How to optimize timing of extubation? Andrew JE Seely MD, PhD, FRCSC
|
|
|
- Merilyn Webster
- 5 years ago
- Views:
Transcription


1 How to optimize timing of extubation? Andrew JE Seely MD, PhD, FRCSC
2 Disclosure Therapeutic Monitoring Systems (TMS) Founder and Chief Science Officer TMS Aim: improve patient care through innovative variability-derived clinical decision support software Issued patents re method and application of multiorgan variability monitoring
3 Why optimize timing of extubation? Prolonged ventilation harms patients Rajakaruna C et al, J Thorac Cardiovasc Surg 2005; Coplin WM et al, AJRCCM 2000; Lone NI, Walsh TS, Crit Care 2011 Extubation failure harms patients Seymour CW et al, Crit Care 2004; Thile AW et al, Crit Care Med 2011; Epstein SK et al, Chest, 1997; Dupont H et al, Intensive Care Med 2001; Rothaar RC et al, Curr Opin Crit Care 2003; Frutos-Vivar F et al, J Crit Care 2011.

4 Optimize timing of extubation? Why? Shorten duration of ventilation & length of stay. Reduce incidence of extubation failure. Improve patient care. Reduce costs of care. How?


5 W. Edwards Demming ( ) Importance of Process
6 Summary of process to optimize timing of extubation Best practice weaning, preparing for extubation. Plan in place for the event of failed extubation. Repeatedly re-assess readiness for extubation. Evaluate risk & consequences of failed extubation. Assist the Decision to Extubate? Mitigate risk of extubation failure. Extubate!
7 Best Practice Weaning Use protocols attempting to minimize sedation Protocolized rehabilitation, early mobilization Schmidt et al, ATS/ACCP Guidelines, AJRCCM 2017 Wean to partial support ventilation asap Assuming absence of strong effort, severe ARDS
8 Establish plans if failed extubation prior to extubation Extubation failure is rapid & unpredictable, and may indicate need for tracheostomy Need to know what action is indicated in event of failure, prior to extubation Many patients do not want re-intubation, tracheostomy, prolonged ventilation and rehab Ideal opportunity exists for establishing goals of care prior to extubation
9 Repeatedly reassess readiness for extubation How? Spontaneous Breathing trial (SBT) Mimic and thus predict ability to tolerate unassisted breathing SBT as soon as SBT readiness criteria met: resolution of initial reason for intubation, cardiovascular stability (minimal or no vasopressors), adequate mentation, adequate respiratory function (F<35, MIP < 20-25, Vt > 5ml/kg, VC > 10ml/kg, f/vt < 105), adequate oxygenation defined as PaO2/FiO2 150 mm Hg with PEEP up to 8 cm H2O. Boles JM et al. Eur Respir J 2007 Once daily screening will shorten LOS & costs Ely E et al, NEJM 1996; Girard TD et al, Lancet 2008
10 Evaluating SBT Success? Criteria for passing SBT include respiratory pattern, adequate gas exchange, haemodynamic stability and subject comfort. Boles JM et al. Eur Respir J 2007 Pass SBT if absence of agitation, anxiety, diaphoresis, worsened hypoxemia, tachypnea, arrhythmia, rapid shallow breathing, hypotension No strict thresholds of success vs. failure
11 SBT Technique Controversy No Support (T-piece) vs PS support? T-Piece: greater specificity (higher true negative rate) PS support: higher readiness, no evidence of more failure SBT Duration: min ATS/ACCP Guidelines, AJRCCM, Jan 2017 If vented>24 hrs, initial SBT should be with inspiratory pressure augmentation (5 8cm H2O) rather than without. FAST Trial underway (PI Karen Burns) 2x2 RCT: SBT technique & frequency, 250/750 pts enrolled


12 Assess risk factors for extubation failure Etiology of Extubation Failure Airway Airway obstruction Excessive secretions Impaired cough Aspiration Decreased LOC Can t breathe without ET tube Non-Airway Congestive heart failure hypoxemia hypoventilation Pulmonary disease Decreased LOC Can t breathe without vent support Epstein SK et al, AJRCCM 1998

13 Large Multicenter study Cough - Secretions + Resp failure Coma 1514 patients; 157 EF (10.4%) 45% airway, 50% breathing; 5% mixed (26 ICUs)
14 Risk Factors for Extubation Failure Non-modifiable factors: age, cardiorespiratory disease, APACHE II, pneumonia as indication for intubation During SBT: high f/vt>105 (>60?), PCO 2 >44, increase in BNP Potentially modifiable: + ve fluid balance last 24 hrs, GCS<8 (?), PaO 2 /FiO 2 <200, peak exp flow <60 L/min, ++ secretions, weak cough, Hg<100 F Frutos Vivar et al Chest 2006; A Thille et al, AJRCCM 2013


15 Estimate risk of failed extubation / time Assess risk factors of extubation failure Identify modifiable risk factors; reduce them if possible, prior to extubation Clinicians should be more vigilant in identifying who is at high risk for extubation failure... one can recommend delaying extubation if the risk factor can be substantially corrected in 1 3 days. Epstein S, Crit Care 2004.
16 Assess consequences of extubation failure Overall frailty, potential for myocardial ischemia, mild organ dysfunction all augment risk of harm due to extubation failure Etiology of extubation failure (non-airway worse than airway) and time to re-intubation are independent predictors of poor outcome Epstein SK et al, AJRCCM 1998

17 Individualized process of assessment? First SBT: with 5-8 cm H 2 O support Subsequent SBT technique modified by perceived consequences of failed extubation T-piece test results may be too conservative if the clinicians are very cautious and/or if the prevalence of extubation failure is low (e.g., failed in postoperative extubation: patients). consider On the T-piece other hand, and the longer low-ps test may SBT underestimate to increase the specificity risk of extubation (true failure, negative especially rate). if the clinician is overoptimistic or if the prevalence of extubation Patients without: failure use is 5-8 high cm H 2 O PS during Patients with potential serious consequences of SBT A Thille, JC Richard, L Brochard, AJRCCM 2013
18 Mitigate risk of Extubation Failure Pre-extubation: Consider diuresis, afterload control, inotropic support as required Absence of cuff leak: consider systemic steroids at least 4 hrs before extubation Post-extubation Impaired ability to expectorate, dead space ventilation, impaired oxygenation, consider high flow high humidity (HFH) O 2 Poor LV fxn, COPD, weakness, hypercapnea, consider noninvasive ventilation (NINV) Multiple factors, high risk, consider intermittent NINV & HFH
19 Assist clinicians with extubation decision making? What might be beneficial? Complete holistic patient evaluation Optimal prediction extubation outcomes Standardized patient assessment
, 9 respiratory rate variability (RRV) metrics associated with EF (p-values 0.00004-0.")
20 Weaning and Variability Evaluation (WAVE) study Multicenter observational study (721 pts, 12 sites, 434 high quality data) Observed a 12% extubation failure (EF) rate (re-intubation <48 hours) ClinicalTrials.gov NCT Registered 13 October Statistical analysis: 1 heart rate variability (HRV), 9 respiratory rate variability (RRV) metrics associated with EF (p-values ) Predictive modelling: WAVE score (ave of 5 univariate RRV logistic regression models) was best predictor of EF, superior to AND complementary with RSBI, RR, or clinical judgement

21 WAVE score WAVE score correlates with probability of extubation failure Goal: Identify low risk and high risk patients 4% risk of Extubation failure 25% risk of Extubation failure Provide clinical decision support, not decisionmaking WAVE Score Quartiles



22 Value PPV 36% ROC AUC 0.87 RSBI PPV 42% Clinical impression ROC AUC 0.82

 synoptic report Assist & improve extubation")
23 Extubation Advisor TM Optimal prediction extubation outcomes Respiratory rate variability AND best current practice Standardized multidisciplinary assessment Summary (one-page) synoptic report Assist & improve extubation decision making
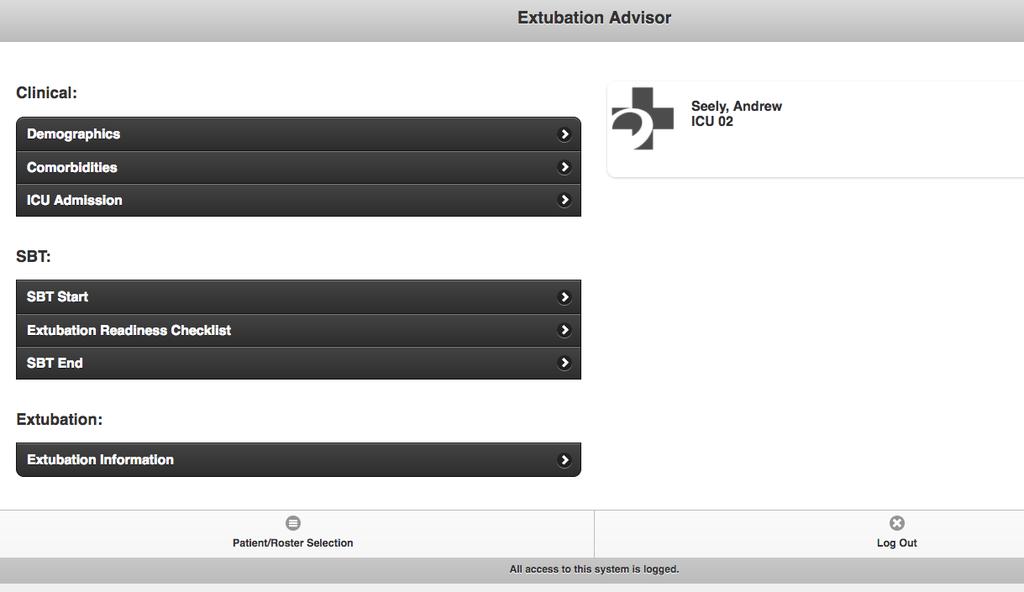
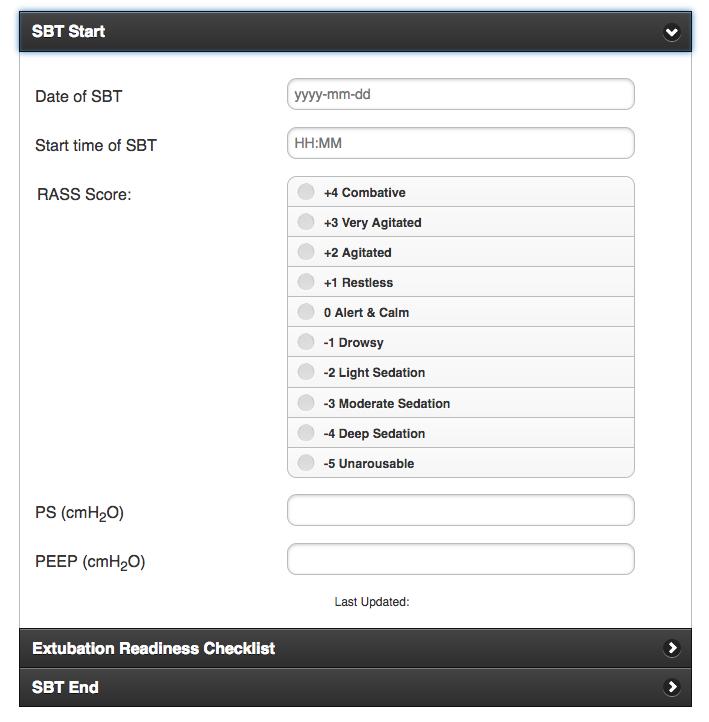
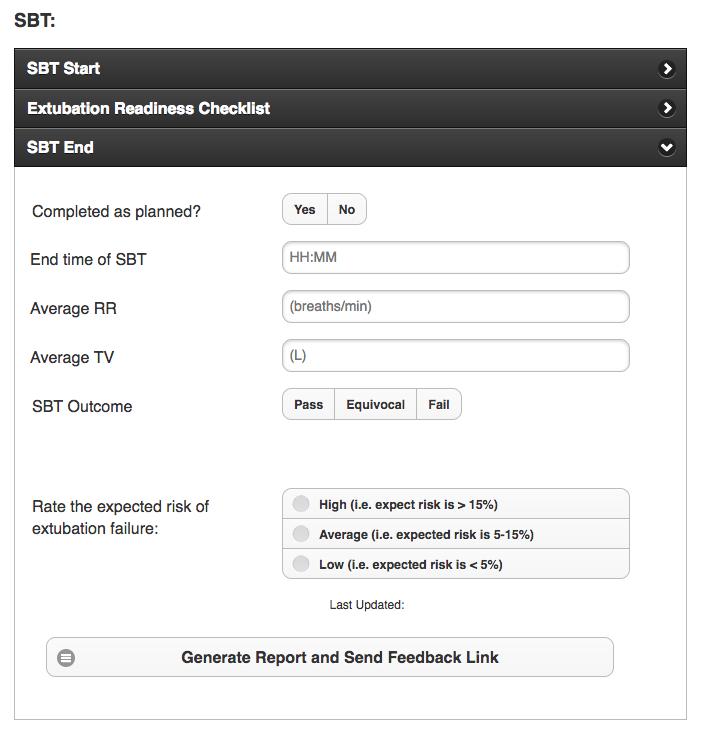
24 Extubation Advisor Input Screens
 Days in ICU: 2 MRN: 88888888 Days on Ventilator: 2 Sex: F RT Impression: Low Risk Phase I Single center study (Co-PI A Sarti) June 2017 to Oct 2018: Enrolled 117")

25 Extubation Advisor Extubation Advisor TM SBT Synoptic Report Overall Assessment of Extubation Failure Risk: Standard (RSBI): Wave Score: Low Risk Low Risk Name: Anstee, Caitlin Bed Number: ICU 12 DOB: (34) Days in ICU: 2 MRN: Days on Ventilator: 2 Sex: F RT Impression: Low Risk Phase I Single center study (Co-PI A Sarti) June 2017 to Oct 2018: Enrolled 117 patients Entered 240 SBT forms Generated 231 SBT reports Recorded 78 extubations Completed 52 questionnaires Conducted 15 interviews Results pending. Patient Information: Comorbidities: Major Cardiac Illness, Diabetes Reason for Admission: Shock - Septic - Lung SBT Information: Start: :30 End: :00 Completed as planned? Yes Possible Last SBT? RASS Score: +1 PS: 1 cmh 2 O PEEP: 1 cmh 2 O Measured Vitals during SBT: Average BP: 103/52.6 Average HR: 67.8 beats/min Average RR: 14.3 breaths/min Average O 2 Sat: 95.9 % MAP: 70.6 mmhg Standard: Average RR: 1 breaths/min Average TV: 1L Average RSBI: 1 (< 60 = low risk; = average risk; > 110 = high risk.) Extubation Advisor TM Decision Support: Extubation Readiness Checklist: Improved from admission Cuff Leak Present Strong Cough Spontaneous Cough Gag Present No or Intermittent Sedatives able to lift head off pillow for > 5 sec High Dose Pressors Required No Cuff Leak Present SpO2 < 90% FiO2 > 40% on PEEP > 5cm H 2 O Does Not Obey Commands Weak Hand Grip Positive Fluid Balance Last 24H Poor Urine Output Respiratory Therapist Impression: SBT Outcome: Pass RT Perception of Risk of Extubation Failure: Low Wave Score TM : 0.41 (Based on respiratory rate variablility. Low variability = high score and a high probability of extubation failure.) Risk of Extubation Failure: LOW Fold Increase: 40% of normal risk. Note: The WAVE Score TM provides an estimate of the risk of extubation failure (defined as the need for re-intubation within 48 h after extubation). This risk estimate is based on a model incorporating measurements of the patient's heart rate and respiratory rate variability in the period around a spontaneous breathing trial (SBT). The decision to separate a patient from mechanical ventilation must incorporate all available more information, please refer to the Extubation Advisor TM Instructions for Use. Report Generated: T14:14:30-04:00 Respiratory Therapist: Caitlin Anstee
26 Summary 1. Best practice weaning, preparing for extubation. Spontaneous breathing, protocolized sedation, early mobilization 2. Plan in place in the event of failed extubation. Opportunity to understand patient s goals of care & limits to care 3. Repeatedly re-assess readiness for extubation. Perform SBTs as soon as possible and daily, look to extubate if success 4. Evaluate risk & consequences of failed extubation. Identify & correct risk factors, modify SBT if potential harm from EF 5. Assist the decision to extubate? Offer optimal prediction and standardized assessment 6. Mitigate risk of extubation failure. Selective non-invasive ventilation, High flow High humidity O 2, steroids
27 Thank you.

28 and medicine!
29 Lack of Standardized Practice No universal SBT performance or reporting Analysis of 931 SBTs in 680 pts (8 NA centers) Inter-institutional variation in SBT performance, including ventilator settings, sedation, oxygenation and SBT reporting (checklists, MD communication)
30 Acknowledgements Canadian Critical Care Trials Group S Dhanani, K Burns, N Ferguson, J Marshall, G Rubenfeld, C Martin, F Lellouche, S Mehta, P Dodek, R Zarychanski, D Scales, Y Skrobik. Ottawa Hospital Research Institute Collaborators T Ramsay, A Sarti, D Kubelik, D Fergusson, L McIntyre, D Maziak Ottawa Dynamical Analysis Laboratory team C Herry, N Scales, K Newman Clinical research coordinators A Fazekas, C Anstee, E Delic I Watpool, R Porteous, B Gomes,... Therapeutic Monitoring Systems D Longbottom, W Threader, D McNair Funding CIHR (2005, 2010), AFP Innovation (2009, 2014, 2016), PSI (2017)
31 Why optimize timing of extubation? Prolonged ventilation harms patients Ventilation causes muscle atrophy, weakness, VAP,... Prolonged ventilation after cardiac surgery increases mortality 6x and costs 8x. Rajakaruna C et al, J Thorac Cardiovasc Surg 2005 Delayed extubation after brain injury associated with increased mortality, LOS and VAP Coplin WM et al, AJRCCM 2000 Prolonged ventilation (>21d) spent longer in hosp post ICU (17 vs 7 days) & increased mortality (40% vs 34%) Lone NI, Walsh TS, Crit Care 2011
32 Why optimize timing of extubation? Extubation failure harms patients Extubation failure: incidence 15% Yang KL, Tobin MJ, NEJM 1991; Esteban A et al, AJRCCM 1999; Epstein S, Chest 2001; Frutos-Vivar F et al, J Crit Care 2011 Extubation failure associated with increased mortality, duration of ventilation, length of stay, rehab, independent of illness severity Thile AW et al, Crit Care Med 2011; Epstein SK et al, Chest, 1997; Dupont H et al, Intensive Care Med 2001; Rothaar RC et al, Curr Opin Crit Care 2003; Frutos-Vivar F et al, J Crit Care Extubation failure costs additional $34,000/pt Seymour CW et al, Crit Care 2004.




33 How should we seek to improve care by influencing clinical decision making? Thinking Fast: System One Fast, instinctive, emotional Prone to repeated mistakes: Examples: Loss aversion: give more weight to potential losses than gains Status quo bias: prefer status quo Endowment effect: overestimation of what we already have Thinking Slow: System Two Slow, learned, deliberate Able to correct System I errors Daniel Kahneman Amos Tversky Thus, goals in introducing CDS are to: Aim to standardize processes of assessment & decision making Aim to systematically support & augment System Two thinking
34 Weaning and Variability Evaluation (Wave) Hypothesis: Decreased HRV and/or RRV during SBT is associated with and predicts extubation failure. Design: Multicenter, waived consent, observational study, record HRV & RRV during last SBT prior to extubation. Aims: (1) Determine if altered HRV and/or RRV are associated with extubation failure; (2) develop a predictive model to predict extubation outcomes; (3) determine if variability offers added value to traditional predictors of extubation outcomes.

35 Reduced RRV = reduced adaptability Restrictive Lung Disease Controls Diminished variability = diminished adaptability = decreased capacity to tolerate increased workload.
36 E.g. reduced respiratory variability First multicenter study (4 units). N=51 (32 extubation success, 14 failure ) Breathing variability is greater in patients successfully separated from ET tube. Successful extubation Failed extubation Good ariability Reduced variability Example of reduced variability predicting poor outcome



37 Variability and Extubation N=52 N=78 N=51 N=24 11 N=32 N=42
38 Extubation Decision Making? Will the patient be able to sustain spontaneous ventilation following tube removal, and protect his or her airway after extubation? Tobin M, Am J Resp Crit Care Med 2012 Clinicians should be more vigilant in identifying who is at high risk for extubation failure... one can recommend delaying extubation if the risk factor can be substantially corrected in 1 3 days. Epstein S, Crit Care 2004.
Weaning from Mechanical Ventilation. Dr Azmin Huda Abdul Rahim
 Weaning from Mechanical Ventilation Dr Azmin Huda Abdul Rahim Content Definition Classification Weaning criteria Weaning methods Criteria for extubation Introduction Weaning comprises 40% of the duration
Weaning from Mechanical Ventilation Dr Azmin Huda Abdul Rahim Content Definition Classification Weaning criteria Weaning methods Criteria for extubation Introduction Weaning comprises 40% of the duration
Optimize vent weaning and SBT outcomes. Identify underlying causes for SBT failures. Role SBT and weaning protocol have in respiratory care
 Optimize vent weaning and SBT outcomes Identify underlying causes for SBT failures Role SBT and weaning protocol have in respiratory care Lower risk of developing complications Lower risk of VAP, other
Optimize vent weaning and SBT outcomes Identify underlying causes for SBT failures Role SBT and weaning protocol have in respiratory care Lower risk of developing complications Lower risk of VAP, other
Liberation from Mechanical Ventilation in Critically Ill Adults
 Liberation from Mechanical Ventilation in Critically Ill Adults 2017 ACCP/ATS Clinical Practice Guidelines Timothy D. Girard, MD, MSCI Clinical Research, Investigation, and Systems Modeling of Acute Illness
Liberation from Mechanical Ventilation in Critically Ill Adults 2017 ACCP/ATS Clinical Practice Guidelines Timothy D. Girard, MD, MSCI Clinical Research, Investigation, and Systems Modeling of Acute Illness
Weaning and extubation in PICU An evidence-based approach
 Weaning and extubation in PICU An evidence-based approach Suchada Sritippayawan, MD. Div. Pulmonology & Crit Care Dept. Pediatrics Faculty of Medicine Chulalongkorn University Kanokporn Udomittipong, MD.
Weaning and extubation in PICU An evidence-based approach Suchada Sritippayawan, MD. Div. Pulmonology & Crit Care Dept. Pediatrics Faculty of Medicine Chulalongkorn University Kanokporn Udomittipong, MD.
17400 Medina Road, Suite 100 Phone: Minneapolis, MN Fax:
 17400 Medina Road, Suite 100 Phone: 763-398-8300 Minneapolis, MN 55447-1341 Fax: 763-398-8400 www.pulmonetic.com Clinical Bulletin To: Cc: From: Domestic Sales Representatives and International Distributors
17400 Medina Road, Suite 100 Phone: 763-398-8300 Minneapolis, MN 55447-1341 Fax: 763-398-8400 www.pulmonetic.com Clinical Bulletin To: Cc: From: Domestic Sales Representatives and International Distributors
Extubation Failure & Delay in Brain-Injured Patients
 Extubation Failure & Delay in Brain-Injured Patients Niall D. Ferguson, MD, FRCPC, MSc Director, Critical Care Medicine University Health Network & Mount Sinai Hospital Associate Professor of Medicine
Extubation Failure & Delay in Brain-Injured Patients Niall D. Ferguson, MD, FRCPC, MSc Director, Critical Care Medicine University Health Network & Mount Sinai Hospital Associate Professor of Medicine
NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity
 NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Use of NIV 1998-2010 50 45 40 35 30 25 20 15 10 5 0 1998
NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Use of NIV 1998-2010 50 45 40 35 30 25 20 15 10 5 0 1998
UCH WEANING FROM MECHANICAL VENTILATION PATHWAY
 UCH WEANING FROM MECHANICAL VENTILATION PATHWAY WAKE WARM AND WEAN. POST OPERATIVE PATIENTS WHO HAVE BEEN VENTILATED < 24 HOURS DAILY EXTUBATION SCREEN A DAILY SCREEN TO BE CARRIED OUT ON ALL PATIENTS
UCH WEANING FROM MECHANICAL VENTILATION PATHWAY WAKE WARM AND WEAN. POST OPERATIVE PATIENTS WHO HAVE BEEN VENTILATED < 24 HOURS DAILY EXTUBATION SCREEN A DAILY SCREEN TO BE CARRIED OUT ON ALL PATIENTS
The Art and Science of Weaning from Mechanical Ventilation
 The Art and Science of Weaning from Mechanical Ventilation Shekhar T. Venkataraman M.D. Professor Departments of Critical Care Medicine and Pediatrics University of Pittsburgh School of Medicine Some definitions
The Art and Science of Weaning from Mechanical Ventilation Shekhar T. Venkataraman M.D. Professor Departments of Critical Care Medicine and Pediatrics University of Pittsburgh School of Medicine Some definitions
Surgery Grand Rounds. Non-invasive Ventilation: A valuable tool. James Cromie, PGY 3 8/24/09
 Surgery Grand Rounds Non-invasive Ventilation: A valuable tool James Cromie, PGY 3 8/24/09 History of mechanical ventilation 1930 s: use of iron lung 1940 s: First NIV system (Bellevue Hospital) 1950 s:
Surgery Grand Rounds Non-invasive Ventilation: A valuable tool James Cromie, PGY 3 8/24/09 History of mechanical ventilation 1930 s: use of iron lung 1940 s: First NIV system (Bellevue Hospital) 1950 s:
Effectiveness and safety of a protocolized mechanical ventilation and weaning strategy of COPD patients by respiratory therapists
 Original Article Effectiveness and safety of a protocolized mechanical ventilation and weaning strategy of COPD patients by respiratory therapists Cenk Kirakli, Ozlem Ediboglu, Ilknur Naz, Pinar Cimen,
Original Article Effectiveness and safety of a protocolized mechanical ventilation and weaning strategy of COPD patients by respiratory therapists Cenk Kirakli, Ozlem Ediboglu, Ilknur Naz, Pinar Cimen,
Spontaneous Breathing Trial and Mechanical Ventilation Weaning Process
 Page 1 of 5 ASSESSMENT INTERVENTION Patient receiving mechanical ventilation Baseline ventilatory mode/ settings RT and RN to assess criteria 1 for SBT Does patient meet criteria? RT to initiate SBT Does
Page 1 of 5 ASSESSMENT INTERVENTION Patient receiving mechanical ventilation Baseline ventilatory mode/ settings RT and RN to assess criteria 1 for SBT Does patient meet criteria? RT to initiate SBT Does
Weaning: The key questions
 Weaning from mechanical ventilation Weaning / Extubation failure: Is it a real problem in the PICU? Reported extubation failure rates in PICUs range from 4.1% to 19% Baisch SD, Wheeler WB, Kurachek SC,
Weaning from mechanical ventilation Weaning / Extubation failure: Is it a real problem in the PICU? Reported extubation failure rates in PICUs range from 4.1% to 19% Baisch SD, Wheeler WB, Kurachek SC,
PAPER DE LA VNI EN LA RETIRADA DE LA VENTILACIÓ INVASIVA I FRACÀS D EXTUBACIÓ
 PAPER DE LA VNI EN LA RETIRADA DE LA VENTILACIÓ INVASIVA I FRACÀS D EXTUBACIÓ Dr. Miquel Ferrer UVIIR, Servei de Pneumologia, Hospital Clínic, IDIBAPS, CibeRes, Barcelona. E- mail: miferrer@clinic.ub.es
PAPER DE LA VNI EN LA RETIRADA DE LA VENTILACIÓ INVASIVA I FRACÀS D EXTUBACIÓ Dr. Miquel Ferrer UVIIR, Servei de Pneumologia, Hospital Clínic, IDIBAPS, CibeRes, Barcelona. E- mail: miferrer@clinic.ub.es
NIV in hypoxemic patients
 NIV in hypoxemic patients Massimo Antonelli, MD Dept. of Intensive Care & Anesthesiology Università Cattolica del Sacro Cuore Rome - Italy Conflict of interest (research grants and consultations): Maquet
NIV in hypoxemic patients Massimo Antonelli, MD Dept. of Intensive Care & Anesthesiology Università Cattolica del Sacro Cuore Rome - Italy Conflict of interest (research grants and consultations): Maquet
MECHANICAL VENTILATION PROTOCOLS
 GENERAL or SURGICAL Initial Ventilator Parameters Ventilator Management (see appendix I) Assess Patient Data (see appendix II) Data Collection Mode: Tidal Volume: FIO2: PEEP: Rate: I:E Ratio: ACUTE PHASE
GENERAL or SURGICAL Initial Ventilator Parameters Ventilator Management (see appendix I) Assess Patient Data (see appendix II) Data Collection Mode: Tidal Volume: FIO2: PEEP: Rate: I:E Ratio: ACUTE PHASE
Recovery from ICU-acquired weakness; do not forget the respiratory muscles!
 Recovery from ICU-acquired weakness; do not forget the respiratory muscles! Beatrix Clerckx Department of Rehabilitation Sciences, Department of Intensive Care Medicine, University Hospitals Leuven, Catholic
Recovery from ICU-acquired weakness; do not forget the respiratory muscles! Beatrix Clerckx Department of Rehabilitation Sciences, Department of Intensive Care Medicine, University Hospitals Leuven, Catholic
Keeping Patients Off the Vent: Bilevel, HFNC, Neither?
 Keeping Patients Off the Vent: Bilevel, HFNC, Neither? Robert Kempainen, MD Pulmonary and Critical Care Medicine Hennepin County Medical Center University of Minnesota School of Medicine Objectives Summarize
Keeping Patients Off the Vent: Bilevel, HFNC, Neither? Robert Kempainen, MD Pulmonary and Critical Care Medicine Hennepin County Medical Center University of Minnesota School of Medicine Objectives Summarize
Landmark articles on ventilation
 Landmark articles on ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity ARDS AECC DEFINITION-1994 ALI Acute onset Bilateral chest infiltrates PCWP
Landmark articles on ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity ARDS AECC DEFINITION-1994 ALI Acute onset Bilateral chest infiltrates PCWP
1. Screening to identify SBT candidates
 Karen E. A. Burns MD, FRCPC, MSc (Epid) Associate Professor, Clinician Scientist St. Michael s Hospital, Toronto, Canada burnsk@smh.ca Review evidence supporting: 1. Screening to identify SBT candidates
Karen E. A. Burns MD, FRCPC, MSc (Epid) Associate Professor, Clinician Scientist St. Michael s Hospital, Toronto, Canada burnsk@smh.ca Review evidence supporting: 1. Screening to identify SBT candidates
Test Bank Pilbeam's Mechanical Ventilation Physiological and Clinical Applications 6th Edition Cairo
 Instant dowload and all chapters Test Bank Pilbeam's Mechanical Ventilation Physiological and Clinical Applications 6th Edition Cairo https://testbanklab.com/download/test-bank-pilbeams-mechanical-ventilation-physiologicalclinical-applications-6th-edition-cairo/
Instant dowload and all chapters Test Bank Pilbeam's Mechanical Ventilation Physiological and Clinical Applications 6th Edition Cairo https://testbanklab.com/download/test-bank-pilbeams-mechanical-ventilation-physiologicalclinical-applications-6th-edition-cairo/
Concerns and Controversial Issues in NPPV. Concerns and Controversial Issues in Noninvasive Positive Pressure Ventilation
 : Common Therapy in Daily Practice Concerns and Controversial Issues in Noninvasive Positive Pressure Ventilation Rongchang Chen Guangzhou Institute of Respiratory Disease as the first choice of mechanical
: Common Therapy in Daily Practice Concerns and Controversial Issues in Noninvasive Positive Pressure Ventilation Rongchang Chen Guangzhou Institute of Respiratory Disease as the first choice of mechanical
Noninvasive Ventilation: Non-COPD Applications
 Noninvasive Ventilation: Non-COPD Applications NONINVASIVE MECHANICAL VENTILATION Why Noninvasive Ventilation? Avoids upper A respiratory airway trauma system lacerations, protective hemorrhage strategy
Noninvasive Ventilation: Non-COPD Applications NONINVASIVE MECHANICAL VENTILATION Why Noninvasive Ventilation? Avoids upper A respiratory airway trauma system lacerations, protective hemorrhage strategy
Surviving Sepsis Campaign. Guidelines for Management of Severe Sepsis/Septic Shock. An Overview
 Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
Home Mechanical Ventilation. Anthony Bateman
 Home Mechanical Ventilation Anthony Bateman What is Long Term Ventilation? LTV is the provision of respiratory support to individuals with non-acute respiratory failure Progression of expected disease
Home Mechanical Ventilation Anthony Bateman What is Long Term Ventilation? LTV is the provision of respiratory support to individuals with non-acute respiratory failure Progression of expected disease
ARDS: an update 6 th March A. Hakeem Al Hashim, MD, FRCP SQUH
 ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv
 Rv") ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
Case Scenarios. Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC. Consultant, Critical Care Medicine Medanta, The Medicity
 Case Scenarios Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Case 1 A 36 year male with cirrhosis and active GI bleeding is intubated to protect his airway,
Case Scenarios Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Case 1 A 36 year male with cirrhosis and active GI bleeding is intubated to protect his airway,
Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor
 Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
Outcomes From Severe ARDS Managed Without ECMO. Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016
 Outcomes From Severe ARDS Managed Without ECMO Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016 Severe ARDS Berlin Definition 2012 P:F ratio 100 mm Hg Prevalence:
Outcomes From Severe ARDS Managed Without ECMO Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016 Severe ARDS Berlin Definition 2012 P:F ratio 100 mm Hg Prevalence:
Sedation Hold/Interruption and Weaning Protocol ( Wake-up and Breathe )
") PROTOCOL Sedation Hold/Interruption and Weaning Protocol ( Wake-up and Breathe ) Page 1 of 6 Scope: Population: Outcome: Critical care clinicians and providers. All ICU patients intubated or mechanically
PROTOCOL Sedation Hold/Interruption and Weaning Protocol ( Wake-up and Breathe ) Page 1 of 6 Scope: Population: Outcome: Critical care clinicians and providers. All ICU patients intubated or mechanically
FAILURE OF NONINVASIVE VENTILATION FOR DE NOVO ACUTE HYPOXEMIC RESPIRATORY FAILURE: ROLE OF TIDAL VOLUME
 FAILURE OF NONINVASIVE VENTILATION FOR DE NOVO ACUTE HYPOXEMIC RESPIRATORY FAILURE: ROLE OF TIDAL VOLUME Guillaume CARTEAUX, Teresa MILLÁN-GUILARTE, Nicolas DE PROST, Keyvan RAZAZI, Shariq ABID, Arnaud
FAILURE OF NONINVASIVE VENTILATION FOR DE NOVO ACUTE HYPOXEMIC RESPIRATORY FAILURE: ROLE OF TIDAL VOLUME Guillaume CARTEAUX, Teresa MILLÁN-GUILARTE, Nicolas DE PROST, Keyvan RAZAZI, Shariq ABID, Arnaud
Year in Review Intensive Care Training Program Radboud University Medical Centre Nijmegen
 Year in Review 2013 Intensive Care Training Program Radboud University Medical Centre Nijmegen Contents ARDS Ventilator associated pneumonia Tracheostomy and endotracheal intubation Enteral feeding Fluid
Year in Review 2013 Intensive Care Training Program Radboud University Medical Centre Nijmegen Contents ARDS Ventilator associated pneumonia Tracheostomy and endotracheal intubation Enteral feeding Fluid
Difficult weaning from mechanical ventilation
 Difficult weaning from mechanical ventilation Paolo Biban, MD Director, Neonatal and Paediatric Intensive Care Unit Division of Paediatrics, Major City Hospital Azienda Ospedaliera Universitaria Integrata
Difficult weaning from mechanical ventilation Paolo Biban, MD Director, Neonatal and Paediatric Intensive Care Unit Division of Paediatrics, Major City Hospital Azienda Ospedaliera Universitaria Integrata
CSIM annual meeting Acute respiratory failure. Dr. John Ronald, FRCPC Int Med, Resp, CCM. October 10, 2018
 CSIM annual meeting - 2018 Acute respiratory failure Dr. John Ronald, FRCPC Int Med, Resp, CCM. October 10, 2018 NRGH affiliated with UBC medicine Disclosures None relevant to this presentation. Also no
CSIM annual meeting - 2018 Acute respiratory failure Dr. John Ronald, FRCPC Int Med, Resp, CCM. October 10, 2018 NRGH affiliated with UBC medicine Disclosures None relevant to this presentation. Also no
Ventilatory Management of ARDS. Alexei Ortiz Milan; MD, MSc
 Ventilatory Management of ARDS Alexei Ortiz Milan; MD, MSc 2017 Outline Ventilatory management of ARDS Protected Ventilatory Strategy Use of NMB Selection of PEEP Driving pressure Lung Recruitment Prone
Ventilatory Management of ARDS Alexei Ortiz Milan; MD, MSc 2017 Outline Ventilatory management of ARDS Protected Ventilatory Strategy Use of NMB Selection of PEEP Driving pressure Lung Recruitment Prone
Noninvasive respiratory support:why is it working?
 Noninvasive respiratory support:why is it working? Paolo Pelosi Department of Surgical Sciences and Integrated Diagnostics (DISC) IRCCS San Martino IST University of Genoa, Genoa, Italy ppelosi@hotmail.com
Noninvasive respiratory support:why is it working? Paolo Pelosi Department of Surgical Sciences and Integrated Diagnostics (DISC) IRCCS San Martino IST University of Genoa, Genoa, Italy ppelosi@hotmail.com
Noninvasive ventilation: Selection of patient, interfaces, initiation and weaning
 CME article Johnson S, et al: Noninvasive ventilation Noninvasive ventilation: Selection of patient, interfaces, initiation and weaning Saumy Johnson, Ramesh Unnikrishnan * Email: ramesh.unnikrishnan@manipal.edu
CME article Johnson S, et al: Noninvasive ventilation Noninvasive ventilation: Selection of patient, interfaces, initiation and weaning Saumy Johnson, Ramesh Unnikrishnan * Email: ramesh.unnikrishnan@manipal.edu
Mechanical Ventilation in COPD patients
 Mechanical Ventilation in COPD patients Θεόδωρος Βασιλακόπουλος Καθηγητής Πνευμονολογίας-Εντατικής Θεραπείας Εθνικό & Καποδιστριακό Πανεπιστήμιο Αθηνών Νοσοκομείο «ο Ευαγγελισμός» Adjunct Professor, McGill
Mechanical Ventilation in COPD patients Θεόδωρος Βασιλακόπουλος Καθηγητής Πνευμονολογίας-Εντατικής Θεραπείας Εθνικό & Καποδιστριακό Πανεπιστήμιο Αθηνών Νοσοκομείο «ο Ευαγγελισμός» Adjunct Professor, McGill
Although the literature reports that approximately. off a ventilator
 Taking your patient off a ventilator Although the literature reports that approximately 33% of patients in the ICU require mechanical ventilation (MV),! the figure is closer to 90% for the critically SONIA
Taking your patient off a ventilator Although the literature reports that approximately 33% of patients in the ICU require mechanical ventilation (MV),! the figure is closer to 90% for the critically SONIA
UPDATE IN HOSPITAL MEDICINE
 UPDATE IN HOSPITAL MEDICINE FLORIDA CHAPTER ACP MEETING 2016 Himangi Kaushal, M.D., F.A.C.P. Program Director Memorial Healthcare System Internal Medicine Residency DISCLOSURES None OBJECTIVES Review some
UPDATE IN HOSPITAL MEDICINE FLORIDA CHAPTER ACP MEETING 2016 Himangi Kaushal, M.D., F.A.C.P. Program Director Memorial Healthcare System Internal Medicine Residency DISCLOSURES None OBJECTIVES Review some
Recognizing and Correcting Patient-Ventilator Dysynchrony
 2019 KRCS Annual State Education Seminar Recognizing and Correcting Patient-Ventilator Dysynchrony Eric Kriner BS,RRT Pulmonary Critical Care Clinical Specialist MedStar Washington Hospital Center Washington,
2019 KRCS Annual State Education Seminar Recognizing and Correcting Patient-Ventilator Dysynchrony Eric Kriner BS,RRT Pulmonary Critical Care Clinical Specialist MedStar Washington Hospital Center Washington,
Crit Vent Bundle for Mechanical Ventilation (337) [337] Physician - Also, enter Critical Care Admission Orders
![Crit Vent Bundle for Mechanical Ventilation (337) [337] Physician - Also, enter Critical Care Admission Orders](/thumbs/83/87321224.jpg "Crit Vent Bundle for Mechanical Ventilation (337) [337] Physician - Also, enter Critical Care Admission Orders") Crit Vent Bundle for Mechanical Ventilation (337) [337] Physician - Also, enter Critical Care Admission Orders Initial Vent Settings (Single Response) [6360] If no previous orders and no choice made by
Crit Vent Bundle for Mechanical Ventilation (337) [337] Physician - Also, enter Critical Care Admission Orders Initial Vent Settings (Single Response) [6360] If no previous orders and no choice made by
The Berlin Definition: Does it fix anything?
 The Berlin Definition: Does it fix anything? Gordon D. Rubenfeld, MD MSc Professor of Medicine, University of Toronto Chief, Program in Trauma, Emergency, and Critical Care Sunnybrook Health Sciences Centre
The Berlin Definition: Does it fix anything? Gordon D. Rubenfeld, MD MSc Professor of Medicine, University of Toronto Chief, Program in Trauma, Emergency, and Critical Care Sunnybrook Health Sciences Centre
High Flow Oxygen Therapy in Acute Respiratory Failure. Laurent Brochard Toronto
 High Flow Oxygen Therapy in Acute Respiratory Failure Laurent Brochard Toronto Conflicts of interest Our clinical research laboratory has received research grants for clinical research projects from the
High Flow Oxygen Therapy in Acute Respiratory Failure Laurent Brochard Toronto Conflicts of interest Our clinical research laboratory has received research grants for clinical research projects from the
THE USE OF HYPERINFLATION IN THE MANAGEMENT OF INTUBATED AND VENTILATED ADULT PATIENTS RECOMMENDATIONS
 THE USE OF HYPERINFLATION IN THE MANAGEMENT OF INTUBATED AND VENTILATED ADULT PATIENTS RECOMMENDATIONS Recommendation 1 on website Hyperinflation (Ventilator or manual) might be included in the management
THE USE OF HYPERINFLATION IN THE MANAGEMENT OF INTUBATED AND VENTILATED ADULT PATIENTS RECOMMENDATIONS Recommendation 1 on website Hyperinflation (Ventilator or manual) might be included in the management
Wet Lungs Dry lungs Impact on Outcome in ARDS. Charlie Phillips MD Division of PCCM OHSU 2009
 Wet Lungs Dry lungs Impact on Outcome in ARDS Charlie Phillips MD Division of PCCM OHSU 2009 Today s talk Pathophysiology of ARDS The case for dry Targeting EVLW Disclosures Advisor for Pulsion Medical
Wet Lungs Dry lungs Impact on Outcome in ARDS Charlie Phillips MD Division of PCCM OHSU 2009 Today s talk Pathophysiology of ARDS The case for dry Targeting EVLW Disclosures Advisor for Pulsion Medical
Respiratory insufficiency in bariatric patients
 Respiratory insufficiency in bariatric patients Special considerations or just more of the same? Weaning and rehabilation conference 6th November 2015 Definition of obesity Underweight BMI< 18 Normal weight
Respiratory insufficiency in bariatric patients Special considerations or just more of the same? Weaning and rehabilation conference 6th November 2015 Definition of obesity Underweight BMI< 18 Normal weight
CASE PRESENTATION VV ECMO
 CASE PRESENTATION VV ECMO Joshua Huelster, MD Fellow in Critical Care Medicine Department of Pulmonary and Critical Care Medicine Hennepin County Medical Center Disclosure There are no conflicts of interest
CASE PRESENTATION VV ECMO Joshua Huelster, MD Fellow in Critical Care Medicine Department of Pulmonary and Critical Care Medicine Hennepin County Medical Center Disclosure There are no conflicts of interest
Mechanical Ventilation in COPD patients
 Mechanical Ventilation in COPD patients Θεόδωρος Βασιλακόπουλος Καθηγητής Πνευμονολογίας-Εντατικής Θεραπείας Εθνικό & Καποδιστριακό Πανεπιστήμιο Αθηνών Νοσοκομείο «ο Ευαγγελισμός» Adjunct Professor, McGill
Mechanical Ventilation in COPD patients Θεόδωρος Βασιλακόπουλος Καθηγητής Πνευμονολογίας-Εντατικής Θεραπείας Εθνικό & Καποδιστριακό Πανεπιστήμιο Αθηνών Νοσοκομείο «ο Ευαγγελισμός» Adjunct Professor, McGill
NIV use in ED. Dr. Khalfan AL Amrani Emergency Resuscitation Symposium 2 nd May 2016 SQUH
 NIV use in ED Dr. Khalfan AL Amrani Emergency Resuscitation Symposium 2 nd May 2016 SQUH Outline History & Introduction Overview of NIV application Review of proven uses of NIV History of Ventilation 1940
NIV use in ED Dr. Khalfan AL Amrani Emergency Resuscitation Symposium 2 nd May 2016 SQUH Outline History & Introduction Overview of NIV application Review of proven uses of NIV History of Ventilation 1940
The use of proning in the management of Acute Respiratory Distress Syndrome
 Case 3 The use of proning in the management of Acute Respiratory Distress Syndrome Clinical Problem This expanded case summary has been chosen to explore the rationale and evidence behind the use of proning
Case 3 The use of proning in the management of Acute Respiratory Distress Syndrome Clinical Problem This expanded case summary has been chosen to explore the rationale and evidence behind the use of proning
11 th Annual Congress Turkish Thoracic Society. Mechanical Ventilation in Acute Hypoxemic Respiratory Failure
 11 th Annual Congress Turkish Thoracic Society Mechanical Ventilation in Acute Hypoxemic Respiratory Failure Lluis Blanch MD PhD Senior Critical Care Center Scientific Director Corporació Parc Taulí Universitat
11 th Annual Congress Turkish Thoracic Society Mechanical Ventilation in Acute Hypoxemic Respiratory Failure Lluis Blanch MD PhD Senior Critical Care Center Scientific Director Corporació Parc Taulí Universitat
Making vasopressors safer
 Making vasopressors safer Requirements for safe vaspressor use In an ideal world 1. Knowledge of what constitutes optimal vasopressor dosing 2. A culture of cautiousness regarding vasopressors What do
Making vasopressors safer Requirements for safe vaspressor use In an ideal world 1. Knowledge of what constitutes optimal vasopressor dosing 2. A culture of cautiousness regarding vasopressors What do
Sample Case Study. The patient was a 77-year-old female who arrived to the emergency room on
 Sample Case Study The patient was a 77-year-old female who arrived to the emergency room on February 25 th with a chief complaint of shortness of breath and a deteriorating pulmonary status along with
Sample Case Study The patient was a 77-year-old female who arrived to the emergency room on February 25 th with a chief complaint of shortness of breath and a deteriorating pulmonary status along with
Yu-Ching Lu, Ci Tan. O, and MEP > cmh 2
 Original Article Predictors of Weaning Failure in Patients with Chronic Obstructive Pulmonary Disease Yu-Ching Lu, Ci Tan Objective: To research the clinically ventilator weaning value of rapid shallow
Original Article Predictors of Weaning Failure in Patients with Chronic Obstructive Pulmonary Disease Yu-Ching Lu, Ci Tan Objective: To research the clinically ventilator weaning value of rapid shallow
APRV Ventilation Mode
 APRV Ventilation Mode Airway Pressure Release Ventilation A Type of CPAP Continuous Positive Airway Pressure (CPAP) with an intermittent release phase. Patient cycles between two levels of CPAP higher
APRV Ventilation Mode Airway Pressure Release Ventilation A Type of CPAP Continuous Positive Airway Pressure (CPAP) with an intermittent release phase. Patient cycles between two levels of CPAP higher
Outline. Basic principles of lung protective ventilation. The challenging areas. Small tidal volumes Recruitment
 ARDS beyond 6/kg Gordon D. Rubenfeld, MD MSc Professor of Medicine, University of Toronto Chief, Program in Trauma, Emergency, and Critical Care Sunnybrook Health Sciences Centre Outline Basic principles
ARDS beyond 6/kg Gordon D. Rubenfeld, MD MSc Professor of Medicine, University of Toronto Chief, Program in Trauma, Emergency, and Critical Care Sunnybrook Health Sciences Centre Outline Basic principles
Mechanical Ventilation of the Patient with Neuromuscular Disease
 Mechanical Ventilation of the Patient with Neuromuscular Disease Dean Hess PhD RRT Associate Professor of Anesthesia, Harvard Medical School Assistant Director of Respiratory Care, Massachusetts General
Mechanical Ventilation of the Patient with Neuromuscular Disease Dean Hess PhD RRT Associate Professor of Anesthesia, Harvard Medical School Assistant Director of Respiratory Care, Massachusetts General
Invasive mechanical ventilation is
 A randomized, controlled trial of the role of weaning predictors in clinical decision making* Maged A. Tanios, MD, MPH; Michael L. Nevins, MD; Katherine P. Hendra, MD; Pierre Cardinal, MD; Jill E. Allan,
A randomized, controlled trial of the role of weaning predictors in clinical decision making* Maged A. Tanios, MD, MPH; Michael L. Nevins, MD; Katherine P. Hendra, MD; Pierre Cardinal, MD; Jill E. Allan,
9/5/2018. Conflicts of Interests. Pediatric Acute Respiratory Distress Syndrome. Objectives ARDS ARDS. Definitions. None
 Pediatric Acute Respiratory Distress Syndrome Conflicts of Interests Diane C Lipscomb, MD Director Inpatient Pediatric Medical Director Mercy Springfield Associate Clerkship Clinical Director University
Pediatric Acute Respiratory Distress Syndrome Conflicts of Interests Diane C Lipscomb, MD Director Inpatient Pediatric Medical Director Mercy Springfield Associate Clerkship Clinical Director University
REVISTA BRASILEIRA DE ANESTESIOLOGIA
 Rev Bras Anestesiol. 2013;63(1):1-12 REVISTA BRASILEIRA DE ANESTESIOLOGIA Official Publication of the Brazilian Society of Anesthesiology www.sba.com.br/rba/index.asp SCIENTIFIC ARTICLE Respiratory Rate
Rev Bras Anestesiol. 2013;63(1):1-12 REVISTA BRASILEIRA DE ANESTESIOLOGIA Official Publication of the Brazilian Society of Anesthesiology www.sba.com.br/rba/index.asp SCIENTIFIC ARTICLE Respiratory Rate
NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP)
") Introduction NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP) Noninvasive ventilation (NIV) is a method of delivering oxygen by positive pressure mask that allows for the prevention or postponement of invasive
Introduction NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP) Noninvasive ventilation (NIV) is a method of delivering oxygen by positive pressure mask that allows for the prevention or postponement of invasive
Prone ventilation revisited in H1N1 patients
 International Journal of Advanced Multidisciplinary Research ISSN: 2393-8870 www.ijarm.com DOI: 10.22192/ijamr Volume 5, Issue 10-2018 Case Report DOI: http://dx.doi.org/10.22192/ijamr.2018.05.10.005 Prone
International Journal of Advanced Multidisciplinary Research ISSN: 2393-8870 www.ijarm.com DOI: 10.22192/ijamr Volume 5, Issue 10-2018 Case Report DOI: http://dx.doi.org/10.22192/ijamr.2018.05.10.005 Prone
Predictors of Successful Noninvasive Ventilation Treatment for Patients Suffering Acute Respiratory Failure
 ORIGINAL ARTICLE Predictors of Successful Noninvasive Ventilation Treatment for Patients Suffering Acute Respiratory Failure Ming-Shian Lin 1, How-Ran Guo 2,3, Ming-Hua Huang 4, Cheng-Ren Chen 1, Chen-Long
ORIGINAL ARTICLE Predictors of Successful Noninvasive Ventilation Treatment for Patients Suffering Acute Respiratory Failure Ming-Shian Lin 1, How-Ran Guo 2,3, Ming-Hua Huang 4, Cheng-Ren Chen 1, Chen-Long
New York Science Journal 2017;10(5)
") Value of Automatic Tube Compensation during Weaning of Mechanically Ventilated Patient in Medical Intensive Care Unit Mohamed Abouzeid. 1, Ahmed E. Kabil. 2, Ahmed Al-Ashkar 1 and Hafez A. Abdel-Hafeez
Value of Automatic Tube Compensation during Weaning of Mechanically Ventilated Patient in Medical Intensive Care Unit Mohamed Abouzeid. 1, Ahmed E. Kabil. 2, Ahmed Al-Ashkar 1 and Hafez A. Abdel-Hafeez
Ventilator-Associated Event Prevention: Innovations
 Ventilator-Associated Event Prevention: Innovations Michael J. Apostolakos, MD Professor of Medicine Director, Adult Critical Care University of Rochester Mobility/Sedation in the ICU Old teaching: Keep
Ventilator-Associated Event Prevention: Innovations Michael J. Apostolakos, MD Professor of Medicine Director, Adult Critical Care University of Rochester Mobility/Sedation in the ICU Old teaching: Keep
Definitions. Definitions. Weaning. Weaning. Disconnection (Discontinuation) Weaning
 Weaning") Definitions 2 Disconnection (Discontinuation) Implies patient no longer needs that form of therapy 80% of patients requiring temporary MVS do not require weaning Definitions 3 Implies some need for MVS
Definitions 2 Disconnection (Discontinuation) Implies patient no longer needs that form of therapy 80% of patients requiring temporary MVS do not require weaning Definitions 3 Implies some need for MVS
ECMO: a breakthrough in care for respiratory failure. PD Dr. Thomas Müller Regensburg no conflict of interest
 ECMO: a breakthrough in care for respiratory failure? PD Dr. Thomas Müller Regensburg no conflict of interest 1 Overview Mortality of severe ARDS Indication for ECMO PaO 2 /FiO 2 Efficiency of ECMO: gas
ECMO: a breakthrough in care for respiratory failure? PD Dr. Thomas Müller Regensburg no conflict of interest 1 Overview Mortality of severe ARDS Indication for ECMO PaO 2 /FiO 2 Efficiency of ECMO: gas
Sedation and delirium- drugs and clinical management
 Sedation and delirium- drugs and clinical management Shannon S. Carson, MD Associate Professor and Chief Division of Pulmonary and Critical Care Medicine University of North Carolina Probability of transitioning
Sedation and delirium- drugs and clinical management Shannon S. Carson, MD Associate Professor and Chief Division of Pulmonary and Critical Care Medicine University of North Carolina Probability of transitioning
NON-INVASIVE VENTILATION. Lijun Ding 23 Jan 2018
 NON-INVASIVE VENTILATION Lijun Ding 23 Jan 2018 Learning objectives What is NIV The difference between CPAP and BiPAP The indication of the use of NIV Complication of NIV application Patient monitoring
NON-INVASIVE VENTILATION Lijun Ding 23 Jan 2018 Learning objectives What is NIV The difference between CPAP and BiPAP The indication of the use of NIV Complication of NIV application Patient monitoring
The Impact of Patient-Ventilator. Karen J Bosma, MD, FRCPC Critical Care Medicine and Respirology
 Achieving Restful Ventilation: The Impact of Patient-Ventilator Interaction on Sleep Karen J Bosma, MD, FRCPC Critical Care Medicine and Respirology Disclosure Statement I have received a research grant
Achieving Restful Ventilation: The Impact of Patient-Ventilator Interaction on Sleep Karen J Bosma, MD, FRCPC Critical Care Medicine and Respirology Disclosure Statement I have received a research grant
Caring For the ICU Boarder. Kami M. Hu, MD Depts of Emergency & Internal Medicine University of Maryland SOM
 Caring For the ICU Boarder Kami M. Hu, MD Depts of Emergency & Internal Medicine University of Maryland SOM I have no relevant financial relationships with the manufacturer(s) of any commercial product(s)and/or
Caring For the ICU Boarder Kami M. Hu, MD Depts of Emergency & Internal Medicine University of Maryland SOM I have no relevant financial relationships with the manufacturer(s) of any commercial product(s)and/or
WEANING READINESS & SPONTANEOUS BREATHING TRIAL MONITORING
 CLINICAL EVIDENCE GUIDE WEANING READINESS & SPONTANEOUS BREATHING TRIAL MONITORING Weaning readiness and spontaneous breathing trial monitoring protocols can help you make the right weaning decisions at
CLINICAL EVIDENCE GUIDE WEANING READINESS & SPONTANEOUS BREATHING TRIAL MONITORING Weaning readiness and spontaneous breathing trial monitoring protocols can help you make the right weaning decisions at
Changes in Breathing Variables During a 30-Minute Spontaneous Breathing Trial
 Changes in Breathing Variables During a 30-Minute Spontaneous Breathing Trial Juan B Figueroa-Casas MD, Sean M Connery MSc, and Ricardo Montoya RRT BACKGROUND: Spontaneous breathing trials (SBTs) are increasingly
Changes in Breathing Variables During a 30-Minute Spontaneous Breathing Trial Juan B Figueroa-Casas MD, Sean M Connery MSc, and Ricardo Montoya RRT BACKGROUND: Spontaneous breathing trials (SBTs) are increasingly
Bronchoalveolar lavage (BAL) with surfactant in pediatric ARDS
 with surfactant in pediatric ARDS") Bronchoalveolar lavage (BAL) with surfactant in pediatric ARDS M. Luchetti, E. M. Galassini, A. Galbiati, C. Pagani,, F. Silla and G. A. Marraro gmarraro@picu.it www.picu.it Anesthesia and Intensive Care
Bronchoalveolar lavage (BAL) with surfactant in pediatric ARDS M. Luchetti, E. M. Galassini, A. Galbiati, C. Pagani,, F. Silla and G. A. Marraro gmarraro@picu.it www.picu.it Anesthesia and Intensive Care
Post Arrest Ventilation/Oxygenation Management
 Post Arrest Ventilation/Oxygenation Management Richard Branson MSc RRT Professor of Surgery University of Cincinnati Editor-In-Chief Respiratory Care 0 Presenter Disclosure Information Richard Branson
Post Arrest Ventilation/Oxygenation Management Richard Branson MSc RRT Professor of Surgery University of Cincinnati Editor-In-Chief Respiratory Care 0 Presenter Disclosure Information Richard Branson
Proportional Assist Ventilation (PAV) (NAVA) Younes ARRD 1992;145:114. Ventilator output :Triggering, Cycling Control of flow, rise time and pressure
 (NAVA) Younes ARRD 1992;145:114. Ventilator output :Triggering, Cycling Control of flow, rise time and pressure") Conflict of Interest Disclosure Robert M Kacmarek Unconventional Techniques Using Your ICU Ventilator!" 5-5-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston,
Conflict of Interest Disclosure Robert M Kacmarek Unconventional Techniques Using Your ICU Ventilator!" 5-5-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston,
Early Rehabilitation in the ICU: Do We Still Need Chest Physiotherapy?
 Early Rehabilitation in the ICU: Do We Still Need Chest Physiotherapy? Michelle Kho, PT, PhD Assistant Professor, School of Rehabilitation Science, McMaster University Adjunct Assistant Professor, Department
Early Rehabilitation in the ICU: Do We Still Need Chest Physiotherapy? Michelle Kho, PT, PhD Assistant Professor, School of Rehabilitation Science, McMaster University Adjunct Assistant Professor, Department
Update in Hospital Medicine
 Update in Hospital Medicine 2017-2018 Brad Sharpe, MD SFHM UCSF Division of Hospital Medicine 2017-2018 Updated literature March 2017 March 2018 Process: CME collaborative review of journals Including
Update in Hospital Medicine 2017-2018 Brad Sharpe, MD SFHM UCSF Division of Hospital Medicine 2017-2018 Updated literature March 2017 March 2018 Process: CME collaborative review of journals Including
APPENDIX VI HFOV Quick Guide
 APPENDIX VI HFOV Quick Guide Overall goal: Maintain PH in the target range at the minimum tidal volume. This is achieved by favoring higher frequencies over lower P (amplitude). This goal is also promoted
APPENDIX VI HFOV Quick Guide Overall goal: Maintain PH in the target range at the minimum tidal volume. This is achieved by favoring higher frequencies over lower P (amplitude). This goal is also promoted
Variation in the Rapid Shallow Breathing Index Associated With Common Measurement Techniques and Conditions
 Variation in the Rapid Shallow Breathing Index Associated With Common Measurement Techniques and Conditions Kapil N Patel MD, Kalpesh D Ganatra MD, Jason HT Bates PhD, and Michael P Young MD BACKGROUND:
Variation in the Rapid Shallow Breathing Index Associated With Common Measurement Techniques and Conditions Kapil N Patel MD, Kalpesh D Ganatra MD, Jason HT Bates PhD, and Michael P Young MD BACKGROUND:
Weaning from Mechanical Ventilation
 CHAPTER 47 Victor Kim and Gerard J. Criner Weaning from Mechanical Ventilation CHAPTER OUTLINE Learning Objectives Case Study Determining the Cause of Respiratory Failure When is the Patient Ready to Wean?
CHAPTER 47 Victor Kim and Gerard J. Criner Weaning from Mechanical Ventilation CHAPTER OUTLINE Learning Objectives Case Study Determining the Cause of Respiratory Failure When is the Patient Ready to Wean?
ARDS Assisted ventilation and prone position. ICU Fellowship Training Radboudumc
 ARDS Assisted ventilation and prone position ICU Fellowship Training Radboudumc Fig. 1 Physiological mechanisms controlling respiratory drive and clinical consequences of inappropriate respiratory drive
ARDS Assisted ventilation and prone position ICU Fellowship Training Radboudumc Fig. 1 Physiological mechanisms controlling respiratory drive and clinical consequences of inappropriate respiratory drive
What is the next best step?
 Noninvasive Ventilation William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center What is the next best step? 65 year old female
Noninvasive Ventilation William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center What is the next best step? 65 year old female
Non-invasive Positive Pressure Mechanical Ventilation: NIPPV: CPAP BPAP IPAP EPAP. My Real Goals. What s new in 2018? OMG PAP?
 Non-invasive Positive Pressure Mechanical Ventilation: What s new in 2018? Geoffrey R. Connors, MD, FACP Associate Professor of Medicine University of Colorado School of Medicine Division of Pulmonary
Non-invasive Positive Pressure Mechanical Ventilation: What s new in 2018? Geoffrey R. Connors, MD, FACP Associate Professor of Medicine University of Colorado School of Medicine Division of Pulmonary
APHACHE Score as a Predictive Indices for Weanability from Mechanical Ventilation
 ; 1: 18-22 Original Article APHACHE Score as a Predictive Indices for Weanability from Mechanical Ventilation Md. Sayedul Islam Abstract: Objective: To determine the significance of acute physiology and
; 1: 18-22 Original Article APHACHE Score as a Predictive Indices for Weanability from Mechanical Ventilation Md. Sayedul Islam Abstract: Objective: To determine the significance of acute physiology and
Approach to type 2 Respiratory Failure
 Approach to type 2 Respiratory Failure Changing Nature of NIV Not longer just the traditional COPD patients Increasingly Obesity Neuromuscular Pneumonias 3 fold increase in patients with Ph 7.25 and below
Approach to type 2 Respiratory Failure Changing Nature of NIV Not longer just the traditional COPD patients Increasingly Obesity Neuromuscular Pneumonias 3 fold increase in patients with Ph 7.25 and below
An Overview of the Chronic Critical Illness Syndrome (CCIS) and Weaning the PMV Patient
 and Weaning the PMV Patient") An Overview of the Chronic Critical Illness Syndrome (CCIS) and Weaning the PMV Patient Fall 2011 CCIS has been known for some time HISTORICAL PRECURSORS INCLUDE: SIRS Systemic Inflammatory Response Syndrome
An Overview of the Chronic Critical Illness Syndrome (CCIS) and Weaning the PMV Patient Fall 2011 CCIS has been known for some time HISTORICAL PRECURSORS INCLUDE: SIRS Systemic Inflammatory Response Syndrome
Cardiorespiratory Interactions:
 Cardiorespiratory Interactions: The Heart - Lung Connection Jon N. Meliones, MD, MS, FCCM Professor of Pediatrics Duke University Medical Director PCVICU Optimizing CRI Cardiorespiratory Economics O2:
Cardiorespiratory Interactions: The Heart - Lung Connection Jon N. Meliones, MD, MS, FCCM Professor of Pediatrics Duke University Medical Director PCVICU Optimizing CRI Cardiorespiratory Economics O2:
KICU Spontaneous Awakening Trial (SAT) Questionnaire
 Questionnaire") KICU Spontaneous Awakening Trial (SAT) Questionnaire Please select your best answer(s): 1. What is your professional role? 1 Staff Nurse 2 Nurse Manager 3 Nurse Educator 4 Physician 5 Medical Director
KICU Spontaneous Awakening Trial (SAT) Questionnaire Please select your best answer(s): 1. What is your professional role? 1 Staff Nurse 2 Nurse Manager 3 Nurse Educator 4 Physician 5 Medical Director
ARDS: The Evidence. Topics. New definition Breaths: Little or Big? Wet or Dry? Moving or Still? Upside down or Right side up?
 ARDS: The Evidence Todd M Bull MD Professor of Medicine Division of Pulmonary Sciences and Critical Care Division of Cardiology Director Pulmonary Vascular Disease Center Director Center for Lungs and
ARDS: The Evidence Todd M Bull MD Professor of Medicine Division of Pulmonary Sciences and Critical Care Division of Cardiology Director Pulmonary Vascular Disease Center Director Center for Lungs and
Can Goal Directed Sedation Improve Outcomes?
 Can Goal Directed Sedation Improve Outcomes? Yahya SHEHABI, FANZCA, FCICM, EMBA Professor and Program Director Critical care Monash Health and Monash University - Melbourne School of Medicine, University
Can Goal Directed Sedation Improve Outcomes? Yahya SHEHABI, FANZCA, FCICM, EMBA Professor and Program Director Critical care Monash Health and Monash University - Melbourne School of Medicine, University
Learning Objectives. 1. Indications versus contra-indications 2. CPAP versus NiVS 3. Clinical evidence
 Learning Objectives 1. Indications versus contra-indications 2. CPAP versus NiVS 3. Clinical evidence Pre-hospital Non-invasive vventilatory support Marc Gillis, MD Imelda Bonheiden Our goal out there
Learning Objectives 1. Indications versus contra-indications 2. CPAP versus NiVS 3. Clinical evidence Pre-hospital Non-invasive vventilatory support Marc Gillis, MD Imelda Bonheiden Our goal out there
Tailored Volume Resuscitation in the Critically Ill is Achievable. Objectives. Clinical Case 2/16/2018
 Tailored Volume Resuscitation in the Critically Ill is Achievable Heath E Latham, MD Associate Professor Fellowship Program Director Pulmonary and Critical Care Objectives Describe the goal of resuscitation
Tailored Volume Resuscitation in the Critically Ill is Achievable Heath E Latham, MD Associate Professor Fellowship Program Director Pulmonary and Critical Care Objectives Describe the goal of resuscitation
Oxygenation Failure. Increase FiO2. Titrate end-expiratory pressure. Adjust duty cycle to increase MAP. Patient Positioning. Inhaled Vasodilators
 Oxygenation Failure Increase FiO2 Titrate end-expiratory pressure Adjust duty cycle to increase MAP Patient Positioning Inhaled Vasodilators Extracorporeal Circulation ARDS Radiology Increasing Intensity
Oxygenation Failure Increase FiO2 Titrate end-expiratory pressure Adjust duty cycle to increase MAP Patient Positioning Inhaled Vasodilators Extracorporeal Circulation ARDS Radiology Increasing Intensity
STATE OF OKLAHOMA 2014 EMERGENCY MEDICAL SERVICES PROTOCOLS
 3K NON-INVASIVE POSITIVE PRESSURE VENTILATION (NIPPV) ADULT EMT EMT-INTERMEDIATE 85 ADVANCED EMT PARAMEDIC Indications: 1. Dyspnea Uncertain Etiology Adult. 2. Dyspnea Asthma Adult. 3. Dyspnea Chronic
3K NON-INVASIVE POSITIVE PRESSURE VENTILATION (NIPPV) ADULT EMT EMT-INTERMEDIATE 85 ADVANCED EMT PARAMEDIC Indications: 1. Dyspnea Uncertain Etiology Adult. 2. Dyspnea Asthma Adult. 3. Dyspnea Chronic
ARF, Mechaical Ventilation and PFTs: ACOI Board Review 2018
 ARF, Mechaical Ventilation and PFTs: ACOI Board Review 2018 Thomas F. Morley, DO, FACOI, FCCP, FAASM Professor of Medicine Chairman Department of Internal Medicine Director of the Division of Pulmonary,
ARF, Mechaical Ventilation and PFTs: ACOI Board Review 2018 Thomas F. Morley, DO, FACOI, FCCP, FAASM Professor of Medicine Chairman Department of Internal Medicine Director of the Division of Pulmonary,
P-2 EXTUBATION CHECKLIST - A CALL FOR 'MANDATORY' IMPLEMENTATION Collins, Donna 1
 P-2 EXTUBATION CHECKLIST - A CALL FOR 'MANDATORY' IMPLEMENTATION Collins, Donna 1 1 Quality Risk Management, Critical Care Education, Crystal Clear Transitional Care Inc., Saint John, New Brunswick, Canada
P-2 EXTUBATION CHECKLIST - A CALL FOR 'MANDATORY' IMPLEMENTATION Collins, Donna 1 1 Quality Risk Management, Critical Care Education, Crystal Clear Transitional Care Inc., Saint John, New Brunswick, Canada
Lecture Notes. Chapter 2: Introduction to Respiratory Failure
 Lecture Notes Chapter 2: Introduction to Respiratory Failure Objectives Define respiratory failure, ventilatory failure, and oxygenation failure List the causes of respiratory failure Describe the effects
Lecture Notes Chapter 2: Introduction to Respiratory Failure Objectives Define respiratory failure, ventilatory failure, and oxygenation failure List the causes of respiratory failure Describe the effects