Long Term Follow-Up for Differentiated Thyroid Cancer: The Mayo Experience
|
|
|
- Mitchell Dalton
- 6 years ago
- Views:
Transcription
1 Long Term Follow-Up for Differentiated Thyroid Cancer: The Mayo Experience Geoffrey B. Thompson, MD Professor of Surgery College of Medicine, Mayo Clinic
2 Differentiated Thyroid Cancer Objectives Overview and When To Suspect Preoperative Evaluation Extent of Thyroidectomy Extent of Lymphadenectomy RAI TSH Suppression Special Cases
3 THYROID MALIGNANCIES Other Anaplastic FHCC Medullary Papillary
4 Cause-Specific Mortality Rates in FCDC ATC FTC 30 HCC PTC Years after initial treatment Dying of thyroid carcinoma (cumulative %)

5 Thyroid Cancer Incidence Incidence Rate per 100,000 Incidence Mortality Year Davies et al, JAMA 2006;195:2164
6 Thyroid Cancer Incidence Incidence Rate per 100,000 All Papillary Follicular Poorly Differentiated Year Davies et al, JAMA 2006;195:2164

7 Incidence Rate per 100, Thyroid Cancer Incidence cm cm cm > 5.0 cm Year Davies et al, JAMA 2006;195:2164
8 The Problem-Or Is It? 15% of Americans harbor thyroid Ca (45,000,000 people) 47,000 will be clinically detected this year (80 cases per million) 1,500 patients will die
9 Papillary Thyroid Cancer (PTC) Most common endocrine malignancy 80% of new cases worldwide Extent and type of therapy controversial No long-term prospective controlled trials
10 Surgery for PTC...Adjust(ing) the radicalness of therapy to the dangerousness of the cancer The punishment should fit the crime Cady Hayes Martin Lecture Society of Head and Neck Surgeons
11 Preoperative Evaluation Tier 1: History, Exam (US), FNA, TSH Tier 2: Nodal mapping (US), CXR, Vocal Cord Exam Tier 3: CT with contrast, Triple Endoscopy
12 Age < 20 years Male sex Thyroid Nodules Raised Suspicion History of head or neck irradiation Nodule > 4 cm Compressive symptoms including dysphagia, dysphonia, hoarseness, dyspnea, and cough
13 Thyroid Nodules High Suspicion Family history of MTC, MEN 2, PTC, Cowden s, FAP Rapid tumor growth, esp. on L-T4L Firm or hard nodule Fixed to adjacent structures Paralyzed vocal cord Regional lymphadenopathy Distant metastasis


14 Hypoechoic lesion plus one of the following: Microcalcifications Irregular border Central vascularity Taller rather than wide Ultrasound Suspicious Nodules Papini et al, JCEM 2002;87:1941
15 National Cancer Institute Thyroid Fine-Needle Aspiration State of Science Conference Benign Malignant NEW Suspicious for malignancy (risk 50-75%) NEW Follicular lesion of undetermined significance (risk 5-10%) 5 Nondiagnostic (7%) (<6 follicular groups with cells x2)
16 Nodules FNA Number Benign 12,480 (69.0%) Malignant 654 ( 3.5%) Suspicious 1,784 (10.0%) Non-Diagnostic 3,265 (21.0%) Total 18,183 Gharib and Goellner, 1983
17 Suspicious FNA 10 20% of FNA 15-75% are malignant
18 Needle Biopsy or FNA Non diagnostic : Malignant : Benign : Suspicious : Repeat with US Surgery Follow Surgery

19 Hot Nodule About 5% of nodules Almost always benign!
20 Preoperative Evaluation Tier 1: History, Exam (US), FNA, TSH Tier 2: Nodal mapping (US), CXR, Vocal Cord Exam Tier 3: CT with contrast, Triple Endoscopy


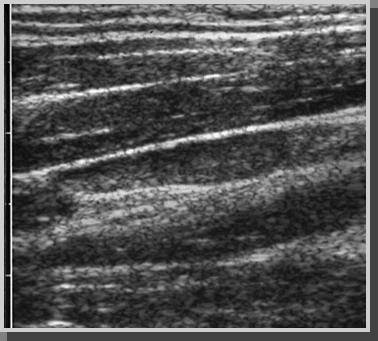
21 Benign Cervical Node Slender Fatty hilum Hilar blood flow


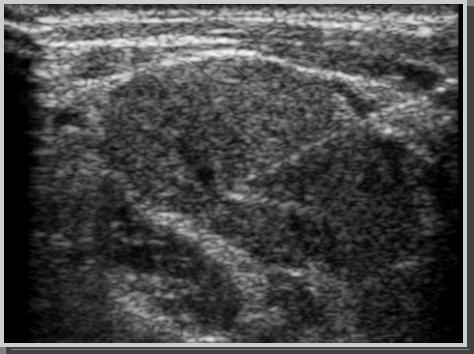
22 Cystic change Malignant Lymph Node


23 Malignant Neck Node 1cm Vascular indentation

24 Malignant Neck Node Calcifications


25 Malignant Neck Node Alteration in architecture and flow

26 Lymph Node Biopsy
27
28 Value of Preoperative Ultrasound in PTC Mayo Clinic: 770 pts ( ) US identified nonpalpable lateral nodes: 15% in first time operations Reops-NLLN NLLN s: 64% ; NCLN s: 28% US altered extent of operation in 41% of initial and 43% of reoperative pts. with palpable nodes Stulak et al. Arch of Surg, 2006



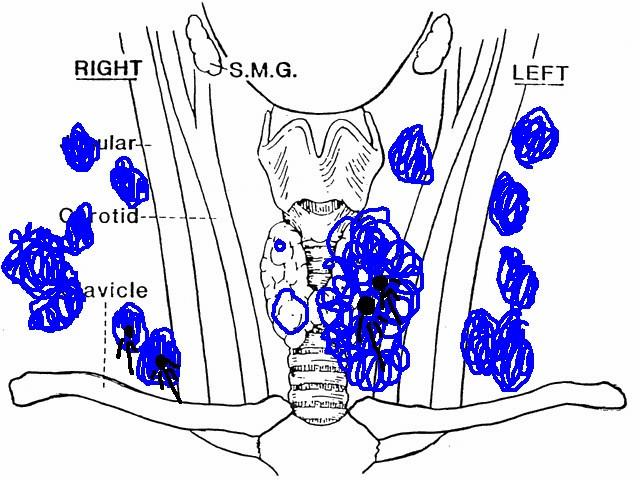
29 Metastatic PTC
30 Preoperative Evaluation Tier 1: History, Exam (US), FNA, TSH Tier 2: Nodal mapping (US), CXR, Vocal Cord Exam Tier 3: CT with contrast, Triple Endoscopy
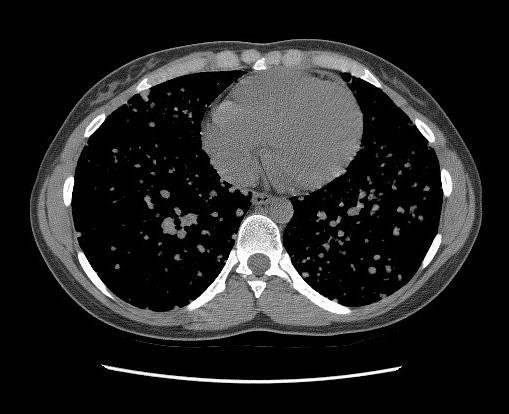
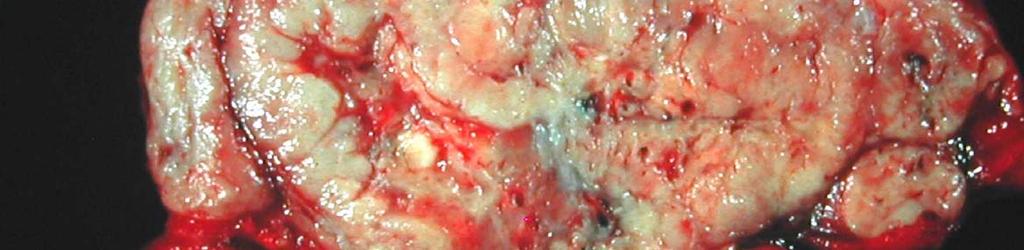
31 75 year old male with hoarseness 8cm grossly invasive FTC
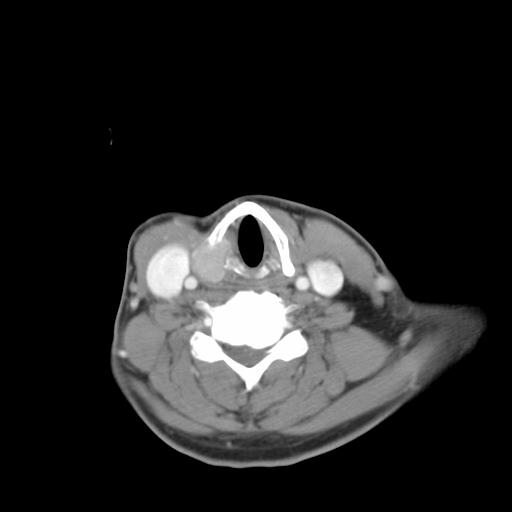
32




