Thyroid Surgery: Lobectomy, total thyroidectomy, LN biopsies or only watchful waiting?
|
|
|
- Julie Neal
- 5 years ago
- Views:
Transcription

1 Thyroid Surgery: Lobectomy, total thyroidectomy, LN biopsies or only watchful waiting? Jacob Moalem, MD, FACS Associate Professor Endocrine Surgery and Endocrinology URMC
2 Agenda 1. When is lobectomy alone vs total thyroidectomy warranted? 2. Understand when watchful waiting may be medically indicated 3. Role of preoperative neck ultrasound, lymph node biopsy/surgery
3 ROLE OF PREOPERATIVE NECK ULTRASOUND, LYMPH NODE BIOPSY/SURGERY 3
4 Role of neck US: In every case An extension of physical exam, no matter the indication Recurrent PTC Newly diagnosed PTC Thyroid nodule eval phpt 4
5 Recurrent PTC Risk stratification How many areas of concern are there? How deep in the TE groove? In an area previously dissected? Establish diagnosis prior to embarking upon high risk redo surgery 5
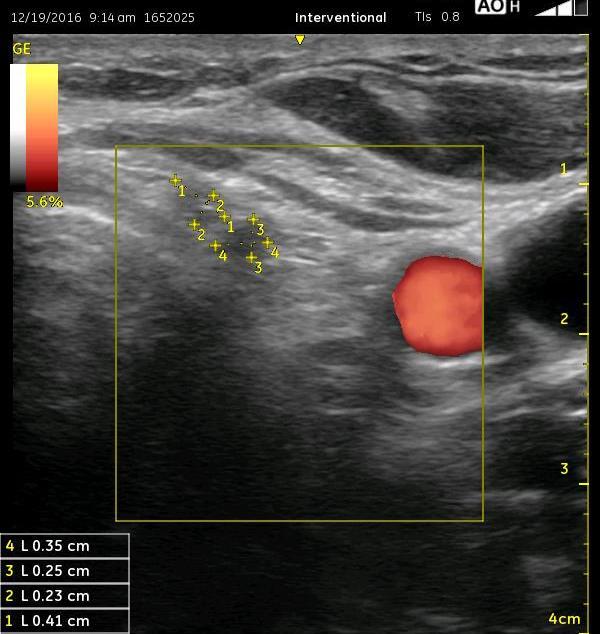
6 Example cases: OD 24, F. Thyroidectomy for Graves disease 2015 Incidental 7, 3 mm mptc July 2018 US : 9 mm hypoechoic mass in thyroid bed recurrent cancer vs. LN metastasis. FNA - PTC 6

7 Office US: 1. It looks like cancer 2. Mass is clearly visible, in its entirety should be relatively easily reachable. 3. Mass is rather anterior should be safely resectable 4. Mass is located 3.5 cm caudal to the incision most likely a level 6 node rather than a thyroid bed recurrence, and should therefore be more easily resectable 7
8 OD OR Findings US guided localization Mass easily identified Area not previously disturbed Central compartment dissection performed Path: Recurrent PTC in 1/14 LN s, 9 mm, +ve ETE 8
9 Role of US example 2 34 YOM, 2015 TTX, central, left lateral neck dissection Bilateral PTC, 6 central, 2 lateral nodes positive Radioiodine 156 mci TG 4.2 (TSH.43), stimulated to 27 Uptake scan: left thyroid bed uptake, no distal uptake US: left central 3, 5 mm nodules FNA : PTC 9
10 10
11 Results for BECKER, TIMOTHY (MRN ) as of 9/22/ :43 1/18/ :59 7/10/ :54 TSH (L) T4 8.6 Free T4 1.7 Thyroglobulin,Qn Thyroglobulin Ab <20 <0.9 11

12 ATA: 12 THYROID, Vol12, number 12, 2002

13 Newly diagnosed cancer confluent adenopathy 13
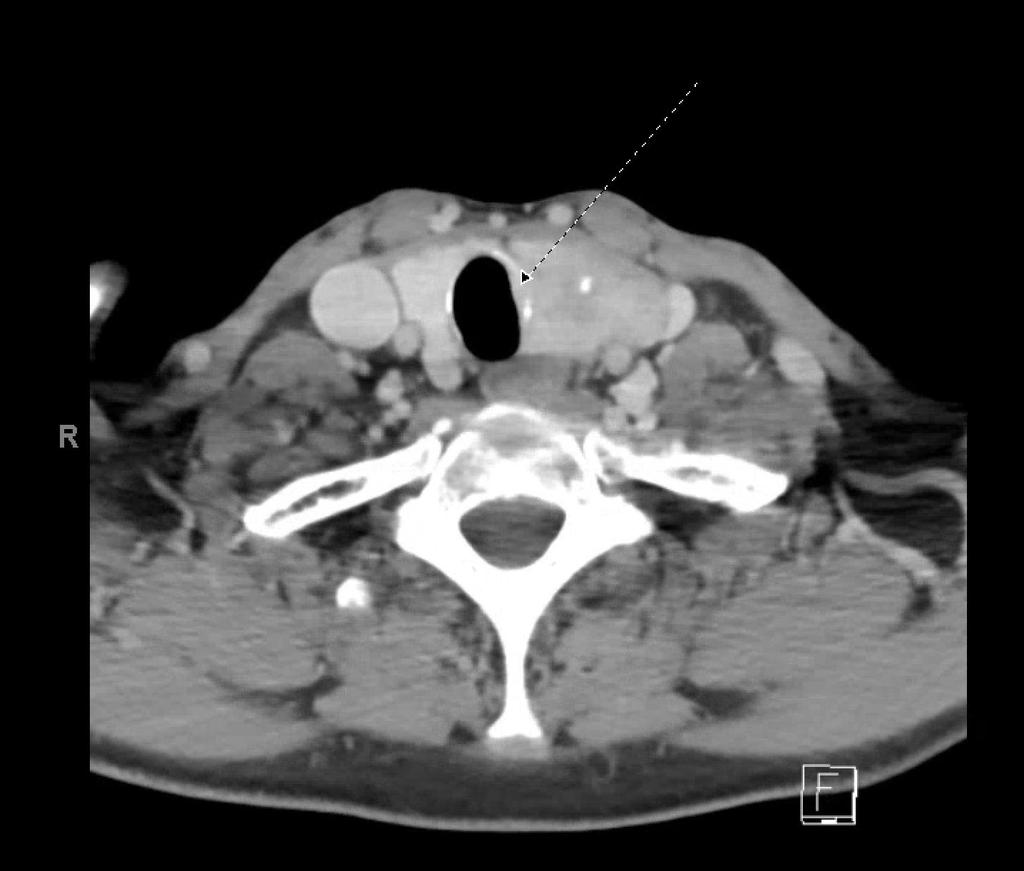
14 Role of CT Scan in advanced DTC (rec 33): Preoperative use of cross-sectional imaging studies with IV contrast is recommended as an adjunct to US for patients with clinical suspicion for advanced disease? Locally invasive primary tumor? bulky nodal involvement retropharyngeal, upper mediastinal 14 THYROID, Vol12, number 12, 2002
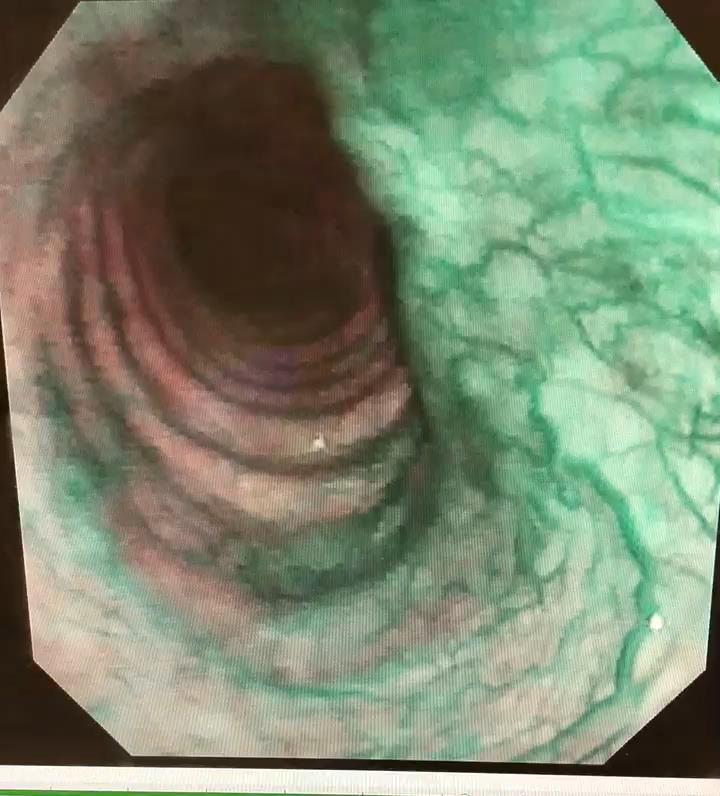
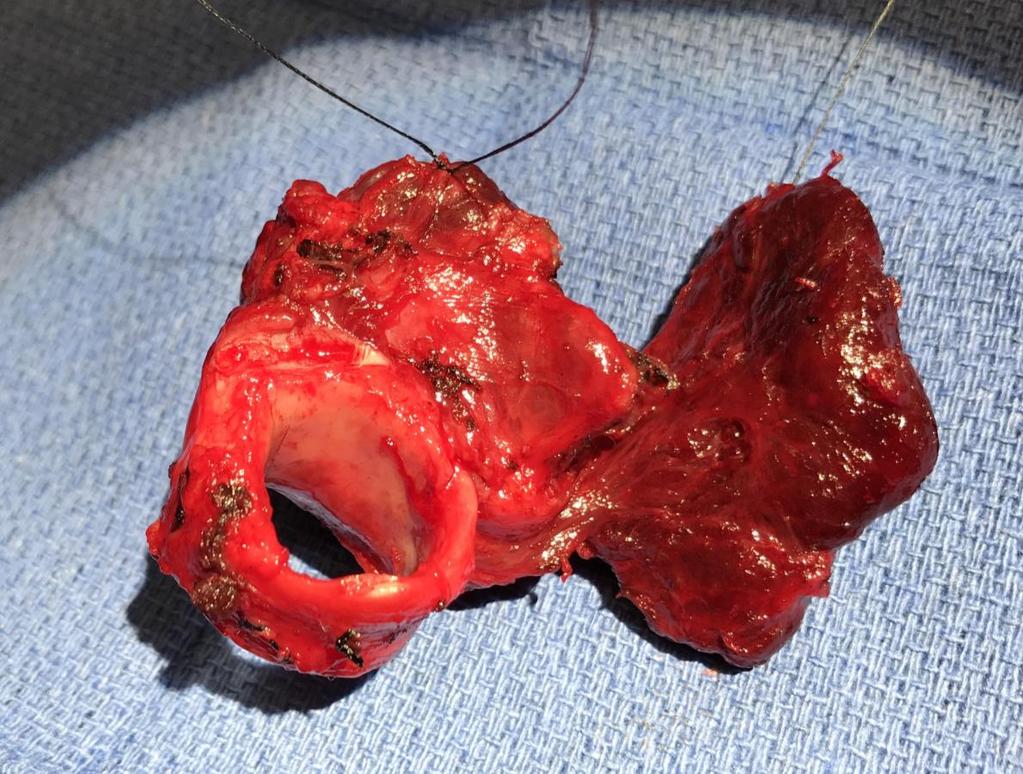
15 Role of axial imaging in advanced PTC: 61 M, Hoarse for 6 months 4 cm left thyroid mass, immobile, rock hard Palpable 3 cm lateral neck node US neck 4 cm left cancer, posterior margin indistinct - left neck lymphadenopathy 15
16 16
17 17
18 18
19 19
20 When should LN Biopsy be done? When it will influence operative management. Will surgery be recommended if positive? If negative? Patient acceptance of large surgery 20

21 39 YO M 3/2016 TTX, bilateral central and right MRLND 1.5 cm non encapsulated PTC 9/12 nodes +ve in central neck, 0.5 cm largest 2/26 nodes +ve in lateral neck, 2.5 cm largest, +ETE 6/ mci TG, TG Ab undetectable Thyroid scan no uptake 5/2018 US neck: 21
22 CD - Cont FNA neck mass histiocytes and cellular debris Core Biopsy - Skeletal muscle and fibrous tissue with eosinophilic amorphous material Redo neck dissection Neck, right lateral, excision: Chronic inflammatory and cystic changes. Foreign body type giant cell reaction to suture material. - Suggestive granulomatous inflammation. - No thyroid tissue or malignancy identified. 22

23 Primary HPT 59 YOF with h/o untreated subclinical hyperthyroidism, afib, now diagnosed with phpt 23

24 24 THYROID, Vol12, number 12, 2002


25 5.3% 25 J Surg Res November ; 178(1):
26 WHEN MAY WATCHFUL WAITING BE MEDICALLY INDICATED? 26

27
28 JAMA. 2017;317(13):
29 JAMA. 2017; 317(13):
30 Cancer Res; AACR.

31 Cancer Res; AACR.

32 Differentiated thyroid cancer
33 The thyroid cancer paradox The cancer you want to get Rare deaths Life-long follow up Rising prevalence Imperfect surveillance Treatment associated morbidity operative reoperative

34 Retrospective analysis that used a variety of medical, personal, legal, and bankruptcy sources covering the Western District of Washington State in US Bankruptcy Court between HEALTH AFFAIRS 32, NO. 6 (2013):
35 2.6x higher bankruptcy rate Younger patients had 2-5x higher rate than older (65+) HEALTH AFFAIRS 32, NO. 6 (2013):
: 1143")
36 HEALTH AFFAIRS 32, NO. 6 (2013):
37 37
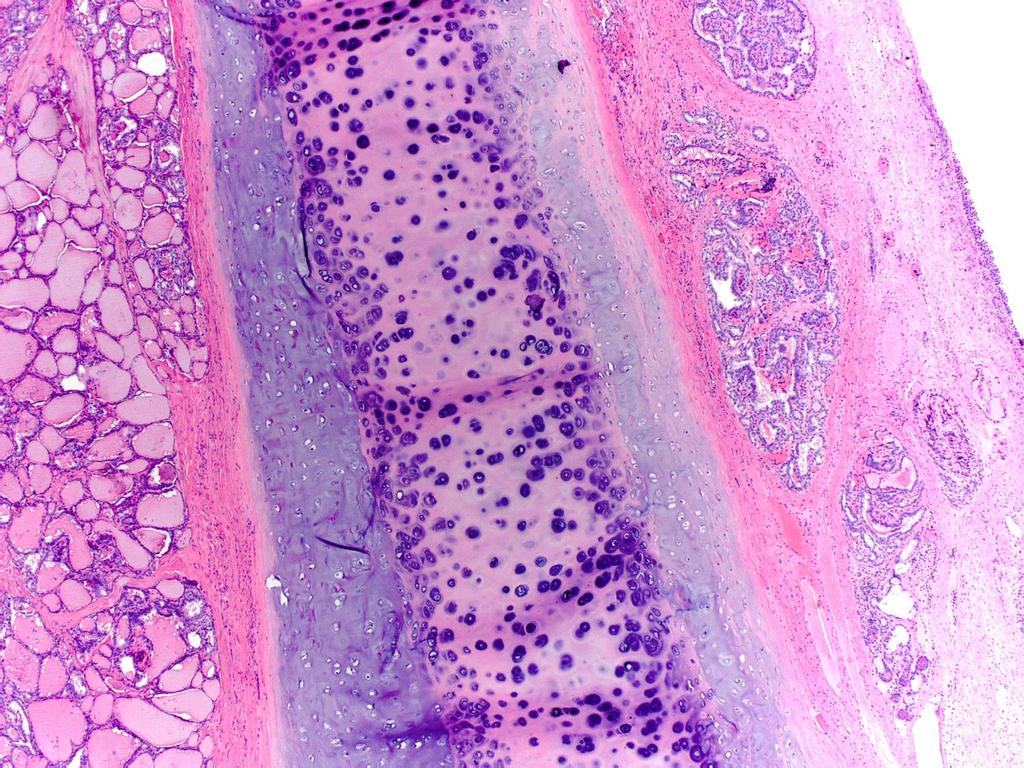
38 Thyroid microcarcinomas (mptc) Japanese experience Account for 30% of PTC A mass screening study for thyroid cancer in Japanese adult women detected mptc in 3.5% of the examinees close to the incidence of latent thyroid cancer >1,000x the reported prevalence of clinical thyroid cancer LN metastasis was pathologically detected in up to 2/3 Unsuspected in 40% 38
39 Ito et al, Thyroid 13, 4, consecutive patients with mptc over 8 years observation vs. surgical treatment unless: Adjacent to the trachea, or possibly invading RLN FNAB suggesting high-grade malignancy LN highly suspicious (or proven) for metastasis in lateral neck 162/732 chose observation initially 56 crossed over to surgical arm during the study Surgical group : =
40 40 Ito et al, Thyroid 13, 4, 2003
41 41 Ito et al, Thyroid 13, 4, 2003
42 Results, Observation group: >70% of mptc s did not increase in size In 18 patients (11%) tumor grew to >1 cm 10 chose continued observation no further change Lateral neck nodes appeared in only 2 patients 42 Ito et al, Thyroid 13, 4, 2003
43 Results, Surgical group 65 crossover patients: Tumor size had increased in 13 (23.2%), decreased in 7 (12.5%), and was unchanged in the remaining 36 (64.3) Outcomes, disease distribution was similar to patients who chose surgery at outset of study 43 Ito et al, Thyroid 13, 4, 2003
44 Lymph node dissection results Surgical group Total thyroidectomy in 44%, lobectomy in remainder Central compartment dissection in 594 (95%) Lateral neck dissection in 51% Performed Positive Central neck 594 (50.5%) 258 (43.4%) Lateral neck (44.5) * * of 141 patients with lateral neck nodes, metastases had been suspected by preoperative US in only 55 (39%) 44 Ito et al, Thyroid 13, 4, 2003
45 45
46 46

47 47 JAMA Otolaryngology Head & Neck Surgery October , 10
48 12.7% 48 JAMA Otolaryngology Head & Neck Surgery October , 10
49 Extent of thyroidectomy: Recommendation 35 (C) If surgery is chosen for patients with thyroid cancer <1 cm without extrathyroidal extension and cn0, the initial surgical procedure should be a thyroid lobectomy unless there are clear indications to remove the contralateral lobe. Thyroid lobectomy alone is sufficient treatment for small, unifocal, intrathyroidal carcinomas in the absence of prior head and neck radiation, familial thyroid carcinoma, or clinically detectable cervical nodal metastases. (Strong recommendation, Moderate-quality evidence) ATA Guidelines, Thyroid, 26, 1, 2016
50 3 WHEN IS LOBECTOMY ALONE VS TOTAL THYROIDECTOMY WARRANTED? 50

51 How to choose: Lobe vs. TTX Benign disease ATUS/FN Cancer 51
52 Total vs. lobe: Considerations in Benign disease Consider R neck separately from left neck Unilateral vs bilateral nodules How confident are we in FNA? How resistant is the patient to ongoing surveillance? Symptoms are they lateralizable? Bilateral? Risk: How challenging is the operation predicted to be? 52
53 Total vs. lobe example case 46 YO F, no risk factors for thyroid cancer, found to have large thyroid nodule during evaluation for dysphagia. US: R 2.2 cm complex nodule, left 3.6 cm solid nodule TSH 1.4, FNA of dominant nodule benign. Options discussed: Expectant management (+/- FNA of the right nodule) Left lobectomy (after FNA of right nodule) Total thyroidectomy 53
54 Total vs. lobe example case #2 68 YO F, no risk factors for thyroid cancer, found to have 12 cm substernal goiter on evaluation for incidental mediastinal mass. Asymptomatic. Pemberton s negative US: R 3.5 cm solid nodule, left large substernal goiter TSH 1.4, FNA of dominant nodule benign. Options discussed: Expectant management (+/- FNA of the right nodule) Left substernal lobectomy (after FNA of right nodule) Total thyroidectomy 54
55 UNILATERAL BENIGN MNG VS SN: CONTRALATERAL RECURRENCE RATES AFTER LOBECTOMY (AAES, 2018) Retrospective of 2,675 lobectomies for MNG or SN 1991 to 2017 : 852 (31.85%) for MNG, and 1,823 (68.15%) for SN 394 (15%) underwent reoperation: 261 (30.6%) with MNG 133 (7.29%) with SN (p<0.0001). 85% of recurrences were as MNG, 3.5% as carcinomas. 55
56 UNILATERAL BENIGN MNG VS SN: CONTRALATERAL RECURRENCE RATES AFTER LOBECTOMY (AAES, 2018) Mean time to recurrence was 14.8 years, no difference between groups Patients with no recurrence were younger (47+15 vs 54+13, p<0.0001) Male patients were less likely to recur, p< Conclusions: Although recurrence rates for MNG compared to SN are higher (30.6% vs 7.29%), lobectomy for unilateral MNG is reasonable and can be regarded as the procedure of choice given the long time to recurrence requiring completion thyroidectomy. 56
57 Lobectomy vs. Total in IDN/DTC Benefits: PTC is often multifocal Questionable relevance Enables 131 I treatment Enhances sensitivity of TG Enables thyroid scanning Often not needed 57
58 Lobectomy vs. Total in IDN/DTC Benefits: PTC is often multifocal Enables 131 I treatment Enhances sensitivity of TG Enables thyroid scanning Risks: Bilateral RLN palsy Hypoparathyroidism Lifelong LT4 requirement High chance of unnecessary surgery 58
59 Patient perspective 59
60 TTX vs. Lobectomy - IDN Marries considerations of patients with known benign nodules who require surgery and those of patients with known thyroid cancer AUS: Are abnormalities architectural or nuclear? Were molecular analytics performed? Do they have sufficient potential to influence the patient s decision making? If IDN proves to be a cancer, how likely is it that radioiodine will be required? Size Likelihood of ETE 60
61 Operative choice in IDN useful considerations How would you react/respond to the idea of having to return to the OR for completion thyroidectomy Knowledge that it is often not as complete as upfront total thyroidectomy If you chose total thyroidectomy, and the pathology report showed no cancer, would you be happy with the diagnosis, or upset with your choice of operation? 61

62 25 year risk of death among 52,117 patients with localized (<2 cm) PTC treated by either lobectomy or total thyroidectomy 62 NEJM 379;4.July 26, 2018

63 63 NEJM 379;4 July 26, 2018
64 Lobectomy vs. total in small PTCconsiderations Contralateral pathology? Requirement for RAI postop? Lymph nodes ETE Aggressive subtype of PTC Surgeon / endocrinologist comfort in doing less 64

65 Extent of thyroidectomy: Recommendation 35 ATA Guidelines, Thyroid, 26, 1, 2016


66 Extent of thyroidectomy: Recommendation 35 ATA Guidelines, Thyroid, 26, 1, 2016
67 ATA Rec 51: Who needs RAI? 67 ATA Guidelines Thyroid. 2016; 26:
68 ATA Rec 51: Who needs RAI? 68
69 Trends in management of DTC Major caveat Much of the evidence for less aggressive management comes from large Endocrine Surgery units with well oiled multidisciplinary teams including expert surgeons, endocrinologists, radiologists, and pathologists 69
70 70
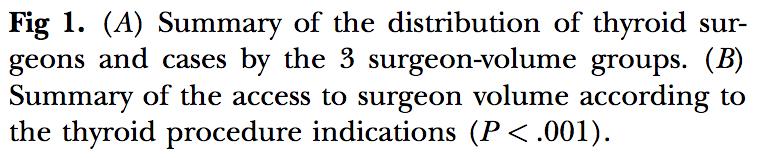
71 surgeon volume is associated with completeness of resection 71
72 Ann Surg 2017;265: ) National Inpatient Sample ( ) 16,954 patients undergoing total thyroidectomy: 47% had thyroid cancer and 53% benign disease Median annual surgeon volume was 7; 51% performed 1 case/y.
 16,954 patients undergoing total")

73 Ann Surg 2017;265: ) National Inpatient Sample ( ) 16,954 patients undergoing total thyroidectomy: 47% had thyroid cancer and 53% benign disease Median annual surgeon volume was 7; 51% performed 1 case/y.


