Diseases of the liver. Morphology and general pathology M.O. Mavlikeev
|
|
|
- Hope Poole
- 5 years ago
- Views:
Transcription

1 Diseases of the liver Morphology and general pathology M.O. Mavlikeev
2 Diseases of the liver The greatest value in human pathology are: Hepatoses Hepatitis Cirrhosis of the liver Liver cancer.
3 Hepatoses A group of liver diseases, which are based on degeneration and necrosis of hepatocytes. Hepatoses are: Hereditary, Acquired: Acute: Massive progressive necrosis of the liver (old name "toxic liver dystrophy") Chronic: Fatty hepatosis (steatosis of the liver).
4 Massive progressive liver necrosis (MPLN) A disease in which large foci of necrosis appear in the liver tissue. Clinically manifested by hepatocellular insufficiency syndrome. Causes of the MPLN: The main significance is the effect of toxic substances: Exogenous origin (fungi, food toxins, arsenic), Endogenous origin (toxicosis of pregnant women - gestosis, thyrotoxicosis).
5 Morphology of MPLN The following stages of MPLN are distinguished: Stage of yellow dystrophy, Stage of red dystrophy.
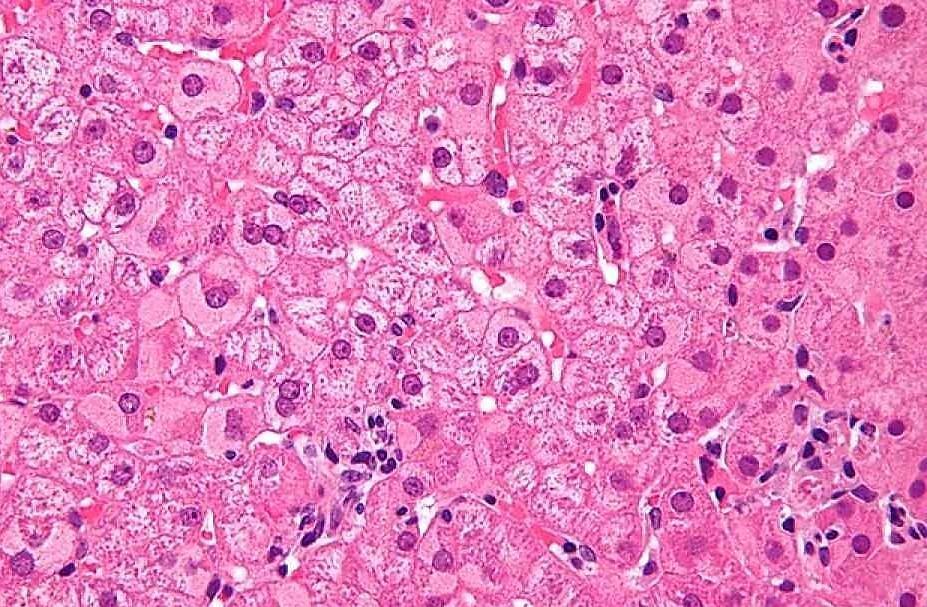
6 Stage of yellow dystrophy It flows in the first week of the disease. Macroscopic picture: The liver is enlarged in size, yellow color, flabby consistency. Microscopic picture: In the hepatocytes of the central parts of the hepatic lobules, foci of necrosis (fat-protein detritus), various in area, on the periphery of the lobules of hepatocytes in a state of fatty dystrophy.

7 Stage of yellow dystrophy of MPLN

8 Stage of yellow dystrophy of MPLN
9 Stage of red dystrophy Occurs in the third week of the disease. Macroscopic picture: The liver is reduced in size, red. Microscopic picture: Fat-protein detritus undergoes resorption, it is leads to baring of thin reticular stroma of the lobules and full-blooded sinusoids; The reticular system collapses, the stroma collapses, all the remaining parts of the lobes converge.
10 Outcomes of MPLN Patients die due to a hepatic coma or from liver-kidney failure. If patients survive, then postnecrotic cirrhosis develops.
11 Fatty hepatosis Chronic disease, in which neutral fat accumulates in hepatocytes in the form of small and large drops. Etiology of fatty hepatosis: Long-term toxic effects on the liver (alcohol, drugs), Disorders of metabolism in diabetes mellitus, Hypoxia of various genesis (anemia), Defective protein nutrition / starvation, Excessive use of fat, General obesity.
12 Morphology of fatty hepatosis Macroscopic picture: The liver is sharply enlarged, Flabby consistency, Ocher-yellow color, The surface of the liver is smooth. Microscopic picture: Drops of neutral fats are found in the cytoplasm of hepatocytes.
13 Morphology of fatty hepatosis Obesity of hepatocytes can be pulverous, small- and largedroplet. Fatty degeneration can appear in single hepatocytes (disseminated obesity), in groups of hepatocytes (zonal obesity) or affect the entire parenchyma (diffuse obesity). Under the influence of intoxication, hypoxia, obesity of centrolobular hepatocytes develops, in the presence of general obesity and protein-vitamin deficiency, mostly obesity of periportal hepatocytes develops. In case of severe fatty infiltration, liver cells die, fatty drops merge and form extracellular fatty cysts; around them there is a cellular reaction and connective tissue grows.
14 Stages of fatty hepatosis 1. Simple obesity, when the destruction of hepatocytes is not expressed and there is no cellular reaction around. 2. Obesity in combination with necrosis of individual hepatocytes and mesenchymal-cell reaction. 3. Obesity of hepatocytes, necrosis of individual hepatocytes, cellular reaction and proliferation of connective tissue with a beginning restructuring of the lobular structure of the liver. The third stage of hepatic steatosis is irreversible and is considered as a precirrhotic one. The outcome of fatty hepatosis is cirrhosis of the liver.

15 Fatty hepatosis


16 Fatty hepatosis on the left picture - staining with hematoxylin and eosin, on the right picture - with Sudan III
17 Hepatitis Hepatitis is a group of inflammatory liver diseases. Hepatitis can be: Primary, that is, develop as an independent disease, Secondary, that is, develop as a manifestation of another disease.
18 Classification of primary hepatitis On the etiology: Viral hepatitis, Alcoholic hepatitis, Medicinal (medicamentous) hepatitis. Autoimmune hepatitis. With the flow: Acute hepatitis Chronic hepatitis.
19 Viral hepatitis Viral hepatitis is caused by hepatitis A-F viruses.
20 Viral hepatitis A Synonym: Botkin's disease. Caused by RNA virus. The virus affects more often organized collectives (kindergartens, schools, military units). The virus has a direct cytotoxic effect, is not retained in the cell. The mechanism of infection is fecal-oral. The incubation period is from 15 to 45 days. Characteristic cyclic icteric or icteric forms. The disease ends in recovery. Elimination of the virus by macrophages occurs with the cell. There is no evidence of a virus or a transition to chronic hepatitis.
21 Viral hepatitis B Caused by DNA virus. The incubation period is days. Transmission routes: parenteral (with injections, blood transfusions, any medical manipulations), sexual. The hepatitis B virus does not have a direct cytopathic effect on hepatocytes, it is reproduced in the hepatocyte and under certain conditions in other cells (lymphocytes, macrophages). The destruction of the hepatocyte and the elimination of the virus are carried out by the cells of the immune system. Often accompanied by the carrier of the virus and the transition to chronic hepatitis.
22 Viral hepatitis B Several antigenic determinants have been found in the hepatitis B virus: HBsAg - surface antigen of the virus, which is reproduced in the cytoplasm of the hepatocyte and serves as an indicator of the carrier of the virus; HBcAg - deep antigen, reproduced in the nucleus, contains DNA - the indicator of replication; HBeAg, which appears in the cytoplasm, reflects the replication activity of the virus.
23 Viral hepatitis B The virus has morphological and serological markers. Its particles are visible in an electron microscope in the nucleus and cytoplasm. HBsAg is detected with the help of histochemical methods (staining with orketin according to Shikata and aldehyde fuchsin). In addition, there are indirect morphological signs of the presence of HBsAg in the cell - "frosted-glass" hepatocytes, and also HBcAg - "sand cores" (small eosinophilic inclusions in the nuclei).
24 "frosted-glass" hepatocytes
25 Viral hepatitis С The causative agent is an RNA-containing virus that has a lipid envelope. The incubation period is days. The main route of transmission is parenteral. There are serological reactions that can diagnose HCV infection. There are no direct morphological markers of the virus. The virus replicates in the hepatocyte and in other cells (lymphocytes, macrophages). Has a cytopathic effect and causes immune disorders. The disease is often found in alcoholics and injecting drug users. Rapidly progressing with the development of chronic forms of hepatitis
26 Viral hepatitis D The delta virus is a defective RNA virus, which causes the disease only in the presence of the surface antigen of the virus B. If infection with virus B and delta virus occurs simultaneously (coinfection), then acute hepatitis occurs immediately. If there is a delta virus infection against the background of an existing human hepatitis B (superinfection), this situation is clinically manifested by exacerbation and rapid progression of the disease, up to the development of liver cirrhosis.
27 Morphology of acute viral hepatitis Macroscopic picture: The liver becomes large, Red. Microscopic picture: Necrosis of hepatocytes (stepped, bridged), Hydropic and balloon dystrophy of hepatocytes, The Kaunsilmen s bodies (apoptosis of hepatocytes), In the portal tracts and in the lobular stroma there is abundant infiltration, represented mainly by lymphocytes and macrophages, with a small admixture of PMNs, Hyperplasia and focal proliferation of Kupffer cells, There are regenerating hepatocytes, Cholestasis is possible.

