Central Sleep Apnea. v Characteristics
|
|
|
- Russell Miles
- 5 years ago
- Views:
Transcription
1 Central Sleep Apnea v Characteristics Respiratory pauses > 10 sec Due to failure of brain s respiratory center to send signal to respiratory muscles Tends to occur in infants (neurological immaturity) or elderly (stroke, neurodegenerative disorder) 1
2 Obstructive Sleep Apnea v 1-4% of population v Pickwick Papers (1837) v Osler (1906) v Guilleminault (1973) - OSAS 2
3 Obstructive Sleep Apnea (OSA) v Characteristics Respiratory pauses > 10 sec (usually longer) Due to upper airway blockage that prevents passage of air Most common form; tends to occur in middle- aged males who are obese or who have physiologically narrow airways 3
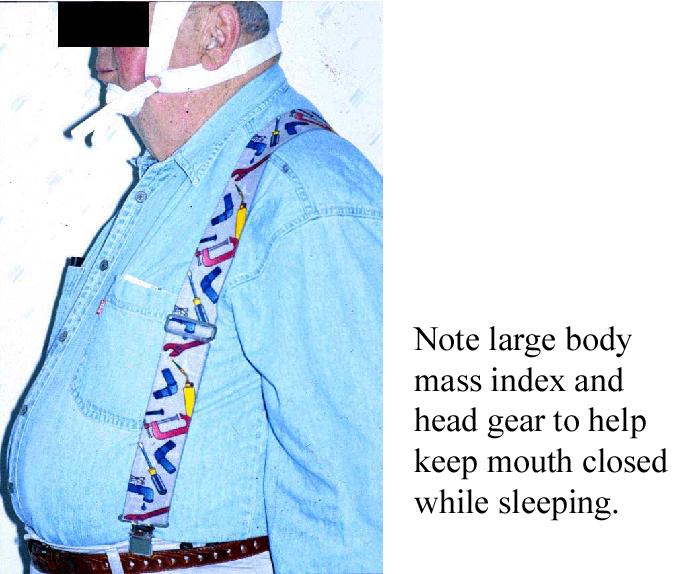
4 Symptoms of OSA v Snoring Loud snoring usually worse when sleeping on back or after alcohol use; breathing pattern may demonstrate periods of silence broken by snorting or gasping v Obesity Body Mass Index > 35 and collar size > 16.5 in correlate with OSA v Daytime sleepiness May report falling asleep at work, while driving, or during sedentary activities 4
5 Associated Symptoms v Mood changes, memory problems, decreased sex drive, nighttime sweating, increased urination at night, heartburn, waking with a dry mouth v Patient may have micrognathia, retrognathia, large tongue, enlarged uvula, crowded airway, difficulty breathing through nostrils v Important to interview bed partner to obtain full symptom picture 5
6 History v Snoring* v Excessive daytime sleepiness* v Restless sleep v Personality changes v Headaches v Sexual dysfunction v Job performance v Sleep hygiene v Bed partner s input * 6
7 Pathophysiology v Pharyngeal collapse v Decreased airway patency v Increase in negative pressure v Becomes a vicious cycle 7
8 v Anatomic narrowing Pathophysiology Requires increased inspiratory pressures v Abnormal neuromuscular control Reflex activation of dilators in response to airway obstruction often fails 8
9 9
10 Diagnosis of OSA v Apnea Complete cessation of breathing > 10 sec v Hypopnea Partial reduction of airflow by > 30% v Oxygen desaturation Oxygen desaturation > 4% from sleep baseline 10
11 Diagnosis of OSA (con t) v Apnea-Hypopnea Index (AHI) Total number of apneas and hypopneas divided by number of hours slept o o o Mild OSA: AHI = 5 14 events per hour Moderate OSA: AHI = events per hour Severe OSA: AHI = 30+ events per hour v Also considered in diagnosis are: Number and severity of oxygen desaturation episodes Number of awakenings Severity of daytime symptoms 11
12 Normal Vs. Disordered Breathing v A few brief respiratory pauses are normal: During transition from wakefulness to sleep During REM sleep when there is a profound loss of muscle tone v OSA is progressive: 1. Intermittent snoring and mild breathing problems 2. Snoring and mild to moderate respiratory pauses 3. Long respiratory pauses, severe drops in oxygen, many arousals during sleep 12
13 Epidemiology of OSA v Prevalence of OSA: 2-9% of women (more frequent postmenopausally) 4-24% of men 32% of men and 19% of women snore nightly v OSA is associated with cardiovascular disorders Hypertension, stroke v Risk factors: Smoking, alcohol use, poor eating habits/obesity 13
14 Epidemiology of OSA (con t) v Social impact: Reduced work productivity Increased rate of automobile accidents Marital stress v Typical presentation: Obese, middle-aged males BUT, OSA can occur in either gender, any age, and any body type 14
15 APNEAS Ì Í Ó HYPOXEMIA Í SLEEP Ó Ó Í DISRUPTION Ó Í Ì Ì Ó DAYTIME Ì SOMNOLENCE Ì Ó Í COGNITIVE Ì DEFICITS 15
16 NATURE OF COGNITIVE DEFICITS  General intellectual functioning  Attention/Vigilance  Memory  Executive function  Manual dexterity 16
17 NOCTURNAL SLEEP IN OSAS CONTROLS BASELINE APNEICS A B Sleep % Wakening 10.7 (6.1) 12.7 (9.4) % Stage (3.6) 33.4 (21.7) % Stage (6.4) 54.0 (20.8) % SWS 10.6 (5.8) 2.5 (3.1) % REM 15.2 (5.9) 9.9 (3.4) Nb of awakenings 33.7 (11.1) 75.7 (55.0) Nb of stage shifts (34.7) (222.3) From Bédard,et al. Sleep
18 COGNITIVE DEFICITS IN OSAS CONTROLS BASELINE A B General functioning Full Scale IQ (8.1) (8.9) Verbal IQ (9.2) (9.9) Performance IQ (7.4) (7.9) Attention Digit Symbol 8.5 (2.1) 7.2 (1.2) Letter Cancellation 1.1 (0.6) 4.0 (3.2) Memory Rey fig. (Imm.) 22.9 (5.0) 18.7 (4.7) Rey fig. (Del.) 21.2 (4.8) 16.5 (5.1) Story WMS (Imm.) 9.7 (1.4) 8.6 (1.7) Story loss WMS 1.2 (1.1) 2.9 (1.9) 18
19 COGNITIVE DEFICITS IN OSAS CONTROLS BASELINE A B Executive functions Rey fig. copy 31.2 ( (3.5) Block design 10.1 (2.7) 8.4 (2.0) Pict. Arrangement 11.0 (1.2) 6.9 (1.6) Mazes (err.) 0.7 (0.8) 3.6 (1.2) Trail B (sec) 70.4 (23.3) 95.4 (33.2) Verbal fluency 40.2 (11.2) 28.2 (9.9) Manual dexteriry Purdue pegboard 15.2 (0.8) 11.9 (1.1) From Bédard,et al. Sleep

20 20
21 21
22 22
23 23

24 24
25 Examination v Tongue v Palate v Uvula v Tonsils v Nasal cavity v Hyoid v Mandible v Maxilla 25

26 26

27 27

28 28
29 29

30 30


31 31

32 32

33 33

34 34

35 35

36 36

37 37
38 38
39 LOC ROC 39 39



40 Differential Amplifier Differential Amplifier Anterior Tibialis EMG Differential Amplifier 40 Sleep Aca demic Awa rd 40
41 41
42 42
43 43
44 44
45 45
46 46
47 47
48 48
49 49
50 50
51 51
52 Treatment v Nonsurgical modalities v Surgical modalities 52
53 Nonsurgical Treatment v Weight loss v Sleep hygiene v Pharmacotherapy v Nasal continuous positive airway pressure v Oral appliances 53
54 Surgical Treatments for OSA v Tracheostomy Drastic option for patients whose breathing is severely compromised (morbidly obese, hypoxemic, or emergency status) v UPPP (uvulopalatopharyngeoplasty) Removes uvula and upper airway soft tissue Reduced AHI by half in only 30-50% of cases v LAUPP (out-patient, laser assisted UPPP) No more successful than UPPP Best indication for snorers with no or mild OSA 54
55 Surgical Treatments (con t) v Cranialfacial surgery: Reshape facial bones v Radio frequency ablation (RFA): Stiffen soft tissue to reduce flutter, reduce tongue thickness, or shrink nasal turbinates Best indication for snorers with no or mild OSA Long term effectiveness unknown v Gastric bypass to reduce obesity: Patients may show a return of sleep apnea 55
56 Surgical Treatments (con t) v Other surgical options designed to improve airway patency: Tonsillectomy Adenoidectomy Correction of deviated nasal septum 56
57 Mechanical Treatments v Nasal CPAP most successful and common treatment Pressurized air delivery via nasal mask (or pillows ) attached by tubing to a compressor v Oral Appliances (mouth pieces) Purpose is to either hold the tongue forward or move the lower jaw forward 80% effective in controlling snoring and mild to moderate OSA; 30% effective in severe OSA Best results for positional apnea 57
58 CPAP THERAPY m Most successful and commonly used medical treatment m Normalizes sleep architecture and abolishes nocturnal hypoxemia m Improves EDS and cognitive functioning m Residual EDS and deficits in executive functions 58

59 59

60 CPAP 60
61 NOCTURNAL SLEEP IN OSAS: Effect of CPAP CONTROLS BASELINE TREATED p APNEICS APNEICS A B C B-C Sleep % Wakening 10.7 (6.1) 12.7 (9.4) 12.9 (3.3) NS % Stage (3.6) 33.4 (21.7) 17.0 (6.5) * % Stage (6.4) 54.0 (20.8) 59.8 (9.4) NS % SWS 10.6 (5.8) 2.5 (3.1) 8.6 (7.0) * % REM 15.2 (5.9) 9.9 (3.4) 15.5 (6.1) ** Nb of awakenings 33.7 (11.1) 75.7 (55.0) 31.7 (15.7) * Nb of stage shifts (34.7) (222.3) (70.7) * From Bédard,et al. Sleep
62 COGNITIVE DEFICITS IN OSAS: Effect of CPAP CONTROLS BASELINE APNEICS TREATED p APNEICS p A B C B-C A-C General functioning Full Scale IQ (8.1) (8.9) (8.7) *** NS Verbal IQ (9.2) (9.9) (8.6) NS NS Performance IQ (7.4) (7.9) (7.9) *** NS Attention Digit Symbol 8.5 (2.1) 7.2 (1.2) 8.9 (1.8) ** NS Letter Cancellation 1.1 (0.6) 4.0 (3.2) 1.5 (4.6) * NS Memory Rey fig. (Imm.) 22.9 (5.0) 18.7 (4.7) 19.4 (6.3) NS NS Rey fig. (Del.) 21.2 (4.8) 16.5 (5.1) 17.2 (7.1) NS NS Story WMS (Imm.) 9.7 (1.4) 8.6 (1.7) 10.8 (3.2) * NS Story loss WMS 1.2 (1.1) 2.9 (1.9) 1.5 (1.3) * NS 62
63 COGNITIVE DEFICITS IN OSAS: Effect of CPAP CONTROLS BASELINE TREATED p p APNEICS APNEICS A B C B-C A-C Executive functions Rey fig. copy 31.2 ( (3.5) 30.5 (2.4) ** NS Block design 10.1 (2.7) 8.4 (2.0) 10.5 (1.9) ** NS Pict. Arrangement 11.0 (1.2) 6.9 (1.6) 8.8 (2.2) ** * Mazes (err.) 0.7 (0.8) 3.6 (1.2) 2.8 (1.0) * ** Trail B (sec) 70.4 (23.3) 95.4 (33.2) 88.0 (14.3) NS * Verbal fluency 40.2 (11.2) 28.2 (9.9) 29.9 (14.5) NS * Manual dexteriry Purdue pegboard 15.2 (0.8) 11.9 (1.1) 13.5 (1.4) ** NS From Bédard,et al. Sleep
64 CPAP Compliance v Two main issues with adherence: 1. Drop outs: o 5-30% of patients discontinue using CPAP 2. Failure to use CPAP as prescribed: o About 50% of patients use CPAP at a minimally acceptable level,, defined as at least 4hrs on 70% of nights o Average usage rates are hrs per night, which is probably less than optimal 64
65 Improving CPAP Compliance v Supportive and cognitive-behavioral techniques are moderately successful Support groups, verbal reinforcement strategies, patient education programs, bibliotherapy, motivational interviewing, systematic desensitization, sensory awareness techniques Systematic desensitization helps prevent discontinuation of CPAP Motivational interviewing is most promising for increasing nightly use time 65

66 Nonsurgical Treatment v Weight loss Get below trigger weight Diet, exercise, bariatric surgery, medications v Sleep hygiene Avoidance of sedatives Positional changes 66
67 Alternative Treatment Strategies v Combined surgical and mechanical treatments Oral appliance may be beneficial after a surgical option that opens nasal airway v Pharmacological treatments There are no successful respiratory stimulants REM suppressants may be beneficial for patients with REM-related apnea 67
68 Behavioral Treatments for OSA v Sleep position training v Weight loss v Modifying lifestyle behaviors Increasing exercise Reducing alcohol use Quitting smoking 68
69 Sleep Position Training v Tennis ball therapy (T-shirt method) Sewn tennis ball to back of pajama top makes supine position uncomfortable May be effective in controlling snoring Few studies have tested the effectiveness of this method, but one study showed a lowering of blood pressure 69
70 Sleep Position Training (con t) v Posture alarm (position monitor) Not all patients can be successfully trained to refrain from supine sleep after using this device for 8 weeks It is unknown how long this training can be maintained without reinforcement In one study of positional OSA, patients showed the best outcome when this treatment was combined with an oral appliance. Patients who were more obese and who had more severe apnea had least successful outcomes 70
71 Weight Loss v Difficult and slow process Patient may require alternative treatment such as CPAP while losing weight Patient often benefits from group treatment and support of spouse in changing eating behaviors Patient should abstain from alcohol use o o High caloric content Reduces tone of upper airway muscles, causing louder and more frequent snoring as well as increased number and length of respiratory pauses 71
72 Weight Loss Rules v Keep a daily record v Eat 3 meals a day with no snacks v Drink water and avoid soft drinks v Reduce portion size v Slow down eating v Stop eating when full v Don t skip breakfast 72
73 Exercise v Using CPAP may provide patient with more energy to engage in physical activities Ways to increase activity: o Take a walk at lunch time o Use stairs instead of elevator o Park farther away from your destination o Ride a bicycle o Stand up when talking on the phone 73
74 Smoking v Patient must be motivated v Probability of success is increased by a program combining behavior change with pharmacological elements 74
75 EFFICACIA DEI TRATTAMENTI 75
76 Obstructive Sleep Apnea Syndrome (OSAS) v Primary goal is to eliminate sleep disordered breathing (SDB) Most behavioral intervention studies have used Apnea Hypopnea Index (AHI) as the primary outcome v Obesity is a major risk factor Adipose tissue in the upper airway Hypotonality of airway dilating muscles Reduced residual lung volume 76
77 Weight Loss for OSAS v Weight loss is a conservative intervention Weight loss reduces the amount of adipose tissue in the oropharynx, improves airway caliber, reduces airway collapsibility, increases residual volume in the lungs and reduces respiratory effort Significant and maintained weight loss can cure OSAS Most effective approach involves a multidisciplinary team, frequent provider contacts, and regular physical activity 77
78 Weight Loss for OSAS (con t) v Most studies investigating weight loss in OSAS patients are uncontrolled with small sample sizes v Collectively, weight loss studies have yielded the following findings: A decrease in weight is associated with a disproportionately larger decrease in apnea events o Peppard et al.: Each percentage change in weight was associated with an approximate 3% change in the AHI 78
79 Weight Loss for OSAS (con t) v Weight loss findings: Weight loss through diet alone or diet and exercise is associated with the following: o o o o o o o o o Reduction in AHI/RDI/SDB and snoring frequency Improved oxygenation Improved daytime sleepiness, mood, and quality of life Improved global measures of sleep Improved blood pressure Improved lung vital capacity and functional residual capacity Improved resistance to upper airway collapse Increased upper airway pressure Decreased soft palate width 79
80 Weight Loss for OSAS (con t) v Weight loss findings (con t): For mild to moderate OSAS, physical conditioning may have an additional or synergistic benefit with weight loss The benefits of weight loss are evident in patients with varying severity of sleep apnea and baseline body weight Studies using weight loss as a conservative control treatment to evaluate CPAP efficacy: o Weight loss was associated with improved AHI. Weight loss patients showed comparable improvement as the CPAP group on steer-clear task and cognitive tests 80
81 Weight Loss for OSAS (con t) v Weight loss findings (con t): Long-term weight loss: o o o Some patients are cured of OSA and/or snoring Relapse of OSAS (by weight gain) is frequent among those previously cured by dietary weight loss (only half of patients remain cured) An individual s response to weight loss is highly variable Weight loss in morbidly obese OSA patients: o Moderate weight loss can lead to substantial improvement in SDB. However, this is not sufficient to produce significant clinical improvement to be used as the primary treatment in morbidly obese patients with severe OSAS 81
82 Weight Loss for OSAS (con t) v Summary of weight loss findings: Weight loss has a beneficial effect on SDB Modest weight loss is likely to reduce the severity of SDB and the risk of developing clinically significant OSAS Even a small degree of weight loss is associated with decreased snoring, decreased AHI, and decreased collapsibility of the airway Weight loss is efficacious in the short-term, but long- term benefits remain to be established The combination of weight loss with other behavioral interventions may be beneficial 82
83 Positional Sleep Apnea v Frequency and severity of SDB is influenced by position in 50-60% of patients v AHI in OSAS patients may be twice as high in supine position compared to lateral position v Positional Sleep Apnea Syndrome: The phenomena in which the AHI during supine sleep position is 2 or more times the AHI during lateral sleep position 83
84 Sleep Position Training for OSAS v Sleep position training for positional sleep apnea Interventions that decrease time spent in supine sleep position should o o Diminish the impact of obesity on the residual capacity of the lungs Reduce the effort required for the mechanics of respiration Positional therapy is a conservative intervention indicated for non-obese patients with position- dependent SDB who don t have significant associated pathologies (oxygen desaturation, cardiac arrhythmias, excessive daytime sleepiness) 84
85 Sleep Position Training for OSAS (con t) v Positional sleep training methods Tennis ball, backpack and softball, foam rubber wedges or sandbag placements, position monitoring device (alarm), elevated upright sleeping position v Position monitoring device (Cartwright et al.) Significantly increased the proportion of total sleep time that the patients spent in the lateral positions Intervention was associated with decreases in the AHI and the number of oxygen desaturation events Learning from one-night positional training was maintained at 3 months in some patients 85
86 Sleep Position Training for OSAS (con t) v Instructions to avoid supine sleep (Cartwright et al.) Patients instructed to diet, exercise, avoid alcohol, and avoid supine sleep (compared to position monitoring alarm group): o o o Showed greater improvement in AHI and comparable ability to avoid supine position The findings support the therapeutic benefit of avoiding the supine position Some patients can learn to avoid supine posture on their own 86
87 Sleep Position Training for OSAS (con t) v Elevated upright sleeping position (McEvoy et al.) Compared to supine sleep, the 60-degree position sleep was associated with a reduction in the AHI and did not disrupt sleep architecture Obese patients and patients who show greater degree of hypoxemia had greater response to this intervention than non-obese patients Significant reduction of SDB can be facilitated by the adoption of a more upright sleep posture 87
88 Sleep Position Training for OSAS (con t) v Foam rubber wedges to maintain lateral sleeping position in snorers (Braver and Block) Resulted in 19% reduction of AHI Snoring was not improved by this intervention v Backpack and softball (Jovic et al.) Significantly reduced time spent in supine position Showed similar improvements in sleep architecture, arousal frequency, daytime sleepiness, mood, and cognitive tests as CPAP Reduced AHI, but not as much as CPAP 88
89 Sleep Position Training for OSAS (con t) v Summary of efficacy studies Although there are only a handful of studies on the efficacy of positional therapy, findings consistently support the therapeutic benefits of this intervention for persons with positional sleep apnea syndrome o o Positional training is a promising noninvasive, inexpensive treatment either as an interim, single therapy, or in combination with other therapies Some benefits of positional intervention may be comparable to that provided by CPAP therapy. Positional therapy may be an effective alternative treatment to CPAP, at least for the short term 89
90 Alternative Therapies for OSAS v Cervical Positional Therapy (Kushida et al.) A custom-designed cervical pillow designed to extend head position to modify upper airway Subjects reported subjective sleep improvement Objective benefits only in patients with mild disease More studies are needed to establish the efficacy of this intervention v Myofunctional Therapy Targets improving tone of the upper airway muscles Has not been scientifically tested 90
91 Alternative Therapies for OSAS (con t) v Sleep Hygiene No published studies on the efficacy of this as a single intervention Alcohol and SDB o o No studies show that eliminating alcohol reduces SDB Studies have demonstrated that alcohol ingestion near bedtime exacerbates SDB (increases apneas and hypoxic events) and can cause male snorers to develop apnea Sleep deprivation o Sleep deprivation may increase severity of OSA, but no studies show that obtaining adequate sleep improves SDB 91
Snoring. Forty-five percent of normal adults snore at least occasionally and 25
 Snoring Insight into sleeping disorders and sleep apnea Forty-five percent of normal adults snore at least occasionally and 25 percent are habitual snorers. Problem snoring is more frequent in males and
Snoring Insight into sleeping disorders and sleep apnea Forty-five percent of normal adults snore at least occasionally and 25 percent are habitual snorers. Problem snoring is more frequent in males and
BTS sleep Course. Module 10 Therapies I: Mechanical Intervention Devices (Prepared by Debby Nicoll and Debbie Smith)
") BTS sleep Course Module 10 Therapies I: Mechanical Intervention Devices (Prepared by Debby Nicoll and Debbie Smith) S1: Overview of OSA Definition History Prevalence Pathophysiology Causes Consequences
BTS sleep Course Module 10 Therapies I: Mechanical Intervention Devices (Prepared by Debby Nicoll and Debbie Smith) S1: Overview of OSA Definition History Prevalence Pathophysiology Causes Consequences
Sleep Disordered Breathing
 Sleep Disordered Breathing SDB SDB Is an Umbrella Term for Many Disorders characterized by a lack of drive to breathe Results n repetitive pauses in breathing with no effort Occurs for a minimum of 10
Sleep Disordered Breathing SDB SDB Is an Umbrella Term for Many Disorders characterized by a lack of drive to breathe Results n repetitive pauses in breathing with no effort Occurs for a minimum of 10
Obstructive Sleep Apnea
 Obstructive Sleep Apnea Introduction Obstructive sleep apnea is an interruption in breathing during sleep. It is caused by throat and tongue muscles collapsing and relaxing. This blocks, or obstructs,
Obstructive Sleep Apnea Introduction Obstructive sleep apnea is an interruption in breathing during sleep. It is caused by throat and tongue muscles collapsing and relaxing. This blocks, or obstructs,
Medicare C/D Medical Coverage Policy
 Medicare C/D Medical Coverage Policy Surgical Treatment of Obstructive Sleep Apnea Origination: June 26, 2000 Review Date: January 18, 2017 Next Review January, 2019 DESCRIPTION OF PROCEDURE OR SERVICE
Medicare C/D Medical Coverage Policy Surgical Treatment of Obstructive Sleep Apnea Origination: June 26, 2000 Review Date: January 18, 2017 Next Review January, 2019 DESCRIPTION OF PROCEDURE OR SERVICE
in China Shanghai Office Beijing Office (+86) (+86)
 (+86)") SLEEP Apnea in China Guide 2018-2019 Shanghai Office (+86) 21 2426 6400 Beijing Office (+86) 010 6464 0611 www.pacificprime.cn Follow us on WeChat t A comprehensive overview of sleep apnea Perhaps you
SLEEP Apnea in China Guide 2018-2019 Shanghai Office (+86) 21 2426 6400 Beijing Office (+86) 010 6464 0611 www.pacificprime.cn Follow us on WeChat t A comprehensive overview of sleep apnea Perhaps you
Sleep Diordered Breathing (Part 1)
") Sleep Diordered Breathing (Part 1) History (for more topics & presentations, visit ) Obstructive sleep apnea - first described by Charles Dickens in 1836 in Papers of the Pickwick Club, Dickens depicted
Sleep Diordered Breathing (Part 1) History (for more topics & presentations, visit ) Obstructive sleep apnea - first described by Charles Dickens in 1836 in Papers of the Pickwick Club, Dickens depicted
Tired of being tired?
 Tired of being tired? Narval CC MRD ResMed.com/Narval Sleepiness and snoring are possible symptoms of sleep apnea. Did you know that one in every four adults has some form of sleep disordered-breathing
Tired of being tired? Narval CC MRD ResMed.com/Narval Sleepiness and snoring are possible symptoms of sleep apnea. Did you know that one in every four adults has some form of sleep disordered-breathing
Brian Palmer, D.D.S, Kansas City, Missouri, USA. April, 2001
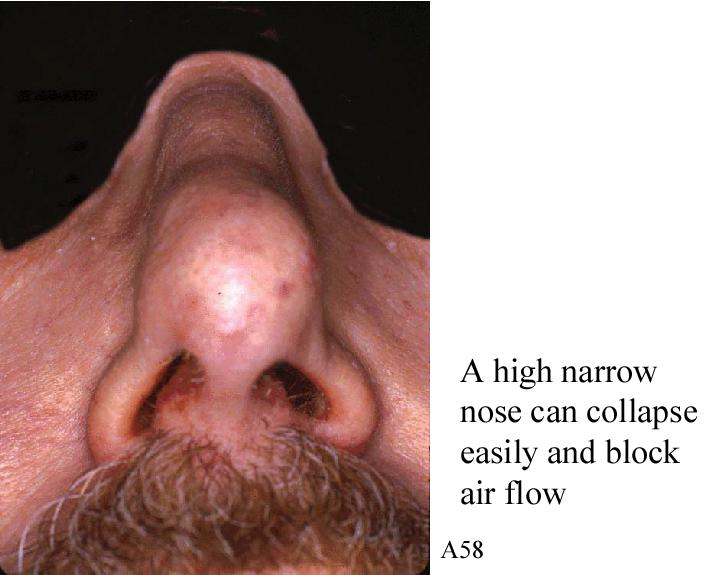
 Brian Palmer, D.D.S, Kansas City, Missouri, USA A1 April, 2001 Disclaimer The information in this presentation is for basic information only and is not to be construed as a diagnosis or treatment for any
Brian Palmer, D.D.S, Kansas City, Missouri, USA A1 April, 2001 Disclaimer The information in this presentation is for basic information only and is not to be construed as a diagnosis or treatment for any
Alaska Sleep Education Center
 Alaska Sleep Education Center The 3 Types of Sleep Apnea Explained: Obstructive, Central, & Mixed Posted by Kevin Phillips on Jan 28, 2015 6:53:00 PM Sleep apnea is a very common sleep disorder, affecting
Alaska Sleep Education Center The 3 Types of Sleep Apnea Explained: Obstructive, Central, & Mixed Posted by Kevin Phillips on Jan 28, 2015 6:53:00 PM Sleep apnea is a very common sleep disorder, affecting
Polysomnography (PSG) (Sleep Studies), Sleep Center
 (Sleep Studies), Sleep Center") Policy Number: 1036 Policy History Approve Date: 07/09/2015 Effective Date: 07/09/2015 Preauthorization All Plans Benefit plans vary in coverage and some plans may not provide coverage for certain service(s)
Policy Number: 1036 Policy History Approve Date: 07/09/2015 Effective Date: 07/09/2015 Preauthorization All Plans Benefit plans vary in coverage and some plans may not provide coverage for certain service(s)
SLEEP APNOEA DR TAN KAH LEONG ALVIN CO-DIRECTOR SLEEP LABORATORY SITE CHIEF SDDC (SLEEP) DEPARTMENT OF OTORHINOLARYNGOLOGY, HEAD & NECK SURGERY
 DEPARTMENT OF OTORHINOLARYNGOLOGY, HEAD & NECK SURGERY") SLEEP APNOEA DR TAN KAH LEONG ALVIN CO-DIRECTOR SLEEP LABORATORY SITE CHIEF SDDC (SLEEP) DEPARTMENT OF OTORHINOLARYNGOLOGY, HEAD & NECK SURGERY
SLEEP APNOEA DR TAN KAH LEONG ALVIN CO-DIRECTOR SLEEP LABORATORY SITE CHIEF SDDC (SLEEP) DEPARTMENT OF OTORHINOLARYNGOLOGY, HEAD & NECK SURGERY
IEHP considers the treatment of obstructive sleep apnea (OSA) medically necessary according to the criteria outlined below:
 medically necessary according to the criteria outlined below:") : Positive Airway Pressure, Oral Appliances, and Surgical Interventions Policy: Obstructive sleep apnea (OSA) is characterized by an interruption of breathing during sleep most commonly due to extra or
: Positive Airway Pressure, Oral Appliances, and Surgical Interventions Policy: Obstructive sleep apnea (OSA) is characterized by an interruption of breathing during sleep most commonly due to extra or
Sleep Apnea. What is sleep apnea? How does it occur? What are the symptoms?
 What is sleep apnea? Sleep Apnea Sleep apnea is a serious sleep problem. If you have it, you stop breathing for more than 10 seconds at a time many times while you sleep. Another term for this problem
What is sleep apnea? Sleep Apnea Sleep apnea is a serious sleep problem. If you have it, you stop breathing for more than 10 seconds at a time many times while you sleep. Another term for this problem
Dental Sleep Medicine Basics
 Dental Sleep Medicine Basics Written By: Patrick Tessier 2018 www.tap.wiki/ Page 1 of 8 INTRODUCTION Here are some basic aspect of Dental Sleep Medicine. This viewpoint is from an industry participant,
Dental Sleep Medicine Basics Written By: Patrick Tessier 2018 www.tap.wiki/ Page 1 of 8 INTRODUCTION Here are some basic aspect of Dental Sleep Medicine. This viewpoint is from an industry participant,
Sleep and the Heart Reversing the Effects of Sleep Apnea to Better Manage Heart Disease
 1 Sleep and the Heart Reversing the Effects of Sleep Apnea to Better Manage Heart Disease Rami Khayat, MD Professor of Internal Medicine Director, OSU Sleep Heart Program Medical Director, Department of
1 Sleep and the Heart Reversing the Effects of Sleep Apnea to Better Manage Heart Disease Rami Khayat, MD Professor of Internal Medicine Director, OSU Sleep Heart Program Medical Director, Department of
SNORING AND OBSTRUCTIVE SLEEP APNOEA WAYS TO DEAL WITH THESE PROBLEMS
 SNORING AND OBSTRUCTIVE SLEEP APNOEA WAYS TO DEAL WITH THESE PROBLEMS Laugh and the world laughs with you; snore and you sleep alone. These words by novelist Anthony Vergess ring true with all too many
SNORING AND OBSTRUCTIVE SLEEP APNOEA WAYS TO DEAL WITH THESE PROBLEMS Laugh and the world laughs with you; snore and you sleep alone. These words by novelist Anthony Vergess ring true with all too many
Mario Kinsella MD FAASM 10/5/2016
 Mario Kinsella MD FAASM 10/5/2016 Repetitive episodes of apnea or reduced airflow Due to upper airway obstruction during sleep Patients often obese Often have hypertension or DM 1 Obstructive apneas, hypopneas,
Mario Kinsella MD FAASM 10/5/2016 Repetitive episodes of apnea or reduced airflow Due to upper airway obstruction during sleep Patients often obese Often have hypertension or DM 1 Obstructive apneas, hypopneas,
OBSTRUCTIVE SLEEP APNEA and WORK Treatment Update
 OBSTRUCTIVE SLEEP APNEA and WORK Treatment Update David Claman, MD Professor of Medicine Director, UCSF Sleep Disorders Center 415-885-7886 Disclosures: None Chronic Sleep Deprivation (0 v 4 v 6 v 8 hrs)
OBSTRUCTIVE SLEEP APNEA and WORK Treatment Update David Claman, MD Professor of Medicine Director, UCSF Sleep Disorders Center 415-885-7886 Disclosures: None Chronic Sleep Deprivation (0 v 4 v 6 v 8 hrs)
Dear, Respectfully, United Sleep Centers SLEEP STUDY DATE: FEBUARY 26, 2015 AT OUR DOWNEY CENTER TIME: 10PM, PLEASE ARRIVE ON TIME
 Sleep Study Instructions SLEEP STUDY DATE: FEBUARY 26, 2015 AT OUR DOWNEY CENTER TIME: 10PM, PLEASE ARRIVE ON TIME ADDRESS: 11411 BROOKSHIRE AVE SUITE 505 DOWNEY, CA Dear, Thank you for choosing us as
Sleep Study Instructions SLEEP STUDY DATE: FEBUARY 26, 2015 AT OUR DOWNEY CENTER TIME: 10PM, PLEASE ARRIVE ON TIME ADDRESS: 11411 BROOKSHIRE AVE SUITE 505 DOWNEY, CA Dear, Thank you for choosing us as
11/19/2012 ก! " Varies 5-86% in men 2-57% in women. Thailand 26.4% (Neruntarut et al, Sleep Breath (2011) 15: )
 15: )") Snoring ก Respiratory sound generated in the upper airway during sleep that typically occurs during inspiration but may occur during expiration ICSD-2, 2005..... ก ก! Prevalence of snoring Varies 5-86%
Snoring ก Respiratory sound generated in the upper airway during sleep that typically occurs during inspiration but may occur during expiration ICSD-2, 2005..... ก ก! Prevalence of snoring Varies 5-86%
Article printed from
 What Are Sleep Disorders? Sleep disorders are conditions that affect how much and how well you sleep. The causes range from poor habits that keep you awake to medical problems that disrupt your sleep cycle.
What Are Sleep Disorders? Sleep disorders are conditions that affect how much and how well you sleep. The causes range from poor habits that keep you awake to medical problems that disrupt your sleep cycle.
Sleep Apnea. Herbert A Berger, MD Pulmonary Division Department of Internal Medicine University of Iowa
 Sleep Apnea Herbert A Berger, MD Pulmonary Division Department of Internal Medicine University of Iowa Disclosures No Relevant Financial Interests to Report Objectives Learn the history and physical examination
Sleep Apnea Herbert A Berger, MD Pulmonary Division Department of Internal Medicine University of Iowa Disclosures No Relevant Financial Interests to Report Objectives Learn the history and physical examination
Surgical Options for the Successful Treatment of Obstructive Sleep Apnea
 Surgical Options for the Successful Treatment of Obstructive Sleep Apnea Benjamin J. Teitelbaum, MD, FACS Otolaryngology Head and Neck Surgery Saint Agnes Medical Center Fresno, California Terms Apnea
Surgical Options for the Successful Treatment of Obstructive Sleep Apnea Benjamin J. Teitelbaum, MD, FACS Otolaryngology Head and Neck Surgery Saint Agnes Medical Center Fresno, California Terms Apnea
Sleep Apnoea. The Story of a Pause
 Sleep Apnoea The Story of a Pause There is almost zero awareness in India that many amongst us maybe living with Sleep Apnoea, which left untreated could be life threatening tomorrow. This largely undiagnosed
Sleep Apnoea The Story of a Pause There is almost zero awareness in India that many amongst us maybe living with Sleep Apnoea, which left untreated could be life threatening tomorrow. This largely undiagnosed
Sleep Apnea: Diagnosis & Treatment
 Disclosure Sleep Apnea: Diagnosis & Treatment Lawrence J. Epstein, MD Sleep HealthCenters Harvard Medical School Chief Medical Officer for Sleep HealthCenters Sleep medicine specialty practice group Consultant
Disclosure Sleep Apnea: Diagnosis & Treatment Lawrence J. Epstein, MD Sleep HealthCenters Harvard Medical School Chief Medical Officer for Sleep HealthCenters Sleep medicine specialty practice group Consultant
Emerging Nursing Roles in Collaborative Management of Sleep Disordered Breathing and Obstructive Sleep Apnoea
 Emerging Nursing Roles in Collaborative Management of Sleep Disordered Breathing and Obstructive Sleep Apnoea Sigma Theta Tau International 28th International Nursing Research Congress 27-31 July 2017
Emerging Nursing Roles in Collaborative Management of Sleep Disordered Breathing and Obstructive Sleep Apnoea Sigma Theta Tau International 28th International Nursing Research Congress 27-31 July 2017
Index. sleep.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Accidents. See Motor vehicle accidents. Acetazolamide, in OSA therapy, 531 Acetylcholinesterase inhibitors, in OSA therapy, 532 533 Acromegaly,
Note: Page numbers of article titles are in boldface type. A Accidents. See Motor vehicle accidents. Acetazolamide, in OSA therapy, 531 Acetylcholinesterase inhibitors, in OSA therapy, 532 533 Acromegaly,
HEALTHY LIFESTYLE, HEALTHY SLEEP. There are many different sleep disorders, and almost all of them can be improved with lifestyle changes.
 HEALTHY LIFESTYLE, HEALTHY SLEEP There are many different sleep disorders, and almost all of them can be improved with lifestyle changes. HEALTHY LIFESTYLE, HEALTHY SLEEP There are many different sleep
HEALTHY LIFESTYLE, HEALTHY SLEEP There are many different sleep disorders, and almost all of them can be improved with lifestyle changes. HEALTHY LIFESTYLE, HEALTHY SLEEP There are many different sleep
Abdussalam Alahmari ENT Resident R2 KAUH 15/12/2015
 Abdussalam Alahmari ENT Resident R2 KAUH 15/12/2015 Physiology of sleep Snoring mechanism, causes, sites, symptoms, and management. Sleep apnea definitions, pathophysiology, risk factors, evaluation of
Abdussalam Alahmari ENT Resident R2 KAUH 15/12/2015 Physiology of sleep Snoring mechanism, causes, sites, symptoms, and management. Sleep apnea definitions, pathophysiology, risk factors, evaluation of
Commissioning Policy Individual Funding Request
 Commissioning Policy Individual Funding Request Continuous Positive Airway Pressure (CPAP) Treatment of Obstructive Sleep Apnoea/Hypopnoea Syndrome (OSAHS) Criteria Based Access Policy Date Adopted: 13
Commissioning Policy Individual Funding Request Continuous Positive Airway Pressure (CPAP) Treatment of Obstructive Sleep Apnoea/Hypopnoea Syndrome (OSAHS) Criteria Based Access Policy Date Adopted: 13
The Agony or the Ecstasy. Familiar?
 The Agony or the Ecstasy Familiar? Snoring Related Complaints Drives wife from bedroom Girlfriend won t marry me Shakes entire house Ask me to leave movies and church Has had to leave boat so friends could
The Agony or the Ecstasy Familiar? Snoring Related Complaints Drives wife from bedroom Girlfriend won t marry me Shakes entire house Ask me to leave movies and church Has had to leave boat so friends could
GOT SLEEP? YOUR COMPLETE GUIDE TO UNDERSTANDING SLEEP APNEA
 Count me. I dare you. GOT SLEEP? YOUR COMPLETE GUIDE TO UNDERSTANDING SLEEP APNEA PRESENTED BY INTRODUCTION So what s the point of this ebook anyway? At The Maxillofacial Surgery Center, we want to inform
Count me. I dare you. GOT SLEEP? YOUR COMPLETE GUIDE TO UNDERSTANDING SLEEP APNEA PRESENTED BY INTRODUCTION So what s the point of this ebook anyway? At The Maxillofacial Surgery Center, we want to inform
Alexandria Workshop on
 Alexandria Workshop on 1 Snoring & OSA Surgery Course Director: Yassin Bahgat MD Claudio Vicini MD Course Board: Filippo Montevecchi MD Pietro Canzi MD Snoring & Obstructive ti Sleep Apnea The basic information
Alexandria Workshop on 1 Snoring & OSA Surgery Course Director: Yassin Bahgat MD Claudio Vicini MD Course Board: Filippo Montevecchi MD Pietro Canzi MD Snoring & Obstructive ti Sleep Apnea The basic information
Healthy Sleep. Frederick Tolle, M.D., dabsm Community Health Network
 Healthy Sleep Frederick Tolle, M.D., dabsm Community Health Network Adults should sleep 7 or more hours per night on a regular basis to promote optimal health. Getting less than 7 hours of sleep on average
Healthy Sleep Frederick Tolle, M.D., dabsm Community Health Network Adults should sleep 7 or more hours per night on a regular basis to promote optimal health. Getting less than 7 hours of sleep on average
Circadian Variations Influential in Circulatory & Vascular Phenomena
 SLEEP & STROKE 1 Circadian Variations Influential in Circulatory & Vascular Phenomena Endocrine secretions Thermo regulations Renal Functions Respiratory control Heart Rhythm Hematologic parameters Immune
SLEEP & STROKE 1 Circadian Variations Influential in Circulatory & Vascular Phenomena Endocrine secretions Thermo regulations Renal Functions Respiratory control Heart Rhythm Hematologic parameters Immune
ROBERT C. PRITCHARD DIRECTOR MICHAEL O. FOSTER ASSISTANT DIR. SLEEP APNEA
 ROBERT C. PRITCHARD DIRECTOR MICHAEL O. FOSTER ASSISTANT DIR. SLEEP APNEA A Person is physically qualified to drive a motor vehicle if that person; -(5) has no established medical history or clinical diagnosis
ROBERT C. PRITCHARD DIRECTOR MICHAEL O. FOSTER ASSISTANT DIR. SLEEP APNEA A Person is physically qualified to drive a motor vehicle if that person; -(5) has no established medical history or clinical diagnosis
National Sleep Disorders Research Plan
 Research Plan Home Foreword Preface Introduction Executive Summary Contents Contact Us National Sleep Disorders Research Plan Return to Table of Contents SECTION 5 - SLEEP DISORDERS SLEEP-DISORDERED BREATHING
Research Plan Home Foreword Preface Introduction Executive Summary Contents Contact Us National Sleep Disorders Research Plan Return to Table of Contents SECTION 5 - SLEEP DISORDERS SLEEP-DISORDERED BREATHING
Helping You to Breathe Better, Sleep Easy & Live Well
 Helping You to Breathe Better, Sleep Easy & Live Well Your Guide to CPAP Therapy info@cansleep.ca Vancouver Island Lower Mainland Fraser Valley Sleep Apnea & Symptoms Obstructive Sleep Apnea (OSA) occurs
Helping You to Breathe Better, Sleep Easy & Live Well Your Guide to CPAP Therapy info@cansleep.ca Vancouver Island Lower Mainland Fraser Valley Sleep Apnea & Symptoms Obstructive Sleep Apnea (OSA) occurs
A friend of mine, a 69-year-old pulmonologist in Port Arthur, Texas, who had OSA, died of a heart attack during sleep on July 13, 2015.
 SINCE U.S. Associate Justice Antonin Scalia, 79, a guest at the Cibolo Creek Ranch, a 30,000-acre luxury resort in West Texas, was found dead in his bedroom, speculation started that he could have died
SINCE U.S. Associate Justice Antonin Scalia, 79, a guest at the Cibolo Creek Ranch, a 30,000-acre luxury resort in West Texas, was found dead in his bedroom, speculation started that he could have died
DOWNLOAD OR READ : TREATMENT FOR SNORING PROBLEMS PDF EBOOK EPUB MOBI
 DOWNLOAD OR READ : TREATMENT FOR SNORING PROBLEMS PDF EBOOK EPUB MOBI Page 1 Page 2 treatment for snoring problems treatment for snoring problems pdf treatment for snoring problems problem, presenting
DOWNLOAD OR READ : TREATMENT FOR SNORING PROBLEMS PDF EBOOK EPUB MOBI Page 1 Page 2 treatment for snoring problems treatment for snoring problems pdf treatment for snoring problems problem, presenting
Anyone of any shape or size may snore, but there are certain features which significantly increase the chance of snoring.
 Snoring Snoring is a common sleep related problem affecting more than 20% of the population at some stage in their lives. Snoring occurs when various parts of the throat, including the soft palate, tonsils
Snoring Snoring is a common sleep related problem affecting more than 20% of the population at some stage in their lives. Snoring occurs when various parts of the throat, including the soft palate, tonsils
Obstructive sleep apnea
 Page1 Obstructive sleep apnea People who have obstructive sleep apnea often snore heavily and have longer breathing pauses while they sleep. Snoring on its own is harmless. But in combination with breathing
Page1 Obstructive sleep apnea People who have obstructive sleep apnea often snore heavily and have longer breathing pauses while they sleep. Snoring on its own is harmless. But in combination with breathing
Questions: What tests are available to diagnose sleep disordered breathing? How do you calculate overall AHI vs obstructive AHI?
 Pediatric Obstructive Sleep Apnea Case Study : Margaret-Ann Carno PhD, CPNP, D,ABSM for the Sleep Education for Pulmonary Fellows and Practitioners, SRN ATS Committee April 2014. Facilitator s guide Part
Pediatric Obstructive Sleep Apnea Case Study : Margaret-Ann Carno PhD, CPNP, D,ABSM for the Sleep Education for Pulmonary Fellows and Practitioners, SRN ATS Committee April 2014. Facilitator s guide Part
SLEEP DISORDERED BREATHING The Clinical Conditions
 SLEEP DISORDERED BREATHING The Clinical Conditions Robert G. Hooper, M.D. In the previous portion of this paper, the definitions of the respiratory events that are the hallmarks of problems with breathing
SLEEP DISORDERED BREATHING The Clinical Conditions Robert G. Hooper, M.D. In the previous portion of this paper, the definitions of the respiratory events that are the hallmarks of problems with breathing
WINDSOR DENTAL CARE 2224 WALKER ROAD SUITE 20 WINDSOR, ON N8W 5L7 PHONE FAX
 The quality of your sleep can impact you emotionally, physically and your overall general health. Poor sleep can cause chronic fatigue, daytime drowsiness, irritability and loss of focus. It affects your
The quality of your sleep can impact you emotionally, physically and your overall general health. Poor sleep can cause chronic fatigue, daytime drowsiness, irritability and loss of focus. It affects your
WHAT YOU NEED TO KNOW ABOUT SLEEP APNEA
 WHAT YOU NEED TO KNOW ABOUT SLEEP APNEA Wayne Driscoll Clinical Education Specialist 2 SLEEP APNEA IN THE NEWS Carrie Fisher died from sleep apnea, other factors, coroner says USA Today NJ Transit engineer
WHAT YOU NEED TO KNOW ABOUT SLEEP APNEA Wayne Driscoll Clinical Education Specialist 2 SLEEP APNEA IN THE NEWS Carrie Fisher died from sleep apnea, other factors, coroner says USA Today NJ Transit engineer
Snoring And Sleep Apnea in the U.S. Definitions Apnea: Cessation of ventilation for > 10 seconds. Defining Severity of OSA
 Snoring and Obstructive Sleep Apnea: Oral Appliance Therapy Management Midwest Society of Orthodontists October 16-17, 2009 Anthony J DiAngelis DMD, MPH Chief, Department of Dentistry, HCMC Professor,
Snoring and Obstructive Sleep Apnea: Oral Appliance Therapy Management Midwest Society of Orthodontists October 16-17, 2009 Anthony J DiAngelis DMD, MPH Chief, Department of Dentistry, HCMC Professor,
Helping You to Breathe Better, Sleep Easy & Live Well
 Helping You to Breathe Better, Sleep Easy & Live Well Your Guide to CPAP Therapy info@cansleep.ca Lower Mainland Vancouver Island Fraser Valley Sleep Apnea & Symptoms Obstructive Sleep Apnea (OSA) occurs
Helping You to Breathe Better, Sleep Easy & Live Well Your Guide to CPAP Therapy info@cansleep.ca Lower Mainland Vancouver Island Fraser Valley Sleep Apnea & Symptoms Obstructive Sleep Apnea (OSA) occurs
OSA - Obstructive sleep apnoea What you need to know if you think you might have OSA
 OSA - Obstructive sleep apnoea What you need to know if you think you might have OSA Obstructive sleep apnoea, or OSA, is a breathing problem that happens when you sleep. It can affect anyone men, women
OSA - Obstructive sleep apnoea What you need to know if you think you might have OSA Obstructive sleep apnoea, or OSA, is a breathing problem that happens when you sleep. It can affect anyone men, women
Management of OSA. saurabh maji
 Management of OSA saurabh maji INTRODUCTION Obstructive sleep apnea is a major public health problem Prevalence of OSAS in INDIA is 2.4% to 4.96% in men and 1% to 2 % in women In the rest of the world
Management of OSA saurabh maji INTRODUCTION Obstructive sleep apnea is a major public health problem Prevalence of OSAS in INDIA is 2.4% to 4.96% in men and 1% to 2 % in women In the rest of the world
DENTIST S INVOLVEMENT IN SNORING AND SLEEP APNEA PART 1 Dr. Brock Rondeau, D.D.S., I.B.O., D.A.B.C.P
 DENTIST S INVOLVEMENT IN SNORING AND SLEEP APNEA PART 1 Dr. Brock Rondeau, D.D.S., I.B.O., D.A.B.C.P It has been estimated that 60 million Americans snore and at least 18 million have obstructive sleep
DENTIST S INVOLVEMENT IN SNORING AND SLEEP APNEA PART 1 Dr. Brock Rondeau, D.D.S., I.B.O., D.A.B.C.P It has been estimated that 60 million Americans snore and at least 18 million have obstructive sleep
Patient Adult Information History
 Patient Adult Information History Patient name: Age: Date: What is the main reason for today s evaluation? Infant History Birth delivery: Normal C-section Delayed Epidural Premature: No Yes If yes, how
Patient Adult Information History Patient name: Age: Date: What is the main reason for today s evaluation? Infant History Birth delivery: Normal C-section Delayed Epidural Premature: No Yes If yes, how
Treatment of Obstructive Sleep Apnea (OSA)
") MP9239 Covered Service: Prior Authorization Required: Additional Information: Yes when meets criteria below Yes as shown below None Prevea360 Health Plan Medical Policy: 1.0 A continuous positive airway
MP9239 Covered Service: Prior Authorization Required: Additional Information: Yes when meets criteria below Yes as shown below None Prevea360 Health Plan Medical Policy: 1.0 A continuous positive airway
Sleep apnea. What is sleep apnea? What are the symptoms of sleep apnea? Symptoms during the day. Symptoms during sleep
 Sleep apnea Your doctor thinks you may have sleep apnea. The purpose of this fact sheet is to inform you about this disease. It also gives you details about the tests done to diagnose it and possible treatments.
Sleep apnea Your doctor thinks you may have sleep apnea. The purpose of this fact sheet is to inform you about this disease. It also gives you details about the tests done to diagnose it and possible treatments.
PEDIATRIC OBSTRUCTIVE SLEEP APNEA (OSA)
") PEDIATRIC OBSTRUCTIVE SLEEP APNEA (OSA) DEFINITION OSA Inspiratory airflow is either partly (hypopnea) or completely (apnea) occluded during sleep. The combination of sleep-disordered breathing with daytime
PEDIATRIC OBSTRUCTIVE SLEEP APNEA (OSA) DEFINITION OSA Inspiratory airflow is either partly (hypopnea) or completely (apnea) occluded during sleep. The combination of sleep-disordered breathing with daytime
PATIENT DEMOGRAPHICS
 PATIENT DEMOGRAPHICS NPSG CPAP CPAP Retitration Split Night PATIENT INFORMATION: Name: Last First Middle Initial Address: City: State: Zip: Social Security #: DOB: Gender: Age: Phone Number: Cell: Work:
PATIENT DEMOGRAPHICS NPSG CPAP CPAP Retitration Split Night PATIENT INFORMATION: Name: Last First Middle Initial Address: City: State: Zip: Social Security #: DOB: Gender: Age: Phone Number: Cell: Work:
Treatment of Snoring. Useful Telephone Numbers. Information for Patients on. North Hampshire ENT Partnership Hampshire Clinic
 Useful Telephone Numbers North Hampshire ENT Partnership Hampshire Clinic - 01256 377733 The Hampshire Clinic Switchboard - 01256 357111 Lyde Ward - 01256 377773 Enbourne Ward - 01256 377772 Frimley Park
Useful Telephone Numbers North Hampshire ENT Partnership Hampshire Clinic - 01256 377733 The Hampshire Clinic Switchboard - 01256 357111 Lyde Ward - 01256 377773 Enbourne Ward - 01256 377772 Frimley Park
Sleep Apnoea. Introduction Symptoms Causes Obtaining a Diagnosis Treatment Complications
 The most common forms of sleep apnoea are normally referred to as obstructive sleep apnoea (OSA) and relate to a condition which causes interruptions in breathing during sleep. People with obstructive
The most common forms of sleep apnoea are normally referred to as obstructive sleep apnoea (OSA) and relate to a condition which causes interruptions in breathing during sleep. People with obstructive
Waking Up To Obstructive Sleep Apnea
 Focus on CME at Memorial University of Newfoundland Waking Up To Obstructive Sleep Apnea Sleep apnea is a very common clinical disorder, which goes undiagnosed in most patients. Family physicians can identify
Focus on CME at Memorial University of Newfoundland Waking Up To Obstructive Sleep Apnea Sleep apnea is a very common clinical disorder, which goes undiagnosed in most patients. Family physicians can identify
No Rest For the Weary: Some Common Sleep Disorders
 No Rest For the Weary: Some Common Sleep Disorders Student Activity 3G Activity Introduction: It seems Mom does know best ; sleep has been proven to be essential to our health and well-being. In order
No Rest For the Weary: Some Common Sleep Disorders Student Activity 3G Activity Introduction: It seems Mom does know best ; sleep has been proven to be essential to our health and well-being. In order
The most accurate predictors of arterial hypertension in patients with Obstructive Sleep Apnea Syndrome
 The most accurate predictors of arterial hypertension in patients with Obstructive Sleep Apnea Syndrome Natsios Georgios University Hospital of Larissa, Greece Definitions Obstructive Sleep Apnea (OSA)
The most accurate predictors of arterial hypertension in patients with Obstructive Sleep Apnea Syndrome Natsios Georgios University Hospital of Larissa, Greece Definitions Obstructive Sleep Apnea (OSA)
EXPLORE NEW POSSIBILITIES
 EXPLORE NEW POSSIBILITIES TREATING SNORING AND SLEEP APNOEA HAS CHANGED FOREVER Introducing the Oventus O 2 Vent, a custom made, comfortable oral appliance with a unique airway design for the treatment
EXPLORE NEW POSSIBILITIES TREATING SNORING AND SLEEP APNOEA HAS CHANGED FOREVER Introducing the Oventus O 2 Vent, a custom made, comfortable oral appliance with a unique airway design for the treatment
Pre-Operative Services Teaching Rounds 11 March 2011
 Pre-Operative Services Teaching Rounds 11 March 2011 Deborah Richman MBChB FFA(SA) Director Pre-Operative Services Department of Anesthesia Stony Brook University Medical Center, NY drichman@notes.cc.sunysb.edu
Pre-Operative Services Teaching Rounds 11 March 2011 Deborah Richman MBChB FFA(SA) Director Pre-Operative Services Department of Anesthesia Stony Brook University Medical Center, NY drichman@notes.cc.sunysb.edu
How To Win Your War Against Snoring And Sleep Apnea
 Page 1 of 1 Contents What Is Sleep Apnea?... 9 Treatments For Central Sleep Apnea... 10 Learning About Sleep Apnea... 11 What Are The Symptoms Of Sleep Apnea?... 12 What Is Causing My Obstructive Sleep
Page 1 of 1 Contents What Is Sleep Apnea?... 9 Treatments For Central Sleep Apnea... 10 Learning About Sleep Apnea... 11 What Are The Symptoms Of Sleep Apnea?... 12 What Is Causing My Obstructive Sleep
This pamphlet has been designed as
 This pamphlet has been designed as an educational resource for patients with Obstructive Sleep Apnea (OSA). The successful use of CPAP requires no further intervention; however, not every patient is able,
This pamphlet has been designed as an educational resource for patients with Obstructive Sleep Apnea (OSA). The successful use of CPAP requires no further intervention; however, not every patient is able,
Emergency Contact Information Name: Phone: Address: Employer Information Employer Name: Address/Street: City: Zip: Phone: Fax:
 SUNSET SLEEP LABS PATIENT INFORMATION FORM Patient Information Name: Sex: M F Date of Birth: Address/Street: City: Zip: Phone: Alt Phone: Parent/Guardian: Phone: Social Security Number: Drivers License:
SUNSET SLEEP LABS PATIENT INFORMATION FORM Patient Information Name: Sex: M F Date of Birth: Address/Street: City: Zip: Phone: Alt Phone: Parent/Guardian: Phone: Social Security Number: Drivers License:
Rediscover the power of sleep
 Rediscover the power of sleep Patient Copy Apnea solutions for all ages Mobile Sleep Services Who We Are An experienced and well trained team of sleep care professionals consisting of Registered Sleep
Rediscover the power of sleep Patient Copy Apnea solutions for all ages Mobile Sleep Services Who We Are An experienced and well trained team of sleep care professionals consisting of Registered Sleep
Sleep and the Heart. Physiologic Changes in Cardiovascular Parameters during Sleep
 Sleep and the Heart Rami N. Khayat, MD Professor of Internal Medicine Medical Director, Department of Respiratory Therapy Division of Pulmonary, Critical Care and Sleep Medicine The Ohio State University
Sleep and the Heart Rami N. Khayat, MD Professor of Internal Medicine Medical Director, Department of Respiratory Therapy Division of Pulmonary, Critical Care and Sleep Medicine The Ohio State University
Sleep and the Heart. Rami N. Khayat, MD
 Sleep and the Heart Rami N. Khayat, MD Professor of Internal Medicine Medical Director, Department of Respiratory Therapy Division of Pulmonary, Critical Care and Sleep Medicine The Ohio State University
Sleep and the Heart Rami N. Khayat, MD Professor of Internal Medicine Medical Director, Department of Respiratory Therapy Division of Pulmonary, Critical Care and Sleep Medicine The Ohio State University
Sleep Center. Have you had a previous sleep study? Yes No If so, when and where? Name of facility Address
 Patient Label For office use only Appt date: Clinician: Sleep Center Main Campus Highlands Ranch Location 1400 Jackson Street 8671 S. Quebec St., Ste 120 Denver, CO 80206 Highlands Ranch, CO 80130 Leading
Patient Label For office use only Appt date: Clinician: Sleep Center Main Campus Highlands Ranch Location 1400 Jackson Street 8671 S. Quebec St., Ste 120 Denver, CO 80206 Highlands Ranch, CO 80130 Leading
Obstructive Sleep Apnea Syndrome. Common sleep disorder causes high blood pressure and heart attacks
 Obstructive Sleep Apnea Syndrome Common sleep disorder causes high blood pressure and heart attacks Message: Sleep apnea is very common. It is estimated that 158 million people worldwide suffer from sleep
Obstructive Sleep Apnea Syndrome Common sleep disorder causes high blood pressure and heart attacks Message: Sleep apnea is very common. It is estimated that 158 million people worldwide suffer from sleep
SLEEP QUESTIONNAIRE. Please briefly describe your sleep or sleep problem:
 SLEEP QUESTIONNAIRE Your answers to the following questions will help us to obtain a better understanding of your sleep problems. Please answer every question to the best of your ability. It is helpful
SLEEP QUESTIONNAIRE Your answers to the following questions will help us to obtain a better understanding of your sleep problems. Please answer every question to the best of your ability. It is helpful
Dr Alireza Yarahmadi and Dr Arvind Perathur Mercy Medical Center - Winter Retreat Des Moines February 2012
 Dr Alireza Yarahmadi and Dr Arvind Perathur Mercy Medical Center - Winter Retreat Des Moines February 2012 Why screen of OSA prior to surgery? What factors increase the risk? When due to anticipate problems?
Dr Alireza Yarahmadi and Dr Arvind Perathur Mercy Medical Center - Winter Retreat Des Moines February 2012 Why screen of OSA prior to surgery? What factors increase the risk? When due to anticipate problems?
SLEEP APNEA. Multimedia Health Education. Disclaimer
 Disclaimer This movie is an educational resource only and should not be used to manage your health. All decisions about the management of Sleep Apnea must be made in conjunction with your Physician or
Disclaimer This movie is an educational resource only and should not be used to manage your health. All decisions about the management of Sleep Apnea must be made in conjunction with your Physician or
Upper Airway Obstruction
 Upper Airway Obstruction Adriaan Pentz Division of Otorhinolaryngology University of Stellenbosch and Tygerberg Hospital Stridor/Stertor Auditory manifestations of disordered respiratory function ie noisy
Upper Airway Obstruction Adriaan Pentz Division of Otorhinolaryngology University of Stellenbosch and Tygerberg Hospital Stridor/Stertor Auditory manifestations of disordered respiratory function ie noisy
RESEARCH PACKET DENTAL SLEEP MEDICINE
 RESEARCH PACKET DENTAL SLEEP MEDICINE American Academy of Dental Sleep Medicine Dental Sleep Medicine Research Packet Page 1 Table of Contents Research: Oral Appliance Therapy vs. Continuous Positive Airway
RESEARCH PACKET DENTAL SLEEP MEDICINE American Academy of Dental Sleep Medicine Dental Sleep Medicine Research Packet Page 1 Table of Contents Research: Oral Appliance Therapy vs. Continuous Positive Airway
Use of Technology in the Assessment of Type 2 Diabetes and Sleep Apnea
 Use of Technology in the Assessment of Type 2 Diabetes and Sleep Apnea Eileen R. Chasens, PhD Associate Professor University of Pittsburgh September 3, 2014 Disclosure I do not own a Smart Phone, I have
Use of Technology in the Assessment of Type 2 Diabetes and Sleep Apnea Eileen R. Chasens, PhD Associate Professor University of Pittsburgh September 3, 2014 Disclosure I do not own a Smart Phone, I have
Infant Sleep Problems and their effects: A Public Health Issue
 Infant Sleep Problems and their effects: A Public Health Issue Wendy Hall, RN, PhD Assessing the Physical Development and Well-Being of Children 8 th Annual Assessment Workshop Outline for Sleep Workshop
Infant Sleep Problems and their effects: A Public Health Issue Wendy Hall, RN, PhD Assessing the Physical Development and Well-Being of Children 8 th Annual Assessment Workshop Outline for Sleep Workshop
OSA in children. About this information. What is obstructive sleep apnoea (OSA)?
?") About this information This information explains all about sleep-related breathing problems in children, focusing on the condition obstructive sleep apnoea (OSA). It tells you what the risk factors are
About this information This information explains all about sleep-related breathing problems in children, focusing on the condition obstructive sleep apnoea (OSA). It tells you what the risk factors are
Sleep Disorders and the Metabolic Syndrome
 Sleep Disorders and the Metabolic Syndrome Tom V. Cloward, M.D. Intermountain Sleep Disorders Center LDS Hospital Objectives Describe how sleep disorders impact your daily medical practice Don Don t do
Sleep Disorders and the Metabolic Syndrome Tom V. Cloward, M.D. Intermountain Sleep Disorders Center LDS Hospital Objectives Describe how sleep disorders impact your daily medical practice Don Don t do
New Patient Sleep Intake
 New Patient Sleep Intake Name: Date of Birth: Primary Care Physician: Date of Visit: Referring Physician and/or Other Physicians: Retail Pharmacy: Mail Order Pharmacy: Address: Mail Order Phone #: Phone
New Patient Sleep Intake Name: Date of Birth: Primary Care Physician: Date of Visit: Referring Physician and/or Other Physicians: Retail Pharmacy: Mail Order Pharmacy: Address: Mail Order Phone #: Phone
Dr. Don McLaughlin N Main St. Rutland VT (802)
") Dr. Don McLaughlin www.snoresnomore.com dr.don@snoresnomore.com 206 N Main St. Rutland VT 05706 (802) 773-7000 Booklet for Better Sleep Working with Sleep Apnea Part 1 of 3 Sick and Tired of Always Being
Dr. Don McLaughlin www.snoresnomore.com dr.don@snoresnomore.com 206 N Main St. Rutland VT 05706 (802) 773-7000 Booklet for Better Sleep Working with Sleep Apnea Part 1 of 3 Sick and Tired of Always Being
GOALS. Obstructive Sleep Apnea and Cardiovascular Disease (OVERVIEW) FINANCIAL DISCLOSURE 2/1/2017
 FINANCIAL DISCLOSURE 2/1/2017") Obstructive Sleep Apnea and Cardiovascular Disease (OVERVIEW) 19th Annual Topics in Cardiovascular Care Steven Khov, DO, FAAP Pulmonary Associates of Lancaster, Ltd February 3, 2017 skhov2@lghealth.org
Obstructive Sleep Apnea and Cardiovascular Disease (OVERVIEW) 19th Annual Topics in Cardiovascular Care Steven Khov, DO, FAAP Pulmonary Associates of Lancaster, Ltd February 3, 2017 skhov2@lghealth.org
What is SDB? Obstructive sleep apnea-hypopnea syndrome (OSAHS)
") Have a Good Sleep? Estimated 70 million Americans have clinically significant sleep problems Chronic insomnias report decreased quality of life, memory and attention problems, decreased physical health
Have a Good Sleep? Estimated 70 million Americans have clinically significant sleep problems Chronic insomnias report decreased quality of life, memory and attention problems, decreased physical health
Asleep at the Wheel Understanding and Preventing Drowsy Driving
 LIFESAVERS April 23, 2018 San Antonio, TX 2:15 3:45 PM Room 214 D Sleepiness and Accidents: A Crash Course EVOLVING SAFETY PRIORITIES AND SOLUTIONS Asleep at the Wheel Understanding and Preventing Drowsy
LIFESAVERS April 23, 2018 San Antonio, TX 2:15 3:45 PM Room 214 D Sleepiness and Accidents: A Crash Course EVOLVING SAFETY PRIORITIES AND SOLUTIONS Asleep at the Wheel Understanding and Preventing Drowsy
SURGERY FOR SNORING AND MILD OBSTRUCTIVE SLEEP APNOEA
 SURGERY FOR SNORING AND MILD OBSTRUCTIVE SLEEP APNOEA INTRODUCTION Snoring with or without excessive daytime somnolence, restless sleep and periods of apnoea are all manifestations of sleep disordered
SURGERY FOR SNORING AND MILD OBSTRUCTIVE SLEEP APNOEA INTRODUCTION Snoring with or without excessive daytime somnolence, restless sleep and periods of apnoea are all manifestations of sleep disordered
SLEEP QUESTIONNAIRE. Name: Home Telephone. Address: Work Telephone: Marital Status: Date of Birth: Age: Sex: Height: Weight: Pharmacy & Phone #:
 q JHMCE q JHS q SMEH SLEEP QUESTIONNAIRE 1. DEMOGRAPHIC DATA Name: Home Telephone Address: Work Telephone: Marital Status: Date of Birth: Age: Sex: Height: Weight: 2. PHYSICIAN INFORMATION Name of Primary
q JHMCE q JHS q SMEH SLEEP QUESTIONNAIRE 1. DEMOGRAPHIC DATA Name: Home Telephone Address: Work Telephone: Marital Status: Date of Birth: Age: Sex: Height: Weight: 2. PHYSICIAN INFORMATION Name of Primary
Learning Objectives. And it s getting worse. The Big Picture. Dr. Roger Roubal
 Learning Objectives How to screen for sleep apnea; questions to ask your patients Industry treatment guidelines; when to consider an oral appliance vs. a CPAP What goals/thresholds to set for successful
Learning Objectives How to screen for sleep apnea; questions to ask your patients Industry treatment guidelines; when to consider an oral appliance vs. a CPAP What goals/thresholds to set for successful
Obstructive Sleep Apnoea. Dr William Man Thoracic and Sleep Medicine, Harefield Hospital
 Obstructive Sleep Apnoea Dr William Man Thoracic and Sleep Medicine, Harefield Hospital Obstructive Sleep Apnoea Common Condition (Syndrome) 3 7% of adult males, 2 5% females Prevalence expected to rise
Obstructive Sleep Apnoea Dr William Man Thoracic and Sleep Medicine, Harefield Hospital Obstructive Sleep Apnoea Common Condition (Syndrome) 3 7% of adult males, 2 5% females Prevalence expected to rise
Facts about Sleep. Circadian rhythms are important in determining human sleep patterns/ sleep-waking cycle
 Sleep Sleep is described as a state of unconsciousness or partial consciousness from which a person can be roused by stimulation Period of rest and recovery People spend about a third of their lives sleeping
Sleep Sleep is described as a state of unconsciousness or partial consciousness from which a person can be roused by stimulation Period of rest and recovery People spend about a third of their lives sleeping
Update on Sleep Apnea Diagnosis and Treatment
 Update on Sleep Apnea Diagnosis and Treatment Damien Stevens MD Pulmonary/Critical Care/Sleep Medicine Medical Director KU Medical Center Sleep Laboratory Objectives Discuss physiology of sleep and obstructive
Update on Sleep Apnea Diagnosis and Treatment Damien Stevens MD Pulmonary/Critical Care/Sleep Medicine Medical Director KU Medical Center Sleep Laboratory Objectives Discuss physiology of sleep and obstructive
Evaluation, Management and Long-Term Care of OSA in Adults
 Evaluation, Management and Long-Term Care of OSA in Adults AUGUST 2015 Providing diagnostic tools and therapies that are evidence-based is a key part of a successful sleep practice. This resource outlines
Evaluation, Management and Long-Term Care of OSA in Adults AUGUST 2015 Providing diagnostic tools and therapies that are evidence-based is a key part of a successful sleep practice. This resource outlines
Sleep Apnea and Fatigue: Impact on Commercial Motor Vehicle Safety
 Sleep Apnea and Fatigue: Impact on Commercial Motor Vehicle Safety Sleep Apnea-Multimodal Transportation Conference American Sleep Apnea Association November 9, 2011 Benisse Lester, MD, Chief Medical Officer
Sleep Apnea and Fatigue: Impact on Commercial Motor Vehicle Safety Sleep Apnea-Multimodal Transportation Conference American Sleep Apnea Association November 9, 2011 Benisse Lester, MD, Chief Medical Officer
AHA Sleep Apnea and Cardiovascular Disease. Slide Set
 AHA 2008 Sleep Apnea and Cardiovascular Disease Slide Set Based on the AHA 2008 Scientific Statement Sleep Apnea and Cardiovascular Disease Virend K. Somers, MD, DPhil, FAHA, FACC Mayo Clinic and Mayo
AHA 2008 Sleep Apnea and Cardiovascular Disease Slide Set Based on the AHA 2008 Scientific Statement Sleep Apnea and Cardiovascular Disease Virend K. Somers, MD, DPhil, FAHA, FACC Mayo Clinic and Mayo
Littleton, CO Welcome Packet 8151 Southpark Lane, Suite 200 Littleton, CO 80120
 Littleton, CO Welcome Packet For any after-hours questions, please call (303) 956-5145 Dear Mountain Sleep Patient, You have been scheduled for a sleep study at 8151 Southpark Lane, Suite 200, Littleton,
Littleton, CO Welcome Packet For any after-hours questions, please call (303) 956-5145 Dear Mountain Sleep Patient, You have been scheduled for a sleep study at 8151 Southpark Lane, Suite 200, Littleton,
Positive Airway Pressure and Oral Devices for the Treatment of Obstructive Sleep Apnea
 Positive Airway Pressure and Oral Devices for the Treatment of Obstructive Sleep Apnea Policy Number: Original Effective Date: MM.01.009 11/01/2009 Line(s) of Business: Current Effective Date: HMO; PPO
Positive Airway Pressure and Oral Devices for the Treatment of Obstructive Sleep Apnea Policy Number: Original Effective Date: MM.01.009 11/01/2009 Line(s) of Business: Current Effective Date: HMO; PPO
Sleep: A Forgotten Component of Overall Health Demarcus Sneed Health and Human Sciences Educator Madison County October 5, 2016
 Sleep: A Forgotten Component of Overall Health Demarcus Sneed Health and Human Sciences Educator Madison County October 5, 2016 Lesson Objectives Understand the importance of having consistent, quality
Sleep: A Forgotten Component of Overall Health Demarcus Sneed Health and Human Sciences Educator Madison County October 5, 2016 Lesson Objectives Understand the importance of having consistent, quality