What you need to know about Delirium in ICU. Dr Valerie Page Watford General Hospital
|
|
|
- Cory Flynn
- 5 years ago
- Views:
Transcription
1 What you need to know about Delirium in ICU Dr Valerie Page Watford General Hospital
2 Delirium and outcome 40 year old ARDS ICU survivor college graduate I have been out of hospital and trying to get on with my life for the past 2 years. I have trouble with people s names that I have worked with for years. I can t remember where I put things at home. I can t help my children with their homework because I can t remember how to do simple multiplication problems.
3 What is happening in the brain? Oxidative stress Neurotransmitter imbalance Neuronal aging Inflammation Abnormal levels of large neutral amino acids

4 VISIONS A 46 year old woman ARDS, no delirium. B 42 year old woman ARDS, 12 days delirium Gunther CCM 2012

5 Global Cognition Scores in Survivors of Critical Illness. Pandharipande P et al. N Engl J Med 2013;369:

6 Post-operative cardiac surgery 225 patients 60 years or over CABG or valve replacement Cognitive function monitored with MMSE Delirium diagnosed using CAM KATZ index of ADLs
7 Results -trajectories 46% patients developed delirium Time to return to preoperative MMSE No delirium: 1 month. Delirium: not returned by 1 year, still improving up to 6 months
8 Cognitive outcomes Hope-ICU Telephone Interview of Cognitive Status Haloperidol Placebo TICS-M Median (IQR) n = (18-27) 21 (18-24) 31 cutoff score separates MCI from normal cognition (sensitivity 71.4%) 27 score separates MCI from dementia (sensitivity 69%).
9 The delirium experience The rest of my stay in ICU was filled with more incidents of despair, humiliation and terror. I saw a patient stabbed to death by his wife, and two people committing suicide. I witnessed arguments, in my mind all caused by me, and the pain I felt as my lungs started to recover was all part of a plan to give me pain inducing drugs in fact I had seen doctors laughing about it. The day after I was extubated I found myself in the High Dependency Unit, where the sheer terror of the execution attempts began.
10 Delirium DSM V Disturbance in attention and awareness Acute onset and fluctuates Disturbance in cognition Not explained by pre-existing, established or evolving neurocognitive disorder and noncomatose patient Evidence for cause American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Arlington, VA: American Psychiatric Publishing.
11 Subsyndromal delirium One or more symptoms Not meeting full criteria Not progressing to delirium Intermediate outcomes
12
13 North America SLEAP trial 420 ventilated patients APACHE 23 54% delirium, 4% ICDSC 0 throughout BRAIN trial 821 patients APACHE 25 74% delirium Mehta S, Cook D, Devlin JW, et al Prevalence, risk factors, and outcomes of delirium in mechanically ventilated adults. Crit Care Med. 2015; 43 : P.P. Pandharipande, T.D. Girard, J.C. Jackson, et al. Long-Term Cognitive Impairment after Critical Illness. N Engl J Med 2013; 369:
14 Netherlands Netherlands: Before/after study: 476 patients before/after study 44% to 97% Observational study: 1112 consecutive patients 50% at least 1 episode van den Boogaard M et al. Haloperidol prophylaxis in critically ill patients with a high risk for delirium. Crit Care Jan 17;17:R9. Klowenberg K et al. The attributable mortality of delirium in critically ill patients: prospective cohort study. BMJ 2014; 349: g6652
15 World ICU population Belgium 15% Germany 26.9% Sweden 39% Australia 12.4% UK 32.4% Van den Boogaard Intensive care medicine 2014; 40: 361-9
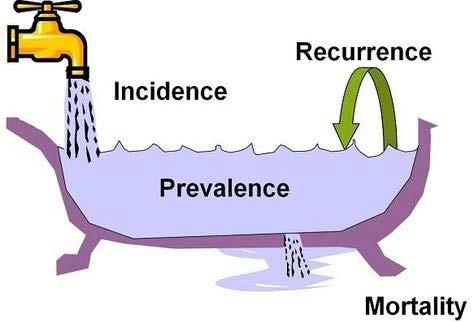
16 Incidence Acute general hospital 1000 beds = 100 delirious patients Critical Care 1:5 high dependency up to 4:5 sick ventilated patients Compare 3:5 with fractured neck of femur
17 Watford Incidence of delirium by subgroup Crit Care 2009; 13: R16 Elective post-operative (n=23) Emergency admissions (n=57) Ventilated patients (n=27) Delirious Not delirious 1 (4%) 22 (96%) 22 (45%) 27 (55%) 17 (63%) 10 (37%)


18 What does it look like?
19 Delirium motoric types Hyperactive psychomotor agitation Hypoactive psychomotor lethargy and sedation, appears quiet & co-operative BUT with inattention and disorganised thinking. Mixed fluctuating hypo/hyperactive symptoms

20 Identification

21 CAM-ICU
22 Diagnosing delirium 46 patients Median age 73 years (IQR = 64 80) CAM-ICU scores during 425 patient days Delirium in 50% of the patients 3 days (range 1 9). Clinical detection 24%

23 Can delirium be diagnosed in sedated patients? Patel SB. AJRCCM 2014;189: Takala J. AJRCCM 2014;189:622-24
24 Sedation related delirium 102 of 256 patients Paired CAM-ICU before and after SAT 28.9% CAM-ICU (n=11)negative after SAT 89% at least 1 day delirium pre vs. 77% post. Outcomes, same for rapidly reversible as no delirium.
25 Can delirium be diagnosed in comatose patients?
26 We Know More sedation, more delirium More delirium, worse outcomes Less sedation, better outcomes Balas MC et al Crit Care Med 2014, Jackson DL et al Crit Care 2010, Dale CR Ann Am Thorac Soc 2014, Shehabi Y et al Intensive Care Med 2013, Tanaka LMS et al, Crit Care 2014, Porhomayon J et al. J Cardiovasc Thorac Res 2015, Girard TD et al. Lancet 2008; 371 (9607)
27 Sedation induced coma RASS -3 to -5 SPICE/ANZICS trial deep sedation throughout the first 48 hours in 171 (68%) patients SPICE group Malaysia deep sedation in 159 (61%) patients and 1,658 (59%) of all RASS assessments at 48 hours. ABC trial day 1, 52% control group, 56% intervention group were in coma. Shehabi Y, et al. Intensive Care Med 2013; 39: 910-8, Shehabi Y et al Sedation Practice in Intensive Care Evaluation (SPICE) Study Investigators; ANZICS Clinical Trials Group. Am J Respir Crit Care Med. 2012; 186: Girard TD et al. Lancet 2008; 371:
28 Watford first 2 days Average number of RASS per shift 3.56 Number of RASS -1 to +1 = 18.7% In 28.3% of patients No correlation with APACHE
29 Delirium or Depression? The symptoms of delirium, when they are present, are prominent and take diagnostic precedence as delirium frequently indicates serious and urgent physical pathology or morbidity. Because of their clinical overlap, in a hospital setting, clinicians should not rule out delirium in any patient with suspected depression Take home messages: O Sullivan et al Lancet Psychiatry 2014
30 Delirium or Depression? Overlapping features Affective changes Sleep disturbance Underactivity or lethargy Apathy Agitation Impaired speed of information processing Delusions or hallucinations Impaired memory
31 Delirium Prominent features Fluctuation in intensity of symptoms Acute onset Altered consciousness Marked inattention Underlying physical cause Disorientation Disorganised thinking Poor comprehension
32 Figure. Multifactorial model of delirium in older people Onset of delirium is dependent on a complex interaction between the patient's baseline vulnerability (predisposing factors) at admission and precipitating factors or noxious insults.. Sharon K Inouye, Rudi GJ Westendorp, Jane S Saczynski Delirium in elderly people, Volume 383, Issue 9920, 2014,

33 Risk factors Host factors Acute illness Iatro/environ Elderly Severe sepsis Sedative/analges Co-morbidities ARDS Immobilisation Pre-existing cognitive impair Hearing/vision impairment MODS Drug OD or illicit drugs TPN Sleep deprivation Neurological dis Nosocomial inf. Malnutrition Alcohol/smoker Met. disturbance Anaemia
34 Sedation score and delirium screening Identify and treat precipitating factor Minimise impact of predisposing factors Pharmacological therapy Management
35 Predisposing factors? Management non-pharmacological Delirium bundle, optimisation of risk factors Address visual, hearing impairment Orientation Familiar nurse Mobilisation Drug overhaul Sleep Naughton et al. J Am Geriatri Soc 2005;53:18-23, Lundstrom et al J Am Geriatri Soc 2005;53:622-28
36 Drugs and delirium Opiate analgesics Benzodiazepines Corticosteroids Anticholinergic load Furosemide Ranitidine Digoxin

37 Brain road map for rounds (script for interdisciplinary communication)
38 SLEEP, ITS IMPORTANCE IN PREVENTING INSANITY We wish we could impress upon all, the vast importance of securing sound and abundant sleep ; if so, we should feel that we had done an immense good to our fellow-beings, not merely in preventing insanity, but other diseases also. American Journal of Insanity Boston Med Surg J 1845; 32:
39 Deep sedation = Sleep deprivation
40 Sleep and sedatives Not cyclical medication specific, dose dependent Decrease in SWS & REM sleep?restorative Benzos and Propofol activate GABA in VLPO suppress histamine release from TMN NA release from LC not inhibited Overdose burst suppression
41 Sleep disturbance - sedatives Observational study 21 ventilated patients Polysomnography Opiates 100%, Benzo 23%, Propofol 82% Normal features of sleep not identified REM in 2 subjects?altered state of consciousness, continual sleep deprivation Gehlbach et al Sleep 2012; 35: 1105
42 Delirium Does sleep deprivation contribute to delirium? Does delirium contribute to sleep deprivation? Review of 17 surgical studies not a risk factor Plausible but not proven
43 Case story Independent Lives alone Widow 2 years Was refused hip operation Suffers from pain
44 Day 8/9 RASS +4 Intermittent fast AF Palliative care referral. Continued quetiapine at night 0.5mgs lorazepam iv Lines out Continue NG feed
45 Day 10 Woke up Asked for her glasses RASS 0 CAM-ICU positive Delirium cleared Discharged to ward
46

47 Patients

48 Friends and Family
49
50 Acknowledgements Professor Danny McAuley, Queens University, Belfast Drs Tim Alce & Annalisa Casarin Research Fellows Xiao Bei Zhao RN Dr Neil Soni, Imperial College, London Watford ICU staff Intensive Care Foundation
Delirium in Critical Care. Recognition, Management, Research tasters. Dr Valerie Page Watford General Hospital
 Delirium in Critical Care. Recognition, Management, Research tasters Dr Valerie Page Watford General Hospital What does it look like? Diagnosing delirium CAM-ICU CAM-ICU Feature 1: Acute onset of mental
Delirium in Critical Care. Recognition, Management, Research tasters Dr Valerie Page Watford General Hospital What does it look like? Diagnosing delirium CAM-ICU CAM-ICU Feature 1: Acute onset of mental
Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh. Professor of Critical Care, Edinburgh University
 Tim Walsh. Professor of Critical Care, Edinburgh University") Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh Professor of Critical Care, Edinburgh University Lecture Plan: a route to clarity What is delirium? Why is delirium important? Step
Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh Professor of Critical Care, Edinburgh University Lecture Plan: a route to clarity What is delirium? Why is delirium important? Step
Delirium in the ICU: Prevention and Treatment. Delirium Defined Officially. Delirium: Really Defined. S. Andrew Josephson, MD
 Delirium in the ICU: Prevention and Treatment S. Andrew Josephson, MD Director, Neurohospitalist Service Medical Director, Inpatient Neurology June 2, 2011 Delirium Defined Officially (DSM-IV-TR) criteria
Delirium in the ICU: Prevention and Treatment S. Andrew Josephson, MD Director, Neurohospitalist Service Medical Director, Inpatient Neurology June 2, 2011 Delirium Defined Officially (DSM-IV-TR) criteria
Delirium in the Elderly
 Delirium in the Elderly ELITE 2017 Liza Genao, MD Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity Very much under-recognized
Delirium in the Elderly ELITE 2017 Liza Genao, MD Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity Very much under-recognized
Management of Delirium in the ICU. Yahya Shehabi
 Management of Delirium in the ICU Yahya Shehabi Hello! Doctor, your patient is CAM + ve Good morning Dr, Am one of the RC, Just examined Mr XXX he is CAM +ve Positive what? Sir replied RC: I meant he is
Management of Delirium in the ICU Yahya Shehabi Hello! Doctor, your patient is CAM + ve Good morning Dr, Am one of the RC, Just examined Mr XXX he is CAM +ve Positive what? Sir replied RC: I meant he is
Delirium in the Elderly
 Delirium in the Elderly ELITE 2015 Mamata Yanamadala M.B.B.S, MS Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity
Delirium in the Elderly ELITE 2015 Mamata Yanamadala M.B.B.S, MS Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity
Strategies to minimize delirium for hip fracture patients
 Strategies to minimize delirium for hip fracture patients Stephen L Kates, M.D. Professor and Chairman Department Date of Orthopaedic Surgery Delirium incidence Up to 61% of hip fracture patients get delirium
Strategies to minimize delirium for hip fracture patients Stephen L Kates, M.D. Professor and Chairman Department Date of Orthopaedic Surgery Delirium incidence Up to 61% of hip fracture patients get delirium
KEY REFERENCES Laying the foundation for D of ABCDEF bundle
 KEY REFERENCES Laying the foundation for D of ABCDEF bundle Ely E. JAMA. 2001;286:2703-2710 (CAM-ICU) Bergeron N. Intensive Care Med. 2001;27:859-864 (ICDSC) Dubois M. Intensive Care Med. 2001;27:1297-1304
KEY REFERENCES Laying the foundation for D of ABCDEF bundle Ely E. JAMA. 2001;286:2703-2710 (CAM-ICU) Bergeron N. Intensive Care Med. 2001;27:859-864 (ICDSC) Dubois M. Intensive Care Med. 2001;27:1297-1304
Conducting Delirium Research
 Optimizing Clinical Trials When Conducting Research Research funding: Disclosure NHLBI, NIA, AstraZeneca John W. Devlin, PharmD, FCCP, FCCM, Professor of Pharmacy, Northeastern University Scientific Staff,
Optimizing Clinical Trials When Conducting Research Research funding: Disclosure NHLBI, NIA, AstraZeneca John W. Devlin, PharmD, FCCP, FCCM, Professor of Pharmacy, Northeastern University Scientific Staff,
Sarah V. Cogle, PharmD, BCCCP Assistant Clinical Professor Auburn University Harrison School of Pharmacy Auburn, AL ALSHP Annual Clinical Meeting
 Sarah V. Cogle, PharmD, BCCCP Assistant Clinical Professor Auburn University Harrison School of Pharmacy Auburn, AL ALSHP Annual Clinical Meeting 2018 I have no actual or potential conflict of interest
Sarah V. Cogle, PharmD, BCCCP Assistant Clinical Professor Auburn University Harrison School of Pharmacy Auburn, AL ALSHP Annual Clinical Meeting 2018 I have no actual or potential conflict of interest
+ Change in baseline mental status, inattention, and either disorganized thinking or altered level of consciousness. Delirium. Disclosure.
 47 th Annual Meeting August 2-4, 2013 Orlando, FL Identification, Prevention and Treatment of Delirium: The Role of the Health System Pharmacist Jennifer Cortes, PharmD, BCPS Medical ICU Clinical Pharmacy
47 th Annual Meeting August 2-4, 2013 Orlando, FL Identification, Prevention and Treatment of Delirium: The Role of the Health System Pharmacist Jennifer Cortes, PharmD, BCPS Medical ICU Clinical Pharmacy
Delirium in the hospitalized patient
 Delirium in the hospitalized patient Jennifer A. Tarin, M.D. Department of Hospital Medicine Geriatric Health Safety Chair Colorado Permanente Medical Group UCLA Reynolds Scholar Delirium Preventing delirium
Delirium in the hospitalized patient Jennifer A. Tarin, M.D. Department of Hospital Medicine Geriatric Health Safety Chair Colorado Permanente Medical Group UCLA Reynolds Scholar Delirium Preventing delirium
ICU Delirium and sedation: understanding their role in long-term patient outcomes. Yoanna Skrobik MD FRCP(c)
") ICU Delirium and sedation: understanding their role in long-term patient outcomes Yoanna Skrobik MD FRCP(c) Conflicts of interest Member, SCCM Pain, Agitation and Delirium guidelines writing committee
ICU Delirium and sedation: understanding their role in long-term patient outcomes Yoanna Skrobik MD FRCP(c) Conflicts of interest Member, SCCM Pain, Agitation and Delirium guidelines writing committee
ICU Delirium in Infants & Children: Cause for Concern or False Alarm. Objectives
 ICU Delirium in Infants & Children: Cause for Concern or False Alarm Peter (Pete) N. Johnson, Pharm.D., BCPS, BCPPS, FPPAG Associate Professor of Pharmacy Practice University of Oklahoma College of Pharmacy
ICU Delirium in Infants & Children: Cause for Concern or False Alarm Peter (Pete) N. Johnson, Pharm.D., BCPS, BCPPS, FPPAG Associate Professor of Pharmacy Practice University of Oklahoma College of Pharmacy
DELIRIUM IN ICU: Prevention and Management. Milind Baldi
 DELIRIUM IN ICU: Prevention and Management Milind Baldi Contents Introduction Risk factors Assessment Prevention Management Introduction Delirium is a syndrome characterized by acute cerebral dysfunction
DELIRIUM IN ICU: Prevention and Management Milind Baldi Contents Introduction Risk factors Assessment Prevention Management Introduction Delirium is a syndrome characterized by acute cerebral dysfunction
Delirium assessment and management. Dr Kim Jeffs Northern Health
 Delirium assessment and management Dr Kim Jeffs Northern Health What do you need to know? Epidemiology How big is the problem? Who is at risk? Assessment Tools for diagnosis Prevention Evidence base Management
Delirium assessment and management Dr Kim Jeffs Northern Health What do you need to know? Epidemiology How big is the problem? Who is at risk? Assessment Tools for diagnosis Prevention Evidence base Management
Overview of Presentation. Delirium Definition. Assessing & Managing ICU Delirium: What is the Evidence?
 Assessing & Managing ICU Delirium: What is the Evidence? Dale Needham, MD, PhD Professor Pulmonary & Critical Care Medicine, and Physical Medicine & Rehabilitation Medical Director, Critical Care Physical
Assessing & Managing ICU Delirium: What is the Evidence? Dale Needham, MD, PhD Professor Pulmonary & Critical Care Medicine, and Physical Medicine & Rehabilitation Medical Director, Critical Care Physical
ABCs of ICU Delirium Marian Maxwell, Pharm.D., BCCCP January 6, 2018
 ABCs of ICU Delirium Marian Maxwell, Pharm.D., BCCCP January 6, 2018 Disclosures I do not have any financial/non-financial relationships to disclose. Learning Objectives Define delirium and discuss the
ABCs of ICU Delirium Marian Maxwell, Pharm.D., BCCCP January 6, 2018 Disclosures I do not have any financial/non-financial relationships to disclose. Learning Objectives Define delirium and discuss the
Do you know. Assessment of Delirium. What is Delirium? Which syndrome occurs more commonly in elderly populations? a. Delirium b.
 Assessment of Delirium Marianne McCarthy, PhD, GNP, PMHNP Arizona State University College of Nursing and Health Innovation What is Delirium? Delirium is a common clinical syndrome characterized by: Inattention
Assessment of Delirium Marianne McCarthy, PhD, GNP, PMHNP Arizona State University College of Nursing and Health Innovation What is Delirium? Delirium is a common clinical syndrome characterized by: Inattention
Delirium and Dementia. Summary
 Delirium and Dementia Paul Kettl, M.D., M.H.A. Summary DELIRIUM Acute brain failure Identify cause (meds, infection) Treat sx Poor prognostic sign DEMENTIA Chronic brain failure AD most common cause Often
Delirium and Dementia Paul Kettl, M.D., M.H.A. Summary DELIRIUM Acute brain failure Identify cause (meds, infection) Treat sx Poor prognostic sign DEMENTIA Chronic brain failure AD most common cause Often
Delirium. Dr. Lesley Wiesenfeld. Deputy Psychiatrist in Chief, Mount Sinai Hospital. Dr. Carole Cohen
 Delirium Dr. Lesley Wiesenfeld Deputy Psychiatrist in Chief, Mount Sinai Hospital Dr. Carole Cohen Department of Psychiatry, University of Toronto and Sunnybrook Health Sciences Centre Case Study Mrs B
Delirium Dr. Lesley Wiesenfeld Deputy Psychiatrist in Chief, Mount Sinai Hospital Dr. Carole Cohen Department of Psychiatry, University of Toronto and Sunnybrook Health Sciences Centre Case Study Mrs B
Drug induced delirium
 Drug induced delirium Knut Erik Hovda, MD, PhD, FACMT, FEAPCCT The Norwegian CBRNe Centre of Medicine Department of Acute Medicine Oslo University hospital Content 1. Introduction 2. Risk factors 3. Prevalence
Drug induced delirium Knut Erik Hovda, MD, PhD, FACMT, FEAPCCT The Norwegian CBRNe Centre of Medicine Department of Acute Medicine Oslo University hospital Content 1. Introduction 2. Risk factors 3. Prevalence
Critical Care Pharmacological Management of Delirium
 Critical Care Pharmacological Management of Delirium Policy Title: in the Critical Care Unit Executive Summary: This policy provides guidance Pharmacological Management of delirium in the Critical Care
Critical Care Pharmacological Management of Delirium Policy Title: in the Critical Care Unit Executive Summary: This policy provides guidance Pharmacological Management of delirium in the Critical Care
Implementation of a Delirium Screening Tool in a Pediatric Intensive Care Unit
 Implementation of a Delirium Screening Tool in a Pediatric Intensive Care Unit BY: ABBY WACHHOLTZ, BSN, RN, PEDIATRIC ACUTE CARE DNP STUDENT Disclosures I have no disclosures. 1 Objectives 1. Recognize
Implementation of a Delirium Screening Tool in a Pediatric Intensive Care Unit BY: ABBY WACHHOLTZ, BSN, RN, PEDIATRIC ACUTE CARE DNP STUDENT Disclosures I have no disclosures. 1 Objectives 1. Recognize
Can Goal Directed Sedation Improve Outcomes?
 Can Goal Directed Sedation Improve Outcomes? Yahya SHEHABI, FANZCA, FCICM, EMBA Professor and Program Director Critical care Monash Health and Monash University - Melbourne School of Medicine, University
Can Goal Directed Sedation Improve Outcomes? Yahya SHEHABI, FANZCA, FCICM, EMBA Professor and Program Director Critical care Monash Health and Monash University - Melbourne School of Medicine, University
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative
 Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Jacinta Lucke Resident Emergency Medicine PHD Gerontology & Geriatrics
 Jacinta Lucke Resident Emergency Medicine PHD Gerontology & Geriatrics TAKE HOME MESSAGE When managing confusion in older patients: Routinely screen for impaired cognition Patients with impaired cognition
Jacinta Lucke Resident Emergency Medicine PHD Gerontology & Geriatrics TAKE HOME MESSAGE When managing confusion in older patients: Routinely screen for impaired cognition Patients with impaired cognition
Delirium in Older Persons: An Investigative Journey
 Delirium in Older Persons: An Investigative Journey Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley F. Levy Family Chair
Delirium in Older Persons: An Investigative Journey Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley F. Levy Family Chair
Fighting the Fog A Collaborative Approach to Decreasing ICU Delirium
 Fighting the Fog A Collaborative Approach to Decreasing ICU Delirium Kimberly Scherr NP Jennifer Barker RN Misericordia Hospital ICU Edmonton, AB CACCN Dynamics Sept 21, 2014 Delirium Delirium is an acute
Fighting the Fog A Collaborative Approach to Decreasing ICU Delirium Kimberly Scherr NP Jennifer Barker RN Misericordia Hospital ICU Edmonton, AB CACCN Dynamics Sept 21, 2014 Delirium Delirium is an acute
Delirium. Dr. John Puxty
 Delirium Dr. John Puxty Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors, causes and main
Delirium Dr. John Puxty Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors, causes and main
Disclosure. Hospira Pharmaceuticals. Unrestricted research funding Honoraria for CME education administered via France Foundation
 Disclosure Hospira Pharmaceuticals Unrestricted research funding Honoraria for CME education administered via France Foundation Economics in Sedation: Responsible Use of the ICU Budget John W. Devlin,
Disclosure Hospira Pharmaceuticals Unrestricted research funding Honoraria for CME education administered via France Foundation Economics in Sedation: Responsible Use of the ICU Budget John W. Devlin,
Delirium. A Plan to Reduce Use of Restraints. David Wensel DO, FAAHPM Medical Director Midland Care
 Delirium A Plan to Reduce Use of Restraints David Wensel DO, FAAHPM Medical Director Midland Care Objectives Define delirium Describe pathophysiology of delirium Understand most common etiologies Define
Delirium A Plan to Reduce Use of Restraints David Wensel DO, FAAHPM Medical Director Midland Care Objectives Define delirium Describe pathophysiology of delirium Understand most common etiologies Define
Delirium Prevention: The State-of-the-Art & Implications to Improve Care in our State
 Delirium Prevention: The State-of-the-Art & Implications to Improve Care in our State Jonny Macias, MD & Michael Malone, MD Aurora Health Care/ University of Wisconsin School of Medicine & Public Health
Delirium Prevention: The State-of-the-Art & Implications to Improve Care in our State Jonny Macias, MD & Michael Malone, MD Aurora Health Care/ University of Wisconsin School of Medicine & Public Health
Management of delirium in mechanically ventilated patients. Advances in Critical Care Medicine King Hussein Cancer Center
 Management of delirium in mechanically ventilated patients Advances in Critical Care Medicine King Hussein Cancer Center Introduction Outline: Prevalence of delirium in ICU Why it is important to screen
Management of delirium in mechanically ventilated patients Advances in Critical Care Medicine King Hussein Cancer Center Introduction Outline: Prevalence of delirium in ICU Why it is important to screen
Delirium Screening: The next nurse sensitive indicator?
 Delirium Screening: The next nurse sensitive indicator? Sharon Gunn, MSN, MA, RN, ACNS-BC, CCRN Clinical Nurse Specialist Critical Care Baylor University Medical Center Dallas, TX Objectives Recognize
Delirium Screening: The next nurse sensitive indicator? Sharon Gunn, MSN, MA, RN, ACNS-BC, CCRN Clinical Nurse Specialist Critical Care Baylor University Medical Center Dallas, TX Objectives Recognize
Sedation and delirium- drugs and clinical management
 Sedation and delirium- drugs and clinical management Shannon S. Carson, MD Associate Professor and Chief Division of Pulmonary and Critical Care Medicine University of North Carolina Probability of transitioning
Sedation and delirium- drugs and clinical management Shannon S. Carson, MD Associate Professor and Chief Division of Pulmonary and Critical Care Medicine University of North Carolina Probability of transitioning
5 older patients become. What is delirium? (Acute confusional state) Where We ve Been and
 Where We ve Been and") Update on Delirium: Where We ve Been and Where We re Going Sharon K. Inouye, M.D., M.P.H. M PH Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley F. Levy
Update on Delirium: Where We ve Been and Where We re Going Sharon K. Inouye, M.D., M.P.H. M PH Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley F. Levy
Ventilator-Associated Event Prevention: Innovations
 Ventilator-Associated Event Prevention: Innovations Michael J. Apostolakos, MD Professor of Medicine Director, Adult Critical Care University of Rochester Mobility/Sedation in the ICU Old teaching: Keep
Ventilator-Associated Event Prevention: Innovations Michael J. Apostolakos, MD Professor of Medicine Director, Adult Critical Care University of Rochester Mobility/Sedation in the ICU Old teaching: Keep
Delirium in Older Persons
 Objectives Delirium in Older Persons ELITE 2018 Liza Isabel Genao, MD Division of Geriatrics Describe rate, cost, complications of delirium Effectively diagnose the syndrome Describe multicomponent model
Objectives Delirium in Older Persons ELITE 2018 Liza Isabel Genao, MD Division of Geriatrics Describe rate, cost, complications of delirium Effectively diagnose the syndrome Describe multicomponent model
Delirium. Geriatric Giants Lecture Series Divisions of Geriatric Medicine and Care of the Elderly University of Alberta
 Delirium Geriatric Giants Lecture Series Divisions of Geriatric Medicine and Care of the Elderly University of Alberta Overview A. Delirium - the nature of the beast B. Significance of delirium C. An approach
Delirium Geriatric Giants Lecture Series Divisions of Geriatric Medicine and Care of the Elderly University of Alberta Overview A. Delirium - the nature of the beast B. Significance of delirium C. An approach
Delirium Pilot Project
 CCU Nurses: Delirium Pilot Project Our unit has been selected to develop and implement a delirium assessment and intervention program. We are beginning Phase 1 with education and assessing for our baseline
CCU Nurses: Delirium Pilot Project Our unit has been selected to develop and implement a delirium assessment and intervention program. We are beginning Phase 1 with education and assessing for our baseline
Sedation of the Critically Ill Patient
 Buffalo theory of sedation It s a well known fact that a herd of buffalo can only move as fast as the slowest buffalo. And when the herd is hunted, it s the slowest and weakest ones at the back that are
Buffalo theory of sedation It s a well known fact that a herd of buffalo can only move as fast as the slowest buffalo. And when the herd is hunted, it s the slowest and weakest ones at the back that are
Disentangling Delirium and Dementia
 Disentangling Delirium and Dementia Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley F. Levy Family Chair Director, Aging
Disentangling Delirium and Dementia Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley F. Levy Family Chair Director, Aging
Geriatrics and Cancer Care
 Geriatrics and Cancer Care Roger Wong, BMSc, MD, FRCPC, FACP Postgraduate Dean of Medical Education Clinical Professor, Division of Geriatric Medicine UBC Faculty of Medicine Disclosure No competing interests
Geriatrics and Cancer Care Roger Wong, BMSc, MD, FRCPC, FACP Postgraduate Dean of Medical Education Clinical Professor, Division of Geriatric Medicine UBC Faculty of Medicine Disclosure No competing interests
Delirium in Hospital Care
 Delirium in Hospital Care Dr John Puxty 1 Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors,
Delirium in Hospital Care Dr John Puxty 1 Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors,
Delirium Assessment. February 24, Susan Schumacher, MS, APRN-BC
 Delirium Assessment February 24, 2016 Susan Schumacher, MS, APRN-BC Objectives Define delirium Differentiate delirium from dementia Identify predisposing and precipitating factors leading to delirium.
Delirium Assessment February 24, 2016 Susan Schumacher, MS, APRN-BC Objectives Define delirium Differentiate delirium from dementia Identify predisposing and precipitating factors leading to delirium.
Delirium Screening Tools: Just- In- Time Education and Evaluation Using the EMR
 Delirium Screening Tools: Just- In- Time Education and Evaluation Using the EMR Implementation of an EMR based protocol for detection of delirium in elderly Medical and palliative care patients Parul Goyal,
Delirium Screening Tools: Just- In- Time Education and Evaluation Using the EMR Implementation of an EMR based protocol for detection of delirium in elderly Medical and palliative care patients Parul Goyal,
Delirium Screening and Prevention Faculty Disclosures
 Delirium Screening and Prevention Faculty Disclosures I have nothing to disclose Kathleen Puntillo RN, PhD, FAAN, FCCM Professor Emeritus School of Nursing, UCSF Objectives Discuss prevalence, risk factors
Delirium Screening and Prevention Faculty Disclosures I have nothing to disclose Kathleen Puntillo RN, PhD, FAAN, FCCM Professor Emeritus School of Nursing, UCSF Objectives Discuss prevalence, risk factors
Sedation and Delirium Questions
 Sedation and Delirium Questions TLC Curriculum William J. Ehlenbach, MD MSc Assistant Professor of Medicine Pulmonary & Critical Care Medicine Question 1 Deep sedation in ventilated critically patients
Sedation and Delirium Questions TLC Curriculum William J. Ehlenbach, MD MSc Assistant Professor of Medicine Pulmonary & Critical Care Medicine Question 1 Deep sedation in ventilated critically patients
ICU Liberation for the Pharmacist. A. Kendall Gross, PharmD, BCPS, BCCCP Critical Care Pharmacist UCSF Medical Center
 ICU Liberation for the Pharmacist A. Kendall Gross, PharmD, BCPS, BCCCP Critical Care Pharmacist UCSF Medical Center Disclosure No conflicts of interest to disclose Objectives o Outline the elements of
ICU Liberation for the Pharmacist A. Kendall Gross, PharmD, BCPS, BCCCP Critical Care Pharmacist UCSF Medical Center Disclosure No conflicts of interest to disclose Objectives o Outline the elements of
Delirium. A Geriatric Syndrome. Jonathan McCaleb, MD, CMD, HMDC UNSOM, Assistant Professor of Medicine Geriatrics / Hospice & Palliative Medicine
 Delirium A Geriatric Syndrome Jonathan McCaleb, MD, CMD, HMDC UNSOM, Assistant Professor of Medicine Geriatrics / Hospice & Palliative Medicine Introduction Common Serious Unrecognized: a medical emergency
Delirium A Geriatric Syndrome Jonathan McCaleb, MD, CMD, HMDC UNSOM, Assistant Professor of Medicine Geriatrics / Hospice & Palliative Medicine Introduction Common Serious Unrecognized: a medical emergency
Do benzos, opioids, or strong anticholinergics cause delirium? Lisa Burry
 Do benzos, opioids, or strong anticholinergics cause delirium? Lisa Burry Delirium in the ICU Occurs in up to 85% of MICU/SICU MV patients 20-50% of lower severity ICU patients develop delirium Hypoactive
Do benzos, opioids, or strong anticholinergics cause delirium? Lisa Burry Delirium in the ICU Occurs in up to 85% of MICU/SICU MV patients 20-50% of lower severity ICU patients develop delirium Hypoactive
Pain, Agitation & Delirium (2013) Immobility & Sleep (2018) Catherine Jones Practice Educator GICU October 2018
 Immobility & Sleep (2018) Catherine Jones Practice Educator GICU October 2018") Pain, Agitation & Delirium (2013) Immobility & Sleep (2018) Catherine Jones Practice Educator GICU October 2018 1 Plan for session Why Pain Agitation & Delirium are important considerations in critical
Pain, Agitation & Delirium (2013) Immobility & Sleep (2018) Catherine Jones Practice Educator GICU October 2018 1 Plan for session Why Pain Agitation & Delirium are important considerations in critical
Delirium. Assessment and Management
 Delirium Assessment and Management Goals and Objectives Participants will: 1. be able to recognize and diagnose the syndrome of delirium. 2. understand the causes of delirium. 3. become knowledgeable about
Delirium Assessment and Management Goals and Objectives Participants will: 1. be able to recognize and diagnose the syndrome of delirium. 2. understand the causes of delirium. 3. become knowledgeable about
譫妄症 (Delirium) Objectives. Epidemiology. Delirium. DSM-5 Diagnostic Criteria. Prognosis 台大醫院老年醫學部陳人豪 2016/8/28
 Objectives. Epidemiology. Delirium. DSM-5 Diagnostic Criteria. Prognosis 台大醫院老年醫學部陳人豪 2016/8/28") 譫妄症 (Delirium) 台大醫院老年醫學部陳人豪 2016/8/28 Objectives Delirium Epidemiology Etiology Diagnosis Evaluation and Management Postoperative delirium Delirium (and acute problematic behavior) in the longterm care
譫妄症 (Delirium) 台大醫院老年醫學部陳人豪 2016/8/28 Objectives Delirium Epidemiology Etiology Diagnosis Evaluation and Management Postoperative delirium Delirium (and acute problematic behavior) in the longterm care
Critical Care Pharmacological Management of Delirium
 Critical Care Pharmacological Management of Delirium Policy Title: in the Critical Care Unit Executive Summary: This policy provides guidance Pharmacological Management of delirium in the Critical Care
Critical Care Pharmacological Management of Delirium Policy Title: in the Critical Care Unit Executive Summary: This policy provides guidance Pharmacological Management of delirium in the Critical Care
Delirium. Approach. Symptom Update Masterclass:
 Symptom Update Masterclass: Delirium Jason Boland Senior Clinical Lecturer and Honorary Consultant in Palliative Medicine Wolfson Centre for Palliative Care Research Hull York Medical School University
Symptom Update Masterclass: Delirium Jason Boland Senior Clinical Lecturer and Honorary Consultant in Palliative Medicine Wolfson Centre for Palliative Care Research Hull York Medical School University
Decreasing Delirium Resolution Times for the Elderly: An Interprofessional Approach
 Decreasing Delirium Resolution Times for the Elderly: An Interprofessional Approach Featuring: Felice Rogers Evans BSN RN BC Ty Breiter MSN RN CNL Tampa General Hospital NICHE exemplar hospital Three time
Decreasing Delirium Resolution Times for the Elderly: An Interprofessional Approach Featuring: Felice Rogers Evans BSN RN BC Ty Breiter MSN RN CNL Tampa General Hospital NICHE exemplar hospital Three time
Delirium Assessment and management in relation to falls risk in hospital
 Delirium Assessment and management in relation to falls risk in hospital A house call - Mrs JM 95-year-old lady Normally cognitively intact Multiple medical problems, including falls Housebound, mobile
Delirium Assessment and management in relation to falls risk in hospital A house call - Mrs JM 95-year-old lady Normally cognitively intact Multiple medical problems, including falls Housebound, mobile
ICU LIBERATION: IMPLEMENTING THE ABCDEF BUNDLE AND IMPROVING THE LIVES OF ICU PATIENTS
 ICU LIBERATION: IMPLEMENTING THE ABCDEF BUNDLE AND IMPROVING THE LIVES OF ICU PATIENTS J. MATTHEW ALDRICH, MD ASSOCIATE CLINICAL PROFESSOR OF ANESTHESIA AND PERIOPERATIVE CARE UNIVERSITY OF CALIFORNIA
ICU LIBERATION: IMPLEMENTING THE ABCDEF BUNDLE AND IMPROVING THE LIVES OF ICU PATIENTS J. MATTHEW ALDRICH, MD ASSOCIATE CLINICAL PROFESSOR OF ANESTHESIA AND PERIOPERATIVE CARE UNIVERSITY OF CALIFORNIA
BRAIN. Tumor byproducts. Autonomic nerves. Somatic nerves. Host immune cells. Cytokines
 Patient s Problems Pain (80%) Fatigue (90%) Weight Loss (80%) Lack of Appetite (80%) Nausea, Vomiting (90%) Anxiety (25%) Shortness of Breath (50%) Confusion-Agitation (80%) Tumor Mass Tumor Function Somatic
Patient s Problems Pain (80%) Fatigue (90%) Weight Loss (80%) Lack of Appetite (80%) Nausea, Vomiting (90%) Anxiety (25%) Shortness of Breath (50%) Confusion-Agitation (80%) Tumor Mass Tumor Function Somatic
PRESCRIBING PRACTICE IN DELIRIUM. John Warburton Critical Care Pharmacist
 PRESCRIBING PRACTICE IN DELIRIUM John Warburton Critical Care Pharmacist Learning outcomes Modifiable medication risk factors for delirium An appreciation of contributing factors modifiable with medicines
PRESCRIBING PRACTICE IN DELIRIUM John Warburton Critical Care Pharmacist Learning outcomes Modifiable medication risk factors for delirium An appreciation of contributing factors modifiable with medicines
Delirium Screening and Prevention. Faculty Disclosures. Objectives 5/13/2014. I have nothing to disclose
 Delirium Screening and Prevention Kathleen Puntillo RN, PhD, FAAN, FCCM Professor Emeritus School of Nursing, UCSF Faculty Disclosures I have nothing to disclose Objectives Discuss prevalence, risk factors
Delirium Screening and Prevention Kathleen Puntillo RN, PhD, FAAN, FCCM Professor Emeritus School of Nursing, UCSF Faculty Disclosures I have nothing to disclose Objectives Discuss prevalence, risk factors
Monday, 23 July 2018: 8:30 AM-9:45 AM STTI Australia
 Shu-Ming Chen RN, PhD, Assistant Professor, College of Nursing, Fooyin University, Kaohsiung, Taiwan, R. O.C. 29th International Nursing Research Congress Monday, 23 July 2018: 8:30 AM-9:45 AM STTI Australia
Shu-Ming Chen RN, PhD, Assistant Professor, College of Nursing, Fooyin University, Kaohsiung, Taiwan, R. O.C. 29th International Nursing Research Congress Monday, 23 July 2018: 8:30 AM-9:45 AM STTI Australia
Canadian Practices for the Treatment of Delirium. Lisa Burry, BScPharm, PharmD
 Canadian Practices for the Treatment of Delirium Lisa Burry, BScPharm, PharmD Disclosures & Acknowledgements Conflicts of interest: None Acknowledgements: our patients and the clinical staff that supported
Canadian Practices for the Treatment of Delirium Lisa Burry, BScPharm, PharmD Disclosures & Acknowledgements Conflicts of interest: None Acknowledgements: our patients and the clinical staff that supported
5 older patients become delirious every minute
 Management of Delirium: Nonpharmacologic and Pharmacologic Approaches Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley
Management of Delirium: Nonpharmacologic and Pharmacologic Approaches Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley
Research & Reviews: Journal of Nursing & Health Sciences
 Research & Reviews: Journal of Nursing & Health Sciences A Cohort Study on Detecting Delirium Using 4 A s Test in a London, UK, Hospital Annalisa Casarin 1,2,3, Pranev Sharma 4, Satyawan Bhat 2,3, Marcela
Research & Reviews: Journal of Nursing & Health Sciences A Cohort Study on Detecting Delirium Using 4 A s Test in a London, UK, Hospital Annalisa Casarin 1,2,3, Pranev Sharma 4, Satyawan Bhat 2,3, Marcela
nicheprogram.org 16th Annual NICHE Conference Forging New Paths and Partnerships 1
 Improving Patient Outcomes in Geriatric Post-Operative Orthopedic Patients: Translating Research into Practice Tripping into The CAM Presented by: Diana LaBumbard, RN, MSN, ACNP/GNP-BC, CWOCN Denise Williams,
Improving Patient Outcomes in Geriatric Post-Operative Orthopedic Patients: Translating Research into Practice Tripping into The CAM Presented by: Diana LaBumbard, RN, MSN, ACNP/GNP-BC, CWOCN Denise Williams,
Cognitive Status. Read each question below to the patient. Score one point for each correct response.
 Diagnosis of dementia or delirium Cognitive Status Six Item Screener Read to the patient: I have a few questions I would like to ask you. First, I am going to name three objects. After I have said all
Diagnosis of dementia or delirium Cognitive Status Six Item Screener Read to the patient: I have a few questions I would like to ask you. First, I am going to name three objects. After I have said all
DELIRIUM. J. Sukanya 28.Jun.12
 DELIRIUM J. Sukanya 28.Jun.12 Outline Why? What? How? What s next? Delirium Introduction Delirium An acute decline in attention and cognition The most frequent neuropsychiatric syndrome A common, life-threatening,
DELIRIUM J. Sukanya 28.Jun.12 Outline Why? What? How? What s next? Delirium Introduction Delirium An acute decline in attention and cognition The most frequent neuropsychiatric syndrome A common, life-threatening,
Delirium in the Elderly
 Delirium in the Elderly Jeffrey M. Burock, MD Division Director/ Psychiatry / Miriam Hospital Clinical Assistant Professor Warren Alpert School Of Medicine Learning Objectives Identify the symptoms of
Delirium in the Elderly Jeffrey M. Burock, MD Division Director/ Psychiatry / Miriam Hospital Clinical Assistant Professor Warren Alpert School Of Medicine Learning Objectives Identify the symptoms of
Update - Delirium in Elders
 Update - Delirium in Elders Impact Recognition Prevention, and Management Michael J. Lichtenstein, MD F. Carter Pannill, Jr. Professor of Medicine Chief, Division of Geriatrics, Gerontology and Palliative
Update - Delirium in Elders Impact Recognition Prevention, and Management Michael J. Lichtenstein, MD F. Carter Pannill, Jr. Professor of Medicine Chief, Division of Geriatrics, Gerontology and Palliative
Disclosures. Post operative Delirium. Set up audience participation. Delirium Definitions. Incidence of Delirium
 Post operative Delirium Disclosures IP for monitoring technology licensed to Medtronic Ken Brady, MD Pediatrics, Anesthesia, Critical Care Texas Children s Hospital Baylor College of Medicine Set up audience
Post operative Delirium Disclosures IP for monitoring technology licensed to Medtronic Ken Brady, MD Pediatrics, Anesthesia, Critical Care Texas Children s Hospital Baylor College of Medicine Set up audience
Palliative Care and Delirium. Ambereen K. Mehta, MD MPH Assistant Professor Division of General Medicine, Geriatrics, and Palliative Care
 Palliative Care and Delirium Ambereen K. Mehta, MD MPH Assistant Professor Division of General Medicine, Geriatrics, and Palliative Care Disclosures I have no personal or professional financial relationships
Palliative Care and Delirium Ambereen K. Mehta, MD MPH Assistant Professor Division of General Medicine, Geriatrics, and Palliative Care Disclosures I have no personal or professional financial relationships
David A Scott Lis Evered. Department of Anaesthesia and Acute Pain Medicine St Vincent s Hospital, Melbourne University of Melbourne
 David A Scott Lis Evered Department of Anaesthesia and Acute Pain Medicine St Vincent s Hospital, Melbourne University of Melbourne This talk will include live polling so please be sure to have the meeting
David A Scott Lis Evered Department of Anaesthesia and Acute Pain Medicine St Vincent s Hospital, Melbourne University of Melbourne This talk will include live polling so please be sure to have the meeting
Conflict of Interest. Patient Case. Objectives. The Balancing Act. Why We Need Sedation
 Agitation in the ICU Have we swung the pendulum too far from benzodiazepines? Conflict of Interest The author of this presentation has no conflicts of interest to disclose Nina Vadiei, PharmD PGY1 Pharmacy
Agitation in the ICU Have we swung the pendulum too far from benzodiazepines? Conflict of Interest The author of this presentation has no conflicts of interest to disclose Nina Vadiei, PharmD PGY1 Pharmacy
Test your Knowledge: Recognizing Delirium
 The Ottawa Hospital Name: Unit: Profession: RN RPN PT OT SW Other Note: Each question has only one correct answer. 1. If a patient is identified as being at high risk for developing delirium, his/her mental
The Ottawa Hospital Name: Unit: Profession: RN RPN PT OT SW Other Note: Each question has only one correct answer. 1. If a patient is identified as being at high risk for developing delirium, his/her mental
Chapter 01 Introduction
 Chapter 01 Introduction Defining the Elderly There is no universally accepted age cut-off defining elderly. This reflects the fact that chronological age itself is less important than biological events
Chapter 01 Introduction Defining the Elderly There is no universally accepted age cut-off defining elderly. This reflects the fact that chronological age itself is less important than biological events
Delirium. Delirium. Delirium Etiology and Pathophysiology. Fall 2018
 Three most common cognitive problems in adults 1. (acute confusion) 2. Dementia 3. Depression These problems often occur together Can you think of common stimuli for each? 1 1 State of temporary but acute
Three most common cognitive problems in adults 1. (acute confusion) 2. Dementia 3. Depression These problems often occur together Can you think of common stimuli for each? 1 1 State of temporary but acute
Jie Chen Department of Critical Care Medicine, Zhongda Hospital, School of Medicine, Southeast University
 Jie Chen Department of Critical Care Medicine, Zhongda Hospital, School of Medicine, Southeast University Crit Care Med. 2004;32(4):955 62. BMJ. 2015;350:h2538. Background Delirium, defined as acute brain
Jie Chen Department of Critical Care Medicine, Zhongda Hospital, School of Medicine, Southeast University Crit Care Med. 2004;32(4):955 62. BMJ. 2015;350:h2538. Background Delirium, defined as acute brain
Supplementary appendix
 Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Page VJ, Casarin A, Ely EW, et al. Evaluation
Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Page VJ, Casarin A, Ely EW, et al. Evaluation
ICU Updates: Delirium in Hospitalized Patients
 ICU Updates: Delirium in Hospitalized Patients James A. Frank, MD Associate Professor Pulmonary and Critical Care UCSF Dept. of Medicine Director, MICU San Francisco VAMC Recognizing and preventing delirium
ICU Updates: Delirium in Hospitalized Patients James A. Frank, MD Associate Professor Pulmonary and Critical Care UCSF Dept. of Medicine Director, MICU San Francisco VAMC Recognizing and preventing delirium
Charles Bernick, MD, MPH Cleveland Clinic Lou Ruvo Center for Brain Health June 2, 2018
 Charles Bernick, MD, MPH Cleveland Clinic Lou Ruvo Center for Brain Health June 2, 2018 Delirium common Prolongs hospitalization Worsens dementia ( if you survive) Increased risk of institutionalization
Charles Bernick, MD, MPH Cleveland Clinic Lou Ruvo Center for Brain Health June 2, 2018 Delirium common Prolongs hospitalization Worsens dementia ( if you survive) Increased risk of institutionalization
What is delirium? not know they are in hospital. think they can see animals who are about to attack them. think they have been kidnapped
 It is common for patients who are critically ill to experience delirium, usually called ICU delirium. This information sheet will explain what it is, what causes it, and what might help patients with delirium.
It is common for patients who are critically ill to experience delirium, usually called ICU delirium. This information sheet will explain what it is, what causes it, and what might help patients with delirium.
Doug Paul, D.O. FACOS Medical Director, Trauma Services Kettering Health Network
 Doug Paul, D.O. FACOS Medical Director, Trauma Services Kettering Health Network A paradigm shift (or revolutionary science) is, a change in the basic assumptions, or paradigms, within the ruling theory
Doug Paul, D.O. FACOS Medical Director, Trauma Services Kettering Health Network A paradigm shift (or revolutionary science) is, a change in the basic assumptions, or paradigms, within the ruling theory
KICU Spontaneous Awakening Trial (SAT) Questionnaire
 Questionnaire") KICU Spontaneous Awakening Trial (SAT) Questionnaire Please select your best answer(s): 1. What is your professional role? 1 Staff Nurse 2 Nurse Manager 3 Nurse Educator 4 Physician 5 Medical Director
KICU Spontaneous Awakening Trial (SAT) Questionnaire Please select your best answer(s): 1. What is your professional role? 1 Staff Nurse 2 Nurse Manager 3 Nurse Educator 4 Physician 5 Medical Director
Perioperative Care of Older Adults
 Perioperative Care of Older Adults SARAH A. WINGFIELD, MD AND THOMAS O. DALTON, MD UNIVERSITY OF TEXAS SOUTHWESTERN MEDICAL CENTER DIVISION OF GERIATRIC MEDICINE We have no disclosures. Objectives -Recognize
Perioperative Care of Older Adults SARAH A. WINGFIELD, MD AND THOMAS O. DALTON, MD UNIVERSITY OF TEXAS SOUTHWESTERN MEDICAL CENTER DIVISION OF GERIATRIC MEDICINE We have no disclosures. Objectives -Recognize
Perioperative Care of Older Adults
 Perioperative Care of Older Adults SARAH A. WINGFIELD, MD AND THOMAS O. DALTON, MD UNIVERSITY OF TEXAS SOUTHWESTERN MEDICAL CENTER DIVISION OF GERIATRIC MEDICINE We have no disclosures. Objectives -Recognize
Perioperative Care of Older Adults SARAH A. WINGFIELD, MD AND THOMAS O. DALTON, MD UNIVERSITY OF TEXAS SOUTHWESTERN MEDICAL CENTER DIVISION OF GERIATRIC MEDICINE We have no disclosures. Objectives -Recognize
Delirium in the intensive care unit: a narrative review of published assessment tools and the relationship between ICU delirium and clinical outcomes
 The Intensive Care Society 2008 Delirium in the intensive care unit: a narrative review of published assessment tools and the relationship between ICU delirium and clinical outcomes C Waters Delirium is
The Intensive Care Society 2008 Delirium in the intensive care unit: a narrative review of published assessment tools and the relationship between ICU delirium and clinical outcomes C Waters Delirium is
Care of Patient with Delirium
 Care of Patient with Delirium Introduction Delirium is an alteration in consciousness involving confusion and other changes in cognitive ability that has a brief duration. 1 Patients specifically at risk
Care of Patient with Delirium Introduction Delirium is an alteration in consciousness involving confusion and other changes in cognitive ability that has a brief duration. 1 Patients specifically at risk
Preventing Postoperative Cognitive Decline in the Elderly
 Preventing Postoperative Cognitive Decline in the Elderly Alex Bekker, M.D., Ph.D Professor and Chair Department of Anesthesiology Rutgers New Jersey Medical School "My brain, that's my second favorite
Preventing Postoperative Cognitive Decline in the Elderly Alex Bekker, M.D., Ph.D Professor and Chair Department of Anesthesiology Rutgers New Jersey Medical School "My brain, that's my second favorite
Confusion in the acute setting Dr Susan Shenkin
 Confusion in the acute setting Dr Susan Shenkin Susan.Shenkin@ed.ac.uk 4 th International Conference, Society for Acute Medicine, Edinburgh 7-8 October 2010 Summary Confusion is not a diagnosis Main differentials
Confusion in the acute setting Dr Susan Shenkin Susan.Shenkin@ed.ac.uk 4 th International Conference, Society for Acute Medicine, Edinburgh 7-8 October 2010 Summary Confusion is not a diagnosis Main differentials
Objectives. Delirium in the Elderly Patient. Disclosure. Arizona Geriatrics Society Fall Symposium 2010
 Delirium in the Elderly Patient Sandra Jacobson, MD Banner Sun Health Research Institute Arizona Geriatrics Society Fall Symposium 2010 Disclosure Dr. Jacobson has disclosed that she does not have any
Delirium in the Elderly Patient Sandra Jacobson, MD Banner Sun Health Research Institute Arizona Geriatrics Society Fall Symposium 2010 Disclosure Dr. Jacobson has disclosed that she does not have any
Renee Flores, MD Division of Geriatrics & Palliative Medicine Department of Internal Medicine
 Renee Flores, MD Division of Geriatrics & Palliative Medicine Department of Internal Medicine Define AMS and delirium Describe how to recognize and diagnose delirium Identify the predisposing or precipitating
Renee Flores, MD Division of Geriatrics & Palliative Medicine Department of Internal Medicine Define AMS and delirium Describe how to recognize and diagnose delirium Identify the predisposing or precipitating
Ohio/Minnesota Collaborative
 Ohio/Minnesota Collaborative Place picture here Delirium Prevention Virtual Learning Session February 24, 2016 Delirium collaboration Ohio and Minnesota HENs In December 2015, the Minnesota and Ohio HENS
Ohio/Minnesota Collaborative Place picture here Delirium Prevention Virtual Learning Session February 24, 2016 Delirium collaboration Ohio and Minnesota HENs In December 2015, the Minnesota and Ohio HENS
What are Appropriate End-points for Delirium Prevention/Treatment Studies
 What are Appropriate End-points for Delirium Prevention/Treatment Studies Pratik Pandharipande, MD, MSCI Professor of Anesthesiology and Surgery Department of Anesthesiology Vanderbilt University School
What are Appropriate End-points for Delirium Prevention/Treatment Studies Pratik Pandharipande, MD, MSCI Professor of Anesthesiology and Surgery Department of Anesthesiology Vanderbilt University School
Early Goal Directed Sedation In Critically Ill Patients
 Early Goal Directed Sedation In Critically Ill Patients Yahya Shehabi, FCICM, FANZCA, EMBA Professor, Intensive Care Medicine Clinical School of Medicine, University New South Wales School of Epidemiology
Early Goal Directed Sedation In Critically Ill Patients Yahya Shehabi, FCICM, FANZCA, EMBA Professor, Intensive Care Medicine Clinical School of Medicine, University New South Wales School of Epidemiology
Jennifer Mando-Vandrick, PharmD, BCPS Clinical Pharmacist, Emergency Department Director, PGY2 Critical Care Pharmacy Residency Duke University
 Jennifer Mando-Vandrick, PharmD, BCPS Clinical Pharmacist, Emergency Department Director, PGY2 Critical Care Pharmacy Residency Duke University Hospital Objectives Review pertinent pharmacotherapy common
Jennifer Mando-Vandrick, PharmD, BCPS Clinical Pharmacist, Emergency Department Director, PGY2 Critical Care Pharmacy Residency Duke University Hospital Objectives Review pertinent pharmacotherapy common
ICU Delirium: Recognition, Management and Long-Term Outcomes
 ICU Delirium: Recognition, Management and Long-Term Outcomes Sandy Staveski RN, PhD, CPNP-AC/PC, CNS Assistant Professor, Nurse Scientist Cincinnati Children s Hospital Medical Center Research in Patient
ICU Delirium: Recognition, Management and Long-Term Outcomes Sandy Staveski RN, PhD, CPNP-AC/PC, CNS Assistant Professor, Nurse Scientist Cincinnati Children s Hospital Medical Center Research in Patient
9/28/2016. Sedation Strategies in the ICU. Outline. ICU sedation. Recent clinical practice guidelines Top 10 myths A practical approach
 Sedation Strategies in the ICU UW Medicine EMS and Trauma Conference Seattle, Washington September 26 th, 2016 C. Terri Hough, MD MSc Associate Professor of Medicine Division of Pulmonary and Critical
Sedation Strategies in the ICU UW Medicine EMS and Trauma Conference Seattle, Washington September 26 th, 2016 C. Terri Hough, MD MSc Associate Professor of Medicine Division of Pulmonary and Critical