TREATMENT FOR HEPATITIS C: NEW TESTS, NEW DRUGS AND NEW RECOMMENDATIONS
|
|
|
- Job Brent McDaniel
- 6 years ago
- Views:
Transcription
1 TREATMENT FOR HEPATITIS C: NEW TESTS, NEW DRUGS AND NEW RECOMMENDATIONS Anthony Martinez, MD Associate Professor of Medicine University at Buffalo Division of GI and Hepatology
2 DISCLOSURE Speaking: Abbvie, Gilead, Bayer, Salix, BMS Consulting: Gilead, Intercept Research: Abbvie, Gilead, Merck, Tobira
3 LEARNING OBJECTIVES: 1.Explain the epidemiology of the hepatitis C virus (HCV). 2. Discuss laboratory testing and diagnosis of HCV infection. 3. Design a therapeutic regimen and monitoring plan for the treatment of HCV.

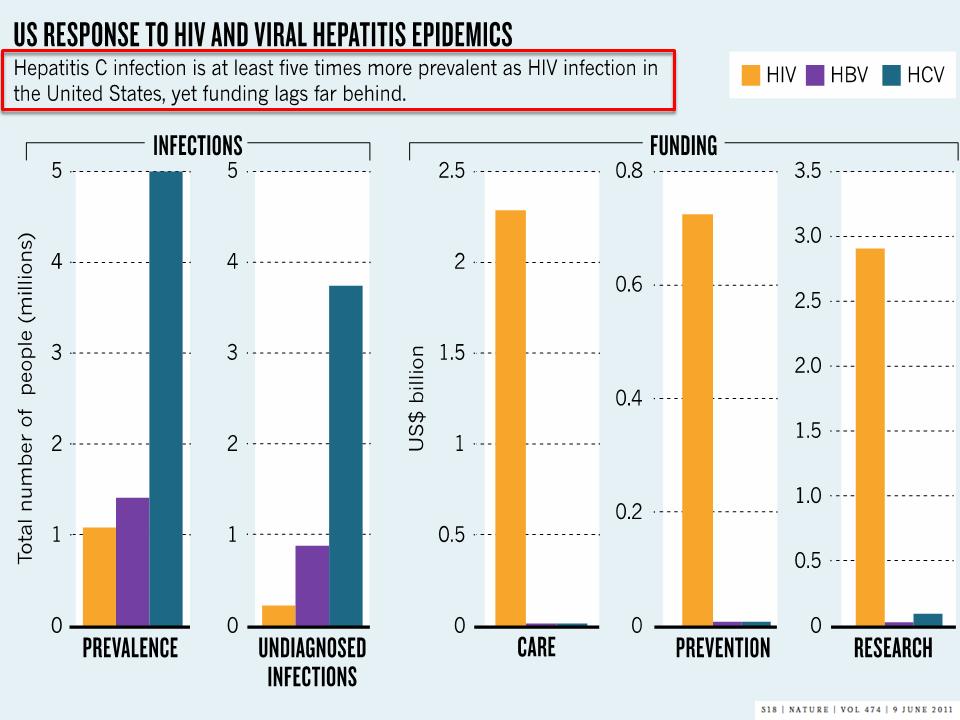
4 Total No. Infected (millions) HCV vs. HIV vs. HBV Prevalence 4 Prevalence of Chronic Viral Infections 2.7 to 3.9 Million 1 75% Unaware of Infection Million 1 21% Unaware of Infection ~800,000 to 1.4 Million 1 65% Unaware of Infection Undiagnosed Diagnosed 0 HIV HBV HCV Estimated 5.2 million persons in US are HCV infected 2 HBV=hepatitis B virus; HCV=hepatitis C virus; HIV=human immunodeficiency virus. 1. Institute of Medicine. Washington, DC: The National Academies Press; Chak E, et al. Liver Int. 2011;31(8):
5 HCV Can Now Be Cured in Most Patients Unlike HIV and HBV infection, HCV infection is a curable disease What does cure mean? Sustained Viral Response Undetectable HCV RNA 12 weeks after completion of antiviral therapy for chronic HCV infection 1 Long term morbidity and mortality benefits 1. Ghany MG, et al. Hepatology. 2009;49(4):
6 Rate per 100,000 People Deaths From HCV vs. HIV 7 6 HIV Change in Mortality Rates From 1999 to Hepatitis C 15,106 12, Hepatitis B 1, Year Ly KN, et al. Ann Intern Med. 2012;156(4):
7 Individuals, N Majority of HCV-Infected Individuals Are Baby Boomers (Born Between ) 1,600,000 Estimated Prevalence by Age Group 1,400,000 1,200,000 1,000, , , , ,000 0 < Birth Year Group Centers for Disease Control and Prevention. MMWR. 2012;61(RR-4):1-32.
8 Most Patients with Chronic Hepatitis C in the US Are Not Aware That They Are Infected ~5,300,000 individuals are infected with the hepatitis C virus in the United States Lack of knowledge & awareness among health care providers Lack of knowledge & awareness among at-risk populations Insufficient understanding about the extent and seriousness of this public health problem 1,325,000 (~25%) AWARE 3,975,000 (~75%) UNAWARE
9 Number of Cases HCV-Related Decompensated Cirrhosis and HCC Projected to Rise in the US 160, , , ,000 80,000 Decompensated Cirrhosis 60,000 40,000 20,000 Hepatocellular Carcinoma HCV-related decompensated cirrhosis and HCC are rising as manifestations of liver disease in aging population % of HCV-related deaths occurred among persons years of age Median age was 57 years; ~20 years less than the average lifespan of persons living in the US 2,* Projection based on a dynamic, multicohort, natural history model of data from the CDC, NHANES, and a review of the medical literature, with conservative estimates of disease progression and complications. Model assumes first-year mortality of 80%-85% for HCC. *During the period from 1999 to Davis GL, et al. Gastroenterology. 2010;138: ; 2. Smith BD, et al. MMWR Recomm Rep. 2012;61(RR-4):1-32.

10 Increasing Health Care Costs Associated With Progressive Liver Disease in the Aging HCV- Infected Population Prevalence (95% CI) Health Care Cost (95% CI) While the prevalence of HCV infection is declining from its peak, the incidence of advanced liver disease and associated health care costs continue to rise Modeling does not take into account any impact of birth cohort screening A system dynamic modeling framework was used to quantify the HCV-infected population, the disease progression, and the associated cost from CI=confidence interval. Razavi H, et al. Hepatology Epub ahead of print.

11 Costs (per-patient-per-month) (US$) All-Cause Health Care Costs by Liver Disease Severity (US$, 2010) Numbers in parentheses are ± standard deviation. *P<.001 and P=.004 vs noncirrhotic liver disease. Total health care costs include pharmacy and medical costs. Pharmacy costs are based on 2-drug therapy with PegIFN and RBV. Adapted from Gordon SC, et al. Hepatology. 2012;56:

12 Estimated Mean Annual Costs Impact of Disease Severity on Health Care Costs in Chronic HCV Infection *Assumes follow-up time not associated with disease severity. ESLD=end-stage liver disease; OLT=orthotopic liver transplantation. Gordon SC, et al. Hepatology. 2012;56:
13 SVR Reduces HCC and Liver-Related Complications in Advanced Fibrosis/Cirrhosis Cumulative Incidence (%) Cumulative Incidence (%) HCC (n=307) Liver-Related Complications* (n=307) Follow-Up (years) Follow-Up (years) *Ascites, variceal bleeding. 307 HCV patients with bridging fibrosis (n=127) or cirrhosis (n=180) were evaluated by Cox regression analysis. Non-SVR in 67% of patients treated with pegylated interferon plus ribavirin. Median follow-up: 3.5 years. Cardoso A-C, et al. J Hepatol. 2010;52:
14 Cumulative Mortality (%) SVR Reduced Risk of All-Cause Mortality in a Retrospective VA Study Genotype 1 (n=12,166) SVR rate: 35% Genotype 2 (n=2904) SVR rate: 72% Genotype 3 (n=1794) SVR rate: 62% Years Years Years Retrospective analysis of veterans who received pegylated interferon plus ribavirin at any VA medical facility ( ). SVR=sustained virological response. Backus LI, et al. Clin Gastroenterol Hepatol. 2011;9:
15
16 Acute HCV Cases By Age in the United States Klevens, CID,

17 Past Month and Past Year Heroin Use among Persons Aged 12 or Older: Samhsa.gov 17

18 Increased Injection Drug Use In Adolescents and Young Adults is Shifting the US HCV Demographic 18
* Erie County (prevalence 1.2%) Erie County (prevalence 2.")
19 Number of HCV Cases HCV Prevalence In NYS HCV Cases NYS (prevalence 0.6%)* Erie County (prevalence 1.2%) Erie County (prevalence 2.9%)** * Excludes NYC ** Based on CDC estimates 19

20 HCV Linking to Care


21 Treatment Cascade for People with Chronic HCV Infection in US Yehia BR et al. PLoS ONE July 2014
22 Updates in HCV Screening
23 Current Status of HCV in the US: Screening and Linkage to Care Rates Remain Low US population with chronic HCV infection 3.2 million HCV detected 1.6 million (50%) Referred to care million (32%-38%) HCV RNA test 630, ,000 (20-23%) Liver biopsy 380, ,000 (12%-18%) Treated 220, ,000 (7-11%) Successfully treated 170, ,000 (5-6%) Holmberg SD et al, New Engl J Med. 2013;

24 CDC Has Revised Screening Recommendations for HCV
25 Candidates for Screening for HCV 2012 Additional Recommendations Recommendations 2 Birth Cohort Screening Adults born during should receive one-time testing for HCV without prior ascertainment of HCV risk Persons who have injected illicit drugs in the recent and remote past Persons with conditions associated with a high prevalence of HCV infection Prior recipients of transfusions or organ transplants prior to July 1992 Children born to HCV-infected mothers Health care, emergency medical and public safety workers after a needle stick injury or mucosal exposure to HCV-positive blood Current sexual partners of HCV-infected persons 1. Centers for Disease Control and Prevention. Recommendations for the identification of chronic hepatitis C virus infection among persons born during MMWR Recomm Rep 2012;61 (RR-4): Centers for Disease Control and Prevention. Recommendations for prevention and control of hepatitis C virus (HCV) infection and HCVrelated chronic disease. MMWR Recomm Rep 1998;47:1-39.
26 Governor Signs Health Care Bill October 2013 Hepatitis C Virus Testing (Chapter 425 of the Laws of 2013) This new law requires a hepatitis C virus screening test to be offered to all patients born between 1945 and 1965 who are receiving health services as a hospital inpatient or receiving primary care services and applies to physicians, physician assistants, and nurse practitioners. The law further requires that the health care provider refer a patient who receives a positive screening test to another provider to receive confirmatory testing and follow-up care. In effect as of January 1, 2014 and expires on January 1, 2020
27 Hepatitis C Screening and Prevalence Among Veterans in 2012 Assess the extent to which Veterans in recent care, particularly those born between , have been screened for HCV Assess HCV infection prevalence by birth cohort to determine if the emphasis on birth cohort screening applied to the VA population Estimate the potential clinical impact of complete birth cohort screening Backus L, et al. AASLD 2013 Oral Presentation #21

28 Veterans with Outpatient Visits in 2012 Backus L, et al. AASLD 2013 Oral Presentation #21
 Veterans in care in 2012 had been screened for HCV Backus L, et al.")
29 HCV Screening Rates ,009,918 of the 5,500,309 (54.7%) Veterans in care in 2012 had been screened for HCV Backus L, et al. AASLD 2013 Oral Presentation #21
30 HCV Ab Prevalence % had viral load or genotype testing Backus L, et al. AASLD 2013 Oral Presentation #21
31 HCV Infection Prevalence Among Veterans in Care in 2012 Born Based on Year of First HCV Screening Backus L, et al. AASLD 2013 Oral Presentation #21
32 Screening In Emergency Department Identifies a Large Cohort of HCV-infected Baby Boomers University of Alabama at Birmingham implemented an opt-out HCV screening model for clinically stable baby boomers ER triage nurses identified all patient born between and administered a brief prescreening questionnaire Exclusion criteria: Prior testing, opt-out or too sick All eligible patients offered HCV screening with confirmatory testing with PCR in Anti-HCV Ab positive persons Galbraith J, et al. AASLD 2013 Abstract

33 Screening In Emergency Department Identifies a Large Cohort of HCV-infected Baby Boomers Over a 6 week period, 1,721 patients born were surveyed Unaware of status, 78.8% Accepted testing, 90.8% HCV seropositive, 12.0% HCV RNA detected, 72.5% Urban EDs are high-prevalence settings; challenges for linkage to care HCV prevalence by health insurance status Uninsured Public / Medicaid Other Medicare Private (18.5%) (17.2%) 35 (16.7%) 10 (4.4%) 33 (10.5%) Non-Reactive Reactive Galbraith JW et al. The Liver Meeting 2013; LB-6 Overall HCV + 12%

34 ICD-9 and CPT HCV Screening Codes


35 HCV Antibody Test Patient exposed to HCV Need HCV RNA test to confirm chronic infection Patient Not Exposed Continue to screen based on active risk factors If HIV positive and CD4 <200, need HCV RNA test
36 HCV Antibody HCV RNA Confirmatory Testing Patient is NOT chronically infected Tell the patient he/she can still become infected if high risk activity continues Educate regarding transmission and exposure Counsel on harm reduction
37 HCV Antibody HCV RNA Confirmatory Testing Patient IS chronically infected Emphasize that HCV is progressive and highlight complications Explain that HCV is curable with oral interferon free regimens Explain how to limit risk of transmission (clean works; don t share razors, toothbrush; bleach for tattooing equipment Advise patient how to prevent further liver damage ETOH cessation
38 Linkage To Care Refer for specialist care REGARDLESS of viral load and liver enzyme levels Viral load level does not correlate with disease severity Liver enzymes may be normal in chronic infection, even with advanced disease Most chronically infected patients have no symptoms Explain what to expect when seen by specialist Emphasize importance of keeping the appointment








39 HCV Screening Algorithm HCV RNA Negative Stop. Patient is a spontaneous resolver (antibody positive, negative viral load) HCV Antibody Screen HCV Antibody Positive Check HCV RNA Quant and Genotype HCV RNA Positive CBC with diff, Comp. Metabolic Panel AFP, RhF PT/INR Platelets <120 Albumin <3.5 INR > 1.3 Bilirubin >2 Do US with PV diameter and Spleen size Consider CT or MRI with and without contrast to confirm cirrhosis and screen for HCC Refer to Liver Clinic
40 HEPATITIS C TREATMENT
41 HCV Therapy: Past, Present and Future Ribavirin Suppression of HCV with DAA combination (PI + NI) Interferon Proof of concept for DAA (PI) Approval of Telaprevir and Boceprevir Approval of Sofsobuvir/L edipasvir and Viekira Pegylated interferons Approval of simeprevir and sofosbuvir w/ifn (G1) -First approved IFNfree therapy: SOF+RBV for GT 2,3
42 Cure Rate* Rising Cure Rates for Chronic HCV 100% 80% Telaprevir or Boceprevir + PegIFN/RBV 70% 2 nd Gen DAAs IFN-Free Regimens >90% 3 rd Gen DAAs IFN-Free Regimens >95% 60% 40% 20% IFN 16% IFN/RBV 35% PegIFN/RBV 44% 0% *Cure rates based on data from clinical trials Year
43 Characteristics of HCV DAA Classes Characteristic Protease inhibitors (SMV, PAR/r, GRZ) Nucleos(t)ide Polymerase inhibitors (SOF) Nonnucleoside Polymerase inhibitors (DAS) NS5A inhibitors (LDV, OMB, DCV, ELB) Potency High; Variable among genotypes Moderate-high Pangenotypic Variable; variable among genotypes High; variable among genotypes Barrier to Resistance Low 1a < 1b High 1a = 1b Very Low 1a < 1b Low 1a < 1b Drug Interaction CYP3A4 OATP1B1/3 P-gp UGT1A1 Minimal CYP2C8 UGT1A1 OATP1B1/3, BCRP, P-gp UGT1A1 Dosing QD QD QD to BID QD
44 HCV Treatment Paradigm Shift Then Difficult regimens weeks of treatment Moderately successful Support patients to manage extensive side effects and drug-drug interactions Now Easier regimens 8-12 weeks of treatment Highly successful Prepare patients for treatment and a cure 44
45 When and in Whom to Initiate HCV Therapy Treatment is recommended for patients with chronic HCV infection (Class I, Level A) Treatment is assigned the highest priority for those patients with advanced fibrosis (METAVIR F3), those with compensated cirrhosis (METAVIR F4), liver transplant recipients, and patients with severe extrahepatic HCV (cryoglobulinemia, DM, debilitating fatigue) Based on available resources, treatment should be prioritized as necessary so that patients at high risk for liverrelated complications (those with HIV, HBV) and severe extrahepatic hepatitis C complications are given high priority AASLD, IDSA, IAS USA. Recommendations for testing, managing, and treating hepatitis C. Accessed August 12, 2014.
46 Initial Tx Recommendations Genotype 1a/b Regimen Daily fixed-dose combination of ledipasvir (90 mg)/sofosbuvir (400 mg) for 8-12 weeks. Daily fixed-dose combination of paritaprevir (150 mg)/ritonavir (100 mg)/ombitasvir (25 mg) plus twice-daily dosed dasabuvir (250 mg) and weightbased RBV (1000 mg [<75 kg] to 1200 mg [>75 kg]) for 12 weeks (no cirrhosis) or 24 weeks (cirrhosis)
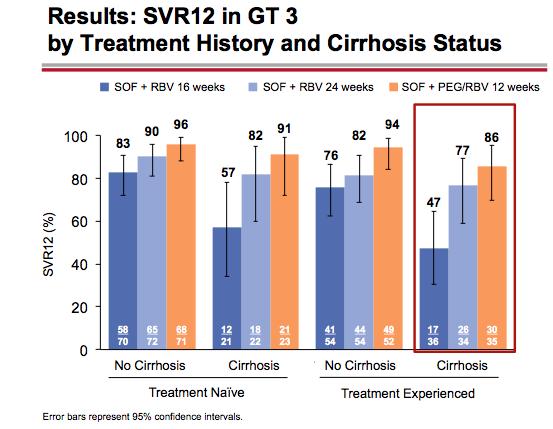
47 Initial Tx Recommendations Genotype Regimen 2 Daily sofosbuvir (400 mg) and weightbased RBV (1000 mg [<75 kg] to 1200 mg [>75 kg]) for 12 weeks is recommended for treatment-naive patients (consider 16 weeks in cirrhotics) 3 Daily sofosbuvir (400 mg) and weightbased RBV (1000 mg [<75 kg] to 1200 mg [>75 kg]) for 24 weeks
48 Initial Tx Recommendations Genotype Regimen 4, 6 Daily fixed-dose combination of ledipasvir (90 mg)/sofosbuvir (400 mg) for 12 weeks (Geno 4 and 6) Daily fixed-dose combination of paritaprevir (150 mg)/ritonavir (100 mg)/ombitasvir (25 mg) and weightbased RBV (1000 mg [<75 kg] to 1200 mg [>75 kg]) for 12 weeks (Geno 4) 5 Daily sofosbuvir (400 mg) and weightbased RBV (1000 mg [<75 kg] to 1200 mg [>75 kg]) plus weekly PEG-IFN for 12 weeks
, a hepatitis C virus (HCV) NS5A inhibitor, and sofosbuvir (400 mg), an HCV nucleotide analog NS5B polymerase inhibitor Is an interferon (IFN)-free and ribavirin (RBV)-free regimen")
49 New HCV Treatment: SOF/LDV Indicated for the treatment of chronic hepatitis C (CHC) genotype (GT) 1 infection in adults SOF/LDV The first and only once-daily, single-tablet regimen containing ledipasvir (90 mg), a hepatitis C virus (HCV) NS5A inhibitor, and sofosbuvir (400 mg), an HCV nucleotide analog NS5B polymerase inhibitor Is an interferon (IFN)-free and ribavirin (RBV)-free regimen Pill not actual size


50 New HCV Treatment: SOF/LDV Sofosbuvir An inhibitor of the HCV NS5B RNA-dependent RNA polymerase, which is required for viral replication Ledipasvir An inhibitor of the HCV NS5A protein, which is required for viral replication
51 Background Ledipasvir Potency against HCV GT 1a and 1b 1 Effective against NS5B RAV S282T 2 Once-daily, oral, 90 mg LDV NS5A inhibitor Sofosbuvir Potent antiviral activity against HCV GT 1 6 High barrier to resistance Once-daily, oral, 400-mg tablet approved for use with other agents to treat HCV infection SOF nucleotide polymerase inhibitor Ledipasvir/Sofosbuvir FDC Once-daily, oral fixed-dose (400/90 mg) combination tablet No food effect >2000 patients treated LDV NS5A inhibitor SOF nucleotide polymerase inhibitor 1. Lawitz E, et al. EASL 2011, poster 1219; 2. Cheng G, et al. EASL 2012, poster 1172.
52 New HCV Treatment: Harvoni The recommended dosage of HARVONI for adults is one tablet taken orally once daily with or without food RECOMMENDED REGIMEN AND TREATMENT DURATION IN GT1 CHC PATIENTS 1 Treatment-naïve HARVONI TABLET DAILY patients with or without cirrhosis Treatmentexperienced patients b without cirrhosis Treatmentexperienced patients b with cirrhosis 12 weeks a 12 weeks 24 weeks a HARVONI for 8 weeks can be considered in treatment-naïve patients without cirrhosis who have pre-treatment HCV RNA less than 6 million IU/mL. b Treatment-experienced patients who have failed treatment with either peginterferon (Peg-IFN) alfa + RBV or an HCV protease inhibitor (PI) + Peg-IFN alfa + RBV. Relapse rates are affected by baseline host and viral factors and differ between treatment durations for certain subgroups No dose recommendation can be given for patients with severe renal impairment (estimated Glomerular Filtration Rate [egfr] <30 ml/min/1.73m 2 ) or with end stage renal disease (ESRD) due to higher exposures (up to 20-fold) of the predominant sofosbuvir metabolite 4
53 SVR12, % HARVONI Provided High SVR12 Rates in CHC GT 1 Subjects Regardless of the inclusion of RBV OVERALL SVR12 RATES ACROSS ION STUDIES % 96% 99% 93% 97% 99% 94% 96% 99% a ION-3 8 Weeks ION-3 12 Weeks ION-1 12 Weeks b ION-2 12 Weeks ION-2 24 Weeks HARVONI HARVONI + RBV a Excluding 1 subject with GT 4 infection. 1 b SVR rates for all treatment-naïve subjects enrolled in the 24-week treatment groups (N = 434) were not available at the time of the interim analysis. HCV RNA analyzed by COBAS TaqMan HCV Test v2.0 HPS, with lower limit of quantification (LLOQ) of 25 IU/mL HARVONI US full Prescribing Information. Gilead Sciences, Inc. Foster City, CA. March Afdhal N, et al. N Engl J Med. 2014;370: Afdhal N, et al. N Engl J Med. 2014;370: Kowdley KK, et al. N Engl J Med. 2014;370:
54 Adding RBV to HARVONI resulted in an increased incidence of adverse reactions 2-4 IMPORTANT SAFETY INFORMATION: ADVERSE REACTIONS 1 Most common ( 10%, all grades) adverse reactions were fatigue and headache ADVERSE REACTIONS (ALL GRADES) REPORTED IN SUBJECTS RECEIVING 8, 12, OR 24 WEEKS OF TREATMENT WITH HARVONI ± RBV 2-4 HARVONI 8 Weeks N = 215 HARVONI + RBV 8 Weeks N = 216 HARVONI 12 Weeks N = 539 HARVONI + RBV 12 Weeks N = 328 HARVONI 24 Weeks N = 326 HARVONI + RBV 24 Weeks N = 328 Fatigue 21% 35% 22% 38% 24% 40% Headache 14% 25% 21% 23% 24% 30% Nausea 7% 18% 11% 17% 11% 17% Insomnia 5% 12% 8% 19% 9% 20% Diarrhea 7% 6% 7% 7% 10% 9% The majority of adverse reactions with HARVONI alone occurred at a severity of grade 1 1 Direct comparison across studies should not be made due to differing study designs. 1. HARVONI US full Prescribing Information. Gilead Sciences, Inc. Foster City, CA. March Afdhal N, et al. N Engl J Med. 2014;370: Afdhal N, et al. N Engl J Med. 2014;370: Kowdley KK, et al. N Engl J Med. 2014;370:
55 HARVONI, a once-daily single-tablet regimen, Delivered High SVR12 Rates in the treatment of adults with CHC GT 1 Subjects Without Cirrhosis Subjects with Compensated Cirrhosis Treatment-Naïve 96%-99% SVR12 with 12 weeks of treatment 97% SVR12 with 8 weeks of treatment (baseline HCV RNA <6 million IU/mL) 94% SVR12 with 12 weeks of treatment Treatment-Experienced a 95% SVR12 with 12 weeks of treatment 100% SVR12 with 24 weeks of treatment Coadministration with amiodarone may result in serious symptomatic bradycardia. Use of HARVONI with amiodarone is not recommended Rifampin and St. John s wort are not recommended for use with HARVONI as they may significantly decrease ledipasvir and sofosbuvir plasma concentrations HARVONI is not recommended for use with other products containing sofosbuvir (SOVALDI) a Treatment-experienced patients who have failed treatment with Peg-IFN alfa + RBV ± HCV PI. HARVONI US full Prescribing Information. Gilead Sciences, Inc. Foster City, CA. March 2015.
56 AbbVie HCV Program Viekira Pak
57 AbbVie HCV Clinical Development Program Phase 2a Phase 3 Special Patient Populations PILOT GT1 naïve N=11 ABT-450/r + ABT RBV CO-PILOT GT1 naïve/experienced, N=50 ABT-450/r + ABT RBV Phase 2b AVIATOR GT1 naïve/experienced, N=571 ABT-450/r ABT-267 +/- ABT-333 +/- RBV NAVIGATOR GT1, 2, 3 naïve, N=60 ABT-450/r + ABT-267 +/- RBV SAPPHIRE I GT1 naïve, N= 631 ABT-450/r/ABT ABT RBV SAPPHIRE II GT1 experienced, N=394 ABT/450/r/ABT ABT RBV PEARL-II GT1b experienced, N= 179 ABT-450/r/ABT ABT-333 +/- RBV PEARL-III GT1b naïve, N=419 ABT-450/r/ABT ABT-333 +/- RBV TURQUOISE I (HIV/HCV) GT1 naïve/experienced, N= 300 ABT-450/r/ABT ABT RBV TURQUOISE II (Compensated Cirrhosis) GT1 naïve/experienced, N= 380 ABT-450/r/ABT ABT RBV M (Liver Transplant Recipients) GT1 naïve/experienced, N= 30 ABT-450/r/ABT ABT RBV Comparative Trials MALACHITE I GT1 naïve, N= 314 ABT-450/r/ABT ABT RBV Compared to TPV+ PegIFN + RBV PEARL I GT1b, 4 naïve/experienced N=320 ABT-450/r +ABT-267 +/- RBV PEARL-IV GT1a naïve, N=305 ABT-450/r/ABT ABT-333 +/- RBV MALACHITE II GT1 experienced, N= 150 ABT-450/r/ABT ABT RBV TPV + PegIFN + RBV Source: Data on File, AbbVie.

58 Viekira Pak For Genotype 1 With or Without Weight Based RIBAVIRIN Gastroenterology , DOI: ( /j.gastro ) Copyright 2014 AGA Institute


59 VIEKIRA PAK Label
60 HCV Treatment Genotype 2 and 3
61 SVR12 (%) SOF/RBV GT 2 or 3 Treatment-Naive and Experienced: VALENCE No cirrhosis Cirrhosis Overall SOF/RBV x 12w (GT2, n = 73) or 24 W (GT3, n = 250) G2 (blue); G3 (red) Zeuzem et al, N Engl J Med 2014; 370:1993
62
63 Genotype 3 Ally-3 ALLY-3 0 Weeks EOT SVR Treatment-naive 19% w/ cirrhosis N = 101 Daclatasvir + sofosbuvir 99% 90% Prior treatment 25% w/ cirrhosis N = 51 Daclatasvir + sofosbuvir 99% 86% SVR F0-F3 = 96% (105/109) SVR F4 = 63% (20/32) No SAEs related to treatment, no premature D/C due to AEs Most AEs mild: fatigue, headache, nausea, diarrhea Longer duration being examined for cirrhotics Nelson D et al, Hepatology 2015;61:1127
64 SVR12 for SOF + GS-5816 (pangenotypic NS5A) ± RBV for 12 Wk in Treatment-Naive Patients with GT 1-3 HCV 12 weeks w/o RBV GT 1, 2, 3 Noncirrhotic SOF + GS mg SOF + GS mg GT 1 GT 2 GT 3 Tran, Abst # 80, AASLD 2014







65 HCV - Beginning of the end? Or the end of the beginning? Can we engage the epidemic s base? Even more new agents on the way SVR just about 100% Regimens safer, shorter, easier IFN and liver biopsy gone Infrastructure? Cost? 65
66 Conclusion Need to diagnose more patients infected with HCV and link them into care Recently updated screening guidelines are expected to identify more cases of HCV but we need to improve our screening practices Dramatic improvement in antiviral therapies that yield % cure using well tolerated regimens Decrease rates of liver cancer, liver failure and mortality with better therapies Continued follow up needed in cirrhotic patients even with SVR including HCC surveillance
67
68 QUESTIONS?
Ari Bunim, M.D. Director of Hepatology New York Hospital Queens Assistant Professor of Clinical Medicine Weill Cornell Medical College
 Ari Bunim, M.D. Director of Hepatology New York Hospital Queens Assistant Professor of Clinical Medicine Weill Cornell Medical College New York State Law Goes into Effect January 1, 2014 Hepatitis C Virus
Ari Bunim, M.D. Director of Hepatology New York Hospital Queens Assistant Professor of Clinical Medicine Weill Cornell Medical College New York State Law Goes into Effect January 1, 2014 Hepatitis C Virus
The Dawn of a New Era: Hepatitis C
 The Dawn of a New Era: Hepatitis C Naudia L. Jonassaint Assistant Professor of Medicine and Surgery University Pittsburgh School of Medicine December 1, 2015 Objectives After presentation the learner should
The Dawn of a New Era: Hepatitis C Naudia L. Jonassaint Assistant Professor of Medicine and Surgery University Pittsburgh School of Medicine December 1, 2015 Objectives After presentation the learner should
Eliminating Hepatitis C from New Zealand
 Eliminating Hepatitis C from New Zealand Catherine Stedman Associate Professor of Medicine, University of Otago, Christchurch Gastroenterology Department, Christchurch Hospital Disclosures I have the following
Eliminating Hepatitis C from New Zealand Catherine Stedman Associate Professor of Medicine, University of Otago, Christchurch Gastroenterology Department, Christchurch Hospital Disclosures I have the following
Update on Real-World Experience With HARVONI
 Update on Real-World Experience With A RESOURCE FOR PAYERS This information is intended for payers only. The HCV-TARGET and TRIO studies were supported by Gilead Sciences, Inc. Real-world experience data
Update on Real-World Experience With A RESOURCE FOR PAYERS This information is intended for payers only. The HCV-TARGET and TRIO studies were supported by Gilead Sciences, Inc. Real-world experience data
5/12/2016. Learning Objectives. Management of Hepatitis C Virus Genotype 2 or 3 Infected Treatment-Naive or Experienced Patients
 5/12/216 Management of Hepatitis C Virus Genotype 2 or 3 Infected Treatment-Naive or Experienced Patients Alexander Monto, MD Professor of Clinical Medicine University of California San Francisco San Francisco,
5/12/216 Management of Hepatitis C Virus Genotype 2 or 3 Infected Treatment-Naive or Experienced Patients Alexander Monto, MD Professor of Clinical Medicine University of California San Francisco San Francisco,
Why make this statement?
 HCV Council 2014 10 clinical practice statements were evaluated by the Council A review of the available literature was conducted The level of support and level of evidence for the statements were discussed
HCV Council 2014 10 clinical practice statements were evaluated by the Council A review of the available literature was conducted The level of support and level of evidence for the statements were discussed
Associate Professor of Medicine University of Chicago
 Nancy Reau, MD Associate Professor of Medicine University of Chicago Management of Hepatitis C: New Drugs and New Paradigms HCV is More Lethal than HIV Infection HCV superseded HIV as a cause of death
Nancy Reau, MD Associate Professor of Medicine University of Chicago Management of Hepatitis C: New Drugs and New Paradigms HCV is More Lethal than HIV Infection HCV superseded HIV as a cause of death
Update on Real-World Experience With HARVONI
 Update on Real-World Experience With A RESOURCE FOR PAYERS MAY 217 This information is intended for payers only. The HCV-TARGET study was supported by Gilead Sciences, Inc. Real-world experience data were
Update on Real-World Experience With A RESOURCE FOR PAYERS MAY 217 This information is intended for payers only. The HCV-TARGET study was supported by Gilead Sciences, Inc. Real-world experience data were
Update in the Management of Hepatitis C: What Does the Future Hold
 Update in the Management of Hepatitis C: What Does the Future Hold Paul Y Kwo, MD, FACG Professor of Medicine Mdi Medical ldirector, Liver Transplantation tti Gastroenterology/Hepatology Division Indiana
Update in the Management of Hepatitis C: What Does the Future Hold Paul Y Kwo, MD, FACG Professor of Medicine Mdi Medical ldirector, Liver Transplantation tti Gastroenterology/Hepatology Division Indiana
Hepatitis C in Correctional Facilities: Big Problem, Bigger Opportunity. Cody A. Chastain, MD
 Hepatitis C in Correctional Facilities: Big Problem, Bigger Opportunity Cody A. Chastain, MD Disclosures Research supported by Gilead Sciences Inc.: Site investigator for HIV/HCV SWITCH Registry Study
Hepatitis C in Correctional Facilities: Big Problem, Bigger Opportunity Cody A. Chastain, MD Disclosures Research supported by Gilead Sciences Inc.: Site investigator for HIV/HCV SWITCH Registry Study
Ledipasvir-Sofosbuvir (Harvoni)
") HEPATITIS WEB STUDY HEPATITIS C ONLINE Ledipasvir-Sofosbuvir (Harvoni) Robert G. Gish MD Professor, Consultant, Stanford University Medical Center Senior Medical Director, St Josephs Hospital and Medical
HEPATITIS WEB STUDY HEPATITIS C ONLINE Ledipasvir-Sofosbuvir (Harvoni) Robert G. Gish MD Professor, Consultant, Stanford University Medical Center Senior Medical Director, St Josephs Hospital and Medical
4/30/2015. Interactive Case-Based Presentations and Audience Discussion. Debika Bhattacharya, MD, MSc. Learning Objectives
 4/3/215 Interactive Case-Based Presentations and Audience Discussion Debika Bhattacharya, MD, MSc Assistant Clinical Professor University of California Los Angeles Los Angeles, California Formatted:4-27-215
4/3/215 Interactive Case-Based Presentations and Audience Discussion Debika Bhattacharya, MD, MSc Assistant Clinical Professor University of California Los Angeles Los Angeles, California Formatted:4-27-215
Case 4: A 61-year-old man with HCV genotype 3 with cirrhosis. Ira M. Jacobson, M.D. Weill Cornell Medical College New York, New York USA
 Case 4: A 61-year-old man with HCV genotype 3 with cirrhosis Ira M. Jacobson, M.D. Weill Cornell Medical College New York, New York USA 1 Genotype 3 case 61-year-old man with HCV genotype 3 Cirrhosis on
Case 4: A 61-year-old man with HCV genotype 3 with cirrhosis Ira M. Jacobson, M.D. Weill Cornell Medical College New York, New York USA 1 Genotype 3 case 61-year-old man with HCV genotype 3 Cirrhosis on
2017 Bruce Lucas Hepatology and Liver Transplant Symposium October 13th 2017 Management of Hepatitis C in Pre- and Post-Transplant Patients
 2017 Bruce Lucas Hepatology and Liver Transplant Symposium October 13th 2017 Management of Hepatitis C in Pre- and Post-Transplant Patients Jens Rosenau, MD Associate Professor of Medicine Acting Director
2017 Bruce Lucas Hepatology and Liver Transplant Symposium October 13th 2017 Management of Hepatitis C in Pre- and Post-Transplant Patients Jens Rosenau, MD Associate Professor of Medicine Acting Director
Hepatitis C in Dr. Michael Bays D.O.
 Hepatitis C in 2015 Dr. Michael Bays D.O. HCV Virology Member of the Flavivirus family (Yellow Fever, Dengue) Hepacivirus genus Enveloped, positive, singlestranded RNA virus 9.6 Kb genome encodes a single
Hepatitis C in 2015 Dr. Michael Bays D.O. HCV Virology Member of the Flavivirus family (Yellow Fever, Dengue) Hepacivirus genus Enveloped, positive, singlestranded RNA virus 9.6 Kb genome encodes a single
Rome, February nd Riunione Annuale AISF th AISF ANNUAL MEETING
 Rome, February 20-21 nd 2014 Riunione Annuale AISF 2014 14 th AISF ANNUAL MEETING Present and future treatment strategies for patients with HCV infection: chronic hepatitis and special populations IFN
Rome, February 20-21 nd 2014 Riunione Annuale AISF 2014 14 th AISF ANNUAL MEETING Present and future treatment strategies for patients with HCV infection: chronic hepatitis and special populations IFN
6/2/2015. Interactive Case-Based Presentations and Audience Discussion
 6/2/215 Interactive Case-Based Presentations and Audience Discussion Andrew Aronsohn, MD Assistant Professor of Medicine University of Chicago Medical Center Chicago, Illinois Formatted:5-6-215 Washington,
6/2/215 Interactive Case-Based Presentations and Audience Discussion Andrew Aronsohn, MD Assistant Professor of Medicine University of Chicago Medical Center Chicago, Illinois Formatted:5-6-215 Washington,
Hepatitis C Treatment 2014
 Hepatitis C Treatment 214 Brendan M. McGuire, MD UAB Liver Center Outline Epidemiology/National History Terminology for Treatment Treatment Considerations Current Treatment Options Genotype 1 (GT 1) Genotype
Hepatitis C Treatment 214 Brendan M. McGuire, MD UAB Liver Center Outline Epidemiology/National History Terminology for Treatment Treatment Considerations Current Treatment Options Genotype 1 (GT 1) Genotype
Harvoni. Harvoni (ledipasvir & sofosbuvir) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: Harvoni Page: 1 of 7 Last Review Date: June 19, 2015 Harvoni Description Harvoni (ledipasvir &
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: Harvoni Page: 1 of 7 Last Review Date: June 19, 2015 Harvoni Description Harvoni (ledipasvir &
Treatment of Unique Populations Raymond T. Chung, MD
 Treatment of Unique Populations Raymond T. Chung, MD Director of Hepatology and Liver Center Vice Chief, Gastroenterology Kevin and Polly Maroni Research Scholar Mass General Hospital Disclosures Research
Treatment of Unique Populations Raymond T. Chung, MD Director of Hepatology and Liver Center Vice Chief, Gastroenterology Kevin and Polly Maroni Research Scholar Mass General Hospital Disclosures Research
Harvoni. Harvoni (ledipasvir & sofosbuvir) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.03.32 Subject: Harvoni Page: 1 of 7 Last Review Date: December 3, 2015 Harvoni Description Harvoni (ledipasvir
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.03.32 Subject: Harvoni Page: 1 of 7 Last Review Date: December 3, 2015 Harvoni Description Harvoni (ledipasvir
Dr. Siddharth Srivastava
 Dr. Siddharth Srivastava MD, DM (Gastroenterology) Associate Professor GIPMER, New Delhi Rashtriya Gaurav Award 2013 for work on hepatitis B and C Set up Liver clinic at GIPMER and in charge EUS laboratory.
Dr. Siddharth Srivastava MD, DM (Gastroenterology) Associate Professor GIPMER, New Delhi Rashtriya Gaurav Award 2013 for work on hepatitis B and C Set up Liver clinic at GIPMER and in charge EUS laboratory.
Harvoni. Harvoni (ledipasvir & sofosbuvir) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.01.32 Subject: Harvoni Page: 1 of 9 Last Review Date: December 2, 2016 Harvoni Description Harvoni (ledipasvir
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.01.32 Subject: Harvoni Page: 1 of 9 Last Review Date: December 2, 2016 Harvoni Description Harvoni (ledipasvir
Evolution of Therapy in HCV
 Hepatitis C: Update on New Therapies and AASLD 13 David Bernstein, MD, FACP, AGAF, FACP Professor of Medicine Hofstra North Shore-LIJ School of Medicine Evolution of Therapy in HCV 199 1999 1 13 (%) SVR
Hepatitis C: Update on New Therapies and AASLD 13 David Bernstein, MD, FACP, AGAF, FACP Professor of Medicine Hofstra North Shore-LIJ School of Medicine Evolution of Therapy in HCV 199 1999 1 13 (%) SVR
Initial Treatment of HCV G Hugo E. Vargas, MD Professor of Medicine Medical, Director Office of Clinical Research Mayo Clinic Arizona
 Initial Treatment of HCV G1 2016 Hugo E. Vargas, MD Professor of Medicine Medical, Director Office of Clinical Research Mayo Clinic Arizona Disclosure Information Disclosure Information Dr. Vargas receives
Initial Treatment of HCV G1 2016 Hugo E. Vargas, MD Professor of Medicine Medical, Director Office of Clinical Research Mayo Clinic Arizona Disclosure Information Disclosure Information Dr. Vargas receives
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Hepatitis C First Generation Agents Page 1 of 16 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: See also: Hepatitis C First Generation Agents - Through Preferred
Hepatitis C First Generation Agents Page 1 of 16 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: See also: Hepatitis C First Generation Agents - Through Preferred
Treatments of Genotype 2, 3,and 4: Now and in the future
 Treatments of Genotype 2, 3,and 4: Now and in the future THERAPY FOR THE TREATMENT OF GENOTYPE 2 1 GT 2 and GT 3 Treatment-Naïve: SOF+RBV vs PEG-IFN+RBV FISSION Study Design HCV GT 2 and GT 3 Treatment-naïve
Treatments of Genotype 2, 3,and 4: Now and in the future THERAPY FOR THE TREATMENT OF GENOTYPE 2 1 GT 2 and GT 3 Treatment-Naïve: SOF+RBV vs PEG-IFN+RBV FISSION Study Design HCV GT 2 and GT 3 Treatment-naïve
The Changing World of Hepatitis C
 The Changing World of Hepatitis C Alnoor Ramji Gastroenterology & Hepatology Clinical Associate Professor Division of Gastroenterology University Of British Columbia St. Paul s Hospital Site Disclosures
The Changing World of Hepatitis C Alnoor Ramji Gastroenterology & Hepatology Clinical Associate Professor Division of Gastroenterology University Of British Columbia St. Paul s Hospital Site Disclosures
HEPATITIS C: UPDATE AND MANAGEMENT
 HEPATITIS C: UPDATE AND MANAGEMENT José Franco, MD Professor of Medicine Associate Dean for Educational Improvement Associate Director, Kern Institute STAR Center Director José Franco, MD Disclosures I
HEPATITIS C: UPDATE AND MANAGEMENT José Franco, MD Professor of Medicine Associate Dean for Educational Improvement Associate Director, Kern Institute STAR Center Director José Franco, MD Disclosures I
Harvoni. Harvoni (ledipasvir & sofosbuvir) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.01.32 Subject: Harvoni Page: 1 of 9 Last Review Date: March 18, 2016 Harvoni Description Harvoni (ledipasvir
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.01.32 Subject: Harvoni Page: 1 of 9 Last Review Date: March 18, 2016 Harvoni Description Harvoni (ledipasvir
Patient Discussion Guide
 Patient Discussion Guide INFORMATION AND ANSWERS TO AID YOUR COUNSELING OF PATIENTS Please click to see full Prescribing Information for HARVONI, including BOXED WARNING. CHRONIC HEPATITIS C (HEP C) GENOTYPE
Patient Discussion Guide INFORMATION AND ANSWERS TO AID YOUR COUNSELING OF PATIENTS Please click to see full Prescribing Information for HARVONI, including BOXED WARNING. CHRONIC HEPATITIS C (HEP C) GENOTYPE
Update on the Treatment of HCV
 Update on the Treatment of HCV K. Rajender Reddy, MD Professor of Medicine Director of Hepatology Director, Viral Hepatitis Center University of Pennsylvania Philadelphia, USA 1 K. Rajender Reddy, MD Disclosure
Update on the Treatment of HCV K. Rajender Reddy, MD Professor of Medicine Director of Hepatology Director, Viral Hepatitis Center University of Pennsylvania Philadelphia, USA 1 K. Rajender Reddy, MD Disclosure
HCV In 2015: Maximizing SVR
 HCV In 2015: Maximizing SVR Alnoor Ramji Gastroenterology & Hepatology Clinical Associate Professor Division of Gastroenterology University Of British Columbia ramji_a@hotmail.com Disclosures (within Last
HCV In 2015: Maximizing SVR Alnoor Ramji Gastroenterology & Hepatology Clinical Associate Professor Division of Gastroenterology University Of British Columbia ramji_a@hotmail.com Disclosures (within Last
HCV Treatment Failure: What Next? Dr Ashley Brown, Imperial College Healthcare NHS Trust, London
 HCV Treatment Failure: What Next? Dr Ashley Brown, Imperial College Healthcare NHS Trust, London European HIV Hepatitis Co-infection Conference QEII Conference Centre 10 th December 2015 Dr Ashley Brown
HCV Treatment Failure: What Next? Dr Ashley Brown, Imperial College Healthcare NHS Trust, London European HIV Hepatitis Co-infection Conference QEII Conference Centre 10 th December 2015 Dr Ashley Brown
Future strategies with new DAAs
 Future strategies with new DAAs Ola Weiland professor New direct antiviral drugs Case no 1 male with genotype 2b Male with gt 2b chronic HCV Male with gt 2b relapse afer peg-ifn + RBV during 24 weeks
Future strategies with new DAAs Ola Weiland professor New direct antiviral drugs Case no 1 male with genotype 2b Male with gt 2b chronic HCV Male with gt 2b relapse afer peg-ifn + RBV during 24 weeks
Tough Cases in HIV/HCV Coinfection
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER Tough Cases in HIV/HCV Coinfection John Scott, MD, MSc Assistant Professor University of Washington Presentation prepared by: J Scott Last Updated: Jun 5, 2014
NORTHWEST AIDS EDUCATION AND TRAINING CENTER Tough Cases in HIV/HCV Coinfection John Scott, MD, MSc Assistant Professor University of Washington Presentation prepared by: J Scott Last Updated: Jun 5, 2014
Clinical Criteria for Hepatitis C (HCV) Therapy
 Therapy") Diagnosis Clinical Criteria for Hepatitis C (HCV) Therapy Must have chronic hepatitis C (HCV infection > 6 months), genotype and sub-genotype specified to determine the length of therapy; Liver biopsy
Diagnosis Clinical Criteria for Hepatitis C (HCV) Therapy Must have chronic hepatitis C (HCV infection > 6 months), genotype and sub-genotype specified to determine the length of therapy; Liver biopsy
TREATMENT OF GENOTYPE 2
 Treatment of Genotype 2, 3,and 4 David E. Bernstein, MD, FACG Advisory Committee/Board Member: AbbVie Pharmaceuticals, Gilead, Merck, Janssen Consultant: AbbVie Pharmaceuticals, Bristol-Myers Squibb, Gilead,
Treatment of Genotype 2, 3,and 4 David E. Bernstein, MD, FACG Advisory Committee/Board Member: AbbVie Pharmaceuticals, Gilead, Merck, Janssen Consultant: AbbVie Pharmaceuticals, Bristol-Myers Squibb, Gilead,
EASL 2013 Interferon Free, All Oral Regimens for Hepatitis C. Maria Buti Hospital Universitario Valle Hebron Barcelona Spain
 EASL 2013 Interferon Free, All Oral Regimens for Hepatitis C Maria Buti Hospital Universitario Valle Hebron Barcelona Spain The first Results with Oral therapy: a Protease Inhibitor and NS5A inhibitor
EASL 2013 Interferon Free, All Oral Regimens for Hepatitis C Maria Buti Hospital Universitario Valle Hebron Barcelona Spain The first Results with Oral therapy: a Protease Inhibitor and NS5A inhibitor
Hepatitis C Emerging Treatment Paradigms
 Hepatitis C Emerging Treatment Paradigms David R Nelson MD Assistant Vice President for Research Professor of Medicine Director, Clinical and Translational Science Institute University of Florida Gainesville,
Hepatitis C Emerging Treatment Paradigms David R Nelson MD Assistant Vice President for Research Professor of Medicine Director, Clinical and Translational Science Institute University of Florida Gainesville,
HCV Treatment of Genotype 1: Now and in the Future
 HCV Treatment of Genotype 1: Now and in the Future Bruce R. Bacon, MD, FACG James F. King, MD Endowed Chair in Gastroenterology Professor of Internal Medicine Co-Director of the Abdominal Transplant Program
HCV Treatment of Genotype 1: Now and in the Future Bruce R. Bacon, MD, FACG James F. King, MD Endowed Chair in Gastroenterology Professor of Internal Medicine Co-Director of the Abdominal Transplant Program
IFN-free for Genotype 1 HCV: the current landscape. Prof. Graham R Foster
 IFN-free for Genotype 1 HCV: the current landscape Prof. Graham R Foster Wonderful new drugs are coming Poordad F, et al. New Engl J Med 2014; online DOI: 10.1056/NEJMoa1402869. 2 The New Drugs Two treatment
IFN-free for Genotype 1 HCV: the current landscape Prof. Graham R Foster Wonderful new drugs are coming Poordad F, et al. New Engl J Med 2014; online DOI: 10.1056/NEJMoa1402869. 2 The New Drugs Two treatment
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Hepatitis C Second Generation Antivirals Page 1 of 30 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: See also: Hepatitis C Second Generation Antivirals Through
Hepatitis C Second Generation Antivirals Page 1 of 30 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: See also: Hepatitis C Second Generation Antivirals Through
PHARMACY PRIOR AUTHORIZATION Hepatitis C Clinical Guideline
 PHARMACY PRIOR AUTHORIZATION Hepatitis C Clinical Guideline Preferred Regimen Based on Diagnosis: Mavyret (glecaprevir/pibrentasvir ) Non-Preferred: Daklinza (daclatasvir) Epclusa (sofosbuvir/velpatasvir)
PHARMACY PRIOR AUTHORIZATION Hepatitis C Clinical Guideline Preferred Regimen Based on Diagnosis: Mavyret (glecaprevir/pibrentasvir ) Non-Preferred: Daklinza (daclatasvir) Epclusa (sofosbuvir/velpatasvir)
A treatment revolution: current management for chronic HCV
 A treatment revolution: current management for chronic HCV Ray Chung, M.D. Director of Hepatology and Liver Center Kevin and Polly Maroni Research Scholar Massachusetts General Hospital Disclosures Research
A treatment revolution: current management for chronic HCV Ray Chung, M.D. Director of Hepatology and Liver Center Kevin and Polly Maroni Research Scholar Massachusetts General Hospital Disclosures Research
HCV in 2017: New Therapies and New Opportunities. Presentation prepared by: Date prepared: OBJECTIVES
 Project ECHO HCV Collaborative HCV in 217: New Therapies and New Opportunities Paulina Deming, PharmD Assistant Director Hepatitis C Programs, ECHO Institute Associate Professor College of Pharmacy University
Project ECHO HCV Collaborative HCV in 217: New Therapies and New Opportunities Paulina Deming, PharmD Assistant Director Hepatitis C Programs, ECHO Institute Associate Professor College of Pharmacy University
Hepatitis C Elimination: Screening, Linkage and Treatment. Eric Lawitz, MD The Texas Liver Institute San Antonio, Texas
 Hepatitis C Elimination: Screening, Linkage and Treatment Eric Lawitz, MD The Texas Liver Institute San Antonio, Texas Hepatitis C: Worldwide Presence Worldwide prevalence: 130-150 million Viral hepatitis
Hepatitis C Elimination: Screening, Linkage and Treatment Eric Lawitz, MD The Texas Liver Institute San Antonio, Texas Hepatitis C: Worldwide Presence Worldwide prevalence: 130-150 million Viral hepatitis
The HCV Pipeline Ira M. Jacobson, MD, FACP, FACG, AGAF. Slide Presentation. IFN-free DAA combinations (G1)
") Slide Presentation The HCV Pipeline Vincent Astor Distinguished Professor of Medicine Chief, Division of Gastroenterology and Hepatology Medical Director, Center for the Study of Hepatitis C Weill Cornell
Slide Presentation The HCV Pipeline Vincent Astor Distinguished Professor of Medicine Chief, Division of Gastroenterology and Hepatology Medical Director, Center for the Study of Hepatitis C Weill Cornell
AASLD/IDSA HCV treatment guidelines. Arthur Y. Kim, MD Massachusetts General Hospital Harvard Medical School
 AASLD/IDSA HCV treatment guidelines Arthur Y. Kim, MD Massachusetts General Hospital Harvard Medical School Disclosure Statement for Arthur Kim Grant/research support to institution, last 12 months: Gilead
AASLD/IDSA HCV treatment guidelines Arthur Y. Kim, MD Massachusetts General Hospital Harvard Medical School Disclosure Statement for Arthur Kim Grant/research support to institution, last 12 months: Gilead
Hepatitis C Agents
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.01.41 Subject: Hepatitis C Agents Page: 1 of 20 Last Review Date: March 16, 2018 Hepatitis C Agents Description
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.01.41 Subject: Hepatitis C Agents Page: 1 of 20 Last Review Date: March 16, 2018 Hepatitis C Agents Description
Hepatitis C Agents
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.01.41 Subject: Hepatitis C Agents Page: 1 of 19 Last Review Date: December 8, 2017 Hepatitis C Agents
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.01.41 Subject: Hepatitis C Agents Page: 1 of 19 Last Review Date: December 8, 2017 Hepatitis C Agents
How to optimize treatment in G3 patients? Jérôme GOURNAY, MD Hépatologie Centre Hospitalier Universitaire de Nantes France
 How to optimize treatment in G3 patients? Jérôme GOURNAY, MD Hépatologie Centre Hospitalier Universitaire de Nantes France Paris Hepatitis Conference, January 12, 2016 Disclosures I have received funding
How to optimize treatment in G3 patients? Jérôme GOURNAY, MD Hépatologie Centre Hospitalier Universitaire de Nantes France Paris Hepatitis Conference, January 12, 2016 Disclosures I have received funding
What is the Optimized Treatment Duration? To Overtreat versus Undertreat. Nancy Reau, MD Associate Professor of Medicine University of Chicago
 What is the Optimized Treatment Duration? To Overtreat versus Undertreat Nancy Reau, MD Associate Professor of Medicine University of Chicago Learning Objectives: 1. Discuss patient populations appropriate
What is the Optimized Treatment Duration? To Overtreat versus Undertreat Nancy Reau, MD Associate Professor of Medicine University of Chicago Learning Objectives: 1. Discuss patient populations appropriate
IFN-free therapy in naïve HCV GT1 patients
 IFN-free therapy in naïve HCV GT1 patients Paris Hepatitis Conference Paris, 12th January, 2015 Pr Tarik Asselah MD, PhD; Service d Hépatologie & INSERM U773 University Paris Diderot, Hôpital Beaujon,
IFN-free therapy in naïve HCV GT1 patients Paris Hepatitis Conference Paris, 12th January, 2015 Pr Tarik Asselah MD, PhD; Service d Hépatologie & INSERM U773 University Paris Diderot, Hôpital Beaujon,
Antiviral agents in HCV
 Antiviral agents in HCV : Upcoming Therapeutic Options Su Jong Yu, M.D., Ph.D. Department of Internal Medicine, Liver Research Institute, Seoul National University College of Medicine Estimated 170 Million
Antiviral agents in HCV : Upcoming Therapeutic Options Su Jong Yu, M.D., Ph.D. Department of Internal Medicine, Liver Research Institute, Seoul National University College of Medicine Estimated 170 Million
3/25/2014. HCV: A New Era Objectives. Implementing HCV Therapy in a Primary Care Practice. Hepatitis C: A Global Health Problem.
 Implementing HCV Therapy in a Primary Care Practice Anthony Martinez, MD Associate Professor of Medicine Medical Director, Hepatology University at Buffalo HCV: A New Era Objectives Update HCV related
Implementing HCV Therapy in a Primary Care Practice Anthony Martinez, MD Associate Professor of Medicine Medical Director, Hepatology University at Buffalo HCV: A New Era Objectives Update HCV related
Hepatitis C Genotypes
 9/2/21 OBJECTIVES Project ECHO HCV Collaborative HCV in 21: New Therapies and New Opportunities Paulina Deming, PharmD Assistant Director Hepatitis C Programs, ECHO Institute Associate Professor College
9/2/21 OBJECTIVES Project ECHO HCV Collaborative HCV in 21: New Therapies and New Opportunities Paulina Deming, PharmD Assistant Director Hepatitis C Programs, ECHO Institute Associate Professor College
VII CURSO AVANCES EN INFECCIÓN VIH Y HEPATITIS VIRALES
 VII CURSO AVANCES EN INFECCIÓN VIH Y HEPATITIS VIRALES REGIMENES TERAPÊUTICOS DE LA HEPATITIS C, INTERFERÓN FREE A Coruña 2 Febrero 2013 Rui Sarmento e Castro Centro Hospitalar do Porto HJU ECS Universidade
VII CURSO AVANCES EN INFECCIÓN VIH Y HEPATITIS VIRALES REGIMENES TERAPÊUTICOS DE LA HEPATITIS C, INTERFERÓN FREE A Coruña 2 Febrero 2013 Rui Sarmento e Castro Centro Hospitalar do Porto HJU ECS Universidade
Selecting HCV Treatment
 Selecting HCV Treatment Caveats Focus on treatment selection for genotypes 1, 2, and 3. Majority of US population infected with GT 1, 2, or 3 GT 4 treatment closely reflects GT 1 treatment GT 5 and 6 are
Selecting HCV Treatment Caveats Focus on treatment selection for genotypes 1, 2, and 3. Majority of US population infected with GT 1, 2, or 3 GT 4 treatment closely reflects GT 1 treatment GT 5 and 6 are
Hepatitis C Update: What s New in 2017
 Hepatitis C Update: What s New in 2017 Cody A. Chastain, MD Assistant Professor of Medicine Viral Hepatitis Program Division of Infectious Diseases Vanderbilt University Medical Center Cody.a.Chastain@Vanderbilt.edu
Hepatitis C Update: What s New in 2017 Cody A. Chastain, MD Assistant Professor of Medicine Viral Hepatitis Program Division of Infectious Diseases Vanderbilt University Medical Center Cody.a.Chastain@Vanderbilt.edu
Drug Class Monograph
 Drug Class Monograph Class: Chronic Hepatitis C Drugs(s): Daclatasvir (Daklinza), Dasabuvir/ombitasivir/paritaprevir/ritonavir (Viekira Pak), Elbasvir/grazoprevir (Zepatier), Peginterferon alfa-2a (Pegasys),
Drug Class Monograph Class: Chronic Hepatitis C Drugs(s): Daclatasvir (Daklinza), Dasabuvir/ombitasivir/paritaprevir/ritonavir (Viekira Pak), Elbasvir/grazoprevir (Zepatier), Peginterferon alfa-2a (Pegasys),
Treatment of hepatitis C today and tomorrow Antonio Craxì GI & Liver Unit, Di.Bi.M.I.S., University of Palermo, Italy
 Treatment of hepatitis C today and tomorrow Antonio Craxì GI & Liver Unit, Di.Bi.M.I.S., University of Palermo, Italy antonio.craxi@unipa.it Ad Board and grants: Abbvie, Achillion, BristolMyers Squibb,
Treatment of hepatitis C today and tomorrow Antonio Craxì GI & Liver Unit, Di.Bi.M.I.S., University of Palermo, Italy antonio.craxi@unipa.it Ad Board and grants: Abbvie, Achillion, BristolMyers Squibb,
Hepatitis C in Special Populations
 Hepatitis C in Special Populations David E. Bernstein, MD, FACG Vice Chairman of Medicine for Clinical Trials Chief, Division of Hepatology and Sandra Atlas Bass Center for Liver Diseases Northwell Health
Hepatitis C in Special Populations David E. Bernstein, MD, FACG Vice Chairman of Medicine for Clinical Trials Chief, Division of Hepatology and Sandra Atlas Bass Center for Liver Diseases Northwell Health
CURRENT TREATMENTS. Mitchell L Shiffman, MD Director Liver Institute of Virginia. Richmond and Newport News, VA, USA
 CURRENT TREATMENTS FOR HCV Mitchell L Shiffman, MD Director Liver Institute of Virginia Bon Secours Health System Richmond and Newport News, VA, USA Liver Institute of Virginia Education, Research and
CURRENT TREATMENTS FOR HCV Mitchell L Shiffman, MD Director Liver Institute of Virginia Bon Secours Health System Richmond and Newport News, VA, USA Liver Institute of Virginia Education, Research and
Drug Class Prior Authorization Criteria Hepatitis C
 Drug Class Prior Authorization Criteria Hepatitis C Line of Business: Medicaid P & T Approval Date: Interim Criteria Pending P&T Approval Effective Date: August 16, 2018 This drug class prior authorization
Drug Class Prior Authorization Criteria Hepatitis C Line of Business: Medicaid P & T Approval Date: Interim Criteria Pending P&T Approval Effective Date: August 16, 2018 This drug class prior authorization
Updates in the Treatment of Hepatitis C
 Disclosures Updates in the Treatment of Hepatitis C Arslan Kahloon M.D Assistant Professor of Medicine University of Tennessee, Chattanooga I have no conflicts of interest or financial sponsorship to disclose
Disclosures Updates in the Treatment of Hepatitis C Arslan Kahloon M.D Assistant Professor of Medicine University of Tennessee, Chattanooga I have no conflicts of interest or financial sponsorship to disclose
Pivotal New England Journal of Medicine papers 2014 Phase 3 Trial data
 4 th HCV Therapy Advances Meeting Paris, December 12-13, 14 Pivotal New England Journal of Medicine papers 14 Phase 3 Trial data Stefan Zeuzem, MD University of Frankfurt Germany Disclosures Consultancies:
4 th HCV Therapy Advances Meeting Paris, December 12-13, 14 Pivotal New England Journal of Medicine papers 14 Phase 3 Trial data Stefan Zeuzem, MD University of Frankfurt Germany Disclosures Consultancies:
Program Disclosure. A maximum of 1.5 contact hours may be earned for successful completion of this activity.
 Program Disclosure This activity has been planned and implemented in accordance with the accreditation requirements and policies of the Accreditation Council for Continuing Medical Education (ACCME) through
Program Disclosure This activity has been planned and implemented in accordance with the accreditation requirements and policies of the Accreditation Council for Continuing Medical Education (ACCME) through
10/21/2016. Susanna Naggie, MD, MHS Associate Professor of Medicine Duke University Durham, North Carolina. Learning Objectives
 A Crash Course on the AASLD/IDSA Hepatitis C Virus Infection Treatment Guidelines: What s New Susanna Naggie, MD, MHS Associate Professor of Medicine Duke University Durham, North Carolina FORMATTED: 1/3/16
A Crash Course on the AASLD/IDSA Hepatitis C Virus Infection Treatment Guidelines: What s New Susanna Naggie, MD, MHS Associate Professor of Medicine Duke University Durham, North Carolina FORMATTED: 1/3/16
Hepatitis C Infection: Updated Information for Front Line Workers in Primary Care Settings MAMTA K. JAIN, MD, MPH 2/14/18
 Hepatitis C Infection: Updated Information for Front Line Workers in Primary Care Settings MAMTA K. JAIN, MD, MPH 2/14/18 Overview Hepatitis C Virus Prevalence Effects of Hepatitis C Prevention Diagnosis
Hepatitis C Infection: Updated Information for Front Line Workers in Primary Care Settings MAMTA K. JAIN, MD, MPH 2/14/18 Overview Hepatitis C Virus Prevalence Effects of Hepatitis C Prevention Diagnosis
Introduction. The ELECTRON Trial
 63rd AASLD November 9-13, 12 Boston, Massachusetts Faculty Douglas T. Dieterich, MD Professor of Medicine and Director of CME Department of Medicine Director of Outpatient Hepatology Division of Liver
63rd AASLD November 9-13, 12 Boston, Massachusetts Faculty Douglas T. Dieterich, MD Professor of Medicine and Director of CME Department of Medicine Director of Outpatient Hepatology Division of Liver
Hepatitis C Update: Screening, Diagnosis, and Treatment
 Mountain West AIDS Education and Training Center Hepatitis C Update: Screening, Diagnosis, and Treatment Brian R. Wood, MD (bwood2@uw.edu) Assistant Professor of Medicine, University of Washington Medical
Mountain West AIDS Education and Training Center Hepatitis C Update: Screening, Diagnosis, and Treatment Brian R. Wood, MD (bwood2@uw.edu) Assistant Professor of Medicine, University of Washington Medical
Drug Class Monograph
 Drug Class Monograph Class: Chronic Hepatitis C Drugs(s): Daclatasvir (Daklinza), Dasabuvir/ombitasivir/paritaprevir/ritonavir (Viekira XR), Elbasvir/grazoprevir (Zepatier), Peginterferon alfa-2a (Pegasys),
Drug Class Monograph Class: Chronic Hepatitis C Drugs(s): Daclatasvir (Daklinza), Dasabuvir/ombitasivir/paritaprevir/ritonavir (Viekira XR), Elbasvir/grazoprevir (Zepatier), Peginterferon alfa-2a (Pegasys),
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Hepatitis C Second Generation Antivirals Page 1 of 32 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: See also: Hepatitis C Second Generation Antivirals Through
Hepatitis C Second Generation Antivirals Page 1 of 32 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: See also: Hepatitis C Second Generation Antivirals Through
Harvoni: solution to HCV
 Harvoni: solution to HCV PRESENTATION BY: PATRICK HO, USC PHARM D. CANDIDATE OF 2017 MENTOR: DR. CRAIG STERN, PHARMD, MBA, RPH, FASCP, FASHP, FICA, FLMI, FAMCP Hepatitis C (HCV) Inflammation of the liver,
Harvoni: solution to HCV PRESENTATION BY: PATRICK HO, USC PHARM D. CANDIDATE OF 2017 MENTOR: DR. CRAIG STERN, PHARMD, MBA, RPH, FASCP, FASHP, FICA, FLMI, FAMCP Hepatitis C (HCV) Inflammation of the liver,
ICVH 2016 Oral Presentation: 28
 Ledipasvir/Sofosbuvir Is Safe and Effective for the Treatment of Patients with Genotype 1 Chronic HCV Infection in Both HCV Mono- and HIV/HCV Coinfected Patients A Luetkemeyer 1, C Cooper 2, P Kwo 3, K
Ledipasvir/Sofosbuvir Is Safe and Effective for the Treatment of Patients with Genotype 1 Chronic HCV Infection in Both HCV Mono- and HIV/HCV Coinfected Patients A Luetkemeyer 1, C Cooper 2, P Kwo 3, K
Feeling right at home
 Feeling right at home Getting to Cure From Cure to Eradication Jordan J. Feld MD MPH Toronto Centre for Liver Disease Sandra Rotman Centre for Global Health University of Toronto SVR Dramatic Improvements
Feeling right at home Getting to Cure From Cure to Eradication Jordan J. Feld MD MPH Toronto Centre for Liver Disease Sandra Rotman Centre for Global Health University of Toronto SVR Dramatic Improvements
New developments in HCV research and their implications for front-line practice
 New developments in HCV research and their implications for front-line practice Dr. Curtis Cooper Associate Professor, University of Ottawa Director, Ottawa Hospital Viral Hepatitis Program June 17, 2013
New developments in HCV research and their implications for front-line practice Dr. Curtis Cooper Associate Professor, University of Ottawa Director, Ottawa Hospital Viral Hepatitis Program June 17, 2013
Hepatitis C Prior Authorization Policy
 Hepatitis C Prior Authorization Policy Line of Business: Medi-Cal P&T Approval Date: November 15, 2017 Effective Date: January 1, 2018 This policy has been developed through review of medical literature,
Hepatitis C Prior Authorization Policy Line of Business: Medi-Cal P&T Approval Date: November 15, 2017 Effective Date: January 1, 2018 This policy has been developed through review of medical literature,
Chronic Hepatitis C Drug Class Monograph
 Chronic Hepatitis C Drug Class Monograph Line of Business: Medi-Cal Effective Date: July 10, 2017 (Interim Guidelines; Final Review and Approval by the P&T Subcommittee Pending) This policy has been developed
Chronic Hepatitis C Drug Class Monograph Line of Business: Medi-Cal Effective Date: July 10, 2017 (Interim Guidelines; Final Review and Approval by the P&T Subcommittee Pending) This policy has been developed
Can we afford to Cure all HIV-HCV Co-infected Patients of HCV?
 Can we afford to Cure all HIV-HCV Co-infected Patients of HCV? Michael S. Saag, MD Professor of Medicine University of Alabama at Birmingham Birmingham, Alabama FINAL AU EDITED: 09-17-14 Disclosure Dr
Can we afford to Cure all HIV-HCV Co-infected Patients of HCV? Michael S. Saag, MD Professor of Medicine University of Alabama at Birmingham Birmingham, Alabama FINAL AU EDITED: 09-17-14 Disclosure Dr
Chronic Hepatitis C Drug Class Prior Authorization Protocol
 Line of Business: Medi-Cal Effective Date: August 16, 2017 Revision Date: August 16, 2017 Chronic Hepatitis C Drug Class Prior Authorization Protocol This policy has been developed through review of medical
Line of Business: Medi-Cal Effective Date: August 16, 2017 Revision Date: August 16, 2017 Chronic Hepatitis C Drug Class Prior Authorization Protocol This policy has been developed through review of medical
Antiviral treatment in HCV cirrhotic patients on waiting list
 Antiviral treatment in HCV cirrhotic patients on waiting list Krzysztof Tomasiewicz Department of Hepatology and Infectious Diseases Medical University of Lublin, Poland Disclosures Consultancy/Advisory
Antiviral treatment in HCV cirrhotic patients on waiting list Krzysztof Tomasiewicz Department of Hepatology and Infectious Diseases Medical University of Lublin, Poland Disclosures Consultancy/Advisory
JOHNS HOPKINS HEALTHCARE
 JOHNS HOPKINS HEALTHCARE Subject: Clinical Criteria for Hepatitis C (HCV) Therapy Department: Pharmacy Lines of Business: PPMCO Policy Number: MEDS92 Effective Date: 04/15/2015 Revision Date: 08/15/2015
JOHNS HOPKINS HEALTHCARE Subject: Clinical Criteria for Hepatitis C (HCV) Therapy Department: Pharmacy Lines of Business: PPMCO Policy Number: MEDS92 Effective Date: 04/15/2015 Revision Date: 08/15/2015
HCV: Racial Disparities. Charles D. Howell, M.D., A.G.A.F Professor of Medicine University of Maryland School of Medicine Baltimore, MD
 HCV: Racial Disparities Charles D. Howell, M.D., A.G.A.F Professor of Medicine University of Maryland School of Medicine Baltimore, MD Charles Howell Disclosures Research Grants Boehringer Ingelheim, Inc.
HCV: Racial Disparities Charles D. Howell, M.D., A.G.A.F Professor of Medicine University of Maryland School of Medicine Baltimore, MD Charles Howell Disclosures Research Grants Boehringer Ingelheim, Inc.
Direct Acting Antivirals for the Treatment of Hepatitis C Infection
 Hepatitis C Core Curriculum, Module 2 Direct Acting Antivirals for the Treatment of Hepatitis C Infection Jason J. Schafer, PharmD, MPH, BCPS, AAHIVP Objectives Discuss the evolution of hepatitis C treatment
Hepatitis C Core Curriculum, Module 2 Direct Acting Antivirals for the Treatment of Hepatitis C Infection Jason J. Schafer, PharmD, MPH, BCPS, AAHIVP Objectives Discuss the evolution of hepatitis C treatment
HEPATITIS WEB STUDY. Treatment of Hepatitis C following Liver Transplantation
 HEPATITIS WEB STUDY Treatment of Hepatitis C following Liver Transplantation Terry D. Box, MD Associate Professor of Medicine Division of Gastroenterology/Hepatology University of Utah Health Sciences
HEPATITIS WEB STUDY Treatment of Hepatitis C following Liver Transplantation Terry D. Box, MD Associate Professor of Medicine Division of Gastroenterology/Hepatology University of Utah Health Sciences
Primary Care Approach to Diagnosis and Management of Chronic Hepatitis C Brian Viviano, D.O.
 Primary Care Approach to Diagnosis and Management of Chronic Hepatitis C Brian Viviano, D.O. Objectives Epidemiology of chronic hepatitis C CDC guidelines on screening or hepatitis C Diagnosing hepatitis
Primary Care Approach to Diagnosis and Management of Chronic Hepatitis C Brian Viviano, D.O. Objectives Epidemiology of chronic hepatitis C CDC guidelines on screening or hepatitis C Diagnosing hepatitis
Clinical Сase A previously relapse to PEG IFN + RBV in HCV G3a patient. Konstantin Zhdanov
 Clinical Сase A previously relapse to PEG IFN + RBV in HCV G3a patient Konstantin Zhdanov Genotype 3 in Europe Canada Norway Germany Sweden Czech Republic Poland Approximately 1/3 of HCV-infected patients
Clinical Сase A previously relapse to PEG IFN + RBV in HCV G3a patient Konstantin Zhdanov Genotype 3 in Europe Canada Norway Germany Sweden Czech Republic Poland Approximately 1/3 of HCV-infected patients
Hepatitis C Genotype 1 (GT 1) Patients in the United States (US)
 Patients in the United States (US)") Hepatitis C Genotype 1 (GT 1) Patients in the United States (US) INDICATION is indicated with or without ribavirin for the treatment of patients with chronic hepatitis C virus (HCV) genotype 1, 4, 5, or
Hepatitis C Genotype 1 (GT 1) Patients in the United States (US) INDICATION is indicated with or without ribavirin for the treatment of patients with chronic hepatitis C virus (HCV) genotype 1, 4, 5, or
1/16/2019. Goals of HCV Therapy. Objectives. Treating Hepatitis C and HIV Co Infection. Cure Defined as sustained virologic response (SVR)
") HCV ECHO WESTERN STATES HCV ECHO WESTERN STATES Treating Hepatitis C and HIV Co Infection Paulina Deming, Pharm D Associate Professor, College of Pharmacy Assistant Director, Viral Hepatitis Programs,
HCV ECHO WESTERN STATES HCV ECHO WESTERN STATES Treating Hepatitis C and HIV Co Infection Paulina Deming, Pharm D Associate Professor, College of Pharmacy Assistant Director, Viral Hepatitis Programs,
Management of Chronic HCV 2017 and Beyond
 Management of Chronic HCV 2017 and Beyond Blaire E Burman, MD Virginia Mason Gastroenterology & Hepatology Relevant Disclosures No financial disclosures to report Leaning Objectives Burden of HCV Prevalence
Management of Chronic HCV 2017 and Beyond Blaire E Burman, MD Virginia Mason Gastroenterology & Hepatology Relevant Disclosures No financial disclosures to report Leaning Objectives Burden of HCV Prevalence
HCV Management in Decompensated Cirrhosis: Current Therapies
 Treatment of Patients with Decompensated Cirrhosis and Liver Transplant Recipients Paul Y. Kwo, MD, FACG Professor of Medicine Gastroenterology/Hepatology Division Stanford University email pkwo@stanford.edu
Treatment of Patients with Decompensated Cirrhosis and Liver Transplant Recipients Paul Y. Kwo, MD, FACG Professor of Medicine Gastroenterology/Hepatology Division Stanford University email pkwo@stanford.edu
New Hepatitis C Antivirals
 New Hepatitis C Antivirals Kris Stewart, BSP, MD, FRCPC Drug Therapy Conference College of Medicine, University of Saskatchewan September 23, 2016 Disclosures I have received research and program support
New Hepatitis C Antivirals Kris Stewart, BSP, MD, FRCPC Drug Therapy Conference College of Medicine, University of Saskatchewan September 23, 2016 Disclosures I have received research and program support
Drug Class Prior Authorization Criteria Hepatitis C
 Drug Class Prior Authorization Criteria Hepatitis C Line of Business: Medicaid P & T Approval Date: Interim (pending P&T approval) Effective Date: July 1, 2018 This policy has been developed through review
Drug Class Prior Authorization Criteria Hepatitis C Line of Business: Medicaid P & T Approval Date: Interim (pending P&T approval) Effective Date: July 1, 2018 This policy has been developed through review
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Hepatitis C First Generation Agents Page 1 of 18 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: See also: Hepatitis C First Generation Agents - Through Preferred
Hepatitis C First Generation Agents Page 1 of 18 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: See also: Hepatitis C First Generation Agents - Through Preferred
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: (Harvoni) Reference Number: CP.CPA.175 Effective Date: 11.01.16 Last Review Date: 08.18 Line of Business: Commercial Revision Log See Important Reminder at the end of this policy for important
Clinical Policy: (Harvoni) Reference Number: CP.CPA.175 Effective Date: 11.01.16 Last Review Date: 08.18 Line of Business: Commercial Revision Log See Important Reminder at the end of this policy for important
Experience with pre-transplant antiviral treatment: PEG/RBV and DAA. Xavier Forns, MD Liver Unit Hospital Clínic IDIBAPS and CIBREHD Barcelona
 Experience with pre-transplant antiviral treatment: PEG/RBV and DAA Xavier Forns, MD Liver Unit Hospital Clínic IDIBAPS and CIBREHD Barcelona Interferon-free regimens G1b nulls Asunaprevir (PI) + Daclatasvir
Experience with pre-transplant antiviral treatment: PEG/RBV and DAA Xavier Forns, MD Liver Unit Hospital Clínic IDIBAPS and CIBREHD Barcelona Interferon-free regimens G1b nulls Asunaprevir (PI) + Daclatasvir
Hepatitis C: The New World of Treatment
 Hepatitis C: The New World of Treatment Aban 1395, NIOC Hospital Shahin Merat, M.D. Professor of Medicine Digestive Disease Research Institute Tehran University of Medical Sciences 1 Drugs NS5B polymerase
Hepatitis C: The New World of Treatment Aban 1395, NIOC Hospital Shahin Merat, M.D. Professor of Medicine Digestive Disease Research Institute Tehran University of Medical Sciences 1 Drugs NS5B polymerase
Program Disclosure. Provider is approved by the California Board of Registered Nursing, Provider #13664, for 1.5 contact hours.
 Program Disclosure This activity has been planned and implemented in accordance with the Essential Areas and policies of the Accreditation Council for Continuing Medical Education (ACCME) through the joint-sponsorship
Program Disclosure This activity has been planned and implemented in accordance with the Essential Areas and policies of the Accreditation Council for Continuing Medical Education (ACCME) through the joint-sponsorship