Part 2: Early detection, assessment and treatment in relation to the new guidelines. Christopher Patterson McMaster University
|
|
|
- Phillip Booth
- 5 years ago
- Views:
Transcription

1 Part 2: Early detection, assessment and treatment in relation to the new guidelines Christopher Patterson McMaster University
2 C. Patterson MD, FRCPC Division of Geriatric Medicine, McMaster University Disclosure: Relationships with commercial interests Grants/Research support: CIHR, Heart & Stroke Foundation Speakers bureaux, honoraria: Alzheimer s Society, Dementia iance Consulting fees: Nil Other: Secretarial support from Hamilton Health Sciences Potential for conflict of interest: Nil Potential for bias: Nil
3 Why did we need another CCCDTD? New definitions and conceptualization of AD Availability of biomarkers (CSF, amyloid and functional MRI neuroimaging) Ethical concerns about clinical use (misuse) of biomarkers Some important therapeutic updates Target audience: non dementologist specialists, FMDs
 CMAJ, Alzheimer s & Dementia Montréal, May 4-5 2012")
 No industry")
4 Building upon 1989 & 1999 cccd Posting background papers to website Comments added on line Voting online Advanced dissemination strategy (specific $) CMAJ, Alzheimer s & Dementia Montréal, May Adherence to AGREE template (21/22 criteria) Use of GRADE evidence classification Ethics consultant and consumer involvement Advanced knowledge translation strategy (DKTN, publications, web based) No industry funding
5 Steering Committee Christopher Patterson (Co-Chair) Serge Gauthier (Co-Chair) Howard Chertkow Michael Gordon (Ethics consultant) Pedro Rosa-Neto Ken Rockwood (CDKTN) Jean-Paul Soucy
6 cccdtd4 addressed the following topics: Definitions Neuroimaging (clinical and research recommendations) Liquid biomarkers Early onset dementia Rapidly progressive dementia Pharmacology update Knowledge translation
7 Theoretical changes of biomarkers in AD Sperling R et al Alz Dement 2011; 7: 280
8 A new lexicon of Alzheimer s Disease (IWG) Dubois B et al. Lancet Neurol 2010; 9: 1118
9 A new lexicon of Alzheimer s Disease (IWG) Dubois B et al. Lancet Neurol 2010; 9: 1118
10 Definitions For We recommend the adoption of the 2011 NIA-AA criteria proposed by the working group for: Dementia Probable and possible AD Core clinical criteria for MCI We recommend the 2011 ASA/AHA recommendations for the diagnosis of VCI
11 Dementia (NIA-AA) is diagnosed when there are cognitive or behavioural symptoms which: 1. Interfere with function at work or usual activities 2. Represent a decline from previous function 3. Are not explained by delirium or major psychiatric disorder 4. Cognitive impairment is detected by: (a) history (person and knowledgeable informant) (b) mental status or bedside neuropsychological testing
12 5. The cognitive or behavioural impairment involves a minimum of 2 of the following domains (a) memory (b) reasoning, handling complex tasks, judgment (c) impaired visuospatial function (d) language (e) changes in personality behaviour or comportment McKhann G et al. Alzheimer s and Dementia 2011; 7: 263


13 Note that: Dementia is a clinical diagnosis Loss of function is central Memory loss is not an essential feature Cognitive scores are an addition to, and not a replacement for complete assessment
14 Alzheimer s disease (probable) NIA-AA Dementia Insidious onset Clear cut history of worsening Initial and prominent cognitive deficits on history and examination in one of: (a) amnestic presentation
15 (b) non amnestic presentation language (PNFA) visuospatial (PCA) executive Not probable AD if: Substantial evidence of cerebrovascular disease Core features of LBD Prominent features of Behavioural variant FTD Prominent features of semantic dementia or PPA Other neurological or non neurological illness or drugs McKhann G et al Alz Dement 2011; 7: 263
16 Vascular Cognitive Impairment: Probable VaD (NIA-AA) Dementia The deficits in ADL are independent of the motor/sensory sequelae of the vascular event. There is no history of gradually progressive cognitive deficits before or after the stroke that suggests the presence of a nonvascular neurodegenerative disorder. Gorelick P et al. Stroke 2011; 42: 2672
17 Vascular Cognitive Impairment: Probable VaD (NIA-AA) There is cognitive impairment and imaging evidence of cerebrovascular disease and (a) There is a clear temporal relationship between a vascular event (e.g. clinical stroke) and onset of cognitive deficits, or (b) There is a clear relationship in the severity and pattern of cognitive impairment and the presence of diffuse, subcortical cerebrovascular disease pathology (e.g. as in CADASIL). Gorelick P et al. Stroke 2011; 42: 2672
18 cccdtd4 did not address: DLB (Parkinsonism, fluctuation, hallucinations, REM sleep disorder, neuroleptic sensitivity) FTD (behaviour-disinhibition, apathy, loss of insight and judgement; language-progessive expressive aphasia) NPH (triad of gait apraxia, incontinence, cognitive deficits)
19 Definitions Research recommendation: We recommend the IWG definition of asymptomatic at-risk for AD states for research purpose. We recommend reassessment of the utility of the concept of prodromal AD in the future when AD-PP biomarkers are available, validated, and ready for use in Canada.

20 Neuroimaging
21 Neuroimaging - Structural imaging: CT & MRI For the assessment of a person with cognitive impairment, at least one structural imaging procedure (CT or MRI of the brain) is recommended to establish the presence of clinically unsuspected cerebrovascular disease and to rule out potentially reversible structural etiologies. (Grade 1B) For 26% 74% Against We suggest that a head MRI is preferred when a radiologist/neuroradiologist and/or a cognitive specialist (neurologist, geriatrician, or geriatric psychiatrist) can interpret patterns of atrophy and other features that may provide added diagnostic and predictive value as deemed appropriate by the specialist. (Grade 2B) 90% 10%
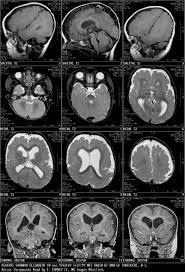
22 NPH Gross ventricular dilatation, little atrophy Alzheimer s disease atrophy, especially hippocampi

23 NPH Gross ventricular dilatation, little atrophy Alzheimer s disease atrophy, especially hippocampi
24 Neuroimaging - Structural imaging: CT & MRI Standardization of clinical acquisition of core MRI dementia sequences is recommended in Canadian centres that have radiologists and cognitive specialists with expertise in assessing cognitive disorders, particularly when repeat MRI images can provide additional diagnostic, prognostic and safety information. (Grade 1B). For Against We suggest that when available in the clinic, cognition specialists may use the computer images of the brain to educate a person with cognitive impairment and family members about changes in the brain. This knowledge may reinforce adherence to vascular risk factor management and to lifestyle modification to improve brain health. (Grade 2C). 73.3% 26.7%
25 Neuroimaging New indication for structural imaging: CT & MRI In addition to previously listed indications for structural imaging, a CT or MRI should done in the assessment of a person with cognitive impairment if the presence of unsuspected cerebrovascular disease would change the clinical management. For
 Florbetapir now approved by")
26 Amyloid Imaging with PiB (Pittsburg compound B) Florbetapir now approved by FDA
27 Definitions Given that the presence of brain amyloid in normal people is of uncertain significance, the CCCD discourages the use of amyloid imaging in individuals without memory loss, outside of the research setting. For The medical community should be clear in its discussions with patients, the media and the general population that presence of brain amyloid in normal people is of unclear significance at the present time.
28 Neuroimaging - Amyloid Imaging For At present, there is no clinical indication for amyloid imaging in cognitively normal individuals, initial investigation of cognitive complaints, differentiating AD from other Aβ - associated dementia (e.g. DLB, CAA), differentiating between AD clinical variants (e.g. classic amnestic AD vs. PCA or lvppa), and differentiating between non-ad causes of dementia (e.g. molecular subtypes of FTLD).
29 Neuroimaging - Amyloid Imaging Should this technique become available to Canadian clinicians in the future, we recommend against its use in cognitively normal individuals or initial investigation of cognitive complaints (Grade 1B). When faced with amyloid test results obtained outside Canada, physicians should be very cautious in their interpretation, i.e. used in isolation this test cannot diagnose AD, MCI, or differentiate normal from abnormal aging, and we recommend they consult with a dementia specialist familiar with this technique. For
30 Neuroimaging - Amyloid Imaging For Amyloid imaging is not currently approved in Canada. Should amyloid imaging become available in Canadian clinicians in the future, it must not be considered a routine test and we recommend it as an adjunct to a comprehensive evaluation for complex atypical presentations in referral to tertiary care Memory Clinics when a more accurate clinical diagnosis is needed (Grade 1B).
