ICU Delirium A Real Epidemic (or are we delirious)?
|
|
|
- Georgiana Greer
- 5 years ago
- Views:
Transcription
1 ICU Delirium A Real Epidemic (or are we delirious)? CCCF: Toronto October 2014 Jesse Hall MD University of Chicago Section of Pulmonary and Critical Care Medicine
2 Faculty Disclosures Dr. Hall receives honoraria from the ACCP for board review course and SEEK receives honoraria from McGraw-Hill and Taylor-Francis publishing
3 10 Big Mistakes in Intensive Care Medicine (JLV, JBH, AS) 1-We focus too much on syndromes prominently ARDS, sepsis, acute kidney injury (AKI), and we spend much time redefining them. Even though we considered sepsis as a too vaguely defined entity, treatments were studied in prospective trials. Most were unsuccessful.. Better identification of patient populations is the key. Instead of general phenotypes (fever and tachycardia), we should uncover the basic cellular alterations characterizing critical illness, and by doing so better characterize the patients' status.

4 ICU delirium is our neurologic syndrome
 came into wide Application in")
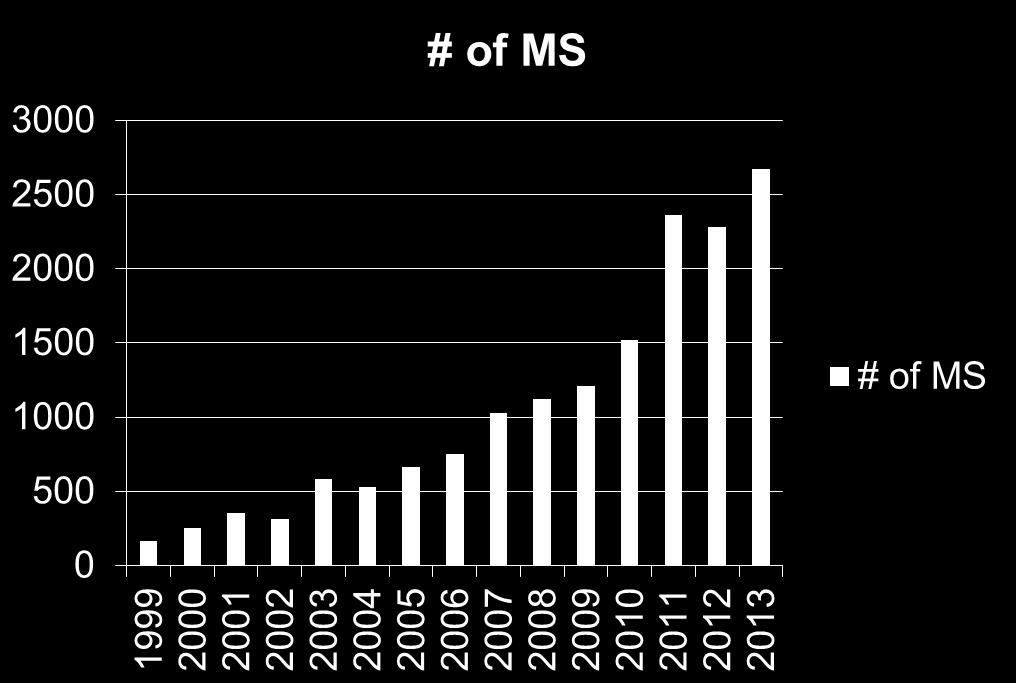
5 J Crit Care 2011 Both the Confusion Assessment Method for the ICU (North America) and the Intensive Care Delirium Screening Check List (Europe) came into wide Application in
6 LOS, mortality, morbidity assoc with ICU delirium Ely, JAMA 2004
7 LOS, mortality, morbidity assoc with ICU delirium Ely, JAMA 2004
8 Cox Model HR Age 1.03 IADL 1.30 Comorbidity 1.21 Delirium day 1.10 For each day of delirium, 1-yr mortality increased by 10% Pisani MA et al., AJRCCM 180: 1092

9 Don t just stand there.. AJRCCM 2014

10 Don t just stand there.. AJRCCM 2014
11 What is the true incidence of delirium in the ICU? Case Mix Assessment Tool Sedation Practice 32% 81%
12 All cases of delirium are created equal, but some are more equal than others.
13 Confusion Assessment Method for the Intensive Care Unit (CAM-ICU) Coma

14 A Day in the Life of RASS RASS Time
15 Sedatives and Delirium Ely EW, JAMA 291: 1753
16 Remarkably in > 10 yrs of reporting the incidence of delirium/coma, determining its association with outcomes, and even conducting interventional trials, we have not attempted to disentangle (within the limits of necessary patient care) the sedation-delirium problem

17 AJRCCM 2014
18 Patel et al 29% of patients scored as delirious had delirium absent when reassessed after sedation hold (up to 2 hrs) CAM-ICU 10.5 x more likely to dx delirium if done during sedation administration than after hold This rapidly reversible delirium showed reduced LOS, duration of MV, and improved survival as compared to persistent delirium AJRCCM 2014

19 AJRCCM 2014
20 AJRCCM 2014

21 AJRCCM 2014
22 Point 1 and its corollaries 1/4 to 1/3 of MV patients who would be scored by CAM-ICU as delirious have a rapidly reversible delirium demonstrable by sedation hold and their delirium does not associate with poor outcome Should be built into monitoring for delirium These patients should be stratified (excluded?) in intervention trials These patients not likely to yield fruitful results in mechanistic studies
23 Potential reversible causes of delirium that might not result in long-term brain dysfunction Drugs Hepatic encephalopathy Electrolyte disturbances Cerebral edema Hypothermia
24 The typical severely ill ARDS patient with exposures to both reversible and non-reversible insults Short-term coma/delirium near universal Extensive delirium testing in extreme AHRF not feasible Longterm neuropsychiatric dysfunction near universal Imaging studies not clear as to a macroscopic lesion (perhaps just volume loss VISIONS MRI data) Correlations not tight for hypoxemia, PPV exposures

25 Toward a better understanding of the brain in critical illness AJRCCM 2013
26 A bad brain-ventilator connection Murine model of high + low pressure MV with hippocampal apoptosis and Akt survival pathway studied Studies also done in vagotomized, haloperidol-treated, and local brain dopamine-blocked animals Findings MV triggers hippocampal apoptosis as a result of type 2 dopaminergic receptor activation in response to vagal signaling also causes alterations in dysbindin 1, a protein known to regulate cell surface D2R recycling in neurons Dysbindin 1 results confirmed in brain slices of humans who had undergone MV AJRCCM 2013

27 AJRCCM 2013

28 AJRCCM 2013

29
30 Point 2 For the pool of patients in whom we know delirium strongly associates with poor longterm outcome We need to better understand mechanisms linking brain injury to ICU diseases and interventions/environment, such as MV In addition to minimizing exposure to the injurious force (eg high lung vols/pressures) we need to consider interruption of adverse neural pathways or enhancement of neuroprotective pathways
Management of Delirium in the ICU. Yahya Shehabi
 Management of Delirium in the ICU Yahya Shehabi Hello! Doctor, your patient is CAM + ve Good morning Dr, Am one of the RC, Just examined Mr XXX he is CAM +ve Positive what? Sir replied RC: I meant he is
Management of Delirium in the ICU Yahya Shehabi Hello! Doctor, your patient is CAM + ve Good morning Dr, Am one of the RC, Just examined Mr XXX he is CAM +ve Positive what? Sir replied RC: I meant he is
9/28/2016. Sedation Strategies in the ICU. Outline. ICU sedation. Recent clinical practice guidelines Top 10 myths A practical approach
 Sedation Strategies in the ICU UW Medicine EMS and Trauma Conference Seattle, Washington September 26 th, 2016 C. Terri Hough, MD MSc Associate Professor of Medicine Division of Pulmonary and Critical
Sedation Strategies in the ICU UW Medicine EMS and Trauma Conference Seattle, Washington September 26 th, 2016 C. Terri Hough, MD MSc Associate Professor of Medicine Division of Pulmonary and Critical
Sedation and Delirium Questions
 Sedation and Delirium Questions TLC Curriculum William J. Ehlenbach, MD MSc Assistant Professor of Medicine Pulmonary & Critical Care Medicine Question 1 Deep sedation in ventilated critically patients
Sedation and Delirium Questions TLC Curriculum William J. Ehlenbach, MD MSc Assistant Professor of Medicine Pulmonary & Critical Care Medicine Question 1 Deep sedation in ventilated critically patients
Sedation and delirium- drugs and clinical management
 Sedation and delirium- drugs and clinical management Shannon S. Carson, MD Associate Professor and Chief Division of Pulmonary and Critical Care Medicine University of North Carolina Probability of transitioning
Sedation and delirium- drugs and clinical management Shannon S. Carson, MD Associate Professor and Chief Division of Pulmonary and Critical Care Medicine University of North Carolina Probability of transitioning
Conducting Delirium Research
 Optimizing Clinical Trials When Conducting Research Research funding: Disclosure NHLBI, NIA, AstraZeneca John W. Devlin, PharmD, FCCP, FCCM, Professor of Pharmacy, Northeastern University Scientific Staff,
Optimizing Clinical Trials When Conducting Research Research funding: Disclosure NHLBI, NIA, AstraZeneca John W. Devlin, PharmD, FCCP, FCCM, Professor of Pharmacy, Northeastern University Scientific Staff,
Delirium in the ICU: Prevention and Treatment. Delirium Defined Officially. Delirium: Really Defined. S. Andrew Josephson, MD
 Delirium in the ICU: Prevention and Treatment S. Andrew Josephson, MD Director, Neurohospitalist Service Medical Director, Inpatient Neurology June 2, 2011 Delirium Defined Officially (DSM-IV-TR) criteria
Delirium in the ICU: Prevention and Treatment S. Andrew Josephson, MD Director, Neurohospitalist Service Medical Director, Inpatient Neurology June 2, 2011 Delirium Defined Officially (DSM-IV-TR) criteria
ICU Delirium in Infants & Children: Cause for Concern or False Alarm. Objectives
 ICU Delirium in Infants & Children: Cause for Concern or False Alarm Peter (Pete) N. Johnson, Pharm.D., BCPS, BCPPS, FPPAG Associate Professor of Pharmacy Practice University of Oklahoma College of Pharmacy
ICU Delirium in Infants & Children: Cause for Concern or False Alarm Peter (Pete) N. Johnson, Pharm.D., BCPS, BCPPS, FPPAG Associate Professor of Pharmacy Practice University of Oklahoma College of Pharmacy
ICU Delirium and sedation: understanding their role in long-term patient outcomes. Yoanna Skrobik MD FRCP(c)
") ICU Delirium and sedation: understanding their role in long-term patient outcomes Yoanna Skrobik MD FRCP(c) Conflicts of interest Member, SCCM Pain, Agitation and Delirium guidelines writing committee
ICU Delirium and sedation: understanding their role in long-term patient outcomes Yoanna Skrobik MD FRCP(c) Conflicts of interest Member, SCCM Pain, Agitation and Delirium guidelines writing committee
Brain dysfunction in the ICU
 High cortisol levels are associated with brain dysfunction but low prolactin cortisol ratio levels are associated with nosocomial infection in severe sepsis Duc Nam Nguyen Luc Huyghens Johan Schiettecatte
High cortisol levels are associated with brain dysfunction but low prolactin cortisol ratio levels are associated with nosocomial infection in severe sepsis Duc Nam Nguyen Luc Huyghens Johan Schiettecatte
DELIRIUM IN ICU: Prevention and Management. Milind Baldi
 DELIRIUM IN ICU: Prevention and Management Milind Baldi Contents Introduction Risk factors Assessment Prevention Management Introduction Delirium is a syndrome characterized by acute cerebral dysfunction
DELIRIUM IN ICU: Prevention and Management Milind Baldi Contents Introduction Risk factors Assessment Prevention Management Introduction Delirium is a syndrome characterized by acute cerebral dysfunction
Early Goal Directed Sedation In Critically Ill Patients
 Early Goal Directed Sedation In Critically Ill Patients Yahya Shehabi, FCICM, FANZCA, EMBA Professor, Intensive Care Medicine Clinical School of Medicine, University New South Wales School of Epidemiology
Early Goal Directed Sedation In Critically Ill Patients Yahya Shehabi, FCICM, FANZCA, EMBA Professor, Intensive Care Medicine Clinical School of Medicine, University New South Wales School of Epidemiology
Delirium Pilot Project
 CCU Nurses: Delirium Pilot Project Our unit has been selected to develop and implement a delirium assessment and intervention program. We are beginning Phase 1 with education and assessing for our baseline
CCU Nurses: Delirium Pilot Project Our unit has been selected to develop and implement a delirium assessment and intervention program. We are beginning Phase 1 with education and assessing for our baseline
Do you know. Assessment of Delirium. What is Delirium? Which syndrome occurs more commonly in elderly populations? a. Delirium b.
 Assessment of Delirium Marianne McCarthy, PhD, GNP, PMHNP Arizona State University College of Nursing and Health Innovation What is Delirium? Delirium is a common clinical syndrome characterized by: Inattention
Assessment of Delirium Marianne McCarthy, PhD, GNP, PMHNP Arizona State University College of Nursing and Health Innovation What is Delirium? Delirium is a common clinical syndrome characterized by: Inattention
Can Goal Directed Sedation Improve Outcomes?
 Can Goal Directed Sedation Improve Outcomes? Yahya SHEHABI, FANZCA, FCICM, EMBA Professor and Program Director Critical care Monash Health and Monash University - Melbourne School of Medicine, University
Can Goal Directed Sedation Improve Outcomes? Yahya SHEHABI, FANZCA, FCICM, EMBA Professor and Program Director Critical care Monash Health and Monash University - Melbourne School of Medicine, University
Update in Critical Care Medicine
 Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative
 Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Liberation from Mechanical Ventilation in Critically Ill Adults
 Liberation from Mechanical Ventilation in Critically Ill Adults 2017 ACCP/ATS Clinical Practice Guidelines Timothy D. Girard, MD, MSCI Clinical Research, Investigation, and Systems Modeling of Acute Illness
Liberation from Mechanical Ventilation in Critically Ill Adults 2017 ACCP/ATS Clinical Practice Guidelines Timothy D. Girard, MD, MSCI Clinical Research, Investigation, and Systems Modeling of Acute Illness
Overview of Presentation. Delirium Definition. Assessing & Managing ICU Delirium: What is the Evidence?
 Assessing & Managing ICU Delirium: What is the Evidence? Dale Needham, MD, PhD Professor Pulmonary & Critical Care Medicine, and Physical Medicine & Rehabilitation Medical Director, Critical Care Physical
Assessing & Managing ICU Delirium: What is the Evidence? Dale Needham, MD, PhD Professor Pulmonary & Critical Care Medicine, and Physical Medicine & Rehabilitation Medical Director, Critical Care Physical
Mechanical ventilation induced or exacerbated right ventricular failure
 Mechanical ventilation induced or exacerbated right ventricular failure Toronto 2016 Jesse Hall MD Professor of Medicine, Anesthesia & Critical Care University of Chicago Faculty Disclosures Dr. Hall
Mechanical ventilation induced or exacerbated right ventricular failure Toronto 2016 Jesse Hall MD Professor of Medicine, Anesthesia & Critical Care University of Chicago Faculty Disclosures Dr. Hall
Sedation of the Critically Ill Patient
 Buffalo theory of sedation It s a well known fact that a herd of buffalo can only move as fast as the slowest buffalo. And when the herd is hunted, it s the slowest and weakest ones at the back that are
Buffalo theory of sedation It s a well known fact that a herd of buffalo can only move as fast as the slowest buffalo. And when the herd is hunted, it s the slowest and weakest ones at the back that are
Targeting depression after ARDS. Neill Adhikari Sunnybrook Health Sciences and University of Toronto 29 October 2012
 Targeting depression after ARDS Neill Adhikari Sunnybrook Health Sciences and University of Toronto 29 October 2012 None Conflicts of interest Objectives Review epidemiology of depression after ARDS Review
Targeting depression after ARDS Neill Adhikari Sunnybrook Health Sciences and University of Toronto 29 October 2012 None Conflicts of interest Objectives Review epidemiology of depression after ARDS Review
Disclosure. Hospira Pharmaceuticals. Unrestricted research funding Honoraria for CME education administered via France Foundation
 Disclosure Hospira Pharmaceuticals Unrestricted research funding Honoraria for CME education administered via France Foundation Economics in Sedation: Responsible Use of the ICU Budget John W. Devlin,
Disclosure Hospira Pharmaceuticals Unrestricted research funding Honoraria for CME education administered via France Foundation Economics in Sedation: Responsible Use of the ICU Budget John W. Devlin,
Sleep in the ICU: helped by drugs? Yoanna Skrobik MD FRCP(c) MSc.
 MSc.") Sleep in the ICU: helped by drugs? Yoanna Skrobik MD FRCP(c) MSc. Conflicts of interest Member, SCCM Pain, Agitation and Delirium guidelines writing committee Vice-chair, SCCM Pain, Agitation, Delirium,
Sleep in the ICU: helped by drugs? Yoanna Skrobik MD FRCP(c) MSc. Conflicts of interest Member, SCCM Pain, Agitation and Delirium guidelines writing committee Vice-chair, SCCM Pain, Agitation, Delirium,
Management of delirium in mechanically ventilated patients. Advances in Critical Care Medicine King Hussein Cancer Center
 Management of delirium in mechanically ventilated patients Advances in Critical Care Medicine King Hussein Cancer Center Introduction Outline: Prevalence of delirium in ICU Why it is important to screen
Management of delirium in mechanically ventilated patients Advances in Critical Care Medicine King Hussein Cancer Center Introduction Outline: Prevalence of delirium in ICU Why it is important to screen
KEY REFERENCES Laying the foundation for D of ABCDEF bundle
 KEY REFERENCES Laying the foundation for D of ABCDEF bundle Ely E. JAMA. 2001;286:2703-2710 (CAM-ICU) Bergeron N. Intensive Care Med. 2001;27:859-864 (ICDSC) Dubois M. Intensive Care Med. 2001;27:1297-1304
KEY REFERENCES Laying the foundation for D of ABCDEF bundle Ely E. JAMA. 2001;286:2703-2710 (CAM-ICU) Bergeron N. Intensive Care Med. 2001;27:859-864 (ICDSC) Dubois M. Intensive Care Med. 2001;27:1297-1304
Supplementary appendix
 Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Page VJ, Casarin A, Ely EW, et al. Evaluation
Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Page VJ, Casarin A, Ely EW, et al. Evaluation
Canadian Practices for the Treatment of Delirium. Lisa Burry, BScPharm, PharmD
 Canadian Practices for the Treatment of Delirium Lisa Burry, BScPharm, PharmD Disclosures & Acknowledgements Conflicts of interest: None Acknowledgements: our patients and the clinical staff that supported
Canadian Practices for the Treatment of Delirium Lisa Burry, BScPharm, PharmD Disclosures & Acknowledgements Conflicts of interest: None Acknowledgements: our patients and the clinical staff that supported
Monitoring the Brain
 Cognition Monitoring the Brain Michael Ramsay MD FRCA Chairman Department of Anesthesia Baylor University Medical Center President Baylor Research Institute Dallas Texas Speaker Disclosure I have received
Cognition Monitoring the Brain Michael Ramsay MD FRCA Chairman Department of Anesthesia Baylor University Medical Center President Baylor Research Institute Dallas Texas Speaker Disclosure I have received
Sepsis Awareness and Education
 Sepsis Awareness and Education Meets the updated New York State Department of Health (NYSDOH) requirements for Infection Control and Barrier Precautions coursework Element VII: Sepsis Awareness and Education
Sepsis Awareness and Education Meets the updated New York State Department of Health (NYSDOH) requirements for Infection Control and Barrier Precautions coursework Element VII: Sepsis Awareness and Education
ICU Liberation for the Pharmacist. A. Kendall Gross, PharmD, BCPS, BCCCP Critical Care Pharmacist UCSF Medical Center
 ICU Liberation for the Pharmacist A. Kendall Gross, PharmD, BCPS, BCCCP Critical Care Pharmacist UCSF Medical Center Disclosure No conflicts of interest to disclose Objectives o Outline the elements of
ICU Liberation for the Pharmacist A. Kendall Gross, PharmD, BCPS, BCCCP Critical Care Pharmacist UCSF Medical Center Disclosure No conflicts of interest to disclose Objectives o Outline the elements of
What are Appropriate End-points for Delirium Prevention/Treatment Studies
 What are Appropriate End-points for Delirium Prevention/Treatment Studies Pratik Pandharipande, MD, MSCI Professor of Anesthesiology and Surgery Department of Anesthesiology Vanderbilt University School
What are Appropriate End-points for Delirium Prevention/Treatment Studies Pratik Pandharipande, MD, MSCI Professor of Anesthesiology and Surgery Department of Anesthesiology Vanderbilt University School
New approaches of sedation in critically ill patients.
 New approaches of sedation in critically ill patients. Jean Mantz, MD, PhD Professor and Chair, Department of Anesthesia and Critical Care F- Paris Val de Seine University Hospitals Univ Paris Diderot,
New approaches of sedation in critically ill patients. Jean Mantz, MD, PhD Professor and Chair, Department of Anesthesia and Critical Care F- Paris Val de Seine University Hospitals Univ Paris Diderot,
Outcome of patients with hematologic malignancy admitted to the ICU
 Outcome of patients with hematologic malignancy admitted to the ICU Geeta Mehta MD, FRCPC Mount Sinai Hospital Toronto, Canada CCCF November 2, 2016 Disclosures Hematologic Malignancy Advances in diagnostics,
Outcome of patients with hematologic malignancy admitted to the ICU Geeta Mehta MD, FRCPC Mount Sinai Hospital Toronto, Canada CCCF November 2, 2016 Disclosures Hematologic Malignancy Advances in diagnostics,
Wake up and Breathe: A journey in quality improvement and unintended benefits
 Wake up and Breathe: A journey in quality improvement and unintended benefits Jeffrey Singh MD FRCPC MSc Toronto Western Hospital Interdepartmental Division of Critical Care University of Toronto Disclosures
Wake up and Breathe: A journey in quality improvement and unintended benefits Jeffrey Singh MD FRCPC MSc Toronto Western Hospital Interdepartmental Division of Critical Care University of Toronto Disclosures
ICU LIBERATION: IMPLEMENTING THE ABCDEF BUNDLE AND IMPROVING THE LIVES OF ICU PATIENTS
 ICU LIBERATION: IMPLEMENTING THE ABCDEF BUNDLE AND IMPROVING THE LIVES OF ICU PATIENTS J. MATTHEW ALDRICH, MD ASSOCIATE CLINICAL PROFESSOR OF ANESTHESIA AND PERIOPERATIVE CARE UNIVERSITY OF CALIFORNIA
ICU LIBERATION: IMPLEMENTING THE ABCDEF BUNDLE AND IMPROVING THE LIVES OF ICU PATIENTS J. MATTHEW ALDRICH, MD ASSOCIATE CLINICAL PROFESSOR OF ANESTHESIA AND PERIOPERATIVE CARE UNIVERSITY OF CALIFORNIA
ABCs of ICU Delirium Marian Maxwell, Pharm.D., BCCCP January 6, 2018
 ABCs of ICU Delirium Marian Maxwell, Pharm.D., BCCCP January 6, 2018 Disclosures I do not have any financial/non-financial relationships to disclose. Learning Objectives Define delirium and discuss the
ABCs of ICU Delirium Marian Maxwell, Pharm.D., BCCCP January 6, 2018 Disclosures I do not have any financial/non-financial relationships to disclose. Learning Objectives Define delirium and discuss the
Cognitive Outcomes after Critical Illness LUNG DAY 2010
 Cognitive Outcomes after Critical Illness LUNG DAY 2010 C. Terri Hough, MD MSc Assistant Professor of Medicine Pulmonary and Critical Care Medicine Harborview Medical Center Acknowledgements Bill Ehlenbach
Cognitive Outcomes after Critical Illness LUNG DAY 2010 C. Terri Hough, MD MSc Assistant Professor of Medicine Pulmonary and Critical Care Medicine Harborview Medical Center Acknowledgements Bill Ehlenbach
Occurrence of delirium is severely underestimated in the ICU during daily care
 Intensive Care Med (2009) 35:1276 1280 DOI 10.1007/s00134-009-1466-8 BRIEF REPORT Peter E. Spronk Bea Riekerk José Hofhuis Johannes H. Rommes Occurrence of delirium is severely underestimated in the ICU
Intensive Care Med (2009) 35:1276 1280 DOI 10.1007/s00134-009-1466-8 BRIEF REPORT Peter E. Spronk Bea Riekerk José Hofhuis Johannes H. Rommes Occurrence of delirium is severely underestimated in the ICU
Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh. Professor of Critical Care, Edinburgh University
 Tim Walsh. Professor of Critical Care, Edinburgh University") Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh Professor of Critical Care, Edinburgh University Lecture Plan: a route to clarity What is delirium? Why is delirium important? Step
Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh Professor of Critical Care, Edinburgh University Lecture Plan: a route to clarity What is delirium? Why is delirium important? Step
COGNITIVE DYSFUNCTION IN THE ELDERLY PATIENT QUIZ #34
 COGNITIVE DYSFUNCTION IN THE ELDERLY PATIENT QUIZ #34 M. ANGELE THEARD, MD STAFF ANESTHESIOLOGIST LEGACY EMANUEL MEDICAL CENTER PORTLAND, OR QUIZ TEAM: SHOBANA RAJAN, MD SUNEETA GOLLAPUDY, MD VERGHESE
COGNITIVE DYSFUNCTION IN THE ELDERLY PATIENT QUIZ #34 M. ANGELE THEARD, MD STAFF ANESTHESIOLOGIST LEGACY EMANUEL MEDICAL CENTER PORTLAND, OR QUIZ TEAM: SHOBANA RAJAN, MD SUNEETA GOLLAPUDY, MD VERGHESE
BRAIN DYSFUNCTION DURING SEPSIS When and how should we monitor the brain in sepsis?
 BRAIN DYSFUNCTION DURING SEPSIS When and how should we monitor the brain in sepsis? andrea.polito@rpc.aphp.fr University of Versailles Raymond Poincaré Teaching Hospital Garches - France SEPTIC PATIENTS
BRAIN DYSFUNCTION DURING SEPSIS When and how should we monitor the brain in sepsis? andrea.polito@rpc.aphp.fr University of Versailles Raymond Poincaré Teaching Hospital Garches - France SEPTIC PATIENTS
+ Change in baseline mental status, inattention, and either disorganized thinking or altered level of consciousness. Delirium. Disclosure.
 47 th Annual Meeting August 2-4, 2013 Orlando, FL Identification, Prevention and Treatment of Delirium: The Role of the Health System Pharmacist Jennifer Cortes, PharmD, BCPS Medical ICU Clinical Pharmacy
47 th Annual Meeting August 2-4, 2013 Orlando, FL Identification, Prevention and Treatment of Delirium: The Role of the Health System Pharmacist Jennifer Cortes, PharmD, BCPS Medical ICU Clinical Pharmacy
BPG 06: Sedation. Patients receive appropriate sedation to meet their needs, optimising comfort and with minimal adverse effects.
 Statement of Best Practice BPG 06: Sedation Patients receive appropriate sedation to meet their needs, optimising comfort and with minimal adverse effects. 1: Introduction Indication for sedation will
Statement of Best Practice BPG 06: Sedation Patients receive appropriate sedation to meet their needs, optimising comfort and with minimal adverse effects. 1: Introduction Indication for sedation will
Fighting the Fog A Collaborative Approach to Decreasing ICU Delirium
 Fighting the Fog A Collaborative Approach to Decreasing ICU Delirium Kimberly Scherr NP Jennifer Barker RN Misericordia Hospital ICU Edmonton, AB CACCN Dynamics Sept 21, 2014 Delirium Delirium is an acute
Fighting the Fog A Collaborative Approach to Decreasing ICU Delirium Kimberly Scherr NP Jennifer Barker RN Misericordia Hospital ICU Edmonton, AB CACCN Dynamics Sept 21, 2014 Delirium Delirium is an acute
Do benzos, opioids, or strong anticholinergics cause delirium? Lisa Burry
 Do benzos, opioids, or strong anticholinergics cause delirium? Lisa Burry Delirium in the ICU Occurs in up to 85% of MICU/SICU MV patients 20-50% of lower severity ICU patients develop delirium Hypoactive
Do benzos, opioids, or strong anticholinergics cause delirium? Lisa Burry Delirium in the ICU Occurs in up to 85% of MICU/SICU MV patients 20-50% of lower severity ICU patients develop delirium Hypoactive
No Brain is an Island Considerations in the ICU
 No Brain is an Island Considerations in the ICU GEMSSTAR Meeting 2018 Michael Avidan, MBBCh, FCA(SA) Dr. Seymour and Rose T Brown Professor of Anesthesiology Acknowledgements National Institute on Aging
No Brain is an Island Considerations in the ICU GEMSSTAR Meeting 2018 Michael Avidan, MBBCh, FCA(SA) Dr. Seymour and Rose T Brown Professor of Anesthesiology Acknowledgements National Institute on Aging
Delirium in the intensive care unit: a narrative review of published assessment tools and the relationship between ICU delirium and clinical outcomes
 The Intensive Care Society 2008 Delirium in the intensive care unit: a narrative review of published assessment tools and the relationship between ICU delirium and clinical outcomes C Waters Delirium is
The Intensive Care Society 2008 Delirium in the intensive care unit: a narrative review of published assessment tools and the relationship between ICU delirium and clinical outcomes C Waters Delirium is
Implementation of a Delirium Screening Tool in a Pediatric Intensive Care Unit
 Implementation of a Delirium Screening Tool in a Pediatric Intensive Care Unit BY: ABBY WACHHOLTZ, BSN, RN, PEDIATRIC ACUTE CARE DNP STUDENT Disclosures I have no disclosures. 1 Objectives 1. Recognize
Implementation of a Delirium Screening Tool in a Pediatric Intensive Care Unit BY: ABBY WACHHOLTZ, BSN, RN, PEDIATRIC ACUTE CARE DNP STUDENT Disclosures I have no disclosures. 1 Objectives 1. Recognize
Rehabilitation after Critical Illness: What Should this Look Like?
 Rehabilitation after Critical Illness: What Should this Look Like? Margaret Herridge MD MPH Associate Professor of Medicine Interdepartmental Division of Critical Care University of Toronto Canadian Critical
Rehabilitation after Critical Illness: What Should this Look Like? Margaret Herridge MD MPH Associate Professor of Medicine Interdepartmental Division of Critical Care University of Toronto Canadian Critical
Disparities in the ICU: The Elderly? Shannon S. Carson, MD Associate Professor Pulmonary and Critical Care Medicine University of North Carolina
 Disparities in the ICU: The Elderly? Shannon S. Carson, MD Associate Professor Pulmonary and Critical Care Medicine University of North Carolina Critical Care Is Care of the Elderly 15,757 consecutive
Disparities in the ICU: The Elderly? Shannon S. Carson, MD Associate Professor Pulmonary and Critical Care Medicine University of North Carolina Critical Care Is Care of the Elderly 15,757 consecutive
Current awareness of delirium in the intensive care unit: a postal survey in the Netherlands
 SPECIAL REPORT Current awareness of delirium in the intensive care unit: a postal survey in the Netherlands F.L. Cadogan 1, B. Riekerk 2, R. Vreeswijk 1, J.H. Rommes 2, A.C. Toornvliet 1, M.L.H. Honing
SPECIAL REPORT Current awareness of delirium in the intensive care unit: a postal survey in the Netherlands F.L. Cadogan 1, B. Riekerk 2, R. Vreeswijk 1, J.H. Rommes 2, A.C. Toornvliet 1, M.L.H. Honing
Disentangling Delirium and Dementia
 Disentangling Delirium and Dementia Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley F. Levy Family Chair Director, Aging
Disentangling Delirium and Dementia Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley F. Levy Family Chair Director, Aging
Outcomes From Severe ARDS Managed Without ECMO. Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016
 Outcomes From Severe ARDS Managed Without ECMO Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016 Severe ARDS Berlin Definition 2012 P:F ratio 100 mm Hg Prevalence:
Outcomes From Severe ARDS Managed Without ECMO Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016 Severe ARDS Berlin Definition 2012 P:F ratio 100 mm Hg Prevalence:
ICU Updates: Delirium in Hospitalized Patients
 ICU Updates: Delirium in Hospitalized Patients James A. Frank, MD Associate Professor Pulmonary and Critical Care UCSF Dept. of Medicine Director, MICU San Francisco VAMC Recognizing and preventing delirium
ICU Updates: Delirium in Hospitalized Patients James A. Frank, MD Associate Professor Pulmonary and Critical Care UCSF Dept. of Medicine Director, MICU San Francisco VAMC Recognizing and preventing delirium
DELIRIUM. J. Sukanya 28.Jun.12
 DELIRIUM J. Sukanya 28.Jun.12 Outline Why? What? How? What s next? Delirium Introduction Delirium An acute decline in attention and cognition The most frequent neuropsychiatric syndrome A common, life-threatening,
DELIRIUM J. Sukanya 28.Jun.12 Outline Why? What? How? What s next? Delirium Introduction Delirium An acute decline in attention and cognition The most frequent neuropsychiatric syndrome A common, life-threatening,
What you need to know about Delirium in ICU. Dr Valerie Page Watford General Hospital
 What you need to know about Delirium in ICU Dr Valerie Page Watford General Hospital Delirium and outcome 40 year old ARDS ICU survivor college graduate I have been out of hospital and trying to get on
What you need to know about Delirium in ICU Dr Valerie Page Watford General Hospital Delirium and outcome 40 year old ARDS ICU survivor college graduate I have been out of hospital and trying to get on
Doug Paul, D.O. FACOS Medical Director, Trauma Services Kettering Health Network
 Doug Paul, D.O. FACOS Medical Director, Trauma Services Kettering Health Network A paradigm shift (or revolutionary science) is, a change in the basic assumptions, or paradigms, within the ruling theory
Doug Paul, D.O. FACOS Medical Director, Trauma Services Kettering Health Network A paradigm shift (or revolutionary science) is, a change in the basic assumptions, or paradigms, within the ruling theory
Executive Sponsorship of Delirium Initiatives Lessons from ICU Liberation
 Executive Sponsorship of Delirium Initiatives Lessons from ICU Liberation J. Matthew Aldrich, MD Co-Chair, SCCM ICU Liberation Committee Associate Professor Medical Director, Critical Care Medicine UCSF
Executive Sponsorship of Delirium Initiatives Lessons from ICU Liberation J. Matthew Aldrich, MD Co-Chair, SCCM ICU Liberation Committee Associate Professor Medical Director, Critical Care Medicine UCSF
Sarah V. Cogle, PharmD, BCCCP Assistant Clinical Professor Auburn University Harrison School of Pharmacy Auburn, AL ALSHP Annual Clinical Meeting
 Sarah V. Cogle, PharmD, BCCCP Assistant Clinical Professor Auburn University Harrison School of Pharmacy Auburn, AL ALSHP Annual Clinical Meeting 2018 I have no actual or potential conflict of interest
Sarah V. Cogle, PharmD, BCCCP Assistant Clinical Professor Auburn University Harrison School of Pharmacy Auburn, AL ALSHP Annual Clinical Meeting 2018 I have no actual or potential conflict of interest
ICU Updates: Delirium in Hospitalized Patients
 Outline James A. Frank, MD Associate Professor Pulmonary and Critical Care UCSF Dept. of Medicine Director, MICU San Francisco VAMC ICU Updates: in Hospitalized Patients Recognizing and preventing delirium
Outline James A. Frank, MD Associate Professor Pulmonary and Critical Care UCSF Dept. of Medicine Director, MICU San Francisco VAMC ICU Updates: in Hospitalized Patients Recognizing and preventing delirium
Prolonged Mechanical Ventilation
 Prolonged Mechanical Ventilation Shannon S. Carson, MD Associate Professor and Chief Pulmonary and Critical Care Medicine University of North Carolina AJRCCM 2010 Projected Growth of Prolonged Acute MV
Prolonged Mechanical Ventilation Shannon S. Carson, MD Associate Professor and Chief Pulmonary and Critical Care Medicine University of North Carolina AJRCCM 2010 Projected Growth of Prolonged Acute MV
The Berlin Definition: Does it fix anything?
 The Berlin Definition: Does it fix anything? Gordon D. Rubenfeld, MD MSc Professor of Medicine, University of Toronto Chief, Program in Trauma, Emergency, and Critical Care Sunnybrook Health Sciences Centre
The Berlin Definition: Does it fix anything? Gordon D. Rubenfeld, MD MSc Professor of Medicine, University of Toronto Chief, Program in Trauma, Emergency, and Critical Care Sunnybrook Health Sciences Centre
Complicated Withdrawal
 Complicated Withdrawal Shamim Nejad, MD Director, Adult Burns & Trauma Psychiatry Division of Psychiatry and Medicine Medical Director, Addiction Consultation Team MGH Center for Addiction Medicine Massachusetts
Complicated Withdrawal Shamim Nejad, MD Director, Adult Burns & Trauma Psychiatry Division of Psychiatry and Medicine Medical Director, Addiction Consultation Team MGH Center for Addiction Medicine Massachusetts
PRESCRIBING PRACTICE IN DELIRIUM. John Warburton Critical Care Pharmacist
 PRESCRIBING PRACTICE IN DELIRIUM John Warburton Critical Care Pharmacist Learning outcomes Modifiable medication risk factors for delirium An appreciation of contributing factors modifiable with medicines
PRESCRIBING PRACTICE IN DELIRIUM John Warburton Critical Care Pharmacist Learning outcomes Modifiable medication risk factors for delirium An appreciation of contributing factors modifiable with medicines
Sepsis-3: clarity or confusion
 Sepsis-3: clarity or confusion Christopher W. Seymour, MD MSc The CRISMA Center Assistant Professor of Critical Care Medicine & Emergency Medicine University of Pittsburgh School of Medicine Can an otherwise
Sepsis-3: clarity or confusion Christopher W. Seymour, MD MSc The CRISMA Center Assistant Professor of Critical Care Medicine & Emergency Medicine University of Pittsburgh School of Medicine Can an otherwise
Nutrition in the critically ill elderly (geriatric) patient CHRISTINA NIEUWOUDT RD(SA) SASPEN/CCSSA CONGRESS 2017
 patient CHRISTINA NIEUWOUDT RD(SA) SASPEN/CCSSA CONGRESS 2017") Nutrition in the critically ill elderly (geriatric) patient CHRISTINA NIEUWOUDT RD(SA) SASPEN/CCSSA CONGRESS 2017 CONTENT WHO is the critically ill elderly (geriatric) patient? WHY look at the critically
Nutrition in the critically ill elderly (geriatric) patient CHRISTINA NIEUWOUDT RD(SA) SASPEN/CCSSA CONGRESS 2017 CONTENT WHO is the critically ill elderly (geriatric) patient? WHY look at the critically
Jie Chen Department of Critical Care Medicine, Zhongda Hospital, School of Medicine, Southeast University
 Jie Chen Department of Critical Care Medicine, Zhongda Hospital, School of Medicine, Southeast University Crit Care Med. 2004;32(4):955 62. BMJ. 2015;350:h2538. Background Delirium, defined as acute brain
Jie Chen Department of Critical Care Medicine, Zhongda Hospital, School of Medicine, Southeast University Crit Care Med. 2004;32(4):955 62. BMJ. 2015;350:h2538. Background Delirium, defined as acute brain
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Accelerated intravascular coagulation and fibrinolysis (AICF) in liver disease, 390 391 Acid suppression in liver disease, 403 404 ACLF.
Index Note: Page numbers of article titles are in boldface type. A Accelerated intravascular coagulation and fibrinolysis (AICF) in liver disease, 390 391 Acid suppression in liver disease, 403 404 ACLF.
Dexmedetomidine: the various roles and utilization strategies. Julie Belfer, PharmD September 2014
 Dexmedetomidine: the various roles and utilization strategies Julie Belfer, PharmD September 2014 Disclosure No disclosures concerning possible financial or personal relationships with commercial entities
Dexmedetomidine: the various roles and utilization strategies Julie Belfer, PharmD September 2014 Disclosure No disclosures concerning possible financial or personal relationships with commercial entities
Beyond the Golden Hour: Caring for the ICU Boarder
 Beyond the Golden Hour: Caring for the ICU Boarder Kami M. Hu, MD Dept. of Emergency Medicine Dept. of Pulmonology & Critical Care University of Maryland SOM I have no relevant financial relationships
Beyond the Golden Hour: Caring for the ICU Boarder Kami M. Hu, MD Dept. of Emergency Medicine Dept. of Pulmonology & Critical Care University of Maryland SOM I have no relevant financial relationships
Rounds in the ICU. Eran Segal, MD Director General ICU Sheba Medical Center
 Rounds in the ICU Eran Segal, MD Director General ICU Sheba Medical Center Real Clinical cases (including our mistakes) Emphasis on hemodynamic monitoring Usually no single correct answer We will conduct
Rounds in the ICU Eran Segal, MD Director General ICU Sheba Medical Center Real Clinical cases (including our mistakes) Emphasis on hemodynamic monitoring Usually no single correct answer We will conduct
Caring For the ICU Boarder. Kami M. Hu, MD Depts of Emergency & Internal Medicine University of Maryland SOM
 Caring For the ICU Boarder Kami M. Hu, MD Depts of Emergency & Internal Medicine University of Maryland SOM I have no relevant financial relationships with the manufacturer(s) of any commercial product(s)and/or
Caring For the ICU Boarder Kami M. Hu, MD Depts of Emergency & Internal Medicine University of Maryland SOM I have no relevant financial relationships with the manufacturer(s) of any commercial product(s)and/or
Example Clinician Educational Material for Providers of Immune Effector Cellular Therapy
 Example Clinician Educational Material for Providers of Immune Effector Cellular Therapy Disclaimer: This example is just one of many potential examples of clinician education material that can be provided
Example Clinician Educational Material for Providers of Immune Effector Cellular Therapy Disclaimer: This example is just one of many potential examples of clinician education material that can be provided
ETIOLOGY AND PATHOGENESIS OF HYPOXIC-ISCHEMIC ENCEPHALOPATHY
 ETIOLOGY AND PATHOGENESIS OF HYPOXIC-ISCHEMIC ENCEPHALOPATHY HYPOXIC-ISCHEMIC ENCEPHALOPATHY Hypoxic-İschemic Encephalopathy Encephalopathy due to hypoxic-ischemic injury [Hypoxic-ischemic encephalopathy
ETIOLOGY AND PATHOGENESIS OF HYPOXIC-ISCHEMIC ENCEPHALOPATHY HYPOXIC-ISCHEMIC ENCEPHALOPATHY Hypoxic-İschemic Encephalopathy Encephalopathy due to hypoxic-ischemic injury [Hypoxic-ischemic encephalopathy
CPR What Works, What Doesn t
 Resuscitation 2017 ECMO and ECLS April 1, 2017 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN Circulation 2013;128:417-35
Resuscitation 2017 ECMO and ECLS April 1, 2017 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN Circulation 2013;128:417-35
Outline. Basic principles of lung protective ventilation. The challenging areas. Small tidal volumes Recruitment
 ARDS beyond 6/kg Gordon D. Rubenfeld, MD MSc Professor of Medicine, University of Toronto Chief, Program in Trauma, Emergency, and Critical Care Sunnybrook Health Sciences Centre Outline Basic principles
ARDS beyond 6/kg Gordon D. Rubenfeld, MD MSc Professor of Medicine, University of Toronto Chief, Program in Trauma, Emergency, and Critical Care Sunnybrook Health Sciences Centre Outline Basic principles
Delirium in Critical Care. Recognition, Management, Research tasters. Dr Valerie Page Watford General Hospital
 Delirium in Critical Care. Recognition, Management, Research tasters Dr Valerie Page Watford General Hospital What does it look like? Diagnosing delirium CAM-ICU CAM-ICU Feature 1: Acute onset of mental
Delirium in Critical Care. Recognition, Management, Research tasters Dr Valerie Page Watford General Hospital What does it look like? Diagnosing delirium CAM-ICU CAM-ICU Feature 1: Acute onset of mental
Making vasopressors safer
 Making vasopressors safer Requirements for safe vaspressor use In an ideal world 1. Knowledge of what constitutes optimal vasopressor dosing 2. A culture of cautiousness regarding vasopressors What do
Making vasopressors safer Requirements for safe vaspressor use In an ideal world 1. Knowledge of what constitutes optimal vasopressor dosing 2. A culture of cautiousness regarding vasopressors What do
The Effect of a Quality Improvement Intervention on Perceived Sleep Quality and Cognition in a Medical ICU*
 The Effect of a Quality Improvement Intervention on Perceived Sleep Quality and Cognition in a Medical ICU* Biren B. Kamdar, MD, MBA, MHS 1,2 ; Lauren M. King, RN, MSN 1,3 ; Nancy A. Collop, MD 4 ; Sruthi
The Effect of a Quality Improvement Intervention on Perceived Sleep Quality and Cognition in a Medical ICU* Biren B. Kamdar, MD, MBA, MHS 1,2 ; Lauren M. King, RN, MSN 1,3 ; Nancy A. Collop, MD 4 ; Sruthi
Complicated Withdrawal
 Complicated Withdrawal Shamim Nejad, MD Medical Director, Psycho-Oncology Services Swedish Cancer Institute Swedish Medical Center Seattle, Washington Shamim.Nejad@Swedish.org Disclosures: Shamim Nejad,
Complicated Withdrawal Shamim Nejad, MD Medical Director, Psycho-Oncology Services Swedish Cancer Institute Swedish Medical Center Seattle, Washington Shamim.Nejad@Swedish.org Disclosures: Shamim Nejad,
ANWICU knowledge
 ANWICU knowledge www.anwicu.org.uk This presentation is provided by ANWICU We are a collaborative association of ICUs in the North West of England. Permission to provide this presentation has been granted
ANWICU knowledge www.anwicu.org.uk This presentation is provided by ANWICU We are a collaborative association of ICUs in the North West of England. Permission to provide this presentation has been granted
Preventing Postoperative Cognitive Decline in the Elderly
 Preventing Postoperative Cognitive Decline in the Elderly Alex Bekker, M.D., Ph.D Professor and Chair Department of Anesthesiology Rutgers New Jersey Medical School "My brain, that's my second favorite
Preventing Postoperative Cognitive Decline in the Elderly Alex Bekker, M.D., Ph.D Professor and Chair Department of Anesthesiology Rutgers New Jersey Medical School "My brain, that's my second favorite
NIH Public Access Author Manuscript Crit Care Med. Author manuscript; available in PMC 2015 December 01.
 NIH Public Access Author Manuscript Published in final edited form as: Crit Care Med. 2014 December ; 42(12): e791 e795. doi:10.1097/ccm.0000000000000660. Effectiveness of Implementing a Wake up and Breathe
NIH Public Access Author Manuscript Published in final edited form as: Crit Care Med. 2014 December ; 42(12): e791 e795. doi:10.1097/ccm.0000000000000660. Effectiveness of Implementing a Wake up and Breathe
Delirium. Delirium. Delirium Etiology and Pathophysiology. Fall 2018
 Three most common cognitive problems in adults 1. (acute confusion) 2. Dementia 3. Depression These problems often occur together Can you think of common stimuli for each? 1 1 State of temporary but acute
Three most common cognitive problems in adults 1. (acute confusion) 2. Dementia 3. Depression These problems often occur together Can you think of common stimuli for each? 1 1 State of temporary but acute
INTENSIVE INSULIN THERAPY: A Long History of Conflicting Data.
 INTENSIVE INSULIN THERAPY: A Long History of Conflicting Data. Candice Preslaski, PharmD BCPS Clinical Pharmacist Specialist SICU Denver Health Medical Center December 2014 OBJECTIVES Review the risk factors
INTENSIVE INSULIN THERAPY: A Long History of Conflicting Data. Candice Preslaski, PharmD BCPS Clinical Pharmacist Specialist SICU Denver Health Medical Center December 2014 OBJECTIVES Review the risk factors
Weaning and extubation in PICU An evidence-based approach
 Weaning and extubation in PICU An evidence-based approach Suchada Sritippayawan, MD. Div. Pulmonology & Crit Care Dept. Pediatrics Faculty of Medicine Chulalongkorn University Kanokporn Udomittipong, MD.
Weaning and extubation in PICU An evidence-based approach Suchada Sritippayawan, MD. Div. Pulmonology & Crit Care Dept. Pediatrics Faculty of Medicine Chulalongkorn University Kanokporn Udomittipong, MD.
Kendiss Olafson MD FRCPC MPH Section of Critical Care University of Manitoba
 Kendiss Olafson MD FRCPC MPH Section of Critical Care University of Manitoba Outline Sedation in ICU Purpose/Goals Common Drugs Sedation delivery strategies Mobility in the ICU Weakness with critical illness
Kendiss Olafson MD FRCPC MPH Section of Critical Care University of Manitoba Outline Sedation in ICU Purpose/Goals Common Drugs Sedation delivery strategies Mobility in the ICU Weakness with critical illness
TOO COOL OR NOT TOO COOL- THERAPEUTIC HYPOTHERMIA IN THE ICU SCCM TX 2017 TED WU MD PEDIATRIC CRITICAL CARE UNIVERSITY OF TEXAS HEALTH SAN ANTONIO
 TOO COOL OR NOT TOO COOL- THERAPEUTIC HYPOTHERMIA IN THE ICU SCCM TX 2017 TED WU MD PEDIATRIC CRITICAL CARE UNIVERSITY OF TEXAS HEALTH SAN ANTONIO DISCLOSURE I have no relationships with commercial companies
TOO COOL OR NOT TOO COOL- THERAPEUTIC HYPOTHERMIA IN THE ICU SCCM TX 2017 TED WU MD PEDIATRIC CRITICAL CARE UNIVERSITY OF TEXAS HEALTH SAN ANTONIO DISCLOSURE I have no relationships with commercial companies
12/4/2017. Disclosure. Educational Objectives. Has been consultant for Bard, Chiesi
 Temperature Management in Neuro ICU Kiwon Lee, MD, FACP, FAHA, FCCM Professor of Neurology, RWJ Medical School Chief of Neurology, RWJ University Hospital Director, RWJ Comprehensive Stroke Center Director,
Temperature Management in Neuro ICU Kiwon Lee, MD, FACP, FAHA, FCCM Professor of Neurology, RWJ Medical School Chief of Neurology, RWJ University Hospital Director, RWJ Comprehensive Stroke Center Director,
QuickTime and a DV - NTSC decompressor are needed to see this picture.
 QuickTime and a DV - NTSC decompressor are needed to see this picture. Case Presentation (Actual Case) 66 y/o Female c/o Hip Pain Fell, but no pre-fall symptoms Did not hit head or have LOC PMHx: DM, ESRD,
QuickTime and a DV - NTSC decompressor are needed to see this picture. Case Presentation (Actual Case) 66 y/o Female c/o Hip Pain Fell, but no pre-fall symptoms Did not hit head or have LOC PMHx: DM, ESRD,
Approach to Severe Sepsis. Jan Hau Lee, MBBS, MRCPCH. MCI Children s Intensive Care Unit KK Women s and Children's Hospital, Singapore
 Approach to Severe Sepsis Jan Hau Lee, MBBS, MRCPCH. MCI Children s Intensive Care Unit KK Women s and Children's Hospital, Singapore 1 2 No conflict of interest Overview Epidemiology of Pediatric Severe
Approach to Severe Sepsis Jan Hau Lee, MBBS, MRCPCH. MCI Children s Intensive Care Unit KK Women s and Children's Hospital, Singapore 1 2 No conflict of interest Overview Epidemiology of Pediatric Severe
Targeted temperature management after post-anoxic brain insult: where do we stand?
 Targeted temperature management after post-anoxic brain insult: where do we stand? Alain Cariou Intensive Care Unit Cochin University Hospital Paris Descartes University INSERM U970 (France) COI Disclosure
Targeted temperature management after post-anoxic brain insult: where do we stand? Alain Cariou Intensive Care Unit Cochin University Hospital Paris Descartes University INSERM U970 (France) COI Disclosure
Collaborative Regional Benchmarking Group (North of England, North Yorkshire & Humber and West Yorkshire)
") Best Practice Guidance Sedation These recommendations are bound by the current evidence and best practice at the time of writing and so will be subject to change as further developments are made in this
Best Practice Guidance Sedation These recommendations are bound by the current evidence and best practice at the time of writing and so will be subject to change as further developments are made in this
NYSPFP HIIN: VAE/Delirium Prevention. Operationalizing the Pain, Agitation and Delirium Assessments
 NYSPFP HIIN: VAE/Delirium Prevention Operationalizing the Pain, Agitation and Delirium Assessments March 28, 2017 1 Agenda Topic Welcome and Introductions A Guide for Success: Implementing the Confusion
NYSPFP HIIN: VAE/Delirium Prevention Operationalizing the Pain, Agitation and Delirium Assessments March 28, 2017 1 Agenda Topic Welcome and Introductions A Guide for Success: Implementing the Confusion
Conflict of Interest. Patient Case. Objectives. The Balancing Act. Why We Need Sedation
 Agitation in the ICU Have we swung the pendulum too far from benzodiazepines? Conflict of Interest The author of this presentation has no conflicts of interest to disclose Nina Vadiei, PharmD PGY1 Pharmacy
Agitation in the ICU Have we swung the pendulum too far from benzodiazepines? Conflict of Interest The author of this presentation has no conflicts of interest to disclose Nina Vadiei, PharmD PGY1 Pharmacy
Noninvasive Ventilation: Non-COPD Applications
 Noninvasive Ventilation: Non-COPD Applications NONINVASIVE MECHANICAL VENTILATION Why Noninvasive Ventilation? Avoids upper A respiratory airway trauma system lacerations, protective hemorrhage strategy
Noninvasive Ventilation: Non-COPD Applications NONINVASIVE MECHANICAL VENTILATION Why Noninvasive Ventilation? Avoids upper A respiratory airway trauma system lacerations, protective hemorrhage strategy
Clinical Practice Guidelines for the Management of Pain, Agitation, and Delirium in Adult Patients
 Clinical Practice Guidelines for the Management of Pain, Agitation, and Delirium in Adult Patients in the Intensive Care Unit January 2013 Volume 41 Number 1 Society of Critical Care Medicine 本檔僅供內部教學使用檔案內所使用之照片之版權仍屬於原期刊公開使用時,
Clinical Practice Guidelines for the Management of Pain, Agitation, and Delirium in Adult Patients in the Intensive Care Unit January 2013 Volume 41 Number 1 Society of Critical Care Medicine 本檔僅供內部教學使用檔案內所使用之照片之版權仍屬於原期刊公開使用時,
Critical illness- A new co-morbidity?
 Critical illness- A new co-morbidity? Brian H Cuthbertson Chief, Department of Critical Care Medicine Sunnybrook Health Sciences Centre Professor of Anaesthesia University of Toronto Toronto, Canada Critical
Critical illness- A new co-morbidity? Brian H Cuthbertson Chief, Department of Critical Care Medicine Sunnybrook Health Sciences Centre Professor of Anaesthesia University of Toronto Toronto, Canada Critical
Intravenous Vitamin C. Severe Sepsis Acute Lung Injury
 Intravenous Vitamin C Severe Sepsis Acute Lung Injury Alpha A. (Berry) Fowler, III, MD Professor of Medicine VCU Pulmonary Disease and Critical Care Medicine I Have No Disclosures Bacterial Sepsis Approximately
Intravenous Vitamin C Severe Sepsis Acute Lung Injury Alpha A. (Berry) Fowler, III, MD Professor of Medicine VCU Pulmonary Disease and Critical Care Medicine I Have No Disclosures Bacterial Sepsis Approximately
ICU Acquired Weakness Mobilisation Nutrition. ICU Acquired Weakness CRITICALLY ILL 20/10/2017. X. Wittebole Critical Care Department
 ICU Acquired Weakness Mobilisation Nutrition X. Wittebole Critical Care Department CRITICALLY ILL 2 ICU Acquired Weakness 1915: Sr W. OSLER The Principles of Medicine VIIIth Edition «Neuromuscular Dysfunction
ICU Acquired Weakness Mobilisation Nutrition X. Wittebole Critical Care Department CRITICALLY ILL 2 ICU Acquired Weakness 1915: Sr W. OSLER The Principles of Medicine VIIIth Edition «Neuromuscular Dysfunction