131-I Therapy Planning in Thyroid Cancer: The role of diagnostic radioiodine scans
|
|
|
- Lee Thornton
- 6 years ago
- Views:
Transcription
1 131-I Therapy Planning in Thyroid Cancer: The role of diagnostic radioiodine scans Anca M. Avram, M.D. Associate Professor of Radiology Department of Nuclear Medicine University of Michigan Ann Arbor, USA
2 Disclosures Nothing to disclose
3 Objectives: define the role of pre-ablation scans with SPECT/CT for: 1. post-operative staging in thyroid cancer 2. post-operative risk stratification in thyroid cancer 3. post-operative management 4. Identification of regional and distant metastases I therapy planning: ablation, adjuvant treatment, targeted treatment for metastatic disease, dosimetry-guided 131-I therapy
4 Differentiated Thyroid Cancer (DTC) Most common forms of thyroid cancer are: Papillary carcinoma (~80% of cases) Follicular carcinoma (~10% of cases) In DTC, tumor cells retain the characteristics of normal differentiated thyroid cells. Preferential ability to take up and store iodine Secrete thyroglobulin (Tg)


5 2.6 x increased incidence of Thy CA Context This trend continues for the past 30 years 87% of new cases are T1 tumors ( 2 cm)
6 Differentiated Thyroid Cancer Generally a slow-growing tumor 98% 5-year survival rate with less advanced stages ~50% 5-year survival in advanced cases (distant mets) Risk of recurrence, despite improvements in disease management Life-long monitoring used to detect persistent and recurrent disease at the earliest possible stage
7 DTC: At A Glance DTC is The 8 th in the top 10 common cancers: (AFTER: 1. Breast 2: Lung; 3. Prostate; 4. Colon; 5. Melanoma; 6. Bladder; 7. NHL; 9. Kidney; 10. Endometrial ) Estimated New Cases in 2015: 62,450 Estimated Deaths in 2015: 1,950 (3%) Large population of DTC survivors that need surveillance
8 2015 ATA Guidelines published in Jan, 2016 issue of THYROID monumental effort (16 authors; exhaustive literature review) Eval. of quality of evidence (good, moderate, weak) ACP grading system of Rec. (strong, weak, no rec) 133 pages 1078 references 101 recommendations
9
10 2015 ATA Guidelines There is a broad range of new or modified recommendations in 2015 as compared to 2009 ATA Guidelines: - 8 New Clinical Questions - 21 New Recommendations - 21 significantly changed Recommendations
11 The Result: a seismic shift in thyroid cancer management Initial treatment: dramatic pendulum swing away from prior standard of care for thyroid cancer treatment (i.e. total thyroidectomy, central neck dissection, post-op RAI Rx) to: Less than total thyroidectomy for PTC < 4 cm Not using RAI in the majority of patients (~ 85%) of thyroid cancer pts. Surveillance strategy: shift away from Dx and/or PostRx Scans to US surveillance and serial Tg testing
12 Initial Treatment Strategy is predicated on Risk Stratification (which is based on an estimation of the risk for recurrence) The Risk of Recurrence Estimation is based on retrospective studies from 3 continents which have reported on the proportion of pts. with NO Evidence of Disease in each 2009 ATA category AFTER total thyroidectomy + RAI Remnant Ablation NED is defined as: stim. Tg < 1 ng/ml + - no clinical or radiological evidence of ds. (the length of follow-up is critical usually 2 years)
13 NED after Total Thyroidectomy + RAI Rx: ATA Low Risk: 78 91% NED 9 22% ATA Intermediate Risk: Persistent Ds NED 36 48% ATA High Risk: 30 32% NED 68 70%
14 Post-operative management Total thyroidectomy neck dissection Risk stratification (Histopathology) Management without Ablation (Low-risk) Hypothyroid/rh-TSH stimulated Fixed Dose 131-I Ablation (Intermediate and High-Risk) mci 131-I for ablation >100 mci 131-I for therapy Post therapy 131-I scan at 5 7 days ATA Guidelines for Thyroid Cancer
; E: Recommends against (fair evidence); F: Strongly recommends against (good evidence); I: Recommends neither for nor")
15 ATA: A: Strongly recommends (good evidence); B: Recommends (fair evidence); C: Recommends (expert opinion); D: Recommends against (expert opinion); E: Recommends against (fair evidence); F: Strongly recommends against (good evidence); I: Recommends neither for nor against
16 What Dose of 131-I therapy? Versus What Target for 131-I therapy? Individualized 131-I therapy What is the contribution of diagnostic Radio-iodine scans to management?
17 Accurate Staging is Important knowing the extent of disease makes a difference Staging predicts survival Staging determines the strategy for initial treatment and for long-term surveillance AJCC TNM 7 th Ed. was used for staging patients after total thyroidectomy
18 Patients with stage I-II disease have favorable prognosis (mortality < 1% at 20 years) (low risk group) Prognosis Mortality increases to 25-40% among patients at stages III and IV (high risk group) Jonklaas J et. al. Thyroid (12):
19 DTC Staging AJCC 7 th Ed Age < 45 Age 45 Stage I any T, any N, M0 T1, N0, M0 Stage II any T, any N, M1 T2, N0, M0 Stage III n/a T3, N0, M0 T1-T2-T3, N1a, M0 Stage IVA n/a T4a, N0-N1a, M0 T1-T4a, N1b, M0 Stage IVB n/a T4b, any N, M0 Stage IVC n/a any T, any N, M1
20 2009 ATA Risk Stratification ATA Low Risk: no regional or distant metastases complete tumor resection, no evidence of invasion non-aggressive histology ATA Intermediate Risk: microscopic invasion in peri-thyroidal tissues cervical nodal metastases (or 131-I uptake outside of thyroid bed on PostRx Scan) aggressive histology or vascular invasion ATA High Risk: macroscopic invasion, incomplete resection distant metastases Tg. out of proportion of PostRx. findings
21 2015 ATA Pediatric Risk Stratification Low-risk patients: Disease grossly confined to the thyroid N0 or Nx or Incidental N1a (microscopic metastasis to a small number of central neck nodes) Intermediate-risk patients: microscopic invasion in peri-thyroidal tissues cervical nodal metastases: Extensive N1a, or minimal N1b aggressive histology or vascular invasion High-risk patients: macroscopic invasion, incomplete resection; extensive N1b distant metastases 2015 ATA Pediatric Thyroid Cancer Guidelines

22 2015 ATA RECURRENCE RISK
23 ATA Guidelines: Selective use of 131-I therapy Low risk, and selected medium-risk patients are no longer recommended ablation after total thyroidectomy. Management decisions are predicated by histopathologybased risk stratification. A post-therapy scan may not exist in all patients. Without a diagnostic scan to complete staging after total thyroidectomy, regional or distant metastases may not be recognized and addressed at an early stage.
24 Individualized 131-I Treatment Patient-specific 131-I therapy prescription: - Clinical data (patient s age and clinical presentation: with/without palpable lymphadenopathy) - Surgical pathology report: defining T and N depending on the extent of surgical dissection - Post-operative Tg levels (suppressed/stimulated; Thyrogen vs. hypothyroid stimulation) - Diagnostic imaging findings: neck US and DxWBS (123-I vs. 131-I scans, planar SPECT/CT imaging)
25 Progress: Hybrid SPECT/CT camera Co-registration of functional and anatomic data Superior image quality: Improved spatial resolution Improved contrast resolution Application of scatter rejection algorithms Iterative Reconstruction SPECT CT-based Attenuation Correction High quality images can be achieved with tracer doses of 131-I.
26 SPECT/CT Improved I-131 SPECT imaging Facilitates activity localization, attenuation & partial volume correction High energy collimator Sensitivity higher for ME, but desired geometric events higher for HE Thicker NaI crystal Efficiency for 364 kev photons 2 times higher for 15.9 mm vs. 9.5 mm Dead time correction for post-therapy imaging Count-rates should be < 50 kcps. Earliest imaging at 1 4 days Scatter correction Triple Energy Window correction. Iterative reconstruction with accurate system model Commercial software only models geometric component of CDR Dewaraja et al. MIRD 24. JNM 2013
27 Concordance: Diagnostic vs. Post-therapy scans McDougall IR et al. Nucl Med Comm, 1997: (2 mci) 131-I pre-ablation and post-rx (8d) planar scans were concordant in 274 of 280 patients (98%); in 2% pts. a relative decreased uptake in the previously detected foci was seen on the post-rx. Avram AM et al. JCEM, 2013: (1 mci) 131-I pre-ablation and post-rx (2d) planar scans were concordant in 280 of 303 patients (92%): - in only 4 of 303 pts. (1.3%) a relative decreased uptake in the previously detected foci was seen on the post-rx. - in 6% pts. additional foci were detected on post-rx scan (in only 1.4% pts. the findings upstaged the patient)
28 UM Experience: individualized 131-I therapy Focus: To assess the contribution of diagnostic 131 I scans with SPECT-CT for: Differentiated Thyroid Cancer (DTC) 1. Staging 2. Risk Stratification 3. Management
29 Why is this important? Define instances where initial staging based on clinical & surgical pathology (ptnm) changes after diagnostic 131 I imaging - Complete patients risk-stratification - Define if the patient will / (will not) benefit from therapeutic 131 I administration - Define the target of 131 I therapy
30 Study Design All patients were initially staged and risk stratified by Endocrinologist based on clinical and surgical pathology (ptnm) All 131 I scans were interpreted to assess for thyroid remnant, nodal or distant metastases (2 independent readers) All patients were re-staged and re-stratified after incorporating the information from diagnostic 131 I SPECT-CT to arrive at final TNM and final Risk Stratification
31 Study Design The impact of findings on DxWBS + SPECT/CT were assess regarding changes in management: the decision of treat or withhold 131-I therapy based on risk stratification the decision to refer to surgery for resection of bulky residual metastatic disease the prescribed 131-I activity defined as: Low-activity (30-50 mci) Medium activity ( mci) High activity ( 200 mci)
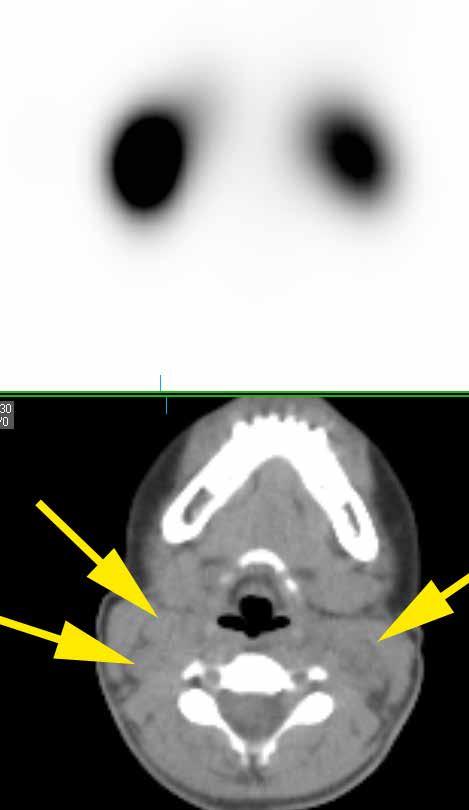
32 University of Michigan Protocol Diagnostic 131 I scans (37 MBq, 1 mci) are performed in all pts. at 4 weeks after total thyroidectomy 24 h whole body (WB) and static planar images of the neck and chest 24 h SPECT-CT imaging for: characterization of central neck activity: thyroid remnant vs. nodal metastasis anatomic localization of distant disease evaluation of suspected physiologic mimics
33 Methods 320 consecutive pts. (47 ± 16 yrs, range 10 90) Female 68%; Male 32% Avram AM et al. J Clin Endocrinol Metab 2013; 98(3):
34 Methods: Tumor Characteristics Size: cm; range: cm Multifocality: 144 (45%) Vascular invasion, present: 96 (30%) Capsular invasion, present: 202 (63%) Extrathyroidal extension, yes: 116 (36%) Surgical margins: Positive 26%; Negative 72%; Unknown 2% Neck nodal metastases, pn1*** 149 (47%) *** before diagnostic imaging
35 Methods: Laboratory results TSH <30 miu/l 15 (5%) 30 miu/l 305 (95%) Thyroglobulin <0.5 ng/ml 74 (23%) 0.5 ng/ml to <10 ng/ml 149 (47%) 10 ng/ml to <100 ng/ml 66 (21%) 100 ng/ml to <1,000 ng/ml 22 (7%) 1,000 ng/ml 9 (3%) Anti-Tg. Ab., present 50 (16%)
36 Results in Younger patients (n= 138) 131 I Fused Imaging revealed: Nodal Mets. in 61 (44%) Young pts. Unsuspected Nodal Mets in 24 of 63 (38%) initially assigned pn0 or pnx N1 Residual post-surgery Nodal Mets in 37 of 75 (49%) pn1pts. Distant Mets. in 5 (4%) Young pts. (upstaged to Stage II disease)
37 Avram AM et al. J Clin Endocrinol Metab 2013; 98(3):

38 14 year old girl with bulky cervical nodal mets. T3, N1b, M0; Stage I
39

40 planar anterior image planar posterior image 23 year old woman with mptc 3.5 cm tumor with +ETE; 23+/30 bilateral neck pt4a, N1b, M0; stage I

41 Restaging: T4a, N1b, M1; Stage II
42 Results in Older patients (n=182) 131 I Fused Imaging Upstaged 46 (25%) pts. Nodal Mets. in 46 (25%) Older pts. Unsuspected Nodal Mets in 26 of 108 (24%) initially assigned pn0 or pnx N1 Residual post-surgery Nodal Mets in 25 of 74 (34%) pn1pts. Distant Mets. in 18 (10%) Older pts.
43 Avram AM et al. J Clin Endocrinol Metab 2013; 98(3):


44 65 yo woman, mptc 1.2 cm and 0.5 cm tumors 0/3 nodes central neck pt1b, N0, M0; Stage I

45 Restaging T1b, N1b, M0; Stage IV A
46 56 year old woman 1.2 cm PTC, no ETE 0/3 central nodes pt1b, N0, M0; Stage I



47 Restaging T1b, N0, M1; Stage IV C SPECT/CT: right thyroid remnant; liver metastasis


48 Diagnostic (1 mci) 131-I scan at 6 Mos. after 200 mci RAI Rx: interval resolution of liver metastasis and of thyroid remnant tissue
49 Sub-analysis of T1 Tumors n =116 (36%) T1 a ( 1.0 cm) n=49 (15%) T1b ( 2.0 cm) n=67 (21%) Dx. Scans detected: - Nodal Mets in 22% - Distant Mets in 4% Dx. Scans detected: - Nodal Mets in 52% - Distant Mets in 4.5% Risk for distant metastases increased in Multifocal tumors Avram AM et al. J Clin Endocrinol Metab 2013; 98(3):
50 Pre-ablation Scans Complete Staging Characterization of N status and M status detected regional mets. in 35% pts. detected distant mets. in 8% pts. Changes TNM staging: 4% of young pts. 25% of older pts. Avram AM et al. J Clin Endocrinol Metab 2013; 98(3):
51 Pre-ablation Scans Complete Risk Stratification Univ. of Michigan experience in 320 patients Risk Stratification performed by Endocrinologist before and after information from pre-ablation scans was made available: 15% pts. (48/320) changed risk stratification after imaging information on nodal and distant metastatic status - 28 pts. were changed to Intermediate Risk from Low Risk - 20 pts. were changed to High Risk (3 from LR and 17 IR) Avram AM et al. J Clin Endocrinol Metab 2015 May;100(5):
52 Pre-ablation Scans Complete Risk Stratification Postoperative Patients ( n=320) Cervical Nodal Metastases No Nodes on SPECT/CT Nodes on SPECT/CT Total (%) pn (20) pn1a (27) pn1b (20) pnx (33) Total Distant Metastases M0 M1 Total cm cm Total ATA Risk Stratification Initial (ptn) Final (after imaging) Low Risk 97 (30%) 66 (20%) Med. Risk 190 (60%) 201 (63%) High Risk 33 (10%) 53 (17%) Avram AM et al. J Clin Endocrinol Metab 2015 May;100(5):
53 Pre-ablation Scans contribute to Management Univ. of Michigan experience in 320 patients Management changed in 31% pts. (99/320) due to: Both Imaging and Tg information (n = 87) Imaging information (n = 7) Tg. level, being out of proportion to DxWBS findings (n = 5) Avram AM et al. J Clin Endocrinol Metab 2015 May;100(5):
54 Decisions to treat or withhold RAI based on Risk Stratification Avram AM et al. J Clin Endocrinol Metab 2015 May;100(5):
55 Impact of initial and final Risk Stratification on 131-I Therapy Avram AM et al. J Clin Endocrinol Metab 2015 May;100(5):

56 Identification of Distant Metastases led to dosimetrically guided RAI Rx. 32 year old woman 1.8 cm follicular-variant PTC left lobe; + margins - 15+/27 nodes central neck - 6+/46 nodes left neck - TSH 118 mu/l - Tg 862 ng/ml

57

58 Dosimetry Calculations - Whole Body Dosimetry: 0.56 cgy/mci adm. activity - Blood Dosimetry: 0.62 cgy/mci adm. activity RAI Rx. 320 mci 131-I therapy
59 131 I Blood Dosimetry Original method Leeper. Endocrinol Metab Clin N Am 1980;9:383 Blood (as surrogate for bone marrow). Samples at 6, 24, 48, 72, 96 h, Calculate radiation dose absorbed to blood Goal: <200 cgy (rads) Circulating T4 increases absorbed dose in bone marrow over that in body.
60 131 I Whole Body Dosimetry Method using uptake probe or camera: count 2 h after oral dose 131 I = 100%; count 2 days = % or residual fraction. Calculation of administered dose, goal at 2 days <80 mci; calculate 80 mci/residual fraction = upper limit.
61 Well-differentiated Thyroid Carcinoma Guidelines Prevent Toxicity* from 131 -I 1. Body retention of 131-I at 48 h**: 120 mci, but 80 mci if diffuse lung metastases 2. Absorbed radiation to blood: 200 cgy *prevent marrow depress & pneumonitis. **dominates unless tumor makes T4. Benua et al. AJR 1962;87:171.

 right neck (9+/26) left")
62 Identification of large residual metastases led to surgical referral 45 year old man with 3.5 cm PTC 30+/58 bilateral metastatic lymph nodes: central neck (17+/17) right neck (9+/26) left neck (4+/15)
 at the sternal notch and in the left")
63 3 large residual metastatic lymph nodes (~ 1 x 1.2 cm) at the sternal notch and in the left supraclavicular area.

64 Surgical referral prior to 131-I therapy
65 Diagnostic radioiodine scans provide information which can alter clinical strategy Proposed changes in management based on information provided by radioiodine scans include: deciding whether to give or withhold 131-I treatment, indicating and guiding the extent of surgery when large metastatic deposits are present adjusting the prescribed 131-I activity for remnant ablation, adjuvant therapy or targeted treatment Indicating the need for alternative imaging strategies such as 18F-FDG PET when negative 131-I scans and elevated THYG levels Individualized approach in patient management
66 Question 1 What is the MOST common type of thyroid cancer?
67 Q1: Most common thyroid cancer type is: a) Follicular Thyroid Cancer b) Hurthle Cell Thyroid Cancer c) Medullary Thyroid Cancer d) Papillary Thyroid Cancer
68 Q1: Most common thyroid cancer type is: a) Follicular Thyroid Cancer b) Hurthle Cell Thyroid Cancer c) Medullary Thyroid Cancer d) Papillary Thyroid Cancer
69 Q1: Answers D is the correct answer: Papillary Thyroid Cancer (PTC) represents 80% of all cases of DTC
70 Question 2 Regarding therapeutic approach, what is the most important feature of DTC?
71 Q2: Regarding therapy approach, the most important feature of DTC is: a) The histologic subtype b) Surgical resection margins c) Ability to concentrate iodine (NIS expression and function) d) The extent of local-regional spread
72 Q2: Regarding therapy approach, the most important feature of DTC is: a) The histologic subtype b) Surgical resection margins c) Ability to concentrate iodine (NIS expression and function) d) The extent of local-regional spread
73 Q2 Answers C is the correct answer Well Differentiated thyroid cancer cells maintain the ability to uptake and concentrate 131-I due to constitutive NIS expression. TSH stimulation increases the expression and function of NIS in thyroid cancer cell, resulting in increased 131-I uptake and retention within the tumor cell (i.e. radiation absorbed dose to tumor) Adequate patient preparation (low-iodine diet, TSH stimulation) is important for optimizing 131-I therapy
74 Question 3 Pre-ablation radioiodine scans with SPECT/CT are MOST useful for which of the following?
75 Q3: Pre-ablation Scan is MOST useful for: a) To complete post-operative thyroid cancer staging prior to 131-I therapy b) To determine the dose of 131-I therapy c) To alter the pre-operative management d) To perform whole body dosimetry calculations
76 Q3: Pre-ablation Scan is MOST useful for: a) To complete post-operative thyroid cancer staging prior to 131-I therapy b) To determine the dose of 131-I therapy c) To alter the pre-operative management d) To perform whole body dosimetry calculations
77 Q3: Answers A is the correct answer: Preablation radio-iodine scans with SPECT/CT complete initial staging before management decisions regarding 131-I therapy are made. detected regional metastases in 35% patients and distant metastases in 8% patients change in staging in 4% of younger patients (age < 45 years) and 25% of older patients (age 45 years) Avram AM et al. J Clin Endocrinol Metab 2013; 98(3):

78 Question 4 Which one of the following is the MOST important advantage of SPECT/CT when applied to radioiodine scintigraphy?
79 Q4: SPECT/CT is MOST useful for: a) Improved characterization of primary tumor (T) status b) Detection of regional metastases by improved characterization of nodal metastasis versus thyroid remnant c) Detection of distant metastasis (M) d) Improved characterization of oral radioiodine uptake as salivary secretions versus metastatic lesions
80 Q4: SPECT/CT is MOST useful for: a) Improved characterization of primary tumor (T) status b) Detection of regional metastases by improved characterization of nodal metastasis versus thyroid remnant c) Detection of distant metastasis (M) d) Improved characterization of oral radioiodine uptake as salivary secretions versus metastatic lesions
81 Q4: Answers B is the correct answer: SPECT/CT localizes focal activity to cervical lymph nodes and/or paratracheal activity in the surgical bed Review the surgical pathology report for tumor invasiveness into local structures and completion of surgical resection; these elements are of critical importance when interpreting the significance of paratracheal central neck activity as benign thyroid remnant versus residual disease. Avram AM. J Nucl Med. 2012;53(5):
82 Question 5 Incorporating SPECT/CT into the protocol of pre-ablation radio-iodine scans is MOST useful for which of the following?
83 Q5: SPECT/CT is MOST useful for: a) Reduces equivocal interpretations on planar radioiodine scintigraphy b) Identifies physiologic radioiodine biodistribution patterns c) Increases the specificity for disease detection as compared to planar radioiodine imaging d) Improves the outcome of 131-I therapy
84 Q5: SPECT/CT is MOST useful for: a) Reduces equivocal interpretations on planar radioiodine scintigraphy b) Identifies physiologic radioiodine biodistribution patterns c) increases the specificity for disease detection as compared to planar radioiodine imaging d) Improves the outcome of 131-I therapy
85 Q5: Answers C is the correct answer: SPECT/CT increase diagnostic test performance mainly by an increase in Specificity: planar studies demonstrated a sensitivity of 41%, specificity of 68% SPECT-CT demonstrated a sensitivity of 50%, specificity of 100% Barwick T et al. Eur J Endocrinol 2010;162(6):1131-9
Anca M. Avram, M.D. Professor of Radiology
 Thyroid Cancer Theranostics: the case for pre-treatment diagnostic staging 131-I scans for 131-I therapy planning Anca M. Avram, M.D. Professor of Radiology Department of Nuclear Medicine University of
Thyroid Cancer Theranostics: the case for pre-treatment diagnostic staging 131-I scans for 131-I therapy planning Anca M. Avram, M.D. Professor of Radiology Department of Nuclear Medicine University of
Nuclear Medicine in Thyroid Cancer. Phillip J. Koo, MD Division Chief of Diagnostic Imaging
 Nuclear Medicine in Thyroid Cancer Phillip J. Koo, MD Division Chief of Diagnostic Imaging Financial Disclosures Bayer Janssen Learning Objectives To learn the advantages and disadvantages of SPECT/CT
Nuclear Medicine in Thyroid Cancer Phillip J. Koo, MD Division Chief of Diagnostic Imaging Financial Disclosures Bayer Janssen Learning Objectives To learn the advantages and disadvantages of SPECT/CT
Gerard M. Doherty, MD
 Surgical Management of Differentiated Thyroid Cancer: Update on 2015 ATA Guidelines Gerard M. Doherty, MD Chair of Surgery Utley Professor of Surgery and Medicine Boston University Surgeon-in-Chief Boston
Surgical Management of Differentiated Thyroid Cancer: Update on 2015 ATA Guidelines Gerard M. Doherty, MD Chair of Surgery Utley Professor of Surgery and Medicine Boston University Surgeon-in-Chief Boston
Dynamic Risk Stratification:
 Dynamic Risk Stratification: Using Risk Estimates to Guide Initial Management R Michael Tuttle, MD Clinical Director, Endocrinology Service Memorial Sloan Kettering Cancer Center Professor of Medicine
Dynamic Risk Stratification: Using Risk Estimates to Guide Initial Management R Michael Tuttle, MD Clinical Director, Endocrinology Service Memorial Sloan Kettering Cancer Center Professor of Medicine
I-131 ABLATION AND ADJUVANT THERAPY OF THYROID CANCER
 AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGISTS Advances in Medical and Surgical Management of Thyroid Cancer January 23-24, 2015 I-131 ABLATION AND ADJUVANT THERAPY OF THYROID CANCER 2015 Leonard Wartofsky,
AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGISTS Advances in Medical and Surgical Management of Thyroid Cancer January 23-24, 2015 I-131 ABLATION AND ADJUVANT THERAPY OF THYROID CANCER 2015 Leonard Wartofsky,
Strategies for detection of recurrent disease in longterm follow-up of differentiated thyroid cancer
 Strategies for detection of recurrent disease in longterm follow-up of differentiated thyroid cancer A rational approach to longterm follow-up based on dynamic risk assessment. World Congress on Thyroid
Strategies for detection of recurrent disease in longterm follow-up of differentiated thyroid cancer A rational approach to longterm follow-up based on dynamic risk assessment. World Congress on Thyroid
Risk Adapted Follow-Up
 Risk Adapted Follow-Up Individualizing Follow- Up Strategies R Michael Tuttle, MD Clinical Director, Endocrinology Service Memorial Sloan Kettering Cancer Center Professor of Medicine Weill Medical College
Risk Adapted Follow-Up Individualizing Follow- Up Strategies R Michael Tuttle, MD Clinical Director, Endocrinology Service Memorial Sloan Kettering Cancer Center Professor of Medicine Weill Medical College
SPECT/CT in Endocrine Diseases and Dosimetry
 SPECT/CT in Endocrine Diseases and Dosimetry Heather A. Jacene, MD Division of Nuclear Medicine Russell H. Morgan Dept. of Radiology and Radiological Science Johns Hopkins University Baltimore, MD Disclosures
SPECT/CT in Endocrine Diseases and Dosimetry Heather A. Jacene, MD Division of Nuclear Medicine Russell H. Morgan Dept. of Radiology and Radiological Science Johns Hopkins University Baltimore, MD Disclosures
2015 American Thyroid Association Thyroid Nodule and Cancer Guidelines
 2015 American Thyroid Association Thyroid Nodule and Cancer Guidelines Angela M. Leung, MD, MSc, ECNU November 5, 2016 Outline Workup of nontoxic thyroid nodule(s) Ultrasound FNAB Management of FNAB results
2015 American Thyroid Association Thyroid Nodule and Cancer Guidelines Angela M. Leung, MD, MSc, ECNU November 5, 2016 Outline Workup of nontoxic thyroid nodule(s) Ultrasound FNAB Management of FNAB results
4/22/2010. Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey.
 Management of Differentiated Thyroid Cancer: Head Neck Surgeon Perspective Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey Thyroid gland Small endocrine gland:
Management of Differentiated Thyroid Cancer: Head Neck Surgeon Perspective Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey Thyroid gland Small endocrine gland:
- RET/PTC rearrangement: 20% papillary thyroid cancer - RET: medullary thyroid cancer
 Thyroid Cancer UpToDate: Introduction: Risk Factors: Biology: Symptoms: Diagnosis: 1. Lenvina is the first line therapy with powerful durable response and superior PFS in pts with RAI-refractory disease.
Thyroid Cancer UpToDate: Introduction: Risk Factors: Biology: Symptoms: Diagnosis: 1. Lenvina is the first line therapy with powerful durable response and superior PFS in pts with RAI-refractory disease.
PEDIATRIC Ariel Katz MD
 PEDIATRIC Ariel Katz MD Dept. Otolaryngology Head &Neck Surgery Wolfson Medical Center Holon, Israel OBJECTIVES Overview/Background Epidemiology/Etiology Intro to Guidelines Workup Treatment Follow-Up
PEDIATRIC Ariel Katz MD Dept. Otolaryngology Head &Neck Surgery Wolfson Medical Center Holon, Israel OBJECTIVES Overview/Background Epidemiology/Etiology Intro to Guidelines Workup Treatment Follow-Up
Thyroid remnant volume and Radioiodine ablation in Differentiated thyroid carcinoma.
 ORIGINAL ARTICLE Thyroid remnant volume and Radioiodine ablation in Differentiated thyroid carcinoma. Md. Sayedur Rahman Miah, Md. Reajul Islam, Tanjim Siddika Institute of Nuclear Medicine & Allied Sciences,
ORIGINAL ARTICLE Thyroid remnant volume and Radioiodine ablation in Differentiated thyroid carcinoma. Md. Sayedur Rahman Miah, Md. Reajul Islam, Tanjim Siddika Institute of Nuclear Medicine & Allied Sciences,
1. Protocol Summary Summary of Trial Design. IoN
 1. Protocol Summary 1.1. Summary of Trial Design Title: Short Title/acronym: IoN Is ablative radioiodine Necessary for low risk differentiated thyroid cancer patients IoN EUDRACT no: 2011-000144-21 Sponsor
1. Protocol Summary 1.1. Summary of Trial Design Title: Short Title/acronym: IoN Is ablative radioiodine Necessary for low risk differentiated thyroid cancer patients IoN EUDRACT no: 2011-000144-21 Sponsor
WTC 2013 Panel Discussion: Minimal disease
 WTC 2013 Panel Discussion: Minimal disease Susan J. Mandel MD MPH Panelists Ken Ain Yasuhiro Ito Stephanie Lee Erich Sturgis Mark Urken Faculty/Presenter Disclosure Relationships with commercial interests
WTC 2013 Panel Discussion: Minimal disease Susan J. Mandel MD MPH Panelists Ken Ain Yasuhiro Ito Stephanie Lee Erich Sturgis Mark Urken Faculty/Presenter Disclosure Relationships with commercial interests
THE JOURNAL OF NUCLEAR MEDICINE Vol. 53 No. 5 May 2012 Avram
 Supplemental Table 1: Studies reporting utility of Post-Rx. 131-I SPECT-CT for evaluation of differentiated thyroid cancer Author No. Pts/Scans Setting Scan type Camera Site of Radioactivity Foci Journal
Supplemental Table 1: Studies reporting utility of Post-Rx. 131-I SPECT-CT for evaluation of differentiated thyroid cancer Author No. Pts/Scans Setting Scan type Camera Site of Radioactivity Foci Journal
The use of Radioactive Iodine (RAI) for Differentiated Thyroid Cancer
 for Differentiated Thyroid Cancer") The use of Radioactive Iodine (RAI) for Differentiated Thyroid Cancer Wendy Sacks, M.D. Cedars Sinai Medical Center California Chapter Annual Meeting, AACE Nov 5, 2016 Increasing Incidence of Thyroid Cancer
The use of Radioactive Iodine (RAI) for Differentiated Thyroid Cancer Wendy Sacks, M.D. Cedars Sinai Medical Center California Chapter Annual Meeting, AACE Nov 5, 2016 Increasing Incidence of Thyroid Cancer
Imaging in Thyroid Cancer
 Imaging in Thyroid Cancer Susan J. Mandel MD MPH University of Pennsylvania School of Medicine Philadelphia, PA I-123 Ultrasound Background Radioiodine ablation of thyroid remnants after surgery is a generally
Imaging in Thyroid Cancer Susan J. Mandel MD MPH University of Pennsylvania School of Medicine Philadelphia, PA I-123 Ultrasound Background Radioiodine ablation of thyroid remnants after surgery is a generally
Thyroid Cancer: Imaging Techniques (Nuclear Medicine)
") Thyroid Cancer: Imaging Techniques (Nuclear Medicine) Andrei Iagaru, MD MIPS Molecular Imaging Program at Stanford Stanford University School of Medicine Department of Radiology Introduction Ø There are
Thyroid Cancer: Imaging Techniques (Nuclear Medicine) Andrei Iagaru, MD MIPS Molecular Imaging Program at Stanford Stanford University School of Medicine Department of Radiology Introduction Ø There are
Pediatric Thyroid Cancer Lung Metastases. Liora Lazar MD
 Pediatric Thyroid Cancer Lung Metastases Liora Lazar MD Differentiated thyroid cancer (DTC) The 3rd most common solid tumor in childhood and adolescence Accounting for 1.5%-3% of all childhood cancers
Pediatric Thyroid Cancer Lung Metastases Liora Lazar MD Differentiated thyroid cancer (DTC) The 3rd most common solid tumor in childhood and adolescence Accounting for 1.5%-3% of all childhood cancers
42 yr old male with h/o Graves disease and prior I 131 treatment presents with hyperthyroidism and undetectable TSH. 2 hr uptake 20%, 24 hr uptake 50%
 Pinhole images of the neck are acquired in multiple projections, 24hrs after the oral administration of approximately 200 µci of I123. Usually, 24hr uptake value if also calculated (normal 24 hr uptake
Pinhole images of the neck are acquired in multiple projections, 24hrs after the oral administration of approximately 200 µci of I123. Usually, 24hr uptake value if also calculated (normal 24 hr uptake
Differentiated Thyroid Cancer: Initial Management
 Page 1 ATA HOME GIVE ONLINE ABOUT THE ATA JOIN THE ATA MEMBER SIGN-IN INFORMATION FOR PATIENTS FIND A THYROID SPECIALIST Home Management Guidelines for Patients with Thyroid Nodules and Differentiated
Page 1 ATA HOME GIVE ONLINE ABOUT THE ATA JOIN THE ATA MEMBER SIGN-IN INFORMATION FOR PATIENTS FIND A THYROID SPECIALIST Home Management Guidelines for Patients with Thyroid Nodules and Differentiated
Case 4: Disseminated bone metastases from differentiated follicular thyroid cancer
 Case 4: Disseminated bone metastases from differentiated follicular thyroid cancer Giuliano Mariani Regional Center of Nuclear Medicine, University of Pisa Medical School, Pisa (Italy) Disseminated bone
Case 4: Disseminated bone metastases from differentiated follicular thyroid cancer Giuliano Mariani Regional Center of Nuclear Medicine, University of Pisa Medical School, Pisa (Italy) Disseminated bone
Adjuvant therapy for thyroid cancer
 Carcinoma of the thyroid Adjuvant therapy for thyroid cancer John Hay Department of Radiation Oncology Vancouver Cancer Centre Department of Surgery UBC 1% of all new malignancies 0.5% in men 1.5% in women
Carcinoma of the thyroid Adjuvant therapy for thyroid cancer John Hay Department of Radiation Oncology Vancouver Cancer Centre Department of Surgery UBC 1% of all new malignancies 0.5% in men 1.5% in women
RESEARCH ARTICLE. Importance of Postoperative Stimulated Thyroglobulin Level at the Time of 131 I Ablation Therapy for Differentiated Thyroid Cancer
 RESEARCH ARTICLE Importance of Postoperative Stimulated Thyroglobulin Level at the Time of 131 I Ablation Therapy for Differentiated Thyroid Cancer Zekiye Hasbek 1 *, Bulent Turgut 1, Fatih Kilicli 2,
RESEARCH ARTICLE Importance of Postoperative Stimulated Thyroglobulin Level at the Time of 131 I Ablation Therapy for Differentiated Thyroid Cancer Zekiye Hasbek 1 *, Bulent Turgut 1, Fatih Kilicli 2,
Differentiated Thyroid Cancer: Reclassification of the Risk of Recurrence Based on the Response to Initial Treatment
 ORIGINAL ARTICLE Differentiated Thyroid Cancer: Reclassification of the Risk of Recurrence Based on the Response to Initial Treatment Martínez MP, Lozano Bullrich MP, Rey M, Ridruejo MC, Bomarito MJ, Claus
ORIGINAL ARTICLE Differentiated Thyroid Cancer: Reclassification of the Risk of Recurrence Based on the Response to Initial Treatment Martínez MP, Lozano Bullrich MP, Rey M, Ridruejo MC, Bomarito MJ, Claus
THYROID CANCER IN CHILDREN. Humberto Lugo-Vicente MD FACS FAAP Professor Pediatric Surgery UPR School of Medicine
 THYROID CANCER IN CHILDREN Humberto Lugo-Vicente MD FACS FAAP Professor Pediatric Surgery UPR School of Medicine Thyroid nodules Rare Female predominance 4-fold as likely to be malignant Hx Radiation exposure?
THYROID CANCER IN CHILDREN Humberto Lugo-Vicente MD FACS FAAP Professor Pediatric Surgery UPR School of Medicine Thyroid nodules Rare Female predominance 4-fold as likely to be malignant Hx Radiation exposure?
A Review of Differentiated Thyroid Cancer
 A Review of Differentiated Thyroid Cancer April 21 st, 2016 FPON Webcast Jonn Wu BMSc MD FRCPC Radiation Oncologist, Vancouver Centre Chair, Provincial H&N Tumour Group, BCCA Clinical Associate Professor,
A Review of Differentiated Thyroid Cancer April 21 st, 2016 FPON Webcast Jonn Wu BMSc MD FRCPC Radiation Oncologist, Vancouver Centre Chair, Provincial H&N Tumour Group, BCCA Clinical Associate Professor,
How good are we at finding nodules? Thyroid Nodules Thyroid Cancer Epidemiology Initial management Long-term follow up Disease-free status
 New Perspectives in Thyroid Cancer Jennifer Sipos, MD Assistant Professor of Medicine Division of Endocrinology The Ohio State University Outline Thyroid Nodules Thyroid Cancer Epidemiology Initial management
New Perspectives in Thyroid Cancer Jennifer Sipos, MD Assistant Professor of Medicine Division of Endocrinology The Ohio State University Outline Thyroid Nodules Thyroid Cancer Epidemiology Initial management
Thyroid Cancer: When to Treat? MEGAN R. HAYMART, MD
 Thyroid Cancer: When to Treat? MEGAN R. HAYMART, MD ASSOCIATE PROFESSOR OF MEDICINE UNIVERSITY OF MICHIGAN MICHIGAN AACE 2018 ANNUAL MEETING Thyroid Cancer: When Not to Treat? FOCUS WILL BE ON LOW-RISK
Thyroid Cancer: When to Treat? MEGAN R. HAYMART, MD ASSOCIATE PROFESSOR OF MEDICINE UNIVERSITY OF MICHIGAN MICHIGAN AACE 2018 ANNUAL MEETING Thyroid Cancer: When Not to Treat? FOCUS WILL BE ON LOW-RISK
Thyroid Surgery: Lobectomy, total thyroidectomy, LN biopsies or only watchful waiting?
 Thyroid Surgery: Lobectomy, total thyroidectomy, LN biopsies or only watchful waiting? Jacob Moalem, MD, FACS Associate Professor Endocrine Surgery and Endocrinology URMC Agenda 1. When is lobectomy alone
Thyroid Surgery: Lobectomy, total thyroidectomy, LN biopsies or only watchful waiting? Jacob Moalem, MD, FACS Associate Professor Endocrine Surgery and Endocrinology URMC Agenda 1. When is lobectomy alone
Key Topics in Thyroid Cancer Worldwide epidemic What Should the Endocrinologist and Surgeon do?
 Key Topics in Thyroid Cancer Worldwide epidemic What Should the Endocrinologist and Surgeon do? Martin Schlumberger Gustave Presenter Roussy Name and Université Paris Saclay, Villejuif, France 1 Disclosure
Key Topics in Thyroid Cancer Worldwide epidemic What Should the Endocrinologist and Surgeon do? Martin Schlumberger Gustave Presenter Roussy Name and Université Paris Saclay, Villejuif, France 1 Disclosure
How Will (Should) the Latest Guidelines Affect the Endocrinologist s Management of Thyroid Cancer? AACE 2017
 the Latest Guidelines Affect the Endocrinologist s Management of Thyroid Cancer? AACE 2017") How Will (Should) the Latest Guidelines Affect the Endocrinologist s Management of Thyroid Cancer? AACE 2017 Bryan R. Haugen, MD University of Colorado, School of Medicine Outline Some statistics New guidelines
How Will (Should) the Latest Guidelines Affect the Endocrinologist s Management of Thyroid Cancer? AACE 2017 Bryan R. Haugen, MD University of Colorado, School of Medicine Outline Some statistics New guidelines
Disclosures Nodal Management in Differentiated Thyroid Carcinoma
 Disclosures Nodal Management in Differentiated Thyroid Carcinoma Nothing to disclose Jonathan George, MD, MPH Assistant Professor UCSF Head and Neck Oncologic & Endocrine Surgery Objectives Overview Describe
Disclosures Nodal Management in Differentiated Thyroid Carcinoma Nothing to disclose Jonathan George, MD, MPH Assistant Professor UCSF Head and Neck Oncologic & Endocrine Surgery Objectives Overview Describe
Preoperative Evaluation
 Preoperative Evaluation Lateral compartment lymph nodes are easier to detect and are amenable to FNA Central compartment lymph nodes are much more difficult to detect and FNA (Tg washout testing is compromised)
Preoperative Evaluation Lateral compartment lymph nodes are easier to detect and are amenable to FNA Central compartment lymph nodes are much more difficult to detect and FNA (Tg washout testing is compromised)
The International Federation of Head and Neck Oncologic Societies. Current Concepts in Head and Neck Surgery and Oncology
 The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
Persistent & Recurrent Differentiated Thyroid Cancer
 Persistent & Recurrent Differentiated Thyroid Cancer Electron Kebebew University of California, San Francisco Department of Surgery Objectives Risk factors for persistent & recurrent disease Causes of
Persistent & Recurrent Differentiated Thyroid Cancer Electron Kebebew University of California, San Francisco Department of Surgery Objectives Risk factors for persistent & recurrent disease Causes of
Success rate of thyroid remnant ablation for differentiated thyroid cancer based on 5550 MBq post-therapy scan
 ORIGINAL ARTICLE Success rate of thyroid remnant ablation for differentiated thyroid cancer based on 5550 MBq post-therapy scan I. Hommel 1 *, G.F. Pieters 1, A.J.M. Rijnders 2, M.M. van Borren 3, H. de
ORIGINAL ARTICLE Success rate of thyroid remnant ablation for differentiated thyroid cancer based on 5550 MBq post-therapy scan I. Hommel 1 *, G.F. Pieters 1, A.J.M. Rijnders 2, M.M. van Borren 3, H. de
Thyroid Nodule. Disclosure. Learning Objectives P A P A P A 3/18/2014. Nothing to disclose.
 Thyroid Nodule Evaluating the patient with a thyroid nodule and some management options. Miguel V. Valdez PA C Disclosure Nothing to disclose. Learning Objectives Examination of thyroid gland Options for
Thyroid Nodule Evaluating the patient with a thyroid nodule and some management options. Miguel V. Valdez PA C Disclosure Nothing to disclose. Learning Objectives Examination of thyroid gland Options for
Thyroid Gland. Protocol applies to all malignant tumors of the thyroid gland, except lymphomas.
 Thyroid Gland Protocol applies to all malignant tumors of the thyroid gland, except lymphomas. Procedures Cytology (No Accompanying Checklist) Partial Thyroidectomy Total Thyroidectomy With/Without Lymph
Thyroid Gland Protocol applies to all malignant tumors of the thyroid gland, except lymphomas. Procedures Cytology (No Accompanying Checklist) Partial Thyroidectomy Total Thyroidectomy With/Without Lymph
Towards a selective use of postoperative radioiodine in thyroid cancer patients
 Towards a selective use of postoperative radioiodine in thyroid cancer patients Martin Schlumberger Gustave Presenter Roussy Name and Université Paris Saclay, Villejuif, France 1 Disclosure Relevant financial
Towards a selective use of postoperative radioiodine in thyroid cancer patients Martin Schlumberger Gustave Presenter Roussy Name and Université Paris Saclay, Villejuif, France 1 Disclosure Relevant financial
Differentiated Thyroid Carcinoma
 Differentiated Thyroid Carcinoma The GOOD cancer? Jennifer Sipos, MD Associate Professor of Medicine Director, Benign Thyroid Program Division of Endocrinology, Diabetes and Metabolism The Ohio State University
Differentiated Thyroid Carcinoma The GOOD cancer? Jennifer Sipos, MD Associate Professor of Medicine Director, Benign Thyroid Program Division of Endocrinology, Diabetes and Metabolism The Ohio State University
Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer
 Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer AACE - Advances in Medical and Surgical Management of Thyroid Cancer - 2018 Robert A. Levine, MD, FACE, ECNU Thyroid Center of New Hampshire Geisel
Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer AACE - Advances in Medical and Surgical Management of Thyroid Cancer - 2018 Robert A. Levine, MD, FACE, ECNU Thyroid Center of New Hampshire Geisel
Thyroid INTRODUCTION ANATOMY SUMMARY OF CHANGES
 AJC 7/14/06 1:19 PM Page 67 Thyroid C73.9 Thyroid gland SUMMARY OF CHANGES Tumor staging (T) has been revised and the categories redefined. T4 is now divided into T4a and T4b. Nodal staging (N) has been
AJC 7/14/06 1:19 PM Page 67 Thyroid C73.9 Thyroid gland SUMMARY OF CHANGES Tumor staging (T) has been revised and the categories redefined. T4 is now divided into T4a and T4b. Nodal staging (N) has been
Case-Based Discussion of Thyroid Cancer Therapy
 Case-Based Discussion of Thyroid Cancer Therapy Matthew D. Ringel, MD Ralph W. Kurtz Chair and Professor of Medicine Director, Division of Endocrinology The Ohio State University Co-Leader, Molecular Biology
Case-Based Discussion of Thyroid Cancer Therapy Matthew D. Ringel, MD Ralph W. Kurtz Chair and Professor of Medicine Director, Division of Endocrinology The Ohio State University Co-Leader, Molecular Biology
THYROID CANCER IN CHILDREN
 THYROID CANCER IN CHILDREN Isabel ROCA, Montserrat NEGRE Joan CASTELL HU VALL HEBRON BARCELONA EPIDEMIOLOGY ADULTS males 1,2-2,6 cases /100.000 females 2,0-3,8 cases /100.000 0,02-0,3 / 100.000 children
THYROID CANCER IN CHILDREN Isabel ROCA, Montserrat NEGRE Joan CASTELL HU VALL HEBRON BARCELONA EPIDEMIOLOGY ADULTS males 1,2-2,6 cases /100.000 females 2,0-3,8 cases /100.000 0,02-0,3 / 100.000 children
New Visions in PET: Surgical Decision Making and PET/CT
 New Visions in PET: Surgical Decision Making and PET/CT Stanley J. Goldsmith, MD Director, Nuclear Medicine Professor, Radiology & Medicine New York Presbyterian Hospital- Weill Cornell Medical Center
New Visions in PET: Surgical Decision Making and PET/CT Stanley J. Goldsmith, MD Director, Nuclear Medicine Professor, Radiology & Medicine New York Presbyterian Hospital- Weill Cornell Medical Center
What s an NIFTP? Keeping Up To Date in Thyroid 2018
 What s an NIFTP? Keeping Up To Date in Thyroid 2018 Kathleen Hands, MD, FACE, ECNU Director, Thyroid Center of South Texas Assistant Clinical Professor UTHSCSA DrHands@Thyroid-Center.com 210-844-6163 text
What s an NIFTP? Keeping Up To Date in Thyroid 2018 Kathleen Hands, MD, FACE, ECNU Director, Thyroid Center of South Texas Assistant Clinical Professor UTHSCSA DrHands@Thyroid-Center.com 210-844-6163 text
Thyroid Cancer & rhtsh: When and How?
 Thyroid Cancer & rhtsh: When and How? 8 th Postgraduate Course in Endocrine Surgery Capsis Beach, Crete, September 21, 2006 Quan-Yang Duh, Professor of Surgery, UCSF Increasing Incidence of Thyroid Cancer
Thyroid Cancer & rhtsh: When and How? 8 th Postgraduate Course in Endocrine Surgery Capsis Beach, Crete, September 21, 2006 Quan-Yang Duh, Professor of Surgery, UCSF Increasing Incidence of Thyroid Cancer
Current Issues in Thyroid Cancer Surgery in 2017
 Current Issues in Thyroid Cancer Surgery in 2017 Dr. David Goldstein MD Msc FRCSC FACS Associate Professor, Department Otolaryngology Head & Neck Surgery, U of T Department of Surgical Oncology, Princess
Current Issues in Thyroid Cancer Surgery in 2017 Dr. David Goldstein MD Msc FRCSC FACS Associate Professor, Department Otolaryngology Head & Neck Surgery, U of T Department of Surgical Oncology, Princess
Correspondence should be addressed to Stan H. M. Van Uum;
 Oncology Volume 2016, Article ID 6496750, 6 pages http://dx.doi.org/10.1155/2016/6496750 Research Article Recombinant Human Thyroid Stimulating Hormone versus Thyroid Hormone Withdrawal for Radioactive
Oncology Volume 2016, Article ID 6496750, 6 pages http://dx.doi.org/10.1155/2016/6496750 Research Article Recombinant Human Thyroid Stimulating Hormone versus Thyroid Hormone Withdrawal for Radioactive
YCN Thyroid NSSG. *** VALID ON DATE OF PRINTING ONLY - all guidelines available at *** page 1 of 8 version number: 1.
 YCN Thyroid NSSG Guidelines on Indications for Thyroid Surgery, Prophylactic Level 6 and Radioiodine plus follow-up of low risk differentiated thyroid cancer page 1 of 8 i Document Control Title Author(s)
YCN Thyroid NSSG Guidelines on Indications for Thyroid Surgery, Prophylactic Level 6 and Radioiodine plus follow-up of low risk differentiated thyroid cancer page 1 of 8 i Document Control Title Author(s)
Ultrasound for Pre-operative Evaluation of Well Differentiated Thyroid Cancer
 Ultrasound for Pre-operative Evaluation of Well Differentiated Thyroid Cancer Its Not Just About the Nodes AACE Advances in Medical and Surgical Management of Thyroid Cancer - 2017 Robert A. Levine, MD,
Ultrasound for Pre-operative Evaluation of Well Differentiated Thyroid Cancer Its Not Just About the Nodes AACE Advances in Medical and Surgical Management of Thyroid Cancer - 2017 Robert A. Levine, MD,
AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS
 AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS PAPILLARY THYROID CARCINOMA Clinical Any age Microscopic to large Female: Male= 2-4:1 Radiation history Lymph nodes Prognosis
AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS PAPILLARY THYROID CARCINOMA Clinical Any age Microscopic to large Female: Male= 2-4:1 Radiation history Lymph nodes Prognosis
10/24/2008. Surgery for Well-differentiated Thyroid Carcinoma- The Primary
 Surgery for Well-differentiated Thyroid Carcinoma- The Primary Head and Neck Endocrine Surgery Department of Otolaryngology-Head and Neck Surgery, UCSF October 24-25, 2008 Robert A. Sofferman, MD Professor
Surgery for Well-differentiated Thyroid Carcinoma- The Primary Head and Neck Endocrine Surgery Department of Otolaryngology-Head and Neck Surgery, UCSF October 24-25, 2008 Robert A. Sofferman, MD Professor
I treatment for differentiated thyroid carcinoma Current guidelines
 131 I treatment for differentiated thyroid carcinoma Current guidelines François Jamar, UCL Brussels francois.jamar@uclouvain.be IAEA-Belnuc Theranostics course Brussels, October 5 th, 2017 131 I treatment
131 I treatment for differentiated thyroid carcinoma Current guidelines François Jamar, UCL Brussels francois.jamar@uclouvain.be IAEA-Belnuc Theranostics course Brussels, October 5 th, 2017 131 I treatment
PET/CT Frequently Asked Questions
 PET/CT Frequently Asked Questions General Q: Is FDG PET specific for cancer? A: No, it is a marker of metabolism. In general, any disease that causes increased metabolism can result in increased FDG uptake
PET/CT Frequently Asked Questions General Q: Is FDG PET specific for cancer? A: No, it is a marker of metabolism. In general, any disease that causes increased metabolism can result in increased FDG uptake
Reference No: Author(s) Approval date: October committee. September Operational Date: Review:
 Approval date: October committee. September Operational Date: Review:") Reference No: Title: Author(s) Systemic Anti-Cancer Therapy (SACT) guidelines for Thyroid cancer Dr Fionnuala Houghton Consultant Clinical Oncologist & Dr Lois Mulholland Consultant Clinical Oncologist
Reference No: Title: Author(s) Systemic Anti-Cancer Therapy (SACT) guidelines for Thyroid cancer Dr Fionnuala Houghton Consultant Clinical Oncologist & Dr Lois Mulholland Consultant Clinical Oncologist
Definition of Synoptic Reporting
 Definition of Synoptic Reporting The CAP has developed this list of specific features that define synoptic reporting formatting: 1. All required cancer data from an applicable cancer protocol that are
Definition of Synoptic Reporting The CAP has developed this list of specific features that define synoptic reporting formatting: 1. All required cancer data from an applicable cancer protocol that are
Long Term Follow-Up for Differentiated Thyroid Cancer: The Mayo Experience
 Long Term Follow-Up for Differentiated Thyroid Cancer: The Mayo Experience Geoffrey B. Thompson, MD Professor of Surgery College of Medicine, Mayo Clinic Differentiated Thyroid Cancer Objectives Overview
Long Term Follow-Up for Differentiated Thyroid Cancer: The Mayo Experience Geoffrey B. Thompson, MD Professor of Surgery College of Medicine, Mayo Clinic Differentiated Thyroid Cancer Objectives Overview
Management guideline for patients with differentiated thyroid cancer. Teeraporn Ratanaanekchai ENT, KKU 17 October 2007
 Management guideline for patients with differentiated thyroid Teeraporn Ratanaanekchai ENT, KKU 17 October 2007 Incidence (Srinagarind Hospital, 2005, both sex) Site (all) cases % 1. Liver 1178 27 2. Lung
Management guideline for patients with differentiated thyroid Teeraporn Ratanaanekchai ENT, KKU 17 October 2007 Incidence (Srinagarind Hospital, 2005, both sex) Site (all) cases % 1. Liver 1178 27 2. Lung
Editorial Process: Submission:07/27/2017 Acceptance:01/06/2018
 DOI:10.22034/APJCP.2018.19.2.303 Hybrid Imaging in Thyroid Carcinoma REVIEW Editorial Process: Submission:07/27/2017 Acceptance:01/06/2018 Hybrid SPECT/CT Imaging in the Management of Differentiated Thyroid
DOI:10.22034/APJCP.2018.19.2.303 Hybrid Imaging in Thyroid Carcinoma REVIEW Editorial Process: Submission:07/27/2017 Acceptance:01/06/2018 Hybrid SPECT/CT Imaging in the Management of Differentiated Thyroid
Case 5: Thyroid cancer in 42 yr-old woman with Graves disease
 Case 5: Thyroid cancer in 42 yr-old woman with Graves disease Giuliano Mariani Regional Center of Nuclear Medicine, University of Pisa Medical School, Pisa (Italy) Thyroid cancer in 42 yr-old woman with
Case 5: Thyroid cancer in 42 yr-old woman with Graves disease Giuliano Mariani Regional Center of Nuclear Medicine, University of Pisa Medical School, Pisa (Italy) Thyroid cancer in 42 yr-old woman with
Endocrine, Original Article The Impact of Thyroid Stunning on Radioactive Iodine Ablation Compared to Other Risk Factors
 68 Endocrine, Original Article The Impact of Thyroid Stunning on Radioactive Iodine Ablation Compared to Other Risk Factors Abd El-Kareem, M *, El-Refaie, SH *, Zaher, A **, Abo-Gaba, Ml * and Abdo, S
68 Endocrine, Original Article The Impact of Thyroid Stunning on Radioactive Iodine Ablation Compared to Other Risk Factors Abd El-Kareem, M *, El-Refaie, SH *, Zaher, A **, Abo-Gaba, Ml * and Abdo, S
Los Angeles Radiological Society 62 nd Annual Midwinter Radiology Conference January 31, 2010
 Los Angeles Radiological Society 62 nd Annual Midwinter Radiology Conference January 31, 2010 Self Assessment Module on Nuclear Medicine and PET/CT Case Review FDG PET/CT IN LYMPHOMA AND MELANOMA Submitted
Los Angeles Radiological Society 62 nd Annual Midwinter Radiology Conference January 31, 2010 Self Assessment Module on Nuclear Medicine and PET/CT Case Review FDG PET/CT IN LYMPHOMA AND MELANOMA Submitted
34 year-old Female with Thyroid Cancer
 34 year-old Female with Thyroid Cancer KATIE O SULLIVAN, MD FELLOW, ADULT/PEDIATRIC ENDOCRINOLOGY UNIVERSITY OF CHICAGO ENDORAMA THURSDAY, SEPTEMBER 15 TH, 2016 Disclosures: I do not have any relevant
34 year-old Female with Thyroid Cancer KATIE O SULLIVAN, MD FELLOW, ADULT/PEDIATRIC ENDOCRINOLOGY UNIVERSITY OF CHICAGO ENDORAMA THURSDAY, SEPTEMBER 15 TH, 2016 Disclosures: I do not have any relevant
Clinical indications for positron emission tomography
 Clinical indications for positron emission tomography Oncology applications Brain and spinal cord Parotid Suspected tumour recurrence when anatomical imaging is difficult or equivocal and management will
Clinical indications for positron emission tomography Oncology applications Brain and spinal cord Parotid Suspected tumour recurrence when anatomical imaging is difficult or equivocal and management will
Ini7al Staging of Follicular Cell-derived Thyroid Cancers: the ATA 2015 IRS and AJCC 8th Ed. Cancer Staging Systems
 12/25/17 9th Annual AACE Advances in Thyroid Cancer Course Tempe, Arizona January 12-13, 2018. Ini7al Staging of Follicular Cell-derived Thyroid Cancers: the ATA 2015 IRS and AJCC 8th Ed. Cancer Staging
12/25/17 9th Annual AACE Advances in Thyroid Cancer Course Tempe, Arizona January 12-13, 2018. Ini7al Staging of Follicular Cell-derived Thyroid Cancers: the ATA 2015 IRS and AJCC 8th Ed. Cancer Staging
Thyroid Pathology: It starts and ends with the gross. Causes of Thyrophobia. Agenda. Diagnostic ambiguity. Treatment/prognosis disconnect
 Thyroid Pathology: It starts and ends with the gross Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for
Thyroid Pathology: It starts and ends with the gross Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for
Case #1: 75 y/o Male (treated and followed by prostate cancer oncology specialist ).
.") SOLID TUMORS WORKSHOP Cases for review Prostate Cancer Case #1: 75 y/o Male (treated and followed by prostate cancer oncology specialist ). January 2009 PSA 4.4, 20% free; August 2009 PSA 5.2; Sept 2009
SOLID TUMORS WORKSHOP Cases for review Prostate Cancer Case #1: 75 y/o Male (treated and followed by prostate cancer oncology specialist ). January 2009 PSA 4.4, 20% free; August 2009 PSA 5.2; Sept 2009
Management of Recurrent Thyroid Cancer
 Management of Recurrent Thyroid Cancer Eric Genden, MD, MHA Isidore Professor and Chairman Department of Otolaryngology- Head and Neck Surgery Senior Associate Dean for Clinical Affairs The Icahn School
Management of Recurrent Thyroid Cancer Eric Genden, MD, MHA Isidore Professor and Chairman Department of Otolaryngology- Head and Neck Surgery Senior Associate Dean for Clinical Affairs The Icahn School
THYROID FUNCTION TEST and RADIONUCLIDE THERAPY
 THYROID FUNCTION TEST and RADIONUCLIDE THERAPY Ajalaya Teyateeti, M.D. Division of Nuclear Medicine Department of Radiology I. Thyroid function test OUTLINE Application and interpretation of in vitro TFT
THYROID FUNCTION TEST and RADIONUCLIDE THERAPY Ajalaya Teyateeti, M.D. Division of Nuclear Medicine Department of Radiology I. Thyroid function test OUTLINE Application and interpretation of in vitro TFT
RESEARCH ARTICLE. Comparison of Presentation and Clinical Outcome between Children and Young Adults with Differentiated Thyroid Cancer
 RESEARCH ARTICLE Comparison of Presentation and Clinical Outcome between Children and Young Adults with Jian-Tao Wang 1,2&, Rui Huang 1&, An-Ren Kuang 1 * Abstract Background: The aim of the present study
RESEARCH ARTICLE Comparison of Presentation and Clinical Outcome between Children and Young Adults with Jian-Tao Wang 1,2&, Rui Huang 1&, An-Ren Kuang 1 * Abstract Background: The aim of the present study
Thyroid and Adrenal Gland
 Thyroid and Adrenal Gland NAACCR 2011 2012 Webinar Series 12/1/11 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
Thyroid and Adrenal Gland NAACCR 2011 2012 Webinar Series 12/1/11 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
저작권법에따른이용자의권리는위의내용에의하여영향을받지않습니다.
 저작자표시 - 비영리 - 변경금지 2.0 대한민국 이용자는아래의조건을따르는경우에한하여자유롭게 이저작물을복제, 배포, 전송, 전시, 공연및방송할수있습니다. 다음과같은조건을따라야합니다 : 저작자표시. 귀하는원저작자를표시하여야합니다. 비영리. 귀하는이저작물을영리목적으로이용할수없습니다. 변경금지. 귀하는이저작물을개작, 변형또는가공할수없습니다. 귀하는, 이저작물의재이용이나배포의경우,
저작자표시 - 비영리 - 변경금지 2.0 대한민국 이용자는아래의조건을따르는경우에한하여자유롭게 이저작물을복제, 배포, 전송, 전시, 공연및방송할수있습니다. 다음과같은조건을따라야합니다 : 저작자표시. 귀하는원저작자를표시하여야합니다. 비영리. 귀하는이저작물을영리목적으로이용할수없습니다. 변경금지. 귀하는이저작물을개작, 변형또는가공할수없습니다. 귀하는, 이저작물의재이용이나배포의경우,
Distant and Lymph Node Metastases of Thyroid Nodules with No Pathological Evidence of Malignancy: A Limitation of Pathological Examination
 Endocrine Journal 2008, 55 (5), 889 894 Distant and Lymph Node Metastases of Thyroid Nodules with No Pathological Evidence of Malignancy: A Limitation of Pathological Examination YASUHIRO ITO, TOMONORI
Endocrine Journal 2008, 55 (5), 889 894 Distant and Lymph Node Metastases of Thyroid Nodules with No Pathological Evidence of Malignancy: A Limitation of Pathological Examination YASUHIRO ITO, TOMONORI
Role of Radio-Iodine Ablation According to Risk Stratification in Well Differentiated Thyroid Cancer
 Journal of the Egyptian Nat. Cancer Inst., Vol. 13, No. 1, March: 6369, 2001 Role of RadioIodine Ablation According to Risk Stratification in Well Differentiated Thyroid Cancer HOSNA MOUSTAFA, M.D.*; SHEREEN
Journal of the Egyptian Nat. Cancer Inst., Vol. 13, No. 1, March: 6369, 2001 Role of RadioIodine Ablation According to Risk Stratification in Well Differentiated Thyroid Cancer HOSNA MOUSTAFA, M.D.*; SHEREEN
American College of Radiology ACR Appropriateness Criteria
 American College of Radiology ACR Criteria Thyroid Carcinoma Variant 1: T1a N0 M0 papillary thyroid cancer: 40-year-old woman. 30 mci with thyrotropin 100 mci with thyrotropin 30 mci with thyroid hormone
American College of Radiology ACR Criteria Thyroid Carcinoma Variant 1: T1a N0 M0 papillary thyroid cancer: 40-year-old woman. 30 mci with thyrotropin 100 mci with thyrotropin 30 mci with thyroid hormone
International Czech and Slovak cooperation in the treatment of patients with differentiated thyroid cancer
 Nuclear Medicine Review 2006 Vol. 9, No. 1, pp. 84 88 Copyright 2006 Via Medica ISSN 1506 9680 International Czech and Slovak cooperation in the treatment of patients with differentiated thyroid cancer
Nuclear Medicine Review 2006 Vol. 9, No. 1, pp. 84 88 Copyright 2006 Via Medica ISSN 1506 9680 International Czech and Slovak cooperation in the treatment of patients with differentiated thyroid cancer
Case Scenario 1 Worksheet. Primary Site C44.4 Morphology 8743/3 Laterality 0 Stage/ Prognostic Factors
 CASE SCENARIO 1 9/10/13 HISTORY: Patient is a 67-year-old white male and presents with lesion located 4-5cm above his right ear. The lesion has been present for years. No lymphadenopathy. 9/10/13 anterior
CASE SCENARIO 1 9/10/13 HISTORY: Patient is a 67-year-old white male and presents with lesion located 4-5cm above his right ear. The lesion has been present for years. No lymphadenopathy. 9/10/13 anterior