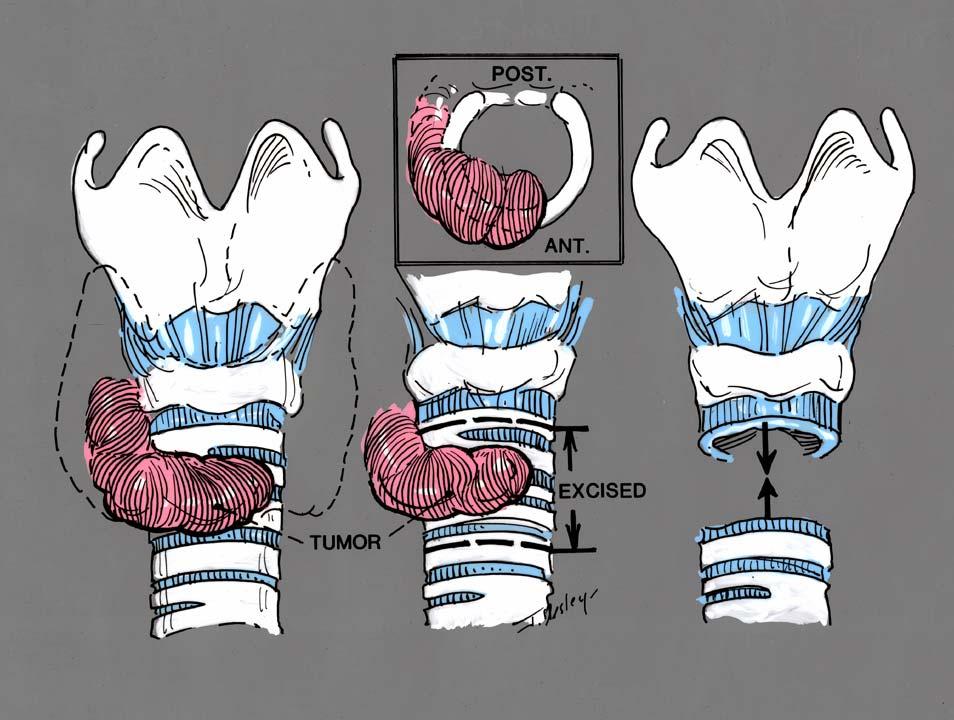
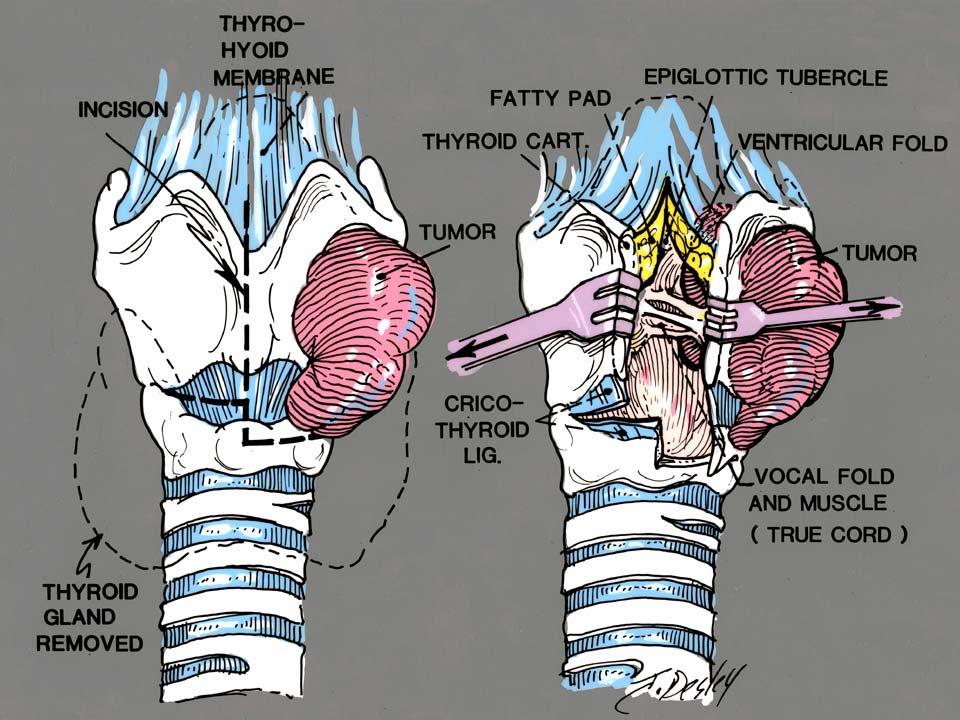
33 Stages of Tracheal Invasion in Thyroid Cancer Invasion of perichrondrium without infiltration of cartilage or soft tissue between cartilages Invasion of cartilage Invasion of lamina propria of tracheal mucosa Invasion of mucosa Grillo HC. Surgery of the trachea and Bronchi BC Decker Inc. Hamilton London Shin DH et al., Human Pathol 1993;24:
34
35
36
37
38 Thyroid Nodules Goals Treat thyroid cancer! Avoid unnecessary surgery! Select pts for appropriate adjuvant therapies
39 Staging and Risk Assessment- Determine Risk of Death/Recurrence Application of TSH suppression Application of remnant ablation with I-131 Application of Radioiodine Scanning and/or stimulated Tg testing
40 Papillary and Follicular Thyroid Cancer 1,355 patients (OSU, US Air Force) Median follow-up: 15.7 years 30 years: Survival 76% Recurrence 30% CSM 8% Mazzaferri EL. Am J Med 1994;97:418
41 Papillary and Follicular Thyroid Cancer Cancer death rate reduced by: female sex surgery more extensive than lobectomy 131 I plus thyroid hormone therapy Recurrence reduced to less than 1/3 with RRA vs T4 alone Mazzaferri EL. Am J Med 1994;97:418
42 Impact of I 131 on DTC Recurrence and Mortality Cum ulative m ortality Mazzaferri 1997 Cum ulative recurrence Years after initial therapy Years after initial therapy No Therapy T4-only I131 and T4 No Therapy T4-only I131 and T4 Mazzaferri et al 1997
43 Papillary Thyroid Cancer Is all of this true?


44 Risk Assessment in Thyroid Carcinoma 1.5mm Papillary microcancer

45 Risk Assessment in Thyroid Carcinoma 8cm grossly invasive FTC
46 ptnm Staging for FCDTC 2002 Classification I II 45 years TxNxM0 TxNxM1 45 years T1N0M0 T2N0M0 III IVA IVB IVC - T3N0M0 / T1-3N1aM0 - T4aNxM0 / T1-3N1bM0 - T4bNxM0 - TxNxM1 Greene et al 2003
47 PTC Survival by TNM Stage Surviving papillary thyroid carcinoma (%) n=2, P= Years after initial treatment TNM stage I 1,360 (60%) II 493 (22%) III 399 (17%) IV 32 (1%)
48 PTC Prognostic Factors Well-Established Independent Prognostic Factors Age Extrathyroidal tumor invasion Primary tumor size Distant metastases Incomplete tumor resection Less Certain Prognostic Factors Gender Lymph node metastases Tumor multicentricity Vascular invasion Morphologic variants of PTC* *tall cell, columnar cell, diffuse sclerosing Kebebew & Clark, 2001
49 Prognostic Schemes for DTC Age Sex Size Multicentricity Grade Histology Invasion Nodes Metastases Complete excision EORTC AGES AMES MACIS OSU SKMMC X X X X -- X -- X -- X -- X PTC X -- X -- X X X X X -- X -- X -- X PTC X -- X X X X X X X -- X -- X -- X X X X X --
50 Differentiated Thyroid Carcinoma Metastasis (distant) Age (at diagnosis) MACIS (PTC) Completeness of primary tumor resection Invasion of extrathyroidal structures Size (of primary tumor)
51 MACIS Prognostic Scoring System Score = 3.1 (if age = 39 yrs) or 0.08 X age (if age = 40 yrs) X tumor size (cm-max max diameter) + 1 (if incompletely resected) + 1 (if locally invasive) + 3 (distant spread)
52 Survival by MACIS 20 yrs <6 99% % % >8 24%
53 Papillary Thyroid Carcinoma Presenting Disease p TNM Stages MACIS Scores I (60%) <6 (84%) III (18%) II (21%) 6+ (16%) IV (1%) Hay et al, 2002 N = 2,
54 CSM from PTC in High- and Low-Risk Groups TNM, AGES, AMES, MACIS Dying of papillary carcinoma (cumulative %) TNM AMES III + IV (431) I + II (1,853) High (269) Low (2,015) AGES MACIS Years after initial treatment 4+ (322) <4 (1,962) 6+ (384) <6 (1,900)
55
56 Extent of Thyroidectomy (PTC) Recommendations American Thyroid Association Near-total or Total AACE Near-total or Total Society of Surgical Oncology Low Risk: Unilateral Lobectomy High Risk: Total thyroidectomy
57
58 Papillary Thyroid Cancer (PTC) Societal recommendations Bilobar resection (BLR) = Near total / Total thyroidectomy Radioiodine remnant ablation (RRA)
59 Papillary Thyroid Carcinoma Trends in Extent of Surgery & RRA Remnant ablation 80 Bilateral lobar resection (2,179) 80 n= Patients (%) n = 2,512 p< % 46% 20 0 Unilateral lobectomy (293) % 3% Hay et al, 2002
60 Papillary Thyroid Cancer (PTC) Why? (Multicentric Cancer) Improves cause-specific specific mortality (CSM) Reduces tumor recurrence (TR) Facilitates radioiodine scanning and use of therapeutic RAI Improves effectiveness of thyroglobulin (Tg) screening
61 Cause-Specific Survival by MACIS Score <6 (1,900 : 83%) (201 : 9%) Survival (%) n=2,284 P= MACIS score (75 : 3%) 8 8 (108 : 5%) Years after initial treatment
62 Cumulative % with occurrence Papillary Thyroid Carcinoma MACIS <6 N=296 P=0.31 Comparison of Outcome Mortality MACIS 6+ N=391 P=0.007 UL (160) BLR (136) UL (60) BLR (331) N=256 P<0.001 Recurrence N=280 P=0.015 Years After Initial Surgery UL (135) BLR (121) UL (29) BLR (241) Hay et al, 2002
63 PTC In low-risk patients: No survival benefit: : unilateral lobectomy vs bilobar resection Hay et al 1987 TR higher with unilateral procedure Grant et al 1988, Hay et al 1988
64 Risk of Locoregional Recurrence Unilateral Lobectomy 4x-7x higher compared to 20 years
65 Low-Risk DTC Patients: Limited Surgery? Local Recurrence Patient anxiety Physician anxiety Surgeon anxiety Need for reoperation Time away Cost
66 PTC In high-risk patients CSM and TR rates higher: : unilateral lobectomy vs BLR Hay et al 1987
67 Low-Risk DTC Patients: Limited Surgery? Total Thyroidectomy (Morbidity) The risk of permanent hypoparathyroidism is significantly greater than lesser resections in many series 3% vs Mayo Clinic (Total vs NT) Rates as high as 15-20% have been reported Hay et al. Surgery 1998; 124:
68 PTC Near-Total vs Total Thyroidectomy (BLR) No difference in CSM or TR in either low- or high-risk groups - Hay et al 1987
69 Papillary Thyroid Carcinoma Patients undergoing remnant ablation (%) Changing Frequency of Remnant Ablation Hay et al, 2002 RRA after BLR n = 1,423 p <
70 Papillary Thyroid Carcinoma Overall Outcome Occurrence (%) Mortality from PTC n = 2,512 Mayo Clinic Recurrence, any site n = 2, Years After Operation Hay et al, 2002
71 Papillary Thyroid Carcinoma Occurrence of postoperative events (cumulative %) Overall Outcome Postoperative nodes Local recurrences Distant metastases N = 2, Hay et al, 2002 Years After Initial Surgery
72 Papillary Thyroid Carcinoma Cause Specific Mortality 10-yr mortality from PTC (%) MACIS <6 N=1,835 P= MACIS 6+ N=339 P= Hay et al, 2002
73 Papillary Thyroid Carcinoma Tumor Recurrence 10-yr recurrence from PTC (%) MACIS <6 N=1,827 P= MACIS 6+ N=241 P= Hay et al, 2002
74 Radio-iodine iodine Remnant Ablation Routine Administration I-131 in moderate dose is safe Ablation of the thyroid remnant decreases the risk of recurrent disease All patients should be offered this therapy Selective Administration Morbidity from I-131, I while rare, does occur Most patients with DTC are at very low risk of death or recurrence Treatment should be offered selectively
75 Survival (T x N 0 M 0, MACIS<6) 100 Survival (%) I 131 Ablation (n=195) No Ablation (n=441) Years from diagnosis 636 node negative patients; total or near-total TTX;
76 Survival (T x N 1 M 0, MACIS<6) Survival (cause-specific) I 131 Ablation (n=303) No Ablation (n=224) Years from diagnosis 527 node positive patients; total or near-total TTX;
77 Recurrence (T x N 0 M 0, MACIS<6) I 131 Ablation No Ablation Years from diagnosis 636 node negative patients; total or near-total TTX;
78 Recurrence (T x N 1 M 0, MACIS<6) 100 I 131 Ablation No Ablation Years from diagnosis 527 node positive patients; total or near-total TTX;
79 Carcinogenesis with I populations (Sweden, Italy, France) 6841 patients Mean dose I mci Mean F/U of 13 years Incidence of 2 nd malignancy Increased risk for cancer of: Salivary gland 7.5 Bone & soft tissue 4.0 Uterus / female genital 2.3 Colorectal 1.3 Relative Risk Dose dependent risk increase * * Bone and soft tissue Dose of I-131 (mci) Rubino 2003
80 Post-operative operative Remnant Ablation: ATA Guidelines 2009 RRA recommended for - Patients with Stage III and IV disease - >45 years, node positive, invasive, metastatic - Patients with Stage II disease (<45 years) - <45 years, metastatic - Most older patients with Stage II disease - >45 years with larger tumors (> 2 cm) - Selected patients with Stage I disease - multifocal; nodes; invasion; non-ptc PTC
81 Recommendation 32 RAI ablation is recommended for all patients with: Distant metastases, gross extrathyroidal extension and tumor size > 4 cm Even in the absence of other high risk features
82 Recommendation 32 Radioiodine ablation may be helpful for tumors cm in diameter, in patients with lymph node metastases, or other high risk features including histologic variants that would place the patient in an intermediate or high risk group
83 Recommendation 32 Remnant ablation is not recommended for unifocal or multifocal cancers <1cm in the absence of other high risk features

84 Extent of Lymphadenectomy
85 Most recurrences in PTC (esp. low-risk) are nodal
86 Regional Lymph Node Metastases Influence on prognosis is questionable Effect on survival (rarity) Little if any in most cases Older patients Bilateral jugular nodes (extensive) Extracapsular spread, matted nodes Locally advanced primary Possible exceptions
87 Why Perform Cervical Lymphadenectomies Positive nodes in select groups worsen prognosis Nodes beget nodes recurrence May become destructive over time (especially older patients) Cannot rely upon RAI to fix shoddy surgery
88 Why Perform Cervical Lymphadenectomies? Thyroglobulin levels (withdrawal, Thyrogen stimulated) High resolution ultrasound Endocrinologists Radioiodine and PET scans Tg mrna
89



90
91 PTC Berry-Picking vs Formal Nodal Dissection Nodal recurrences increased in all series Reoperations more difficult Increased morbidity Metastatic carcinoma in lymph nodes > 3 mm always associated with disease in smaller lymphatics Noguchi et al 1970, 1987
92 Best to avoid going back to the central compartment
93 Routine Removal of Central Compartment Nodes Advocated by some groups Only if FS Only for larger 1 1 tumors (> cm) Only if grossly involved Increased hypoparathyroidism, neuropraxia
94 They Will Come Back To Haunt Us and Our Patients
95 Lateral Neck Dissection Therapeutic Biopsy positive Ultrasound positive Gross involvement
96
97

98
99
100

101
102
103
104
105
106

107
108 Prophylactic Central Lymph Node Dissection Should be performed for T3 and T4 tumors. It is optional for T1 and T2 tumors (ATA Recommendations 2009)
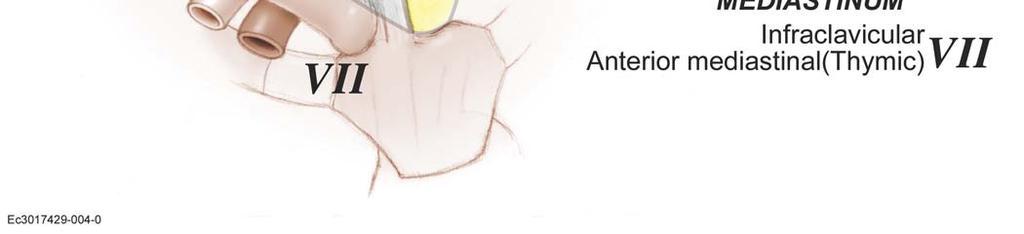
109 Practical Algorithm FNA for PTC (or suspicious) US Mapping ± FNA Lateral Nodes Lateral Nodes Extensive MRND +TTx +CCND Limited SND +TTx +CCND MRND = modified radical neck dissection SND = selective (lateral) neck dissection Total Thyroidectomy (TTx) CN s s grossly CN s s grossly Multifocal Tumor unifocal Larger tumor < 1 cm Extrathyroidal Intrathyroidal Bilateral level VI ± VII Delphian Pretracheal Ipsilateral level VI Delphian Pretracheal
110 Recommendations BLR and central node dissection (CND) reduces TR in low-risk patients BLR and CND reduces TR and CSM in high-risk patients RRA does not further reduce CSM or TR in MACIS low-risk patients
111 TSH Suppression and Outcomes 683 patients with DTC followed at 14 institutions up to 10 years Majority (90%) were PTC A: Stage I & II B: Stage III & IV % Free of Progressive Disease A B TSH Suppression p = 0.03 Follow-up Cooper et al 1998



112 Childhood PTC
113 Ian D. Hay, MD, PhD


114 215 consecutive PTC patients aged <21 years January 1, December 31, 2008 Followed to June 2009
115 Childhood and Adolescent PTC Treated at Mayo Clinic during Conclusion Patients with PTC before age 21 typically were node- positive and 1/3 recurred in 30 yr Extent of initial surgery,, but not radioiodine remnant ablation, influenced recurrence rates PTC patients <21 yr at diagnosis enjoyed a 98% cause- specific survival at 60 postop yr However, such patients experienced excessive all- causes mortality after 30 years


116 Mortality Rates from All Causes in Childhood and Adolescent PTC Cohort


117 Childhood and Adolescent PTC Treated at Mayo Clinic during
118 PAPILLARY THYROID MICROCARCINOMA An innocuous occurrence in our opinion Unless higher risk features are present at the time of diagnosis Manage accordingly
119 Follicular Thyroid Cancer (FTC) 10-15% 15% of thyroid malignancies Cytology insufficient Capsular / vascular invasion 90% unifocal Hematogenous spread Lung and bone metastases: 15% Nodal metastases: FCC 5%

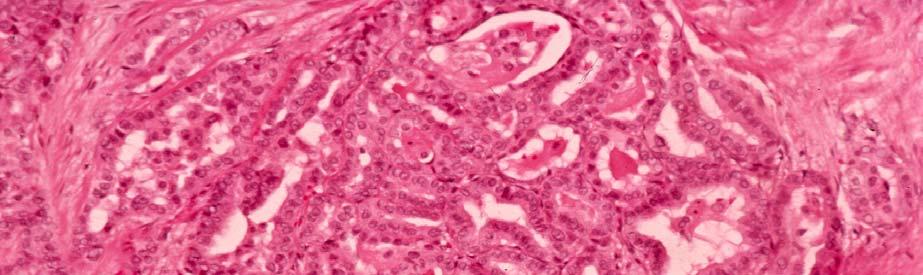
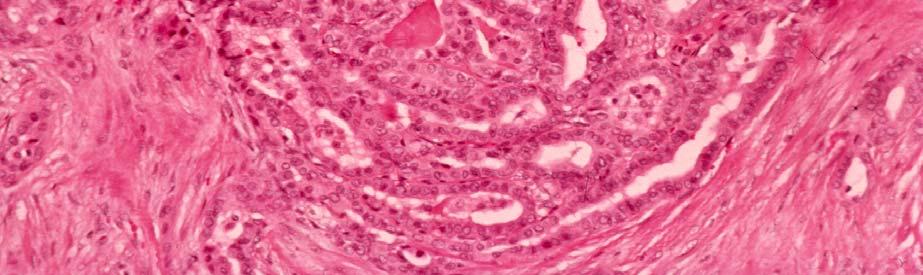
120 Papillary Thyroid Carcinoma-FNAB


121 Widely Invasive Follicular Carcinoma


122 Hurthle Cell Adenoma or Carcinoma?

123 Follicular Carcinoma-Capsular Capsular Invasion

124 Follicular Carcinoma Minimally Invasive Into Capsular Vessel

125 Frozen Section-Modified Toluidine Blue Stain Vascular Invasion


126 Follicular Neoplasms: Frozen Section Dependent Upon: Good pathologists Significant exposure to frozen section, especially thyroid Superb support system
127 Follicular Neoplasms: Frozen Section Results: 1023 Patients 286 (28%) 737 (72%) Mean age: 52.1 years
128 Follicular Neoplasms: Pathology Perm Section Ca Non-Ca Frozen Section Ca Non-Ca Total 65 TP 18 FN 83 7 FP 933 TN /83 (78%) Ca Dx by FS
129
130 Follicular Thyroid Cancer Lymph node metastases (< 5%) Usually associated with locally advanced tumor Worse prognosis
131 FTC Minimally Invasive (80%) Widely Invasive (20%) Microscopic vascular and capsular invasion Gross involvement of vessels and contiguous structures
132 FTC Prognostic indicators Age > 50 Marked vascular invasion Metastatic disease Brennan et al, 1991
133 FTC High risk (2/3 risk factors) Survival: 47% and 5 and 20 years Low risk (0-1/3 risk factors) Survival: 99% and 5 and 20 years
134 100 FTC Low risk (n=82) Cumulative % surviving follicular cancer High risk (n=18) Years after initial treatment Brennan et al, 1991
135 FTC Tumors < 2 cm with minimal capsular invasion alone No metastases or deaths Recent 10-year follow-up Lobectomy Alone van Heerden et al, 1992
136 Hurthle Cell Cancer <5% of all thyroid cancers More locally aggressive Less avidity for RAI Nodal metastases in 1/3
137 Follicular and Hurthle Cell Carcinoma Lymph node mets from FTC rare (<5%); if present consider FVPTC Routine CCND and LND for FTC not necessary unless positive nodes are present grossly or by US HCC has positive nodes in up to 30%; manage nodes like PTC
138 FTC/HCC Treatment: Total / NT Thyroidectomy Sample central nodes* Formal node dissection when nodes CCND for HCC RRA, THST except in small tumors with minimal capsular invasion *may be only indication of FVPTC
139 Summary Total or Near-Total Thyroidectomy Central Compartment Lymphadenectomy (PTC, HCC) Lateral lymphadenectomy based on pre-op Ultrasound RRA based on Risk Assessment TSH Suppression based on Risk Assessment
140 If all else fails.