31 Neuroimaging PET & SPECT For a patient with a diagnosis of dementia who has undergone the recommended baseline clinical and structural brain imaging evaluation and who has been evaluated by a dementia specialist but whose underlying pathological process is still unclear, preventing adequate clinical management, we recommend that the specialist obtain a 18F- FDG PET scan for differential diagnosis purposes (Grade 1B). For For a patient with a diagnosis of dementia who has undergone the recommended baseline clinical and structural brain imaging evaluation and who has been evaluated by a dementia specialist but whose underlying pathological process is still unclear, preventing adequate clinical management, and who cannot be practically referred for an 18F-FDG PET scan, we recommend that a SPECT rcbf study be performed for differential diagnosis purposes (Grade 2C).
32 Liquid Biomarkers For Against Plasma Ab1-42 Ab1-42 levels are not recommended for clinical practice. Measures of CSF Ab1-42, total tau and phosphorylated tau at ser 181 are recommended for the biomarker workup of patients with atypical dementia. Measures of CSF Ab1-42, total tau and phosphorylated tau at ser 181 should be collected following a specific protocol and the quantification must be carried out by an experienced lab with a validated technology and continuous participation in quality control programs. 64.3% 35.7% 71.4% 28.6%
33 Early Onset Dementia For patients with early onset dementia should be referred to a memory clinic, preferably one with access to genetic counselling and testing when appropriate. The cost of genetic counseling and testing should be covered by public funding. Physicians should be sensitive to the special issues associated with early onset dementia, particularly in regard to loss of employment and access to support services appropriate for that age group.
34 Early Onset Dementia Research recommendations For Against Considering the rarity of early onset dementia, a national registry for interested at risk individuals, mutation carriers and symptomatic patients will facilitate therapeutic research. Health Policy recommendation: 88.9% 11.1% 83.3% 16.7% This registry should be supported by public funding.
35 Rapidly Progressive Dementia It is suggested that RPD be defined as a dementia which develops within 12 months after the appearance of first cognitive symptoms. (Grade 2C) For Against 94.1% 5.9% It is suggested that individuals suspected of RPD be referred to physicians who are experienced and have access to the diagnostic facilities able to mount an organized and comprehensive diagnostic procedure (Grade 2C) 94.1% 5.9% After exclusion of delirium and evident underlying causes of RPD, it is suggested that a diagnostic strategy for RPD be based of the prevalence of causes of RPD in case series. (Grade 2B)
36 Rapidly Progressive Dementia The diagnostic strategy should emphasize the detection of potentially curable conditions, such as infections, immune mediated and toxic metabolic causes. Table 6 outlines such an approach (Grade 2B) For Against For individuals with AD, it is suggested that a decline of 3 or more points on the MMSE in 6 months, which identifies a group with a worse prognosis, is a signal to explore comorbid conditions and review pharmacological management (Grade 2B) 94.1% 5.9%

37 Update on Pharmacological Treatment
38 Update on Pharmacological Treatment Many cases of dementia have more than one condition contributing to causation. Most commonly this will be a combination of Alzheimer s disease with other brain pathology. We recommend that management be based on what is (are) felt to be the predominant contributing cause(s). (Grade 1B) We recommend cholinesterase inhibitors as a treatment option for Alzheimer s disease with cerebrovascular disease. (Grade 1B) For
39 Update on Pharmacological Treatment Cholinesterase inhibitors are recommended as a treatment option for dementia associated with Parkinson s disease. (Grade 1A) For There is insufficient and inconsistent evidence on which to make a recommendation either for or against the use of the currently available cholinesterase inhibitors for the treatment of probable or possible vascular dementia. (Grade 2B) three cholinesterase inhibitors have demonstrated efficacy for mild to severe AD. We recommend a trial of a ChEI for most patients with AD. (Grade1A)
40 Update on Pharmacological Treatment Direct comparisons do not suggest differences between cholinesterase inhibitors (Grade 2B). Selection of agent will be based on adverse effect profile, ease of use, familiarity, and differences between the agents in their pharmacokinetics and other mechanisms of action. For Against 94.1% 5.9% Combination therapy of a cholinesterase inhibitor and memantine is rational (as the medications have different mechanisms of action) and appears to be safe, but there is insufficient evidence to recommend for or against this combination (Grade 2B)
41 DOMINO study: donepezil and memantine in mod/severe AD Howard R et al. N. Engl J Med 2012; 366: 892
42 Update on Pharmacological Treatment Discontinuing cholinesterase inhibitors in patients with moderate to severe Alzheimer s disease may lead to worse cognitive function and greater functional impairment as compared to continued therapy (Level 2B). This must be balanced with the risk for known side-effects and drug costs if therapy continues. It is suggested that cholinesterase inhibitors be discontinued when: a) The patient and/or their proxy decision maker decide to stop after being appraised of the risks and benefits of continuation and discontinuation b) The patient is sufficiently non-adherent with the medication that continued prescription of it would be useless, and it is not possible to establish a system for the administration of the medication to rectify the problem; c) The patient s rate of cognitive, functional, and/or behavioural decline is greater on treatment compared to that prior to being treated; d) The patient experiences intolerable side effects that are definitely or probably related to the cholinesterase inhibitor; e) The comorbidities of the patient make continued use of the agent either unacceptably risky or futile (e.g., terminally ill); or, f) The patient's dementia progresses to a stage (e.g., Global Deterioration Scale stage 7) where there would be no clinically meaningful benefit from continued therapy. Continued Next slide
43 Update on Pharmacological Treatment When a decision has been made to discontinue therapy because of a perceived lack of effectiveness, it is suggested that the dose be tapered before stopping the agent and that the patient be monitored over the next 1-3 months for evidence of an observable decline. If this occurs, it is suggested that consideration be given to reinstating therapy. (Level 2C) For % Against If the patient had an inadequate response to non pharmacological interventions or has a major affective disorder, severe dysthymia, or severe emotional lability, we recommend that a trial of an antidepressant could be considered. (Grade 2A) %
44 Update on Pharmacological Treatment Based on good evidence we recommend that valproate should not be used for agitation and aggression in AD (Grade 1A) There is no good evidence to recommend for or against the use of cholinesterase inhibitors and/or memantine for the treatment of neuropsychiatric symptoms as a primary indication (Grade 2B) For
45 Update on Pharmacological Treatment For We suggest that Risperidone, olanzapine and aripiprazole be used for severe agitation, aggression and psychosis associated with dementia where there is risk of harm to the patient and/or others. The potential benefit of all antipsychotics must be weighed against the significant risks such as cerebrovascular adverse events and mortality. (Grade 2A)
46 Update on Pharmacological Treatment There is insufficient evidence to recommend for or against the use of quetiapine in the management of severe agitation, aggression and psychosis associated with dementia (Grade 2B) For There is insufficient evidence to recommend for or against the use of SSRIs or trazodone in the management of agitated patients. (Grade 2B)
47 Summary Emergence of CSF and neuroimaging biomarkers have prompted new recommendations for clinical practice Clinical definitions are little changed Few new pharmacological recommendations (valproate, memantine) EOD and RPD recommendations Extensive research agenda
:")
48 Can Geriatr J 2012; 15(4): 120-6
Disclosure Statement
 Recommendations on MCI from the Third and Fourth Canadian Consensus Conferences on Diagnosis and Therapy of Dementia/ Quatrieme Conférence Canadienne Consensuelle sur la Démence 2012. Dr. Howard Chertkow
Recommendations on MCI from the Third and Fourth Canadian Consensus Conferences on Diagnosis and Therapy of Dementia/ Quatrieme Conférence Canadienne Consensuelle sur la Démence 2012. Dr. Howard Chertkow
Recommendations for the Diagnosis and Treatment of Dementia 2012
 Recommendations for the Diagnosis and Treatment of Dementia 2012 Based on the Canadian Consensus Conference on the Diagnosis and Treatment of Dementia (CCCDTD4) 2012 Gauthier S, Patterson C, Chertkow H,
Recommendations for the Diagnosis and Treatment of Dementia 2012 Based on the Canadian Consensus Conference on the Diagnosis and Treatment of Dementia (CCCDTD4) 2012 Gauthier S, Patterson C, Chertkow H,
Recommendations for the Diagnosis and Treatment of Dementia 2012
 Recommendations for the Diagnosis and Treatment of Dementia 2012 Based on the Canadian Consensus Conference on the Diagnosis and Treatment of Dementia (4 th CCCDTD) 2012 Gauthier S, Patterson C, Chertkow
Recommendations for the Diagnosis and Treatment of Dementia 2012 Based on the Canadian Consensus Conference on the Diagnosis and Treatment of Dementia (4 th CCCDTD) 2012 Gauthier S, Patterson C, Chertkow
Form D1: Clinician Diagnosis
 Initial Visit Packet Form D: Clinician Diagnosis NACC Uniform Data Set (UDS) ADC name: Subject ID: Form date: / / Visit #: Examiner s initials: INSTRUCTIONS: This form is to be completed by the clinician.