28 Acute viral hepatitis

29 Acute viral hepatitis

30 Kaunsilmen s bodies
31 Phases of acute viral hepatitis The incubation period (varies from 2 to 26 weeks); Pre-jaundice (prodromal) period, characterized by nonspecific symptoms; Jaundice period, developed clinical manifestations; Period of convalescence (recovery).
32 Clinical and morphological forms of acute viral hepatitis Cyclic icteric (classical manifestation of hepatitis A); Without jaundice (80% of hepatitis C and 70% of hepatitis B); Subclinical (inapparens); Lightning (fulminant) with massive progressive necrosis of hepatocytes; Cholestatic (with the involvement of small bile ducts and cholestasis of varying severity).
33 Chronic hepatitis (CH) A group of liver diseases in which chronic inflammation predominates. May be caused by all hepatitis viruses, except for hepatitis A virus. To confirm the clinical diagnosis, a morphological examination of the liver biopsy is necessary.
34 Classification of chronic hepatitis Classification of chronic hepatitis recommended by the International Congress of Gastroenterologists in Los Angeles (1994) and takes into account three categories of evaluation: Etiology, Degree of activity of the process, Stage of the disease.
35 Classification of chronic hepatitis The following types of etiology are distinguished: Viral, Autoimmune, Drug, Cryptogenic (unidentified etiology).
36 Degree of activity CH All chronic hepatitis are considered active. The degree of activity of the process is assessed using histological activity index (HAI) - Knodell index. In the biopsy of the liver, the following morphologist is assessed: Periportal and bridge necrosis (0-10 points), Intralobular focal necrosis and hepatocyte dystrophy (0-4 points), Inflammatory infiltrate in portal tracts (0-4 points), Fibrosis (0-4 points).
37 Degree of activity CH HAI 1-3 points corresponds to chronic hepatitis with minimal activity. HAI 4-8 points indicates a low degree of activity, a mild course of chronic hepatitis. HAI 9-12 points corresponds to chronic hepatitis of moderate activity, HAI points corresponds to high activity, severe chronic hepatitis.
38 Stage of chronic hepatitis The stage of chronic hepatitis is determined on the basis of an assessment of the severity of fibrosis (grade IV). I stage of chronic hepatitis: fibrosis unobtrusive, limited only to portal tracts. II stage of chronic hepatitis: portal and initial periportal fibrosis - portal tracts become process, stellate. III stage of chronic hepatitis: port-portal connective tissue septa are formed. IV stage of chronic hepatitis: in addition to port-portal septa, incomplete port-central and incomplete translobular septa form; This stage is pre-cirrhotic.
39 Morphology of chronic viral hepatitis (CVH) Microscopic picture: Hydropic and balloon dystrophy of hepatocytes, Fatty degeneration of hepatocytes (only with CVH C), Apoptotic bodies (Kaunsilmen's bodies), Step and bridge-like necrosis of hepatocytes (with moderate and high CH activity), Lympho-macrophage infiltration in portal tracts (with minimal CH activity), The spread of lympho-macrophage infiltrate through the border plate into the hepatic lobe (with high CH activity),
40 Morphology of CVH Microscopic picture: The appearance of lymphoid follicles in the portal stroma and within the lobules (only with CVH C), Hyperplasia and proliferation of Kupffer cells, Proliferation of small bile ducts (with CVH C), Sclerosis (fibrosis) of portal tracts.

41 Chronic viral hepatitis with minimal activity

42 Chronic viral hepatitis with high activity
43 Autoimmune hepatitis In the patient s serum autoantibodies to a specific hepatic protein (LSP) of hepatocellular membranes are detected. The LSP titer correlates with the severity of the inflammatory reaction in the liver and the biochemical changes in the blood.
44 Autoimmune hepatitis The morphological picture corresponds to chronic hepatitis of a high degree of activity. The distinctive features are: The appearance in the portal tracts of lymphoid follicles, next to which macrophage granulomas can form; In lymphomacrofagal infiltrate a large number of plasma cells synthesizing immunoglobulins, which can be detected on membranes of hepatocytes with the help of immunohistochemical methods.
45 Alcoholic hepatitis It develops after 3 to 5 years of systematic alcohol consumption, but only in 35% of patients with alcoholism. One of the mechanisms of liver damage is the direct cytopathic action of acetaldehyde, the main metabolite of ethanol. The binding of acetaldehyde to the main proteins of the cytoskeleton can lead to irreversible cell damage, disrupting the secretion of the protein and promoting the formation of balloon dystrophy of hepatocytes. Stable compounds of acetaldehyde with extracellular matrix proteins in the Dysse space contribute to fibrogenesis (activation of Ito cells) and lead to the development of sclerosis.
46 Alcoholic hepatitis Macroscopic picture: The liver has a mottled appearance, Red with bilious areas, Its size is normal or slightly enlarged, On a cut small nodules and whitish interlayers (the beginning of formation of a cirrhosis) are often visible.
47 Alcoholic hepatitis Microscopic picture: Fat and balloon dystrophy of hepatocytes, The appearance of intracellular eosinophilic inclusions (alcoholic hyaline or Mallory's body), Mainly leukocyte infiltration, Development of connective tissue around the central veins (perivennular fibrosis), individual hepatocytes (pericellular fibrosis) and in portal tracts; Sometimes there are signs of cholestasis.
 with alcoholic")
48 Mallory s bodies (alcoholic hyaline) with alcoholic hepatitis
49 Alcoholic hepatitis With frequent episodes of acute alcohol intoxication, alcoholic hepatitis progresses to micronodular cirrhosis, which is observed in 30% of patients with alcoholic hepatitis.
50 Liver cirrhosis Chronic liver disease, characterized by structural rearrangement of the organ with wrinkling and formation of nodes - false lobules.
51 Morphology of liver cirrhosis Diffuse fibrosis (in the form of thin interlayers or wide septums). Deformation of the liver. Disturbance of the lobular structure of the liver parenchyma. Formation of nodes-regenerates (false lobules) as a result of a violation of hepatocyte regeneration. Dystrophy and necrosis of hepatocytes. Inflammatory infiltration in the parenchyma and septums.
52 Classification of liver cirrhosis On the etiology: Hereditary (with hemochromatosis, Wilson's disease, alpha 1-antitrypsin deficiency, etc.) Purchased: Toxic (more often alcoholic), Infectious (more often viral), Biliary, Exchange-alimentary, Dyscirculatory (nutmeg), Cryptogenic (of unknown origin), Mixed origin.
53 Classification of liver cirrhosis According to the macroscopic picture: Macronodular cirrhosis, Micronodular cirrhosis, Mixed cirrhosis of the liver. The criterion is the size of the regeneration nodes. In the case of micronodular cirrhosis, the size of the nodules does not exceed 3 mm, with a macronodular size - can reach several centimeters.

54 Micronodular liver cirrhosis

55 Macronodular liver cirrhosis
56 Classification of liver cirrhosis Histologically distinguish: Monolobular, Multilobular, Monomultilobular liver cirrhosis Criterion are the features of the structure of the regeneration nodes. In monolobular cirrhosis of the liver, the regenerate nodes are built on the basis of a single fragmented lobule. With multilobular cirrhosis of the liver, the fragments of several lobules are part of the regeneration unit. Monomultilobular cirrhosis of the liver is characterized by a combination of the first two species.
57 Classification of liver cirrhosis On morphogenesis distinguish: Post-necrotic, Portal, Mixed cirrhosis of the liver.
58 Postnecrotic liver cirrhosis Postnecrotic cirrhosis develops rapidly (sometimes for several months). It is associated with a variety of causes, most often a fulminant form of viral hepatitis B and toxic damage. It develops as a result of massive hepatocyte necrosis. In the areas of necrosis, the stroma collapses and the proliferation of connective tissue with the formation of broad fibrous fields. For postnecrotic liver cirrhosis, early liver-cell failure and late portal hypertension are characteristic.
59 Postnecrotic liver cirrhosis Macroscopic picture: The liver is reduced in size, Dense consistency, Surface is macronodular, On the parenchyma section is formed by nodes of different sizes, exceeding 1 cm in diameter and separated by dense wide grayish interlayers of connective tissue.

60 Postnecrotic liver cirrhosis

61 Postnecrotic liver cirrhosis
62 Postnecrotic liver cirrhosis Microscopic picture: The lobular structure of the liver is disturbed, Different sizes nodes of regeneration, Radial orientation of the beams is broken, The central vein is absent or displaced to the periphery, Wide connective tissue interlayers (septa) between regeneration sites, The phenomenon of convergence of triads (3 or more in one FV) Lympho-macrophagal infiltration in septums, Proliferating bile ducts in septums, Hydropic and balloon dystrophy of hepatocytes, Many regenerating hepatocytes.

63 The phenomenon of convergence of triads
64 Portal liver cirrhosis It is formed due to the wedging of fibrous septa from the portal tracts and / or central veins, which leads to the connection of the central veins with portal vessels and the appearance of small false lobules. Characterized by the homogeneity of the microscopic picture - a thin-looped connective tissue network, small sizes of false lobules. Portal cirrhosis usually develops in the final chronic hepatitis of alcoholic or viral (hepatitis C) etiology, which determines the nature of hepatocyte dystrophy (fatty) and the nature of the infiltrate. Portal cirrhosis develops slowly (over a number of years). It is characterized by early signs of portal hypertension and late hepatic-cellular insufficiency.
65 Portal liver cirrhosis Macroscopic picture: In the early stages of the disease the liver is enlarged in size, Dense consistency, The surface is micronodular, the dimensions of the nodes do not exceed 3 mm, Nodes of bright yellow color, separated by thin interlayers of gray, dense connective tissue. In the end of the disease, the liver can diminish in size, acquire a brownish-red color, the size of the nodes can vary from 3 to 10 mm.

66 Portal liver cirrhosis
67 Portal liver cirrhosis Microscopic picture: The normal structure of the liver is broken, Small monomorphic nodes-regenerates (false lobules) are seen, separated by narrow interlayers of connective tissue, Hepatocytes in a condition of fatty and balloon dystrophy, In septa, an infiltrate is found, consisting of polymorphonuclear leukocytes, lymphocytes and macrophages, Proliferation of bile ducts.

