol is to provide the physical therapist with a guideline/treatment
WILLIAM M. ISBELL, MD Jeremy R. Stinson PA-C Post-Operative Rehabilitation Guidelines for Total Shoulder Arthroplasty (TSA) The intent of this protocol is to provide the physical therapist with a guideline/treatment
The Four Phases of Healing During Rehabilitation Following Rotator Cuff Surgery. Phase 1: Immediate postoperative period (weeks 0-6) Goals
 Goals") The Four Phases of Healing During Rehabilitation Following Rotator Cuff Surgery Phase 1: Immediate postoperative period (weeks 0-6) Maintain/protect integrity of repair Gradually increase PROM Diminish
The Four Phases of Healing During Rehabilitation Following Rotator Cuff Surgery Phase 1: Immediate postoperative period (weeks 0-6) Maintain/protect integrity of repair Gradually increase PROM Diminish
SHOULDER ARTHROSCOPY WITH ANTERIOR STABILIZATION / CAPSULORRHAPHY REHABILITATION PROTOCOL
 General Notes As tolerated should be understood to include with safety for the surgical procedure; a sudden increase in pain, swelling, or other undesirable factors are indicators that you are doing too
General Notes As tolerated should be understood to include with safety for the surgical procedure; a sudden increase in pain, swelling, or other undesirable factors are indicators that you are doing too
Charlotte Shoulder Institute
 Charlotte Shoulder Institute Patient Centered. Research Driven. Outcome Maximized. James R. Romanowski, M.D. Novant Health Perry & Cook Orthopedics and Sports Medicine 2826 Randolph Rd. Charlotte, NC 28211
Charlotte Shoulder Institute Patient Centered. Research Driven. Outcome Maximized. James R. Romanowski, M.D. Novant Health Perry & Cook Orthopedics and Sports Medicine 2826 Randolph Rd. Charlotte, NC 28211
Shawn Hennigan, MD Total Shoulder Arthroplasty Protocol. Phase 1 Maximum Protection (0-4 weeks)
") Shawn Hennigan, MD Total Shoulder Arthroplasty Protocol Goals for phase 1 Minimize Pain and inflammation Protect integrity of repair Initiate shoulder PROM Reduce muscular inhibition Maintain AROM of elbow,
Shawn Hennigan, MD Total Shoulder Arthroplasty Protocol Goals for phase 1 Minimize Pain and inflammation Protect integrity of repair Initiate shoulder PROM Reduce muscular inhibition Maintain AROM of elbow,
Charlotte Shoulder Institute
 Charlotte Shoulder Institute Patient Centered. Research Driven. Outcome Maximized. James R. Romanowski, M.D. Novant Health Perry & Cook Orthopedics and Sports Medicine 2826 Randolph Rd. Charlotte, NC 28211
Charlotte Shoulder Institute Patient Centered. Research Driven. Outcome Maximized. James R. Romanowski, M.D. Novant Health Perry & Cook Orthopedics and Sports Medicine 2826 Randolph Rd. Charlotte, NC 28211
Rehabilitation Protocol: Massive Rotator Cuff Tear Repair
 Rehabilitation Protocol: Massive Rotator Cuff Tear Repair Department of Orthopaedic Surgery Lahey Hospital & Medical Center, Burlington 781-744-8650 Lahey Outpatient Center, Lexington 781-372-7020 Lahey
Rehabilitation Protocol: Massive Rotator Cuff Tear Repair Department of Orthopaedic Surgery Lahey Hospital & Medical Center, Burlington 781-744-8650 Lahey Outpatient Center, Lexington 781-372-7020 Lahey
Phase I : Immediate Postoperative Phase- Protected Motion. (0-2 Weeks)
") Phase I : Immediate Postoperative Phase- Protected Motion (0-2 Weeks) Appointments Progression Criteria 2 weeks after surgery Rehabilitation appointments begin within 7-10 days of surgery, continue 1-2
Phase I : Immediate Postoperative Phase- Protected Motion (0-2 Weeks) Appointments Progression Criteria 2 weeks after surgery Rehabilitation appointments begin within 7-10 days of surgery, continue 1-2
TALLGRASS ORTHOPEDIC & SPORTS MEDICINE. Phase I Immediate Post-Surgical Phase (Weeks 0-2) Date: Maintain/protect integrity of the repair