Initial Visit Packet Form D: Clinician Diagnosis NACC Uniform Data Set (UDS) ADC name: Subject ID: Form date: / / Visit #: Examiner s initials: INSTRUCTIONS: This form is to be completed by the clinician.
Comments to this discussion are invited on the Alzforum Webinar page. Who Should Use the New Diagnostic Guidelines? The Debate Continues
 Comments to this discussion are invited on the Alzforum Webinar page. Who Should Use the New Diagnostic s? The Debate Continues Ever since new criteria came out for a research diagnosis of prodromal/preclinical
Comments to this discussion are invited on the Alzforum Webinar page. Who Should Use the New Diagnostic s? The Debate Continues Ever since new criteria came out for a research diagnosis of prodromal/preclinical
Diagnosis and Treatment of Alzhiemer s Disease
 Diagnosis and Treatment of Alzhiemer s Disease Roy Yaari, MD, MAS Director, Memory Disorders Clinic, Banner Alzheimer s Institute 602-839-6900 Outline Introduction Alzheimer s disease (AD)Guidelines -revised
Diagnosis and Treatment of Alzhiemer s Disease Roy Yaari, MD, MAS Director, Memory Disorders Clinic, Banner Alzheimer s Institute 602-839-6900 Outline Introduction Alzheimer s disease (AD)Guidelines -revised
Introduction, use of imaging and current guidelines. John O Brien Professor of Old Age Psychiatry University of Cambridge
 Introduction, use of imaging and current guidelines John O Brien Professor of Old Age Psychiatry University of Cambridge Why do we undertake brain imaging in AD and other dementias? Exclude other causes
Introduction, use of imaging and current guidelines John O Brien Professor of Old Age Psychiatry University of Cambridge Why do we undertake brain imaging in AD and other dementias? Exclude other causes
Dementia Update. October 1, 2013 Dylan Wint, M.D. Cleveland Clinic Lou Ruvo Center for Brain Health Las Vegas, Nevada
 Dementia Update October 1, 2013 Dylan Wint, M.D. Cleveland Clinic Lou Ruvo Center for Brain Health Las Vegas, Nevada Outline New concepts in Alzheimer disease Biomarkers and in vivo diagnosis Future trends
Dementia Update October 1, 2013 Dylan Wint, M.D. Cleveland Clinic Lou Ruvo Center for Brain Health Las Vegas, Nevada Outline New concepts in Alzheimer disease Biomarkers and in vivo diagnosis Future trends
Moving Targets: An Update on Diagnosing Dementia in the Clinic
 Moving Targets: An Update on Diagnosing Dementia in the Clinic Eric McDade DO Department of Neurology School of Medicine Alzheimer Disease Research Center Disclosures No relevant financial disclosures
Moving Targets: An Update on Diagnosing Dementia in the Clinic Eric McDade DO Department of Neurology School of Medicine Alzheimer Disease Research Center Disclosures No relevant financial disclosures
Assessing and Managing the Patient with Cognitive Decline
 Assessing and Managing the Patient with Cognitive Decline Center of Excellence For Alzheimer s Disease for State of NY Capital Region Alzheimer s Center of Albany Medical Center Earl A. Zimmerman, MD Professor
Assessing and Managing the Patient with Cognitive Decline Center of Excellence For Alzheimer s Disease for State of NY Capital Region Alzheimer s Center of Albany Medical Center Earl A. Zimmerman, MD Professor
Mild Cognitive Impairment (MCI)
") October 19, 2018 Mild Cognitive Impairment (MCI) Yonas E. Geda, MD, MSc Professor of Neurology and Psychiatry Consultant, Departments of Psychiatry & Psychology, and Neurology Mayo Clinic College of Medicine
October 19, 2018 Mild Cognitive Impairment (MCI) Yonas E. Geda, MD, MSc Professor of Neurology and Psychiatry Consultant, Departments of Psychiatry & Psychology, and Neurology Mayo Clinic College of Medicine
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017.
 DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
DISCLOSURES. Objectives. THE EPIDEMIC of 21 st Century. Clinical Assessment of Cognition: New & Emerging Tools for Diagnosing Dementia NONE TO REPORT
 Clinical Assessment of Cognition: New & Emerging Tools for Diagnosing Dementia DISCLOSURES NONE TO REPORT Freddi Segal Gidan, PA, PhD USC Keck School of Medicine Rancho/USC California Alzheimers Disease
Clinical Assessment of Cognition: New & Emerging Tools for Diagnosing Dementia DISCLOSURES NONE TO REPORT Freddi Segal Gidan, PA, PhD USC Keck School of Medicine Rancho/USC California Alzheimers Disease
September 26 28, 2013 Westin Tampa Harbour Island. Co-sponsored by
 September 26 28, 2013 Westin Tampa Harbour Island Co-sponsored by From Brains at Risk to Cognitive Dysfunction: The Role of Vascular Pathology Ralph Sacco, MD, MS, FAHA, FAAN Miller School of Medicine
September 26 28, 2013 Westin Tampa Harbour Island Co-sponsored by From Brains at Risk to Cognitive Dysfunction: The Role of Vascular Pathology Ralph Sacco, MD, MS, FAHA, FAAN Miller School of Medicine
Regulatory Challenges across Dementia Subtypes European View
 Regulatory Challenges across Dementia Subtypes European View Population definition including Early disease at risk Endpoints in POC studies Endpoints in pivotal trials 1 Disclaimer No CoI The opinions
Regulatory Challenges across Dementia Subtypes European View Population definition including Early disease at risk Endpoints in POC studies Endpoints in pivotal trials 1 Disclaimer No CoI The opinions
Appendix 2 (continued): Recommendations for the management of mild to moderate dementia, dementia with a cerebrovascular component, and for addressing
: Recommendations for the management of mild to moderate dementia, dementia with a cerebrovascular component, and for addressing") a cerebrovascular component, and for addressing ethical issues in dementia (page 1 of 7) Mild to moderate dementia 1. Most patients with dementia can be assessed and managed adequately by their primary
a cerebrovascular component, and for addressing ethical issues in dementia (page 1 of 7) Mild to moderate dementia 1. Most patients with dementia can be assessed and managed adequately by their primary
Dementia Update. Daniel Drubach, M.D. Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota
 Dementia Update Daniel Drubach, M.D. Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota Nothing to disclose Dementia Progressive deterioration in mental function
Dementia Update Daniel Drubach, M.D. Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota Nothing to disclose Dementia Progressive deterioration in mental function
Prof Tim Anderson. Neurologist University of Otago Christchurch
 Prof Tim Anderson Neurologist University of Otago Christchurch Tim Anderson Christchurch Insidious cognitive loss From subjective memory complaints (SMC) to dementia Case 1. AR. 64 yrs Male GP referral
Prof Tim Anderson Neurologist University of Otago Christchurch Tim Anderson Christchurch Insidious cognitive loss From subjective memory complaints (SMC) to dementia Case 1. AR. 64 yrs Male GP referral
Dementia Diagnosis Guidelines Primary Care
 Dementia Diagnosis Guidelines Primary Care Dementia Diagnosis Primary Care Guidelines Introduction Dementia is a long term condition, which primarily affects people over the age of 65 (late on-set dementia)
Dementia Diagnosis Guidelines Primary Care Dementia Diagnosis Primary Care Guidelines Introduction Dementia is a long term condition, which primarily affects people over the age of 65 (late on-set dementia)
Non Alzheimer Dementias
 Non Alzheimer Dementias Randolph B Schiffer Department of Neuropsychiatry and Behavioral Science Texas Tech University Health Sciences Center 9/11/2007 Statement of Financial Disclosure Randolph B Schiffer,,
Non Alzheimer Dementias Randolph B Schiffer Department of Neuropsychiatry and Behavioral Science Texas Tech University Health Sciences Center 9/11/2007 Statement of Financial Disclosure Randolph B Schiffer,,
Dementia Past, Present and Future
 Dementia Past, Present and Future Morris Freedman MD, FRCPC Division of Neurology Baycrest and University of Toronto Rotman Research Institute, Baycrest CNSF 2015 Objectives By the end of this presentation,
Dementia Past, Present and Future Morris Freedman MD, FRCPC Division of Neurology Baycrest and University of Toronto Rotman Research Institute, Baycrest CNSF 2015 Objectives By the end of this presentation,
Neurocognitive Disorders Research to Emerging Therapies
 Neurocognitive Disorders Research to Emerging Therapies Edward Huey, MD Assistant Professor of Psychiatry and Neurology The Taub Institute for Research on Alzheimer s Disease and the Aging Brain Columbia
Neurocognitive Disorders Research to Emerging Therapies Edward Huey, MD Assistant Professor of Psychiatry and Neurology The Taub Institute for Research on Alzheimer s Disease and the Aging Brain Columbia
Personal Reflections on the Design and Delivery of Services to Those with Cognitive Disorders
 Personal Reflections on the Design and Delivery of Services to Those with Cognitive Disorders Dr. David B. Hogan Brenda Strafford Foundation Chair in Geriatric Medicine University of Calgary None to declare
Personal Reflections on the Design and Delivery of Services to Those with Cognitive Disorders Dr. David B. Hogan Brenda Strafford Foundation Chair in Geriatric Medicine University of Calgary None to declare
Approach to Cognitive Disorders in Primary Care
 Approach to Cognitive Disorders in Primary Care What can reasonably be done in an office visit? What about screening for cognitive disorders? USPSTF (2014) doesn t recommend screening: magnitude of clinically
Approach to Cognitive Disorders in Primary Care What can reasonably be done in an office visit? What about screening for cognitive disorders? USPSTF (2014) doesn t recommend screening: magnitude of clinically
BEHAVIOURAL AND PSYCHOLOGICAL SYMPTOMS IN DEMENTIA
 BEHAVIOURAL AND PSYCHOLOGICAL SYMPTOMS IN DEMENTIA Unmet needs What might be your behavioural response to this experience? Content Definition What are BPSD? Prevalence How common are they? Aetiological
BEHAVIOURAL AND PSYCHOLOGICAL SYMPTOMS IN DEMENTIA Unmet needs What might be your behavioural response to this experience? Content Definition What are BPSD? Prevalence How common are they? Aetiological
Objectives. Objectives continued: 3/24/2012. Copyright Do not distribute or replicate without permission 1
 Frontotemporal Degeneration and Primary Progressive Aphasia Caregiver and Professional Education Conference Diana R. Kerwin, MD Assistant Professor of Medicine-Geriatrics Cognitive Neurology and Alzheimer
Frontotemporal Degeneration and Primary Progressive Aphasia Caregiver and Professional Education Conference Diana R. Kerwin, MD Assistant Professor of Medicine-Geriatrics Cognitive Neurology and Alzheimer
Early Onset Dementia From the background to the foreground
 Early Onset Dementia From the background to the foreground Dr Jeremy Isaacs Consultant Neurologist St George s Hospital Excellence in specialist and community healthcare Themes of my talk The early onset
Early Onset Dementia From the background to the foreground Dr Jeremy Isaacs Consultant Neurologist St George s Hospital Excellence in specialist and community healthcare Themes of my talk The early onset
Dementia: It s Not Always Alzheimer s
 Dementia: It s Not Always Alzheimer s A Caregiver s Perspective Diane E. Vance, Ph.D. Mid-America Institute on Aging and Wellness 2017 My Background Caregiver for my husband who had Lewy Body Dementia
Dementia: It s Not Always Alzheimer s A Caregiver s Perspective Diane E. Vance, Ph.D. Mid-America Institute on Aging and Wellness 2017 My Background Caregiver for my husband who had Lewy Body Dementia
MOVEMENT DISORDERS AND DEMENTIA
 MOVEMENT DISORDERS AND DEMENTIA FOCUS ON DEMENTIA WITH LEWY BODIES MADHAVI THOMAS MD NORTH TEXAS MOVEMENT DISORDERS INSTITUTE, INC DEMENTIA de men tia dəˈmen(t)sh(ē)ə/ nounmedicine noun: dementia a chronic
MOVEMENT DISORDERS AND DEMENTIA FOCUS ON DEMENTIA WITH LEWY BODIES MADHAVI THOMAS MD NORTH TEXAS MOVEMENT DISORDERS INSTITUTE, INC DEMENTIA de men tia dəˈmen(t)sh(ē)ə/ nounmedicine noun: dementia a chronic
Dementia and Delirium: A Neurologist s Approach to Altered Mental Status. Case 1 4/7/11. Which of the following evaluations is your next step?
 Dementia and Delirium: A Neurologist s Approach to Altered Mental Status S. Andrew Josephson, MD Director, Neurohospitalist Program Medical Director, Inpatient Neurology University of California San Francisco
Dementia and Delirium: A Neurologist s Approach to Altered Mental Status S. Andrew Josephson, MD Director, Neurohospitalist Program Medical Director, Inpatient Neurology University of California San Francisco
SHARED CARE OF MCI/EARLY DEMENTIA
 SHARED CARE OF MCI/EARLY DEMENTIA BY DR. OLUFEMI BANJO MD, DTM, DCP, DIPA&DS, DHM, M.Med.Sc, FRCP(C) GERIATRIC PSYCHIATRIST. ASSISTANT MEDICAL DIRECTOR, ADULT MENTAL HEALTH AND ADDICTION, GRAND RIVER HOSPITAL
SHARED CARE OF MCI/EARLY DEMENTIA BY DR. OLUFEMI BANJO MD, DTM, DCP, DIPA&DS, DHM, M.Med.Sc, FRCP(C) GERIATRIC PSYCHIATRIST. ASSISTANT MEDICAL DIRECTOR, ADULT MENTAL HEALTH AND ADDICTION, GRAND RIVER HOSPITAL
New diagnostic criteria for Alzheimer s disease and mild cognitive impairment for the practical neurologist
 New diagnostic criteria for Alzheimer s disease and mild cognitive impairment for the practical neurologist Andrew E Budson, 1,2 Paul R Solomon 2,3 1 Center for Translational Cognitive Neuroscience, VA
New diagnostic criteria for Alzheimer s disease and mild cognitive impairment for the practical neurologist Andrew E Budson, 1,2 Paul R Solomon 2,3 1 Center for Translational Cognitive Neuroscience, VA
Improving diagnosis of Alzheimer s disease and lewy body dementia. Brain TLC October 2018
 Improving diagnosis of Alzheimer s disease and lewy body dementia Brain TLC October 2018 Plan for this discussion: Introduction to AD and LBD Why do we need to improve diagnosis? What progress has been
Improving diagnosis of Alzheimer s disease and lewy body dementia Brain TLC October 2018 Plan for this discussion: Introduction to AD and LBD Why do we need to improve diagnosis? What progress has been
Dementia: How to explain the diagnosis to patients and relatives
 GPHot Topics (April 2017): Dementia: How to explain the diagnosis to patients and relatives mohammad somauroo Consultant Physician with specialist interest in Community Geriatrics Royal Liverpool and Broadgreen
GPHot Topics (April 2017): Dementia: How to explain the diagnosis to patients and relatives mohammad somauroo Consultant Physician with specialist interest in Community Geriatrics Royal Liverpool and Broadgreen
Mild Cognitive Impairment
 Mild Cognitive Impairment The Role of the Family Physicians McGill Refresher Course December 2018 Fadi Massoud MD FRCPC, Internist-Geriatrician Centre Hospitalier Charles LeMoyne & Institut Universitaire
Mild Cognitive Impairment The Role of the Family Physicians McGill Refresher Course December 2018 Fadi Massoud MD FRCPC, Internist-Geriatrician Centre Hospitalier Charles LeMoyne & Institut Universitaire
Brain imaging for the diagnosis of people with suspected dementia
 Why do we undertake brain imaging in dementia? Brain imaging for the diagnosis of people with suspected dementia Not just because guidelines tell us to! Exclude other causes for dementia Help confirm diagnosis
Why do we undertake brain imaging in dementia? Brain imaging for the diagnosis of people with suspected dementia Not just because guidelines tell us to! Exclude other causes for dementia Help confirm diagnosis
Neuroimaging for dementia diagnosis. Guidance from the London Dementia Clinical Network
 Neuroimaging for dementia diagnosis Guidance from the London Dementia Clinical Network Authors Dr Stephen Orleans-Foli Consultant Psychiatrist, West London Mental Health NHS Trust Dr Jeremy Isaacs Consultant
Neuroimaging for dementia diagnosis Guidance from the London Dementia Clinical Network Authors Dr Stephen Orleans-Foli Consultant Psychiatrist, West London Mental Health NHS Trust Dr Jeremy Isaacs Consultant
Psychiatric and Behavioral Symptoms in Alzheimer s and Other Dementias. Aaron H. Kaufman, MD
 Psychiatric and Behavioral Symptoms in Alzheimer s and Other Dementias Aaron H. Kaufman, MD Psychiatric and Behavioral Symptoms in Alzheimer s and Other Dementias Aaron H. Kaufman, M.D. Health Sciences
Psychiatric and Behavioral Symptoms in Alzheimer s and Other Dementias Aaron H. Kaufman, MD Psychiatric and Behavioral Symptoms in Alzheimer s and Other Dementias Aaron H. Kaufman, M.D. Health Sciences
FRONTOTEMPORAL DEGENERATION: OVERVIEW, TRENDS AND DEVELOPMENTS
 FRONTOTEMPORAL DEGENERATION: OVERVIEW, TRENDS AND DEVELOPMENTS Norman L. Foster, M.D. Director, Center for Alzheimer s Care, Imaging and Research Chief, Division of Cognitive Neurology, Department of Neurology
FRONTOTEMPORAL DEGENERATION: OVERVIEW, TRENDS AND DEVELOPMENTS Norman L. Foster, M.D. Director, Center for Alzheimer s Care, Imaging and Research Chief, Division of Cognitive Neurology, Department of Neurology
Assessment at the bedside or in the clinic using the history, examination and laboratory tests to distinguish between different types of dementia
 Assessment at the bedside or in the clinic using the history, examination and laboratory tests to distinguish between different types of dementia AP Passmore Content Common dementia syndromes (older people)
Assessment at the bedside or in the clinic using the history, examination and laboratory tests to distinguish between different types of dementia AP Passmore Content Common dementia syndromes (older people)
Clinical Diagnosis. Step 1: Dementia or not? Diagnostic criteria for dementia (DSM-IV)
") Step 1: Dementia or not? Diagnostic criteria for dementia (DSM-IV) A. The development of multiple cognitive deficits manifested by both 1 and 2 1 1. Memory impairment 2. One (or more) of the following
Step 1: Dementia or not? Diagnostic criteria for dementia (DSM-IV) A. The development of multiple cognitive deficits manifested by both 1 and 2 1 1. Memory impairment 2. One (or more) of the following
DRUG THERAPY CHOICES FOR THE DEMENTED PATIENT Past, Present and Future
 DRUG THERAPY CHOICES FOR THE DEMENTED PATIENT Past, Present and Future Daniel S. Sitar Professor Emeritus University of Manitoba Email: Daniel.Sitar@umanitoba.ca March 6, 2018 INTRODUCTION EPIDEMIOLOGY
DRUG THERAPY CHOICES FOR THE DEMENTED PATIENT Past, Present and Future Daniel S. Sitar Professor Emeritus University of Manitoba Email: Daniel.Sitar@umanitoba.ca March 6, 2018 INTRODUCTION EPIDEMIOLOGY
Disclosure. Speaker Bureaus. Grant Support. Pfizer Forest Norvartis. Pan American Health Organization/WHO NIA HRSA
 Disclosure Speaker Bureaus Pfizer Forest Norvartis Grant Support Pan American Health Organization/WHO NIA HRSA How Common is Psychosis in Alzheimer s Disease? Review of 55 studies 41% of those with Alzheimer
Disclosure Speaker Bureaus Pfizer Forest Norvartis Grant Support Pan American Health Organization/WHO NIA HRSA How Common is Psychosis in Alzheimer s Disease? Review of 55 studies 41% of those with Alzheimer
DEMENTIA, THE BRAIN AND HOW IT WORKS AND WHY YOU MATTER
 OVERCOMING THE CHALLENGES OF MANAGING CHRONIC DISEASES IN PERSONS WITH DEMENTIA DEMENTIA, THE BRAIN AND HOW IT WORKS AND WHY YOU MATTER LEARNING OBJECTIVES Be familiar with the diagnostic criteria for
OVERCOMING THE CHALLENGES OF MANAGING CHRONIC DISEASES IN PERSONS WITH DEMENTIA DEMENTIA, THE BRAIN AND HOW IT WORKS AND WHY YOU MATTER LEARNING OBJECTIVES Be familiar with the diagnostic criteria for
Diagnosis before NIA AA The impact of FDG PET in. Diagnosis after NIA AA Neuropathology and PET image 2015/10/16
 The impact of FDG PET in degenerative dementia diagnosis Jung Lung, Hsu MD, Ph.D (Utrecht) Section of dementia and cognitive impairment Department of Neurology Chang Gung Memorial Hospital, Linkou, Taipei
The impact of FDG PET in degenerative dementia diagnosis Jung Lung, Hsu MD, Ph.D (Utrecht) Section of dementia and cognitive impairment Department of Neurology Chang Gung Memorial Hospital, Linkou, Taipei
3/7/2017. Alzheimer s and Dementia Research: An Advanced Discussion. Alzheimer s and Dementia Research: An Advanced Discussion
 Alzheimer s and Dementia Research: An Advanced Discussion Brad Boeve, MD Department of Neurology Mayo Clinic Alzheimer s and Dementia Research: An Advanced Discussion Theoretical Constructs in Aging/Dementia
Alzheimer s and Dementia Research: An Advanced Discussion Brad Boeve, MD Department of Neurology Mayo Clinic Alzheimer s and Dementia Research: An Advanced Discussion Theoretical Constructs in Aging/Dementia
DEMENTIA AND MEDICATION
 DEMENTIA AND MEDICATION Dr. Siobhan Ni Bhriain, MRCP, MRCPsych. Clinical Director, Tallaght and SJH MHS, Consultant Old Age Psychiatrist, Chair, DSIDC Steering Committee. SUMMARY OF TODAY S TALK Dementia-definition,
DEMENTIA AND MEDICATION Dr. Siobhan Ni Bhriain, MRCP, MRCPsych. Clinical Director, Tallaght and SJH MHS, Consultant Old Age Psychiatrist, Chair, DSIDC Steering Committee. SUMMARY OF TODAY S TALK Dementia-definition,
What if it s not Alzheimer s? Update on Lewy body dementia and frontotemporal dementia
 What if it s not Alzheimer s? Update on Lewy body dementia and frontotemporal dementia Dementia: broad term for any acquired brain condition impairing mental function such that ADLs are impaired. Includes:
What if it s not Alzheimer s? Update on Lewy body dementia and frontotemporal dementia Dementia: broad term for any acquired brain condition impairing mental function such that ADLs are impaired. Includes:
GERIATRIC MENTAL HEALTH AND MEDICATION TREATMENT
 Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences GERIATRIC MENTAL HEALTH AND MEDICATION TREATMENT RUTH KOHEN ASSOCIATE PROFESSOR UW DEPARTMENT OF PSYCHIATRY 5-4-2017
Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences GERIATRIC MENTAL HEALTH AND MEDICATION TREATMENT RUTH KOHEN ASSOCIATE PROFESSOR UW DEPARTMENT OF PSYCHIATRY 5-4-2017
Evaluations. Alzheimer s Disease A Public Health Response. Viewer Call-In. July 19, Guest Speakers. Thanks to our Sponsors:
 Alzheimer s Disease A Public Health Response July 19, 2007 1 2 Guest Speakers Thanks to our Sponsors: Earl A. Zimmerman, M.D. Bender Endowed Chair of Neurology and Director of the Alzheimer s Center at
Alzheimer s Disease A Public Health Response July 19, 2007 1 2 Guest Speakers Thanks to our Sponsors: Earl A. Zimmerman, M.D. Bender Endowed Chair of Neurology and Director of the Alzheimer s Center at
Optimal Management of Challenging Behaviours in Dementia: An Update on Pharmacologic and Non-Pharmacologic Approaches
 Optimal Management of Challenging Behaviours in Dementia: An Update on Pharmacologic and Non-Pharmacologic Approaches Andrea Iaboni, MD, DPhil, FRCPC Toronto Rehab Institute, UHN Learning objectives Recognize
Optimal Management of Challenging Behaviours in Dementia: An Update on Pharmacologic and Non-Pharmacologic Approaches Andrea Iaboni, MD, DPhil, FRCPC Toronto Rehab Institute, UHN Learning objectives Recognize
I have no relevant financial disclosures
 1 ADVANCED INSIGHTS INTO THE PREVENTION, TREATMENT AND MANAGEMENT OF ALZHEIMER S DISEASE Naushira Pandya, MD, CMD, FACP Professor and Chair, Department of Geriatrics Director, Geriatrics Education Center
1 ADVANCED INSIGHTS INTO THE PREVENTION, TREATMENT AND MANAGEMENT OF ALZHEIMER S DISEASE Naushira Pandya, MD, CMD, FACP Professor and Chair, Department of Geriatrics Director, Geriatrics Education Center
Neuro degenerative PET image from FDG, amyloid to Tau
 Neuro degenerative PET image from FDG, amyloid to Tau Kun Ju Lin ( ) MD, Ph.D Department of Nuclear Medicine and Molecular Imaging Center, Chang Gung Memorial Hospital ( ) Department of Medical Imaging
Neuro degenerative PET image from FDG, amyloid to Tau Kun Ju Lin ( ) MD, Ph.D Department of Nuclear Medicine and Molecular Imaging Center, Chang Gung Memorial Hospital ( ) Department of Medical Imaging
Mild Cognitive Impairment or Mild Neurocognitive Disorder: Implications for Clinical Practice. Hypothesized Key Players in the Pathogenesis of AD
 AD is a Neurodegenerative Disease as Seen in the PET Scan and is Characterized by Amyloid Plaques and Neurofibrillary Tangles Mild Cognitive Impairment or Mild Neurocognitive Disorder: Implications for
AD is a Neurodegenerative Disease as Seen in the PET Scan and is Characterized by Amyloid Plaques and Neurofibrillary Tangles Mild Cognitive Impairment or Mild Neurocognitive Disorder: Implications for
Diagnosing Dementia: Signs & symptoms, differential diagnosis of common dementias, and non-degenerative memory loss
 Diagnosing Dementia: Signs & symptoms, differential diagnosis of common dementias, and non-degenerative memory loss Incidence of Common Neurological Diseases Incidence New Cases Disease (per 100,000) (per
Diagnosing Dementia: Signs & symptoms, differential diagnosis of common dementias, and non-degenerative memory loss Incidence of Common Neurological Diseases Incidence New Cases Disease (per 100,000) (per
Diagnosis and management of non-alzheimer dementias. Melissa Yu, M.D. Department of Neurology
 Diagnosis and management of non-alzheimer dementias Melissa Yu, M.D. Department of Neurology AGENDA Introduction When to think of alternate diagnoses Other forms of dementia Other reasons for confusion
Diagnosis and management of non-alzheimer dementias Melissa Yu, M.D. Department of Neurology AGENDA Introduction When to think of alternate diagnoses Other forms of dementia Other reasons for confusion
A BRIEF LOOK AT DEMENTIA
 Dementia A BRIEF LOOK AT DEMENTIA David Kaufman, MD Neurology Consultants of Bellin Health November 2, 2017 Defined as a progressive decline in cognitive function that impairs daily activities. Always
Dementia A BRIEF LOOK AT DEMENTIA David Kaufman, MD Neurology Consultants of Bellin Health November 2, 2017 Defined as a progressive decline in cognitive function that impairs daily activities. Always
Do not copy or distribute without permission. S. Weintraub, CNADC, NUFSM, 2009
 Sandra Weintraub, Ph.D. Clinical Core Director, Cognitive Neurology and Alzheimer s Disease Center Northwestern University Feinberg School of Medicine Chicago, Illinois Dementia: a condition caused by
Sandra Weintraub, Ph.D. Clinical Core Director, Cognitive Neurology and Alzheimer s Disease Center Northwestern University Feinberg School of Medicine Chicago, Illinois Dementia: a condition caused by
WHAT IS DEMENTIA? An acquired syndrome of decline in memory and other cognitive functions sufficient to affect daily life in an alert patient
 DEMENTIA WHAT IS DEMENTIA? An acquired syndrome of decline in memory and other cognitive functions sufficient to affect daily life in an alert patient Progressive and disabling Not an inherent aspect of
DEMENTIA WHAT IS DEMENTIA? An acquired syndrome of decline in memory and other cognitive functions sufficient to affect daily life in an alert patient Progressive and disabling Not an inherent aspect of
Appendix K: Evidence review flow charts
 K.1 Dementia diagnosis K.1.1 Dementia diagnosis What are the most effective methods of primary assessment to decide whether a person with suspected dementia should be referred to a dementia service? What
K.1 Dementia diagnosis K.1.1 Dementia diagnosis What are the most effective methods of primary assessment to decide whether a person with suspected dementia should be referred to a dementia service? What
Memory Matters: Learning Objectives: Synapses, Age, and Health. Neuronal Synapses DISCLOSURE DECLARATION. Cognition and Normal Aging
 Standard Deviations from Mean Memory Matters: Preventing and Treating Late-Life, Cognitive Decline Daniel L. Murman, MD, MS Director, Behavioral and Geriatric Neurology Program Professor & Vice Chair,
Standard Deviations from Mean Memory Matters: Preventing and Treating Late-Life, Cognitive Decline Daniel L. Murman, MD, MS Director, Behavioral and Geriatric Neurology Program Professor & Vice Chair,
Diagnosing & managing dementia & delirium
 Aging: Its complex management Dunedin School of Medicine Diagnosing & managing dementia & delirium Falling Confusion Incontinence A. John Campbell University of Otago Medical School New Zealand Impaired
Aging: Its complex management Dunedin School of Medicine Diagnosing & managing dementia & delirium Falling Confusion Incontinence A. John Campbell University of Otago Medical School New Zealand Impaired
HOW TO PREVENT COGNITIVE DECLINE.AT MCI STAGE?
 EAMA CORE CURRICULUM HOW TO PREVENT COGNITIVE DECLINE.AT MCI STAGE? Sofia Duque Orthogeriatric Unit São Francisco Xavier Hospital Occidental Lisbon Hospital Center University Geriatric Unit, Faculty of
EAMA CORE CURRICULUM HOW TO PREVENT COGNITIVE DECLINE.AT MCI STAGE? Sofia Duque Orthogeriatric Unit São Francisco Xavier Hospital Occidental Lisbon Hospital Center University Geriatric Unit, Faculty of
Mild cognitive impairment A view on grey areas of a grey area diagnosis
 Mild cognitive impairment A view on grey areas of a grey area diagnosis Dr Sergi Costafreda Senior Lecturer Division of Psychiatry, UCL Islington Memory Service, C&I NHS FT s.costafreda@ucl.ac.uk London
Mild cognitive impairment A view on grey areas of a grey area diagnosis Dr Sergi Costafreda Senior Lecturer Division of Psychiatry, UCL Islington Memory Service, C&I NHS FT s.costafreda@ucl.ac.uk London
OLD AGE PSYCHIATRY. Dementia definition TYPES OF DEMENTIA. Other causes. Psychiatric disorders of the elderly. Dementia.
 Psychiatric disorders of the elderly OLD AGE PSYCHIATRY Dementia Depression Delusional disorder/late onset schizophrenia Delirium Dementia definition LOCALISATION OF CEREBRAL FUNCTION Impairment of multiple
Psychiatric disorders of the elderly OLD AGE PSYCHIATRY Dementia Depression Delusional disorder/late onset schizophrenia Delirium Dementia definition LOCALISATION OF CEREBRAL FUNCTION Impairment of multiple
Dementia. Dr Maria Foundas Consultant Physician. Training support Skills development Competency Assessment Scholarships Education
 Dementia Dr Maria Foundas Consultant Physician Training support Skills development Competency Assessment Scholarships Education Preamble and disclaimer These slides are made available by the Western Australian
Dementia Dr Maria Foundas Consultant Physician Training support Skills development Competency Assessment Scholarships Education Preamble and disclaimer These slides are made available by the Western Australian
10 Facts We All Need to Know About Dementia (MNCD) in Old Age
 in Old Age") 10 Facts We All Need to Know About Dementia (MNCD) in Old Age DUNCAN ROBERTSON FRCP (LOND & EDIN) FRCPC MEDICAL ADVISOR TO ADVANCING DEMENTIA DIAGNOSIS AND MANAGEMENT IN ALBERTA AND PRIMARY HEALTH CARE
10 Facts We All Need to Know About Dementia (MNCD) in Old Age DUNCAN ROBERTSON FRCP (LOND & EDIN) FRCPC MEDICAL ADVISOR TO ADVANCING DEMENTIA DIAGNOSIS AND MANAGEMENT IN ALBERTA AND PRIMARY HEALTH CARE
Alzheimer's Disease An update on diagnostic criteria & Neuropsychiatric symptoms. l The diagnosis of AD l Neuropsychiatric symptoms l Place of the ICT
 Alzheimer's Disease An update on diagnostic criteria & Neuropsychiatric symptoms State of the art lecture March 4-2012 Philippe H Robert, Philippe Nice - France Robert The diagnosis of AD Neuropsychiatric
Alzheimer's Disease An update on diagnostic criteria & Neuropsychiatric symptoms State of the art lecture March 4-2012 Philippe H Robert, Philippe Nice - France Robert The diagnosis of AD Neuropsychiatric
PROJECTION: Worlds dementia population is expected to triple by 2050
 DEMENTIA C L I S K C O N S U LTA N T P H Y S I C I A N I N A C U T E M E D I C I N E A N D G E R I AT R I C M E D I C I N E, B A R N E T H O S P I TA L, R O YA L F R E E N H S F O U N D AT I O N T R U
DEMENTIA C L I S K C O N S U LTA N T P H Y S I C I A N I N A C U T E M E D I C I N E A N D G E R I AT R I C M E D I C I N E, B A R N E T H O S P I TA L, R O YA L F R E E N H S F O U N D AT I O N T R U
Recommendations For the Use of Donepezil
 Recommendations For the Use of Donepezil The trial of donepezil in patients with mild to moderate dementia due to probable AD was one recommendation made by the Canadian Consensus Conference on Dementia.
Recommendations For the Use of Donepezil The trial of donepezil in patients with mild to moderate dementia due to probable AD was one recommendation made by the Canadian Consensus Conference on Dementia.
Alzheimer disease and other types of
 CMAJ Early release, published at www.cmaj.ca on April 11, 2016. Subject to revision. Practice CME Innovations Amyloid imaging for dementia in Canada Robert Laforce Jr MD PhD, Mohamed Réda Bensaïdane MSc
CMAJ Early release, published at www.cmaj.ca on April 11, 2016. Subject to revision. Practice CME Innovations Amyloid imaging for dementia in Canada Robert Laforce Jr MD PhD, Mohamed Réda Bensaïdane MSc
The Basics of Alzheimer s Disease
 2017 Memory Loss Conference The Basics of Alzheimer s Disease Tom Ala, MD Center for Alzheimer s Disease and Related Disorders Southern Illinois University School of Medicine Springfield, Illinois SIU
2017 Memory Loss Conference The Basics of Alzheimer s Disease Tom Ala, MD Center for Alzheimer s Disease and Related Disorders Southern Illinois University School of Medicine Springfield, Illinois SIU
Common Forms of Dementia Handout Package
 Common Forms of Dementia Handout Package Common Forms of Dementia 1 Learning Objectives As a result of working through this module, you should be better able to: 1. Describe clinical features of 4 major
Common Forms of Dementia Handout Package Common Forms of Dementia 1 Learning Objectives As a result of working through this module, you should be better able to: 1. Describe clinical features of 4 major
The added value of the IWG-2 diagnostic criteria for Alzheimer s disease
 The added value of the IWG-2 diagnostic criteria for Alzheimer s disease Miami, January 2016 Bruno Dubois Head of the Dementia Research Center (IMMA) Director of INSERM Research Unit (ICM) Salpêtrière
The added value of the IWG-2 diagnostic criteria for Alzheimer s disease Miami, January 2016 Bruno Dubois Head of the Dementia Research Center (IMMA) Director of INSERM Research Unit (ICM) Salpêtrière
Dementia and Delirium:
 Dementia and Delirium: A Neurologist s Approach to Altered Mental Status S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Senior Executive
Dementia and Delirium: A Neurologist s Approach to Altered Mental Status S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Senior Executive
I do not have any disclosures
 Alzheimer s Disease: Update on Research, Treatment & Care Clinicopathological Classifications of FTD and Related Disorders Keith A. Josephs, MST, MD, MS Associate Professor & Consultant of Neurology Mayo
Alzheimer s Disease: Update on Research, Treatment & Care Clinicopathological Classifications of FTD and Related Disorders Keith A. Josephs, MST, MD, MS Associate Professor & Consultant of Neurology Mayo
DEMENTIA 101: WHAT IS HAPPENING IN THE BRAIN? Philip L. Rambo, PhD
 DEMENTIA 101: WHAT IS HAPPENING IN THE BRAIN? Philip L. Rambo, PhD OBJECTIVES Terminology/Dementia Basics Most Common Types Defining features Neuro-anatomical/pathological underpinnings Neuro-cognitive
DEMENTIA 101: WHAT IS HAPPENING IN THE BRAIN? Philip L. Rambo, PhD OBJECTIVES Terminology/Dementia Basics Most Common Types Defining features Neuro-anatomical/pathological underpinnings Neuro-cognitive
How to Diagnose Early (Prodromal) Lewy Body Dementia. Ian McKeith MD, FRCPsych, F Med Sci.
 Lewy Body Dementia. Ian McKeith MD, FRCPsych, F Med Sci.") How to Diagnose Early (Prodromal) Lewy Body Dementia Ian McKeith MD, FRCPsych, F Med Sci. Parkinson s Disease Lewy Body Disease Time PD Dementia Lewy Body Dementias Dementia with Lewy Bodies (DLB) Diagnostic
How to Diagnose Early (Prodromal) Lewy Body Dementia Ian McKeith MD, FRCPsych, F Med Sci. Parkinson s Disease Lewy Body Disease Time PD Dementia Lewy Body Dementias Dementia with Lewy Bodies (DLB) Diagnostic
Neuropsychiatric Manifestations in Vascular Cognitive Impairment Patients with and without Dementia
 86 Neuropsychiatric Manifestations in Vascular Cognitive Impairment Patients with and without Dementia Pai-Yi Chiu 1,3, Chung-Hsiang Liu 2, and Chon-Haw Tsai 2 Abstract- Background: Neuropsychiatric profile
86 Neuropsychiatric Manifestations in Vascular Cognitive Impairment Patients with and without Dementia Pai-Yi Chiu 1,3, Chung-Hsiang Liu 2, and Chon-Haw Tsai 2 Abstract- Background: Neuropsychiatric profile
Dementia NICE Guidelines Update. Key points for primary care - NICE guideline (June 2018 update ) 26 September 2018
 26 September 2018") Dementia NICE Guidelines Update Key points for primary care - NICE guideline (June 2018 update ) 26 September 2018 How NICE guidelines are reviewed Multidisciplinary guideline committee established Review
Dementia NICE Guidelines Update Key points for primary care - NICE guideline (June 2018 update ) 26 September 2018 How NICE guidelines are reviewed Multidisciplinary guideline committee established Review
Recognizing Dementia can be Tricky
 Dementia Abstract Recognizing Dementia can be Tricky Dementia is characterized by multiple cognitive impairments that cause significant functional decline. Based on this brief definition, the initial expectation
Dementia Abstract Recognizing Dementia can be Tricky Dementia is characterized by multiple cognitive impairments that cause significant functional decline. Based on this brief definition, the initial expectation
Issues to Consider in the Clinical Evaluation and Development of Drugs for Alzheimer s Disease. The University of Tokyo Hospital
 Project to Promote the Development of Innovative Pharmaceuticals, Medical Devices, and Regenerative Medical Products (Ministry of Health, Labour, and Welfare) Regulatory Science Research for the Establishment
Project to Promote the Development of Innovative Pharmaceuticals, Medical Devices, and Regenerative Medical Products (Ministry of Health, Labour, and Welfare) Regulatory Science Research for the Establishment
Imaging of Alzheimer s Disease: State of the Art
 July 2015 Imaging of Alzheimer s Disease: State of the Art Neir Eshel, Harvard Medical School Year IV Outline Our patient Definition of dementia Alzheimer s disease Epidemiology Diagnosis Stages of progression
July 2015 Imaging of Alzheimer s Disease: State of the Art Neir Eshel, Harvard Medical School Year IV Outline Our patient Definition of dementia Alzheimer s disease Epidemiology Diagnosis Stages of progression
Dementia. Stephen S. Flitman, MD Medical Director 21st Century Neurology
 Dementia Stephen S. Flitman, MD Medical Director 21st Century Neurology www.neurozone.org Dementia is a syndrome Progressive memory loss, plus Progressive loss of one or more cognitive functions: Language
Dementia Stephen S. Flitman, MD Medical Director 21st Century Neurology www.neurozone.org Dementia is a syndrome Progressive memory loss, plus Progressive loss of one or more cognitive functions: Language
Vascular Dementia. Laura Pedelty, PhD MD The University of Illinois at Chicago and Jesse Brown VA Medical Center
 Vascular Dementia Laura Pedelty, PhD MD The University of Illinois at Chicago and Jesse Brown VA Medical Center none Disclosures Objectives To review the definition of Vascular Cognitive Impairment (VCI);
Vascular Dementia Laura Pedelty, PhD MD The University of Illinois at Chicago and Jesse Brown VA Medical Center none Disclosures Objectives To review the definition of Vascular Cognitive Impairment (VCI);
Evaluation and Treatment of Dementia
 Evaluation and Treatment of Dementia Jeffrey M. Burns, MD Edward H. Hashinger Professor of Neurology Co-Director, KU Alzheimer s Disease Center Director, Clinical and Translational Science Unit Disclosures
Evaluation and Treatment of Dementia Jeffrey M. Burns, MD Edward H. Hashinger Professor of Neurology Co-Director, KU Alzheimer s Disease Center Director, Clinical and Translational Science Unit Disclosures
UDS version 3 Summary of major changes to UDS form packets
 UDS version 3 Summary of major changes to UDS form packets from version 2 to VERSION 3 february 18 final Form A1: Subject demographics Updated question on principal referral source to add additional options
UDS version 3 Summary of major changes to UDS form packets from version 2 to VERSION 3 february 18 final Form A1: Subject demographics Updated question on principal referral source to add additional options
Form A3: Subject Family History
 Initial Visit Packet NACC Uniform Data Set (UDS) Form A: Subject Family History ADC name: Subject ID: Form date: / / Visit #: Examiner s initials: INSTRUCTIONS: This form is to be completed by a clinician
Initial Visit Packet NACC Uniform Data Set (UDS) Form A: Subject Family History ADC name: Subject ID: Form date: / / Visit #: Examiner s initials: INSTRUCTIONS: This form is to be completed by a clinician
#CHAIR2015. Miami, Florida. September 24 26, JW Marriott Miami. Sponsored by
 #CHAIR2015 September 24 26, 2015 JW Marriott Miami Miami, Florida Sponsored by Case Challenge Workshop Alzheimer s Disease Anand Kumar, MD University of Illinois at Chicago, College of Medicine Chicago,
#CHAIR2015 September 24 26, 2015 JW Marriott Miami Miami, Florida Sponsored by Case Challenge Workshop Alzheimer s Disease Anand Kumar, MD University of Illinois at Chicago, College of Medicine Chicago,
The place for treatments of associated neuropsychiatric and other symptoms
 The place for treatments of associated neuropsychiatric and other symptoms Luca Pani dg@aifa.gov.it London, 25 th November 2014 Workshop on Alzheimer s Disease European Medicines Agency London, UK Public
The place for treatments of associated neuropsychiatric and other symptoms Luca Pani dg@aifa.gov.it London, 25 th November 2014 Workshop on Alzheimer s Disease European Medicines Agency London, UK Public
Appendix L: Research recommendations
 1 L.1 Dementia diagnosis (amyloid PET imaging) recommendation 1 Index Test Reference Test(s) Does amyloid PET imaging provide additional diagnostic value, and is it cost effective, for the diagnosis of
1 L.1 Dementia diagnosis (amyloid PET imaging) recommendation 1 Index Test Reference Test(s) Does amyloid PET imaging provide additional diagnostic value, and is it cost effective, for the diagnosis of
White matter hyperintensities correlate with neuropsychiatric manifestations of Alzheimer s disease and frontotemporal lobar degeneration
 White matter hyperintensities correlate with neuropsychiatric manifestations of Alzheimer s disease and frontotemporal lobar degeneration Annual Scientific Meeting Canadian Geriatric Society Philippe Desmarais,
White matter hyperintensities correlate with neuropsychiatric manifestations of Alzheimer s disease and frontotemporal lobar degeneration Annual Scientific Meeting Canadian Geriatric Society Philippe Desmarais,
8/14/2018. The Evolving Concept of Alzheimer s Disease. Epochs of AD Research. Diagnostic schemes have evolved with the research
 The Evolving Concept of Alzheimer s Disease David S. Geldmacher, MD, FACP Warren Family Endowed Chair in Neurology Department of Neurology UAB School of Medicine Epochs of AD Research Epoch Years Key Event
The Evolving Concept of Alzheimer s Disease David S. Geldmacher, MD, FACP Warren Family Endowed Chair in Neurology Department of Neurology UAB School of Medicine Epochs of AD Research Epoch Years Key Event
Stephen Salloway, M.D., M.S. Disclosure of Interest
 Challenges in the Early Diagnosis of Alzheimer s Disease Stephen Salloway, MD, MS Professor of Neurology and Psychiatry Alpert Medical School, Brown University 2 nd Annual Early Alzheimer s Educational
Challenges in the Early Diagnosis of Alzheimer s Disease Stephen Salloway, MD, MS Professor of Neurology and Psychiatry Alpert Medical School, Brown University 2 nd Annual Early Alzheimer s Educational
Dementia: A Comprehensive Update Neuroimaging, CSF, and genetic biomarkers in dementia
 Dementia: A Comprehensive Update 2016 Neuroimaging, CSF, and genetic biomarkers in dementia Bradford C. Dickerson, M.D. Associate Professor of Neurology, Harvard Medical School Departments of Neurology
Dementia: A Comprehensive Update 2016 Neuroimaging, CSF, and genetic biomarkers in dementia Bradford C. Dickerson, M.D. Associate Professor of Neurology, Harvard Medical School Departments of Neurology
Alzheimer s Disease without Dementia
 Alzheimer s Disease without Dementia Dr Emer MacSweeney CEO & Consultant Neuroradiologist Re:Cognition Health London Osteopathic Society 13 September 2016 Early diagnosis of Alzheimer s Disease How and
Alzheimer s Disease without Dementia Dr Emer MacSweeney CEO & Consultant Neuroradiologist Re:Cognition Health London Osteopathic Society 13 September 2016 Early diagnosis of Alzheimer s Disease How and
Dementia. Assessing Brain Damage. Mental Status Examination
 Dementia Assessing Brain Damage Mental status examination Information about current behavior and thought including orientation to reality, memory, and ability to follow instructions Neuropsychological
Dementia Assessing Brain Damage Mental status examination Information about current behavior and thought including orientation to reality, memory, and ability to follow instructions Neuropsychological
Diagnosis and management of Dementia
 Diagnosis and management of Dementia Dr. Jahnavi Kedare Associate Professor Dept. of Psychiatry, T. N. Medical College B. Y. L. Nair Hospital, Mumbai Prevalence of Dementia Lower than developed countries
Diagnosis and management of Dementia Dr. Jahnavi Kedare Associate Professor Dept. of Psychiatry, T. N. Medical College B. Y. L. Nair Hospital, Mumbai Prevalence of Dementia Lower than developed countries
ALZHEIMER S DISEASE OVERVIEW. Jeffrey Cummings, MD, ScD Cleveland Clinic Lou Ruvo Center for Brain Health
 ALZHEIMER S DISEASE OVERVIEW Jeffrey Cummings, MD, ScD Cleveland Clinic Lou Ruvo Center for Brain Health Prevalence AD: DEMOGRAPHY AND CLINICAL FEATURES Risk and protective factors Clinical features and
ALZHEIMER S DISEASE OVERVIEW Jeffrey Cummings, MD, ScD Cleveland Clinic Lou Ruvo Center for Brain Health Prevalence AD: DEMOGRAPHY AND CLINICAL FEATURES Risk and protective factors Clinical features and
CTFPHC Working Group Members:
 Cognitive Impairment - Guideline Presentation Speaker deck OVERVIEW We will review the following: 1. Background on Cognitive Impairment 2. Methods of the CTFPHC 3. Recommendations and Key Findings 4. Implementation
Cognitive Impairment - Guideline Presentation Speaker deck OVERVIEW We will review the following: 1. Background on Cognitive Impairment 2. Methods of the CTFPHC 3. Recommendations and Key Findings 4. Implementation