68 Portal liver cirrhosis
69 Biliary liver cirrhosis Is a true portal cirrhosis. It happens to be primary and secondary. Primary biliary liver cirrhosis is rare, is an autoimmune disease, based on intrahepatic destructive cholangitis and cholangiolitis Secondary biliary cirrhosis is more common, associated with obstruction of extrahepatic bile ducts (stones, parasites, tumors).
70 Biliary liver cirrhosis Macroscopic picture: The liver is enlarged in size, Dense consistency, Dark green color, Surface is micronodular. Microscopic picture: Bile stasis, The appearance of bile ("bile lake") in hepatocytes.

71 Biliary liver cirrhosis

72 Biliary liver cirrhosis
73 Liver cirrhosis syndromes All forms of liver cirrhosis lead to the development of: Syndrome of hepatocellular (hepatic-cell) insufficiency, Syndrome of portal hypertension.
74 Hepatocellular insufficiency Appears when more than 80% of the liver parenchyma is lost. It can lead not only necrosis of hepatocytes, but also a violation of blood supply to the body and loss of normal liver architecture. Hepatic-cell insufficiency manifests itself as the inability of the liver to release certain substances (bilirubin), neutralize toxic exo- and endogenous products (ammonia), the inability to synthesize proteins (clotting factors and albumins).
75 Hepatocellular insufficiency Clinically manifested by the following symptoms and syndromes: Jaundice (often mixed type), Deficiency of clotting factors (coagulopathy), Hypoalbuminemia (as a consequence, edema), Hyperestrogenemia (manifested by erythema of the palms, telangiectasia, hair loss, testicular atrophy and gynecomastia), Encephalopathy (by reducing detoxification in the liver), Neurological disorders.


76 Ascites and telangiectasia
77 Portal hypertension It is develops with increased pressure in the portal vein. In liver cirrhosis, this is due to increased resistance to blood flow due to diffuse proliferation of connective tissue in the organ and a violation of the usual circulation of blood and lymph. Clinically manifested: Ascites, Activation of portocaval and kavakaval anastomoses (varicose veins of the esophagus, anterior abdominal wall - "Medusa's head", hemorrhoids), Splenomegaly.


78 "Medusa's head"


79 Normal spleen Splenomegaly

80 Varicose-dilated esophagus veins
81 Complications and causes of death in liver cirrhosis Hepatic coma. Bleeding from varicose-dilated esophagus veins. Ascites-peritonitis. Thrombosis of the portal vein. Hepatocellular carcinoma.

82 Rupture of varicose-dilated esophagus veins
83 Liver cancer Primary malignant liver tumors in 85% of cases are hepatocellular carcinoma. In 5-10% of cases, cholangiocellular adenocarcinoma (cholangiocellular cancer) is detected.
84 Hepatocellular carcinoma Malignant tumor, developing from hepatocytes. Morbidity has geographical differences, which is explained by the consumption of grain contaminated with aflotoxins (Aspergillus flavus). In 70-80% of patients, the tumor occurs against the background of liver cirrhosis associated with HBV and HCV infection. The prognosis is unfavorable: 90% of patients die within 6 months.
85 Hepatocellular carcinoma Macroscopically, the tumor is represented by one or a number of nodes of greenish color (since its cells produce bile). All forms of the tumor can lead to an increase in liver mass to
86 Hepatocellular carcinoma Histologically, in most cases, the tumor has a trabecular structure. Tumor cells are larger than hepatocytes, with abundant eosinophilic cytoplasm. Cells form two-, three- or multi-nuclear trabeculae and strands. Between them there are sinusoids, sometimes bile capillaries. In the tumor tissue are constantly found areas of necrosis, hemorrhage, sometimes cholestasis.
87 Hepatocellular carcinoma The tumor has invasive growth, especially the invasion of the veins, often accompanied by portal vein thrombosis. Metastasizes hematogenous in 50% of cases.

88 Hepatocellular carcinoma

89 Hepatocellular carcinoma
90 Cholangiocellular cancer Malignant tumor originating from the epithelium of the bile ducts. It occurs less frequently than hepatocellular carcinoma. It is not associated with liver cirrhosis and HBV infection. More often observed in the East, which is associated with helminthic invasion (Opistorchis sinensis).
91 Cholangiocellular cancer Macroscopically it looks like a dense whitish node (multicentric growth possible). Histologically, the tumor has the structure of adenocarcinoma. Characteristically mucus production. Metastasizes primarily lymphogenically.

92 Cholangiocellular cancer

93 Cholangiocellular cancer
94 Cholecystitis Cholecystitis is an inflammation of the gallbladder. On the clinical course, acute and chronic cholecystitis is isolated. Often complicates the course of cholelithiasis (calculous cholecystitis). Acute cholecystitis occurs in the form of catarrhal, fibrinous or purulent (phlegmonous) inflammation. Complicated by perforation of the wall and bile peritonitis. When the bladder duct is obstructed by a stone, a dropsy may develop (accumulation in the lumen of the bladder of the secretion of the mucosa with thinning of the wall of the gallbladder) or empyema (purulent exudate in the lumen) of the gallbladder.

95 Acute purulent cholecystitis
96 Cholecystitis Chronic cholecystitis is a consequence of acute inflammation. Macroscopically, the wall of the gallbladder becomes whitish, thickens, compacted due to sclerosis ("porcelain" gallbladder). Microscopically detected lymphohistiocytic infiltration and sclerosis of the wall of the gallbladder, focal or diffuse mucosal atrophy. In some cases, cholesterol deposition occurs in the wall of the gallbladder - cholesterosis of the gallbladder, as a result of which a large number of xanthomous (foamy) cells appear in the wall of the gallbladder.

97 " Porcelain" gallbladder

98 Chronic calculous cholecystitis

99 Chronic cholecystitis

100 Gallbladder cholesterosis

101 Gallbladder cholesterosis
102 Cholelithiasis Gallstone disease (cholelithiasis) is a disease characterized by the formation of stones in the gallbladder. Factors promoting stone formation: Changes in the quality of bile: Excess pigments, Excess cholesterol compared with bile salts and lecithin; Inflammation; Cholestasis.
103 Cholelithiasis The composition of the gallbladder stones are: Cholesterol; Pigmented; Calcareous; Mixed (more than 80% of all stones). Complications of cholelithiasis: Inflammation (acute and chronic cholecystitis); obstruction: A cystic duct (empyema, mukocele); Common bile duct (subhepatic jaundice); Fater's nipple (subhepatic jaundice, pancreatitis); Sores and perforation - bile peritonitis; Calcification of the lumen of the small intestine.

104 Levels of biliary tract obstructed by stone Сystic duct Common bile duct Wirsung's duct Fater's nipple


105 Stones in the gallbladder and choledochus
106 Pancreatitis Pancreatitis is an inflammation of the pancreas. According to the clinical course, acute and chronic pancreatitis is isolated. Acute pancreatitis develops when bile enters the excretory duct of the gland during poisoning with alcohol or poor-quality food. Morphologically acute pancreatitis is manifested by severe inflammatory edema, necrosis of fatty tissue and parenchyma, hemorrhages, foci of suppuration. If hemorrhages predominate, they speak of hemorrhagic pancreatitis, in cases of predominance of purulent inflammation - purulent pancreatitis, necrotic changes - pancreanecrosis.

107 Acute hemorrhagic pancreatitis

108 Acute hemorrhagic pancreatitis


109 Pancreanecrosis
110 Pancreatitis Chronic pancreatitis is characterized by the prevalence of sclerotic changes, the formation of cysts, foci of calcification. The pancreas decreases and becomes dense. Possible development of diabetes. With chronic pancreatitis caused by alcohol abuse, the drainage function of the excretory ducts is disrupted, the secret thickens and cysts of the ducts are formed. Around these ducts connective tissue grows, there are roundcell infiltrates - chronic pancreatitis of alcoholic etiology is formed. Cysts can rupture and cause severe peritonitis.