141 Thyroid Cancer Strategy Meeting? Should we give radioiodine today?
142 THANK YOU
4/22/2010. Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey.
 Management of Differentiated Thyroid Cancer: Head Neck Surgeon Perspective Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey Thyroid gland Small endocrine gland:
Management of Differentiated Thyroid Cancer: Head Neck Surgeon Perspective Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey Thyroid gland Small endocrine gland:
Ultrasound for Pre-operative Evaluation of Well Differentiated Thyroid Cancer
 Ultrasound for Pre-operative Evaluation of Well Differentiated Thyroid Cancer Its Not Just About the Nodes AACE Advances in Medical and Surgical Management of Thyroid Cancer - 2017 Robert A. Levine, MD,
Ultrasound for Pre-operative Evaluation of Well Differentiated Thyroid Cancer Its Not Just About the Nodes AACE Advances in Medical and Surgical Management of Thyroid Cancer - 2017 Robert A. Levine, MD,
Gerard M. Doherty, MD
 Surgical Management of Differentiated Thyroid Cancer: Update on 2015 ATA Guidelines Gerard M. Doherty, MD Chair of Surgery Utley Professor of Surgery and Medicine Boston University Surgeon-in-Chief Boston
Surgical Management of Differentiated Thyroid Cancer: Update on 2015 ATA Guidelines Gerard M. Doherty, MD Chair of Surgery Utley Professor of Surgery and Medicine Boston University Surgeon-in-Chief Boston
Persistent & Recurrent Differentiated Thyroid Cancer
 Persistent & Recurrent Differentiated Thyroid Cancer Electron Kebebew University of California, San Francisco Department of Surgery Objectives Risk factors for persistent & recurrent disease Causes of
Persistent & Recurrent Differentiated Thyroid Cancer Electron Kebebew University of California, San Francisco Department of Surgery Objectives Risk factors for persistent & recurrent disease Causes of
Management guideline for patients with differentiated thyroid cancer. Teeraporn Ratanaanekchai ENT, KKU 17 October 2007
 Management guideline for patients with differentiated thyroid Teeraporn Ratanaanekchai ENT, KKU 17 October 2007 Incidence (Srinagarind Hospital, 2005, both sex) Site (all) cases % 1. Liver 1178 27 2. Lung
Management guideline for patients with differentiated thyroid Teeraporn Ratanaanekchai ENT, KKU 17 October 2007 Incidence (Srinagarind Hospital, 2005, both sex) Site (all) cases % 1. Liver 1178 27 2. Lung
Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer
 Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer AACE - Advances in Medical and Surgical Management of Thyroid Cancer - 2018 Robert A. Levine, MD, FACE, ECNU Thyroid Center of New Hampshire Geisel
Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer AACE - Advances in Medical and Surgical Management of Thyroid Cancer - 2018 Robert A. Levine, MD, FACE, ECNU Thyroid Center of New Hampshire Geisel
2015 American Thyroid Association Thyroid Nodule and Cancer Guidelines
 2015 American Thyroid Association Thyroid Nodule and Cancer Guidelines Angela M. Leung, MD, MSc, ECNU November 5, 2016 Outline Workup of nontoxic thyroid nodule(s) Ultrasound FNAB Management of FNAB results
2015 American Thyroid Association Thyroid Nodule and Cancer Guidelines Angela M. Leung, MD, MSc, ECNU November 5, 2016 Outline Workup of nontoxic thyroid nodule(s) Ultrasound FNAB Management of FNAB results
Differentiated Thyroid Carcinoma
 Differentiated Thyroid Carcinoma The GOOD cancer? Jennifer Sipos, MD Associate Professor of Medicine Director, Benign Thyroid Program Division of Endocrinology, Diabetes and Metabolism The Ohio State University
Differentiated Thyroid Carcinoma The GOOD cancer? Jennifer Sipos, MD Associate Professor of Medicine Director, Benign Thyroid Program Division of Endocrinology, Diabetes and Metabolism The Ohio State University
THYROID CANCER IN CHILDREN. Humberto Lugo-Vicente MD FACS FAAP Professor Pediatric Surgery UPR School of Medicine
 THYROID CANCER IN CHILDREN Humberto Lugo-Vicente MD FACS FAAP Professor Pediatric Surgery UPR School of Medicine Thyroid nodules Rare Female predominance 4-fold as likely to be malignant Hx Radiation exposure?
THYROID CANCER IN CHILDREN Humberto Lugo-Vicente MD FACS FAAP Professor Pediatric Surgery UPR School of Medicine Thyroid nodules Rare Female predominance 4-fold as likely to be malignant Hx Radiation exposure?
Preoperative Evaluation
 Preoperative Evaluation Lateral compartment lymph nodes are easier to detect and are amenable to FNA Central compartment lymph nodes are much more difficult to detect and FNA (Tg washout testing is compromised)
Preoperative Evaluation Lateral compartment lymph nodes are easier to detect and are amenable to FNA Central compartment lymph nodes are much more difficult to detect and FNA (Tg washout testing is compromised)
PEDIATRIC Ariel Katz MD
 PEDIATRIC Ariel Katz MD Dept. Otolaryngology Head &Neck Surgery Wolfson Medical Center Holon, Israel OBJECTIVES Overview/Background Epidemiology/Etiology Intro to Guidelines Workup Treatment Follow-Up
PEDIATRIC Ariel Katz MD Dept. Otolaryngology Head &Neck Surgery Wolfson Medical Center Holon, Israel OBJECTIVES Overview/Background Epidemiology/Etiology Intro to Guidelines Workup Treatment Follow-Up
Differentiated Thyroid Cancer: Initial Management
 Page 1 ATA HOME GIVE ONLINE ABOUT THE ATA JOIN THE ATA MEMBER SIGN-IN INFORMATION FOR PATIENTS FIND A THYROID SPECIALIST Home Management Guidelines for Patients with Thyroid Nodules and Differentiated
Page 1 ATA HOME GIVE ONLINE ABOUT THE ATA JOIN THE ATA MEMBER SIGN-IN INFORMATION FOR PATIENTS FIND A THYROID SPECIALIST Home Management Guidelines for Patients with Thyroid Nodules and Differentiated
Dynamic Risk Stratification:
 Dynamic Risk Stratification: Using Risk Estimates to Guide Initial Management R Michael Tuttle, MD Clinical Director, Endocrinology Service Memorial Sloan Kettering Cancer Center Professor of Medicine
Dynamic Risk Stratification: Using Risk Estimates to Guide Initial Management R Michael Tuttle, MD Clinical Director, Endocrinology Service Memorial Sloan Kettering Cancer Center Professor of Medicine
The International Federation of Head and Neck Oncologic Societies. Current Concepts in Head and Neck Surgery and Oncology
 The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
How good are we at finding nodules? Thyroid Nodules Thyroid Cancer Epidemiology Initial management Long-term follow up Disease-free status
 New Perspectives in Thyroid Cancer Jennifer Sipos, MD Assistant Professor of Medicine Division of Endocrinology The Ohio State University Outline Thyroid Nodules Thyroid Cancer Epidemiology Initial management
New Perspectives in Thyroid Cancer Jennifer Sipos, MD Assistant Professor of Medicine Division of Endocrinology The Ohio State University Outline Thyroid Nodules Thyroid Cancer Epidemiology Initial management
Reoperative central neck surgery
 Reoperative central neck surgery R. Pandev, I. Tersiev, M. Belitova, A. Kouizi, D. Damyanov University Clinic of Surgery, Section Endocrine Surgery University Hospital Queen Johanna ISUL Medical University
Reoperative central neck surgery R. Pandev, I. Tersiev, M. Belitova, A. Kouizi, D. Damyanov University Clinic of Surgery, Section Endocrine Surgery University Hospital Queen Johanna ISUL Medical University
Approach to Thyroid Nodules
 Approach to Thyroid Nodules Alice Y.Y. Cheng, MD, FRCPC Twitter: @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
Approach to Thyroid Nodules Alice Y.Y. Cheng, MD, FRCPC Twitter: @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
Disclosures Nodal Management in Differentiated Thyroid Carcinoma
 Disclosures Nodal Management in Differentiated Thyroid Carcinoma Nothing to disclose Jonathan George, MD, MPH Assistant Professor UCSF Head and Neck Oncologic & Endocrine Surgery Objectives Overview Describe
Disclosures Nodal Management in Differentiated Thyroid Carcinoma Nothing to disclose Jonathan George, MD, MPH Assistant Professor UCSF Head and Neck Oncologic & Endocrine Surgery Objectives Overview Describe
- RET/PTC rearrangement: 20% papillary thyroid cancer - RET: medullary thyroid cancer
 Thyroid Cancer UpToDate: Introduction: Risk Factors: Biology: Symptoms: Diagnosis: 1. Lenvina is the first line therapy with powerful durable response and superior PFS in pts with RAI-refractory disease.
Thyroid Cancer UpToDate: Introduction: Risk Factors: Biology: Symptoms: Diagnosis: 1. Lenvina is the first line therapy with powerful durable response and superior PFS in pts with RAI-refractory disease.
Thyroid Surgery: Lobectomy, total thyroidectomy, LN biopsies or only watchful waiting?
 Thyroid Surgery: Lobectomy, total thyroidectomy, LN biopsies or only watchful waiting? Jacob Moalem, MD, FACS Associate Professor Endocrine Surgery and Endocrinology URMC Agenda 1. When is lobectomy alone
Thyroid Surgery: Lobectomy, total thyroidectomy, LN biopsies or only watchful waiting? Jacob Moalem, MD, FACS Associate Professor Endocrine Surgery and Endocrinology URMC Agenda 1. When is lobectomy alone
WTC 2013 Panel Discussion: Minimal disease
 WTC 2013 Panel Discussion: Minimal disease Susan J. Mandel MD MPH Panelists Ken Ain Yasuhiro Ito Stephanie Lee Erich Sturgis Mark Urken Faculty/Presenter Disclosure Relationships with commercial interests
WTC 2013 Panel Discussion: Minimal disease Susan J. Mandel MD MPH Panelists Ken Ain Yasuhiro Ito Stephanie Lee Erich Sturgis Mark Urken Faculty/Presenter Disclosure Relationships with commercial interests
Review Article Management of thyroid carcinoma Alauddin M, Joarder AH
 Management of thyroid carcinoma Alauddin M, Joarder AH The ORION Medical Journal 2004 May;18:163-166 Overview The two most common forms of thyroid cancer, papillaryand follicular thyroid cancer, together
Management of thyroid carcinoma Alauddin M, Joarder AH The ORION Medical Journal 2004 May;18:163-166 Overview The two most common forms of thyroid cancer, papillaryand follicular thyroid cancer, together
The International Federation of Head and Neck Oncologic Societies. Current Concepts in Head and Neck Surgery and Oncology
 The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
Adjuvant therapy for thyroid cancer
 Carcinoma of the thyroid Adjuvant therapy for thyroid cancer John Hay Department of Radiation Oncology Vancouver Cancer Centre Department of Surgery UBC 1% of all new malignancies 0.5% in men 1.5% in women
Carcinoma of the thyroid Adjuvant therapy for thyroid cancer John Hay Department of Radiation Oncology Vancouver Cancer Centre Department of Surgery UBC 1% of all new malignancies 0.5% in men 1.5% in women
Current Issues in Thyroid Cancer Surgery in 2017
 Current Issues in Thyroid Cancer Surgery in 2017 Dr. David Goldstein MD Msc FRCSC FACS Associate Professor, Department Otolaryngology Head & Neck Surgery, U of T Department of Surgical Oncology, Princess
Current Issues in Thyroid Cancer Surgery in 2017 Dr. David Goldstein MD Msc FRCSC FACS Associate Professor, Department Otolaryngology Head & Neck Surgery, U of T Department of Surgical Oncology, Princess
Thyroid Pathology: It starts and ends with the gross. Causes of Thyrophobia. Agenda. Diagnostic ambiguity. Treatment/prognosis disconnect
 Thyroid Pathology: It starts and ends with the gross Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for
Thyroid Pathology: It starts and ends with the gross Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for
Objectives. 1)To recall thyroid nodule ultrasound characteristics that increase the risk of malignancy
To recall thyroid nodule ultrasound characteristics that increase the risk of malignancy") Evaluation and Management of Thyroid Nodules in Primary Care Chris Sadler, MA, PA C, CDE, DFAAPA Medical Science Outcomes Liaison Intarcia Diabetes and Endocrine Associates La Jolla, CA Past President
Evaluation and Management of Thyroid Nodules in Primary Care Chris Sadler, MA, PA C, CDE, DFAAPA Medical Science Outcomes Liaison Intarcia Diabetes and Endocrine Associates La Jolla, CA Past President
Thyroid Cancer: When to Treat? MEGAN R. HAYMART, MD
 Thyroid Cancer: When to Treat? MEGAN R. HAYMART, MD ASSOCIATE PROFESSOR OF MEDICINE UNIVERSITY OF MICHIGAN MICHIGAN AACE 2018 ANNUAL MEETING Thyroid Cancer: When Not to Treat? FOCUS WILL BE ON LOW-RISK
Thyroid Cancer: When to Treat? MEGAN R. HAYMART, MD ASSOCIATE PROFESSOR OF MEDICINE UNIVERSITY OF MICHIGAN MICHIGAN AACE 2018 ANNUAL MEETING Thyroid Cancer: When Not to Treat? FOCUS WILL BE ON LOW-RISK
Thyroid nodules 3/22/2011. Most thyroid nodules are benign. Thyroid nodules: differential diagnosis
 Most thyroid nodules are benign Thyroid nodules Postgraduate Course in General Surgery thyroid nodules occur in 77% of the world s population palpable thyroid nodules occur in about 5% of women and 1%
Most thyroid nodules are benign Thyroid nodules Postgraduate Course in General Surgery thyroid nodules occur in 77% of the world s population palpable thyroid nodules occur in about 5% of women and 1%
Thyroid nodules. Most thyroid nodules are benign
 Thyroid nodules Postgraduate Course in General Surgery Jessica E. Gosnell MD Assistant Professor March 22, 2011 Most thyroid nodules are benign thyroid nodules occur in 77% of the world s population palpable
Thyroid nodules Postgraduate Course in General Surgery Jessica E. Gosnell MD Assistant Professor March 22, 2011 Most thyroid nodules are benign thyroid nodules occur in 77% of the world s population palpable
Risk Adapted Follow-Up
 Risk Adapted Follow-Up Individualizing Follow- Up Strategies R Michael Tuttle, MD Clinical Director, Endocrinology Service Memorial Sloan Kettering Cancer Center Professor of Medicine Weill Medical College
Risk Adapted Follow-Up Individualizing Follow- Up Strategies R Michael Tuttle, MD Clinical Director, Endocrinology Service Memorial Sloan Kettering Cancer Center Professor of Medicine Weill Medical College
Evaluation and Management of Thyroid Nodules. Nick Vernetti, MD, FACE Palm Medical Group Las Vegas, Nevada
 Evaluation and Management of Thyroid Nodules Nick Vernetti, MD, FACE Palm Medical Group Las Vegas, Nevada Disclosure Consulting Amgen Speaking Amgen Objectives Understand the significance of incidental
Evaluation and Management of Thyroid Nodules Nick Vernetti, MD, FACE Palm Medical Group Las Vegas, Nevada Disclosure Consulting Amgen Speaking Amgen Objectives Understand the significance of incidental
Objectives. How to Investigate Thyroid Nodules like A Pro
 How to Investigate Thyroid Nodules like A Pro Chris Sadler, MA, PA C, CDE, DFAAPA Medical Science Outcomes Liaison Intarcia Diabetes and Endocrine Associates La Jolla, CA Past President ASEPA Disclosures
How to Investigate Thyroid Nodules like A Pro Chris Sadler, MA, PA C, CDE, DFAAPA Medical Science Outcomes Liaison Intarcia Diabetes and Endocrine Associates La Jolla, CA Past President ASEPA Disclosures
5/18/2013. Most thyroid nodules are benign. Thyroid nodules: new techniques in evaluation
 Most thyroid nodules are benign Thyroid nodules: new techniques in evaluation Incidence Etiology Risk factors Diagnosis Gene classification system Treatment Postgraduate Course in General Surgery Jessica
Most thyroid nodules are benign Thyroid nodules: new techniques in evaluation Incidence Etiology Risk factors Diagnosis Gene classification system Treatment Postgraduate Course in General Surgery Jessica
Thyroid Nodule. Disclosure. Learning Objectives P A P A P A 3/18/2014. Nothing to disclose.
 Thyroid Nodule Evaluating the patient with a thyroid nodule and some management options. Miguel V. Valdez PA C Disclosure Nothing to disclose. Learning Objectives Examination of thyroid gland Options for
Thyroid Nodule Evaluating the patient with a thyroid nodule and some management options. Miguel V. Valdez PA C Disclosure Nothing to disclose. Learning Objectives Examination of thyroid gland Options for
Strategies for detection of recurrent disease in longterm follow-up of differentiated thyroid cancer
 Strategies for detection of recurrent disease in longterm follow-up of differentiated thyroid cancer A rational approach to longterm follow-up based on dynamic risk assessment. World Congress on Thyroid
Strategies for detection of recurrent disease in longterm follow-up of differentiated thyroid cancer A rational approach to longterm follow-up based on dynamic risk assessment. World Congress on Thyroid
What s an NIFTP? Keeping Up To Date in Thyroid 2018
 What s an NIFTP? Keeping Up To Date in Thyroid 2018 Kathleen Hands, MD, FACE, ECNU Director, Thyroid Center of South Texas Assistant Clinical Professor UTHSCSA DrHands@Thyroid-Center.com 210-844-6163 text
What s an NIFTP? Keeping Up To Date in Thyroid 2018 Kathleen Hands, MD, FACE, ECNU Director, Thyroid Center of South Texas Assistant Clinical Professor UTHSCSA DrHands@Thyroid-Center.com 210-844-6163 text
10/24/2008. Surgery for Well-differentiated Thyroid Carcinoma- The Primary
 Surgery for Well-differentiated Thyroid Carcinoma- The Primary Head and Neck Endocrine Surgery Department of Otolaryngology-Head and Neck Surgery, UCSF October 24-25, 2008 Robert A. Sofferman, MD Professor
Surgery for Well-differentiated Thyroid Carcinoma- The Primary Head and Neck Endocrine Surgery Department of Otolaryngology-Head and Neck Surgery, UCSF October 24-25, 2008 Robert A. Sofferman, MD Professor
Volume 2 Issue ISSN
 Volume 2 Issue 3 2012 ISSN 2250-0359 Correlation of fine needle aspiration and final histopathology in thyroid disease: a series of 702 patients managed in an endocrine surgical unit *Chandrasekaran Maharajan
Volume 2 Issue 3 2012 ISSN 2250-0359 Correlation of fine needle aspiration and final histopathology in thyroid disease: a series of 702 patients managed in an endocrine surgical unit *Chandrasekaran Maharajan
Thyroid Nodules. Dr. HAKIMI, SpAK Dr. MELDA DELIANA, SpAK Dr. SISKA MAYASARI LUBIS, SpA
 Thyroid Nodules ENDOCRINOLOGY DIVISION ENDOCRINOLOGY DIVISION Dr. HAKIMI, SpAK Dr. MELDA DELIANA, SpAK Dr. SISKA MAYASARI LUBIS, SpA Anatomical Considerations The Thyroid Nodule Congenital anomalies Thyroglossal
Thyroid Nodules ENDOCRINOLOGY DIVISION ENDOCRINOLOGY DIVISION Dr. HAKIMI, SpAK Dr. MELDA DELIANA, SpAK Dr. SISKA MAYASARI LUBIS, SpA Anatomical Considerations The Thyroid Nodule Congenital anomalies Thyroglossal
3/29/2012. Thyroid cancer- what s new. Thyroid Cancer. Thyroid cancer is now the most rapidly increasing cancer in women
 Thyroid cancer- what s new Thyroid Cancer Changing epidemiology Molecular markers Lymph node dissection Technical advances rhtsh Genetic testing and prophylactic surgery Vandetanib What s new? Jessica
Thyroid cancer- what s new Thyroid Cancer Changing epidemiology Molecular markers Lymph node dissection Technical advances rhtsh Genetic testing and prophylactic surgery Vandetanib What s new? Jessica
Thyroid nodules - medical and surgical management. Endocrinology and Endocrine Surgery Manchester Royal Infirmary
 Thyroid nodules - medical and surgical management JRE Davis NR Parrott Endocrinology and Endocrine Surgery Manchester Royal Infirmary Thyroid nodules - prevalence Thyroid nodules common, increase with
Thyroid nodules - medical and surgical management JRE Davis NR Parrott Endocrinology and Endocrine Surgery Manchester Royal Infirmary Thyroid nodules - prevalence Thyroid nodules common, increase with
Pediatric Thyroid Cancer Lung Metastases. Liora Lazar MD
 Pediatric Thyroid Cancer Lung Metastases Liora Lazar MD Differentiated thyroid cancer (DTC) The 3rd most common solid tumor in childhood and adolescence Accounting for 1.5%-3% of all childhood cancers
Pediatric Thyroid Cancer Lung Metastases Liora Lazar MD Differentiated thyroid cancer (DTC) The 3rd most common solid tumor in childhood and adolescence Accounting for 1.5%-3% of all childhood cancers
Management of Recurrent Thyroid Cancer
 Management of Recurrent Thyroid Cancer Eric Genden, MD, MHA Isidore Professor and Chairman Department of Otolaryngology- Head and Neck Surgery Senior Associate Dean for Clinical Affairs The Icahn School
Management of Recurrent Thyroid Cancer Eric Genden, MD, MHA Isidore Professor and Chairman Department of Otolaryngology- Head and Neck Surgery Senior Associate Dean for Clinical Affairs The Icahn School
How Will (Should) the Latest Guidelines Affect the Endocrinologist s Management of Thyroid Cancer? AACE 2017
 the Latest Guidelines Affect the Endocrinologist s Management of Thyroid Cancer? AACE 2017") How Will (Should) the Latest Guidelines Affect the Endocrinologist s Management of Thyroid Cancer? AACE 2017 Bryan R. Haugen, MD University of Colorado, School of Medicine Outline Some statistics New guidelines
How Will (Should) the Latest Guidelines Affect the Endocrinologist s Management of Thyroid Cancer? AACE 2017 Bryan R. Haugen, MD University of Colorado, School of Medicine Outline Some statistics New guidelines
Management of Thyroid Nodules
 Management of Thyroid Nodules 38 y/o female with solid 1.5 cm right Thyroid nodule. TSH=0.68 Vincent J. Reid, MD., FACS Thyroid Cancer Incidence & Mortality 1974 to 2004 Overall Women Men Mortality 1 Cancer
Management of Thyroid Nodules 38 y/o female with solid 1.5 cm right Thyroid nodule. TSH=0.68 Vincent J. Reid, MD., FACS Thyroid Cancer Incidence & Mortality 1974 to 2004 Overall Women Men Mortality 1 Cancer
Dilemmas in Cytopathology and Histopathology
 Dilemmas in Cytopathology and Histopathology Yuri E. Nikiforov, MD, PhD Division of Molecular & Genomic Pathology University of Pittsburgh Medical Center, USA Objectives Discuss new WHO classification
Dilemmas in Cytopathology and Histopathology Yuri E. Nikiforov, MD, PhD Division of Molecular & Genomic Pathology University of Pittsburgh Medical Center, USA Objectives Discuss new WHO classification
YCN Thyroid NSSG. *** VALID ON DATE OF PRINTING ONLY - all guidelines available at *** page 1 of 8 version number: 1.
 YCN Thyroid NSSG Guidelines on Indications for Thyroid Surgery, Prophylactic Level 6 and Radioiodine plus follow-up of low risk differentiated thyroid cancer page 1 of 8 i Document Control Title Author(s)
YCN Thyroid NSSG Guidelines on Indications for Thyroid Surgery, Prophylactic Level 6 and Radioiodine plus follow-up of low risk differentiated thyroid cancer page 1 of 8 i Document Control Title Author(s)
Thyroid Nodules. Hossein Gharib, MD, MACP, MACE
 Thyroid Nodules Hossein Gharib, MD, MACP, MACE Professor of Medicine Mayo Clinic College of Medicine President Elect, American College of Endocrinology University Course January 2008 CP1294362-1 Thyroid
Thyroid Nodules Hossein Gharib, MD, MACP, MACE Professor of Medicine Mayo Clinic College of Medicine President Elect, American College of Endocrinology University Course January 2008 CP1294362-1 Thyroid
40 TH EUROPEAN CONGRESS 0F CYTOLOGY LIVERPOOL, UK October 2-5, 2016
 Outcomes from the diagnostic approach of thyroid lesions using US-FNA and LBC in clinical practice Emmanouel Mastorakis MD PhD Cytopathologist Director in Cytopathology Laboratory Regional General Hospital
Outcomes from the diagnostic approach of thyroid lesions using US-FNA and LBC in clinical practice Emmanouel Mastorakis MD PhD Cytopathologist Director in Cytopathology Laboratory Regional General Hospital
AACE Thyroid Cancer Tumor board 25 years of the Endocrine and Surgery collaboration
 AACE Thyroid Cancer Tumor board 25 years of the Endocrine and Surgery collaboration Dr. Peter Singer, Endocrinology Dr. Peter Sadow, Pathology Moderator Dr. Greg Randolph, Otolaryngology Relevant Financial
AACE Thyroid Cancer Tumor board 25 years of the Endocrine and Surgery collaboration Dr. Peter Singer, Endocrinology Dr. Peter Sadow, Pathology Moderator Dr. Greg Randolph, Otolaryngology Relevant Financial
Shifting Paradigms and Debates in the Management of Well-differentiated Thyroid Cancer
 DEBATE WJOES Shifting Paradigms and Debates in the Management of Well-differentiated Thyroid Cancer Shifting Paradigms and Debates in the Management of Well-differentiated Thyroid Cancer Ashok R Shaha
DEBATE WJOES Shifting Paradigms and Debates in the Management of Well-differentiated Thyroid Cancer Shifting Paradigms and Debates in the Management of Well-differentiated Thyroid Cancer Ashok R Shaha
Thyroid INTRODUCTION ANATOMY SUMMARY OF CHANGES
 AJC 7/14/06 1:19 PM Page 67 Thyroid C73.9 Thyroid gland SUMMARY OF CHANGES Tumor staging (T) has been revised and the categories redefined. T4 is now divided into T4a and T4b. Nodal staging (N) has been
AJC 7/14/06 1:19 PM Page 67 Thyroid C73.9 Thyroid gland SUMMARY OF CHANGES Tumor staging (T) has been revised and the categories redefined. T4 is now divided into T4a and T4b. Nodal staging (N) has been
The use of Radioactive Iodine (RAI) for Differentiated Thyroid Cancer
 for Differentiated Thyroid Cancer") The use of Radioactive Iodine (RAI) for Differentiated Thyroid Cancer Wendy Sacks, M.D. Cedars Sinai Medical Center California Chapter Annual Meeting, AACE Nov 5, 2016 Increasing Incidence of Thyroid Cancer
The use of Radioactive Iodine (RAI) for Differentiated Thyroid Cancer Wendy Sacks, M.D. Cedars Sinai Medical Center California Chapter Annual Meeting, AACE Nov 5, 2016 Increasing Incidence of Thyroid Cancer
New York, the nation s thyroid gland. Christopher Morley ( ), "Shore Leave"
, Shore Leave") New York, the nation s thyroid gland Christopher Morley (1890-1957), "Shore Leave" Thyroid Literature Medline Thyroid disease 136,053 Thyroid tumors 33,554 New Paper on Thyroid Disease Every 3 Hours New
New York, the nation s thyroid gland Christopher Morley (1890-1957), "Shore Leave" Thyroid Literature Medline Thyroid disease 136,053 Thyroid tumors 33,554 New Paper on Thyroid Disease Every 3 Hours New
I-131 ABLATION AND ADJUVANT THERAPY OF THYROID CANCER
 AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGISTS Advances in Medical and Surgical Management of Thyroid Cancer January 23-24, 2015 I-131 ABLATION AND ADJUVANT THERAPY OF THYROID CANCER 2015 Leonard Wartofsky,
AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGISTS Advances in Medical and Surgical Management of Thyroid Cancer January 23-24, 2015 I-131 ABLATION AND ADJUVANT THERAPY OF THYROID CANCER 2015 Leonard Wartofsky,
1. Protocol Summary Summary of Trial Design. IoN
 1. Protocol Summary 1.1. Summary of Trial Design Title: Short Title/acronym: IoN Is ablative radioiodine Necessary for low risk differentiated thyroid cancer patients IoN EUDRACT no: 2011-000144-21 Sponsor
1. Protocol Summary 1.1. Summary of Trial Design Title: Short Title/acronym: IoN Is ablative radioiodine Necessary for low risk differentiated thyroid cancer patients IoN EUDRACT no: 2011-000144-21 Sponsor
AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS
 AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS PAPILLARY THYROID CARCINOMA Clinical Any age Microscopic to large Female: Male= 2-4:1 Radiation history Lymph nodes Prognosis
AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS PAPILLARY THYROID CARCINOMA Clinical Any age Microscopic to large Female: Male= 2-4:1 Radiation history Lymph nodes Prognosis
Oh, I get it, the TSH goes up and down
 Evaluation and Management of the Thyroid Nodule Oh, I get it, the TSH goes up and down UCSF Head and Neck Conference October 24, 2008 Peter A. Singer, M.D. Professor and Chief Clinical Endocrinology University
Evaluation and Management of the Thyroid Nodule Oh, I get it, the TSH goes up and down UCSF Head and Neck Conference October 24, 2008 Peter A. Singer, M.D. Professor and Chief Clinical Endocrinology University
Key Topics in Thyroid Cancer Worldwide epidemic What Should the Endocrinologist and Surgeon do?
 Key Topics in Thyroid Cancer Worldwide epidemic What Should the Endocrinologist and Surgeon do? Martin Schlumberger Gustave Presenter Roussy Name and Université Paris Saclay, Villejuif, France 1 Disclosure
Key Topics in Thyroid Cancer Worldwide epidemic What Should the Endocrinologist and Surgeon do? Martin Schlumberger Gustave Presenter Roussy Name and Université Paris Saclay, Villejuif, France 1 Disclosure
Adina Alazraki, MD, FAAP Assistant Professor Radiology and Pediatrics Emory University and Children s Healthcare of Atlanta
 Adina Alazraki, MD, FAAP Assistant Professor Radiology and Pediatrics Emory University and Children s Healthcare of Atlanta Review recently published pediatric guidelines for management of thyroid nodules
Adina Alazraki, MD, FAAP Assistant Professor Radiology and Pediatrics Emory University and Children s Healthcare of Atlanta Review recently published pediatric guidelines for management of thyroid nodules
Follicular Derived Thyroid Tumors
 Follicular Derived Thyroid Tumors Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for Medical Sciences
Follicular Derived Thyroid Tumors Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for Medical Sciences
131-I Therapy Planning in Thyroid Cancer: The role of diagnostic radioiodine scans
 131-I Therapy Planning in Thyroid Cancer: The role of diagnostic radioiodine scans Anca M. Avram, M.D. Associate Professor of Radiology Department of Nuclear Medicine University of Michigan Ann Arbor,
131-I Therapy Planning in Thyroid Cancer: The role of diagnostic radioiodine scans Anca M. Avram, M.D. Associate Professor of Radiology Department of Nuclear Medicine University of Michigan Ann Arbor,
Sonographic Features of Thyroid Nodules & Guidelines for Management
 Sonographic Features of Thyroid Nodules & Guidelines for Management Mark A. Lupo, MD, FACE, ECNU Thyroid & Endocrine Center of Florida Assistant Clinical Professor of Medicine Florida State University,
Sonographic Features of Thyroid Nodules & Guidelines for Management Mark A. Lupo, MD, FACE, ECNU Thyroid & Endocrine Center of Florida Assistant Clinical Professor of Medicine Florida State University,
Treatment of Cervical Lymph Node Metastases Differentiated Thyroid Cancer
 Treatment of Cervical Lymph Node Metastases Differentiated Thyroid Cancer Well Differentiated Thyroid Cancer Natural History and Prognosis EORTC AGES AMES MACIS QuickTime and a TIFF (LZW) decompressor
Treatment of Cervical Lymph Node Metastases Differentiated Thyroid Cancer Well Differentiated Thyroid Cancer Natural History and Prognosis EORTC AGES AMES MACIS QuickTime and a TIFF (LZW) decompressor
Prophylactic Central Compartment Neck Dissection(CCND) for Papillary Thyroid Cancer: Con
 for Papillary Thyroid Cancer: Con") Prophylactic Central Compartment Neck Dissection(CCND) for Papillary Thyroid Cancer: Con Christopher R. McHenry, M.D. Vice Chairman Department of Surgery MetroHealth Medical Center Professor of Surgery
Prophylactic Central Compartment Neck Dissection(CCND) for Papillary Thyroid Cancer: Con Christopher R. McHenry, M.D. Vice Chairman Department of Surgery MetroHealth Medical Center Professor of Surgery
Thyroid Nodules. Family Medicine Refresher Course Geeta Lal MD, FACS April 2, No financial disclosures
 Thyroid Nodules Family Medicine Refresher Course Geeta Lal MD, FACS April 2, 2014 No financial disclosures Objectives Review epidemiology Work up of Thyroid nodules Indications for FNAB Evolving role of
Thyroid Nodules Family Medicine Refresher Course Geeta Lal MD, FACS April 2, 2014 No financial disclosures Objectives Review epidemiology Work up of Thyroid nodules Indications for FNAB Evolving role of
5/3/2017. Ahn et al N Engl J Med 2014; 371
 Alan Failor, M.D. Clinical Professor of Medicine Division of Metabolism, Endocrinology and Nutrition University of Washington April 20, 2017 No disclosures to report 1. Appropriately evaluate s in adult
Alan Failor, M.D. Clinical Professor of Medicine Division of Metabolism, Endocrinology and Nutrition University of Washington April 20, 2017 No disclosures to report 1. Appropriately evaluate s in adult
Surgical Management of Differentiated Thyroid Cancer
 Vanderbilt University Surgical Grand Rounds May 7, 2010 Surgical Management of Differentiated Thyroid Cancer Carmen C Solórzano, MD, FACS Associate Professor Endocrine and Surgical Oncology Vanderbilt
Vanderbilt University Surgical Grand Rounds May 7, 2010 Surgical Management of Differentiated Thyroid Cancer Carmen C Solórzano, MD, FACS Associate Professor Endocrine and Surgical Oncology Vanderbilt
Thyroid US. Background: Thyroid/Neck US. Use of Office Ultrasound in the Thyroid Surgery Practice
 2010 UCSF Head and Neck Endocrine Surgery Course Use of Office Ultrasound in the Thyroid Surgery Practice Lisa A. Orloff, MD FACS Dept of Otolaryngology-Head and Neck Surgery University of California,
2010 UCSF Head and Neck Endocrine Surgery Course Use of Office Ultrasound in the Thyroid Surgery Practice Lisa A. Orloff, MD FACS Dept of Otolaryngology-Head and Neck Surgery University of California,
CAP Cancer Protocol and ecc Summary of Changes for August 2014 Thyroid Agile Release
 CAP Cancer Protocol and ecc Summary of Changes for August 2014 Thyroid Agile Release 2 REVISION HISTORY Date Author / Editor Comments 5/19/2014 Jaleh Mirza Created the document 8/12/2014 Samantha Spencer/Jaleh
CAP Cancer Protocol and ecc Summary of Changes for August 2014 Thyroid Agile Release 2 REVISION HISTORY Date Author / Editor Comments 5/19/2014 Jaleh Mirza Created the document 8/12/2014 Samantha Spencer/Jaleh
Thyroid Gland. Protocol applies to all malignant tumors of the thyroid gland, except lymphomas.
 Thyroid Gland Protocol applies to all malignant tumors of the thyroid gland, except lymphomas. Procedures Cytology (No Accompanying Checklist) Partial Thyroidectomy Total Thyroidectomy With/Without Lymph
Thyroid Gland Protocol applies to all malignant tumors of the thyroid gland, except lymphomas. Procedures Cytology (No Accompanying Checklist) Partial Thyroidectomy Total Thyroidectomy With/Without Lymph
Long-term Follow-up for Patients with Papillary Thyroid Carcinoma Treated as Benign Nodules
 Long-term Follow-up for Patients with Papillary Thyroid Carcinoma Treated as Benign Nodules YASUHIRO ITO, TAKUYA HIGASHIYAMA, YUUKI TAKAMURA, AKIHIRO MIYA, KAORU KOBAYASHI, FUMIO MATSUZUKA, KANJI KUMA
Long-term Follow-up for Patients with Papillary Thyroid Carcinoma Treated as Benign Nodules YASUHIRO ITO, TAKUYA HIGASHIYAMA, YUUKI TAKAMURA, AKIHIRO MIYA, KAORU KOBAYASHI, FUMIO MATSUZUKA, KANJI KUMA
Ultrasound-Guided Fine-Needle Aspiration of Thyroid Nodules: New events
 Ultrasound-Guided Fine-Needle Aspiration of Thyroid Nodules: New events Sandrine Rorive, M.D., PhD. Erasme Hospital - Université Libre de Bruxelles (ULB) INTRODUCTION The assessment of thyroid nodules
Ultrasound-Guided Fine-Needle Aspiration of Thyroid Nodules: New events Sandrine Rorive, M.D., PhD. Erasme Hospital - Université Libre de Bruxelles (ULB) INTRODUCTION The assessment of thyroid nodules
Thyroid Neoplasm. ORL-Head and neck Surgery 2014
 In The Name of God Thyroid Neoplasm ORL-Head and neck Surgery 2014 Malignant Neoplasm By age 90, virtually everyone has nodules Estimates of cancer prevalence at autopsy 4% to 36% Why these lesions are
In The Name of God Thyroid Neoplasm ORL-Head and neck Surgery 2014 Malignant Neoplasm By age 90, virtually everyone has nodules Estimates of cancer prevalence at autopsy 4% to 36% Why these lesions are
Review Article Management of papillary and follicular (differentiated) thyroid carcinoma-an update
 thyroid carcinoma-an update") Bangladesh J Otorhinolaryngol 2010; 16(2): 126-130 Review Article Management of papillary and follicular (differentiated) thyroid carcinoma-an update Md. Abdul Mobin Choudhury 1, Md. Abdul Alim Shaikh
Bangladesh J Otorhinolaryngol 2010; 16(2): 126-130 Review Article Management of papillary and follicular (differentiated) thyroid carcinoma-an update Md. Abdul Mobin Choudhury 1, Md. Abdul Alim Shaikh
Thyroid and Adrenal Gland
 Thyroid and Adrenal Gland NAACCR 2011 2012 Webinar Series 12/1/11 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
Thyroid and Adrenal Gland NAACCR 2011 2012 Webinar Series 12/1/11 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
Research Article Papillary Thyroid Cancer, Macrofollicular Variant: The Follow-Up and Analysis of Prognosis of 5 Patients
 yroid Research, Article ID 818134, 4 pages http://dx.doi.org/10.1155/2014/818134 Research Article Papillary Thyroid Cancer, Macrofollicular Variant: The Follow-Up and Analysis of Prognosis of 5 Patients
yroid Research, Article ID 818134, 4 pages http://dx.doi.org/10.1155/2014/818134 Research Article Papillary Thyroid Cancer, Macrofollicular Variant: The Follow-Up and Analysis of Prognosis of 5 Patients
Case Scenario 1: Thyroid
 Case Scenario 1: Thyroid History and Physical Patient is an otherwise healthy 80 year old female with the complaint of a neck mass first noticed two weeks ago. The mass has increased in size and is palpable.
Case Scenario 1: Thyroid History and Physical Patient is an otherwise healthy 80 year old female with the complaint of a neck mass first noticed two weeks ago. The mass has increased in size and is palpable.
An Alphabet Soup of Thyroid Neoplasms
 Overall Objectives An Alphabet Soup of Thyroid Neoplasms Lester D. R. Thompson www.lester-thompson.com What is the current management of papillary carcinoma? What are the trends and what can we do differently?
Overall Objectives An Alphabet Soup of Thyroid Neoplasms Lester D. R. Thompson www.lester-thompson.com What is the current management of papillary carcinoma? What are the trends and what can we do differently?
What you need to know about Thyroid Cancer
 What you need to know about Thyroid Cancer This booklet has been designed to help you to learn more about your thyroid cancer. It covers the most important areas and answers some of the frequently asked
What you need to know about Thyroid Cancer This booklet has been designed to help you to learn more about your thyroid cancer. It covers the most important areas and answers some of the frequently asked
Case-Based Discussion of Thyroid Cancer Therapy
 Case-Based Discussion of Thyroid Cancer Therapy Matthew D. Ringel, MD Ralph W. Kurtz Chair and Professor of Medicine Director, Division of Endocrinology The Ohio State University Co-Leader, Molecular Biology
Case-Based Discussion of Thyroid Cancer Therapy Matthew D. Ringel, MD Ralph W. Kurtz Chair and Professor of Medicine Director, Division of Endocrinology The Ohio State University Co-Leader, Molecular Biology
B. Environmental Factors. a. The major risk factor to papillary thyroid cancer is exposure to ionizing radiation, during the first 2 decades of life.
 B. Environmental Factors. a. The major risk factor to papillary thyroid cancer is exposure to ionizing radiation, during the first 2 decades of life. b. Deficiency of dietary iodine: - Is linked with a
B. Environmental Factors. a. The major risk factor to papillary thyroid cancer is exposure to ionizing radiation, during the first 2 decades of life. b. Deficiency of dietary iodine: - Is linked with a
Overview. Extraglandular Thyroid Lymphatics. Management of the Lateral Neck in Well-Differentiated Thyroid Carcinoma. David W. Eisele, M.D., F.A.C.S.
 Management of the Lateral Neck in Well-Differentiated Thyroid Carcinoma David W. Eisele, M.D., F.A.C.S. Head and Neck Surgery and Oncology U.C.S.F. Comprehensive Cancer Center University of California,
Management of the Lateral Neck in Well-Differentiated Thyroid Carcinoma David W. Eisele, M.D., F.A.C.S. Head and Neck Surgery and Oncology U.C.S.F. Comprehensive Cancer Center University of California,
A variation in recurrence patterns of papillary thyroid cancer with disease progression: A long-term follow-up study
 ORIGINAL ARTICLE A variation in recurrence patterns of papillary thyroid cancer with disease progression: A long-term follow-up study Joon-Hyop Lee, MD, Yoo Seung Chung, MD, PhD,* Young Don Lee, MD, PhD
ORIGINAL ARTICLE A variation in recurrence patterns of papillary thyroid cancer with disease progression: A long-term follow-up study Joon-Hyop Lee, MD, Yoo Seung Chung, MD, PhD,* Young Don Lee, MD, PhD
(Not so) New Guidelines for Management of Thyroid Nodules and Differentiated Thyroid Cancer Minnesota/Midwest Chapter of AACE
 New Guidelines for Management of Thyroid Nodules and Differentiated Thyroid Cancer Minnesota/Midwest Chapter of AACE") (Not so) New Guidelines for Management of Thyroid Nodules and Differentiated Thyroid Cancer Minnesota/Midwest Chapter of AACE Bryan R. Haugen, MD University of Colorado, School of Medicine Outline Some
(Not so) New Guidelines for Management of Thyroid Nodules and Differentiated Thyroid Cancer Minnesota/Midwest Chapter of AACE Bryan R. Haugen, MD University of Colorado, School of Medicine Outline Some
Papillary Thyroid Microcarcinoma Presenting as Horner s Syndrome: A Novel Clinical Presentation
 Case Report American Journal of Cancer Case Reports http://ivyunion.org/index.php/ajccr/ Page 1 of 6 Papillary Thyroid Microcarcinoma Presenting as Horner s Syndrome: A Novel Clinical Presentation Ammara
Case Report American Journal of Cancer Case Reports http://ivyunion.org/index.php/ajccr/ Page 1 of 6 Papillary Thyroid Microcarcinoma Presenting as Horner s Syndrome: A Novel Clinical Presentation Ammara
Distant and Lymph Node Metastases of Thyroid Nodules with No Pathological Evidence of Malignancy: A Limitation of Pathological Examination
 Endocrine Journal 2008, 55 (5), 889 894 Distant and Lymph Node Metastases of Thyroid Nodules with No Pathological Evidence of Malignancy: A Limitation of Pathological Examination YASUHIRO ITO, TOMONORI
Endocrine Journal 2008, 55 (5), 889 894 Distant and Lymph Node Metastases of Thyroid Nodules with No Pathological Evidence of Malignancy: A Limitation of Pathological Examination YASUHIRO ITO, TOMONORI
Well-differentiated Thyroid Cancer. Anton Sharapov, R4
 Well-differentiated Thyroid Cancer Anton Sharapov, R4 Outline Types of DTC Diagnosis of DTC Treatment options Extent of surgery Follow up cases A bit of history Theodore Kocher, Bern, Switzerland 1872,
Well-differentiated Thyroid Cancer Anton Sharapov, R4 Outline Types of DTC Diagnosis of DTC Treatment options Extent of surgery Follow up cases A bit of history Theodore Kocher, Bern, Switzerland 1872,
Changing trends in the management of well-differentiated thyroid carcinoma in Korea
 2016, 63 (6), 515-521 Original Changing trends in the management of well-differentiated thyroid carcinoma in Korea Yong Sang Lee, Hang-Seok Chang and Cheong Soo Park Thyroid Cancer Center, Department of
2016, 63 (6), 515-521 Original Changing trends in the management of well-differentiated thyroid carcinoma in Korea Yong Sang Lee, Hang-Seok Chang and Cheong Soo Park Thyroid Cancer Center, Department of
Clinical and Molecular Approach to Using Thyroid Needle Biopsy for Nodular Disease
 Clinical and Molecular Approach to Using Thyroid Needle Biopsy for Nodular Disease Robert L. Ferris, MD, PhD Department of Otolaryngology/Head and Neck Surgery and Yuri E. Nikiforov, MD, PhD Division of
Clinical and Molecular Approach to Using Thyroid Needle Biopsy for Nodular Disease Robert L. Ferris, MD, PhD Department of Otolaryngology/Head and Neck Surgery and Yuri E. Nikiforov, MD, PhD Division of
Managing Thyroid Microcarcinomas
 Review Article http://dx.doi.org/10.3349/ymj.2012.53.1.1 pissn: 0513-5796, eissn: 1976-2437 Yonsei Med J 53(1):1-14, 2012 Managing Thyroid Microcarcinomas Ernest L. Mazzaferri Division of Endocrinology,
Review Article http://dx.doi.org/10.3349/ymj.2012.53.1.1 pissn: 0513-5796, eissn: 1976-2437 Yonsei Med J 53(1):1-14, 2012 Managing Thyroid Microcarcinomas Ernest L. Mazzaferri Division of Endocrinology,
Clinical Guidance in Thyroid Cancers. Stephen Robinson Imperial at St Mary s On behalf of BTA
 Clinical Guidance in Thyroid Cancers Stephen Robinson Imperial at St Mary s On behalf of BTA Background to thyroid cancer Incidence probably increasing slowly 1971-95; 2.3 women 0.9 men /100,000 2001;
Clinical Guidance in Thyroid Cancers Stephen Robinson Imperial at St Mary s On behalf of BTA Background to thyroid cancer Incidence probably increasing slowly 1971-95; 2.3 women 0.9 men /100,000 2001;
Advances in the management of thyroid cancer
 International Journal of Surgery (2005) 3, 213e220 www.int-journal-surgery.com REVIEW Advances in the management of thyroid cancer Ashok R. Shaha* Memorial Sloan-Kettering Cancer Center, 1275 York Avenue,
International Journal of Surgery (2005) 3, 213e220 www.int-journal-surgery.com REVIEW Advances in the management of thyroid cancer Ashok R. Shaha* Memorial Sloan-Kettering Cancer Center, 1275 York Avenue,
TBSRTC 1- Probabilistic approach and Relationship to Clinical Algorithms
 The Benefits of a Uniform Reporting System for Thyroid Cytopathology BETHESDA REPORTING SYSTEM Prof. Fernando Schmitt Department of Pathology and Oncology, Medical Faculty of Porto University Head of Molecular
The Benefits of a Uniform Reporting System for Thyroid Cytopathology BETHESDA REPORTING SYSTEM Prof. Fernando Schmitt Department of Pathology and Oncology, Medical Faculty of Porto University Head of Molecular
MTP: Thyroid Nodules
 Canadian Endocrine Update MTP: Thyroid Nodules Deric Morrison MD, FRCP, ECNU Assistant Professor, Division of Endocrinology and Metabolism, Western University April 2014 Faculty/Presenter Disclosure Faculty:
Canadian Endocrine Update MTP: Thyroid Nodules Deric Morrison MD, FRCP, ECNU Assistant Professor, Division of Endocrinology and Metabolism, Western University April 2014 Faculty/Presenter Disclosure Faculty:
USGFNA of thyroid nodules
 US Guided FNA (USGFNA) of neck masses INTERVENTIONAL HEAD & NECK ULTRASOUND Brendan C. Stack, Jr., MD., FACS, FACE Professor Otolaryngology-Head and Neck Surgery Indications Technique Interpretation Results
US Guided FNA (USGFNA) of neck masses INTERVENTIONAL HEAD & NECK ULTRASOUND Brendan C. Stack, Jr., MD., FACS, FACE Professor Otolaryngology-Head and Neck Surgery Indications Technique Interpretation Results
A Review of Differentiated Thyroid Cancer
 A Review of Differentiated Thyroid Cancer April 21 st, 2016 FPON Webcast Jonn Wu BMSc MD FRCPC Radiation Oncologist, Vancouver Centre Chair, Provincial H&N Tumour Group, BCCA Clinical Associate Professor,
A Review of Differentiated Thyroid Cancer April 21 st, 2016 FPON Webcast Jonn Wu BMSc MD FRCPC Radiation Oncologist, Vancouver Centre Chair, Provincial H&N Tumour Group, BCCA Clinical Associate Professor,
42 yr old male with h/o Graves disease and prior I 131 treatment presents with hyperthyroidism and undetectable TSH. 2 hr uptake 20%, 24 hr uptake 50%
 Pinhole images of the neck are acquired in multiple projections, 24hrs after the oral administration of approximately 200 µci of I123. Usually, 24hr uptake value if also calculated (normal 24 hr uptake
Pinhole images of the neck are acquired in multiple projections, 24hrs after the oral administration of approximately 200 µci of I123. Usually, 24hr uptake value if also calculated (normal 24 hr uptake
Exercise 15: CSv2 Data Item Coding Instructions ANSWERS
 Exercise 15: CSv2 Data Item Coding Instructions ANSWERS CS Tumor Size Tumor size is the diameter of the tumor, not the depth or thickness of the tumor. Chest x-ray shows 3.5 cm mass; the pathology report
Exercise 15: CSv2 Data Item Coding Instructions ANSWERS CS Tumor Size Tumor size is the diameter of the tumor, not the depth or thickness of the tumor. Chest x-ray shows 3.5 cm mass; the pathology report