Renee Flores, MD Division of Geriatrics & Palliative Medicine Department of Internal Medicine
|
|
|
- Melissa Washington
- 5 years ago
- Views:
Transcription

1 Renee Flores, MD Division of Geriatrics & Palliative Medicine Department of Internal Medicine
2
3
4 Define AMS and delirium Describe how to recognize and diagnose delirium Identify the predisposing or precipitating risk factors for delirium in elderly patients Demonstrate how to evaluate and treat elderly patients with delirium Evaluate and apply interventions to prevent delirium
5 Approx. ⅓ of pts. 70 years old admitted to the medicine service experience delirium: ½ of these are delirious on admission while other ½ develop delirium in the hospital. A systematic review found that persistence rates for delirium at hospital D/C and at 1, 3 and 6 months after D/C were 45%, 33%, 26% and 21%, respectively. In SNF, approx. 15% of new admissions meet criteria for delirium.
6 Literature shows that when delirium persists beyond 6 months, it is likely that the patient will have cognitive decline, resulting condition could be dementia/mild cognitive impairment (MCI), depending on its severity. A meta-analysis of 3,000 patients followed for a mean of 22.7 months found that delirium was independently associated with an increased risk of death (OR 2.0; 95% CI ), institutionalization (OR 2.4; 95% CI ) dementia (OR 12.5; 95% CI ).
7 Under-recognition of delirium is a major problem, with only 12%-35% of all cases recognized in routine care. CAM is the most useful bedside assessment tool for delirium. 4 key features of CAM are: Acute change or fluctuating course Inattention Disorganized thinking Altered level of consciousness
8
9 SAS Score
10 Underlying co-morbid conditions must be taken into account Depression can sometimes be confused with hypoactive delirium and mania with hyperactive delirium. Hyperactive delirium accounts for only 25% of cases with the remaining being hypoactive quiet delirium. Hypoactive delirium is associated with an equal or poorer prognosis than delirium with hyperactive or normal psychomotor features.
11 One of the best documented mechanism is cholinergic deficiency. This is classically seen in overdoses of anticholinergic medications like atropine. A second potential mechanism is inflammation, seen classically in post-op patients and in those with cancer or infection. Literature shows an association of delirium with increased levels of CRP, IL-1, IL-6 and TNF-α. Inflammation can break the blood-brain barrier allowing toxic medications and cytokines greater access to the CNS.
12 Can be classified into 2 groups: baseline factors that predispose patients to delirium and acute factors that precipitate delirium. Baseline factors: Advanced age Preexisting dementia Preexisting functional impairment in ADL Male gender Sensory impairment (hearing and visual loss) Depressive symptoms Medical comorbidity

13 Acute precipitating factors: Medications (most common) Surgery Uncontrolled Pain Low Hb Bed rest Physical restraints
14 D Drugs (BNZ, H2 blockers, Opioids, Anticholinergics, antidepressants, Antipsychotics) E Electrolyte imbalance ( Na and Ca), Eyes & Ears L Liver disease I Infection/Intoxication/Insomnia/Intracranial tumor R Retention (urinary or fecal) I Ischemia (MI, CVA, PAD, CAD) U Urea/ARF M Metabolic ( thyroid, B12, cortisol, blood sugar, hypoxia)
15 Agent AE Agent Adverse Events
16 Agent AE
17
18
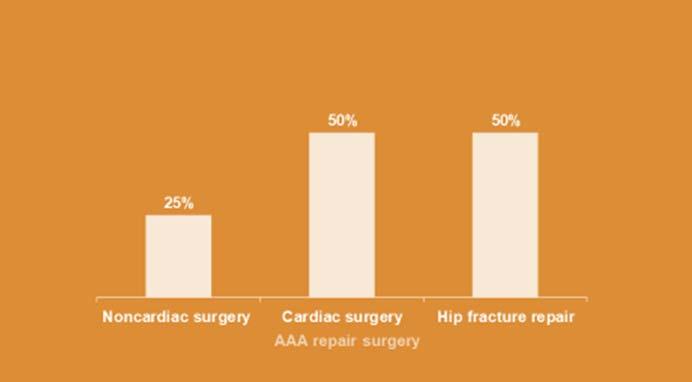
19 The incidence is 15% after elective non-cardiac surgery and up to 50% after high risk procedures such as hip fracture repair, AAA repair and CABG. Total dose of anesthetics used during the procedure also play an important route. It is important to note that high levels of pain have also been associated with delirium.
20 Strategies to provide adequate analgesia with minimally effective doses of opioids should be used. Low post-op Hb level (<30%) has also been associated with delirium, although transfusions have not been shown to reduce delirium.
21 Eight strong recommendations: benefits clearly outweighed the risks, or the risks clearly outweighed the benefits. Multicomponent nonpharmacologic interventions delivered by an interprofessional team should be administered to at risk older adults to prevent delirium. Ongoing educational programs regarding delirium should be provided for health care professionals. A medical evaluation should be performed to identify and manage underlying contributors to delirium. Pain management (preferably with nonopioid medications) should be optimized to prevent postoperative delirium. Medications with high risk of precipitating delirium should be avoided. Cholinesterase inhibitors should not be newly prescribed to prevent or treat postoperative delirium. Benzodiazepines should not be used as first line treatment of agitation associated with delirium. Antipsychotics and benzodiazepines should be avoided for treatment of hypoactive delirium.

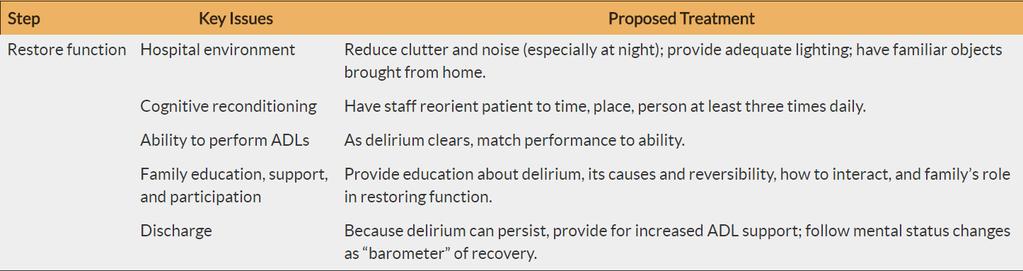
22 Step Key Issues Proposed Treatment

23 Step Key Issues Proposed Treatment
24
25 Target for Prevention Cognitive impairment Sleep deprivation Immobility Visual impairment Hearing impairment Dehydration Intervention Orientation, board with names, daily schedule, reorientating communication Nonpharm: warm milk/herbal tea, music, massage, noise reduction; melatonin or ramelteon Early mobilization, ambulation or range of motion 3x/d Visual aids and adaptive equipment Amplification, cerumen disimpaction, special communication techniques Early recognition and repletion
26 Urinary catheters should be avoided unless absolutely required for monitoring fluids or treating urinary retention. Bowel stimulants and stool softeners can be used to prevent obstipation, particularly in those taking opioids. Complete bed rest should be avoided because it can lead to increasing disability through disuse of muscles and development of pressure ulcers and atelectasis in the lungs. Malnutrition can be prevented through use of nutritional supplements and careful attention to intake of food and fluids.
27 Ensure safety Use families or sitters as first line Physical restraints can lead to serious injury or death and may worsen agitation and delirium. Use soft restraints or mitts only as a last resort to maintain pt safety (eg to prevent pt from pulling out tubes or catheters)
28 The lowest dose of the least toxic agent should be used for the shortest time possible. Except in unusual cases (alcohol withdrawal), antipsychotics have a more risk:benefit ratio than BNZ or other sedatives. Use of antipsychotics for delirium is off-label there are no FDA-approved drugs for the indication of delirium.
29 Haloperidol and Risperidone have the least sedation but the greatest risk of EPS. Quetiapine is most sedating and has the least EPS effects.
30 It is important to point that many cognitive deficits associated with delirium can continue, abating weeks and even months after the illness. Careful monitoring of mental status and providing adequate functional supports during this period are necessary to give the patient maximal chance of returning to his or her baseline level.
31 The first key step in delirium management is accurate diagnosis; several brief diagnostic assessments are available that operationalize the Confusion Assessment Method diagnostic algorithm after administration of a brief mental status examination that includes testing attention All delirious patients require a thorough evaluation for reversible causes; all correctable contributing factors should be addressed. In addition to the established associations of delirium with death, functional decline, and nursing home placement, new evidence shows that patients with delirium are at increased risk of prolonged cognitive decline and dementia. Pharmacologic intervention should be reserved for key target symptoms that cannot be adequately managed with nonpharmacologic interventions; low-dose, high-potency antipsychotics are usually the treatment of choice. Proactive, multifactorial interventions have reduced the incidence, severity, and duration of delirium.
32 GRS 9 th Edition AGS Expert Panel on Postoperative Delirium. Clinical Practice Guidelines for Postoperative Delirium in Older Adults. New York: American Geriatrics Society; Hshieh TT, Yue J, Oh E, et al. Effectiveness of multicomponent nonpharmacological delirium interventions: a meta-analysis. JAMA Intern Med. 2015;175(4): Inouye SK, Westendorp RG, Saczynski JS. Delirium in elderly people. Lancet. 2014;383(9920): Marcantonio ER, Ngo LH, O Connor M, et al. 3D-CAM: derivation and validation of a 3-minute diagnostic interview for CAM-defined delirium. Ann Intern Med. 2014;161(8):


33
34 PMH. Mrs. Tufts is 75 year old retired school teacher who comes to the hospital for acute confusion. she lives in a small, older home. She has HTN, DM, hyperlipidemia, CAD s/p stent in 2000, CHF, atrial fibrillation, CKD, GERD, migraines, osteoarthritis, COPD, & hypothyroidism.
35 MEDS. MEDICATIONS : Lisinopril 40 mg po qday Metoprolol tartrate 50 mg po qday Atorvastatin 40 mg po qday Aspirin 325 mg po qday Coumadin 3 mg po qhs Omeprazole 40 mg po qday Glyburide 10 mg po qday Metformin 1000 mg po bid Pioglitazone 45 mg po qday Ntg 0.4 mg SC prn chest pain Digoxin 0.25 mg po qdaily Amitriptyline 25 mg po qhs Ibuprofen 400 mg po tid Meloxicam 7.5 mg po bid Naproxen 250 mg po bid Citalopram 20 mg po qday Sertraline 25 mg po qday Furosemide 20 mg po qday KCL 20 meq po qday Clopidogrel 75 mg po qday Atrovent 17mcg /actuation 1 puff bid Combivent 1 puff every 6hrs prn Advair 250/50 mcg 1 puff bid Ambien 10 mg o qhs Levothyroxine 50mcgpo qhs.
36 MEDICATIONS : Lisinopril 40 mg po qday Metoprolol tartrate 50 mg po qday Atorvastatin 40 mg po qday Aspirin 325 mg po qday Coumadin 3 mg po qhs Omeprazole 40 mg po qday Glyburide 10 mg po qday Metformin 1000 mg po bid Pioglitazone 45 mg po qday Ntg 0.4 mg SC prn chest pain Digoxin 0.25 mg po qdaily Amitriptyline 25 mg po qhs Ibuprofen 400 mg po tid Meloxicam 7.5 mg po bid Naproxen 250 mg po bid Citalopram 20 mg po qday Sertraline 25 mg po qday Furosemide 20 mg po qday KCL 20 meq po qday Clopidogrel 75 mg po qday Atrovent 17mcg /actuation 1 puff bid Combivent 1 puff every 6hrs prn Advair 250/50 mcg 1 puff bid Ambien 10 mg o qhs Levothyroxine 50mcgpo qhs. MEDS that can cause delirium.


37 Allergies: Latex, sulfas SOCIAL : 30 pack year, quit 5 years back. No alcohol or illicit drug use Surgeries: Cholecystectomy Stents VITALS: BP 110/70 mm Hg Pulse :60 RR:14 Temp 98 F Standing up 100/70 mm Hg
38 Which one of the following is the most appropriate next step in her care? A. Obtain computed tomography of the head with contrast. B. Administer a high-potency, low-dose antipsychotic agent. C. Perform physical examination and order laboratory tests. D. Transfer to ICU for observation. E. Obtain psychiatric consultation.
39 Which one of the following is the most appropriate next step in her care? A. Obtain computed tomography of the head with contrast. B. Administer a high-potency, low-dose antipsychotic agent. C. Perform physical examination and order laboratory tests. D. Transfer to ICU for observation. E. Obtain psychiatric consultation.
40 Which one of the following classes of medication is the most common cause of delirium in hospitalized older adults? A. Angiotensin-receptor blockers B. H2-receptor antagonists C. Selective serotonin-reuptake inhibitors D. H1-receptor antagonists E. HMG-CoA reductase inhibitors
41 Which one of the following classes of medication is the most common cause of delirium in hospitalized older adults? A. Angiotensin-receptor blockers B. H2-receptor antagonists C. Selective serotonin-reuptake inhibitors D. H1-receptor antagonists E. HMG-CoA reductase inhibitors
42 Strong evidence suggests that delirium is an important, independent predictor of all of the following EXCEPT: A. Death B. New institutionalization C. Dementia D. Functional decline E. Delusional disorder
43 Strong evidence suggests that delirium is an important, independent predictor of all of the following EXCEPT: A. Death B. New institutionalization C. Dementia D. Functional decline E. Delusional disorder

44
Delirium in the Elderly
 Delirium in the Elderly ELITE 2015 Mamata Yanamadala M.B.B.S, MS Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity
Delirium in the Elderly ELITE 2015 Mamata Yanamadala M.B.B.S, MS Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity
Delirium in the Elderly
 Delirium in the Elderly ELITE 2017 Liza Genao, MD Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity Very much under-recognized
Delirium in the Elderly ELITE 2017 Liza Genao, MD Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity Very much under-recognized
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative
 Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
5 older patients become delirious every minute
 Management of Delirium: Nonpharmacologic and Pharmacologic Approaches Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley
Management of Delirium: Nonpharmacologic and Pharmacologic Approaches Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley
Delirium in Older Persons
 Objectives Delirium in Older Persons ELITE 2018 Liza Isabel Genao, MD Division of Geriatrics Describe rate, cost, complications of delirium Effectively diagnose the syndrome Describe multicomponent model
Objectives Delirium in Older Persons ELITE 2018 Liza Isabel Genao, MD Division of Geriatrics Describe rate, cost, complications of delirium Effectively diagnose the syndrome Describe multicomponent model
5 older patients become. What is delirium? (Acute confusional state) Where We ve Been and
 Where We ve Been and") Update on Delirium: Where We ve Been and Where We re Going Sharon K. Inouye, M.D., M.P.H. M PH Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley F. Levy
Update on Delirium: Where We ve Been and Where We re Going Sharon K. Inouye, M.D., M.P.H. M PH Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley F. Levy
Delirium. Dr. Lesley Wiesenfeld. Deputy Psychiatrist in Chief, Mount Sinai Hospital. Dr. Carole Cohen
 Delirium Dr. Lesley Wiesenfeld Deputy Psychiatrist in Chief, Mount Sinai Hospital Dr. Carole Cohen Department of Psychiatry, University of Toronto and Sunnybrook Health Sciences Centre Case Study Mrs B
Delirium Dr. Lesley Wiesenfeld Deputy Psychiatrist in Chief, Mount Sinai Hospital Dr. Carole Cohen Department of Psychiatry, University of Toronto and Sunnybrook Health Sciences Centre Case Study Mrs B
Delirium in Hospital Care
 Delirium in Hospital Care Dr John Puxty 1 Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors,
Delirium in Hospital Care Dr John Puxty 1 Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors,
Delirium. Dr. John Puxty
 Delirium Dr. John Puxty Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors, causes and main
Delirium Dr. John Puxty Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors, causes and main
Delirium. Delirium. Delirium Etiology and Pathophysiology. Fall 2018
 Three most common cognitive problems in adults 1. (acute confusion) 2. Dementia 3. Depression These problems often occur together Can you think of common stimuli for each? 1 1 State of temporary but acute
Three most common cognitive problems in adults 1. (acute confusion) 2. Dementia 3. Depression These problems often occur together Can you think of common stimuli for each? 1 1 State of temporary but acute
Strategies to minimize delirium for hip fracture patients
 Strategies to minimize delirium for hip fracture patients Stephen L Kates, M.D. Professor and Chairman Department Date of Orthopaedic Surgery Delirium incidence Up to 61% of hip fracture patients get delirium
Strategies to minimize delirium for hip fracture patients Stephen L Kates, M.D. Professor and Chairman Department Date of Orthopaedic Surgery Delirium incidence Up to 61% of hip fracture patients get delirium
Palliative Care and Delirium. Ambereen K. Mehta, MD MPH Assistant Professor Division of General Medicine, Geriatrics, and Palliative Care
 Palliative Care and Delirium Ambereen K. Mehta, MD MPH Assistant Professor Division of General Medicine, Geriatrics, and Palliative Care Disclosures I have no personal or professional financial relationships
Palliative Care and Delirium Ambereen K. Mehta, MD MPH Assistant Professor Division of General Medicine, Geriatrics, and Palliative Care Disclosures I have no personal or professional financial relationships
Do you know. Assessment of Delirium. What is Delirium? Which syndrome occurs more commonly in elderly populations? a. Delirium b.
 Assessment of Delirium Marianne McCarthy, PhD, GNP, PMHNP Arizona State University College of Nursing and Health Innovation What is Delirium? Delirium is a common clinical syndrome characterized by: Inattention
Assessment of Delirium Marianne McCarthy, PhD, GNP, PMHNP Arizona State University College of Nursing and Health Innovation What is Delirium? Delirium is a common clinical syndrome characterized by: Inattention
譫妄症 (Delirium) Objectives. Epidemiology. Delirium. DSM-5 Diagnostic Criteria. Prognosis 台大醫院老年醫學部陳人豪 2016/8/28
 Objectives. Epidemiology. Delirium. DSM-5 Diagnostic Criteria. Prognosis 台大醫院老年醫學部陳人豪 2016/8/28") 譫妄症 (Delirium) 台大醫院老年醫學部陳人豪 2016/8/28 Objectives Delirium Epidemiology Etiology Diagnosis Evaluation and Management Postoperative delirium Delirium (and acute problematic behavior) in the longterm care
譫妄症 (Delirium) 台大醫院老年醫學部陳人豪 2016/8/28 Objectives Delirium Epidemiology Etiology Diagnosis Evaluation and Management Postoperative delirium Delirium (and acute problematic behavior) in the longterm care
Chapter 01 Introduction
 Chapter 01 Introduction Defining the Elderly There is no universally accepted age cut-off defining elderly. This reflects the fact that chronological age itself is less important than biological events
Chapter 01 Introduction Defining the Elderly There is no universally accepted age cut-off defining elderly. This reflects the fact that chronological age itself is less important than biological events
Delirium. A Geriatric Syndrome. Jonathan McCaleb, MD, CMD, HMDC UNSOM, Assistant Professor of Medicine Geriatrics / Hospice & Palliative Medicine
 Delirium A Geriatric Syndrome Jonathan McCaleb, MD, CMD, HMDC UNSOM, Assistant Professor of Medicine Geriatrics / Hospice & Palliative Medicine Introduction Common Serious Unrecognized: a medical emergency
Delirium A Geriatric Syndrome Jonathan McCaleb, MD, CMD, HMDC UNSOM, Assistant Professor of Medicine Geriatrics / Hospice & Palliative Medicine Introduction Common Serious Unrecognized: a medical emergency
Delirium. Assessment and Management
 Delirium Assessment and Management Goals and Objectives Participants will: 1. be able to recognize and diagnose the syndrome of delirium. 2. understand the causes of delirium. 3. become knowledgeable about
Delirium Assessment and Management Goals and Objectives Participants will: 1. be able to recognize and diagnose the syndrome of delirium. 2. understand the causes of delirium. 3. become knowledgeable about
Charles Bernick, MD, MPH Cleveland Clinic Lou Ruvo Center for Brain Health June 2, 2018
 Charles Bernick, MD, MPH Cleveland Clinic Lou Ruvo Center for Brain Health June 2, 2018 Delirium common Prolongs hospitalization Worsens dementia ( if you survive) Increased risk of institutionalization
Charles Bernick, MD, MPH Cleveland Clinic Lou Ruvo Center for Brain Health June 2, 2018 Delirium common Prolongs hospitalization Worsens dementia ( if you survive) Increased risk of institutionalization
Delirium and cognitive impairment in the perioperative
 Delirium and cognitive impairment in the perioperative period Richard Sztramko Assistant Professor, McMaster University Divisions of Geriatrics and General Internal Medicine Disclosures Chief Medical Officer
Delirium and cognitive impairment in the perioperative period Richard Sztramko Assistant Professor, McMaster University Divisions of Geriatrics and General Internal Medicine Disclosures Chief Medical Officer
Update - Delirium in Elders
 Update - Delirium in Elders Impact Recognition Prevention, and Management Michael J. Lichtenstein, MD F. Carter Pannill, Jr. Professor of Medicine Chief, Division of Geriatrics, Gerontology and Palliative
Update - Delirium in Elders Impact Recognition Prevention, and Management Michael J. Lichtenstein, MD F. Carter Pannill, Jr. Professor of Medicine Chief, Division of Geriatrics, Gerontology and Palliative
Delirium and Dementia. Summary
 Delirium and Dementia Paul Kettl, M.D., M.H.A. Summary DELIRIUM Acute brain failure Identify cause (meds, infection) Treat sx Poor prognostic sign DEMENTIA Chronic brain failure AD most common cause Often
Delirium and Dementia Paul Kettl, M.D., M.H.A. Summary DELIRIUM Acute brain failure Identify cause (meds, infection) Treat sx Poor prognostic sign DEMENTIA Chronic brain failure AD most common cause Often
Delirium in Older Persons: An Investigative Journey
 Delirium in Older Persons: An Investigative Journey Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley F. Levy Family Chair
Delirium in Older Persons: An Investigative Journey Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley F. Levy Family Chair
Delirium. Geriatric Giants Lecture Series Divisions of Geriatric Medicine and Care of the Elderly University of Alberta
 Delirium Geriatric Giants Lecture Series Divisions of Geriatric Medicine and Care of the Elderly University of Alberta Overview A. Delirium - the nature of the beast B. Significance of delirium C. An approach
Delirium Geriatric Giants Lecture Series Divisions of Geriatric Medicine and Care of the Elderly University of Alberta Overview A. Delirium - the nature of the beast B. Significance of delirium C. An approach
The Agitated. Older Patient: old. What To Do? Michelle Gibson, MD, CCFP Presented at Brockville General Hospital Rounds, May 2003
 Focus on CME at Queen s University Focus on CME at Queen s University The Agitated The Older Patient: What To Do? Michelle Gibson, MD, CCFP Presented at Brockville General Hospital Rounds, May 2003 Both
Focus on CME at Queen s University Focus on CME at Queen s University The Agitated The Older Patient: What To Do? Michelle Gibson, MD, CCFP Presented at Brockville General Hospital Rounds, May 2003 Both
nicheprogram.org 16th Annual NICHE Conference Forging New Paths and Partnerships 1
 Improving Patient Outcomes in Geriatric Post-Operative Orthopedic Patients: Translating Research into Practice Tripping into The CAM Presented by: Diana LaBumbard, RN, MSN, ACNP/GNP-BC, CWOCN Denise Williams,
Improving Patient Outcomes in Geriatric Post-Operative Orthopedic Patients: Translating Research into Practice Tripping into The CAM Presented by: Diana LaBumbard, RN, MSN, ACNP/GNP-BC, CWOCN Denise Williams,
Learning Objectives. Delirium. Delirium. Delirium. Terminal Restlessness 3/28/2016
 Terminal Restlessness Dr. Christopher Churchill St. Cloud VA Health Care System EC&R Service Line Director & Medical Director Hospice & Palliative Care March 31, 2016 Learning Objectives Different Terminology
Terminal Restlessness Dr. Christopher Churchill St. Cloud VA Health Care System EC&R Service Line Director & Medical Director Hospice & Palliative Care March 31, 2016 Learning Objectives Different Terminology
Why Target Delirium for Surgical Quality Improvement?
 Why Target Delirium for Surgical Quality Improvement? Tom Robinson MD FACS thomas.robinson@ucdenver.edu July 22, 2018 Disclosures Tom Robinson has no disclosures. Who Cares About the Brain? Acute Organ
Why Target Delirium for Surgical Quality Improvement? Tom Robinson MD FACS thomas.robinson@ucdenver.edu July 22, 2018 Disclosures Tom Robinson has no disclosures. Who Cares About the Brain? Acute Organ
Delirium in the hospitalized patient
 Delirium in the hospitalized patient Jennifer A. Tarin, M.D. Department of Hospital Medicine Geriatric Health Safety Chair Colorado Permanente Medical Group UCLA Reynolds Scholar Delirium Preventing delirium
Delirium in the hospitalized patient Jennifer A. Tarin, M.D. Department of Hospital Medicine Geriatric Health Safety Chair Colorado Permanente Medical Group UCLA Reynolds Scholar Delirium Preventing delirium
Disclosures. Post operative Delirium. Set up audience participation. Delirium Definitions. Incidence of Delirium
 Post operative Delirium Disclosures IP for monitoring technology licensed to Medtronic Ken Brady, MD Pediatrics, Anesthesia, Critical Care Texas Children s Hospital Baylor College of Medicine Set up audience
Post operative Delirium Disclosures IP for monitoring technology licensed to Medtronic Ken Brady, MD Pediatrics, Anesthesia, Critical Care Texas Children s Hospital Baylor College of Medicine Set up audience
Disclosures No financial conflicts of interest. Key Questions
 Hospital Delirium: New Evidence in Diagnosis & Treatment Ethan Cumbler MD, FHM, FACP Professor of Medicine Medical Director Acute Care For Elderly Unit University of Colorado School of Medicine Disclosures
Hospital Delirium: New Evidence in Diagnosis & Treatment Ethan Cumbler MD, FHM, FACP Professor of Medicine Medical Director Acute Care For Elderly Unit University of Colorado School of Medicine Disclosures
DELIRIUM DR S A R A H A B D E L A T I S A S DR H I L A R Y W O L F E N D A L E S T 4
 DELIRIUM DR S A R A H A B D E L A T I S A S DR H I L A R Y W O L F E N D A L E S T 4 AIMS Define delirium Identify: Different types of delirium Risk factors Preventable causes Screening tools Management
DELIRIUM DR S A R A H A B D E L A T I S A S DR H I L A R Y W O L F E N D A L E S T 4 AIMS Define delirium Identify: Different types of delirium Risk factors Preventable causes Screening tools Management
Delirium. A Plan to Reduce Use of Restraints. David Wensel DO, FAAHPM Medical Director Midland Care
 Delirium A Plan to Reduce Use of Restraints David Wensel DO, FAAHPM Medical Director Midland Care Objectives Define delirium Describe pathophysiology of delirium Understand most common etiologies Define
Delirium A Plan to Reduce Use of Restraints David Wensel DO, FAAHPM Medical Director Midland Care Objectives Define delirium Describe pathophysiology of delirium Understand most common etiologies Define
Delirium Prevention: The State-of-the-Art & Implications to Improve Care in our State
 Delirium Prevention: The State-of-the-Art & Implications to Improve Care in our State Jonny Macias, MD & Michael Malone, MD Aurora Health Care/ University of Wisconsin School of Medicine & Public Health
Delirium Prevention: The State-of-the-Art & Implications to Improve Care in our State Jonny Macias, MD & Michael Malone, MD Aurora Health Care/ University of Wisconsin School of Medicine & Public Health
Delirium Pilot Project
 CCU Nurses: Delirium Pilot Project Our unit has been selected to develop and implement a delirium assessment and intervention program. We are beginning Phase 1 with education and assessing for our baseline
CCU Nurses: Delirium Pilot Project Our unit has been selected to develop and implement a delirium assessment and intervention program. We are beginning Phase 1 with education and assessing for our baseline
Delirium in the Elderly
 Delirium in the Elderly Jeffrey M. Burock, MD Division Director/ Psychiatry / Miriam Hospital Clinical Assistant Professor Warren Alpert School Of Medicine Learning Objectives Identify the symptoms of
Delirium in the Elderly Jeffrey M. Burock, MD Division Director/ Psychiatry / Miriam Hospital Clinical Assistant Professor Warren Alpert School Of Medicine Learning Objectives Identify the symptoms of
Delirium assessment and management. Dr Kim Jeffs Northern Health
 Delirium assessment and management Dr Kim Jeffs Northern Health What do you need to know? Epidemiology How big is the problem? Who is at risk? Assessment Tools for diagnosis Prevention Evidence base Management
Delirium assessment and management Dr Kim Jeffs Northern Health What do you need to know? Epidemiology How big is the problem? Who is at risk? Assessment Tools for diagnosis Prevention Evidence base Management
Jacinta Lucke Resident Emergency Medicine PHD Gerontology & Geriatrics
 Jacinta Lucke Resident Emergency Medicine PHD Gerontology & Geriatrics TAKE HOME MESSAGE When managing confusion in older patients: Routinely screen for impaired cognition Patients with impaired cognition
Jacinta Lucke Resident Emergency Medicine PHD Gerontology & Geriatrics TAKE HOME MESSAGE When managing confusion in older patients: Routinely screen for impaired cognition Patients with impaired cognition
+ Change in baseline mental status, inattention, and either disorganized thinking or altered level of consciousness. Delirium. Disclosure.
 47 th Annual Meeting August 2-4, 2013 Orlando, FL Identification, Prevention and Treatment of Delirium: The Role of the Health System Pharmacist Jennifer Cortes, PharmD, BCPS Medical ICU Clinical Pharmacy
47 th Annual Meeting August 2-4, 2013 Orlando, FL Identification, Prevention and Treatment of Delirium: The Role of the Health System Pharmacist Jennifer Cortes, PharmD, BCPS Medical ICU Clinical Pharmacy
Objectives. Delirium in the Elderly Patient. Disclosure. Arizona Geriatrics Society Fall Symposium 2010
 Delirium in the Elderly Patient Sandra Jacobson, MD Banner Sun Health Research Institute Arizona Geriatrics Society Fall Symposium 2010 Disclosure Dr. Jacobson has disclosed that she does not have any
Delirium in the Elderly Patient Sandra Jacobson, MD Banner Sun Health Research Institute Arizona Geriatrics Society Fall Symposium 2010 Disclosure Dr. Jacobson has disclosed that she does not have any
Geriatrics and Cancer Care
 Geriatrics and Cancer Care Roger Wong, BMSc, MD, FRCPC, FACP Postgraduate Dean of Medical Education Clinical Professor, Division of Geriatric Medicine UBC Faculty of Medicine Disclosure No competing interests
Geriatrics and Cancer Care Roger Wong, BMSc, MD, FRCPC, FACP Postgraduate Dean of Medical Education Clinical Professor, Division of Geriatric Medicine UBC Faculty of Medicine Disclosure No competing interests
Drugs that poison the elderly
 Drugs that poison the elderly Brent Tipping Sub-specialist Geriatrician and Specialist Physician Division of Geriatric Medicine, Department of Medicine University of the Witwatersrand To treat or not to
Drugs that poison the elderly Brent Tipping Sub-specialist Geriatrician and Specialist Physician Division of Geriatric Medicine, Department of Medicine University of the Witwatersrand To treat or not to
Delirium Assessment. February 24, Susan Schumacher, MS, APRN-BC
 Delirium Assessment February 24, 2016 Susan Schumacher, MS, APRN-BC Objectives Define delirium Differentiate delirium from dementia Identify predisposing and precipitating factors leading to delirium.
Delirium Assessment February 24, 2016 Susan Schumacher, MS, APRN-BC Objectives Define delirium Differentiate delirium from dementia Identify predisposing and precipitating factors leading to delirium.
Delirium Assessment and management in relation to falls risk in hospital
 Delirium Assessment and management in relation to falls risk in hospital A house call - Mrs JM 95-year-old lady Normally cognitively intact Multiple medical problems, including falls Housebound, mobile
Delirium Assessment and management in relation to falls risk in hospital A house call - Mrs JM 95-year-old lady Normally cognitively intact Multiple medical problems, including falls Housebound, mobile
DELIRIUM. Sabitha Rajan, MD, MSc, FHM Scott &White Healthcare Texas A&M Health Science Center School of Medicine
 DELIRIUM Sabitha Rajan, MD, MSc, FHM Scott &White Healthcare Texas A&M Health Science Center School of Medicine Disclosure Milliman Care Guidelines - Editor Objectives Define delirium Epidemiology Diagnose
DELIRIUM Sabitha Rajan, MD, MSc, FHM Scott &White Healthcare Texas A&M Health Science Center School of Medicine Disclosure Milliman Care Guidelines - Editor Objectives Define delirium Epidemiology Diagnose
Guidelines for Management and Prevention of Delirium In Geriatric Trauma Patients
 Guidelines for Management and Prevention of Delirium In Geriatric Trauma Patients Objectives: Provide a guideline for recognizing and managing delirium in geriatric trauma patients. Provide a template
Guidelines for Management and Prevention of Delirium In Geriatric Trauma Patients Objectives: Provide a guideline for recognizing and managing delirium in geriatric trauma patients. Provide a template
Test your Knowledge: Recognizing Delirium
 The Ottawa Hospital Name: Unit: Profession: RN RPN PT OT SW Other Note: Each question has only one correct answer. 1. If a patient is identified as being at high risk for developing delirium, his/her mental
The Ottawa Hospital Name: Unit: Profession: RN RPN PT OT SW Other Note: Each question has only one correct answer. 1. If a patient is identified as being at high risk for developing delirium, his/her mental
PRESCRIBING PRACTICE IN DELIRIUM. John Warburton Critical Care Pharmacist
 PRESCRIBING PRACTICE IN DELIRIUM John Warburton Critical Care Pharmacist Learning outcomes Modifiable medication risk factors for delirium An appreciation of contributing factors modifiable with medicines
PRESCRIBING PRACTICE IN DELIRIUM John Warburton Critical Care Pharmacist Learning outcomes Modifiable medication risk factors for delirium An appreciation of contributing factors modifiable with medicines
9/19/2018. Common Medical Issues and Management in the Geriatric Trauma Patient. Disclosures. Objectives. I have no financial disclosures
 Common Medical Issues and Management in the Geriatric Trauma Patient 2018 UW Medicine EMS & Trauma Conference September 17, 2018 Joe C. Huang, M.D. Clinical Instructor Medical Director, Geriatrics-Palliative
Common Medical Issues and Management in the Geriatric Trauma Patient 2018 UW Medicine EMS & Trauma Conference September 17, 2018 Joe C. Huang, M.D. Clinical Instructor Medical Director, Geriatrics-Palliative
How to prevent delirium in nursing home. Dr. Sophie ALLEPAERTS Geriatric department CHU-Liège Belgium
 How to prevent delirium in nursing home Dr. Sophie ALLEPAERTS Geriatric department CHU-Liège Belgium 1 CONFLICT OF INTEREST DISCLOSURE I have no potential conflict of interest to report 2 Outline 1. Introduction
How to prevent delirium in nursing home Dr. Sophie ALLEPAERTS Geriatric department CHU-Liège Belgium 1 CONFLICT OF INTEREST DISCLOSURE I have no potential conflict of interest to report 2 Outline 1. Introduction
Delirium in the ICU: Prevention and Treatment. Delirium Defined Officially. Delirium: Really Defined. S. Andrew Josephson, MD
 Delirium in the ICU: Prevention and Treatment S. Andrew Josephson, MD Director, Neurohospitalist Service Medical Director, Inpatient Neurology June 2, 2011 Delirium Defined Officially (DSM-IV-TR) criteria
Delirium in the ICU: Prevention and Treatment S. Andrew Josephson, MD Director, Neurohospitalist Service Medical Director, Inpatient Neurology June 2, 2011 Delirium Defined Officially (DSM-IV-TR) criteria
Delirium in the Emergency Department. Emergency Medicine Rounds April 14, 2015 Paul R. Vanhoutte
 Delirium in the Emergency Department Emergency Medicine Rounds April 14, 2015 Paul R. Vanhoutte Goals of Rounds: Review Definition Management An Understanding What is important is to spread confusion,
Delirium in the Emergency Department Emergency Medicine Rounds April 14, 2015 Paul R. Vanhoutte Goals of Rounds: Review Definition Management An Understanding What is important is to spread confusion,
Perioperative Care of Older Adults
 Perioperative Care of Older Adults SARAH A. WINGFIELD, MD AND THOMAS O. DALTON, MD UNIVERSITY OF TEXAS SOUTHWESTERN MEDICAL CENTER DIVISION OF GERIATRIC MEDICINE We have no disclosures. Objectives -Recognize
Perioperative Care of Older Adults SARAH A. WINGFIELD, MD AND THOMAS O. DALTON, MD UNIVERSITY OF TEXAS SOUTHWESTERN MEDICAL CENTER DIVISION OF GERIATRIC MEDICINE We have no disclosures. Objectives -Recognize
Perioperative Care of Older Adults
 Perioperative Care of Older Adults SARAH A. WINGFIELD, MD AND THOMAS O. DALTON, MD UNIVERSITY OF TEXAS SOUTHWESTERN MEDICAL CENTER DIVISION OF GERIATRIC MEDICINE We have no disclosures. Objectives -Recognize
Perioperative Care of Older Adults SARAH A. WINGFIELD, MD AND THOMAS O. DALTON, MD UNIVERSITY OF TEXAS SOUTHWESTERN MEDICAL CENTER DIVISION OF GERIATRIC MEDICINE We have no disclosures. Objectives -Recognize
Iatrogenic Delirium. Heather Carey, PharmD, BCPP Clinical Psychiatric Pharmacist University Hospitals Richmond Medical Center
 Iatrogenic Delirium Heather Carey, PharmD, BCPP Clinical Psychiatric Pharmacist University Hospitals Richmond Medical Center Objectives Discuss proposed mechanisms of medication induced delirium Identify
Iatrogenic Delirium Heather Carey, PharmD, BCPP Clinical Psychiatric Pharmacist University Hospitals Richmond Medical Center Objectives Discuss proposed mechanisms of medication induced delirium Identify
Geriatric Grand Rounds
 Geriatric Grand Rounds Prevalence and Risk Factors of Delirium in Older Patients Admitted to a Community Based Acute Care Hospital Tuesday, October 27, 2009 12:00 noon Dr. Bill Black Auditorium Glenrose
Geriatric Grand Rounds Prevalence and Risk Factors of Delirium in Older Patients Admitted to a Community Based Acute Care Hospital Tuesday, October 27, 2009 12:00 noon Dr. Bill Black Auditorium Glenrose
Drug induced delirium
 Drug induced delirium Knut Erik Hovda, MD, PhD, FACMT, FEAPCCT The Norwegian CBRNe Centre of Medicine Department of Acute Medicine Oslo University hospital Content 1. Introduction 2. Risk factors 3. Prevalence
Drug induced delirium Knut Erik Hovda, MD, PhD, FACMT, FEAPCCT The Norwegian CBRNe Centre of Medicine Department of Acute Medicine Oslo University hospital Content 1. Introduction 2. Risk factors 3. Prevalence
DELIRIUM. J. Sukanya 28.Jun.12
 DELIRIUM J. Sukanya 28.Jun.12 Outline Why? What? How? What s next? Delirium Introduction Delirium An acute decline in attention and cognition The most frequent neuropsychiatric syndrome A common, life-threatening,
DELIRIUM J. Sukanya 28.Jun.12 Outline Why? What? How? What s next? Delirium Introduction Delirium An acute decline in attention and cognition The most frequent neuropsychiatric syndrome A common, life-threatening,
Objec&ves. Dr. Dallas Seitz and Dr. Agata Szlanta
 Dr. Dallas Seitz and Dr. Agata Szlanta Objec&ves Understand the differential diagnosis and presentation of delirium in older adults; Review the risk factors and precipitants for delirium; and Discuss delirium
Dr. Dallas Seitz and Dr. Agata Szlanta Objec&ves Understand the differential diagnosis and presentation of delirium in older adults; Review the risk factors and precipitants for delirium; and Discuss delirium
g Prevention, Diagnosis, and Management in Palliative Care
 8/3/2012 Improving p g Prevention, Diagnosis, g and Management in Palliative Care MN Rural Palliative Care Networking Group Quarterly Education Session June 27,2012 Sandra W. Gordon-Kolb, MD, MMM, CPE
8/3/2012 Improving p g Prevention, Diagnosis, g and Management in Palliative Care MN Rural Palliative Care Networking Group Quarterly Education Session June 27,2012 Sandra W. Gordon-Kolb, MD, MMM, CPE
DIAH MUSTIKA HW SpS,KIC Intensive Care Unit of Emergency Department Naval Hospital dr RAMELAN, Surabaya
 DIAH MUSTIKA HW SpS,KIC Intensive Care Unit of Emergency Department Naval Hospital dr RAMELAN, Surabaya Encephalopathy is a common complication of systemic illness or direct brain injury. Acute confusional
DIAH MUSTIKA HW SpS,KIC Intensive Care Unit of Emergency Department Naval Hospital dr RAMELAN, Surabaya Encephalopathy is a common complication of systemic illness or direct brain injury. Acute confusional
Symptom Management Pocket Guides: DELIRIUM
 Symptom Management Pocket Guides: DELIRIUM August 2010 DELIRIUM Page Considerations. 1 Assessment 2 Diagnosis. 3 Non-Pharmacological treatment 3 Pharmacological treatment. 5 Mild Delirium... 6 Moderate
Symptom Management Pocket Guides: DELIRIUM August 2010 DELIRIUM Page Considerations. 1 Assessment 2 Diagnosis. 3 Non-Pharmacological treatment 3 Pharmacological treatment. 5 Mild Delirium... 6 Moderate
Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh. Professor of Critical Care, Edinburgh University
 Tim Walsh. Professor of Critical Care, Edinburgh University") Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh Professor of Critical Care, Edinburgh University Lecture Plan: a route to clarity What is delirium? Why is delirium important? Step
Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh Professor of Critical Care, Edinburgh University Lecture Plan: a route to clarity What is delirium? Why is delirium important? Step
Delirium and Dementia
 Delirium and Dementia Elder Friendly Care in Acute Care Seniors Health Strategic Clinical Network Acute Care Stress Blender Poor Poor sleep At-Risk Older Adult TREAT CAUSE immediately & aggressively. Increased
Delirium and Dementia Elder Friendly Care in Acute Care Seniors Health Strategic Clinical Network Acute Care Stress Blender Poor Poor sleep At-Risk Older Adult TREAT CAUSE immediately & aggressively. Increased
Delirium, Depression and Dementia
 Delirium, Depression and Dementia Martha Watson, MS, APRN, GCNS Some material included in this presentation is adapted from: NICHE (2009). Geriatric Resource Nurse Core Curriculum [Power Point presentation].
Delirium, Depression and Dementia Martha Watson, MS, APRN, GCNS Some material included in this presentation is adapted from: NICHE (2009). Geriatric Resource Nurse Core Curriculum [Power Point presentation].
Polypharmacy & De-prescribing In Older Adults
 Polypharmacy & De-prescribing In Older Adults Maryland Association of Osteopathic Physicians Annual Meeting September 15, 2018 Elizabeth Phung, DO Lead Clinical Associate Physician Beacham Center for Geriatric
Polypharmacy & De-prescribing In Older Adults Maryland Association of Osteopathic Physicians Annual Meeting September 15, 2018 Elizabeth Phung, DO Lead Clinical Associate Physician Beacham Center for Geriatric
Managing Delirium in Hospitalized Older Adults
 Marquette University e-publications@marquette College of Nursing Faculty Research and Publications Nursing, College of 10-1-2015 Managing Delirium in Hospitalized Older Adults Margaret J. Bull Marquette
Marquette University e-publications@marquette College of Nursing Faculty Research and Publications Nursing, College of 10-1-2015 Managing Delirium in Hospitalized Older Adults Margaret J. Bull Marquette
Care of Patient with Delirium
 Care of Patient with Delirium Introduction Delirium is an alteration in consciousness involving confusion and other changes in cognitive ability that has a brief duration. 1 Patients specifically at risk
Care of Patient with Delirium Introduction Delirium is an alteration in consciousness involving confusion and other changes in cognitive ability that has a brief duration. 1 Patients specifically at risk
Delirium Screening: The next nurse sensitive indicator?
 Delirium Screening: The next nurse sensitive indicator? Sharon Gunn, MSN, MA, RN, ACNS-BC, CCRN Clinical Nurse Specialist Critical Care Baylor University Medical Center Dallas, TX Objectives Recognize
Delirium Screening: The next nurse sensitive indicator? Sharon Gunn, MSN, MA, RN, ACNS-BC, CCRN Clinical Nurse Specialist Critical Care Baylor University Medical Center Dallas, TX Objectives Recognize
Disentangling Delirium and Dementia
 Disentangling Delirium and Dementia Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley F. Levy Family Chair Director, Aging
Disentangling Delirium and Dementia Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley F. Levy Family Chair Director, Aging
Management of Delirium in the ICU. Yahya Shehabi
 Management of Delirium in the ICU Yahya Shehabi Hello! Doctor, your patient is CAM + ve Good morning Dr, Am one of the RC, Just examined Mr XXX he is CAM +ve Positive what? Sir replied RC: I meant he is
Management of Delirium in the ICU Yahya Shehabi Hello! Doctor, your patient is CAM + ve Good morning Dr, Am one of the RC, Just examined Mr XXX he is CAM +ve Positive what? Sir replied RC: I meant he is
Decreasing Delirium Resolution Times for the Elderly: An Interprofessional Approach
 Decreasing Delirium Resolution Times for the Elderly: An Interprofessional Approach Featuring: Felice Rogers Evans BSN RN BC Ty Breiter MSN RN CNL Tampa General Hospital NICHE exemplar hospital Three time
Decreasing Delirium Resolution Times for the Elderly: An Interprofessional Approach Featuring: Felice Rogers Evans BSN RN BC Ty Breiter MSN RN CNL Tampa General Hospital NICHE exemplar hospital Three time
Delirium: A Condition of All Ages. Delirium, also known as acute confusional state, Definition. Epidemiology
 Focus on CME at the University of Calgary : A Condition of All Ages While delirium can strike at any age, physicians need to be particularly watchful for it in elderly patients, so that a search for the
Focus on CME at the University of Calgary : A Condition of All Ages While delirium can strike at any age, physicians need to be particularly watchful for it in elderly patients, so that a search for the
Cases in Delirium for Family Physicians
 Friday General Session Cases in Delirium for Family Physicians Dale Moquist, MD Former Geriatric Coordinator Memorial Hermann Family Medicine Residency Horseshoe Bay, Texas Educational Objectives By the
Friday General Session Cases in Delirium for Family Physicians Dale Moquist, MD Former Geriatric Coordinator Memorial Hermann Family Medicine Residency Horseshoe Bay, Texas Educational Objectives By the
COMMON DRUG RELATED PROBLEMS SEEN IN PACE AND MECHANISMS TO MITIGATE RISK
 COMMON DRUG RELATED PROBLEMS SEEN IN PACE AND MECHANISMS TO MITIGATE RISK Robert L Alesiani, PharmD, CGP Chief Pharmacotherapy Officer CareKinesis, Inc. (a Tabula Rasa Healthcare Company) 2 3 4 5 Pharmacogenomics
COMMON DRUG RELATED PROBLEMS SEEN IN PACE AND MECHANISMS TO MITIGATE RISK Robert L Alesiani, PharmD, CGP Chief Pharmacotherapy Officer CareKinesis, Inc. (a Tabula Rasa Healthcare Company) 2 3 4 5 Pharmacogenomics
Delirium. Approach. Symptom Update Masterclass:
 Symptom Update Masterclass: Delirium Jason Boland Senior Clinical Lecturer and Honorary Consultant in Palliative Medicine Wolfson Centre for Palliative Care Research Hull York Medical School University
Symptom Update Masterclass: Delirium Jason Boland Senior Clinical Lecturer and Honorary Consultant in Palliative Medicine Wolfson Centre for Palliative Care Research Hull York Medical School University
Delirium in Cancer: Psychopharmacologic Management
 Delirium in Cancer: Psychopharmacologic Management William Breitbart, MD Professor and Chief, Psychiatry Service Memorial Sloan-Kettering Cancer Center New York, New York Delirium in Patients with Cancer
Delirium in Cancer: Psychopharmacologic Management William Breitbart, MD Professor and Chief, Psychiatry Service Memorial Sloan-Kettering Cancer Center New York, New York Delirium in Patients with Cancer
Critical Care Pharmacological Management of Delirium
 Critical Care Pharmacological Management of Delirium Policy Title: in the Critical Care Unit Executive Summary: This policy provides guidance Pharmacological Management of delirium in the Critical Care
Critical Care Pharmacological Management of Delirium Policy Title: in the Critical Care Unit Executive Summary: This policy provides guidance Pharmacological Management of delirium in the Critical Care
Strategies to Recognize & B.E.A.T. Delirium. Amy E. Seitz Cooley, MS, RN, ACNS-BC Clinical Nurse Specialist York College of Pennsylvania DNP Student
 Strategies to Recognize & B.E.A.T. Delirium Amy E. Seitz Cooley, MS, RN, ACNS-BC Clinical Nurse Specialist York College of Pennsylvania DNP Student The very first requirement in a hospital is that it should
Strategies to Recognize & B.E.A.T. Delirium Amy E. Seitz Cooley, MS, RN, ACNS-BC Clinical Nurse Specialist York College of Pennsylvania DNP Student The very first requirement in a hospital is that it should
Improving Delirium Management: Mapping Out One Unit s Journey. Geriatrics Institute June 27, 2013
 Improving Delirium Management: Mapping Out One Unit s Journey Geriatrics Institute June 27, 2013 Rebecca Ramsden, NP Mary Ann Hamelin, CNS Susanne Loay, RN Objectives Background RNAO Best Practice Guideline
Improving Delirium Management: Mapping Out One Unit s Journey Geriatrics Institute June 27, 2013 Rebecca Ramsden, NP Mary Ann Hamelin, CNS Susanne Loay, RN Objectives Background RNAO Best Practice Guideline
Critical Care Pharmacological Management of Delirium
 Critical Care Pharmacological Management of Delirium Policy Title: in the Critical Care Unit Executive Summary: This policy provides guidance Pharmacological Management of delirium in the Critical Care
Critical Care Pharmacological Management of Delirium Policy Title: in the Critical Care Unit Executive Summary: This policy provides guidance Pharmacological Management of delirium in the Critical Care
ICU Updates: Delirium in Hospitalized Patients
 ICU Updates: Delirium in Hospitalized Patients James A. Frank, MD Associate Professor Pulmonary and Critical Care UCSF Dept. of Medicine Director, MICU San Francisco VAMC Recognizing and preventing delirium
ICU Updates: Delirium in Hospitalized Patients James A. Frank, MD Associate Professor Pulmonary and Critical Care UCSF Dept. of Medicine Director, MICU San Francisco VAMC Recognizing and preventing delirium
Hospitalization- Associated Disability
 Hospitalization- Associated Disability Deborah Villarreal, MD Assistant Professor Geriatric and Palliative Medicine An Unfortunately Common Scenario Mrs.G 70 y/o BF DM type II, HTN, s/p CVA, OA, OP admitted
Hospitalization- Associated Disability Deborah Villarreal, MD Assistant Professor Geriatric and Palliative Medicine An Unfortunately Common Scenario Mrs.G 70 y/o BF DM type II, HTN, s/p CVA, OA, OP admitted
The Geriatrician in the Trauma Service. Trauma Quality Improvement Program (TQIP) Annual Scientific Meeting and Training 2013
 Annual Scientific Meeting and Training 2013") The Geriatrician in the Trauma Service Trauma Quality Improvement Program (TQIP) Annual Scientific Meeting and Training 2013 Challenges of the Geriatric Trauma Patient Challenges of the Geriatric Patient
The Geriatrician in the Trauma Service Trauma Quality Improvement Program (TQIP) Annual Scientific Meeting and Training 2013 Challenges of the Geriatric Trauma Patient Challenges of the Geriatric Patient
PSYCHOSOCIAL SYMPTOMS (DELIRIUM)
") PSYCHOSOCIAL SYMPTOMS (DELIRIUM) Rut Kiman MD, MSc Head Pediatric Palliative Care Team Hospital Nacional Prof. A. Posadas Buenos Aires -Argentina Senior Lecturer. Pediatric Department School of Medicine.
PSYCHOSOCIAL SYMPTOMS (DELIRIUM) Rut Kiman MD, MSc Head Pediatric Palliative Care Team Hospital Nacional Prof. A. Posadas Buenos Aires -Argentina Senior Lecturer. Pediatric Department School of Medicine.
Practical Management of the Delirious Patient with Mental Retardation by the Nurse Anesthetist
 Practical Management of the Delirious Patient with Mental Retardation by the Nurse Anesthetist 1. Basic Facts on Delirium The nurse anesthetist plays an important role in prevention of delirium among surgical
Practical Management of the Delirious Patient with Mental Retardation by the Nurse Anesthetist 1. Basic Facts on Delirium The nurse anesthetist plays an important role in prevention of delirium among surgical
Do benzos, opioids, or strong anticholinergics cause delirium? Lisa Burry
 Do benzos, opioids, or strong anticholinergics cause delirium? Lisa Burry Delirium in the ICU Occurs in up to 85% of MICU/SICU MV patients 20-50% of lower severity ICU patients develop delirium Hypoactive
Do benzos, opioids, or strong anticholinergics cause delirium? Lisa Burry Delirium in the ICU Occurs in up to 85% of MICU/SICU MV patients 20-50% of lower severity ICU patients develop delirium Hypoactive
Interprofessional Outpatient Clinic Polypharmacy Management. Objectives
 Interprofessional Outpatient Clinic Polypharmacy Management Brett Hoffecker, MD University of Kansas School of Medicine Wichita Family Medicine Residency Program at Via Christi April 10th, 2015 Objectives
Interprofessional Outpatient Clinic Polypharmacy Management Brett Hoffecker, MD University of Kansas School of Medicine Wichita Family Medicine Residency Program at Via Christi April 10th, 2015 Objectives
Delirium. Quick reference guide. Issue date: July Diagnosis, prevention and management
 Issue date: July 2010 Delirium Diagnosis, prevention and management Developed by the National Clinical Guideline Centre for Acute and Chronic Conditions About this booklet This is a quick reference guide
Issue date: July 2010 Delirium Diagnosis, prevention and management Developed by the National Clinical Guideline Centre for Acute and Chronic Conditions About this booklet This is a quick reference guide
POLYPHARMACY IN OLDER ADULTS AND BEERS CRITERIA UPDATE
 POLYPHARMACY IN OLDER ADULTS AND BEERS CRITERIA UPDATE Jeannie Kim Lee, PharmD, BCPS, CGP Clinical Pharmacy Director College of Pharmacy The University of Arizona Learning Objectives: State the risks of
POLYPHARMACY IN OLDER ADULTS AND BEERS CRITERIA UPDATE Jeannie Kim Lee, PharmD, BCPS, CGP Clinical Pharmacy Director College of Pharmacy The University of Arizona Learning Objectives: State the risks of
Canadian Practices for the Treatment of Delirium. Lisa Burry, BScPharm, PharmD
 Canadian Practices for the Treatment of Delirium Lisa Burry, BScPharm, PharmD Disclosures & Acknowledgements Conflicts of interest: None Acknowledgements: our patients and the clinical staff that supported
Canadian Practices for the Treatment of Delirium Lisa Burry, BScPharm, PharmD Disclosures & Acknowledgements Conflicts of interest: None Acknowledgements: our patients and the clinical staff that supported
Aging Research Day March 8, 2012
 Aging Research Day March 8, 2012 Heidi R. Wierman, MD Mane Medical Center Division Director, Geriatrics Assistant Professor, Tufts School of Medicine Overview 1.Brief Delirium Review 2.Describe HELP function
Aging Research Day March 8, 2012 Heidi R. Wierman, MD Mane Medical Center Division Director, Geriatrics Assistant Professor, Tufts School of Medicine Overview 1.Brief Delirium Review 2.Describe HELP function
Delirium is defined as an acute
 Marisa Wan, MD, FRCPC, Jocelyn M. Chase, MD, FRCPC Delirium in older adults: Diagnosis, prevention, and treatment Recognizing delirium promptly and treating the underlying cause can prevent the significant
Marisa Wan, MD, FRCPC, Jocelyn M. Chase, MD, FRCPC Delirium in older adults: Diagnosis, prevention, and treatment Recognizing delirium promptly and treating the underlying cause can prevent the significant
Dilemmas in the Care of Geriatric Hospitalized Patients October 6, 2015
 Dilemmas in the Care of Geriatric Hospitalized Patients October 6, 2015 Jeff Wallace, MD, MPH Professor, Division of Geriatrics Department of Medicine University of Colorado, Denver CO Dilemma #1: Anticoagulants
Dilemmas in the Care of Geriatric Hospitalized Patients October 6, 2015 Jeff Wallace, MD, MPH Professor, Division of Geriatrics Department of Medicine University of Colorado, Denver CO Dilemma #1: Anticoagulants
MN/OH Delirium Collaborative. Place picture here
 MN/OH Delirium Collaborative Place picture here November 16, 2017 Housekeeping Introductions: MHA- Naira Polonsky OHA- Rosalie Weakland OHA- Jim Guliano In December 2015, the Minnesota and Ohio HENS began
MN/OH Delirium Collaborative Place picture here November 16, 2017 Housekeeping Introductions: MHA- Naira Polonsky OHA- Rosalie Weakland OHA- Jim Guliano In December 2015, the Minnesota and Ohio HENS began
H.E.L.P. ing Elder Trauma Patients Avoid Delirium and Functional Decline
 H.E.L.P. ing Elder Trauma Patients Avoid Delirium and Functional Decline Montreal ITC 2014 Sept. 26 Joann Creager, CNS Geriatrics, Manager, MUHC Elder Friendly Hospital Presentation Overview 1. Elder patient
H.E.L.P. ing Elder Trauma Patients Avoid Delirium and Functional Decline Montreal ITC 2014 Sept. 26 Joann Creager, CNS Geriatrics, Manager, MUHC Elder Friendly Hospital Presentation Overview 1. Elder patient
2/11/2015. Valarie Petersen, DNP, FNP-BC, GCNS-BC
 Valarie Petersen, DNP, FNP-BC, GCNS-BC Physiological changes decreased brain weight and cortical cell count, loss of myelin from fibers Short term memory difficulty Lengthened reaction time Sleeping patterns
Valarie Petersen, DNP, FNP-BC, GCNS-BC Physiological changes decreased brain weight and cortical cell count, loss of myelin from fibers Short term memory difficulty Lengthened reaction time Sleeping patterns
Sedation and Delirium Questions
 Sedation and Delirium Questions TLC Curriculum William J. Ehlenbach, MD MSc Assistant Professor of Medicine Pulmonary & Critical Care Medicine Question 1 Deep sedation in ventilated critically patients
Sedation and Delirium Questions TLC Curriculum William J. Ehlenbach, MD MSc Assistant Professor of Medicine Pulmonary & Critical Care Medicine Question 1 Deep sedation in ventilated critically patients
Fairview Southdale Hospital Total Points: 50 RN/LPN Medication Assessment Passing: 45
 Fairview Southdale Hospital Total Points: 50 RN/LPN Medication Assessment Passing: 45 1. Your diabetic patient is to be started on an insulin drip at 8 units/hour. The insulin is supplied: 100 units in
Fairview Southdale Hospital Total Points: 50 RN/LPN Medication Assessment Passing: 45 1. Your diabetic patient is to be started on an insulin drip at 8 units/hour. The insulin is supplied: 100 units in
Home Care and Hospice Association of New Jersey Annual Conference 2017
 Home Care and Hospice Association of New Jersey Annual Conference 2017 I D E N T I F I C A T I O N A N D M A N A G E M E N T O F D E L I R I U M E L I Z A B E T H M A G E R - O C O N N O R A C H P N DR
Home Care and Hospice Association of New Jersey Annual Conference 2017 I D E N T I F I C A T I O N A N D M A N A G E M E N T O F D E L I R I U M E L I Z A B E T H M A G E R - O C O N N O R A C H P N DR
Residents Who Don t Sleep
 Residents Who Don t Sleep Case study........................................... An 86 yr. old woman has diagnoses of Alzheimer s disease, congestive heart failure, constipation, depression, hypertension
Residents Who Don t Sleep Case study........................................... An 86 yr. old woman has diagnoses of Alzheimer s disease, congestive heart failure, constipation, depression, hypertension