The International Federation of Head and Neck Oncologic Societies. Current Concepts in Head and Neck Surgery and Oncology
|
|
|
- Lucas Welch
- 5 years ago
- Views:
Transcription


1 The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology
2 The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology Thyroid Cancer Treatment of the Neck Ashok Shaha
3 Thyroid Literature Medline Thyroid disease 136,053 Thyroid tumors 33,554 New Paper on Thyroid Disease Every 3 Hours New Paper on Thyroid Cancer Every 8 Hours Thyroid Google search Thyroid Cancer Google search 36 million 21 million
4 American Thyroid Association (ATA) Consensus Review of the Anatomy, Terminology and Rationale for Lateral Neck Dissection in Differentiated Thyroid Cancers The ATA Surgical Affairs Committee Lateral Neck Dissection for Well Differentiated Thyroid Cancer Sub- Committee Robert L. Ferris, MD, PhD David Goldenberg, MD Megan Haymart, MD Ashok Shaha, MD Sheila Sheth, MD Julie Ann Sosa, MD Brendan C. Stack, Jr., MD Ralph P. Tufano, MD


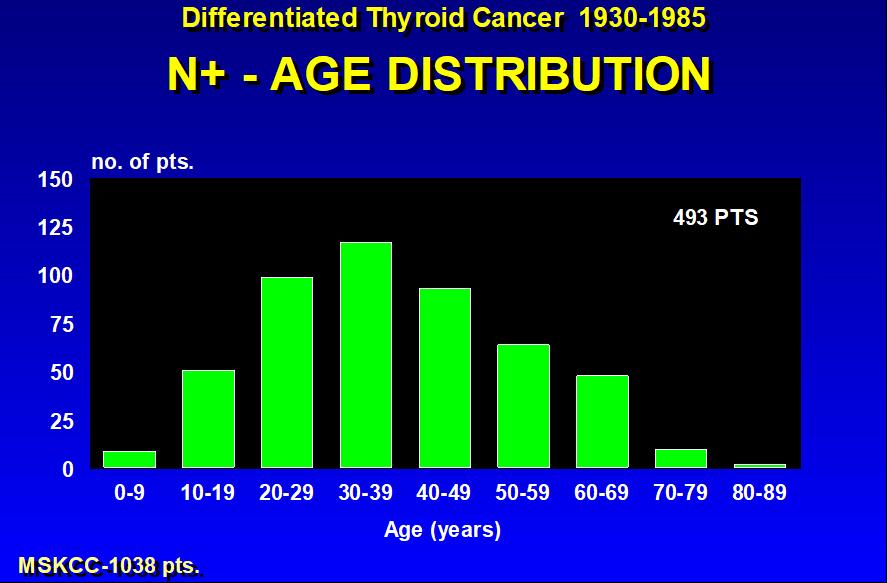
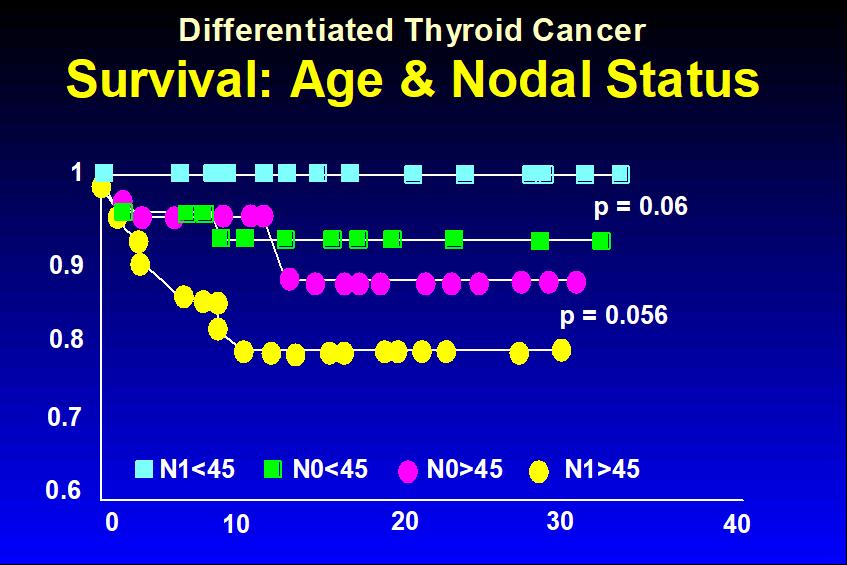
5 Lymphatic Drainage of the Thyroid Gland Bilateral drainage, extensive High incidence of regional metastasis 40-70% Multiple nodal groups at risk Lymphatic channels parallel venous drainage Must be considered when managing thyroid cancer
6 AJCC/UICC 2011 Staging Nodal Staging for Thyroid Cancer N x regional lymph nodes cannot be assessed N 0 No regional lymph node metastasis N 1 Regional lymph node metastasis N 1a Metastasis to Level VI pretracheal, paratracheal, prelaryngeal, delphian N 1b Metastasis to unilateral, bilateral or contralateral cervical or superior mediastinal lymph nodes
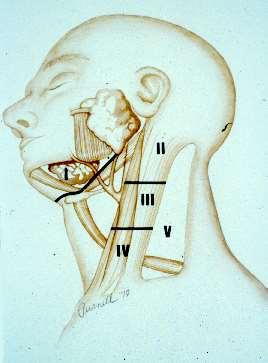
7

8 Diagrammatic Representation of the Neck Showing Various Nodal Levels and Sublevels
9 Differentiated Carcinoma of the Thyroid Prognostic Factors MSKCC Mayo Lahey Karolinska GAMES AGES MACIS AMES DAMES Grade Age Metastases Age DNA Age Grade Age Age Metastases Completeness Metastases Metastases of resection Extension Extension Invasion Extension Extension Size Size Size Size Size
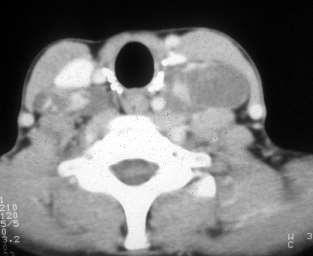
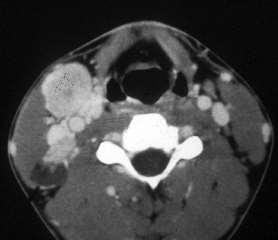
10 Pre-op Evaluation of the Neck CT scan Ultrasound: Suspected nodes Location FNA-Cytology, Thyroglobulin wash Evaluation of contralateral neck Parapharyngeal and retropharyngeal nodes
11
12
13 Thyroid Node-Met Detailed histologic characteristics Probably increases the risk of loco-regional metastases Extra-thyroidal extension (minor vs gross) Multifocality (microscopic vs macroscopic) Vascular invasion (intrathyroidal, extrathyroidal)
14 Thyroid- Node Met Clinco-pathologic features of the primary tumor Predict loco-regional metastases Size of the primary tumor > 0.5 cm in PTC > 2 cm in FTC/HCC Histology of the primary tumor PTC =TCV > FTC = HCC Age of the patient Children > Adults Genotyping BRAF positive
15
16
17
18
 40 30 20 21% 10 0 7% 3% 0-5 LN+ 6-10 LN+ > 10 LN+ (n=66) (n=29) (n=19) Leboulleux, JCEM,")
19 Recurrence (%) Number of LN s Predicts Recurrence (148 pts with LN mets, s/p total tx & routine VI, III, IV) % % 3% 0-5 LN LN+ > 10 LN+ (n=66) (n=29) (n=19) Leboulleux, JCEM, 2005
20 Recurrence (%) LN Extracapsular Extension & Recurrence (148 pts with LN mets, s/p total tx & routine VI, III, IV) > 3 (n=72) (n=23) (n=19) LN with Extracapsular Extension Leboulleux, JCEM, 2005
21 Factors: Loco-Regional Recurrence: Fewer than 5 Metastatic LN s 3% pn1 but cn0 4% 1-3 LN s with ENE 4% All Metastatic LN s < 2mm 5% 6-10 metastatic LN s 7% Fewer than 5 metastatic LN s 8% More than 5 metastatic LN s 19% More than 10 metastatic LN s 21% Any metastatic LN > 1cm 32% >3 metastatic LN s with ENE 32% Any metastatic LN > 3cm 73%
22 Management Guidelines for Patients with Thyroid Nodules and Differentiated Thyroid Cancer The American Thyroid Association Guidelines Taskforce 2009 Update R27b Prophylactic central-compartment neck dissection (ipsilateral or bilateral) may be performed in patients with papillary thyroid carcinoma with clinically uninvolved central neck lymph nodes, especially for advanced primary tumors (T3 or T4.) Recommendation C
23 Management of Neck in Thyroid Cancer Clinically Negative Intraoperative Management Look for TE groove nodes Look for sup mediastinal nodes Look for jugular nodes If any of these enlarged - do the respective clearance Central compartment clearance
24 Management of Neck in Thyroid Cancer Clinically Positive Intraoperative Management Berry picking not recommended, higher incidence of neck recurrence Modified neck dissection Preserving SCM IJV Accessory nerve Submandibular sal gland (Level I) RND - rarely indicated

25 Incision for Thyroidectomy and Neck Dissection
