The Harvard community has made this article openly available. Please share how this access benefits you. Your story matters
|
|
|
- Wesley Cecil Hubbard
- 5 years ago
- Views:
Transcription
1 A Contemporary, Population-Based Analysis of the Incidence, Cost, Outcomes, and Preoperative Risk Prediction of Postoperative Delirium Following Major Urologic Cancer Surgeries The Harvard community has made this article openly available. Please share how this access benefits you. Your story matters Citation Ha, Albert Sangji A Contemporary, Population-Based Analysis of the Incidence, Cost, Outcomes, and Preoperative Risk Prediction of Postoperative Delirium Following Major Urologic Cancer Surgeries. Doctoral dissertation, Harvard Medical School. Citable link Terms of Use This article was downloaded from Harvard University s DASH repository, and is made available under the terms and conditions applicable to Other Posted Material, as set forth at nrs.harvard.edu/urn-3:hul.instrepos:dash.current.terms-ofuse#laa
2 Abstract Introduction Postoperative delirium is associated with poor outcomes and increased healthcare costs across numerous surgical and medical disciplines. Although characterized in other surgical fields, the population-based incidence, outcomes, and cost of delirium have not been assessed in major urologic cancer surgeries. We sought to evaluate the incidence, outcomes, and cost of postoperative delirium after major urologic cancer surgeries, specifically after radical prostatectomy (RP), radical nephrectomy (RN), partial nephrectomy (PN), and radical cystectomy (RC) in the USA. We have also developed a preoperative risk prediction model specific to major urologic cancer surgeries to identify patients at high risk for postoperative delirium. Methods Using the Premier Hospital Database, we retrospectively identified patients who underwent radical prostatectomy (RP), radical nephrectomy (RN), partial nephrectomy (PN), and radical cystectomy (RC) from 2003 to Postoperative delirium was identified using ICD-9 codes, as well as postoperative use of antipsychotics, sitters, and restraints. We constructed regression models to assess for mortality, discharge disposition, length of stay (LOS), and direct hospital costs. A preoperative risk stratification scoring system was also developed using known risk factors of delirium. The entire cohort was randomly divided into training (70%) and validation (30%) cohorts. Preoperative patient, hospital, and surgical characteristics associated with delirium were analyzed using multivariate regression, and a risk prediction score was developed 2
3 using the training cohort. Its performance was quantified using Receiver Operating Characteristic (ROC) analysis in both cohorts. Results We identified 165,387 patients representing a weighted total of 1,097,355 patients. 30,063 (2.7%) experienced postoperative delirium. The greatest incidence of delirium occurred after RC, with 6,268 cases (11%). Delirious patients had greater adjusted odds of in-hospital mortality (OR 3.65; p <0.001), 90-day mortality (OR 1.47; p = 0.013), discharge with home health services (OR 2.25; p <0.001), discharge to skilled nursing facilities (OR 4.64; p <0.001), and 0.9-day increase in median LOS (p <0.001). Delirious patients also experienced a $2,697 increase in direct admission costs (p <0.001), with the greatest costs in RC patients ($30,859 vs. $26,607; p<0.001). The largest driver of costs was in room and board across all surgeries (p<0.001). Our training and validation cohorts consisted of a weighted total of 767,408 and 329,926 patients, respectively. Our final model revealed many factors that increase risk for delirium, all which were used to create a preoperative risk score. The additive score was predictive of delirium in both the training (OR: 1.35, 95% CI, , p<0.001) and validation cohorts (OR: 1.34, 95% CI , p<0.001). The score also demonstrated good discrimination in predicting delirium in the training (AUC: 0.74, 95% CI, ) and validation (AUC: 0.75, 95% CI, ) cohorts. Conclusion Patients with postoperative delirium experienced worse outcomes, prolonged LOS, and increased admission costs following major urologic cancer surgeries. In particular, the largest incidence and costs occurred in delirious patients after RC. Moreover, the results of the pre- 3
4 operative risk prediction tool for delirium following major urologic cancer surgeries are promising given their consistency with published delirium risk factors and ease of use. Further testing will shed light on its clinical utility. Keywords postoperative delirium, risk prediction, cystectomy, prostatectomy, nephrectomy, nephrectomy, healthcare costs, outcomes 4
5 TABLE OF CONTENTS Section Page Abstract Glossary and Abbreviations Introduction Methods Results Discussion Conclusion, Summary, and Future Directions Tables and Figures References Appendix
6 Glossary of Abbreviations GU Genitourinary RP Radical Prostatectomy RN Radical Nephrectomy PN Partial Nephrectomy RC Radical Cystectomy ICU Intensive Care Unit ICD-9 International Classification of Disease, Ninth Revision CCI Charlson Comorbidity Index LOS Length of Stay ROC Receiver Operating Characteristic AUC Area Under the Curve BMI Body Mass Index CI Confidence Interval OR Odds Ratio IQR Interquartile Range IRR Incidence Rate Ratio USD United States Dollars 6
7 Introduction Delirium is defined as an acute decline in cognitive function and is associated with cognitive deficits in memory, perception, and altered thoughts or fluctuations in consciousness (1,2). It is a common complication among elderly hospitalized patients and has been associated with increased adverse outcomes across medical and surgical disciplines. For example, past studies have identified an increase in-hospital and one-year mortality in patients with delirium. In addition, delirium has been associated with postoperative complications and poor postoperative recovery resulting in increased length of stay and discharge to rehabilitation (3). Recent evidence also suggests that the cognitive impact of delirium may include long lasting mental health conditions such as cognitive impairment (4) and post-traumatic stress disorder (5). As a result, it is estimated that the management of delirium contributes $38 billion to $152 billion per year to healthcare spending in the US (6). Although delirium has been extensively studied in other surgical fields, research on the incidence and outcomes of postoperative delirium in urologic cancer surgeries remains sparse. Several studies have estimated the incidence of postoperative delirium to be between 6.0% and 9.0% following radical prostatectomy (7), and between 1.8% to 29% following radical cystectomy (8,9). However, such studies have been limited by small sample sizes and restricted to single institutions. Similar research into patient and hospital outcomes of postoperative delirium in urologic cancer surgeries have been limited by small sample sizes (8). To date, population-based approaches to analyze postoperative delirium in urologic cancer surgeries have not been performed. 7
8 In regards to risk prediction rules for delirium, several tools have previously been described in the perioperative setting. Marcantonio et al. was first to construct a clinical risk prediction rule to identify postoperative delirium in non-cardiac surgeries; however, urologic surgeries had been under-represented in the sample (10). Recently, Rudolph et al. developed a generalized risk stratification model for medical and surgical delirium at a tertiary Veterans Administration hospital; however, the study also under-represented urologic surgeries in the sample (11). Other delirium risk prediction tools for delirium have also been constructed exclusively for specific surgical specialties such as cardiac, vascular and orthopedic surgeries (12-15). While such models seem promising, most rely on resource-intense cognitive tests that may limit their clinical utility, especially in a busy clinical practice (10,14). Currently, no convenient preoperative risk prediction model specific to urologic cancer surgeries has been released. The purpose of this investigation is to perform a contemporary population-based analysis to estimate the incidence, cost, and outcomes associated with postoperative delirium after major urologic cancer surgeries, as well as construct a preoperative risk prediction rule to preemptively identify patients at high-risk for this condition. Specifically, we will first characterize the incidence of delirium after radical prostatectomy (RP), radical nephrectomy (RN), partial nephrectomy (PN), and radical cystectomy (RC) in the entire cohort. We will then delineate the association between postoperative delirium and negative outcomes that affect patients, as well as demonstrate the economic impact of this complication. In addition, to facilitate the construction of the preoperative risk prediction model, we will first randomly divide the cohort into both training and validation cohorts. We will then construct a preoperative risk prediction model for 8
9 postoperative delirium in the training cohort and finally assess the performance of this risk model in the validation cohort. 9
10 Methods Data Source The Premier Hospital Database (Premier Inc., Charlotte, NC, USA) is an all payer hospital discharge database that contains more than 45 million inpatient discharges from over 700 hospitals across the USA, amounting to approximately 20% of total annual discharges. Longitudinal analysis was possible because of unique patient identifiers. This study received exemption from our hospital Institutional Review Board. Overall Study Cohort and Covariates Using International Classification of Disease, ninth revision (ICD-9) diagnosis and procedure codes, we identified all adult patients who underwent RP, RN, PN, and RC from 2003 to 2013 (Table 8). Patient, hospital, and surgical characteristics associated with outcomes and costs were captured. Patient characteristics included age (<60, 60-69, 70-79, and 80 years), gender, race (White, Black, Hispanic, and other/unknown), marital status (unmarried and married), insurance status (Medicare, Medicaid, private, and other), and obesity. Hospital characteristics included teaching status, hospital size (<400, , and >600 beds), location (urban and rural) and geographical region (Northeast, Midwest, West, and South). Surgical characteristics included type of surgery (RP, RN, PN, and RC), operative time (0-4, 4-6, 6-8, and 8+ hours), and surgical approach (open vs. laparoscopic and robotic). 10
11 Identification of Postoperative Delirium Retrospectively identifying postoperative delirium using ICD-9 codes has been previously reported to be specific but not sensitive (16). To augment our capture rate, we utilized a composite of surrogate variables that identify unique elements of delirium management identified in a patient s hospital bill. These include ICD-9 diagnosis codes (Table 9), as well as postoperative use of sitters, restraints, and antipsychotics (2,17-21). To reduce misclassification bias, we excluded the use of restraints on the day of surgery or in the Intensive Care Unit (ICU). Antipsychotic medications such as haloperidol, risperidone, olanzapine, and quetiapine have previously been commonly used in the treatment of delirium (21), and their postoperative use was subsequently identified to capture management of postoperative delirium. Duration of delirium was calculated as the number of consecutive post-operative days in which at least one of the antipsychotics, sitters, or restraints was used. Outcomes and Cost Outcomes include direct hospital admission costs, in-hospital mortality, 90-day mortality, hospital length of stay (LOS), and discharge disposition such as home with healthcare, skilled nursing facility, and other (e.g. short-term general hospital, or hospice). In-hospital mortality was defined as Clavien 5 (postoperative mortality) of the Clavien classification system, which is recommended by the International Consultation on Urological Disease European Association of Urology (22). The Premier Hospital Database provides direct hospitalization costs that are distinct from hospital charges and do not need to be converted from hospital charges (23). Direct hospital costs were further subdivided into categories (e.g. room and board, radiology, or operative room costs) 11
12 to compare resource utilization among different types of urologic cancer surgeries. To facilitate comparison, all costs were adjusted to 2013 US dollars using the medical component of the Consumer Price Index. Construction of Training and Validation Cohorts and Identification of Preoperative Risk Factors The aggregate cohort was randomly divided into training (70%) and validation (30%) cohorts. Preoperative patient, hospital, and surgical characteristics were analyzed in both cohorts. Patient characteristics included age (<60, 60-69, 70-79, and 80 years), gender, race (White, Black, Hispanic, and other/unknown), marital status (unmarried and married), insurance status (Medicare, Medicaid, private, and other), obesity, and comorbid conditions. Hospital characteristics included teaching status, hospital size (<400, , or >600 beds), location (urban and rural) and geographical region (Northeast, Midwest, West, or South). Surgical characteristics included surgery type (RP, RN, PN, or RC), operative time (0-4, 4-6, 6-8, and 8+ hours), and surgical approach (open vs. laparoscopic/robotic). Predisposing risk factors of delirium such as history of sleep disturbances, hearing impairment, vision impairment, dementia, depression and/or anxiety, alcohol abuse, and preoperative immobility have been well-established in the literature (3,24,25). Preoperative patient, hospital, and surgical characteristics were analyzed in both training and validation cohorts (Table 2). Statistical Analysis Patient, hospital, and surgical characteristics for patients were summarized using descriptive statistics. Categorical variables were compared using chi-squared tests while 12
13 continuous variables were assessed via Students t-test. Binary and multivariable logistic regression was used to analyze 90-day mortality and discharge disposition, respectively. Hospital direct admission costs were analyzed using a multivariable generalized linear model conforming to a gamma distribution to account for skewed distribution of costs. Hospital LOS was modeled using negative binomial regression. Preoperative delirium risk factors from relevant patient and hospital characteristics; comorbidities; and surgical characteristics were analyzed using univariate and multivariate logistic regression for the training cohort. The results of the multivariable model from the training cohort were used to construct a risk prediction score based on the non-transformed beta coefficients. The risk score as a continuous variable was further stratified into categorical risk groups (low, intermediate, high, and very high risk) roughly based on the corresponding mean and standard deviation. Performance of the risk score was quantified and validated using Receiver Operating Characteristic (ROC) analysis in both the training and validation cohorts. All models were survey-weighted, clustered by hospitals to achieve nationally representative estimates, and adjusted for all relevant patient, hospital, and surgical characteristics. Statistical analysis was performed on Stata version 14.1 (College Station, TX). All tests were two-sided, and a p-value <0.05 was considered statistically significant. 13
14 Results Overall Characteristics of Hospitals and Patients Baseline patient, hospital, and surgical characteristics of patients with and without postoperative delirium are outlined in Table 1. The final cohort was made up of 165,387 patients, representing a weighted population of 1,097,335 patients in the United States from 2003 to Following stratification by type of surgery, a weighted total of 630,353 patients undergoing RP, 305,503 patients for RN, 104,217 patients for PN, and 241,263 for RC were identified. Statistically significant, preoperative characteristics were identified in patients with postoperative delirium. The mean age of patients experiencing delirium was 68.3 years vs years in those without delirium (p <0.001). A greater percentage of delirious patients were male (66.5% vs. 60.7%; p <0.001), white (75.4% vs. 71.2%; p = 0.001), and unmarried (46% vs. 33%; p <0.001). Such patients tended to have a greater number of comorbidities, reflected by a higher proportion of patients with Charlson Comorbidity Index (CCI) score greater than or equal to 4 (36% vs. 11%; p <0.001). These patients were also more likely to utilize either Medicare (69.7% vs. 39.5%) or Medicaid (5.6% vs. 2.4%; p <0.001). Patients with delirium experienced longer operative times of either 6 to 8 hours (12.1% vs. 6.5%) or greater than 8 hours (13.7% vs. 73%; p <0.001), and underwent a greater percentage of open surgical approaches vs. laparoscopic or robotic approaches (64.2% vs. 51.1%; p <0.001). In regards to pre-disposing risk factors, patients with postoperative delirium had increased sleep difficulties (p<0.001), hearing loss (p<0.001), vision loss (p = 0.003), dementia (p<0.001), depression/anxiety (p<0.001), alcohol abuse (p<0.001), and baseline immobility (p<0.001). Higher rates of comorbidities that include congestive heart failure, chronic pulmonary disease, cerebrovascular disease, diabetes, liver 14
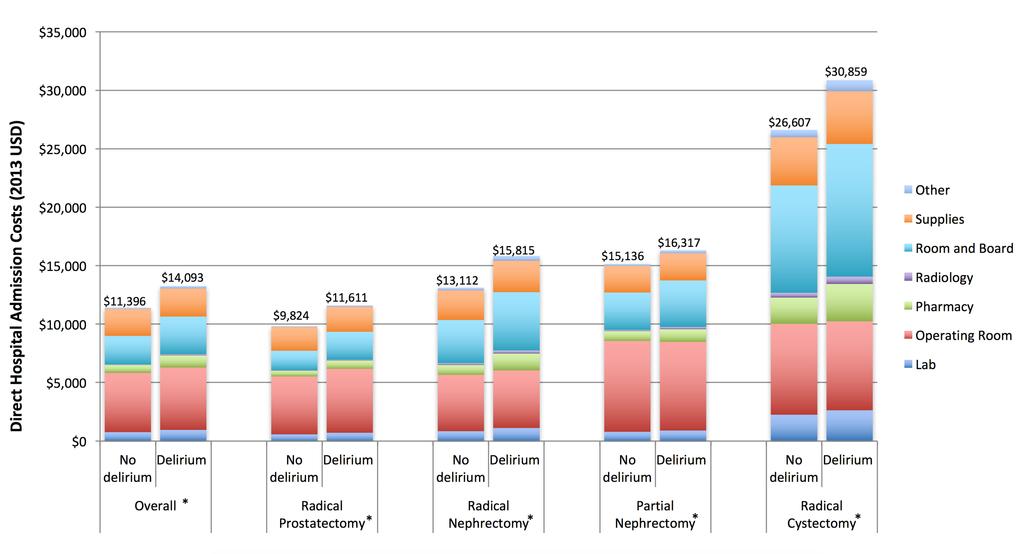
15 disease, metastatic solid tumors, peripheral vascular disease, and renal disease (p <0.001) were also found. No statistically significant differences were identified among hospital size, location, region, or teaching hospital status in patients with and without delirium. Incidence, Onset, and Duration of Delirium A weighted total of 30,063 patients (2.7%) experienced postoperative delirium (Table 3). When stratified by type of surgery, 5,986/630,353 (1.0%; 95% CI, 0.8%-1.1%) of RP patients experienced postoperative delirium while 14,431/305,503 (4.7%; 95% CI, 4.4%-5.1%) and 3,377/103,217 (3.2%; 95% CI, 2.8%-3.8%) patients experienced this after RN and PN, respectively. The highest incidence of delirium was identified to be 6,268/57,262 (11.0%; 95% CI, 10.0%-11.9%) in the in the RC cohort. The median duration of delirium was similar across all types of surgeries at 2 days, albeit with different interquartile ranges of 1 to 3 days (RP), 1 to 5 days (RN), 1 to 4 days (PN), and 1 to 5 days (RC). Cost and Outcomes Patients with delirium also experienced a $2,697 (95% CI $2,250-$3,3144; p <0.001) increase in direct hospital admission costs compared with those without delirium. When subdivided by types of hospital costs, patients with delirium incurred a higher total cost of inpatient lab, pharmacy, radiology, room and board, operating room, supply, and other expenses across all urologic cancer surgeries (p <0.001) (Figure 1). In particular, the greatest difference in direct hospital admission costs is seen in delirious patients after RC ($30,859 vs. $26,607; p<0.001). 15
16 Patients with postoperative delirium had a greater risk of adverse outcomes and increased hospital costs (Table 4). After adjusting for relevant patient, surgical, and perioperative characteristics, patients with delirium were more likely to experience both in-hospital mortality (OR, 3.71; 95% CI, ; p <0.001) and 90-day mortality (OR, 1.48; 95% CI, ; p = 0.012) than those without delirium. Moreover, delirious patients were more likely to be discharged to higher level care facilities, which include disposition to home with additional health care (OR, 2.39; 95% CI, ; p <0.001) or disposition to skilled nursing facilities (OR, 4.98; 95% CI, ; p <0.001). Length of stay also varied significantly based on the presence of delirium. On adjusted analysis, patients with delirium experienced a 0.90-day increase in hospital stay (95% CI, ; p <0.001). Training and Validation Cohorts Our aggregate cohort was randomly subdivided into training and validation cohorts of 115,770 and 49,617 patients from 490 hospitals, respectively. These values represented a weighted population of 767,408 patients in the training cohort and 329,926 patients in the validation cohort. Following stratification by surgery type, the training cohort consisted of 440,684 patients undergoing RP; 214,099 patients for RN; 72,354 patients for PN, and 40,271 for RC. The validation cohort consisted of 189,669 patients undergoing RP; 91,403 for RN; 31,863 for PN, and 16,991 for RC. Baseline characteristics, risk factors, and preoperative co-morbidities of patients of training and validation cohorts are outlined in Table 2. Overall, the training and validation cohorts were similar in their preoperative patient, hospital, and surgical characteristics. Despite random assignment, the training cohort consisted of fewer people with obesity (p = 0.02), a 16
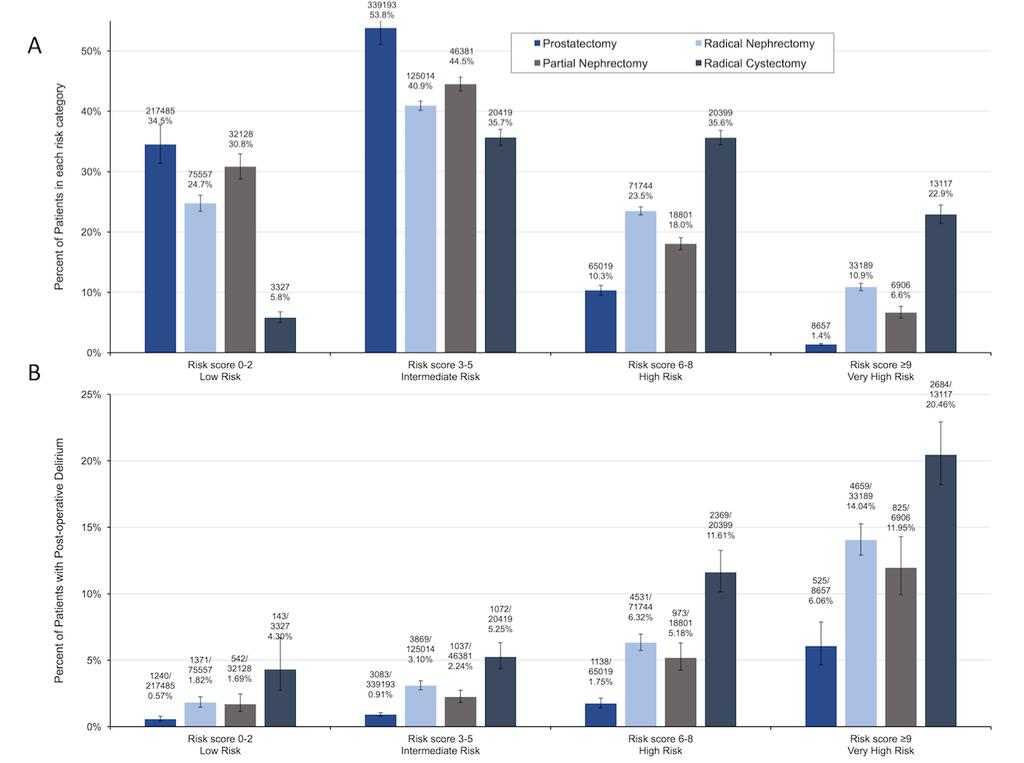
17 higher rate of cerebrovascular disease (p = 0.05), and a lower rate of peripheral vascular disease (p = 0.03). Identifying Preoperative Risk Factors of Delirium Multivariate logistic regression model was developed using preoperative patient-specific and surgical characteristics suggested to be associated with postoperative delirium (Table 5) (26,27). This adjusted model demonstrated in the training cohort that male, white, and unmarried patients had significantly greater adjusted odds of developing postoperative delirium in all genitourinary (GU) surgeries. Compared to patients younger than 60 years old, patients aged 70 to 79 years (OR: 3.03; 95% CI: ; p <0.001) and patients aged greater or equal to 80 years (OR: 1.90; 95% CI: , p<0.001) had a significantly higher risk of postoperative delirium. A history of alcohol dependence (OR: 4.43; 95% CI: ; p <0.001), dementia (OR: 3.38; 95% CI: ; p <0.001), and immobility (OR: 4.05; 95% CI: ; p <0.001) had the strongest association with postoperative delirium. Many additional medical comorbidities were also significantly associated with delirium; however, significant associations with postoperative delirium were not found in patients with obesity, peripheral vascular disease, and liver dysfunction. Many of the risk factors found to be significant in our multivariable model remained significant after stratification by type of surgery. Delirium Risk Prediction Model Our preoperative risk prediction model constructed from the training cohort data is shown in Table 6. The mean score in patients without delirium was 3.9 (SD 2.3) compared to 6.7 (SD 3.6) in patients with delirium (p <0.001). Numerical scores of the preoperative delirium risk 17
18 prediction model were further categorized into low (risk score 0-2), intermediate (risk score 3-5), high (risk score 6-8), and very high (risk score 9) risk groups (Figure 3). The majority of patients undergoing RP were found to be in the low to intermediate risk group (88.3%), while those undergoing RC had the highest percentage of patients at the high and very high risk category (58.5%). Figure 3B illustrates the percentage of patients that have developed postoperative delirium by surgery type and risk category. In each of the four surgeries, increasing delirium risk was associated with increased delirium. In particular, RC had the highest incidence of delirium across all surgeries, with 4.30% at low-risk, 5.25% at intermediate risk, 11.61% at high risk, and 20.46% at very high-risk. Evaluation of the Clinical Prediction Score Each added point on the risk score was associated with an increased predicted probability of developing postoperative delirium across all GU surgeries (OR: 1.35; 95% CI: ; p <0.001, Figure 2A in blue) in the training cohort. Additional analysis on the validation cohort yielded similar results (OR: 1.34; 95% CI: ; p <0.001, Figure 3A in red). The risk score was also predictive of delirium by surgery type in both the training and validation cohorts (Figure 2B). The risk prediction model demonstrated good calibration in predicting postoperative delirium across all GU surgeries in both the training (ROC area: 0.74; 95% CI: ) and validation cohorts (ROC area: 0.75; 95% CI: , Figure 2B). Its predictive power was maintained with corresponding ROC values for both training and validation cohorts when stratified by surgery type. 18
19 Discussion This study performed the first contemporary, population-based analysis of postoperative delirium in major urologic cancer surgeries. The overall incidence of postoperative delirium was 2.7%. Stratification by type of surgery revealed a similar duration of delirium but different estimates of incidence, with the highest incidence of 11% in RC patients. Patients who developed postoperative delirium following urologic cancer surgeries had worse outcomes in mortality, disposition to higher level care facilities, length of hospital stay, and hospital costs. In particular, the high direct hospital admission costs were the result of increasing laboratory, room and board, and hospital staffing expenses required to care for patients with delirium. Moreover, our preoperative risk prediction score of postoperative delirium has revealed a wide range of clinically relevant risk factors that contribute to the risk of postoperative delirium (Table 6). Each 1-point increase in the risk score corresponds to a 1.34 (validation) to 1.35 (training) increase in odds of developing delirium. Further stratification of the score in risk categories reveals a stepwise increase in delirium incidence from the low to very high risk groups (Figure 3B). In particular, patients following RC are found to be in the high to very high risk categories, which correlate with higher rates of postoperative delirium. Although research on postoperative delirium has been extensive in other surgical specialties, prior investigations in delirium following urologic cancers surgeries have been less robust and have been differentiated by methods used to measure this condition. For example, in the context of bladder cancer and radical cystectomy, Shabsigh et al. estimated the incidence of postoperative delirium to be 1.8% via a retrospective, chart-based approach (28). This estimate suggests that such postoperative complications are coded as rare events in a patient s hospital 19
20 course. In contrast, in a single institution, prospective pilot study, Large et al. demonstrated that the incidence of postoperative delirium, when measured with standardized criteria such as the Confusion Assessment Method (29), was much higher at 29% (23). Our population-based analysis identified the incidence of delirium to be 11% after RC, a finding that is not only between the two previous estimates, but also one that affirms the significant burden of delirium following RC. The incidence of delirium after urologic cancer surgeries follows a similar pattern in other procedures, with lower reported incidences when using chart-based, retrospective assessments (particular nephrectomy at 0.25% (3) and radical prostatectomy at 6% to 9%(28)). Because our approach combines information from ICD-9 coding, acute medication use, postoperative restraints, and use of sitters to increase the sensitivity of our capture rate, our estimates falls in-between retrospective and prospective estimates. Understanding the financial impact of delirium remains essential to effectively utilize resources and improve clinical management. In the surgical setting, the financial impact of delirium has only been demonstrated after elective orthopedic surgery. Franco et al. demonstrated an increase in the technical, or supply-related costs associated with delirium but did not examine the granular detail outlining specific costs increases by procedure type (30). Our results, in contrast, provide a population-based analysis that highlights the effects of postoperative delirium on the utilization of hospital resources across major urologic cancer surgeries in the US. In particular, our results illustrate the $4,252 increase in direct hospital admission costs to care for patients with delirium following RC. With the growing number of elderly patients with high perioperative risk undergoing this procedure for muscle-invasive bladder cancer, these results affirm the need to devise novel strategies to effectively prevent and manage this complication. 20
21 The population undergoing urologic cancer surgeries has become increasingly vulnerable to postoperative complications such as delirium, in part due to issues such as increased number of comorbidities, increased frailty, and decreased physiologic reserve (31). In the setting of bladder cancer, radical cystectomy remains one of the most complex procedures in urologic cancer surgery. Despite improvements in perioperative care and surgical techniques, radical cystectomy remains burdened with high rates of morbidity (28% to 57%) and mortality (2% to 5%) (32). Preoperative identification of the risk of these patients including the risk of postoperative delirium would enable targeted delirium surveillance, implementation of preventative strategies, and a thorough disclosure of risk versus benefit. Marcantonio et al. was the first to design a postoperative delirium risk prediction rule for non-cardiac surgeries, (10) and subsequently, other risk prediction tools have been designed for use in other types of medical and surgical fields (11,14,15). Similar to prior models and analyses of preoperative risk factors for delirium, our model highlights predisposing risk factors such as cognitive impairment, older age, male gender, functional impairment, sensory impairment, depression, and increased comorbidities were highly associated with delirium in urologic cancer surgeries. In particular, dementia, alcohol abuse, and immobility were the most significant risk factors for delirium (26,33). Finally, while most prior risk prediction models are oftentimes labor intensive and require a battery of clinical instruments, our risk prediction model incorporates readily available patient information without the use of involved assessments to enhance perioperative planning for patients at high risk of delirium. At present, the etiology of postoperative delirium remains incompletely understood. Recent evidence, however, suggests that delirium can be triggered by the release of inflammatory mediators resulting in neuroinflammatory changes (34). The relationships between 21
22 surgical approach and postsurgical inflammatory cytokine pathways with delirium may provide additional insights. For example, Fracalanza et al. has demonstrated increased levels of C- Reactive Protein (CRP) and Interleukin 6 (IL-6) following open radical prostatectomy vs. robotic-assisted laparoscopic prostatectomy, suggesting that an open surgical approach may contribute to worsened post-surgical inflammation (35). Other studies have corroborated these findings of higher postoperative IL-6 levels in patients undergoing open colon surgery and cholecystectomy compared to laparoscopic approaches (36,37). Higher preoperative and postoperative levels of inflammatory markers such as CRP and IL-6 have been associated with postoperative delirium (8). Therefore, the increased inflammatory mediators released after an open surgical approach may be the underlying mechanisms driving the association with delirium found in this study. However, the decision to proceed with an open vs. minimally invasive approach often hinges on patient-specific and tumor-specific characteristics, and it is reasonable to suggest that patients who are not candidates for minimally invasive surgery have additional, unmeasured confounders that increase the risk of delirium. Therefore, further investigation is necessary to elucidate the mechanisms behind postoperative delirium and surgical approach in urologic cancer surgeries. In the era of healthcare quality, the management of postoperative delirium has become an increasing priority. In the surgical setting, early geriatric medicine consultation has been shown to reduce the incidence and severity of postoperative delirium in hip fracture patients (38), a finding that increasingly emphasizes the multidisciplinary role of delirium management. Other programs such as the Hospital Elder Life Program, which utilizes multidisciplinary teams to implement strategies such as reorientation, sensory support, hydration protocols, and sleep optimization, have shown considerable benefit and cost savings of roughly $9000 per year (39). 22
23 Moreover, several different pharmacological approaches have been considered to target specific features of delirium. For example, strategies such as the use of melatonin have been proposed to regulate the circadian rhythm of postsurgical patients (40,41). Additional pharmacologic strategies have also focused on reducing medications that increase risk of delirium such as opioids, anticholinergics, and sedatives (7). Finally, emerging data on the perioperative management of high risk patients suggest that reducing anesthetic depth and initiating prophylactic low-dose haloperidol may reduce postoperative delirium (30). Overall, the predictive risk stratification model that we developed in the current study may serve to better identify those patients at risk and to apply targeted interventions to prevent postoperative delirium among patients undergoing major urologic cancer surgery. Several important limitations must be taken into consideration. Classically, postoperative delirium has been diagnosed by applying diagnostic criteria after a comprehensive mental status interview (28,32). Moreover, retrospective identification of delirium using features of an administrative database including ICD-9 diagnostic codes has been reported to be specific but not sensitive due to the lack of clinical granularity required for a sufficient diagnosis (16,42). As a result, prior studies that have utilized this approach have suffered from limited interpretability. In contrast, our population-based approach used a combination of ICD-9 codes and other elements that represent postoperative delirium management and treatment to improve our capture rate. Nonetheless, it is possible that this combination still under-represents the true rates of postoperative delirium. Moreover, certain risk factors such as immobility, hearing loss, and vision loss have traditionally been quantified using interviewer-based clinical instruments(11) and may be subject to unmeasured confounding. 23
24 Other limitations of our study include sampling of US hospitals, a consequence that may not accurately represent the incidence, outcomes, and cost of postoperative delirium in other countries. Moreover, to minimize sampling bias, clustered statistical analysis while accounting for survey weights were used. Misclassification bias due to coding errors may also exist due to the secondary analysis performed on administrative data. Finally, detailed oncological and clinical information such as tumor staging, grade, and pathological characteristics, chemotherapy use, American Society of Anesthesiologists score, and use of postoperative care pathways and outpatient management strategies could not be reliably captured with the available data. 24
25 Conclusions, Summary, and Future Directions In conclusion, this contemporary evaluation of postoperative delirium in patients undergoing radical prostatectomy, radical nephrectomy, partial nephrectomy, and radical cystectomy in the US found that patients with postoperative delirium experience increased mortality, prolonged LOS, and higher direct hospital costs. In particular, the greatest incidence and adverse outcomes of postoperative delirium occur in patients undergoing radical cystectomy. Our results also illustrate the first population-based, preoperative risk prediction model for postoperative delirium in patients undergoing major urologic cancer surgeries. The results of our risk prediction model are promising given its overall consistency with published delirium risk factors and ease of use to identify patients at differing levels of risk for postoperative delirium. Our score could be used to help identify patients at a high risk of developing postoperative delirium in order to initiate targeting interventions and prevention strategies. However, further testing of this model will ultimately shed insight on its overall clinical utility. Most importantly, continued research in developing preventative strategies for delirium is essential for increasing the quality of contemporary urologic surgical care. 25
26 Tables and Figures Table 1 Patient, Hospital, and Surgical Characteristics for patients with and without postoperative delirium following radical prostatectomy, radical nephrectomy, partial nephrectomy, and radical cystectomy in the USA from 2003 to Radical Prostatectomy N = 630,353 Radical Nephrectomy N = 305,503 Delirium Status No Yes P-value No Yes Partial Nephrectomy N = 104,217 P- value No Yes N = 3,377 N = 50,993 Radical Cystectomy N = 57,261 P- value No Yes P-value N = 6,268 Variables N = 624,367 N = 5,986 N = 291,072 N = 14,431 N = 100,839 Patient Characteristics Age, (%) < < < < < Gender, (%) Male Female - $ Race, (%) White Non-white BMI (kg/m 2 ), (%) Obesity ( 30) Not obese (<30) Marital Status, (%) Married < < Not married Insurance Status, (%) Medicare Medicaid < < < <0.001 Private Other
27 <0.001 <0.001 <0.001 <0.001 Charlson Comorbidity index, (%) Hospital Characteristics Hospital beds, (%) < > Teaching Hospital, (%) Vicinity to city center, (%) Rural Urban Region, (%) Midwest Northeast South West Surgical Characteristics Lymph Node Dissection, (%) Lap/Robotic, (%) Open surgery, (%) Lap/Robotic, (%) < Operative time (hours) < < < PRBC Transfusion 0-4 units < < < < units ICU Admission < < < <
28 All patients received a baseline Charlson Comorbidity Index score of 2 due to presence of tumor without metastasis $Gender N/A for Radical Prostatectomy patients PRBC = Packed Red Blood Cells ICU = Intensive Care Unit 28
29 Table 2 Patient, Hospital, and Surgical Characteristics of the Training and Validation Cohorts Variable N = 767,408 Training N = 329,926 Validation P-value Patient Characteristics Age in yr., no. (%): 0.14 < (37.3) (37.8) (40.2) (40.3) (18.2) (17.7) (4.3) (4.3) Gender, no. (%): 0.85 Male (83.4%) (83.4%) Female (16.6%) (16.6%) Race, no. (%): 0.39 White (71.2) (71.5) Non-white (28.8) (28.5) BMI (kg/m 2 ), no. (%): 0.02 Obese ( 30) (93.1) (93.5) Not obese (<30) (6.9) (6.5) Marital Status, no. (%): 0.89 Married (66.7) (66.6) Not married (33.3) (33.4) Insurance Status, no. (%): 0.10 Medicare (40.5) (39.8) Medicaid (2.5) 8300 (2.5) Private (51.8) (52.4) Other (5.2) (5.3) Charlson comorbidity index, no. (%): (65.6) (65.5) (22.1) (22.2) (12.3) (12.3) Hospital Characteristics Hospital beds, no. (%): 0.48 < (11.3) (11.5) (39.8) (39.4) (27.4) (27.8) > (21.5) (21.3) Teaching Hospital, no. (%): (29.3) (29.4) 0.80 Vicinity to city center, no. (%): Rural (4.1) (4.1) Urban (95.9) (95.9) Region, no. (%): 0.39 Midwest (21.8) (22.2) Northeast (17.2) (17.3) South (39) (38.6) West (22) (22) Delirium Risk Factors Sleep Difficulties, no. (%): (4.5) (4.6) 0.52 Hearing Loss, no. (%): 5520 (0.7) 2634 (0.8) 0.09 Vision loss, no. (%): 8297 (1.1) 3613 (1.1) 0.81
30 Dementia, no. (%): 1701 (0.2) 578 (0.2) 0.12 Depression/Anxiety, no. (%): (2.2) 6904 (2.1) 0.51 Alcohol abuse, no. (%): 5730 (0.8) 2388 (0.7) 0.66 Immobility, no. (%): 379 (0.1) 122 (0) 0.39 Comorbidities Congestive Heart Failure, no. (%): (2.8) 9305 (2.8) 0.85 Chronic Pulmonary Disease, no. (%): (12.3) (12.3) 0.99 Cerebrovascular disease, no. (%): (1.6) 4845 (1.5) 0.05 Diabetes, no. (%): (17) (17.1) 0.81 Liver disease, no. (%): 2683 (0.4) 1070 (0.3) 0.51 Metastatic solid tumor, no. (%): (5.5) (5.7) 0.18 Peripheral vascular disease, no. (%): (2.2) 7761 (2.4) 0.03 Renal Insufficiency, no. (%): (5.6) (5.6) 0.95 Surgical Characteristics Surgery, no. (%): 0.57 Prostatectomy (57.4) (57.5) Radical Nephrectomy (27.9) (27.7) Partial Nephrectomy (9.4) (9.7) Radical cystectomy (5.3) (5.2) Operative time (hours), no. (%): (58) (57.2) (28) (28.5) (6.6) (6.7) (7.4) (7.7) Lymph Node Dissection, no. (%): (32.1) (32.1) 0.85 Surgical Approach, no. (%): 0.36 Open Surgery (51.3) (51.6) Laparoscopic/Robotic (48.7) (48.4) All patients received a baseline Charlson Comorbidity Index score of 2 due to presence of tumor without metastasis 30
31 Table 3 Incidence, Duration, and Onset of Postoperative Delirium in Four Major Urologic Cancer Surgeries Overall N = 1,097,335 RP N = 630,353 RN N = 305,503 PN N = 104,217 RC N = 57,262 Delirium Status No Yes No Yes No Yes No Yes No Yes Incidence (%) 1,067,272 (97.3) 30,063 (2.7) 624,367 (99.1) 5,986 (1) 291,072 (95.3) 14,431 (4.7) 100,839 (96.8) 3,377 (3.2) 50,993 (89.1) 6,268 (11) Duration (days), Median (IQR) - 2 (1, 4) - 2 (1, 3) - 2 (1, 5) - 2 (1, 4) - 2 (1, 5) RP = Radical Prostatectomy, RN = Radical Nephrectomy, PN = Partial Nephrectomy, RC = Radical Cystectomy 31
32 Table 4 Mortality, discharge disposition, direct admission costs, and hospital length of stay outcomes associated with postoperative delirium in the USA from 2003 to All costs were inflated to 2013 US dollars Categorical outcomes 90-d Mortality, no. (%): Disposition, no. (%): Unadjusted Analysis Adjusted Analysis $ Overall No Delirium Delirium OR (95% CI) P-value OR (95% CI) P-value (0.5) (0.4) (4.7) ( ) <0.001 ( ) Home Health Care 97,763 (8.9) 91,059 (8.5) 6,704 (22.3) 4.66 ( ) < ( ) <0.001 Skilled Nursing Facility 29,865 (2.7) 23,249 (2.2) 6,616 (22) 18.0 ( ) < ( ) <0.001 In-Hospital Death 3,936 (0.4) 2,801 (0.3) 1,135 (3.8) 25.7 ( ) < ( ) <0.001 Other 4061 (0.4) 3403 (0.3) 659 (2.2) 12.3 ( ) < ( ) <0.001 Unadjusted Analysis Adjusted Analysis $ Continuous Outcomes Overall No Delirium Delirium β (95%CI) P-value β (95%CI) P-value Admission Cost (USD), Median (IQR) 10,876 (8,131, 14,977) 10,771 (8,079, 14,718) 18,710 (12,170, 31,534) 17,261 (15,602-18,919) < ,697 (2,250-3,144) <0.001 Length of Stay (days), Median (IQR) 3 (2, 4) 3 (2, 4) 7 (4, 11) 6.18 (5.7, 6.7) < ( ) <0.001 LOS = Length of Stay, IQR = Interquartile Range, USD = United States Dollars, OR = Odds Ratio, CI = Confidence Interval, β = Beta Coefficient $Adjusted for delirium, patient (age, race, gender, marital status, obesity, Charlson Comorbidity Index, Insurance status), hospital (size, teaching status, region, urban vs. rural), and perioperative characteristics (type of surgery, open vs. minimally invasive, OR time, number of packed RBC use greater than 4 units, ICU admission, soft tissue infection, sepsis, urinary tract infection, other postoperative infections, pneumonia, aspiration, ileus, peritonitis, perforation, GI hemorrhage, acute renal failure, DVT, arrhythmias, myocardial infarction, cardiac arrest, respiratory failure, and cerebrovascular incident) 32
33 Table 5 Preoperative Risk Factors of Delirium for the Training Cohort Covariates Multivariate $ All GU Surgeries OR (95% CI), Significance Multivariate RP OR (95% CI), Significance Multivariate PN OR (95% CI), Significance Multivariate RN OR (95% CI), Significance Multivariate RC OR (95% CI), Significance Age <60 Ref Ref Ref Ref Ref [ ] 0.94 [ ] 1.26 [ ] 1.20 [ ] 1.18 [ ] [ ] *** 1.24 [ ] 1.86 [ ] *** 2.17 [ ] *** 2.09 [ ] *** [ ] *** 2.01 [ ] 4.39 [ ] *** 3.45 [ ] *** 2.74 [ ] *** White Race 1.15 [ ] * 1.16 [ ] 1.13 [ ] 1.15 [ ] 1.17 [ ] Male 1.29 [ ] *** [ ] 1.22 [ ] ** 1.61 [ ] *** BMI (kg/m 2 ) [ ] 1.01 [ ] 1.12 [ ] 1.14 [ ] 1.16 [ ] Unmarried 1.38 [ ] *** 1.97 [ ] *** 1.30 [ ] 1.20 [ ] ** 1.29 [ ] ** Sleep Disturbance 1.21 [ ] * 1.32 [ ] 1.85 [ ] * 0.96 [ ] 1.20 [ ] Hearing Loss 1.21 [ ] 1.47 [ ] 2.07 [ ] 0.99 [ ] 1.04 [ ] Vision Loss 2.27 [ ] * 1.23 [ ] 2.35 [ ] 3.50 [ ] ** 0.36 [ ] Dementia 3.38 [ ] *** 4.33 [ ] * 3.91 [ ] ** 2.88 [ ] *** 4.25 [ ] *** Alcohol Abuse 4.43 [ ] *** 5.16 [ ] *** 3.68 [ ] *** 4.81 [ ] *** 3.09 [ ] *** Depression and/or 1.65 [ ] *** 1.98 [ ] ** 1.53 [ ] 1.71 [ ] *** 1.23 [ ] Anxiety Immobility 4.05 [ ] *** [ ] ** 1.25 [ ] CHF 2.06 [ ] *** 4.43 [ ] *** 1.32 [ ] 1.79 [ ] *** 2.80 [ ] *** CPD 1.50 [ ] *** 1.96 [ ] *** 1.50 [ ] * 1.52 [ ] *** 1.17 [ ] CVD 2.57 [ ] *** 2.96 [ ] *** 2.63 [ ] *** 2.59 [ ] *** 2.50 [ ] *** Diabetes 1.18 [ ] ** 1.36 [ ] * 1.12 [ ] 1.14 [ ] 1.13 [ ] Liver Dysfunction 1.15 [ ] 2.27 [ ] 1.39 [ ] 0.87 [ ] 2.33 [ ] Renal Insufficiency 1.40 [ ] *** 1.87 [ ] ** 1.28 [ ] 1.53 [ ] *** 1.15 [ ] Metastases 1.17 [ ] * 1.55 [ ] 1.11 [ ] 1.24 [ ] * 1.06 [ ] PVD 1.12 [ ] 1.65 [ ] 1.37 [ ] 0.99 [ ] 1.14 [ ] Open Surgery 1.33 [ ] *** 1.41 [ ] * 1.21 [ ] 1.40 [ ] *** 1.07 [ ] $ Also adjusted for type of surgery Removed due to the absence of cases * p <0.05 ** p <0.01 *** p <0.001 RP = Radical Prostatectomy; PN = Partial Nephrectomy; RN = Radical Nephrectomy; RC = Radical cystectomy; CHF = Congestive Heart Failure; CPD = Chronic Pulmonary Disease; CVD: Cerebrovascular Disease; PVD = Peripheral Vascular Disease 33
34 Table 6 Preoperative Risk Score Model for Delirium Preoperative Risk Prediction Score 1 point 2 points 4 points White race Depression and/or Anxiety Vision Loss Male gender Chronic Pulmonary Disease Cerebrovascular disease Unmarried Renal Insufficiency 5 points Open surgery 3 points Age 80 years Sleep Disorder Age years Dementia Diabetes Congestive Heart Failure 6 Points Metastases Alcohol Abuse Immobility 34
35 Table 7 Distribution of Delirium Risk Prediction Scores by Surgery Surgery Overall No delirium Delirium P-value All Genitourinary Surgery 4 (2.4) 3.9 (2.3) 6.7 (3.7) <0.001 Radical Prostatectomy 3.4 (1.7) 3.4 (1.7) 4.5 (2.6) <0.001 Partial Nephrectomy 4.1 (2.7) 4 (2.6) 6.1 (3.8) <0.001 Radical Nephrectomy 4.7 (2.9) 4.6 (2.8) 7.1 (3.6) <0.001 Radical Cystectomy 6.4 (3.1) 6.2 (3) 8.3 (3.4) <0.001 Scores displayed as Mean (SD) Table 8 ICD-9 codes for Urologic Cancer Surgeries Surgery Type ICD-9 Procedure ICD-9 Diagnosis Prostate Cancer 60.5, Kidney Cancer/Renal Mass 55.4 $ 223.0, 223.1, 189.0, 189.1, 189.2, 189.8, Kidney Cancer/Renal Mass 55.51, 55.52, , 198.0, 198.1, , 593.2, 593.9, , , , V10.52, V16.51 Bladder Cancer 57.71, , 188.1, 188.2, 188.3, 188.4, 188.5, 188.6, 188.7, 188.8, 188.9, $Denotes partial nephrectomy 35
36 Table 9 ICD-9 Codes for Delirium and Major Risk Factors Variable Brief Description ICD-9 Codes Outcome Delirium Delirium and/or acute changes in cognition , , 290.2, 290.3, , , 290.8, 290.9, , , , , , , , 292.9, 293.0, 293.1, , , , , , 293.9, 294.9, 298.1, 298.2, 298.8, 298.9, , , 308.0, 308.1, 308.2, 308.3, 308.4, 308.9, 310.1, 310.9, , 348.3, , , , 437.2, 572.2, 768.7, , , , , , , Preoperative Risk Factors Alcohol Abuse Sleep Disturbance Hearing Loss Vision Loss Dementia Depression Anxiety Immobility Alcohol abuse and alcohol-related medical complications Sleep-related medical problems such as sleep apnea, insomnia, and circadian rhythm disorders Hearing difficulties and/or loss Vision impairment in one or both eyes Dementia Depression and/or anxiety Preoperative immobility 291.0, 291.1, 291.2, 291.3, 291.4, 291.5, , , , 291.9, 303.0, , , , 303.9, , , , 305.0, , , , 357.5, 425.5, 535.3, , 571.0, 571.1, 571.2, 571.3, 790.3, 977.3, , 307.4, , , , , , , , , , , , , , , , 327.2, , , , , , , , 327.3, , , , , , , , , 327.4, , , , , , , , , , 327.8, 780.5, , , , , , , , , , 387.0, 387.1, 387.2, 387.8, 387.9, 388.0, , , 388.1, , , 388.2, 388.3, , , 388.4, , , , , 388.5, 389.0, , , , , , , , 389.1, , , , , , , , , 389.2, , , 389.7, 389.8, 389.9, 744.0, , , , , , , 367.1, 368.3, , , , , , , , , , , , , , , , , , , , , , , 369.3, 369.4, 369.6, , , , , , , , , , 369.7, , , , , , , 369.8, , 290.1, , , 290.4, , 291.2, , 294.2, , 331.0, , , 331.2, , , , 331.9, , , , , , , , 296.3, , , , , , , 300.0, , , , 309.1, , 93.51, 93.52, 93.53, 93.54, 93.55, 93.56, 93.57, 93.58,
37 Figure 1 Adjusted hospital admission costs by delirium status and type of surgery in the United States from 2003 to Direct hospital admission costs were adjusted for delirium status, patient characteristics (age, race, gender, marital status, obesity, Charlson Comorbidity Index, insurance status), hospital characteristics (size, teaching status, region, urban vs. rural), and perioperative characteristics (type of surgery, open vs. minimally invasive, OR time, number of packed RBC use greater than 4 units, ICU admission, soft tissue infection, sepsis, urinary tract infection, other postoperative infections, pneumonia, aspiration, ileus, peritonitis, perforation, GI hemorrhage, acute renal failure, DVT, arrhythmias, myocardial infarction, cardiac arrest, respiratory failure, and cerebrovascular incident). Hospital admission costs were sub-divided by categories that include supplies, room and board, radiology, pharmacy, operating room, lab, and other hospital costs. All costs were inflated to 2013 US dollars. * Significance difference in total costs (p<0.001). 37
38 38
39 Figure 2 Predicted Probability and Receiver Operating Characteristic (ROC) Curve Analysis by the Preoperative Delirium Risk Score. A illustrates predicted probability curve of the preoperative risk prediction model. The blue shading represents the training cohort, while the red shading represents the validation cohort. B illustrates the Area Under the Curve (AUC) Analysis of the risk prediction model of the training (blue) and validation (red) cohorts. Additional sub-group analysis of the predicted probability curve and the AUC analysis are shown. 39
40 40
41 Figure 3 Percent of patients of postoperative delirium by delirium risk prediction in the training cohort. Part A illustrates the percent of patients at risk of postoperative delirium in low, intermediate, high, and very high risk categories as classified by the delirium risk prediction score. Part B illustrates the percent of patients with postoperative delirium in each, respective risk category. 41
42 42
SUPPLEMENTARY DATA. Supplementary Figure S1. Cohort definition flow chart.
 Supplementary Figure S1. Cohort definition flow chart. Supplementary Table S1. Baseline characteristics of study population grouped according to having developed incident CKD during the follow-up or not
Supplementary Figure S1. Cohort definition flow chart. Supplementary Table S1. Baseline characteristics of study population grouped according to having developed incident CKD during the follow-up or not
Supplementary Online Content
 Supplementary Online Content Gershengorn HB, Scales DC, Kramer A, Wunsch H. Association between overnight extubations and outcomes in the intensive care unit. JAMA Intern Med. Published online September
Supplementary Online Content Gershengorn HB, Scales DC, Kramer A, Wunsch H. Association between overnight extubations and outcomes in the intensive care unit. JAMA Intern Med. Published online September
Category Code Procedure description
 Supplemental Table 1: ICD-9 codes for procedures/surgeries Category Code Procedure description Cesarean 74 Cesarean Section And Removal Of Fetus Cesarean 74.0 Classical cesarean section Cesarean 74.1 Low
Supplemental Table 1: ICD-9 codes for procedures/surgeries Category Code Procedure description Cesarean 74 Cesarean Section And Removal Of Fetus Cesarean 74.0 Classical cesarean section Cesarean 74.1 Low
The Pennsylvania State University. The Graduate School. Department of Public Health Sciences
 The Pennsylvania State University The Graduate School Department of Public Health Sciences THE LENGTH OF STAY AND READMISSIONS IN MASTECTOMY PATIENTS A Thesis in Public Health Sciences by Susie Sun 2015
The Pennsylvania State University The Graduate School Department of Public Health Sciences THE LENGTH OF STAY AND READMISSIONS IN MASTECTOMY PATIENTS A Thesis in Public Health Sciences by Susie Sun 2015
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative
 Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Exploring the Relationship Between Substance Abuse and Dependence Disorders and Discharge Status: Results and Implications
 MWSUG 2017 - Paper DG02 Exploring the Relationship Between Substance Abuse and Dependence Disorders and Discharge Status: Results and Implications ABSTRACT Deanna Naomi Schreiber-Gregory, Henry M Jackson
MWSUG 2017 - Paper DG02 Exploring the Relationship Between Substance Abuse and Dependence Disorders and Discharge Status: Results and Implications ABSTRACT Deanna Naomi Schreiber-Gregory, Henry M Jackson
GSK Medicine: Study Number: Title: Rationale: Study Period: Objectives: Indication: Study Investigators/Centers: Research Methods: Data Source
 The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
Using claims data to investigate RT use at the end of life. B. Ashleigh Guadagnolo, MD, MPH Associate Professor M.D. Anderson Cancer Center
 Using claims data to investigate RT use at the end of life B. Ashleigh Guadagnolo, MD, MPH Associate Professor M.D. Anderson Cancer Center Background 25% of Medicare budget spent on the last year of life.
Using claims data to investigate RT use at the end of life B. Ashleigh Guadagnolo, MD, MPH Associate Professor M.D. Anderson Cancer Center Background 25% of Medicare budget spent on the last year of life.
TOTAL HIP AND KNEE REPLACEMENTS. FISCAL YEAR 2002 DATA July 1, 2001 through June 30, 2002 TECHNICAL NOTES
 TOTAL HIP AND KNEE REPLACEMENTS FISCAL YEAR 2002 DATA July 1, 2001 through June 30, 2002 TECHNICAL NOTES The Pennsylvania Health Care Cost Containment Council April 2005 Preface This document serves as
TOTAL HIP AND KNEE REPLACEMENTS FISCAL YEAR 2002 DATA July 1, 2001 through June 30, 2002 TECHNICAL NOTES The Pennsylvania Health Care Cost Containment Council April 2005 Preface This document serves as
5 older patients become delirious every minute
 Management of Delirium: Nonpharmacologic and Pharmacologic Approaches Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley
Management of Delirium: Nonpharmacologic and Pharmacologic Approaches Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley
Accelero Identifies Opportunities to Provide Greater Value in Hip Fracture Care
 Accelero Health Partners, 2015 WHITE PAPER Accelero Identifies Opportunities to Provide Greater Value in Hip Fracture Care Jason Pry, Senior Director ABSTRACT Every year more than a quarter of a million
Accelero Health Partners, 2015 WHITE PAPER Accelero Identifies Opportunities to Provide Greater Value in Hip Fracture Care Jason Pry, Senior Director ABSTRACT Every year more than a quarter of a million
Delirium in the Elderly
 Delirium in the Elderly ELITE 2017 Liza Genao, MD Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity Very much under-recognized
Delirium in the Elderly ELITE 2017 Liza Genao, MD Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity Very much under-recognized
Recognition of Complications After Pancreaticoduodenectomy for Cancer Determines Inpatient Mortality
 ORIGINAL ARTICLE Recognition of Complications After Pancreaticoduodenectomy for Cancer Determines Inpatient Mortality Evan S Glazer 1, Albert Amini 1, Tun Jie 1, Rainer WG Gruessner 1, Robert S Krouse
ORIGINAL ARTICLE Recognition of Complications After Pancreaticoduodenectomy for Cancer Determines Inpatient Mortality Evan S Glazer 1, Albert Amini 1, Tun Jie 1, Rainer WG Gruessner 1, Robert S Krouse
Iftekhar Kalsekar 1*, Chia-Wen Hsiao 2, Hang Cheng 2, Sashi Yadalam 1, Brian Po-Han Chen 2, Laura Goldstein 2 and Andrew Yoo 1
 Kalsekar et al. Health Economics Review (2017) 7:22 DOI 10.1186/s13561-017-0160-8 RESEARCH Economic burden of cancer among patients with surgical resections of the lung, rectum, liver and uterus: results
Kalsekar et al. Health Economics Review (2017) 7:22 DOI 10.1186/s13561-017-0160-8 RESEARCH Economic burden of cancer among patients with surgical resections of the lung, rectum, liver and uterus: results
5 older patients become. What is delirium? (Acute confusional state) Where We ve Been and
 Where We ve Been and") Update on Delirium: Where We ve Been and Where We re Going Sharon K. Inouye, M.D., M.P.H. M PH Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley F. Levy
Update on Delirium: Where We ve Been and Where We re Going Sharon K. Inouye, M.D., M.P.H. M PH Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley F. Levy
In each hospital-year, we calculated a 30-day unplanned. readmission rate among patients who survived at least 30 days
 Romley JA, Goldman DP, Sood N. US hospitals experienced substantial productivity growth during 2002 11. Health Aff (Millwood). 2015;34(3). Published online February 11, 2015. Appendix Adjusting hospital
Romley JA, Goldman DP, Sood N. US hospitals experienced substantial productivity growth during 2002 11. Health Aff (Millwood). 2015;34(3). Published online February 11, 2015. Appendix Adjusting hospital
Predicting Short Term Morbidity following Revision Hip and Knee Arthroplasty
 Predicting Short Term Morbidity following Revision Hip and Knee Arthroplasty A Review of ACS-NSQIP 2006-2012 Arjun Sebastian, M.D., Stephanie Polites, M.D., Kristine Thomsen, B.S., Elizabeth Habermann,
Predicting Short Term Morbidity following Revision Hip and Knee Arthroplasty A Review of ACS-NSQIP 2006-2012 Arjun Sebastian, M.D., Stephanie Polites, M.D., Kristine Thomsen, B.S., Elizabeth Habermann,
Appendix Identification of Study Cohorts
 Appendix Identification of Study Cohorts Because the models were run with the 2010 SAS Packs from Centers for Medicare and Medicaid Services (CMS)/Yale, the eligibility criteria described in "2010 Measures
Appendix Identification of Study Cohorts Because the models were run with the 2010 SAS Packs from Centers for Medicare and Medicaid Services (CMS)/Yale, the eligibility criteria described in "2010 Measures
Delirium in the Elderly
 Delirium in the Elderly ELITE 2015 Mamata Yanamadala M.B.B.S, MS Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity
Delirium in the Elderly ELITE 2015 Mamata Yanamadala M.B.B.S, MS Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity
The Relationship Between Surgical Volume and Patient Outcomes in Urologic Malignancies
 The Relationship Between Surgical Volume and Patient Outcomes in Urologic Malignancies Geoffrey Gotto PGY-5 UBC Department of Urologic Sciences October 8 th, 2008 Objective To review the literature on
The Relationship Between Surgical Volume and Patient Outcomes in Urologic Malignancies Geoffrey Gotto PGY-5 UBC Department of Urologic Sciences October 8 th, 2008 Objective To review the literature on
MAKING THE NSQIP PARTICIPANT USE DATA FILE (PUF) WORK FOR YOU
 WORK FOR YOU") MAKING THE NSQIP PARTICIPANT USE DATA FILE (PUF) WORK FOR YOU Hani Tamim, PhD Clinical Research Institute Department of Internal Medicine American University of Beirut Medical Center Beirut - Lebanon Participant
MAKING THE NSQIP PARTICIPANT USE DATA FILE (PUF) WORK FOR YOU Hani Tamim, PhD Clinical Research Institute Department of Internal Medicine American University of Beirut Medical Center Beirut - Lebanon Participant
Accelero Identifies Opportunities to Provide Greater Value in Hip Fracture Care
 Accelero Identifies Opportunities to Provide Greater Value in Hip Fracture Care Every year more than a quarter of a million people over the age of 65 are admitted to a hospital with a hip fracture. Mortality
Accelero Identifies Opportunities to Provide Greater Value in Hip Fracture Care Every year more than a quarter of a million people over the age of 65 are admitted to a hospital with a hip fracture. Mortality
ACS-NSQIP 2015 Julietta Chang MD, Ali Aminian MD, Stacy A Brethauer MD, Philip R Schauer MD Bariatric and Metabolic Institute
 ACS-NSQIP 2015 Julietta Chang MD, Ali Aminian MD, Stacy A Brethauer MD, Philip R Schauer MD Bariatric and Metabolic Institute Disclosures Authors: No disclosures ACS-NSQIP Disclaimer: The American College
ACS-NSQIP 2015 Julietta Chang MD, Ali Aminian MD, Stacy A Brethauer MD, Philip R Schauer MD Bariatric and Metabolic Institute Disclosures Authors: No disclosures ACS-NSQIP Disclaimer: The American College
Risk of Fractures Following Cataract Surgery in Medicare Beneficiaries
 Risk of Fractures Following Cataract Surgery in Medicare Beneficiaries Victoria L. Tseng, MD, Fei Yu, PhD, Flora Lum, MD, Anne L. Coleman, MD, PhD JAMA. 2012;308(5):493-501 Background Visual impairment
Risk of Fractures Following Cataract Surgery in Medicare Beneficiaries Victoria L. Tseng, MD, Fei Yu, PhD, Flora Lum, MD, Anne L. Coleman, MD, PhD JAMA. 2012;308(5):493-501 Background Visual impairment
JAMA, January 11, 2012 Vol 307, No. 2
 JAMA, January 11, 2012 Vol 307, No. 2 Dementia is associated with increased rates and often poorer outcomes of hospitalization Worsening cognitive status Adequate chronic disease management is more difficult
JAMA, January 11, 2012 Vol 307, No. 2 Dementia is associated with increased rates and often poorer outcomes of hospitalization Worsening cognitive status Adequate chronic disease management is more difficult
Delirium. Dr. John Puxty
 Delirium Dr. John Puxty Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors, causes and main
Delirium Dr. John Puxty Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors, causes and main
Supplementary Online Content
 Supplementary Online Content Valley TS, Sjoding MW, Ryan AM, Iwashyna TJ, Cooke CR. Association of intensive care unit admission with mortality among older patients with pneumonia. JAMA. doi:10.1001/jama.2015.11068.
Supplementary Online Content Valley TS, Sjoding MW, Ryan AM, Iwashyna TJ, Cooke CR. Association of intensive care unit admission with mortality among older patients with pneumonia. JAMA. doi:10.1001/jama.2015.11068.
Supplementary Online Content
 Supplementary Online Content Pincus D, Ravi B, Wasserstein D. Association between wait time and 30-day mortality in adults undergoing hip fracture surgery. JAMA. doi: 10.1001/jama.2017.17606 eappendix
Supplementary Online Content Pincus D, Ravi B, Wasserstein D. Association between wait time and 30-day mortality in adults undergoing hip fracture surgery. JAMA. doi: 10.1001/jama.2017.17606 eappendix
Appendix 1: Supplementary tables [posted as supplied by author]
![Appendix 1: Supplementary tables [posted as supplied by author]](/thumbs/81/83505567.jpg "Appendix 1: Supplementary tables [posted as supplied by author]") Appendix 1: Supplementary tables [posted as supplied by author] Table A. International Classification of Diseases, Ninth Revision, Clinical Modification Codes Used to Define Heart Failure, Acute Myocardial
Appendix 1: Supplementary tables [posted as supplied by author] Table A. International Classification of Diseases, Ninth Revision, Clinical Modification Codes Used to Define Heart Failure, Acute Myocardial
Update - Delirium in Elders
 Update - Delirium in Elders Impact Recognition Prevention, and Management Michael J. Lichtenstein, MD F. Carter Pannill, Jr. Professor of Medicine Chief, Division of Geriatrics, Gerontology and Palliative
Update - Delirium in Elders Impact Recognition Prevention, and Management Michael J. Lichtenstein, MD F. Carter Pannill, Jr. Professor of Medicine Chief, Division of Geriatrics, Gerontology and Palliative
TITLE: Patterns of Care, Utilization, and Outcomes of Treatments For Localized Prostate Cancer
 AWARD NUMBER: W81XWH-08-1-0283 TITLE: Patterns of Care, Utilization, and Outcomes of Treatments For Localized Prostate Cancer PRINCIPAL INVESTIGATOR: Jim C. Hu, M D CONTRACTING ORGANIZATION: Brigham and
AWARD NUMBER: W81XWH-08-1-0283 TITLE: Patterns of Care, Utilization, and Outcomes of Treatments For Localized Prostate Cancer PRINCIPAL INVESTIGATOR: Jim C. Hu, M D CONTRACTING ORGANIZATION: Brigham and
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Bucholz EM, Butala NM, Ma S, Normand S-LT, Krumholz HM. Life
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Bucholz EM, Butala NM, Ma S, Normand S-LT, Krumholz HM. Life
Jacqueline C. Barrientos, Nicole Meyer, Xue Song, Kanti R. Rai ASH Annual Meeting Abstracts 2015:3301
 Characterization of atrial fibrillation and bleeding risk factors in patients with CLL: A population-based retrospective cohort study of administrative medical claims data in the U.S. Jacqueline C. Barrientos,
Characterization of atrial fibrillation and bleeding risk factors in patients with CLL: A population-based retrospective cohort study of administrative medical claims data in the U.S. Jacqueline C. Barrientos,
Pregnancy complications in women with rare tumor suppressor syndromes affecting central and peripheral nervous system
 Pregnancy complications in women with rare tumor suppressor syndromes affecting central and peripheral nervous system The Harvard community has made this article openly available. Please share how this
Pregnancy complications in women with rare tumor suppressor syndromes affecting central and peripheral nervous system The Harvard community has made this article openly available. Please share how this
Appendix 1. Frailty as a confounder of the effectiveness of preventive treatment. Abbreviations: t1 = time one. t2 = time 2. This model indicates the
 Appendix 1. Frailty as a confounder of the effectiveness of preventive treatment. Abbreviations: t1 = time one. t2 = time 2. This model indicates the interrelatedness of comorbidity, frailty, and ADL dependency,
Appendix 1. Frailty as a confounder of the effectiveness of preventive treatment. Abbreviations: t1 = time one. t2 = time 2. This model indicates the interrelatedness of comorbidity, frailty, and ADL dependency,
BIOSTATISTICAL METHODS
 BIOSTATISTICAL METHODS FOR TRANSLATIONAL & CLINICAL RESEARCH PROPENSITY SCORE Confounding Definition: A situation in which the effect or association between an exposure (a predictor or risk factor) and
BIOSTATISTICAL METHODS FOR TRANSLATIONAL & CLINICAL RESEARCH PROPENSITY SCORE Confounding Definition: A situation in which the effect or association between an exposure (a predictor or risk factor) and
Technical appendix: The impact of integrated care teams on hospital use in North East Hampshire and Farnham
 Improvement Analytics Unit September 2018 Technical appendix: The impact of integrated care teams on hospital use in North East Hampshire and Farnham Therese Lloyd, Richard Brine, Rachel Pearson, Martin
Improvement Analytics Unit September 2018 Technical appendix: The impact of integrated care teams on hospital use in North East Hampshire and Farnham Therese Lloyd, Richard Brine, Rachel Pearson, Martin
Supplementary Digital Content Section A Procedural codes to define study population
 Supplementary Digital Content Section A Procedural codes to define study population Procedure CCI codes ORTHOPEDIC Total hip replacement 1.VA.53.LA-PN ; 1.VA.53.PN-PN Total knee replacement 1.VG.53 VASCULAR
Supplementary Digital Content Section A Procedural codes to define study population Procedure CCI codes ORTHOPEDIC Total hip replacement 1.VA.53.LA-PN ; 1.VA.53.PN-PN Total knee replacement 1.VG.53 VASCULAR
Delirium. A Plan to Reduce Use of Restraints. David Wensel DO, FAAHPM Medical Director Midland Care
 Delirium A Plan to Reduce Use of Restraints David Wensel DO, FAAHPM Medical Director Midland Care Objectives Define delirium Describe pathophysiology of delirium Understand most common etiologies Define
Delirium A Plan to Reduce Use of Restraints David Wensel DO, FAAHPM Medical Director Midland Care Objectives Define delirium Describe pathophysiology of delirium Understand most common etiologies Define
Best Papers. F. Fusco
 Best Papers UROLOGY F. Fusco Best papers - 2015 RP/RT Oncological outcomes RP/RT IN ct3 Utilization trends RP/RT Complications Evolving role of elnd /Salvage LND This cohort reflects the current clinical
Best Papers UROLOGY F. Fusco Best papers - 2015 RP/RT Oncological outcomes RP/RT IN ct3 Utilization trends RP/RT Complications Evolving role of elnd /Salvage LND This cohort reflects the current clinical
Geriatric Hip Fracture Co-Management. Pannida Wattanapanom, M.D., FACP.
 Geriatric Hip Fracture Co-Management Pannida Wattanapanom, M.D., FACP. An 80 year old man with a hip fracture The General Medicine approach: Medical clearance for surgery Role of Geriatrician Assess caused
Geriatric Hip Fracture Co-Management Pannida Wattanapanom, M.D., FACP. An 80 year old man with a hip fracture The General Medicine approach: Medical clearance for surgery Role of Geriatrician Assess caused
Supplementary Online Content
 Supplementary Online Content Lee JS, Nsa W, Hausmann LRM, et al. Quality of care for elderly patients hospitalized for pneumonia in the United States, 2006 to 2010. JAMA Intern Med. Published online September
Supplementary Online Content Lee JS, Nsa W, Hausmann LRM, et al. Quality of care for elderly patients hospitalized for pneumonia in the United States, 2006 to 2010. JAMA Intern Med. Published online September
Research Article Blood Transfusions in Total Hip and Knee Arthroplasty: An Analysis of Outcomes
 e Scientific World Journal, Article ID 623460, 10 pages http://dx.doi.org/10.1155/2014/623460 Research Article Blood Transfusions in Total Hip and Knee Arthroplasty: An Analysis of Outcomes Thomas Danninger,
e Scientific World Journal, Article ID 623460, 10 pages http://dx.doi.org/10.1155/2014/623460 Research Article Blood Transfusions in Total Hip and Knee Arthroplasty: An Analysis of Outcomes Thomas Danninger,
Care of older people in surgery (COPS)
") Care of older people in surgery (COPS) Who, what, and does it make a difference Professor Jacqueline Close Geriatrician - POWH Clinical Director Falls, Balance and Injury Research Centre Early Mobilisation
Care of older people in surgery (COPS) Who, what, and does it make a difference Professor Jacqueline Close Geriatrician - POWH Clinical Director Falls, Balance and Injury Research Centre Early Mobilisation
Improved IPGM: Demonstrating the Value to both Patients and Hospitals
 Improved IPGM: Demonstrating the Value to both Patients and Hospitals Osama Hamdy, MD, PhD, FACE Medical Director, Inpatient Diabetes Program Joslin Diabetes Center Harvard Medical School, Boston, MA Cost
Improved IPGM: Demonstrating the Value to both Patients and Hospitals Osama Hamdy, MD, PhD, FACE Medical Director, Inpatient Diabetes Program Joslin Diabetes Center Harvard Medical School, Boston, MA Cost
Hu J, Gonsahn MD, Nerenz DR. Socioeconomic status and readmissions: evidence from an urban teaching hospital. Health Aff (Millwood). 2014;33(5).
. 2014;33(5).") Appendix Definitions of Index Admission and Readmission Definitions of index admission and readmission follow CMS hospital-wide all-cause unplanned readmission (HWR) measure as far as data are available.
Appendix Definitions of Index Admission and Readmission Definitions of index admission and readmission follow CMS hospital-wide all-cause unplanned readmission (HWR) measure as far as data are available.
Supplementary Online Content
 Supplementary Online Content Inohara T, Xian Y, Liang L, et al. Association of intracerebral hemorrhage among patients taking non vitamin K antagonist vs vitamin K antagonist oral anticoagulants with in-hospital
Supplementary Online Content Inohara T, Xian Y, Liang L, et al. Association of intracerebral hemorrhage among patients taking non vitamin K antagonist vs vitamin K antagonist oral anticoagulants with in-hospital
As the proportion of the elderly in the
 CANCER When the cancer patient is elderly, how do you weigh the risks of surgery? Marguerite Palisoul, MD Dr. Palisoul is Fellow in the Department of Obstetrics and Gynecology, Division of Gynecologic
CANCER When the cancer patient is elderly, how do you weigh the risks of surgery? Marguerite Palisoul, MD Dr. Palisoul is Fellow in the Department of Obstetrics and Gynecology, Division of Gynecologic
A DISSERTATION SUBMITTED TO THE FACULTY OF THE GRADUATE SCHOOL OF THE UNIVERSITY OF MINNESOTA BY. Helen Mari Parsons
 A Culture of Quality? Lymph Node Evaluation for Colon Cancer Care A DISSERTATION SUBMITTED TO THE FACULTY OF THE GRADUATE SCHOOL OF THE UNIVERSITY OF MINNESOTA BY Helen Mari Parsons IN PARTIAL FULFILLMENT
A Culture of Quality? Lymph Node Evaluation for Colon Cancer Care A DISSERTATION SUBMITTED TO THE FACULTY OF THE GRADUATE SCHOOL OF THE UNIVERSITY OF MINNESOTA BY Helen Mari Parsons IN PARTIAL FULFILLMENT
State of the State: Hospital Performance in Pennsylvania September 2012
 State of the State: Hospital Performance in Pennsylvania September 2012 Measuring Progress in PA Hospital Performance: Process Measures 1 PA Hospital Performance: Process Measures We examined the latest
State of the State: Hospital Performance in Pennsylvania September 2012 Measuring Progress in PA Hospital Performance: Process Measures 1 PA Hospital Performance: Process Measures We examined the latest
Ankle fractures are one of
 Elevated Risks of Ankle Fracture Surgery in Patients With Diabetes Nelson F. SooHoo, MD, Lucie Krenek, MD, Michael Eagan, MD, and David S. Zingmond, MD, PhD Ankle fractures are one of the most common types
Elevated Risks of Ankle Fracture Surgery in Patients With Diabetes Nelson F. SooHoo, MD, Lucie Krenek, MD, Michael Eagan, MD, and David S. Zingmond, MD, PhD Ankle fractures are one of the most common types
CRAIOVA UNIVERSITY OF MEDICINE AND PHARMACY FACULTY OF MEDICINE ABSTRACT DOCTORAL THESIS
 CRAIOVA UNIVERSITY OF MEDICINE AND PHARMACY FACULTY OF MEDICINE ABSTRACT DOCTORAL THESIS RISK FACTORS IN THE EMERGENCE OF POSTOPERATIVE RENAL FAILURE, IMPACT OF TREATMENT WITH ACE INHIBITORS Scientific
CRAIOVA UNIVERSITY OF MEDICINE AND PHARMACY FACULTY OF MEDICINE ABSTRACT DOCTORAL THESIS RISK FACTORS IN THE EMERGENCE OF POSTOPERATIVE RENAL FAILURE, IMPACT OF TREATMENT WITH ACE INHIBITORS Scientific
The Harvard community has made this article openly available. Please share how this access benefits you. Your story matters
 Non#ST#Elevation Myocardial Infarction in the United States: Contemporary Trends in Incidence, Utilization of the Early Invasive Strategy, and In#Hospital Outcomes The Harvard community has made this article
Non#ST#Elevation Myocardial Infarction in the United States: Contemporary Trends in Incidence, Utilization of the Early Invasive Strategy, and In#Hospital Outcomes The Harvard community has made this article
Technical Appendix for Outcome Measures
 Study Overview Technical Appendix for Outcome Measures This is a report on data used, and analyses done, by MPA Healthcare Solutions (MPA, formerly Michael Pine and Associates) for Consumers CHECKBOOK/Center
Study Overview Technical Appendix for Outcome Measures This is a report on data used, and analyses done, by MPA Healthcare Solutions (MPA, formerly Michael Pine and Associates) for Consumers CHECKBOOK/Center
Methods to Control for Bias in Observational Studies. Anne P. Ehlers. A thesis submitted in partial fulfillment of the requirements for the degree of
 Methods to Control for Bias in Observational Studies Anne P. Ehlers A thesis submitted in partial fulfillment of the requirements for the degree of Master of Public Health University of Washington 2016
Methods to Control for Bias in Observational Studies Anne P. Ehlers A thesis submitted in partial fulfillment of the requirements for the degree of Master of Public Health University of Washington 2016
Table 2. Distribution of Normalized Inverse Probability of Treatment Weights. Healthcare costs (US $2012) Notes:
 Notes:") 228 COMPARISON OF HEALTHCARE RESOURCE UTILIZATION AND MEDICAID SPENDING AMONG PATIENTS WITH SCHIZOPHRENIA TREATED WITH ONCE MONTHLY PALIPERIDONE PALMITATE OR ORAL ATYPICAL ANTIPSYCHOTICS USING THE INVERSE
228 COMPARISON OF HEALTHCARE RESOURCE UTILIZATION AND MEDICAID SPENDING AMONG PATIENTS WITH SCHIZOPHRENIA TREATED WITH ONCE MONTHLY PALIPERIDONE PALMITATE OR ORAL ATYPICAL ANTIPSYCHOTICS USING THE INVERSE
Tennessee Department of Health in collaboration with Tennessee State University and University of Tennessee Health Science Center
 Tennessee Department of Health in collaboration with Tennessee State University and University of Tennessee Health Science Center 2006 Tennessee Department of Health 2006 ACKNOWLEDGEMENTS CONTRIBUTING
Tennessee Department of Health in collaboration with Tennessee State University and University of Tennessee Health Science Center 2006 Tennessee Department of Health 2006 ACKNOWLEDGEMENTS CONTRIBUTING
Surgical Management of Metastatic and Locally Recurrent Kidney Cancer: Does it Make Sense?
 Surgical Management of Metastatic and Locally Recurrent Kidney Cancer: Does it Make Sense? Philippe E. Spiess, MD, FACS Associate Member Department of GU Oncology Department of Tumor Biology Moffitt Cancer
Surgical Management of Metastatic and Locally Recurrent Kidney Cancer: Does it Make Sense? Philippe E. Spiess, MD, FACS Associate Member Department of GU Oncology Department of Tumor Biology Moffitt Cancer
Saman Arbabi M.D., M.P.H., F.A.C.S. Kathleen O'Connell M.D. Bryce Robinson M.D., M.S., F.A.C.S., F.C.C.M
 Form "EAST Multicenter Study Proposal" Study Title Primary investigator / Senior researcher Email of Primary investigator / Senior researcher Co-primary investigator Are you a current member of EAST? If
Form "EAST Multicenter Study Proposal" Study Title Primary investigator / Senior researcher Email of Primary investigator / Senior researcher Co-primary investigator Are you a current member of EAST? If
Improving Healthcare Utilization in Injured Older Adults
 Improving Healthcare Utilization in Injured Older Adults G ERIATRIC T R A U MA I N I T I AT I V E S AT S TA N F O R D H E A LT H C A R E J U LY 12, 2018 Objectives Background on Geriatric Trauma Population
Improving Healthcare Utilization in Injured Older Adults G ERIATRIC T R A U MA I N I T I AT I V E S AT S TA N F O R D H E A LT H C A R E J U LY 12, 2018 Objectives Background on Geriatric Trauma Population
Delirium in Older Persons: An Investigative Journey
 Delirium in Older Persons: An Investigative Journey Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley F. Levy Family Chair
Delirium in Older Persons: An Investigative Journey Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley F. Levy Family Chair
Since 1980, obesity has more than doubled worldwide, and in 2008 over 1.5 billion adults aged 20 years were overweight.
 Impact of metabolic comorbidity on the association between body mass index and health-related quality of life: a Scotland-wide cross-sectional study of 5,608 participants Dr. Zia Ul Haq Doctoral Research
Impact of metabolic comorbidity on the association between body mass index and health-related quality of life: a Scotland-wide cross-sectional study of 5,608 participants Dr. Zia Ul Haq Doctoral Research
UNTHSC TCOM Geriatric Competencies Curriculum Mapping Document
 INSTRUCTIONS: Place a "B" (Basic), "I" (Intermediate), or "A" (Advanced) in the box next to the Geriatric Competency to indicate the Geraitaric Competency being taught, the corresponding Method of Subject
INSTRUCTIONS: Place a "B" (Basic), "I" (Intermediate), or "A" (Advanced) in the box next to the Geriatric Competency to indicate the Geraitaric Competency being taught, the corresponding Method of Subject
Complications in robotic surgery!! Review of the literature! RALP, RAPN and RARC!
 Complications in robotic surgery Review of the literature RALP, RAPN and RARC Anna Wallerstedt, MD Karolinska University Hospital Stockholm, Sweden Agenda The importance of reporting surgical complications
Complications in robotic surgery Review of the literature RALP, RAPN and RARC Anna Wallerstedt, MD Karolinska University Hospital Stockholm, Sweden Agenda The importance of reporting surgical complications
Background Information
 Background Information Age plays an important role in patients selection for spinal surgeries as it is associated with increased morbidity and mortality Consequences of suffering postoperative complications
Background Information Age plays an important role in patients selection for spinal surgeries as it is associated with increased morbidity and mortality Consequences of suffering postoperative complications
Integrating Geriatrics into Oncology Care
 Integrating Geriatrics into Oncology Care William Dale, MD, PhD Chief, Geriatrics & Palliative Medicine Director, Specialized Oncology Care & Research in the Elderly (SOCARE) Clinic University of Chicago
Integrating Geriatrics into Oncology Care William Dale, MD, PhD Chief, Geriatrics & Palliative Medicine Director, Specialized Oncology Care & Research in the Elderly (SOCARE) Clinic University of Chicago
NQF-ENDORSED VOLUNTARY CONSENSUS STANDARDS FOR HOSPITAL CARE. Measure Information Form Collected For: CMS Outcome Measures (Claims Based)
") Last Updated: Version 4.3 NQF-ENDORSED VOLUNTARY CONSENSUS STANDARDS FOR HOSPITAL CARE Measure Information Form Collected For: CMS Outcome Measures (Claims Based) Measure Set: CMS Mortality Measures Set
Last Updated: Version 4.3 NQF-ENDORSED VOLUNTARY CONSENSUS STANDARDS FOR HOSPITAL CARE Measure Information Form Collected For: CMS Outcome Measures (Claims Based) Measure Set: CMS Mortality Measures Set
Preoperative tests (update)
") National Institute for Health and Care Excellence. Preoperative tests (update) Routine preoperative tests for elective surgery NICE guideline NG45 Appendix N: Research recommendations April 2016 Developed
National Institute for Health and Care Excellence. Preoperative tests (update) Routine preoperative tests for elective surgery NICE guideline NG45 Appendix N: Research recommendations April 2016 Developed
A17/B17: Delirium Can Be Deadly: Save Lives With a Standardized Approach to Delirium IHI 25th Annual National Forum, December 10, 2013
 A17/B17: Delirium Can Be Deadly: Save Lives With a Standardized Approach to Delirium IHI 25th Annual National Forum, December 10, 2013 Clay Angel, MD, Hospital Medicine; Chief of Continuum/SNF Kristen
A17/B17: Delirium Can Be Deadly: Save Lives With a Standardized Approach to Delirium IHI 25th Annual National Forum, December 10, 2013 Clay Angel, MD, Hospital Medicine; Chief of Continuum/SNF Kristen
Perioperative Care of Older Adults
 Perioperative Care of Older Adults SARAH A. WINGFIELD, MD AND THOMAS O. DALTON, MD UNIVERSITY OF TEXAS SOUTHWESTERN MEDICAL CENTER DIVISION OF GERIATRIC MEDICINE We have no disclosures. Objectives -Recognize
Perioperative Care of Older Adults SARAH A. WINGFIELD, MD AND THOMAS O. DALTON, MD UNIVERSITY OF TEXAS SOUTHWESTERN MEDICAL CENTER DIVISION OF GERIATRIC MEDICINE We have no disclosures. Objectives -Recognize
Perioperative Care of Older Adults
 Perioperative Care of Older Adults SARAH A. WINGFIELD, MD AND THOMAS O. DALTON, MD UNIVERSITY OF TEXAS SOUTHWESTERN MEDICAL CENTER DIVISION OF GERIATRIC MEDICINE We have no disclosures. Objectives -Recognize
Perioperative Care of Older Adults SARAH A. WINGFIELD, MD AND THOMAS O. DALTON, MD UNIVERSITY OF TEXAS SOUTHWESTERN MEDICAL CENTER DIVISION OF GERIATRIC MEDICINE We have no disclosures. Objectives -Recognize
Improving the quality of care of patients with delirium
 Improving the quality of care of patients with delirium Alasdair MacLullich MRCP(UK), PhD Professor of Geriatric Medicine University of Edinburgh Scotland How are we doing now? We are doing badly. Difficult
Improving the quality of care of patients with delirium Alasdair MacLullich MRCP(UK), PhD Professor of Geriatric Medicine University of Edinburgh Scotland How are we doing now? We are doing badly. Difficult
Recovery trajectories following critical illness: Can we really modify them? Tim Walsh Professor of Critical Care, Edinburgh University
 Recovery trajectories following critical illness: Can we really modify them? Tim Walsh Professor of Critical Care, Edinburgh University Considerations What is the problem? What is the current evidence
Recovery trajectories following critical illness: Can we really modify them? Tim Walsh Professor of Critical Care, Edinburgh University Considerations What is the problem? What is the current evidence
ROBOTIC VS OPEN RADICAL CYSTECTOMY
 ROBOTIC VS OPEN RADICAL CYSTECTOMY A REVIEW Colin Lundeen December 14, 2016 Objectives Review the history of radical cystectomy Critically analyze recent RCTs comparing open radical cystectomy (ORC) to
ROBOTIC VS OPEN RADICAL CYSTECTOMY A REVIEW Colin Lundeen December 14, 2016 Objectives Review the history of radical cystectomy Critically analyze recent RCTs comparing open radical cystectomy (ORC) to
Delirium in Hospital Care
 Delirium in Hospital Care Dr John Puxty 1 Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors,
Delirium in Hospital Care Dr John Puxty 1 Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors,
Impact of Screening Colonoscopy on Outcomes in Colon Cancer Surgery
 Impact of Screening Colonoscopy on Outcomes in Colon Cancer Surgery The Harvard community has made this article openly available. Please share how this access benefits you. Your story matters. Citation
Impact of Screening Colonoscopy on Outcomes in Colon Cancer Surgery The Harvard community has made this article openly available. Please share how this access benefits you. Your story matters. Citation
Physician specialty and the outcomes and cost of admissions for end-stage liver disease Ko C W, Kelley K, Meyer K E
 Physician specialty and the outcomes and cost of admissions for end-stage liver disease Ko C W, Kelley K, Meyer K E Record Status This is a critical abstract of an economic evaluation that meets the criteria
Physician specialty and the outcomes and cost of admissions for end-stage liver disease Ko C W, Kelley K, Meyer K E Record Status This is a critical abstract of an economic evaluation that meets the criteria
Rates and patterns of participation in cardiac rehabilitation in Victoria
 Rates and patterns of participation in cardiac rehabilitation in Victoria Vijaya Sundararajan, MD, MPH, Stephen Begg, MS, Michael Ackland, MBBS, MPH, FAPHM, Ric Marshall, PhD Victorian Department of Human
Rates and patterns of participation in cardiac rehabilitation in Victoria Vijaya Sundararajan, MD, MPH, Stephen Begg, MS, Michael Ackland, MBBS, MPH, FAPHM, Ric Marshall, PhD Victorian Department of Human
PERIOPERATIVE ANESTHETIC RISK IN THE GERIATRIC PATIENT
 PERIOPERATIVE ANESTHETIC RISK IN THE GERIATRIC PATIENT Susan H. Noorily, M.D. Clinical Professor of Anesthesiology Medical Director University Preoperative Medicine Center IMPORTANCE Half of all currently
PERIOPERATIVE ANESTHETIC RISK IN THE GERIATRIC PATIENT Susan H. Noorily, M.D. Clinical Professor of Anesthesiology Medical Director University Preoperative Medicine Center IMPORTANCE Half of all currently
Chapter 2: Identification and Care of Patients With CKD
 Chapter 2: Identification and Care of Patients With CKD Over half of patients in the Medicare 5% sample (aged 65 and older) had at least one of three diagnosed chronic conditions chronic kidney disease
Chapter 2: Identification and Care of Patients With CKD Over half of patients in the Medicare 5% sample (aged 65 and older) had at least one of three diagnosed chronic conditions chronic kidney disease
Why Target Delirium for Surgical Quality Improvement?
 Why Target Delirium for Surgical Quality Improvement? Tom Robinson MD FACS thomas.robinson@ucdenver.edu July 22, 2018 Disclosures Tom Robinson has no disclosures. Who Cares About the Brain? Acute Organ
Why Target Delirium for Surgical Quality Improvement? Tom Robinson MD FACS thomas.robinson@ucdenver.edu July 22, 2018 Disclosures Tom Robinson has no disclosures. Who Cares About the Brain? Acute Organ
APPENDIX: Supplementary Materials for Advance Directives And Nursing. Home Stays Associated With Less Aggressive End-Of-Life Care For
 Nicholas LH, Bynum JPW, Iwashnya TJ, Weir DR, Langa KM. Advance directives and nursing home stays associated with less aggressive end-of-life care for patients with severe dementia. Health Aff (MIllwood).
Nicholas LH, Bynum JPW, Iwashnya TJ, Weir DR, Langa KM. Advance directives and nursing home stays associated with less aggressive end-of-life care for patients with severe dementia. Health Aff (MIllwood).
Surgery in Frail Elders. Emily Finlayson, MD, MS Department of Surgery University of California, San Francisco September, 2011
 Surgery in Frail Elders Emily Finlayson, MD, MS Department of Surgery University of California, San Francisco September, 2011 What we re going to cover Mortality after surgery in the elderly Fact v Fantasy
Surgery in Frail Elders Emily Finlayson, MD, MS Department of Surgery University of California, San Francisco September, 2011 What we re going to cover Mortality after surgery in the elderly Fact v Fantasy
Chapter 2: Identification and Care of Patients With CKD
 Chapter 2: Identification and Care of Patients With Over half of patients from the Medicare 5% sample (restricted to age 65 and older) have a diagnosis of chronic kidney disease (), cardiovascular disease,
Chapter 2: Identification and Care of Patients With Over half of patients from the Medicare 5% sample (restricted to age 65 and older) have a diagnosis of chronic kidney disease (), cardiovascular disease,
Predictors of Post-injury Mortality in Elderly Patients with Trauma: A Master's Thesis
 University of Massachusetts Medical School escholarship@umms GSBS Dissertations and Theses Graduate School of Biomedical Sciences 7-21-2016 Predictors of Post-injury Mortality in Elderly Patients with
University of Massachusetts Medical School escholarship@umms GSBS Dissertations and Theses Graduate School of Biomedical Sciences 7-21-2016 Predictors of Post-injury Mortality in Elderly Patients with
National Bowel Cancer Audit. Detection and management of outliers: Clinical Outcomes Publication
 National Bowel Cancer Audit Detection and management of outliers: Clinical Outcomes Publication November 2017 1 National Bowel Cancer Audit (NBOCA) Detection and management of outliers Clinical Outcomes
National Bowel Cancer Audit Detection and management of outliers: Clinical Outcomes Publication November 2017 1 National Bowel Cancer Audit (NBOCA) Detection and management of outliers Clinical Outcomes
Delirium. Geriatric Giants Lecture Series Divisions of Geriatric Medicine and Care of the Elderly University of Alberta
 Delirium Geriatric Giants Lecture Series Divisions of Geriatric Medicine and Care of the Elderly University of Alberta Overview A. Delirium - the nature of the beast B. Significance of delirium C. An approach
Delirium Geriatric Giants Lecture Series Divisions of Geriatric Medicine and Care of the Elderly University of Alberta Overview A. Delirium - the nature of the beast B. Significance of delirium C. An approach
EPO-144 Patients with Morbid Obesity and Congestive Heart Failure Have Longer Operative Time and Room Time in Total Hip Arthroplasty
 SESUG 2016 EPO-144 Patients with Morbid Obesity and Congestive Heart Failure Have Longer Operative Time and Room Time in Total Hip Arthroplasty ABSTRACT Yubo Gao, University of Iowa Hospitals and Clinics,
SESUG 2016 EPO-144 Patients with Morbid Obesity and Congestive Heart Failure Have Longer Operative Time and Room Time in Total Hip Arthroplasty ABSTRACT Yubo Gao, University of Iowa Hospitals and Clinics,
Patient Selection for Surgery in RCC with Thrombus. E. Jason Abel, M.D.
 Patient Selection for Surgery in RCC with Thrombus E. Jason Abel, M.D. RCC with venous invasion Venous invasion occurs in ~10% of RCC Surgery more complex Increased risk for morbidity Thrombus may be confined
Patient Selection for Surgery in RCC with Thrombus E. Jason Abel, M.D. RCC with venous invasion Venous invasion occurs in ~10% of RCC Surgery more complex Increased risk for morbidity Thrombus may be confined
Geriatric Grand Rounds
 Geriatric Grand Rounds Prevalence and Risk Factors of Delirium in Older Patients Admitted to a Community Based Acute Care Hospital Tuesday, October 27, 2009 12:00 noon Dr. Bill Black Auditorium Glenrose
Geriatric Grand Rounds Prevalence and Risk Factors of Delirium in Older Patients Admitted to a Community Based Acute Care Hospital Tuesday, October 27, 2009 12:00 noon Dr. Bill Black Auditorium Glenrose
patient characteriuics Chapter Two introduction 58 increasing complexity of the patient population 60 epo use & anemia in the pre-esrd period 62
 introduction 58 < increasing complexity of the patient population 6 < epo use & anemia in the pre-esrd period 62 < biochemical & physical characteristics at initiation 64 < estimated gfr at intiation &
introduction 58 < increasing complexity of the patient population 6 < epo use & anemia in the pre-esrd period 62 < biochemical & physical characteristics at initiation 64 < estimated gfr at intiation &
Factors Associated with Initial Treatment for Clinically Localized Prostate Cancer
 Factors Associated with Initial Treatment for Clinically Localized Prostate Cancer Preliminary Results from the National Program of Cancer Registries Patterns of Care Study (PoC1) NAACCR Annual Meeting
Factors Associated with Initial Treatment for Clinically Localized Prostate Cancer Preliminary Results from the National Program of Cancer Registries Patterns of Care Study (PoC1) NAACCR Annual Meeting
Preoperative Anemia versus Blood Transfusion: Which is the Culprit for Worse Outcomes in Cardiac Surgery?
 Preoperative Anemia versus Blood Transfusion: Which is the Culprit for Worse Outcomes in Cardiac Surgery? Damien J. LaPar MD, MSc, James M. Isbell MD, MSCI, Jeffrey B. Rich MD, Alan M. Speir MD, Mohammed
Preoperative Anemia versus Blood Transfusion: Which is the Culprit for Worse Outcomes in Cardiac Surgery? Damien J. LaPar MD, MSc, James M. Isbell MD, MSCI, Jeffrey B. Rich MD, Alan M. Speir MD, Mohammed
Appendix. Potentially Preventable Complications (PPCs) identify. complications that can occur during an admission. There are 64
 identify. complications that can occur during an admission. There are 64") Calikoglu S, Murray R, Feeney D. Hospital pay-for-performance programs in Maryland produced strong results, including reduced hospital-acquired infections. Health Aff (Millwood). 2012;31(12). Appendix
Calikoglu S, Murray R, Feeney D. Hospital pay-for-performance programs in Maryland produced strong results, including reduced hospital-acquired infections. Health Aff (Millwood). 2012;31(12). Appendix
Reducing Variation in Perioperative Fluid Utilization Results in Improved Surgical Outcomes
 Reducing Variation in Perioperative Fluid Utilization Results in Improved Surgical Outcomes A Quality Improvement and Cost Savings Initiative for Hospitals, Surgeons and Anesthesiologists Hypoperfusion
Reducing Variation in Perioperative Fluid Utilization Results in Improved Surgical Outcomes A Quality Improvement and Cost Savings Initiative for Hospitals, Surgeons and Anesthesiologists Hypoperfusion
Delirium and cognitive impairment in the perioperative
 Delirium and cognitive impairment in the perioperative period Richard Sztramko Assistant Professor, McMaster University Divisions of Geriatrics and General Internal Medicine Disclosures Chief Medical Officer
Delirium and cognitive impairment in the perioperative period Richard Sztramko Assistant Professor, McMaster University Divisions of Geriatrics and General Internal Medicine Disclosures Chief Medical Officer
Finland and Sweden and UK GP-HOSP datasets
 Web appendix: Supplementary material Table 1 Specific diagnosis codes used to identify bladder cancer cases in each dataset Finland and Sweden and UK GP-HOSP datasets Netherlands hospital and cancer registry
Web appendix: Supplementary material Table 1 Specific diagnosis codes used to identify bladder cancer cases in each dataset Finland and Sweden and UK GP-HOSP datasets Netherlands hospital and cancer registry
Building a Standards and Verification Program for Older Adults. Melissa Hornor, MD GSI/SEGUE Session: American Geriatric Society May 20, 2017
 Building a Standards and Verification Program for Older Adults Melissa Hornor, MD GSI/SEGUE Session: American Geriatric Society May 20, 2017 Disclosures 2016-2018 ACS/JAHF James C. Thompson Geriatric Surgery
Building a Standards and Verification Program for Older Adults Melissa Hornor, MD GSI/SEGUE Session: American Geriatric Society May 20, 2017 Disclosures 2016-2018 ACS/JAHF James C. Thompson Geriatric Surgery
The Harvard community has made this article openly available. Please share how this access benefits you. Your story matters.
 Higher Rates of Packed Red Blood Cell and Fresh Frozen Plasma Transfusion are Associated with Increased Death and Complication in Non-Massively Transfused Patients: An Explanation for the Increased Burden
Higher Rates of Packed Red Blood Cell and Fresh Frozen Plasma Transfusion are Associated with Increased Death and Complication in Non-Massively Transfused Patients: An Explanation for the Increased Burden
Delirium. Delirium. Delirium Etiology and Pathophysiology. Fall 2018
 Three most common cognitive problems in adults 1. (acute confusion) 2. Dementia 3. Depression These problems often occur together Can you think of common stimuli for each? 1 1 State of temporary but acute
Three most common cognitive problems in adults 1. (acute confusion) 2. Dementia 3. Depression These problems often occur together Can you think of common stimuli for each? 1 1 State of temporary but acute