Early-Detection Pediatric Sepsis Algorithm
|
|
|
- Eugene Stanley
- 6 years ago
- Views:
Transcription

1 Early-Detection Pediatric Sepsis Algorithm Matthew Eisenberg, MD, Division of Emergency Medicine Kate Madden, MD, MMSc, Division of Critical Care Medicine Boston Children s Hospital and Harvard Medical School, Boston, MA Session #29: March 6,
2 Conflict of Interest Statistical and project management support for this study were provided by an electronic medical record vendor Drs. Madden and Eisenberg received no financial support and have no other disclosures or conflicts of interest 2
3 Agenda Background Creating a pediatric sepsis detection algorithm Algorithm performance Implementation into clinical workflows Future directions 3
4 Learning Objectives Recognize the process used to develop and evaluate the pediatric sepsis algorithm at Boston Children s Hospital Describe the range of operating characteristics of the pediatric sepsis algorithm based on different changes to the algorithm Identify the strategy for inserting the algorithm into clinical workflows Discuss the plans to iterate on the algorithm moving forward 4

5 Background Pediatric vs. adult sepsis Quality improvement efforts in pediatric sepsis Source: Childrens Hospital Photo Exhibit 5

6 March 28 Rory Staunton, a 12 year-old cut his arm during basketball practice in school Rory woke up vomiting and complaining of pain in his leg. He later developed a fever of 104 March 29 - morning 6 March 29 7:14 pm Rory went to the emergency room and was discharged two hours later, after being diagnosed with "acute febrile gastritis" (the flu) Rory Staunton died in intensive care of septic shock brought on by the infection April 1
7 Pediatric Sepsis 4,000 children die annually of sepsis in the U.S. more than cancer (~1,800) or gun violence (~1,700) #1 cause of mortality in children worldwide Adults vs. Kids Adult sepsis criteria SCCM/ES-ICM Sepsis 3 (JAMA 2016) Defines sepsis with organ dysfunction Organ dysfunction not a sensitive sign in pediatrics Children develop shock later in course 7
8 The Challenge of Recognition Adults Sepsis identification tools based on one set of criteria Organ dysfunction included in sepsis definition Hypotension an earlier sign Children Vital sign & lab criteria differ based on age groups Tools must incorporate many different age-based cutoffs Organ dysfunction a later sign Hypotension occurs late 8

9 Paul, Pediatrics,
10 Care Element Pre-intervention Post-intervention Adherence, n (%) Improving Adherence Adherence, to n PALS (%) Septic Shock Guidelines P Value Recognition within 5 min 180 (79) 113 (97).011 Vascular access within 5 min 84 (67) 104 (90) < ml/kg IV fluid within 60 min 47 (37) 85 (73) <.001 Antibiotics within 60 min 88 (70) 99 (86).02 Vasoactive agents started at 60 min 44 (35) 79 (68) <.001 Overall bundle adherence 24 (19) 90 (78) <.001 Appropriate fluid mechanism used (pressure bag, rapid-infuser, manual push) Paul, Pediatrics, (49) 110 (95) <
11 Algorithmic Alert Physician Judgement (PJ) Combination Severe Sepsis + Severe Sepsis - Severe Sepsis + 11 Severe Sepsis - Severe Sepsis + Severe Sepsis - Alert ,220 PJ Either ,249 Alert ,216 PJ ,341 Both ,187 Sum 88 19, , ,436 PPV Either Sensitivity Either + 97 Proportion of all patients with a positive screen for potential sepsis algorithmic alerts % (3,301) physician judgment (PJ) - 0.8% (159) combined either positive % (3,334) Balamuth, Acad Emerg Med, 2015


12 2 Step Alert Process Balamuth, Annals of Emerg Med,
13 Balamuth, Annals of Emerg Med,
14 Process measures Sepsis collaborative Outcome measures - sepsis mortality - rapid transfers and bounce backs - initial clinical assessment - timely first and third bolus - timely antibiotics - timely transfer to ICU Balancing measure - false positive rate Supplemental measures - hospital LOS - ICU LOS - days on vasopressors - lab bundle obtained (cbc, lactate, blood cx) 14

15 Creating a Pediatric Sepsis Detection Algorithm Algorithm creation Defining sepsis gold standard 15 Source: Childrens Hospital Photo Exhibit
16 Project Goal Develop an automated sepsis screening tool to alert clinicians of children at risk of severe sepsis Earlier detection more rapid intervention Prevent missed cases 16
17 Partnering with the Vendor Vendor had pre-existing adult sepsis screening tool Not designed for use in children Vendor team Performance improvement strategists Statisticians BCH team Critical care and emergency medicine physicians 17
18 Challenges Difficult to distinguish sepsis from vital signs/labs alone Most detection tools have low specificity High risk of alarm fatigue Sepsis and severe sepsis are not easily defined Gold standard needed to evaluate tool performance Diagnosis codes inaccurate 18
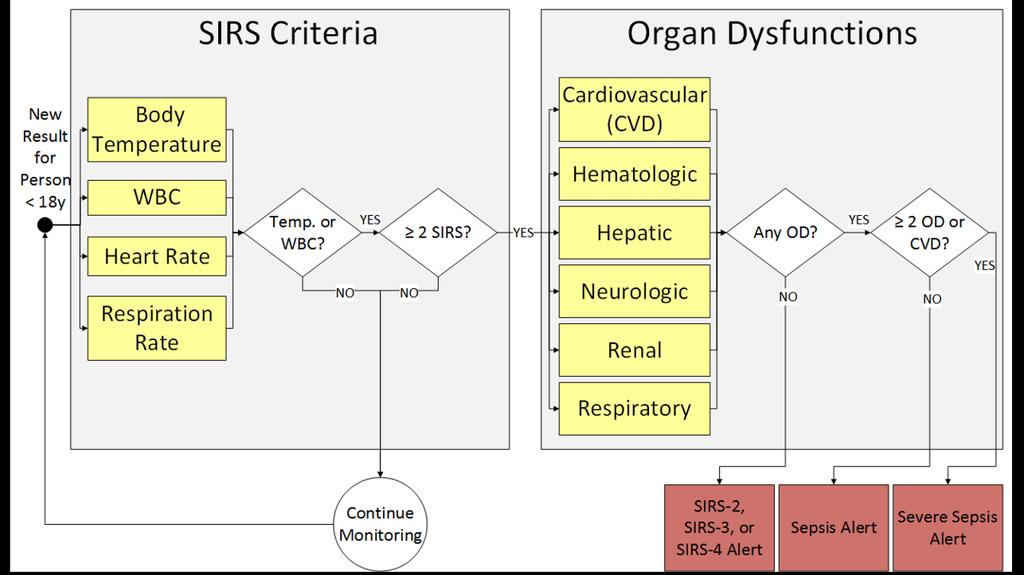
19 Methods Alerts based on accepted vital sign and lab values* for: Systemic inflammatory response syndrome (SIRS) Sepsis Severe sepsis/septic shock Run tool in silent mode for 5 months Compare silent alerts to pre-defined gold standard cohort to assess/maximize tool performance *Goldstein, Pediatr Crit Care Med,
20 Alert Levels: SIRS alert: 2, 3 or 4 SIRS criteria without organ dysfunction Sepsis alert: SIRS with 1 organ dysfunctions (non-cardiac) Suspected infection planned for future eval Severe sepsis: SIRS and cardiac dysfunction or 2 other organ dysfunctions 20
21 21
22 Defining Organ Dysfunction Cardiovascular Organ Dysfunction Sub Algorithms Hypotension or vasoactive drug or 2 of: acidosis, elevated lactate, oliguria, prolonged capillary refill, core peripheral temp gap Respiratory: Hypoxia, hypercarbia, ventilator support Neurologic: Altered mental status Hematologic: Low platelets, elevated INR Renal: Elevated creatinine Hepatic: Elevated bilirubin or ALT 22 Core Body Temp (or Body Temp & Core Route) to Peripheral (or body Temp & Peripheral Route) Gap Body Temperature to Peripheral (or Body Temperature & Peripheral Route) Gap High INR 50% decline in platelet count from highest value over 72 hours (PLATELET_CNT) Low Platelets (PLATELET_CNT) ANC < 500 (NEUTROPHIL_ABSO LUTE_OBSTYPE) High Capillary Refill (CAPILLARY_REFILL_OBSTYPE, CAP_REFILL_OVER_3, CAP_REFILL_UNDER_3) Low Arterial HCO3 (BICARBONATE_ART ERIAL) High Arterial Lactate (LACTIC_ACID) Temperature Gap Pulse Quality (PULSE_QUALITY_A BNORMAL_CLIN) Skin Assessment (PURPURA_CLIN, SKI N_ASSESSMENT_AB NORMAL_CLIN) Hematologic Dysfunction 2 criteria Low Systolic BP (adjusted for age) (SYSTOLIC_BLOOD_P RESSURE) Current administrations of vasoactive drugs High Bilirubin (excluded for age 0-7 days) (BILIRUBIN) High ALT (adjusted for age 0-7 days) (ALT_SER_PLAS) Low Glasgow Coma Score (MENTAL_STAT_CHNG_GLO_COMA, MENTAL_STAT_CHNG_PED_COMA) Decrease in Coma Score of 3 points over 72 Hours (MENTAL_STAT_CHNG_GLO_COMA, MENTAL_STAT_CHNG_PED_COMA) Mental Status identified as Decreased, Irritability, Confusion, inappropriate crying or drowsiness, poor interaction with parents, lethargy, diminished arousability, or obtunded (ALTERED_MENTAL_STATUS_CLIN, IRRITABILITY_CLIN, CONFUSION_CLIN, LETHARGY_CLIN, CRYING_EXCESSIVE_OR_INAPPROPRIATE_CLIN, DROWSINESS_CLIN, OBTUNDED_CLIN) High Creatinine (adjusted for age) (CREATININE) Cardiovascular Dysfunction Creatinine value doubled value lowest value over 72 hours (CREATININE) Low PaO2/FiO2 Exclude in presence of DX: Cyanotic (PaO2, FiO2) heart disease High PaCO2 PaCO2 increase of 20 mmhg 72 Hours High FiO2 (FiO2) Hepatic Dysfunction Neurologic Dysfunction Renal Dysfunction Respiratory Dysfunction
23 Defining gold standard sepsis cohort No single test defines sepsis ICD codes are inaccurate Defined gold standard by clinician intention to treat severe sepsis Also adopted by IPSO sepsis collaborative 23
24 Defining severe sepsis Patient with suspected infection (SI) SEPSIS-3* Criteria: Blood culture within 72 hours before/24 hours after IV antibiotic AND One of the following between 4 hours before and 6 hours after SI 35 cc/kg or 2 L or 2 boluses of isotonic IVF within 2 hours or IV vasopressor or transfer to ICU *Singer, JAMA,
25 Intention to Treat 25
26 Defining severe sepsis To ensure no missed cases, also reviewed all charts of: Patients with diagnosis code for severe sepsis or septic shock Patients who died and had diagnosis code for infectious disease 26
27 Results: Data set All Inpatient and ED encounters over 5 months in ,286 encounters 22,766 unique persons Excluded neonatal ICU Neonatal sepsis is different entity, has different definitions Excluded both alerts and episodes of sepsis that occurred in NICU Exception: patient alerted in another location (e.g. ED) then transferred to NICU 27
28 Results: Gold Standard Cohort 342 patient encounters (1.5%) met gold standard Intention to treat: 335 encounters Severe sepsis diagnosis code: 7 unique encounters Death with infectious disease diagnosis code: 0 unique encounters 28

29 Algorithm Performance Performance of the initial algorithm Iterations to improve performance Final performance characteristics Source: Childrens Hospital Photo Exhibit 29
30 Alert location on patient & encounter level GS alerts = alert within 48 hours of meeting gold standard for sepsis 30

31 Alert by severity level 31
32 Contribution of variables to alerts 32
33 Iterations of algorithm analyzed Goldstein reference ranges Different respiratory rate ranges: No Respiratory Rates 25% and 50% increases in Goldstein RR ref. ranges 25% and 50% increases in Goldstein RR ref. ranges without SIRS-2 alerts Bonafide 75 th, 80 th, 85 th and 90 th percentile RR for ref. range cutoffs Goldstein, Pediatr Crit Care Med, 2005; Bonafide, Pediatrics, Different lookback periods HR AND Temp within 30 minutes of each other Temp. 4h, blood gases 6h, other labs 24h Different SIRS variables No SIRS-2 alerts Restrictive SIRS Different iterations of bands: Immature Granulocytes instead of bands No bands
34 Alternate Vital Sign Criteria Age Groups Goldstein RR Bonafide 75% RR Bonafide 95% RR 0-6 days days month - 1 year years years years Goldstein, Pediatr Crit Care Med, 2005; Bonafide, Pediatrics,
 14.2% 9.7% 7.9% 6.8% 8.")
35 Test Characteristics of Alert Iterations Metric Goldstein Bonafide 75% Bonafide 95% No RR No SIRS-2 Sensitivity 87.7% 83.9% 80.4% 75.4% 79.8% Specificity 86.9% 91.4% 93.2% 94.2% 92.8% PPV 9.2% 13.0% 15.2% 16.5% 14.4% Person Alerts (%) 14.2% 9.7% 7.9% 6.8% 8.3% Goldstein, Pediatr Crit Care Med, 2005; Bonafide, Pediatrics,
36 Unit specific performance Emergency Department Alert Severity # Alerts # Alerted Persons PPV SIRS 1,157 1,085 9% Sepsis % Severe Sepsis % All 1,397 1,213 12% Alert Severity Intensive Care Unit # Alerts # Alerted Persons PPV SIRS % Sepsis % Severe Sepsis % All 1, % PPV in other inpatient services 5% 36

37 Implementation into Clinical Workflows Current state Implementation in the emergency department 37 Source: Childrens Hospital Photo Exhibit

38 Current state of sepsis process Sepsis screening tool Emergency department: embedded in EHR Rest of hospital: paper form Sepsis/septic shock order sets Tracking board icons: ED only Sepsis huddles QI: Education/socialization, PDSA cycles, measurement 38
39 Caution: alert fatigue Children frequently have abnormal vital signs when febrile, scared or in pain Few of these children actually have severe sepsis Most children with severe sepsis are identified by clinicians Added value of alert can be low Risk of alert fatigue is high 39
40 Caution: alert fatigue Recent study of an electronic sepsis surveillance system in an adult ER showed high alert fatigue and no improvement in outcomes Sensitivity of alert 80%; PPV 15% Alert fatigue Only two-thirds of patients with documented sepsis had a clinician respond to the alert >20% of patients with sepsis had a clinician respond that sepsis was not present Austrian, JAMIA,
41 How to reconcile Alerts are important but PPV is low Clinician judgment still necessary Healthy vs. immunocompromised Sick vs. Not sick Solution in BCH ED: 2 stage process SIRS or Sepsis alert secondary screen Severe sepsis alert (higher PPV): sepsis huddle 41
42 Stage 1: Automated Alert +SIRS/SEPSIS ALERT Alert goes to attending, trainee and RN assigned on tracking board No assignment Any RN with relationship 42
43 Stage 2: Active Screening +SIRS/SEPSIS ALERT RN Fills out Sepsis Screen 43
44 Active Screen Link within discern notification to clickable form Question 1: Does patient have fever or do you suspect infection If no form closes If yes answer question 2 Question 2: Does the patient have any of the following: Immuno-compromise or high risk of sepsis (e.g. CVL) Altered mental status Altered pulses/perfusion Positive screen if yes to both questions 44
45 ED sepsis protocol 45

46 Future Directions Project impact and results Version 2 and beyond Source: Childrens Hospital Photo Exhibit 46
47 What s next Continued cycles of improvement Adding to the model to further improve PPV Risk of infection History of chemo order, indwelling lines Suspected infection Microbial test or antimicrobial given Changes in vital signs 47
48 What s next Complete ED implementation and evaluate Prospective study ongoing Outcomes: missed cases, timeliness of interventions, ICU LOS, mortality Test and apply in other venues within the hospital Different rules based on location ICUs vs inpatient surgical vs medical or oncology Different notification and suppression rules 48
49 Thank you BCH Team Elliot Melendez, MD Marvin Harper, MD EMR Team Jeff Christianson, PhD Abbey Logan, Strategist Justin Kimbrell, Sr. Strategist 49
50 Questions Contact Info: Please complete online session evaluation 50
Staging Sepsis for the Emergency Department: Physician
 Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Sepsis Awareness and Education
 Sepsis Awareness and Education Meets the updated New York State Department of Health (NYSDOH) requirements for Infection Control and Barrier Precautions coursework Element VII: Sepsis Awareness and Education
Sepsis Awareness and Education Meets the updated New York State Department of Health (NYSDOH) requirements for Infection Control and Barrier Precautions coursework Element VII: Sepsis Awareness and Education
Sepsis Early Recognition and Management. Therese Hughes, PhD, MPA, RN
 Sepsis Early Recognition and Management Therese Hughes, PhD, MPA, RN 1 Sepsis a Deadly Progression Affects millions around the world each year, killing one in four Contributes to approximately 50% of all
Sepsis Early Recognition and Management Therese Hughes, PhD, MPA, RN 1 Sepsis a Deadly Progression Affects millions around the world each year, killing one in four Contributes to approximately 50% of all
Sepsis 3 & Early Identification. Disclosures. Objectives 9/19/2016. David Carlbom, MD Medical Director, HMC Sepsis Program
 Sepsis 3 & Early Identification David Carlbom, MD Medical Director, HMC Sepsis Program Disclosures I have no relevant financial relationships with a commercial interest and will not discuss off-label use
Sepsis 3 & Early Identification David Carlbom, MD Medical Director, HMC Sepsis Program Disclosures I have no relevant financial relationships with a commercial interest and will not discuss off-label use
SEPSIS UPDATE WHY DO WE NEED A CORE MEASURE CHAD M. KOVALA DO, FACOEP, FACEP
 SEPSIS UPDATE WHY DO WE NEED A CORE MEASURE CHAD M. KOVALA DO, FACOEP, FACEP OBJECTIVES Arise, ProMISE, ProCESS Key points in sepsis management The CMS sepsis core measure COST OF SEPSIS CARE IN US Most
SEPSIS UPDATE WHY DO WE NEED A CORE MEASURE CHAD M. KOVALA DO, FACOEP, FACEP OBJECTIVES Arise, ProMISE, ProCESS Key points in sepsis management The CMS sepsis core measure COST OF SEPSIS CARE IN US Most
NYSDOH Sepsis Q&A Session from February 2018 Data Abstraction Meetings Table of Content
 NYSDOH Sepsis Q&A Session from February 2018 Data Abstraction Meetings Table of Content Adherence variables Q: within 3 hours of the start datetime. How can we document that monotherapy was started before
NYSDOH Sepsis Q&A Session from February 2018 Data Abstraction Meetings Table of Content Adherence variables Q: within 3 hours of the start datetime. How can we document that monotherapy was started before
Core Measures SEPSIS UPDATES
 Patricia Walker, RN-BC, BSN Evidence Based Practice Manager Quality Management Services UCLA Health System, Ronald Reagan Medical Center Core Measures SEPSIS UPDATES Severe Sepsis and Septic Shock Based
Patricia Walker, RN-BC, BSN Evidence Based Practice Manager Quality Management Services UCLA Health System, Ronald Reagan Medical Center Core Measures SEPSIS UPDATES Severe Sepsis and Septic Shock Based
What is sepsis? RECOGNITION. Sepsis I Know It When I See It 9/21/2017
 Sepsis I Know It When I See It September 15, 2017 Matthew Exline, MD MPH Medical Director, Medical ICU What is sepsis? I shall not today attempt further to define the kinds of material [b]ut I know it
Sepsis I Know It When I See It September 15, 2017 Matthew Exline, MD MPH Medical Director, Medical ICU What is sepsis? I shall not today attempt further to define the kinds of material [b]ut I know it
Understand the scope of sepsis morbidity and mortality Identify risk factors that predispose a patient to development of sepsis Define and know the
 Understand the scope of sepsis morbidity and mortality Identify risk factors that predispose a patient to development of sepsis Define and know the differences between sepsis, severe sepsis and septic
Understand the scope of sepsis morbidity and mortality Identify risk factors that predispose a patient to development of sepsis Define and know the differences between sepsis, severe sepsis and septic
SEPSIS SYNDROME
 INTRODUCTION Sepsis has been defined as a life threatening condition that arises when the body s response to an infection injures its own tissues and organs. Sepsis may lead to shock, multiple organ failure
INTRODUCTION Sepsis has been defined as a life threatening condition that arises when the body s response to an infection injures its own tissues and organs. Sepsis may lead to shock, multiple organ failure
2016 Sepsis Update: Pearls, Pitfalls, and Core Measure Quicksand
 2016 Sepsis Update: Pearls, Pitfalls, and Core Measure Quicksand Jack Perkins, MD FACEP, FAAEM, FACP Assistant Professor of Emergency and Internal Medicine Virginia Tech Carilion School of Medicine Why
2016 Sepsis Update: Pearls, Pitfalls, and Core Measure Quicksand Jack Perkins, MD FACEP, FAAEM, FACP Assistant Professor of Emergency and Internal Medicine Virginia Tech Carilion School of Medicine Why
Pediatric Sepsis Treatment:
 Disclosures Pediatric Sepsis Treatment: (treat) Early & (reevaluate) Often None June 11, 2018 Leslie Dervan, MD MS Pacific Northwest Sepsis Conference 1 Agenda Sepsis: pathophysiology at-a-glance Pediatric
Disclosures Pediatric Sepsis Treatment: (treat) Early & (reevaluate) Often None June 11, 2018 Leslie Dervan, MD MS Pacific Northwest Sepsis Conference 1 Agenda Sepsis: pathophysiology at-a-glance Pediatric
Inpatient Quality Reporting Program
 SEP-1 Early Management Bundle, Severe Sepsis/Septic Shock Part III: Measure updates and Abstraction Guidance Questions and Answers Moderator: Candace Jackson, RN Inpatient Quality Reporting (IQR) Program
SEP-1 Early Management Bundle, Severe Sepsis/Septic Shock Part III: Measure updates and Abstraction Guidance Questions and Answers Moderator: Candace Jackson, RN Inpatient Quality Reporting (IQR) Program
SEPSIS: IT ALL BEGINS WITH INFECTION. Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft.
 SEPSIS: IT ALL BEGINS WITH INFECTION Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft. Worth 1 2 3 OBJECTIVES Review the new Sepsis 3 definitions of sepsis
SEPSIS: IT ALL BEGINS WITH INFECTION Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft. Worth 1 2 3 OBJECTIVES Review the new Sepsis 3 definitions of sepsis
Sepsis Bundle Project (SEP) Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: April 2015 Most recent Revision: December 2018
 Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: April 2015 Most recent Revision: December 2018") Sepsis Bundle Project (SEP) Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: April 2015 Most recent Revision: December 2018 Objectives 1. To identify the symptom of severe sepsis and septic shock syndrome.
Sepsis Bundle Project (SEP) Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: April 2015 Most recent Revision: December 2018 Objectives 1. To identify the symptom of severe sepsis and septic shock syndrome.
SURVIVING SEPSIS: Early Management Saves Lives
 SURVIVING SEPSIS: Early Management Saves Lives Pat Posa RN, BSN, MSA System Performance Improvement Leader St. Joseph Mercy Health System Ann Arbor, MI Patricia.posa@stjoeshealth.org Objectives a. Understand
SURVIVING SEPSIS: Early Management Saves Lives Pat Posa RN, BSN, MSA System Performance Improvement Leader St. Joseph Mercy Health System Ann Arbor, MI Patricia.posa@stjoeshealth.org Objectives a. Understand
What the ED clinician needs to know about SEPSIS - 3. Anna Morgan Consultant EM Barts Health
 What the ED clinician needs to know about SEPSIS - 3 Anna Morgan Consultant EM Barts Health Aims: (1) To review the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3) (2)
What the ED clinician needs to know about SEPSIS - 3 Anna Morgan Consultant EM Barts Health Aims: (1) To review the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3) (2)
Effectively Managing Sepsis Denials
 Effectively Managing Sepsis Denials Krysten Brooks, RN, BSN, MBA Senior Inpatient Consultant 3M Health Information Systems This is the Full Title of a Session Atlanta, GA 1 Learning Objectives At the completion
Effectively Managing Sepsis Denials Krysten Brooks, RN, BSN, MBA Senior Inpatient Consultant 3M Health Information Systems This is the Full Title of a Session Atlanta, GA 1 Learning Objectives At the completion
Current State of Pediatric Sepsis. Jason Clayton, MD PhD Pediatric Critical Care 9/19/2018
 Current State of Pediatric Sepsis Jason Clayton, MD PhD Pediatric Critical Care 9/19/2018 Objectives Review the history of pediatric sepsis Review the current definition of pediatric sepsis Review triage
Current State of Pediatric Sepsis Jason Clayton, MD PhD Pediatric Critical Care 9/19/2018 Objectives Review the history of pediatric sepsis Review the current definition of pediatric sepsis Review triage
Sepsis Care and the New Core Measures. Daniel S. Hagg, MD January 15, 2016
 Sepsis Care and the New Core Measures Daniel S. Hagg, MD January 15, 2016 Outline What is sepsis? A brief history of sepsis care How should we take care of septic patients now? Core measures What strategies
Sepsis Care and the New Core Measures Daniel S. Hagg, MD January 15, 2016 Outline What is sepsis? A brief history of sepsis care How should we take care of septic patients now? Core measures What strategies
Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014
 December 17, 2014") Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014 Presenters Mark Blaney, RN Regional Nurse Educator CHI Franciscan Health Karen Lautermilch Director, Quality & Performance
Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014 Presenters Mark Blaney, RN Regional Nurse Educator CHI Franciscan Health Karen Lautermilch Director, Quality & Performance
Sepsis care and the new core measures
 Sepsis care and the new core measures Daniel S. Hagg, MD January 15, 2016 Outline What is sepsis? A brief history of sepsis care How should we take care of septic patients now? Core measures What strategies
Sepsis care and the new core measures Daniel S. Hagg, MD January 15, 2016 Outline What is sepsis? A brief history of sepsis care How should we take care of septic patients now? Core measures What strategies
Septic Shock and Awe. Pediatrics
 Septic Shock and Awe Binita Patel, MD Associate Professor, Baylor College of Medicine, Section of Emergency Medicine Chief of Quality, Pediatric Emergency Medicine Medical Director, Main Campus Aka: She
Septic Shock and Awe Binita Patel, MD Associate Professor, Baylor College of Medicine, Section of Emergency Medicine Chief of Quality, Pediatric Emergency Medicine Medical Director, Main Campus Aka: She
Sepsis is an important issue. Clinician s decision-making capability. Guideline recommendations
 Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012 Clinicians decision-making capability Guideline recommendations Sepsis is an important issue 8.7%
Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012 Clinicians decision-making capability Guideline recommendations Sepsis is an important issue 8.7%
Sepsis 3.0: The Impact on Quality Improvement Programs
 Sepsis 3.0: The Impact on Quality Improvement Programs Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care Warren Alpert Medical School of Brown University
Sepsis 3.0: The Impact on Quality Improvement Programs Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care Warren Alpert Medical School of Brown University
BREAK 11:10-11:
 1. Sepsis Tom Heaps 09:30-10:20 2. Oncological Emergencies Clare Pollard 10:20-11:10 ------------------------ BREAK 11:10-11:30 ------------------------ 3. Diabetic Ketoacidosis Tom Heaps 11:30-12:20 4.
1. Sepsis Tom Heaps 09:30-10:20 2. Oncological Emergencies Clare Pollard 10:20-11:10 ------------------------ BREAK 11:10-11:30 ------------------------ 3. Diabetic Ketoacidosis Tom Heaps 11:30-12:20 4.
PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT
 PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT Melanie Sanchez, RN, MSNE, OCN, CCRN Clinical Nurse III City of Hope National Medical Center HOW THE EXPERTS TREAT HEMATOLOGIC MALIGNANCIES LAS VEGAS, NV
PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT Melanie Sanchez, RN, MSNE, OCN, CCRN Clinical Nurse III City of Hope National Medical Center HOW THE EXPERTS TREAT HEMATOLOGIC MALIGNANCIES LAS VEGAS, NV
IDENTIFYING SEPSIS IN THE PREHOSPITAL SETTING
 IDENTIFYING SEPSIS IN THE PREHOSPITAL SETTING Christopher Hunter, MD, PhD, FACEP Director, Health Services Department Associate Medical Director, Orange County EMS System Medical Director, Orlando Health
IDENTIFYING SEPSIS IN THE PREHOSPITAL SETTING Christopher Hunter, MD, PhD, FACEP Director, Health Services Department Associate Medical Director, Orange County EMS System Medical Director, Orlando Health
Sepsis as Seen by the CMO. Randy C. Roth, MD Chief Medical Officer
 Sepsis as Seen by the CMO Randy C. Roth, MD Chief Medical Officer 1 Challenges of Sepsis Sepsis, like many disease processes, is much more than a clinical challenge. For Hospitalists, we are treating the
Sepsis as Seen by the CMO Randy C. Roth, MD Chief Medical Officer 1 Challenges of Sepsis Sepsis, like many disease processes, is much more than a clinical challenge. For Hospitalists, we are treating the
Sepsis-3: clarity or confusion
 Sepsis-3: clarity or confusion Christopher W. Seymour, MD MSc The CRISMA Center Assistant Professor of Critical Care Medicine & Emergency Medicine University of Pittsburgh School of Medicine Can an otherwise
Sepsis-3: clarity or confusion Christopher W. Seymour, MD MSc The CRISMA Center Assistant Professor of Critical Care Medicine & Emergency Medicine University of Pittsburgh School of Medicine Can an otherwise
Inpatient Quality Reporting Program
 SEP-1 Early Management Bundle, Severe Sepsis/Septic Shock Part II Questions and Answers Moderator: Candace Jackson, RN Inpatient Quality Reporting (IQR) Program Lead Hospital Inpatient Value, Incentives,
SEP-1 Early Management Bundle, Severe Sepsis/Septic Shock Part II Questions and Answers Moderator: Candace Jackson, RN Inpatient Quality Reporting (IQR) Program Lead Hospital Inpatient Value, Incentives,
OHSU. Update in Sepsis
 Update in Sepsis Jonathan Pak, MD June 1, 2017 Structure of Talk 1. Sepsis-3: The latest definition 2. Clinical Management - Is EGDT dead? - Surviving Sepsis Campaign Guidelines 3. A novel therapy: Vitamin
Update in Sepsis Jonathan Pak, MD June 1, 2017 Structure of Talk 1. Sepsis-3: The latest definition 2. Clinical Management - Is EGDT dead? - Surviving Sepsis Campaign Guidelines 3. A novel therapy: Vitamin
R2R: Severe sepsis/septic shock. Surat Tongyoo Critical care medicine Siriraj Hospital
 R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
Pediatric Emergency Preparedness Training Seminar: NY State Sepsis Initiative Update May 24 th, 2017
 Pediatric Emergency Preparedness Training Seminar: NY State Sepsis Initiative Update May 24 th, 2017 Marcus Friedrich, MD, MBA, FACP Medical Director Office of Quality and Patient Safety NYSDOH Marcus.Friedrich@health.ny.gov
Pediatric Emergency Preparedness Training Seminar: NY State Sepsis Initiative Update May 24 th, 2017 Marcus Friedrich, MD, MBA, FACP Medical Director Office of Quality and Patient Safety NYSDOH Marcus.Friedrich@health.ny.gov
The Septic Patient. Dr Arunraj Navaratnarajah. Renal SpR Imperial College NHS Healthcare Trust
 The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
Initial Resuscitation of Sepsis & Septic Shock
 Initial Resuscitation of Sepsis & Septic Shock Dr. Fatema Ahmed MD (Critical Care Medicine) FCPS (Medicine) Associate professor Dept. of Critical Care Medicine BIRDEM General Hospital Is Sepsis a known
Initial Resuscitation of Sepsis & Septic Shock Dr. Fatema Ahmed MD (Critical Care Medicine) FCPS (Medicine) Associate professor Dept. of Critical Care Medicine BIRDEM General Hospital Is Sepsis a known
The changing face of
 The changing face of sepsis. @SepsisUK Dr Ron Daniels B.E.M. CEO, UK Sepsis Trust CEO, Global Sepsis Alliance Special Adviser (maternal sepsis) to WHO Breast cancer Cognitive impairment Mild 3.8 7.1
The changing face of sepsis. @SepsisUK Dr Ron Daniels B.E.M. CEO, UK Sepsis Trust CEO, Global Sepsis Alliance Special Adviser (maternal sepsis) to WHO Breast cancer Cognitive impairment Mild 3.8 7.1
Sepsis. From EMS to ER to ICU. What we need to be doing
 Sepsis From EMS to ER to ICU What we need to be doing NEHAL BHATT, MD ATHENS PULMONARY, CRITICAL CARE AND SLEEP Objectives 1. Define the changes to the definition of Sepsis 2. Describe the assessment,
Sepsis From EMS to ER to ICU What we need to be doing NEHAL BHATT, MD ATHENS PULMONARY, CRITICAL CARE AND SLEEP Objectives 1. Define the changes to the definition of Sepsis 2. Describe the assessment,
4/5/2018. Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY. I have no financial disclosures
 Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY I have no financial disclosures 1 Objectives Why do we care about sepsis Understanding the core measures by Centers for Medicare
Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY I have no financial disclosures 1 Objectives Why do we care about sepsis Understanding the core measures by Centers for Medicare
Sepsis or Severe Sepsis? Is there a right thing, and how do we do it?
 Sepsis or Severe Sepsis? Is there a right thing, and how do we do it? Steven Q Simpson, MD, FCCP, FACP Professor of Medicine Division of Pulmonary and Critical Care University of Kansas Disclosures No
Sepsis or Severe Sepsis? Is there a right thing, and how do we do it? Steven Q Simpson, MD, FCCP, FACP Professor of Medicine Division of Pulmonary and Critical Care University of Kansas Disclosures No
John Park, MD Assistant Professor of Medicine
 John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
Updates On Sepsis Updates based on 2016 updates on sepsis from The International Surviving Sepsis Campaign
 Updates On Sepsis Updates based on 2016 updates on sepsis from The International Surviving Sepsis Campaign Dr. Joseph K Erbe, DO Medical Director Hospitalist Division of Medicine Objectives 1. Review the
Updates On Sepsis Updates based on 2016 updates on sepsis from The International Surviving Sepsis Campaign Dr. Joseph K Erbe, DO Medical Director Hospitalist Division of Medicine Objectives 1. Review the
Sepsis Update: Focus on Early Recognition and Intervention. Disclosures
 Sepsis Update: Focus on Early Recognition and Intervention Jessie Roske, MD October 2017 Disclosures I have no actual or potential conflict of interest in relation to this program/presentation. I will
Sepsis Update: Focus on Early Recognition and Intervention Jessie Roske, MD October 2017 Disclosures I have no actual or potential conflict of interest in relation to this program/presentation. I will
Example Clinician Educational Material for Providers of Immune Effector Cellular Therapy
 Example Clinician Educational Material for Providers of Immune Effector Cellular Therapy Disclaimer: This example is just one of many potential examples of clinician education material that can be provided
Example Clinician Educational Material for Providers of Immune Effector Cellular Therapy Disclaimer: This example is just one of many potential examples of clinician education material that can be provided
SEPSIS & SEPTIC SHOCK
 SEPSIS & SEPTIC SHOCK DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none Steps taken to review and mitigate potential bias
SEPSIS & SEPTIC SHOCK DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none Steps taken to review and mitigate potential bias
Inpatient Quality Reporting (IQR) Program
 Program") Hypotension Inpatient Quality Reporting (IQR) Program SEP-1 Early Management Bundle, Severe Sepsis/ Septic Shock: v5.1 Measure Updates Questions and Answers Moderator: Candace Jackson, RN Project Lead,
Hypotension Inpatient Quality Reporting (IQR) Program SEP-1 Early Management Bundle, Severe Sepsis/ Septic Shock: v5.1 Measure Updates Questions and Answers Moderator: Candace Jackson, RN Project Lead,
Sepsis: Identification and Management in an Acute Care Setting
 Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Communicable Diseases EMT REFRESHER NCCP 2018 JTEMPLE
 Communicable Diseases EMT REFRESHER NCCP 2018 JTEMPLE When are Standard Precautions used? The use of Standard Precautions during patient care is determined by the nature of the anticipated interaction
Communicable Diseases EMT REFRESHER NCCP 2018 JTEMPLE When are Standard Precautions used? The use of Standard Precautions during patient care is determined by the nature of the anticipated interaction
Fluid Resuscitation and Monitoring in Sepsis. Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS
 Fluid Resuscitation and Monitoring in Sepsis Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS Learning Objectives Compare and contrast fluid resuscitation strategies in septic shock Discuss available
Fluid Resuscitation and Monitoring in Sepsis Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS Learning Objectives Compare and contrast fluid resuscitation strategies in septic shock Discuss available
Sepsis: Management ANUPOL PANITCHOTE, MD. Division of Critical Care Medicine Department of Medicine, Khon Kaen University, Thailand
 Sepsis: Management ANUPOL PANITCHOTE, MD. Division of Critical Care Medicine Department of Medicine, Khon Kaen University, Thailand Vital signs Symptoms LAB BT > 38.3 or < 36 ๐ C HR > 90 bpm RR > 20 /min
Sepsis: Management ANUPOL PANITCHOTE, MD. Division of Critical Care Medicine Department of Medicine, Khon Kaen University, Thailand Vital signs Symptoms LAB BT > 38.3 or < 36 ๐ C HR > 90 bpm RR > 20 /min
Sepsis Story At Intermountain Healthcare Intensive Medicine Clinical Program
 Sepsis Story At Intermountain Healthcare 2004-2012 Intensive Medicine Clinical Program The International Surviving Sepsis Campaign Was Organized In 2002 During The ESICM International Meeting In Barcelona,
Sepsis Story At Intermountain Healthcare 2004-2012 Intensive Medicine Clinical Program The International Surviving Sepsis Campaign Was Organized In 2002 During The ESICM International Meeting In Barcelona,
3 papers from ED. counting sepsis sepsis 3 wet or dry?
 3 papers from ED counting sepsis sepsis 3 wet or dry? 5 million deaths/yr globally 24 billion USD annually in US system causes or contributes to half of US hospital deaths BP GCS RR From: The Third International
3 papers from ED counting sepsis sepsis 3 wet or dry? 5 million deaths/yr globally 24 billion USD annually in US system causes or contributes to half of US hospital deaths BP GCS RR From: The Third International
Critical Care Treatment Guidelines
 Critical Care Treatment Guidelines West Virginia Office of Emergency Medical Services CCT Guidelines CCT Guidelines TABLE OF CONTENTS Preface Acknowledgments Using the Guidelines INITIAL TREATMENT / UNIVERSAL
Critical Care Treatment Guidelines West Virginia Office of Emergency Medical Services CCT Guidelines CCT Guidelines TABLE OF CONTENTS Preface Acknowledgments Using the Guidelines INITIAL TREATMENT / UNIVERSAL
Inflammatory Statements
 Inflammatory Statements Using ETCO 2 Analysis in Sepsis Syndromes George A. Ralls M.D. Orange County EMS System Sepsis Sepsis Over 750,000 cases annually Expected growth of 1.5% per year Over 215,000 deaths
Inflammatory Statements Using ETCO 2 Analysis in Sepsis Syndromes George A. Ralls M.D. Orange County EMS System Sepsis Sepsis Over 750,000 cases annually Expected growth of 1.5% per year Over 215,000 deaths
Tailored Volume Resuscitation in the Critically Ill is Achievable. Objectives. Clinical Case 2/16/2018
 Tailored Volume Resuscitation in the Critically Ill is Achievable Heath E Latham, MD Associate Professor Fellowship Program Director Pulmonary and Critical Care Objectives Describe the goal of resuscitation
Tailored Volume Resuscitation in the Critically Ill is Achievable Heath E Latham, MD Associate Professor Fellowship Program Director Pulmonary and Critical Care Objectives Describe the goal of resuscitation
Objectives. Epidemiology of Sepsis. Review Guidelines for Resuscitation. Tx: EGDT, timing/choice of abx, activated
 Update on Surviving Sepsis 2008 Objectives Epidemiology of Sepsis Definition of Sepsis and Septic Shock Review Guidelines for Resuscitation Dx: Lactate, t cultures, SVO2 Tx: EGDT, timing/choice of abx,
Update on Surviving Sepsis 2008 Objectives Epidemiology of Sepsis Definition of Sepsis and Septic Shock Review Guidelines for Resuscitation Dx: Lactate, t cultures, SVO2 Tx: EGDT, timing/choice of abx,
Admissions with severe sepsis in adult, general critical care units in England, Wales and Northern Ireland
 Admissions with severe sepsis in adult, general critical care units in England, Wales and Northern Ireland Question For all admissions to adult, general critical care units in the Case Mix Programme Database
Admissions with severe sepsis in adult, general critical care units in England, Wales and Northern Ireland Question For all admissions to adult, general critical care units in the Case Mix Programme Database
Early-goal-directed therapy and protocolised treatment in septic shock
 CAT reviews Early-goal-directed therapy and protocolised treatment in septic shock Journal of the Intensive Care Society 2015, Vol. 16(2) 164 168! The Intensive Care Society 2014 Reprints and permissions:
CAT reviews Early-goal-directed therapy and protocolised treatment in septic shock Journal of the Intensive Care Society 2015, Vol. 16(2) 164 168! The Intensive Care Society 2014 Reprints and permissions:
Using Big Data to Prevent Infections
 Using Big Data to Prevent Infections A thought paper by Scalable Health Big Data Analytics Reduces Infections in Hospitals Healthcare Associated Infections (HAIs) are developed while patients are receiving
Using Big Data to Prevent Infections A thought paper by Scalable Health Big Data Analytics Reduces Infections in Hospitals Healthcare Associated Infections (HAIs) are developed while patients are receiving
SUCCESS IN SEPSIS MORTALITY REDUCTION. Maryanne Whitney RN MSN CNS Improvement Advisor, Cynosure Health HRET HEN AK Webinar
 SUCCESS IN SEPSIS MORTALITY REDUCTION Maryanne Whitney RN MSN CNS Improvement Advisor, Cynosure Health HRET HEN AK Webinar Got Sepsis? Now What?- Alerts & Bundles Maryanne Whitney RN, MS, CNS Improvement
SUCCESS IN SEPSIS MORTALITY REDUCTION Maryanne Whitney RN MSN CNS Improvement Advisor, Cynosure Health HRET HEN AK Webinar Got Sepsis? Now What?- Alerts & Bundles Maryanne Whitney RN, MS, CNS Improvement
Early Recognition and Timely Management of Sepsis Amid Changes in Definitions
 Early Recognition and Timely Management of Sepsis Amid Changes in Definitions Tze Shien Lo, MD, FACP Chief, Infectious Disease Service Fargo VA Medical Center Professor of Medicine UND School of Medicine
Early Recognition and Timely Management of Sepsis Amid Changes in Definitions Tze Shien Lo, MD, FACP Chief, Infectious Disease Service Fargo VA Medical Center Professor of Medicine UND School of Medicine
Nothing to disclose 9/25/2017
 Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Nothing to disclose 1 Explain
Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Nothing to disclose 1 Explain
Is nosocomial infection the major cause of death in sepsis?
 Is nosocomial infection the major cause of death in sepsis? Warren L. Lee, MD PhD, FRCPC Department of Medicine University of Toronto There are no specific therapies for sepsis the graveyard for pharmaceutical
Is nosocomial infection the major cause of death in sepsis? Warren L. Lee, MD PhD, FRCPC Department of Medicine University of Toronto There are no specific therapies for sepsis the graveyard for pharmaceutical
BC Sepsis Network Emergency Department Sepsis Guidelines
 The provincial Sepsis Clinical Expert Group developed the BC, taking into account the most up-to-date literature (references below) and expert opinion. For more information about the guidelines, and to
The provincial Sepsis Clinical Expert Group developed the BC, taking into account the most up-to-date literature (references below) and expert opinion. For more information about the guidelines, and to
9/25/2017. Nothing to disclose
 Nothing to disclose Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Explain
Nothing to disclose Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Explain
Andrea Blotsky MDCM FRCPC General Internal Medicine, McGill University Thursday, October 15, 2015
 The TIMES Project: (Time to Initiation of Antibiotic Therapy in Medical Patients Presenting to the Emergency Department with Sepsis) - Preliminary Findings Andrea Blotsky MDCM FRCPC General Internal Medicine,
The TIMES Project: (Time to Initiation of Antibiotic Therapy in Medical Patients Presenting to the Emergency Department with Sepsis) - Preliminary Findings Andrea Blotsky MDCM FRCPC General Internal Medicine,
Troubleshooting Audio
 Welcome! Audio for this event is available via ReadyTalk Internet Streaming. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming audio. Limited dial-in lines
Welcome! Audio for this event is available via ReadyTalk Internet Streaming. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming audio. Limited dial-in lines
SHOCK. Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital
 SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
Inpatient Quality Reporting (IQR) Program
 Program") The Clinician Perspective on Sepsis Care: Early Management Bundle for Severe Sepsis/Septic Shock Questions & Answers Moderator Candace Jackson, RN Project Lead, Hospital Inpatient Quality Reporting (IQR)
The Clinician Perspective on Sepsis Care: Early Management Bundle for Severe Sepsis/Septic Shock Questions & Answers Moderator Candace Jackson, RN Project Lead, Hospital Inpatient Quality Reporting (IQR)
Immunomodulation and Sepsis in Oncological Patients. Imad Haddad, M.D. Medical Director, PICU Banner Children s Hospital at BDMC
 Immunomodulation and Sepsis in Oncological Patients Imad Haddad, M.D. Medical Director, PICU Banner Children s Hospital at BDMC 1 Objectives Immune dys-regulation in oncological septic patients Implementation
Immunomodulation and Sepsis in Oncological Patients Imad Haddad, M.D. Medical Director, PICU Banner Children s Hospital at BDMC 1 Objectives Immune dys-regulation in oncological septic patients Implementation
Sepsis and Septicemia: Clear up Coding and Documentation Confusion october 2009
 Sepsis and Septicemia: Clear Up Coding and Documentation Confusion W h i t e p a p e r Sepsis. Severe sepsis. SIRS. Septicemia. Unfortunately, this isn t a case of tomato, tomahto. Coders and physicians
Sepsis and Septicemia: Clear Up Coding and Documentation Confusion W h i t e p a p e r Sepsis. Severe sepsis. SIRS. Septicemia. Unfortunately, this isn t a case of tomato, tomahto. Coders and physicians
Update on Sepsis Diagnosis and Management
 CHAPTER 12 Update on Sepsis Diagnosis and Management Kevin Alexander, DPM INTRODUCTION Sepsis and septic shock have become a large problem in the health care system that affects at least 1 million people
CHAPTER 12 Update on Sepsis Diagnosis and Management Kevin Alexander, DPM INTRODUCTION Sepsis and septic shock have become a large problem in the health care system that affects at least 1 million people
Frank Sebat, MD - June 29, 2006
 Types of Shock Hypovolemic Shock Low blood volume decreasing cardiac output. AN INTEGRATED SYSTEM OF CARE FOR PATIENTS AT RISK SHOCK TEAM and RAPID RESPONSE TEAM Septic or Distributive Shock Decrease in
Types of Shock Hypovolemic Shock Low blood volume decreasing cardiac output. AN INTEGRATED SYSTEM OF CARE FOR PATIENTS AT RISK SHOCK TEAM and RAPID RESPONSE TEAM Septic or Distributive Shock Decrease in
Sepsis. Current Dilemmas in Diagnosing Sepsis. Chapter 2
 Chapter 2 Current Dilemmas in Diagnosing Derek Braun Derek Braun, Banner Health, 2901 N. Central Ave. Ste 180, Phoenix, AZ 85012 Email: derek.braun@bannerhealth.com Abbreviations: APACHE : Acute Physiology,
Chapter 2 Current Dilemmas in Diagnosing Derek Braun Derek Braun, Banner Health, 2901 N. Central Ave. Ste 180, Phoenix, AZ 85012 Email: derek.braun@bannerhealth.com Abbreviations: APACHE : Acute Physiology,
Sepsis: Mitigating Denials Amid Definition Disparity
 Sepsis: Mitigating Denials Amid Definition Disparity White Paper - April 2017 Sepsis Criteria at a Glance The Society of Critical Care Medicine (SCCM) met in 2016 to update the definition of sepsis. During
Sepsis: Mitigating Denials Amid Definition Disparity White Paper - April 2017 Sepsis Criteria at a Glance The Society of Critical Care Medicine (SCCM) met in 2016 to update the definition of sepsis. During
Sepsis in primary care. what is good care?
 Sepsis in primary care @SepsisUK what is good care? Emmanuel Nsutebu Consultant Infectious Disease Physician & Clinical lead for sepsis Tropical and Infectious Disease Unit Royal Liverpool Hospital Do
Sepsis in primary care @SepsisUK what is good care? Emmanuel Nsutebu Consultant Infectious Disease Physician & Clinical lead for sepsis Tropical and Infectious Disease Unit Royal Liverpool Hospital Do
12/12/2017. Notice. Sepsis is defined as life-threatening organ dysfunction due to a dysregulated host response to infection.
 Notice All EMS Live@Nite presentations will be recorded (both audio and video) and available for public viewing online. By participating in EMS Live@Nite, you consent to audio and video recording and its/their
Notice All EMS Live@Nite presentations will be recorded (both audio and video) and available for public viewing online. By participating in EMS Live@Nite, you consent to audio and video recording and its/their
IV fluid administration in sepsis. Dr David Inwald Consultant in PICU St Mary s Hospital, London CATS, London
 IV fluid administration in sepsis Dr David Inwald Consultant in PICU St Mary s Hospital, London CATS, London The talk What is septic shock? What are the recommendations? What is the evidence? Do we follow
IV fluid administration in sepsis Dr David Inwald Consultant in PICU St Mary s Hospital, London CATS, London The talk What is septic shock? What are the recommendations? What is the evidence? Do we follow
Septic Shock. Rontgene M. Solante, MD, FPCP,FPSMID
 Septic Shock Rontgene M. Solante, MD, FPCP,FPSMID Learning Objectives Identify situations wherein high or low BP are hemodynamically significant Recognize complications arising from BP emergencies Manage
Septic Shock Rontgene M. Solante, MD, FPCP,FPSMID Learning Objectives Identify situations wherein high or low BP are hemodynamically significant Recognize complications arising from BP emergencies Manage
Hospital Inpatient Quality Reporting (IQR) Program
 Program") SEP-1 Early Management Bundle, Severe Sepsis/Septic Shock: v5.3a Measure Updates Questions and Answers Speaker Noel Albritton, RN, BS Lead Solutions Specialist Hospital Inpatient and Outpatient Process
SEP-1 Early Management Bundle, Severe Sepsis/Septic Shock: v5.3a Measure Updates Questions and Answers Speaker Noel Albritton, RN, BS Lead Solutions Specialist Hospital Inpatient and Outpatient Process
Key Points. Angus DC: Crit Care Med 29:1303, 2001
 Sepsis Key Points Sepsis is the combination of a known or suspected infection and an accompanying systemic inflammatory response (SIRS) Severe sepsis is sepsis with acute dysfunction of one or more organ
Sepsis Key Points Sepsis is the combination of a known or suspected infection and an accompanying systemic inflammatory response (SIRS) Severe sepsis is sepsis with acute dysfunction of one or more organ
EFFECT OF EARLY VASOPRESSIN VS NOREPINEPHRINE ON KIDNEY FAILURE IN PATIENTS WITH SEPTIC SHOCK. Alexandria Rydz
 EFFECT OF EARLY VASOPRESSIN VS NOREPINEPHRINE ON KIDNEY FAILURE IN PATIENTS WITH SEPTIC SHOCK Alexandria Rydz BACKGROUND- SEPSIS Sepsis is defined as life-threatening organ dysfunction caused by a dysregulated
EFFECT OF EARLY VASOPRESSIN VS NOREPINEPHRINE ON KIDNEY FAILURE IN PATIENTS WITH SEPTIC SHOCK Alexandria Rydz BACKGROUND- SEPSIS Sepsis is defined as life-threatening organ dysfunction caused by a dysregulated
Sepsis and Septic Shock: New Definitions for Adults
 PL Detail-Document #320424 This PL Detail-Document gives subscribers additional insight related to the Recommendations published in PHARMACIST S LETTER / PRESCRIBER S LETTER April 2016 Sepsis and Septic
PL Detail-Document #320424 This PL Detail-Document gives subscribers additional insight related to the Recommendations published in PHARMACIST S LETTER / PRESCRIBER S LETTER April 2016 Sepsis and Septic
Evidence- Based Medicine Fluid Therapy
 Evidence- Based Medicine Fluid Therapy Ndidi Musa M.D. Assosciate Professor of Pediatrics Medical College of Wisconsin/ Children s Hospital of Wisconsin Disclosures A. I have no relevant financial relationships
Evidence- Based Medicine Fluid Therapy Ndidi Musa M.D. Assosciate Professor of Pediatrics Medical College of Wisconsin/ Children s Hospital of Wisconsin Disclosures A. I have no relevant financial relationships
Sepsis Denials. Presented by James Donaher, RHIA, CDIP, CCS, CCS-P
 Sepsis Denials Presented by James Donaher, RHIA, CDIP, CCS, CCS-P Sepsis-1 2 From the first Sepsis Definition Conference in 1991 Defined sepsis as systemic response syndrome (SIRS) due to infection SIRS
Sepsis Denials Presented by James Donaher, RHIA, CDIP, CCS, CCS-P Sepsis-1 2 From the first Sepsis Definition Conference in 1991 Defined sepsis as systemic response syndrome (SIRS) due to infection SIRS
APACHE II: A Severity of Disease Classification System Standard Operating Procedure for Accurate Calculations
 BACKGROUND APACHE II: A Severity of Disease Classification System Standard Operating Procedure for Accurate Calculations The APACHE prognostic scoring system was developed in 1981 at the George Washington
BACKGROUND APACHE II: A Severity of Disease Classification System Standard Operating Procedure for Accurate Calculations The APACHE prognostic scoring system was developed in 1981 at the George Washington
Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University
 Dr Mubarak Abdelrahman Assistant Professor Jazan University") Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University SHOCK Definition: Shock is a syndrome = inability to provide sufficient oxygenated blood to tissues. Oxygen
Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University SHOCK Definition: Shock is a syndrome = inability to provide sufficient oxygenated blood to tissues. Oxygen
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016
 Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
SEP-1 CHALLENGING CASES WITH DR. TOWNSEND
 UW MEDICINE PATIENTS ARE FIRST SEP-1 CHALLENGING CASES WITH DR. TOWNSEND AMADAE AREVALO RN, MSN, CCRN KATIE MEHRING RN, BSN, CCDS AMANDA SIGALA, RN, BSN, MPH, CPHQ JUNE 12, 2018 OBJECTIVES 1. Summarize
UW MEDICINE PATIENTS ARE FIRST SEP-1 CHALLENGING CASES WITH DR. TOWNSEND AMADAE AREVALO RN, MSN, CCRN KATIE MEHRING RN, BSN, CCDS AMANDA SIGALA, RN, BSN, MPH, CPHQ JUNE 12, 2018 OBJECTIVES 1. Summarize
The Artificial Intelligence Clinician learns optimal treatment strategies for sepsis in intensive care
 SUPPLEMENTARY INFORMATION Articles https://doi.org/10.1038/s41591-018-0213-5 In the format provided by the authors and unedited. The Artificial Intelligence Clinician learns optimal treatment strategies
SUPPLEMENTARY INFORMATION Articles https://doi.org/10.1038/s41591-018-0213-5 In the format provided by the authors and unedited. The Artificial Intelligence Clinician learns optimal treatment strategies
Pediatric Diabetic Ketoacidosis (DKA) General Pediatrics Admission Order Set
 General Pediatrics Admission Order Set") Admitting MRP: Pediatrics: Dr. / Dr. on call to cover until 08:00 am Service: Medicine Team 1 Medicine Team 2 Medical subspecialty Diagnosis: Diabetic Ketoacidosis (DKA) Estimated length of stay Less than
Admitting MRP: Pediatrics: Dr. / Dr. on call to cover until 08:00 am Service: Medicine Team 1 Medicine Team 2 Medical subspecialty Diagnosis: Diabetic Ketoacidosis (DKA) Estimated length of stay Less than
Diagnosis and Management of Sepsis. Disclosures
 Diagnosis and Management of Sepsis David Shimabukuro, MDCM Medical Director, 13 ICU Physician Lead, UCSF Sepsis Bundle Compliance and Mortality Reduction I have no disclosures Disclosures 1 The following
Diagnosis and Management of Sepsis David Shimabukuro, MDCM Medical Director, 13 ICU Physician Lead, UCSF Sepsis Bundle Compliance and Mortality Reduction I have no disclosures Disclosures 1 The following
Approach to Severe Sepsis. Jan Hau Lee, MBBS, MRCPCH. MCI Children s Intensive Care Unit KK Women s and Children's Hospital, Singapore
 Approach to Severe Sepsis Jan Hau Lee, MBBS, MRCPCH. MCI Children s Intensive Care Unit KK Women s and Children's Hospital, Singapore 1 2 No conflict of interest Overview Epidemiology of Pediatric Severe
Approach to Severe Sepsis Jan Hau Lee, MBBS, MRCPCH. MCI Children s Intensive Care Unit KK Women s and Children's Hospital, Singapore 1 2 No conflict of interest Overview Epidemiology of Pediatric Severe
SEPSIS: GETTING STARTED
 SEPSIS: GETTING STARTED Ohio Sepsis Initiative July 15, 2015 SEPSIS INCIDENCE Definition: the number of severe sepsis or septic shock encounters using the following ICD-9 codes (995.91 Sepsis, 995.92 severe
SEPSIS: GETTING STARTED Ohio Sepsis Initiative July 15, 2015 SEPSIS INCIDENCE Definition: the number of severe sepsis or septic shock encounters using the following ICD-9 codes (995.91 Sepsis, 995.92 severe
Stayin Alive: Pediatric Advanced Life Support (PALS) Updated Guidelines
 Updated Guidelines") Stayin Alive: Pediatric Advanced Life Support (PALS) Updated Guidelines Margaret Oates, PharmD, BCPPS Pediatric Critical Care Specialist GSHP Summer Meeting July 16, 2016 Disclosures I have nothing to
Stayin Alive: Pediatric Advanced Life Support (PALS) Updated Guidelines Margaret Oates, PharmD, BCPPS Pediatric Critical Care Specialist GSHP Summer Meeting July 16, 2016 Disclosures I have nothing to
The Oxford AHSN Sepsis Pathway
 From confusion to consensus: The Oxford AHSN Sepsis Pathway Andrew Brent Sepsis Clinical Lead, Oxford AHSN & Oxford University Hospitals NHS Foundation Trust 2013 2014 2015 2016 2017 From: The Third International
From confusion to consensus: The Oxford AHSN Sepsis Pathway Andrew Brent Sepsis Clinical Lead, Oxford AHSN & Oxford University Hospitals NHS Foundation Trust 2013 2014 2015 2016 2017 From: The Third International
Use of Blood Lactate Measurements in the Critical Care Setting
 Use of Blood Lactate Measurements in the Critical Care Setting John G Toffaletti, PhD Director of Blood Gas and Clinical Pediatric Labs Professor of Pathology Duke University Medical Center Chief, VAMC
Use of Blood Lactate Measurements in the Critical Care Setting John G Toffaletti, PhD Director of Blood Gas and Clinical Pediatric Labs Professor of Pathology Duke University Medical Center Chief, VAMC
Sepsis Update Allina Critical Care Conference February 28, 2018
 Sepsis Update Allina Critical Care Conference February 28, 2018 Sandy Fritzlar, MD Medical Director of the Allina Sepsis Program Emergency Care Consultants OBJECTIVES A brief HISTORY of Sepsis Understand
Sepsis Update Allina Critical Care Conference February 28, 2018 Sandy Fritzlar, MD Medical Director of the Allina Sepsis Program Emergency Care Consultants OBJECTIVES A brief HISTORY of Sepsis Understand