26 Practical Tips for Neck Dissection in Thyroid Cancer Review pre-op imaging very carefully CT/MRI/Ultrasound Review thyroid bed and paratracheal area Pre-op status of vocal cords and calcium levels Necklace incision Identify accessory nerve
27 Practical Tips for Neck Dissection in Thyroid Cancer Look for jugulodigastric nodes Avoid dissection on the surface of submandibular salivary gland Look for supraclavicular and retrojugular node Look for pre and paratracheal nodes Avoid lymphatic injury chyle leak, chyloma
28 Delphian Node Metastases in Thyroid Cancer 101 patients with Pap Ca 25% had metastatic tumor to the Delphian node Relation of Delphian node positivity with primary tumor and extra-thyroidal extension Association with additional node metastases to the central and lateral compartment Delphian node metastases is associated with heavier nodal burden Iyer/Shaha et al, Ann Surg 2011
29 Complications Paratracheal dissection - Hypoparathyroidism Lymphatic/chyle leaks - Parathyroid autotransplantation RLN injury Accessory nerve injury Horner s Syndrome
30 Neck Dissection Modified neck dissection Selective neck dissection Compartment-oriented neck dissection Radical neck dissection
31 Neck Dissection for Thyroid Cancer Role of pre-op ultrasound and U/S -guided FNA Microdissection (Tissel) Use of Gamma probe for intra-op localization Parathyroid autotransplantation
32 Sentinel Node Biopsy in Thyroid Cancer SLN can be located with radionucleide or Blue dye Limited or no clinical application
33 Rising Thyroglobulin Generally recurrence in nodes U/S and FNA CT scan Neck dissection RAI Impact on recurrent long term
34 Good judgment comes from experience; and experience comes from bad judgment!
35 Elective ND Radical ND U/S & U/S FNA No clinical finding Rising TGB No prognostic implication Thyroglobulin follow-up Only therapeutic ND Clinical follow-up Central compartment ND
36 Extent of Metastatic Disease in Neck Nodes from Papillary Ca of the Thyroid Type Micrometastasis Mini metastasis (by U/S of Tg) Minivolume metastasis Large volume metastasis Import on Outcome None None None Maybe (Regional or distant) Major metastasis Yes, older pt (Regional or distant)
37 Selective Paratracheal Node Dissection 304 patients with Papillary Cancer No prophylactic node dissection Only therapeutic 37% had therapeutic central compartment dissection Only 3 of 161 low risk patients developed central compartment recurrence (1.8%) Monchik et al., Surgery 2009
38 PET Scan & Neck Node Metastasis The nodal mets not responding to RAI and not localized by RAI PET positive Surgery preferred approach
39 Surgery for Recurrent Nodal Disease Frequent problem May be difficult to find the disease Missing neck nodes May be many other nodes Thyroglobulin may not become normal Other nodes may become obvious requiring further surgery Higher incidence of complications May not have much effect on long term outcome or
40 Recurrent Neck Disease A Scientific Reality OR Iatrogenic Problem Victim of Technology A Balance Between Risk of the Disease & Risk of the Treatment
41 Surgical experience is an important consideration while debating the issue of central compartment dissection Recurrence in the low-risk group necessitating central compartment reoperation is quite rare and in the high-risk group it is probably unavoidable It is important to develop a balance between the risk of recurrence against the benefit from elective nodal dissection Primum non nocere FIRST DO NO HARM Surgery 2009; 146;1224-7

42 The good physician treats the disease; the great physician treats the patient who has the disease. - Sir William Osler
43 Radiofrequency ablation of regional recurrence from welldifferentiated thyroid malignancy Dupuy DE, Monchik JM, et al Rhode Island Hospital, Providence, RI Surgery Dec; 130(6):971-7.
44 Percutaneous ethanol injection for treatment of cervical lymph node metastases in patients with papillary thyroid carcinoma Lewis BD, Hay ID, et al Dept. of Radiology, Mayo Clinic, Rochester, MN AJR Am J Roentgenol Mar;178(3):
45
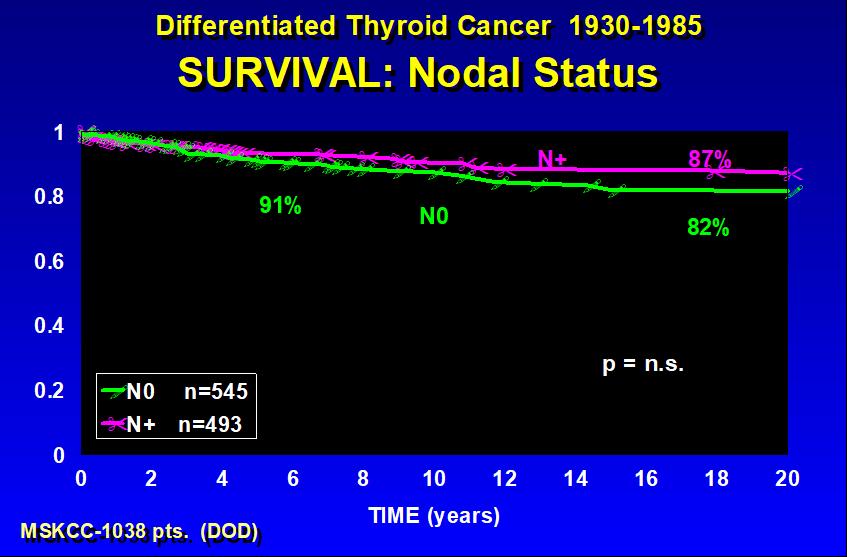
46 Summary High incidence of nodal mets in differentiated thyroid ca - But biologic difference - No survival impact Elective node dissection - not recommended Central compartment clearance - look for paratracheal and sup mediastinal and jugular nodes Lateral neck dissection - only if palpable nodes Modified neck dissection for clinical nodes Preserve SCM, IJV, XI and Level I No berry picking Role of RAI

47 Summary Patients with multiple positive neck nodes from papillary ca may have additional paratracheal, sup mediastinal, or lateral neck nodes, and may remain with persistent mild hyperthyroglobulinemia. We may not achieve biochemical cure.