74 6,261 total thyroidectomy patients 74 Surgery2013;154:
75 Volume- outcome relationship in thyroid surgery: Low surgeon volume is clearly associated with: Less complete resections Higher rates of complications Higher hospital charges 75
76 76
Gerard M. Doherty, MD
 Surgical Management of Differentiated Thyroid Cancer: Update on 2015 ATA Guidelines Gerard M. Doherty, MD Chair of Surgery Utley Professor of Surgery and Medicine Boston University Surgeon-in-Chief Boston
Surgical Management of Differentiated Thyroid Cancer: Update on 2015 ATA Guidelines Gerard M. Doherty, MD Chair of Surgery Utley Professor of Surgery and Medicine Boston University Surgeon-in-Chief Boston
Current Issues in Thyroid Cancer Surgery in 2017
 Current Issues in Thyroid Cancer Surgery in 2017 Dr. David Goldstein MD Msc FRCSC FACS Associate Professor, Department Otolaryngology Head & Neck Surgery, U of T Department of Surgical Oncology, Princess
Current Issues in Thyroid Cancer Surgery in 2017 Dr. David Goldstein MD Msc FRCSC FACS Associate Professor, Department Otolaryngology Head & Neck Surgery, U of T Department of Surgical Oncology, Princess
Ultrasound for Pre-operative Evaluation of Well Differentiated Thyroid Cancer
 Ultrasound for Pre-operative Evaluation of Well Differentiated Thyroid Cancer Its Not Just About the Nodes AACE Advances in Medical and Surgical Management of Thyroid Cancer - 2017 Robert A. Levine, MD,
Ultrasound for Pre-operative Evaluation of Well Differentiated Thyroid Cancer Its Not Just About the Nodes AACE Advances in Medical and Surgical Management of Thyroid Cancer - 2017 Robert A. Levine, MD,
Preoperative Evaluation
 Preoperative Evaluation Lateral compartment lymph nodes are easier to detect and are amenable to FNA Central compartment lymph nodes are much more difficult to detect and FNA (Tg washout testing is compromised)
Preoperative Evaluation Lateral compartment lymph nodes are easier to detect and are amenable to FNA Central compartment lymph nodes are much more difficult to detect and FNA (Tg washout testing is compromised)
How good are we at finding nodules? Thyroid Nodules Thyroid Cancer Epidemiology Initial management Long-term follow up Disease-free status
 New Perspectives in Thyroid Cancer Jennifer Sipos, MD Assistant Professor of Medicine Division of Endocrinology The Ohio State University Outline Thyroid Nodules Thyroid Cancer Epidemiology Initial management
New Perspectives in Thyroid Cancer Jennifer Sipos, MD Assistant Professor of Medicine Division of Endocrinology The Ohio State University Outline Thyroid Nodules Thyroid Cancer Epidemiology Initial management
Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer
 Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer AACE - Advances in Medical and Surgical Management of Thyroid Cancer - 2018 Robert A. Levine, MD, FACE, ECNU Thyroid Center of New Hampshire Geisel
Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer AACE - Advances in Medical and Surgical Management of Thyroid Cancer - 2018 Robert A. Levine, MD, FACE, ECNU Thyroid Center of New Hampshire Geisel
4/22/2010. Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey.
 Management of Differentiated Thyroid Cancer: Head Neck Surgeon Perspective Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey Thyroid gland Small endocrine gland:
Management of Differentiated Thyroid Cancer: Head Neck Surgeon Perspective Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey Thyroid gland Small endocrine gland:
Differentiated Thyroid Carcinoma
 Differentiated Thyroid Carcinoma The GOOD cancer? Jennifer Sipos, MD Associate Professor of Medicine Director, Benign Thyroid Program Division of Endocrinology, Diabetes and Metabolism The Ohio State University
Differentiated Thyroid Carcinoma The GOOD cancer? Jennifer Sipos, MD Associate Professor of Medicine Director, Benign Thyroid Program Division of Endocrinology, Diabetes and Metabolism The Ohio State University
2015 American Thyroid Association Thyroid Nodule and Cancer Guidelines
 2015 American Thyroid Association Thyroid Nodule and Cancer Guidelines Angela M. Leung, MD, MSc, ECNU November 5, 2016 Outline Workup of nontoxic thyroid nodule(s) Ultrasound FNAB Management of FNAB results
2015 American Thyroid Association Thyroid Nodule and Cancer Guidelines Angela M. Leung, MD, MSc, ECNU November 5, 2016 Outline Workup of nontoxic thyroid nodule(s) Ultrasound FNAB Management of FNAB results
PEDIATRIC Ariel Katz MD
 PEDIATRIC Ariel Katz MD Dept. Otolaryngology Head &Neck Surgery Wolfson Medical Center Holon, Israel OBJECTIVES Overview/Background Epidemiology/Etiology Intro to Guidelines Workup Treatment Follow-Up
PEDIATRIC Ariel Katz MD Dept. Otolaryngology Head &Neck Surgery Wolfson Medical Center Holon, Israel OBJECTIVES Overview/Background Epidemiology/Etiology Intro to Guidelines Workup Treatment Follow-Up
THYROID CANCER IN CHILDREN. Humberto Lugo-Vicente MD FACS FAAP Professor Pediatric Surgery UPR School of Medicine
 THYROID CANCER IN CHILDREN Humberto Lugo-Vicente MD FACS FAAP Professor Pediatric Surgery UPR School of Medicine Thyroid nodules Rare Female predominance 4-fold as likely to be malignant Hx Radiation exposure?
THYROID CANCER IN CHILDREN Humberto Lugo-Vicente MD FACS FAAP Professor Pediatric Surgery UPR School of Medicine Thyroid nodules Rare Female predominance 4-fold as likely to be malignant Hx Radiation exposure?
Approach to Thyroid Nodules
 Approach to Thyroid Nodules Alice Y.Y. Cheng, MD, FRCPC Twitter: @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
Approach to Thyroid Nodules Alice Y.Y. Cheng, MD, FRCPC Twitter: @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
Thyroid Cancer: When to Treat? MEGAN R. HAYMART, MD
 Thyroid Cancer: When to Treat? MEGAN R. HAYMART, MD ASSOCIATE PROFESSOR OF MEDICINE UNIVERSITY OF MICHIGAN MICHIGAN AACE 2018 ANNUAL MEETING Thyroid Cancer: When Not to Treat? FOCUS WILL BE ON LOW-RISK
Thyroid Cancer: When to Treat? MEGAN R. HAYMART, MD ASSOCIATE PROFESSOR OF MEDICINE UNIVERSITY OF MICHIGAN MICHIGAN AACE 2018 ANNUAL MEETING Thyroid Cancer: When Not to Treat? FOCUS WILL BE ON LOW-RISK
5/3/2017. Ahn et al N Engl J Med 2014; 371
 Alan Failor, M.D. Clinical Professor of Medicine Division of Metabolism, Endocrinology and Nutrition University of Washington April 20, 2017 No disclosures to report 1. Appropriately evaluate s in adult
Alan Failor, M.D. Clinical Professor of Medicine Division of Metabolism, Endocrinology and Nutrition University of Washington April 20, 2017 No disclosures to report 1. Appropriately evaluate s in adult
WTC 2013 Panel Discussion: Minimal disease
 WTC 2013 Panel Discussion: Minimal disease Susan J. Mandel MD MPH Panelists Ken Ain Yasuhiro Ito Stephanie Lee Erich Sturgis Mark Urken Faculty/Presenter Disclosure Relationships with commercial interests
WTC 2013 Panel Discussion: Minimal disease Susan J. Mandel MD MPH Panelists Ken Ain Yasuhiro Ito Stephanie Lee Erich Sturgis Mark Urken Faculty/Presenter Disclosure Relationships with commercial interests
Thyroid nodules. Most thyroid nodules are benign
 Thyroid nodules Postgraduate Course in General Surgery Jessica E. Gosnell MD Assistant Professor March 22, 2011 Most thyroid nodules are benign thyroid nodules occur in 77% of the world s population palpable
Thyroid nodules Postgraduate Course in General Surgery Jessica E. Gosnell MD Assistant Professor March 22, 2011 Most thyroid nodules are benign thyroid nodules occur in 77% of the world s population palpable
Disclosures Nodal Management in Differentiated Thyroid Carcinoma
 Disclosures Nodal Management in Differentiated Thyroid Carcinoma Nothing to disclose Jonathan George, MD, MPH Assistant Professor UCSF Head and Neck Oncologic & Endocrine Surgery Objectives Overview Describe
Disclosures Nodal Management in Differentiated Thyroid Carcinoma Nothing to disclose Jonathan George, MD, MPH Assistant Professor UCSF Head and Neck Oncologic & Endocrine Surgery Objectives Overview Describe
Differentiated Thyroid Cancer: Initial Management
 Page 1 ATA HOME GIVE ONLINE ABOUT THE ATA JOIN THE ATA MEMBER SIGN-IN INFORMATION FOR PATIENTS FIND A THYROID SPECIALIST Home Management Guidelines for Patients with Thyroid Nodules and Differentiated
Page 1 ATA HOME GIVE ONLINE ABOUT THE ATA JOIN THE ATA MEMBER SIGN-IN INFORMATION FOR PATIENTS FIND A THYROID SPECIALIST Home Management Guidelines for Patients with Thyroid Nodules and Differentiated
Persistent & Recurrent Differentiated Thyroid Cancer
 Persistent & Recurrent Differentiated Thyroid Cancer Electron Kebebew University of California, San Francisco Department of Surgery Objectives Risk factors for persistent & recurrent disease Causes of
Persistent & Recurrent Differentiated Thyroid Cancer Electron Kebebew University of California, San Francisco Department of Surgery Objectives Risk factors for persistent & recurrent disease Causes of
Thyroid Nodule. Disclosure. Learning Objectives P A P A P A 3/18/2014. Nothing to disclose.
 Thyroid Nodule Evaluating the patient with a thyroid nodule and some management options. Miguel V. Valdez PA C Disclosure Nothing to disclose. Learning Objectives Examination of thyroid gland Options for
Thyroid Nodule Evaluating the patient with a thyroid nodule and some management options. Miguel V. Valdez PA C Disclosure Nothing to disclose. Learning Objectives Examination of thyroid gland Options for
Reoperative central neck surgery
 Reoperative central neck surgery R. Pandev, I. Tersiev, M. Belitova, A. Kouizi, D. Damyanov University Clinic of Surgery, Section Endocrine Surgery University Hospital Queen Johanna ISUL Medical University
Reoperative central neck surgery R. Pandev, I. Tersiev, M. Belitova, A. Kouizi, D. Damyanov University Clinic of Surgery, Section Endocrine Surgery University Hospital Queen Johanna ISUL Medical University
Thyroid nodules - medical and surgical management. Endocrinology and Endocrine Surgery Manchester Royal Infirmary
 Thyroid nodules - medical and surgical management JRE Davis NR Parrott Endocrinology and Endocrine Surgery Manchester Royal Infirmary Thyroid nodules - prevalence Thyroid nodules common, increase with
Thyroid nodules - medical and surgical management JRE Davis NR Parrott Endocrinology and Endocrine Surgery Manchester Royal Infirmary Thyroid nodules - prevalence Thyroid nodules common, increase with
Dynamic Risk Stratification:
 Dynamic Risk Stratification: Using Risk Estimates to Guide Initial Management R Michael Tuttle, MD Clinical Director, Endocrinology Service Memorial Sloan Kettering Cancer Center Professor of Medicine
Dynamic Risk Stratification: Using Risk Estimates to Guide Initial Management R Michael Tuttle, MD Clinical Director, Endocrinology Service Memorial Sloan Kettering Cancer Center Professor of Medicine
AACE Thyroid Cancer Tumor board 25 years of the Endocrine and Surgery collaboration
 AACE Thyroid Cancer Tumor board 25 years of the Endocrine and Surgery collaboration Dr. Peter Singer, Endocrinology Dr. Peter Sadow, Pathology Moderator Dr. Greg Randolph, Otolaryngology Relevant Financial
AACE Thyroid Cancer Tumor board 25 years of the Endocrine and Surgery collaboration Dr. Peter Singer, Endocrinology Dr. Peter Sadow, Pathology Moderator Dr. Greg Randolph, Otolaryngology Relevant Financial
Minimalistic Initial Therapy Options For Low Risk Papillary Thyroid Cancer
 Minimalistic Initial Therapy Options For Low Risk Papillary Thyroid Cancer An emphasis on proper patient selection R Michael Tuttle, MD Clinical Director, Endocrinology Service Memorial Sloan Kettering
Minimalistic Initial Therapy Options For Low Risk Papillary Thyroid Cancer An emphasis on proper patient selection R Michael Tuttle, MD Clinical Director, Endocrinology Service Memorial Sloan Kettering
42 yr old male with h/o Graves disease and prior I 131 treatment presents with hyperthyroidism and undetectable TSH. 2 hr uptake 20%, 24 hr uptake 50%
 Pinhole images of the neck are acquired in multiple projections, 24hrs after the oral administration of approximately 200 µci of I123. Usually, 24hr uptake value if also calculated (normal 24 hr uptake
Pinhole images of the neck are acquired in multiple projections, 24hrs after the oral administration of approximately 200 µci of I123. Usually, 24hr uptake value if also calculated (normal 24 hr uptake
Thyroid US. Background: Thyroid/Neck US. Use of Office Ultrasound in the Thyroid Surgery Practice
 2010 UCSF Head and Neck Endocrine Surgery Course Use of Office Ultrasound in the Thyroid Surgery Practice Lisa A. Orloff, MD FACS Dept of Otolaryngology-Head and Neck Surgery University of California,
2010 UCSF Head and Neck Endocrine Surgery Course Use of Office Ultrasound in the Thyroid Surgery Practice Lisa A. Orloff, MD FACS Dept of Otolaryngology-Head and Neck Surgery University of California,
Risk Adapted Follow-Up
 Risk Adapted Follow-Up Individualizing Follow- Up Strategies R Michael Tuttle, MD Clinical Director, Endocrinology Service Memorial Sloan Kettering Cancer Center Professor of Medicine Weill Medical College
Risk Adapted Follow-Up Individualizing Follow- Up Strategies R Michael Tuttle, MD Clinical Director, Endocrinology Service Memorial Sloan Kettering Cancer Center Professor of Medicine Weill Medical College
Long Term Follow-Up for Differentiated Thyroid Cancer: The Mayo Experience
 Long Term Follow-Up for Differentiated Thyroid Cancer: The Mayo Experience Geoffrey B. Thompson, MD Professor of Surgery College of Medicine, Mayo Clinic Differentiated Thyroid Cancer Objectives Overview
Long Term Follow-Up for Differentiated Thyroid Cancer: The Mayo Experience Geoffrey B. Thompson, MD Professor of Surgery College of Medicine, Mayo Clinic Differentiated Thyroid Cancer Objectives Overview
5/18/2013. Most thyroid nodules are benign. Thyroid nodules: new techniques in evaluation
 Most thyroid nodules are benign Thyroid nodules: new techniques in evaluation Incidence Etiology Risk factors Diagnosis Gene classification system Treatment Postgraduate Course in General Surgery Jessica
Most thyroid nodules are benign Thyroid nodules: new techniques in evaluation Incidence Etiology Risk factors Diagnosis Gene classification system Treatment Postgraduate Course in General Surgery Jessica
Thyroid nodules 3/22/2011. Most thyroid nodules are benign. Thyroid nodules: differential diagnosis
 Most thyroid nodules are benign Thyroid nodules Postgraduate Course in General Surgery thyroid nodules occur in 77% of the world s population palpable thyroid nodules occur in about 5% of women and 1%
Most thyroid nodules are benign Thyroid nodules Postgraduate Course in General Surgery thyroid nodules occur in 77% of the world s population palpable thyroid nodules occur in about 5% of women and 1%
Objectives. How to Investigate Thyroid Nodules like A Pro
 How to Investigate Thyroid Nodules like A Pro Chris Sadler, MA, PA C, CDE, DFAAPA Medical Science Outcomes Liaison Intarcia Diabetes and Endocrine Associates La Jolla, CA Past President ASEPA Disclosures
How to Investigate Thyroid Nodules like A Pro Chris Sadler, MA, PA C, CDE, DFAAPA Medical Science Outcomes Liaison Intarcia Diabetes and Endocrine Associates La Jolla, CA Past President ASEPA Disclosures
Surgical Treatment for Papillary Thyroid Carcinoma in Japan: Differences from Other Countries
 REVIEW ARTICLE J Korean Thyroid Assoc Vol. 4, No. 2, November 2011 Surgical Treatment for Papillary Thyroid Carcinoma in Japan: Differences from Other Countries Yasuhiro Ito, MD and Akira Miyauchi, MD
REVIEW ARTICLE J Korean Thyroid Assoc Vol. 4, No. 2, November 2011 Surgical Treatment for Papillary Thyroid Carcinoma in Japan: Differences from Other Countries Yasuhiro Ito, MD and Akira Miyauchi, MD
How Will (Should) the Latest Guidelines Affect the Endocrinologist s Management of Thyroid Cancer? AACE 2017
 the Latest Guidelines Affect the Endocrinologist s Management of Thyroid Cancer? AACE 2017") How Will (Should) the Latest Guidelines Affect the Endocrinologist s Management of Thyroid Cancer? AACE 2017 Bryan R. Haugen, MD University of Colorado, School of Medicine Outline Some statistics New guidelines
How Will (Should) the Latest Guidelines Affect the Endocrinologist s Management of Thyroid Cancer? AACE 2017 Bryan R. Haugen, MD University of Colorado, School of Medicine Outline Some statistics New guidelines
Objectives. 1)To recall thyroid nodule ultrasound characteristics that increase the risk of malignancy
To recall thyroid nodule ultrasound characteristics that increase the risk of malignancy") Evaluation and Management of Thyroid Nodules in Primary Care Chris Sadler, MA, PA C, CDE, DFAAPA Medical Science Outcomes Liaison Intarcia Diabetes and Endocrine Associates La Jolla, CA Past President
Evaluation and Management of Thyroid Nodules in Primary Care Chris Sadler, MA, PA C, CDE, DFAAPA Medical Science Outcomes Liaison Intarcia Diabetes and Endocrine Associates La Jolla, CA Past President
Long-term Follow-up for Patients with Papillary Thyroid Carcinoma Treated as Benign Nodules
 Long-term Follow-up for Patients with Papillary Thyroid Carcinoma Treated as Benign Nodules YASUHIRO ITO, TAKUYA HIGASHIYAMA, YUUKI TAKAMURA, AKIHIRO MIYA, KAORU KOBAYASHI, FUMIO MATSUZUKA, KANJI KUMA
Long-term Follow-up for Patients with Papillary Thyroid Carcinoma Treated as Benign Nodules YASUHIRO ITO, TAKUYA HIGASHIYAMA, YUUKI TAKAMURA, AKIHIRO MIYA, KAORU KOBAYASHI, FUMIO MATSUZUKA, KANJI KUMA
Pediatric Thyroid Cancer Lung Metastases. Liora Lazar MD
 Pediatric Thyroid Cancer Lung Metastases Liora Lazar MD Differentiated thyroid cancer (DTC) The 3rd most common solid tumor in childhood and adolescence Accounting for 1.5%-3% of all childhood cancers
Pediatric Thyroid Cancer Lung Metastases Liora Lazar MD Differentiated thyroid cancer (DTC) The 3rd most common solid tumor in childhood and adolescence Accounting for 1.5%-3% of all childhood cancers
Papillary Thyroid Microcarcinoma Presenting as Horner s Syndrome: A Novel Clinical Presentation
 Case Report American Journal of Cancer Case Reports http://ivyunion.org/index.php/ajccr/ Page 1 of 6 Papillary Thyroid Microcarcinoma Presenting as Horner s Syndrome: A Novel Clinical Presentation Ammara
Case Report American Journal of Cancer Case Reports http://ivyunion.org/index.php/ajccr/ Page 1 of 6 Papillary Thyroid Microcarcinoma Presenting as Horner s Syndrome: A Novel Clinical Presentation Ammara
Megan R. Haymart, MD 83 rd Annual Meeting of the ATA October 16, 2013
 Megan R. Haymart, MD 83 rd Annual Meeting of the ATA October 16, 2013 Disclosure: Nothing to Disclose Learning Objectives Thyroid cancer - diagnosis - prognosis - treatment - follow-up Thyroid function
Megan R. Haymart, MD 83 rd Annual Meeting of the ATA October 16, 2013 Disclosure: Nothing to Disclose Learning Objectives Thyroid cancer - diagnosis - prognosis - treatment - follow-up Thyroid function
Mandana Moosavi 1 and Stuart Kreisman Background
 Case Reports in Endocrinology Volume 2016, Article ID 6471081, 4 pages http://dx.doi.org/10.1155/2016/6471081 Case Report A Case Report of Dramatically Increased Thyroglobulin after Lymph Node Biopsy in
Case Reports in Endocrinology Volume 2016, Article ID 6471081, 4 pages http://dx.doi.org/10.1155/2016/6471081 Case Report A Case Report of Dramatically Increased Thyroglobulin after Lymph Node Biopsy in
Prophylactic Central Compartment Neck Dissection(CCND) for Papillary Thyroid Cancer: Con
 for Papillary Thyroid Cancer: Con") Prophylactic Central Compartment Neck Dissection(CCND) for Papillary Thyroid Cancer: Con Christopher R. McHenry, M.D. Vice Chairman Department of Surgery MetroHealth Medical Center Professor of Surgery
Prophylactic Central Compartment Neck Dissection(CCND) for Papillary Thyroid Cancer: Con Christopher R. McHenry, M.D. Vice Chairman Department of Surgery MetroHealth Medical Center Professor of Surgery
131-I Therapy Planning in Thyroid Cancer: The role of diagnostic radioiodine scans
 131-I Therapy Planning in Thyroid Cancer: The role of diagnostic radioiodine scans Anca M. Avram, M.D. Associate Professor of Radiology Department of Nuclear Medicine University of Michigan Ann Arbor,
131-I Therapy Planning in Thyroid Cancer: The role of diagnostic radioiodine scans Anca M. Avram, M.D. Associate Professor of Radiology Department of Nuclear Medicine University of Michigan Ann Arbor,
Initial surgery for differentiated thyroid cancer: What is the appropriate extent and attendant risks and benefits?
 Initial surgery for differentiated thyroid cancer: What is the appropriate extent and attendant risks and benefits? Julie Ann Sosa, MD MA FACS Professor of Surgery and Medicine Chief, Section of Endocrine
Initial surgery for differentiated thyroid cancer: What is the appropriate extent and attendant risks and benefits? Julie Ann Sosa, MD MA FACS Professor of Surgery and Medicine Chief, Section of Endocrine
10/24/2008. Surgery for Well-differentiated Thyroid Carcinoma- The Primary
 Surgery for Well-differentiated Thyroid Carcinoma- The Primary Head and Neck Endocrine Surgery Department of Otolaryngology-Head and Neck Surgery, UCSF October 24-25, 2008 Robert A. Sofferman, MD Professor
Surgery for Well-differentiated Thyroid Carcinoma- The Primary Head and Neck Endocrine Surgery Department of Otolaryngology-Head and Neck Surgery, UCSF October 24-25, 2008 Robert A. Sofferman, MD Professor
Strategies for detection of recurrent disease in longterm follow-up of differentiated thyroid cancer
 Strategies for detection of recurrent disease in longterm follow-up of differentiated thyroid cancer A rational approach to longterm follow-up based on dynamic risk assessment. World Congress on Thyroid
Strategies for detection of recurrent disease in longterm follow-up of differentiated thyroid cancer A rational approach to longterm follow-up based on dynamic risk assessment. World Congress on Thyroid
New York, the nation s thyroid gland. Christopher Morley ( ), "Shore Leave"
, Shore Leave") New York, the nation s thyroid gland Christopher Morley (1890-1957), "Shore Leave" Thyroid Literature Medline Thyroid disease 136,053 Thyroid tumors 33,554 New Paper on Thyroid Disease Every 3 Hours New
New York, the nation s thyroid gland Christopher Morley (1890-1957), "Shore Leave" Thyroid Literature Medline Thyroid disease 136,053 Thyroid tumors 33,554 New Paper on Thyroid Disease Every 3 Hours New
Thyroid Neoplasm. ORL-Head and neck Surgery 2014
 In The Name of God Thyroid Neoplasm ORL-Head and neck Surgery 2014 Malignant Neoplasm By age 90, virtually everyone has nodules Estimates of cancer prevalence at autopsy 4% to 36% Why these lesions are
In The Name of God Thyroid Neoplasm ORL-Head and neck Surgery 2014 Malignant Neoplasm By age 90, virtually everyone has nodules Estimates of cancer prevalence at autopsy 4% to 36% Why these lesions are
(Not so) New Guidelines for Management of Thyroid Nodules and Differentiated Thyroid Cancer Minnesota/Midwest Chapter of AACE
 New Guidelines for Management of Thyroid Nodules and Differentiated Thyroid Cancer Minnesota/Midwest Chapter of AACE") (Not so) New Guidelines for Management of Thyroid Nodules and Differentiated Thyroid Cancer Minnesota/Midwest Chapter of AACE Bryan R. Haugen, MD University of Colorado, School of Medicine Outline Some
(Not so) New Guidelines for Management of Thyroid Nodules and Differentiated Thyroid Cancer Minnesota/Midwest Chapter of AACE Bryan R. Haugen, MD University of Colorado, School of Medicine Outline Some
Thyroid Gland. Protocol applies to all malignant tumors of the thyroid gland, except lymphomas.
 Thyroid Gland Protocol applies to all malignant tumors of the thyroid gland, except lymphomas. Procedures Cytology (No Accompanying Checklist) Partial Thyroidectomy Total Thyroidectomy With/Without Lymph
Thyroid Gland Protocol applies to all malignant tumors of the thyroid gland, except lymphomas. Procedures Cytology (No Accompanying Checklist) Partial Thyroidectomy Total Thyroidectomy With/Without Lymph
Management of Thyroid Nodules. February 2 nd, 2018 Sarah Hopkins
 Management of Thyroid Nodules February 2 nd, 2018 Sarah Hopkins No disclosures Goals: Review Initial Evaluation of Thyroid Nodules Review Indications for Biopsy Approach to Multinodular Goiter Review Management
Management of Thyroid Nodules February 2 nd, 2018 Sarah Hopkins No disclosures Goals: Review Initial Evaluation of Thyroid Nodules Review Indications for Biopsy Approach to Multinodular Goiter Review Management
Disclosures. Learning objectives. Case 1A. Autoimmune Thyroid Disease: Medical and Surgical Issues. I have nothing to disclose.
 Disclosures Autoimmune Thyroid Disease: Medical and Surgical Issues I have nothing to disclose. Chrysoula Dosiou, MD, MS Clinical Assistant Professor Division of Endocrinology Stanford University School
Disclosures Autoimmune Thyroid Disease: Medical and Surgical Issues I have nothing to disclose. Chrysoula Dosiou, MD, MS Clinical Assistant Professor Division of Endocrinology Stanford University School
CAP Cancer Protocol and ecc Summary of Changes for August 2014 Thyroid Agile Release
 CAP Cancer Protocol and ecc Summary of Changes for August 2014 Thyroid Agile Release 2 REVISION HISTORY Date Author / Editor Comments 5/19/2014 Jaleh Mirza Created the document 8/12/2014 Samantha Spencer/Jaleh
CAP Cancer Protocol and ecc Summary of Changes for August 2014 Thyroid Agile Release 2 REVISION HISTORY Date Author / Editor Comments 5/19/2014 Jaleh Mirza Created the document 8/12/2014 Samantha Spencer/Jaleh
Review Article Management of thyroid carcinoma Alauddin M, Joarder AH
 Management of thyroid carcinoma Alauddin M, Joarder AH The ORION Medical Journal 2004 May;18:163-166 Overview The two most common forms of thyroid cancer, papillaryand follicular thyroid cancer, together
Management of thyroid carcinoma Alauddin M, Joarder AH The ORION Medical Journal 2004 May;18:163-166 Overview The two most common forms of thyroid cancer, papillaryand follicular thyroid cancer, together
Thyroid Ultrasound for the Endocrine Surgeon: A Valuable Clinical Tool that Enhances Diagnostic and Therapeutic Outcomes
 Thyroid Ultrasound for the Endocrine Surgeon: A Valuable Clinical Tool that Enhances Diagnostic and Therapeutic Outcomes Allan Siperstein MD The Cleveland Clinic Audience Quiz Taken ultrasound course Perform
Thyroid Ultrasound for the Endocrine Surgeon: A Valuable Clinical Tool that Enhances Diagnostic and Therapeutic Outcomes Allan Siperstein MD The Cleveland Clinic Audience Quiz Taken ultrasound course Perform
40 TH EUROPEAN CONGRESS 0F CYTOLOGY LIVERPOOL, UK October 2-5, 2016
 Outcomes from the diagnostic approach of thyroid lesions using US-FNA and LBC in clinical practice Emmanouel Mastorakis MD PhD Cytopathologist Director in Cytopathology Laboratory Regional General Hospital
Outcomes from the diagnostic approach of thyroid lesions using US-FNA and LBC in clinical practice Emmanouel Mastorakis MD PhD Cytopathologist Director in Cytopathology Laboratory Regional General Hospital
Women s Health in General Practice Symposium 2015 Thyroid & Parathyroid Cases
 Women s Health in General Practice Symposium 2015 Thyroid & Parathyroid Cases Bill Fleming Epworth Freemasons Hospital 1 Common Endocrine Presentations anatomical problems thyroid nodule / goitre embryological
Women s Health in General Practice Symposium 2015 Thyroid & Parathyroid Cases Bill Fleming Epworth Freemasons Hospital 1 Common Endocrine Presentations anatomical problems thyroid nodule / goitre embryological
Thyroid Nodules. Family Medicine Refresher Course Geeta Lal MD, FACS April 2, No financial disclosures
 Thyroid Nodules Family Medicine Refresher Course Geeta Lal MD, FACS April 2, 2014 No financial disclosures Objectives Review epidemiology Work up of Thyroid nodules Indications for FNAB Evolving role of
Thyroid Nodules Family Medicine Refresher Course Geeta Lal MD, FACS April 2, 2014 No financial disclosures Objectives Review epidemiology Work up of Thyroid nodules Indications for FNAB Evolving role of
The International Federation of Head and Neck Oncologic Societies. Current Concepts in Head and Neck Surgery and Oncology
 The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
Case-Based Discussion of Thyroid Cancer Therapy
 Case-Based Discussion of Thyroid Cancer Therapy Matthew D. Ringel, MD Ralph W. Kurtz Chair and Professor of Medicine Director, Division of Endocrinology The Ohio State University Co-Leader, Molecular Biology
Case-Based Discussion of Thyroid Cancer Therapy Matthew D. Ringel, MD Ralph W. Kurtz Chair and Professor of Medicine Director, Division of Endocrinology The Ohio State University Co-Leader, Molecular Biology
I-131 ABLATION AND ADJUVANT THERAPY OF THYROID CANCER
 AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGISTS Advances in Medical and Surgical Management of Thyroid Cancer January 23-24, 2015 I-131 ABLATION AND ADJUVANT THERAPY OF THYROID CANCER 2015 Leonard Wartofsky,
AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGISTS Advances in Medical and Surgical Management of Thyroid Cancer January 23-24, 2015 I-131 ABLATION AND ADJUVANT THERAPY OF THYROID CANCER 2015 Leonard Wartofsky,
AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS
 AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS PAPILLARY THYROID CARCINOMA Clinical Any age Microscopic to large Female: Male= 2-4:1 Radiation history Lymph nodes Prognosis
AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS PAPILLARY THYROID CARCINOMA Clinical Any age Microscopic to large Female: Male= 2-4:1 Radiation history Lymph nodes Prognosis
Management of Recurrent Thyroid Cancer
 Management of Recurrent Thyroid Cancer Eric Genden, MD, MHA Isidore Professor and Chairman Department of Otolaryngology- Head and Neck Surgery Senior Associate Dean for Clinical Affairs The Icahn School
Management of Recurrent Thyroid Cancer Eric Genden, MD, MHA Isidore Professor and Chairman Department of Otolaryngology- Head and Neck Surgery Senior Associate Dean for Clinical Affairs The Icahn School
Oh, I get it, the TSH goes up and down
 Evaluation and Management of the Thyroid Nodule Oh, I get it, the TSH goes up and down UCSF Head and Neck Conference October 24, 2008 Peter A. Singer, M.D. Professor and Chief Clinical Endocrinology University
Evaluation and Management of the Thyroid Nodule Oh, I get it, the TSH goes up and down UCSF Head and Neck Conference October 24, 2008 Peter A. Singer, M.D. Professor and Chief Clinical Endocrinology University
- RET/PTC rearrangement: 20% papillary thyroid cancer - RET: medullary thyroid cancer
 Thyroid Cancer UpToDate: Introduction: Risk Factors: Biology: Symptoms: Diagnosis: 1. Lenvina is the first line therapy with powerful durable response and superior PFS in pts with RAI-refractory disease.
Thyroid Cancer UpToDate: Introduction: Risk Factors: Biology: Symptoms: Diagnosis: 1. Lenvina is the first line therapy with powerful durable response and superior PFS in pts with RAI-refractory disease.
34 year-old Female with Thyroid Cancer
 34 year-old Female with Thyroid Cancer KATIE O SULLIVAN, MD FELLOW, ADULT/PEDIATRIC ENDOCRINOLOGY UNIVERSITY OF CHICAGO ENDORAMA THURSDAY, SEPTEMBER 15 TH, 2016 Disclosures: I do not have any relevant
34 year-old Female with Thyroid Cancer KATIE O SULLIVAN, MD FELLOW, ADULT/PEDIATRIC ENDOCRINOLOGY UNIVERSITY OF CHICAGO ENDORAMA THURSDAY, SEPTEMBER 15 TH, 2016 Disclosures: I do not have any relevant
Surgical Management of Thyroid Disease. Tom Shi Connally, MD, FACS
 Surgical Management of Thyroid Disease Tom Shi Connally, MD, FACS Disclosures Speaker Bureau: Veracyte Castle Diagnostics Objectives Understand the role of ultrasound and FNA in managing thyroid cancer
Surgical Management of Thyroid Disease Tom Shi Connally, MD, FACS Disclosures Speaker Bureau: Veracyte Castle Diagnostics Objectives Understand the role of ultrasound and FNA in managing thyroid cancer
Research Article Papillary Thyroid Cancer, Macrofollicular Variant: The Follow-Up and Analysis of Prognosis of 5 Patients
 yroid Research, Article ID 818134, 4 pages http://dx.doi.org/10.1155/2014/818134 Research Article Papillary Thyroid Cancer, Macrofollicular Variant: The Follow-Up and Analysis of Prognosis of 5 Patients
yroid Research, Article ID 818134, 4 pages http://dx.doi.org/10.1155/2014/818134 Research Article Papillary Thyroid Cancer, Macrofollicular Variant: The Follow-Up and Analysis of Prognosis of 5 Patients
What s an NIFTP? Keeping Up To Date in Thyroid 2018
 What s an NIFTP? Keeping Up To Date in Thyroid 2018 Kathleen Hands, MD, FACE, ECNU Director, Thyroid Center of South Texas Assistant Clinical Professor UTHSCSA DrHands@Thyroid-Center.com 210-844-6163 text
What s an NIFTP? Keeping Up To Date in Thyroid 2018 Kathleen Hands, MD, FACE, ECNU Director, Thyroid Center of South Texas Assistant Clinical Professor UTHSCSA DrHands@Thyroid-Center.com 210-844-6163 text
Exercise 15: CSv2 Data Item Coding Instructions ANSWERS
 Exercise 15: CSv2 Data Item Coding Instructions ANSWERS CS Tumor Size Tumor size is the diameter of the tumor, not the depth or thickness of the tumor. Chest x-ray shows 3.5 cm mass; the pathology report
Exercise 15: CSv2 Data Item Coding Instructions ANSWERS CS Tumor Size Tumor size is the diameter of the tumor, not the depth or thickness of the tumor. Chest x-ray shows 3.5 cm mass; the pathology report
Volume 2 Issue ISSN
 Volume 2 Issue 3 2012 ISSN 2250-0359 Correlation of fine needle aspiration and final histopathology in thyroid disease: a series of 702 patients managed in an endocrine surgical unit *Chandrasekaran Maharajan
Volume 2 Issue 3 2012 ISSN 2250-0359 Correlation of fine needle aspiration and final histopathology in thyroid disease: a series of 702 patients managed in an endocrine surgical unit *Chandrasekaran Maharajan
Sonographic Features of Thyroid Nodules & Guidelines for Management
 Sonographic Features of Thyroid Nodules & Guidelines for Management Mark A. Lupo, MD, FACE, ECNU Thyroid & Endocrine Center of Florida Assistant Clinical Professor of Medicine Florida State University,
Sonographic Features of Thyroid Nodules & Guidelines for Management Mark A. Lupo, MD, FACE, ECNU Thyroid & Endocrine Center of Florida Assistant Clinical Professor of Medicine Florida State University,
A variation in recurrence patterns of papillary thyroid cancer with disease progression: A long-term follow-up study
 ORIGINAL ARTICLE A variation in recurrence patterns of papillary thyroid cancer with disease progression: A long-term follow-up study Joon-Hyop Lee, MD, Yoo Seung Chung, MD, PhD,* Young Don Lee, MD, PhD
ORIGINAL ARTICLE A variation in recurrence patterns of papillary thyroid cancer with disease progression: A long-term follow-up study Joon-Hyop Lee, MD, Yoo Seung Chung, MD, PhD,* Young Don Lee, MD, PhD
Introduction. Materials and methods Y-N XU 1,2, J-D WANG 1,2
 1 di 5 11/04/2016 17:54 G Chir Vol. 31 - n. 5 - pp. 205-209 Maggio 2010 Y-N XU 1,2, J-D WANG 1,2 Introduction The World Health Organization (WHO) defined papillary thyroid microcarcinomas (PTMC) as tumors
1 di 5 11/04/2016 17:54 G Chir Vol. 31 - n. 5 - pp. 205-209 Maggio 2010 Y-N XU 1,2, J-D WANG 1,2 Introduction The World Health Organization (WHO) defined papillary thyroid microcarcinomas (PTMC) as tumors
PAPILLARY THYROID CARCINOMA PRESENTING AS A LATERAL NECK MASS MASS. Dr. Pamela Hanson DO PGY3
 PAPILLARY THYROID CARCINOMA PRESENTING AS A LATERAL NECK MASS MASS Dr. Pamela Hanson DO PGY3 MK CASE PRESENTATION 28 yo Female presented to the ENT Clinic in October 2016, with the complaint of chronic
PAPILLARY THYROID CARCINOMA PRESENTING AS A LATERAL NECK MASS MASS Dr. Pamela Hanson DO PGY3 MK CASE PRESENTATION 28 yo Female presented to the ENT Clinic in October 2016, with the complaint of chronic
Thyroid Nodules: What to do next?
 Thyroid Nodules: What to do next? Ally P. H. Prebtani Professor of Medicine Internal Medicine, Endocrinology & Metabolism McMaster University Canada Copyright 2017 by Sea Courses Inc. All rights reserved.
Thyroid Nodules: What to do next? Ally P. H. Prebtani Professor of Medicine Internal Medicine, Endocrinology & Metabolism McMaster University Canada Copyright 2017 by Sea Courses Inc. All rights reserved.
Thyroid Nodules. Dr. HAKIMI, SpAK Dr. MELDA DELIANA, SpAK Dr. SISKA MAYASARI LUBIS, SpA
 Thyroid Nodules ENDOCRINOLOGY DIVISION ENDOCRINOLOGY DIVISION Dr. HAKIMI, SpAK Dr. MELDA DELIANA, SpAK Dr. SISKA MAYASARI LUBIS, SpA Anatomical Considerations The Thyroid Nodule Congenital anomalies Thyroglossal
Thyroid Nodules ENDOCRINOLOGY DIVISION ENDOCRINOLOGY DIVISION Dr. HAKIMI, SpAK Dr. MELDA DELIANA, SpAK Dr. SISKA MAYASARI LUBIS, SpA Anatomical Considerations The Thyroid Nodule Congenital anomalies Thyroglossal
Evaluation of thyroid isthmusectomy as a potential treatment for papillary thyroid carcinoma limited to the isthmus: A clinical study of 73 patients
 ORIGINAL ARTICLE Evaluation of thyroid isthmusectomy as a potential treatment for papillary thyroid carcinoma limited to the isthmus: A clinical study of 73 patients Jianbiao Wang, MM, 1 Haili Sun, BM,
ORIGINAL ARTICLE Evaluation of thyroid isthmusectomy as a potential treatment for papillary thyroid carcinoma limited to the isthmus: A clinical study of 73 patients Jianbiao Wang, MM, 1 Haili Sun, BM,
Management guideline for patients with differentiated thyroid cancer. Teeraporn Ratanaanekchai ENT, KKU 17 October 2007
 Management guideline for patients with differentiated thyroid Teeraporn Ratanaanekchai ENT, KKU 17 October 2007 Incidence (Srinagarind Hospital, 2005, both sex) Site (all) cases % 1. Liver 1178 27 2. Lung
Management guideline for patients with differentiated thyroid Teeraporn Ratanaanekchai ENT, KKU 17 October 2007 Incidence (Srinagarind Hospital, 2005, both sex) Site (all) cases % 1. Liver 1178 27 2. Lung
Evaluation and Management of Thyroid Nodules. Overview of Thyroid Nodules and Their Management. Thyroid Nodule detection: U/S versus Exam
 Overview of Thyroid Nodules and Their Management Matthew D. Ringel, M.D. Professor of Medicine Divisions of Endocrinology and Oncology, The Ohio State University Co-Director, Thyroid Cancer Unit Arthur
Overview of Thyroid Nodules and Their Management Matthew D. Ringel, M.D. Professor of Medicine Divisions of Endocrinology and Oncology, The Ohio State University Co-Director, Thyroid Cancer Unit Arthur
Thyroid Nodules. Hossein Gharib, MD, MACP, MACE
 Thyroid Nodules Hossein Gharib, MD, MACP, MACE Professor of Medicine Mayo Clinic College of Medicine President Elect, American College of Endocrinology University Course January 2008 CP1294362-1 Thyroid
Thyroid Nodules Hossein Gharib, MD, MACP, MACE Professor of Medicine Mayo Clinic College of Medicine President Elect, American College of Endocrinology University Course January 2008 CP1294362-1 Thyroid
An Unexpected Cause of Hypoglycemia
 An Unexpected Cause of Hypoglycemia Stacey A. Milan, MD FACS Surgical Oncology Nothing to disclose Disclosures Objectives Identify indications for workup of hypoglycemia Define work up for hypoglycemic
An Unexpected Cause of Hypoglycemia Stacey A. Milan, MD FACS Surgical Oncology Nothing to disclose Disclosures Objectives Identify indications for workup of hypoglycemia Define work up for hypoglycemic
A Review of Differentiated Thyroid Cancer
 A Review of Differentiated Thyroid Cancer April 21 st, 2016 FPON Webcast Jonn Wu BMSc MD FRCPC Radiation Oncologist, Vancouver Centre Chair, Provincial H&N Tumour Group, BCCA Clinical Associate Professor,
A Review of Differentiated Thyroid Cancer April 21 st, 2016 FPON Webcast Jonn Wu BMSc MD FRCPC Radiation Oncologist, Vancouver Centre Chair, Provincial H&N Tumour Group, BCCA Clinical Associate Professor,
Distant and Lymph Node Metastases of Thyroid Nodules with No Pathological Evidence of Malignancy: A Limitation of Pathological Examination
 Endocrine Journal 2008, 55 (5), 889 894 Distant and Lymph Node Metastases of Thyroid Nodules with No Pathological Evidence of Malignancy: A Limitation of Pathological Examination YASUHIRO ITO, TOMONORI
Endocrine Journal 2008, 55 (5), 889 894 Distant and Lymph Node Metastases of Thyroid Nodules with No Pathological Evidence of Malignancy: A Limitation of Pathological Examination YASUHIRO ITO, TOMONORI
Imaging in Thyroid Cancer
 Imaging in Thyroid Cancer Susan J. Mandel MD MPH University of Pennsylvania School of Medicine Philadelphia, PA I-123 Ultrasound Background Radioiodine ablation of thyroid remnants after surgery is a generally
Imaging in Thyroid Cancer Susan J. Mandel MD MPH University of Pennsylvania School of Medicine Philadelphia, PA I-123 Ultrasound Background Radioiodine ablation of thyroid remnants after surgery is a generally
Thyroid Nodules. No conflicts. Overview 5/16/2017. UCSF Internal Medicine Updates May 22, 2017 Elizabeth Murphy, MD, DPhil
 Thyroid Nodules UCSF Internal Medicine Updates May 22, 2017 Elizabeth Murphy, MD, DPhil No conflicts Overview Thyroid nodule and cancer review Ultrasound FNA cytology Nodule follow up Putting it all together
Thyroid Nodules UCSF Internal Medicine Updates May 22, 2017 Elizabeth Murphy, MD, DPhil No conflicts Overview Thyroid nodule and cancer review Ultrasound FNA cytology Nodule follow up Putting it all together
TBSRTC 1- Probabilistic approach and Relationship to Clinical Algorithms
 The Benefits of a Uniform Reporting System for Thyroid Cytopathology BETHESDA REPORTING SYSTEM Prof. Fernando Schmitt Department of Pathology and Oncology, Medical Faculty of Porto University Head of Molecular
The Benefits of a Uniform Reporting System for Thyroid Cytopathology BETHESDA REPORTING SYSTEM Prof. Fernando Schmitt Department of Pathology and Oncology, Medical Faculty of Porto University Head of Molecular
Evaluation and Management of Thyroid Nodules. Nick Vernetti, MD, FACE Palm Medical Group Las Vegas, Nevada
 Evaluation and Management of Thyroid Nodules Nick Vernetti, MD, FACE Palm Medical Group Las Vegas, Nevada Disclosure Consulting Amgen Speaking Amgen Objectives Understand the significance of incidental
Evaluation and Management of Thyroid Nodules Nick Vernetti, MD, FACE Palm Medical Group Las Vegas, Nevada Disclosure Consulting Amgen Speaking Amgen Objectives Understand the significance of incidental
Managing Thyroid Microcarcinomas
 Review Article http://dx.doi.org/10.3349/ymj.2012.53.1.1 pissn: 0513-5796, eissn: 1976-2437 Yonsei Med J 53(1):1-14, 2012 Managing Thyroid Microcarcinomas Ernest L. Mazzaferri Division of Endocrinology,
Review Article http://dx.doi.org/10.3349/ymj.2012.53.1.1 pissn: 0513-5796, eissn: 1976-2437 Yonsei Med J 53(1):1-14, 2012 Managing Thyroid Microcarcinomas Ernest L. Mazzaferri Division of Endocrinology,
Dilemmas in Cytopathology and Histopathology
 Dilemmas in Cytopathology and Histopathology Yuri E. Nikiforov, MD, PhD Division of Molecular & Genomic Pathology University of Pittsburgh Medical Center, USA Objectives Discuss new WHO classification
Dilemmas in Cytopathology and Histopathology Yuri E. Nikiforov, MD, PhD Division of Molecular & Genomic Pathology University of Pittsburgh Medical Center, USA Objectives Discuss new WHO classification
New technologies in Endocrine Surgery
 New technologies in Endocrine Surgery 1. Nerve monitoring 2. New technologies in Endocrine Surgery Jessica E. Gosnell MD Post graduate course in General Surgery March 28, 2012 1 2 Recurrent laryngeal nerve
New technologies in Endocrine Surgery 1. Nerve monitoring 2. New technologies in Endocrine Surgery Jessica E. Gosnell MD Post graduate course in General Surgery March 28, 2012 1 2 Recurrent laryngeal nerve
3/29/2012. Thyroid cancer- what s new. Thyroid Cancer. Thyroid cancer is now the most rapidly increasing cancer in women
 Thyroid cancer- what s new Thyroid Cancer Changing epidemiology Molecular markers Lymph node dissection Technical advances rhtsh Genetic testing and prophylactic surgery Vandetanib What s new? Jessica
Thyroid cancer- what s new Thyroid Cancer Changing epidemiology Molecular markers Lymph node dissection Technical advances rhtsh Genetic testing and prophylactic surgery Vandetanib What s new? Jessica
Osman Ilkay Ozdamar, 1 Gul Ozbilen Acar, 1 Cigdem Kafkasli, 1 M. Tayyar Kalcioglu, 1 Tulay Zenginkinet, 2 and H. Gonca Tamer 3. 1.
 Case Reports in Otolaryngology Volume 2015, Article ID 79658, 4 pages http://dx.doi.org/10.1155/2015/79658 Case Report Papillary Thyroid Microcarcinoma with a Large Cystic Dilated Lymph Node Metastasis
Case Reports in Otolaryngology Volume 2015, Article ID 79658, 4 pages http://dx.doi.org/10.1155/2015/79658 Case Report Papillary Thyroid Microcarcinoma with a Large Cystic Dilated Lymph Node Metastasis
Work Up & Evaluation of Thyroid Nodules In 2013: State of The Art
 Work Up & Evaluation of Thyroid Nodules In 2013: State of The Art BC Surgical Oncology Network, Fall Update Todd McMullen MD PhD FRCSC FACS Endocrine Surgeon Divisions of General Surgery and Oncology Director,
Work Up & Evaluation of Thyroid Nodules In 2013: State of The Art BC Surgical Oncology Network, Fall Update Todd McMullen MD PhD FRCSC FACS Endocrine Surgeon Divisions of General Surgery and Oncology Director,
Case Scenario #1 Larynx
 Case Scenario #1 Larynx 56 year old white female who presented with a 2 month history of hoarseness treated with antibiotics, but with no improvement. In the last 3 weeks, she has had a 15 lb weight loss,
Case Scenario #1 Larynx 56 year old white female who presented with a 2 month history of hoarseness treated with antibiotics, but with no improvement. In the last 3 weeks, she has had a 15 lb weight loss,
USGFNA of thyroid nodules
 US Guided FNA (USGFNA) of neck masses INTERVENTIONAL HEAD & NECK ULTRASOUND Brendan C. Stack, Jr., MD., FACS, FACE Professor Otolaryngology-Head and Neck Surgery Indications Technique Interpretation Results
US Guided FNA (USGFNA) of neck masses INTERVENTIONAL HEAD & NECK ULTRASOUND Brendan C. Stack, Jr., MD., FACS, FACE Professor Otolaryngology-Head and Neck Surgery Indications Technique Interpretation Results
MTP: Thyroid Nodules
 Canadian Endocrine Update MTP: Thyroid Nodules Deric Morrison MD, FRCP, ECNU Assistant Professor, Division of Endocrinology and Metabolism, Western University April 2014 Faculty/Presenter Disclosure Faculty:
Canadian Endocrine Update MTP: Thyroid Nodules Deric Morrison MD, FRCP, ECNU Assistant Professor, Division of Endocrinology and Metabolism, Western University April 2014 Faculty/Presenter Disclosure Faculty:
Thyroid and Parathyroid Surgery
 Med 5 Surgery Refresher Course 2013 2014 Thyroid and Parathyroid Surgery Dr Shirley Liu Resident Specialist Honorary Clinical Assistant Professor Team 2 Surgery Prince of Wales Hospital Case scenario:
Med 5 Surgery Refresher Course 2013 2014 Thyroid and Parathyroid Surgery Dr Shirley Liu Resident Specialist Honorary Clinical Assistant Professor Team 2 Surgery Prince of Wales Hospital Case scenario:
 To the Patient and Family This booklet has been written for people who have received a diagnosis of thyroid cancer or who are being tested for this illness. If you have questions that are not answered
To the Patient and Family This booklet has been written for people who have received a diagnosis of thyroid cancer or who are being tested for this illness. If you have questions that are not answered
American Head and Neck Society - Journal Club Volume 22, July 2018
 - Table of Contents click the page number to go to the summary and full article link. Location and Causation of Residual Lymph Node Metastasis After Surgical Treatment of Regionally Advanced Differentiated
- Table of Contents click the page number to go to the summary and full article link. Location and Causation of Residual Lymph Node Metastasis After Surgical Treatment of Regionally Advanced Differentiated
PRACTICE GUIDELINES: Thyroid Nodules and Cancer 2017 ESEO Alexandria
 PRACTICE GUIDELINES: Thyroid Nodules and Cancer 2017 ESEO Alexandria James V. Hennessey MD Associate Professor of Medicine Harvard Medical School Case 1 28 year old woman sees OB for routine visit ROS:
PRACTICE GUIDELINES: Thyroid Nodules and Cancer 2017 ESEO Alexandria James V. Hennessey MD Associate Professor of Medicine Harvard Medical School Case 1 28 year old woman sees OB for routine visit ROS: