Sarena Ravi MD, MPH Endocrinologist. Franciscan Physicians Network Division of Endocrinology Chicago, IL
|
|
|
- Jeremy Grant
- 5 years ago
- Views:
Transcription
1 Sarena Ravi MD, MPH Endocrinologist Franciscan Physicians Network Division of Endocrinology Chicago, IL
2 Definition & Diagnosis of Osteoporosis Management of Osteoporosis in all Populations Long term Management of Osteoporosis
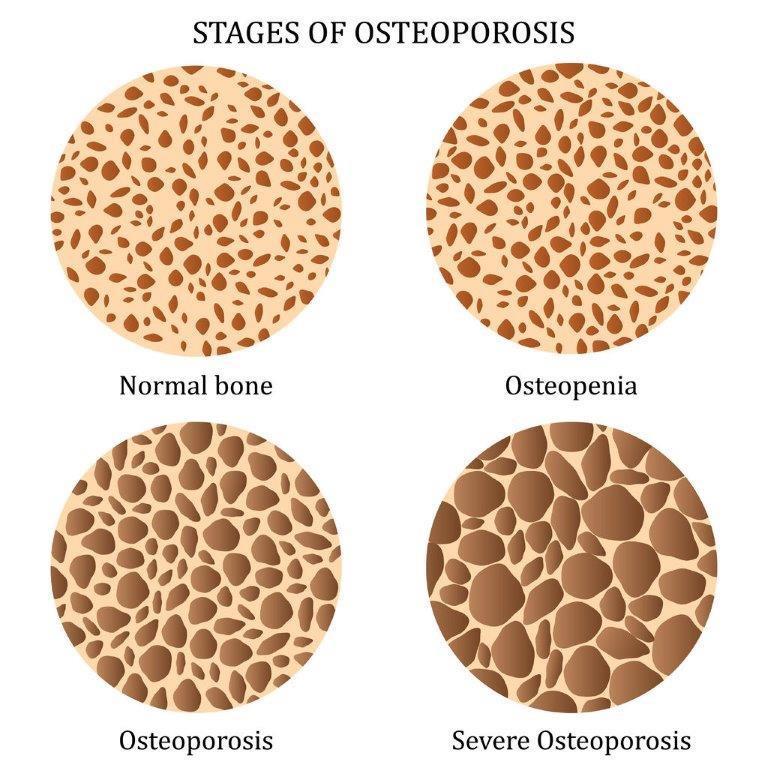
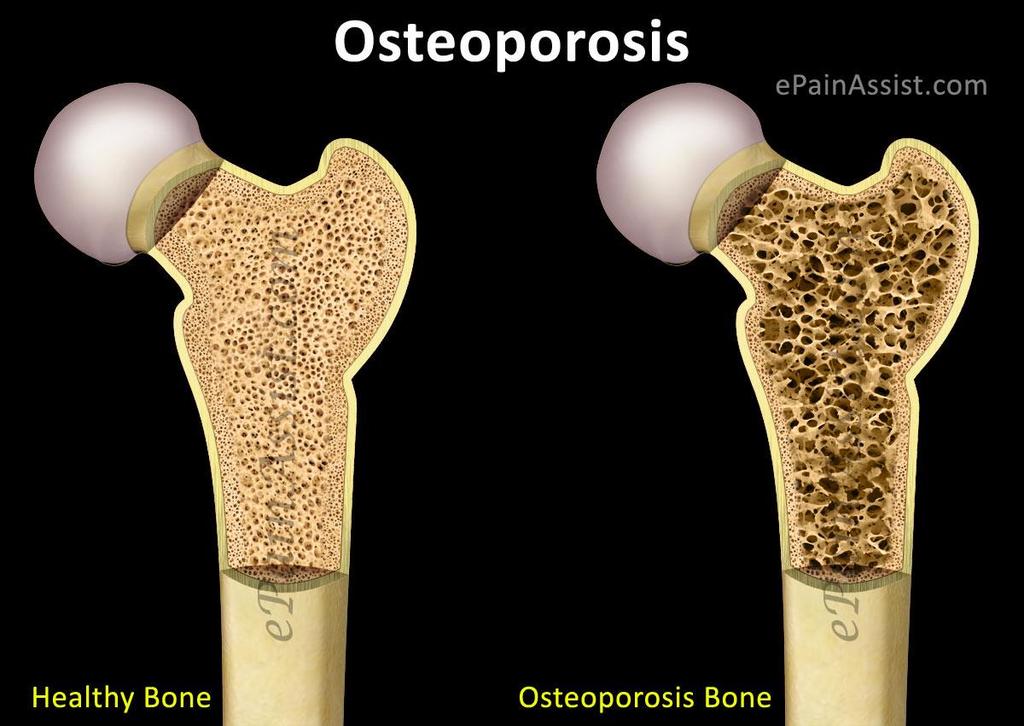
3 Characterized by low bone mass Micro-architectural Disruption Increased Skeletal Fragility Influenced and affected by bone mineral density rates of bone resorption and formation (turnover) bone geometry (size and shape of bone) microarchitecture
4
5

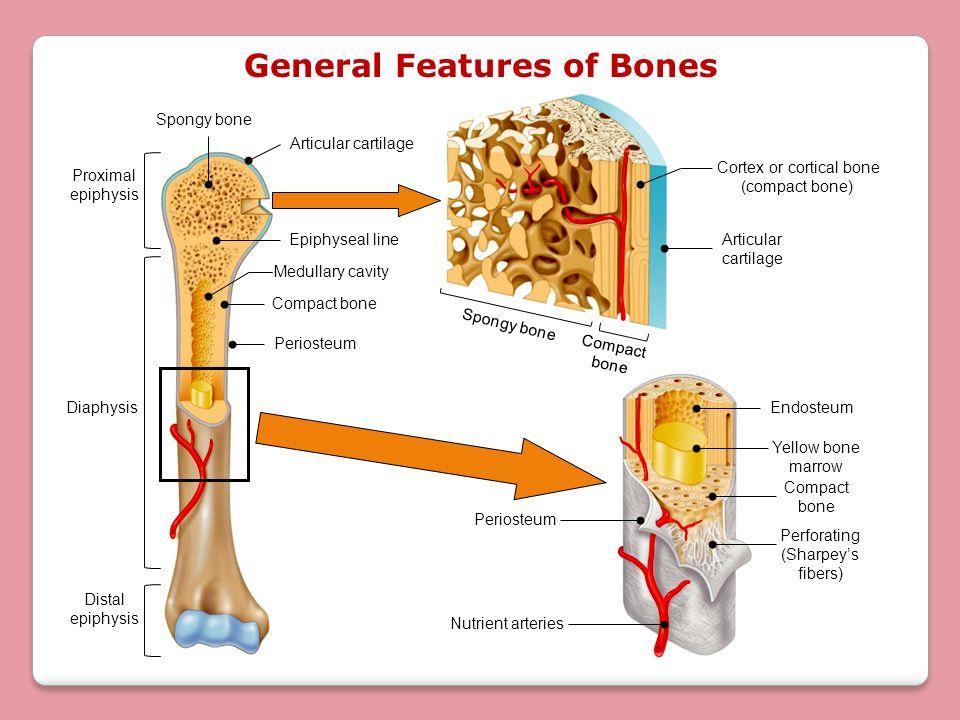
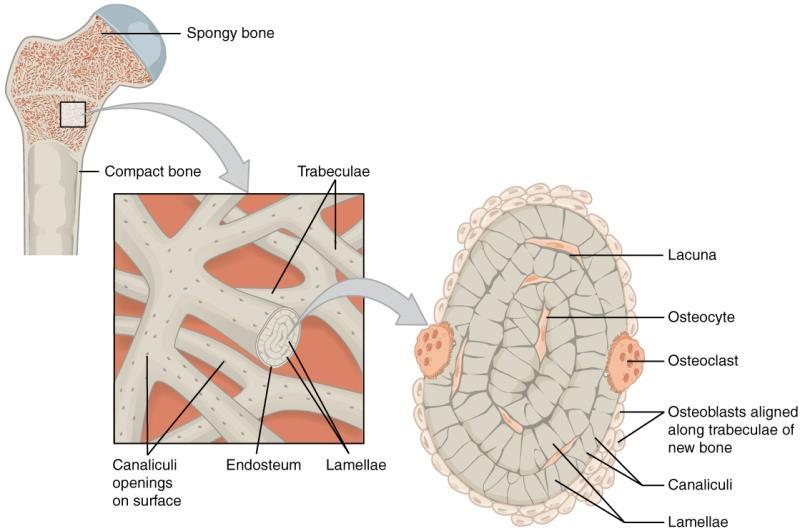
6 Cortical and Trabecular Bone Cortical Bone 80% of all the bone in the body 20% of Bone Turnover Trabecular Bone 20% of all bone in the body 80% of Bone Turnover
7
8 T-score <= -2.5 SD s at any site based upon BMD measurement by dual-energy x-ray absorptiometry (DXA) Fragility Fracture! Particularly at the spine, hip, wrist, humerus, rib, and pelvis Commonly missed FRAGILITY fracture means Osteoporosis BMD assessment by DXA does not apply in presence of fragility fracture
9 A T-score that is 1 to 2.5 SD below the young adult mean is termed low bone mass (osteopenia) Normal bone density is defined as a value within 1 SD of the mean value in the young adult reference population There are actually more fractures in patients with a T-score between - 1 and -2.5 because there are so many more patients in this category
10 Bone Fractures which occur spontaneously or from minor trauma Spine, hip, wrist, humerus, rib, and pelvis Clinical diagnosis of Osteoporosis can be made without BMD Fragility fracture result from mechanical forces that would not ordinarily result in fracture: Fall from a standing height or less Bending, vacuuming, picking up something, coughing and sneezing, walking, daily chores, ect Unknown fracture is incidentally found on imaging
11 57 year old, post-menopausal female Referred to me for thyroid lab abnormality autoimmune hyperthyroidism During Chart Review saw imaging fro 2012 reported vertebral compression fracture DXA scan T-scores were not <= -2.5 (did not report osteoporosis) Was told probably early stages of osteoporosis and did not initiate treatment or refer to specialist Patient herself recalls feeling sudden pain in her back that year while vacuuming (no trauma) Is this Osteoporosis? YES!! In setting of fragility fracture BMD/T-score does not apply! Should this be treated? YES!! Initiated treatment with IV Zolendronic Acid
12 Reference population in which the T-score -2.5 SDs below the mean were standardized to were young, Caucasian females Currently extrapolated to older Men > age 50 Above definition of osteoporosis based on population of Caucasian Females WHO does not have enough data to create definitions for Men or other Ethnic Groups Even in setting of fragility fracture DXA may not be able to report osteoporosis Above Criteria cannot be used in Pre-menopausal women and Men <50 Cannot be used in children
13 WHO: all cut-off values are somewhat arbitrary, but a measured value of bone mineral more than 2.5 standard deviations below the mean for young healthy women at any site (spine, hip, mid-radius) identifies 30 % of all postmenopausal women as having osteoporosis, more than half of whom will have sustained a prior fracture of the proximal femur, spine, distal forearm, proximal humerus or pelvis. Other reasons DXA findings not always accurate: Positioning and errors by technician Variability in machine same machine should be used each time Errors in demographic reporting (age, ect ) Wrong scan mode, invalid skeletal site, inability to report LSC, artifacts, arthritis, ect
14 T-Score WHO Criteria should NOT be applied to Pre-Menopausal women or Men <50 Relationship between BMD and fracture risk is not the same in younger women/men Z-Score Comparison of the patients BMD to an age-matched population -2 or below is considered below expected range for age Coexisting problems should be investigated such as alcoholism and steroid therapy Applied in Children, Men <50, and Pre-Menopausal women
15 Who should be screened for Osteoporosis? National Osteoporosis Foundation (NOF): Women >65 and Men >70 (regardless of clinical RF) Younger Postmenopausal women, women in menopausal transition, and men age with clinical risk factors Adults with fragility fracture >50 years Adults with underlying chronic conditions (eg RA), chronic glucocorticoid use, or other pharmaceutical therapies associated with low BMD AACE Similar to NOF Any adult with a fragility fracture No recommended guidelines for men
16 Clinical Risk Factors & Secondary Causes of Osteoporosis that support early screening: (Women <65, Pre-menopausal, Men 50-69, Men <50) Drugs: Glucocorticoids, Immunosuppressants, Anti-seizure, GnRH agonists/antagonists, Heparin, Chemotherapy GI/Nutrition: Liver disease, Chronic cholestasis, Gastrectomy/GI Surgeries, Malabsorption, Pancreatic disorder, Vit D/Ca deficiency Endocrine: Cushing s, Acromegaly, Adrenal Insufficiency, Eating Disorders, Hyperparathyroidism, Hyperthyroidism, Hyperprolactinemia, Hypogonadism, DM
17 Clinical Risk Factors & Secondary Causes of Osteoporosis that support early screening: (Women <65, Pre-menopausal, Men 50-69, Men <50) Marrow Related Disorders: Hemochromatosis, Multiple Myeloma, Sarcoidosis, SSA/Thalassemia, Lymphoma, ect Organ Transplantation Misc/Genetic: Hemophilia, Idiopathic Hypercalciuria, Ankylosing spondylitis, MS, RA, OI
18 Who should be treated? Management Varies: Post-Menopausal Females and Men > 50 T-score and BMD used to guide treatment/management WHO criteria on T-score should be used Pre-Menopausal Females and Men < 50 WHO criteria on T-score should NOT be used Relationship between BMD and fracture not the same in younger men/women Z-Scores (esp children)
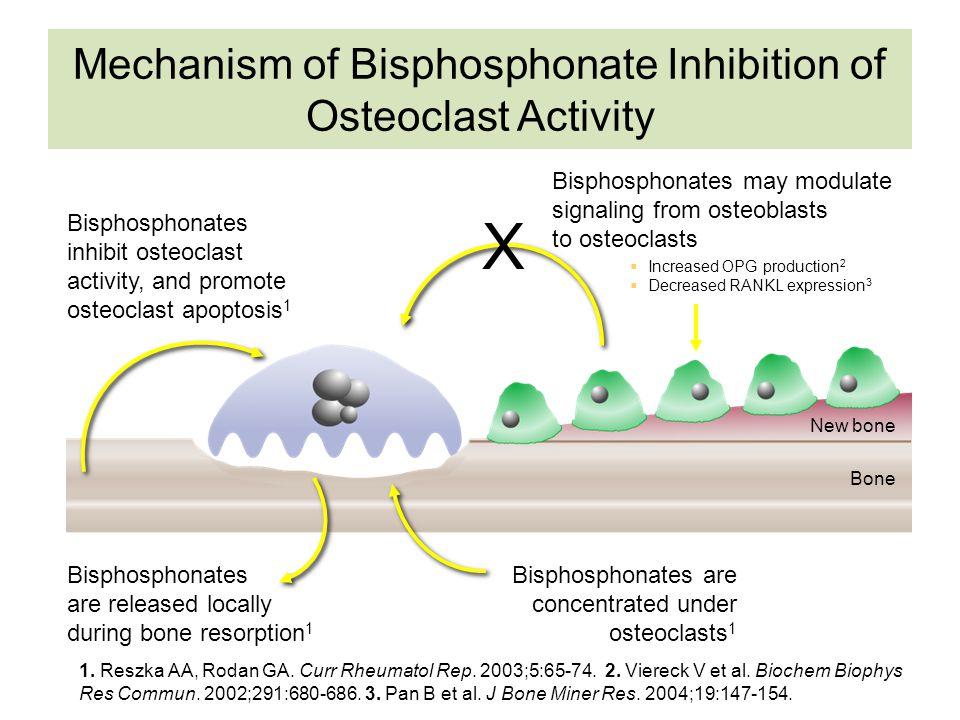
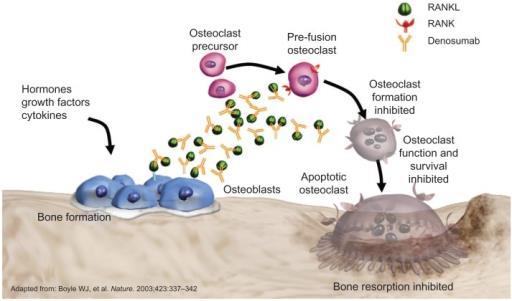
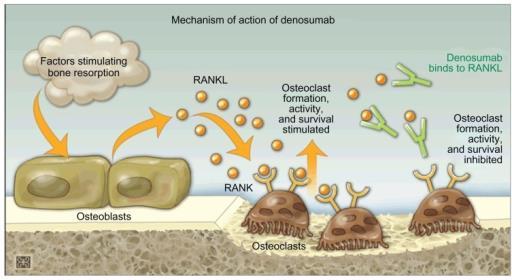
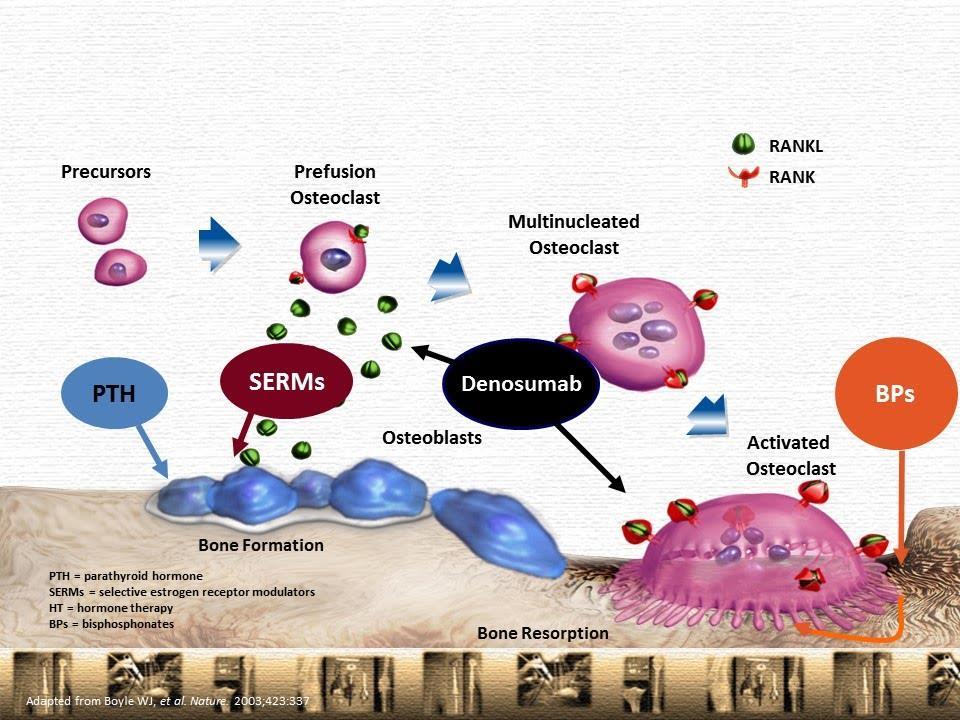
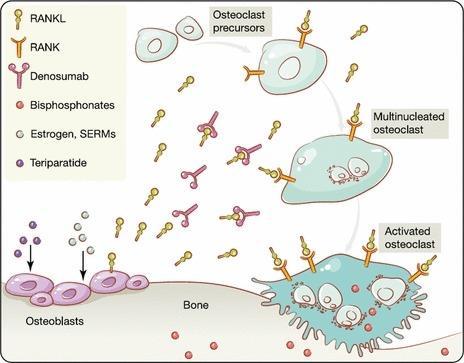
19 Lifestyle measurements & Fall precautions Smoking, Alcohol, Exercise, Diet, Hip Protectors Calcium + Vitamin D Pharmacological Therapy: Bisphosphonates: Anti-resorptive therapy Reduce activity of bone-resorbing Osteoclasts Alendronate, Ibandronate, Risedronate, and Zoledronic Acid Denosumab: Anti-resorptive therapy Decreases formation, differentiation, of Osteoclasts and decreases function of active Osteoclasts Raloxifene Teriparatide/Abaloparatide Anabolic agent
20
21
22
23
24
25
26 T-Score <= -2.5 at any site (AACE) Total hip, Femoral Neck, Lumbar Spine, 33% (1/3 rd ) or Radius Even in the absence of prevalent fracture Osteopenia (T-Score between -1.0 and -2.5) if Fracture Risk is High! Chronic Glucocorticoid Use High Frax Score Fragility Fracture!! Regardless of T-score
27 Osteopenia with high FRAX Score Treat same way as osteoporosis! FRAX Score 10-year probability for Major osteoporotic fracture and Hip fracture >= 20% for Major Treatment with pharmacologic therapy >= 3% for Hip Treatment with pharmacologic therapy Age, height, weight, family history, parent with hip fx, prior fracture, smoking, alcohol use, secondary causes, RA, steroid use, ethnicity, BMD at femoral neck, type of DXA machine All these factors used to calculate FRAX Score Calculation tool where we enter the date score is then given Does not apply when T-score <= -2.5 or if Fragility Fracture Already Osteoporosis! Does not apply to patients already being treated for Osteoporosis
28 Indicate patient s RISK for Fracture Low Mild Moderate High Management Varies LOW Risk Osteopenia No pharmacological treatment Lifestyle measures, Ca, Vitamin D, Fall Precaution
29 MILD Risk Pharmacological Therapy Osteopenia with high FRAX Score/High Fracture Risk Initiate with Bisphosphonates (if no C/I) Treat for 3-5 years (IV/PO) DXA/BMD every 1-2 years Increasing or stable Initiate Drug Holiday End Drug Holiday and Re-Initiate Pharmacological Therapy if: Fragility Fracture Significant Decline in BMD based LSC
30 Moderate Fracture Risk Osteoporosis Per WHO Criteria for T-score No Prior Fragility Fracture, No chronic steroid therapy, T-score not severely low Pharmacological Therapy Bisphosphonates or Denosumab DXA every 1-2 years Increasing or stable BMD Drug Holiday Resume Therapy If: Fragility fracture Significant Decline in BMD Bone Turnover Markers rise to pre-treatment levels Resume therapy 3-5 years after drug holiday
31 Moderate Fracture Risk Osteoporosis Per WHO Criteria for T-score No Prior Fragility Fracture, No chronic steroid therapy, T-score not severely low Pharmacological Therapy Bisphosphonates or Denosumab DXA every 1-2 years Decrease in BMD or Fragility Fracture Assess Compliance Re-evaluate for Secondary Causes! Switch to Injectable if on PO Switch to Anabolic agent (Teriparatide) if on Injectable
32 High Fracture Risk Prior Fragility Fracture Advanced Age, Frailty, Glucocorticoids, Very Low T-Scores, Fall Risk Pharmacological Therapy Teriparatide/Abaloparatide, Denosumab, Zoledronic Acid DXA /BMD yearly or every 1-2 years Denosumab Continue therapy (Drug holiday?) Significant Decline in BMD Teriparatide or anabolic agent Teriparatide (Anabolic) - Only up to 2 years max Sequential Therapy with oral/iv antiresorptive agent! BMD begins to decline after ending therapy Zoledronic Acid Continue for 6 years Significant Decline in BMD Anabolic Agent (Teriparatide)
33 Lifestyle changes (diet, smoking, alcohol, ect ) Calcium + Vitamin D (adequate dietary and supplemental intake) FDA Approved Therapy: Alendronate, Risedronate, Zoledronic Acid Hip Fracture Zoledronic Acid Ibandronate not approved Teriparatide (Abaloparatide only for post-menopausal females) Denosumab only for men receiving ADT for prostate cancer Not YET been shown to prevent fracture in other men Used in clinical practice still does have beneficial effect on BMD Intolerant to other therapies or Impaired Renal Function
34 HYPOGONADISM and OSTEOPOROSIS For men at high risk of fracture and on testosterone therapy Add agent with proven anti-fracture efficacy (e.g. a bisphosphonate or teriparatide). Men at borderline/moderate high risk for fracture with hypogonadism Testosterone therapy in lieu of a bone drug After 2 years of testosterone therapy BMD T-score <-2.5 Add Established Osteoporosis therapy If Testosterone therapy contraindicated Osteoporosis therapy Contraindications to all approved Osteoporosis therapy Suggest testosterone therapy for men at high risk for fracture If established hypogonadism
35 Secondary Causes!! BMD/DXA Testing in these populations if: History of Fragility Fracture Diseases, conditions, or medications associated with low bone mass/bone loss Considering pharmacologic therapy for osteoporosis Monitoring Drug Therapy for Osteoporosis Women in Menopausal Transition if RF are present Low body weight, prior low-trauma fracture, high risk medications, ect
36 Secondary Causes!! Management Ca + Vitamin D (diet + supplements) Weight Bearing Exercises/Lifestyle changes (smoking, alcohol, nutrition ) Treatment of Secondary Causes! Not the same as post-menopausal or men > 50 Pharmacologic Treatment in Selected Cases Refer to Specialist!! Endocrine, Rheumatology, University Center, Specialized Bone Center, ect
37 Table 11 Causes of Secondary Osteoporosis in Adults Endocrine or metabolic causes Nutritional/GI conditions Drugs Disorders of collagen metabolism Other Acromegaly Diabetes mellitus Type 1 Type 2 Growth hormone deficiency Hypercortisolism Hyperparathyroidism Hyperthyroidism Hypogonadism Hypophosphatasia Porphyria Pregnancy Alcoholism Anorexia nervosa Calcium deficiency Chronic liver disease Malabsorption syndromes/ malnutrition (including celiac disease, cystic fibrosis, Crohn s disease, and gastric resection or bypass) Total parenteral nutrition Vitamin D deficiency Antiepileptic drugsa Aromatase inhibitors Chemotherapy/ immunosuppressants Depo-Provera Glucocorticoids Gonadotropin-releasing hormone agents Heparin Lithium Proton pump inhibitors Selective serotonin reuptake inhibitors Thiazolidinediones Thyroid hormone (in supraphysiologic doses) Ehlers-Danlos syndrome Homocystinuria due to cystathionine deficiency Marfan syndrome Osteogenesis imperfect AIDS/HIV AS COPD Gaucher disease Hemophilia Hypercalciuria Immobilization Major depression Myeloma and some cancers Organ transplantation Renal insufficiency/ failure Renal tubular acidosis Rheumatoid arthritis Systemic mastocytosis Thalassemia