The International Federation of Head and Neck Oncologic Societies. Current Concepts in Head and Neck Surgery and Oncology
 The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
Disclosures Nodal Management in Differentiated Thyroid Carcinoma
 Disclosures Nodal Management in Differentiated Thyroid Carcinoma Nothing to disclose Jonathan George, MD, MPH Assistant Professor UCSF Head and Neck Oncologic & Endocrine Surgery Objectives Overview Describe
Disclosures Nodal Management in Differentiated Thyroid Carcinoma Nothing to disclose Jonathan George, MD, MPH Assistant Professor UCSF Head and Neck Oncologic & Endocrine Surgery Objectives Overview Describe
Gerard M. Doherty, MD
 Surgical Management of Differentiated Thyroid Cancer: Update on 2015 ATA Guidelines Gerard M. Doherty, MD Chair of Surgery Utley Professor of Surgery and Medicine Boston University Surgeon-in-Chief Boston
Surgical Management of Differentiated Thyroid Cancer: Update on 2015 ATA Guidelines Gerard M. Doherty, MD Chair of Surgery Utley Professor of Surgery and Medicine Boston University Surgeon-in-Chief Boston
Ultrasound for Pre-operative Evaluation of Well Differentiated Thyroid Cancer
 Ultrasound for Pre-operative Evaluation of Well Differentiated Thyroid Cancer Its Not Just About the Nodes AACE Advances in Medical and Surgical Management of Thyroid Cancer - 2017 Robert A. Levine, MD,
Ultrasound for Pre-operative Evaluation of Well Differentiated Thyroid Cancer Its Not Just About the Nodes AACE Advances in Medical and Surgical Management of Thyroid Cancer - 2017 Robert A. Levine, MD,
Thyroid INTRODUCTION ANATOMY SUMMARY OF CHANGES
 AJC 7/14/06 1:19 PM Page 67 Thyroid C73.9 Thyroid gland SUMMARY OF CHANGES Tumor staging (T) has been revised and the categories redefined. T4 is now divided into T4a and T4b. Nodal staging (N) has been
AJC 7/14/06 1:19 PM Page 67 Thyroid C73.9 Thyroid gland SUMMARY OF CHANGES Tumor staging (T) has been revised and the categories redefined. T4 is now divided into T4a and T4b. Nodal staging (N) has been
Reoperative central neck surgery
 Reoperative central neck surgery R. Pandev, I. Tersiev, M. Belitova, A. Kouizi, D. Damyanov University Clinic of Surgery, Section Endocrine Surgery University Hospital Queen Johanna ISUL Medical University
Reoperative central neck surgery R. Pandev, I. Tersiev, M. Belitova, A. Kouizi, D. Damyanov University Clinic of Surgery, Section Endocrine Surgery University Hospital Queen Johanna ISUL Medical University
Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer
 Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer AACE - Advances in Medical and Surgical Management of Thyroid Cancer - 2018 Robert A. Levine, MD, FACE, ECNU Thyroid Center of New Hampshire Geisel
Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer AACE - Advances in Medical and Surgical Management of Thyroid Cancer - 2018 Robert A. Levine, MD, FACE, ECNU Thyroid Center of New Hampshire Geisel
Persistent & Recurrent Differentiated Thyroid Cancer
 Persistent & Recurrent Differentiated Thyroid Cancer Electron Kebebew University of California, San Francisco Department of Surgery Objectives Risk factors for persistent & recurrent disease Causes of
Persistent & Recurrent Differentiated Thyroid Cancer Electron Kebebew University of California, San Francisco Department of Surgery Objectives Risk factors for persistent & recurrent disease Causes of
Management guideline for patients with differentiated thyroid cancer. Teeraporn Ratanaanekchai ENT, KKU 17 October 2007
 Management guideline for patients with differentiated thyroid Teeraporn Ratanaanekchai ENT, KKU 17 October 2007 Incidence (Srinagarind Hospital, 2005, both sex) Site (all) cases % 1. Liver 1178 27 2. Lung
Management guideline for patients with differentiated thyroid Teeraporn Ratanaanekchai ENT, KKU 17 October 2007 Incidence (Srinagarind Hospital, 2005, both sex) Site (all) cases % 1. Liver 1178 27 2. Lung
Management of Recurrent Thyroid Cancer
 Management of Recurrent Thyroid Cancer Eric Genden, MD, MHA Isidore Professor and Chairman Department of Otolaryngology- Head and Neck Surgery Senior Associate Dean for Clinical Affairs The Icahn School
Management of Recurrent Thyroid Cancer Eric Genden, MD, MHA Isidore Professor and Chairman Department of Otolaryngology- Head and Neck Surgery Senior Associate Dean for Clinical Affairs The Icahn School
4/22/2010. Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey.
 Management of Differentiated Thyroid Cancer: Head Neck Surgeon Perspective Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey Thyroid gland Small endocrine gland:
Management of Differentiated Thyroid Cancer: Head Neck Surgeon Perspective Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey Thyroid gland Small endocrine gland:
Preoperative Evaluation
 Preoperative Evaluation Lateral compartment lymph nodes are easier to detect and are amenable to FNA Central compartment lymph nodes are much more difficult to detect and FNA (Tg washout testing is compromised)
Preoperative Evaluation Lateral compartment lymph nodes are easier to detect and are amenable to FNA Central compartment lymph nodes are much more difficult to detect and FNA (Tg washout testing is compromised)
Treatment of Cervical Lymph Node Metastases Differentiated Thyroid Cancer
 Treatment of Cervical Lymph Node Metastases Differentiated Thyroid Cancer Well Differentiated Thyroid Cancer Natural History and Prognosis EORTC AGES AMES MACIS QuickTime and a TIFF (LZW) decompressor
Treatment of Cervical Lymph Node Metastases Differentiated Thyroid Cancer Well Differentiated Thyroid Cancer Natural History and Prognosis EORTC AGES AMES MACIS QuickTime and a TIFF (LZW) decompressor
Surgery for Recurrent Thyroid cancer: Considerations and limitations
 Surgery for Recurrent Thyroid cancer: Considerations and limitations 2016 Thyroid Master Class February 13, 2016 Ara A. Chalian MD, FACS Surgical Patient Safety Officer University Of Pennsylvania Health
Surgery for Recurrent Thyroid cancer: Considerations and limitations 2016 Thyroid Master Class February 13, 2016 Ara A. Chalian MD, FACS Surgical Patient Safety Officer University Of Pennsylvania Health
WTC 2013 Panel Discussion: Minimal disease
 WTC 2013 Panel Discussion: Minimal disease Susan J. Mandel MD MPH Panelists Ken Ain Yasuhiro Ito Stephanie Lee Erich Sturgis Mark Urken Faculty/Presenter Disclosure Relationships with commercial interests
WTC 2013 Panel Discussion: Minimal disease Susan J. Mandel MD MPH Panelists Ken Ain Yasuhiro Ito Stephanie Lee Erich Sturgis Mark Urken Faculty/Presenter Disclosure Relationships with commercial interests
Dr J K Jekel Dept. Surgery University of Pretoria
 Dr J K Jekel Dept. Surgery University of Pretoria No Maybe ( T`s and C`s apply ) 1. Total thyroidectomy 2. Neck dissection only if nodes are involved 3. Ablative dose or doses of Radioactive Iodine 4.
Dr J K Jekel Dept. Surgery University of Pretoria No Maybe ( T`s and C`s apply ) 1. Total thyroidectomy 2. Neck dissection only if nodes are involved 3. Ablative dose or doses of Radioactive Iodine 4.
Dynamic Risk Stratification:
 Dynamic Risk Stratification: Using Risk Estimates to Guide Initial Management R Michael Tuttle, MD Clinical Director, Endocrinology Service Memorial Sloan Kettering Cancer Center Professor of Medicine
Dynamic Risk Stratification: Using Risk Estimates to Guide Initial Management R Michael Tuttle, MD Clinical Director, Endocrinology Service Memorial Sloan Kettering Cancer Center Professor of Medicine
How good are we at finding nodules? Thyroid Nodules Thyroid Cancer Epidemiology Initial management Long-term follow up Disease-free status
 New Perspectives in Thyroid Cancer Jennifer Sipos, MD Assistant Professor of Medicine Division of Endocrinology The Ohio State University Outline Thyroid Nodules Thyroid Cancer Epidemiology Initial management
New Perspectives in Thyroid Cancer Jennifer Sipos, MD Assistant Professor of Medicine Division of Endocrinology The Ohio State University Outline Thyroid Nodules Thyroid Cancer Epidemiology Initial management
Strategies for detection of recurrent disease in longterm follow-up of differentiated thyroid cancer
 Strategies for detection of recurrent disease in longterm follow-up of differentiated thyroid cancer A rational approach to longterm follow-up based on dynamic risk assessment. World Congress on Thyroid
Strategies for detection of recurrent disease in longterm follow-up of differentiated thyroid cancer A rational approach to longterm follow-up based on dynamic risk assessment. World Congress on Thyroid
2015 American Thyroid Association Thyroid Nodule and Cancer Guidelines
 2015 American Thyroid Association Thyroid Nodule and Cancer Guidelines Angela M. Leung, MD, MSc, ECNU November 5, 2016 Outline Workup of nontoxic thyroid nodule(s) Ultrasound FNAB Management of FNAB results
2015 American Thyroid Association Thyroid Nodule and Cancer Guidelines Angela M. Leung, MD, MSc, ECNU November 5, 2016 Outline Workup of nontoxic thyroid nodule(s) Ultrasound FNAB Management of FNAB results
Overview. Extraglandular Thyroid Lymphatics. Management of the Lateral Neck in Well-Differentiated Thyroid Carcinoma. David W. Eisele, M.D., F.A.C.S.
 Management of the Lateral Neck in Well-Differentiated Thyroid Carcinoma David W. Eisele, M.D., F.A.C.S. Head and Neck Surgery and Oncology U.C.S.F. Comprehensive Cancer Center University of California,
Management of the Lateral Neck in Well-Differentiated Thyroid Carcinoma David W. Eisele, M.D., F.A.C.S. Head and Neck Surgery and Oncology U.C.S.F. Comprehensive Cancer Center University of California,
New York, the nation s thyroid gland. Christopher Morley ( ), "Shore Leave"
, Shore Leave") New York, the nation s thyroid gland Christopher Morley (1890-1957), "Shore Leave" Thyroid Literature Medline Thyroid disease 136,053 Thyroid tumors 33,554 New Paper on Thyroid Disease Every 3 Hours New
New York, the nation s thyroid gland Christopher Morley (1890-1957), "Shore Leave" Thyroid Literature Medline Thyroid disease 136,053 Thyroid tumors 33,554 New Paper on Thyroid Disease Every 3 Hours New
Shifting Paradigms and Debates in the Management of Well-differentiated Thyroid Cancer
 DEBATE WJOES Shifting Paradigms and Debates in the Management of Well-differentiated Thyroid Cancer Shifting Paradigms and Debates in the Management of Well-differentiated Thyroid Cancer Ashok R Shaha
DEBATE WJOES Shifting Paradigms and Debates in the Management of Well-differentiated Thyroid Cancer Shifting Paradigms and Debates in the Management of Well-differentiated Thyroid Cancer Ashok R Shaha
Evaluation of thyroid isthmusectomy as a potential treatment for papillary thyroid carcinoma limited to the isthmus: A clinical study of 73 patients
 ORIGINAL ARTICLE Evaluation of thyroid isthmusectomy as a potential treatment for papillary thyroid carcinoma limited to the isthmus: A clinical study of 73 patients Jianbiao Wang, MM, 1 Haili Sun, BM,
ORIGINAL ARTICLE Evaluation of thyroid isthmusectomy as a potential treatment for papillary thyroid carcinoma limited to the isthmus: A clinical study of 73 patients Jianbiao Wang, MM, 1 Haili Sun, BM,
Risk Adapted Follow-Up
 Risk Adapted Follow-Up Individualizing Follow- Up Strategies R Michael Tuttle, MD Clinical Director, Endocrinology Service Memorial Sloan Kettering Cancer Center Professor of Medicine Weill Medical College
Risk Adapted Follow-Up Individualizing Follow- Up Strategies R Michael Tuttle, MD Clinical Director, Endocrinology Service Memorial Sloan Kettering Cancer Center Professor of Medicine Weill Medical College
THYROID CANCER IN CHILDREN. Humberto Lugo-Vicente MD FACS FAAP Professor Pediatric Surgery UPR School of Medicine
 THYROID CANCER IN CHILDREN Humberto Lugo-Vicente MD FACS FAAP Professor Pediatric Surgery UPR School of Medicine Thyroid nodules Rare Female predominance 4-fold as likely to be malignant Hx Radiation exposure?
THYROID CANCER IN CHILDREN Humberto Lugo-Vicente MD FACS FAAP Professor Pediatric Surgery UPR School of Medicine Thyroid nodules Rare Female predominance 4-fold as likely to be malignant Hx Radiation exposure?
Management of Thyroid Nodules
 Management of Thyroid Nodules 38 y/o female with solid 1.5 cm right Thyroid nodule. TSH=0.68 Vincent J. Reid, MD., FACS Thyroid Cancer Incidence & Mortality 1974 to 2004 Overall Women Men Mortality 1 Cancer
Management of Thyroid Nodules 38 y/o female with solid 1.5 cm right Thyroid nodule. TSH=0.68 Vincent J. Reid, MD., FACS Thyroid Cancer Incidence & Mortality 1974 to 2004 Overall Women Men Mortality 1 Cancer
Current Issues in Thyroid Cancer Surgery in 2017
 Current Issues in Thyroid Cancer Surgery in 2017 Dr. David Goldstein MD Msc FRCSC FACS Associate Professor, Department Otolaryngology Head & Neck Surgery, U of T Department of Surgical Oncology, Princess
Current Issues in Thyroid Cancer Surgery in 2017 Dr. David Goldstein MD Msc FRCSC FACS Associate Professor, Department Otolaryngology Head & Neck Surgery, U of T Department of Surgical Oncology, Princess
Thyroid Cancer: When to Treat? MEGAN R. HAYMART, MD
 Thyroid Cancer: When to Treat? MEGAN R. HAYMART, MD ASSOCIATE PROFESSOR OF MEDICINE UNIVERSITY OF MICHIGAN MICHIGAN AACE 2018 ANNUAL MEETING Thyroid Cancer: When Not to Treat? FOCUS WILL BE ON LOW-RISK
Thyroid Cancer: When to Treat? MEGAN R. HAYMART, MD ASSOCIATE PROFESSOR OF MEDICINE UNIVERSITY OF MICHIGAN MICHIGAN AACE 2018 ANNUAL MEETING Thyroid Cancer: When Not to Treat? FOCUS WILL BE ON LOW-RISK
Long Term Follow-Up for Differentiated Thyroid Cancer: The Mayo Experience
 Long Term Follow-Up for Differentiated Thyroid Cancer: The Mayo Experience Geoffrey B. Thompson, MD Professor of Surgery College of Medicine, Mayo Clinic Differentiated Thyroid Cancer Objectives Overview
Long Term Follow-Up for Differentiated Thyroid Cancer: The Mayo Experience Geoffrey B. Thompson, MD Professor of Surgery College of Medicine, Mayo Clinic Differentiated Thyroid Cancer Objectives Overview
Prophylactic Central Compartment Neck Dissection(CCND) for Papillary Thyroid Cancer: Con
 for Papillary Thyroid Cancer: Con") Prophylactic Central Compartment Neck Dissection(CCND) for Papillary Thyroid Cancer: Con Christopher R. McHenry, M.D. Vice Chairman Department of Surgery MetroHealth Medical Center Professor of Surgery
Prophylactic Central Compartment Neck Dissection(CCND) for Papillary Thyroid Cancer: Con Christopher R. McHenry, M.D. Vice Chairman Department of Surgery MetroHealth Medical Center Professor of Surgery
Minimalistic Initial Therapy Options For Low Risk Papillary Thyroid Cancer
 Minimalistic Initial Therapy Options For Low Risk Papillary Thyroid Cancer An emphasis on proper patient selection R Michael Tuttle, MD Clinical Director, Endocrinology Service Memorial Sloan Kettering
Minimalistic Initial Therapy Options For Low Risk Papillary Thyroid Cancer An emphasis on proper patient selection R Michael Tuttle, MD Clinical Director, Endocrinology Service Memorial Sloan Kettering
CAP Cancer Protocol and ecc Summary of Changes for August 2014 Thyroid Agile Release
 CAP Cancer Protocol and ecc Summary of Changes for August 2014 Thyroid Agile Release 2 REVISION HISTORY Date Author / Editor Comments 5/19/2014 Jaleh Mirza Created the document 8/12/2014 Samantha Spencer/Jaleh
CAP Cancer Protocol and ecc Summary of Changes for August 2014 Thyroid Agile Release 2 REVISION HISTORY Date Author / Editor Comments 5/19/2014 Jaleh Mirza Created the document 8/12/2014 Samantha Spencer/Jaleh
6. Cervical Lymph Nodes and Unknown Primary Tumors of the Head and Neck
 1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
Avi Khafif, MD, Rami Ben-Yosef, MD, Avrum Abergel, MD, Ada Kesler, MD, Roee Landsberg, MD, Dan M. Fliss, MD
 ORIGINAL ARTICLE ELECTIVE PARATRACHEAL NECK DISSECTION FOR LATERAL METASTASES FROM PAPILLARY CARCINOMA OF THE THYROID: IS IT INDICATED? Avi Khafif, MD, Rami Ben-Yosef, MD, Avrum Abergel, MD, Ada Kesler,
ORIGINAL ARTICLE ELECTIVE PARATRACHEAL NECK DISSECTION FOR LATERAL METASTASES FROM PAPILLARY CARCINOMA OF THE THYROID: IS IT INDICATED? Avi Khafif, MD, Rami Ben-Yosef, MD, Avrum Abergel, MD, Ada Kesler,
40 TH EUROPEAN CONGRESS 0F CYTOLOGY LIVERPOOL, UK October 2-5, 2016
 Outcomes from the diagnostic approach of thyroid lesions using US-FNA and LBC in clinical practice Emmanouel Mastorakis MD PhD Cytopathologist Director in Cytopathology Laboratory Regional General Hospital
Outcomes from the diagnostic approach of thyroid lesions using US-FNA and LBC in clinical practice Emmanouel Mastorakis MD PhD Cytopathologist Director in Cytopathology Laboratory Regional General Hospital
10/24/2008. Surgery for Well-differentiated Thyroid Carcinoma- The Primary
 Surgery for Well-differentiated Thyroid Carcinoma- The Primary Head and Neck Endocrine Surgery Department of Otolaryngology-Head and Neck Surgery, UCSF October 24-25, 2008 Robert A. Sofferman, MD Professor
Surgery for Well-differentiated Thyroid Carcinoma- The Primary Head and Neck Endocrine Surgery Department of Otolaryngology-Head and Neck Surgery, UCSF October 24-25, 2008 Robert A. Sofferman, MD Professor
Prediction of ipsilateral and contralateral central lymph node metastasis in unilateral papillary thyroid carcinoma: a retrospective study
 Original Article Prediction of ipsilateral and contralateral central lymph node metastasis in unilateral papillary thyroid carcinoma: a retrospective study Qiang Chen, Xiu-He Zou, Tao Wei, Qiu-Shi Huang,
Original Article Prediction of ipsilateral and contralateral central lymph node metastasis in unilateral papillary thyroid carcinoma: a retrospective study Qiang Chen, Xiu-He Zou, Tao Wei, Qiu-Shi Huang,
Central and lateral neck dissection for differentiated thyroid cancer Diferansiye tiroid kanserlerinde santral ve lateral boyun diseksiyonu tekniği
 Central and lateral neck dissection for differentiated thyroid cancer Diferansiye tiroid kanserlerinde santral ve lateral boyun diseksiyonu tekniği Leigh Delbridge President, International Association
Central and lateral neck dissection for differentiated thyroid cancer Diferansiye tiroid kanserlerinde santral ve lateral boyun diseksiyonu tekniği Leigh Delbridge President, International Association
Head & Neck Clinical Sub Group. Network Agreed Imaging Guidelines for UAT and Thyroid Cancer. Measure Nos: 11-1C-105i & 11-1C-106i
 Greater Manchester, Lancashire & South Cumbria Strategic Clinical Network & Senate Head & Neck Clinical Sub Group Network Agreed Imaging Guidelines for UAT and Thyroid Cancer Measure Nos: 11-1C-105i &
Greater Manchester, Lancashire & South Cumbria Strategic Clinical Network & Senate Head & Neck Clinical Sub Group Network Agreed Imaging Guidelines for UAT and Thyroid Cancer Measure Nos: 11-1C-105i &
Thyroid Surgery: Lobectomy, total thyroidectomy, LN biopsies or only watchful waiting?
 Thyroid Surgery: Lobectomy, total thyroidectomy, LN biopsies or only watchful waiting? Jacob Moalem, MD, FACS Associate Professor Endocrine Surgery and Endocrinology URMC Agenda 1. When is lobectomy alone
Thyroid Surgery: Lobectomy, total thyroidectomy, LN biopsies or only watchful waiting? Jacob Moalem, MD, FACS Associate Professor Endocrine Surgery and Endocrinology URMC Agenda 1. When is lobectomy alone
Differentiated Thyroid Cancer: Initial Management
 Page 1 ATA HOME GIVE ONLINE ABOUT THE ATA JOIN THE ATA MEMBER SIGN-IN INFORMATION FOR PATIENTS FIND A THYROID SPECIALIST Home Management Guidelines for Patients with Thyroid Nodules and Differentiated
Page 1 ATA HOME GIVE ONLINE ABOUT THE ATA JOIN THE ATA MEMBER SIGN-IN INFORMATION FOR PATIENTS FIND A THYROID SPECIALIST Home Management Guidelines for Patients with Thyroid Nodules and Differentiated
Canadian Scientific Journal. Intraoperative color detection of lymph nodes metastases in thyroid cancer
 Canadian Scientific Journal 2 (2014) Contents lists available at Canadian Scientific Journal Canadian Scientific Journal journal homepage: Intraoperative color detection of lymph nodes metastases in thyroid
Canadian Scientific Journal 2 (2014) Contents lists available at Canadian Scientific Journal Canadian Scientific Journal journal homepage: Intraoperative color detection of lymph nodes metastases in thyroid
Thyroid Gland. Protocol applies to all malignant tumors of the thyroid gland, except lymphomas.
 Thyroid Gland Protocol applies to all malignant tumors of the thyroid gland, except lymphomas. Procedures Cytology (No Accompanying Checklist) Partial Thyroidectomy Total Thyroidectomy With/Without Lymph
Thyroid Gland Protocol applies to all malignant tumors of the thyroid gland, except lymphomas. Procedures Cytology (No Accompanying Checklist) Partial Thyroidectomy Total Thyroidectomy With/Without Lymph
3/29/2012. Thyroid cancer- what s new. Thyroid Cancer. Thyroid cancer is now the most rapidly increasing cancer in women
 Thyroid cancer- what s new Thyroid Cancer Changing epidemiology Molecular markers Lymph node dissection Technical advances rhtsh Genetic testing and prophylactic surgery Vandetanib What s new? Jessica
Thyroid cancer- what s new Thyroid Cancer Changing epidemiology Molecular markers Lymph node dissection Technical advances rhtsh Genetic testing and prophylactic surgery Vandetanib What s new? Jessica
How Will (Should) the Latest Guidelines Affect the Endocrinologist s Management of Thyroid Cancer? AACE 2017
 the Latest Guidelines Affect the Endocrinologist s Management of Thyroid Cancer? AACE 2017") How Will (Should) the Latest Guidelines Affect the Endocrinologist s Management of Thyroid Cancer? AACE 2017 Bryan R. Haugen, MD University of Colorado, School of Medicine Outline Some statistics New guidelines
How Will (Should) the Latest Guidelines Affect the Endocrinologist s Management of Thyroid Cancer? AACE 2017 Bryan R. Haugen, MD University of Colorado, School of Medicine Outline Some statistics New guidelines
PEDIATRIC Ariel Katz MD
 PEDIATRIC Ariel Katz MD Dept. Otolaryngology Head &Neck Surgery Wolfson Medical Center Holon, Israel OBJECTIVES Overview/Background Epidemiology/Etiology Intro to Guidelines Workup Treatment Follow-Up
PEDIATRIC Ariel Katz MD Dept. Otolaryngology Head &Neck Surgery Wolfson Medical Center Holon, Israel OBJECTIVES Overview/Background Epidemiology/Etiology Intro to Guidelines Workup Treatment Follow-Up
Clinical Guidance in Thyroid Cancers. Stephen Robinson Imperial at St Mary s On behalf of BTA
 Clinical Guidance in Thyroid Cancers Stephen Robinson Imperial at St Mary s On behalf of BTA Background to thyroid cancer Incidence probably increasing slowly 1971-95; 2.3 women 0.9 men /100,000 2001;
Clinical Guidance in Thyroid Cancers Stephen Robinson Imperial at St Mary s On behalf of BTA Background to thyroid cancer Incidence probably increasing slowly 1971-95; 2.3 women 0.9 men /100,000 2001;
What? When? Why? (How?)
") Surgery of the Central Neck in Thyroid Cancer Dana M Hartl MD PhD Haïtham Mirghani MD Nothing to disclose Disclosure 2 Central Neck Dissection What? When? Why? (How?) What is it? Terminology for neck dissection
Surgery of the Central Neck in Thyroid Cancer Dana M Hartl MD PhD Haïtham Mirghani MD Nothing to disclose Disclosure 2 Central Neck Dissection What? When? Why? (How?) What is it? Terminology for neck dissection
FACULTY OF MEDICINE SIRIRAJ HOSPITAL
 Neck Dissection Pornchai O-charoenrat MD, PhD Division of Head, Neck and Breast Surgery Department of Surgery FACULTY OF MEDICINE SIRIRAJ HOSPITAL Introduction Status of the cervical lymph nodes is the
Neck Dissection Pornchai O-charoenrat MD, PhD Division of Head, Neck and Breast Surgery Department of Surgery FACULTY OF MEDICINE SIRIRAJ HOSPITAL Introduction Status of the cervical lymph nodes is the
Thyroid Neoplasm. ORL-Head and neck Surgery 2014
 In The Name of God Thyroid Neoplasm ORL-Head and neck Surgery 2014 Malignant Neoplasm By age 90, virtually everyone has nodules Estimates of cancer prevalence at autopsy 4% to 36% Why these lesions are
In The Name of God Thyroid Neoplasm ORL-Head and neck Surgery 2014 Malignant Neoplasm By age 90, virtually everyone has nodules Estimates of cancer prevalence at autopsy 4% to 36% Why these lesions are
Case Scenario #1 Larynx
 Case Scenario #1 Larynx 56 year old white female who presented with a 2 month history of hoarseness treated with antibiotics, but with no improvement. In the last 3 weeks, she has had a 15 lb weight loss,
Case Scenario #1 Larynx 56 year old white female who presented with a 2 month history of hoarseness treated with antibiotics, but with no improvement. In the last 3 weeks, she has had a 15 lb weight loss,
This form may provide more data elements than required for collection by standard setters such as NCI SEER, CDC NPCR, and CoC NCDB.
 1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
Thyroid Nodule. Disclosure. Learning Objectives P A P A P A 3/18/2014. Nothing to disclose.
 Thyroid Nodule Evaluating the patient with a thyroid nodule and some management options. Miguel V. Valdez PA C Disclosure Nothing to disclose. Learning Objectives Examination of thyroid gland Options for
Thyroid Nodule Evaluating the patient with a thyroid nodule and some management options. Miguel V. Valdez PA C Disclosure Nothing to disclose. Learning Objectives Examination of thyroid gland Options for
Imaging in Thyroid Cancer
 Imaging in Thyroid Cancer Susan J. Mandel MD MPH University of Pennsylvania School of Medicine Philadelphia, PA I-123 Ultrasound Background Radioiodine ablation of thyroid remnants after surgery is a generally
Imaging in Thyroid Cancer Susan J. Mandel MD MPH University of Pennsylvania School of Medicine Philadelphia, PA I-123 Ultrasound Background Radioiodine ablation of thyroid remnants after surgery is a generally
Initial surgery for differentiated thyroid cancer: What is the appropriate extent and attendant risks and benefits?
 Initial surgery for differentiated thyroid cancer: What is the appropriate extent and attendant risks and benefits? Julie Ann Sosa, MD MA FACS Professor of Surgery and Medicine Chief, Section of Endocrine
Initial surgery for differentiated thyroid cancer: What is the appropriate extent and attendant risks and benefits? Julie Ann Sosa, MD MA FACS Professor of Surgery and Medicine Chief, Section of Endocrine
Frequency and pattern of central lymph node metastasis in papillary carcinoma of the thyroid isthmus
 ORIGINAL ARTICLE Frequency and pattern of central lymph node metastasis in papillary carcinoma of the thyroid isthmus Chang Myeon Song, MD, 1 Dong Won Lee, MD, 1 Yong Bae Ji, MD, PhD, 1 Jin Hyeok Jeong,
ORIGINAL ARTICLE Frequency and pattern of central lymph node metastasis in papillary carcinoma of the thyroid isthmus Chang Myeon Song, MD, 1 Dong Won Lee, MD, 1 Yong Bae Ji, MD, PhD, 1 Jin Hyeok Jeong,
Dilemmas in Cytopathology and Histopathology
 Dilemmas in Cytopathology and Histopathology Yuri E. Nikiforov, MD, PhD Division of Molecular & Genomic Pathology University of Pittsburgh Medical Center, USA Objectives Discuss new WHO classification
Dilemmas in Cytopathology and Histopathology Yuri E. Nikiforov, MD, PhD Division of Molecular & Genomic Pathology University of Pittsburgh Medical Center, USA Objectives Discuss new WHO classification
Differentiated Thyroid Carcinoma
 Differentiated Thyroid Carcinoma The GOOD cancer? Jennifer Sipos, MD Associate Professor of Medicine Director, Benign Thyroid Program Division of Endocrinology, Diabetes and Metabolism The Ohio State University
Differentiated Thyroid Carcinoma The GOOD cancer? Jennifer Sipos, MD Associate Professor of Medicine Director, Benign Thyroid Program Division of Endocrinology, Diabetes and Metabolism The Ohio State University
The International Federation of Head and Neck Oncologic Societies. Current Concepts in Head and Neck Surgery and Oncology
 The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
What s an NIFTP? Keeping Up To Date in Thyroid 2018
 What s an NIFTP? Keeping Up To Date in Thyroid 2018 Kathleen Hands, MD, FACE, ECNU Director, Thyroid Center of South Texas Assistant Clinical Professor UTHSCSA DrHands@Thyroid-Center.com 210-844-6163 text
What s an NIFTP? Keeping Up To Date in Thyroid 2018 Kathleen Hands, MD, FACE, ECNU Director, Thyroid Center of South Texas Assistant Clinical Professor UTHSCSA DrHands@Thyroid-Center.com 210-844-6163 text
Pediatric Thyroid Cancer Lung Metastases. Liora Lazar MD
 Pediatric Thyroid Cancer Lung Metastases Liora Lazar MD Differentiated thyroid cancer (DTC) The 3rd most common solid tumor in childhood and adolescence Accounting for 1.5%-3% of all childhood cancers
Pediatric Thyroid Cancer Lung Metastases Liora Lazar MD Differentiated thyroid cancer (DTC) The 3rd most common solid tumor in childhood and adolescence Accounting for 1.5%-3% of all childhood cancers
AJCC Staging of Head & Neck Cancer (7 th edition, 2010) -LIP & ORAL CAVITY-
 -LIP & ORAL CAVITY-") TX: primary tumor cannot be assessed T0: no evidence of primary tumor Tis: carcinoma in situ. T1: tumor is 2 cm or smaller AJCC Staging of Head & Neck Cancer (7 th edition, 2010) -LIP & ORAL CAVITY- T2:
TX: primary tumor cannot be assessed T0: no evidence of primary tumor Tis: carcinoma in situ. T1: tumor is 2 cm or smaller AJCC Staging of Head & Neck Cancer (7 th edition, 2010) -LIP & ORAL CAVITY- T2:
An Unexpected Cause of Hypoglycemia
 An Unexpected Cause of Hypoglycemia Stacey A. Milan, MD FACS Surgical Oncology Nothing to disclose Disclosures Objectives Identify indications for workup of hypoglycemia Define work up for hypoglycemic
An Unexpected Cause of Hypoglycemia Stacey A. Milan, MD FACS Surgical Oncology Nothing to disclose Disclosures Objectives Identify indications for workup of hypoglycemia Define work up for hypoglycemic
AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS
 AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS PAPILLARY THYROID CARCINOMA Clinical Any age Microscopic to large Female: Male= 2-4:1 Radiation history Lymph nodes Prognosis
AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS PAPILLARY THYROID CARCINOMA Clinical Any age Microscopic to large Female: Male= 2-4:1 Radiation history Lymph nodes Prognosis
- RET/PTC rearrangement: 20% papillary thyroid cancer - RET: medullary thyroid cancer
 Thyroid Cancer UpToDate: Introduction: Risk Factors: Biology: Symptoms: Diagnosis: 1. Lenvina is the first line therapy with powerful durable response and superior PFS in pts with RAI-refractory disease.
Thyroid Cancer UpToDate: Introduction: Risk Factors: Biology: Symptoms: Diagnosis: 1. Lenvina is the first line therapy with powerful durable response and superior PFS in pts with RAI-refractory disease.
EVERYTHING YOU WANTED TO KNOW ABOUT. Robin Billet, MA, CTR, Head & Neck CTAP Member May 9, 2013
 EVERYTHING YOU WANTED TO KNOW ABOUT. Robin Billet, MA, CTR, Head & Neck CTAP Member May 9, 2013 Head and Neck Coding and Staging Head and Neck Coding and Staging Anatomy & Primary Site Sequencing and MPH
EVERYTHING YOU WANTED TO KNOW ABOUT. Robin Billet, MA, CTR, Head & Neck CTAP Member May 9, 2013 Head and Neck Coding and Staging Head and Neck Coding and Staging Anatomy & Primary Site Sequencing and MPH
Review Article Management of thyroid carcinoma Alauddin M, Joarder AH
 Management of thyroid carcinoma Alauddin M, Joarder AH The ORION Medical Journal 2004 May;18:163-166 Overview The two most common forms of thyroid cancer, papillaryand follicular thyroid cancer, together
Management of thyroid carcinoma Alauddin M, Joarder AH The ORION Medical Journal 2004 May;18:163-166 Overview The two most common forms of thyroid cancer, papillaryand follicular thyroid cancer, together
Thyroid nodules - medical and surgical management. Endocrinology and Endocrine Surgery Manchester Royal Infirmary
 Thyroid nodules - medical and surgical management JRE Davis NR Parrott Endocrinology and Endocrine Surgery Manchester Royal Infirmary Thyroid nodules - prevalence Thyroid nodules common, increase with
Thyroid nodules - medical and surgical management JRE Davis NR Parrott Endocrinology and Endocrine Surgery Manchester Royal Infirmary Thyroid nodules - prevalence Thyroid nodules common, increase with
Oral cancer: Prognosis & Treatment. Dr. Hani Al Sheikh Radhi
 Oral cancer: Prognosis & Treatment Dr. Hani Al Sheikh Radhi Prognostic factors in Oral caner TNM staging T stage N stage M stage Site Histological Factors Vascular & Perineural Invasion Surgical Margins
Oral cancer: Prognosis & Treatment Dr. Hani Al Sheikh Radhi Prognostic factors in Oral caner TNM staging T stage N stage M stage Site Histological Factors Vascular & Perineural Invasion Surgical Margins
Adjuvant therapy for thyroid cancer
 Carcinoma of the thyroid Adjuvant therapy for thyroid cancer John Hay Department of Radiation Oncology Vancouver Cancer Centre Department of Surgery UBC 1% of all new malignancies 0.5% in men 1.5% in women
Carcinoma of the thyroid Adjuvant therapy for thyroid cancer John Hay Department of Radiation Oncology Vancouver Cancer Centre Department of Surgery UBC 1% of all new malignancies 0.5% in men 1.5% in women
YCN Thyroid NSSG. *** VALID ON DATE OF PRINTING ONLY - all guidelines available at *** page 1 of 8 version number: 1.
 YCN Thyroid NSSG Guidelines on Indications for Thyroid Surgery, Prophylactic Level 6 and Radioiodine plus follow-up of low risk differentiated thyroid cancer page 1 of 8 i Document Control Title Author(s)
YCN Thyroid NSSG Guidelines on Indications for Thyroid Surgery, Prophylactic Level 6 and Radioiodine plus follow-up of low risk differentiated thyroid cancer page 1 of 8 i Document Control Title Author(s)
Neck Dissection. Asst Professor Jeeve Kanagalingam MA (Cambridge), BM BCh (Oxford), MRCS (Eng), DLO, DOHNS, FRCS ORL-HNS (Eng), FAMS (ORL)
, BM BCh (Oxford), MRCS (Eng), DLO, DOHNS, FRCS ORL-HNS (Eng), FAMS (ORL)") Neck Dissection Asst Professor Jeeve Kanagalingam MA (Cambridge), BM BCh (Oxford), MRCS (Eng), DLO, DOHNS, FRCS ORL-HNS (Eng), FAMS (ORL) History radical neck Henry Butlin proposed enbloc removal of upper
Neck Dissection Asst Professor Jeeve Kanagalingam MA (Cambridge), BM BCh (Oxford), MRCS (Eng), DLO, DOHNS, FRCS ORL-HNS (Eng), FAMS (ORL) History radical neck Henry Butlin proposed enbloc removal of upper
Salivary Glands tumors
 Salivary Glands tumors Sal.Gl. 1 Salivary Glands tumors Work-up procedure TNM staging Primary treatment Follow-up Treatment of recurrent and/or metastatic disease References Sal.Gl. 2 Standard clinical
Salivary Glands tumors Sal.Gl. 1 Salivary Glands tumors Work-up procedure TNM staging Primary treatment Follow-up Treatment of recurrent and/or metastatic disease References Sal.Gl. 2 Standard clinical
Changing trends in the management of well-differentiated thyroid carcinoma in Korea
 2016, 63 (6), 515-521 Original Changing trends in the management of well-differentiated thyroid carcinoma in Korea Yong Sang Lee, Hang-Seok Chang and Cheong Soo Park Thyroid Cancer Center, Department of
2016, 63 (6), 515-521 Original Changing trends in the management of well-differentiated thyroid carcinoma in Korea Yong Sang Lee, Hang-Seok Chang and Cheong Soo Park Thyroid Cancer Center, Department of
NAACCR Hospital Registry Webinar Series
 NAACCR Hospital Registry Webinar Series Shannon Vann, CTR Jim Hofferkamp, CTR Webinar Series 1 Abstracting Thyroid Cancer Incidence & Image source: Thyroid ABC Health and Well Being Webinar Series 2 Anatomy
NAACCR Hospital Registry Webinar Series Shannon Vann, CTR Jim Hofferkamp, CTR Webinar Series 1 Abstracting Thyroid Cancer Incidence & Image source: Thyroid ABC Health and Well Being Webinar Series 2 Anatomy
LYMPHATIC DRAINAGE IN THE HEAD & NECK
 LYMPHATIC DRAINAGE IN THE HEAD & NECK Like other parts of the body, the head and neck contains lymph nodes (commonly called glands). Which form part of the overall Lymphatic Drainage system of the body.
LYMPHATIC DRAINAGE IN THE HEAD & NECK Like other parts of the body, the head and neck contains lymph nodes (commonly called glands). Which form part of the overall Lymphatic Drainage system of the body.
131-I Therapy Planning in Thyroid Cancer: The role of diagnostic radioiodine scans
 131-I Therapy Planning in Thyroid Cancer: The role of diagnostic radioiodine scans Anca M. Avram, M.D. Associate Professor of Radiology Department of Nuclear Medicine University of Michigan Ann Arbor,
131-I Therapy Planning in Thyroid Cancer: The role of diagnostic radioiodine scans Anca M. Avram, M.D. Associate Professor of Radiology Department of Nuclear Medicine University of Michigan Ann Arbor,
34 year-old Female with Thyroid Cancer
 34 year-old Female with Thyroid Cancer KATIE O SULLIVAN, MD FELLOW, ADULT/PEDIATRIC ENDOCRINOLOGY UNIVERSITY OF CHICAGO ENDORAMA THURSDAY, SEPTEMBER 15 TH, 2016 Disclosures: I do not have any relevant
34 year-old Female with Thyroid Cancer KATIE O SULLIVAN, MD FELLOW, ADULT/PEDIATRIC ENDOCRINOLOGY UNIVERSITY OF CHICAGO ENDORAMA THURSDAY, SEPTEMBER 15 TH, 2016 Disclosures: I do not have any relevant
10. HPV-Mediated (p16+) Oropharyngeal Cancer
 Oropharyngeal Cancer") 1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
Management of Neck Metastasis from Unknown Primary
 Management of Neck Metastasis from Unknown Primary.. Definition Histologic evidence of malignancy in the cervical lymph node (s) with no apparent primary site of original tumour Diagnosis after a thorough
Management of Neck Metastasis from Unknown Primary.. Definition Histologic evidence of malignancy in the cervical lymph node (s) with no apparent primary site of original tumour Diagnosis after a thorough
Papillary Thyroid Microcarcinoma Presenting as Horner s Syndrome: A Novel Clinical Presentation
 Case Report American Journal of Cancer Case Reports http://ivyunion.org/index.php/ajccr/ Page 1 of 6 Papillary Thyroid Microcarcinoma Presenting as Horner s Syndrome: A Novel Clinical Presentation Ammara
Case Report American Journal of Cancer Case Reports http://ivyunion.org/index.php/ajccr/ Page 1 of 6 Papillary Thyroid Microcarcinoma Presenting as Horner s Syndrome: A Novel Clinical Presentation Ammara
Cutaneous Melanoma: Epidemiology (USA) The Sentinel Node in Head and Neck Melanoma. Cutaneous Melanoma: Epidemiology (USA)
 The Sentinel Node in Head and Neck Melanoma. Cutaneous Melanoma: Epidemiology (USA)") The Sentinel Node in Head and Neck Melanoma Cutaneous Melanoma: Epidemiology (USA) 6 th leading cause of cancer among men and women 68,720 new cases of invasive melanoma in 2009 8,650 deaths from melanoma
The Sentinel Node in Head and Neck Melanoma Cutaneous Melanoma: Epidemiology (USA) 6 th leading cause of cancer among men and women 68,720 new cases of invasive melanoma in 2009 8,650 deaths from melanoma
Review Article Thyroidectomy and Lymph Node Dissection in Papillary Thyroid Carcinoma
 SAGE-Hindawi Access to Research Thyroid Research Volume 2011, Article ID 634170, 6 pages doi:10.4061/2011/634170 Review Article Thyroidectomy and Lymph Node Dissection in Papillary Thyroid Carcinoma Yasuhiro
SAGE-Hindawi Access to Research Thyroid Research Volume 2011, Article ID 634170, 6 pages doi:10.4061/2011/634170 Review Article Thyroidectomy and Lymph Node Dissection in Papillary Thyroid Carcinoma Yasuhiro
This form may provide more data elements than required for collection by standard setters such as NCI SEER, CDC NPCR, and CoC NCDB.
