Early Mobility: The Experiences of Two ICUs
|
|
|
- Allen Tyler
- 6 years ago
- Views:
Transcription
1 Early Mobility: The Experiences of Two ICUs Sharon Dickinson MSN, RN, ANP, ACNS-BC, CCRN Clinical Nurse Specialist SICU/Rapid Response Sarah Taylor MSN, RN, ACNS-BC Clinical Nurse Specialist TBICU University of Michigan Health System Ann Arbor, MI
2 Disclosures Nothing to disclose
3 Objectives At the end of the presentation the learner will be able to: Describe the process of developing an early mobility protocol for ICU patients and how to modify to adapt to specific patient populations Define the impact a mobility protocol can have on: ICU LOS Hospital LOS Deposition
4 Historical Background Early ambulation first introduced in WW II Expedited recovery for soldiers to return to war Rheums Dis Clinic NA 1990;16: Early Rising After Operation NEJM 1942; 14: Benefits of early mobility were clear First, morale is greatly improved General health and strength are better maintained & convalescence is more rapid
5 Risks associated with immobility. Complications can be significant for bedridden, critically ill patients Multiple random trials have associated bed rest with HARM Neuromuscular dysfunction Stevens RD, et. Al., Intensive Care Medicine, 2007, Angela KM, et. Al., ICU Director, 2012 Delayed weaning from mechanical ventilation - Morris PE., Crit Care Clin, 2007 Neuropsychiatric, cognitive dysfunction - Pisani MA et al., AJRCCM, 2010
6 Is mobility important for ICU patients? Evidence suggests yes! Decreased LOS in ICU Decreased days on ventilator Decreased pressure ulcer rates Improved mortality
7 Protocols/Guidelines can help improve getting patients moving The greatest impact of early mobilization is through standardized mobility protocols or programs. Pashikanti, L and Von Ah, Diane, 2012
8 Do we actively mobilize our patients? MTQIP survey results 80% admit their patients to the ICU with a bedrest order 70% mobilize (bedside PT, OOB to chair, standing and/or walking) patients only after they are hemodynamically stable Reasons to withhold mobility included: FIO2 >60%, Ventrics, Epidurals, sedation, unclear spines. So the answer is mostly no. But would a mobility protocol really make a difference?
9 How Did we build the Protocol? Dickinson S, Tschannan D and Shever L, Can the Use of an Early Mobility Program Reduce the Incidence of Pressure Ulcers in a Surgical Critical Care Unit? Critical Care Nurse Quarterly Jan-Mar How Did We Do This?? No definitive literature to guide our protocol Utilized Evidence from: Rehabilitation Medicine Immunology Gerontology Biological Sciences/Medical Sciences Physiotherapy Research
10 Literature Review Title: Early Intensive Care Unit Mobility Therapy in the Treatment of Acute Respiratory Failure Purpose: To assess the frequency of physical therapy, site of initiation of physical therapy, and patient outcomes comparing respiratory failure patients who received usual care compared with patients who received physical therapy from a Mobility Team using the mobility protocol. Method: Prospective cohort study of MICU patients with acute respiratory failure requiring mechanical ventilation on admission. An ICU Mobility Team (ICU RN, Nursing Assistant, PT) initiated the protocol within 48 hours of mechanical ventilation. Results: A Mobility Team using a mobility protocol initiated earlier physical therapy was feasible, safe, did not increase costs, and was associated with decreased ICU and hospital LOS in survivors who received physical therapy during ICU treatment versus patients who received usual care. Morris, Goad, Thompson, Taylor, et al., 2008
11 Literature review Title: Early Physical and Occupational Therapy in Mechanically Ventilated, Critically Ill Patients: A Randomized Controlled Trial Purpose: To assess the efficacy of combining daily interruption of sedation with physical and occupational therapy on functional outcomes in patients receiving mechanical ventilation in intensive care. Method: Prospective, randomized controlled trial of sedated adults. Patients were randomized to early exercise an mobilization (PT and OT) during periods of sedation interruption or to therapy as ordered per primary team during sedation holiday. Results: Return to independent functional status at hospital discharge occurred in significantly more patients from the intervention group versus control. Intervention group also had significantly shorter duration of delirium and more ventilator-free days during 28-day follow-up than controls. Interruption of sedation combined with PT and OT in the earliest days of critical illness was safe and well tolerated. Schweickert, Pohlman, Pohlman, Nigos, et al., 2009


12 Barriers to Overcome Bed rest as an admission order selection Concern for the safety of tubes and lines Patient size Hemodynamic/respirator y instability Sedation protocols Limited resources (people and equipment) Fear by all

13 Early Mobility Program Moving and Grooving Early Mobility Program Initiated in the Surgical ICU 2010 Adopted and started in the Trauma Burn ICU April Sharon Dickinson, The University of Michigan Health System
 FiO2 < or equal to 80% (Used to be 60%) Peep less than or equal to 10 cm H2O Goals: 1.")

, ICP monitoring")
14 Inclusion Criteria: Early activity is initiated when the patient achieves physiological stabilization Low dose catecholamine drips should not preclude the patient from early mobility (i.e. low dose norepi, phenylephrine, vasopressin) FiO2 < or equal to 80% (Used to be 60%) Peep less than or equal to 10 cm H2O Goals: 1. Every patient should be evaluated for early mobility. 2. Small efforts can yield large results. 3. Never give up! Poor tolerance during one episode does not predict future tolerance. 4. Evaluate patient readiness and response to current therapy and ability to progress. *Possible criteria to withhold early mobility: hypoxia, hemodynamic instability (escalation of vasopressors in the last 12 hours), ICP monitoring or unstable cardiac rhythm (life threatening rhythm that compromises blood pressure in past 24 hours) or new cardiac arrhythmia & epidural.
15 HOW DID WE MODIFY FOR BURN PATIENTS?


16 Inclusion Criteria: Trauma Burn Special Considerations: Goals: Early activity is initiated when the patient achieves physiological stabilization Low dose catecholamine drips should not preclude the patient from early mobility (i.e. low dose norepi, phenylephrine, vasopressin) FiO2 < or equal to 60% Peep less than or equal to 10 cm H2O ROM should only be performed on nonimpaired joints or those with stable orthopedic injuries See post-op wound sheet for activity restrictions s/p grafting Spinal cord injury pts. need abd. binder, Juzos or ACE, and proper chair for mobility ACE wraps to lower extremities if burn present 1. Every patient should be evaluated for early mobility. 2. Small efforts can yield large results. 3. Never give up! Poor tolerance during one episode does not predict future tolerance. 4. Evaluate patient readiness and response to current therapy and ability to progress. *Possible criteria to withhold early mobility: hypoxia, hemodynamic instability (escalation of vasopressors in the last 12 hours), ICP monitoring or unstable cardiac rhythm (life threatening rhythm that compromises blood pressure in past 24 hours) or new cardiac arrhythmia, epidural, & critical/difficult airways. *Special considerations need to be addressed for: spinal clearance, orthopedic injuries and newly placed skin grafts prior to starting ROM.
17 Burn Algorithm s/p Grafting Taylor, Manning, & Quarles

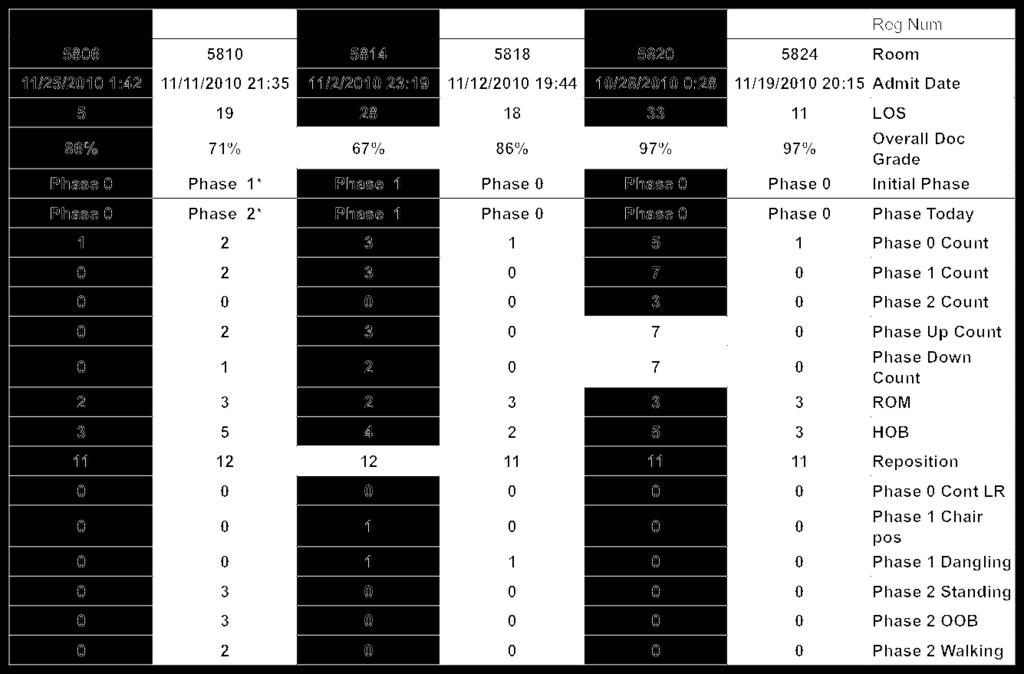
18 Tracking the data
19 OUTCOMES
20 TBICU: Patients Pre-Initiation Data Period : December 11, April 29, 2012 Post-Initiation Data Period: April 30, August 31, 2012 Pre Post % Change Admissions: Case Mix: Burn Trauma Post-Op Trauma Non-Op All Other
21 TBICU: LOS Pre Post % Change ICU Length of Stay Average Median Minimum Maximum Hosp Length of Stay Average Median Minimum Maximum Acuity down 11.1% in Post-Implementation period. This led to an expected decrease in ICU and hospital length of stay (LOS) as well as decreased ICU and hospital mortality rates. Case mix shows a significant increase in Burn and Post-Op trauma admissions in the Post-Implementation period.
22 Mortality Pre Post % Change ICU Disposition Status Live Dead Mortality Rate Hosp Disposition Status Live Dead Mortality Rate More patients were leaving the unit and hospital alive!
23 SICU outcomes -When combined with our CCI Bundle. Datapoint Pre-Implementation Avg (Total) Post-Implementation Avg (Total) % Change Patient CCI Encounters % SICU-Only Readmissions % Age % Day 1 APACHE % ICU LOS % Hosp LOS % Vent LOS % Total Group Vent Days (835) (622) -25.5% CRRT Days % Total Group CRRT Days (351) (224) -36.2% ICU Disposition Pre-Implementation Post-Implementation % Change Alive % Dead % Rate 31.3% 16.7% -46.6% Hosp Disposition Pre-Implementation Post-Implementation % Change Alive % Dead % Rate 39.3% 22.0% -44.0%
24 THE CHALLENGE OF THE DIFFICULT ICU PATIENT


25 CRRT/ECMO Patient Being Mobilized..
26 70% TBSA Burn Patient
27 Conclusions.. It is easy and safe to mobilize patients Standardized protocols help to define expectations and will enhance mobility Even the most complicated ICU patients can get up and moving with standardized protocols (burns, trauma, ventilated, CRRT, ECMO, other) Standardized mobility protocols can improve outcomes: ICU, LOS, Vent days, CRRT days, Disposition, and other areas not discussed (i.e. pressure ulcer free days and patient well being)

28 Questions?
29 References. Allen C. Glasziou P, Del Mar C. Bed rest: a potential harmful treatment needing more careful evaluation. Lancet. 1999; 354: American Nurses Association. Nursing report card for acute care. Washington, DC: American Nurses Association Bower RG. Consequences of bed rest. Critical Care Medicine. 2009; 37. (10): Bruunsgaard, H. Physical activity and modulation of systemic low-level inflammation. J Leukoc Biol Oct;78(4): Dammeyer J, Dickinson S, Packard D, Baldwin N, Ricklemann C. Building a protocol to guide mobility in the ICU. Crit Care Nurs Q Jan-Mar;36(1): doi: /CNQ.0b013e acd. Morris PE. Moving our critically ill patients: mobility barriers and benefits. Critical Care Clinics. 2007; 23(1);1-20. Morris, P., Goad, A., Thompson, C., Taylor, K., et al. (2008). Early intensive care unit mobility therapy in the treatment of acute respiratory failure. Critical Care Medicine, 36(8), doi: /CCM.0b013e318180b90e
30 References Needham DM, Korupolu R, Zanni JM, Pradhan P, Colantuoni E, Palmer JB, Brower RG, & Fan E. Early physical medicine and rehabilitation for patients with acute respiratory failure: a quality improvement project. Arch Phys Med Rehabil Apr;91(4): doi: /j.apmr Perme, C. & Chandrashekar, R. Early mobility and walking program for patients in intensive care units: creating a standard of care. Am J Crit Care May;18(3): doi: /ajcc Schweickert, W., Pohlman, M., Pohlman, A., Nigos, C., et al. (2009). Early physical and occupational therapy in mechanically ventilated, critically ill patients: A randomised controlled trial. Lancet 373, doi: /S (09) Winkelman, C. (2007). Inactivity and inflammation in the critically ill patient. Critical Care Clinics 23, doi: /j.ccc
The Michigan Trauma Quality Improvement Program. Kalamazoo, MI May 15, 2013
 The Michigan Trauma Quality Improvement Program Kalamazoo, MI May 15, 2013 Agenda Sarah Taylor and Sharon Dickinson ICU Mobility Judy Mikhail Trauma Service FTE Survey BCBS Physician Uplift Cardiothoracic
The Michigan Trauma Quality Improvement Program Kalamazoo, MI May 15, 2013 Agenda Sarah Taylor and Sharon Dickinson ICU Mobility Judy Mikhail Trauma Service FTE Survey BCBS Physician Uplift Cardiothoracic
What About All Those Critical Lines? Lines, catheters and drains can be accommodated, secured EVD line stationary bike
 What About All Those Critical Lines? Lines, catheters and drains can be accommodated, secured EVD line stationary bike What About All Those Critical Lines?. Patient lines and drains can be accommodated
What About All Those Critical Lines? Lines, catheters and drains can be accommodated, secured EVD line stationary bike What About All Those Critical Lines?. Patient lines and drains can be accommodated
Start Walking: Improving Outcomes through Use of an Early Progressive Mobility Program. Theresa Murray MSN,RN, CCRN,CCNS Samantha Lichti BSN, RN
 Start Walking: Improving Outcomes through Use of an Early Progressive Mobility Program Theresa Murray MSN,RN, CCRN,CCNS Samantha Lichti BSN, RN Challenge, Journey, Evolution Everest is 29, 035 ft. 5 ½
Start Walking: Improving Outcomes through Use of an Early Progressive Mobility Program Theresa Murray MSN,RN, CCRN,CCNS Samantha Lichti BSN, RN Challenge, Journey, Evolution Everest is 29, 035 ft. 5 ½
Early and Structured Rehabilitation Team Collaboration. David McWilliams Clinical Specialist Physiotherapist - UHB
 Early and Structured Rehabilitation Team Collaboration David McWilliams Clinical Specialist Physiotherapist - UHB Start early Moving through milestones Schweikert et al (2009) Increase frequency of higher
Early and Structured Rehabilitation Team Collaboration David McWilliams Clinical Specialist Physiotherapist - UHB Start early Moving through milestones Schweikert et al (2009) Increase frequency of higher
ICU Rehabilitation: Current Issues Changing the ICU Paradigm: Role of Early Mobilization
 ICU Rehabilitation: Current Issues Changing the ICU Paradigm: Role of Early Mobilization Carolyn L. Rochester, M.D. Yale University School of Medicine VA Connecticut Healthcare System August 29, 2015 WFSICCM,
ICU Rehabilitation: Current Issues Changing the ICU Paradigm: Role of Early Mobilization Carolyn L. Rochester, M.D. Yale University School of Medicine VA Connecticut Healthcare System August 29, 2015 WFSICCM,
MARIA KOBYLECKY RN, MScN, CNCC JEANENE LUCKHART BSc, Grad Dip PT CELINA ROGERS RRT SUZANNE WATTS BHSc PT
 MARIA KOBYLECKY RN, MScN, CNCC JEANENE LUCKHART BSc, Grad Dip PT CELINA ROGERS RRT SUZANNE WATTS BHSc PT Objectives Understand some of the detrimental effects of critical illness, prolonged bed rest and
MARIA KOBYLECKY RN, MScN, CNCC JEANENE LUCKHART BSc, Grad Dip PT CELINA ROGERS RRT SUZANNE WATTS BHSc PT Objectives Understand some of the detrimental effects of critical illness, prolonged bed rest and
Early Physical Rehabilitation in the ICU and Ventilator Liberation
 Early Physical Rehabilitation in the ICU and Ventilator Liberation 本檔僅供內部教學使用檔案內所使用之照片之版權仍屬於原期刊公開使用時, 須獲得原期刊之同意授權 Respiratory Care 2012 Oct Vol 57 No 10 Pedro A Mendez-Tellez MD and Dale M Needham MD PhD
Early Physical Rehabilitation in the ICU and Ventilator Liberation 本檔僅供內部教學使用檔案內所使用之照片之版權仍屬於原期刊公開使用時, 須獲得原期刊之同意授權 Respiratory Care 2012 Oct Vol 57 No 10 Pedro A Mendez-Tellez MD and Dale M Needham MD PhD
CRITICALLY APPRAISED PAPER (CAP)
") CRITICALLY APPRAISED PAPER (CAP) Schweickert, W. D., Pohlman, M. C., Pohlman, A. S., Nigos, C., Pawlik, A. J., Esbrook, C. L., Kress, J.P. (2009). Early physical and occupational therapy in mechanically
CRITICALLY APPRAISED PAPER (CAP) Schweickert, W. D., Pohlman, M. C., Pohlman, A. S., Nigos, C., Pawlik, A. J., Esbrook, C. L., Kress, J.P. (2009). Early physical and occupational therapy in mechanically
Text-based Document. Meta-Analysis of the Effects of Early Mobilization on Mechanically Ventilated Patients. Downloaded 1-Jul :41:43
 The Henderson Repository is a free resource of the Honor Society of Nursing, Sigma Theta Tau International. It is dedicated to the dissemination of nursing research, researchrelated, and evidence-based
The Henderson Repository is a free resource of the Honor Society of Nursing, Sigma Theta Tau International. It is dedicated to the dissemination of nursing research, researchrelated, and evidence-based
Time is Muscle. In this talk, I will address 3 ques7ons: School of Rehabilita?on Science Reaching Further
 School of Rehabilita?on Science Reaching Further Time is Muscle Michelle Kho, PT, PhD Canada Research Chair in Cri?cal Care Rehabilita?on and Knowledge Transla?on McMaster University, Hamilton, ON Clinician
School of Rehabilita?on Science Reaching Further Time is Muscle Michelle Kho, PT, PhD Canada Research Chair in Cri?cal Care Rehabilita?on and Knowledge Transla?on McMaster University, Hamilton, ON Clinician
Early Mobility and Walking Program for Patients in Intensive Care Units: Creating a Standard of Care
 1 of 11 06/08/2009 12:52 www.medscape.com From American Journal of Critical Care Early Mobility and Walking Program for Patients in Intensive Care Units: Creating a Standard of Care Creating a Standard
1 of 11 06/08/2009 12:52 www.medscape.com From American Journal of Critical Care Early Mobility and Walking Program for Patients in Intensive Care Units: Creating a Standard of Care Creating a Standard
CRITICALLY APPRAISED PAPER (CAP)
") CRITICALLY APPRAISED PAPER (CAP) FOCUSED QUESTION Is early mobilization safe and more effective than usual care in promoting recovery and functional independence in clients in the intensive care unit (ICU)
CRITICALLY APPRAISED PAPER (CAP) FOCUSED QUESTION Is early mobilization safe and more effective than usual care in promoting recovery and functional independence in clients in the intensive care unit (ICU)
prolonged bed rest and inactivity EARLY REHABILITATION IN THE ICU:
 Mortality and ARDS EARLY REHABILITATION IN THE ICU: MOVE IT or LOSE IT Progress of Intensive Care Medicine has resulted in significantly improved survival of cri:cally ill pa:ents. Rik Gosselink Dept Rehabilita>on
Mortality and ARDS EARLY REHABILITATION IN THE ICU: MOVE IT or LOSE IT Progress of Intensive Care Medicine has resulted in significantly improved survival of cri:cally ill pa:ents. Rik Gosselink Dept Rehabilita>on
Early Rehabilitation in the ICU: Do We Still Need Chest Physiotherapy?
 Early Rehabilitation in the ICU: Do We Still Need Chest Physiotherapy? Michelle Kho, PT, PhD Assistant Professor, School of Rehabilitation Science, McMaster University Adjunct Assistant Professor, Department
Early Rehabilitation in the ICU: Do We Still Need Chest Physiotherapy? Michelle Kho, PT, PhD Assistant Professor, School of Rehabilitation Science, McMaster University Adjunct Assistant Professor, Department
Liberation from Mechanical Ventilation in Critically Ill Adults
 Liberation from Mechanical Ventilation in Critically Ill Adults 2017 ACCP/ATS Clinical Practice Guidelines Timothy D. Girard, MD, MSCI Clinical Research, Investigation, and Systems Modeling of Acute Illness
Liberation from Mechanical Ventilation in Critically Ill Adults 2017 ACCP/ATS Clinical Practice Guidelines Timothy D. Girard, MD, MSCI Clinical Research, Investigation, and Systems Modeling of Acute Illness
An Innovative Mobilization Framework for Delirium Management: How to Un-paralyze the Assessment and Implementation Process
 An Innovative Mobilization Framework for Delirium Management: How to Un-paralyze the Assessment and Implementation Process Melissa Redlich PCM RNBN Christine Filipek CNE RNBN CNCC(C) Stephanie McLeod RNBN
An Innovative Mobilization Framework for Delirium Management: How to Un-paralyze the Assessment and Implementation Process Melissa Redlich PCM RNBN Christine Filipek CNE RNBN CNCC(C) Stephanie McLeod RNBN
KICU Spontaneous Awakening Trial (SAT) Questionnaire
 Questionnaire") KICU Spontaneous Awakening Trial (SAT) Questionnaire Please select your best answer(s): 1. What is your professional role? 1 Staff Nurse 2 Nurse Manager 3 Nurse Educator 4 Physician 5 Medical Director
KICU Spontaneous Awakening Trial (SAT) Questionnaire Please select your best answer(s): 1. What is your professional role? 1 Staff Nurse 2 Nurse Manager 3 Nurse Educator 4 Physician 5 Medical Director
Surgery Grand Rounds. Non-invasive Ventilation: A valuable tool. James Cromie, PGY 3 8/24/09
 Surgery Grand Rounds Non-invasive Ventilation: A valuable tool James Cromie, PGY 3 8/24/09 History of mechanical ventilation 1930 s: use of iron lung 1940 s: First NIV system (Bellevue Hospital) 1950 s:
Surgery Grand Rounds Non-invasive Ventilation: A valuable tool James Cromie, PGY 3 8/24/09 History of mechanical ventilation 1930 s: use of iron lung 1940 s: First NIV system (Bellevue Hospital) 1950 s:
Critically ill patients frequently
 Clinical trials of early mobilization of critically ill patients John P. Kress, MD Intensive care unit-acquired weakness is a common complication of critical illness leading to severe functional impairment
Clinical trials of early mobilization of critically ill patients John P. Kress, MD Intensive care unit-acquired weakness is a common complication of critical illness leading to severe functional impairment
ICU Early Mobilization at UCSF
 ICU Early Mobilization at UCSF Critical Care Medicine & Trauma Conference San Francisco, CA June 5, 2010 Presented by Heidi Engel, PT, DPT Heidi.Engel@ucsfmedctr.org Can We Do Better? Herridge MS. Mobile,
ICU Early Mobilization at UCSF Critical Care Medicine & Trauma Conference San Francisco, CA June 5, 2010 Presented by Heidi Engel, PT, DPT Heidi.Engel@ucsfmedctr.org Can We Do Better? Herridge MS. Mobile,
Sara Combilizer. Multifunctional positioning aid for early mobilisation and ICU Rehabilitation. with people in mind
 Sara Combilizer Multifunctional positioning aid for early mobilisation and ICU Rehabilitation with people in mind Importance of mobilisation A structured rehabilitation programme counteracts the adverse
Sara Combilizer Multifunctional positioning aid for early mobilisation and ICU Rehabilitation with people in mind Importance of mobilisation A structured rehabilitation programme counteracts the adverse
Sara Combilizer. Multifunctional aid for early mobilization and ICU Rehabilitation. with people in mind
 Sara Combilizer Multifunctional aid for early mobilization and ICU Rehabilitation with people in mind Importance of mobilisation By counteracting the adverse effects of immobility and enhancing the function
Sara Combilizer Multifunctional aid for early mobilization and ICU Rehabilitation with people in mind Importance of mobilisation By counteracting the adverse effects of immobility and enhancing the function
 PHYSIOTHERAPY IN INTENSIVE CARE: how the evidence has changed since 2000 Kathy Stiller Physiotherapy Department Royal Adelaide Hospital Adelaide South Australia Kathy.Stiller@health.sa.gov.au Aim review
PHYSIOTHERAPY IN INTENSIVE CARE: how the evidence has changed since 2000 Kathy Stiller Physiotherapy Department Royal Adelaide Hospital Adelaide South Australia Kathy.Stiller@health.sa.gov.au Aim review
Optimize vent weaning and SBT outcomes. Identify underlying causes for SBT failures. Role SBT and weaning protocol have in respiratory care
 Optimize vent weaning and SBT outcomes Identify underlying causes for SBT failures Role SBT and weaning protocol have in respiratory care Lower risk of developing complications Lower risk of VAP, other
Optimize vent weaning and SBT outcomes Identify underlying causes for SBT failures Role SBT and weaning protocol have in respiratory care Lower risk of developing complications Lower risk of VAP, other
Prolonged Mechanical Ventilation
 Prolonged Mechanical Ventilation Shannon S. Carson, MD Associate Professor and Chief Pulmonary and Critical Care Medicine University of North Carolina AJRCCM 2010 Projected Growth of Prolonged Acute MV
Prolonged Mechanical Ventilation Shannon S. Carson, MD Associate Professor and Chief Pulmonary and Critical Care Medicine University of North Carolina AJRCCM 2010 Projected Growth of Prolonged Acute MV
Physiotherapy on the Intensive Care Unit. Information for patients, their family and carers
 Physiotherapy on the Intensive Care Unit Information for patients, their family and carers A team of Specialist Physiotherapists works in the Intensive Care Units within the Oxford University Hospitals
Physiotherapy on the Intensive Care Unit Information for patients, their family and carers A team of Specialist Physiotherapists works in the Intensive Care Units within the Oxford University Hospitals
Nutrition and Sepsis
 Nutrition and Sepsis Todd W. Rice, MD, MSc Associate Professor of Medicine Vanderbilt University 2017 DNS Symposium June 2, 2017 Case 55 y.o. male COPD, DM, HTN, presents with pneumonia and septic shock.
Nutrition and Sepsis Todd W. Rice, MD, MSc Associate Professor of Medicine Vanderbilt University 2017 DNS Symposium June 2, 2017 Case 55 y.o. male COPD, DM, HTN, presents with pneumonia and septic shock.
Ventilator-Associated Event Prevention: Innovations
 Ventilator-Associated Event Prevention: Innovations Michael J. Apostolakos, MD Professor of Medicine Director, Adult Critical Care University of Rochester Mobility/Sedation in the ICU Old teaching: Keep
Ventilator-Associated Event Prevention: Innovations Michael J. Apostolakos, MD Professor of Medicine Director, Adult Critical Care University of Rochester Mobility/Sedation in the ICU Old teaching: Keep
The implementation of an early rehabilitation program is associated with reduced length of stay: A multi-icu study
 Original article The implementation of an early rehabilitation program is associated with reduced length of stay: A multi-icu study Journal of the Intensive Care Society 2016, Vol. 17(1) 2 11! The Intensive
Original article The implementation of an early rehabilitation program is associated with reduced length of stay: A multi-icu study Journal of the Intensive Care Society 2016, Vol. 17(1) 2 11! The Intensive
The Art and Science of Weaning from Mechanical Ventilation
 The Art and Science of Weaning from Mechanical Ventilation Shekhar T. Venkataraman M.D. Professor Departments of Critical Care Medicine and Pediatrics University of Pittsburgh School of Medicine Some definitions
The Art and Science of Weaning from Mechanical Ventilation Shekhar T. Venkataraman M.D. Professor Departments of Critical Care Medicine and Pediatrics University of Pittsburgh School of Medicine Some definitions
Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill
 Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill Joe Palumbo PGY-2 Critical Care Pharmacy Resident Buffalo General Medical Center Disclosures
Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill Joe Palumbo PGY-2 Critical Care Pharmacy Resident Buffalo General Medical Center Disclosures
MOVE IT or LOSE IT EARLY REHABILITATION IN THE ICU: Deconditioning Inactivity. Rik Gosselink, PT,PhD Dept Rehabilitation Sciences KU Leuven
 Deconditioning Inactivity Eal functioning Retained secretions Lung collaps Weaning EARLY REHABILITATION IN THE ICU: Deconditioning Inactivity MOVE IT or LOSE IT Rik Gosselink, PT,PhD Dept Rehabilitation
Deconditioning Inactivity Eal functioning Retained secretions Lung collaps Weaning EARLY REHABILITATION IN THE ICU: Deconditioning Inactivity MOVE IT or LOSE IT Rik Gosselink, PT,PhD Dept Rehabilitation
Sara Combilizer. Multifunctional aid for early mobilization and ICU rehabilitation. with people in mind
 Sara Combilizer Multifunctional aid for early mobilization and ICU rehabilitation with people in mind Importance of mobilization Enhancing the functionality of body mechanics from the beginning of a structured
Sara Combilizer Multifunctional aid for early mobilization and ICU rehabilitation with people in mind Importance of mobilization Enhancing the functionality of body mechanics from the beginning of a structured
Rehabilitation therapy and outcomes in acute respiratory failure: An observational pilot project
 Journal of Critical Care (2010) 25, 254 262 Rehabilitation therapy and outcomes in acute respiratory failure: An observational pilot project Jennifer M. Zanni PT, MSPT a,c, Radha Korupolu MBBS, MS b, Eddy
Journal of Critical Care (2010) 25, 254 262 Rehabilitation therapy and outcomes in acute respiratory failure: An observational pilot project Jennifer M. Zanni PT, MSPT a,c, Radha Korupolu MBBS, MS b, Eddy
Outcomes From Severe ARDS Managed Without ECMO. Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016
 Outcomes From Severe ARDS Managed Without ECMO Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016 Severe ARDS Berlin Definition 2012 P:F ratio 100 mm Hg Prevalence:
Outcomes From Severe ARDS Managed Without ECMO Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016 Severe ARDS Berlin Definition 2012 P:F ratio 100 mm Hg Prevalence:
DELIRIUM IN ICU: Prevention and Management. Milind Baldi
 DELIRIUM IN ICU: Prevention and Management Milind Baldi Contents Introduction Risk factors Assessment Prevention Management Introduction Delirium is a syndrome characterized by acute cerebral dysfunction
DELIRIUM IN ICU: Prevention and Management Milind Baldi Contents Introduction Risk factors Assessment Prevention Management Introduction Delirium is a syndrome characterized by acute cerebral dysfunction
Update in Critical Care Medicine
 Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
ICU Acquired Weakness Mobilisation Nutrition. ICU Acquired Weakness CRITICALLY ILL 20/10/2017. X. Wittebole Critical Care Department
 ICU Acquired Weakness Mobilisation Nutrition X. Wittebole Critical Care Department CRITICALLY ILL 2 ICU Acquired Weakness 1915: Sr W. OSLER The Principles of Medicine VIIIth Edition «Neuromuscular Dysfunction
ICU Acquired Weakness Mobilisation Nutrition X. Wittebole Critical Care Department CRITICALLY ILL 2 ICU Acquired Weakness 1915: Sr W. OSLER The Principles of Medicine VIIIth Edition «Neuromuscular Dysfunction
Hips & Knees Priority Action Team
 Hips & Knees Priority Action Team Current State Data Refresh September 5, 27 Overview Population Profile Health Status Utilization of Hip & Knee Total Joint Services 1 1 Population Profile 2 SouthWest
Hips & Knees Priority Action Team Current State Data Refresh September 5, 27 Overview Population Profile Health Status Utilization of Hip & Knee Total Joint Services 1 1 Population Profile 2 SouthWest
9/28/2016. Sedation Strategies in the ICU. Outline. ICU sedation. Recent clinical practice guidelines Top 10 myths A practical approach
 Sedation Strategies in the ICU UW Medicine EMS and Trauma Conference Seattle, Washington September 26 th, 2016 C. Terri Hough, MD MSc Associate Professor of Medicine Division of Pulmonary and Critical
Sedation Strategies in the ICU UW Medicine EMS and Trauma Conference Seattle, Washington September 26 th, 2016 C. Terri Hough, MD MSc Associate Professor of Medicine Division of Pulmonary and Critical
TALK TRAUMA Clearing the C-Spine. David Ouellette
 TALK TRAUMA 2011 Clearing the C-Spine David Ouellette Case #1 - Mother / Daughter MVC 34 y/o female Dangerous mechanism CHI Mumbling incoherently Femur # - distracting injury ETOH - 22 9 y/o female Dangerous
TALK TRAUMA 2011 Clearing the C-Spine David Ouellette Case #1 - Mother / Daughter MVC 34 y/o female Dangerous mechanism CHI Mumbling incoherently Femur # - distracting injury ETOH - 22 9 y/o female Dangerous
Rehabilitation within critical care
 Rehabilitation within critical care Why consider Rehab on ITU? 110,000 people admitted to critical care units in England and Wales each year (ICNARC) 75% survive and are discharged home Long Term Effects
Rehabilitation within critical care Why consider Rehab on ITU? 110,000 people admitted to critical care units in England and Wales each year (ICNARC) 75% survive and are discharged home Long Term Effects
SARASOTA MEMORIAL HOSPITAL DEPARTMENT POLICY
 PS1006 SARASOTA MEMORIAL HOSPITAL DEPARTMENT POLICY TITLE: ADMISSION/DISCHARGE CRITERIA: CARDIOVASCULAR THORACIC STEP DOWN UNIT (CVTSDU) EFFECTIVE DATE: REVISED DATE: POLICY TYPE: (Cardiac) 8/03 1/19 DEPARTMENTAL
PS1006 SARASOTA MEMORIAL HOSPITAL DEPARTMENT POLICY TITLE: ADMISSION/DISCHARGE CRITERIA: CARDIOVASCULAR THORACIC STEP DOWN UNIT (CVTSDU) EFFECTIVE DATE: REVISED DATE: POLICY TYPE: (Cardiac) 8/03 1/19 DEPARTMENTAL
Exercise in ICU/CCU Assist. Prof. Visal Kantaratanakul, MD, * Board Certified in Rehabilitation Medicine * Director, Samitivej Srinakarin
 Exercise in ICU/CCU Assist. Prof. Visal Kantaratanakul, MD, * Board Certified in Rehabilitation Medicine * Director, Samitivej Srinakarin Rehabilitation Center * Member, Exercise Expert Committee, Ministry
Exercise in ICU/CCU Assist. Prof. Visal Kantaratanakul, MD, * Board Certified in Rehabilitation Medicine * Director, Samitivej Srinakarin Rehabilitation Center * Member, Exercise Expert Committee, Ministry
Disclosures. Objectives. Procalcitonin: Pearls and Pitfalls in Daily Practice
 Procalcitonin: Pearls and Pitfalls in Daily Practice Sarah K Harrison, PharmD, BCCCP Clinical Pearl Disclosures The author of this presentation has no disclosures concerning possible financial or personal
Procalcitonin: Pearls and Pitfalls in Daily Practice Sarah K Harrison, PharmD, BCCCP Clinical Pearl Disclosures The author of this presentation has no disclosures concerning possible financial or personal
Can Goal Directed Sedation Improve Outcomes?
 Can Goal Directed Sedation Improve Outcomes? Yahya SHEHABI, FANZCA, FCICM, EMBA Professor and Program Director Critical care Monash Health and Monash University - Melbourne School of Medicine, University
Can Goal Directed Sedation Improve Outcomes? Yahya SHEHABI, FANZCA, FCICM, EMBA Professor and Program Director Critical care Monash Health and Monash University - Melbourne School of Medicine, University
SARASOTA MEMORIAL HOSPITAL NURSING DEPARTMENT POLICY
 PS1070 SARASOTA MEMORIAL HOSPITAL NURSING DEPARTMENT POLICY TITLE: ADMISSION/DISCHARGE CRITERIA: CARDIOVASCULAR INTENSIVE Job Title of Reviewer: Director, CVICU EFFECTIVE DATE: REVIEWED/REVISED DATE: POLICY
PS1070 SARASOTA MEMORIAL HOSPITAL NURSING DEPARTMENT POLICY TITLE: ADMISSION/DISCHARGE CRITERIA: CARDIOVASCULAR INTENSIVE Job Title of Reviewer: Director, CVICU EFFECTIVE DATE: REVIEWED/REVISED DATE: POLICY
UPMC Critical Care
 UPMC Critical Care www.ccm.upmc.edu CRISMA Critical Care Medicine the University of Pittsburgh Optimal use of ICU resources Derek C. Angus, MD, MPH, FRCP The CRISMA Laboratory Critical Care Medicine School
UPMC Critical Care www.ccm.upmc.edu CRISMA Critical Care Medicine the University of Pittsburgh Optimal use of ICU resources Derek C. Angus, MD, MPH, FRCP The CRISMA Laboratory Critical Care Medicine School
Should Early Mobilization Be Routine in Mechanically Ventilated Patients?
 Should Early Mobilization Be Routine in Mechanically Ventilated Patients? Ulrich H Schmidt MD PhD MBA, Lauren Knecht MD, and Neil R MacIntyre MD FAARC Introduction Early Mobilization: The Case for Routine
Should Early Mobilization Be Routine in Mechanically Ventilated Patients? Ulrich H Schmidt MD PhD MBA, Lauren Knecht MD, and Neil R MacIntyre MD FAARC Introduction Early Mobilization: The Case for Routine
Early Goal Directed Sedation In Critically Ill Patients
 Early Goal Directed Sedation In Critically Ill Patients Yahya Shehabi, FCICM, FANZCA, EMBA Professor, Intensive Care Medicine Clinical School of Medicine, University New South Wales School of Epidemiology
Early Goal Directed Sedation In Critically Ill Patients Yahya Shehabi, FCICM, FANZCA, EMBA Professor, Intensive Care Medicine Clinical School of Medicine, University New South Wales School of Epidemiology
Reasons for Extending Length of Stay in Inpatient Spinal Cord Rehabilitation
 Reasons for Extending Length of Stay in Inpatient Spinal Cord Rehabilitation September 5, 2012 Heather Flett MSc, BScPT, BA Advanced Practice Leader- Spinal Cord Rehab Toronto Rehab UHN, University of
Reasons for Extending Length of Stay in Inpatient Spinal Cord Rehabilitation September 5, 2012 Heather Flett MSc, BScPT, BA Advanced Practice Leader- Spinal Cord Rehab Toronto Rehab UHN, University of
REHABILITATION OF PATIENTS MANAGED IN ICU
 REHABILITATION OF PATIENTS MANAGED IN ICU RECOMMENDATIONS Safety to mobilize / exercise: on the website Recommendation 1 All critically ill patients nursed in ICU should be screened closely before active
REHABILITATION OF PATIENTS MANAGED IN ICU RECOMMENDATIONS Safety to mobilize / exercise: on the website Recommendation 1 All critically ill patients nursed in ICU should be screened closely before active
UH Case Medical Center Adult Inpatient Telemetry Admission, Transfer and Discharge Guidelines
 UH Case Medical Center Adult Inpatient Telemetry Admission, Transfer and Discharge Guidelines STATEMENT OF PURPOSE: To facilitate appropriate geo-location placement of patients who require telemetry monitoring
UH Case Medical Center Adult Inpatient Telemetry Admission, Transfer and Discharge Guidelines STATEMENT OF PURPOSE: To facilitate appropriate geo-location placement of patients who require telemetry monitoring
Challenges in Diagnosis, Surveillance and Prevention of Ventilator-associated pneumonia
 Challenges in Diagnosis, Surveillance and Prevention of Ventilator-associated pneumonia Massachusetts Coalition for the Prevention of Errors November 6, 2008 Michael Klompas MD, MPH, FRCPC Brigham and
Challenges in Diagnosis, Surveillance and Prevention of Ventilator-associated pneumonia Massachusetts Coalition for the Prevention of Errors November 6, 2008 Michael Klompas MD, MPH, FRCPC Brigham and
Intensive care in the very old. Hans Flaatten
 Intensive care in the very old Hans Flaatten What is considered old and very old? WHO definition Old 60, suggested 65 in developed countries Very old No accepted definition 75 and 80 are often used as
Intensive care in the very old Hans Flaatten What is considered old and very old? WHO definition Old 60, suggested 65 in developed countries Very old No accepted definition 75 and 80 are often used as
Disclosures. Learning Outcomes: 5/7/2011. Pulmonary vs. Skin Outcomes: Do We Really Need to Select. Ventilator-Associated Pneumonia(VAP)
") Disclosures Pulmonary vs. Skin Outcomes: Do We Really Need to Select Just One? Kathleen M. Vollman MSN, RN, CCNS, FCCM, FAAN Clinical Nurse Specialist/Educator/Consultant ADVANCING NURSING kvollman@comcast.net
Disclosures Pulmonary vs. Skin Outcomes: Do We Really Need to Select Just One? Kathleen M. Vollman MSN, RN, CCNS, FCCM, FAAN Clinical Nurse Specialist/Educator/Consultant ADVANCING NURSING kvollman@comcast.net
REHABILITATION UNIT ANNUAL OUTCOMES REPORT Prepared by
 REHABILITATION UNIT ANNUAL OUTCOMES Prepared by REPORT - 2014 Keir Ringquist, PT, PhD, GCS Rehabilitation Program Manager Director of Occupational and Physical Therapy DEMOGRAPHICS OF THE REHABILITATION
REHABILITATION UNIT ANNUAL OUTCOMES Prepared by REPORT - 2014 Keir Ringquist, PT, PhD, GCS Rehabilitation Program Manager Director of Occupational and Physical Therapy DEMOGRAPHICS OF THE REHABILITATION
VOLUME-BASED VS. RATE-BASED FEEDING
 VOLUME-BASED VS. RATE-BASED FEEDING Amanda Holyk Critical Care Pharmacist Mount Nittany Medical Center Society of Critical Care Medicine Annual Symposium November 10, 2017 0 Disclosure I have no actual
VOLUME-BASED VS. RATE-BASED FEEDING Amanda Holyk Critical Care Pharmacist Mount Nittany Medical Center Society of Critical Care Medicine Annual Symposium November 10, 2017 0 Disclosure I have no actual
ICU Liberation for the Pharmacist. A. Kendall Gross, PharmD, BCPS, BCCCP Critical Care Pharmacist UCSF Medical Center
 ICU Liberation for the Pharmacist A. Kendall Gross, PharmD, BCPS, BCCCP Critical Care Pharmacist UCSF Medical Center Disclosure No conflicts of interest to disclose Objectives o Outline the elements of
ICU Liberation for the Pharmacist A. Kendall Gross, PharmD, BCPS, BCCCP Critical Care Pharmacist UCSF Medical Center Disclosure No conflicts of interest to disclose Objectives o Outline the elements of
DIAGRAM OF THE PRESENTATION. Post ICU Rehabilitation. Effective strategies in ICU. During two last decades
 1 1st European Conference on Weaning & Rehabilitation in Critically ill Patients INTERNATIONAL EARLY MOBILISATION NETWORK Post ICU Rehabilitation Serafeim N. Nanas Professor of Critical Care Medicine Evaggelismos
1 1st European Conference on Weaning & Rehabilitation in Critically ill Patients INTERNATIONAL EARLY MOBILISATION NETWORK Post ICU Rehabilitation Serafeim N. Nanas Professor of Critical Care Medicine Evaggelismos
The Use of Metabolic Resuscitation in Sepsis
 The Use of Metabolic Resuscitation in Sepsis Jennifer M. Roth, PharmD, BCPS, BCCCP Critical Care Clinical Specialist - Surgical Trauma ICU Baylor University Medical Center Disclosures No conflicts of interest
The Use of Metabolic Resuscitation in Sepsis Jennifer M. Roth, PharmD, BCPS, BCCCP Critical Care Clinical Specialist - Surgical Trauma ICU Baylor University Medical Center Disclosures No conflicts of interest
Frequently Asked Questions: Riverview Rehabilitation Center
 Frequently Asked Questions: Riverview Rehabilitation Center WHAT SERVICES ARE PROVIDED? Riverview Rehabilitation Center provides a comprehensive, interdisciplinary and functionally based treatment program
Frequently Asked Questions: Riverview Rehabilitation Center WHAT SERVICES ARE PROVIDED? Riverview Rehabilitation Center provides a comprehensive, interdisciplinary and functionally based treatment program
Proprietary Acute Care Indicators
 Proprietary Acute Care Indicators Indicator 1a: Device-Associated Infections in the Intensive Care Unit Central Line-Associated Bloodstream Infections in the APICU, CCU, MICU, M/S ICU, & SICU Ventilator-Associated
Proprietary Acute Care Indicators Indicator 1a: Device-Associated Infections in the Intensive Care Unit Central Line-Associated Bloodstream Infections in the APICU, CCU, MICU, M/S ICU, & SICU Ventilator-Associated
The Seated Patient 15 th Biennial Conference New Orleans
 The Seated Patient 15 th Biennial Conference New Orleans Track 1 March 11, 2017 Christine Berke MSN APRN-NP CWOCN-AP Nebraska Medicine cberke@nebraskamed.com 2017 National Pressure Ulcer Advisory Panel
The Seated Patient 15 th Biennial Conference New Orleans Track 1 March 11, 2017 Christine Berke MSN APRN-NP CWOCN-AP Nebraska Medicine cberke@nebraskamed.com 2017 National Pressure Ulcer Advisory Panel
OHSU. Update in Sepsis
 Update in Sepsis Jonathan Pak, MD June 1, 2017 Structure of Talk 1. Sepsis-3: The latest definition 2. Clinical Management - Is EGDT dead? - Surviving Sepsis Campaign Guidelines 3. A novel therapy: Vitamin
Update in Sepsis Jonathan Pak, MD June 1, 2017 Structure of Talk 1. Sepsis-3: The latest definition 2. Clinical Management - Is EGDT dead? - Surviving Sepsis Campaign Guidelines 3. A novel therapy: Vitamin
Year in Review: Critical Care Medicine
 Year in Review: Critical Care Medicine No disclosures Eric J. Seeley, M.D. Assistant Professor of Medicine Division of Pulmonary and Critical Care Medicine Why I Selected These Studies High quality studies
Year in Review: Critical Care Medicine No disclosures Eric J. Seeley, M.D. Assistant Professor of Medicine Division of Pulmonary and Critical Care Medicine Why I Selected These Studies High quality studies
Critical Care RN Needs Assessment 2010
 Critical Care RN Needs Assessment 2010 OO9d, 2010 Critical Care Needs Assessment Survey Results.pdf 1. Identify the area you work on. Percent SSDU 17.2% 10 NSDU 3.4% 2 NSCU 13.8% 8 BICU 8.6% 5 SICU 31.0%
Critical Care RN Needs Assessment 2010 OO9d, 2010 Critical Care Needs Assessment Survey Results.pdf 1. Identify the area you work on. Percent SSDU 17.2% 10 NSDU 3.4% 2 NSCU 13.8% 8 BICU 8.6% 5 SICU 31.0%
Critical Illness and Homelessness
 Critical Illness and Homelessness Jan O Friedrich, MD DPhil Associate Professor of Medicine, University of Toronto Medical Director, MSICU St. Michael s Hospital, Toronto, Canada Critical Care Canada Forum
Critical Illness and Homelessness Jan O Friedrich, MD DPhil Associate Professor of Medicine, University of Toronto Medical Director, MSICU St. Michael s Hospital, Toronto, Canada Critical Care Canada Forum
International Journal of Scientific & Engineering Research, Volume 7, Issue 1, January ISSN
 International Journal of Scientific & Engineering Research, Volume 7, Issue 1, January-2016 1589 Early goal directed Physiotherapy in Patients undergoing Extracorporeal cardiac life support Gottschalk,
International Journal of Scientific & Engineering Research, Volume 7, Issue 1, January-2016 1589 Early goal directed Physiotherapy in Patients undergoing Extracorporeal cardiac life support Gottschalk,
CORTICOSTEROID USE IN SEPTIC SHOCK THE ONGOING DEBATE DIEM HO, PHARMD PGY1 PHARMACY RESIDENT VALLEY BAPTIST MEDICAL CENTER BROWNSVILLE
 CORTICOSTEROID USE IN SEPTIC SHOCK THE ONGOING DEBATE DIEM HO, PHARMD PGY1 PHARMACY RESIDENT VALLEY BAPTIST MEDICAL CENTER BROWNSVILLE 1 ABBREVIATIONS ACCP = American College of Chest Physicians ARF =
CORTICOSTEROID USE IN SEPTIC SHOCK THE ONGOING DEBATE DIEM HO, PHARMD PGY1 PHARMACY RESIDENT VALLEY BAPTIST MEDICAL CENTER BROWNSVILLE 1 ABBREVIATIONS ACCP = American College of Chest Physicians ARF =
Quand doit-on commencer à mobiliser les patients
 Universidad de Concepción Quand doit-on commencer à mobiliser les patients Cheryl HICKMANN Doctorant Université Catholique de Louvain (UCL) Intensive Care Unit, Saint-Luc University Hospital, Brussels,
Universidad de Concepción Quand doit-on commencer à mobiliser les patients Cheryl HICKMANN Doctorant Université Catholique de Louvain (UCL) Intensive Care Unit, Saint-Luc University Hospital, Brussels,
ENHANCED RECOVERY AFTER SURGERY (ERAS) PATHWAYS PARESH C. SHAH MD FACS VICE CHAIR OF SURGERY DIRECTOR OF GENERAL SURGERY
 PATHWAYS PARESH C. SHAH MD FACS VICE CHAIR OF SURGERY DIRECTOR OF GENERAL SURGERY") Department of Surgery Divison of General Surgery ENHANCED RECOVERY AFTER SURGERY (ERAS) PATHWAYS PARESH C. SHAH MD FACS VICE CHAIR OF SURGERY DIRECTOR OF GENERAL SURGERY December 2016 Disclosure Paresh
Department of Surgery Divison of General Surgery ENHANCED RECOVERY AFTER SURGERY (ERAS) PATHWAYS PARESH C. SHAH MD FACS VICE CHAIR OF SURGERY DIRECTOR OF GENERAL SURGERY December 2016 Disclosure Paresh
Safety of physical therapy interventions in critically ill patients: A single center prospective evaluation of 1,110 ICU admissions
 Accepted Manuscript Safety of physical therapy interventions in critically ill patients: A single center prospective evaluation of 1,110 ICU admissions Thiti Sricharoenchai MD, Ann M. Parker MD, Jennifer
Accepted Manuscript Safety of physical therapy interventions in critically ill patients: A single center prospective evaluation of 1,110 ICU admissions Thiti Sricharoenchai MD, Ann M. Parker MD, Jennifer
Improving Healthcare Utilization in Injured Older Adults
 Improving Healthcare Utilization in Injured Older Adults G ERIATRIC T R A U MA I N I T I AT I V E S AT S TA N F O R D H E A LT H C A R E J U LY 12, 2018 Objectives Background on Geriatric Trauma Population
Improving Healthcare Utilization in Injured Older Adults G ERIATRIC T R A U MA I N I T I AT I V E S AT S TA N F O R D H E A LT H C A R E J U LY 12, 2018 Objectives Background on Geriatric Trauma Population
Advocacy = Safety. Notes on Hospitals: Learning Objectives At the completion of this activity, the participant will be able to:
 Early Progressive Mobility is a Must: Evidence Based Strategies for Achieving Safe Mobility Practices Kathleen Vollman MSN, RN, CCNS, FCCM, FAAN Clinical Nurse Specialist/Educator/Consultant ADVANCING
Early Progressive Mobility is a Must: Evidence Based Strategies for Achieving Safe Mobility Practices Kathleen Vollman MSN, RN, CCNS, FCCM, FAAN Clinical Nurse Specialist/Educator/Consultant ADVANCING
Sentinel Stroke National Audit Programme (SSNAP)
") Sentinel Stroke National Audit Programme (SSNAP) Changes over Time: 4 years of data April 2013 March 2017 National results Based on stroke patients admitted to and/or discharged from hospital between April
Sentinel Stroke National Audit Programme (SSNAP) Changes over Time: 4 years of data April 2013 March 2017 National results Based on stroke patients admitted to and/or discharged from hospital between April
REHABILITATION UNIT ANNUAL OUTCOMES REPORT
 REHABILITATION UNIT ANNUAL OUTCOMES REPORT - 2013 Prepared by Keir Ringquist, PT, PhD, GCS Rehabilitation Program Manager Director of Occupational and Physical Therapy 1 DEMOGRAPHICS OF THE REHABILITATION
REHABILITATION UNIT ANNUAL OUTCOMES REPORT - 2013 Prepared by Keir Ringquist, PT, PhD, GCS Rehabilitation Program Manager Director of Occupational and Physical Therapy 1 DEMOGRAPHICS OF THE REHABILITATION
Division of Acute Care Surgery Clinical Practice Policies, Guidelines, and Algorithms: Enteral Nutrition Algorithm Clinical Practice Guideline
 Division of Acute Care Surgery Clinical Practice Policies, Guidelines, and Algorithms: Enteral Nutrition Algorithm Clinical Practice Guideline Original Date: 08/2011 Purpose: To promote the early use of
Division of Acute Care Surgery Clinical Practice Policies, Guidelines, and Algorithms: Enteral Nutrition Algorithm Clinical Practice Guideline Original Date: 08/2011 Purpose: To promote the early use of
Guidelines and Protocols
 TITLE: CHEST TRAUMA PURPOSE: Provides a standardized treatment algorithm for patients with chest trauma PROCESS: I. INITIAL ASSESSMENT OF THORACIC TRAUMA A. Penetrating Thoracic Trauma 1. Hemodynamically
TITLE: CHEST TRAUMA PURPOSE: Provides a standardized treatment algorithm for patients with chest trauma PROCESS: I. INITIAL ASSESSMENT OF THORACIC TRAUMA A. Penetrating Thoracic Trauma 1. Hemodynamically
An Overview of the Chronic Critical Illness Syndrome (CCIS) and Weaning the PMV Patient
 and Weaning the PMV Patient") An Overview of the Chronic Critical Illness Syndrome (CCIS) and Weaning the PMV Patient Fall 2011 CCIS has been known for some time HISTORICAL PRECURSORS INCLUDE: SIRS Systemic Inflammatory Response Syndrome
An Overview of the Chronic Critical Illness Syndrome (CCIS) and Weaning the PMV Patient Fall 2011 CCIS has been known for some time HISTORICAL PRECURSORS INCLUDE: SIRS Systemic Inflammatory Response Syndrome
ICU Early Mobilization at UCSF
 ICU Early Mobilization at UCSF Presented by Heidi Engel, PT, DPT Heidi.Engel@ucsfmedctr.org Presentation Objectives Review of patient functional decline related to an ICU stay Define early ICU mobilization
ICU Early Mobilization at UCSF Presented by Heidi Engel, PT, DPT Heidi.Engel@ucsfmedctr.org Presentation Objectives Review of patient functional decline related to an ICU stay Define early ICU mobilization
Rehabilitation so much to offer, often too late. Desiree Cox Practice Manager Life St Dominic s Rehabilitation Unit East London
 Rehabilitation so much to offer, often too late Desiree Cox Practice Manager Life St Dominic s Rehabilitation Unit East London OUTLINE The ICU Environment The psychological effects Can Rehabilitation
Rehabilitation so much to offer, often too late Desiree Cox Practice Manager Life St Dominic s Rehabilitation Unit East London OUTLINE The ICU Environment The psychological effects Can Rehabilitation
Effect of post-intubation hypotension on outcomes in major trauma patients
 Effect of post-intubation hypotension on outcomes in major trauma patients Dr. Robert S. Green Professor, Emergency Medicine and Critical Care Dalhousie University Medical Director, Trauma Nova Scotia
Effect of post-intubation hypotension on outcomes in major trauma patients Dr. Robert S. Green Professor, Emergency Medicine and Critical Care Dalhousie University Medical Director, Trauma Nova Scotia
Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh. Professor of Critical Care, Edinburgh University
 Tim Walsh. Professor of Critical Care, Edinburgh University") Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh Professor of Critical Care, Edinburgh University Lecture Plan: a route to clarity What is delirium? Why is delirium important? Step
Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh Professor of Critical Care, Edinburgh University Lecture Plan: a route to clarity What is delirium? Why is delirium important? Step
Sepsis 3.0: The Impact on Quality Improvement Programs
 Sepsis 3.0: The Impact on Quality Improvement Programs Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care Warren Alpert Medical School of Brown University
Sepsis 3.0: The Impact on Quality Improvement Programs Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care Warren Alpert Medical School of Brown University
ARDS and Ventilators PG26 Update in Surgical Critical Care October 9, 2013
 ARDS and Ventilators PG26 Update in Surgical Critical Care October 9, 2013 Pauline K. Park MD, FACS, FCCM University of Michigan School of Medicine Ann Arbor, MI OVERVIEW New Berlin definition of ARDS
ARDS and Ventilators PG26 Update in Surgical Critical Care October 9, 2013 Pauline K. Park MD, FACS, FCCM University of Michigan School of Medicine Ann Arbor, MI OVERVIEW New Berlin definition of ARDS
Tracheostomy practice in adults with acute respiratory failure
 本檔僅供內部教學使用檔案內所使用之照片之版權仍屬於原期刊公開使用時, 須獲得原期刊之同意授權 Tracheostomy practice in adults with acute respiratory failure Bradley D. Freeman, MD, FACS; Peter E. Morris, MD, FCCP Crit Care Med 2012 Vol. 40, No. 10
本檔僅供內部教學使用檔案內所使用之照片之版權仍屬於原期刊公開使用時, 須獲得原期刊之同意授權 Tracheostomy practice in adults with acute respiratory failure Bradley D. Freeman, MD, FACS; Peter E. Morris, MD, FCCP Crit Care Med 2012 Vol. 40, No. 10
Disclosure. Hospira Pharmaceuticals. Unrestricted research funding Honoraria for CME education administered via France Foundation
 Disclosure Hospira Pharmaceuticals Unrestricted research funding Honoraria for CME education administered via France Foundation Economics in Sedation: Responsible Use of the ICU Budget John W. Devlin,
Disclosure Hospira Pharmaceuticals Unrestricted research funding Honoraria for CME education administered via France Foundation Economics in Sedation: Responsible Use of the ICU Budget John W. Devlin,
ICU MANAGEMENT PLUS: TRANSFORMING CARE IN THE INTENSIVE CARE UNIT EARLY MOBILISATION OF CRITICALLY ILL PATIENTS: SERIES - PART ONE
 ICU MANAGEMENT T H E O F F I C I A L M A N AG E M E N T A N D P R AC T I C E J O U R N A L V O L U M E 9 - I S S U E 3 - A U T U M N 2 0 0 9 DISASTER: ARE YOU PREPARED? PLUS: EARLY MOBILISATION OF CRITICALLY
ICU MANAGEMENT T H E O F F I C I A L M A N AG E M E N T A N D P R AC T I C E J O U R N A L V O L U M E 9 - I S S U E 3 - A U T U M N 2 0 0 9 DISASTER: ARE YOU PREPARED? PLUS: EARLY MOBILISATION OF CRITICALLY
Withdrawal of Care in the ICU
 Withdrawal of Care in the ICU Arlene Bobonich, MD Director, Inpatient Palliative Medicine PinnacleHealth System WHO IS DRIVING THE BUS? WHERE IS THE BUS GOING? HOW DO YOU GET OFF THE BUS? WHO GETS THROWN
Withdrawal of Care in the ICU Arlene Bobonich, MD Director, Inpatient Palliative Medicine PinnacleHealth System WHO IS DRIVING THE BUS? WHERE IS THE BUS GOING? HOW DO YOU GET OFF THE BUS? WHO GETS THROWN
ANWICU knowledge
 ANWICU knowledge www.anwicu.org.uk This presentation is provided by ANWICU We are a collaborative association of ICUs in the North West of England. Permission to provide this presentation has been granted
ANWICU knowledge www.anwicu.org.uk This presentation is provided by ANWICU We are a collaborative association of ICUs in the North West of England. Permission to provide this presentation has been granted
Sharp HealthCare Hospice and Palliative Care
 Sharp HealthCare Hospice and Palliative Care The Continuum for Advanced Illness and End Stage Disease Management (AAC) Daniel R. Hoefer, MD CMO, Outpatient Palliative Care and Hospice Suzi K. Johnson,
Sharp HealthCare Hospice and Palliative Care The Continuum for Advanced Illness and End Stage Disease Management (AAC) Daniel R. Hoefer, MD CMO, Outpatient Palliative Care and Hospice Suzi K. Johnson,
NIV in hypoxemic patients
 NIV in hypoxemic patients Massimo Antonelli, MD Dept. of Intensive Care & Anesthesiology Università Cattolica del Sacro Cuore Rome - Italy Conflict of interest (research grants and consultations): Maquet
NIV in hypoxemic patients Massimo Antonelli, MD Dept. of Intensive Care & Anesthesiology Università Cattolica del Sacro Cuore Rome - Italy Conflict of interest (research grants and consultations): Maquet
How Biodex programs give UHS Pruitt the clinical advantage BIODEX
 CASESTUDY How Biodex programs give UHS Pruitt the clinical advantage UHS Pruitt Corporation BIODEX Biodex Medical Systems, Inc. 20 Ramsey Road, Shirley, New York, 11967-4704, Tel: 800-224-6339 (Int l 631-924-9000),
CASESTUDY How Biodex programs give UHS Pruitt the clinical advantage UHS Pruitt Corporation BIODEX Biodex Medical Systems, Inc. 20 Ramsey Road, Shirley, New York, 11967-4704, Tel: 800-224-6339 (Int l 631-924-9000),
Outline. Basic principles of lung protective ventilation. The challenging areas. Small tidal volumes Recruitment
 ARDS beyond 6/kg Gordon D. Rubenfeld, MD MSc Professor of Medicine, University of Toronto Chief, Program in Trauma, Emergency, and Critical Care Sunnybrook Health Sciences Centre Outline Basic principles
ARDS beyond 6/kg Gordon D. Rubenfeld, MD MSc Professor of Medicine, University of Toronto Chief, Program in Trauma, Emergency, and Critical Care Sunnybrook Health Sciences Centre Outline Basic principles
APRV: An Update CHLOE STEINSHOUER, MD PULMONARY & SLEEP CONSULTANTS OF KANSAS 04/06/2017
 APRV: An Update CHLOE STEINSHOUER, MD PULMONARY & SLEEP CONSULTANTS OF KANSAS 04/06/2017 Disclosures No conflicts of interest Objectives Attendees will be able to: Define the mechanism of APRV Describe
APRV: An Update CHLOE STEINSHOUER, MD PULMONARY & SLEEP CONSULTANTS OF KANSAS 04/06/2017 Disclosures No conflicts of interest Objectives Attendees will be able to: Define the mechanism of APRV Describe
EAST MULTICENTER STUDY DATA COLLECTION TOOL
 EAST MULTICENTER STUDY DATA COLLECTION TOOL Multicenter Study: Effect of Regional Anesthesia on Delirium in Geriatric Trauma Patients with Multiple Rib Fractures Enrolling Center: Enrolling Co-investigators:
EAST MULTICENTER STUDY DATA COLLECTION TOOL Multicenter Study: Effect of Regional Anesthesia on Delirium in Geriatric Trauma Patients with Multiple Rib Fractures Enrolling Center: Enrolling Co-investigators:
Outcomes of an accelerated discharge pathway after spinal fusion
 Outcomes of an accelerated discharge pathway after spinal fusion Sarah Temby The Royal Children s Hospital March 2017 Background Scoliosis = Lateral curvature and rotation of the spine Adolescent Idiopathic
Outcomes of an accelerated discharge pathway after spinal fusion Sarah Temby The Royal Children s Hospital March 2017 Background Scoliosis = Lateral curvature and rotation of the spine Adolescent Idiopathic
Effectiveness and Safety of the Awakening and Breathing Coordination, Delirium
 Online Data Supplement Effectiveness and Safety of the Awakening and Breathing Coordination, Delirium Monitoring/Management, and Early Exercise/Mobility (ABCDE) Bundle Authors-Michele C. Balas, Eduard
Online Data Supplement Effectiveness and Safety of the Awakening and Breathing Coordination, Delirium Monitoring/Management, and Early Exercise/Mobility (ABCDE) Bundle Authors-Michele C. Balas, Eduard
Can We Ever Get To Never? Reducing Infec8ons in a Surgical ICU. Wendy L. Wahl, MD, FACS, FCCM October 12, 2010 Michigan TQIP
 Can We Ever Get To Never? Reducing Infec8ons in a Surgical ICU Wendy L. Wahl, MD, FACS, FCCM October 12, 2010 Michigan TQIP The Unit 10 ICU beds, 6 floor status beds Trauma, Burns, Emergent General Surgery
Can We Ever Get To Never? Reducing Infec8ons in a Surgical ICU Wendy L. Wahl, MD, FACS, FCCM October 12, 2010 Michigan TQIP The Unit 10 ICU beds, 6 floor status beds Trauma, Burns, Emergent General Surgery