THROID ABNORMALITIES AMIR ZIAEE
|
|
|
- Emery Thompson
- 5 years ago
- Views:
Transcription

1 THROID ABNORMALITIES AMIR ZIAEE 1


2 Thyroid Hormone Synthesis Table Characteristics of Circulating T4 and T3 Hormone Property T4 T3 Serum concentrations Total hormone 8 μg/dl 0.14 μg/dl Fraction of total hormone in the free form 0.02% 0.3% Free hormone M M Serum half-life 7 d 0.75 d Fraction directly from the thyroid 100% 20% Production rate, including peripheral conversion 90 μg/d 32 μg/d Intracellular hormone fraction ~20% ~70% Relative metabolic potency Receptor binding M M SOURCES OF T3 Thyroid gland %20 Peripheral tissue T4 to T3 Conversion %80 2
3 Factors thet impair peripheral conversion of T4 to T3 Physiological Pathologic pharmacologic Fetal and early neonatal life Old age? Fasting,malnutrition Hepatic or renal dysfunction Systemic illness Trauma,postoperative state Drugs ( PTU,glucocurticoids,propranolol,amiodarone) Oral cholecystographic agents MAJOR PLASMA CARRIER PROTEINS FOR TYROID HORMONES Thyroxine-binding globulin(tbg) Transthyretin (prealbumin) Albumin 3
4 Factors associated with altered binding of T4 by TBG Increased binding Pregnancy Neonatal state Estogens Tamoxifen OCP Acute intermittent porphyria Infectious and chronia active hepatitis Biliary cirrhosis Genetic factors Perphenazine HIV infection Decreased binding Androgens Large doses of glucocurticoids Active acromegaly Nephrotic syndrome Major systemic illness Genetic factors asparginase Hypothyroidism 4
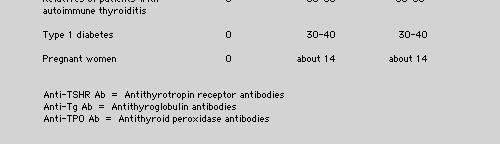
5 Causes of hypothyroidism Primary Chronic autoimmune thyroiditisgoitrous & atrophic forms Radiation Surgery Infiltrative disease(amyloidosis,sclerodermia) Iodine deficiency Biosynthetic defect Drugs (lithium,iodine,contrast agents) Secondary Pituitary disease Hypothalamic disease Incidence of hypothyroidism* Female 40/10,000 Male 6/10,000 Prevalence of Hypothyroidism* Female %9.3 Male %1.3 *2779 people in UK with a medium age of 58 years Whickham survey 1995 Thyroid autoimmunity Suseptibility factors Humoral lfactors Cell mediated factors 5


6 6
 The facies in pituitary myxedema is often characterized by skin of normal thickness, covered by fine wrinkles. Puffiness is usually less than in primary myxedema. The eyelids are often edematous.")