New York, the nation s thyroid gland. Christopher Morley ( ), "Shore Leave"
, Shore Leave") New York, the nation s thyroid gland Christopher Morley (1890-1957), "Shore Leave" Thyroid Literature Medline Thyroid disease 136,053 Thyroid tumors 33,554 New Paper on Thyroid Disease Every 3 Hours New
New York, the nation s thyroid gland Christopher Morley (1890-1957), "Shore Leave" Thyroid Literature Medline Thyroid disease 136,053 Thyroid tumors 33,554 New Paper on Thyroid Disease Every 3 Hours New
AN INTRODUCTION TO NUCLEAR MEDICINE
 AN INTRODUCTION TO NUCLEAR MEDICINE WITH RESPECT TO THYROID DISORDERS By: B.Shafiei MD Nuclear Physician Taleghani Medical Center Radioactive: An element with Unstable Nucleus (Excess Energy), can achieve
AN INTRODUCTION TO NUCLEAR MEDICINE WITH RESPECT TO THYROID DISORDERS By: B.Shafiei MD Nuclear Physician Taleghani Medical Center Radioactive: An element with Unstable Nucleus (Excess Energy), can achieve
Review Article Management of papillary and follicular (differentiated) thyroid carcinoma-an update
 thyroid carcinoma-an update") Bangladesh J Otorhinolaryngol 2010; 16(2): 126-130 Review Article Management of papillary and follicular (differentiated) thyroid carcinoma-an update Md. Abdul Mobin Choudhury 1, Md. Abdul Alim Shaikh
Bangladesh J Otorhinolaryngol 2010; 16(2): 126-130 Review Article Management of papillary and follicular (differentiated) thyroid carcinoma-an update Md. Abdul Mobin Choudhury 1, Md. Abdul Alim Shaikh
Radiology- Pathology Conference 4/29/2012. Lymph Nodes. John McGrath
 Radiology- Pathology Conference 4/29/2012 Lymph Nodes John McGrath 1 Presentation material is for education purposes only. All rights reserved. 2012 URMC Radiology Page 1 of 24 Case 1: 51 year-old male
Radiology- Pathology Conference 4/29/2012 Lymph Nodes John McGrath 1 Presentation material is for education purposes only. All rights reserved. 2012 URMC Radiology Page 1 of 24 Case 1: 51 year-old male
(Not so) New Guidelines for Management of Thyroid Nodules and Differentiated Thyroid Cancer Minnesota/Midwest Chapter of AACE
 New Guidelines for Management of Thyroid Nodules and Differentiated Thyroid Cancer Minnesota/Midwest Chapter of AACE") (Not so) New Guidelines for Management of Thyroid Nodules and Differentiated Thyroid Cancer Minnesota/Midwest Chapter of AACE Bryan R. Haugen, MD University of Colorado, School of Medicine Outline Some
(Not so) New Guidelines for Management of Thyroid Nodules and Differentiated Thyroid Cancer Minnesota/Midwest Chapter of AACE Bryan R. Haugen, MD University of Colorado, School of Medicine Outline Some
Nuclear Medicine Head and Neck Region. Bán Zsuzsanna, MD University of Pécs, Department of Nuclear Medicine
 Nuclear Medicine Head and Neck Region Bán Zsuzsanna, MD University of Pécs, Department of Nuclear Medicine Thyroid scintigraphy Parathyroid scintigraphy F18-FDG PET examinations in head and neck cancer
Nuclear Medicine Head and Neck Region Bán Zsuzsanna, MD University of Pécs, Department of Nuclear Medicine Thyroid scintigraphy Parathyroid scintigraphy F18-FDG PET examinations in head and neck cancer
Four Cases of Malignant Pleural Effusion in Patients with Papillary Thyroid Carcinoma
 Endocrinol Metab 26(4):330-334, December 2011 CASE REPORT Four Cases of Malignant Pleural Effusion in Patients with Papillary Thyroid Carcinoma Min Ji Jeon, Ji Hye Yim, Eui Young Kim, Won Gu Kim, Tae Yong
Endocrinol Metab 26(4):330-334, December 2011 CASE REPORT Four Cases of Malignant Pleural Effusion in Patients with Papillary Thyroid Carcinoma Min Ji Jeon, Ji Hye Yim, Eui Young Kim, Won Gu Kim, Tae Yong
Dilemmas in Cytopathology and Histopathology
 Dilemmas in Cytopathology and Histopathology Yuri E. Nikiforov, MD, PhD Division of Molecular & Genomic Pathology University of Pittsburgh Medical Center, USA Objectives Discuss new WHO classification
Dilemmas in Cytopathology and Histopathology Yuri E. Nikiforov, MD, PhD Division of Molecular & Genomic Pathology University of Pittsburgh Medical Center, USA Objectives Discuss new WHO classification
Carcinoma tiroideo differenziato: gestione della persistenza biochimica di malattia
 Carcinoma tiroideo differenziato: gestione della persistenza biochimica di malattia Massimo Torlontano U.O. Endocrinologia IRCCS Casa Sollievo della Sofferenza Thyroid cancer Incidence 1975-2009 (USA)
Carcinoma tiroideo differenziato: gestione della persistenza biochimica di malattia Massimo Torlontano U.O. Endocrinologia IRCCS Casa Sollievo della Sofferenza Thyroid cancer Incidence 1975-2009 (USA)
Staging for Residents, Nurses, and Multidisciplinary Health Care Team
 Staging for Residents, Nurses, and Multidisciplinary Health Care Team Donna M. Gress, RHIT, CTR Validating science. Improving patient care. Learning Objectives Introduce the concept and history of stage
Staging for Residents, Nurses, and Multidisciplinary Health Care Team Donna M. Gress, RHIT, CTR Validating science. Improving patient care. Learning Objectives Introduce the concept and history of stage
A variation in recurrence patterns of papillary thyroid cancer with disease progression: A long-term follow-up study
 ORIGINAL ARTICLE A variation in recurrence patterns of papillary thyroid cancer with disease progression: A long-term follow-up study Joon-Hyop Lee, MD, Yoo Seung Chung, MD, PhD,* Young Don Lee, MD, PhD
ORIGINAL ARTICLE A variation in recurrence patterns of papillary thyroid cancer with disease progression: A long-term follow-up study Joon-Hyop Lee, MD, Yoo Seung Chung, MD, PhD,* Young Don Lee, MD, PhD
Index. Surg Oncol Clin N Am 16 (2007) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Surg Oncol Clin N Am 16 (2007) 465 469 Index Note: Page numbers of article titles are in boldface type. A Adjuvant therapy, preoperative for gastric cancer, staging and, 339 B Breast cancer, metabolic
Surg Oncol Clin N Am 16 (2007) 465 469 Index Note: Page numbers of article titles are in boldface type. A Adjuvant therapy, preoperative for gastric cancer, staging and, 339 B Breast cancer, metabolic
Radiation Therapy for Thyroid Cancer. When is Radiation Therapy indicated in Thyroid Cancer of Follicular or Parafollicular Cell Origin?
 When is Radiation Therapy indicated in Thyroid Cancer of Follicular or Parafollicular Cell Origin? Jeanne Marie Quivey MD FACR October 200 Radiation Therapy for Thyroid Cancer Radioactive 3- I (RAI) External
When is Radiation Therapy indicated in Thyroid Cancer of Follicular or Parafollicular Cell Origin? Jeanne Marie Quivey MD FACR October 200 Radiation Therapy for Thyroid Cancer Radioactive 3- I (RAI) External
CAP Cancer Protocol and ecc Summary of Changes for August 2014 Thyroid Agile Release
 CAP Cancer Protocol and ecc Summary of Changes for August 2014 Thyroid Agile Release 2 REVISION HISTORY Date Author / Editor Comments 5/19/2014 Jaleh Mirza Created the document 8/12/2014 Samantha Spencer/Jaleh
CAP Cancer Protocol and ecc Summary of Changes for August 2014 Thyroid Agile Release 2 REVISION HISTORY Date Author / Editor Comments 5/19/2014 Jaleh Mirza Created the document 8/12/2014 Samantha Spencer/Jaleh
Management of Thyroid Nodules
 Management of Thyroid Nodules 38 y/o female with solid 1.5 cm right Thyroid nodule. TSH=0.68 Vincent J. Reid, MD., FACS Thyroid Cancer Incidence & Mortality 1974 to 2004 Overall Women Men Mortality 1 Cancer
Management of Thyroid Nodules 38 y/o female with solid 1.5 cm right Thyroid nodule. TSH=0.68 Vincent J. Reid, MD., FACS Thyroid Cancer Incidence & Mortality 1974 to 2004 Overall Women Men Mortality 1 Cancer
Austin Radiological Association Nuclear Medicine Procedure THERAPY FOR THYROID CANCER (I-131 as Sodium Iodide)
") Austin Radiological Association Nuclear Medicine Procedure THERAPY FOR THYROID CANCER (I-131 as Sodium Iodide) Overview Indications I-131 therapy for Thyroid Cancer, of the papillo-follicular type, is
Austin Radiological Association Nuclear Medicine Procedure THERAPY FOR THYROID CANCER (I-131 as Sodium Iodide) Overview Indications I-131 therapy for Thyroid Cancer, of the papillo-follicular type, is
With the exception of unifocal microcarcinoma with
 Impact of I SPECT/Spiral CT on Nodal Staging of Differentiated Thyroid Carcinoma at the First Radioablation Daniela Schmidt 1, Attila Szikszai 1, Rainer Linke 1, Werner Bautz 2, and Torsten Kuwert 1 1
Impact of I SPECT/Spiral CT on Nodal Staging of Differentiated Thyroid Carcinoma at the First Radioablation Daniela Schmidt 1, Attila Szikszai 1, Rainer Linke 1, Werner Bautz 2, and Torsten Kuwert 1 1
Adina Alazraki, MD, FAAP Assistant Professor Radiology and Pediatrics Emory University and Children s Healthcare of Atlanta
 Adina Alazraki, MD, FAAP Assistant Professor Radiology and Pediatrics Emory University and Children s Healthcare of Atlanta Review recently published pediatric guidelines for management of thyroid nodules
Adina Alazraki, MD, FAAP Assistant Professor Radiology and Pediatrics Emory University and Children s Healthcare of Atlanta Review recently published pediatric guidelines for management of thyroid nodules
ACOS Inquiry and Response Selected Inquires CS Tumor Size/Extension Evaluation, CS Lymph Nodes Evaluation, CS Metastasis at Diagnosis Evaluation *
 ACOS Inquiry and Response Selected Inquires CS Tumor Size/Extension Evaluation, CS Lymph Nodes Evaluation, CS Metastasis at Diagnosis Evaluation * CS Tumor Size/Extension Evaluation 24842 12/11/2007: Q:
ACOS Inquiry and Response Selected Inquires CS Tumor Size/Extension Evaluation, CS Lymph Nodes Evaluation, CS Metastasis at Diagnosis Evaluation * CS Tumor Size/Extension Evaluation 24842 12/11/2007: Q:
Case Scenario 1: Thyroid
 Case Scenario 1: Thyroid History and Physical Patient is an otherwise healthy 80 year old female with the complaint of a neck mass first noticed two weeks ago. The mass has increased in size and is palpable.
Case Scenario 1: Thyroid History and Physical Patient is an otherwise healthy 80 year old female with the complaint of a neck mass first noticed two weeks ago. The mass has increased in size and is palpable.