Standard Operating Procedure Outreach For Injecting Drug Users
|
|
|
- Melina Goodman
- 6 years ago
- Views:
Transcription
1
2
3 OUTREACH Standard Operating Procedure Outreach For Injecting Drug Users Currently 'Injecting Drug Users' (IDUs) are referred to as 'People Who Inject Drugs' (PWID). However, the term 'Injecting Drug Users' (IDUs), has been used in this document to maintain consistency with the term used presently in the National AIDS Control Program" Supported by The Global Fund to Fight AIDS, Tuberculosis and Malaria - Round-9 India HIV-IDU Grant No. IDA-910-G21-H with Emmanuel Hospital Association as Principal Recipient
4 STANDARD OPERATING PROCEDURE
5 OUTREACH Preface In India, Targeted Intervention (TI), under the National AIDS Control Program (NACP) framework, is one of the core strategies for HIV prevention amongst injecting drug users (IDUs). Apart from providing primary health services that include health education, abscess management, treatment referrals, etc., the TIs are also designated centres for providing harm reduction services such as Needle Syringe Exchange Program (NSEP) and Opioid Substitution Therapy (OST). The services under the TIs are executed through a peer based outreach as well as a static premise based approach, i.e., through Drop-In Centres (DIC) which in turn serves as the nodal hub for all the above activities to be executed. To further strengthen these established mechanisms under the NACP and to further expand the reach to vulnerable IDUs, United Nations Offi ce on Drugs and Crime (UNODC) in India provides technical assistance to the National AIDS Control Organisation (NACO) through the Global Fund Round 9 Project (i.e., Project Hifazat), amongst others. In doing so, UNODC supports NACO through technical assistance for undertaking the following: 1) Conduct Operational Research 2) Develop Quality Assurance SOPs 3) Develop Capacity Building/ Training Materials 4) Training of Master Trainers It is in this context that a series of seven Standard Operating Procedures (SOPs) including the present one on Outreach has been developed. This SOP also feeds into the broader NACP goals and helps strengthen and consolidate the gains of the TIs towards scaling up of critical services. This SOP on Outreach is the third in a series of seven SOPs developed. The main purpose of this SOP is to help address the operational challenges of program implementation with specifi c reference to outreach planning, outreach planning tools, steps in conducting outreach, services to be provided during outreach, formats for documentation and challenges during outreach. This SOP therefore, has also been developed with a vision to serve as an invaluable tool for the service providers engaged in IDU TIs in India and to enable them to deliver quality services. Contributions from the Technical Working Group of Project Hifazat which included representatives from NACO, Project Management Unit (PMU) of Project HIFAZAT, SHARAN, Indian Harm Reduction Network and Emmanuel Hospital Association was critical towards articulating and consolidating inputs that went into finalizing this SOP.
6 STANDARD OPERATING PROCEDURE
7 OUTREACH Acknowledgement The UN Offi ce on Drugs and Crime, Regional Offi ce for South Asia (UNODC ROSA) in partnership with national government counterparts from the drugs and HIV sectors and with leading non-governmental organizations in the countries of South Asia is implementing a project titled Prevention of transmission of HIV among drug users in SAARC countries (RAS/H13). As part of this regional initiative UNODC is also engaged in the implementation of the Global Fund Round-9 IDU-HIV Project (i.e. HIFAZAT). Project HIFAZAT aims to strengthen the capacities, reach and quality of harm reduction among IDUs in India. It involves providing support for scaling up of services for IDUs through the National AIDS Control Program. We would like to acknowledge the invaluable feedback and support received from various stakeholders including National AIDS Control Organisation (NACO), Project Management Unit (PMU) of Project HIFAZAT, Emmanuel Hospital Association (the principal recipient of the grant Global Fund to Fight AIDS, Tuberculosis and Malaria-India HIV-IDU Grant No. IDA-910-G21-H ), SHARAN, Indian Harm Reduction Network and individual experts who have contributed signifi cantly in the development of this document. Special thanks are due to the UNODC Project H13 team for their persistent and meticulous efforts in conceptualizing and consolidating this document.
8 Abbreviations AIDS Acquired Immunodefi ciency Syndrome IEC Information, Education and Communication ANM Auxiliary Nurse Midwife MSJE Ministry of Social Justice and ART Anti Retroviral Therapy Empowerment ARV Anti Retroviral M & E Monitoring and Evaluation BBV Blood-Borne Virus NACO National AIDS Control Organisation BCC Behaviour Change Communication NGO Non Governmental Organization BSS Behavioural Surveillance Survey NACP National AIDS Control Program CBO Community Based Organization NS Needles and Syringes CM Community Mobilizer NSEP Needle Syringe Exchange Program CRT Crisis Response Team OI Opportunistic Infection CSO Civil Society Organization ORW Outreach Worker CSS Community System Strengthening OST Opioid Substitution Therapy DDRC Drug Demand Reduction Centre PE Peer Educator DIC Drop-In Centre PEP Post-Exposure Prophylaxis DOTS Directly observed Treatment Short- PLHA People Living with HIV/AIDS Course PLHIV People Living with HIV FGD Focus Group Discussion PM Project Manager FIDU Female Injecting Drug User PPB Puncture Proof Box FSW Female Sex Worker PPTCT Prevention of Parent To Child Hep B Hepatitis B Transmission Hep C Hepatitis C PWID Person Who Injects Drugs HIV Human Immunodefi ciency Virus RCH Reproductive and Child Health HRG HR HSS IBBS High Risk Groups Harm Reduction HIV Sentinel Surveillance Integrated Biological and Behavioural Surveillance RNTCP SACS STD STI Revised National Tuberculosis Control Program State AIDS Control Society Sexually Transmitted Disease Sexually Transmitted Infection ICTC Integrated Counselling and Testing SW Sex Worker Centre TB Tuberculosis IDU Injecting Drug User TI Targeted Intervention STANDARD OPERATING PROCEDURE
9 OUTREACH Contents 1. Introduction Background and Purpose 1 2. Outreach General Considerations Why is Outreach Essential? Principles of Outreach Services through Outreach Staff for Conducting Outreach Roles and Responsibilities Steps in Outreach 9 3. Outreach Planning Social Mapping Spot Analysis Contact Mapping Work Plan Conducting Outreach Services Provided through Outreach Documentation Individual PE Tracking Other Formats - PE Records/Formats for ORWs Monitoring and Management Issues Monitoring Outreach Managing PEs Managing ORWs Challenges References 31
10 STANDARD OPERATING PROCEDURE
11 OUTREACH 1 1. Introduction 1.1 Background and Purpose There are an estimated 2 million to 3.1 million people living with HIV/AIDS in India and the adult HIV prevalence is approximately 0.36% 1. HIV in India is not a generalized epidemic, but it is concentrated among certain groups practicing high risk behaviours. Injecting Drug Users (IDUs) form such a group, which is vulnerable to the spread of HIV infection and other blood-borne viruses. The practice of injecting drug use and unsafe sex among IDUs is associated with an increase in HIV prevalence rates among IDUs. As per the recent sentinel surveillance exercise, HIV prevalence among IDUs is 9.2% at the national level. The goal of the third phase of National AIDS Control Program (NACP) is to halt and reverse the HIV epidemic in India by One of the important components of NACP is to provide prevention, treatment, care and support for those at highest risk of HIV through Targeted Interventions (TIs). NACO has responded by scaling up the targeted interventions for IDUs and presently more than 260 TIs are catering to 76 per cent of the estimated IDUs. The services currently provided for IDUs under the NACP can be divided into three tiers. Services and commodities provided by TIs Tier 1 Tier 2 Linkage by TI to other areas (services not provided by TI) Tier 3 Needle Syringe Exchange Outreach and counselling Condoms Basic STI Services Advocacy Opioid Substitution Therapy (OST) Linkages to: DOTS, ICTC, ART RCH services Detox and Rehab Centres Figure 1. Tiers of Harm Reduction 1 (NACO 2008)
12 Tier 1: Services Provided Directly by IDU TIs Needle Syringe Exchange Program (NSEP). Outreach, Information Education and Communication (IEC), Behaviour Change Communication (BCC). Free distribution and social marketing of condoms. HIV counselling for IDUs and their sex partners. Primary health care (sexually transmitted infection treatment, abscess management). Tier 2: Opioid Substitution Therapy (OST) Provided through: NGO TIs. Government hospitals, in collaboration with IDU TIs. Currently, involves provision of buprenorphine. Plan to initiate methadone as another option. Tier 3: Services through Referrals and Linkages Linkages with key health services: Directly Observed Treatment, Short-Course (DOTS), Opportunistic Infection (OI) management, Sexually Transmitted Infection (STI) clinics, Integrated Counselling and Testing Centres (ICTC), Antiretroviral Therapy (ART), Prevention of Parent to Child Transmission (PPTCT), People Living with HIV and AIDS (PLHA) networks for home based care and support, linkages with the MSJE supported centres and other private detoxifi cation and rehabilitation centres. Other linkages and referrals: psychiatric services within government settings and NGOs, agencies providing shelter, nutrition and vocational support Linking with programs for PLHIV as well as other drug user networks, including Narcotic Anonymous, etc. 2 STANDARD OPERATING PROCEDURE
13 OUTREACH 3 While the services listed in tiers 1 and 2 are provided directly through NGOs or through government healthcare settings in collaboration with the NGOs, those in tier 3 (referral and linkages) are provided by TIs through established referral linkages with the agencies that provide the linked services. An important strategy employed by the IDU TI is provision of services through outreach settings. Indeed, this is the backbone for service provision by the TIs. Purpose of the Standard Operating Procedure (SOP) This Standad Operating Procedure (SOP) is designed to support organizations providing outreach services under the harm reduction program by building the capacities of TI staff for improving the effectiveness and quality of outreach activities, contextual clarity in planning, conducting and monitoring of outreach activities in the IDU TI settings. It also provides information about essential requirements and detailed process for the development of outreach activity. The main purpose of this SOP is to: Assist the outreach team in effective planning and conduct of outreach. Ensure better management by Project Manager through effective monitoring and support. Set standards for uniform implementation/operation. Thus, the SOP is intended for all staff working in a TI setting for IDUs. However, specifi cally, the outreach workers under IDU/TIs should benefi t from the SOP.
14 2. Outreach General Considerations Outreach is a systematic approach to deliver harm reduction services to people who inject drugs and to their sex partners/spouses in their own environments. 2.1 Why is Outreach Essential? Traditionally, the approach to providing services is to set up centres and cater to the clients who visit these centres. However, people who have high risk behaviour and are termed as High-Risk Groups (HRGs) are reluctant to access such centres. This is because: Drug use is not a socially approved behaviour. The general community looks down upon people who use drugs. This is especially true for those who inject drugs. Drug use is illegal. This affects the ability of IDUs to come forward and seek services. IDUs tend to remain hidden and are not ready to reveal themselves. Preconceived notions regarding IDUs, that exist amongst some service providers, also act as barriers to IDUs accessing services from fi xed sites. The daily life of an IDU centres on fi nding money, buying drugs and injecting every day. As a result, he/she is not able to focus on other needs or seek help. As a result of the above, it becomes necessary for service providers to reach out to IDUs at places where they are most likely to be found. This method of service provision is referred to as outreach. Reaching out to IDUs and their sex partners through the PEs and ORWs, with the prime objective of preventing transmission of Blood-Borne Viruses (BBV) by reducing needle, syringe and equipment sharing, is an essential strategy of harm reduction. Outreach Enables Scaling-up provision of services and reaching out to IDUs who are hidden, stigmatized and discriminated against. Identifying new IDUs. Linking them to appropriate services, such as DOTS, STI, ICTC, ART, which will help them to access other health related services. Accessing services like primary healthcare. Reaching IDUs who do not want to access services from the DIC. Observing and understanding injecting behaviour, drug sharing culture, IDU networks and risk taking behaviours. Gathering information from the fi eld which can be used for effective planning, effective outreach, and meeting possible challenges. 4 STANDARD OPERATING PROCEDURE
15 OUTREACH Principles of Outreach Outreach for IDUs is based on several principles which are interlinked and dependent on each other. If one principle is not followed, the overall outreach objective can be compromised. Effective outreach, that helps in bringing services to the doorstep of IDUs, has to be based on these principles: Respect: service providers should respect and trust IDUs as individuals. Team work: delivering outreach is team work. Effi cient team work helps in ensuring greater delivery of services. Non-judgmental: service providers should not have preconceived negative notions about the benefi ciaries. Such judgemental attitudes act as impediments for successful service delivery including outreach. Empowerment: providers of outreach services should empower the IDU clients to take decisions for their own health and welfare. A client-generated demand helps in greater acceptability of services provided by the TI. Do no harm: the service provider should ensure that clients/benefi ciaries are not harmed in his/her attempt to provide services. 2.3 Services through Outreach An effective outreach strategy should ensure that at least 80% 2 of the estimated IDUs under the coverage area receive the following components as a package and not as stand-alone services. Services Provided through Outreach Education, advice and information either in individual or in group settings on: Risks of Human Immunodefi ciency Virus (HIV), Hepatitis B Virus (HBV), Hepatitis C Virus (HCV), STIs and means of reducing these risks. Safer injecting and safer sex practices, including prevention and management of overdose. Services for abscess management, STI diagnosis and treatment, HIV testing, ART and TB treatment which may be available at the DIC and/or other facilities. Regular distribution of the following, as per need of the IDUs and their regular sex partners: New needles and syringes. Abscess prevention materials alcohol swabs, cotton swabs, distilled water, etc. Condoms free as well as socially marketed. IEC materials, as and when required. Collection of used/old needles and syringes. Referral services to appropriate healthcare and other agencies. 2 WHO, UNODC, UNAIDS technical guide for countries to set targets for universal access to HIV prevention, treatment and care for injecting drug users.
16 2.4 Staff for Conducting Outreach Roles and Responsibilities Outreach is conducted as a team with planned services at predetermined sites/routes. Outreach team consists of: Outreach Workers Peer Educators Apart from this, the counsellor/anm conducts outreach on a need basis. Finally, the project manager also conducts fi eld visits in outreach area to monitor outreach work being delivered. Additionally, he/she is responsible for the overall management and supervision of outreach, including procurement and stock management. Outreach Workers Outreach workers should be current or ex-drug users. Apart from conducting outreach, ORWs support and supervise PEs in planning and conducting outreach, monitor the quality of services provided, ensure effective working systems, and consolidate collected data and information from the PEs. At some places, the ORW can also be a non-idu, but he/she should have an excellent understanding of the geographical terrain, including the local language and customs followed locally. Additionally, the ORW should have a good rapport with the IDU community and should understand the issues and challenges faced by IDUs. Key roles and responsibilities of the ORW in an outreach setting are to: Develop outreach plan in consultation with PEs and IDUs from the hotspots. Facilitate weekly work plan for his/her team of PEs. Develop a list of target areas with social mapping of each target area. Co-ordinate outreach activities and visit hotspots with PEs on a regular basis. Supervise outreach and monitor PE activities. Ensure regular and uninterrupted supply of harm reduction materials for each outreach visit. Provide referral and networking services with other agencies. Provide information on HIV/AIDS, hepatitis, STIs, safer injecting, safer sex practices, overdose management, early treatment and services available to IDUs. Establish systems of regular contact with secondary outlets. Identify stakeholders for advocacy for creating an 'enabling environment. Collect data and consolidate the same from the fi eld/pe. Criteria for a Good Outreach Worker Non-judgmental attitude and willingness to work for IDU community. Previous experience of working in IDU TI (desirable). Belief in one s ability to lead a team of peer educators and be led by senior TI staff. Strong facilitation skills. Communication skills. Knowledge of local language. Ability to document. Ability to lead small group discussions. 6 STANDARD OPERATING PROCEDURE
17 OUTREACH 7 Peer Educators A peer educator in an IDU-TI should be a current or ex-injector who works towards infl uencing attitudes to bring about behaviour change among IDUs. PEs are responsible for providing information on HIV/ STI, hepatitis, harm reduction including overdose prevention, condom promotion and engaging IDUs in group discussions, meetings and events. Each PE will target/cover between IDUs. Selection and retention of PEs is an important issue in an IDU TI. Key roles and responsibilities of the PE in an outreach setting are to: Conduct outreach and maintain contact with IDUs at least once in 15 days. Identify new IDUs and contact them. Provide dialogue-based inter-personal communication. Encourage service uptake (Needle and Syringe, condoms). Motivate IDUs to attend DIC regularly. Demonstrate safer injection and condom use. Invite and organize group discussions. Advocate with local level stakeholders. Provide referral and networking information. Take notes in fi eld diary/note book. File reports. Attend trainings. Attend weekly planning and review meetings. Train new PEs (within the project and outside). The Ideal PE for Various Audiences Target audience Female injecting drug users. Female injecting drug users who are also sex workers. Male IDU. Spouse of male IDU. IDU who are also MSM. Who will be the ideal PE Female current/ex-injecting drug user. FIDU sex worker can be current or ex-user. Male current/ex-injector. Spouse of current/ex-injectors. MSM IDU. Selection Criteria for PEs Qualities to look for in a PE are: Ability to give time for the project. Acceptability to the target community (IDUs) as a peer trust, known, language, age, behaviour and gender. Knowledge of the local context. Tolerance and respect for others. Good listening, communication and inter-personal skills. Self-confi dence and potential to be a leader. Good role model. Open to learning new things from the fi eld. Commitment gives time and support to the IDUs in crisis. Sensitive to the values of the community and maintains confi dentiality.
18 Auxiliary Nurse Midwife (ANM)/Counsellor In addition to DIC related activities, the ANM/ counsellor also has to visit the fi eld to conduct some of outreach based activities. The counsellor also assists the project manager to monitor outreach services being provided in the project area. Key roles and responsibilities of the ANM/ counsellor in an outreach setting are to: Conduct counselling (individual and group), for IDUs who are not able to visit the DIC. Motivate IDUs who are not willing to visit DIC. Motivate IDUs for HIV testing as well as other referral services. Make home-visits to access the partners of IDUs. Conduct Focus Group Discussions (FGDs) among the IDUs to understand the adequacy of services being provided by outreach team. Interact with the general community, obtain feedback and gain insight into their thoughts and opinions. Project Manager The Project Manager (PM) is the most senior of the TI staff and gives overall direction to outreach as well as other services being provided in the IDU TI. He/ she is responsible for ensuring that outreach activities are being conducted in accordance with the project framework. The PM must understand the challenges faced by outreach team in the fi eld, address them and also keep the morale of outreach staff high. Key roles and responsibilities of the PM in an outreach setting are to: Ensure that outreach team conducts outreach planning before conducting outreach. Ensure that outreach team meets each other on a weekly basis to update on the activities conducted in the previous week and plan for the coming week. Ensure that suffi cient commodities are available at the DIC/Non Governmental Organization (NGO) offi ce for conducting outreach activities. Set-up a routine monitoring mechanism for supervision of outreach work. Ensure that there is a backup plan for outreach staff taking leave/being absent from providing outreach services. Ensure that staff drop-outs are replaced urgently to avoid any lapse in outreach services. Monitor outreach activities, through routine fi eld visits, interactions with staff members, general community and benefi ciaries (IDU clients) and provide regular feedback. Build the morale of the staff to ensure that burnout among the staff is minimized. Build the capacity of outreach team through trainings/exposure visits on a regular basis. 8 STANDARD OPERATING PROCEDURE
19 OUTREACH Steps in Outreach Outreach can be divided into three steps: Planning Monitoring Conducting All the three steps are interrelated, with each one infl uencing the other. Though it would seem that conducting outreach is the main step, it should be remembered that planning and monitoring are important steps that need to be carried out regularly to take stock of the changing scenarios in the fi eld. Effective outreach depends on planning and monitoring.
20 3. Outreach Planning Outreach planning is a process to facilitate individual level planning and follow-up of service intake, based on high risk and vulnerability. Effective outreach planning will ensure: Maximum IDUs are covered in a given period of time. Optimal services are provided to every IDU client. The existing human resources of the TI project are optimally utilized. The team for outreach planning consists of the PEs, the ORWs and the PM. The PEs bring in the data/ information from the fi eld and the ORWs process this information by using various tools. PM should supervise and provide inputs when necessary to make the plan robust and practicable. Local high risk group mapping data (can be obtained from the SACS, if available) List of hotspots (these can be identifi ed through fi eld visits by the PEs and ORWs) Local Behavioural Surveillance Survey (BSS), HIV Sentinel Surveillance (HSS), Integrated Biological and Behavioural Surveillance Survey (IBBS) data (can be obtained from SACS, if under BSS/HSS/ IBBS sentinel surveillance site) Information from baseline assessments (if conducted) The team should gather as many of these resources as possible in order to make the planning easier and more effective. Outreach Planning Tools Outreach planning is made easier by the use of a Outreach planning team Project Coordinator/ Project Manager ORW I ORW 2 ORW 3 PE 1 PE 2 PE 3 PE 4 PE 1 PE 2 PE 3 PE 4 PE 1 PE 2 PE 3 PE 4 IDU IDU IDU Even before the team sits down for the actual planning, the following should be gathered and kept ready: The geographical maps of the area to be covered under the TI (these can be collected from the local administration panchayat, municipal corporation, etc.) number of aids, called planning tools. The tools used in the context of IDU TIs are: Social mapping. Spot analysis. Contact mapping. Work plans. Outreach activities. 10 STANDARD OPERATING PROCEDURE
21 OUTREACH 11 SOCIAL MAP - area marking IDU gathering places, stakeholders OUTREACH - fi eld work starts SPOT ANALYSIS - selected spots from social map are analyzed to understand the number of clients, types of drugs used, frequency of injection, etc. WORKPLAN - made after gaining all possible information and plan maximum contacts amongst the PE with time, NS etc. CONTACT MAPPING - plan made with PE to delegate the number of IDU to each PE 3.1 Social Mapping A social map is a rough diagram of the intervention area showing an overview of the sites where IDUs gather/come together. It is a visual illustration of the sites/areas where IDUs gather (hotspots) as well as service points such as hospitals, NGO, clinics, referral centres, etc. The social map should be updated as per the local situation. For example, if there is frequent movement of hotspots, the social map may be updated once every two to three months. At places, where the hotspots do not change frequently, the social maps may be updated once every six months. Who should draw the map? IDUs, PEs led by ORW How is the map to be drawn? Arrange chart paper, pencils, colour pens, scale, etc. Divide the participants, PE and IDUs into groups and ask them to draw the map showing all the places which are important for them. Give them 20 minutes to draw. An ORW would normally have one social map but if the area is too large, it may be subdivided and social maps can then be drawn separately for each sub-area. Mapping can be conducted either in the fi eld or at the DIC by PEs and ORWs. The IDU clients should be involved in the mapping; overall the process should be facilitated by a senior staff member, preferably the PM. What is important in a social map? The key principle of drawing a social map is to provide a visual overview of the area. This enables creation of an effective outreach plan for PEs. Direction coordinates, i.e., North South, West and East (NSEW), IDU gathering place, peddling areas, temples, cemeteries, NGOs, hospitals, churches, and other relevant services that IDUs can access or avail should be marked. An index or legend should



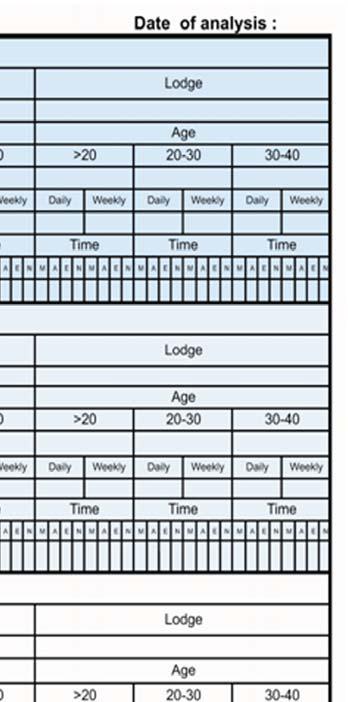
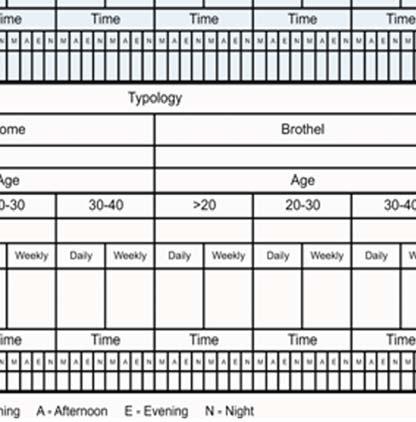
22 be provided In each social map. This index is the main indicator of the signs/drawing, that help in reading and understanding the map. Why is it important to analyze spots? In each social map, there are spots where IDUs congregate at certain times of the day. This spot becomes important to analyze. This is done through 'Spot Analysis' for effective outreach planning. Sample maps are given below: 3.2 Spot Analysis A hotspot is extracted from a social map by identifying common places where IDUs gather at certain times of the day. The objective is to fi nd the right time to meet maximum IDUs, and provide services and referrals to them. The information collected during needs assessment, related to each high risk spot/site in their respective project areas, is then compiled. Each spot is different from the other and a project site will usually have more than one site or hotspot. Spot analysis should give the break-up of IDUs in a particular spot according to their: Time of availability IDUs may frequent the particular hotspot to buy drugs, inject, or rest after injecting. The time at which they are available should be recorded, and may be divided into morning, afternoon, evening and night. Age of the IDU. Sample 1 After drawing the social map, one hotspot (for e.g., North AOC (Imphal) in the above sample) is selected from the social map. A detailed analysis of the hotspot is then conducted. In the next map (sample 2) the yellow circled site/spot will be analysed for best outreach services. Sample 2 Type of drugs injected. Volume of injecting This is a rough calculation of the number and frequency of injecting episodes. Classically, it is divided into high volume (more than three episodes per day), Medium volume (one to three episodes per day) and low volume (less than one injecting episode per day). Another simple way of calculating the injecting episodes is to divide the IDUs into two categories daily injectors (at least one injecting episode per day) and non-daily injectors (less than one injecting episode per day). This manner of division is easier and helps the program to prioritize individuals who have to be provided NSEP services on a daily basis. 12 STANDARD OPERATING PROCEDURE
23 OUTREACH 13 The spot analysis format is provided as Annexure 1. Who: ORWs and PEs along with IDU clients, facilitated by senior staff. How: through a group discussion with IDUs engaged in needs assessment, facilitated by senior staff. Explain the link between the social map and spot analysis. Follow the steps or questions: What is learned during the situation and needs assessment process? What information is required about IDUs operating in a spot? (E.g. volume of clients, typology of drugs, age groups, frequency of injection per day/week.) When to go? This will help in establishing the time of operation and frequency of operation required per week, etc. Divide the participants as per taluka or ward number to complete the analysis exercise. After completion of the exercise, each group presents and discusses the process that they adopted to do this analysis. What is the analysis for the spot and what is the plan? Spot analysis should be done every time there is a change in the spot. If there are no changes, then once every six months is suggested. After spot analysis the potential client (PWID) names and code numbers are written down in another format contact mapping. In the above diagram numbers circled are estimated total IDU population and numbers in different colors represent each PE and ORW. For example out of 50 estimated IDU, only = 27 IDU are known and rest 33 are not known. The outreach team will plan how to increase contact to all 50 IDU in one small spot. 3.3 Contact Mapping Contact mapping helps participants to map their contacts with IDUs in each spot and helps in analysing their needs. After the spot analysis is completed, the names of the potential IDU clients are written down in the contact mapping format. Who: PEs facilitated by ORWs How: the group (of PEs and ORWs) should be divided as per taluka, ward or site and the following steps undertaken: Each group draws a map of the town or site with estimated number of IDUs in each spot. Use a colour code assign a different colour to each ORW and PE in marking the number of IDUs each PE and ORW knows. Using colour coding will simplify the process of identifying which (PE) is most suitable for each spot. Also answer the following questions where is the contact limited; what is the reason for the limited contacts; what can be done in each specifi c area/spot to increase the contacts. Example : Spot Analysis
 and overlapping can be avoided through this exercise.")



24 Analyze who reaches whom and who are left out. One contact may be known to more than one ORW/ PE (common contacts by ORW/PE) and overlapping can be avoided through this exercise. Example: Contact Mapping risk and vulnerability profi les of each IDU (Annexure 2). Field level environment and setting can change very quickly, hence some sites may need planning to be done weekly, but mostly sites would need monthly planning and revisiting of work plans. Geographic networks and social networks of peers enable better outreach planning. Similarly risk and vulnerability exercise is also covered by spot analysis. 3.4 Work Plan This is the output of the entire outreach planning process. It provides a work plan to regularly reach out to individual IDUs with requisite services based on Who: PEs and ORWs can make the work plan to cover and address the needs of IDUs. How: using the spot analysis, social mapping, contact mapping and gap analysis, the team can develop weekly target plans for outreach to cover each area. The weekly plan for each PE can be different as per the variation in needs, spots, risks and vulnerabilities. Planning a meeting 14 STANDARD OPERATING PROCEDURE
25 OUTREACH Conducting Outreach Following are the steps in conducting outreach: Step 1: Building rapport with the IDU and general community This is a critical prerequisite to conduct street/ community outreach. Good rapport will enable the outreach team to deliver services effectively without interference. Step 2: Delivering services in the field; referrals to DIC and other services The outreach plan discussed in the earlier section should be completed before systematically delivering services in the fi eld. This helps in ensuring that all the IDUs are optimally covered with services in a timely manner. Step 3: Creating an enabling environment An enabling environment is required for effective delivery of and access to services. IDUs being stigmatized and discriminated against are more hidden and fear accessing services. The outreach team should understand the barriers in service delivery by talking to IDUs and PEs so that an appropriate advocacy campaign can be conducted. Step 4: Documentation and analyses Services provided should be documented and collected and data should be analyzed for re-planning or re-strategizing outreach. Re-planning is done after understanding the gaps in consultation with PEs and IDUs. Documentation should focus on coverage of target and regularity of accessing services. Senior staff or PM should be consulted when certain gaps or issues cannot be addressed. Where should outreach be done? Outreach should be done at identifi ed hotspots or locations where IDUs inject drugs or gather: Places where IDUs and sex partners congregate (buying drugs, shooting galleries, if any, or common places where they gather regularly). Space near locations where other medical and social support services are located. Mobile outreach units e.g. mobile vans. What should be the outreach hour? Outreach should happen at a time when IDUs gather (e.g., to buy drugs). This can be in the evening or early morning. Appropriate measures should be taken to ensure safety of staff (PE and ORW) engaged in outreach. Who leads outreach? The PE should lead the outreach each PE should interact with individual IDUs on a one-to-one basis and distribute needles, syringes, condoms, etc. Outreach workers should supervise and provide support as and when required. How many clients can be served in a single day? The number of contacts in a single day depends on the target and plan considering site, average gathering of IDUs, risk, vulnerability, and frequency of injection. Spot analysis and contact mapping help in making plans for single day. A single PE has IDUs as part of the outreach target. However, in some cases, all the IDUs may not be met by a PE in a single day. In such cases, the PE should plan in such a way that he/she is able to meet all the targets every alternate day. Alternatively, the ORW should cover for the PE, wherever the PE fails to meet the target allotted to him/her. What needs to be carried during outreach? Identity card for security reasons. Some NGOs also carry a copy of the district SP s letter acknowledging the NGO s work and fi eld area.
26 IEC materials. Needles 26 and 24 gauge. Alcohol swabs, distilled water. Syringes 1 ml, 2 ml and 5 ml. Disposable gloves for collecting used needles and syringes. Puncture proof container to receive used/ returned needles and syringes. Tongs for picking up used needles and syringes. Condoms for distribution and a penis model for condom demonstration. Scissors, betadine ointment and lotions, bandage, spirit, plaster. 4.1 Services Provided through Outreach a. Needle Syringe Program NSEP 1 facilitates safe injecting practices by providing clean injecting equipment and ensuring safe disposal options for used equipment. Clean needles and syringes are the tools to prevent HIV and other blood-borne diseases. Hence, providing needles and syringes whenever needed is essential to make each injection safe from diseases. Needles and syringes should be provided according to the need of the individual IDU. This is to be calculated based on the information available from the need assessment conducted with individual IDUs in the fi eld. The distribution of needles, syringes and medi-swabs should be supplemented with information on safer injecting practices. On-site demonstration of safer injecting skills should be performed by the PEs. Collection and removal of used needles and syringes from circulation is important to reduce re-use. PEs should encourage returning of used needles and syringes. They should follow proper guidelines for collection and safe disposal of used needles and syringes. The procedure to be followed for collection of needles and syringes is laid out in the ÂGuidelines on Safe Disposal of Used Needles and Syringes in the Context of Targeted Intervention for Injecting Drug Users - NACO, 2009Ê. Adherence to these guidelines is essential. b. Behaviour Change Communication (BCC) What: BCC is an interactive process with communities to develop tailored messages and approaches using a variety of communication channels to develop positive behaviours. Why: behaviour change is one of the essential elements to reduce harm in each client. Normally people resist changing in spite of knowing facts and information. Therefore, a well-planned strategy to regularly engage IDUs with different communication methods allows change to happen and be sustained. Target group IDU Spouses, regular sex partners of IDUs Objective of BCC Motivate/sustain safer injecting practices and safer sex. Assist in acquiring knowledge on self-care, life skills to enable safer behaviour with their partners and also seek reproductive health care as and when needed. 1 The details can be found in the SOP on NSEP developed by UNODC as part of the GFATM Round 9 program. 16 STANDARD OPERATING PROCEDURE



27 OUTREACH 17 How: One-to-one: using tools like fl ip books/ charts, IEC materials. It is done to motivate safer injecting practices and safer sex. Details on how to inject safely are provided in the SOP on abscess prevention and management. Group education: a group of more than two and less than eight is appropriate. Group education is done to share knowledge, information and skills. Counselling: can be done in the fi eld but is more effective at the DIC. IEC: includes brochures, posters, street plays, fl ip charts. IEC should be developed by assessing the behavioural risk. Behaviour change communication should focus on: Drug related harm. Ways to reduce harm. Safer injecting practices such as NSEP, prevention and management of overdose, etc. Safer sex, negotiation skills. Accessing available health services. Ways to prevent and manage abscess. Capacity building of IDUs on correct condom use, safer injecting practices. Advocacy among key stakeholder for creating a supportive environment. Additional topics for group discussion should be planned in discussion with the IDUs and sessions should be planned accordingly. For example, a site may have frequent drug overdose. In such a case, education should be provided about how drug overdose happens, how to avoid overdose, and how to manage overdose. Information should be provided on naloxone, an emergency lifesaving medicine for opioid drug overdose. Focus group discussion at the hotspot
28 A focus group discussion with current IDUs to understand the causes and issues related to drug overdose was done at one of the hotspots in Imphal, Manipur. The team developed a set of probing/leading questions and one of them facilitated the whole discussion. The criterion for attending was overdose in the last one month. The focus group discussion lasted for about an hour, and the facilitator was able to impart education to the IDUs on reasons for occurrence of overdose, apart from understanding the factors associated with overdose. Similar FGDs can be done to understand more about other issues, challenges which may hamper intervention programs, e.g., why IDUs are not keen to get HIV tested, how IDUs share injecting equipment, use of condoms, fear of HIV/ART, etc. c. Condom Promotion What: to promote safer sex by encouraging proper condom use, providing skills to use condoms and information on the purpose of condoms. Also ensure regular supply of condoms as per requirement. Why: to ensure consistent use of condoms among IDUs and their sex partners. The TI should focus on regular sex partners as it is important to prevent both receiving and onward transmission of STIs, HIV and other blood-borne diseases through the sexual route. Ensuring availability, accessibility and, correct and consistent use of condoms by the HRGs is the key to HIV prevention. How: strategies to be followed are - Primary strategy: free supply of condoms to male as well as female IDUs, some of whom may also be sex workers and spouses/ partners of male IDUs. Secondary strategy: social marketing done through TIs or Community Based Organizations (CBOs) in collaboration with social marketing agencies. Distribution channels Direct: condoms given directly during fi eld visits or at DIC. Indirect: distribution done though condom outlets like public toilets, paan shops, lodges, etc. d. Referrals All services required for IDUs and their sex partners cannot be provided through outreach. Thus, referral for suitable services will be needed to suit the requirements of the IDUs and their sex partners. The IDUs and their sex partners may not always be comfortable accessing these services through referral. Accompanied referral, with ORWs/PEs accompanying the IDUs or sex partner to various services at least in the initial stages, should be provided. e. Creating an Enabling Environment What: harm reduction services require a supportive environment from community, families, society and law enforcement agencies including pressure groups (in certain places). Why: IDUs often face stigma and harassment because of a number of reasons making access to services a challenging task for IDUs. The PE and ORW, in consultation with other staff, need to create a good environment for accessing services. Effectiveness of the program is enhanced by having a supportive environment. How: at the onset of the intervention, meetings should be organized with law enforcement personnel and community leaders on the issues of IDUs. Advocacy with law enforcement agencies gaining support for harm reduction 18 STANDARD OPERATING PROCEDURE
29 OUTREACH 19 services is essential to avoid harassment of IDU clients or the fi eld staff by the police while providing/receiving services. Senior police officers Visit senior police offi cers and give them updates on the project including reports, pictures, and issues on a regular basis. Get support for the TI project Generate support by sharing challenges with the local police team, get no objection certifi cate from district police offi cer for smooth functioning of the TI, explain the goals and how this will help in preventing further spread of HIV among the general population by giving IDUs an opportunity to change by providing the right information. Give offi cials the contact numbers of TI staff, to be shared with any IDU to be referred to the project. Educate police officers on drug use issues and risks After gaining trust, explain the risk involved to the police while frisking the IDU clients. Explain the risk that the police may face due to accidental needle stick injury resulting in infection with Blood Borne Viruses (BBV). Additionally the police should be educated on Post-Exposure Prophylaxis that are available in the near by health centres. Focus should be on changing the attitude of the police by reinforcing the message that drug dependence/addiction is a health problem and a number of harms can be prevented by providing appropriate services. Use supportive police to do more advocacy After conducting training for police identify champions who have shown understanding on harm reduction. They can be tapped for further training to gain more support amongst police personnel. Periodic visits to the police station In consultation with the district offi cer, arrange regular visits, preferably monthly, by the NGO team to update on program achievements and issues Case Study Advocacy Meetings Some of the TI partners conducted an advocacy meeting by inviting a high-ranking police offi cer to attend a meeting focused on issues related to drug policy and the work being done by NGOs in preventing HIV among IDUs. The meeting was organized by a group of NGOs working in an IDU TI. Many lower level police offi cers also accompanied the senior offi cer to the meeting. A month after conducting the meeting, two staff members of the IDU TI were detained in the police station as they had been helping an IDU who had developed OD and subsequently died. However, when the TI NGO project director visited the police station, the station house offi cer immediately recognized him and the work being done by the organization. He offered the TI staff members tea and the detained staff was released. This relationship helped in maintaining a cordial working environment between the police and the IDU TI NGO.

30 faced by the fi eld staff in service provision. Avoid disclosing identity of the clients which may break the trust between the NGO team and the IDU. If the IDU suspects that the NGO is helping police in their activities, he/ she may stop taking services from the NGO. Ask all of them to help, assist and participate in wider consultations. Build community (IDU) ownership of the TI by: Collectivization: making a collective, united effort by IDUs. Creation of space for community events. Community awareness meeting in progress Drugs, HIV events, meetings with police and community NGOs should invite police offi cers to attend general meetings and invite them as special invitees when observing important days/events (e.g. World AIDS Day). This encourages partnership efforts and supportive attitudes amongst police, NGO and fi nally the IDU. Working with the IDU community Involving the community, IDUs, spouses, FIDUs, in designing services makes the harm reduction services more acceptable to the IDU clients and increases the uptake of these services. Identify supporters and opponents, and work accordingly. Identify the key decision makers and opinion leaders. Building capacity of IDUs and their sex partners to assume ownership of the program. Raising public awareness amongst general population Advocacy with general population is also needed on harm reduction, how stigma leads to more challenges in the whole public health works, etc.general population needs: Awareness on drug use facts and issues to decrease stigma. Information on harm reduction as it is new and many will not know the benefi ts. Clarify that HR does not promote drugs and sex it helps to reduce risks. There is always misconception or misunderstanding that HR encourages antisocial and illegal practices. 20 STANDARD OPERATING PROCEDURE
31 OUTREACH Documentation Documentation of regular outreach activities is important for keeping track of the changing scenario at the fi eld level. Thus, improved planning, monitoring of the activities and performance of the PEs and the ORWs is required. 5.1 Individual PE Tracking What: information of day-to-day outreach and other services provided is recorded in the PE log book or diary. On returning from the fi eld, the PE can transfer the record/data on to the individual PE tracking sheet (see Annexure 2).The main services recorded are: One page for each PE. Name and code of IDUs met during the month. Their risk and vulnerability assessment. Number of needles and syringes distributed. Number of condoms distributed. Number of IDUs who attended clinic, were referred to ICTC/ART/Revised National TB Control Program (RNTCP), etc. Report of experience of violence or harassment especially by pressure groups and police. Number of BCC contacts. Number of referrals made during the month. Who: PE and ORW transfer daily notes/data within two days time for maintaining quality of the data. This helps in weekly review meetings to update the target achievement, re-prioritize IDUs who need to be reached in the following week, etc. 5.2 Other Formats PE Outreach planning tools: contact mapping, spot analysis, social mapping. These tools are essential for making weekly plans and ORW and other staff can monitor the effectiveness of a PE by using these tools. Field observation/daily notes: should be maintained daily. Weekly planning and activity sheet (Annexure 2): this is maintained weekly and submitted to the ORW. PE activity can be checked weekly and sometimes the ORW can make fi eld visits. 5.3 Records/Formats for ORWs IDU/HRG registration contains information of the IDU, profi le e.g., name, age sex, address, etc. Monthly summary sheet (Annexure 3). Weekly meeting register (planning) to be maintained by ORW. Field diary of ORW. ORW weekly report (Annexure 4). How: Use formats (Annexure 2) to update individual tracking grids weekly.
32 6. Monitoring and Management Issues 6.1 Monitoring Outreach What: the following activities should be monitored weekly: Coverage of IDUs and their sex partners as per target and coverage plan. Reaching out to the identifi ed IDUs with services as per plan. Needle and syringe supply as per calculated demands. Other provisions for safer injecting (cotton swabs, distilled water, as planned by the TI). Condom supply as per calculated demand. Referral to DIC. Follow-up on referrals. BCC at the fi eld level. Monitoring should also be done fortnightly to see whether: New clients entering into the hotspots are being identifi ed and registered. Old, registered clients leaving (not coming to the hotspots), moving from one hotspot to another are being recorded. New and emerging hotspots and changes in terms of geographical location, number of IDUs, etc. in the present ones are being documented and plans are being made to respond to the changing scenario/s. Profi le of IDUs is being updated to document the changing behaviour pattern e.g. the drugs being injected, the injecting and sexual practices, etc. Liaison with the stakeholders is being done regularly. Level of acceptability in the community is increasing or decreasing. Who: monitoring is conducted at two levels: Field level by the ORW with the PEs. TI level by the PM with ORWs and PEs. How: at the fi eld level, the ORW should regularly observe the PEs and their interactions with the IDUs and local people. He/she should also make it a point to personally meet at least a few IDUs at each hotspot and discuss whether: They are being contacted regularly at a time suitable to them. They are receiving needles, syringes and other provisions for safer injecting as well as condoms as per their requirements. The conduct of the PEs is appropriate. Other services are required. He/she should also discuss issues related to IDU's drug use, injecting and sexual practices, new IDUs, emerging hotspots, etc. The ORW should conduct weekly meetings for each hotspot with the relevant PEs and discuss the following: Coverage Contacts made Needle and syringe supply Other provisions 22 STANDARD OPERATING PROCEDURE
33 OUTREACH 23 Condom supply Referral to DIC BCC at the fi eld level Follow-up Record/documentation review: the ORW should also check the relevant sections of the PE diary, tracking sheet to check for contacts with clients- (both 1-1 & 1-group), number of needles, syringes and condoms distributed, referrals and follow ups and check if they are matching. At the TI level the PM should monitor the outreach at least on a fortnightly basis. The PM should visit the hotspots two to three times a week. He/she should make a plan for regular visits to all the hotspots. There should also be some surprise visits conducted. During the visits the PM should be meeting: Some IDUs. Some stakeholders (locals - tea, paan sellers, pharmaceutical shop owners - staff, community leaders/key infl uencers, police, etc.). The PEs and ORWs working in the hotspot. The PM should also review the following records/ documents at least every fortnight: Outreach plan, including spot analysis. Needle and syringe stock register (this will provide the situation of the stock and also the number of needles and syringes received by individual PEs and ORWs). DIC registration records (number of clients who have been referred from the outreach). DIC service utilisation registers (abscess management, counselling, STI treatment, referral etc.). PE weekly planning and activity sheet (Annexure 2) and PE-wise individual HRG compiled sheet for IDU intervention (by ORW) (Form C). Monthly CMIS report. The PM should also conduct review meetings at the DIC with the ORWs at least once in a month. During the review meeting the PM should base the discussion on his/her fi ndings from: Field visits. Record/documentation review. 6.2 Managing PEs Outreach workers should directly supervise the PEs. The supervision should be supportive in nature, keeping in mind PE's strengths and weaknesses. Review performance of PE every six month. This is done by reviewing the records maintained by the PE, observation of the work done by the PE in the fi eld and the fi eld level monitoring conducted by ORW. Each PE should be given a 12-month agreement and the agreement should be renewed based on performance. Weekly meetings with PEs help bring focus to challenges faced by the PEs in the fi eld. ORWs and the PM should ensure discussion regarding these challenges and plan to address them. Rotation of PEs after completion of the contact list is also preferred to get new users or new contacts. Current IDUs working as PEs may not be able to perform effectively if his/her daily drug use is becoming unmanageable. Providing counselling with proper focus on work as a reminder is always helpful.
34 Provide support and encouragement to PEs to get on OST as OST makes the PE s life more stable and he/she and improves ability to work more effectively. 6.3 Managing ORWs ORWs are supervised by the project manager who should: Review performance of ORW with the output, contacts and monitoring of outreach. This requires review of the performance of the PE also, as the main role of ORW is to manage PEs. Attend the weekly meetings to understand the work activities, processes and plans. This enables immediate attention to be focussed on addressing the gaps and misunderstandings between staff and also external challenges. Ensure opportunity is given to ORWs to attend relevant trainings (internal or external). Follow NGO rules when dealing with ORWs who are ex-users and have relapsed. At the same time support should be provided to the ORW. 24 STANDARD OPERATING PROCEDURE
35 OUTREACH Challenges What Inability to carry needles and syringes by IDU Pregnancy and heroin use Addressing burnout Suggestion or Option This may happen in certain areas. PEs and ORWs should always carry their ID cards. The crisis response team should make advocacy efforts to reduce police harassment and allow IDUs to bring back used needles and syringes for proper disposal. A pregnant woman who uses heroin puts her foetus at risk of being aborted. There may be complications for the mother as well. Hence, it is advisable to refer pregnant FIDUs to OST for the safety of the foetus and the mother. Burnout may be related to psychosocial states; chronic emotional strains; lack of experience; role confl ict and confusion; workload; misunderstanding between staff or with IDUs; organizational demands It can be prevented through use of clear job descriptions, realistic expectations of ORWs/PEs and supportive supervision. Relapse Relapse can be caused by stress and exposure to high risk situations. PEs and ORWs are vulnerable to relapse due to their psychological states; proximity to drug use; physical pain; inability to manage large amounts of cash; etc. It can be prevented through organizational rules, individual preparation for outreach work, by appropriate supervision and assistance from other outreach workers. As a basic rule PEs and ORWs should never go to the fi eld alone. Pairing them up greatly reduces chances of relapse due to exposure to drugs. Regular counselling and sharing in group meetings can further reduce chances of relapse. Clear guidelines regarding relapse of PEs and ORWs should be developed at the organizational level with emphasis on seeking treatment in case of relapse and providing opportunities to re-join service upon treatment completion. This helps the PEs and ORWs have greater confi dence in the system and continue work with reduced apprehensions regarding relapse. Police arrest of PEs and/or ORWs Senior staff of the TI project should provide necessary help to the PE/ ORW in case they are apprehended by the police while on duty or for reasons of distribution of needles and syringes. Regular advocacy with law enforcement is necessary if such arrests occur frequently.
36 What Police arrest of IDU Suggestion or Option If the IDU is on ART/OST the individual will suffer without medication. Crisis response team (CRT) in the TI should be made aware of such a crisis and should be empowered to deal with the issue of access to health/services. If the arrest is related to some crime committed, CRT may not be able to help much but should ensure that the IDU receives his/her medications as required. Advocacy meetings should be held with the law enforcement agencies to ensure that the treatment is not affected and the health of the IDU is not compromised. Home based IDU Initial contacts can be made through a link person, but the PE should clearly state his/her identity, name of the NGO and the services offered. Contact details including phone numbers should be shared to enable the IDU to contact outreach staff as and when needed. Such IDUs should specially be assured of confi dentiality and all efforts should be made to ensure that it the confi dentiality is not breached. Some IDUs can be sick at home and may not be in a position to move out to seek services. They may need to be linked to the ANMs/doctors and requisite services to help tide over the crisis period 26 STANDARD OPERATING PROCEDURE



37 OUTREACH 27 Annexure 1: Spot Analysis
38 Annexure2: PE Weekly Activity Plan Sl. No PE Weekly Planning & Activity Sheet (IDUs) Name of the PE District Name of the hot spot/s Name of the For the month supervising ORW Name of the HRB Groups UID Number STI Referral due/over due Risk Assessment Total Total distributed through 1-5 Week Services PE's Symbol for Identifying HRB Groups High number of drug using partners > 3 per month Sharing of needles/syringes (Yes/No) Injecting > 3 times a day STI reported in last three months Use of Alcohol & other drugs apart from injections Unsafe sex (sex with non regular partner) Mobility from one hotspot to another Condom requirement per week Needles/syringes requirement per week # of syringes distributed # of syringes returned STI referrel visited Abscess treatment Condom use during last sex Needle/syringe not shared during last injecting episode Risk Vulnerability # of contacts # of condom distribution Group ICTC Date: (end of the wek) # of referrals (STI & others centers) Report access by HRB Groups ICTC ART 28 STANDARD OPERATING PROCEDURE

39 OUTREACH 29 Annexure 3: Monthly Summary Sheet

40 Annexure 4: ORW Weekly Report 30 STANDARD OPERATING PROCEDURE
41 OUTREACH References 1. National AIDS Control Organisation, Ministry of Health & Family Welfare, Government of India Targeted Interventions Under NACP III. Volume I. Core High Risk Groups. Policies&Guidelines/NACP-III.pdf 2. National AIDS Control Organisation, Guidelines on Safe Disposal of Used Needles Syringes in Context of Targeted Intervention for Injecting Drug Users. nacoonline.org/upload/ngotargeted/ wastedisposalguidelineforiduti.pdf 4. United Nations Offi ce on Drugs and Crime, Staying safe A manual to train Outreach workers in IDU TI interventions (Draft stage). 5. United Nations Offi ce on Drugs and Crime, 2012, Staying Safe. A Manual to Train Peer Educators in IDU TIs (Draft stage). 6. United Nations Offi ce on Drugs and Crime, 2011, Counselling in Targeted Interventions For Injecting Drug Users. documents/southasia//trainingmanuals/a_ counsellors_handbook.pdf 3. National AIDS Control Organisation. A Manual on Working with Injecting Drug Users. A Training manual. nacoonline.org/upload/ngo & Targeted/ Capacity Building/Training Module/Training Package for working with IDU/A manual Working with Injecting Drug Users a Trainers Manual.pdf
42 Notes STANDARD OPERATING PROCEDURE
43

44
Harm Reduction in Nigeria
 Harm Reduction in Nigeria Needs, gaps, and responses to ensure access to effective HIV prevention, treatment and care for people who inject drugs February 2018 This document is made possible by the generous
Harm Reduction in Nigeria Needs, gaps, and responses to ensure access to effective HIV prevention, treatment and care for people who inject drugs February 2018 This document is made possible by the generous
TARGET INTERVENTION (SIMS Reporting Indicator Definitions)
") TARGET INTERVENTION (SIMS Reporting Indicator Definitions) One of the most critical programme elements of NACP III is the provision of targeted prevention interventions for high risk groups and male bridge
TARGET INTERVENTION (SIMS Reporting Indicator Definitions) One of the most critical programme elements of NACP III is the provision of targeted prevention interventions for high risk groups and male bridge
HIV Prevention, Care and Treatment Services in Prisons of North-Eastern States of India
 HIV Prevention, Care and Treatment Services in Prisons of North-Eastern States of India About the Project The prevalence of HIV, and other blood borne viruses in prison populations is many times higher
HIV Prevention, Care and Treatment Services in Prisons of North-Eastern States of India About the Project The prevalence of HIV, and other blood borne viruses in prison populations is many times higher
About Project Sunrise
 1 2 About Project Sunrise FHI 360 has been awarded a five year project titled Sunrise by the Centers for Disease Control and Prevention (CDC). The project aims to complement the ongoing National AIDS Control
1 2 About Project Sunrise FHI 360 has been awarded a five year project titled Sunrise by the Centers for Disease Control and Prevention (CDC). The project aims to complement the ongoing National AIDS Control
Annex A: Impact, Outcome and Coverage Indicators (including Glossary of Terms)
") IMPACT INDICATORS (INDICATORS PER GOAL) HIV/AIDS TUBERCULOSIS MALARIA Reduced HIV prevalence among sexually active population Reduced HIV prevalence in specific groups (sex workers, clients of sex workers,
IMPACT INDICATORS (INDICATORS PER GOAL) HIV/AIDS TUBERCULOSIS MALARIA Reduced HIV prevalence among sexually active population Reduced HIV prevalence in specific groups (sex workers, clients of sex workers,
World Health Organization. A Sustainable Health Sector
 World Health Organization A Sustainable Health Sector Response to HIV Global Health Sector Strategy for HIV/AIDS 2011-2015 (DRAFT OUTLINE FOR CONSULTATION) Version 2.1 15 July 2010 15 July 2010 1 GLOBAL
World Health Organization A Sustainable Health Sector Response to HIV Global Health Sector Strategy for HIV/AIDS 2011-2015 (DRAFT OUTLINE FOR CONSULTATION) Version 2.1 15 July 2010 15 July 2010 1 GLOBAL
The Comprehensive Package: The simple truth about our response to drug related HIV. Dr. Monica Beg, Signe Rotberga UNODC
 The Comprehensive Package: The simple truth about our response to drug related HIV Dr. Monica Beg, Signe Rotberga UNODC HIV among injecting drug users Why is it so important? 30% global HIV infections
The Comprehensive Package: The simple truth about our response to drug related HIV Dr. Monica Beg, Signe Rotberga UNODC HIV among injecting drug users Why is it so important? 30% global HIV infections
Guidelines For Services Providing Injecting Equipment
 Guidelines For Services Providing Injecting Equipment Best Practice Recommendations For Commissioners and Injecting Equipment Provision (IEP) Services in Scotland (Scottish Government 2010) January 2014
Guidelines For Services Providing Injecting Equipment Best Practice Recommendations For Commissioners and Injecting Equipment Provision (IEP) Services in Scotland (Scottish Government 2010) January 2014
TB/HIV Care s Experience Setting up PrEP Sites and Engaging Potential Service Users. John Mutsambi and Peggy Modikoe TB/HIV Care
 TB/HIV Care s Experience Setting up PrEP Sites and Engaging Potential Service Users John Mutsambi and Peggy Modikoe TB/HIV Care Session Objectives Objectives Define the scope of activities to prepare for
TB/HIV Care s Experience Setting up PrEP Sites and Engaging Potential Service Users John Mutsambi and Peggy Modikoe TB/HIV Care Session Objectives Objectives Define the scope of activities to prepare for
MINISTRY OF HEALTH STRATEGIC FRAMEWORK OF COMMUNICATION FOR HIV/AIDS AND STIs INTRODUCTION
 MINISTRY OF HEALTH STRATEGIC FRAMEWORK OF COMMUNICATION FOR HIV/AIDS AND STIs INTRODUCTION Communication for HIV/AIDS (SFC HIV/AIDS AND STI) represents an important strategy of the National Programme on
MINISTRY OF HEALTH STRATEGIC FRAMEWORK OF COMMUNICATION FOR HIV/AIDS AND STIs INTRODUCTION Communication for HIV/AIDS (SFC HIV/AIDS AND STI) represents an important strategy of the National Programme on
HIV/AIDS Prevention, Treatment and Care among Injecting Drug Users and in Prisons
 HIV/AIDS Prevention, Treatment and Care among Injecting Drug Users and in Prisons Ministerial Meeting on Urgent response to the HIV/AIDS epidemics in the Commonwealth of Independent States Moscow, 31 March
HIV/AIDS Prevention, Treatment and Care among Injecting Drug Users and in Prisons Ministerial Meeting on Urgent response to the HIV/AIDS epidemics in the Commonwealth of Independent States Moscow, 31 March
KENYA AIDS STRATEGIC FRAMEWORK 2014/ /2019
 KENYA AIDS STRATEGIC FRAMEWORK 2014/2015-2018/2019 2 Kenya Aids Strategic Framework 2014/2015 2018/2019 1. Introduction The Kenya AIDS Strategic Framework (KASF 2014/15 2018/19) has been developed in the
KENYA AIDS STRATEGIC FRAMEWORK 2014/2015-2018/2019 2 Kenya Aids Strategic Framework 2014/2015 2018/2019 1. Introduction The Kenya AIDS Strategic Framework (KASF 2014/15 2018/19) has been developed in the
United Nations Development Programme (UNDP) Sudan. Grant Closure Plan HIV Round 5 Global Fund Grant Grant Number: SUD-506-G08-H. Sudan.
 Sudan. Grant Closure Plan HIV Round 5 Global Fund Grant Grant Number: SUD-506-G08-H. Sudan.") United Nations Development Programme (UNDP) Sudan Grant Closure Plan HIV Round 5 Global Fund Grant Grant Number: SUD-506-G08-H Sudan June 2012 Grant Closure Plan, Global Fund Round 5 HIV/AIDS Grant, UNDP
United Nations Development Programme (UNDP) Sudan Grant Closure Plan HIV Round 5 Global Fund Grant Grant Number: SUD-506-G08-H Sudan June 2012 Grant Closure Plan, Global Fund Round 5 HIV/AIDS Grant, UNDP
ACTION PLAN. of the implementation of the National Strategic Plan on the Response to HIV Epidemic
 ACTION PLAN of the implementation of the National Strategic Plan on the Response to HIV Epidemic NN Priority activities Implementing Ministry, agency, organization Timeframe 1 2 3 4 Section 1. Development
ACTION PLAN of the implementation of the National Strategic Plan on the Response to HIV Epidemic NN Priority activities Implementing Ministry, agency, organization Timeframe 1 2 3 4 Section 1. Development
Technical Guidance Note for Global Fund HIV Proposals
 Technical Guidance Note for Global Fund HIV Proposals UNAIDS I World Health Organization I 2011 Rationale for including this activity in the proposal The World Health Organization (WHO), the Joint United
Technical Guidance Note for Global Fund HIV Proposals UNAIDS I World Health Organization I 2011 Rationale for including this activity in the proposal The World Health Organization (WHO), the Joint United
As a result of this training, participants will be able to:
 Addressing Prevention with HIV Positive Clients 1 Day Training This one-day training will prepare participants to help people living with HIV to avoid sexual and substance use behaviors that can result
Addressing Prevention with HIV Positive Clients 1 Day Training This one-day training will prepare participants to help people living with HIV to avoid sexual and substance use behaviors that can result
APPLICANT REQUEST FOR MATCHING FUNDS. IMPORTANT: To complete this form, refer to the Instructions for Matching Funds Requests.
 APPLICANT REQUEST FOR MATCHING FUNDS IMPORTANT: To complete this form, refer to the Instructions for Matching Funds Requests. SUMMARY INFORMATION Applicant CCM GHANA Funding request which this matching
APPLICANT REQUEST FOR MATCHING FUNDS IMPORTANT: To complete this form, refer to the Instructions for Matching Funds Requests. SUMMARY INFORMATION Applicant CCM GHANA Funding request which this matching
EVALUATION TOOLS...123
 EVALUATION TOOLS...123 f Daily evaluation...124 f End of course evaluation...125 f Pre- and post-tests...127 We learned more new technique and method to improve our course at the present The tree gives
EVALUATION TOOLS...123 f Daily evaluation...124 f End of course evaluation...125 f Pre- and post-tests...127 We learned more new technique and method to improve our course at the present The tree gives
U-landshjelp fra Folk til Folk, Norge
 U-landshjelp fra Folk til Folk, Norge HOPE - Delhi Annual Report - January to December, 2016 Introduction Prevention is the mainstay of the national strategy to control HIV/AIDS. In the interest of overall
U-landshjelp fra Folk til Folk, Norge HOPE - Delhi Annual Report - January to December, 2016 Introduction Prevention is the mainstay of the national strategy to control HIV/AIDS. In the interest of overall
The role of UNODC in working law enforcement agencies to promote harm reduction. IHRC, Bangkok, 23 April 2009
 The role of UNODC in working law enforcement agencies to promote harm reduction IHRC, Bangkok, 23 April 2009 Drug control has focused mostly on law enforcement Public health which is the first principle
The role of UNODC in working law enforcement agencies to promote harm reduction IHRC, Bangkok, 23 April 2009 Drug control has focused mostly on law enforcement Public health which is the first principle
SUMMARY OF INTERIM REPORT
 EUROPEAN COMMISSION HEALTH AND CONSUMERS DIRECTORATE-GENERAL EXECUTIVE AGENCY FOR HEALTH AND CONSUMERS Health unit SUMMARY OF INTERIM REPORT Title: Empowering Civil Society and Public Health System to
EUROPEAN COMMISSION HEALTH AND CONSUMERS DIRECTORATE-GENERAL EXECUTIVE AGENCY FOR HEALTH AND CONSUMERS Health unit SUMMARY OF INTERIM REPORT Title: Empowering Civil Society and Public Health System to
South Asia Multi Sector briefs on HIV/AIDS
 South Asia Multi Sector briefs on HIV/AIDS Transport and Infrastructure Why HIV and AIDS Matter to the Transport and other Infrastructure Sectors Between 2-3.5 million people in South Asia are living with
South Asia Multi Sector briefs on HIV/AIDS Transport and Infrastructure Why HIV and AIDS Matter to the Transport and other Infrastructure Sectors Between 2-3.5 million people in South Asia are living with
Note: Staff who work in case management programs should attend the AIDS Institute training, "Addressing Prevention in HIV Case Management.
 Addressing Prevention with HIV Positive Clients This one-day training will prepare participants to help people living with HIV to avoid sexual and substance use behaviors that can result in transmitting
Addressing Prevention with HIV Positive Clients This one-day training will prepare participants to help people living with HIV to avoid sexual and substance use behaviors that can result in transmitting
Submitted to U-landshjelp fra Folk til Folk, Norge
 Submitted to U-landshjelp fra Folk til Folk, Norge HOPE- DELHI Annual Report January to December, 2014 Background of the Project HPPI initiated a Targeted Intervention (TI) project for the Female Sex Workers
Submitted to U-landshjelp fra Folk til Folk, Norge HOPE- DELHI Annual Report January to December, 2014 Background of the Project HPPI initiated a Targeted Intervention (TI) project for the Female Sex Workers
National AIDS Control Program (NACP)
") www.swaniti.in National AIDS Control Program (NACP) AIDS is a global pandemic that affects 34 million people worldwide. According to United Nations programme on HIV and AIDS (UNAIDS), 3.4 million of these
www.swaniti.in National AIDS Control Program (NACP) AIDS is a global pandemic that affects 34 million people worldwide. According to United Nations programme on HIV and AIDS (UNAIDS), 3.4 million of these
Mid-term Review of the UNGASS Declaration of. Commitment on HIV/AIDS. Ireland 2006
 Mid-term Review of the UNGASS Declaration of Commitment on HIV/AIDS Ireland 2006 Irish Role in Global Response Just as the HIV/AIDS epidemic is a global threat, addressing the challenge of the epidemic
Mid-term Review of the UNGASS Declaration of Commitment on HIV/AIDS Ireland 2006 Irish Role in Global Response Just as the HIV/AIDS epidemic is a global threat, addressing the challenge of the epidemic
Tajikistan National Report. Summary HARM REDUCTION WORKS FUND IT! Arguments for strategic investment. Summary of National Report: Tajikistan
 HARM REDUCTION WORKS FUND IT! National Report Summary Arguments for strategic investment With the support of The present document contains a summary of the key conclusions and recommendations provided
HARM REDUCTION WORKS FUND IT! National Report Summary Arguments for strategic investment With the support of The present document contains a summary of the key conclusions and recommendations provided
Empowering Communities for Prevention of Drug Abuse and HIV in India. Project G86 Presentation for PAC 17 Oct 05 Northeast component
 Empowering Communities for Prevention of Drug Abuse and HIV in India Project G86 Presentation for PAC 17 Oct 05 Northeast component G86 The project duration of G86 is 36 months, the main focus are the
Empowering Communities for Prevention of Drug Abuse and HIV in India Project G86 Presentation for PAC 17 Oct 05 Northeast component G86 The project duration of G86 is 36 months, the main focus are the
The President s Emergency Plan for AIDS Relief: Indicators, Reporting Requirements, and Guidelines for Focus Countries. Revised for FY2006 Reporting
 The President s Emergency Plan for AIDS Relief: Indicators, Reporting Requirements, and Guidelines for Focus Countries Revised for FY2006 Reporting July 29, 2005 Contents INTRODUCTION...3 Emergency Plan
The President s Emergency Plan for AIDS Relief: Indicators, Reporting Requirements, and Guidelines for Focus Countries Revised for FY2006 Reporting July 29, 2005 Contents INTRODUCTION...3 Emergency Plan
Towards universal access
 Key messages Towards universal access Scaling up priority HIV/AIDS interventions in the health sector September 2009 Progress report Towards universal access provides a comprehensive global update on progress
Key messages Towards universal access Scaling up priority HIV/AIDS interventions in the health sector September 2009 Progress report Towards universal access provides a comprehensive global update on progress
Implementation of PrEP in Kenya
 Implementation of PrEP in Kenya National AIDs & STI Control Program Ministry of Health November 2017 HIV in Kenya Context Kenya has the world s fourth largest HIV burden, 1.5 million people living with
Implementation of PrEP in Kenya National AIDs & STI Control Program Ministry of Health November 2017 HIV in Kenya Context Kenya has the world s fourth largest HIV burden, 1.5 million people living with
HIV and Sexual reproductive health integration: reaching adolescents and young people. What does this (the above) look like for key populations.
 look like for key populations.") HIV and Sexual reproductive health integration: reaching adolescents and young people. What does this (the above) look like for key populations. JIM, IRENE FRIDAY Presentation Outline Definition of Terms
HIV and Sexual reproductive health integration: reaching adolescents and young people. What does this (the above) look like for key populations. JIM, IRENE FRIDAY Presentation Outline Definition of Terms
Rapid Assessment of Sexual and Reproductive Health
 NIGER Rapid Assessment of Sexual and Reproductive Health and HIV Linkages This summary highlights the experiences, results and actions from the implementation of the Rapid Assessment Tool for Sexual and
NIGER Rapid Assessment of Sexual and Reproductive Health and HIV Linkages This summary highlights the experiences, results and actions from the implementation of the Rapid Assessment Tool for Sexual and
HIV and Hepatitis C Infection among Persons who Inject Drugs: Global Overview and Policy Implications
 HIV and Hepatitis C Infection among Persons who Inject Drugs: Global Overview and Policy Implications Don Des Jarlais, Ph.D. Professor of Psychiatry, Icahn School of Medicine at Mount Sinai UNODC 2014
HIV and Hepatitis C Infection among Persons who Inject Drugs: Global Overview and Policy Implications Don Des Jarlais, Ph.D. Professor of Psychiatry, Icahn School of Medicine at Mount Sinai UNODC 2014
As a result of this training, participants will be able to:
 Addressing Sexual Risk with Drug Users and their Partners 1 Day Training This one-day training will build participant knowledge and skills in offering sexual harm reduction options to substance users.
Addressing Sexual Risk with Drug Users and their Partners 1 Day Training This one-day training will build participant knowledge and skills in offering sexual harm reduction options to substance users.
Female injecting drug users and female sex partners of men who inject drugs Assessing care needs and developing responsive services
 Female injecting drug users and female sex partners of men who inject drugs Assessing care needs and developing responsive services Project HIFAZAT: Strengthen the capacity, reach and quality of IDU harm
Female injecting drug users and female sex partners of men who inject drugs Assessing care needs and developing responsive services Project HIFAZAT: Strengthen the capacity, reach and quality of IDU harm
Part 1: Introduction & Overview
 Part 1: Introduction & Overview We envision a collaborative, participative partnership around IDU that: Provides all relevant and interested stakeholders with a voice and role. Promotes awareness of the
Part 1: Introduction & Overview We envision a collaborative, participative partnership around IDU that: Provides all relevant and interested stakeholders with a voice and role. Promotes awareness of the
UNGASS Declaration of Commitment on HIV/AIDS: Core Indicators revision
 UNGASS Declaration of Commitment on HIV/AIDS: Core Indicators revision Updated version following MERG recommendations Context In light of country reports, regional workshops and comments received by a
UNGASS Declaration of Commitment on HIV/AIDS: Core Indicators revision Updated version following MERG recommendations Context In light of country reports, regional workshops and comments received by a
Prevention and control of Hepatitis B and C among vulnerable groups Estonia: People who use drugs
 Prevention and control of Hepatitis B and C among vulnerable groups Estonia: People who use drugs Aljona Kurbatova National Institute for Health Development Estonia Estimated number of people who inject
Prevention and control of Hepatitis B and C among vulnerable groups Estonia: People who use drugs Aljona Kurbatova National Institute for Health Development Estonia Estimated number of people who inject
ASEAN Declaration of Commitment on HIV and AIDS: Fast-Tracking and Sustaining HIV and AIDS Responses To End the AIDS Epidemic by 2030
 ASEAN Declaration of Commitment on HIV and AIDS: Fast-Tracking and Sustaining HIV and AIDS Responses To End the AIDS Epidemic by 2030 1. WE, the Heads of State and Government of the Association of Southeast
ASEAN Declaration of Commitment on HIV and AIDS: Fast-Tracking and Sustaining HIV and AIDS Responses To End the AIDS Epidemic by 2030 1. WE, the Heads of State and Government of the Association of Southeast
10.4 Advocacy, Communication and Social Mobilization Working Group: summary strategic plan,
 10.4 Advocacy, Communication and Social Mobilization Working Group: summary strategic plan, 2006 2015 Introduction A significant scaling-up of advocacy, communication and social mobilization for TB will
10.4 Advocacy, Communication and Social Mobilization Working Group: summary strategic plan, 2006 2015 Introduction A significant scaling-up of advocacy, communication and social mobilization for TB will
HIV Prevention Prioritization & Implementation Brief: Anambra State
 HIV Prevention Prioritization & Implementation Brief: Anambra State Introduction The HIV epidemic in Nigeria is complex, with substantial heterogeneity in HIV prevalence across different regions and diverse
HIV Prevention Prioritization & Implementation Brief: Anambra State Introduction The HIV epidemic in Nigeria is complex, with substantial heterogeneity in HIV prevalence across different regions and diverse
IDU Outreach Project. Program Guidelines
 Ministry of Health and Long-Term Care Ministère de la Santé et des Soins de longue dureé Prepared by: AIDS Bureau Revision Date: April 2001 TABLE OF CONTENTS 1 Introduction...1 1.1 Program Goals... 2 1.2
Ministry of Health and Long-Term Care Ministère de la Santé et des Soins de longue dureé Prepared by: AIDS Bureau Revision Date: April 2001 TABLE OF CONTENTS 1 Introduction...1 1.1 Program Goals... 2 1.2
HIV AND PEOPLE WHO INJECT DRUGS
 UNAIDS 2017 HIV AND PEOPLE WHO INJECT DRUGS People who use and inject drugs are among the groups at highest risk of exposure to HIV, but remain marginalized and out of reach of health and social services.
UNAIDS 2017 HIV AND PEOPLE WHO INJECT DRUGS People who use and inject drugs are among the groups at highest risk of exposure to HIV, but remain marginalized and out of reach of health and social services.
Drug Use, Harm Reduction, and HIP
 Drug Use, Harm Reduction, and HIP Strategies for Engaging PWIDs in HIV Prevention Services Presented by: Katie Burk, MPH Narelle Ellendon, RN Harm Reduction Coalition Founded in 1993 by needle exchange
Drug Use, Harm Reduction, and HIP Strategies for Engaging PWIDs in HIV Prevention Services Presented by: Katie Burk, MPH Narelle Ellendon, RN Harm Reduction Coalition Founded in 1993 by needle exchange
Rapid Assessment of Sexual and Reproductive Health
 BOTSWANA Rapid Assessment of Sexual and Reproductive Health and HIV Linkages This summary highlights the experiences, results and actions from the implementation of the Rapid Assessment Tool for Sexual
BOTSWANA Rapid Assessment of Sexual and Reproductive Health and HIV Linkages This summary highlights the experiences, results and actions from the implementation of the Rapid Assessment Tool for Sexual
UNGASS COUNTRY PROGRESS REPORT Republic of Armenia
 UNGASS COUNTRY PROGRESS REPORT Republic of Armenia Reporting period: January 2006 December 2007 I. Status at a glance The Armenia UNGASS Country Progress Report was developed under the overall guidance
UNGASS COUNTRY PROGRESS REPORT Republic of Armenia Reporting period: January 2006 December 2007 I. Status at a glance The Armenia UNGASS Country Progress Report was developed under the overall guidance
Strengthening the Evidence for HIV Investments: Allocative Efficiency of HIV Responses: Results and Experiences
 Strengthening the Evidence for HIV Investments: Allocative Efficiency of HIV Responses: Results and Experiences Presentation by: Dr Maxim Berdnikov, Global Fund Importance of Evidence of Impact under the
Strengthening the Evidence for HIV Investments: Allocative Efficiency of HIV Responses: Results and Experiences Presentation by: Dr Maxim Berdnikov, Global Fund Importance of Evidence of Impact under the
SEHAT-The Health Initiative
 SEHAT-The Health Initiative Supported by: INDIA VISION FOUNDATION Presented by C. R. Garg Amrita Bahl Background HIV in India 1,065,070,607: Population of India (July 2004 est.) 5.1 million: Estimated
SEHAT-The Health Initiative Supported by: INDIA VISION FOUNDATION Presented by C. R. Garg Amrita Bahl Background HIV in India 1,065,070,607: Population of India (July 2004 est.) 5.1 million: Estimated
Innovative Approaches for Eliminating Mother-to-Child Transmission of HIV. Male Champions: Men as Change Agents in Uganda MALE CHAMPIONS
 Innovative Approaches for Eliminating Mother-to-Child Transmission of HIV Male Champions: Men as Change Agents in Uganda MALE CHAMPIONS 1 Optimizing HIV Treatment Access for Pregnant and Breastfeeding
Innovative Approaches for Eliminating Mother-to-Child Transmission of HIV Male Champions: Men as Change Agents in Uganda MALE CHAMPIONS 1 Optimizing HIV Treatment Access for Pregnant and Breastfeeding
Hepatitis C Strategy. About us. What is hepatitis C?
 Hepatitis C Strategy About us We support people to take control of their lives and make positive changes. For fifty years we have made a difference to people who want to change their relationship with
Hepatitis C Strategy About us We support people to take control of their lives and make positive changes. For fifty years we have made a difference to people who want to change their relationship with
CONCEPT NOTE Reducing Drug Demand and HIV in Afghanistan Time Frame: June 2010 July 2012
 Background CONCEPT NOTE Reducing Drug Demand and HIV in Afghanistan Time Frame: June 2010 July 2012 Drug abuse in Afghanistan was traditionally limited and customary bound. However due to internal and
Background CONCEPT NOTE Reducing Drug Demand and HIV in Afghanistan Time Frame: June 2010 July 2012 Drug abuse in Afghanistan was traditionally limited and customary bound. However due to internal and
ANNUAL PROJECT PROGRESS REPORT FOR 2008 (draft)
") ANNUAL PROJECT PROGRESS REPORT FOR 2008 (draft) Project Title: HIV/AIDS prevention and care among injecting drug users and in prison settings in Estonia, Latvia and Lithuania Project Number: XEEJ20 Total
ANNUAL PROJECT PROGRESS REPORT FOR 2008 (draft) Project Title: HIV/AIDS prevention and care among injecting drug users and in prison settings in Estonia, Latvia and Lithuania Project Number: XEEJ20 Total
KAZAKHSTAN. National Focal Point. Drug Abuse and Drug Dependence Treatment Situation. Territory : 2,717,300 km 2 Capital: Astana BASIC DATA
 KAZAKHSTAN Territory : 2,717,300 km 2 Capital: Astana Map No. 3771 Rev. 6 UNITED NATIONS January 2004 BASIC DATA Total population (millions) 2009 15.5* Population under age15 (as % of total) 2010 23.8*
KAZAKHSTAN Territory : 2,717,300 km 2 Capital: Astana Map No. 3771 Rev. 6 UNITED NATIONS January 2004 BASIC DATA Total population (millions) 2009 15.5* Population under age15 (as % of total) 2010 23.8*
HIV Prevention Service Provider Survey 2014
 Respondent Demographics This survey will help the Florida HIV Prevention Planning Group (PPG) establish the resources and unmet needs of the communities we serve. Please take a few minutes to complete
Respondent Demographics This survey will help the Florida HIV Prevention Planning Group (PPG) establish the resources and unmet needs of the communities we serve. Please take a few minutes to complete
LOGFRAME TEMPLATE FOR SWAZILAND. SIDA s Contributions
 1 Outcome 7 countries have addressed barriers to efficient and effective linkages between HIV and SRHR policies and services as part of strengthening health systems to increase access to and use of a broad
1 Outcome 7 countries have addressed barriers to efficient and effective linkages between HIV and SRHR policies and services as part of strengthening health systems to increase access to and use of a broad
Methadone Treatment as a Harm Reduction Strategy, Gender Sensitive Programming and Evidence-based Strategies
 Methadone Treatment as a Harm Reduction Strategy, Gender Sensitive Programming and Evidence-based Strategies Wendee Wechsberg, PhD, Senior Director Substance Abuse Treatment Evaluations and Interventions
Methadone Treatment as a Harm Reduction Strategy, Gender Sensitive Programming and Evidence-based Strategies Wendee Wechsberg, PhD, Senior Director Substance Abuse Treatment Evaluations and Interventions
GLOBAL AIDS MONITORING REPORT
 KINGDOM OF SAUDI ARABIA MINISTRY OF HEALTH GLOBAL AIDS MONITORING REPORT COUNTRY PROGRESS REPORT 2017 KINGDOM OF SAUDI ARABIA Submission date: March 29, 2018 1 Overview The Global AIDS Monitoring 2017
KINGDOM OF SAUDI ARABIA MINISTRY OF HEALTH GLOBAL AIDS MONITORING REPORT COUNTRY PROGRESS REPORT 2017 KINGDOM OF SAUDI ARABIA Submission date: March 29, 2018 1 Overview The Global AIDS Monitoring 2017
Steady Ready Go! teady Ready Go. Every day, young people aged years become infected with. Preventing HIV/AIDS in young people
 teady Ready Go y Ready Preventing HIV/AIDS in young people Go Steady Ready Go! Evidence from developing countries on what works A summary of the WHO Technical Report Series No 938 Every day, 5 000 young
teady Ready Go y Ready Preventing HIV/AIDS in young people Go Steady Ready Go! Evidence from developing countries on what works A summary of the WHO Technical Report Series No 938 Every day, 5 000 young
Building a New Approach to Health Care Services for Hard to Reach Clients
 Building a New Approach to Health Care Services for Hard to Reach Clients Community Discussion and Open House January 30, 2013 Fernwood Community Association 1923 Fernwood Street February 6, 2013 North
Building a New Approach to Health Care Services for Hard to Reach Clients Community Discussion and Open House January 30, 2013 Fernwood Community Association 1923 Fernwood Street February 6, 2013 North
PROJECT ŚVETANA (Dawn) Elimination of new HIV infections among children by Scaling up PPTCT services in private health sector
 Elimination of new HIV infections among children by Scaling up PPTCT services in private health sector") PROJECT ŚVETANA (Dawn) Elimination of new HIV infections among children by Scaling up PPTCT services in private health sector Supported by Global Fund for AIDS, TB and Malaria (GFATM) Oct 2015 Dec 2017
PROJECT ŚVETANA (Dawn) Elimination of new HIV infections among children by Scaling up PPTCT services in private health sector Supported by Global Fund for AIDS, TB and Malaria (GFATM) Oct 2015 Dec 2017
Technical Guidance for Global Fund HIV Proposals
 Technical Guidance for Global Fund HIV Proposals FINAL DRAFT DOCUMENT The document will remain in a final draft form for Round 9 and will be finalized for the Round 10 Resource Toolkit. If you would like
Technical Guidance for Global Fund HIV Proposals FINAL DRAFT DOCUMENT The document will remain in a final draft form for Round 9 and will be finalized for the Round 10 Resource Toolkit. If you would like
Taking away the chaos The health needs of people who inject drugs in public places in Glasgow city centre
 Taking away the chaos The health needs of people who inject drugs in public places in Glasgow city centre Plain-language summary The health needs of people who inject drugs in public places in Glasgow
Taking away the chaos The health needs of people who inject drugs in public places in Glasgow city centre Plain-language summary The health needs of people who inject drugs in public places in Glasgow
BUDGET AND RESOURCE ALLOCATION MATRIX
 Strategic Direction/Function ILO Strengthened capacity of young people, youth-led organizations, key service providers and partners to develop, implement, monitor and evaluate HIV prevention programmes
Strategic Direction/Function ILO Strengthened capacity of young people, youth-led organizations, key service providers and partners to develop, implement, monitor and evaluate HIV prevention programmes
Combating HIV/AIDS and stigmatisation
 Goal and objectives Indicators Sources of verification Programme goal Health of vulnerable people has improved. Programme objective Georgian Red Cross has strengthened capacity to improve health of vulnerable
Goal and objectives Indicators Sources of verification Programme goal Health of vulnerable people has improved. Programme objective Georgian Red Cross has strengthened capacity to improve health of vulnerable
HIV PREVENTION, DIAGNOSIS, TREATMENT AND CARE FOR KEY POPULATIONS
 POLICY BRIEF HIV PREVENTION, DIAGNOSIS, TREATMENT AND CARE FOR KEY POPULATIONS CONSOLIDATED GUIDELINES JULY 2014 Policy brief: Consolidated guidelines on HIV prevention, diagnosis, treatment and care for
POLICY BRIEF HIV PREVENTION, DIAGNOSIS, TREATMENT AND CARE FOR KEY POPULATIONS CONSOLIDATED GUIDELINES JULY 2014 Policy brief: Consolidated guidelines on HIV prevention, diagnosis, treatment and care for
Needle and Syringe Programs - 17 October 2013
 Needle and Syringe Programs - 17 October 2013 ANCD Position Paper: Needle and Syringe Programs MEDIA RELEASE 17 October 2013 The Australian National Council on Drugs (ANCD) has today released a position
Needle and Syringe Programs - 17 October 2013 ANCD Position Paper: Needle and Syringe Programs MEDIA RELEASE 17 October 2013 The Australian National Council on Drugs (ANCD) has today released a position
COUNTRY PROFILE: INDIA INDIA COMMUNITY HEALTH PROGRAMS NOVEMBER 2013
 COUNTRY PROFILE: INDIA NOVEMBER 2013 Advancing Partners & Communities Advancing Partners & Communities (APC) is a five-year cooperative agreement funded by the U.S. Agency for International Development
COUNTRY PROFILE: INDIA NOVEMBER 2013 Advancing Partners & Communities Advancing Partners & Communities (APC) is a five-year cooperative agreement funded by the U.S. Agency for International Development
Improving NSP and Harm Reduction Services. Jason Farrell, European HCV and Drug Use Initiative
 Improving NSP and Harm Reduction Services Jason Farrell, European HCV and Drug Use Initiative Presentation Overview With the growing need to treat HCV, NSP programs have been identified in numerous stakeholder
Improving NSP and Harm Reduction Services Jason Farrell, European HCV and Drug Use Initiative Presentation Overview With the growing need to treat HCV, NSP programs have been identified in numerous stakeholder
Nepal Red Cross Society HIV Programme
 EXECUTIVE SUMMARY Nepal Red Cross Society HIV Programme 2008-2010 1. Nepal is considered to have a concentrated Human Immunodeficiency Virus (HIV) epidemic, with an estimated 75,000 persons living with
EXECUTIVE SUMMARY Nepal Red Cross Society HIV Programme 2008-2010 1. Nepal is considered to have a concentrated Human Immunodeficiency Virus (HIV) epidemic, with an estimated 75,000 persons living with
Direct Clinical Services
 Health4Men Health4Men Established in 2008 as a project of the Anova Health Institute, in partnership with the South African Department of Health, and in response to the NSP. The brief was to develop MSMfocused
Health4Men Health4Men Established in 2008 as a project of the Anova Health Institute, in partnership with the South African Department of Health, and in response to the NSP. The brief was to develop MSMfocused
SOUTH ASIA HIV PROGRAMME ( ) Red Cross and Red Crescent Global Alliance on HIV
 Red Cross and Red Crescent Global Alliance on HIV") SOUTH ASIA HIV PROGRAMME (2008-2010) Red Cross and Red Crescent Global Alliance on HIV HIV and AIDS in South Asia An estimated 2.67 million people are infected with HIV in South Asia and approximately
SOUTH ASIA HIV PROGRAMME (2008-2010) Red Cross and Red Crescent Global Alliance on HIV HIV and AIDS in South Asia An estimated 2.67 million people are infected with HIV in South Asia and approximately
IMPACT AND OUTCOME INDICATORS IN THE NATIONAL HIV MONITORING AND EVALUATION FRAMEWORK
 IMPACT AND OUTCOME S IN THE NATIONAL HIV MONITORING AND EVALUATION FRAMEWORK 2008-2012 1. HIV Prevention IMPACT S 1. Percentage of young women and men aged 15 24 who are HIV infected (UNGASS (22), MKUKUTA)
IMPACT AND OUTCOME S IN THE NATIONAL HIV MONITORING AND EVALUATION FRAMEWORK 2008-2012 1. HIV Prevention IMPACT S 1. Percentage of young women and men aged 15 24 who are HIV infected (UNGASS (22), MKUKUTA)
GOVERNMENT OF SIERRA LEONE NATIONAL HIV/AIDS POLICY
 National HIV/AIDS Policy GOVERNMENT OF SIERRA LEONE NATIONAL HIV/AIDS POLICY NATIONAL HIV/AIDS POLICY FOR SIERRA LEONE 1. ACRONYMS CBOs - Community Based Organisations CAC/DAC/RAC - Chiefdom AIDS Committee/District
National HIV/AIDS Policy GOVERNMENT OF SIERRA LEONE NATIONAL HIV/AIDS POLICY NATIONAL HIV/AIDS POLICY FOR SIERRA LEONE 1. ACRONYMS CBOs - Community Based Organisations CAC/DAC/RAC - Chiefdom AIDS Committee/District
Children and AIDS Fourth Stocktaking Report 2009
 Children and AIDS Fourth Stocktaking Report 2009 The The Fourth Fourth Stocktaking Stocktaking Report, Report, produced produced by by UNICEF, UNICEF, in in partnership partnership with with UNAIDS, UNAIDS,
Children and AIDS Fourth Stocktaking Report 2009 The The Fourth Fourth Stocktaking Stocktaking Report, Report, produced produced by by UNICEF, UNICEF, in in partnership partnership with with UNAIDS, UNAIDS,
MYANMAR SEX WORK & HIV MYANMAR SEX WORK & HIV
 e SEX WORK & HIV SEX WORK & HIV Myanmar, formerly known as Burma, has a population of 50 million people [1]. The estimated nation wide population of sex workers in 2007 was between 40,000 and 80,000 and
e SEX WORK & HIV SEX WORK & HIV Myanmar, formerly known as Burma, has a population of 50 million people [1]. The estimated nation wide population of sex workers in 2007 was between 40,000 and 80,000 and
The new German strategy on HIV, Hepatitis B, C and STI, an integrated approach. Ines Perea Ministry of Health, Germany
 The new German strategy on HIV, Hepatitis B, C and STI, an integrated approach Ines Perea Ministry of Health, Germany Reasons for a new strategy in 2016 New international agreements (SDG s) Renewed political
The new German strategy on HIV, Hepatitis B, C and STI, an integrated approach Ines Perea Ministry of Health, Germany Reasons for a new strategy in 2016 New international agreements (SDG s) Renewed political
Working Document on Monitoring and Evaluating of National ART Programmes in the Rapid Scale-up to 3 by 5
 Working Document on Monitoring and Evaluating of National ART Programmes in the Rapid Scale-up to 3 by 5 Introduction Currently, five to six million people infected with HIV in the developing world need
Working Document on Monitoring and Evaluating of National ART Programmes in the Rapid Scale-up to 3 by 5 Introduction Currently, five to six million people infected with HIV in the developing world need
Bangladesh United Nations Regional Task Force on Injecting Drug Use and HIV/AIDS in Asia and the Pacific Baseline Assessment Dec 2006
 ACRONYMS BANGLADESH AIDS AusAID BSS CHR CSW DfID (UK) DGHS DNC DU GOs HIV HR ICDDR, B IDUs IEC LCCS MSM NAC NASP NCB NEP NGOs NNCB NSEP OST OW PLI PLWHA RSRA Acquired Immunodeficiency Syndrome Australian
ACRONYMS BANGLADESH AIDS AusAID BSS CHR CSW DfID (UK) DGHS DNC DU GOs HIV HR ICDDR, B IDUs IEC LCCS MSM NAC NASP NCB NEP NGOs NNCB NSEP OST OW PLI PLWHA RSRA Acquired Immunodeficiency Syndrome Australian
Minister s Opioid Emergency Response Commission Recommendations to the Minister Updated July 5, 2018
 The Minister s Opioid Emergency Response Commission was established May 31, 2017 to support the Government of Alberta s urgent response to the opioid crisis. As part of its mandate, the Commission is responsible
The Minister s Opioid Emergency Response Commission was established May 31, 2017 to support the Government of Alberta s urgent response to the opioid crisis. As part of its mandate, the Commission is responsible
The road towards universal access
 The road towards universal access Scaling up access to HIV prevention, treatment, care and support 22 FEB 2006 The United Nations working together on the road towards universal access. In a letter dated
The road towards universal access Scaling up access to HIV prevention, treatment, care and support 22 FEB 2006 The United Nations working together on the road towards universal access. In a letter dated
Update on Community-based harm reduction services in Nelson Mandela Bay 25/10/2018
 Update on Community-based harm reduction services in Nelson Mandela Bay 25/10/2018 Overview Background to injecting drug use Overview of harm reduction Data on Hepatitis Summary of services provided by
Update on Community-based harm reduction services in Nelson Mandela Bay 25/10/2018 Overview Background to injecting drug use Overview of harm reduction Data on Hepatitis Summary of services provided by
NATIONAL PROGRAMME ON THE RESPONSE TO THE HIV EPIDEMIC
 NATIONAL PROGRAMME ON THE RESPONSE TO THE HIV EPIDEMIC 2013-2016 TABLE OF CONTENTS Abbreviations... 3 I Terms and definitions... 4 II Introduction... 6 III Goal of the National Programme on the Response
NATIONAL PROGRAMME ON THE RESPONSE TO THE HIV EPIDEMIC 2013-2016 TABLE OF CONTENTS Abbreviations... 3 I Terms and definitions... 4 II Introduction... 6 III Goal of the National Programme on the Response
Differentiated Care for Antiretroviral Therapy for Key Populations: Case Examples from the LINKAGES Project
 Differentiated Care for Antiretroviral Therapy for Key Populations: Case Examples from the LINKAGES Project NOVEMBER 2017 An estimated 37 million people are living with HIV today. A response to the need
Differentiated Care for Antiretroviral Therapy for Key Populations: Case Examples from the LINKAGES Project NOVEMBER 2017 An estimated 37 million people are living with HIV today. A response to the need
Challenges in Scaling-up TB/HIV collaborative activities in a diverse HIV epidemic -India
 Challenges in Scaling-up TB/HIV collaborative activities in a diverse HIV epidemic -India Dr. B. B. Rewari WHO National Consultant National Programme Officer (ART) National AIDS Control Organisation New
Challenges in Scaling-up TB/HIV collaborative activities in a diverse HIV epidemic -India Dr. B. B. Rewari WHO National Consultant National Programme Officer (ART) National AIDS Control Organisation New
Executive Board of the United Nations Development Programme, the United Nations Population Fund and the United Nations Office for Project Services
 United Nations Executive Board of the United Nations Development Programme, the United Nations Population Fund and the United Nations Office for Project Services Distr.: General 12 July 2011 Original:
United Nations Executive Board of the United Nations Development Programme, the United Nations Population Fund and the United Nations Office for Project Services Distr.: General 12 July 2011 Original:
DEPARTMENT OF HEALTH RESPONSE TO KEY POPULATIONS
 DEPARTMENT OF HEALTH RESPONSE TO KEY POPULATIONS KEY POPULATIONS PREVENTION INTERVENTIONS Ms E Marumo HIV PREVENTION STRATEGIES 13 June 2017 1 Background SA has about 7.1 million people living with HIV
DEPARTMENT OF HEALTH RESPONSE TO KEY POPULATIONS KEY POPULATIONS PREVENTION INTERVENTIONS Ms E Marumo HIV PREVENTION STRATEGIES 13 June 2017 1 Background SA has about 7.1 million people living with HIV
Getting There: Community Policing to Police Social Responsibility Law enforcement & HIV prevention
 Getting There: Community Policing to Police Social Responsibility Law enforcement & HIV prevention Soumen Mitra Inspector General of Police CID Calcutta India Perception in conflict The burden of the badge
Getting There: Community Policing to Police Social Responsibility Law enforcement & HIV prevention Soumen Mitra Inspector General of Police CID Calcutta India Perception in conflict The burden of the badge
Bukoba Combination Prevention Evaluation: Effective Approaches to Linking People Living with HIV to Care and Treatment Services in Tanzania
 Bukoba Combination Prevention Evaluation: Effective Approaches to Linking People Living with HIV to Care and Treatment Services in Tanzania COUNTRY: Tanzania Tanzania has successfully implemented the standard
Bukoba Combination Prevention Evaluation: Effective Approaches to Linking People Living with HIV to Care and Treatment Services in Tanzania COUNTRY: Tanzania Tanzania has successfully implemented the standard
Executive Board of the United Nations Development Programme, the United Nations Population Fund and the United Nations Office for Project Services
 United Nations Executive Board of the United Nations Development Programme, the United Nations Population Fund and the United Nations Office for Project Services Distr.: General 15 April 2011 Original:
United Nations Executive Board of the United Nations Development Programme, the United Nations Population Fund and the United Nations Office for Project Services Distr.: General 15 April 2011 Original:
ISHTAR - PROGRAMME REVIEW REPORT
 JULY 31, 2017 ISHTAR - PROGRAMME REVIEW REPORT 2014-2016 ISHTAR MANAGEMENT Nairobi Acronym: AIDS Acquired Immune Deficiency Syndrome ART Anti-Retroviral Therapy. CASCO County AIDS and STI Coordinator CD4
JULY 31, 2017 ISHTAR - PROGRAMME REVIEW REPORT 2014-2016 ISHTAR MANAGEMENT Nairobi Acronym: AIDS Acquired Immune Deficiency Syndrome ART Anti-Retroviral Therapy. CASCO County AIDS and STI Coordinator CD4
National HIV/STI Programme Overview
 National HIV/STI Programme Overview HIV/AIDS IN JAMAICA Sero-prevalence among adults 1.7% Estimated No. with HIV/AIDS 27,000 (?31,000) Est. No. unaware of HIV status 15,000 No. of persons in need of ARV
National HIV/STI Programme Overview HIV/AIDS IN JAMAICA Sero-prevalence among adults 1.7% Estimated No. with HIV/AIDS 27,000 (?31,000) Est. No. unaware of HIV status 15,000 No. of persons in need of ARV
LEARNING LESSONS THROUGH DATA TRIANGULATION: VULNERABILITY OF SURAT CITY TO HIV EPIDEMIC
 Original article LEARNING LESSONS THROUGH DATA TRIANGULATION: VULNERABILITY OF SURAT CITY TO HIV EPIDEMIC Anjali Modi 1, J K Kosambiya 2, H K Sondharwa 3, Manish Kumar 4 Financial Support: None declared
Original article LEARNING LESSONS THROUGH DATA TRIANGULATION: VULNERABILITY OF SURAT CITY TO HIV EPIDEMIC Anjali Modi 1, J K Kosambiya 2, H K Sondharwa 3, Manish Kumar 4 Financial Support: None declared
Groups of young people in Uganda that need to be targeted with HIV interventions
 Module 5: HIV/AIDS and young people - Adolescent health and development with a particular focus on sexual and reproductive health - Assignment Peter James Ibembe Reproductive Health Uganda, Kampala, Uganda
Module 5: HIV/AIDS and young people - Adolescent health and development with a particular focus on sexual and reproductive health - Assignment Peter James Ibembe Reproductive Health Uganda, Kampala, Uganda
FPA Sri Lanka Policy: Men and Sexual and Reproductive Health
 FPA Sri Lanka Policy: Men and Sexual and Reproductive Health Introduction 1. FPA Sri Lanka is committed to working with men and boys as clients, partners and agents of change in our efforts to meet the
FPA Sri Lanka Policy: Men and Sexual and Reproductive Health Introduction 1. FPA Sri Lanka is committed to working with men and boys as clients, partners and agents of change in our efforts to meet the
HCV Action and Bristol & Severn ODN workshop, 14 th September 2017: Summary report
 HCV Action and Bristol & Severn ODN workshop, 14 th September 2017: Summary report About HCV Action HCV Action is a network, co-ordinated by The Hepatitis C Trust, that brings together health professionals
HCV Action and Bristol & Severn ODN workshop, 14 th September 2017: Summary report About HCV Action HCV Action is a network, co-ordinated by The Hepatitis C Trust, that brings together health professionals
Becoming a harm reduction distribution agency in Toronto - information session
 Becoming a harm reduction distribution agency in Toronto - information session Kris Guthrie, RN BScN Health Promotion Specialist, The Works Toronto Public Health May 2016 Overview Brief backgrounder Harm
Becoming a harm reduction distribution agency in Toronto - information session Kris Guthrie, RN BScN Health Promotion Specialist, The Works Toronto Public Health May 2016 Overview Brief backgrounder Harm
Implementation Status & Results India India: Third National HIV/AIDS Control Project (P078538)
") Public Disclosure Authorized Public Disclosure Authorized The World Bank Implementation Status & Results India India: Third National HIV/AIDS Control Project (P078538) Operation Name: India: Third National
Public Disclosure Authorized Public Disclosure Authorized The World Bank Implementation Status & Results India India: Third National HIV/AIDS Control Project (P078538) Operation Name: India: Third National
Performance Management Plan Indicator Worksheet #1
 Performance Management Plan Indicator Worksheet #1 Adapted from Investing in People: Indicators and Definitions (USAID) 1. Name and number of Strategic Objective: Reduced mother-to-child transmission of
Performance Management Plan Indicator Worksheet #1 Adapted from Investing in People: Indicators and Definitions (USAID) 1. Name and number of Strategic Objective: Reduced mother-to-child transmission of
Version for the Silent Procedure 29 April Agenda item January Hepatitis
 Version for the Silent Procedure 29 April 2014 134th session EB134.R18 Agenda item 10.5 25 January 2014 Hepatitis The Executive Board, Having considered the report on hepatitis, 1 RECOMMENDS to the Sixty-seventh
Version for the Silent Procedure 29 April 2014 134th session EB134.R18 Agenda item 10.5 25 January 2014 Hepatitis The Executive Board, Having considered the report on hepatitis, 1 RECOMMENDS to the Sixty-seventh