Semivoluntary movement (=unvoluntary)
|
|
|
- Rachel Turner
- 5 years ago
- Views:
Transcription

1 EXTRAPYRAMIDAL DISORDERS = Movement disorders = Degenerative disease 1
2 4 types of movements: Voluntary movement Semivoluntary movement (=unvoluntary) Involuntary movement Automatic movement 2

3 3
4 Movement disorders = Extrapyramidal disorder Disorder of regulation of voluntary motoric activity without direct influence towards muscle strength, sensibility, or cerebellum. 4
5 Extrapyramidal disorder Hyperkinetic disorder: abnormal involuntary movements Hypokinetic disorder: reduction of movements. = Movement disorders are caused by dysfunction of basal ganglia 5
6 Basal ganglia: Caudate nucleus Putamen Globus pallidus Subthalamic nucleus Substantia nigra 6
7 Diseases & syndrome with abnormal movements: Essential tremor (familial / benign) Parkinsonism Progressive supranuclear palsy Idiopathic torsion dystonia Chorea sydenham Sindroma Gilles de la Tourette Drug-induced movement disorders, etc. 7
8 Parkinsonism = Parkinson syndrome 1. Primary / Idiopathic = Paralysis agitans = Parkinson disease 2. Secondary/Symptomatic = Causes: - arteriosclerosis - anoxia /cerebral ischemia - drugs - toxic agent - encephalitis etc. 8
9 Parkinsonism (CON T) 3. Paraparkinson / Parkinson plus - Wilson disease - Huntington disease - Normotensive Hydrocephalus 9
10 Parkinson disease = Parkinson idiopathic = Paralysis agitans - Most commonly be found - Middle age to old age 10
11 Etiology and pathogenesis The certain Etiology is unknown PD is due to cells degeneration dopamine decreased in substantia nigra 11
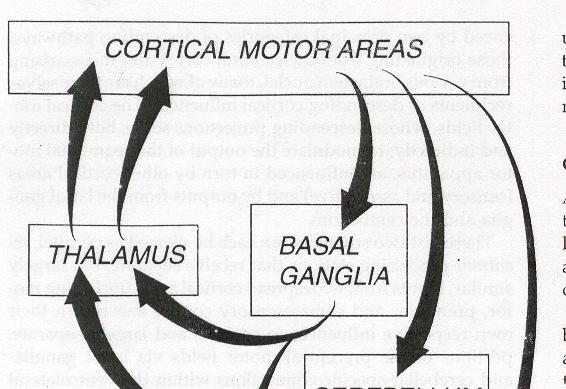
12 ACh DA I DA ACh I ACh i DA 12
13 Hypotesis: Aging process: dopaminergic neuronal death!!! anti oxydative-protective mechanism decreased Environmental toxin: - heavy metal (Iron, Zinc, mercury etc) - MPTP Genetic sensitivity Oxydative stress: dopamine reaction free radicals 13
14 Pathology Cutting of mid-brain: degeneration & neuronal death which contain melanin in substansia-nigra. Microscopic: In compacta zone: - Most of neuron are loss - Residual : containings Lewy-bodies 14
15 Lewy bodies in subst.nigra: 15
16 Clinical findings. Triad of symptoms: - rigidity - tremor - bradikinesis 1. tremor: - pill rolling tremor - during tension!!!, sleep - disappear - resting tremor = Parkinsonian tremor 16
17 Clinical findings (Con t) 2. Rigidity : cogwheel phenomenon. 3. Bradikinese 4. Weakness & fatique 5. Dystonia 6. Parkinsonian facies mask-like 7. Micrographia 8. Gait: Festinant gait = Parkinsonian gait 17
18 Clinical findings (con t) 9. freezing: late stage, suddlenly stop walking 10. Slowly speaking and monotone 11. Eye movements: - lack of blinking - eye movement disturb. - Glabella reflex (+) 12. Pain: paresthesia of limbs 18
19 Clinical findings (con t) 13. ANS disturbance: - salivary / excessive sweating -urinary incontinence etc. 14. Saliva!!! sialorrhea 15. Hypotension orthostatic hypotension 16. Depression 17. Dementia 19
20 Gait: 20

21 Tremor: 21

22 Rising: 22

23 Sitting: 23

24 Hypomimia: 24

25 Retropulsion: 25

26 Freezing: 26
27 Diagnostic procedure Diagnosis is made clinically based on clinical symptoms found EEG examination : may show diffuse slow wave MRI & CT Scan : may show cortical atrophy. 27
28 Treatment It is considered: due to dopamine deficiency in CNS. 1. Levodopa 2. Anticholinergic drugs: trihexyphenidyl 3. Antihistamine: diphenhydramine 4. Bromocriptine 5. Amantadine 6. Selegiline 28
29 TH DD L-tyrosine l-dopa DA TH: tyrosine hydroxylase DD: dopa-decarboxylase DA located outside vesicles will be catalyzed by enzymes : MAO(monoamine-oxydase) inside the neuron cell COMT(catechol-o-methyl-transferase) outside the neuron cell. 29
30 In peripheral : 1. l-dopa dopamine I dopa-decarboxylase v ^ dopa-decarboxylase inhibitor = carbidopa sinemet = benserazide madopar b 30
31 2. l-dopa dopamine I catechol-o-methyltransferase (COMT) v ^ COMT inhibitor : - tolcapone - entacapone 31
32 Prognosis: The prognosis is still poor. 32
33 Diseases & syndromes with abnormal movements : Essential tremor (familial / benign) Parkinsonism Progressive supranuclear palsy Idiopathic torsion dystonia Chorea sydenham Sindroma Gilles de la Tourette Drug-induced movement disorders, etc. 33
34 Parkinsonism = Parkinson syndrome 1. Primary/ Idiopathic = Paralysis agitans = Parkinson disease 2. Secondary / Symptomatic = Well known causes : - arteriosclerosis - anoxia / cerebral ischemia - drugs - toxic agents - encephalitis, etc. 34
35 Parkinsonism (Con t) 3. Paraparkinson / Parkinson plus - Wilson disease - Huntington disease - Normotensive Hydrocephalus 35
36 ESSENTIAL TREMOR Familial tremor Benign tremor Autosomal dominant Begin at teen-agers or young adults 36
37 Tremor usually affect one or both hands, head and voices, whereas foot is not affected. Neurological assessments show no other abnormality. Despite the longer the tremor the clearer the symptoms, usually it does not disturb,but the patient feels ashamed. 37
38 Sometimes it disturbs fine and difficult movements, writing and speaking when laryngeal muscle is involved. Consuming small amount of alcohol temporary improvement is reported, but the mechanism has not been known yet. 38
39 Treatment - Diazepam 6 15 mg per day - Propranolol mg per day - Primidone - Alprazolam - Not responsive: # thalamotomy # thalamic stimulation 39
40 CHOREA SYDENHAM Affecting children and young adults resulting from complication of streptococcus hemolytic A infection and the possible basic pathological features is arteritis. Approximately 30% of cases occur 2 or 3 months following rheumatoid fever or polyarthritis, the rest without such historys. 40
41 Onset can be acute or gradually within 4-6 months, can also occur during pregnancy or oral contraceptive users. Symptoms including abnormal chorea movements, sometimes unilaterally in mild cases. Changes of behavior In children may reveal easily to anger and doughty Labile of emotions 41
42 In 30% of cases involves the heart Treatment: bed rest, sedatives, prophylaxis antibiotics even though without acute rheumatoid fever. Penicillin injection to be continued orally until 20 years of age to prevent staphylococcal infection. The prognosis basically lies on the complication of the heart. 42
43 Drug-induced movement disorders 1. Parkinsonism 2. Acute dystonia or dyskinesis 3. Akathisia 4. Tardive dyskinesis 5. Neuroleptic malignant syndrome 6. Others. 43
44 Parkinsonism. Complication of dopamine receptor inhibitor drugs: - phenothiazine - butyrophenone - thioxanthene - metoclopramide 44
45 Parkinsonism (Con t) Symptoms : - rigidity - mask-like face - bradykinesis - tremor (seldom) Treatment : - Discontinue the drug - anti-cholinergic drugs (trihexyphenidyl) 45
46 Acute dystonia / dyskinesia blepharospasm torticollis facial grimacing following phenothiazine administration. Treatment: Intravenous anti-cholinergicdrug (benztropine 2 mg or diphenhydramine 50 mg). 46

47 Blepharospasm 47
48 Akathisia Motoric restlessness, compulsion to move or inability to sit still for more than a short period of time, keep standing or walking. Receiving phenothiazine Treatment: - Lowering the dose if possible - propranolol mg/hari - anticholinergic drugs / benzodiazepines 48
49 Tardive dyskinesia Repetitive involuntary movements of the mouth, tongue and lips, occasionally accompanied by dystonic posturing or choreoathetotic movements of trunk and limbs. Mostly following administration of neurolep tic, metoclopramide, antihistamines, tricyclic antidepressant and chronic alcohol abuse. 49

50 50
51 Tardive dyskinesia (Con t) Treatment: - Dopamine antagonists : haloperidol - Catecholamine-depleting agents: reserpine, tetrabenazine. - Baclofen - Calcium channel blocking agents - Vitamin E, etc. 51
52 Neuroleptic malignant syndrome An acute idiosyncratic reaction to - neuroleptic medication due to central dopamine receptor blockade. May also originate from non-neurololeptic drugs: metoclopramide, domperidone, amphetamines, reserpine, tetrabenazine, tricyclic antidepressants with lithium or with MAO inhibitor and withdrawal of antiparkinsonian medication. 52
53 Neuroleptic malignant syndrome(con t) The use of cocaine and 3.4 methy- lene dioxymethamphetamine (MDMA) = Ecstasy Symptoms are usually abrupt in onset, fever, encephalopathy with fluctuating confusion and agitation progressing to coma, labile BP, tachycardia, diaphoresis in association with dystonia and tremor. The couse is often rapid in untreated cases wit deterioration leading to cardiac failure, pulmonary congestion, pneumonia, renal failure and death. 53
54 Neuroleptic malignant syndrome (Con t) Treatment: - Discontinue the neuroleptic drugs - Control of body temperature - Monitor the BP, urine, electrolytes, temperature change - Administer bromocriptine mg/day by NGT - Dantrolene sodium i.v and convert to oral as improvement occurs. 54
55 Others: Levodopa various abnormal movement is related to dosage. Bromocriptine, anticholinergic drugs, phenytoin, carbamazepine, amphetamine, lithium and oral contraceptive may also result in chorea ect. 55
Parkinson s Disease. Sirilak yimcharoen
 Parkinson s Disease Sirilak yimcharoen EPIDEMIOLOGY ~1% of people over 55 years Age range 35 85 years peak age of onset is in the early 60s ~5% of cases characterized by an earlier age of onset (typically
Parkinson s Disease Sirilak yimcharoen EPIDEMIOLOGY ~1% of people over 55 years Age range 35 85 years peak age of onset is in the early 60s ~5% of cases characterized by an earlier age of onset (typically
Pharmacologic Treatment of Parkinson s Disease. Nicholas J. Silvestri, M.D. Assistant Professor of Neurology
 + Pharmacologic Treatment of Parkinson s Disease Nicholas J. Silvestri, M.D. Assistant Professor of Neurology + Overview n Brief review of Parkinson s disease (PD) n Clinical manifestations n Pathophysiology
+ Pharmacologic Treatment of Parkinson s Disease Nicholas J. Silvestri, M.D. Assistant Professor of Neurology + Overview n Brief review of Parkinson s disease (PD) n Clinical manifestations n Pathophysiology
Professor Tim Anderson
 Professor Tim Anderson Neurologist University of Otago Christchurch 11:00-11:55 WS #91: Shakes Jerks and Spasms - Recognition and Differential Diagnosis 12:05-13:00 WS #102: Shakes Jerks and Spasms - Recognition
Professor Tim Anderson Neurologist University of Otago Christchurch 11:00-11:55 WS #91: Shakes Jerks and Spasms - Recognition and Differential Diagnosis 12:05-13:00 WS #102: Shakes Jerks and Spasms - Recognition
Pharmacologic Treatment of Parkinson s Disease. Nicholas J. Silvestri, M.D. Associate Professor of Neurology
 + Pharmacologic Treatment of Parkinson s Disease Nicholas J. Silvestri, M.D. Associate Professor of Neurology + Disclosures n NO SIGNIFICANT FINANCIAL, GENERAL, OR OBLIGATION INTERESTS TO REPORT + Learning
+ Pharmacologic Treatment of Parkinson s Disease Nicholas J. Silvestri, M.D. Associate Professor of Neurology + Disclosures n NO SIGNIFICANT FINANCIAL, GENERAL, OR OBLIGATION INTERESTS TO REPORT + Learning
Movement Disorders. Eric Kraus, MD! Neurology!
 Movement Disorders Eric Kraus, MD! Neurology! Classify Bradykinesia! Tic! Myoclonus! Tremor! Dystonia! Athetosis! Chorea! Ballismus! Case 1 This 64 year-old female has had progression of a tremor over
Movement Disorders Eric Kraus, MD! Neurology! Classify Bradykinesia! Tic! Myoclonus! Tremor! Dystonia! Athetosis! Chorea! Ballismus! Case 1 This 64 year-old female has had progression of a tremor over
History Parkinson`s disease. Parkinson's disease was first formally described in 1817 by a London physician named James Parkinson
 Parkinsonismm History Parkinson`s disease Parkinson's disease was first formally described in 1817 by a London physician named James Parkinson Definition : Parkinsonism: Parkinsonism is a progressive neurological
Parkinsonismm History Parkinson`s disease Parkinson's disease was first formally described in 1817 by a London physician named James Parkinson Definition : Parkinsonism: Parkinsonism is a progressive neurological
Parkinson s disease Therapeutic strategies. Surat Tanprawate, MD Division of Neurology University of Chiang Mai
 Parkinson s disease Therapeutic strategies Surat Tanprawate, MD Division of Neurology University of Chiang Mai 1 Scope Modality of treatment Pathophysiology of PD and dopamine metabolism Drugs Are there
Parkinson s disease Therapeutic strategies Surat Tanprawate, MD Division of Neurology University of Chiang Mai 1 Scope Modality of treatment Pathophysiology of PD and dopamine metabolism Drugs Are there
Parts of the motor circuits
 MOVEMENT DISORDERS Parts of the motor circuits cortical centers: there are centers in all the cortical lobes subcortical centers: caudate nucleus putamen pallidum subthalamical nucleus (Luys) nucleus ruber
MOVEMENT DISORDERS Parts of the motor circuits cortical centers: there are centers in all the cortical lobes subcortical centers: caudate nucleus putamen pallidum subthalamical nucleus (Luys) nucleus ruber
Basal ganglia Sujata Sofat, class of 2009
 Basal ganglia Sujata Sofat, class of 2009 Basal ganglia Objectives Describe the function of the Basal Ganglia in movement Define the BG components and their locations Describe the motor loop of the BG
Basal ganglia Sujata Sofat, class of 2009 Basal ganglia Objectives Describe the function of the Basal Ganglia in movement Define the BG components and their locations Describe the motor loop of the BG
Identification number: TÁMOP /1/A
 Manifestation of Novel Social Challenges of the European Union in the Teaching Material of Medical Biotechnology Master s Programmes at the University of Pécs and at the University of Debrecen Identification
Manifestation of Novel Social Challenges of the European Union in the Teaching Material of Medical Biotechnology Master s Programmes at the University of Pécs and at the University of Debrecen Identification
Drug Therapy of Parkinsonism. Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia
 Drug Therapy of Parkinsonism Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Parkinsonism is a progressive neurological disorder of muscle movement, usually
Drug Therapy of Parkinsonism Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Parkinsonism is a progressive neurological disorder of muscle movement, usually
Parkinsonism or Parkinson s Disease I. Symptoms: Main disorder of movement. Named after, an English physician who described the then known, in 1817.
 Parkinsonism or Parkinson s Disease I. Symptoms: Main disorder of movement. Named after, an English physician who described the then known, in 1817. Four (4) hallmark clinical signs: 1) Tremor: (Note -
Parkinsonism or Parkinson s Disease I. Symptoms: Main disorder of movement. Named after, an English physician who described the then known, in 1817. Four (4) hallmark clinical signs: 1) Tremor: (Note -
Extrapyramidal Motor System. Basal Ganglia or Striatum. Basal Ganglia or Striatum 3/3/2010
 Extrapyramidal Motor System Basal Ganglia or Striatum Descending extrapyramidal paths receive input from other parts of motor system: From the cerebellum From the basal ganglia or corpus striatum Caudate
Extrapyramidal Motor System Basal Ganglia or Striatum Descending extrapyramidal paths receive input from other parts of motor system: From the cerebellum From the basal ganglia or corpus striatum Caudate
Martin A. Samuels, M.D. MOVEMENT DISORDERS
 Martin A. Samuels, M.D. MOVEMENT DISORDERS I. Nomenclature of Movement Disorders A. Too Little Movement 1. Paralysis (paresis) 2. Rigidity a. spasticity (pyramidal) b. "lead pipe" (extra pyramidal) c.
Martin A. Samuels, M.D. MOVEMENT DISORDERS I. Nomenclature of Movement Disorders A. Too Little Movement 1. Paralysis (paresis) 2. Rigidity a. spasticity (pyramidal) b. "lead pipe" (extra pyramidal) c.
Pathogenesis of Degenerative Diseases and Dementias. D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria)
. M. Path (U. of Alexandria)") Pathogenesis of Degenerative Diseases and Dementias D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria) Dementias Defined: as the development of memory impairment and other cognitive deficits
Pathogenesis of Degenerative Diseases and Dementias D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria) Dementias Defined: as the development of memory impairment and other cognitive deficits
Movement Disorders: A Brief Overview
 Movement Disorders: A Brief Overview Albert Hung, MD, PhD Massachusetts General Hospital Harvard Medical School August 17, 2006 Cardinal Features of Parkinsonism Tremor Rigidity Bradykinesia Postural imbalance
Movement Disorders: A Brief Overview Albert Hung, MD, PhD Massachusetts General Hospital Harvard Medical School August 17, 2006 Cardinal Features of Parkinsonism Tremor Rigidity Bradykinesia Postural imbalance
Professor Tim Anderson
 Professor Tim Anderson Neurologist University of Otago Christchurch 11:00-11:55 WS #91: Shakes Jerks and Spasms - Recognition and Differential Diagnosis 12:05-13:00 WS #102: Shakes Jerks and Spasms - Recognition
Professor Tim Anderson Neurologist University of Otago Christchurch 11:00-11:55 WS #91: Shakes Jerks and Spasms - Recognition and Differential Diagnosis 12:05-13:00 WS #102: Shakes Jerks and Spasms - Recognition
Parkinson's Disease. Robert L. Copeland, Ph.D. Howard University College of Medicine Department of Pharmacology
 Parkinson's Disease Robert L. Copeland, Ph.D. Howard University College of Medicine Department of Pharmacology 18 February 2002 Parkinson Disease Neurological disease affecting over four million patients
Parkinson's Disease Robert L. Copeland, Ph.D. Howard University College of Medicine Department of Pharmacology 18 February 2002 Parkinson Disease Neurological disease affecting over four million patients
Margo J Nell Dept Pharmacology
 Margo J Nell Dept Pharmacology 1 The extra pyramidal system Separation of cortico-spinal system (pyramidal system, (PS)) from the basal ganglia (extra pyramidal motor system (EPS)) because they produce
Margo J Nell Dept Pharmacology 1 The extra pyramidal system Separation of cortico-spinal system (pyramidal system, (PS)) from the basal ganglia (extra pyramidal motor system (EPS)) because they produce
Treatment of Parkinson s Disease and of Spasticity. Satpal Singh Pharmacology and Toxicology 3223 JSMBS
 Treatment of Parkinson s Disease and of Spasticity Satpal Singh Pharmacology and Toxicology 3223 JSMBS singhs@buffalo.edu 716-829-2453 1 Disclosures NO SIGNIFICANT FINANCIAL, GENERAL, OR OBLIGATION INTERESTS
Treatment of Parkinson s Disease and of Spasticity Satpal Singh Pharmacology and Toxicology 3223 JSMBS singhs@buffalo.edu 716-829-2453 1 Disclosures NO SIGNIFICANT FINANCIAL, GENERAL, OR OBLIGATION INTERESTS
475 GERIATRIC PSYCHOPHARMACOLOGY (p.1)
") 475 GERIATRIC PSYCHOPHARMACOLOGY (p.1) I. General Information? Use lower doses? Start low and go slow? Expect prolonged elimination ½ lives? Expect sedative-hypnotics to be dementing, to impair cognitive
475 GERIATRIC PSYCHOPHARMACOLOGY (p.1) I. General Information? Use lower doses? Start low and go slow? Expect prolonged elimination ½ lives? Expect sedative-hypnotics to be dementing, to impair cognitive
Parkinson s Disease in the Elderly A Physicians perspective. Dr John Coyle
 Parkinson s Disease in the Elderly A Physicians perspective Dr John Coyle Overview Introduction Epidemiology and aetiology Pathogenesis Diagnosis and clinical features Treatment Psychological issues/ non
Parkinson s Disease in the Elderly A Physicians perspective Dr John Coyle Overview Introduction Epidemiology and aetiology Pathogenesis Diagnosis and clinical features Treatment Psychological issues/ non
A. General features of the basal ganglia, one of our 3 major motor control centers:
 Reading: Waxman pp. 141-146 are not very helpful! Computer Resources: HyperBrain, Chapter 12 Dental Neuroanatomy Suzanne S. Stensaas, Ph.D. April 22, 2010 THE BASAL GANGLIA Objectives: 1. What are the
Reading: Waxman pp. 141-146 are not very helpful! Computer Resources: HyperBrain, Chapter 12 Dental Neuroanatomy Suzanne S. Stensaas, Ph.D. April 22, 2010 THE BASAL GANGLIA Objectives: 1. What are the
The motor regulator. 1) Basal ganglia/nucleus
 Basal ganglia/nucleus") The motor regulator 1) Basal ganglia/nucleus Neural structures involved in the control of movement Basal Ganglia - Components of the basal ganglia - Function of the basal ganglia - Connection and circuits
The motor regulator 1) Basal ganglia/nucleus Neural structures involved in the control of movement Basal Ganglia - Components of the basal ganglia - Function of the basal ganglia - Connection and circuits
A. General features of the basal ganglia, one of our 3 major motor control centers:
 Reading: Waxman pp. 141-146 are not very helpful! Computer Resources: HyperBrain, Chapter 12 Dental Neuroanatomy Suzanne S. Stensaas, Ph.D. March 1, 2012 THE BASAL GANGLIA Objectives: 1. What are the main
Reading: Waxman pp. 141-146 are not very helpful! Computer Resources: HyperBrain, Chapter 12 Dental Neuroanatomy Suzanne S. Stensaas, Ph.D. March 1, 2012 THE BASAL GANGLIA Objectives: 1. What are the main
VL VA BASAL GANGLIA. FUNCTIONAl COMPONENTS. Function Component Deficits Start/initiation Basal Ganglia Spontan movements
 BASAL GANGLIA Chris Cohan, Ph.D. Dept. of Pathology/Anat Sci University at Buffalo I) Overview How do Basal Ganglia affect movement Basal ganglia enhance cortical motor activity and facilitate movement.
BASAL GANGLIA Chris Cohan, Ph.D. Dept. of Pathology/Anat Sci University at Buffalo I) Overview How do Basal Ganglia affect movement Basal ganglia enhance cortical motor activity and facilitate movement.
III./3.1. Movement disorders with akinetic rigid symptoms
 III./3.1. Movement disorders with akinetic rigid symptoms III./3.1.1. Parkinson s disease Parkinson s disease (PD) is the second most common neurodegenerative disorder worldwide after Alzheimer s disease.
III./3.1. Movement disorders with akinetic rigid symptoms III./3.1.1. Parkinson s disease Parkinson s disease (PD) is the second most common neurodegenerative disorder worldwide after Alzheimer s disease.
Disorders of Movement M A R T I N H A R L E Y N E U R O L O G Y
 Disorders of Movement M A R T I N H A R L E Y N E U R O L O G Y Educational Objectives Improved history taking in patients with movement disorders. Develop a systematic approach to observing and describing
Disorders of Movement M A R T I N H A R L E Y N E U R O L O G Y Educational Objectives Improved history taking in patients with movement disorders. Develop a systematic approach to observing and describing
PARKINSON S DISEASE. Nigrostriatal Dopaminergic Neurons 5/11/16 CARDINAL FEATURES OF PARKINSON S DISEASE. Parkinson s disease
 5/11/16 PARKINSON S DISEASE Parkinson s disease Prevalence increases with age (starts 40s60s) Seen in all ethnic groups, M:F about 1.5:1 Second most common neurodegenerative disease Genetics role greater
5/11/16 PARKINSON S DISEASE Parkinson s disease Prevalence increases with age (starts 40s60s) Seen in all ethnic groups, M:F about 1.5:1 Second most common neurodegenerative disease Genetics role greater
Neurodegenerative Disease. April 12, Cunningham. Department of Neurosciences
 Neurodegenerative Disease April 12, 2017 Cunningham Department of Neurosciences NEURODEGENERATIVE DISEASE Any of a group of hereditary and sporadic conditions characterized by progressive dysfunction,
Neurodegenerative Disease April 12, 2017 Cunningham Department of Neurosciences NEURODEGENERATIVE DISEASE Any of a group of hereditary and sporadic conditions characterized by progressive dysfunction,
movement disorders for psychiatrists
 Movement disorders for psychiatrists Nandakumar Narayanan Assistant Professor, Neurology University of Iowa Thanks to Dr. Rodnitkzy Funding for my lab National Institutes of Health Carver Medical Trust
Movement disorders for psychiatrists Nandakumar Narayanan Assistant Professor, Neurology University of Iowa Thanks to Dr. Rodnitkzy Funding for my lab National Institutes of Health Carver Medical Trust
ANTIPARKINSONIAN DRUGS. DRUGs ACT ON CNS (Pharmacology) Unit-5(8)
 Unit-5(8)") ANTIPARKINSONIAN DRUGS DRUGs ACT ON CNS (Pharmacology) Unit-5(8) Parkinsonism (PD) Extrapyramidal motor function disorder characterized by Rigidity Tremor Hypokinesia/Bradykinesia Impairment of postural
ANTIPARKINSONIAN DRUGS DRUGs ACT ON CNS (Pharmacology) Unit-5(8) Parkinsonism (PD) Extrapyramidal motor function disorder characterized by Rigidity Tremor Hypokinesia/Bradykinesia Impairment of postural
Movement Disorders. Psychology 372 Physiological Psychology. Background. Myasthenia Gravis. Many Types
 Background Movement Disorders Psychology 372 Physiological Psychology Steven E. Meier, Ph.D. Listen to the audio lecture while viewing these slides Early Studies Found some patients with progressive weakness
Background Movement Disorders Psychology 372 Physiological Psychology Steven E. Meier, Ph.D. Listen to the audio lecture while viewing these slides Early Studies Found some patients with progressive weakness
Evaluation and Management of Parkinson s Disease in the Older Patient
 Evaluation and Management of Parkinson s Disease in the Older Patient David A. Hinkle, MD, PhD Comprehensive Movement Disorders Clinic Pittsburgh Institute for Neurodegenerative Diseases University of
Evaluation and Management of Parkinson s Disease in the Older Patient David A. Hinkle, MD, PhD Comprehensive Movement Disorders Clinic Pittsburgh Institute for Neurodegenerative Diseases University of
Drugs used in Parkinsonism
 Drugs used in Parkinsonism قادة فريق علم األدوية : لي التميمي & عبدالرحمن ذكري الشكر موصول ألعضاء الفريق املتميزين : جومانة القحطاني ندى الصومالي روان سعد القحطاني pharma436@outlook.com @pharma436 Your
Drugs used in Parkinsonism قادة فريق علم األدوية : لي التميمي & عبدالرحمن ذكري الشكر موصول ألعضاء الفريق املتميزين : جومانة القحطاني ندى الصومالي روان سعد القحطاني pharma436@outlook.com @pharma436 Your
Parkinson s Disease. Patients will ask you. 8/14/2015. Objectives
 Parkinson s Disease Jean Van Kingsley MS, FNP-BC Objectives Describe the pathophysiolgy of PD. Review clinical charachteristics of PD. Identify management strategies, to maximize functional status. Recognize
Parkinson s Disease Jean Van Kingsley MS, FNP-BC Objectives Describe the pathophysiolgy of PD. Review clinical charachteristics of PD. Identify management strategies, to maximize functional status. Recognize
Optimizing Clinical Communication in Parkinson s Disease:
 Optimizing Clinical Communication in Parkinson s Disease:,Strategies for improving communication between you and your neurologist PFNCA Symposium March 25, 2017 Pritha Ghosh, MD Assistant Professor of
Optimizing Clinical Communication in Parkinson s Disease:,Strategies for improving communication between you and your neurologist PFNCA Symposium March 25, 2017 Pritha Ghosh, MD Assistant Professor of
Chapter 161 Antipsychotics
 Chapter 161 Antipsychotics Episode Overview Extrapyramidal syndromes are a common complication of antipsychotic medications. First line treatment is benztropine or diphenhydramine. Lorazepam is used in
Chapter 161 Antipsychotics Episode Overview Extrapyramidal syndromes are a common complication of antipsychotic medications. First line treatment is benztropine or diphenhydramine. Lorazepam is used in
8/28/2017. Behind the Scenes of Parkinson s Disease
 BEHIND THE SCENCES IN Parkinson s Disease Behind the Scenes of Parkinson s Disease Anna Marie Wellins DNP, ANP C Objectives Describe prevalence of Parkinson's disease (PD) Describe the hallmark pathologic
BEHIND THE SCENCES IN Parkinson s Disease Behind the Scenes of Parkinson s Disease Anna Marie Wellins DNP, ANP C Objectives Describe prevalence of Parkinson's disease (PD) Describe the hallmark pathologic
parts of the gastrointenstinal tract. At the end of April 2008, it was temporarily withdrawn from the US Market because of problems related to
 parts of the gastrointenstinal tract. At the end of April 2008, it was temporarily withdrawn from the US Market because of problems related to crystallization of the drug, which caused unreliable drug
parts of the gastrointenstinal tract. At the end of April 2008, it was temporarily withdrawn from the US Market because of problems related to crystallization of the drug, which caused unreliable drug
DIFFERENTIAL DIAGNOSIS SARAH MARRINAN
 Parkinson s Academy Registrar Masterclass Sheffield DIFFERENTIAL DIAGNOSIS SARAH MARRINAN 17 th September 2014 Objectives Importance of age in diagnosis Diagnostic challenges Brain Bank criteria Differential
Parkinson s Academy Registrar Masterclass Sheffield DIFFERENTIAL DIAGNOSIS SARAH MARRINAN 17 th September 2014 Objectives Importance of age in diagnosis Diagnostic challenges Brain Bank criteria Differential
Parkinson s Disease Update. Presented by Joanna O Leary, MD Movement disorder neurologist Providence St. Vincent s
 Parkinson s Disease Update Presented by Joanna O Leary, MD Movement disorder neurologist Providence St. Vincent s What is a movement disorder? Neurological disorders that affect ability to move by causing
Parkinson s Disease Update Presented by Joanna O Leary, MD Movement disorder neurologist Providence St. Vincent s What is a movement disorder? Neurological disorders that affect ability to move by causing
ASHI691: Why We Fall Apart: The Neuroscience and Neurophysiology of Aging. Dr. Olav E. Krigolson Lecture 5: PARKINSONS DISEASE
 ASHI691: Why We Fall Apart: The Neuroscience and Neurophysiology of Aging Dr. Olav E. Krigolson krigolson@uvic.ca Lecture 5: PARKINSONS DISEASE The Basal Ganglia Primary motor cortex Execution of movement
ASHI691: Why We Fall Apart: The Neuroscience and Neurophysiology of Aging Dr. Olav E. Krigolson krigolson@uvic.ca Lecture 5: PARKINSONS DISEASE The Basal Ganglia Primary motor cortex Execution of movement
Neurodegenerative diseases
 Neurodegenerative diseases Hiwa K. Saaed, PhD Department of Pharmacology & Toxicology College of Pharmacy University of Sulaimani Hiwa.saaed@univsul.edu.iq 2018-19 Neurodegenerative diseases of the CNS
Neurodegenerative diseases Hiwa K. Saaed, PhD Department of Pharmacology & Toxicology College of Pharmacy University of Sulaimani Hiwa.saaed@univsul.edu.iq 2018-19 Neurodegenerative diseases of the CNS
COALINGA STATE HOSPITAL. Effective Date: August 31, 2006
 COALINGA STATE HOSPITAL NURSING POLICY AND PROCEDURE MANUAL SECTION Emergency Procedures POLICY NUMBER: 717 Effective Date: August 31, 2006 SUBJECT: NEUROLEPTIC MALIGNANT SYNDROME 1. PURPOSE: To provide
COALINGA STATE HOSPITAL NURSING POLICY AND PROCEDURE MANUAL SECTION Emergency Procedures POLICY NUMBER: 717 Effective Date: August 31, 2006 SUBJECT: NEUROLEPTIC MALIGNANT SYNDROME 1. PURPOSE: To provide
Department of Neurology, Rigshospitalet, 9 Blegdamsvej, PAULSON, O.B. Involuntary Movements. Tohoku J. Exp. Med., 1990, 161,
 Tohoku J. Exp. Med., 1990, 161, Suppl., 21-27 Involuntary Movements OLAF B. PAULSON Department of Neurology, Rigshospitalet, 9 Blegdamsvej, DK-2100, Copenhagen, Denmark PAULSON, O.B. Involuntary Movements.
Tohoku J. Exp. Med., 1990, 161, Suppl., 21-27 Involuntary Movements OLAF B. PAULSON Department of Neurology, Rigshospitalet, 9 Blegdamsvej, DK-2100, Copenhagen, Denmark PAULSON, O.B. Involuntary Movements.
Parkinson s Disease. Prevalence. Mark S. Baron, M.D. Cardinal Features. Clinical Characteristics. Not Just a Movement Disorder
 Prevalence Parkinson s Disease Mark S. Baron, M.D. Associate Professor of Neurology Movement Disorders Section VCU School of Medicine Common disorder Approaching 1% by 65 yrs of age, 2% by 80 yrs of age
Prevalence Parkinson s Disease Mark S. Baron, M.D. Associate Professor of Neurology Movement Disorders Section VCU School of Medicine Common disorder Approaching 1% by 65 yrs of age, 2% by 80 yrs of age
Involuntary Movements in Children and Adolescents: Is it Seizure, Tic or Something Else?
 Involuntary Movements in Children and Adolescents: Is it Seizure, Tic or Something Else? California Association of Nurse Practitioners Monterey, March 22, 2013 Julie Sprague-McRae, MS, RN, PPCNP-BC Ruth
Involuntary Movements in Children and Adolescents: Is it Seizure, Tic or Something Else? California Association of Nurse Practitioners Monterey, March 22, 2013 Julie Sprague-McRae, MS, RN, PPCNP-BC Ruth
An approach to movement disorders. Kailash Bhatia, DM, FRCP Professor of Clinical Neurology Institute of Neurology Queen Square, London
 An approach to movement disorders Kailash Bhatia, DM, FRCP Professor of Clinical Neurology Institute of Neurology Queen Square, London Neurology Diagnosis Two main questions: What parts of the nervous
An approach to movement disorders Kailash Bhatia, DM, FRCP Professor of Clinical Neurology Institute of Neurology Queen Square, London Neurology Diagnosis Two main questions: What parts of the nervous
Differential Diagnosis of Hypokinetic Movement Disorders
 Differential Diagnosis of Hypokinetic Movement Disorders Dr Donald Grosset Consultant Neurologist - Honorary Professor Institute of Neurological Sciences - Glasgow University Hypokinetic Parkinson's Disease
Differential Diagnosis of Hypokinetic Movement Disorders Dr Donald Grosset Consultant Neurologist - Honorary Professor Institute of Neurological Sciences - Glasgow University Hypokinetic Parkinson's Disease
Parkinson s Disease Update
 Parkinson s Disease Update Elise Anderson MD Providence Center for Parkinson s Disease October 26, 2017 11/6/2017 1 Disclosures GE Speaker, DaTSCAN 11/6/2017 2 Outline PD diagnosis Motor and nonmotor symptoms
Parkinson s Disease Update Elise Anderson MD Providence Center for Parkinson s Disease October 26, 2017 11/6/2017 1 Disclosures GE Speaker, DaTSCAN 11/6/2017 2 Outline PD diagnosis Motor and nonmotor symptoms
Strick Lecture 4 March 29, 2006 Page 1
 Strick Lecture 4 March 29, 2006 Page 1 Basal Ganglia OUTLINE- I. Structures included in the basal ganglia II. III. IV. Skeleton diagram of Basal Ganglia Loops with cortex Similarity with Cerebellar Loops
Strick Lecture 4 March 29, 2006 Page 1 Basal Ganglia OUTLINE- I. Structures included in the basal ganglia II. III. IV. Skeleton diagram of Basal Ganglia Loops with cortex Similarity with Cerebellar Loops
DRUG TREATMENT OF PARKINSON S DISEASE. Mr. D.Raju, M.pharm, Lecturer
 DRUG TREATMENT OF PARKINSON S DISEASE Mr. D.Raju, M.pharm, Lecturer PARKINSON S DISEASE (parkinsonism) is a neurodegenerative disorder which affects t h e b a s a l g a n g l i a - and is associated with
DRUG TREATMENT OF PARKINSON S DISEASE Mr. D.Raju, M.pharm, Lecturer PARKINSON S DISEASE (parkinsonism) is a neurodegenerative disorder which affects t h e b a s a l g a n g l i a - and is associated with
Extrapyramidal Symptoms Associated with Antipsychotic Use
 Extrapyramidal Symptoms Associated with Antipsychotic Use Tamara Pringsheim, MD, FRCPC, FAAN Associate Professor, University of Calgary Department of Clinical Neurosciences, Psychiatry, Pediatrics and
Extrapyramidal Symptoms Associated with Antipsychotic Use Tamara Pringsheim, MD, FRCPC, FAAN Associate Professor, University of Calgary Department of Clinical Neurosciences, Psychiatry, Pediatrics and
Parkinson s Disease Current Treatment Options
 Parkinson s Disease Current Treatment Options Daniel Kassicieh, D.O., FAAN Sarasota Neurology, P.A. PD: A Chronic Neurodegenerative Ds. 1 Million in USA Epidemiology 50,000 New Cases per Year Majority
Parkinson s Disease Current Treatment Options Daniel Kassicieh, D.O., FAAN Sarasota Neurology, P.A. PD: A Chronic Neurodegenerative Ds. 1 Million in USA Epidemiology 50,000 New Cases per Year Majority
Parkinson s Disease and Its Treatment
 Parkinson s Disease and Its Treatment By H. David Bergman, Ph.D. Dean, Southwestern Oklahoma State University, College of Pharmacy Goals and Objectives Goals: To provide the pharmacist with information
Parkinson s Disease and Its Treatment By H. David Bergman, Ph.D. Dean, Southwestern Oklahoma State University, College of Pharmacy Goals and Objectives Goals: To provide the pharmacist with information
MOVEMENT OUTLINE. The Control of Movement: Muscles! Motor Reflexes Brain Mechanisms of Movement Mirror Neurons Disorders of Movement
 MOVEMENT 2 Dr. Steinmetz 3 OUTLINE The Control of Movement: Muscles! Motor Reflexes Brain Mechanisms of Movement Mirror Neurons Disorders of Movement Parkinson s Disease Huntington s Disease 1 4 TYPES
MOVEMENT 2 Dr. Steinmetz 3 OUTLINE The Control of Movement: Muscles! Motor Reflexes Brain Mechanisms of Movement Mirror Neurons Disorders of Movement Parkinson s Disease Huntington s Disease 1 4 TYPES
DISORDERS OF THE MOTOR SYSTEM. Jeanette J. Norden, Ph.D. Professor Emerita Vanderbilt University School of Medicine
 DISORDERS OF THE MOTOR SYSTEM Jeanette J. Norden, Ph.D. Professor Emerita Vanderbilt University School of Medicine THE MOTOR SYSTEM To understand disorders of the motor system, we need to review how a
DISORDERS OF THE MOTOR SYSTEM Jeanette J. Norden, Ph.D. Professor Emerita Vanderbilt University School of Medicine THE MOTOR SYSTEM To understand disorders of the motor system, we need to review how a
Drugs Affecting the Central Nervous System
 Asst Prof Inam S Arif isamalhaj@yahoo.com Drugs Affecting the Central Nervous System Ass Efferent neurons in ANS Neurodegenerative Diseases Parkinson s Disease Multiple Sclerosis Alzheimer s Disease
Asst Prof Inam S Arif isamalhaj@yahoo.com Drugs Affecting the Central Nervous System Ass Efferent neurons in ANS Neurodegenerative Diseases Parkinson s Disease Multiple Sclerosis Alzheimer s Disease
Basal Ganglia. Today s lecture is about Basal Ganglia and it covers:
 Basal Ganglia Motor system is complex interaction between Lower motor neurons (spinal cord and brainstem circuits) and Upper motor neurons (pyramidal and extrapyramidal tracts) plus two main regulators
Basal Ganglia Motor system is complex interaction between Lower motor neurons (spinal cord and brainstem circuits) and Upper motor neurons (pyramidal and extrapyramidal tracts) plus two main regulators
Introductory Clinical Pharmacology Chapter 32 Antiparkinsonism Drugs
 Introductory Clinical Pharmacology Chapter 32 Antiparkinsonism Drugs Dopaminergic Drugs: Actions Symptoms of parkinsonism are caused by depletion of dopamine in CNS Amantadine: makes more of dopamine available
Introductory Clinical Pharmacology Chapter 32 Antiparkinsonism Drugs Dopaminergic Drugs: Actions Symptoms of parkinsonism are caused by depletion of dopamine in CNS Amantadine: makes more of dopamine available
PARKINSON S MEDICATION
 PARKINSON S MEDICATION History 1940 50 s Neurosurgeons operated on basal ganglia. Improved symptoms. 12% mortality 1960 s: Researchers identified low levels of dopamine caused Parkinson s leading to development
PARKINSON S MEDICATION History 1940 50 s Neurosurgeons operated on basal ganglia. Improved symptoms. 12% mortality 1960 s: Researchers identified low levels of dopamine caused Parkinson s leading to development
Alison Charleston 1 st September 2016
 Alison Charleston 1 st September 2016 Clinical features of Parkinson s disease Differential diagnosis Management of the motor features Non-motor and neuropsychiatric aspects 100-200 per 100,000 prevalence
Alison Charleston 1 st September 2016 Clinical features of Parkinson s disease Differential diagnosis Management of the motor features Non-motor and neuropsychiatric aspects 100-200 per 100,000 prevalence
March 2004 Parkinson s Disease H01
 W-F Professional Associates, Inc. 400 Lake Cook Rd., Suite 207 Deerfield, IL 60015 847-945-8050 March 2004 Parkinson s Disease 707-000-04-003-H01 FLORIDA PHARMACISTS READ THIS VERY IMPORTANT CE BROKER
W-F Professional Associates, Inc. 400 Lake Cook Rd., Suite 207 Deerfield, IL 60015 847-945-8050 March 2004 Parkinson s Disease 707-000-04-003-H01 FLORIDA PHARMACISTS READ THIS VERY IMPORTANT CE BROKER
MOVEMENT DISORDERS UPDATE H. MURRAY TODD, M.D., F.A.A.N.
 MOVEMENT DISORDERS UPDATE H. MURRAY TODD, M.D., F.A.A.N. Movement Disorders Hypokinesia : decreased voluntary and automatic movements Hyperkinesia : excessive movements HYPOKINESIAS Parkinson s disease
MOVEMENT DISORDERS UPDATE H. MURRAY TODD, M.D., F.A.A.N. Movement Disorders Hypokinesia : decreased voluntary and automatic movements Hyperkinesia : excessive movements HYPOKINESIAS Parkinson s disease
Clinical Features and Treatment of Parkinson s Disease
 Clinical Features and Treatment of Parkinson s Disease Richard Camicioli, MD, FRCPC Cognitive and Movement Disorders Department of Medicine University of Alberta 1 Objectives To review the diagnosis and
Clinical Features and Treatment of Parkinson s Disease Richard Camicioli, MD, FRCPC Cognitive and Movement Disorders Department of Medicine University of Alberta 1 Objectives To review the diagnosis and
Scott J Sherman MD, PhD The University of Arizona PARKINSON DISEASE
 Scott J Sherman MD, PhD The University of Arizona PARKINSON DISEASE LEARNING OBJECTIVES The Course Participant will: 1. Be familiar with the pathogenesis of Parkinson s Disease (PD) 2. Understand clinical
Scott J Sherman MD, PhD The University of Arizona PARKINSON DISEASE LEARNING OBJECTIVES The Course Participant will: 1. Be familiar with the pathogenesis of Parkinson s Disease (PD) 2. Understand clinical
Dr Barry Snow. Neurologist Auckland District Health Board
 Dr Barry Snow Neurologist Auckland District Health Board Dystonia and Parkinson s disease Barry Snow Gowers 1888: Tetanoid chorea Dystonia a movement disorder characterized by sustained or intermittent
Dr Barry Snow Neurologist Auckland District Health Board Dystonia and Parkinson s disease Barry Snow Gowers 1888: Tetanoid chorea Dystonia a movement disorder characterized by sustained or intermittent
Prior Authorization with Quantity Limit Program Summary
 Gocovri (amantadine) Prior Authorization with Quantity Limit Program Summary This prior authorization applies to Commercial, NetResults A series, SourceRx and Health Insurance Marketplace formularies.
Gocovri (amantadine) Prior Authorization with Quantity Limit Program Summary This prior authorization applies to Commercial, NetResults A series, SourceRx and Health Insurance Marketplace formularies.
Drug Management of Parkinsonism. By Prof. Mohammad Saleh M. Hassan PhD. (Pharma); MSc. (Ped.); MHPE (Ed.)
; MSc. (Ped.); MHPE (Ed.)") Drug Management of Parkinsonism By Prof. Mohammad Saleh M. Hassan PhD. (Pharma); MSc. (Ped.); MHPE (Ed.) Drug management of Parkinsonism Levodopa Ergot derivatives noamine Oxidaes Inhibitors Catechol-Omethyl
Drug Management of Parkinsonism By Prof. Mohammad Saleh M. Hassan PhD. (Pharma); MSc. (Ped.); MHPE (Ed.) Drug management of Parkinsonism Levodopa Ergot derivatives noamine Oxidaes Inhibitors Catechol-Omethyl
Tremor 101. Objectives 9/30/2015. Importance of tremors
 Tremor 101 Umer Akbar, MD Assistant Professor, Brown University Movement Disorders Program, Rhode Island Hospital & Butler Hospital Objectives Recognize and describe the qualities of common types of tremor
Tremor 101 Umer Akbar, MD Assistant Professor, Brown University Movement Disorders Program, Rhode Island Hospital & Butler Hospital Objectives Recognize and describe the qualities of common types of tremor
M. Carranza M. R. Snyder J. Davenport Shaw T. A. Zesiewicz. Parkinson s Disease. A Guide to Medical Treatment
 M. Carranza M. R. Snyder J. Davenport Shaw T. A. Zesiewicz Parkinson s Disease A Guide to Medical Treatment SEEd srl. All rights reserved Piazza Carlo Emanuele II, 19 10123 Torino, Italy Tel. 011.566.02.58
M. Carranza M. R. Snyder J. Davenport Shaw T. A. Zesiewicz Parkinson s Disease A Guide to Medical Treatment SEEd srl. All rights reserved Piazza Carlo Emanuele II, 19 10123 Torino, Italy Tel. 011.566.02.58
PARKINSON S PRIMER. Dr. Kathryn Giles MD, MSc, FRCPC Cambridge, Ontario, Canada
 PARKINSON S PRIMER Dr. Kathryn Giles MD, MSc, FRCPC Cambridge, Ontario, Canada COPYRIGHT 2017 BY SEA COURSES INC. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
PARKINSON S PRIMER Dr. Kathryn Giles MD, MSc, FRCPC Cambridge, Ontario, Canada COPYRIGHT 2017 BY SEA COURSES INC. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
Lecture 5 Skeletal muscle relaxants. Pharmacologic management of parkinsonism and other movement disorders.
 Lecture 5 Skeletal muscle relaxants. Pharmacologic management of parkinsonism and other movement disorders. I. SKELETAL MUSCLE RELAXANTS Skeletal muscle relaxants are pharmacologically active substances
Lecture 5 Skeletal muscle relaxants. Pharmacologic management of parkinsonism and other movement disorders. I. SKELETAL MUSCLE RELAXANTS Skeletal muscle relaxants are pharmacologically active substances
Movement disorders. Dr Rick Leventer Royal Children s Hospital
 Movement disorders Dr Rick Leventer Royal Children s Hospital richard.leventer@rch.org.au Movement disorders! conditions that affect the speed, fluency, quality, and ease of movement! usually affect TONE
Movement disorders Dr Rick Leventer Royal Children s Hospital richard.leventer@rch.org.au Movement disorders! conditions that affect the speed, fluency, quality, and ease of movement! usually affect TONE
Parkinson s Disease: initial diagnosis, initial treatment & non-motor features. J. Timothy Greenamyre, MD, PhD
 Parkinson s Disease: initial diagnosis, initial treatment & non-motor features J. Timothy Greenamyre, MD, PhD Involuntary tremulous motion, with lessened muscular power, in parts not in action and even
Parkinson s Disease: initial diagnosis, initial treatment & non-motor features J. Timothy Greenamyre, MD, PhD Involuntary tremulous motion, with lessened muscular power, in parts not in action and even
Damage on one side.. (Notes) Just remember: Unilateral damage to basal ganglia causes contralateral symptoms.
 Just remember: Unilateral damage to basal ganglia causes contralateral symptoms.") Lecture 20 - Basal Ganglia Basal Ganglia (Nolte 5 th Ed pp 464) Damage to the basal ganglia produces involuntary movements. Although the basal ganglia do not influence LMN directly (to cause this involuntary
Lecture 20 - Basal Ganglia Basal Ganglia (Nolte 5 th Ed pp 464) Damage to the basal ganglia produces involuntary movements. Although the basal ganglia do not influence LMN directly (to cause this involuntary
Visualization and simulated animations of pathology and symptoms of Parkinson s disease
 Visualization and simulated animations of pathology and symptoms of Parkinson s disease Prof. Yifan HAN Email: bctycan@ust.hk 1. Introduction 2. Biochemistry of Parkinson s disease 3. Course Design 4.
Visualization and simulated animations of pathology and symptoms of Parkinson s disease Prof. Yifan HAN Email: bctycan@ust.hk 1. Introduction 2. Biochemistry of Parkinson s disease 3. Course Design 4.
Parkinson Disease. Lorraine Kalia, MD, PhD, FRCPC. Presented by: Ontario s Geriatric Steering Committee
 Parkinson Disease Lorraine Kalia, MD, PhD, FRCPC Key Learnings Parkinson Disease (L. Kalia) Key Learnings Parkinson disease is the most common but not the only cause of parkinsonism Parkinson disease is
Parkinson Disease Lorraine Kalia, MD, PhD, FRCPC Key Learnings Parkinson Disease (L. Kalia) Key Learnings Parkinson disease is the most common but not the only cause of parkinsonism Parkinson disease is
First described by James Parkinson in his classic 1817 monograph, "An Essay on the Shaking Palsy"
 Parkinson's Disease First described by James Parkinson in his classic 1817 monograph, "An Essay on the Shaking Palsy" Parkinson s disease (PD) is a neurological disorder characterized by a progressive
Parkinson's Disease First described by James Parkinson in his classic 1817 monograph, "An Essay on the Shaking Palsy" Parkinson s disease (PD) is a neurological disorder characterized by a progressive
An Approach to Patients with Movement Disorders
 An Approach to Patients with Movement Disorders Joaquim Ferreira, MD, PhD Laboratory of Clinical Pharmacology and Therapeutics Faculty of Medicine University of Lisbon EDUCATIONAL TOOLS MDS video library
An Approach to Patients with Movement Disorders Joaquim Ferreira, MD, PhD Laboratory of Clinical Pharmacology and Therapeutics Faculty of Medicine University of Lisbon EDUCATIONAL TOOLS MDS video library
2-The age at onset of PD is variable, usually between 50 and 80 years, with a mean onset of 55 years (1).
.") Parkinson Disease 1-Parkinson disease (PD) is a chronic, progressive movement disorder resulting from loss of dopamine from the nigrostriatal tracts in the brain, and is characterized by rigidity, bradykinesia,
Parkinson Disease 1-Parkinson disease (PD) is a chronic, progressive movement disorder resulting from loss of dopamine from the nigrostriatal tracts in the brain, and is characterized by rigidity, bradykinesia,
Evaluation of Parkinson s Patients and Primary Care Providers
 Evaluation of Parkinson s Patients and Primary Care Providers 2018 Movement Disorders Half Day Symposium Elise Anderson MD Medical Co-Director, PBSI Movement Disorders 6/28/2018 1 Disclosures GE Speaker,
Evaluation of Parkinson s Patients and Primary Care Providers 2018 Movement Disorders Half Day Symposium Elise Anderson MD Medical Co-Director, PBSI Movement Disorders 6/28/2018 1 Disclosures GE Speaker,
Chapter 8. Parkinsonism. M.G.Rajanandh, Dept. of Pharmacy Practice, SRM College of Pharmacy, SRM University.
 Chapter 8 Parkinsonism M.G.Rajanandh, Dept. of Pharmacy Practice, SRM College of Pharmacy, SRM University. Definition of Parkinson s Disease Parkinson's disease is a progressive, neurodegenerative disease
Chapter 8 Parkinsonism M.G.Rajanandh, Dept. of Pharmacy Practice, SRM College of Pharmacy, SRM University. Definition of Parkinson s Disease Parkinson's disease is a progressive, neurodegenerative disease
Elements for a public summary
 VI.2 VI.2.1 Elements for a public summary Overview of disease epidemiology Parkinson s disease affects individuals globally (WHO 2006). It is the most common serious movement disorder, including speech
VI.2 VI.2.1 Elements for a public summary Overview of disease epidemiology Parkinson s disease affects individuals globally (WHO 2006). It is the most common serious movement disorder, including speech
Chapter 20. Media Directory. Amyotrophic Lateral Sclerosis. Alzheimer s Disease. Huntington s Chorea. Multiple Sclerosis
 Chapter 20 Drugs for Degenerative Diseases of the Nervous System Slide 18 Media Directory Levadopa Animation Upper Saddle River, New Jersey 07458 All rights reserved. Alzheimer s Disease Amyotrophic Lateral
Chapter 20 Drugs for Degenerative Diseases of the Nervous System Slide 18 Media Directory Levadopa Animation Upper Saddle River, New Jersey 07458 All rights reserved. Alzheimer s Disease Amyotrophic Lateral
Treatment of Parkinson s Disease: Present and Future
 Treatment of Parkinson s Disease: Present and Future Karen Blindauer, MD Professor of Neurology Director of Movement Disorders Program Medical College of Wisconsin Neuropathology: Loss of Dopamine- Producing
Treatment of Parkinson s Disease: Present and Future Karen Blindauer, MD Professor of Neurology Director of Movement Disorders Program Medical College of Wisconsin Neuropathology: Loss of Dopamine- Producing
PARKINS ON CENTER. Parkinson s Disease: Diagnosis and Management. Learning Objectives: Recognition of PD OHSU. Disclosure Information
 OHSU PARKINS ON CENTER Parkinson s Disease: Diagnosis and Management for Every MD Disclosure Information Grants/Research Support: National Parkinson Foundation, NIH, Michael J. Fox Foundation Consultant:
OHSU PARKINS ON CENTER Parkinson s Disease: Diagnosis and Management for Every MD Disclosure Information Grants/Research Support: National Parkinson Foundation, NIH, Michael J. Fox Foundation Consultant:
10th Medicine Review Course st July Prakash Kumar
 10th Medicine Review Course 2018 21 st July 2018 Drug Therapy for Parkinson's disease Prakash Kumar National Neuroscience Institute Singapore General Hospital Sengkang General Hospital Singhealth Duke-NUS
10th Medicine Review Course 2018 21 st July 2018 Drug Therapy for Parkinson's disease Prakash Kumar National Neuroscience Institute Singapore General Hospital Sengkang General Hospital Singhealth Duke-NUS
Objectives. Distinguishing Parkinson s disease from other parkinsonian and tremor syndromes. Characteristics. Basal Ganglia Structures
 12:45 1:30 pm PD or not PD? Distinguishing Parkinson s Disease From Other Parkinsonian and Tremor Syndromes SPEAKER Jennifer G. Goldman, MD, MS Presenter Disclosure Information The following relationships
12:45 1:30 pm PD or not PD? Distinguishing Parkinson s Disease From Other Parkinsonian and Tremor Syndromes SPEAKER Jennifer G. Goldman, MD, MS Presenter Disclosure Information The following relationships
Functional Distinctions
 Functional Distinctions FUNCTION COMPONENT DEFICITS Start Basal Ganglia Spontaneous Movements Move UMN/LMN Cerebral Cortex Brainstem, Spinal cord Roots/peripheral nerves Plan Cerebellum Ataxia Adjust Cerebellum
Functional Distinctions FUNCTION COMPONENT DEFICITS Start Basal Ganglia Spontaneous Movements Move UMN/LMN Cerebral Cortex Brainstem, Spinal cord Roots/peripheral nerves Plan Cerebellum Ataxia Adjust Cerebellum
Cardinal Features of Parkinson s. Management of Parkinson s Disease. Drug Induced Parkinson s. Other Parkinson s Symptoms.
 Cardinal Features of Parkinson s Management of Parkinson s Disease Kristin S. Meyer, PharmD, CGP, FASHP Assistant Professor of Pharmacy Practice Drake University & Iowa Veterans Home Spring 2009 Tremor
Cardinal Features of Parkinson s Management of Parkinson s Disease Kristin S. Meyer, PharmD, CGP, FASHP Assistant Professor of Pharmacy Practice Drake University & Iowa Veterans Home Spring 2009 Tremor
Medications used to treat Parkinson s disease
 Medications used to treat Parkinson s disease Edwin B. George, M.D., Ph.D. Director of Wayne State University Movement Disorder Clinic University Health Center Neurology Clinic University Health The John
Medications used to treat Parkinson s disease Edwin B. George, M.D., Ph.D. Director of Wayne State University Movement Disorder Clinic University Health Center Neurology Clinic University Health The John
Parkinson s Disease Initial Clinical and Diagnostic Evaluation. J. Timothy Greenamyre, MD, PhD
 Parkinson s Disease Initial Clinical and Diagnostic Evaluation J. Timothy Greenamyre, MD, PhD Involuntary tremulous motion, with lessened muscular power, in parts not in action and even when supported
Parkinson s Disease Initial Clinical and Diagnostic Evaluation J. Timothy Greenamyre, MD, PhD Involuntary tremulous motion, with lessened muscular power, in parts not in action and even when supported
Sign up to receive ATOTW weekly -
 PARKINSON S DISEASE ANAESTHESIA TUTORIAL OF THE WEEK 45 1 st FEBRUARY 2007 Dr Ritu Gupta ritugupta@doctors.org.uk MCQ s 1. During anaesthesia, a patient with Parkinson s disease on levodopa should not
PARKINSON S DISEASE ANAESTHESIA TUTORIAL OF THE WEEK 45 1 st FEBRUARY 2007 Dr Ritu Gupta ritugupta@doctors.org.uk MCQ s 1. During anaesthesia, a patient with Parkinson s disease on levodopa should not
Hyperkinetic movement disorders are. Hyperkinetic Movement Disorders. Cases in Movement Disorders. James case. About Tom
 Hyperkinetic Movement Disorders Sarah Furtado, MD, PhD, FRCPC James case A mother brings her son James, 10, to your office because of repetitive sniffing sounds and repetitive eye blinking. This sniffing
Hyperkinetic Movement Disorders Sarah Furtado, MD, PhD, FRCPC James case A mother brings her son James, 10, to your office because of repetitive sniffing sounds and repetitive eye blinking. This sniffing
STEADY YOUR APPROACH TO TREMOR (OVERVIEW OF DIFFERENTIAL DIAGNOSIS)
") STEADY YOUR APPROACH TO TREMOR (OVERVIEW OF DIFFERENTIAL DIAGNOSIS) Karen M. Thomas D.O. Diplomate, ABPN Director of Movement Disorders Program Director of Comprehensive Parkinson s Disease Program Sentara
STEADY YOUR APPROACH TO TREMOR (OVERVIEW OF DIFFERENTIAL DIAGNOSIS) Karen M. Thomas D.O. Diplomate, ABPN Director of Movement Disorders Program Director of Comprehensive Parkinson s Disease Program Sentara
The symptoms of the Parkinson s disease may vary from person to person. The symptoms might include the following:
 1 PARKINSON S DISEASE Parkinson's disease is a long term disease related to the central nervous system that mainly affects the motor system, resulting in the loss of dopamine, which helps in producing
1 PARKINSON S DISEASE Parkinson's disease is a long term disease related to the central nervous system that mainly affects the motor system, resulting in the loss of dopamine, which helps in producing
Dystonia: Title. A real pain in the neck. in All the Wrong Places
 Focus on CME at the University of Western Ontario Dystonia: Title in All the Wrong Places A real pain in the neck By Mandar Jog, MD, FRCPC and; Mary Jenkins, MD, FRCPC What is dystonia? Dystonia is a neurologic
Focus on CME at the University of Western Ontario Dystonia: Title in All the Wrong Places A real pain in the neck By Mandar Jog, MD, FRCPC and; Mary Jenkins, MD, FRCPC What is dystonia? Dystonia is a neurologic
UNIVERSITY OF JORDAN FACULTY OF MEDICINE DEPARTMENT OF PHYSIOLOGY & BIOCHEMISTRY NEUROPHYSIOLOGY (MEDICAL) Spring, 2014
 Spring, 2014") UNIVERSITY OF JORDAN FACULTY OF MEDICINE DEPARTMENT OF PHYSIOLOGY & BIOCHEMISTRY NEUROPHYSIOLOGY (MEDICAL) Spring, 2014 Textbook of Medical Physiology by: Guyton & Hall, 11 th edition 2006 Eman Al-Khateeb,
UNIVERSITY OF JORDAN FACULTY OF MEDICINE DEPARTMENT OF PHYSIOLOGY & BIOCHEMISTRY NEUROPHYSIOLOGY (MEDICAL) Spring, 2014 Textbook of Medical Physiology by: Guyton & Hall, 11 th edition 2006 Eman Al-Khateeb,