38 All Populations with Osteoporosis/Low BMD: CBC/CMP/Phos PTH TSH Vitamin D levels Celiac SPEP/UPEP Test for Cushing s If Clinically Suspicious 24 Hr Urinary Calcium Suspicion of malabsorption, Kidney stones, PTH disorder, Bariatric/GI surgeries More Extensive Testing/Secondary Workup: Pre-Menopausal Females and Men <50 Post-Menopause and Men >50 If Suspicious Clinical Features Present
39 Ca + Vitamin D Supplementation or Adequate Dietary Intake Men > 50 and Post-Menopausal Females Treat if Osteoporosis Present Any dose or duration of GC Men > 50 and Post-Menopausal Females Osteopenia and High risk Treat with Pharmacological Therapy Any dose or duration of GC Therapy All Other Men > 50 and Post-Menopausal Females Prednisone >= 7.5 mg/day or Equivalent for greater than 3 months Treat with Pharmacological Therapy For Prevention Men < 50 and Pre-Menopausal Females Hypogonadism, Fragility Fracture, Z-Scores, Accelerated Bone Loss on DXA Individualized to Patient Refer Specialist
40 Refer to Endocrinology, Rheumatology, University Bone Clinic Pre-menopausal females & Men < 50 Management is Different! Secondary Causes MUST be Investigated and Treated Pediatric Population and Very Young Men/Women Post-Menopausal Women and Men > 50 Chronic management requires experience reading DXA images, BMD comparisons using LSC, Knowledge on Contraindications and SE of Osteoporosis Therapy Chronic management by same provider(s) crucial for appropriate long term care May not have access to prior DXA s for comparisons Patients may not know prior treatments or remember where they were treated Also may now know what years and duration they were treated for osteo Decisions on terminating or continuing Drug Holidays will be difficult
41 Osteoporosis and Chronic Kidney Disease (CKD) Risk for CKD-MBD (Mineral Bone Disease) Renal Osteodystrophy: Adynamic Bone Disease & Osteomalacia Underproduction of Bone Cannot treat with Osteoporosis Therapy Bisphosphonates not recommended in GFR < 35 Specialized Bone Centers may still administer them Anabolic Agents (Forteo & Tymlos) Must be used with caution Risk of 2ndary Hyper-PTH in CKD Denusomab can possibly used in GFR < 30 Not recommended due to risk of Hypocalcemia Very Close Monitoring Underproduction of Bone Cannot treat with Osteoporosis Therapy All cases should have close monitoring by multiple specialists including Nephrology
42 When taking history from New Patients I took Fosamax for 1-2 years was told to stop because it wasn t working I took Fosamax for 12 years I believe I ve been on Fosamax, and Boniva for a few years, and also Actonel I m not sure when my last DXA scan was, or where I had it, or who my doctor was at the time
43 I had a compression fracture, DXA was normal so was never treated I took Fosamax from in my late 30 s early 40 s I ve been on Prolia for few years no never seen Nephrology (Female pt with GFR in the 30 s) I ve been on Fosamax for more than 5 years, I was told to continue it GFR declined to 20 s (Diabetic Nephropathy)
44 When taking history from New Patients I took Fosamax for 1-2 years was told to stop because it wasn t working I took Fosamax for 12 years All Bisphosphonates and Denosumab have a recommended length of treatment before a Drug Holiday Improvements should be assessed over a 3-10 year period not just 1-2 years I believe I ve been on Fosamax, and Boniva for a few years, and also Actonel Makes it difficult to decide on terminating or continuing a Drug Holiday I m not sure when my last DXA scan was, or where I had it, or who my doctor was at the time Without prior DXA/BMD, cannot compare to recent numbers Stability vs. Significant Changes in BMD helps determine further management
45 When taking history from New Patients I had a vertebral fracture DXA was normal so was never treated First Case: Fragility fracture Osteoporosis!! I took Fosamax from in my late 30 s early 40 s How was Osteoporosis diagnosed? (Z-score or T-score?) Secondary work up?? I ve been on Prolia for few years no never seen Nephrology Female pt with GFR in the 30 s Risk for Adynamic Bone Disease should be assessed I ve been on Fosamax for several years, I was told to continue it GFR declined to 20 s (Diabetic Nephropathy) Bisphosphonates should not be used GFR < 35
46 Referred to me for uncontrolled IDDM with hypoglycemia in setting of CKD Chart Review: Osteoporosis diagnosed in 2011 (T-score) Never Treated : Multiple (3) Vertebral fractures developed GFR declined from 50 s to 20 s Significant Chronic Back Pain, Severe decline in mobility, Impaired Ambulation with Inability to do Several Daily Activities Compression fractures led to Central Canal compromise with Spinal Cord Compression Transferred to University Hospital for Neurosurgery management Post-Discharge Months of Rehab
47 GFR Decline from 50 s to 20 s in 1 year ( ) Treatment BEFORE Decline in GFR would have been greatly beneficial Untreated Osteoporosis & Overlooking Fragility Fractures Very Debilitating for patient Increased Morbidity Significant Increases in Cost
48 MAJOR POINTS Fragility Fracture Osteoporosis! Long Term Management Contraindications in therapy (eg GFR..) Dx of Osteoporosis Begin Therapy Commonly Overlooked Secondary Work-up Pre-Menopausal Females and Men < 50 More in depth Secondary work up! Osteopenia with High Risk Treat as Osteoporosis! Chronic Glucocorticoids Assess Fracture Risk
49 Clinical Practice Guidelines for the Diagnosis and Treatment of Postmenopausal Osteoporosis - AACE/ACE Postmenopausal Osteoporosis CPG. Camacho, Pauline M et al Endocr Pract. 2016;22(Suppl 4) Osteoporosis in Men: An Endocrine Society Clinical Practice Guideline. Watts, Nelson B et al. The Journal of Clinical Endocrinology & Metabolism, Volume 97, Issue 6, 1 June 2012, Pages American College of Rheumatology Guideline for the Prevention and Treatment of Glucocorticoid-Induced Osteoporosis. Buckley L, et al. Arthritis Rheumatol. 2017;69(8):1521. Epub 2017 Jun 6. Factors related to variation in premenopausal bone mineral status: a health promotion approach. Tudor-Locke C, McColl RS SO Osteoporos Int. 2000;11(1):1. Epidemiology and clinical features of osteoporosis in young individuals.aukhosla S, Lufkin EG, Hodgson SF, Fitzpatrick LA, Melton LJ 3rd SO Bone. 1994;15(5):551. Low bone mass in premenopausal parous women: identification and the effect of an information and bone density feedback program. AUJones G, Scott F SOJ Clin Densitom. 1999;2(2):109.
BMD: A Continuum of Risk WHO Bone Density Criteria
 Pathogenesis of Osteoporosis Osteoporosis Diagnosis: BMD, FRAX and Assessment of Secondary Osteoporosis AGING MENOPAUSE OTHER RISK FACTORS RESORPTION > FORMATION Bone Loss LOW PEAK BONE MASS Steven T Harris
Pathogenesis of Osteoporosis Osteoporosis Diagnosis: BMD, FRAX and Assessment of Secondary Osteoporosis AGING MENOPAUSE OTHER RISK FACTORS RESORPTION > FORMATION Bone Loss LOW PEAK BONE MASS Steven T Harris
Osteoporosis/Fracture Prevention
 Osteoporosis/Fracture Prevention NATIONAL GUIDELINE SUMMARY This guideline was developed using an evidence-based methodology by the KP National Osteoporosis/Fracture Prevention Guideline Development Team
Osteoporosis/Fracture Prevention NATIONAL GUIDELINE SUMMARY This guideline was developed using an evidence-based methodology by the KP National Osteoporosis/Fracture Prevention Guideline Development Team
Osteoporosis. Treatment of a Silently Developing Disease
 Osteoporosis Treatment of a Silently Developing Disease Marc K. Drezner, MD Senior Associate Dean Emeritus Professor of Medicine Emeritus University of Wisconsin-Madison Auditorium The Forest at Duke October
Osteoporosis Treatment of a Silently Developing Disease Marc K. Drezner, MD Senior Associate Dean Emeritus Professor of Medicine Emeritus University of Wisconsin-Madison Auditorium The Forest at Duke October
Disclosure and Conflicts of Interest Steven T Harris MD Osteoporosis Diagnosis: BMD, FRAX and Assessment of Secondary Osteoporosis
 Osteoporosis Diagnosis: BMD, FRAX and Assessment of Secondary Osteoporosis Steven T Harris MD FACP Clinical Professor of Medicine University of California, San Francisco Disclosure and Conflicts of Interest
Osteoporosis Diagnosis: BMD, FRAX and Assessment of Secondary Osteoporosis Steven T Harris MD FACP Clinical Professor of Medicine University of California, San Francisco Disclosure and Conflicts of Interest
Practical Management Of Osteoporosis
 Practical Management Of Osteoporosis CONFERENCE 2012 Education Centre, Bournemouth.19 November The following companies have given funding towards the cost of this meeting but have no input into the agenda
Practical Management Of Osteoporosis CONFERENCE 2012 Education Centre, Bournemouth.19 November The following companies have given funding towards the cost of this meeting but have no input into the agenda
IEHP UM Subcommittee Approved Authorization Guidelines DEXA Scan
 Policy: IEHP UM Subcommittee Approved Authorization Guidelines IEHP considers bone mineral density testing using DEXA medically necessary for members who meet any of the following criteria: Women aged
Policy: IEHP UM Subcommittee Approved Authorization Guidelines IEHP considers bone mineral density testing using DEXA medically necessary for members who meet any of the following criteria: Women aged
Osteoporosis Agents Drug Class Prior Authorization Protocol
 Osteoporosis Agents Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review of
Osteoporosis Agents Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review of
Current and Emerging Strategies for Osteoporosis
 Current and Emerging Strategies for Osteoporosis I have nothing to disclose. Anne Schafer, MD Assistant Professor of Medicine Division of Endocrinology & Metabolism December 12, 2014 Outline Osteoporosis
Current and Emerging Strategies for Osteoporosis I have nothing to disclose. Anne Schafer, MD Assistant Professor of Medicine Division of Endocrinology & Metabolism December 12, 2014 Outline Osteoporosis
John J. Wolf, DO Family Medicine
 John J. Wolf, DO Family Medicine Objectives: 1. Review incidence & Risk of Osteoporosis 2.Review indications for testing 3.Review current pharmacologic & Non pharmacologic Tx options 4.Understand & Utilize
John J. Wolf, DO Family Medicine Objectives: 1. Review incidence & Risk of Osteoporosis 2.Review indications for testing 3.Review current pharmacologic & Non pharmacologic Tx options 4.Understand & Utilize
CASE 1 WHY IS IT IMPORTANT TO TREAT? FACTS CONCERNS
 4:30-5:15pm Ask the Expert: Osteoporosis SPEAKERS Silvina Levis, MD OSTEOPOROSIS - FACTS 1:3 older women and 1:5 older men will have a fragility fracture after age 50 After 3 years of treatment, depending
4:30-5:15pm Ask the Expert: Osteoporosis SPEAKERS Silvina Levis, MD OSTEOPOROSIS - FACTS 1:3 older women and 1:5 older men will have a fragility fracture after age 50 After 3 years of treatment, depending
Osteoporosis/Fracture Prevention Clinician Guide SEPTEMBER 2017
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Osteoporosis/Fracture Prevention Clinician Guide SEPTEMBER 2017 Introduction This Clinician Guide was developed to assist Primary Care physicians
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Osteoporosis/Fracture Prevention Clinician Guide SEPTEMBER 2017 Introduction This Clinician Guide was developed to assist Primary Care physicians
OSTEOPOROSIS: AN OPPORTUNITY OR OBLIGATION
 OSTEOPOROSIS: AN OPPORTUNITY OR OBLIGATION Debra L. Sietsema, PhD, RN Director, Bone Health Clinical Operations October 5, 2016 OTA NP/PA Course 1 Osteoporosis Definition A skeletal disorder characterized
OSTEOPOROSIS: AN OPPORTUNITY OR OBLIGATION Debra L. Sietsema, PhD, RN Director, Bone Health Clinical Operations October 5, 2016 OTA NP/PA Course 1 Osteoporosis Definition A skeletal disorder characterized
Osteoporosis Management
 Osteoporosis Management Lisa Voss PA C, CCD Laura Frontiero NP C, CCD Kaiser Healthy Bones Program San Diego Disclosures: Nothing to disclose www.zazzle.com 1 Overview How to diagnose Osteoporosis FRAX
Osteoporosis Management Lisa Voss PA C, CCD Laura Frontiero NP C, CCD Kaiser Healthy Bones Program San Diego Disclosures: Nothing to disclose www.zazzle.com 1 Overview How to diagnose Osteoporosis FRAX
Case Finding and Risk Assessment for Osteoporosis
 Case Finding and Risk Assessment for Osteoporosis Patient may present as a fragility fracture or risk fracture Fragility fracture age 50 Clinical risk factors aged 50 Very strong clinical risk factors
Case Finding and Risk Assessment for Osteoporosis Patient may present as a fragility fracture or risk fracture Fragility fracture age 50 Clinical risk factors aged 50 Very strong clinical risk factors
Pharmacy Management Drug Policy
 SUBJECT: - Forteo (teriparatide), Prolia (denosumab), Tymlos (abaloparatide) POLICY NUMBER: Pharmacy-35 EFFECTIVE DATE: 9/07 LAST REVIEW DATE: 9/29/2017 If the member s subscriber contract excludes coverage
SUBJECT: - Forteo (teriparatide), Prolia (denosumab), Tymlos (abaloparatide) POLICY NUMBER: Pharmacy-35 EFFECTIVE DATE: 9/07 LAST REVIEW DATE: 9/29/2017 If the member s subscriber contract excludes coverage
AACE/ACE Osteoporosis Treatment Decision Tool
 AACE/ACE Osteoporosis Treatment Decision Tool What is Osteoporosis? OSTEOPOROSIS is defined as reduced bone strength leading to an increased risk of fracture. Osteoporosis, or porous bones, occurs when
AACE/ACE Osteoporosis Treatment Decision Tool What is Osteoporosis? OSTEOPOROSIS is defined as reduced bone strength leading to an increased risk of fracture. Osteoporosis, or porous bones, occurs when
Download slides:
 Download slides: https://www.tinyurl.com/m67zcnn https://tinyurl.com/kazchbn OSTEOPOROSIS REVIEW AND UPDATE Boca Raton Regional Hospital Internal Medicine Conference 2017 Benjamin Wang, M.D., FRCPC Division
Download slides: https://www.tinyurl.com/m67zcnn https://tinyurl.com/kazchbn OSTEOPOROSIS REVIEW AND UPDATE Boca Raton Regional Hospital Internal Medicine Conference 2017 Benjamin Wang, M.D., FRCPC Division
Osteoporosis and Lupus. Andrew Ruthberg, MD University Rheumatologists
 Osteoporosis and Lupus Andrew Ruthberg, MD University Rheumatologists 1 Forget the medical terminology (osteoporosis, osteopenia, low bone mass, DEXA, DXA, T score etc) The bottom line is that you don
Osteoporosis and Lupus Andrew Ruthberg, MD University Rheumatologists 1 Forget the medical terminology (osteoporosis, osteopenia, low bone mass, DEXA, DXA, T score etc) The bottom line is that you don
Forteo (teriparatide) Prior Authorization Program Summary
 Prior Authorization Program Summary") Forteo (teriparatide) Prior Authorization Program Summary FDA APPROVED INDICATIONS DOSAGE 1 FDA Indication 1 : Forteo (teriparatide) is indicated for: the treatment of postmenopausal women with osteoporosis
Forteo (teriparatide) Prior Authorization Program Summary FDA APPROVED INDICATIONS DOSAGE 1 FDA Indication 1 : Forteo (teriparatide) is indicated for: the treatment of postmenopausal women with osteoporosis
Understanding the Development of Osteoporosis and Preventing Fractures: WHO Do We Treat Now?