 1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
14. Mucosal Melanoma of the Head and Neck
 1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
I-131 ABLATION AND ADJUVANT THERAPY OF THYROID CANCER
 AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGISTS Advances in Medical and Surgical Management of Thyroid Cancer January 23-24, 2015 I-131 ABLATION AND ADJUVANT THERAPY OF THYROID CANCER 2015 Leonard Wartofsky,
AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGISTS Advances in Medical and Surgical Management of Thyroid Cancer January 23-24, 2015 I-131 ABLATION AND ADJUVANT THERAPY OF THYROID CANCER 2015 Leonard Wartofsky,
Thyroid nodules. Most thyroid nodules are benign
 Thyroid nodules Postgraduate Course in General Surgery Jessica E. Gosnell MD Assistant Professor March 22, 2011 Most thyroid nodules are benign thyroid nodules occur in 77% of the world s population palpable
Thyroid nodules Postgraduate Course in General Surgery Jessica E. Gosnell MD Assistant Professor March 22, 2011 Most thyroid nodules are benign thyroid nodules occur in 77% of the world s population palpable
Thyroid and Adrenal Gland
 Thyroid and Adrenal Gland NAACCR 2011 2012 Webinar Series 12/1/11 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
Thyroid and Adrenal Gland NAACCR 2011 2012 Webinar Series 12/1/11 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
Surgical Management of Differentiated Thyroid Cancer
 Vanderbilt University Surgical Grand Rounds May 7, 2010 Surgical Management of Differentiated Thyroid Cancer Carmen C Solórzano, MD, FACS Associate Professor Endocrine and Surgical Oncology Vanderbilt
Vanderbilt University Surgical Grand Rounds May 7, 2010 Surgical Management of Differentiated Thyroid Cancer Carmen C Solórzano, MD, FACS Associate Professor Endocrine and Surgical Oncology Vanderbilt
Accepted 12 August 2013 Published online 27 November 2013 in Wiley Online Library (wileyonlinelibrary.com). DOI /hed.23451
. DOI /hed.23451") ORIGINAL ARTICLE Risk factors and clinical indication of metastasis to lymph nodes posterior to right recurrent laryngeal nerve in papillary thyroid carcinoma: A single-center study in China Zhang Pinyi,
ORIGINAL ARTICLE Risk factors and clinical indication of metastasis to lymph nodes posterior to right recurrent laryngeal nerve in papillary thyroid carcinoma: A single-center study in China Zhang Pinyi,
The role of prophylactic central compartment lymph node dissection in differentiated thyroid carcinoma
 Original Research Article The role of prophylactic central compartment lymph node dissection in differentiated thyroid carcinoma Nived Rao 1, M. Muralidhar 2*, M. Srinivasulu 3 1Senior Resident in Surgical
Original Research Article The role of prophylactic central compartment lymph node dissection in differentiated thyroid carcinoma Nived Rao 1, M. Muralidhar 2*, M. Srinivasulu 3 1Senior Resident in Surgical
Central Lymph Node Dissection In Patients With Papillary Thyroid Cancer: A Population Level Analysis Of Cases
 Yale University EliScholar A Digital Platform for Scholarly Publishing at Yale Yale Medicine Thesis Digital Library School of Medicine January 2013 Central Lymph Node Dissection In Patients With Papillary
Yale University EliScholar A Digital Platform for Scholarly Publishing at Yale Yale Medicine Thesis Digital Library School of Medicine January 2013 Central Lymph Node Dissection In Patients With Papillary
42 yr old male with h/o Graves disease and prior I 131 treatment presents with hyperthyroidism and undetectable TSH. 2 hr uptake 20%, 24 hr uptake 50%
 Pinhole images of the neck are acquired in multiple projections, 24hrs after the oral administration of approximately 200 µci of I123. Usually, 24hr uptake value if also calculated (normal 24 hr uptake
Pinhole images of the neck are acquired in multiple projections, 24hrs after the oral administration of approximately 200 µci of I123. Usually, 24hr uptake value if also calculated (normal 24 hr uptake
3/23/2017. Disclosure of Relevant Financial Relationships. Pathologic Staging Updates in Breast Cancer. Pathologic Staging Updates Breast Cancer
 Pathologic Staging Updates in Breast Cancer Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content of CME
Pathologic Staging Updates in Breast Cancer Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content of CME
Thyroid nodules 3/22/2011. Most thyroid nodules are benign. Thyroid nodules: differential diagnosis
 Most thyroid nodules are benign Thyroid nodules Postgraduate Course in General Surgery thyroid nodules occur in 77% of the world s population palpable thyroid nodules occur in about 5% of women and 1%
Most thyroid nodules are benign Thyroid nodules Postgraduate Course in General Surgery thyroid nodules occur in 77% of the world s population palpable thyroid nodules occur in about 5% of women and 1%
Oncological outcomes for patients with well differentiated thyroid cancer Nixon, I.J.
 UvA-DARE (Digital Academic Repository) Oncological outcomes for patients with well differentiated thyroid cancer Nixon, I.J. Link to publication Citation for published version (APA): Nixon, I. J. (2013).
UvA-DARE (Digital Academic Repository) Oncological outcomes for patients with well differentiated thyroid cancer Nixon, I.J. Link to publication Citation for published version (APA): Nixon, I. J. (2013).
New technologies in Endocrine Surgery
 New technologies in Endocrine Surgery 1. Nerve monitoring 2. New technologies in Endocrine Surgery Jessica E. Gosnell MD Post graduate course in General Surgery March 28, 2012 1 2 Recurrent laryngeal nerve
New technologies in Endocrine Surgery 1. Nerve monitoring 2. New technologies in Endocrine Surgery Jessica E. Gosnell MD Post graduate course in General Surgery March 28, 2012 1 2 Recurrent laryngeal nerve
THYROID CANCER IN CHILDREN
 THYROID CANCER IN CHILDREN Isabel ROCA, Montserrat NEGRE Joan CASTELL HU VALL HEBRON BARCELONA EPIDEMIOLOGY ADULTS males 1,2-2,6 cases /100.000 females 2,0-3,8 cases /100.000 0,02-0,3 / 100.000 children
THYROID CANCER IN CHILDREN Isabel ROCA, Montserrat NEGRE Joan CASTELL HU VALL HEBRON BARCELONA EPIDEMIOLOGY ADULTS males 1,2-2,6 cases /100.000 females 2,0-3,8 cases /100.000 0,02-0,3 / 100.000 children
Thyroid Pathology: It starts and ends with the gross. Causes of Thyrophobia. Agenda. Diagnostic ambiguity. Treatment/prognosis disconnect
 Thyroid Pathology: It starts and ends with the gross Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for
Thyroid Pathology: It starts and ends with the gross Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for