111 Chronic alcoholic pancreatitis

112 Chronic pancreatitis

113 Morphological study in the diagnosis of liver disease To establish the diagnosis, a liver biopsy is used. In addition, using biopsy, you can: Determine the activity of the process and the stage of the disease; Evaluate the effectiveness of therapy; To recognize and exclude other pathological processes.
114 Types of liver biopsies For intravital diagnosis of liver diseases are used: Surgical biopsy (marginal resection), Various variants of puncture biopsy (blind and sighting). Edge resection, performed with laparotomy, allows you to explore subcapsular areas. Puncture biopsy has fewer limitations and allows you to explore different zones of the liver at different depths: With Mengini needle (percutaneous in VIII - IX intercostal space on the right mid-axillary line).
115 Complications of puncture biopsy Compose 0.3% of cases for tens of thousands of studies: Pleurisy, Perihepatitis, Bleeding, Intrahepatic hematoma, Hemobiology, Arteriovenous fistula, Bile peritonitis, and others.
116 Requirements for liver biopsy sample To enable the researcher to give a responsible conclusion, the tissue sample must be at least 2 cm long and contain four portal tracts (Sherlock Sherlock, J. Dooley, 1999).
Gastrointestinal System: Accessory Organ Disorders
 Gastrointestinal System: Accessory Organ Disorders Mary DeLetter, PhD, RN Associate Professor Dept. of Baccalaureate and Graduate Nursing Eastern Kentucky University Disorders of Accessory Organs Portal
Gastrointestinal System: Accessory Organ Disorders Mary DeLetter, PhD, RN Associate Professor Dept. of Baccalaureate and Graduate Nursing Eastern Kentucky University Disorders of Accessory Organs Portal
Liver, Pancreas and Gall Bladder Pathology
 Liver, Pancreas and Gall Bladder Pathology SCBM342 Systemic Pathology Witchuda Payuhakrit, Ph.D. (Pathobiology) Email: witchuda.pay@mahidol.ac.th Objectives 1. Understand etiology and pathogenesis of common
Liver, Pancreas and Gall Bladder Pathology SCBM342 Systemic Pathology Witchuda Payuhakrit, Ph.D. (Pathobiology) Email: witchuda.pay@mahidol.ac.th Objectives 1. Understand etiology and pathogenesis of common
LIVER DISEASES. Pathology Department, Zhejiang University School of Medicine,
 LIVER DISEASES Pathology Department, Zhejiang University School of Medicine, 马丽琴,maliqin198@zju.edu.cn Viral Hepatitis Cirrhosis of liver Liver cancer Viral Hepatitis DEFINITION Primary hepatic infections
LIVER DISEASES Pathology Department, Zhejiang University School of Medicine, 马丽琴,maliqin198@zju.edu.cn Viral Hepatitis Cirrhosis of liver Liver cancer Viral Hepatitis DEFINITION Primary hepatic infections
Disorders of the Liver and Pancreas
 Disorders of the Liver and Pancreas Liver Lobule Hexagonal plates Sinusoids Triads Bile duct branch Arteriole Venuole Blood flows from periphery to Central vein Space of Dissé Lobular Microanatomy Hepatocytes
Disorders of the Liver and Pancreas Liver Lobule Hexagonal plates Sinusoids Triads Bile duct branch Arteriole Venuole Blood flows from periphery to Central vein Space of Dissé Lobular Microanatomy Hepatocytes
Pathology of the Liver and Biliary Tract 5 Diseases of the Biliary Tract. Shannon Martinson, April 2016
 Pathology of the Liver and Biliary Tract 5 Diseases of the Biliary Tract Shannon Martinson, April 2016 http://people.upei.ca/smartinson/ OUTLINE Normal anatomy & function Hepatobiliary Injury and responses
Pathology of the Liver and Biliary Tract 5 Diseases of the Biliary Tract Shannon Martinson, April 2016 http://people.upei.ca/smartinson/ OUTLINE Normal anatomy & function Hepatobiliary Injury and responses
Pathology of the Liver and Biliary Tract 5 Diseases of the Biliary Tract. Shannon Martinson, March 2017
 Pathology of the Liver and Biliary Tract 5 Diseases of the Biliary Tract Shannon Martinson, March 2017 http://people.upei.ca/smartinson/ OUTLINE Normal anatomy & function Hepatobiliary injury and responses
Pathology of the Liver and Biliary Tract 5 Diseases of the Biliary Tract Shannon Martinson, March 2017 http://people.upei.ca/smartinson/ OUTLINE Normal anatomy & function Hepatobiliary injury and responses
-sheet 3. -Waseem Alhaj. Maha Shomaf
 -sheet 3 -Basheer egbaria -Waseem Alhaj Maha Shomaf 1 P a g e Viral hepatitis have many types each type is associated with different outcomes complication, some can result in acute one,others result in
-sheet 3 -Basheer egbaria -Waseem Alhaj Maha Shomaf 1 P a g e Viral hepatitis have many types each type is associated with different outcomes complication, some can result in acute one,others result in
Histology. The pathology of the. bile ducts. pancreas. liver. The lecture in summary. Vt-2006
 Vt-2006 The pathology of the liver, bile ducts and pancreas Richard Palmqvist Docent, ST-läkare, Klin Pat Lab, Labcentrum The lecture in summary Introduction, histology & physiology in brief General phenomenon
Vt-2006 The pathology of the liver, bile ducts and pancreas Richard Palmqvist Docent, ST-läkare, Klin Pat Lab, Labcentrum The lecture in summary Introduction, histology & physiology in brief General phenomenon
PATHOLOGY OF LIVER & BILIARY TRACT. Lecture 5. Idiopathic & proliferative conditions; diseases of the biliary tract
 PATHOLOGY OF LIVER & BILIARY TRACT Lecture 5 Idiopathic & proliferative conditions; diseases of the biliary tract Enrique Aburto Winter 2015 IX. Diseases of uncertain origin Equine serum hepatitis Idiopathic
PATHOLOGY OF LIVER & BILIARY TRACT Lecture 5 Idiopathic & proliferative conditions; diseases of the biliary tract Enrique Aburto Winter 2015 IX. Diseases of uncertain origin Equine serum hepatitis Idiopathic
Slide 7 demonstrates acute pericholangitisis with neutrophils around proliferating bile ducts.
 Many of the histologic images and the tables are from MacSween s Pathology of the Liver (5 th Edition). Other images were used from an online source called PathPedia.com. A few images from other sources
Many of the histologic images and the tables are from MacSween s Pathology of the Liver (5 th Edition). Other images were used from an online source called PathPedia.com. A few images from other sources
Liver Failure. The most severe clinical consequence of liver disease is liver failure:
 Liver diseases I The major primary diseases of the liver are: - Viral hepatitis, - Nonalcoholic fatty liver disease (NAFLD), - Alcoholic liver disease, - Hepatocellular carcinoma (HCC) Hepatic damage also
Liver diseases I The major primary diseases of the liver are: - Viral hepatitis, - Nonalcoholic fatty liver disease (NAFLD), - Alcoholic liver disease, - Hepatocellular carcinoma (HCC) Hepatic damage also
Case n 1 ( B 92 / 4208 ) Case n 2 ( B 00 / 8249 ) Case n 3 ( B 98 / 8352 )
 Case n 2 ( B 00 / 8249 ) Case n 3 ( B 98 / 8352 )") Slide Seminar Case n 1 ( B 92 / 4208 ) 16 month-old girl. HBV serology +. Clinic in favour of chronic hepatitis. 4 portal triads! classification limited Viral B chronic hepatitis Mild activity (Fig. 1
Slide Seminar Case n 1 ( B 92 / 4208 ) 16 month-old girl. HBV serology +. Clinic in favour of chronic hepatitis. 4 portal triads! classification limited Viral B chronic hepatitis Mild activity (Fig. 1
Digestive system L 4. Lecturer Dr. Firdous M. Jaafar Department of Anatomy/Histology section
 Digestive system L 4 Lecturer Dr. Firdous M. Jaafar Department of Anatomy/Histology section objectives 1-Describe the structure of liver. 2-Define liver lobule, and identify its zones. 3-Define portal
Digestive system L 4 Lecturer Dr. Firdous M. Jaafar Department of Anatomy/Histology section objectives 1-Describe the structure of liver. 2-Define liver lobule, and identify its zones. 3-Define portal
Liver Disease. By: Michael Martins
 Liver Disease By: Michael Martins Recently I have been getting a flurry of patients that have some serious liver complications. This week s literature review will be the dental management of the patients
Liver Disease By: Michael Martins Recently I have been getting a flurry of patients that have some serious liver complications. This week s literature review will be the dental management of the patients
Epithelial tumors. Dr. F.F. Khuzin, PhD Dr. M.O. Mavlikeev
 Epithelial tumors Dr. F.F. Khuzin, PhD Dr. M.O. Mavlikeev Epithelial tumors Tumors from the epithelium are the most frequent among tumors. There are 2 group features of these tumors: The presence in most
Epithelial tumors Dr. F.F. Khuzin, PhD Dr. M.O. Mavlikeev Epithelial tumors Tumors from the epithelium are the most frequent among tumors. There are 2 group features of these tumors: The presence in most
Chapter 18 LIVER BILIARY TRACT
 Chapter 18 LIVER & BILIARY TRACT DUCT SYSTEM N O FIBROUS TISSUE PORTAL TRIAD CENTRAL VEIN PATTERNS OF HEPATIC INJURY Degeneration: Balooning, feathery degeneration, fat, pigment Inflammation:
Chapter 18 LIVER & BILIARY TRACT DUCT SYSTEM N O FIBROUS TISSUE PORTAL TRIAD CENTRAL VEIN PATTERNS OF HEPATIC INJURY Degeneration: Balooning, feathery degeneration, fat, pigment Inflammation:
How to Approach a Medical Liver Biopsy. 9 th Bryan Warren School of Pathology Pancreatic and Liver Pathology. Sarajevo, 6 th -7 th November 2015
 1 A Brief Introduction to the Liver Sessions 9 th Bryan Warren School of Pathology Pancreatic and Liver Pathology Sarajevo, 6 th -7 th November 2015 Stefan Hübscher, Institute of Immunology & Immunotherapy,
1 A Brief Introduction to the Liver Sessions 9 th Bryan Warren School of Pathology Pancreatic and Liver Pathology Sarajevo, 6 th -7 th November 2015 Stefan Hübscher, Institute of Immunology & Immunotherapy,
Diseases of liver. Dr. Mohamed. A. Mahdi 4/2/2019. Mob:
 Diseases of liver Dr. Mohamed. A. Mahdi Mob: 0123002800 4/2/2019 Cirrhosis Cirrhosis is a complication of many liver disease. Permanent scarring of the liver. A late-stage liver disease. The inflammation
Diseases of liver Dr. Mohamed. A. Mahdi Mob: 0123002800 4/2/2019 Cirrhosis Cirrhosis is a complication of many liver disease. Permanent scarring of the liver. A late-stage liver disease. The inflammation
Histopathology: Cell necrosis and cytoplasmic accumulations
 Histopathology: Cell necrosis and cytoplasmic accumulations These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you
Histopathology: Cell necrosis and cytoplasmic accumulations These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you
LIVER PHYSIOLOGY AND DISEASE
 GASTROENTEROLOGY C opy ri~ht 1972 by The Williams & Wilkins Co. Vol. 62. No.3 Printed in U.S.A. LIVER PHYSIOLOGY AND DISEASE SPLENOMEGALY IN UNCOMPLICATED BILIARY TRACT AND PANCREATIC DISEASE PETER B.
GASTROENTEROLOGY C opy ri~ht 1972 by The Williams & Wilkins Co. Vol. 62. No.3 Printed in U.S.A. LIVER PHYSIOLOGY AND DISEASE SPLENOMEGALY IN UNCOMPLICATED BILIARY TRACT AND PANCREATIC DISEASE PETER B.
Approach to the Patient with Liver Disease
 Approach to the Patient with Liver Disease Diagnosis of liver disease Careful history taking Physical examination Laboratory tests Radiologic examination and imaging studies Liver biopsy Liver diseases
Approach to the Patient with Liver Disease Diagnosis of liver disease Careful history taking Physical examination Laboratory tests Radiologic examination and imaging studies Liver biopsy Liver diseases
Basic patterns of liver damage what information can a liver biopsy provide and what clinical information does the pathologist need?
 Basic patterns of liver damage what information can a liver biopsy provide and what clinical information does the pathologist need? Rob Goldin r.goldin@imperial.ac.uk Fatty liver disease Is there fatty
Basic patterns of liver damage what information can a liver biopsy provide and what clinical information does the pathologist need? Rob Goldin r.goldin@imperial.ac.uk Fatty liver disease Is there fatty
Hepatitis. Dr. Mohamed. A. Mahdi 5/2/2019. Mob:
 Hepatitis Dr. Mohamed. A. Mahdi Mob: 0123002800 5/2/2019 Hepatitis Hepatitis means the inflammation of the liver. May cause by viruses or bacteria, parasites, radiation, drugs, chemical and toxins (alcohol).
Hepatitis Dr. Mohamed. A. Mahdi Mob: 0123002800 5/2/2019 Hepatitis Hepatitis means the inflammation of the liver. May cause by viruses or bacteria, parasites, radiation, drugs, chemical and toxins (alcohol).
Pathophysiology I Liver and Biliary Disease
 Pathophysiology I Liver and Biliary Disease The Liver The liver is located in the right upper portion of the abdominal cavity just beneath the right side of the rib cage. The liver has many functions that
Pathophysiology I Liver and Biliary Disease The Liver The liver is located in the right upper portion of the abdominal cavity just beneath the right side of the rib cage. The liver has many functions that
Viral Hepatitis (I) Luigi Terracciano Department of Pathology University Hospital Basel. Basel,
 Luigi Terracciano Department of Pathology University Hospital Basel. Basel,") Viral Hepatitis (I) Luigi Terracciano Department of Pathology University Hospital Basel Basel, 19. 04. 2016 Definition Hepatitis means inflammation of the liver characterized by a variable combination
Viral Hepatitis (I) Luigi Terracciano Department of Pathology University Hospital Basel Basel, 19. 04. 2016 Definition Hepatitis means inflammation of the liver characterized by a variable combination
Disorders of the Liver, Gallbladder and Pancreas
 Disorders of the Liver, Gallbladder and Pancreas Objectives: Disorders of the liver Disorders of the gall bladder Disorders of the pancreas Part 1: Disorders of the Liver 1 Jaundice: is a manifestation
Disorders of the Liver, Gallbladder and Pancreas Objectives: Disorders of the liver Disorders of the gall bladder Disorders of the pancreas Part 1: Disorders of the Liver 1 Jaundice: is a manifestation
Canine Liver Eneku Wilfred Bovine Pathology
 2012-1-3 Canine Liver Eneku Wilfred Bovine Pathology Contributor: New Mexico Department of Agriculture Veterinary Diagnostic Services Signalment: 5 month old male Weimaraner dog (Canis familiaris) History:
2012-1-3 Canine Liver Eneku Wilfred Bovine Pathology Contributor: New Mexico Department of Agriculture Veterinary Diagnostic Services Signalment: 5 month old male Weimaraner dog (Canis familiaris) History:
Anatomy of the biliary tract
 Harvard-MIT Division of Health Sciences and Technology HST.121: Gastroenterology, Fall 2005 Instructors: Dr. Jonathan Glickman Anatomy of the biliary tract Figure removed due to copyright reasons. Biliary
Harvard-MIT Division of Health Sciences and Technology HST.121: Gastroenterology, Fall 2005 Instructors: Dr. Jonathan Glickman Anatomy of the biliary tract Figure removed due to copyright reasons. Biliary
PITFALLS IN THE DIAGNOSIS OF MEDICAL LIVER DISEASE WITH TWO CONCURRENT ETIOLOGIES I HAVE NOTHING TO DISCLOSE CURRENT ISSUES IN ANATOMIC PATHOLOGY 2017
 CURRENT ISSUES IN ANATOMIC PATHOLOGY 2017 I HAVE NOTHING TO DISCLOSE Linda Ferrell PITFALLS IN THE DIAGNOSIS OF MEDICAL LIVER DISEASE WITH TWO CONCURRENT ETIOLOGIES Linda Ferrell, MD, UCSF THE PROBLEM
CURRENT ISSUES IN ANATOMIC PATHOLOGY 2017 I HAVE NOTHING TO DISCLOSE Linda Ferrell PITFALLS IN THE DIAGNOSIS OF MEDICAL LIVER DISEASE WITH TWO CONCURRENT ETIOLOGIES Linda Ferrell, MD, UCSF THE PROBLEM
Section 8 Liver and Gallbladder
 General and Systemic Histopathology C601 and C602 Section 8 As we will see in this unit, the liver is subject to many types of injury. Additionally, many systemic diseases have a liver component and sometimes
General and Systemic Histopathology C601 and C602 Section 8 As we will see in this unit, the liver is subject to many types of injury. Additionally, many systemic diseases have a liver component and sometimes
Extracellular degeneration
 Extracellular degeneration By Dr. Hemn Hassan Othman PhD, Pathology Fall 2016 1/17/2017 1 Extracellular Degenerations I / Hyaline Degeneration (Hyalinization): The ward hyaline is derived from the Latin
Extracellular degeneration By Dr. Hemn Hassan Othman PhD, Pathology Fall 2016 1/17/2017 1 Extracellular Degenerations I / Hyaline Degeneration (Hyalinization): The ward hyaline is derived from the Latin
Liver Diseases. Yasmine Lashine MD, PhD
 Liver Diseases Yasmine Lashine MD, PhD ILOs Recognize different causes of Live failure Recall and understand clinical picture and complication of Liver failure Discuss causes and clinical picture of hepatic
Liver Diseases Yasmine Lashine MD, PhD ILOs Recognize different causes of Live failure Recall and understand clinical picture and complication of Liver failure Discuss causes and clinical picture of hepatic
Autoimmune Liver Diseases
 2nd Pannonia Congress of pathology Hepato-biliary pathology Autoimmune Liver Diseases Vera Ferlan Marolt Institute of pathology, Medical faculty, University of Ljubljana Slovenia Siofok, Hungary, May 2012
2nd Pannonia Congress of pathology Hepato-biliary pathology Autoimmune Liver Diseases Vera Ferlan Marolt Institute of pathology, Medical faculty, University of Ljubljana Slovenia Siofok, Hungary, May 2012
Malignant Focal Liver Lesions
 Malignant Focal Liver Lesions Other Than HCC Pablo R. Ros, MD, MPH, PhD Departments of Radiology and Pathology University Hospitals Cleveland Medical Center Case Western Reserve University Pablo.Ros@UHhospitals.org
Malignant Focal Liver Lesions Other Than HCC Pablo R. Ros, MD, MPH, PhD Departments of Radiology and Pathology University Hospitals Cleveland Medical Center Case Western Reserve University Pablo.Ros@UHhospitals.org
Cellular Injury. Intracellular degeneration. By Dr. Hemn Hassan Othman PhD, Pathology Fall /20/2018 1
 Cellular Injury Intracellular degeneration By Dr. Hemn Hassan Othman PhD, Pathology Fall 2018 10/20/2018 1 Types of cell injury Cell injury is divided into: 1. Reversible cell injury 2. Irreversible cell
Cellular Injury Intracellular degeneration By Dr. Hemn Hassan Othman PhD, Pathology Fall 2018 10/20/2018 1 Types of cell injury Cell injury is divided into: 1. Reversible cell injury 2. Irreversible cell
Gastrointes*nal and Liver Pathology. Kris*ne Kra5s, M.D.
 Gastrointes*nal and Liver Pathology Kris*ne Kra5s, M.D. GI Pathology Outline Esophagus Stomach Intes*ne Liver Gallbladder Pancreas GI Pathology Outline Esophagus Stomach Intes*ne Liver Hepa**s Alcoholic
Gastrointes*nal and Liver Pathology Kris*ne Kra5s, M.D. GI Pathology Outline Esophagus Stomach Intes*ne Liver Gallbladder Pancreas GI Pathology Outline Esophagus Stomach Intes*ne Liver Hepa**s Alcoholic
Pathology of the Liver and Biliary Tract 1 Normal Liver; Hepatic Injury, Response, and Failure
 Pathology of the Liver and Biliary Tract 1 Normal Liver; Hepatic Injury, Response, and Failure Shannon Martinson, August 2017 http://people.upei.ca/smartinson/ WELCOME! Dr Boute is the coordinator Course
Pathology of the Liver and Biliary Tract 1 Normal Liver; Hepatic Injury, Response, and Failure Shannon Martinson, August 2017 http://people.upei.ca/smartinson/ WELCOME! Dr Boute is the coordinator Course
What Is Cirrhosis? CIRRHOSIS. Cirrhosis occurs when the liver is. by chronic conditions and diseases. permanently scarred or injured
 What Is Cirrhosis? Cirrhosis occurs when the liver is permanently scarred or injured by chronic conditions and diseases. Common causes of cirrhosis include: Long-term alcohol abuse. Chronic viral hepatitis
What Is Cirrhosis? Cirrhosis occurs when the liver is permanently scarred or injured by chronic conditions and diseases. Common causes of cirrhosis include: Long-term alcohol abuse. Chronic viral hepatitis
Pathological Classification of Hepatocellular Carcinoma
 3 rd APASL Single Topic Conference: HCC in 3D Pathological Classification of Hepatocellular Carcinoma Glenda Lyn Y. Pua, M.D. HCC Primary liver cancer is the 2 nd most common cancer in Asia HCC is the
3 rd APASL Single Topic Conference: HCC in 3D Pathological Classification of Hepatocellular Carcinoma Glenda Lyn Y. Pua, M.D. HCC Primary liver cancer is the 2 nd most common cancer in Asia HCC is the
Hemosiderin. Livia Vida 2018
 Hemosiderin Livia Vida 2018 Questions Histochemical caracteristics of the different pigments. Exogenous pigments. Hemoglobinogenic pigments. Causes and forms of jaundice. Hemoglobinogenic pigments. Pathological
Hemosiderin Livia Vida 2018 Questions Histochemical caracteristics of the different pigments. Exogenous pigments. Hemoglobinogenic pigments. Causes and forms of jaundice. Hemoglobinogenic pigments. Pathological
Nottingham Patterns of liver fibrosis and their clinical significance
 Nottingham 2006 Patterns of liver fibrosis and their clinical significance Alastair D Burt Professor of Pathology and Dean of Clinical Medicine University of Newcastle upon Tyne Collapse of reticulin
Nottingham 2006 Patterns of liver fibrosis and their clinical significance Alastair D Burt Professor of Pathology and Dean of Clinical Medicine University of Newcastle upon Tyne Collapse of reticulin
Alpha-fetoprotein
 Other Names/Abbreviations AFP 190.25 - Alpha-fetoprotein Alpha-fetoprotein (AFP) is a polysaccharide found in some carcinomas. It is effective as a biochemical marker for monitoring the response of certain
Other Names/Abbreviations AFP 190.25 - Alpha-fetoprotein Alpha-fetoprotein (AFP) is a polysaccharide found in some carcinomas. It is effective as a biochemical marker for monitoring the response of certain
Jaundice. Agnieszka Dobrowolska- Zachwieja, MD, PhD
 Jaundice Agnieszka Dobrowolska- Zachwieja, MD, PhD Jaundice definition Jaundice, as in the French jaune, refers to the yellow discoloration of the skin. It arises from the abnormal accumulation of bilirubin
Jaundice Agnieszka Dobrowolska- Zachwieja, MD, PhD Jaundice definition Jaundice, as in the French jaune, refers to the yellow discoloration of the skin. It arises from the abnormal accumulation of bilirubin
A Review of Liver Function Tests. James Gray Gastroenterology Vancouver
 A Review of Liver Function Tests James Gray Gastroenterology Vancouver Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
A Review of Liver Function Tests James Gray Gastroenterology Vancouver Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
Evaluation of Liver Mass Lesions. American College of Gastroenterology 2013 Regional Postgraduate Course
 Evaluation of Liver Mass Lesions American College of Gastroenterology 2013 Regional Postgraduate Course Lewis R. Roberts, MB ChB, PhD Division of Gastroenterology and Hepatology Mayo Clinic College of
Evaluation of Liver Mass Lesions American College of Gastroenterology 2013 Regional Postgraduate Course Lewis R. Roberts, MB ChB, PhD Division of Gastroenterology and Hepatology Mayo Clinic College of
Alpha-fetoprotein
 Other Names/Abbreviations AFP 190.25 - Alpha-fetoprotein Alpha-fetoprotein (AFP) is a polysaccharide found in some carcinomas. It is effective as a biochemical marker for monitoring the response of certain
Other Names/Abbreviations AFP 190.25 - Alpha-fetoprotein Alpha-fetoprotein (AFP) is a polysaccharide found in some carcinomas. It is effective as a biochemical marker for monitoring the response of certain
Hepatocytes produce. Proteins Clotting factors Hormones. Bile Flow
 R.J.Bailey MD Hepatocytes produce Proteins Clotting factors Hormones Bile Flow Trouble.. for the liver! Trouble for the Liver Liver Gall Bladder Common Alcohol Hep C Fatty Liver Cancer Drugs Viruses Uncommon
R.J.Bailey MD Hepatocytes produce Proteins Clotting factors Hormones Bile Flow Trouble.. for the liver! Trouble for the Liver Liver Gall Bladder Common Alcohol Hep C Fatty Liver Cancer Drugs Viruses Uncommon
Morphological changes (accumulations) occur inside and outside cells
 occur inside and outside cells") MIXED ACCUMULATIONS (DEGENERATIONS) Morphological changes (accumulations) occur inside and outside cells The group includes: - chromoproteins metabolism disturbances; - lipoproteins metabolism disturbances;
MIXED ACCUMULATIONS (DEGENERATIONS) Morphological changes (accumulations) occur inside and outside cells The group includes: - chromoproteins metabolism disturbances; - lipoproteins metabolism disturbances;
Steatotic liver disease
 Steatotic liver disease Fatty liver disease Prof. Dr. ANNE HOORENS Non-Neoplastic Liver Pathology December 8th 2018 Working Group of Digestive Pathology Belgian Society of Pathology OUTLINE NAFLD = Non-Alcoholic
Steatotic liver disease Fatty liver disease Prof. Dr. ANNE HOORENS Non-Neoplastic Liver Pathology December 8th 2018 Working Group of Digestive Pathology Belgian Society of Pathology OUTLINE NAFLD = Non-Alcoholic
Chapter 18 Liver and Gallbladder
 Chapter 18 Liver and Gallbladder 解剖學科徐淑媛 本堂重點 1. Liver : functions & histology 2. Gallbladder Physiology Liver Produce circulating plasma proteins Vitamin Iron Degradation Metabolism Bile manufacture (exocrine)
Chapter 18 Liver and Gallbladder 解剖學科徐淑媛 本堂重點 1. Liver : functions & histology 2. Gallbladder Physiology Liver Produce circulating plasma proteins Vitamin Iron Degradation Metabolism Bile manufacture (exocrine)
World Health Organization. Western Pacific Region
 Basic modules for hepatitis 1 Basic Module 1 Liver anatomy and physiology 2 Position of liver Midline Located in right upper abdomen Protected by the right rib cage Right upper Measures: 12 15 cm in vertical
Basic modules for hepatitis 1 Basic Module 1 Liver anatomy and physiology 2 Position of liver Midline Located in right upper abdomen Protected by the right rib cage Right upper Measures: 12 15 cm in vertical
Alpha-fetoprotein
 Other Names/Abbreviations AFP 190.25 - Alpha-fetoprotein Alpha-fetoprotein (AFP) is a polysaccharide found in some carcinomas. It is effective as a biochemical marker for monitoring the response of certain
Other Names/Abbreviations AFP 190.25 - Alpha-fetoprotein Alpha-fetoprotein (AFP) is a polysaccharide found in some carcinomas. It is effective as a biochemical marker for monitoring the response of certain
Basic patterns of liver damage what information can a liver biopsy provide and what clinical information does the pathologist need?
 Basic patterns of liver damage what information can a liver biopsy provide and what clinical information does the pathologist need? Rob Goldin r.goldin@imperial.ac.uk @robdgol FATTY LIVER DISEASE Brunt
Basic patterns of liver damage what information can a liver biopsy provide and what clinical information does the pathologist need? Rob Goldin r.goldin@imperial.ac.uk @robdgol FATTY LIVER DISEASE Brunt
Cholangiocarcinoma (Bile Duct Cancer)
") Cholangiocarcinoma (Bile Duct Cancer) The Bile Duct System (Biliary Tract) A network of bile ducts (tubes) connects the liver and the gallbladder to the small intestine. This network begins in the liver
Cholangiocarcinoma (Bile Duct Cancer) The Bile Duct System (Biliary Tract) A network of bile ducts (tubes) connects the liver and the gallbladder to the small intestine. This network begins in the liver
Liver Tumors. Prof. Dr. Ahmed El - Samongy
 Liver Tumors Prof. Dr. Ahmed El - Samongy Objective 1. Identify the most important features of common benign liver tumors 2. Know the risk factors, diagnosis, and management of hepatocellular carcinoma
Liver Tumors Prof. Dr. Ahmed El - Samongy Objective 1. Identify the most important features of common benign liver tumors 2. Know the risk factors, diagnosis, and management of hepatocellular carcinoma
BREAST PATHOLOGY. Fibrocystic Changes
 BREAST PATHOLOGY Lesions of the breast are very common, and they present as palpable, sometimes painful, nodules or masses. Most of these lesions are benign. Breast cancer is the 2 nd most common cause
BREAST PATHOLOGY Lesions of the breast are very common, and they present as palpable, sometimes painful, nodules or masses. Most of these lesions are benign. Breast cancer is the 2 nd most common cause
Avian Pathology. Bacterial diseases: histo slides. ECVP-ESVP Summer School 2012 Frédérique NGUYEN
 Avian Pathology Bacterial diseases: histo slides ECVP-ESVP Summer School 2012 Frédérique NGUYEN Bacterial diseases: histo slides B1. Turkey. Organs? Morphologic diagnosis? Special procedure? B2. Hen. Organ?
Avian Pathology Bacterial diseases: histo slides ECVP-ESVP Summer School 2012 Frédérique NGUYEN Bacterial diseases: histo slides B1. Turkey. Organs? Morphologic diagnosis? Special procedure? B2. Hen. Organ?
Supplemental Tables. Parasitic Schistosomiasis increase < 1. Genetic Hemochromatosis increase < 1. autoimmune Autoimmune hepatitis (AIH) increase < 1
 increase < 1") Supplemental Tables Supplemental Table 1 Various etiologies of liver cirrhosis and their association with liver stiffness and AST/ALT ratio Disease category Cause Example LS AST/ALT Inflammatory liver
Supplemental Tables Supplemental Table 1 Various etiologies of liver cirrhosis and their association with liver stiffness and AST/ALT ratio Disease category Cause Example LS AST/ALT Inflammatory liver
AMR in Liver Transplantation: Incidence
 AMR in Liver Transplantation: Incidence Primary AMR 1/3 to 1/2 of ABO-incompatible transplants Uncommon with ABO-compatible transplant Secondary AMR Unknown incidence: rarely tested Why is AMR uncommon
AMR in Liver Transplantation: Incidence Primary AMR 1/3 to 1/2 of ABO-incompatible transplants Uncommon with ABO-compatible transplant Secondary AMR Unknown incidence: rarely tested Why is AMR uncommon
CHAPTER 1. Alcoholic Liver Disease
 CHAPTER 1 Alcoholic Liver Disease Major Lesions of Alcoholic Liver Disease Alcoholic fatty liver - >90% of binge and chronic drinkers Alcoholic hepatitis precursor of cirrhosis Alcoholic cirrhosis end
CHAPTER 1 Alcoholic Liver Disease Major Lesions of Alcoholic Liver Disease Alcoholic fatty liver - >90% of binge and chronic drinkers Alcoholic hepatitis precursor of cirrhosis Alcoholic cirrhosis end
Viral hepatitis Blood Born hepatitis. Dr. MONA BADR Assistant Professor College of Medicine & KKUH
 Viral hepatitis Blood Born hepatitis Dr. MONA BADR Assistant Professor College of Medicine & KKUH Outline Introduction to hepatitis Characteristics of viral hepatitis Mode of transmission Markers of hepatitis
Viral hepatitis Blood Born hepatitis Dr. MONA BADR Assistant Professor College of Medicine & KKUH Outline Introduction to hepatitis Characteristics of viral hepatitis Mode of transmission Markers of hepatitis
HOW TO DEAL WITH THOSE ABNORMAL LIVER ENZYMES David C. Twedt DVM, DACVIM Colorado State University Fort Collins, CO
 HOW TO DEAL WITH THOSE ABNORMAL LIVER ENZYMES David C. Twedt DVM, DACVIM Colorado State University Fort Collins, CO The identification of abnormal liver enzymes usually indicates liver damage but rarely
HOW TO DEAL WITH THOSE ABNORMAL LIVER ENZYMES David C. Twedt DVM, DACVIM Colorado State University Fort Collins, CO The identification of abnormal liver enzymes usually indicates liver damage but rarely
Gastroenterology. Certification Examination Blueprint. Purpose of the exam
 Gastroenterology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified gastroenterologist
Gastroenterology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified gastroenterologist
Atrophy. Dystrophy. II. practical training 2 rd year Dentistry. Lucie Tučková
 Atrophy. Dystrophy. II. practical training 2 rd year Dentistry Lucie Tučková Atrophy Decrease in size of the cell or organ Reduction in cell size and/or cell number, or both Atrophic cells may have diminished
Atrophy. Dystrophy. II. practical training 2 rd year Dentistry Lucie Tučková Atrophy Decrease in size of the cell or organ Reduction in cell size and/or cell number, or both Atrophic cells may have diminished
LIVER CIRRHOSIS. The liver extracts nutrients from the blood and processes them for later use.
 LIVER CIRRHOSIS William Sanchez, M.D. & Jayant A. Talwalkar, M.D., M.P.H. Advanced Liver Disease Study Group Miles and Shirley Fiterman Center for Digestive Diseases Mayo College of Medicine Rochester,
LIVER CIRRHOSIS William Sanchez, M.D. & Jayant A. Talwalkar, M.D., M.P.H. Advanced Liver Disease Study Group Miles and Shirley Fiterman Center for Digestive Diseases Mayo College of Medicine Rochester,
HISTOPL4THOLOG1CAL STUDY OF LIVER
 HISTOPL4THOLOG1CAL STUDY OF LIVER 6.1 Inti-oduction The structural and functional organization of the liver has been described by hepatic lobule and hepatic acinus models, respectively (Jarvelainen, 2000).
HISTOPL4THOLOG1CAL STUDY OF LIVER 6.1 Inti-oduction The structural and functional organization of the liver has been described by hepatic lobule and hepatic acinus models, respectively (Jarvelainen, 2000).
End Stage Liver Disease & Disease Specific Indications for Liver Transplant. Susan Kang, RN, MSN, ANP-BC
 End Stage Liver Disease & Disease Specific Indications for Liver Transplant Susan Kang, RN, MSN, ANP-BC Introduction (https://www.srtr.org) What does the liver do? STORAGE METABOLIC DETOXIFICATION SYNTHETIC
End Stage Liver Disease & Disease Specific Indications for Liver Transplant Susan Kang, RN, MSN, ANP-BC Introduction (https://www.srtr.org) What does the liver do? STORAGE METABOLIC DETOXIFICATION SYNTHETIC
End Stage Liver Disease & Disease Specific Indications for Liver Transplant Susan Kang, RN, MSN, ANP BC
 End Stage Liver Disease & Disease Specific Indications for Liver Transplant Susan Kang, RN, MSN, ANP BC Introduction (https://www.srtr.org) 1 What does the liver do? STORAGE METABOLIC DETOXIFICATION SYNTHETIC
End Stage Liver Disease & Disease Specific Indications for Liver Transplant Susan Kang, RN, MSN, ANP BC Introduction (https://www.srtr.org) 1 What does the liver do? STORAGE METABOLIC DETOXIFICATION SYNTHETIC
Sinusoids and venous sinuses
 LYMPHOID SYSTEM General aspects Consists of organs that are made of lymphoid tissue; Immune defense Breakdown of red blood cells. 1 Sinusoids In place of capillaries Endothelium; often fenestrated More
LYMPHOID SYSTEM General aspects Consists of organs that are made of lymphoid tissue; Immune defense Breakdown of red blood cells. 1 Sinusoids In place of capillaries Endothelium; often fenestrated More
Interesting Cases from Liver Tumor Board. Jeffrey C. Weinreb, M.D.,FACR Yale University School of Medicine
 Interesting Cases from Liver Tumor Board Jeffrey C. Weinreb, M.D.,FACR Yale University School of Medicine jeffrey.weinreb@yale.edu Common Liver Diseases Hemangioma Cyst FNH Focal Fat/Sparing THID Non-Cirrhotic
Interesting Cases from Liver Tumor Board Jeffrey C. Weinreb, M.D.,FACR Yale University School of Medicine jeffrey.weinreb@yale.edu Common Liver Diseases Hemangioma Cyst FNH Focal Fat/Sparing THID Non-Cirrhotic
Virion Genome Genes and proteins Viruses and hosts Diseases Distinctive characteristics
 Hepadnaviruses Virion Genome Genes and proteins Viruses and hosts Diseases Distinctive characteristics Hepatitis viruses A group of unrelated pathogens termed hepatitis viruses cause the vast majority
Hepadnaviruses Virion Genome Genes and proteins Viruses and hosts Diseases Distinctive characteristics Hepatitis viruses A group of unrelated pathogens termed hepatitis viruses cause the vast majority
CrackCast Episode 28 Jaundice
 CrackCast Episode 28 Jaundice Episode overview: 1) Describe heme metabolism 2) List common pre-hepatic/hepatic/post-hepatic causes of jaundice Wisecracks: 1) What are clinical signs of liver disease? 2)
CrackCast Episode 28 Jaundice Episode overview: 1) Describe heme metabolism 2) List common pre-hepatic/hepatic/post-hepatic causes of jaundice Wisecracks: 1) What are clinical signs of liver disease? 2)
Navigating the Biliary Tract with CT & MR: An Imaging Approach to Bile Duct Obstruction
 Navigating the Biliary Tract with CT & MR: An Imaging Approach to Bile Duct Obstruction Ann S. Fulcher, MD Medical College of Virginia Virginia Commonwealth University Richmond, Virginia Objectives To
Navigating the Biliary Tract with CT & MR: An Imaging Approach to Bile Duct Obstruction Ann S. Fulcher, MD Medical College of Virginia Virginia Commonwealth University Richmond, Virginia Objectives To
Cirrhosis of the Liver
 235 60th Street, West New York, NJ 07093 T: (201) 854-4646 F: (201) 854-4647 810 Main Street, Hackensack, NJ 07601 T: (201) 488-0095 Cirrhosis of the Liver The liver, the largest organ in the body, is
235 60th Street, West New York, NJ 07093 T: (201) 854-4646 F: (201) 854-4647 810 Main Street, Hackensack, NJ 07601 T: (201) 488-0095 Cirrhosis of the Liver The liver, the largest organ in the body, is
Role of Liver Biopsy. Role of Liver Biopsy 9/3/2009. Liver Biopsies in Viral Hepatitis: Beyond Grading and Staging
 Liver Biopsies in Viral Hepatitis: Beyond Grading and Staging for further reference: Liver biopsy assessment in chronic viral hepatitis: a personal, practical approach Neil Theise, MD. Depts of Pathology
Liver Biopsies in Viral Hepatitis: Beyond Grading and Staging for further reference: Liver biopsy assessment in chronic viral hepatitis: a personal, practical approach Neil Theise, MD. Depts of Pathology
What is Liver Cancer? About the Liver
 Your liver is important and it has many functions. The top three are that it cleans your blood of toxins, gives you energy and produces bile for digestion. What is Liver Cancer? Cancer starts when cells
Your liver is important and it has many functions. The top three are that it cleans your blood of toxins, gives you energy and produces bile for digestion. What is Liver Cancer? Cancer starts when cells
LYMPH GLAND. By : Group 1
 LYMPH GLAND By : Group 1 ANATOMY LYMPH NODE Lymphatic Organs Red bone marrow Thymus gland Lymph nodes Lymph nodules Spleen Primary organs Secondary organs Lymph Nodes Firm, smooth-surfaced, bean-shaped
LYMPH GLAND By : Group 1 ANATOMY LYMPH NODE Lymphatic Organs Red bone marrow Thymus gland Lymph nodes Lymph nodules Spleen Primary organs Secondary organs Lymph Nodes Firm, smooth-surfaced, bean-shaped
Lymphoid System: cells of the immune system. Answer Sheet
 Lymphoid System: cells of the immune system Answer Sheet Q1 Which areas of the lymph node have most CD3 staining? A1 Most CD3 staining is present in the paracortex (T cell areas). This is towards the outside
Lymphoid System: cells of the immune system Answer Sheet Q1 Which areas of the lymph node have most CD3 staining? A1 Most CD3 staining is present in the paracortex (T cell areas). This is towards the outside
Anatomy Jessica Ferguson Ashley Dobos May 31, 2006 LIVER
 Anatomy Jessica Ferguson Ashley Dobos May 31, 2006 LIVER 1) Other Names: Reidel s Lobe normal anatomic variant; projection of the right lobe that can extend as far as the iliac crest (Tempkin, p.54, Anatomy).
Anatomy Jessica Ferguson Ashley Dobos May 31, 2006 LIVER 1) Other Names: Reidel s Lobe normal anatomic variant; projection of the right lobe that can extend as far as the iliac crest (Tempkin, p.54, Anatomy).
Viral Hepatitis. Background
 Viral Hepatitis Background Hepatitis or inflammation of the liver can be caused by infectious and noninfectious problems. Infectious etiologies include viruses, bacteria, fungi and parasites. Noninfectious
Viral Hepatitis Background Hepatitis or inflammation of the liver can be caused by infectious and noninfectious problems. Infectious etiologies include viruses, bacteria, fungi and parasites. Noninfectious
Appendix 5. EFSUMB Newsletter. Gastroenterological Ultrasound
 EFSUMB Newsletter 87 Examinations should encompass the full range of pathological conditions listed below A log book listing the types of examinations undertaken should be kept Training should usually
EFSUMB Newsletter 87 Examinations should encompass the full range of pathological conditions listed below A log book listing the types of examinations undertaken should be kept Training should usually
Imaging in breast cancer. Mammography and Ultrasound Donya Farrokh.MD Radiologist Mashhad University of Medical Since
 Imaging in breast cancer Mammography and Ultrasound Donya Farrokh.MD Radiologist Mashhad University of Medical Since A mammogram report is a key component of the breast cancer diagnostic process. A mammogram
Imaging in breast cancer Mammography and Ultrasound Donya Farrokh.MD Radiologist Mashhad University of Medical Since A mammogram report is a key component of the breast cancer diagnostic process. A mammogram
WSC , Conference 9, Case 1. Tissue from a nyala.
 WSC 2009-2010, Conference 9, Case 1. Tissue from a nyala. MICROSCOPIC DESCRIPTION: Heart, atrium (1 pt.): Approximately 40% of the atrial myocardium is replaced by areas of fibrous connective tissue (1
WSC 2009-2010, Conference 9, Case 1. Tissue from a nyala. MICROSCOPIC DESCRIPTION: Heart, atrium (1 pt.): Approximately 40% of the atrial myocardium is replaced by areas of fibrous connective tissue (1
Radiology of hepatobiliary diseases
 GI cycle - Lecture 14 436 Teams Radiology of hepatobiliary diseases Objectives 1. To Interpret plan x-ray radiograph of abdomen with common pathologies. 2. To know the common pathologies presentation.
GI cycle - Lecture 14 436 Teams Radiology of hepatobiliary diseases Objectives 1. To Interpret plan x-ray radiograph of abdomen with common pathologies. 2. To know the common pathologies presentation.
Imaging Guided Biopsy. Edited & Presented by ; Hussien A.B ALI DINAR. Msc Lecturer,Reporting Sonographer
 Imaging Guided Biopsy Edited & Presented by ; Hussien A.B ALI DINAR. Msc Lecturer,Reporting Sonographer Objective By the End of this lessons you should : Define what biopsy Justify Aim to perform biopsy
Imaging Guided Biopsy Edited & Presented by ; Hussien A.B ALI DINAR. Msc Lecturer,Reporting Sonographer Objective By the End of this lessons you should : Define what biopsy Justify Aim to perform biopsy
Imaging of liver and pancreas
 Imaging of liver and pancreas.. Disease of the liver Focal liver disease Diffusion liver disease Focal liver disease Benign Cyst Abscess Hemangioma FNH Hepatic adenoma HCC Malignant Fibrolamellar carcinoma
Imaging of liver and pancreas.. Disease of the liver Focal liver disease Diffusion liver disease Focal liver disease Benign Cyst Abscess Hemangioma FNH Hepatic adenoma HCC Malignant Fibrolamellar carcinoma
Cholelithiasis (Gallstones)
") GALL BLADDER Cholelithiasis (Gallstones) Gallstones afflict 10-20% of adult populations in northern hemisphere Western countries. Adult prevalence rates are higher in Latin American countries (20-40%)
GALL BLADDER Cholelithiasis (Gallstones) Gallstones afflict 10-20% of adult populations in northern hemisphere Western countries. Adult prevalence rates are higher in Latin American countries (20-40%)
LIVER & SPLEEN. Color index: Slides.. Important..Notes..Extra..
 LIVER & SPLEEN Color index: Slides.. Important..Notes..Extra.. Objectives: By the end of this lecture, the student should be able to describe: 1. The histological structure of liver with special emphasis
LIVER & SPLEEN Color index: Slides.. Important..Notes..Extra.. Objectives: By the end of this lecture, the student should be able to describe: 1. The histological structure of liver with special emphasis
Slide 154: Pancreas, H&E
 Slide 154: Pancreas, H&E the pancreas, located adjacent to the duodenum, is a mixed exocrine and endocrine gland; it is usually readily identifiable by the presence of the interspersed endocrine pancreatic
Slide 154: Pancreas, H&E the pancreas, located adjacent to the duodenum, is a mixed exocrine and endocrine gland; it is usually readily identifiable by the presence of the interspersed endocrine pancreatic
Pancreas composed of 2 parts: 1- exocrine gland 2- endocrine gland
 pancreas Pancreas composed of 2 parts: 1- exocrine gland 2- endocrine gland Acute pancreatitis Inflammation of the pancreas associated with acinar cell injury Clinical features: 1-abdominal pain cardinal
pancreas Pancreas composed of 2 parts: 1- exocrine gland 2- endocrine gland Acute pancreatitis Inflammation of the pancreas associated with acinar cell injury Clinical features: 1-abdominal pain cardinal
Diseases of the breast (1 of 2)
") Diseases of the breast (1 of 2) Introduction A histology introduction Normal ducts and lobules of the breast are lined by two layers of cells a layer of luminal cells overlying a second layer of myoepithelial
Diseases of the breast (1 of 2) Introduction A histology introduction Normal ducts and lobules of the breast are lined by two layers of cells a layer of luminal cells overlying a second layer of myoepithelial
Jordan University Faculty Of Medicine. Breast. Dr. Ahmed Salman. Assistant professor of anatomy & embryology
 Jordan University Faculty Of Medicine Breast Dr. Ahmed Salman Assistant professor of anatomy & embryology The breasts are specialized accessory glands of the skin that secretes milk. They are situated
Jordan University Faculty Of Medicine Breast Dr. Ahmed Salman Assistant professor of anatomy & embryology The breasts are specialized accessory glands of the skin that secretes milk. They are situated
DIFFERENTIAL DIAGNOSIS OF JAUNDICE
 CHARLES L. HARTSOCK, M.D. The yellow or greenish yellow staining of the blood plasma and body tissues, to which the clinical term jaundice has been applied, is due to an excessive amount of one of the
CHARLES L. HARTSOCK, M.D. The yellow or greenish yellow staining of the blood plasma and body tissues, to which the clinical term jaundice has been applied, is due to an excessive amount of one of the
2014 CURRENT ISSUES IN PATHOLOGY
 2014 CURRENT ISSUES IN PATHOLOGY SPECIAL STAINS IN LIVER BIOPSY PATHOLOGY Sanjay Kakar, MD University of California, San Francisco Trichrome stain : (1) Assess degree of fibrosis. H&E stain is not reliable
2014 CURRENT ISSUES IN PATHOLOGY SPECIAL STAINS IN LIVER BIOPSY PATHOLOGY Sanjay Kakar, MD University of California, San Francisco Trichrome stain : (1) Assess degree of fibrosis. H&E stain is not reliable
DIGESTIVE SYSTEM II ACCESSORY DIGESTIVE ORGANS
 DIGESTIVE SYSTEM II ACCESSORY DIGESTIVE ORGANS Dr. Larry Johnson Texas A& M University Objectives Distinguish between the parotid and submandibular salivary glands. Understand and identify the structural
DIGESTIVE SYSTEM II ACCESSORY DIGESTIVE ORGANS Dr. Larry Johnson Texas A& M University Objectives Distinguish between the parotid and submandibular salivary glands. Understand and identify the structural
Liver Pathology Lab 1. Shannon Martinson, 2017
 Liver Pathology Lab 1 Shannon Martinson, 2017 http://people.upei.ca/smartinson/ Case 1 Signalment: 10 year old MC DSH cat History: Inappetence and weight loss Fluid in the abdomen noted on US Esophageal
Liver Pathology Lab 1 Shannon Martinson, 2017 http://people.upei.ca/smartinson/ Case 1 Signalment: 10 year old MC DSH cat History: Inappetence and weight loss Fluid in the abdomen noted on US Esophageal
Cholangitis/ Cholangiohepatitis Syndrome (Inflammation of the Bile Duct System and Liver) Basics
 Basics") Glendale Animal Hospital 623-934-7243 www.familyvet.com Cholangitis/ Cholangiohepatitis Syndrome (Inflammation of the Bile Duct System and Liver) Basics OVERVIEW The liver is the largest gland in the body;
Glendale Animal Hospital 623-934-7243 www.familyvet.com Cholangitis/ Cholangiohepatitis Syndrome (Inflammation of the Bile Duct System and Liver) Basics OVERVIEW The liver is the largest gland in the body;
Liver failure &portal hypertension
 Liver failure &portal hypertension Objectives: by the end of this lecture each student should be able to : Diagnose liver failure (acute or chronic) List the causes of acute liver failure Diagnose and
Liver failure &portal hypertension Objectives: by the end of this lecture each student should be able to : Diagnose liver failure (acute or chronic) List the causes of acute liver failure Diagnose and
SECTION 2 CELL INJURY
 Adapted myocyte Normal myocyte Reversibly-injured myocyte SECTION 2 CELL INJURY Cell death 5/4/2014 1 5/4/2014 2 Reversible Degeneration Irreversible Cellular Swelling Fatty Change Hyaline Change Amyloid
Adapted myocyte Normal myocyte Reversibly-injured myocyte SECTION 2 CELL INJURY Cell death 5/4/2014 1 5/4/2014 2 Reversible Degeneration Irreversible Cellular Swelling Fatty Change Hyaline Change Amyloid