 Understanding the Development of Osteoporosis and Preventing Fractures: WHO Do We Treat Now? Steven M. Petak, MD, JD, FACE, FCLM Texas Institute for Reproductive Medicine And Endocrinology, Houston, Texas
Understanding the Development of Osteoporosis and Preventing Fractures: WHO Do We Treat Now? Steven M. Petak, MD, JD, FACE, FCLM Texas Institute for Reproductive Medicine And Endocrinology, Houston, Texas
Clinician s Guide to Prevention and Treatment of Osteoporosis
 Clinician s Guide to Prevention and Treatment of Osteoporosis Published: 15 August 2014 committee of the National Osteoporosis Foundation (NOF) Tipawan khiemsontia,md outline Basic pathophysiology screening
Clinician s Guide to Prevention and Treatment of Osteoporosis Published: 15 August 2014 committee of the National Osteoporosis Foundation (NOF) Tipawan khiemsontia,md outline Basic pathophysiology screening
Chau Nguyen, D.O. Rheumatologist Clinical Assistant Professor of Internal Medicine at Western University of Health Sciences
 Chau Nguyen, D.O Rheumatologist Clinical Assistant Professor of Internal Medicine at Western University of Health Sciences I do not have any relationship with the manufacturer of any commercial products
Chau Nguyen, D.O Rheumatologist Clinical Assistant Professor of Internal Medicine at Western University of Health Sciences I do not have any relationship with the manufacturer of any commercial products
Clinical Practice. Presented by: Internist, Endocrinologist
 Clinical Practice Management of Osteoporosis Presented by: SaeedBehradmanesh, h MD Internist, Endocrinologist Iran, Isfahan, Feb. 2017 Definition: A disease characterized by low bone mass and microarchitectural
Clinical Practice Management of Osteoporosis Presented by: SaeedBehradmanesh, h MD Internist, Endocrinologist Iran, Isfahan, Feb. 2017 Definition: A disease characterized by low bone mass and microarchitectural
nogg Guideline for the diagnosis and management of osteoporosis in postmenopausal women and men from the age of 50 years in the UK
 nogg NATIONAL OSTEOPOROSIS GUIDELINE GROUP Guideline for the diagnosis and management of osteoporosis in postmenopausal women and men from the age of 50 years in the UK Produced by J Compston, A Cooper,
nogg NATIONAL OSTEOPOROSIS GUIDELINE GROUP Guideline for the diagnosis and management of osteoporosis in postmenopausal women and men from the age of 50 years in the UK Produced by J Compston, A Cooper,
Bone Densitometry Pathway
 Bone Densitometry Pathway The goal of the Bone Densitometry pathway is to manage our diagnosed osteopenic and osteoporotic patients, educate and monitor the patient population at risk for bone density
Bone Densitometry Pathway The goal of the Bone Densitometry pathway is to manage our diagnosed osteopenic and osteoporotic patients, educate and monitor the patient population at risk for bone density
Comprehensive Review of Osteoporosis. Alyse Chandler, PharmD, BCPS, CDE March 11, 2018
 Comprehensive Review of Osteoporosis Alyse Chandler, PharmD, BCPS, CDE March 11, 2018 Objectives At the completion of this activity, the pharmacist will be able to: 1. Evaluate AACE/ACE 2016 osteoporosis
Comprehensive Review of Osteoporosis Alyse Chandler, PharmD, BCPS, CDE March 11, 2018 Objectives At the completion of this activity, the pharmacist will be able to: 1. Evaluate AACE/ACE 2016 osteoporosis
Osteoporosis: A Tale of 3 Task Forces!
 Osteoporosis: A Tale of 3 Task Forces! Robert A. Adler, MD McGuire Veterans Affairs Medical Center Virginia Commonwealth University Richmond, Virginia, USA Disclosures The opinions are those of the speaker
Osteoporosis: A Tale of 3 Task Forces! Robert A. Adler, MD McGuire Veterans Affairs Medical Center Virginia Commonwealth University Richmond, Virginia, USA Disclosures The opinions are those of the speaker
The Bare Bones of Osteoporosis. Wendy Rosenthal, PharmD
 The Bare Bones of Osteoporosis Wendy Rosenthal, PharmD Definition A systemic skeletal disease characterized by low bone mass and microarchitectural deterioration of bone tissue, with a consequent increase
The Bare Bones of Osteoporosis Wendy Rosenthal, PharmD Definition A systemic skeletal disease characterized by low bone mass and microarchitectural deterioration of bone tissue, with a consequent increase
Pharmacy Management Drug Policy
 SUBJECT: - Forteo (teriparatide), Prolia (denosumab), Tymlos (abaloparatide), Boniva injection (Ibandronate) POLICY NUMBER: Pharmacy-35 EFFECTIVE DATE: 9/07 LAST REVIEW DATE: 10/15/2018 If the member s
SUBJECT: - Forteo (teriparatide), Prolia (denosumab), Tymlos (abaloparatide), Boniva injection (Ibandronate) POLICY NUMBER: Pharmacy-35 EFFECTIVE DATE: 9/07 LAST REVIEW DATE: 10/15/2018 If the member s
Using the FRAX Tool. Osteoporosis Definition
 How long will your bones remain standing? Using the FRAX Tool Gary Salzman M.D. Director Banner Good Samaritan/ Hayden VAMC Internal Medicine Geriatric Fellowship Program Phoenix, Arizona Using the FRAX
How long will your bones remain standing? Using the FRAX Tool Gary Salzman M.D. Director Banner Good Samaritan/ Hayden VAMC Internal Medicine Geriatric Fellowship Program Phoenix, Arizona Using the FRAX
Beyond the Break. After Breast Cancer: Osteoporosis in Survivorship. Dr Alexandra Ginty CCFP(EM) FCFP Regional Primary Care Lead CCO
 FCFP Regional Primary Care Lead CCO") Beyond the Break After Breast Cancer: Osteoporosis in Survivorship Dr Alexandra Ginty CCFP(EM) FCFP Regional Primary Care Lead CCO Disclosures No disclosures Osteoporosis in Breast Cancer Survivorship
Beyond the Break After Breast Cancer: Osteoporosis in Survivorship Dr Alexandra Ginty CCFP(EM) FCFP Regional Primary Care Lead CCO Disclosures No disclosures Osteoporosis in Breast Cancer Survivorship
Objectives: What is Osteoporosis 10/8/2015. Bone Health/ Osteoporosis: BASICS OF SCREENING, INTERPRETING, AND TREATING
 Bone Health/ Osteoporosis: BASICS OF SCREENING, INTERPRETING, AND TREATING TIFFANY PAUL, APN, CNP, CCD Objectives: Review the diagnosis of Osteoporosis Describe the basics of a bone density exam Identify
Bone Health/ Osteoporosis: BASICS OF SCREENING, INTERPRETING, AND TREATING TIFFANY PAUL, APN, CNP, CCD Objectives: Review the diagnosis of Osteoporosis Describe the basics of a bone density exam Identify
Osteoporosis Treatment Overview. Colton Larson RFUMS October 26, 2018
 Osteoporosis Treatment Overview Colton Larson RFUMS October 26, 2018 Burden of Disease Most common bone disease 9.9 million Americans + 43.1 million Americans have low bone mineral density (BMD) Stealthy
Osteoporosis Treatment Overview Colton Larson RFUMS October 26, 2018 Burden of Disease Most common bone disease 9.9 million Americans + 43.1 million Americans have low bone mineral density (BMD) Stealthy
Osteoporosis - New Guidelines. Michelle Glass B.Sc. (Pharm) June 15, 2011
 June 15, 2011") Osteoporosis - New Guidelines Michelle Glass B.Sc. (Pharm) June 15, 2011 Outline What is Osteoporosis? Who is at risk? What treatments are available? Role of the Pharmacy technician Definition of Osteoporosis
Osteoporosis - New Guidelines Michelle Glass B.Sc. (Pharm) June 15, 2011 Outline What is Osteoporosis? Who is at risk? What treatments are available? Role of the Pharmacy technician Definition of Osteoporosis
Parathyroid Hormone Analog for Osteoporosis Prior Authorization with Quantity Limit Criteria Program Summary
 Parathyroid Hormone Analog for Osteoporosis Prior Authorization with Quantity Limit Criteria Program Summary This prior authorization program applies to Commercial, NetResults A series, NetResults F series
Parathyroid Hormone Analog for Osteoporosis Prior Authorization with Quantity Limit Criteria Program Summary This prior authorization program applies to Commercial, NetResults A series, NetResults F series
Osteoporosis. Overview
 v2 Osteoporosis Overview Osteoporosis is defined as compromised bone strength that increases risk of fracture (NIH Consensus Conference, 2000). Bone strength is characterized by bone mineral density (BMD)
v2 Osteoporosis Overview Osteoporosis is defined as compromised bone strength that increases risk of fracture (NIH Consensus Conference, 2000). Bone strength is characterized by bone mineral density (BMD)
Skeletal Manifestations
 Skeletal Manifestations of Metabolic Bone Disease Mishaela R. Rubin, MD February 21, 2008 The Three Ages of Women Gustav Klimt 1905 1 Lecture Outline Osteoporosis epidemiology diagnosis secondary causes
Skeletal Manifestations of Metabolic Bone Disease Mishaela R. Rubin, MD February 21, 2008 The Three Ages of Women Gustav Klimt 1905 1 Lecture Outline Osteoporosis epidemiology diagnosis secondary causes
Osteoporosis. Open Access. John A. Kanis. Diseases, University of Sheffield, UK
 Journal of Medical Sciences (2010); 3(3): 00-00 Review Article Osteoporosis Open Access John A. Kanis WHO Collaborating Centre for Metabolic Bone Diseases, University of Sheffield, UK incorporated into
Journal of Medical Sciences (2010); 3(3): 00-00 Review Article Osteoporosis Open Access John A. Kanis WHO Collaborating Centre for Metabolic Bone Diseases, University of Sheffield, UK incorporated into
What is Osteoporosis?
 What is Osteoporosis? 2000 NIH Definition A skeletal disorder characterized by compromised bone strength predisposing a person to an increased risk of fracture. Bone strength reflects the integration of
What is Osteoporosis? 2000 NIH Definition A skeletal disorder characterized by compromised bone strength predisposing a person to an increased risk of fracture. Bone strength reflects the integration of
Interpreting DEXA Scan and. the New Fracture Risk. Assessment. Algorithm
 Interpreting DEXA Scan and the New Fracture Risk Assessment Algorithm Prof. Samir Elbadawy *Osteoporosis affect 30%-40% of women in western countries and almost 15% of men after the age of 50 years. Osteoporosis
Interpreting DEXA Scan and the New Fracture Risk Assessment Algorithm Prof. Samir Elbadawy *Osteoporosis affect 30%-40% of women in western countries and almost 15% of men after the age of 50 years. Osteoporosis
Osteoporosis: Are your bones at risk of fracturing? Rachel Wallwork, MD Internal medicine resident Massachusetts General Hospital
 Osteoporosis: Are your bones at risk of fracturing? Rachel Wallwork, MD Internal medicine resident Massachusetts General Hospital What is Osteoporosis? Osteoporosis causes bones to lose density, become
Osteoporosis: Are your bones at risk of fracturing? Rachel Wallwork, MD Internal medicine resident Massachusetts General Hospital What is Osteoporosis? Osteoporosis causes bones to lose density, become
Kristen M. Nebel, DO PENN/ LGHP Geriatrics. Temple Family Medicine Review
 Kristen M. Nebel, DO PENN/ LGHP Geriatrics 10/3/17 Temple Family Medicine Review OBJECTIVES Define Revised 2017 American College of Physician Recommendations Screening, Prevention and Treatment Application
Kristen M. Nebel, DO PENN/ LGHP Geriatrics 10/3/17 Temple Family Medicine Review OBJECTIVES Define Revised 2017 American College of Physician Recommendations Screening, Prevention and Treatment Application
This Coverage Policy applies to Individual Health Insurance Marketplace benefit plans only.
 This Coverage Policy applies to Individual Health Insurance Marketplace benefit plans only. INJECTABLE OSTEOPOSIS AGENTS SUBJECT Pharmacologic Agents: Bisphosphonates: Boniva IV (ibandronate) Reclast (zoledronic
This Coverage Policy applies to Individual Health Insurance Marketplace benefit plans only. INJECTABLE OSTEOPOSIS AGENTS SUBJECT Pharmacologic Agents: Bisphosphonates: Boniva IV (ibandronate) Reclast (zoledronic
Osteoporosis in Men Wendy Rosenthal PharmD. This program has been brought to you by PharmCon
 Osteoporosis in Men Wendy Rosenthal PharmD This program has been brought to you by PharmCon Osteoporosis in Men Speaker: Dr. Wendy Rosenthal, President of MedOutcomes, will be the presenter for this webcast.
Osteoporosis in Men Wendy Rosenthal PharmD This program has been brought to you by PharmCon Osteoporosis in Men Speaker: Dr. Wendy Rosenthal, President of MedOutcomes, will be the presenter for this webcast.
Pharmacy Management Drug Policy
 Clinical criteria used to make utilization review decisions are based on credible scientific evidence published in peer reviewed medical literature generally recognized by the medical community. Guidelines
Clinical criteria used to make utilization review decisions are based on credible scientific evidence published in peer reviewed medical literature generally recognized by the medical community. Guidelines
Osteoporosis: An Overview. Carolyn J. Crandall, MD, MS
 Osteoporosis: An Overview Carolyn J. Crandall, MD, MS Osteoporosis: An Overview Carolyn J. Crandall, MD, MS Professor of Medicine David Geffen School of Medicine at UCLA Objectives Review osteoporosis
Osteoporosis: An Overview Carolyn J. Crandall, MD, MS Osteoporosis: An Overview Carolyn J. Crandall, MD, MS Professor of Medicine David Geffen School of Medicine at UCLA Objectives Review osteoporosis
They are updated regularly as new NICE guidance is published. To view the latest version of this NICE Pathway see:
 : assessing the risk of fragility fracture bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to be used online. They are updated regularly as new
: assessing the risk of fragility fracture bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to be used online. They are updated regularly as new
Osteoporosis challenges
 Osteoporosis challenges Osteoporosis challenges Who should have a fracture risk assessment? Who to treat? Drugs, holidays and unusual adverse effects Fracture liaison service? The size of the problem 1
Osteoporosis challenges Osteoporosis challenges Who should have a fracture risk assessment? Who to treat? Drugs, holidays and unusual adverse effects Fracture liaison service? The size of the problem 1
1
 www.osteoporosis.ca 1 2 Overview of the Presentation Osteoporosis: An Overview Bone Basics Diagnosis of Osteoporosis Drug Therapies Risk Reduction Living with Osteoporosis 3 What is Osteoporosis? Osteoporosis:
www.osteoporosis.ca 1 2 Overview of the Presentation Osteoporosis: An Overview Bone Basics Diagnosis of Osteoporosis Drug Therapies Risk Reduction Living with Osteoporosis 3 What is Osteoporosis? Osteoporosis:
2016 AACE/ACE POSTMENOPAUSAL OSTEOPOROSIS GUIDELINES: Practical Applications. Outline. The Process. Osteoporosis Diagnosis NEW CLINICAL DEFINITION
 2016 AACE/ACE POSTMENOPAUSAL OSTEOPOROSIS GUIDELINES: Practical Applications Steven M. Petak MD, JD, MACE, FACP Associate Clinical Professor Weill-Cornell Medical College Division Head and Chief of Endocrinology
2016 AACE/ACE POSTMENOPAUSAL OSTEOPOROSIS GUIDELINES: Practical Applications Steven M. Petak MD, JD, MACE, FACP Associate Clinical Professor Weill-Cornell Medical College Division Head and Chief of Endocrinology
10/26/2017. Aging Population = more osteoporosis
 Sandra Scholten, FNP-BC Discuss burden of osteoporosis (OP) and clinical consequences of OP fractures. Define OP and techniques used to assess bone density and quality. Improve awareness, diagnosis, and
Sandra Scholten, FNP-BC Discuss burden of osteoporosis (OP) and clinical consequences of OP fractures. Define OP and techniques used to assess bone density and quality. Improve awareness, diagnosis, and
Module 5 - Speaking of Bones Osteoporosis For Health Professionals: Fracture Risk Assessment. William D. Leslie, MD MSc FRCPC
 Module 5 - Speaking of Bones Osteoporosis For Health Professionals: Fracture Risk Assessment William D. Leslie, MD MSc FRCPC Case #1 Age 53: 3 years post-menopause Has always enjoyed excellent health with
Module 5 - Speaking of Bones Osteoporosis For Health Professionals: Fracture Risk Assessment William D. Leslie, MD MSc FRCPC Case #1 Age 53: 3 years post-menopause Has always enjoyed excellent health with
New Developments in Osteoporosis: Screening, Prevention and Treatment
 Osteoporosis: Overview New Developments in Osteoporosis: Screening, Prevention and Treatment Judith Walsh, MD, MPH Departments of Medicine and Epidemiology and Biostatistics UCSF Definitions Risk factors
Osteoporosis: Overview New Developments in Osteoporosis: Screening, Prevention and Treatment Judith Walsh, MD, MPH Departments of Medicine and Epidemiology and Biostatistics UCSF Definitions Risk factors
Management of Osteoporosis : What Do the Guidelines Say? Robert D. Blank, MD, PhD Endocrinology, U of Wisconsin GRECC Service, Middleton VAMC
 Management of Osteoporosis : What Do the Guidelines Say? Robert D. Blank, MD, PhD Endocrinology, U of Wisconsin GRECC Service, Middleton VAMC Learning Goals Review guidelines for osteoporosis Consider
Management of Osteoporosis : What Do the Guidelines Say? Robert D. Blank, MD, PhD Endocrinology, U of Wisconsin GRECC Service, Middleton VAMC Learning Goals Review guidelines for osteoporosis Consider
Aromatase Inhibitors & Osteoporosis
 Aromatase Inhibitors & Osteoporosis Miss Sarah Horn Consultant Oncoplastic Breast Surgeon April 2018 Aims Role of Aromatase Inhibitors (AI) in breast cancer treatment AI s effects on bone health Bone health
Aromatase Inhibitors & Osteoporosis Miss Sarah Horn Consultant Oncoplastic Breast Surgeon April 2018 Aims Role of Aromatase Inhibitors (AI) in breast cancer treatment AI s effects on bone health Bone health
OSTEOPOROSIS IN MEN. Nelson B. Watts, MD OSTEOPOROSIS AND BONE HEALTH SERVICES CINCINNATI, OHIO
 OSTEOPOROSIS IN MEN Nelson B. Watts, MD OSTEOPOROSIS AND BONE HEALTH SERVICES CINCINNATI, OHIO DISCLOSURES Speakers Bureau: Amgen, Radius Consultant: Abbvie, Amgen, Janssen, Radius, Sanofi Watts NB et
OSTEOPOROSIS IN MEN Nelson B. Watts, MD OSTEOPOROSIS AND BONE HEALTH SERVICES CINCINNATI, OHIO DISCLOSURES Speakers Bureau: Amgen, Radius Consultant: Abbvie, Amgen, Janssen, Radius, Sanofi Watts NB et
Management of postmenopausal osteoporosis
 Management of postmenopausal osteoporosis Yeap SS, Hew FL, Chan SP, on behalf of the Malaysian Osteoporosis Society Committee Working Group for the Clinical Guidance on the Management of Osteoporosis,
Management of postmenopausal osteoporosis Yeap SS, Hew FL, Chan SP, on behalf of the Malaysian Osteoporosis Society Committee Working Group for the Clinical Guidance on the Management of Osteoporosis,
NEW DEVELOPMENTS IN OSTEOPOROSIS: SCREENING, PREVENTION AND TREATMENT
 NEW DEVELOPMENTS IN OSTEOPOROSIS: SCREENING, PREVENTION AND TREATMENT Judith Walsh, MD, MPH Departments of Medicine and Epidemiology and Biostatistics UCSF OSTEOPOROSIS: OVERVIEW Definitions Risk factors
NEW DEVELOPMENTS IN OSTEOPOROSIS: SCREENING, PREVENTION AND TREATMENT Judith Walsh, MD, MPH Departments of Medicine and Epidemiology and Biostatistics UCSF OSTEOPOROSIS: OVERVIEW Definitions Risk factors
Major Recommendations Recommendations apply to postmenopausal women and men age 50 and older.
 Clinical Practice Guideline Effective August 2007 (Revised 10/09) This guideline is based upon the guideline developed by an expert committee of the National Osteoporosis Foundation (NOF) in collaboration
Clinical Practice Guideline Effective August 2007 (Revised 10/09) This guideline is based upon the guideline developed by an expert committee of the National Osteoporosis Foundation (NOF) in collaboration
New 2010 Osteoporosis Guidelines: What you and your health provider need to know QUESTIONS&ANSWERS
 New 2010 Osteoporosis Guidelines: What you and your health provider need to know QUESTIONS&ANSWERS Wednesday, December 1, 2010 1:00 p.m. to 2:00 p.m. ET 1. I m 55 years old. I ve been taking Fosavance
New 2010 Osteoporosis Guidelines: What you and your health provider need to know QUESTIONS&ANSWERS Wednesday, December 1, 2010 1:00 p.m. to 2:00 p.m. ET 1. I m 55 years old. I ve been taking Fosavance
Overview. Bone Biology Osteoporosis Osteomalacia Paget s Disease Cases. People Centred Positive Compassion Excellence
 Overview Osteoporosis and Metabolic Bone Disease Dr Chandini Rao Consultant Rheumatologist Bone Biology Osteoporosis Osteomalacia Paget s Disease Cases Bone Biology Osteoporosis Increased bone remodelling
Overview Osteoporosis and Metabolic Bone Disease Dr Chandini Rao Consultant Rheumatologist Bone Biology Osteoporosis Osteomalacia Paget s Disease Cases Bone Biology Osteoporosis Increased bone remodelling
DXA When to order? How to interpret? Dr Nikhil Tandon Department of Endocrinology and Metabolism All India Institute of Medical Sciences New Delhi
 DXA When to order? How to interpret? Dr Nikhil Tandon Department of Endocrinology and Metabolism All India Institute of Medical Sciences New Delhi Clinical Utility of Bone Densitometry Diagnosis (DXA)
DXA When to order? How to interpret? Dr Nikhil Tandon Department of Endocrinology and Metabolism All India Institute of Medical Sciences New Delhi Clinical Utility of Bone Densitometry Diagnosis (DXA)
Men and Osteoporosis So you think that it can t happen to you
 Men and Osteoporosis So you think that it can t happen to you Jonathan D. Adachi MD, FRCPC Alliance for Better Bone Health Chair in Rheumatology Professor, Department of Medicine Michael G. DeGroote School
Men and Osteoporosis So you think that it can t happen to you Jonathan D. Adachi MD, FRCPC Alliance for Better Bone Health Chair in Rheumatology Professor, Department of Medicine Michael G. DeGroote School
Osteoporosis Clinical Guideline. Rheumatology January 2017
 Osteoporosis Clinical Guideline Rheumatology January 2017 Introduction Osteoporosis is a condition of low bone mass leading to an increased risk of low trauma fractures. The prevalence of osteoporosis
Osteoporosis Clinical Guideline Rheumatology January 2017 Introduction Osteoporosis is a condition of low bone mass leading to an increased risk of low trauma fractures. The prevalence of osteoporosis
Pathway from Fracture or Risk Factor to Treatment
 Appendix 6A - Guidance on Diagnosis and Management of Osteoporosis Pathway from Fracture or Risk Factor to Treatment Fragility Fracture = fracture sustained from a low energy fall from standing height
Appendix 6A - Guidance on Diagnosis and Management of Osteoporosis Pathway from Fracture or Risk Factor to Treatment Fragility Fracture = fracture sustained from a low energy fall from standing height
Use of DXA / Bone Density in the Care of Your Patients. Brenda Lee Holbert, M.D. Associate Professor Senior Staff Radiologist
 Use of DXA / Bone Density in the Care of Your Patients Brenda Lee Holbert, M.D. Associate Professor Senior Staff Radiologist Important Websites Resources for Clinicians and Patients www.nof.org www.iofbonehealth.org
Use of DXA / Bone Density in the Care of Your Patients Brenda Lee Holbert, M.D. Associate Professor Senior Staff Radiologist Important Websites Resources for Clinicians and Patients www.nof.org www.iofbonehealth.org
Fragility Fractures and Secondary Fracture Prevention DeAnn Stowe, RN, MSN, ACNP-BC Cox Health- South Fracture Liaison Service
 Fragility Fractures and Secondary Fracture Prevention DeAnn Stowe, RN, MSN, ACNP-BC Cox Health- South Fracture Liaison Service Objectives Define Fragility Fractures and discuss importance of identification
Fragility Fractures and Secondary Fracture Prevention DeAnn Stowe, RN, MSN, ACNP-BC Cox Health- South Fracture Liaison Service Objectives Define Fragility Fractures and discuss importance of identification
OSTEOPOROSIS AND WHAT TO DO AFTER A VERTEBRAL FRACTURE. Lydia Au Geriatrics Ng Teng Fong Hospital
 OSTEOPOROSIS AND WHAT TO DO AFTER A VERTEBRAL FRACTURE Lydia Au Geriatrics Ng Teng Fong Hospital LET S START WITH WHAT YOU WANT TO KNOW AND DO WITH A VERT FRACTURE Vertebral fractures Most common (550K
OSTEOPOROSIS AND WHAT TO DO AFTER A VERTEBRAL FRACTURE Lydia Au Geriatrics Ng Teng Fong Hospital LET S START WITH WHAT YOU WANT TO KNOW AND DO WITH A VERT FRACTURE Vertebral fractures Most common (550K
Treatments for Osteoporosis Expected Benefits, Potential Harms and Drug Holidays. Suzanne Morin MD FRCP FACP McGill University May 2014
 Treatments for Osteoporosis Expected Benefits, Potential Harms and Drug Holidays Suzanne Morin MD FRCP FACP McGill University May 2014 Learning Objectives Overview of osteoporosis management Outline efficacy
Treatments for Osteoporosis Expected Benefits, Potential Harms and Drug Holidays Suzanne Morin MD FRCP FACP McGill University May 2014 Learning Objectives Overview of osteoporosis management Outline efficacy
Osteoporosis. When we talk about osteoporosis, we have to be familiar with the constituents of bone and what it is formed of.
 Osteoporosis When we talk about osteoporosis, we have to be familiar with the constituents of bone and what it is formed of. Osteoblasts by definition are those cells present in the bone and are involved
Osteoporosis When we talk about osteoporosis, we have to be familiar with the constituents of bone and what it is formed of. Osteoblasts by definition are those cells present in the bone and are involved
Management of Osteoporosis Clinical Practice Guideline September 2013
 Management of Osteoporosis Clinical Practice Guideline September 2013 MedStar Health and MedStar Family Choice accept and endorse the clinical guidelines set forth by the National Osteoporosis Foundation
Management of Osteoporosis Clinical Practice Guideline September 2013 MedStar Health and MedStar Family Choice accept and endorse the clinical guidelines set forth by the National Osteoporosis Foundation
AETNA BETTER HEALTH Prior Authorization guideline for Injectable Osteoporosis Agents
 AETNA BETTER HEALTH Prior Authorization guideline for Injectable Osteoporosis Agents Injectable Osteoporosis Agents Forteo (teriparatide); zoledronic acid Prolia (denosumab)] Authorization guidelines For
AETNA BETTER HEALTH Prior Authorization guideline for Injectable Osteoporosis Agents Injectable Osteoporosis Agents Forteo (teriparatide); zoledronic acid Prolia (denosumab)] Authorization guidelines For
Page 1
 Osteoporosis Osteoporosis is a condition characterised by weakened bones that fracture easily. After menopause many women are at risk of developing osteoporosis. Peak bone mass is usually reached during
Osteoporosis Osteoporosis is a condition characterised by weakened bones that fracture easily. After menopause many women are at risk of developing osteoporosis. Peak bone mass is usually reached during
Osteoporosis. Current Trend in Osteoporosis Management for Elderly in HK- Medical Perspective. Old Definition of Osteoporosis
 Current Trend in Osteoporosis Management for Elderly in HK- Medical Perspective Dr Dicky T.K. Choy Physician Jockey Club Centre for Osteoporosis Care and Control, CUHK Osteoporosis Global public health
Current Trend in Osteoporosis Management for Elderly in HK- Medical Perspective Dr Dicky T.K. Choy Physician Jockey Club Centre for Osteoporosis Care and Control, CUHK Osteoporosis Global public health
BAD TO THE BONE. Peter Jones, Rheumatologist QE Health, Rotorua. GP CME Conference Rotorua, June 2008
 BAD TO THE BONE Peter Jones, Rheumatologist QE Health, Rotorua GP CME Conference Rotorua, June 2008 Agenda Osteoporosis in Men Vitamin D and Calcium Long-term treatment with Bisphosphonates Pathophysiology
BAD TO THE BONE Peter Jones, Rheumatologist QE Health, Rotorua GP CME Conference Rotorua, June 2008 Agenda Osteoporosis in Men Vitamin D and Calcium Long-term treatment with Bisphosphonates Pathophysiology
Healthy Bones: Osteoporosis Management. Laurel Short, MSN, FNP-C
 Healthy Bones: Osteoporosis Management Laurel Short, MSN, FNP-C Disclosure I have no current affiliation or financial interest with any grantor or commercial interests that may have direct interest in
Healthy Bones: Osteoporosis Management Laurel Short, MSN, FNP-C Disclosure I have no current affiliation or financial interest with any grantor or commercial interests that may have direct interest in
COURSE OUTLINE - Module I
 Module I MEDICAL DISCLAIMER The information in this program is for educational purposes only. It is meant to as a guide towards health and does not replace the evaluation by and advice of a qualified licensed
Module I MEDICAL DISCLAIMER The information in this program is for educational purposes only. It is meant to as a guide towards health and does not replace the evaluation by and advice of a qualified licensed
Update on Osteoporosis 2016
 WELCOME! Update on Osteoporosis 2016 Jennifer J. Kelly, D.O., F.A.C.E. Associate Professor of Medicine Division of Endocrinology, Diabetes and Metabolism Upstate Medical University Director of the Clinical
WELCOME! Update on Osteoporosis 2016 Jennifer J. Kelly, D.O., F.A.C.E. Associate Professor of Medicine Division of Endocrinology, Diabetes and Metabolism Upstate Medical University Director of the Clinical
Learning Objectives. Controversies in Osteoporosis Prevention and Management. Etiology. Presenter Disclosure Information. Epidemiology.
 12:45 1:30pm Controversies in Osteoporosis Prevention and Management SPEAKER Carolyn Crandall, MD, MS Presenter Disclosure Information The following relationships exist related to this presentation: Carolyn
12:45 1:30pm Controversies in Osteoporosis Prevention and Management SPEAKER Carolyn Crandall, MD, MS Presenter Disclosure Information The following relationships exist related to this presentation: Carolyn
SpongeBone Menopants*
 SpongeBone Menopants* Adam Fershko, MD, FACP Kettering Health Network *Postmenopausal Osteoporosis Objectives O Epidemiology O Clinical significance O Pathophysiology O Screening and Diagnosis O Treatment
SpongeBone Menopants* Adam Fershko, MD, FACP Kettering Health Network *Postmenopausal Osteoporosis Objectives O Epidemiology O Clinical significance O Pathophysiology O Screening and Diagnosis O Treatment
DISCLAIMER DO NOT DISTRIBUTE
 DISCLAIMER The information contained in this presentation is not intended as a substitute for professional medical advice, diagnosis, or treatment. It is provided for educational purposes only. You assume
DISCLAIMER The information contained in this presentation is not intended as a substitute for professional medical advice, diagnosis, or treatment. It is provided for educational purposes only. You assume
Osteoporosis and Bone Health. Heather Schickedanz, MD Geriatric Knowledge Network, 08/10/16
 Osteoporosis and Bone Health Heather Schickedanz, MD Geriatric Knowledge Network, 08/10/16 1 Learning Objectives Recognize the risk factors for osteoporosis Diagnose and treat osteoporosis Reduce the risk
Osteoporosis and Bone Health Heather Schickedanz, MD Geriatric Knowledge Network, 08/10/16 1 Learning Objectives Recognize the risk factors for osteoporosis Diagnose and treat osteoporosis Reduce the risk
OSTEOPOROSIS: PREVENTION AND MANAGEMENT
 OSTEOPOROSIS: OVERVIEW OSTEOPOROSIS: PREVENTION AND MANAGEMENT Judith Walsh, MD, MPH Departments of Medicine and Epidemiology and Biostatistics UCSF Definitions Key Risk factors Screening and Monitoring
OSTEOPOROSIS: OVERVIEW OSTEOPOROSIS: PREVENTION AND MANAGEMENT Judith Walsh, MD, MPH Departments of Medicine and Epidemiology and Biostatistics UCSF Definitions Key Risk factors Screening and Monitoring
Management of Osteoporosis
 Management of Osteoporosis Clinical Practice Guideline These guidelines are provided to assist physicians and other clinicians in making decisions regarding the care of their patients. They are not a substitute
Management of Osteoporosis Clinical Practice Guideline These guidelines are provided to assist physicians and other clinicians in making decisions regarding the care of their patients. They are not a substitute
Guideline for the investigation and management of osteoporosis. for hospitals and General Practice
 Guideline for the investigation and management of osteoporosis for hospitals and General Practice Background Low bone density is an important risk factor for fracture. The aim of assessing bone density
Guideline for the investigation and management of osteoporosis for hospitals and General Practice Background Low bone density is an important risk factor for fracture. The aim of assessing bone density
8/6/2018. Glucocorticoid induced osteoporosis: overlooked and undertreated? Disclosure. Objectives. Overview
 Disclosure Glucocorticoid induced osteoporosis: overlooked and undertreated? I have no financial disclosure relevant to this presentation Tasma Harindhanavudhi, MD Division of Diabetes and Endocrinology
Disclosure Glucocorticoid induced osteoporosis: overlooked and undertreated? I have no financial disclosure relevant to this presentation Tasma Harindhanavudhi, MD Division of Diabetes and Endocrinology
Advanced medicine conference. Monday 20 Tuesday 21 June 2016
 Advanced medicine conference Monday 20 Tuesday 21 June 2016 Osteoporosis: recent advances in risk assessment and management Juliet Compston Emeritus Professor of Bone Medicine Cambridge Biomedical Campus
Advanced medicine conference Monday 20 Tuesday 21 June 2016 Osteoporosis: recent advances in risk assessment and management Juliet Compston Emeritus Professor of Bone Medicine Cambridge Biomedical Campus
Osteoporosis: A Tale of 3 Task Forces!
 Osteoporosis: A Tale of 3 Task Forces! Robert A. Adler, MD McGuire Veterans Affairs Medical Center Virginia Commonwealth University Richmond, Virginia, USA Disclosures The opinions are those of the speaker
Osteoporosis: A Tale of 3 Task Forces! Robert A. Adler, MD McGuire Veterans Affairs Medical Center Virginia Commonwealth University Richmond, Virginia, USA Disclosures The opinions are those of the speaker
11/4/2018. Osteoporosis Update. ACP Oregon Chapter November 9 th, 2018 Sarah Hopkins Providence Medical Group Endocrinology East. No disclosures.
 Osteoporosis Update ACP Oregon Chapter November 9 th, 2018 Sarah Hopkins Providence Medical Group Endocrinology East No disclosures. 1 Goals Review screening recommendations and workup of secondary causes
Osteoporosis Update ACP Oregon Chapter November 9 th, 2018 Sarah Hopkins Providence Medical Group Endocrinology East No disclosures. 1 Goals Review screening recommendations and workup of secondary causes
Disclosures. Diagnostic Challenges in Osteoporosis: Whom To Treat 9/25/2014
 Disclosures Diagnostic Challenges in Osteoporosis: Whom To Treat Ethel S. Siris, MD Columbia University Medical Center New York, NY Consultant on scientific issues for: AgNovos Amgen Eli Lilly Merck Novartis
Disclosures Diagnostic Challenges in Osteoporosis: Whom To Treat Ethel S. Siris, MD Columbia University Medical Center New York, NY Consultant on scientific issues for: AgNovos Amgen Eli Lilly Merck Novartis
Division of Nephrology, Bone and Mineral Metabolism
 Osteoporosis and fractures Measurement of bone density Diagnosis of osteoporosis Bone biopsy Newer therapies and challenges Osteoporosis: Definition Normal Bone Osteoporotic Bone NIH Definition:..A skeletal
Osteoporosis and fractures Measurement of bone density Diagnosis of osteoporosis Bone biopsy Newer therapies and challenges Osteoporosis: Definition Normal Bone Osteoporotic Bone NIH Definition:..A skeletal
Dumfries and Galloway. Treatment Protocol for Osteoporosis
 Dumfries and Galloway Treatment Protocol for Osteoporosis DIAGNOSIS OF OSTEOPOROSIS 2 Diagnostic Criteria 2 REFERRAL CRITERIA FOR DEXA 3 TREATMENT 4 Non-Drug Therapy : for all 4 Non-Drug Therapy : in the
Dumfries and Galloway Treatment Protocol for Osteoporosis DIAGNOSIS OF OSTEOPOROSIS 2 Diagnostic Criteria 2 REFERRAL CRITERIA FOR DEXA 3 TREATMENT 4 Non-Drug Therapy : for all 4 Non-Drug Therapy : in the
MEDICAL POLICY MEDICARE ADVANTAGE ONLY (See Product Variations)
") Original Issue Date (Created): 11/1/2010 Most Recent Review Date (Revised): 1/18/2018 Effective Date: 9/1/2018 POLICY PRODUCT VARIATIONS DESCRIPTION/BACKGROUND RATIONALE DEFINITIONS BENEFIT VARIATIONS
Original Issue Date (Created): 11/1/2010 Most Recent Review Date (Revised): 1/18/2018 Effective Date: 9/1/2018 POLICY PRODUCT VARIATIONS DESCRIPTION/BACKGROUND RATIONALE DEFINITIONS BENEFIT VARIATIONS
Because the low bone mass and deterioration
 OSTEOPOROSIS A look at recent expert guidelines and key studies in bone health, the findings of which affect your patients young and old Steven R. Goldstein, MD Dr. Goldstein is Professor of Obstetrics
OSTEOPOROSIS A look at recent expert guidelines and key studies in bone health, the findings of which affect your patients young and old Steven R. Goldstein, MD Dr. Goldstein is Professor of Obstetrics
ACP Colorado-Evidence Based Management of Osteoporosis
 ACP Colorado-Evidence Based Management of Osteoporosis Micol S. Rothman, MD Associate Professor of Medicine and Radiology Clinical Director Metabolic Bone Program University of Colorado School of Medicine
ACP Colorado-Evidence Based Management of Osteoporosis Micol S. Rothman, MD Associate Professor of Medicine and Radiology Clinical Director Metabolic Bone Program University of Colorado School of Medicine
Talking to patients with osteoporosis about initiating therapy
 Talking to patients with osteoporosis about initiating therapy Deborah Sellmeyer, MD Director, Johns Hopkins Metabolic Bone Center Dept of Medicine, Division of Endocrinology Disclosure DSMB member for
Talking to patients with osteoporosis about initiating therapy Deborah Sellmeyer, MD Director, Johns Hopkins Metabolic Bone Center Dept of Medicine, Division of Endocrinology Disclosure DSMB member for
Prevalence of Osteoporosis 5/3/2017. Rhiannon Anderson, PA-C, FLS Linda Mitchell, PA-C, FLS, DEXA Specialist
 Rhiannon Anderson, PA-C, FLS Linda Mitchell, PA-C, FLS, DEXA Specialist Prevalence of Osteoporosis 1.5 million fractures annually in the U.S. Overall lifetime risk for an osteoporotic fracture is about
Rhiannon Anderson, PA-C, FLS Linda Mitchell, PA-C, FLS, DEXA Specialist Prevalence of Osteoporosis 1.5 million fractures annually in the U.S. Overall lifetime risk for an osteoporotic fracture is about
Osteoporosis Physician Performance Measurement Set. October 2006
 American Academy of Family Physicians/American Academy of Orthopaedic Surgeons/American Association of Clinical Endocrinologists/American College of Rheumatology/The Endocrine Society/Physician Consortium
American Academy of Family Physicians/American Academy of Orthopaedic Surgeons/American Association of Clinical Endocrinologists/American College of Rheumatology/The Endocrine Society/Physician Consortium
Chapter 39: Exercise prescription in those with osteoporosis
 Chapter 39: Exercise prescription in those with osteoporosis American College of Sports Medicine. (2010). ACSM's resource manual for guidelines for exercise testing and prescription (6th ed.). New York:
Chapter 39: Exercise prescription in those with osteoporosis American College of Sports Medicine. (2010). ACSM's resource manual for guidelines for exercise testing and prescription (6th ed.). New York: