CIWA-AR CLINICAL INSTITUTE WITHDRAWAL ASSESSMENT FOR ALCOHOL SCALE
|
|
|
- Kellie Warren
- 5 years ago
- Views:
Transcription
1 CIWA-AR CLINICAL INSTITUTE WITHDRAWAL ASSESSMENT FOR ALCOHOL SCALE SAM G CAMPBELL MB BCH, FCFP(EM), DIP PEC(SA), FCCHL, FRCP(EDIN) PROFESSOR OF EMERGENCY MEDICINE DALHOUSIE UNIVERSITY, HALIFAX, NOVA SCOTIA.

2 OBJECTIVES Discuss the pathophysiology of alcohol withdrawal syndrome (AWS) Develop an approach to treating AWS, guided by the revised CIWA scale Review challenges of AWS management and the limitations of the CIWA Scale
3 CFPC CoI Templates: Slide 1 used in Faculty presentation only. FACULTY/PRESENTER DISCLOSURE Faculty: Sam Campbell Relationships with financial sponsors: Grants/Research Support: Penthrox Speakers Bureau/Honoraria: Nil Consulting Fees: Nil Patents: Nil Other: Employee of PraxES Emergency Specialists Inc
4 CFPC CoI Templates: Slide 2 DISCLOSURE OF FINANCIAL SUPPORT Potential for conflict(s) of interest: None

5 CFPC CoI Templates: Slide 3 MITIGATING POTENTIAL BIAS (NON-FINANCIAL DISCLOSURE) Alcoholism is far, far bigger than withdrawal I m only talking about withdrawal I have always thought I knew more about how to do this than I discovered The guidelines and cutoffs vary as do the drug recommendations I tried to make sense in the NS context I am going to suggest the impossible But it gives us direction In our context the impossible is frequently considered standard of care!
6 CASES: 78 year old man recovering from an urgent hip hemi-arthroplasty develops tachycardia, hypertension, fever, and agitation. 42 year old homeless man presents after a witnessed grand mal seizure tremulous and tachycardic 52 yr old woman dragged in by her daughter who says you have to fix her drinking Vitals are normal, ETOH yr old man presents from cells, where he was unable to stand. He has had fecal and urinary incontinence and manages only to tell you to -off. 27 year old falls off his bicycle whilst hammered. His (inebriated) friends joke that this is his normal Friday night state
7 CASES 44 year old man presents as Suicidal alcoholic x 20 yrs, lost job, family, house, several DUI s 55 yr old lady Alcoholic for years husband has cut her off, she is shaky and anxious. Asking for ativan. 60 year old in a rollover MVC, obviously intoxicated, rib fractures, but stable. Several trips to detox in past few years

8 TERMINOLOGY Withdrawal Characteristic group of signs & symptoms that typically develop after rapid, marked decrease or discontinuation of a substance of dependence, which may or may not be clinically significantly or life threatening. 8
 Increased hand tremor Insomnia Nausea or vomiting Transient visual, tactile, or auditory hallucinations Psychomotor agitation Anxiety Grand mal")
9 ETOH WITHDRAWAL: DIAGNOSTIC CRITERIA Cessation of (or reduction in) EtOH use that has been heavy & prolonged Two (or more) of the following, developing within several hours to a few days later: Autonomic hyperactivity (sweating, tachycardia) Increased hand tremor Insomnia Nausea or vomiting Transient visual, tactile, or auditory hallucinations Psychomotor agitation Anxiety Grand mal seizures Symptoms cause clinically significant distress or impairment in social, occupational, or other important areas of functioning Symptoms are not due to a general medical condition or another mental disorder
 Major excitatory neurotransmitter Chronic EtOH exposure inhibits NMDA receptors increase in NMDA receptor concentration neuron hyperexcitability Am Fam Physician.")
10 PATHOPHYSIOLOGY OF ETOH WITHDRAWAL 10 GABA (Gama amino butyric acid) Major inhibitory neurotransmitter Chronic EtOH exposure enhances GABA effects decrease in GABA A alpha 1 receptor activity NMDA (N-methyl-D-aspartate) Major excitatory neurotransmitter Chronic EtOH exposure inhibits NMDA receptors increase in NMDA receptor concentration neuron hyperexcitability Am Fam Physician Mar 15;69(6):

11 - GABA receptor is the brake - NMDA receptor is the accelerator 11 EtOH Withdrawal is the brain accelerating without brakes...
12 FACTORS AFFECTING COURSE OF WITHDRAWAL 12 Severity & duration of withdrawal depend on: 1. Nature of substance 2. Half-life & duration of action 3. Length of time substance used 4. Amount used 5. Use of other substances 6. Presence of other medical & psychiatric conditions 7. Individual biopsychosocial variables
13 RISK OF WITHDRAWAL The severity of withdrawal is partially dose-related. Alcohol withdrawal requiring treatment is rare in people consuming fewer than six drinks per day, (except in older adults) Withdrawal severity varies widely. Some people who drink very heavily experience few or no symptoms of withdrawal, whereas others experience severe symptoms.
14 RISK OF WITHDRAWAL Elderly patients: may develop significant withdrawal symptoms even if they were consuming < 6 drinks per day have a more complicated withdrawal course because they often have concurrent health problems and may be frail Past withdrawal predicts future episodes. Patients with a history of delirium tremens and withdrawal seizures are at high risk of reoccurrence if they return to drinking and stop again Kindling phenomenon

15 COURSE OF ETOH WITHDRAWAL Symptom Onset after last drink Tremulousness Hallucinations Seizures Delirium Tremens 6 36 hours hours 6 48 hours hours Symptoms peak at two to three days, although they can last up to seven days.
16 SYMPTOMS AND SIGNS The most reliable sign of alcohol withdrawal is postural and intention tremor Ask patients to hold their hands out in front of them, to reach for an object or to walk across the room. The tremor may not be visible when the patient is at rest. Other signs include diaphoresis, tachycardia and hypertension. Anxiety, nausea and headache are common symptoms.
17 DISTINGUISHING BETWEEN WITHDRAWAL AND ANXIETY Withdrawal should be suspected if: the patient reports having > 6 drinks per day (except older adults) drinking begins at a predictable time in the morning or afternoon symptoms include sweating or tremor symptoms are quickly relieved by alcohol Hx of withdrawal in the past, or withdrawal seizures. A tongue tremor is difficult to feign and is a more sensitive sign of alcoholic tremor than hand tremor

18 HALLUCINATIONS Occurs within hours of last drink 3 10% of cases develop hallucinations Duration is variable Usually visual (e.g., pink elephants) Occasionally auditory, tactile, or olfactory EtOH Hallucinosis: reality testing 20 is intact
19 SEIZURES Occur within 6 48 hours of last drink 11-35% of patients develop seizures in hospital setting Risk correlates with duration EtOH use Manifests as grand mal tonic-clonic activity Always consider other causes 40% are single episodes 30% of untreated patients go on to develop delirium tremens 21
 Risk 51 100 101 200 201 300 3x 8x 20x 10 gm = 1 beer 22 Stephen KC. Alcohol Consumption & Withdrawal in New-Onset Seizures.")
20 SEIZURES EtOH is an independent, dose related risk factor for seizures Retrospective study of 308 patients in a city hospital with new onset of seizures during EtOH withdrawal EtOH (gm/day) Risk x 8x 20x 10 gm = 1 beer 22 Stephen KC. Alcohol Consumption & Withdrawal in New-Onset Seizures. NEJM, 1988

21 DELIRIUM TREMENS Begins 3 to 5 days after last drink Occurs in less than 5% of withdrawal patients Not always predictable or preventable Usually lasts 2-3 days, but can last up to 30 days Delirium can occur with/without tremens Risk factors Acute concurrent medical illness History of seizures or delirium tremens Heavier & longer EtOH history Age > 60 Elevated BAL on admission (greater than 300 mg/dl) 23
22 DIAGNOSING DELIRIUM TREMENS The most severe form of alcohol withdrawal manifested by altered mental status and autonomic hyperactivity which can progress to cardiovascular collapse Signs and Symptoms: (in addition to those of basic alcohol withdrawal) Hypertension Tachycardia Hyperthermia Severe Agitation Diaphoresis

23 WITHDRAWAL SYMPTOMS TIMELINE


24 LABORATORY FINDINGS IN PATIENTS WITH ALCOHOL WITHDRAWAL In mild cases of withdrawal, blood work is rarely helpful and is unlikely to change management. However, in patients with severe alcohol withdrawal, especially patients with delirium tremens, blood work can help rule out other causes of delirium, screen for alcoholic ketoacidosis and electrolyte abnormalities. Ethanol Level is rarely helpful and is unlikely to change management Except if diagnosis is uncertain Consider a baseline ECG in patients who require admission for alcohol withdrawal. A urine drug screen rarely changes management
25 TREATMENT OBJECTIVES Reduce symptoms Prevent seizures Prevent delirium tremens Prevent &/or manage medical complications & co-morbidities Prevent recurrence
26 TREATMENT OBJECTIVES 1. provide a safe withdrawal from the drug(s) of dependence and enable the patient to become drug-free 2. provide a withdrawal that is humane and thus protects the patient s dignity 3. prepare the patient for ongoing treatment of his or her dependence on alcohol or other drugs The American Society of Addiction Medicine

27 SUPPORTIVE CARE Ensure ABCs!... Secure patient in safe environment Be nice! Provide IV hydration as needed Correct electrolyte imbalances Provide nutritional support No-one grows up wanting to be an alcoholic!
28 SUPPORTIVE CARE Nursing care: reassurance, orientation, empathetic communication Monitor for signs & symptoms of withdrawal Consider psych referral to Psychiatry if suicidal/ homicidal ideation &/or psychotic symptoms

29 ROLE OF PHARMACOTHERAPY Stabilize psychological or physiological withdrawal symptoms Control autonomic overdrive Manage medical emergencies Remediate non-life threatening, relapse-triggering symptoms Stabilize co-morbid conditions
 Short- vs.")
30 BENZODIAZEPINES Ideal for management of EtOH withdrawal symptoms Cross-tolerance with EtOH Fairly wide therapeutic window (compared to barbiturates) Short- vs. long-acting Liver disease may limit use of long acting benzos

31 BENZODIAZEPINES LONG-ACTING Diazepam or Chlordiazepoxide Advantages withdrawal is smoother, rebound withdrawal symptoms are less likely more effective in preventing complications such as seizures Disadvantages Not reliable IM Excreted hepatically
32 BENZODIAZEPINES SHORT-ACTING Lorazepam Advantages PO, IM or IV no significant active metabolites They are metabolized & excreted principally through kidneys (& do not jeopardize already-damaged liver) Disadvantages They need to be administered more frequently Have the potential for withdrawal syndrome themselves
33 Symptom-triggered regimen Administer the CIWA-Ar every hour to assess the patient s need for medication. Administer one of the following medications every hour when the CIWA-Ar score > 8 to 10 points: Chlordiazepoxide (Librium), 50 to 100 mg Diazepam (Valium), 10 to 20 mg Lorazepam (Ativan), 2 to 4 mg
34

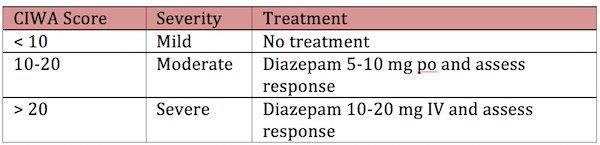
35 SEVERE WITHDRAWAL first dose of diazepam 10mg IV, and repeat in 5 minutes PRN. Then double the dose to 20 mg and continue with 20mg, 30mg, 30mg, 40mg, 40mg every 5 minutes as needed.

36 OTHER MEDICATIONS Beta-blockers & Clonidine Reduce autonomic hyper-arousal (tachycardia, hypertension) May reduce total dosage of benzos & result in less sedation Do not reduce risk of seizures or delirium tremens

37 OTHER MEDICATIONS Carbamazepine Reduces risk of seizure activity Does little for autonomic hyper-arousal Requires monitoring of CBC, LFTs, & serum levels Risks include liver & bone marrow toxicity

38 OTHER MEDICATIONS Antipsychotic agents Not a strong role in AWS Can be used for management of agitation, aggression, & psychotic symptoms Can also lower seizure threshold and prolong the QT
39 THIAMINE & MULTIVITAMINS 30-80% of patients are deficient Thiamine does not reduce risk of seizures or delirium tremens Thiamine does reduce risk of Wernicke s encephalopathy Give thiamine mg IV (before glucose) Add MV 1 tab po qd
40 CLINICAL INSTITUTE WITHDRAWAL ASSESSMENT FOR ALCOHOL, CIWA-AR (REVISED VERSION), 10 item scale, each item scored independently Summation of the scores yields an aggregate value that correlates to the severity of alcohol withdrawal, to guide management The maximum score is 67 Mild withdrawal <15 (start Rx at 8-10) Moderate :16 20 Severe >20.
41 CLINICAL INSTITUTE WITHDRAWAL ASSESSMENT FOR ALCOHOL, CIWA-AR (REVISED VERSION), Can be administered in under 2 minutes Care guided by the CIWA has been shown to: Have high inter-rater reliability providing an efficient and objective means of assessing alcohol withdrawal Decrease treatment duration and total use of benzodiazepines. Decrease over-sedation and under-treatment
42 USING THE CIWA-AR WITHDRAWAL SCALE A score of 8-10 or more indicates the need for benzodiazepines Benzos stopped when the patient scores less than 8 on two consecutive readings at least one hour apart.
43 CLINICAL INSTITUTE WITHDRAWAL ASSESSMENT FOR ALCOHOL SCALE Nausea & vomiting Tremor Sweating Anxiety Agitation Tactile disturbances Auditory disturbances Visual disturbances Headache or head fullness Disorientation

44 CIWA -AR IS NOTA DIAGNOSTIC TEST FOR WITHDRAWAL. The CIWA-Ar is only intended to be used for assessment of withdrawal severity once the diagnosis has been made.

45 ROUTINE VS. SYMPTOM-DRIVEN PROTOCOLS Study: 100 VA patients in EtOH withdrawal Outcomes Treatment time = 68 hrs vs. 9 hrs. Total dose Chlordiazepoxide = 425 mg vs. 100 mg Advantages Reduced hospital length of stay Reduced total dosage of medication Reduced cost of care Less sedation
46 Total CIWA-Ar score <15-18 symptom driven regimen or higher - scheduled medication regimen + PRN for breakthrough; reassessment every hour for at least 8 hours until score is < 8 for 2 hours Consider transfer to ICU if score > 35
47 Fixed-schedule regimen Administer one of the following medications every 6 hours: Diazepam, four doses of 10 mg, then eight doses of 5 mg Lorazepam, four doses of 2 mg, then eight doses of 1 mg Chlordiazepoxide, four doses of 50 mg, then eight doses of 25 mg Provide additional medication as needed when symptoms are not controlled (i.e., the CIWA-Ar score remains > 8 to 10 points).

48 51 CIWA-AR
 home-based management ED Based management hospital-based")
49 TREATMENT SETTINGS FOR ALCOHOL WITHDRAWAL office-based management withdrawal management services (Detox) home-based management ED Based management hospital-based management

50 OFFICE-BASED WITHDRAWAL MANAGEMENT No history of severe withdrawal (seizures or delirium tremens) < 65 No significant medical or mental health comorbidities Patient committed to abstinence and a treatment plan Patient agrees to attend a withdrawal management program You have time, space and personnel Follow the protocol:
 CIWA scores continue to climb despite following CIWA protocol. CIWA score is >10 after four doses of diazepam 80 mg.")
51 INDICATIONS FOR TRANSFERRING PATIENTS TO AN ED Severe withdrawal, with a CIWA score > 20, with hallucinations or other concerning symptoms. Seizure, impending delirium or psychosis (e.g., confusion, hallucinations). The patient shows any sign of acute medical illness (e.g., fever, dyspnea) CIWA scores continue to climb despite following CIWA protocol. CIWA score is >10 after four doses of diazepam 80 mg. Persistent tachycardia, >120 bpm or irregular beats. Suicidal ideation

52 DISCHARGE FROM THE EMERGENCY DEPARTMENT Treatment is completed when the patient is comfortable and has minimal tremor, and the CIWA score is less than 8 on two consecutive readings. If the patient is still in some withdrawal, prescribe two or three 10 mg diazepam tablets, to be taken one tablet every four hours, preferably to be dispensed by a partner or friend. The patient should agree not to drink while taking benzodiazepines. Send the patient home if an escort is available; otherwise, send the patient to a local withdrawal management service for admission. Have the patient followed-up in one or two days.
53 WITHDRAWAL MANAGEMENT SERVICES (DETOX) Most patients who do not need further medical interventions for withdrawal should be referred to withdrawal management services, which are non-medical and community based. Provide a safe place for people who are attempting to withdraw from any substance. Withdrawal management services provide counselling and treatment referral. You can phone a withdrawal management service to find out whether beds are available, but patients need to call or visit the service themselves to secure an assessment.
54 HOME-BASED WITHDRAWAL MANAGEMENT No history of severe withdrawal (e.g., seizures, delirium, hospital admissions) or withdrawal requiring medical management. The patient has recently gone without drinking for five or more days and withdrawal symptoms did not progress to more severe withdrawal requiring medical management. A support person (partner, family member or friend) agrees to dispense the medication. A treatment plan is in place (e.g., medications for alcohol use disorders, ongoing counselling, other treatment groups). The patient and the patient's support person agree to go to the emergency department if withdrawal symptoms become more severe. The patient is less than 65 years old and has no significant comorbidities or severe mental health problems. The patient agrees not to drink while taking medication.
55 HOME-BASED WITHDRAWAL PROTOCOL The patient has the last drink between 6:00 and 8:00 p.m. the night before. The patient takes 10 mg of diazepam, dispensed by the support person, starting the next morning, every four hours as needed for tremor. Prescribe no more than 40 mg of diazepam. Reassess the patient the next day (by phone or in person). The patient visits the clinic within two to three days. Connecting to community withdrawal management In some communities, an addiction service worker from a withdrawal management service will visit patients in their homes to monitor home-based withdrawal and to arrange formal treatment.
56 EMERGENCY DEPARTMENT OR OTHER HOSPITAL-BASED WITHDRAWAL MANAGEMENT History of severe withdrawal requiring hospitalization (e.g., delirium tremens) use alcohol very heavily (i.e., more than 12 to 15 drinks per day) have a history of withdrawal seizures have significant medical or mental health comorbidities are 65 years old or more are suicidal cannot be monitored appropriately in your office for reasons of time or space are unable to take oral diazepam. Emergency department treatment for these patients often involves intravenous rehydration, psychiatric assessment and monitoring of electrolytes, vital signs and cardiac function.
57 CHALLENGES OF ALCOHOL WITHDRAWAL MANAGEMENT Patients can be challenging Denial Non-compliance Unruly behavior Complicated by mental health issues Self medication Other substance use
58 I WORRY THAT SOME PATIENTS WITH ANXIETY ISSUES END UP SCORING HIGH ON CIWA. ~ ANTHONY WORSHAM, MD, UNIVERSITY OF NEW MEXICO CIWA too many subjective elements Patient-reported symptoms can be related to something else Patients with CIWA >20 are so confused and agitated that they can t describe their symptoms Co-morbidities and nurses inexperience with CIWA scoring can complicate treatment decisions By a CIWA of 8 the horse may be out of the barn If ETOH cessation is not the patient s goal, maybe ETOH is a better agent! Today s Hospitalist, October 2015
59 ETOH WITHDRAWAL DIFFERENTIAL DIAGNOSIS (OR CO-DIAGNOSES) Acute stimulant intoxication cocaine, methamphetamine, caffeine Alcohol intoxication can mimic withdrawal! Sepsis Thyrotoxicosis Heat stroke Hypoglycemia Intracranial processes (e.g., trauma, CVA) Encephalitis/encephalopathy
60 INAPPROPRIATE USE OF CIWA-AR 57% of patients who started on a CIWA-Ar protocol had either zero or one documented risk factor for AWS (19% and 38% respectively). 20% had no documentation of recent alcohol use 14% were unable to communicate 19% of medical records lacked documentation of provider awareness of the ordered protocol Benzodiazepine associated adverse events were documented in 15% Am J Drug Alcohol Abuse. 2018;44(4):
61 INAPPROPRIATE USE OF CIWA-AR language barrier exists Inability to provide a reliable history because of delirium, dementia, psychosis, etc. Can Fam Physician 2017 Sep; 63(9):
62 STOPPING OR DISCHARGING PREMATURELY Patients with a CIWA score <10 yet still have a severe alcohol withdrawal tremor are at risk of complications of alcohol withdrawal if discharged from the ED.
63 HOW MUCH BENZO? ENOUGH! BUT NOT FOR LONG Because clinicians often are reluctant to administer exceptionally high dosages, under treatment of alcohol withdrawal is a common problem There is a risk of replacing an alcohol addiction with benzodiazepine dependence or adding another addiction. The combination of benzodiazepines and alcohol can amplify the adverse psychological effects of each other causing enhanced depressive effects on mood and increase suicidal actions Am Fam Physician Mar 15;69(6): Alcohol use and anxiety Am J Psychiatry. 2007;164 (8): 1270
64 Patients who are discharged from the ED with a prescription for benzodiazepines are put at increased risk for sedative overdose, drug seeking behavior and drug dependence. It is strongly discouraged that patients be provided a take-away supply or prescription for benzodiazepines. The long half-life of diazepam will protect patients from developing serious symptoms of withdrawal, and if adequately treated in the ED, no additional medications will be required.

65 P R O T R A C T E D WITHDRAWAL SYNDROME Duration 6 12 MONTHS Features Insomnia Depression Anxiety Irritability Mood swings Cognitive deficits 79
66 PREVENTION Early identification of problem drinking allows prevention or treatment of complications, including severe withdrawal. All adult and adolescent patients should be screened to detect problem drinking. Patients who screen positive for problem drinking should receive a brief intervention designed to moderate their drinking. Am Fam Physician Feb 1;71(3):
67 FUTURE DIRECTIONS Baclofen may relieve severe withdrawal symptoms and reduced craving in alcoholdependent patients. Gabapentin, which is structurally similar to GABA, has been effective in the treatment of alcohol withdrawal in small studies. Vigabatrin, which irreversibly blocks GABA transaminase, may improve withdrawal symptoms NS Standard substance withdrawal pathway from start to infinity.
68 CASES: 78 year old man recovering from an urgent hip hemi-arthroplasty develops tachycardia, hypertension, fever, and agitation. 42 year old homeless man presents after a witnessed grand mal seizure tremulous and tachycardic 52 yr old woman dragged in by her daughter who says you have to fix her drinking Vitals are normal, ETOH yr old man presents from cells, where he was unable to stand. He has had fecal and urinary incontinence and manages only to tell you to -off.
69 CASES 27 year old falls off his bicycle whilst hammered. His (inebriated) friends joke that this is his normal Friday night state 44 year old man presents as Suicidal alcoholic x 20 yrs, lost job, family, house, several DUI s 55 yr old lady Alcoholic for years husband has cut her off, she is shaky and anxious. Asking for ativan. 60 year old in a rollover MVC, obviously intoxicated, rib fractures, but stable. Several trips to detox in past few years

70 DISCUSSION
Alcohol withdrawal. Clinical features
 Alcohol withdrawal Clinical features Severity increase with amount consumed; uncommon with < drinks per day. Predictable pattern: patients with previous withdrawal seizures are at high risk for recurrence.
Alcohol withdrawal Clinical features Severity increase with amount consumed; uncommon with < drinks per day. Predictable pattern: patients with previous withdrawal seizures are at high risk for recurrence.
Multiple Choice Questions
 Multiple Choice Questions 25yo M presents without psychiatric or medical history, with complaint of tremor to the ER. He denies drinking alcohol but his friend at bedside takes you to the side and reports
Multiple Choice Questions 25yo M presents without psychiatric or medical history, with complaint of tremor to the ER. He denies drinking alcohol but his friend at bedside takes you to the side and reports
Withdrawal.
 Withdrawal Shamim Nejad, MD Director, Adult Burns & Trauma Psychiatry Division of Psychiatry and Medicine Medical Director, Addiction Consultation Team MGH Center for Addiction Medicine Massachusetts General
Withdrawal Shamim Nejad, MD Director, Adult Burns & Trauma Psychiatry Division of Psychiatry and Medicine Medical Director, Addiction Consultation Team MGH Center for Addiction Medicine Massachusetts General
Please review the following slides prior to class. Information from these slides will be used to answer patient cases. Come prepared!
 Please review the following slides prior to class Information from these slides will be used to answer patient cases. Come prepared! Alcohol and Opiate Dependence Reference Slides Substances of Abuse A
Please review the following slides prior to class Information from these slides will be used to answer patient cases. Come prepared! Alcohol and Opiate Dependence Reference Slides Substances of Abuse A
Provider Update: Alcohol Withdrawal Order Set Edits
 Provider Update: Alcohol Withdrawal Order Set Edits Situation: A revised Alcohol Withdrawal Order Set and new CIWA-Ar scoring tool will go LIVE February 12, 2018. Background: The latest guidelines for
Provider Update: Alcohol Withdrawal Order Set Edits Situation: A revised Alcohol Withdrawal Order Set and new CIWA-Ar scoring tool will go LIVE February 12, 2018. Background: The latest guidelines for
Complicated Withdrawal
 Complicated Withdrawal Shamim Nejad, MD Director, Adult Burns & Trauma Psychiatry Division of Psychiatry and Medicine Medical Director, Addiction Consultation Team MGH Center for Addiction Medicine Massachusetts
Complicated Withdrawal Shamim Nejad, MD Director, Adult Burns & Trauma Psychiatry Division of Psychiatry and Medicine Medical Director, Addiction Consultation Team MGH Center for Addiction Medicine Massachusetts
Complicated Withdrawal
 Complicated Withdrawal Shamim Nejad, MD Medical Director, Psycho-Oncology Services Swedish Cancer Institute Swedish Medical Center Seattle, Washington Shamim.Nejad@Swedish.org Disclosures: Shamim Nejad,
Complicated Withdrawal Shamim Nejad, MD Medical Director, Psycho-Oncology Services Swedish Cancer Institute Swedish Medical Center Seattle, Washington Shamim.Nejad@Swedish.org Disclosures: Shamim Nejad,
AACN PCCN Review. Behavioral
 AACN PCCN Review Behavioral Presenter: Carol A. Rauen, RN, MS, CCNS, CCRN, PCCN, CEN Independent Clinical Nurse Specialist & Education Consultant rauen.carol104@gmail.com 0 Behavioral I. INTRODUCTION PCCN
AACN PCCN Review Behavioral Presenter: Carol A. Rauen, RN, MS, CCNS, CCRN, PCCN, CEN Independent Clinical Nurse Specialist & Education Consultant rauen.carol104@gmail.com 0 Behavioral I. INTRODUCTION PCCN
ALCOHOL WITHDRAWAL GUIDELINES
 ALCOHOL WITHDRAWAL GUIDELINES Policy author Accountable Executive Lead Approving body Policy reference Dr M Lewis, Gastroenterologist; Professor J A Vale, Clinical Toxicologist; Dr D A Robertson, Alcohol
ALCOHOL WITHDRAWAL GUIDELINES Policy author Accountable Executive Lead Approving body Policy reference Dr M Lewis, Gastroenterologist; Professor J A Vale, Clinical Toxicologist; Dr D A Robertson, Alcohol
Guidelines for the In-Patient Management of Alcohol Withdrawal at Frimley Park Hospital NHS Foundation Trust
 Guidelines for the In-Patient Management of Alcohol Withdrawal at Frimley Park Hospital NHS Foundation Trust Authors: Dr Aftab Ala, Consultant Gastroenterologist & Hepatologist Dr Tasneem Pirani, ST4 in
Guidelines for the In-Patient Management of Alcohol Withdrawal at Frimley Park Hospital NHS Foundation Trust Authors: Dr Aftab Ala, Consultant Gastroenterologist & Hepatologist Dr Tasneem Pirani, ST4 in
Current Clinical Patterns in the Management of Alcohol Withdrawal Syndrome (AWS)
") 1 Current Clinical Patterns in the Management of Alcohol Withdrawal Syndrome (AWS) The goal of the survey is to evaluate current practices for the inpatient management of AWS in adult hospitals located
1 Current Clinical Patterns in the Management of Alcohol Withdrawal Syndrome (AWS) The goal of the survey is to evaluate current practices for the inpatient management of AWS in adult hospitals located
DRAFT FOR CONSULTATION
 1) What is the accuracy of a tool and/or clinical judgement for the a) assessment b) monitoring of patients at risk of acute alcohol withdrawal? 2) Does the assessment and monitoring of patients with acute
1) What is the accuracy of a tool and/or clinical judgement for the a) assessment b) monitoring of patients at risk of acute alcohol withdrawal? 2) Does the assessment and monitoring of patients with acute
Management of high risk MMT patients. Meldon Kahan MD Methadone Prescribers Conference Toronto, Nov 15, 2013
 Management of high risk MMT patients Meldon Kahan MD Methadone Prescribers Conference Toronto, Nov 15, 2013 CFPC CoI Templates: Slide 1 Faculty Disclosure Faculty: Meldon Kahan Relationships with commercial
Management of high risk MMT patients Meldon Kahan MD Methadone Prescribers Conference Toronto, Nov 15, 2013 CFPC CoI Templates: Slide 1 Faculty Disclosure Faculty: Meldon Kahan Relationships with commercial
ALCOHOL USE DISORDER WITHDRAWAL MANAGEMENT AND LONG TERM TREATMENT ANA HOLTEY, MD ADDICTION MEDICINE FELLOW UNIVERSITY OF UTAH HEALTH
 ALCOHOL USE DISORDER WITHDRAWAL MANAGEMENT AND LONG TERM TREATMENT ANA HOLTEY, MD ADDICTION MEDICINE FELLOW UNIVERSITY OF UTAH HEALTH Prevalence of 12-Month Alcohol Use, High-Risk Drinking, and DSM-IV
ALCOHOL USE DISORDER WITHDRAWAL MANAGEMENT AND LONG TERM TREATMENT ANA HOLTEY, MD ADDICTION MEDICINE FELLOW UNIVERSITY OF UTAH HEALTH Prevalence of 12-Month Alcohol Use, High-Risk Drinking, and DSM-IV
WHEN AND HOW TO USE BENZODIAZEPINES IN TREATING ANXIETY: AM I WITHHOLDING TREATMENT IF I DON'T USE BENZODIAZEPINES?
 Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences WHEN AND HOW TO USE BENZODIAZEPINES IN TREATING ANXIETY: AM I WITHHOLDING TREATMENT IF I DON'T USE BENZODIAZEPINES?
Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences WHEN AND HOW TO USE BENZODIAZEPINES IN TREATING ANXIETY: AM I WITHHOLDING TREATMENT IF I DON'T USE BENZODIAZEPINES?
Managing presenting alcohol users an Introduction to SPECTRUM (CRI) By Dr Gideon Felton MRCPsych Consultant Psychiatrist and Clinical Lead
 By Dr Gideon Felton MRCPsych Consultant Psychiatrist and Clinical Lead") Managing presenting alcohol users an Introduction to SPECTRUM (CRI) By Dr Gideon Felton MRCPsych Consultant Psychiatrist and Clinical Lead PLAN OF PRESENTATION Assessment of alcohol dependence Psychiatric
Managing presenting alcohol users an Introduction to SPECTRUM (CRI) By Dr Gideon Felton MRCPsych Consultant Psychiatrist and Clinical Lead PLAN OF PRESENTATION Assessment of alcohol dependence Psychiatric
Basics of Benzodiazepine Use Disorder. DATE: June 12, 2018 PRESENTED BY: Melissa B. Weimer, DO, MCR
 Basics of Benzodiazepine Use Disorder DATE: June 12, 2018 PRESENTED BY: Melissa B. Weimer, DO, MCR Disclosures Speaker: Melissa Weimer, DO, MCR, has nothing to disclose. Planning Committee: The members
Basics of Benzodiazepine Use Disorder DATE: June 12, 2018 PRESENTED BY: Melissa B. Weimer, DO, MCR Disclosures Speaker: Melissa Weimer, DO, MCR, has nothing to disclose. Planning Committee: The members
Complicated Withdrawal
 Complicated Withdrawal Shamim Nejad, MD Medical Director, Division of Psychosocial Oncology Swedish Cancer Institute Swedish Medical Center Seattle, Washington Shamim.Nejad@Swedish.org Disclosures: Shamim
Complicated Withdrawal Shamim Nejad, MD Medical Director, Division of Psychosocial Oncology Swedish Cancer Institute Swedish Medical Center Seattle, Washington Shamim.Nejad@Swedish.org Disclosures: Shamim
Psychopharmacology in the Emergency Room. Michael D. Jibson, M.D., Ph.D. Associate Professor of Psychiatry University of Michigan
 Psychopharmacology in the Emergency Room Michael D. Jibson, M.D., Ph.D. Associate Professor of Psychiatry University of Michigan Pretest 1. Appropriate target symptoms for emergency room medication treatment
Psychopharmacology in the Emergency Room Michael D. Jibson, M.D., Ph.D. Associate Professor of Psychiatry University of Michigan Pretest 1. Appropriate target symptoms for emergency room medication treatment
Basics of Benzodiazepine Use Disorder. DATE: March 20, 2018 PRESENTED BY: Melissa B. Weimer, DO, MCR
 Basics of Benzodiazepine Use Disorder DATE: March 20, 2018 PRESENTED BY: Melissa B. Weimer, DO, MCR Disclosures Speaker: Melissa Weimer, DO, MCR, has nothing to disclose. Planning Committee: The members
Basics of Benzodiazepine Use Disorder DATE: March 20, 2018 PRESENTED BY: Melissa B. Weimer, DO, MCR Disclosures Speaker: Melissa Weimer, DO, MCR, has nothing to disclose. Planning Committee: The members
Benzodiazepines: Comparative Effectiveness and Strategies for Discontinuation. Ann M. Hamer, PharmD, BCPP Rural Oregon Academic Detailing Project
 Benzodiazepines: Comparative Effectiveness and Strategies for Discontinuation Ann M. Hamer, PharmD, BCPP Rural Oregon Academic Detailing Project This project is funded through a grant from the Pew Charitable
Benzodiazepines: Comparative Effectiveness and Strategies for Discontinuation Ann M. Hamer, PharmD, BCPP Rural Oregon Academic Detailing Project This project is funded through a grant from the Pew Charitable
Chapter 7. Screening and Assessment
 Chapter 7 Screening and Assessment Screening And Assessment Starting the dialogue and begin relationship Each are sizing each other up Information gathering Listening to their story Asking the questions
Chapter 7 Screening and Assessment Screening And Assessment Starting the dialogue and begin relationship Each are sizing each other up Information gathering Listening to their story Asking the questions
Methodist Hospital Alcohol Withdrawal Suggested Guidelines
 Methodist Hospital Alcohol Withdrawal Suggested Guidelines S. Prizada Sattar, MD Teri L Gabel, Pharm.D.,BCPP Sidney Kauzlarich, MD Subhash Bhatia, MD Mitzi Bollinger, RN S. Prizada Sattar, MD 6-20-3 Rationale
Methodist Hospital Alcohol Withdrawal Suggested Guidelines S. Prizada Sattar, MD Teri L Gabel, Pharm.D.,BCPP Sidney Kauzlarich, MD Subhash Bhatia, MD Mitzi Bollinger, RN S. Prizada Sattar, MD 6-20-3 Rationale
Alcohol Detoxification (Inpatient) Prescribing Guidelines
 Prescribing Guidelines") Alcohol Detoxification (Inpatient) Prescribing Guidelines Author: Sponsor/Executive: Responsible committee: Consultation & Approval: (Committee/Groups which signed off the procedure, including date) This
Alcohol Detoxification (Inpatient) Prescribing Guidelines Author: Sponsor/Executive: Responsible committee: Consultation & Approval: (Committee/Groups which signed off the procedure, including date) This
Basics of Benzodiazepine Use Disorder. DATE: October 3, 2017 PRESENTED BY: Melissa B. Weimer, DO, MCR
 Basics of Benzodiazepine Use Disorder DATE: October 3, 2017 PRESENTED BY: Melissa B. Weimer, DO, MCR Disclosures Speaker disclosure: One time lecture sponsored by Indivior about overlap of pain and opioid
Basics of Benzodiazepine Use Disorder DATE: October 3, 2017 PRESENTED BY: Melissa B. Weimer, DO, MCR Disclosures Speaker disclosure: One time lecture sponsored by Indivior about overlap of pain and opioid
Long term pharmacotherapy for Alcohol Dependence: Anti Craving agents
 Long term pharmacotherapy for Alcohol Dependence: Anti Craving agents Myth or Reality? Complete Recovery means a medication-free state True or False? Treatment of Alcoholism Assessment Motivation Alcohol
Long term pharmacotherapy for Alcohol Dependence: Anti Craving agents Myth or Reality? Complete Recovery means a medication-free state True or False? Treatment of Alcoholism Assessment Motivation Alcohol
Management of Alcohol Dependence
 STANDARD TREATMENT GUIDELINES Management of Alcohol Dependence Quick Reference Guide February 2016 Ministry of Health & Family Welfare Government of India 1 Table of Contents Objectives-... 3 Diagnosis...
STANDARD TREATMENT GUIDELINES Management of Alcohol Dependence Quick Reference Guide February 2016 Ministry of Health & Family Welfare Government of India 1 Table of Contents Objectives-... 3 Diagnosis...
Education Pack for the Alcohol Liaison Nurse Service
 Education Pack for the Alcohol Liaison Nurse Service Welcome to the Alcohol Liaison Nurse Service, this pack is designed to help you get the most out of your time here with us today and set some objectives
Education Pack for the Alcohol Liaison Nurse Service Welcome to the Alcohol Liaison Nurse Service, this pack is designed to help you get the most out of your time here with us today and set some objectives
ROLE OF HEALTH CARE PROVIDERS IN THE MANAGEMENT OF ALCOHOL AND DRUG USE RELATED PROBLEMS
 ROLE OF HEALTH CARE PROVIDERS IN THE MANAGEMENT OF ALCOHOL AND DRUG USE RELATED PROBLEMS Dr. Anita Rao? ASK SCREEN Refer HELP T T Ranganathan Clinical Research Foundation TTK Hospital IV Main Road, Indira
ROLE OF HEALTH CARE PROVIDERS IN THE MANAGEMENT OF ALCOHOL AND DRUG USE RELATED PROBLEMS Dr. Anita Rao? ASK SCREEN Refer HELP T T Ranganathan Clinical Research Foundation TTK Hospital IV Main Road, Indira
Using Benzodiazepines in Primary Care
 Using Benzodiazepines in Primary Care Spencer A. Tighe MD, FRCPC Saturday, Feb. 16, 2008 Overview Historical context Drug information Indications Side effects Abuse vs. physical dependence Clinical practice
Using Benzodiazepines in Primary Care Spencer A. Tighe MD, FRCPC Saturday, Feb. 16, 2008 Overview Historical context Drug information Indications Side effects Abuse vs. physical dependence Clinical practice
Detoxification of Chemically Dependent Inmates Federal Bureau of Prisons Clinical Practice Guidelines August 2009
 Detoxification of Chemically Dependent Inmates Federal Bureau of Prisons Clinical Practice Guidelines August 2009 Clinical guidelines are made available to the public for informational purposes only. The
Detoxification of Chemically Dependent Inmates Federal Bureau of Prisons Clinical Practice Guidelines August 2009 Clinical guidelines are made available to the public for informational purposes only. The
Predictors of Severity of Alcohol Withdrawal in Hospitalized Patients
 Elmer Original Article ress Predictors of Severity of Alcohol Withdrawal in Hospitalized Patients Radhames Ramos a, Thierry Mallet b, Anthony DiVittis c b, d, e, Ronny Cohen Abstract Background: Alcohol
Elmer Original Article ress Predictors of Severity of Alcohol Withdrawal in Hospitalized Patients Radhames Ramos a, Thierry Mallet b, Anthony DiVittis c b, d, e, Ronny Cohen Abstract Background: Alcohol
Delirium. Delirium. Delirium Etiology and Pathophysiology. Fall 2018
 Three most common cognitive problems in adults 1. (acute confusion) 2. Dementia 3. Depression These problems often occur together Can you think of common stimuli for each? 1 1 State of temporary but acute
Three most common cognitive problems in adults 1. (acute confusion) 2. Dementia 3. Depression These problems often occur together Can you think of common stimuli for each? 1 1 State of temporary but acute
*IN10 BIOPSYCHOSOCIAL ASSESSMENT*
 BIOPSYCHOSOCIAL ASSESSMENT 224-008B page 1 of 5 / 06-14 Please complete this questionnaire and give it to your counselor on your first visit. This information will help your clinician gain an understanding
BIOPSYCHOSOCIAL ASSESSMENT 224-008B page 1 of 5 / 06-14 Please complete this questionnaire and give it to your counselor on your first visit. This information will help your clinician gain an understanding
MINOR TRANQUILIZERS CHAPTER TWO : MINOR TRANQUILIZERS
 MINOR TRANQUILIZERS 76. The term 'minor tranquilizers' was introduced into the scientific literature in the 1950s to distinguish the medicines prescribed to reduce anxiety and tension from the major tranquillizers,
MINOR TRANQUILIZERS 76. The term 'minor tranquilizers' was introduced into the scientific literature in the 1950s to distinguish the medicines prescribed to reduce anxiety and tension from the major tranquillizers,
ANTICONVULSANTS IN ALCOHOL WITHDRAWAL TREATMENT: A BETTER WAY?
 Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences ANTICONVULSANTS IN ALCOHOL WITHDRAWAL TREATMENT: A BETTER WAY? RICHARD RIES MD PROFESSOR OF PSYCHIATRY AND DIRECTOR
Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences ANTICONVULSANTS IN ALCOHOL WITHDRAWAL TREATMENT: A BETTER WAY? RICHARD RIES MD PROFESSOR OF PSYCHIATRY AND DIRECTOR
Substance and Alcohol Related Disorders. Substance use Disorder Alcoholism Gambling Disorder
 Substance and Alcohol Related Disorders Substance use Disorder Alcoholism Gambling Disorder What is a Substance Use Disorder? According to the DSM-5, a substance use disorder describes a problematic pattern
Substance and Alcohol Related Disorders Substance use Disorder Alcoholism Gambling Disorder What is a Substance Use Disorder? According to the DSM-5, a substance use disorder describes a problematic pattern
Goals for sedation during mechanical ventilation
 New Uses of Old Medications Gina Riggi, PharmD, BCCCP, BCPS Clinical Pharmacist Trauma ICU Jackson Memorial Hospital Disclosure I do not have anything to disclose Objectives Describe the use of ketamine
New Uses of Old Medications Gina Riggi, PharmD, BCCCP, BCPS Clinical Pharmacist Trauma ICU Jackson Memorial Hospital Disclosure I do not have anything to disclose Objectives Describe the use of ketamine
DRUGS USED IN THE TREATMENT OF ADDICTION JOSEPH A. TRONCALE, MD FASAM RETREAT PREMIERE ADDICTION TREATMENT CENTERS
 DRUGS USED IN THE TREATMENT OF ADDICTION JOSEPH A. TRONCALE, MD FASAM RETREAT PREMIERE ADDICTION TREATMENT CENTERS MAJOR CATEGORIES OF TREATMENTS Detoxification and Post-Acute Withdrawal Maintenance Co-Occurring
DRUGS USED IN THE TREATMENT OF ADDICTION JOSEPH A. TRONCALE, MD FASAM RETREAT PREMIERE ADDICTION TREATMENT CENTERS MAJOR CATEGORIES OF TREATMENTS Detoxification and Post-Acute Withdrawal Maintenance Co-Occurring
General Effects. Special Patient Populations. Alcoholism. Who is an Alcoholic
 Alcohol Use & Abuse in Acutely and Critically Ill Patients: Don t Be Fooled General Effects Christine Schulman, RN, MS, CNS, CCRN Clinical Nurse Specialist & Consultant Trauma & Critical Care Nursing Portland,
Alcohol Use & Abuse in Acutely and Critically Ill Patients: Don t Be Fooled General Effects Christine Schulman, RN, MS, CNS, CCRN Clinical Nurse Specialist & Consultant Trauma & Critical Care Nursing Portland,
Chapter 7. Depressants and Inhalants. Depressants & Inhalants. History: Before Barbiturates 10/1/2012
 Chapter 7 Depressants and Inhalants Depressants & Inhalants Depressants = drugs that slow activity in the central nervous system Include prescription drugs that treat anxiety (sedatives) and insomnia (hypnotics)
Chapter 7 Depressants and Inhalants Depressants & Inhalants Depressants = drugs that slow activity in the central nervous system Include prescription drugs that treat anxiety (sedatives) and insomnia (hypnotics)
Methamphetamine Abuse During Pregnancy
 Methamphetamine Abuse During Pregnancy Robert Davis, MD / r.w.davismd@gmail.com ❶ Statistics ❷ Pregnancy Concerns ❸ Postpartum Concerns ❹ Basic Science ❺ Best Practice Guidelines ❻ Withdrawal ❼ Recovery
Methamphetamine Abuse During Pregnancy Robert Davis, MD / r.w.davismd@gmail.com ❶ Statistics ❷ Pregnancy Concerns ❸ Postpartum Concerns ❹ Basic Science ❺ Best Practice Guidelines ❻ Withdrawal ❼ Recovery
Admit date: 1-WM 2-WM 3.2-WM 3.7-WM 4-WM DSM-V diagnoses: Please list all diagnoses (psychiatric, chemical dependency and medical)
") https://providers.amerigroup.com Substance Use Disorder Withdrawal Management Prior Authorization and Continued Care Request (Use for American Society of Addiction Medicine [ASAM] withdrawal management
https://providers.amerigroup.com Substance Use Disorder Withdrawal Management Prior Authorization and Continued Care Request (Use for American Society of Addiction Medicine [ASAM] withdrawal management
Just Clear Them The Approach to Medical Clearance
 Just Clear Them The Approach to Medical Clearance Dr. Nalin Ahluwalia MD CCFP(EM) Associate Chief of Staff Emergency Physician Oakville Trafalgar Memorial Hospital My Disclosures None! Exemplary patient
Just Clear Them The Approach to Medical Clearance Dr. Nalin Ahluwalia MD CCFP(EM) Associate Chief of Staff Emergency Physician Oakville Trafalgar Memorial Hospital My Disclosures None! Exemplary patient
DISCLAIMER: ECHO Nevada emphasizes patient privacy and asks participants to not share ANY Protected Health Information during ECHO clinics.
 DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
Workshop cases answers
 Workshop cases answers BPSD Workshop: case histories Case 1: Mrs DM Scenario This is an 83 year old lady diagnosed with multi infarct dementia in 2008. Lives with husband and the couple are supported by
Workshop cases answers BPSD Workshop: case histories Case 1: Mrs DM Scenario This is an 83 year old lady diagnosed with multi infarct dementia in 2008. Lives with husband and the couple are supported by
Pharmacological Therapy Policy Practice Guidance Note Management of Acute Alcohol Withdrawal in Adults (Over 18) - V01. Planned review: December 2017
 - V01. Planned review: December 2017") Pharmacological Therapy Policy Practice Guidance Note Management of Acute Alcohol Withdrawal in Adults (Over 18) - V01 V01 issued: Issue 1- Dec 14 Issue 2 April 17 Planned review: December 2017 PPT-PGN
Pharmacological Therapy Policy Practice Guidance Note Management of Acute Alcohol Withdrawal in Adults (Over 18) - V01 V01 issued: Issue 1- Dec 14 Issue 2 April 17 Planned review: December 2017 PPT-PGN
ASAM Criteria, Third Edition Matrix for Matching Adult Severity and Level of Function with Type and Intensity of Service
 1: Acute Intoxication and/or Withdrawal Potential Risk Rating: 0 1: Acute Intoxication and/or Withdrawal Potential Risk Rating: 1 1: Acute Intoxication and/or Withdrawal Potential Risk Rating: 2 The patient
1: Acute Intoxication and/or Withdrawal Potential Risk Rating: 0 1: Acute Intoxication and/or Withdrawal Potential Risk Rating: 1 1: Acute Intoxication and/or Withdrawal Potential Risk Rating: 2 The patient
Medical Necessity Criteria 2017
 Medical Necessity Criteria 2017 The New Directions Medical Necessity Criteria have been revised. The new version will be effective January 1, 2017. See https://www.ndbh.com/providers/behavioralhealthplanproviders.aspx.
Medical Necessity Criteria 2017 The New Directions Medical Necessity Criteria have been revised. The new version will be effective January 1, 2017. See https://www.ndbh.com/providers/behavioralhealthplanproviders.aspx.
Managing presenting problems with benzodiazepines. By Dr Gideon Felton MRCPsych Consultant Psychiatrist and Clinical Lead
 Managing presenting problems with benzodiazepines By Dr Gideon Felton MRCPsych Consultant Psychiatrist and Clinical Lead OUTLINE OF PRESENTATION Why Benzodiazepines (BDZ s) are used Mechanism of Action
Managing presenting problems with benzodiazepines By Dr Gideon Felton MRCPsych Consultant Psychiatrist and Clinical Lead OUTLINE OF PRESENTATION Why Benzodiazepines (BDZ s) are used Mechanism of Action
BENZODIAZEPINES: WHAT YOU DON T KNOW CAN HURT YOU
 BENZODIAZEPINES: WHAT YOU DON T KNOW CAN HURT YOU TABLE OF CONTENTS 4 Benzodiazepine Addiction 8 Xanax Withdrawal Symptoms 11 Professional Help for Benzo Withdrawal is Essential for Success 15 Relapse
BENZODIAZEPINES: WHAT YOU DON T KNOW CAN HURT YOU TABLE OF CONTENTS 4 Benzodiazepine Addiction 8 Xanax Withdrawal Symptoms 11 Professional Help for Benzo Withdrawal is Essential for Success 15 Relapse
Prescribing for substance misuse: alcohol detoxification. Clinical background
 Prescribing for substance misuse: alcohol detoxification POMH-UK Quality Improvement Programme. Topic 14a: baseline Clinical background 1 2014 The Royal College of Psychiatrists. For further information
Prescribing for substance misuse: alcohol detoxification POMH-UK Quality Improvement Programme. Topic 14a: baseline Clinical background 1 2014 The Royal College of Psychiatrists. For further information
Controlled Substance and Wellness Agreement
 Controlled Substance and Wellness Agreement You and your provider have agreed on the use of controlled substance medications to treat your: We want to make sure you know how to manage your new prescription(s)
Controlled Substance and Wellness Agreement You and your provider have agreed on the use of controlled substance medications to treat your: We want to make sure you know how to manage your new prescription(s)
SCREENING FOR COMMON MENTAL DISORDERS DEPRESSIVE AND ANXIETY DISORDERS SUBSTANCE USE DISORDERS
 SCREENING FOR COMMON MENTAL DISORDERS DEPRESSIVE AND ANXIETY DISORDERS SUBSTANCE USE DISORDERS COMMON MENTAL DISORDERS Depressive Disorders Anxiety Disorders Substance use disorders CMD in HIV Twice as
SCREENING FOR COMMON MENTAL DISORDERS DEPRESSIVE AND ANXIETY DISORDERS SUBSTANCE USE DISORDERS COMMON MENTAL DISORDERS Depressive Disorders Anxiety Disorders Substance use disorders CMD in HIV Twice as
Psychopharmacology in the Emergency Room. Michael D. Jibson, M.D., Ph.D. Professor of Psychiatry University of Michigan
 Psychopharmacology in the Emergency Room Michael D. Jibson, M.D., Ph.D. Professor of Psychiatry University of Michigan Pretest 1. Which of the following conditions is LEAST likely to benefit from emergency
Psychopharmacology in the Emergency Room Michael D. Jibson, M.D., Ph.D. Professor of Psychiatry University of Michigan Pretest 1. Which of the following conditions is LEAST likely to benefit from emergency
Drugs, Society and Behavior
 SOCI 270 Drugs, Society and Behavior Spring 2016 Professor Kurt Reymers, Ph.D. Depressants & Inhalants = drugs that slow activity in the central nervous system Includes prescription drugs that treat anxiety
SOCI 270 Drugs, Society and Behavior Spring 2016 Professor Kurt Reymers, Ph.D. Depressants & Inhalants = drugs that slow activity in the central nervous system Includes prescription drugs that treat anxiety
Drug & Alcohol Detox:
 Drug & Alcohol Detox: Beginning Stages of Addiction Treatment If you ve tried to detox on your own and failed, you are not alone. The good news is that research shows those who commit to a rehabilitation
Drug & Alcohol Detox: Beginning Stages of Addiction Treatment If you ve tried to detox on your own and failed, you are not alone. The good news is that research shows those who commit to a rehabilitation
Lorraine Wilson, 74 years of age, is admitted. Alcohol Withdrawal. During Hospitalization. Early recognition and consistent intervention are critical.
 1.9 h o u r s Continuing Education Withdrawal During Hospitalization Early recognition and consistent intervention are critical. Overview: For a chronic drinker, sudden alcohol withdrawal because of an
1.9 h o u r s Continuing Education Withdrawal During Hospitalization Early recognition and consistent intervention are critical. Overview: For a chronic drinker, sudden alcohol withdrawal because of an
A Neurologist s Approach to Altered Mental Status
 A Neurologist s Approach to Altered Mental Status S. Andrew Josephson, MD Department of Neurology University of California San Francisco October 23, 2008 The speaker has no disclosures Case 1 A 71 year-old
A Neurologist s Approach to Altered Mental Status S. Andrew Josephson, MD Department of Neurology University of California San Francisco October 23, 2008 The speaker has no disclosures Case 1 A 71 year-old
Behavioral Health Service Request Form Detox and Substance Abuse Rehab
 Medicaid Call for Pre-Certification of Admissions: 1-855-620-1861 Kentucky Medicaid Fax: 1-877-338-3686 Standard Request Requests for prior authorization (with supporting clinical information and documentation)
Medicaid Call for Pre-Certification of Admissions: 1-855-620-1861 Kentucky Medicaid Fax: 1-877-338-3686 Standard Request Requests for prior authorization (with supporting clinical information and documentation)
ADULT Addictions Treatment: Medically Monitored Residential Treatment (3B)
") ADULT Addictions Treatment: Medically Monitored Residential Treatment (3B) Program Medically Monitored Short Term Residential treatment provides 24 hour professionally directed evaluation, care, and treatment
ADULT Addictions Treatment: Medically Monitored Residential Treatment (3B) Program Medically Monitored Short Term Residential treatment provides 24 hour professionally directed evaluation, care, and treatment
PATHOPHYSIOLOGY AND TREATMENT OF ALCOHOL WITHDRAWAL SYNDROME: A REVIEW
 PATHOPHYSIOLOGY AND TREATMENT OF ALCOHOL WITHDRAWAL SYNDROME: A REVIEW Dana Bartlett, BSN, MSN, MA, CSPI Dana Bartlett is a professional nurse and author. His clinical experience includes 16 years of ICU
PATHOPHYSIOLOGY AND TREATMENT OF ALCOHOL WITHDRAWAL SYNDROME: A REVIEW Dana Bartlett, BSN, MSN, MA, CSPI Dana Bartlett is a professional nurse and author. His clinical experience includes 16 years of ICU
Treatment of Alcohol and Opiate Withdrawal
 Objectives Treatment of Alcohol and Opiate Withdrawal Renee Striker, Pharm.D., BCPS, BCPP Pharmacy Clinical Specialist Huron Hospital East Cleveland, Ohio Outline the diagnostic criteria for substance
Objectives Treatment of Alcohol and Opiate Withdrawal Renee Striker, Pharm.D., BCPS, BCPP Pharmacy Clinical Specialist Huron Hospital East Cleveland, Ohio Outline the diagnostic criteria for substance
PRACTICAL MANAGEMENT OF DEPRESSION IN OLDER ADULTS. Lee A. Jennings, MD MSHS Assistant Professor Division of Geriatrics, UCLA
 CASE #1 PRACTICAL MANAGEMENT OF DEPRESSION IN OLDER ADULTS Lee A. Jennings, MD MSHS Assistant Professor Division of Geriatrics, UCLA OBJECTIVES Epidemiology Presentation in older adults Assessment Treatment
CASE #1 PRACTICAL MANAGEMENT OF DEPRESSION IN OLDER ADULTS Lee A. Jennings, MD MSHS Assistant Professor Division of Geriatrics, UCLA OBJECTIVES Epidemiology Presentation in older adults Assessment Treatment
Alcohol Use in the Elderly
 Substance Use/Abuse in the Geriatric Population Alan L. Schneider, MD DFAPA DABAM Medical Director, Western Region Aetna Behavioral Health Associate Professor of Psychiatry, UCLA School of Medicine Alcohol
Substance Use/Abuse in the Geriatric Population Alan L. Schneider, MD DFAPA DABAM Medical Director, Western Region Aetna Behavioral Health Associate Professor of Psychiatry, UCLA School of Medicine Alcohol
Medication Management. Dr Ajith Weeraman MBBS, MD (Psychiatry), FRANZCP Consultant Psychiatrist Epworth Clinic Camberwell 14 th March 2015
, FRANZCP Consultant Psychiatrist Epworth Clinic Camberwell 14 th March 2015") Medication Management Dr Ajith Weeraman MBBS, MD (Psychiatry), FRANZCP Consultant Psychiatrist Epworth Clinic Camberwell 14 th March 2015 1 Medication Management Objectives: 1. Principles of psycho-pharmacology
Medication Management Dr Ajith Weeraman MBBS, MD (Psychiatry), FRANZCP Consultant Psychiatrist Epworth Clinic Camberwell 14 th March 2015 1 Medication Management Objectives: 1. Principles of psycho-pharmacology
Benzodiazepines. Benzodiazepines
 : History 1950s - Invented by Swiss chemists who identified its sedative effects 1950s 60s - Chlordiazepoxide (Librium) marketed as a safer alternative to barbiturates; along with newer benzodiazepines
: History 1950s - Invented by Swiss chemists who identified its sedative effects 1950s 60s - Chlordiazepoxide (Librium) marketed as a safer alternative to barbiturates; along with newer benzodiazepines
Lorazepam Tablets, USP
 Lorazepam Tablets, USP DESCRIPTION: Lorazepam, an antianxiety agent, has the chemical formula, 7-chloro-5-(o-chlorophenyl)-1,3-dihydro-3-hydroxy-2H -1,4-benzodiazepin-2-one: Cl H N N O Cl OH It is a white
Lorazepam Tablets, USP DESCRIPTION: Lorazepam, an antianxiety agent, has the chemical formula, 7-chloro-5-(o-chlorophenyl)-1,3-dihydro-3-hydroxy-2H -1,4-benzodiazepin-2-one: Cl H N N O Cl OH It is a white
Stabilization Algorithm
 VA/DoD Clinical Practice Guideline for the Management of Substance Use Disorders Stabilization Algorithm Stabilization Pocket Card 1 Patient and Time Information Clinical Institute Withdrawal Assessment
VA/DoD Clinical Practice Guideline for the Management of Substance Use Disorders Stabilization Algorithm Stabilization Pocket Card 1 Patient and Time Information Clinical Institute Withdrawal Assessment
Amy Eisenhauer Developed for Pulse Check 2016
 Amy Eisenhauer Developed for Pulse Check 2016 Understand alcoholism, co-morbid diseases, and treatment options Possible emergent presentations Discuss societal and EMS perceptions of alcohol related illness
Amy Eisenhauer Developed for Pulse Check 2016 Understand alcoholism, co-morbid diseases, and treatment options Possible emergent presentations Discuss societal and EMS perceptions of alcohol related illness
Lead for Gastroenterology Lee Dodge Alcohol Liaison 03/03/2015. Clive Gibson Safeguarding Adults Lead Nurse 03/03/2015
 Acute Alcohol Withdrawal Management for Adult Inpatients Type: Clinical Guideline Register No: 1409 Status: Public on ratification Developed in response to: Best Practice Contributes to CQC Outcome number:
Acute Alcohol Withdrawal Management for Adult Inpatients Type: Clinical Guideline Register No: 1409 Status: Public on ratification Developed in response to: Best Practice Contributes to CQC Outcome number:
Delirium. Assessment and Management
 Delirium Assessment and Management Goals and Objectives Participants will: 1. be able to recognize and diagnose the syndrome of delirium. 2. understand the causes of delirium. 3. become knowledgeable about
Delirium Assessment and Management Goals and Objectives Participants will: 1. be able to recognize and diagnose the syndrome of delirium. 2. understand the causes of delirium. 3. become knowledgeable about
A new model for prescribing varenicline
 Pharmacist Independent Prescribers in partnership with A new model for prescribing varenicline Dear Stop Smoking Advisor You will be aware of the stop smoking drug varenicline that goes under the brand
Pharmacist Independent Prescribers in partnership with A new model for prescribing varenicline Dear Stop Smoking Advisor You will be aware of the stop smoking drug varenicline that goes under the brand
Assessment Main title and management of alcohol dependence and withdrawal in the acute hospital: concise guidance
 CONCISE GUIDANCE Clinical Medicine 01, Vol 1, No : 71 Assessment Main title and management of alcohol dependence and withdrawal in the acute hospital: concise guidance Author head name Stephen Stewart
CONCISE GUIDANCE Clinical Medicine 01, Vol 1, No : 71 Assessment Main title and management of alcohol dependence and withdrawal in the acute hospital: concise guidance Author head name Stephen Stewart
Dexmedetomidine: the various roles and utilization strategies. Julie Belfer, PharmD September 2014
 Dexmedetomidine: the various roles and utilization strategies Julie Belfer, PharmD September 2014 Disclosure No disclosures concerning possible financial or personal relationships with commercial entities
Dexmedetomidine: the various roles and utilization strategies Julie Belfer, PharmD September 2014 Disclosure No disclosures concerning possible financial or personal relationships with commercial entities
Ambulatory Intoxication and Withdrawal Management: A Clinical Monograph
 Ambulatory Intoxication and Withdrawal Management: A Clinical Monograph Revised December 2016 1 Table of Contents I. Ambulatory Intoxication and Withdrawal Management... 3 II. Evaluation and Assessment
Ambulatory Intoxication and Withdrawal Management: A Clinical Monograph Revised December 2016 1 Table of Contents I. Ambulatory Intoxication and Withdrawal Management... 3 II. Evaluation and Assessment
The causes of misuse:
 The Drug Misuse The causes of misuse: Availability of drugs. A vulnerable personality. Adverse social environment. Regular drug taking play a role. Determining misuse and dependence, it is unclear whether
The Drug Misuse The causes of misuse: Availability of drugs. A vulnerable personality. Adverse social environment. Regular drug taking play a role. Determining misuse and dependence, it is unclear whether
Dr. Oslin receives grant support from the NIH, VA, and the Pennsylvania Department of Aging.
 David W. Oslin, MD University of Pennsylvania Philadelphia VAMC Dr. Oslin receives grant support from the NIH, VA, and the Pennsylvania Department of Aging. Dr. Oslin is a consultant to the Hazelden Betty
David W. Oslin, MD University of Pennsylvania Philadelphia VAMC Dr. Oslin receives grant support from the NIH, VA, and the Pennsylvania Department of Aging. Dr. Oslin is a consultant to the Hazelden Betty
Initiation of Clozapine Treatment Community Patients
 Initiation of Clozapine Treatment Community Patients Who Should Read This Policy Target Audience All clinical staff working in the community N/A N/A Initiation of Clozapine Treatment for Patients in the
Initiation of Clozapine Treatment Community Patients Who Should Read This Policy Target Audience All clinical staff working in the community N/A N/A Initiation of Clozapine Treatment for Patients in the
Faculty/Presenter Disclosure
 Faculty/Presenter Disclosure Faculty: Dr. Anthony Kerigan Relationships with commercial interests:* Grants/Research Support: NONE Speakers Bureau/Honoraria: NONE Consulting Fees: NONE Other: NONE Meeting
Faculty/Presenter Disclosure Faculty: Dr. Anthony Kerigan Relationships with commercial interests:* Grants/Research Support: NONE Speakers Bureau/Honoraria: NONE Consulting Fees: NONE Other: NONE Meeting
Chapter 15. Seizures. Learning Objectives. Learning Objectives 9/11/2012
 Chapter 15 Seizures Learning Objectives Demonstrate proper procedure for rectal administration of diazepam, and discuss why rectal administration is sometimes necessary for patient having a seizure Discuss
Chapter 15 Seizures Learning Objectives Demonstrate proper procedure for rectal administration of diazepam, and discuss why rectal administration is sometimes necessary for patient having a seizure Discuss
Main Questions. Why study addiction? Substance Use Disorders, Part 1 Alecia Schweinsburg, MA Abnromal Psychology, Fall Substance Use Disorders
 Substance Use Disorders Main Questions Why study addiction? What is addiction? Why do people become addicted? What do alcohol and drugs do? How do we treat substance use disorders? Why study addiction?
Substance Use Disorders Main Questions Why study addiction? What is addiction? Why do people become addicted? What do alcohol and drugs do? How do we treat substance use disorders? Why study addiction?
Prepared by: Dr. Elizabeth Woodward, University of Toronto Resident in Psychiatry
 Prepared by: Dr. Elizabeth Woodward, University of Toronto Resident in Psychiatry In broad terms, substance use disorders occur when a substance is used in a compulsive manner with a lack of control over
Prepared by: Dr. Elizabeth Woodward, University of Toronto Resident in Psychiatry In broad terms, substance use disorders occur when a substance is used in a compulsive manner with a lack of control over
Delirium. Dr. Lesley Wiesenfeld. Deputy Psychiatrist in Chief, Mount Sinai Hospital. Dr. Carole Cohen
 Delirium Dr. Lesley Wiesenfeld Deputy Psychiatrist in Chief, Mount Sinai Hospital Dr. Carole Cohen Department of Psychiatry, University of Toronto and Sunnybrook Health Sciences Centre Case Study Mrs B
Delirium Dr. Lesley Wiesenfeld Deputy Psychiatrist in Chief, Mount Sinai Hospital Dr. Carole Cohen Department of Psychiatry, University of Toronto and Sunnybrook Health Sciences Centre Case Study Mrs B
1/31/2009. Paroxysmal, uncontrolled electrical discharge of neurons in brain interrupting normal function
 Paroxysmal, uncontrolled electrical discharge of neurons in brain interrupting normal function In epilepsy abnormal neurons undergo spontaneous firing Cause of abnormal firing is unclear Firing spreads
Paroxysmal, uncontrolled electrical discharge of neurons in brain interrupting normal function In epilepsy abnormal neurons undergo spontaneous firing Cause of abnormal firing is unclear Firing spreads
Antidepressants and Sedatives. David G. Standaert, M.D., Ph.D. Massachusetts General Hospital Harvard Medical School
 Antidepressants and Sedatives David G. Standaert, M.D., Ph.D. Massachusetts General Hospital Harvard Medical School Depression A frequent problem, affecting up to 5% of the population Common presentations
Antidepressants and Sedatives David G. Standaert, M.D., Ph.D. Massachusetts General Hospital Harvard Medical School Depression A frequent problem, affecting up to 5% of the population Common presentations
Alcohol withdrawal including the Symptom triggered CIWA score Management
 Alcohol withdrawal including the Symptom triggered CIWA score Management Classification: Policy Lead Author: Ruth Brown Alcohol specialist Nurse Additional author(s): Hailey Pennington Authors Division:
Alcohol withdrawal including the Symptom triggered CIWA score Management Classification: Policy Lead Author: Ruth Brown Alcohol specialist Nurse Additional author(s): Hailey Pennington Authors Division:
,2($".+;2".$;+'#04.23)+ %(+<=>+&"#2+
+ %(+<=>++") 82$2&$%(9+"(:+3"("9%(9+&0330(+&;%.:+"(:+":-.$+,0:-.2+7+,2($".+;2".$;+'#04.23)+ %(++&"#2+,0:-.2+5+++?033-(%&"$%0(++ @A%..)+"(:++ B))2))32($+ M;0-9;$N++ '2#&2'$%0(N+"(:+ 3230#F+ '#04.23)+,0:-.2++O+++++++++
82$2&$%(9+"(:+3"("9%(9+&0330(+&;%.:+"(:+":-.$+,0:-.2+7+,2($".+;2".$;+'#04.23)+ %(++&"#2+,0:-.2+5+++?033-(%&"$%0(++ @A%..)+"(:++ B))2))32($+ M;0-9;$N++ '2#&2'$%0(N+"(:+ 3230#F+ '#04.23)+,0:-.2++O+++++++++
Intro to Concurrent Disorders
 CSAM-SCAM Fundamentals Intro to Concurrent Disorders Presentation provided by Jennifer Brasch, MD, FRCPC Psychiatrist, Concurrent Disorders Program, St. Joseph s Healthcare There are all kinds of addicts,
CSAM-SCAM Fundamentals Intro to Concurrent Disorders Presentation provided by Jennifer Brasch, MD, FRCPC Psychiatrist, Concurrent Disorders Program, St. Joseph s Healthcare There are all kinds of addicts,
Substance Misuse Nurse service Belfast Trust
 Substance Misuse Nurse service Belfast Trust Alcohol is the most widely available socially acceptable drug in Northern Ireland It can be an addictive substance It is a depressant- slows down the central
Substance Misuse Nurse service Belfast Trust Alcohol is the most widely available socially acceptable drug in Northern Ireland It can be an addictive substance It is a depressant- slows down the central
Pharmacological Therapy Policy Practice Guidance Note Management of Acute Alcohol Withdrawal in Adults (Over 18) - V02. Planned review: Dec 2020
 - V02. Planned review: Dec 2020") Pharmacological Therapy Policy Practice Guidance Note Management of Acute Alcohol Withdrawal in Adults (Over 18) - V02 Issue No: Issue 1- Dec 17 Planned review: Dec 2020 PPT-PGN 22 Part of NTW(C)38 Pharmacological
Pharmacological Therapy Policy Practice Guidance Note Management of Acute Alcohol Withdrawal in Adults (Over 18) - V02 Issue No: Issue 1- Dec 17 Planned review: Dec 2020 PPT-PGN 22 Part of NTW(C)38 Pharmacological
Geriatric Alterations Associated with Neurological Conditions
 Geriatric Alterations Associated with Neurological Conditions I have no conflicts of interest. Julie Bronson The Older Adult According to the World Health Organization Africa 50-55 or 50-65 United Nations
Geriatric Alterations Associated with Neurological Conditions I have no conflicts of interest. Julie Bronson The Older Adult According to the World Health Organization Africa 50-55 or 50-65 United Nations
BRAIN. Tumor byproducts. Autonomic nerves. Somatic nerves. Host immune cells. Cytokines
 Patient s Problems Pain (80%) Fatigue (90%) Weight Loss (80%) Lack of Appetite (80%) Nausea, Vomiting (90%) Anxiety (25%) Shortness of Breath (50%) Confusion-Agitation (80%) Tumor Mass Tumor Function Somatic
Patient s Problems Pain (80%) Fatigue (90%) Weight Loss (80%) Lack of Appetite (80%) Nausea, Vomiting (90%) Anxiety (25%) Shortness of Breath (50%) Confusion-Agitation (80%) Tumor Mass Tumor Function Somatic
Delirium. Geriatric Giants Lecture Series Divisions of Geriatric Medicine and Care of the Elderly University of Alberta
 Delirium Geriatric Giants Lecture Series Divisions of Geriatric Medicine and Care of the Elderly University of Alberta Overview A. Delirium - the nature of the beast B. Significance of delirium C. An approach
Delirium Geriatric Giants Lecture Series Divisions of Geriatric Medicine and Care of the Elderly University of Alberta Overview A. Delirium - the nature of the beast B. Significance of delirium C. An approach
Behavioral Health Service Request Form Detox and Substance Abuse Rehab
 Arkansas 855-538-0454 Connecticut 855-538-0454 Florida 855-538-0454 Georgia 800-424-5412 Illinois 800-504-2766 Kentucky 855-620-1861 Louisiana 855-538-0454 Arkansas 855-710-0159 Connecticut 888-365-3233
Arkansas 855-538-0454 Connecticut 855-538-0454 Florida 855-538-0454 Georgia 800-424-5412 Illinois 800-504-2766 Kentucky 855-620-1861 Louisiana 855-538-0454 Arkansas 855-710-0159 Connecticut 888-365-3233
Chapter Goal. Learning Objectives 9/12/2012. Chapter 31. Behavioral Emergencies & Substance Abuse
 Chapter 31 & Chapter Goal Use assessment findings to form field impression & implement management plan for patients with behavioral or drug abuse emergencies Learning Objectives Distinguish between normal
Chapter 31 & Chapter Goal Use assessment findings to form field impression & implement management plan for patients with behavioral or drug abuse emergencies Learning Objectives Distinguish between normal
Acute Alcohol Withdrawal Protocol
 Acute Alcohol Withdrawal Protocol Controlled document This document is uncontrolled when downloaded or printed Reference number Version 1 Author WHHT: C268 Dr Mohamed Shariff Date ratified August 2014
Acute Alcohol Withdrawal Protocol Controlled document This document is uncontrolled when downloaded or printed Reference number Version 1 Author WHHT: C268 Dr Mohamed Shariff Date ratified August 2014
WHAT SHOULD WE DO ABOUT BENZODIAZEPINES? Miriam Komaromy, MD Associate Director, Project ECHO August 2014
 WHAT SHOULD WE DO ABOUT BENZODIAZEPINES? Miriam Komaromy, MD Associate Director, Project ECHO August 2014 EPIDEMIOLOGY OF BENZO USE 7-18% of US population uses a benzo for medical purposes each year Average
WHAT SHOULD WE DO ABOUT BENZODIAZEPINES? Miriam Komaromy, MD Associate Director, Project ECHO August 2014 EPIDEMIOLOGY OF BENZO USE 7-18% of US population uses a benzo for medical purposes each year Average
Anxiolytic, Sedative and Hypnotic Drugs. Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia
 Anxiolytic, Sedative and Hypnotic Drugs Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Anxiolytics: reduce anxiety Sedatives: decrease activity, calming
Anxiolytic, Sedative and Hypnotic Drugs Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Anxiolytics: reduce anxiety Sedatives: decrease activity, calming
Antidepressants: Prof. Riyadh Al_Azzawi F.R.C.Psych
 Antidepressants: Prof. Riyadh Al_Azzawi F.R.C.Psych A. Heterocyclic antidepressants: (tricyclic and tetracyclic ), e.g.amitryptaline,imipramine. B. Monoamine oxidase inhibitors(m.a.o.i), e.g.phenelzine.
Antidepressants: Prof. Riyadh Al_Azzawi F.R.C.Psych A. Heterocyclic antidepressants: (tricyclic and tetracyclic ), e.g.amitryptaline,imipramine. B. Monoamine oxidase inhibitors(m.a.o.i), e.g.phenelzine.