Safe Opioid Prescribing Practices in the Elderly
|
|
|
- Abraham Boyd
- 6 years ago
- Views:
Transcription
1 Safe Opioid Prescribing Practices in the Elderly Masil George, MD Director, Geriatric Palliative Care Program Medical Director, Baptist Hospice This program has been funded under grant #U1QHP28723
2 No financial interests Disclosure
3 Objectives Provide framework for understanding and assessing chronic pain Describe the good, the bad and the ugly aspects of prescription opioid pain medications Define role of opioids in managing chronic non-malignant pain in the geriatric outpatient setting Tips to ensure prescriber responsibility and patient safety

4 The opioid epidemic
5 Facts and Figures Roughly 21 to 29 percent of patients prescribed opioids for chronic pain misuse them. Between 8 and 12 percent develop an opioid use disorder. An estimated 4 to 6 percent who misuse prescription opioids transition to heroin. In 2013, enough opioids prescriptions for all adults in USA About 80 percent of people who use heroin first misused prescription opioids. Source: National Institute on Drug Abuse (NIDA)
6 Facts and Figures The annual number of overdose deaths involving prescription and illicit opioids has nearly quadrupled since In addition, more than 2 million people in the United States are addicted to prescription opioids More than 12 million report having misused these medications in Prescription opioid addiction and misuse are also contributing to a resurgence in heroin use and the spread of HIV and hepatitis C Vivek Murthy, Ending the Opioid Epidemic NEJM Dec 2016

7 A brief history of opioids 3400 BC to 300 AD Hippocrates, Alexander 1500s- Laudanum 1800s- Morphine isolated from opium and heroin synthesized from morphine Opioid schedules War on drugs
8
9 Recent history 1990s- Several new opioid options, extensive marketing Pain the fifth vital sign More people die of opioid overdose than any other year on record, Hydrocodone to schedule II CDC released guidelines for prescribing opioids for chronic pain
10 Ms. KM Ms. KM is a 65 y/o WF presented to clinic to get established, and for pain management PMH of essential Hypertension, Major depression with anxiety, Fibromyalgia, morbid obesity with BMI of 52.1, Lymphedema, admission to psychiatric inpatient unit in 2013 SH- Widow since 2010, Highly educated, moved from out of state Oxycontin 80 mg po bid, and hydrocodone 7.5/325 every 4 hours/ PRN
11 DEFINITION OF PAIN Unpleasant sensory and emotional experience associated with actual or potential tissue damage
12 Types Nociceptive: pains are complication of infiltration of tissue by tumor or tissue injury Somatic: deep aches Visceral: cramping, colicky Neuropathic: complication of injury to the peripheral or central nervous systems Poorly tolerated and difficult to control
13 Acute and chronic pain Acute pain- Comes on quickly, can be severe, lasts short time Chronic pain- Pain that persists longer than course of natural healing
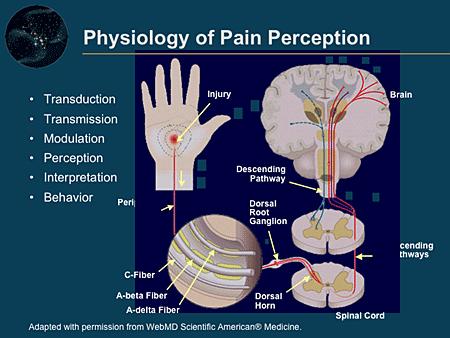
14 Pain physiology
15 Elements of pain assessment Location Intensity or severity Quality (description) Duration Pattern Current treatment/response What has worked in the past?
16 How to assess pain? Verbal pain intensity scale Numeric pain intensity scale Visual analog scale Faces
17 Assessment of Pain Intensity Verbal Pain Intensity Scale Visual Analog Scale No Mild Moderate Severe Very Worst pain pain pain pain severe possible pain pain No pai n Worst possible pain 0 10 Numeric Pain Intensity Scale Faces Scale No Moderate Worst pain pain possible pain Sources: Portenoy RK, Kanner RM, eds. Pain Management: Theory and Practice. FA Davis; 1996:8-1 Wong DL. Waley and Wong sessentials of Pediatric Nursing. 5th ed. Mosby, Inc.; 1997: McCaffery M, Pasero C. Pain: Clinical Manual. Mosby, Inc. 1999:16. 17
18 Multimodal pain assessment tools Brief pain inventory (short form) McGill pain questionnaire Graded chronic pain scale 3 question PEG scale - Pain on average? - Pain interfered with enjoyment of life? - Pain interfered with general activity?
19
20 Pathophysiology of chronic pain Acute pain- Strong relationship between peripheral stimulation and pain perception Chronic pain- created by nervous system secondary to nociceptor activation
21 Chronic pain- It is all in their head Sensitization of pain transmission fibers Death of inhibitory cells Loss of tonic inhibition Structural neuroplastic changes
22 Psychology of pain Psychological factors can dramatically modulate pain related suffering and dysfunction. Expectation of pain, and reinforcement of pain behavior increase pain behavior, and it has now been demonstrated that these factors increase cortical activation associated with experimental pains. Conversely, distraction reduces pain.


23 Tip of the iceberg Chronic Pain Acute Pain Depression Anxiety Addiction Somatoform disorders Personality disorders

24 Pain ladder
25 Non pharmacological pain management CBT- mindful meditation Exercise Acupuncture, Yoga, hypnotherapy, massage TENS Interventional approaches
26 Non opioid pharmacological pain Antidepressants Anticonvulsants Alpha-2 adrenergic agonists Local anesthetics Corticosteroids Baclofen N-methyl-D-aspartate receptor agonists Muscle relaxants Topical creams and gel Neuroleptics Antihistamines Psychostimulants Calcitonin management Pain Management in the Elderly Population: A Review Alan D. Kaye, Amir Baluch, Jared T Scott
27 Opioids- The good Works really well Usually well tolerated Works for pretty much for any type of pain No ceiling effect (only dose limiting side effects) Opioids and the management of chronic severe pain in the elderly Pergolizzi J, Boger RH et al
28 Opioids- the bad Common side effects: Nausea/vomiting (resolved in 3-5 days), sedation, nausea, delayed gastric emptying, sexual dysfunction, sleep disturbance, multiple drug interactions, constipation (never resolves), pruritus, myoclonus, especially for the elderly: delirium, hallucinations, cognitive impairment Other side effects: Opioids induced neruotoxcity, hyperalgesia/allodynia, urinary retention, noncardiogenic edema, seizure, endocrine/immune effects? Respiratory Depression: occurs with excess doses of medication esp in opioid naïve patients; or when opioids requiring reduction Somnolence precedes respiratory depression Opioids and the management of chronic severe pain in the elderly Pergolizzi J, Boger RH et al
29 Opioids- the ugly Pseudo-Addiction Physical dependence confused with psychological dependence Pain-relief seeking, not drug-seeking When right dose used, patient functions better in life, whereas opposite true with the true addict Physical Dependence Tolerance (20-40%) up-regulate opioid receptors to need higher dose for sustained effect Withdrawal (20-40%) after 2 wks, withdrawing drug leads to adrenaline response (sweating, tachycardia, tachypnea, cramps, diarrhea, hypertension); avoid by decreasing drug 25% a day. Psychological Dependence Addiction (0.1% in CA pain) a need to get high where drug controls your life, compulsive uncontrolled behavior to get the drug; lie, cheat, steal. Risk factors for addiction: male, family history, personal history, criminal record, mental health issues
30 CDC guidelines for prescribing opioids for chronic pain 1. Non pharmacological and non opioid pharmacologic therapy is preferred for chronic pain. Only consider opioids if benefits anticipated to outweigh risks 2. Establish realistic treatment goals for pain and function before starting opioids and consider how opioids will be discontinued if benefits do not outweigh risks 3. Discuss known risks and realistic benefits before starting and periodically during therapy 4. When starting opioids for chronic pain, prescribe IR opioids instead of ER/LA 5. Prescribe lowest effective dose, try to keep below 90 MME per day 6. When treating acute pain, try to prescribe for 3 days or less
31 CDC guidelines for prescribing opioids for chronic pain 7. Evaluate within 1 to 4 weeks of starting opioids or dose escalation and every 3 months 8. Mitigate risk- consider naloxone if risk of opioid overdose such as previous history, higher dose (> 50 MMEs) or concurrent benzodiazepines 9. Review state prescription monitoring program when starting opioids and periodically 10. Consider urine drug testing at least annually 11. Avoid prescribing opioids and benzodiazepines concurrently 12. For patients with opioid use disorder, offer or arrange evidencebased medication assisted treatment programs
32 Realistic goals for pain management S- specific M- measureable A- action-oriented R- realistic T- time-sensitive Source: Scope of pain: safe and competent opioid prescribing education
33 Challenges to choosing right opioid Baby Zoomers Comorbidities Polypharmacy Physiological changes Cognitive and communication challenges Opioids and the management of chronic severe pain in the elderly Pergolizzi J, Boger RH et al
34 Special considerations Renal Failure Fentanyl and Methadone are safest, use morphine and oxycodone cautiously, avoid codeine and meperidine Liver Failure- Fentanyl is the safest, Use morphine, oxycodone and dilaudid cautiously and avoid methadone and Codeine Allergy- Find out what patient actually means Source: Pain treatment topics. Opioid safety in patients with hepatic or renal dysfunction, Sarah J Johnson, Pharm D
35 All dollars are not equal 1 US $ = 35,000,000,000,000,000 Z $ Quadrillion Zimbabwean dollars
36 Equianalgesic dosing 1 mg iv Morphine = 3 mg of oral Morphine 5 mg oral Morphine = 1 mg oral Dilaudid 5 mg of iv Morphine = 1 mg iv Dilaudid 1mg iv Dilaudid = 5 mg oral Dilaudid 25mcg/ hr Fentanyl patch= 1mg of iv morphine per hour= 50 to 75 mg of oral morphine over 24 hours 10 mg of oral Morphine = 1 mg of oral Methadone
37 Starting/ titrating/ rotating Tramadol 50 mg, Hydrocodone 5/325, Oxycodone 5 mg Reassure that addiction risk minimal if uses appropriately Advise on side effects and duration of action and dose appropriately (every 4 hours/ PRN oral) Bowel program- Miralax and Senna Titrate to goal every 3 to 5 days, follow up every 3 monthspill counts, PMP Use opioid conversion table and reduce dose by 33 to 50% when rotating from one opioid to another
38 6 A s for follow up Analgesia Activities Adverse effects Aberrant behaviors Affect Adherence
39 Pain management agreement One prescriber, one pharmacy Medications to be taken only as prescribed Refill schedule- call several days prior to running out of medication Lost medications/ prescriptions will be replaced at prescriber discretion Be willing to do urine drug testing, memory testing, driving evaluation, psychiatric evaluation as advised by prescriber Renew yearly
40 Screening for opioid misuse ORT- opioid risk tool PDMP- Prescription drug monitoring program SOAPP- Screener and opioid assessment for patients with pain DIRE- Diagnosis, intractability, risk, efficiency instrument UDT- Urine drug test PPA- Patient/ prescriber agreement
41 Arkansas PDMP Statistics 2015 Data: Controlled substance prescription records in the database Prescriber queries Dispenser queries >28 Million 68,000/mo 30,000/mo Law Enforcement queries 254 Regulatory Board queries 311
42 Opioid induced hyperalgesia State of nociceptive sensitization caused by exposure to opioids It is a distinct, definable, and characteristic phenomenon that could explain loss of opioid efficacy in some patients. Paradoxical response whereby a patient receiving opioids for the treatment of pain could actually be worse due to opioids. A comprehensive review of opioid-induced hyperalgesia. Lee M, Silverman SM et al
43 Discontinuing chronic opioid therapy Opioid withdrawal is associated with physical pain, this does not represent progression of underlying disease. Decrease dose by 5 to 10% each visit that patient is ready for dose reductionindividualize plan Taper opioid over several months A. Lembke, Weighing the risks and benefits of chronic opioid therapy; American Family Physician June 15, 2016
44 Substance Use Disorder in the Elderly On an average day in 2011, there were 2,056 drug-related ED visits by older adults, of which 290 involved illegal drug use, alcohol in combination with other drugs, or nonmedical use of pharmaceuticals -118 involved prescription or nonprescription pain relievers, 80 of which involved narcotic pain relievers specified by name (e.g., hydrocodone, oxycodone); -48 involved benzodiazepines -25 involved alcohol in combination with other drugs -23 involved antidepressants or antipsychotics -13 involved cocaine -7 involved heroin -5 involved marijuana -2 involved illicit amphetamines or methamphetamine Source: SAMSHA- Substance Abuse and Mental Health Services Administration
45 Ending the Opioid Epidemic August US Attorney General Dr. Vivek Murthy send 2.3 million letters to US clinicians. October President Trump declared opioid a public health emergency.
46 Who Treats Addiction? Addiction is defined as a disease by most medical associations, including the American Medical Association and the American Society of Addiction Medicine. Addiction and substance abuse should be managed and treated by a team of trained health care professionals, including physicians, psychologists, licensed counselors, social workers, physician assistants, nurses and nurse practitioners who specialize in addiction care. Source: The National Center on Addiction and Substance Abuse
47 Case Conclusion Ms. KM After detailed discussion with Ms. KM, we decided upon goals which included Physical therapy, weight reduction, sleep hygiene, and increased participation in social activities at the assisted living Facility. Opioids were reduced gradually- 10 mg every 3 to 4 months, and she is currently on 30 mg oxycontin bid (started out at 80 mg bid). She is also on Hydrocodone 5/325 tid, Cymbalta 60 mg po daily, and Neurontin 300 mg po tid.
48 Questions?
HOPE. Considerations. Considerations ISING. Safe Opioid Prescribing Guidelines for ACUTE Non-Malignant Pain
 Due to the high level of prescription drug use and abuse in Lake County, these guidelines have been developed to standardize prescribing habits and limit risk of unintended harm when prescribing opioid
Due to the high level of prescription drug use and abuse in Lake County, these guidelines have been developed to standardize prescribing habits and limit risk of unintended harm when prescribing opioid
Knock Out Opioid Abuse in New Jersey:
 Knock Out Opioid Abuse in New Jersey: A Resource for Safer Prescribing GUIDELINE FOR PRESCRIBING OPIOIDS FOR CHRONIC PAIN IMPROVING PRACTICE THROUGH RECOMMENDATIONS CDC s Guideline for Prescribing Opioids
Knock Out Opioid Abuse in New Jersey: A Resource for Safer Prescribing GUIDELINE FOR PRESCRIBING OPIOIDS FOR CHRONIC PAIN IMPROVING PRACTICE THROUGH RECOMMENDATIONS CDC s Guideline for Prescribing Opioids
Opioid Review and MAT Clinic CDC Guidelines
 1 Opioid Review and MAT Clinic CDC Guidelines January 10, 2018 Housekeeping Use chat feature to inform everyone who s at your clinic Click chat on Zoom option bar Chat Everyone the names of those who are
1 Opioid Review and MAT Clinic CDC Guidelines January 10, 2018 Housekeeping Use chat feature to inform everyone who s at your clinic Click chat on Zoom option bar Chat Everyone the names of those who are
The Prescription Review Program and College Expectations. Dr. Rashmi Chadha MBChB MScCH CCFP MRCGP Dip. ABAM
 The Prescription Review Program and College Expectations Dr. Rashmi Chadha MBChB MScCH CCFP MRCGP Dip. ABAM April 28, 2017 Disclosure Relationship with commercial interests: None Professional roles: Addictions
The Prescription Review Program and College Expectations Dr. Rashmi Chadha MBChB MScCH CCFP MRCGP Dip. ABAM April 28, 2017 Disclosure Relationship with commercial interests: None Professional roles: Addictions
CDC Guideline for Prescribing Opioids for Chronic Pain. Centers for Disease Control and Prevention National Center for Injury Prevention and Control
 CDC Guideline for Prescribing Opioids for Chronic Pain Centers for Disease Control and Prevention National Center for Injury Prevention and Control THE EPIDEMIC Chronic Pain and Prescription Opioids 11%
CDC Guideline for Prescribing Opioids for Chronic Pain Centers for Disease Control and Prevention National Center for Injury Prevention and Control THE EPIDEMIC Chronic Pain and Prescription Opioids 11%
New Guidelines for Prescribing Opioids for Chronic Pain
 New Guidelines for Prescribing Opioids for Chronic Pain Andrew Lowe, Pharm.D. CAPA Meeting October 6, 2016 THE EPIDEMIC Chronic Pain and Prescription Opioids 11% of Americans experience daily (chronic)
New Guidelines for Prescribing Opioids for Chronic Pain Andrew Lowe, Pharm.D. CAPA Meeting October 6, 2016 THE EPIDEMIC Chronic Pain and Prescription Opioids 11% of Americans experience daily (chronic)
No disclosures for any of the speakers!
 Opiate Use Disorders and Pain in the elderly: Integrating care with the pain specialist Gabriel Paulian M.D Christopher Ong, M.D Yuliet Sanchez, M.D Uma Suryadevara, M.D No disclosures for any of the speakers!
Opiate Use Disorders and Pain in the elderly: Integrating care with the pain specialist Gabriel Paulian M.D Christopher Ong, M.D Yuliet Sanchez, M.D Uma Suryadevara, M.D No disclosures for any of the speakers!
New Guidelines for Opioid Prescribing
 New Guidelines for Opioid Prescribing What They Mean for Elders with Chronic Pain Manu Thakral, PhD, ARNP Kaiser Permanente Washington Health Research Institute Kaiser Permanente Washington Health Research
New Guidelines for Opioid Prescribing What They Mean for Elders with Chronic Pain Manu Thakral, PhD, ARNP Kaiser Permanente Washington Health Research Institute Kaiser Permanente Washington Health Research
Universal Precautions and Opioid Risk. Assessment. Questions: How often do you screen your patients for risk of misuse when prescribing opioids?
 Learning objectives 1. Identify the contribution of psychosocial and spiritual factors to pain 2. Incorporate strategies for identifying and mitigating opioid misuse 3. Incorporate non-pharmaceutical modalities
Learning objectives 1. Identify the contribution of psychosocial and spiritual factors to pain 2. Incorporate strategies for identifying and mitigating opioid misuse 3. Incorporate non-pharmaceutical modalities
Safe Prescribing of Drugs with Potential for Misuse/Diversion
 College of Physicians and Surgeons of British Columbia Safe Prescribing of Drugs with Potential for Misuse/Diversion Preamble This document establishes both professional standards as well as guidelines
College of Physicians and Surgeons of British Columbia Safe Prescribing of Drugs with Potential for Misuse/Diversion Preamble This document establishes both professional standards as well as guidelines
Opiate Use Disorder and Opiate Overdose
 Opiate Use Disorder and Opiate Overdose Irene Ortiz, MD Medical Director Molina Healthcare of New Mexico and South Carolina Clinical Professor University of New Mexico School of Medicine Objectives DSM-5
Opiate Use Disorder and Opiate Overdose Irene Ortiz, MD Medical Director Molina Healthcare of New Mexico and South Carolina Clinical Professor University of New Mexico School of Medicine Objectives DSM-5
Canadian Guideline for Opioids for Chronic Non-Cancer Pain. Speaker Disclosure. Objectives. Canadian Guideline for Opioids for Chronic Non-Cancer Pain
 Canadian Guideline for Opioids for Chronic Non-Cancer Pain John Fraser Community Hospital Program New Glasgow November 1, 2017 This speaker has been asked to disclose to the audience any involvement with
Canadian Guideline for Opioids for Chronic Non-Cancer Pain John Fraser Community Hospital Program New Glasgow November 1, 2017 This speaker has been asked to disclose to the audience any involvement with
Rule Governing the Prescribing of Opioids for Pain
 Rule Governing the Prescribing of Opioids for Pain 1.0 Authority This rule is adopted pursuant to Sections 14(e) and 11(e) of Act 75 (2013) and Sections 2(e) and 2a of Act 173 (2016). 2.0 Purpose This
Rule Governing the Prescribing of Opioids for Pain 1.0 Authority This rule is adopted pursuant to Sections 14(e) and 11(e) of Act 75 (2013) and Sections 2(e) and 2a of Act 173 (2016). 2.0 Purpose This
Risk Reduction Strategies in Pain Management
 Risk Reduction Strategies in Pain Management Melissa J. Durham, PharmD, MACM, BCACP, DAAPM Assistant Professor of Clinical Pharmacy USC School of Pharmacy Clinical Pharmacist, The USC Pain Center Learning
Risk Reduction Strategies in Pain Management Melissa J. Durham, PharmD, MACM, BCACP, DAAPM Assistant Professor of Clinical Pharmacy USC School of Pharmacy Clinical Pharmacist, The USC Pain Center Learning
Best Practices in Prescribing Opioids for Chronic Non-cancer Pain
 Best Practices in Prescribing Opioids for Chronic Non-cancer Pain Disclosures S C O T T S T E I G E R, M D, F A C P, D A B A M A S S I S T A N T C L I N I C A L P R O F E S S O R D I V I S I O N O F G
Best Practices in Prescribing Opioids for Chronic Non-cancer Pain Disclosures S C O T T S T E I G E R, M D, F A C P, D A B A M A S S I S T A N T C L I N I C A L P R O F E S S O R D I V I S I O N O F G
Palliative and Hospice Care of the Terminally Ill Introduction
 Palliative and Hospice Care of the Terminally Ill Introduction There has been an increase in life expectancy for men and women of all races to 77.6 years Leading causes of death in older patients are chronic
Palliative and Hospice Care of the Terminally Ill Introduction There has been an increase in life expectancy for men and women of all races to 77.6 years Leading causes of death in older patients are chronic
The Prescription Review Program and College Expectations. Dr. Rashmi Chadha MBChB MScCH CCFP MRCGP Dip. ABAM
 The Prescription Review Program and College Expectations Dr. Rashmi Chadha MBChB MScCH CCFP MRCGP Dip. ABAM October 13, 2017 Disclosure Relationship with commercial interests: None Professional roles:
The Prescription Review Program and College Expectations Dr. Rashmi Chadha MBChB MScCH CCFP MRCGP Dip. ABAM October 13, 2017 Disclosure Relationship with commercial interests: None Professional roles:
SAFE PRESCRIBING: RULES AND REGULATIONS. Michelle Y. Owens, MD MS State Board of Medical Licensure June 30, 2017
 SAFE PRESCRIBING: RULES AND REGULATIONS Michelle Y. Owens, MD MS State Board of Medical Licensure June 30, 2017 DISCLOSURES I have no financial disclosures. OBJECTIVES Discuss the significance of the opiate
SAFE PRESCRIBING: RULES AND REGULATIONS Michelle Y. Owens, MD MS State Board of Medical Licensure June 30, 2017 DISCLOSURES I have no financial disclosures. OBJECTIVES Discuss the significance of the opiate
Prescribing drugs of dependence in general practice, Part C
 HO O Prescribing drugs of dependence in general practice, Part C Key recommendations and practice points for management of pain with opioid therapy H H HO N CH3 Acute pain Acute pain is an unpleasant sensory
HO O Prescribing drugs of dependence in general practice, Part C Key recommendations and practice points for management of pain with opioid therapy H H HO N CH3 Acute pain Acute pain is an unpleasant sensory
Overview of Opioid Use Disorder
 Overview of Opioid Use Disorder Doug Burgess, MD Medical Director of Outpatient Services, Truman Medical Centers Assistant Professor of Psychiatry, University of Missouri- Kansas City Objectives History
Overview of Opioid Use Disorder Doug Burgess, MD Medical Director of Outpatient Services, Truman Medical Centers Assistant Professor of Psychiatry, University of Missouri- Kansas City Objectives History
OPIOIDS: THE GOOD, THE BAD, AND EVERYTHING IN-BETWEEN
 OPIOIDS: THE GOOD, THE BAD, AND EVERYTHING IN-BETWEEN ANTOINETTE BROWN, RPH LAUREL RAMER, 2019 PHARMD CANDIDATE 2018 WYOMING CONFERENCE ON AGING LARAMIE, WY OCTOBER 3, 2018 OBJECTIVES 1. Understand the
OPIOIDS: THE GOOD, THE BAD, AND EVERYTHING IN-BETWEEN ANTOINETTE BROWN, RPH LAUREL RAMER, 2019 PHARMD CANDIDATE 2018 WYOMING CONFERENCE ON AGING LARAMIE, WY OCTOBER 3, 2018 OBJECTIVES 1. Understand the
Understanding and Addressing the Public Health Epidemic of Opioid Abuse
 Understanding and Addressing the Public Health Epidemic of Opioid Abuse LEWIS S. NELSON, M.D. PROFESSOR AND CHAIR OF EMERGENCY MEDICINE DIRECTOR, DIVISION OF MEDICAL TOXICOLOGY RUTGERS NEW JERSEY MEDICAL
Understanding and Addressing the Public Health Epidemic of Opioid Abuse LEWIS S. NELSON, M.D. PROFESSOR AND CHAIR OF EMERGENCY MEDICINE DIRECTOR, DIVISION OF MEDICAL TOXICOLOGY RUTGERS NEW JERSEY MEDICAL
Full details and resource documents available:
 Clinical & Regulatory News by Pharmerica Urinary Tract Infection (UTI) Second Most Common Cause of Hospital Readmission within 30 days UTIs are prevalent and account for up to 22% of infections in LTC,
Clinical & Regulatory News by Pharmerica Urinary Tract Infection (UTI) Second Most Common Cause of Hospital Readmission within 30 days UTIs are prevalent and account for up to 22% of infections in LTC,
Practical Tools to Successfully Taper Prescription Opioids. Melissa Weimer, DO, MCR
 Practical Tools to Successfully Taper Prescription Opioids Melissa Weimer, DO, MCR Objectives Understand how to calculate morphine equivalents per day Understand the steps necessary to plan a successful
Practical Tools to Successfully Taper Prescription Opioids Melissa Weimer, DO, MCR Objectives Understand how to calculate morphine equivalents per day Understand the steps necessary to plan a successful
Summary of Recommendations...3. PEG: A Three-Item Scale Assessing Pain (Appendix A) Chronic Pain Flow Sheet Acute Pain Flow Sheet...
 Chronic Pain Flow Sheet Acute Pain Flow Sheet...") Table of Contents Summary of Recommendations....3 PEG: A Three-Item Scale Assessing Pain (Appendix A)...12 Chronic Pain Flow Sheet...13 Acute Pain Flow Sheet...14 Pocket Guide: Tapering Opioids for Chronic
Table of Contents Summary of Recommendations....3 PEG: A Three-Item Scale Assessing Pain (Appendix A)...12 Chronic Pain Flow Sheet...13 Acute Pain Flow Sheet...14 Pocket Guide: Tapering Opioids for Chronic
Prescribing Opioids in the Opioid Epidemic. Scott Woffinden, PA-C Jason Chapman, JD
 Prescribing Opioids in the Opioid Epidemic Scott Woffinden, PA-C Jason Chapman, JD What's the Problem? http://www.zdoggmd.com/blank-script-taylor-swift-parody/ What's the Problem? CDC 115 Americans die
Prescribing Opioids in the Opioid Epidemic Scott Woffinden, PA-C Jason Chapman, JD What's the Problem? http://www.zdoggmd.com/blank-script-taylor-swift-parody/ What's the Problem? CDC 115 Americans die
UCSF Pediatric Hospital Medicine Boot Camp Pain Session 6/21/14. Cynthia Kim and Stephen Wilson
 UCSF Pediatric Hospital Medicine Boot Camp Pain Session 6/21/14 Cynthia Kim and Stephen Wilson Rules Buzz first and player answers If answer correct, then the player asks teammates if they want to keep
UCSF Pediatric Hospital Medicine Boot Camp Pain Session 6/21/14 Cynthia Kim and Stephen Wilson Rules Buzz first and player answers If answer correct, then the player asks teammates if they want to keep
Pain Management at Stony Brook Medicine
 Pain Management at Stony Brook Medicine Pain Management Policy All patients must have effective pain management Appropriate screening and pain assessment Documentation Care and treatment Pain education
Pain Management at Stony Brook Medicine Pain Management Policy All patients must have effective pain management Appropriate screening and pain assessment Documentation Care and treatment Pain education
Addressing the Opioid Epidemic: Prescribing Opioids for Non-Cancer Pain
 Addressing the Opioid Epidemic: Prescribing Opioids for Non-Cancer Pain Ajay D. Wasan, MD, MSc Professor of Anesthesiology and Psychiatry Vice Chair for Pain Medicine, Department of Anesthesiology University
Addressing the Opioid Epidemic: Prescribing Opioids for Non-Cancer Pain Ajay D. Wasan, MD, MSc Professor of Anesthesiology and Psychiatry Vice Chair for Pain Medicine, Department of Anesthesiology University
Pain Management Strategies Webinar/Teleconference
 Pain Management Strategies Webinar/Teleconference Barry K. Baines, MD April 16, 2009 Objectives Describe the principles of pain management. Identify considerations in the use of opioids. Describe the benefits
Pain Management Strategies Webinar/Teleconference Barry K. Baines, MD April 16, 2009 Objectives Describe the principles of pain management. Identify considerations in the use of opioids. Describe the benefits
Responding to the Opioid Epidemic: Behavioral Health Specialists Role on the Interprofessional Team
 Responding to the Opioid Epidemic: Behavioral Health Specialists Role on the Interprofessional Team Cheryl L Mejta, Ph.D. Nancy H Burley, Ed.D. Serena Wadhwa, Psy. D., LCPC, RYT, CADC Objectives Identify
Responding to the Opioid Epidemic: Behavioral Health Specialists Role on the Interprofessional Team Cheryl L Mejta, Ph.D. Nancy H Burley, Ed.D. Serena Wadhwa, Psy. D., LCPC, RYT, CADC Objectives Identify
Opioid Analgesics: Responsible Prescribing in the Midst of an Epidemic
 Opioid Analgesics: Responsible Prescribing in the Midst of an Epidemic Lucas Buffaloe, MD Associate Professor of Clinical Family and Community Medicine University of Missouri Health Care Goals for today
Opioid Analgesics: Responsible Prescribing in the Midst of an Epidemic Lucas Buffaloe, MD Associate Professor of Clinical Family and Community Medicine University of Missouri Health Care Goals for today
April 26, New Mexico Board of Pharmacy Prescription Monitoring Program (PMP) New Mexico Board of Pharmacy Prescription Monitoring Program (PMP)
 New Mexico Board of Pharmacy Prescription Monitoring Program (PMP)") New Mexico Board of Pharmacy Prescription Monitoring Program (PMP) New Mexico Nurse Practitioner Council New Mexico Board of Pharmacy Prescription Monitoring Program (PMP) Peter Ryba, PharmD PMP Director
New Mexico Board of Pharmacy Prescription Monitoring Program (PMP) New Mexico Nurse Practitioner Council New Mexico Board of Pharmacy Prescription Monitoring Program (PMP) Peter Ryba, PharmD PMP Director
Disclosures. Ms. Walsh has nothing to disclose Ms. Broglio is on the speaker s bureau for Genentech and Meda Pharmaceuticals
 Anne F. Walsh, MSN, ANP BC, ACHPN, CWOCN Kathleen Broglio, MN, ANP BC, ACHPN, CPE Disclosures Ms. Walsh has nothing to disclose Ms. Broglio is on the speaker s bureau for Genentech and Meda Pharmaceuticals
Anne F. Walsh, MSN, ANP BC, ACHPN, CWOCN Kathleen Broglio, MN, ANP BC, ACHPN, CPE Disclosures Ms. Walsh has nothing to disclose Ms. Broglio is on the speaker s bureau for Genentech and Meda Pharmaceuticals
9/30/2017. Case Study: Complete Pain Assessment and Multimodal Approach to Pain Management. Program Objectives. Impact of Poorly Managed Pain
 Case Study: Complete Pain Assessment and Multimodal Approach to Pain Management MARY BETH PARTYKA MSN ADULT NURSE PRACTITIONER ADVOCATE CHRIST MEDICAL CENTER ADULT PAIN SERVICE Program Objectives Identify
Case Study: Complete Pain Assessment and Multimodal Approach to Pain Management MARY BETH PARTYKA MSN ADULT NURSE PRACTITIONER ADVOCATE CHRIST MEDICAL CENTER ADULT PAIN SERVICE Program Objectives Identify
SUMMARY OF ARIZONA OPIOID PRESCRIBING GUIDELINES FOR THE TREATMENT OF CHRONIC NON-TERMINAL PAIN (CNTP)
") 9 SUMMARY OF ARIZONA OPIOID PRESCRIBING GUIDELINES FOR THE TREATMENT OF CHRONIC NON-TERMINAL PAIN (CNTP) SUMMARY OF ARIZONA OPIOID PRESCRIBING GUIDELINES FOR THE TREATMENT OF ACUTE PAIN NONOPIOID TREATMENTS
9 SUMMARY OF ARIZONA OPIOID PRESCRIBING GUIDELINES FOR THE TREATMENT OF CHRONIC NON-TERMINAL PAIN (CNTP) SUMMARY OF ARIZONA OPIOID PRESCRIBING GUIDELINES FOR THE TREATMENT OF ACUTE PAIN NONOPIOID TREATMENTS
Tennessee. Prescribing and Dispensing Profile. Research current through November 2015.
 Prescribing and Dispensing Profile Tennessee Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points
Prescribing and Dispensing Profile Tennessee Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points
Overview of Essentials of Pain Management. Updated 11/2016
 0 Overview of Essentials of Pain Management Updated 11/2016 1 Overview of Essentials of Pain Management 1. Assess pain intensity on a 0 10 scale in which 0 = no pain at all and 10 = the worst pain imaginable.
0 Overview of Essentials of Pain Management Updated 11/2016 1 Overview of Essentials of Pain Management 1. Assess pain intensity on a 0 10 scale in which 0 = no pain at all and 10 = the worst pain imaginable.
Approaches to Responsible Opioid Prescribing. The Opioid Naïve Patient
 Approaches to Responsible Opioid Prescribing The Opioid Naïve Patient Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
Approaches to Responsible Opioid Prescribing The Opioid Naïve Patient Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
ten questions you might have about tapering (and room for your own) an informational booklet for opioid pain treatment
 an informational booklet for opioid pain treatment") ten questions you might have about tapering (and room for your own) an informational booklet for opioid pain treatment This booklet was created to help you learn about tapering. You probably have lots
ten questions you might have about tapering (and room for your own) an informational booklet for opioid pain treatment This booklet was created to help you learn about tapering. You probably have lots
Nociceptive Pain. Pathophysiologic Pain. Types of Pain. At Presentation. At Presentation. Nonpharmacologic Therapy. Modulation
 Learning Objectives Effective, Safe Analgesia An Approach to Appropriate Outpatient Chronic Pain Treatment By the end of this presentation, participants will be able to: Identify multiple factors that
Learning Objectives Effective, Safe Analgesia An Approach to Appropriate Outpatient Chronic Pain Treatment By the end of this presentation, participants will be able to: Identify multiple factors that
THE PROS & CONS OF THE CDC GUIDELINES FOR SAFE OPIOID PRESCRIBING
 THE PROS & CONS OF THE CDC GUIDELINES FOR SAFE OPIOID PRESCRIBING Ernest J Dole, PharmD, PhC, FASHP, BCPS Clinical Pharmacist University of New Mexico Hospitals And Clinical Associate Professor University
THE PROS & CONS OF THE CDC GUIDELINES FOR SAFE OPIOID PRESCRIBING Ernest J Dole, PharmD, PhC, FASHP, BCPS Clinical Pharmacist University of New Mexico Hospitals And Clinical Associate Professor University
NBPDP Drug Utilization Review Process Update
 Bulletin # 802 December 1, 2010 NBPDP Drug Utilization Review Process Update The New Brunswick Prescription Drug Program (NBPDP) employs a Drug Utilization Review (DUR) process which identifies, investigates
Bulletin # 802 December 1, 2010 NBPDP Drug Utilization Review Process Update The New Brunswick Prescription Drug Program (NBPDP) employs a Drug Utilization Review (DUR) process which identifies, investigates
Prescription Opioid Addiction
 CSAM-SCAM Fundamentals Prescription Opioid Addiction Presentation provided by Meldon Kahan, MD Family & Community Medicine University of Toronto Conflict of interest statement I received funds from Rickett
CSAM-SCAM Fundamentals Prescription Opioid Addiction Presentation provided by Meldon Kahan, MD Family & Community Medicine University of Toronto Conflict of interest statement I received funds from Rickett
Pain, Opioids, & Substance Use Disorders
 Pain, Opioids, & Substance Use Disorders Kenny Jackson, PharmD, CPE Professor & Senior Associate Dean for Academic Affairs College of Pharmacy Larkin University Miami, Florida Editor-in-Chief Journal of
Pain, Opioids, & Substance Use Disorders Kenny Jackson, PharmD, CPE Professor & Senior Associate Dean for Academic Affairs College of Pharmacy Larkin University Miami, Florida Editor-in-Chief Journal of
POST OPERATIVE PAIN MANAGEMENT: PAIN AND COMPLICATIONS
 POST OPERATIVE PAIN MANAGEMENT: PAIN AND COMPLICATIONS November 9, 2018 Aimee LaMere, CNP Molly McNaughton, CNP Leslie Weide, MSW, LICSW, ACM Disclosures: Conflict of interest statement: We certify that,
POST OPERATIVE PAIN MANAGEMENT: PAIN AND COMPLICATIONS November 9, 2018 Aimee LaMere, CNP Molly McNaughton, CNP Leslie Weide, MSW, LICSW, ACM Disclosures: Conflict of interest statement: We certify that,
Sharon A Stephen, PhD, ARNP, ACHPN. September 23, 2014
 Sharon A Stephen, PhD, ARNP, ACHPN September 23, 2014 Case-based presentation selected to discuss: Pain assessment Barriers to adequate pain relief Pharmacologic interventions Non-Pharmacologic interventions
Sharon A Stephen, PhD, ARNP, ACHPN September 23, 2014 Case-based presentation selected to discuss: Pain assessment Barriers to adequate pain relief Pharmacologic interventions Non-Pharmacologic interventions
Opioids: Use and Misuse/Steven Feinberg, MD; Scott Levy, MD, MPH, FACOEM
 Western Occupational Health Conference September 14, 2012 Opioid - Use & Misuse Scott Levy, MD MPH FACOEM Steven Feinberg, MD, MPH Disclosure Information Western Occupational Health Conference 2012 Steven
Western Occupational Health Conference September 14, 2012 Opioid - Use & Misuse Scott Levy, MD MPH FACOEM Steven Feinberg, MD, MPH Disclosure Information Western Occupational Health Conference 2012 Steven
PROVIDER BULLETIN. Published by Wyoming Workers Compensation Medical Case Management Unit October 21, 2015
 Matthew H. Mead Governor State of Wyoming Department of Workforce Services DIVISION OF WORKERS COMPENSATION 1510 East Pershing Boulevard, South Wing Cheyenne, Wyoming 82002 http://www.wyomingworkforce.org
Matthew H. Mead Governor State of Wyoming Department of Workforce Services DIVISION OF WORKERS COMPENSATION 1510 East Pershing Boulevard, South Wing Cheyenne, Wyoming 82002 http://www.wyomingworkforce.org
Disclosures. Management of Chronic, Non- Terminal Pain. Learning Objectives. Outline. Drug Schedules. Applicable State Laws
 Disclosures Management of Chronic, Non- Terminal Pain No financial disclosures or conflicts of interest to report Michael A. Smith, PharmD, BCPS Clinical Assistant Professor, University of Michigan College
Disclosures Management of Chronic, Non- Terminal Pain No financial disclosures or conflicts of interest to report Michael A. Smith, PharmD, BCPS Clinical Assistant Professor, University of Michigan College
D. Janene Holladay, M.D. Board Certifications: American Board of Anesthesiology American Board of Pain Medicine American Board of Addiction Medicine
 D. Janene Holladay, M.D. Board Certifications: American Board of Anesthesiology American Board of Pain Medicine American Board of Addiction Medicine Financial Disclosure I have no relevant financial relationships
D. Janene Holladay, M.D. Board Certifications: American Board of Anesthesiology American Board of Pain Medicine American Board of Addiction Medicine Financial Disclosure I have no relevant financial relationships
Subject: Pain Management (Page 1 of 7)
") Subject: Pain Management (Page 1 of 7) Objectives: Managing pain and restoring function are basic goals in helping a patient with chronic non-cancer pain. Federal and state guidelines require that all
Subject: Pain Management (Page 1 of 7) Objectives: Managing pain and restoring function are basic goals in helping a patient with chronic non-cancer pain. Federal and state guidelines require that all
Medication Management
 Marina Treglia, AGPCNP BC April 4, 2019 Medication Management Identify patient criteria for risk mitigation in a medication management program at a multidisciplinary pain clinic Discuss opioid discontinuation
Marina Treglia, AGPCNP BC April 4, 2019 Medication Management Identify patient criteria for risk mitigation in a medication management program at a multidisciplinary pain clinic Discuss opioid discontinuation
Pain Management Wrap-Up Chronic Care. David Tauben, MD Medicine Anesthesia & Pain Medicine
 Pain Management Wrap-Up Chronic Care David Tauben, MD Medicine Anesthesia & Pain Medicine Objectives Understand that Pain is Complex Know how to select Rx based on Pain type Be aware that Rx only reduces
Pain Management Wrap-Up Chronic Care David Tauben, MD Medicine Anesthesia & Pain Medicine Objectives Understand that Pain is Complex Know how to select Rx based on Pain type Be aware that Rx only reduces
Virginia. Prescribing and Dispensing Profile. Research current through November 2015.
 Prescribing and Dispensing Profile Virginia Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points
Prescribing and Dispensing Profile Virginia Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points
Management of Pain - A Comparison of Current Guidelines
 Management of Pain - A Comparison of Current Guidelines The Centers for Disease Control and Prevention (CDC) released a guideline in 2016 regarding the prescribing of opioids for chronic non-cancer pain
Management of Pain - A Comparison of Current Guidelines The Centers for Disease Control and Prevention (CDC) released a guideline in 2016 regarding the prescribing of opioids for chronic non-cancer pain
Opioid Management of Chronic (Non- Cancer) Pain
 Pain") Optima Health Opioid Management of Chronic (Non- Cancer) Pain Guideline History Original Approve Date 5/08 Review/Revise Dates 11/09, 9/11, 9/13, 09/15, 9/17 Next Review Date 9/19 These Guidelines are
Optima Health Opioid Management of Chronic (Non- Cancer) Pain Guideline History Original Approve Date 5/08 Review/Revise Dates 11/09, 9/11, 9/13, 09/15, 9/17 Next Review Date 9/19 These Guidelines are
NEUROPATHIC CANCER PAIN STANDARDS AND GUIDELINES
 NEUROPATHIC CANCER PAIN STANDARDS AND GUIDELINES GENERAL PRINCIPLES Neuropathic pain may be relieved in the majority of patients by multimodal management A careful history and examination are essential.
NEUROPATHIC CANCER PAIN STANDARDS AND GUIDELINES GENERAL PRINCIPLES Neuropathic pain may be relieved in the majority of patients by multimodal management A careful history and examination are essential.
Scope of the Opiate Problem 6/5/18. Chronic Pain Management and the Use of Opioid Medications: The CDC Guideline and Beyond. Overview.
 Chronic Pain Management and the Use of Opioid Medications: The CDC Guideline and Beyond David Anisman, MD Medical Director, Farmington Health Center (Primary Care) Associate Medical Director, Community
Chronic Pain Management and the Use of Opioid Medications: The CDC Guideline and Beyond David Anisman, MD Medical Director, Farmington Health Center (Primary Care) Associate Medical Director, Community
Module 2 Pain Management. Handouts. Pain Is... Please click the links button under the video. You can print and/or save the handouts.
 E L N E C End-of-Life Nursing Education Consortium SuperCore Curriculum Module 2 Pain Management Handouts Please click the links button under the video. You can print and/or save the handouts. Pain Is...
E L N E C End-of-Life Nursing Education Consortium SuperCore Curriculum Module 2 Pain Management Handouts Please click the links button under the video. You can print and/or save the handouts. Pain Is...
Medical Assisted Treatment. Dr. Michael Baldinger Medical Director Haymarket Center Harborview Recovery Center
 Medical Assisted Treatment Dr. Michael Baldinger Medical Director Haymarket Center Harborview Recovery Center Current Trends Prescription Drug Abuse/Addiction Non-medical use of prescription pain killers
Medical Assisted Treatment Dr. Michael Baldinger Medical Director Haymarket Center Harborview Recovery Center Current Trends Prescription Drug Abuse/Addiction Non-medical use of prescription pain killers
California. Prescribing and Dispensing Profile. Research current through November 2015.
 Prescribing and Dispensing Profile California Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points
Prescribing and Dispensing Profile California Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points
Objectives: What is your Definition of Pain? 8/16/2017
 Safe Opioid Management for the Seriously Ill Patient Sam Perna, D.O. Objectives: MDB1 1) Participants will understand the way the body s pain system works. 2) Participants will identify the elements of
Safe Opioid Management for the Seriously Ill Patient Sam Perna, D.O. Objectives: MDB1 1) Participants will understand the way the body s pain system works. 2) Participants will identify the elements of
CDC Guideline for Prescribing Opioids for Chronic Pain
 National Center for Injury Prevention and Control CDC Guideline for Prescribing Opioids for Chronic Pain John Halpin, MD, MPH Medical Officer Division of Unintentional Injury Prevention Prescription Drug
National Center for Injury Prevention and Control CDC Guideline for Prescribing Opioids for Chronic Pain John Halpin, MD, MPH Medical Officer Division of Unintentional Injury Prevention Prescription Drug
Chronic Pain Pharmacist role in the clinic
 Chronic Pain Pharmacist role in the clinic WSPA Annual Meeting 2015 Alvin Goo, PharmD Clinical Associate Professor University of Washington Schools of Pharmacy and Family Medicine Speakers Declaration
Chronic Pain Pharmacist role in the clinic WSPA Annual Meeting 2015 Alvin Goo, PharmD Clinical Associate Professor University of Washington Schools of Pharmacy and Family Medicine Speakers Declaration
PAIN TERMINOLOGY TABLE
 PAIN TERMINOLOGY TABLE TERM DEFINITION HOW TO USE CLINICALLY Acute Pain Pain that is usually temporary and results from something specific, such as a surgery, an injury, or an infection Addiction A chronic
PAIN TERMINOLOGY TABLE TERM DEFINITION HOW TO USE CLINICALLY Acute Pain Pain that is usually temporary and results from something specific, such as a surgery, an injury, or an infection Addiction A chronic
An unpleasant sensory and emotional experience associated with actual or potential tissue damage.
 An unpleasant sensory and emotional experience associated with actual or potential tissue damage. Acute Pain results from disease, inflammation or injury to tissues; generally comes on suddenly and may
An unpleasant sensory and emotional experience associated with actual or potential tissue damage. Acute Pain results from disease, inflammation or injury to tissues; generally comes on suddenly and may
Update on Pain: Collaborative Care for the Complex Patient
 Update on Pain: Collaborative Care for the Complex Patient Nirmala R. Abraham, MD Medical Director Sycamore Pain Management Center Kettering Health Network Objectives Standardized approach to patient care
Update on Pain: Collaborative Care for the Complex Patient Nirmala R. Abraham, MD Medical Director Sycamore Pain Management Center Kettering Health Network Objectives Standardized approach to patient care
Canadian Guideline for Opioids for Chronic Non-Cancer Pain. Speaker Disclosure. Objectives. Canadian Guideline for Opioids for Chronic Non-Cancer Pain
 Canadian Guideline for Opioids for Chronic Non-Cancer Pain John Fraser Community Hospital Program North Sydney April 12, 2018 This speaker has been asked to disclose to the audience any involvement with
Canadian Guideline for Opioids for Chronic Non-Cancer Pain John Fraser Community Hospital Program North Sydney April 12, 2018 This speaker has been asked to disclose to the audience any involvement with
OCCUPATIONAL AND PROFESSIONAL LICENSING MEDICINE AND SURGERY PRACTITIONERS MANAGEMENT OF PAIN AND OTHER CONDITIONS WITH CONTROLLED SUBSTANCES
 TITLE 16 CHAPTER 10 PART 14 OCCUPATIONAL AND PROFESSIONAL LICENSING MEDICINE AND SURGERY PRACTITIONERS MANAGEMENT OF PAIN AND OTHER CONDITIONS WITH CONTROLLED SUBSTANCES 16.10.14.1 ISSUING AGENCY: New
TITLE 16 CHAPTER 10 PART 14 OCCUPATIONAL AND PROFESSIONAL LICENSING MEDICINE AND SURGERY PRACTITIONERS MANAGEMENT OF PAIN AND OTHER CONDITIONS WITH CONTROLLED SUBSTANCES 16.10.14.1 ISSUING AGENCY: New
OPIOID CRISIS: A PERSPECTIVE. Karl J. Haake, MD
 OPIOID CRISIS: A PERSPECTIVE Karl J. Haake, MD LEARNING OBJECTIVES Summarize the history behind the opioid epidemic in America Identify the issues surrounding the the treatment of chronic pain Demonstrate
OPIOID CRISIS: A PERSPECTIVE Karl J. Haake, MD LEARNING OBJECTIVES Summarize the history behind the opioid epidemic in America Identify the issues surrounding the the treatment of chronic pain Demonstrate
Opioid use in older adults Is it a good idea? Regional Geriatric Rounds April 26, 2013
 Opioid use in older adults Is it a good idea? Regional Geriatric Rounds April 26, 2013 Allen R. Huang, MDCM, FRCPC, FACP, AGSF Division of Geriatric Medicine allenhuang@toh.on.ca I have no conflict of
Opioid use in older adults Is it a good idea? Regional Geriatric Rounds April 26, 2013 Allen R. Huang, MDCM, FRCPC, FACP, AGSF Division of Geriatric Medicine allenhuang@toh.on.ca I have no conflict of
Approved Procedures for Prescribing and Monitoring Controlled Substances in South Carolina
 Approved Procedures for Prescribing and Monitoring Controlled Substances in South Carolina Robert B. Hanlin, M.D., FAAFP Vice Chair, Medical Staff Affairs Greenville Health System Greenville, SC Disclosures
Approved Procedures for Prescribing and Monitoring Controlled Substances in South Carolina Robert B. Hanlin, M.D., FAAFP Vice Chair, Medical Staff Affairs Greenville Health System Greenville, SC Disclosures
Opioid Use Disorder. A Telligen White Paper. Katy Brown, PharmD Clinical Pharmacy Specialist
 Opioid Use Disorder A Telligen White Paper Katy Brown, PharmD Clinical Pharmacy Specialist Opioid Use Disorder The use and misuse of opioids has steadily increased since the late 1990 s. When used as prescribed,
Opioid Use Disorder A Telligen White Paper Katy Brown, PharmD Clinical Pharmacy Specialist Opioid Use Disorder The use and misuse of opioids has steadily increased since the late 1990 s. When used as prescribed,
Opioid Induced Hyperalgesia (OIH)
") Opioid Induced Hyperalgesia (OIH) How to Receive Your CE Credits Read your selected course Completed the quiz at the end of the course with a 70% or greater. Complete the evaluation for your selected course.
Opioid Induced Hyperalgesia (OIH) How to Receive Your CE Credits Read your selected course Completed the quiz at the end of the course with a 70% or greater. Complete the evaluation for your selected course.
1/30/2017 SEISMIC UPGRADE FOR THE OPIOID PARADIGM SHIFT ACPE PRE-TEST QUESTIONS. I have no declarations.
 SEISMIC UPGRADE FOR THE OPIOID PARADIGM SHIFT Traci Hamer, PharmD, MAT Kaiser Permanente Northwest Pain Management Pharmacy Services I have no declarations. ACPE PRE-TEST QUESTIONS True/False: Opioids
SEISMIC UPGRADE FOR THE OPIOID PARADIGM SHIFT Traci Hamer, PharmD, MAT Kaiser Permanente Northwest Pain Management Pharmacy Services I have no declarations. ACPE PRE-TEST QUESTIONS True/False: Opioids
3/3/2015 CHRONIC PAIN MARGARET ZOELLERS, MSN, APRN
 CHRONIC PAIN MARGARET ZOELLERS, MSN, APRN 1 Pain that persists or recurs > 3-6 months Pain that persists >1 month after injury/event Commonly seems out of proportion to the physical process Cause may be
CHRONIC PAIN MARGARET ZOELLERS, MSN, APRN 1 Pain that persists or recurs > 3-6 months Pain that persists >1 month after injury/event Commonly seems out of proportion to the physical process Cause may be
PART VI: TAPERING OPIOIDS ROBERT JENKINSON MD MARCH 7, 2018
 PART VI: TAPERING OPIOIDS ROBERT JENKINSON MD MARCH 7, 2018 TAPERING OPIOIDS GETTING STARTED ON OPIOIDS IS EASY BUT GETTING PATIENTS OFF IS HARD WE ARE ARE OBLIGED TO TAPER PATIENTS DOWN AND OFF OPIOIDS
PART VI: TAPERING OPIOIDS ROBERT JENKINSON MD MARCH 7, 2018 TAPERING OPIOIDS GETTING STARTED ON OPIOIDS IS EASY BUT GETTING PATIENTS OFF IS HARD WE ARE ARE OBLIGED TO TAPER PATIENTS DOWN AND OFF OPIOIDS
Acute Pain NETP: SEPTEMBER 2013 COHORT
 Acute Pain NETP: SEPTEMBER 2013 COHORT Pain & Suffering an unpleasant sensory & emotional experience associated with actual or potential tissue damage, or described in terms of such damage International
Acute Pain NETP: SEPTEMBER 2013 COHORT Pain & Suffering an unpleasant sensory & emotional experience associated with actual or potential tissue damage, or described in terms of such damage International
Practical Pain Management Leah Centanni, MSN, FNP-C, Asst. Clinical Professor CANP Conference March 22, 2014
 Practical Pain Management Leah Centanni, MSN, FNP-C, Asst. Clinical Professor CANP Conference March 22, 2014 Overview Types of Pain Physical Examination of Pain Pharmacologic Approach in Pain Management
Practical Pain Management Leah Centanni, MSN, FNP-C, Asst. Clinical Professor CANP Conference March 22, 2014 Overview Types of Pain Physical Examination of Pain Pharmacologic Approach in Pain Management
Acute Pain Management in the Hospital Setting. Alexandra Phan, PharmD PGY-1 Pharmacy Practice Resident Medical Center Hospital Odessa, TX
 Acute Pain Management in the Hospital Setting Alexandra Phan, PharmD PGY-1 Pharmacy Practice Resident Medical Center Hospital Odessa, TX 2 What is Pain? An unpleasant sensory and emotional experience associated
Acute Pain Management in the Hospital Setting Alexandra Phan, PharmD PGY-1 Pharmacy Practice Resident Medical Center Hospital Odessa, TX 2 What is Pain? An unpleasant sensory and emotional experience associated
Narcotic Analgesics. Jacqueline Morgan March 22, 2017
 Narcotic Analgesics Jacqueline Morgan March 22, 2017 Pain Unpleasant sensory and emotional experience with actual or potential tissue damage Universal, complex, subjective experience Number one reason
Narcotic Analgesics Jacqueline Morgan March 22, 2017 Pain Unpleasant sensory and emotional experience with actual or potential tissue damage Universal, complex, subjective experience Number one reason
Managing Pain in Individuals with Serious Illness and Comorbid Substance Use Disorder
 Managing Pain in Individuals with Serious Illness and Comorbid Substance Use Disorder Presented by: Kathleen Broglio, DNP, ANP-BC, ACHPN, CPE, FPCN on December 1, 2016 Webcast Questions and Answers (Answers
Managing Pain in Individuals with Serious Illness and Comorbid Substance Use Disorder Presented by: Kathleen Broglio, DNP, ANP-BC, ACHPN, CPE, FPCN on December 1, 2016 Webcast Questions and Answers (Answers
Addressing Alaska s Opioid Epidemic From Understanding to Action
 Addressing Alaska s Opioid Epidemic From Understanding to Action The opioid epidemic is devastating American families and communities. To curb these trends and save lives, we must help prevent addiction
Addressing Alaska s Opioid Epidemic From Understanding to Action The opioid epidemic is devastating American families and communities. To curb these trends and save lives, we must help prevent addiction
Treatment of Pain in an Emergent Setting
 Updated: October 22, 2018 Prescribing Guidelines for Pennsylvania Treatment of Pain in an Emergent Setting Opioids, including heroin and fentanyl, contribute to thousands of overdose deaths in Pennsylvania
Updated: October 22, 2018 Prescribing Guidelines for Pennsylvania Treatment of Pain in an Emergent Setting Opioids, including heroin and fentanyl, contribute to thousands of overdose deaths in Pennsylvania
INFORMED CONSENT FOR OPIOID TREATMENT FOR NON-CANCER/CANCER PAIN Texas Pain and Regenerative Medicine
 INFORMED CONSENT FOR OPIOID TREATMENT FOR NON-CANCER/CANCER PAIN Texas Pain and Regenerative Medicine The purpose of this agreement is to give you information about the medications you will be taking for
INFORMED CONSENT FOR OPIOID TREATMENT FOR NON-CANCER/CANCER PAIN Texas Pain and Regenerative Medicine The purpose of this agreement is to give you information about the medications you will be taking for
BASICS OF OPIOID PRESCRIBING 10:30-11:45AM
 PROVIDING QUALITY CARE TO PAIN PATIENTS IN IOWA BASICS OF OPIOID PRESCRIBING 10:30-11:45AM ACPE UAN: 107-000-14-013-L01-P Activity Type: Application-Based 0.125 CEU/1.25hr Learning Objectives for Pharmacists:
PROVIDING QUALITY CARE TO PAIN PATIENTS IN IOWA BASICS OF OPIOID PRESCRIBING 10:30-11:45AM ACPE UAN: 107-000-14-013-L01-P Activity Type: Application-Based 0.125 CEU/1.25hr Learning Objectives for Pharmacists:
ScO.S. Academic Detailing for Safer Prescribing
 ScO.S. Academic Detailing for Safer Prescribing Sarah Ball, PharmD Research Assistant Professor MUSC College of Medicine September 6, 2017 Megan Pruitt, PharmD SCORxE Clinical Pharmacy Consultant MUSC
ScO.S. Academic Detailing for Safer Prescribing Sarah Ball, PharmD Research Assistant Professor MUSC College of Medicine September 6, 2017 Megan Pruitt, PharmD SCORxE Clinical Pharmacy Consultant MUSC
Recommendations in Opioid Prescribing Guidelines for Chronic Pain
 Recommendations in Opioid Prescribing Guidelines for Chronic Pain The use of opioids for treating chronic pain has been increasing. 1 In 2010, an estimated 20% of patients presenting to physician offices
Recommendations in Opioid Prescribing Guidelines for Chronic Pain The use of opioids for treating chronic pain has been increasing. 1 In 2010, an estimated 20% of patients presenting to physician offices
PALLIATIVE TREATMENT BY DR. KHRONGKAMOL SIHABAN MEDICAL ONCOLOGIST
 PALLIATIVE TREATMENT BY DR. KHRONGKAMOL SIHABAN MEDICAL ONCOLOGIST TREATMENT IN ONCOLOGY Main treatment : surgery Neoadjuvant treatment : RT, CMT Adjuvant treatment : Tx micrometastatic disease -CMT,Targeted
PALLIATIVE TREATMENT BY DR. KHRONGKAMOL SIHABAN MEDICAL ONCOLOGIST TREATMENT IN ONCOLOGY Main treatment : surgery Neoadjuvant treatment : RT, CMT Adjuvant treatment : Tx micrometastatic disease -CMT,Targeted
Taking Opioids Responsibly for Your Safety and the Safety of Others: Patient Information Guide on Long-term Opioid Therapy for Chronic Pain
 Taking Opioids Responsibly for Your Safety and the Safety of Others: Patient Information Guide on Long-term Opioid Therapy for Chronic Pain Department of Veterans Affairs (VA) and Department of Defense
Taking Opioids Responsibly for Your Safety and the Safety of Others: Patient Information Guide on Long-term Opioid Therapy for Chronic Pain Department of Veterans Affairs (VA) and Department of Defense
Pharmacy Law Disclosure Statement. Objectives 6/11/2016. I have no conflicts of interest to disclose related to this presentation.
 Pharmacy Law 2016 Ronda H. Lacey, J.D., M.S. Pharm Disclosure Statement I have no conflicts of interest to disclose related to this presentation. Objectives At the conclusion of this continuing education
Pharmacy Law 2016 Ronda H. Lacey, J.D., M.S. Pharm Disclosure Statement I have no conflicts of interest to disclose related to this presentation. Objectives At the conclusion of this continuing education
Opioids drive continued increase in drug overdose deaths
 CDC: Drug overdose deaths increase for 11th consecutive year Opioids drive continued increase in drug overdose deaths Atlanta, GA, USA (February 20, 2013) - Drug overdose deaths increased for the 11th
CDC: Drug overdose deaths increase for 11th consecutive year Opioids drive continued increase in drug overdose deaths Atlanta, GA, USA (February 20, 2013) - Drug overdose deaths increased for the 11th
Analgesia for Patients with Substance Abuse Disorders. Lisa Jennings CN November 2015
 Analgesia for Patients with Substance Abuse Disorders Lisa Jennings CN November 2015 Definitions n Addiction: A pattern of drug use characterised by aberrant drug-taking behaviours & the compulsive use
Analgesia for Patients with Substance Abuse Disorders Lisa Jennings CN November 2015 Definitions n Addiction: A pattern of drug use characterised by aberrant drug-taking behaviours & the compulsive use
Legal Issues in Opioid Prescribing
 Legal Issues in Opioid Prescribing Joanne L. Martin, J.D. Legal Counsel Mayo Clinic Rochester, Mn 2015 MFMER slide-1 Conflict of Interest I have no relevant financial relationships to disclose I will not
Legal Issues in Opioid Prescribing Joanne L. Martin, J.D. Legal Counsel Mayo Clinic Rochester, Mn 2015 MFMER slide-1 Conflict of Interest I have no relevant financial relationships to disclose I will not
(Adapted with permission from the D-H Knowledge Map Primary Care Buprenorphine Guidelines)
") Buprenorphine Initiation and Maintenance in Pregnancy (Adapted with permission from the D-H Knowledge Map Primary Care Buprenorphine Guidelines) Assessment The diagnosis of OUD should be confirmed by DSM-5
Buprenorphine Initiation and Maintenance in Pregnancy (Adapted with permission from the D-H Knowledge Map Primary Care Buprenorphine Guidelines) Assessment The diagnosis of OUD should be confirmed by DSM-5
July We hope that our tool will be a useful aid in your efforts to improve pain management in your setting. Sincerely, 7/14
 July 2014 he Knowledge and Attitudes Survey Regarding Pain tool can be used to assess nurses and other professionals in your setting and as a pre and post test evaluation measure for educational programs.
July 2014 he Knowledge and Attitudes Survey Regarding Pain tool can be used to assess nurses and other professionals in your setting and as a pre and post test evaluation measure for educational programs.
Pain Management and Safe use of opioids in hospitals. Kyoung-Sil Kang, PharmD, BCPS Scott Tam, PharmD Lauve Casimir, RN, MSN
 Pain Management and Safe use of opioids in hospitals Kyoung-Sil Kang, PharmD, BCPS Scott Tam, PharmD Lauve Casimir, RN, MSN Bronx Care Health System Bronx Lebanon Hospital Concourse/ Fulton division, Nursing
Pain Management and Safe use of opioids in hospitals Kyoung-Sil Kang, PharmD, BCPS Scott Tam, PharmD Lauve Casimir, RN, MSN Bronx Care Health System Bronx Lebanon Hospital Concourse/ Fulton division, Nursing
Pain Assessment & Management. For General Nursing Orientation
 Pain Assessment & Management For General Nursing Orientation April 2012 Overview Definition of pain Barriers to effective pain management Types of pain Objective pain assessment Approaches to management
Pain Assessment & Management For General Nursing Orientation April 2012 Overview Definition of pain Barriers to effective pain management Types of pain Objective pain assessment Approaches to management
Responding to The Joint Commission Alert on Safe Use of Opioids in Hospitals
 Responding to The Joint Commission Alert on Safe Use of Opioids in Hospitals Suzanne A Nesbit, PharmD, CPE Clinical Pharmacy Specialist, Pain Management The Johns Hopkins Hospital Objectives and Disclosures
Responding to The Joint Commission Alert on Safe Use of Opioids in Hospitals Suzanne A Nesbit, PharmD, CPE Clinical Pharmacy Specialist, Pain Management The Johns Hopkins Hospital Objectives and Disclosures