 Date: Maintain/protect integrity of the repair") TALLGRASS ORTHOPEDIC & SPORTS MEDICINE Name: Date of Surgery: Patient Flow Sheet Arthroscopic Rotator Cuff Repair Small to Medium Tears Benedict Figuerres, MD Phase I Immediate Post-Surgical Phase (Weeks
TALLGRASS ORTHOPEDIC & SPORTS MEDICINE Name: Date of Surgery: Patient Flow Sheet Arthroscopic Rotator Cuff Repair Small to Medium Tears Benedict Figuerres, MD Phase I Immediate Post-Surgical Phase (Weeks
REHABILITATION GUIDELINES FOR SUBSCAPULARIS (+/- SUBACROMIAL DECOMPRESSION) Dr. Carson
 Dr. Carson") REHABILITATION GUIDELINES FOR SUBSCAPULARIS (+/- SUBACROMIAL DECOMPRESSION) Dr. Carson The rehabilitation guidelines are presented in a criterion based progression. General time frames are given for reference
REHABILITATION GUIDELINES FOR SUBSCAPULARIS (+/- SUBACROMIAL DECOMPRESSION) Dr. Carson The rehabilitation guidelines are presented in a criterion based progression. General time frames are given for reference
Arthroscopic SLAP Lesion Repair Rehabilitation Guideline
 Arthroscopic SLAP Lesion Repair Rehabilitation Guideline This rehabilitation program is designed to return the individual to their activities as quickly and safely as possible. It is designed for rehabilitation
Arthroscopic SLAP Lesion Repair Rehabilitation Guideline This rehabilitation program is designed to return the individual to their activities as quickly and safely as possible. It is designed for rehabilitation
TOTAL SHOULDER ARTHROPLASTY, HEMIARTHROPLASTY OR REVERSE ARTHROPLASTY
 TOTAL SHOULDER ARTHROPLASTY, HEMIARTHROPLASTY OR REVERSE ARTHROPLASTY Philosophy The following is an outline of the standard post-operative rehabilitation program following total shoulder arthroplasty.
TOTAL SHOULDER ARTHROPLASTY, HEMIARTHROPLASTY OR REVERSE ARTHROPLASTY Philosophy The following is an outline of the standard post-operative rehabilitation program following total shoulder arthroplasty.
UHealth Sports Medicine
 UHealth Sports Medicine Rehabilitation Guidelines for Arthroscopic Rotator Cuff Repair Type 2 Repairs (+/- subacromial decompression) The rehabilitation guidelines are presented in a criterion based progression.
UHealth Sports Medicine Rehabilitation Guidelines for Arthroscopic Rotator Cuff Repair Type 2 Repairs (+/- subacromial decompression) The rehabilitation guidelines are presented in a criterion based progression.
Avon Office 2 Simsbury Rd. Avon, CT Office: (860) Fax: (860) REHABILITATION AFTER REVERSE SHOULDER ARTHROPLASTY
 Fax: (860) REHABILITATION AFTER REVERSE SHOULDER ARTHROPLASTY") Katherine J. Coyner, MD UCONN Musculoskeletal Institute Medical Arts & Research Building 263 Farmington Ave. Farmington, CT 06030 Office: (860) 679-6600 Fax: (860) 679-6649 www.drcoyner.com Avon Office
Katherine J. Coyner, MD UCONN Musculoskeletal Institute Medical Arts & Research Building 263 Farmington Ave. Farmington, CT 06030 Office: (860) 679-6600 Fax: (860) 679-6649 www.drcoyner.com Avon Office
REVERSE TOTAL SHOULDER ARTHROPLASTY PROTOCOL
 Jennifer L. Cook, MD Stephen A. Hanff, MD Florida Joint Care Institute 2165 Little Road, Trinity, Florida 34655 PH: (727) 372 6637 FAX: (727) 375 5044 REVERSE TOTAL SHOULDER ARTHROPLASTY PROTOCOL Shoulder
Jennifer L. Cook, MD Stephen A. Hanff, MD Florida Joint Care Institute 2165 Little Road, Trinity, Florida 34655 PH: (727) 372 6637 FAX: (727) 375 5044 REVERSE TOTAL SHOULDER ARTHROPLASTY PROTOCOL Shoulder
ROTATOR CUFF REPAIR REHAB PROTOCOL
 Jayesh K. Patel, M.D. Trinity Clinic Orthopaedic and Sports Medicine 1327 Troup Hwy Tyler, TX 75701 (903) 510-8840 ROTATOR CUFF REPAIR REHAB PROTOCOL This rehabilitation protocol has been developed for
Jayesh K. Patel, M.D. Trinity Clinic Orthopaedic and Sports Medicine 1327 Troup Hwy Tyler, TX 75701 (903) 510-8840 ROTATOR CUFF REPAIR REHAB PROTOCOL This rehabilitation protocol has been developed for
Jennifer L. Cook, MD Stephen A. Hanff, MD. Rotator Cuff Type I Repair (Small Large Tear)
") Jennifer L. Cook, MD Stephen A. Hanff, MD Florida Joint Care Institute 2165 Little Road, Trinity, Florida 34655 PH: (727) 372 6637 FAX: (727) 375 5044 Rotator Cuff Type I Repair (Small Large Tear) This
Jennifer L. Cook, MD Stephen A. Hanff, MD Florida Joint Care Institute 2165 Little Road, Trinity, Florida 34655 PH: (727) 372 6637 FAX: (727) 375 5044 Rotator Cuff Type I Repair (Small Large Tear) This
Core deconditioning Smoking Outpatient Phase 1 ROM Other
 whereby the ball does not stay properly centered in the shoulder socket during shoulder movement. This condition may be associated with impingement of the rotator cuff on the acromion bone and coracoacromial
whereby the ball does not stay properly centered in the shoulder socket during shoulder movement. This condition may be associated with impingement of the rotator cuff on the acromion bone and coracoacromial
Rehabilitation Guidelines for Large Rotator Cuff Repair
 Rehabilitation Guidelines for Large Rotator Cuff Repair The true shoulder joint is called the glenohumeral joint and consists humeral head and the glenoid. It is a ball and socket joint. Anatomy of the
Rehabilitation Guidelines for Large Rotator Cuff Repair The true shoulder joint is called the glenohumeral joint and consists humeral head and the glenoid. It is a ball and socket joint. Anatomy of the
Arthroscopic Anterior Stabilization Rehab
 Arthroscopic Anterior Stabilization Rehab Phase I (0-3weeks) Sling immobilization-md directed Codmans/Pendulum exercises Wrist/Elbow ROM Gripping exercises FF-AAROM (supine)-limit to 90 o ER to 0 o Sub
Arthroscopic Anterior Stabilization Rehab Phase I (0-3weeks) Sling immobilization-md directed Codmans/Pendulum exercises Wrist/Elbow ROM Gripping exercises FF-AAROM (supine)-limit to 90 o ER to 0 o Sub
REHABILITATION GUIDELINES FOR ROTATOR CUFF REPAIR FOR TYPE I TEARS (+/- SUBACROMINAL DECOMPRESSION)
") REHABILITATION GUIDELINES FOR ROTATOR CUFF REPAIR FOR TYPE I TEARS (+/- SUBACROMINAL DECOMPRESSION) The rehabilitation guidelines are presented in a criterion based progression. General time frames are
REHABILITATION GUIDELINES FOR ROTATOR CUFF REPAIR FOR TYPE I TEARS (+/- SUBACROMINAL DECOMPRESSION) The rehabilitation guidelines are presented in a criterion based progression. General time frames are
Rotator Cuff Repair Protocol
 Protocol This rehabilitation protocol has been developed for the patient following a rotator cuff surgical procedure. This protocol will vary in length and aggressiveness depending on factors such as:
Protocol This rehabilitation protocol has been developed for the patient following a rotator cuff surgical procedure. This protocol will vary in length and aggressiveness depending on factors such as:
MASSIVE ROTATOR CUFF REPAIR. REHABITATION PROTOCOL >3 cm
 MASSIVE ROTATOR CUFF REPAIR REHABITATION PROTOCOL >3 cm Phase I: (Protective Phase) Weeks 0 to 8 Goals: Minimize pain and inflammatory response Achieve ROM goals Establish stable scapula 1. Elbow, wrist
MASSIVE ROTATOR CUFF REPAIR REHABITATION PROTOCOL >3 cm Phase I: (Protective Phase) Weeks 0 to 8 Goals: Minimize pain and inflammatory response Achieve ROM goals Establish stable scapula 1. Elbow, wrist
Latissimus dorsi tendon transfer protocol
 Department of Rehabilitation Services Physical Therapy The intent of this protocol is to provide the physical therapist with a guideline/treatment protocol for the postoperative rehabilitation management
Department of Rehabilitation Services Physical Therapy The intent of this protocol is to provide the physical therapist with a guideline/treatment protocol for the postoperative rehabilitation management
UHealth Sports Medicine
 UHealth Sports Medicine Rehabilitation Guidelines for Arthroscopic Rotator Cuff Repair Type 1 Repairs (+/- subacromial decompression) The rehabilitation guidelines are presented in a criterion based progression.
UHealth Sports Medicine Rehabilitation Guidelines for Arthroscopic Rotator Cuff Repair Type 1 Repairs (+/- subacromial decompression) The rehabilitation guidelines are presented in a criterion based progression.
CENTER FOR ORTHOPAEDICS AND SPINE CARE PHYSICAL THERAPY PROTOCOL ARTHROSCOPIC SLAP LESION REPAIR (TYPE II) BENJAMIN J. DAVIS, MD
 BENJAMIN J. DAVIS, MD") I. Phase I Immediate Postoperative Phase Restrictive Motion (Day 1 to Week 6) Goals: Protect the anatomic repair Prevent negative effects of immobilization Promote dynamic stability Diminish pain and inflammation
I. Phase I Immediate Postoperative Phase Restrictive Motion (Day 1 to Week 6) Goals: Protect the anatomic repair Prevent negative effects of immobilization Promote dynamic stability Diminish pain and inflammation
Shoulder Impingement Rehabilitation Recommendations
 Shoulder Impingement Rehabilitation Recommendations The following protocol can be utilized for conservative care of shoulder impingement as well as post- operative subacromial decompression (SAD) surgery.
Shoulder Impingement Rehabilitation Recommendations The following protocol can be utilized for conservative care of shoulder impingement as well as post- operative subacromial decompression (SAD) surgery.
ARTHROSCOPIC DECOMPRESSION PROTOCOL Dr. Steven Flores
 ARTHROSCOPIC DECOMPRESSION PROTOCOL Dr. Steven Flores This rehabilitation protocol has been developed for the patient following an arthroscopic decompression surgical procedure. The arthroscopic decompression
ARTHROSCOPIC DECOMPRESSION PROTOCOL Dr. Steven Flores This rehabilitation protocol has been developed for the patient following an arthroscopic decompression surgical procedure. The arthroscopic decompression
Rotator Cuff Repair Protocol
 Rotator Cuff Repair Protocol Applicability: Physician Practices Date Effective: 11/2016 Department: Rehabilitation Services Supersedes: Rotator Cuff Repair (Beattie) Date Last Reviewed / or Date Last Revision:
Rotator Cuff Repair Protocol Applicability: Physician Practices Date Effective: 11/2016 Department: Rehabilitation Services Supersedes: Rotator Cuff Repair (Beattie) Date Last Reviewed / or Date Last Revision:
Type Three Rotator Cuff Repair Arthroscopic Assisted with SAD Large to Massive Tears (Greater than 4 cm)
") Type Three Rotator Cuff Repair Arthroscopic Assisted with SAD Large to Massive Tears (Greater than 4 cm) Therapist Phone I. Phase I - Immediate Post-Surgical Phase (Day 1-10) Goals: Maintain Integrity
Type Three Rotator Cuff Repair Arthroscopic Assisted with SAD Large to Massive Tears (Greater than 4 cm) Therapist Phone I. Phase I - Immediate Post-Surgical Phase (Day 1-10) Goals: Maintain Integrity
Avon Office 2 Simsbury Rd. Avon, CT Office: (860) Fax: (860) Arthroscopic Posterior Labral Repair
 Fax: (860) Arthroscopic Posterior Labral Repair") Katherine J. Coyner, MD UCONN Musculoskeletal Institute Medical Arts & Research Building 263 Farmington Ave. Farmington, CT 06030 Office: (860) 679-6600 Fax: (860) 679-6649 www.drcoyner.com Arthroscopic
Katherine J. Coyner, MD UCONN Musculoskeletal Institute Medical Arts & Research Building 263 Farmington Ave. Farmington, CT 06030 Office: (860) 679-6600 Fax: (860) 679-6649 www.drcoyner.com Arthroscopic
Rotator Cuff Repair Protocol
 Rotator Cuff Repair Protocol Applicability: Physician Practices Date Effective: 11/2016 Department: Rehabilitation Services Supersedes: Rotator Cuff Repair (Beattie) Date Last Reviewed / or Date Last Revision:
Rotator Cuff Repair Protocol Applicability: Physician Practices Date Effective: 11/2016 Department: Rehabilitation Services Supersedes: Rotator Cuff Repair (Beattie) Date Last Reviewed / or Date Last Revision:
Diagnosis: s/p ( LEFT / RIGHT ) AC Joint Reconstruction -- Surgery Date:
 AC Joint Reconstruction -- Surgery Date:") UCLA OUTPATIENT REHABILITATION SERVICES! SANTA MONICA! WESTWOOD 1000 Veteran Ave., A level Phone: (310) 794-1323 Fax: (310) 794-1457 1260 15 th St, Ste. 900 Phone: (310) 319-4646 Fax: (310) 319-2269 FOR
UCLA OUTPATIENT REHABILITATION SERVICES! SANTA MONICA! WESTWOOD 1000 Veteran Ave., A level Phone: (310) 794-1323 Fax: (310) 794-1457 1260 15 th St, Ste. 900 Phone: (310) 319-4646 Fax: (310) 319-2269 FOR
ORTHOPEDIC AND SPORTS MEDICINE CENTER
 ORTHOPEDIC AND SPORTS MEDICINE CENTER SPORTS MEDICINE DIVISION COMBINED REHAB PROTOCOLS AAMC ORTHOPEDIC AND SPORTS MEDICINE SPECIALISTS Office: (410) 268-8862 Fax: (410) 268-0380 Rotator Cuff Repair Rehab
ORTHOPEDIC AND SPORTS MEDICINE CENTER SPORTS MEDICINE DIVISION COMBINED REHAB PROTOCOLS AAMC ORTHOPEDIC AND SPORTS MEDICINE SPECIALISTS Office: (410) 268-8862 Fax: (410) 268-0380 Rotator Cuff Repair Rehab
REHABILITATION GUIDELINES FOR ARTHROSCOPIC CAPSULAR SHIFT
 REHABILITATION GUIDELINES FOR ARTHROSCOPIC CAPSULAR SHIFT The rehabilitation guidelines are presented in a criterion based progression. General time frames are given for reference to the average, but individual
REHABILITATION GUIDELINES FOR ARTHROSCOPIC CAPSULAR SHIFT The rehabilitation guidelines are presented in a criterion based progression. General time frames are given for reference to the average, but individual
Rehabilitation after Arthroscopic Posterior Bankart Repair
 Rehabilitation after Arthroscopic Posterior Bankart Repair Phase 1: 0 to 2 weeks after surgery POSTOPERATIVE INSTRUCTIONS You will wake up in the operating room. A sling and an ice pack will be in place.
Rehabilitation after Arthroscopic Posterior Bankart Repair Phase 1: 0 to 2 weeks after surgery POSTOPERATIVE INSTRUCTIONS You will wake up in the operating room. A sling and an ice pack will be in place.
Theodore B. Shybut, M.D. Orthopedics and Sports Medicine 7200 Cambridge St. #10A Houston, Texas Phone: Fax:
 Theodore B. Shybut, M.D. Orthopedics and Sports Medicine 7200 Cambridge St. #10A Houston, Texas 77030 Phone: 713-986-5590 Fax: 713-986-5521 ROTATOR CUFF REPAIR PROTOCOL This rehabilitation protocol has
Theodore B. Shybut, M.D. Orthopedics and Sports Medicine 7200 Cambridge St. #10A Houston, Texas 77030 Phone: 713-986-5590 Fax: 713-986-5521 ROTATOR CUFF REPAIR PROTOCOL This rehabilitation protocol has
(PROTOCOL #18) REVERSE TOTAL SHOULDER ARTHROPLASTY PROTOCOL
 REVERSE TOTAL SHOULDER ARTHROPLASTY PROTOCOL") The following is a set of general guidelines. It is important to remember that each patient is different. The progression of the patient depends on many factors including age and medical health of the
The following is a set of general guidelines. It is important to remember that each patient is different. The progression of the patient depends on many factors including age and medical health of the
THERMAL - ASSISTED CAPSULORRAPHY With or without SLAP Repair
 THERMAL - ASSISTED CAPSULORRAPHY With or without SLAP Repair **It is important for the clinician to determine the capsular response to the heat probe. Patients that have excessive ROM early in the rehab
THERMAL - ASSISTED CAPSULORRAPHY With or without SLAP Repair **It is important for the clinician to determine the capsular response to the heat probe. Patients that have excessive ROM early in the rehab
Rehabilitation Protocol: Arthroscopic Anterior Capsulolabral Repair of the Shoulder - Bankart Repair Rehabilitation Guidelines
 Rehabilitation Protocol: Arthroscopic Anterior Capsulolabral Repair of the Shoulder - Bankart Repair Rehabilitation Guidelines Department of Orthopaedic Surgery Lahey Hospital & Medical Center, Burlington
Rehabilitation Protocol: Arthroscopic Anterior Capsulolabral Repair of the Shoulder - Bankart Repair Rehabilitation Guidelines Department of Orthopaedic Surgery Lahey Hospital & Medical Center, Burlington
Harold Schock III, MD Rotator Cuff Repair Rehabilitation Protocol
 Harold Schock III, MD Rotator Cuff Repair Rehabilitation Protocol The following document is an evidence-based protocol for arthroscopic rotator cuff repair rehabilitation. The protocol is both chronologically
Harold Schock III, MD Rotator Cuff Repair Rehabilitation Protocol The following document is an evidence-based protocol for arthroscopic rotator cuff repair rehabilitation. The protocol is both chronologically
Rotator Cuff Repair +/- Acromioplasty/Mumford. Phase I: 0 to 2 weeks after surgery
 Rotator Cuff Repair +/- Acromioplasty/Mumford 2. Ensure wound healing Phase I: 0 to 2 weeks after surgery 1. Sling: Use your sling all of the time. 2. Use of the affected arm: You may use your hand on
Rotator Cuff Repair +/- Acromioplasty/Mumford 2. Ensure wound healing Phase I: 0 to 2 weeks after surgery 1. Sling: Use your sling all of the time. 2. Use of the affected arm: You may use your hand on
Reverse Total Shoulder Arthroplasty Protocol
 General Information: Reverse Total Shoulder Arthroplasty Protocol Reverse or Inverse Total Shoulder Arthroplasty (rtsa) is designed specifically for the treatment of glenohumeral (GH) arthritis when it
General Information: Reverse Total Shoulder Arthroplasty Protocol Reverse or Inverse Total Shoulder Arthroplasty (rtsa) is designed specifically for the treatment of glenohumeral (GH) arthritis when it
Reverse Total Shoulder Protocol
 Marion Herring, M.D. OrthoVirginia PH: (804) 270-1305 FX: (804) 273-9294 www.orthovirginia.com Reverse Total Shoulder Protocol General Information: Reverse Total Shoulder Arthroplasty (rtsa) is designed
Marion Herring, M.D. OrthoVirginia PH: (804) 270-1305 FX: (804) 273-9294 www.orthovirginia.com Reverse Total Shoulder Protocol General Information: Reverse Total Shoulder Arthroplasty (rtsa) is designed
SLAP Lesion Type II Repair Rehabilitation Program
 SLAP Lesion Type II Repair Rehabilitation Program The GLSM SLAP Type II Repair Rehabilitation Program is an evidence-based and soft tissue healing dependent program allowing patients to progress to vocational
SLAP Lesion Type II Repair Rehabilitation Program The GLSM SLAP Type II Repair Rehabilitation Program is an evidence-based and soft tissue healing dependent program allowing patients to progress to vocational
Mark Adickes, M.D. Orthopedics and Sports Medicine 7200 Cambridge St. #10A Houston, Texas Phone: Fax:
 Mark Adickes, M.D. Orthopedics and Sports Medicine 7200 Cambridge St. #10A Houston, Texas 77030 Phone: 713-986-6016 Fax: 713-986-5411 ROTATOR CUFF REPAIR PROTOCOL This rehabilitation protocol has been
Mark Adickes, M.D. Orthopedics and Sports Medicine 7200 Cambridge St. #10A Houston, Texas 77030 Phone: 713-986-6016 Fax: 713-986-5411 ROTATOR CUFF REPAIR PROTOCOL This rehabilitation protocol has been
SLAP LESION REPAIR PROTOCOL
 SLAP LESION REPAIR PROTOCOL Clarkstown Division This rehabilitation protocol has been developed for the patient following a SLAP (Superior Labrum Anterior Posterior) repair. It is extremely important to
SLAP LESION REPAIR PROTOCOL Clarkstown Division This rehabilitation protocol has been developed for the patient following a SLAP (Superior Labrum Anterior Posterior) repair. It is extremely important to
Reverse Total Shoulder
 Rehabilitation Protocol: Reverse Total Shoulder Department of Orthopaedic Surgery Lahey Hospital & Medical Center, Burlington 781-744-8650 Lahey Outpatient Center, Lexington 781-372-7020 Lahey Medical
Rehabilitation Protocol: Reverse Total Shoulder Department of Orthopaedic Surgery Lahey Hospital & Medical Center, Burlington 781-744-8650 Lahey Outpatient Center, Lexington 781-372-7020 Lahey Medical
Neofitos Stefanides, M.D., P.C.
 Name: Date: Diagnosis: Date of Surgery: Rotator Cuff Physical Therapy Guidelines and Protocol General Guidelines: - Maintain surgical motion early, but don t push it. - Protect the repair (know what muscles
Name: Date: Diagnosis: Date of Surgery: Rotator Cuff Physical Therapy Guidelines and Protocol General Guidelines: - Maintain surgical motion early, but don t push it. - Protect the repair (know what muscles
CENTER FOR ORTHOPAEDICS AND SPINE CARE PHYSICAL THERAPY PROTOCOL BENJAMIN J. DAVIS, MD Type Two Rotator Cuff Repair
 I. Phase I - Immediate Post-Surgical Phase (Day 1-10) Goals: Maintain Integrity of the Repair Gradually Increase Passive Range of Motion Diminish Pain and Inflammation Prevent Muscular Inhibition Passive
I. Phase I - Immediate Post-Surgical Phase (Day 1-10) Goals: Maintain Integrity of the Repair Gradually Increase Passive Range of Motion Diminish Pain and Inflammation Prevent Muscular Inhibition Passive
Rehabilitation Following Arthroscopic Anterior Shoulder Plication in the Overhead Athlete
 Rehabilitation Following Arthroscopic Anterior Shoulder Plication in the Overhead Athlete PHASE I IMMEDIATE GUARDED MOTION PHASE (Weeks 0-6) Reduce postoperative pain and inflammation Promote capsular
Rehabilitation Following Arthroscopic Anterior Shoulder Plication in the Overhead Athlete PHASE I IMMEDIATE GUARDED MOTION PHASE (Weeks 0-6) Reduce postoperative pain and inflammation Promote capsular
Charlotte Shoulder Institute
 Charlotte Shoulder Institute Patient Centered. Research Driven. Outcome Maximized. James R. Romanowski, M.D. Novant Health Perry & Cook Orthopedics and Sports Medicine 2826 Randolph Rd. Charlotte, NC 28211
Charlotte Shoulder Institute Patient Centered. Research Driven. Outcome Maximized. James R. Romanowski, M.D. Novant Health Perry & Cook Orthopedics and Sports Medicine 2826 Randolph Rd. Charlotte, NC 28211
Reverse Total Shoulder Arthroplasty Protocol Shawn Hennigan, MD
 General Information: Reverse Total Shoulder Arthroplasty Protocol Shawn Hennigan, MD Reverse or Inverse Total Shoulder Arthroplasty (rtsa) is designed specifically for the treatment of glenohumeral (GH)
General Information: Reverse Total Shoulder Arthroplasty Protocol Shawn Hennigan, MD Reverse or Inverse Total Shoulder Arthroplasty (rtsa) is designed specifically for the treatment of glenohumeral (GH)
Joshua D. Stein, M.D. Trinity Clinic Orthopaedic and Sports Medicine 1327 Troup Hwy Tyler, TX (903) ARTHROSCOPIC DECOMPRESSION PROTOCOL
 ARTHROSCOPIC DECOMPRESSION PROTOCOL") Joshua D. Stein, M.D. Trinity Clinic Orthopaedic and Sports Medicine 1327 Troup Hwy Tyler, TX 75701 (903) 510-8840 ARTHROSCOPIC DECOMPRESSION PROTOCOL This rehabilitation protocol has been developed for
Joshua D. Stein, M.D. Trinity Clinic Orthopaedic and Sports Medicine 1327 Troup Hwy Tyler, TX 75701 (903) 510-8840 ARTHROSCOPIC DECOMPRESSION PROTOCOL This rehabilitation protocol has been developed for
Mini Open Rotator Cuff Repair Small Tears < 1 cm
 Mini Open Rotator Cuff Repair Small Tears < 1 cm **It is the treating therapist s responsibility along with the referring physician s guidance to determine the actual progression of the patient within
Mini Open Rotator Cuff Repair Small Tears < 1 cm **It is the treating therapist s responsibility along with the referring physician s guidance to determine the actual progression of the patient within
SLAP LESION REPAIR PROTOCOL Dr. Steven Flores
 SLAP LESION REPAIR PROTOCOL Dr. Steven Flores This rehabilitation protocol has been developed for the patient following a SLAP (Superior Labrum Anterior Posterior) repair. It is extremely important to
SLAP LESION REPAIR PROTOCOL Dr. Steven Flores This rehabilitation protocol has been developed for the patient following a SLAP (Superior Labrum Anterior Posterior) repair. It is extremely important to
PHASE I (Begin PT 3-5 days post-op) DOS:
 DOS:") REHABILITATION GUIDELINES FOR POSTERIOR SHOULDER RECONSTRUCTION +/- LABRAL REPAIRS The rehabilitation guidelines are presented in a criterion based progression. General time frames are given for reference
REHABILITATION GUIDELINES FOR POSTERIOR SHOULDER RECONSTRUCTION +/- LABRAL REPAIRS The rehabilitation guidelines are presented in a criterion based progression. General time frames are given for reference
Charlotte Shoulder Institute
 Charlotte Shoulder Institute Patient Centered. Research Driven. Outcome Maximized. James R. Romanowski, M.D. Gill Orthopaedic Midtown Medical Plaza 1918 Randolph Rd., Suite 700 Charlotte, NC 28211 704-342-3544
Charlotte Shoulder Institute Patient Centered. Research Driven. Outcome Maximized. James R. Romanowski, M.D. Gill Orthopaedic Midtown Medical Plaza 1918 Randolph Rd., Suite 700 Charlotte, NC 28211 704-342-3544
Arthroscopic Bankart Repair Rehabilitation Protocol Dr. Mark Adickes
 Arthroscopic Bankart Repair Rehabilitation Protocol Dr. Mark Adickes Introduction: This rehabilitation protocol has been developed for the patient following an arthroscopic Bankart (anteroinferior labral
Arthroscopic Bankart Repair Rehabilitation Protocol Dr. Mark Adickes Introduction: This rehabilitation protocol has been developed for the patient following an arthroscopic Bankart (anteroinferior labral
Arthroscopic SLAP Repair Protocol
 SPORTS & ORTHOPAEDIC SPECIALISTS Arthroscopic SLAP Repair Protocol 6-8 visits over 12 weeks Emphasis is on AAROM and a high repetition, low weight free weight program Address posterior capsular tightness
SPORTS & ORTHOPAEDIC SPECIALISTS Arthroscopic SLAP Repair Protocol 6-8 visits over 12 weeks Emphasis is on AAROM and a high repetition, low weight free weight program Address posterior capsular tightness
Mini Open Rotator Cuff Repair Large (3 5 cm)
") Mini Open Rotator Cuff Repair Large (3 5 cm) Size: small = < 1 cm, medium = 1 3 cm, large 3 5 cm, massive = > 5 cm **It is the treating therapist s responsibility along with the referring physician s guidance
Mini Open Rotator Cuff Repair Large (3 5 cm) Size: small = < 1 cm, medium = 1 3 cm, large 3 5 cm, massive = > 5 cm **It is the treating therapist s responsibility along with the referring physician s guidance
MOON SHOULDER GROUP NONOPERATIVE TREATMENT OF ROTATOR CUFF TENDONOPATHY PHYSICAL THERAPY GUIDELINES
 MOON SHOULDER GROUP NONOPERATIVE TREATMENT OF ROTATOR CUFF TENDONOPATHY PHYSICAL THERAPY GUIDELINES From: Kuhn JE. Exercise in the treatment of rotator cuff impingement. A systematic review and synthesized
MOON SHOULDER GROUP NONOPERATIVE TREATMENT OF ROTATOR CUFF TENDONOPATHY PHYSICAL THERAPY GUIDELINES From: Kuhn JE. Exercise in the treatment of rotator cuff impingement. A systematic review and synthesized
Phase I: 0 to 3 weeks after surgery
 Dx: Right Left RTC (Massive) Repair Date of Surgery: Patient Name: PT/OT: Please evaluate and treat. Follow attached protocol. 2-3 x per week x 6 weeks. Signature/Date: 2. Ensure wound healing Phase I:
Dx: Right Left RTC (Massive) Repair Date of Surgery: Patient Name: PT/OT: Please evaluate and treat. Follow attached protocol. 2-3 x per week x 6 weeks. Signature/Date: 2. Ensure wound healing Phase I: