An approach to movement disorders. Kailash Bhatia, DM, FRCP Professor of Clinical Neurology Institute of Neurology Queen Square, London
|
|
|
- Ralph Townsend
- 5 years ago
- Views:
Transcription

1 An approach to movement disorders Kailash Bhatia, DM, FRCP Professor of Clinical Neurology Institute of Neurology Queen Square, London
2 Neurology Diagnosis Two main questions: What parts of the nervous system are affected? What is the etiology? Answers based on: History Clinical examination Investigations
3 History and examination in a movement disorder case Three points to stress in history: Birth history- anoxia, peri-natal problems, milestones (delayed onset movement disorders) Family history- positive, negative and absent family history (many movement disorders conditions are inherited) Drug and toxin history: neuroleptics, antiepileptics, illegal substances, toxins (many movement disorders are drug related)
4 Special points in examination of a movement disorder case Cognition/speech Eye movements- saccades and pursuit -Vertical gaze palsy and slow saccades in Progressive supranuclear palsy in a parkinsonian patient - Difficulty initiating saccades in Huntington s disease Gait: Arm swing, stride-length, freezing, postural reflexes Bradykinesia: Repeated finger tapping- decrement and fatiguing, foot tapping
5 History and examination in a movement disorder case Level 1: Phenomenology- What is the main category of movement disorder? Level 2: Distribution of movement disorder, associated signs or features including history (age etc.) to help consider etiology Level 3: Investigations keeping in mind history and signs to arrive at diagnosis
6 Phenomenological Classification of Movement Disorders Movement Disorders are classified broadly into two main groups: HYPOKINETIC DISORDERS: too little movement bradykinesia (slowness of movements) (Parkinson s Disease and other akinetic rigid syndromes) HYPERKINETIC DISORDERS: too much movement dyskinesias- (different types of involuntary movements)
7 Hyperkinetic Disorders Five main types: - Tremor - Tics - Chorea - Myoclonus - Dystonia Decide which group does the patient best fit
8 Tremor Definition: Rhythmic oscillation of a body part. Tremors can be classified as: Rest: occurs when affected body part is at rest Postural: occurs when arms are outstretched Kinetic: occurs during movement of body part.
9 Tremor Resting tremor: - Parkinson s disease and other parkinsonian disorders, dystonic tremor, one component of rubral tremor, severe ET, Postural: - Essential tremor, Physiological - PD, Dystonic tremor etc Kinetic: - Cerebellar disorders
10 Definition: Irregular, brief, purposeless movements that flit from one body part to another Chorea
11 Chorea Many causes: Acquired and inherited -Drugs/ Oral contraceptives - Basal ganglia lesions - Sydenham s chorea -Antiphospholipid antibody syndrome -Huntington s disease/ HD like diseases -Neuroacanthocytosis
12 Chorea 4 main considerations - Age of onset -Type of onset e.g. acute/subacute/ or chronic and worsening - Family history/drug history - Distribution of chorea/other clinical features
13 Tics Brief, repetitive and stereotyped movements or vocalisations. Tics are usually suppressible for a short period of time, but at the expense of mounting inner tension. Very common: 3-4% of the population are affected at some time in their lives, almost always starting in childhood.
14 Tics Motor: - eye blinking - head jerks - arm/leg jerks -complex sequence Vocal: - sniffing - grunting - snorting
15 Gilles de la Tourette Syndrome Typically, onset of persistent multiple motor and vocal tics, often with associated psychiatric disturbance [Attention deficit hyperactivity syndrome (ADHD); Obsessive compulsive disorder (OCD); copropraxia; coprolalia]
16 Myoclonus Definition: Brief shock-like jerks. Many causes -Physiological, -Fragment of epilepsy -Metabolic encephalopathies/ Hypoxia - Progressive myoclonic ataxia/epilepsy -SSPE/CJD/other encephalitides
17 Dystonia Involuntary muscle spasms leading to abnormal posturing of limbs and writhing movements (athetosis). Primary dystonia: without any structural damage often inherited Secondary dystonia: Due to variety of environmental or heredodegenerative causes with structural damage to the CNS Paroxysmal dystonia: brief episodes of dystonia/dyskinesia
18 Primary dystonia: Two main phenotypes depending on age of onset Young onset: (below 28 yrs) lower limb onset, spreads, tends to generalise; cranial-cervical less affected/spared often familial: DYT1 gene +ve Adult onset: affects upper body; focal or segmental; cranio-cervical most common (F>M) mostly sporadic Non-DYT-1 Prevalence: 8, 33, 58*, and even 732**/ 100,000 Prevalence: 3/100,000
19 Dystonia genes Name Gene Mode of Inheritance Clinical Features DYT 1* TOR1A AD Young-onset primary generalized dystonia DYT 2 n.k. AR Recessive young-onset primary dystonia DYT 3 TAF1 XR Dystonia-parkinsonism in Filipino males, Lubag DYT4 n.k. AD Laryngeal dystonia (whispering dysphonia) +/- limb dystonia in a single Australian family DYT 5 (DRD) GTPCH1 AD Young onset dopa-responsive dystonia/parkinsonism DYT 6* THAP1 AD Youngish onset of primary craniocervical and limb dystonia DYT 7 Linkage to 18p AD Single (?) German family with primary craniocervical dystonia DYT 8 (PNKD) MR-1 AD Paroxysmal non-kinesigenic dystonia and chorea precipitated by coffee, alcohol and fatigue (PNKD) DYT 9 Linkage to 1p AD Paroxysmal chorea and ataxia with progressive interictal spasticity DYT 10 (PKD) Linkage to chr. 16 AD Paroxysmal kinesigenic chorea and dystonia precipitated by sudden movement (PKD) DYT 11 Epsilon sarcoglycan gene AD Myoclonus and dystonia DYT 12 ATP1A3 AD Rapid onset of dystonia-parkinsonism following infection/exercise DYT 13 Linkage to 1p36 AD Single Italian family with primary cranio-cervical dystonia DYT 14 Linkage to 14q n.k. Dopa-responsive dystonia parkinsonism DYT15 Linkage to 18p AD Myoclonus and dystonia DYT16 PRKRA AR Young-onset torsion dystonia, parkinsonism in some
20 Other simple facts and points in a movement disorder patient Hemidystonia/Hemichorea always rule out contralateral structural cause (basal ganglia lesion etc) Remember to exclude treatable causes
21 Dopa Responsive dystonia An inherited condition characterised by early onset dystonia and parkinsonism. Responds very well to small doses of levodopa, and response lasts for life. Many people with DRD are misdiagnosed as having other conditions e.g cerebral palsy. Therefore, levodopa should be considered in all patients with dystonia, particularly those with young onset.
22 Wilson s Disease An autosomal recessive defect of copper metabolism. Causes a variety of movement and psychiatric problems e.g. chorea, dystonia, cerebellar syndromes and parkinsonism. Kayser-Fleischer rings are seen, and tests reveal low ceruloplasmin and high plasma and urinary copper. Treatable with copper chelating agents such as D- penicillamine.
23 Test cases Level 1: Phenomenology- What is the main category of movement disorder? Level 2: Distribution of movement disorder, associated signs or features including history (age etc.) to help consider etiology Level 3: Investigations keeping in mind history and signs to arrive at diagnosis
24 Clues Suggesting Symptomatic Dystonia: Unusual pattern for age of onset Rapid progression or early bulbar/ pronounced oromandibular involvement Fixed rather than mobile spasms Hemidystonia Intellectual impairment or seizures Sensorineural Deafness Parkinsonism Abnormalities of eye movements, optic atrophy, RP, loss of postural reflexes, Pyramidal signs
25
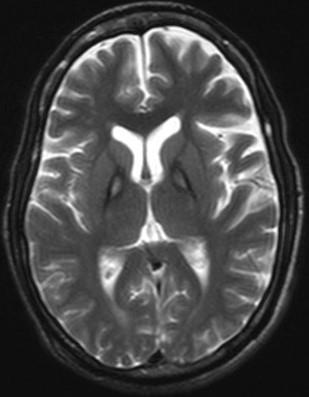
26 Imaging clues Common causes of bilateral holes in the basal ganglia on MRI: Wilson s disease Leigh s syndrome/ mitochondrial disorders Post anoxic/ toxins/ acidosis Infantile striatal necrosis Hemolytic-uremic syndrome Hemidystonia: contralateral basal ganglia lesion
27 Other Findings on Imaging Basal ganglia calcification -Hypoparathyroidism -Fahr s disease -Mitochondrial disease Brain Iron accumulation disorders Caudate atrophy -neuroacanthocytosis -Huntington s disease, HDL2 Cerebral atrophy (variety of degenerative causes)
28 Experience and knowledge Recognise rare conditions or syndromes causing movement disorders
Professor Tim Anderson
 Professor Tim Anderson Neurologist University of Otago Christchurch 11:00-11:55 WS #91: Shakes Jerks and Spasms - Recognition and Differential Diagnosis 12:05-13:00 WS #102: Shakes Jerks and Spasms - Recognition
Professor Tim Anderson Neurologist University of Otago Christchurch 11:00-11:55 WS #91: Shakes Jerks and Spasms - Recognition and Differential Diagnosis 12:05-13:00 WS #102: Shakes Jerks and Spasms - Recognition
Professor Tim Anderson
 Professor Tim Anderson Neurologist University of Otago Christchurch 11:00-11:55 WS #91: Shakes Jerks and Spasms - Recognition and Differential Diagnosis 12:05-13:00 WS #102: Shakes Jerks and Spasms - Recognition
Professor Tim Anderson Neurologist University of Otago Christchurch 11:00-11:55 WS #91: Shakes Jerks and Spasms - Recognition and Differential Diagnosis 12:05-13:00 WS #102: Shakes Jerks and Spasms - Recognition
Movement disorders in childhood: assessment and diagnosis. Lucinda Carr
 Movement disorders in childhood: assessment and diagnosis Lucinda Carr Movement disorders in childhood: Assessment Classification Causes Diagnosis Presentation of movement disorders in childhood: Concerns
Movement disorders in childhood: assessment and diagnosis Lucinda Carr Movement disorders in childhood: Assessment Classification Causes Diagnosis Presentation of movement disorders in childhood: Concerns
Involuntary Movements in Children and Adolescents: Is it Seizure, Tic or Something Else?
 Involuntary Movements in Children and Adolescents: Is it Seizure, Tic or Something Else? California Association of Nurse Practitioners Monterey, March 22, 2013 Julie Sprague-McRae, MS, RN, PPCNP-BC Ruth
Involuntary Movements in Children and Adolescents: Is it Seizure, Tic or Something Else? California Association of Nurse Practitioners Monterey, March 22, 2013 Julie Sprague-McRae, MS, RN, PPCNP-BC Ruth
Diagnosis and treatment of dystonia
 Diagnosis and treatment of dystonia Professor Tom Warner, Reta Lila Weston Institute of Neurological Studies UCL Institute of Neurology National Hospital for Neurology and Neurosurgery Queen Square What
Diagnosis and treatment of dystonia Professor Tom Warner, Reta Lila Weston Institute of Neurological Studies UCL Institute of Neurology National Hospital for Neurology and Neurosurgery Queen Square What
Disorders of Movement M A R T I N H A R L E Y N E U R O L O G Y
 Disorders of Movement M A R T I N H A R L E Y N E U R O L O G Y Educational Objectives Improved history taking in patients with movement disorders. Develop a systematic approach to observing and describing
Disorders of Movement M A R T I N H A R L E Y N E U R O L O G Y Educational Objectives Improved history taking in patients with movement disorders. Develop a systematic approach to observing and describing
Diagnosis and treatment of dystonia
 Diagnosis and treatment of dystonia Professor Tom Warner, Reta Lila Weston Institute of Neurological Studies UCL Institute of Neurology National Hospital for Neurology and Neurosurgery Queen Square What
Diagnosis and treatment of dystonia Professor Tom Warner, Reta Lila Weston Institute of Neurological Studies UCL Institute of Neurology National Hospital for Neurology and Neurosurgery Queen Square What
Movement disorders. Dr Rick Leventer Royal Children s Hospital
 Movement disorders Dr Rick Leventer Royal Children s Hospital richard.leventer@rch.org.au Movement disorders! conditions that affect the speed, fluency, quality, and ease of movement! usually affect TONE
Movement disorders Dr Rick Leventer Royal Children s Hospital richard.leventer@rch.org.au Movement disorders! conditions that affect the speed, fluency, quality, and ease of movement! usually affect TONE
Shake It Off: Recognizing & Treating Movement Disorders
 Ooi Phaik Yee Annual scientific meeting College of Medicine, Academy of Medicine of Malaysia 12 th November 2017 Shake It Off: Recognizing & Treating Movement Disorders MOVEMENT DISORDER A group of symptoms
Ooi Phaik Yee Annual scientific meeting College of Medicine, Academy of Medicine of Malaysia 12 th November 2017 Shake It Off: Recognizing & Treating Movement Disorders MOVEMENT DISORDER A group of symptoms
Department of Neurology, Rigshospitalet, 9 Blegdamsvej, PAULSON, O.B. Involuntary Movements. Tohoku J. Exp. Med., 1990, 161,
 Tohoku J. Exp. Med., 1990, 161, Suppl., 21-27 Involuntary Movements OLAF B. PAULSON Department of Neurology, Rigshospitalet, 9 Blegdamsvej, DK-2100, Copenhagen, Denmark PAULSON, O.B. Involuntary Movements.
Tohoku J. Exp. Med., 1990, 161, Suppl., 21-27 Involuntary Movements OLAF B. PAULSON Department of Neurology, Rigshospitalet, 9 Blegdamsvej, DK-2100, Copenhagen, Denmark PAULSON, O.B. Involuntary Movements.
Movement Disorders Will Garrett, M.D Assistant Professor of Neurology
 Movement Disorders Will Garrett, M.D Assistant Professor of Neurology I. The Basal Ganglia The basal ganglia are composed of several structures including the caudate and putamen (collectively called the
Movement Disorders Will Garrett, M.D Assistant Professor of Neurology I. The Basal Ganglia The basal ganglia are composed of several structures including the caudate and putamen (collectively called the
Dystonia: Title. A real pain in the neck. in All the Wrong Places
 Focus on CME at the University of Western Ontario Dystonia: Title in All the Wrong Places A real pain in the neck By Mandar Jog, MD, FRCPC and; Mary Jenkins, MD, FRCPC What is dystonia? Dystonia is a neurologic
Focus on CME at the University of Western Ontario Dystonia: Title in All the Wrong Places A real pain in the neck By Mandar Jog, MD, FRCPC and; Mary Jenkins, MD, FRCPC What is dystonia? Dystonia is a neurologic
Table of Contents. Preface... xi. Part I: Introduction to Movement Disorders
 Table of Contents Visit www.healthreferenceseries.com to view A Contents Guide to the Health Reference Series, a listing of more than 14,000 topics and the volumes in which they are covered. Preface...
Table of Contents Visit www.healthreferenceseries.com to view A Contents Guide to the Health Reference Series, a listing of more than 14,000 topics and the volumes in which they are covered. Preface...
Dr Barry Snow. Neurologist Auckland District Health Board
 Dr Barry Snow Neurologist Auckland District Health Board Dystonia and Parkinson s disease Barry Snow Gowers 1888: Tetanoid chorea Dystonia a movement disorder characterized by sustained or intermittent
Dr Barry Snow Neurologist Auckland District Health Board Dystonia and Parkinson s disease Barry Snow Gowers 1888: Tetanoid chorea Dystonia a movement disorder characterized by sustained or intermittent
The motor regulator. 1) Basal ganglia/nucleus
 Basal ganglia/nucleus") The motor regulator 1) Basal ganglia/nucleus Neural structures involved in the control of movement Basal Ganglia - Components of the basal ganglia - Function of the basal ganglia - Connection and circuits
The motor regulator 1) Basal ganglia/nucleus Neural structures involved in the control of movement Basal Ganglia - Components of the basal ganglia - Function of the basal ganglia - Connection and circuits
Childhood Movement Disorders Alessandro Capuano, MD, PhD Federica Graziola, MD
 Childhood Movement Disorders Alessandro Capuano, MD, PhD Federica Graziola, MD Movement Disorders Center Department of Neuroscience Bambino Gesù Pediatric Hospital, Rome Two categories: Approach to diagnosis
Childhood Movement Disorders Alessandro Capuano, MD, PhD Federica Graziola, MD Movement Disorders Center Department of Neuroscience Bambino Gesù Pediatric Hospital, Rome Two categories: Approach to diagnosis
GENETICS AND TREATMENT OF DYSTONIA
 GENETICS AND TREATMENT OF DYSTONIA Oksana Suchowersky, M.D., FRCPC, FCCMG Professor of Medicine, Medical Genetics, and Psychiatry Toupin Research Chair in Neurology DYSTONIA Definition: abnormal sustained
GENETICS AND TREATMENT OF DYSTONIA Oksana Suchowersky, M.D., FRCPC, FCCMG Professor of Medicine, Medical Genetics, and Psychiatry Toupin Research Chair in Neurology DYSTONIA Definition: abnormal sustained
Differential Diagnosis of Hypokinetic Movement Disorders
 Differential Diagnosis of Hypokinetic Movement Disorders Dr Donald Grosset Consultant Neurologist - Honorary Professor Institute of Neurological Sciences - Glasgow University Hypokinetic Parkinson's Disease
Differential Diagnosis of Hypokinetic Movement Disorders Dr Donald Grosset Consultant Neurologist - Honorary Professor Institute of Neurological Sciences - Glasgow University Hypokinetic Parkinson's Disease
An Approach to Patients with Movement Disorders
 An Approach to Patients with Movement Disorders Joaquim Ferreira, MD, PhD Laboratory of Clinical Pharmacology and Therapeutics Faculty of Medicine University of Lisbon EDUCATIONAL TOOLS MDS video library
An Approach to Patients with Movement Disorders Joaquim Ferreira, MD, PhD Laboratory of Clinical Pharmacology and Therapeutics Faculty of Medicine University of Lisbon EDUCATIONAL TOOLS MDS video library
Disclosures 2/13/2015. Case: Case (cont)
") Disclosures Recent Advances in Neurology Case Presentation Educational grant support: Medtronic Inc., Merz, Inc., Allergan, Inc. Clinical trial support: Ceregene Inc., MRI Interventions Inc., St. Jude
Disclosures Recent Advances in Neurology Case Presentation Educational grant support: Medtronic Inc., Merz, Inc., Allergan, Inc. Clinical trial support: Ceregene Inc., MRI Interventions Inc., St. Jude
STAFF DEVELOPMENT in SPECIAL EDUCATION
 STAFF DEVELOPMENT in SPECIAL EDUCATION Tourette Syndrome AASEP s Staff Development Course TOURETTE SYNDROME Copyright AASEP (2006) 1 of 6 Course Objectives To provide a definition of Tourette syndrome
STAFF DEVELOPMENT in SPECIAL EDUCATION Tourette Syndrome AASEP s Staff Development Course TOURETTE SYNDROME Copyright AASEP (2006) 1 of 6 Course Objectives To provide a definition of Tourette syndrome
Genetics of parkinsonian and dystonic syndromes
 Genetics of parkinsonian and dystonic syndromes Enza Maria Valente CSS-Mendel Institute, Rome University of Salerno Genetic forms of Parkinson disease 2 polymorphisms (++ in autosomal dominant PD genes:
Genetics of parkinsonian and dystonic syndromes Enza Maria Valente CSS-Mendel Institute, Rome University of Salerno Genetic forms of Parkinson disease 2 polymorphisms (++ in autosomal dominant PD genes:
2/18/ yo man with history of mild developmental delay and chorea of unclear etiology, with new complaints of speech difficulty
 18 yo man with history of mild developmental delay and chorea of unclear etiology, with new complaints of speech difficulty Audrey Foster-Barber UCSF Child Neurology February 18, 2011 Several years of
18 yo man with history of mild developmental delay and chorea of unclear etiology, with new complaints of speech difficulty Audrey Foster-Barber UCSF Child Neurology February 18, 2011 Several years of
STEADY YOUR APPROACH TO TREMOR (OVERVIEW OF DIFFERENTIAL DIAGNOSIS)
") STEADY YOUR APPROACH TO TREMOR (OVERVIEW OF DIFFERENTIAL DIAGNOSIS) Karen M. Thomas D.O. Diplomate, ABPN Director of Movement Disorders Program Director of Comprehensive Parkinson s Disease Program Sentara
STEADY YOUR APPROACH TO TREMOR (OVERVIEW OF DIFFERENTIAL DIAGNOSIS) Karen M. Thomas D.O. Diplomate, ABPN Director of Movement Disorders Program Director of Comprehensive Parkinson s Disease Program Sentara
Phenomenology of Movement Disorders
 Phenomenology of Movement Disorders Raja Mehanna MD Anatomical reasoning Anatomical reasoning Phenomenological reasoning Abnormal movement Hypokinetic Hyperkinetic Ataxia Video 1 But there is a tremor!
Phenomenology of Movement Disorders Raja Mehanna MD Anatomical reasoning Anatomical reasoning Phenomenological reasoning Abnormal movement Hypokinetic Hyperkinetic Ataxia Video 1 But there is a tremor!
DIFFERENTIAL DIAGNOSIS SARAH MARRINAN
 Parkinson s Academy Registrar Masterclass Sheffield DIFFERENTIAL DIAGNOSIS SARAH MARRINAN 17 th September 2014 Objectives Importance of age in diagnosis Diagnostic challenges Brain Bank criteria Differential
Parkinson s Academy Registrar Masterclass Sheffield DIFFERENTIAL DIAGNOSIS SARAH MARRINAN 17 th September 2014 Objectives Importance of age in diagnosis Diagnostic challenges Brain Bank criteria Differential
Moving fast or moving slow: an overview of Movement Disorders
 Moving fast or moving slow: an overview of Movement Disorders Mini Medical School October 25, 2018 Heather Rigby, MD, FRCPC 2014 MFMER slide-1 2014 MFMER slide-2 Basal Ganglia Dysfunction - Movement Disorders
Moving fast or moving slow: an overview of Movement Disorders Mini Medical School October 25, 2018 Heather Rigby, MD, FRCPC 2014 MFMER slide-1 2014 MFMER slide-2 Basal Ganglia Dysfunction - Movement Disorders
CHOREA AND DYSTONIA. Joohi Jimenez-Shahed, MD Baylor College of Medicine Houston, TX
 CHOREA AND DYSTONIA Joohi Jimenez-Shahed, MD Baylor College of Medicine Houston, TX INTRODUCTION The key to successful differential diagnosis and treatment of patients with movement disorders is successful
CHOREA AND DYSTONIA Joohi Jimenez-Shahed, MD Baylor College of Medicine Houston, TX INTRODUCTION The key to successful differential diagnosis and treatment of patients with movement disorders is successful
The Pathogenesis of Dystonia: Past, Present and Future
 The Pathogenesis of Dystonia: Past, Present and Future NIH Grant Disclosures U54 TR001456, R21 NS096445, R56 NS102980 Private Foundation Disclosures Benign Essential Blepharospasm Research Foundation Cure
The Pathogenesis of Dystonia: Past, Present and Future NIH Grant Disclosures U54 TR001456, R21 NS096445, R56 NS102980 Private Foundation Disclosures Benign Essential Blepharospasm Research Foundation Cure
Parkinson s Disease. Sirilak yimcharoen
 Parkinson s Disease Sirilak yimcharoen EPIDEMIOLOGY ~1% of people over 55 years Age range 35 85 years peak age of onset is in the early 60s ~5% of cases characterized by an earlier age of onset (typically
Parkinson s Disease Sirilak yimcharoen EPIDEMIOLOGY ~1% of people over 55 years Age range 35 85 years peak age of onset is in the early 60s ~5% of cases characterized by an earlier age of onset (typically
Movement Disorders. Eric Kraus, MD! Neurology!
 Movement Disorders Eric Kraus, MD! Neurology! Classify Bradykinesia! Tic! Myoclonus! Tremor! Dystonia! Athetosis! Chorea! Ballismus! Case 1 This 64 year-old female has had progression of a tremor over
Movement Disorders Eric Kraus, MD! Neurology! Classify Bradykinesia! Tic! Myoclonus! Tremor! Dystonia! Athetosis! Chorea! Ballismus! Case 1 This 64 year-old female has had progression of a tremor over
VL VA BASAL GANGLIA. FUNCTIONAl COMPONENTS. Function Component Deficits Start/initiation Basal Ganglia Spontan movements
 BASAL GANGLIA Chris Cohan, Ph.D. Dept. of Pathology/Anat Sci University at Buffalo I) Overview How do Basal Ganglia affect movement Basal ganglia enhance cortical motor activity and facilitate movement.
BASAL GANGLIA Chris Cohan, Ph.D. Dept. of Pathology/Anat Sci University at Buffalo I) Overview How do Basal Ganglia affect movement Basal ganglia enhance cortical motor activity and facilitate movement.
PARKINSON S DISEASE: current aspects of ETIOLOGY, DIAGNOSIS and TREATMENT. Dilek Ince Gunal, MD Assoc. Prof
 PARKINSON S DISEASE: current aspects of ETIOLOGY, DIAGNOSIS and TREATMENT Dilek Ince Gunal, MD Assoc. Prof Definition Clinical symptoms: Pathogenesis: Etiology: Neurodegenerative syndrome with chronic,
PARKINSON S DISEASE: current aspects of ETIOLOGY, DIAGNOSIS and TREATMENT Dilek Ince Gunal, MD Assoc. Prof Definition Clinical symptoms: Pathogenesis: Etiology: Neurodegenerative syndrome with chronic,
UNIVERSITY OF JORDAN FACULTY OF MEDICINE DEPARTMENT OF PHYSIOLOGY & BIOCHEMISTRY NEUROPHYSIOLOGY (MEDICAL) Spring, 2014
 Spring, 2014") UNIVERSITY OF JORDAN FACULTY OF MEDICINE DEPARTMENT OF PHYSIOLOGY & BIOCHEMISTRY NEUROPHYSIOLOGY (MEDICAL) Spring, 2014 Textbook of Medical Physiology by: Guyton & Hall, 11 th edition 2006 Eman Al-Khateeb,
UNIVERSITY OF JORDAN FACULTY OF MEDICINE DEPARTMENT OF PHYSIOLOGY & BIOCHEMISTRY NEUROPHYSIOLOGY (MEDICAL) Spring, 2014 Textbook of Medical Physiology by: Guyton & Hall, 11 th edition 2006 Eman Al-Khateeb,
Source: *Dystonia facts medically edited by: Charles Patrick Davis, MD, PhD
 Source: http://www.medicinenet.com/script/main/art.asp?articlekey=349 Dystonia facts* *Dystonia facts medically edited by: Charles Patrick Davis, MD, PhD Dystonia is a disorder of muscle control; it can
Source: http://www.medicinenet.com/script/main/art.asp?articlekey=349 Dystonia facts* *Dystonia facts medically edited by: Charles Patrick Davis, MD, PhD Dystonia is a disorder of muscle control; it can
Hyperkinetic movement disorders are. Hyperkinetic Movement Disorders. Cases in Movement Disorders. James case. About Tom
 Hyperkinetic Movement Disorders Sarah Furtado, MD, PhD, FRCPC James case A mother brings her son James, 10, to your office because of repetitive sniffing sounds and repetitive eye blinking. This sniffing
Hyperkinetic Movement Disorders Sarah Furtado, MD, PhD, FRCPC James case A mother brings her son James, 10, to your office because of repetitive sniffing sounds and repetitive eye blinking. This sniffing
Hubert H. Fernandez, MD
 Hubert H. Fernandez, MD Associate Professor Co-Director, Movement Disorders Center Director, Clinical Trials for Movement Disorders Program Director, Neurology Residency and Movement Disorders Fellowship
Hubert H. Fernandez, MD Associate Professor Co-Director, Movement Disorders Center Director, Clinical Trials for Movement Disorders Program Director, Neurology Residency and Movement Disorders Fellowship
Parkinson s Disease in the Elderly A Physicians perspective. Dr John Coyle
 Parkinson s Disease in the Elderly A Physicians perspective Dr John Coyle Overview Introduction Epidemiology and aetiology Pathogenesis Diagnosis and clinical features Treatment Psychological issues/ non
Parkinson s Disease in the Elderly A Physicians perspective Dr John Coyle Overview Introduction Epidemiology and aetiology Pathogenesis Diagnosis and clinical features Treatment Psychological issues/ non
Hypokinetic Movement Disorders
 Hypokinetic Movement Disorders Ariane Park, MD, MPH Assistant Professor-Clinical Division of Neurology The Ohio State University Wexner Medical Center Hypokinetic movement disorders Diminished voluntary
Hypokinetic Movement Disorders Ariane Park, MD, MPH Assistant Professor-Clinical Division of Neurology The Ohio State University Wexner Medical Center Hypokinetic movement disorders Diminished voluntary
316 Index. 225, 229, 232, 238, 242, 285, 293, 307, 309 dyskinesias, 54,295 dystonias, 54
 Index ABC recording, 22, 176, 178, 187, 193, 194 acral licking, 133 ADHD, 26, 29, 35, 36,44 58, 59,61, 63, 64, 67, 68, 70, 87-92, 102, 122, 222, 245 anxiety, 2, 7, 26, 30, 36,41,44, 59, 62,63,69,70,85,87,91,102,
Index ABC recording, 22, 176, 178, 187, 193, 194 acral licking, 133 ADHD, 26, 29, 35, 36,44 58, 59,61, 63, 64, 67, 68, 70, 87-92, 102, 122, 222, 245 anxiety, 2, 7, 26, 30, 36,41,44, 59, 62,63,69,70,85,87,91,102,
Presented by Joanna O Leary, MD Providence St. Vincent Medical Center Movement Disorder Department
 Presented by Joanna O Leary, MD Providence St. Vincent Medical Center Movement Disorder Department Hyperkinetic movement disorders Increase in muscle movements causing involuntary motion Tremor Dystonia
Presented by Joanna O Leary, MD Providence St. Vincent Medical Center Movement Disorder Department Hyperkinetic movement disorders Increase in muscle movements causing involuntary motion Tremor Dystonia
SELECTIVE VULNERABILITY (HYPOXIA AND HYPOGLYCEMIA)
") DEFICIENCY OF METABOLITE -HYPOXIA AND HYPOGLYCEMIA -HYPOVITAMINOSIS SELECTIVE VULNERABILITY (HYPOXIA AND HYPOGLYCEMIA) -SPECIFIC CELL TYPE NEURONS>OLIGODENDROCYTES>ASTROCYTES -SPECIFIC BRAIN REGION PYRAMIDAL
DEFICIENCY OF METABOLITE -HYPOXIA AND HYPOGLYCEMIA -HYPOVITAMINOSIS SELECTIVE VULNERABILITY (HYPOXIA AND HYPOGLYCEMIA) -SPECIFIC CELL TYPE NEURONS>OLIGODENDROCYTES>ASTROCYTES -SPECIFIC BRAIN REGION PYRAMIDAL
Identification number: TÁMOP /1/A
 Manifestation of Novel Social Challenges of the European Union in the Teaching Material of Medical Biotechnology Master s Programmes at the University of Pécs and at the University of Debrecen Identification
Manifestation of Novel Social Challenges of the European Union in the Teaching Material of Medical Biotechnology Master s Programmes at the University of Pécs and at the University of Debrecen Identification
Types of involuntary movements
 Tremor Types of involuntary movements Dystonia Chorea Myoclonus Tics Tremor Rhythmic shaking of muscles that produces an oscillating movement Parkinsonian tremor Rest tremor > posture > kinetic Re-emergent
Tremor Types of involuntary movements Dystonia Chorea Myoclonus Tics Tremor Rhythmic shaking of muscles that produces an oscillating movement Parkinsonian tremor Rest tremor > posture > kinetic Re-emergent
EPIDEMIOLOGY AND CLASSIFICATION OF MOVEMENT DISORDERS
 EPIDEMIOLOGY AND CLASSIFICATION OF MOVEMENT DISORDERS Njideka U. Okubadejo Professor & Consultant Neurologist College of Medicine, University of Lagos & Lagos University Teaching Hospital, Lagos State,
EPIDEMIOLOGY AND CLASSIFICATION OF MOVEMENT DISORDERS Njideka U. Okubadejo Professor & Consultant Neurologist College of Medicine, University of Lagos & Lagos University Teaching Hospital, Lagos State,
10/13/2017. Disclosures. Deep Brain Stimulation in the Treatment of Movement Disorders. Deep Brain Stimulation: Objectives.
 Deep Brain Stimulation in the Treatment of Movement Disorders Disclosures None Eleanor K Orehek, M.D. Movement Disorders Specialist Noran Neurological Clinic 1 2 Objectives To provide an overview of deep
Deep Brain Stimulation in the Treatment of Movement Disorders Disclosures None Eleanor K Orehek, M.D. Movement Disorders Specialist Noran Neurological Clinic 1 2 Objectives To provide an overview of deep
Pathogenesis of Degenerative Diseases and Dementias. D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria)
. M. Path (U. of Alexandria)") Pathogenesis of Degenerative Diseases and Dementias D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria) Dementias Defined: as the development of memory impairment and other cognitive deficits
Pathogenesis of Degenerative Diseases and Dementias D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria) Dementias Defined: as the development of memory impairment and other cognitive deficits
CLINICAL MANIFESTATIONS AND CLASSIFICATION OF DYSTONIA
 CLINICAL MANIFESTATIONS AND CLASSIFICATION OF DYSTONIA Daniel Tarsy, MD Beth Israel Deaconess Medical Center Harvard Medical School Boston, MA The term dystonia was coined by Oppenheim in 1911 for a disorder
CLINICAL MANIFESTATIONS AND CLASSIFICATION OF DYSTONIA Daniel Tarsy, MD Beth Israel Deaconess Medical Center Harvard Medical School Boston, MA The term dystonia was coined by Oppenheim in 1911 for a disorder
Parkinson s Disease and other related movement disorders a video guide to diagnosis
 Parkinson s Disease and other related movement disorders a video guide to diagnosis Parkinson s Disease Masterclass November 2017 Dr Frank Phelan MidYorkshire Hospitals NHS Trust Ideopathic Parkinson s
Parkinson s Disease and other related movement disorders a video guide to diagnosis Parkinson s Disease Masterclass November 2017 Dr Frank Phelan MidYorkshire Hospitals NHS Trust Ideopathic Parkinson s
Parkinson s Disease. Prevalence. Mark S. Baron, M.D. Cardinal Features. Clinical Characteristics. Not Just a Movement Disorder
 Prevalence Parkinson s Disease Mark S. Baron, M.D. Associate Professor of Neurology Movement Disorders Section VCU School of Medicine Common disorder Approaching 1% by 65 yrs of age, 2% by 80 yrs of age
Prevalence Parkinson s Disease Mark S. Baron, M.D. Associate Professor of Neurology Movement Disorders Section VCU School of Medicine Common disorder Approaching 1% by 65 yrs of age, 2% by 80 yrs of age
Movement Disorders. Psychology 372 Physiological Psychology. Background. Myasthenia Gravis. Many Types
 Background Movement Disorders Psychology 372 Physiological Psychology Steven E. Meier, Ph.D. Listen to the audio lecture while viewing these slides Early Studies Found some patients with progressive weakness
Background Movement Disorders Psychology 372 Physiological Psychology Steven E. Meier, Ph.D. Listen to the audio lecture while viewing these slides Early Studies Found some patients with progressive weakness
Movement Disorders- Parkinson s Disease. Fahed Saada, MD March 8 th, th Family Medicine Refresher Course St.
 Movement Disorders- Parkinson s Disease Fahed Saada, MD March 8 th, 2019 48 th Family Medicine Refresher Course St. Joseph s Health Disclosure ACADIA Pharmaceuticals Objectives Review the classification
Movement Disorders- Parkinson s Disease Fahed Saada, MD March 8 th, 2019 48 th Family Medicine Refresher Course St. Joseph s Health Disclosure ACADIA Pharmaceuticals Objectives Review the classification
Tourette syndrome What is Tourette syndrome? What are the symptoms? What is the course of TS? Can people with TS control their tics? What causes TS?
 Tourette syndrome What is Tourette syndrome? Tourette syndrome (TS) is a neurological disorder characterized by repetitive, stereotyped, involuntary movements and vocalizations called tics. The disorder
Tourette syndrome What is Tourette syndrome? Tourette syndrome (TS) is a neurological disorder characterized by repetitive, stereotyped, involuntary movements and vocalizations called tics. The disorder
Strick Lecture 4 March 29, 2006 Page 1
 Strick Lecture 4 March 29, 2006 Page 1 Basal Ganglia OUTLINE- I. Structures included in the basal ganglia II. III. IV. Skeleton diagram of Basal Ganglia Loops with cortex Similarity with Cerebellar Loops
Strick Lecture 4 March 29, 2006 Page 1 Basal Ganglia OUTLINE- I. Structures included in the basal ganglia II. III. IV. Skeleton diagram of Basal Ganglia Loops with cortex Similarity with Cerebellar Loops
Neurodegenerative Disease. April 12, Cunningham. Department of Neurosciences
 Neurodegenerative Disease April 12, 2017 Cunningham Department of Neurosciences NEURODEGENERATIVE DISEASE Any of a group of hereditary and sporadic conditions characterized by progressive dysfunction,
Neurodegenerative Disease April 12, 2017 Cunningham Department of Neurosciences NEURODEGENERATIVE DISEASE Any of a group of hereditary and sporadic conditions characterized by progressive dysfunction,
III./3.1. Movement disorders with akinetic rigid symptoms
 III./3.1. Movement disorders with akinetic rigid symptoms III./3.1.1. Parkinson s disease Parkinson s disease (PD) is the second most common neurodegenerative disorder worldwide after Alzheimer s disease.
III./3.1. Movement disorders with akinetic rigid symptoms III./3.1.1. Parkinson s disease Parkinson s disease (PD) is the second most common neurodegenerative disorder worldwide after Alzheimer s disease.
IMPAIRMENT OF THE NERVOUS SYSTEM
 IMPAIRMENT OF THE NERVOUS SYSTEM The following information provides criteria for the evaluation of permanent impairment resulting from dysfunction brain, spinal cord and cranial nerves and certain peripheral
IMPAIRMENT OF THE NERVOUS SYSTEM The following information provides criteria for the evaluation of permanent impairment resulting from dysfunction brain, spinal cord and cranial nerves and certain peripheral
Khoo Teik Beng Paediatric Institute Hospital Kuala Lumpur
 PAROXYSMAL NON-EPILEPTIC EVENTS Khoo Teik Beng Paediatric Institute Hospital Kuala Lumpur Epileptic seizures Transient clinical events that result from the abnormal, excessive activity of a set of cerebral
PAROXYSMAL NON-EPILEPTIC EVENTS Khoo Teik Beng Paediatric Institute Hospital Kuala Lumpur Epileptic seizures Transient clinical events that result from the abnormal, excessive activity of a set of cerebral
Hyperkinetic movement disorders: shakes, jumps and jolts
 THE BARE ESSENTIALS Hyperkinetic movement disorders: shakes, jumps and jolts Geraint Fuller Correspondence to G Fuller, Consultant Neurologist, Gloucester Royal Hospital, Great Western Road, Gloucester
THE BARE ESSENTIALS Hyperkinetic movement disorders: shakes, jumps and jolts Geraint Fuller Correspondence to G Fuller, Consultant Neurologist, Gloucester Royal Hospital, Great Western Road, Gloucester
DISORDERS OF THE MOTOR SYSTEM. Jeanette J. Norden, Ph.D. Professor Emerita Vanderbilt University School of Medicine
 DISORDERS OF THE MOTOR SYSTEM Jeanette J. Norden, Ph.D. Professor Emerita Vanderbilt University School of Medicine THE MOTOR SYSTEM To understand disorders of the motor system, we need to review how a
DISORDERS OF THE MOTOR SYSTEM Jeanette J. Norden, Ph.D. Professor Emerita Vanderbilt University School of Medicine THE MOTOR SYSTEM To understand disorders of the motor system, we need to review how a
UvA-DARE (Digital Academic Repository) Genetic architecture of dystonia Groen, Justus. Link to publication
 Genetic architecture of dystonia Groen, Justus. Link to publication") UvA-DARE (Digital Academic Repository) Genetic architecture of dystonia Groen, Justus Link to publication Citation for published version (APA): Groen, J. L. (2014). Genetic architecture of dystonia General
UvA-DARE (Digital Academic Repository) Genetic architecture of dystonia Groen, Justus Link to publication Citation for published version (APA): Groen, J. L. (2014). Genetic architecture of dystonia General
DOWNLOAD OR READ : ON CHOREA AND OTHER ALLIED MOVEMENT DISORDERS OF EARLY LIFE PDF EBOOK EPUB MOBI
 DOWNLOAD OR READ : ON CHOREA AND OTHER ALLIED MOVEMENT DISORDERS OF EARLY LIFE PDF EBOOK EPUB MOBI Page 1 Page 2 on chorea and other allied movement disorders of early life on chorea and other pdf on chorea
DOWNLOAD OR READ : ON CHOREA AND OTHER ALLIED MOVEMENT DISORDERS OF EARLY LIFE PDF EBOOK EPUB MOBI Page 1 Page 2 on chorea and other allied movement disorders of early life on chorea and other pdf on chorea
THIAMINE TRANSPORTER TYPE 2 DEFICIENCY
 THIAMINE TRANSPORTER TYPE 2 DEFICIENCY WHAT IS THE THIAMINE TRANSPORTER TYPE 2 DEFICIENCY (hthtr2)? The thiamine transporter type 2 deficiency (hthtr2) is a inborn error of thiamine metabolism caused by
THIAMINE TRANSPORTER TYPE 2 DEFICIENCY WHAT IS THE THIAMINE TRANSPORTER TYPE 2 DEFICIENCY (hthtr2)? The thiamine transporter type 2 deficiency (hthtr2) is a inborn error of thiamine metabolism caused by
Evolution of a concept: Apraxia/higher level gait disorder. ataxia v. apraxia gait = limb apraxia. low, middle, high gait disturbance levels
 Case #1 81-year-old woman Gait Imbalance: Two Unusual Cases in Older Patients February 2008: 3 years of gradually progressive gait imbalance no vertigo, dizziness or paresthesias etiology unclear on examination
Case #1 81-year-old woman Gait Imbalance: Two Unusual Cases in Older Patients February 2008: 3 years of gradually progressive gait imbalance no vertigo, dizziness or paresthesias etiology unclear on examination
Clinical aspects of pterin disorders
 Clinical aspects of pterin disorders Thomas Opladen, MD University Children s Hospital Department of Inborn Errors of Metabolism Heidelberg Germany Introductory words Brain function depends on the capacity
Clinical aspects of pterin disorders Thomas Opladen, MD University Children s Hospital Department of Inborn Errors of Metabolism Heidelberg Germany Introductory words Brain function depends on the capacity
of common terms Amplitude Resting Position Essential Tremor (ET) Glossary
 Glossary") Essential Tremor (ET) Glossary of common terms Because knowledge is essential to making informed choices, we ve developed this glossary to help ET patients, their loved ones, and caregivers better understand
Essential Tremor (ET) Glossary of common terms Because knowledge is essential to making informed choices, we ve developed this glossary to help ET patients, their loved ones, and caregivers better understand
Update on Parkinson s disease and other Movement Disorders October 2018
 Update on Parkinson s disease and other Movement Disorders October 2018 DR. JONATHAN EVANS CONSULTANT IN NEUROLOGY QUEEN S MEDICAL CENTRE NOTTINGHAM Disclosures: Honoraria UCB, Britannia, Allergan, AbbVie
Update on Parkinson s disease and other Movement Disorders October 2018 DR. JONATHAN EVANS CONSULTANT IN NEUROLOGY QUEEN S MEDICAL CENTRE NOTTINGHAM Disclosures: Honoraria UCB, Britannia, Allergan, AbbVie
National Consensus Statement for Diagnosis and Treatment of Hyperkinetic Motor Disorders
 National Consensus Statement for Diagnosis and Treatment of Hyperkinetic Motor Disorders Edited by Acad. Prof. Dr. Ivan Milanov, MD; Assoc. Prof. Dr. Dimitar Georgiev, MD; Dr. Vesselina Grozeva, MD and
National Consensus Statement for Diagnosis and Treatment of Hyperkinetic Motor Disorders Edited by Acad. Prof. Dr. Ivan Milanov, MD; Assoc. Prof. Dr. Dimitar Georgiev, MD; Dr. Vesselina Grozeva, MD and
Disorders of gait and balance
 Disorders of gait and balance clinical assessment and classification Evžen Růžička Charles University in Prague 1st Medical Faculty and General University Hospital handout additional videos and photos
Disorders of gait and balance clinical assessment and classification Evžen Růžička Charles University in Prague 1st Medical Faculty and General University Hospital handout additional videos and photos
Choreas and paroxysmal disorders. Bedside examination. Chorea
 Focus on: Characteristic of the disorders (clues) Phenomenology -> syndrome Etiologies (diagnostic approach (clues/ tests) Treatment (s) Choreas and paroxysmal disorders Pr. Marie Vidailhet Department
Focus on: Characteristic of the disorders (clues) Phenomenology -> syndrome Etiologies (diagnostic approach (clues/ tests) Treatment (s) Choreas and paroxysmal disorders Pr. Marie Vidailhet Department
DEEP BRAIN STIMULATION
 DEEP BRAIN STIMULATION Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures, medical devices and drugs
DEEP BRAIN STIMULATION Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures, medical devices and drugs
Genetic disorders of the central nervous system have a propensity to cause movement disorders
 ii22 * GENETICS OF MOVEMENT DISORDERS AND ATAXIA See end of article for authors affiliations c HUNTINGTON S Correspondence to: Dr Paul R Jarman, National Hospital for Neurology and Neurosurgery, Queen
ii22 * GENETICS OF MOVEMENT DISORDERS AND ATAXIA See end of article for authors affiliations c HUNTINGTON S Correspondence to: Dr Paul R Jarman, National Hospital for Neurology and Neurosurgery, Queen
MUSCULOSKELETAL AND NEUROLOGICAL DISORDERS
 MUSCULOSKELETAL AND NEUROLOGICAL DISORDERS There are a wide variety of Neurologic and Musculoskeletal disorders which can impact driving safety. Impairment may be the result of altered muscular, skeletal,
MUSCULOSKELETAL AND NEUROLOGICAL DISORDERS There are a wide variety of Neurologic and Musculoskeletal disorders which can impact driving safety. Impairment may be the result of altered muscular, skeletal,
Understanding and treating gait abnormality in Dravet syndrome
 Understanding and treating gait abnormality in Dravet syndrome Anne Stratton, MD, FAAP, FAAPMR Biennial Dravet Syndrome Foundation Family and Professional Conference July 19-22, 2018 Disclosures I have
Understanding and treating gait abnormality in Dravet syndrome Anne Stratton, MD, FAAP, FAAPMR Biennial Dravet Syndrome Foundation Family and Professional Conference July 19-22, 2018 Disclosures I have
Functional Distinctions
 Functional Distinctions FUNCTION COMPONENT DEFICITS Start Basal Ganglia Spontaneous Movements Move UMN/LMN Cerebral Cortex Brainstem, Spinal cord Roots/peripheral nerves Plan Cerebellum Ataxia Adjust Cerebellum
Functional Distinctions FUNCTION COMPONENT DEFICITS Start Basal Ganglia Spontaneous Movements Move UMN/LMN Cerebral Cortex Brainstem, Spinal cord Roots/peripheral nerves Plan Cerebellum Ataxia Adjust Cerebellum
Huntington s Disease COGS 172
 Huntington s Disease COGS 172 Overview Part I: What is HD? - Clinical description and features - Genetic basis and neuropathology - Cell biology, mouse models and therapeutics Part II: HD as a model in
Huntington s Disease COGS 172 Overview Part I: What is HD? - Clinical description and features - Genetic basis and neuropathology - Cell biology, mouse models and therapeutics Part II: HD as a model in
Dysarthria and Dysphagia: a Neurology Perspective William Meador, MD Assistant Professor of Neurology, UAB
 Dysarthria and Dysphagia: a Neurology Perspective William Meador, MD Assistant Professor of Neurology, UAB 2.11.16 Disclosures I have no relevant conflicts or potential conflicts to disclose regarding
Dysarthria and Dysphagia: a Neurology Perspective William Meador, MD Assistant Professor of Neurology, UAB 2.11.16 Disclosures I have no relevant conflicts or potential conflicts to disclose regarding
Deep Brain Stimulation for Parkinson s Disease & Essential Tremor
 Deep Brain Stimulation for Parkinson s Disease & Essential Tremor Albert Fenoy, MD Assistant Professor University of Texas at Houston, Health Science Center Current US Approvals Essential Tremor and Parkinsonian
Deep Brain Stimulation for Parkinson s Disease & Essential Tremor Albert Fenoy, MD Assistant Professor University of Texas at Houston, Health Science Center Current US Approvals Essential Tremor and Parkinsonian
Semivoluntary movement (=unvoluntary)
") EXTRAPYRAMIDAL DISORDERS = Movement disorders = Degenerative disease 1 4 types of movements: Voluntary movement Semivoluntary movement (=unvoluntary) Involuntary movement Automatic movement 2 3 Movement
EXTRAPYRAMIDAL DISORDERS = Movement disorders = Degenerative disease 1 4 types of movements: Voluntary movement Semivoluntary movement (=unvoluntary) Involuntary movement Automatic movement 2 3 Movement
Diagnosing Epilepsy in Children and Adolescents
 2019 Annual Epilepsy Pediatric Patient Care Conference Diagnosing Epilepsy in Children and Adolescents Korwyn Williams, MD, PhD Staff Epileptologist, BNI at PCH Clinical Assistant Professor, Department
2019 Annual Epilepsy Pediatric Patient Care Conference Diagnosing Epilepsy in Children and Adolescents Korwyn Williams, MD, PhD Staff Epileptologist, BNI at PCH Clinical Assistant Professor, Department
Wilson Disease. Maggie Benson Virginia Commonwealth University Department of Physical Therapy
 Wilson Disease Maggie Benson Virginia Commonwealth University Department of Physical Therapy What is Wilson Disease? Wilson Disease (WD)= hepatolenticular degeneration Hereditary disorder Autosomal recessive
Wilson Disease Maggie Benson Virginia Commonwealth University Department of Physical Therapy What is Wilson Disease? Wilson Disease (WD)= hepatolenticular degeneration Hereditary disorder Autosomal recessive
Tremor. Mario Zappia. Università degli Studi di Catania
 Tremor Mario Zappia Università degli Studi di Catania Tremor: Definition Rhythmical, Involuntary, Oscillatory movement of a body part Classification of Dyskinesias Based on Rhythmicity Rhythmical Dyskinesias:
Tremor Mario Zappia Università degli Studi di Catania Tremor: Definition Rhythmical, Involuntary, Oscillatory movement of a body part Classification of Dyskinesias Based on Rhythmicity Rhythmical Dyskinesias:
Prescribing issues in spasticity and dystonia. Professor Rajat Gupta Consultant Paediatric Neurologist Birmingham Children s Hospital
 Prescribing issues in spasticity and dystonia Professor Rajat Gupta Consultant Paediatric Neurologist Birmingham Children s Hospital Cerebral palsy is common, affecting about 2-3 per 1000 children Surveillance
Prescribing issues in spasticity and dystonia Professor Rajat Gupta Consultant Paediatric Neurologist Birmingham Children s Hospital Cerebral palsy is common, affecting about 2-3 per 1000 children Surveillance
Basal Ganglia. Today s lecture is about Basal Ganglia and it covers:
 Basal Ganglia Motor system is complex interaction between Lower motor neurons (spinal cord and brainstem circuits) and Upper motor neurons (pyramidal and extrapyramidal tracts) plus two main regulators
Basal Ganglia Motor system is complex interaction between Lower motor neurons (spinal cord and brainstem circuits) and Upper motor neurons (pyramidal and extrapyramidal tracts) plus two main regulators
Part 1 Parkinson s Disease. COGS 172: Brain Disorders and Cogni5on
 Part 1 Parkinson s Disease COGS 172: Brain Disorders and Cogni5on Background: Neuroanatomy of the motor system Note: Given short time to the final the details of the anatomy will not be in the exam, but
Part 1 Parkinson s Disease COGS 172: Brain Disorders and Cogni5on Background: Neuroanatomy of the motor system Note: Given short time to the final the details of the anatomy will not be in the exam, but
Basal ganglia Sujata Sofat, class of 2009
 Basal ganglia Sujata Sofat, class of 2009 Basal ganglia Objectives Describe the function of the Basal Ganglia in movement Define the BG components and their locations Describe the motor loop of the BG
Basal ganglia Sujata Sofat, class of 2009 Basal ganglia Objectives Describe the function of the Basal Ganglia in movement Define the BG components and their locations Describe the motor loop of the BG
Understanding Dystonia
 Understanding Dystonia Sand Sharks Anthony Richardsen, Lindsey Rathbun, Evan Harrington, Chris Erzen The Essentials What, Why, How What is Dystonia? Dystonias are movement disorders often characterized
Understanding Dystonia Sand Sharks Anthony Richardsen, Lindsey Rathbun, Evan Harrington, Chris Erzen The Essentials What, Why, How What is Dystonia? Dystonias are movement disorders often characterized
Familial dystonia with cerebral calcification
 Familial dystonia with cerebral calcification case report and genetic update M. Signaevski, A.K. Wszolek, A.J. Stoessel, R. Rademakers, and I.R. Mackenzie Vancouver General Hospital, BC, Canada Mayo Clinic
Familial dystonia with cerebral calcification case report and genetic update M. Signaevski, A.K. Wszolek, A.J. Stoessel, R. Rademakers, and I.R. Mackenzie Vancouver General Hospital, BC, Canada Mayo Clinic
Movement Disorders: A Brief Overview
 Movement Disorders: A Brief Overview Albert Hung, MD, PhD Massachusetts General Hospital Harvard Medical School August 17, 2006 Cardinal Features of Parkinsonism Tremor Rigidity Bradykinesia Postural imbalance
Movement Disorders: A Brief Overview Albert Hung, MD, PhD Massachusetts General Hospital Harvard Medical School August 17, 2006 Cardinal Features of Parkinsonism Tremor Rigidity Bradykinesia Postural imbalance
Parkinson Disease. Lorraine Kalia, MD, PhD, FRCPC. Presented by: Ontario s Geriatric Steering Committee
 Parkinson Disease Lorraine Kalia, MD, PhD, FRCPC Key Learnings Parkinson Disease (L. Kalia) Key Learnings Parkinson disease is the most common but not the only cause of parkinsonism Parkinson disease is
Parkinson Disease Lorraine Kalia, MD, PhD, FRCPC Key Learnings Parkinson Disease (L. Kalia) Key Learnings Parkinson disease is the most common but not the only cause of parkinsonism Parkinson disease is
Dystonias. How are the dystonias classified? One way of classifying the dystonias is according to the parts of the body they affect:
 Dystonias What are the dystonias? The dystonias are movement disorders in which sustained muscle contractions cause twisting and repetitive movements or abnormal postures. The movements, which are involuntary
Dystonias What are the dystonias? The dystonias are movement disorders in which sustained muscle contractions cause twisting and repetitive movements or abnormal postures. The movements, which are involuntary
Patient selection for surgery: Hyperkinetic movement disorders
 Patient selection for surgery: Hyperkinetic movement disorders Alfons Schnitzler, MD, PhD Dept. of Neurology, Movement Disorder and Neuromodulation, Heinrich-Heine-University Düsseldorf, Germany Hyperkinetic
Patient selection for surgery: Hyperkinetic movement disorders Alfons Schnitzler, MD, PhD Dept. of Neurology, Movement Disorder and Neuromodulation, Heinrich-Heine-University Düsseldorf, Germany Hyperkinetic
Dr. Alan Carroll MB, BCh, MRC Psych. FRCP(C) Psychiatrist, Clinical Professor of Psychiatry, University of Alberta Glenrose Rehabilitation Hospital
 Psychiatrist, Clinical Professor of Psychiatry, University of Alberta Glenrose Rehabilitation Hospital") Dr. Alan Carroll MB, BCh, MRC Psych. FRCP(C) Psychiatrist, Clinical Professor of Psychiatry, University of Alberta Glenrose Rehabilitation Hospital Introduction! Tics Description and Variation! Tourette
Dr. Alan Carroll MB, BCh, MRC Psych. FRCP(C) Psychiatrist, Clinical Professor of Psychiatry, University of Alberta Glenrose Rehabilitation Hospital Introduction! Tics Description and Variation! Tourette
Tremor What is tremor? What causes tremor? What are the characteristics of tremor? What are the different categories of tremor?
 Tremor What is tremor? Tremor is an unintentional, somewhat rhythmic, muscle movement involving to-and-fro movements (oscillations) of one or more parts of the body. It is the most common of all involuntary
Tremor What is tremor? Tremor is an unintentional, somewhat rhythmic, muscle movement involving to-and-fro movements (oscillations) of one or more parts of the body. It is the most common of all involuntary
Index. Springer-Verlag Wien 2017 C. Falup-Pecurariu et al. (eds.), Movement Disorders Curricula, DOI /
, Movement Disorders Curricula, DOI /") A Abetalipoproteinemia (ALP), 441 Acanthocytosis ALP, 441 HDL2, 441 Acquired dystonias, 261 Action tremor, 304 ADHD. See Attention-deficit hyperactivity disorder (ADHD) Aetiological epidemiology induction
A Abetalipoproteinemia (ALP), 441 Acanthocytosis ALP, 441 HDL2, 441 Acquired dystonias, 261 Action tremor, 304 ADHD. See Attention-deficit hyperactivity disorder (ADHD) Aetiological epidemiology induction
Transcranial sonography in movement disorders
 Transcranial sonography in movement disorders Uwe Walter 1st Residential Training of the European Society of Neurosonology and Cerebral Hemodynamics September 7-12, 2008 Bertinoro, Italy Department of
Transcranial sonography in movement disorders Uwe Walter 1st Residential Training of the European Society of Neurosonology and Cerebral Hemodynamics September 7-12, 2008 Bertinoro, Italy Department of
Movement disorders: The border between the psychogenic and the neurological. Chiclana G, Ojeda J, Mata M, Chiclana C, Gutiérrez G, Miralles A,.
 Movement disorders: The border between the psychogenic and the neurological Chiclana G, Ojeda J, Mata M, Chiclana C, Gutiérrez G, Miralles A,. 1. Introduction 2. Cases Report 3. Conclusions 1. Introduction
Movement disorders: The border between the psychogenic and the neurological Chiclana G, Ojeda J, Mata M, Chiclana C, Gutiérrez G, Miralles A,. 1. Introduction 2. Cases Report 3. Conclusions 1. Introduction
Hunting for Huntington s
 Focus on CME at The University of Western Ontario Hunting for Huntington s Varinder Dua, MBBS, FRCPC Presented at the CME for Regional Mental Health Care, February 2004 Huntington s disease (HD) is a well-defined,
Focus on CME at The University of Western Ontario Hunting for Huntington s Varinder Dua, MBBS, FRCPC Presented at the CME for Regional Mental Health Care, February 2004 Huntington s disease (HD) is a well-defined,
Risk Factors for Blepharospasm
 Risk Factors for Blepharospasm Mark A. Stacy M.D. and Padma R. Mahant, M.D. The Barrow Neurological Institute Phoenix, AZ BACKGROUND Blepharospasm is a focal dystonia characterized by repetitive, sustained
Risk Factors for Blepharospasm Mark A. Stacy M.D. and Padma R. Mahant, M.D. The Barrow Neurological Institute Phoenix, AZ BACKGROUND Blepharospasm is a focal dystonia characterized by repetitive, sustained
Correlates of Tic Disorders. Hyperactivity / motor restlessness Inattentiveness Anxiety Aggression Other
 Tourette Disorder Rarely present in pure form No two individuals with TD are the same Often associated with other symptoms, which may be more disabling than the tics themselves Treatments need to target
Tourette Disorder Rarely present in pure form No two individuals with TD are the same Often associated with other symptoms, which may be more disabling than the tics themselves Treatments need to target