7 Figure 9-3. (A) The classic torpid facies of severe myxedema in a man. The face appears puffy, and the eyelids are edematous. The skin is thickened and dry. (B) The facies in pituitary myxedema is often characterized by skin of normal thickness, covered by fine wrinkles. Puffiness is usually less than in primary myxedema. The eyelids are often edematous. The palpebral fissure may be narrwowed because of blepharoptosis, due to diminished tone of the sympathetic nervous fibers to Müller's levator palpebral superious muscle and is the opposite of the lid retraction seen in thyrotoxicosis. The modest measurable exophthalmos seen in some patients with myxedema is presumably related to accumulation of the same mucous edema in the orbit as is seen elsewhere. It is not progressive and carries no threat to vision, as in the ophthalmopathy of Graves' disease. The tongue is usually large, occasionally to the point of clumsiness. Sometimes a patient will complain of this problem. Sometimes it is smooth, as in pernicious anemia (of course, pernicious anemia may coexist). Patients do not usually complain of soreness of the tongue, as they may in pernicious anemia. When anemia is marked, the tongue may be pale, but more often it is red, in contrast to the pallid face. TSH and Free T4 TSH TSH TSH TSH Free T4 Free T4 Free T4 Free T4 Primary hypothyroidism Mild or Subclinical hypothyroidism Central hypo. NTI Drug effect Normal 7
8 Recommended Uses for TPOAb Measurement Diagnosis of Autoimmune Thyroid Disease. Risk factor for Autoimmune Thyroid Disease. Risk factor for hypothyroidism during Interferon alpha, Interleukin-2 or Lithium therapy. Risk factor for thyroid dysfunction during amiodarone therapy. Risk factor for hypothyroidism in Down s Syndrome patients. Risk factor for thyroid dysfunction during pregnancy and for post-partum thyroiditis. Risk factor for miscarriage and in-vitro fertilization failure. Central Hypothyroidism Imaging (R/O SOL) Functional status of the other axes Transient hypothyroidism Postpartum thyroiditis Subacute thyroiditis After withdrawal of thyroid hormone Therapy in euthyroid patients Following I131 treatment for Graves disease Removal of toxic adenoma or subtotal thyroidectomy for Graves disease 8
9 Subclinical hypothyroidism Unlike patients with overt hypothyroidism, these patients have normal serum levels of T3 and T4 and only mildly elevated serum TSH levels. Such patients are often identified through routine screening or in the course of an evaluation of common nonspecific symptoms or hypercholesterolemia. Subclinical hypothyroidism The worldwide prevalence of subclinical hypothyroidism ranges from 1 to 10 percent; the highest age- and sex-specific rates are in women older than 60 years of age, approaching 20 percent in some reports Up to 75 percent of patients have only mildly elevated serum thyrotropin values (5 to 10 mu per liter), and 50 to 80 percent of patients have positive tests for antibodies against thyroperoxidase, depending on the age, sex, and serum thyrotropin levels. 9
10 It is prudent to keep TSH values in the lower normal range( mu/l), and to avoid TSH levels of <0.1 mu/l Special treatment situation Elderly patients Underlying CAD Pregnancy Concomitant drug administration Surgical patients Increased L-T4 dose requirement Decreased intestinal absorption of T4 Malabsorption(e.g.celiac disease,short bowel syn.) Dietary fiber supplements Drugs:colestipol,colestyramine,sucralfate,aluminium hydroxide,ferrus sulfate Increased need for T4 Weigt gain,pregnancy,estrogens Increased clearance for T4 Phenobarbital,phenytoin,carbamazepin,rifampin Precise mechanism unknown sertraline,chloroquine,lovastatin 10
11 Risk of a suppressed TSH Effects on Bone Mass Cardiac Effects Bone effects Overt thyrotoxicosis is associated with increased bone turne over and negative calcium balance Significant bone loss in postmenopausal(but not in premenopausal) women at the lumbar spine(effect size 0.348,95% 95%CI to 0.202) and the femoral neck(effect size 0.276,95% CI o.470 to 0.089) The detrimental effect appeared more marked on cortical than on trabecular There is little evidence from retrospective studies of an actual increase in Fx incidence Cardiac effects Increased heart rate Atrial fibrillation, 3-fold greater risk of Af over the next decade in thyrotoxic 60-year- olds Increase in myocardial contractility Impaired diastolic relaxation and ventricular filling Modest increase in LV wall thickness 11
12 NTI The global pattern of changes in thyroid physiology that occur durig illness. NTI Low T3 due to inhibition of 5`-monodeiodinase Reverse T3 Low T4 due to reduced protein binding and circulating inhibitors of binding Pituitary thyroid axis Effects of drugs Modifications of thyroid-related hormones during fasting or illness Severity of illness Mild FT4 FT3 rt3 TSH Normal Reduced up to %50 Increased up to twofold Increased up to severalfold Normal Moderate Increased Reduced up Increased up to Normal to %90 Severe Reduced Almost undetectable Variable Reduced 12


13 NTI Thyroid function should not be assesed in seriously ill patients t unless ther is a strong suspicion of thyroid dysfunction Relationship Between Total T4 & T3 In Various Disorders T4 T3 Low Normal.Iodine deficiency.t3 treatment.antithyroid drug therapy.t3- thyrotoxicosis.t3-binding autoantibodies.thyrotoxicosis of any cause.excess T4 ingestion.tbg excess.thr 13


14 Relationship Between total T4 & T3 In Various disorders T4 T3 low Normal.Iodine deficiency.t3 treatment.hypothyroidism.t4 treatment.euthyroid hyprethyroxinemia.thyrotoxicosis with acute or moderate NTI Relationship Between Total T4 & T3 In Various Disorders T4 T3 Low Normal Low.Severe hypo..acute &.Thyrotoxicosis.TBG chronic NTI with severe NTI deficiency.drugs.drugs.fetal life.severe NTI.Restricted nutrition 14
15 TSH 43 (TSH), or thyrotropin : a glycoprotein synthesized and secreted by : the thyrotropes Molecular weight : about 28,000 Structure : composed of two subunits, a and ß Alpha subunit : identical to alpha subunit of FSH, LH, HCG Both subunits are necessary for biological activity. 44 TSH : no carrier protein TSH : unaffected by changes (such as liver or kidney failure, estrogens, and androgens) in proteins that are known to affect thyroid hormone carrier proteins 45 15
16 Secretion : pulsatile with a diurnal rhythm. more than half of pulses occur between 10 PM and 4 AM. Average TSH levels l : 1.6 ± 0.6 mu/l, with: peak values of 3.1 ± 1.3 mu/l at approximately 2 AM and trough values of 0.7 ± 0.3 mu/l at about 4 PM. 46 Third-generation assays have three major advantages over second-generation assays: (1) help distinguish TSH suppression in hyperthyroid patients with coexistent illness from suppression in euthyroid patients with nonthyroidal illness; (2) allow the precise titration of thyroid hormone suppressive therapy; and (3) can distinguish the severity of subclinical hyperthyroidism. 47 TSH Reference Ranges Serum TSH values : higher in neonates and children. Mean euthyroid TSH values: approximate to 1.5 miu/l, (range 0.3 to 4.0 miu/l in iodine-sufficient populations) 48 16
17 Clinical situations associated with subnormal TSH values 49 Clinical situations associated with subnormal TSH values thyroid hormone excess endogenous hyperthyroidism or excess exogenous thyroid hormone points the activation of the negative feedback loop. Prolonged excessive thyroid hormone physiological "atrophy" of the thyroid stimulatory limb of the hypothalamic-pituitary thyroid axis. Thus several months are usually required for the reestablishment of TSH secretion after the relief of thyrotoxicosis. After excess thyroid hormone treatment after the transient hyperthyroidism associated with subacute or some variants of autoimmune thyroiditis Shorter suppression Severe illness 50 Clinical situations associated with subnormal TSH values -dose glucocorticoids Exogenous dopamine Pharmacological amounts of retinoids Points Acutely but not chronically In critically ill patients, this effect of dopamine can be superimposed on the suppressive effects of acute illness on thyroid function, reducing T4 production to even lower levels. Dopamine is sufficiently potent to suppress TSH to normal levels in sick patients with primary hypothyroidism. severe central hypothyroidism associated with very low serum TSH concentration has been reported in patients with cutaneous T-cell lymphoma treated with high-dose retinoid X receptor-selective ligand able to suppress TSH secretion
18 hcg acute psychosis depression agitated psychoses Congenital central hypothyroidism a thyroid stimulator; In normal pregnancy as a slightly subnormal TSH during the first trimester ( mu/l) ; frank, though mild, hyperthyroidism in patients with choriocarcinoma or molar pregnancy. may have high thyroid hormone levels and suppressed or elevated TSH values. Etiology,unkown low serum TSH; may result from mutations affecting TSH alpha gene or the Pit-1 gene 52 Interpretation of TSH and FT4 Results Low Normal Hyperthyroidism (pm mol/l) 4 FT Normal Euthyroidism Low Primary hypothyroidism TSH (miu/l) Interpretation of TSH and FT4 Results Low Normal (pm mmol/l) 4 FT Hyperthyroidism Euthyroid sick syndrome T4 autoantibodies Thyroid hormone resistance syndrome TSH-secreting pituitary adenoma Normal Subclinical Euthyroidism hyperthyroidism T3 thyrotoxicosis Pregnancy (first trimester) Drugs (eg. Glucocorticoids, dopamine, amiodarone) Thyroid hormone resistance syndrome TSH-secreting pituitary adenoma Subclinical (compensated) hypothyroidism Low Central hypothyroidism Central hypothyroidism Euthyroid sick syndrome (more severe, uncommon) Primary hypothyroidism TSH (miu/l) 18
19 Clinical situations associated with elevated TSH values 55 Clinical situations associated with elevated TSH values Points Primary hypothyroidism Iodine deficiency The serum free T4 is low normal or reduced but the serum free T3 values remain normal until the level of thyroid function has markedly deteriorated. Western Europe, South America, Africa and Asia. during the recovery phase after a severe illness A transient effect ; In such patients a "reawakening" of the hypothalamic-pituitary thyroid axis occurs with the improvement in their clinical state. 56 The remainder of the conditions associated with an elevated TSH are extremely rare : partial or complete TSH resistance inactivating point mutations of the TSH receptor gene. In a patient who has an elevated serum FT4, the presence of TSH at normal or increased levels should lead to a search for either resistance to thyroid hormone or a thyrotroph tumor. Hypothalamic-pituitary normal or even modest increases in TSH are explained by the lack of normal dysfunction TSH glycosylation in the TRH-deficient patient. The diagnosis is generally made by finding a serum free T4 index which is reduced to a greater extent than expected from the coincident serum TSH. either elevated or suppressed TSH, Psychiatric illness but the abnormal values are not usually in the range normally associated with symptomatic thyroid 57 dysfunction 19
20 Addison's disease The effect of glucocorticoids to suppress TSH secretion; TSH may be slightly elevated in the absence of primary thyroid disease. the presence of endogenous antimouse gamma globulin antibodies These antibodies, like TSH, can complex the two TSH antibodies resulting in artificially elevated serum TSH assay results in euthyroid patients; forming false bridges between the solid phase and signal antibodies. 58 Clinical situations in which measurements of serum thyrotropin alone may yeild misleading resuls condition Serum TSH Consequences of clinical action based on serum TSH value alone Serum Free T4 (if measured) Heterophil Abs N Failure to Dx thyrotoxicosis Central hypothyroidism TSH-secreting pit. Adenoma Thyroid hormone resistance Poor compliance with T4 therapy Delayed recovery of TSH secretion * TSH may be high in these conditions N* Failure to Dx hypothyroidism and investigate hypoth.-pit. Structure and function N* Failure to Dx thyrotoxicosis and investigate pit. Structure and function N* Failure to recognize the condition Inappropriate increase in dose of T4 N or low Failure to Dx impending hypothyroidism Low low59 Clinical Use of Tg Methods 60 20
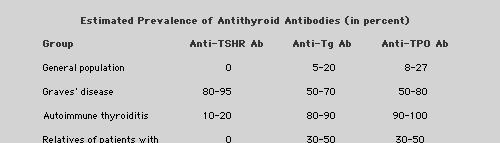
21 Decreased thyroglobulin concentration TSH mediated Absent or decreased synthesis Thyroid hormone replacement Supraphysiologic doses of thyroid hormone Scarcity of thyroid tissue Congenital athyrosis Total thyroidectomy Thyroglobulin synthesis defects 61 Increased thyroglobulin concentration TSH mediated Acute and transient TSH administration Protirelin (TRH) administration Neonatal period (1-96 hours postpartum) Chronic stimulation Iodine deficiency Endemic goiter Goitrogens Reduced thyroid reserve Thyroxinebinding globulin deficiency Resistance to thyroid hormone Non-TSH mediated Substances with TSH-like bioactivity Thyroid-stimulating immunoglobulin in autoimmune (Graves') disease Chorionic gonadotropins trophoblastic disease Pregnancy Abnormal release Autonomous toxic nodules Solitary nontoxic nodules Multinodular goiter Subacute thyroiditis (early phase) Differentiated nonmedullary thyroid carcinoma Neonatal period Direct trauma to the thyroid gland Percutaneous needle aspiration Thyroid or parathyroid surgery Iodine-131 therapy Abnormal clearance Renal failure 62 PREVALENCE OF THYROID AUTOANTIBODIES AND THEIR ROLE IN IMMUNOPATHOLOGY Antibody General Population Graves' Disease Hypothyroid Autoimmune Thyroiditis Role in Immunopathology Anti Tg 3% 12% to 30% 35% to 60% None Anti TPO 10% to 15% 45% to 80% 80% to 99% Complement fixing?significance Anti-TSH receptor 1% to 2%[ 70% to 100% 6% to 60% Stimulate or block the TSH receptor Anti-Na+ /Isymporter 0% 20% 25% 50% to 70% impair I- uptake by symporter in vitro 21
22 Antibody Antithyroglobulin Clear Indication Serial thyroglobulin estimations for thyroid cancer Possible Indication Antithyroid peroxidase Diagnosis of Graves' disease Diagnosis of chronic autoimmune thyroiditis in patients with primary thyroid failure Predicting risk of hypothyroidism when TSH alone is elevated Predicting postpartum thyroiditis in at-risk women Differentiation between transient thyrotoxicosis owing to lymphocytic or subacute thyroiditis Diagnosis of chronic autoimmune thyroiditis in euthyroid patients with goiter or nodules Prediction of hypothyroidism in at-risk groups Antibody Anti-TSH receptor antibodies (TBII) Anti-TSH receptor antibodies by bioassay: stimulating (TSAb) or blocking (TSBAb) Clear Indication To distinguish postpartum thyroiditis from Graves' disease in postpartum thyrotoxicosis Predicting risk of fetal/neonatal thyrotoxicosis in women with previous ablative treatment for Graves' disease or current thionamide therapy Possible Indication In diagnosing euthyroid Graves' ophthalmopathy (TSAb more sensitive) To determine duration of therapy and risk of recurrence in patients receiving thionamide therapy for Graves' disease (especially children) In diagnosing euthyroid Graves' ophthalmopathy To predict transient hypothyroidism (TSBAb) When increased sensitivity in the detection of anti-tsh receptor antibodies is required Advantages and Disadvantages of Different Methods for Measurement of Autoantibodies to TPO and Tg Technique Precision Sensitivity Specificity Cost Immunofluor- escence Hemaggutin- ation ELIZA Low Low Variable Low Low Variable Low Radioassay Low 22
23 Introduction In the 1950s, only one thyroid test was available an indirect estimate of the serum total (free + protein-bound) ti d)thyroxin (TT4) concentration ti Since 1970, radioimmunoassay (RIA) and immunometric assay (IMA) improved the specificity and sensitivity of the methods Thyroid assay Total Hormone Measurements (TT4 and TT3) Total Hormone Measurements (TT4 and TT3) Technically, easier methods to measure TT4 and TT3 (nanomolar) FT4 and FT3 (picomolar) Serum TT4 measurement (four decades) : 1970s: RIA methods Currently: immunometric assay (IMA) Signals: Radioactivity Fluorescence Chemiluminescent enzymes 23
24 Total Hormone Measurements (TT4 and TT3) Total T4 reference have approximated 58 to 160 nmol/l ( µg/dl) for more than two decades. TT3 reference values are also method dependent, with ranges approximating to nmol/l ( ng/dl) Free Hormone Tests (FT4 and FT3) Free Hormone Tests (FT4 and FT3) free hormone hypothesis: free fraction of hormone is responsible for the biologic activity of thyroid hormones at the cellular level 24
25 Free Hormone Tests (FT4 and FT3) Index Methods Free T4 Index (FT4I) Free T3 Index (FT3I) Absolute Methods Equilibrium Dialysis Ultrafiltration Gel Filtration/Adsorption chromatography Comparative Immunoassays Two-Step labeled Hormone One-step Labeled Hormone Analog Labeled Antibody Index Methods (FT4I and FT3I) require two separate measurements: TT4 or TT3 Thyroid Hormone Binding Ratio (THBR) or "Uptake test Free Hormone Indexes (FT4I and FT3I): simple calculations approximation of the free hormone concentration in the presence of abnormal binding proteins estimate free hormone concentrations: 40 y PRINCIPAL DRUGS THAT DISPLACE T4 FROM THYROXINE- BINDING GLOBULIN IN NORMAL HUMAN SERUM Drugs Salicylates Acetyl salicylic acid Salicyl salicyclic acid Furosemide Fenclofenac Mefenamic acid Flufenamic acid Diclofenac Difunisal Phenytoin Carbamazepine Mean Percent Increase in Free T4 Fraction 62 >




26 The Heparin Artifact The effect of heparin in increasing serum free T4 is an important in vitro phenomenon that can lead to spuriously high estimates of circulating free T4 26


27 TBG excess T4 x T3RU = FT4I T3 x T3RU = FT3I TBG deficiency T4 x T3RU = FT4I T3 x T3RU = FT3I 27


28 Hyperthyroidism T4 x T3RU = FT4I T3 x T3RU = FT3I Hypothyroidism T4 x T3RU = FT4I T3 x T3RU = FT3I Questions? 28
Clinical evaluation of. Thyroid function tests
 In the name of God Dr.m.omidi Endocrinologist Assistant stant professor of medicine 25 APR 2012 Clinical evaluation of Thyroid function tests Goal of TFT Evaluation of function of thyroid Monitoring
In the name of God Dr.m.omidi Endocrinologist Assistant stant professor of medicine 25 APR 2012 Clinical evaluation of Thyroid function tests Goal of TFT Evaluation of function of thyroid Monitoring
LABORATORY TESTS FOR EVALUATION OF THYROID DISORDERS
 LABORATORY TESTS FOR EVALUATION OF THYROID DISORDERS Maryam Tohidi Anatomical & clinical pathologist Research Institute for Endocrine Sciences THYROID GLAND (15-25 gr), (12-20 gr), 2 lobes connected by
LABORATORY TESTS FOR EVALUATION OF THYROID DISORDERS Maryam Tohidi Anatomical & clinical pathologist Research Institute for Endocrine Sciences THYROID GLAND (15-25 gr), (12-20 gr), 2 lobes connected by
Chapter I.A.1: Thyroid Evaluation Laboratory Testing
 Chapter I.A.1: Thyroid Evaluation Laboratory Testing Jennifer L. Poehls, MD and Rebecca S. Sippel, MD, FACS THYROID FUNCTION TESTS Overview Thyroid-stimulating hormone (TSH) is produced by the anterior
Chapter I.A.1: Thyroid Evaluation Laboratory Testing Jennifer L. Poehls, MD and Rebecca S. Sippel, MD, FACS THYROID FUNCTION TESTS Overview Thyroid-stimulating hormone (TSH) is produced by the anterior
Sanjay B. Dixit, M.D. BHS Endocrinology Associates November 11, 2017
 Sanjay B. Dixit, M.D. BHS Endocrinology Associates November 11, 2017 I will not be discussing this Outline of discussion Laboratory tests for thyroid function Diagnosis of hypothyroidism Treatment of
Sanjay B. Dixit, M.D. BHS Endocrinology Associates November 11, 2017 I will not be discussing this Outline of discussion Laboratory tests for thyroid function Diagnosis of hypothyroidism Treatment of
Pitfalls of TFTs Interpretation
 Mohammad Reza Bakhtiari DCLS, PhD Pitfalls of TFTs Interpretation CME July 2006 Vol.24 No.7, http://keck.usc.edu HPT axis physiology Log-linear relationship between TSH and FT4 Patient Specific Set Point
Mohammad Reza Bakhtiari DCLS, PhD Pitfalls of TFTs Interpretation CME July 2006 Vol.24 No.7, http://keck.usc.edu HPT axis physiology Log-linear relationship between TSH and FT4 Patient Specific Set Point
Thyroid Function TSH Analyte Information
 Thyroid Function TSH Analyte Information 1 2013-05-01 Thyroid-stimulating hormone (TSH) Introduction Thyroid-stimulating hormone (thyrotropin, TSH) is a glycoprotein with molecular weight of approximately
Thyroid Function TSH Analyte Information 1 2013-05-01 Thyroid-stimulating hormone (TSH) Introduction Thyroid-stimulating hormone (thyrotropin, TSH) is a glycoprotein with molecular weight of approximately
Understanding Thyroid Labs
 Understanding Thyroid Labs Chris Sadler, MA, PA-C, CDE, DFAAPA Senior Medical Science Liaison CVM Janssen Scientific Affairs Diabetes and Endocrine Associates La Jolla, CA Disclosures Employee of Janssen
Understanding Thyroid Labs Chris Sadler, MA, PA-C, CDE, DFAAPA Senior Medical Science Liaison CVM Janssen Scientific Affairs Diabetes and Endocrine Associates La Jolla, CA Disclosures Employee of Janssen
Index. Graves disease, 111 thyroid autoantigens, 110 Autoimmune thyroiditis, 11, 58, 180, 181. B Bamforth Lazarus syndrome, 27
 Index A Adrenergic activation, 77 Allan Herndon Dudley syndrome, 31 Ambulatory practice choice of test, 156, 157 screening general population, thyroid dysfunction, 163, 164 targeted population, 164 167
Index A Adrenergic activation, 77 Allan Herndon Dudley syndrome, 31 Ambulatory practice choice of test, 156, 157 screening general population, thyroid dysfunction, 163, 164 targeted population, 164 167
B-Resistance to the action of hormones, Hormone resistance characterized by receptor mediated, postreceptor.
 Disorders of the endocrine system 38 Disorders of endocrine system mainly are caused by: A-Deficiency or an excess of a single hormone or several hormones: - deficiency :can be congenital or acquired.
Disorders of the endocrine system 38 Disorders of endocrine system mainly are caused by: A-Deficiency or an excess of a single hormone or several hormones: - deficiency :can be congenital or acquired.
Table 1: Thyroid panel. Result (reference interval) TSH 89.5 miu/l ( ) Total T4 5.2 µg/dl ( ) T3 uptake 39% (22-35)
 TSH 89.5 miu/l ( ) Total T4 5.2 µg/dl ( ) T3 uptake 39% (22-35)") Introduction Thyroid disease is the second most common endocrine disorder (behind diabetes), and its prevalence increases with increasing age. The incidence of newly diagnosed thyroid cancer is increasing
Introduction Thyroid disease is the second most common endocrine disorder (behind diabetes), and its prevalence increases with increasing age. The incidence of newly diagnosed thyroid cancer is increasing
THYROID HORMONES: An Overview
 1 SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES DISCIPLINE OF BIOCHEMISTRY AND MOLECULAR BIOLOGY PBL SEMINAR MBBS III; BMLS & BDS Year 3 What are the Thyroid Hormones? THYROID
1 SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES DISCIPLINE OF BIOCHEMISTRY AND MOLECULAR BIOLOGY PBL SEMINAR MBBS III; BMLS & BDS Year 3 What are the Thyroid Hormones? THYROID
Endocrine part two. Presented by Dr. Mohammad Saadeh The requirements for the Clinical Chemistry Philadelphia University Faculty of pharmacy
 Endocrine part two Presented by Dr. Mohammad Saadeh The requirements for the Clinical Chemistry Philadelphia University Faculty of pharmacy Cushing's disease: increased secretion of adrenocorticotropic
Endocrine part two Presented by Dr. Mohammad Saadeh The requirements for the Clinical Chemistry Philadelphia University Faculty of pharmacy Cushing's disease: increased secretion of adrenocorticotropic
Decoding Your Thyroid Tests and Results
 Decoding Your Thyroid Tests and Results Wondering about your thyroid test results? Learn about each test and what low, optimal, and high results may mean so you can work with your doctor to choose appropriate
Decoding Your Thyroid Tests and Results Wondering about your thyroid test results? Learn about each test and what low, optimal, and high results may mean so you can work with your doctor to choose appropriate
Hypothalamo-Pituitary-Thyroid Axis
 SMGr up Hypothalamo-Pituitary-Thyroid Axis Orluwene Chituru Godwill 1 * and Ohiri John U 1 1 Chemical Pathology Department, University of Port Harcourt Teaching Hospital, Nigeria *Corresponding author:
SMGr up Hypothalamo-Pituitary-Thyroid Axis Orluwene Chituru Godwill 1 * and Ohiri John U 1 1 Chemical Pathology Department, University of Port Harcourt Teaching Hospital, Nigeria *Corresponding author:
The interpretation and management of thyroid disorders
 Journal of Endocrinology, Metabolism and Diabetes of South Africa 2015 ; 20(2) http://dx.doi.org/10.1080/16089677.2015.1056468 Open Access article distributed under the terms of the Creative Commons License
Journal of Endocrinology, Metabolism and Diabetes of South Africa 2015 ; 20(2) http://dx.doi.org/10.1080/16089677.2015.1056468 Open Access article distributed under the terms of the Creative Commons License
Diseases of thyroid & parathyroid glands (1 of 2)
") Diseases of thyroid & parathyroid glands (1 of 2) Thyroid diseases Thyrotoxicosis Hypothyroidism Thyroiditis Graves disease Goiters Neoplasms Chronic Lymphocytic (Hashimoto) Thyroiditis Subacute Granulomatous
Diseases of thyroid & parathyroid glands (1 of 2) Thyroid diseases Thyrotoxicosis Hypothyroidism Thyroiditis Graves disease Goiters Neoplasms Chronic Lymphocytic (Hashimoto) Thyroiditis Subacute Granulomatous
Thyroid Disease. I have no disclosures. Overview TSH. Matthew Kim, M.D. July, 2012
 Thyroid Disease I have no disclosures Matthew Kim, M.D. July, 2012 Overview Thyroid Function Tests Hyperthyroidism Hypothyroidism Subclinical Thyroid Disease Thyroid Nodules Questions TSH Best single screening
Thyroid Disease I have no disclosures Matthew Kim, M.D. July, 2012 Overview Thyroid Function Tests Hyperthyroidism Hypothyroidism Subclinical Thyroid Disease Thyroid Nodules Questions TSH Best single screening
university sciences of Isfahan university Com
 Introduce R. Gholamnezhad Lecturer of school of nursing & midwifery of Iran university Ph.D student tof Immunology, Sh School of medical sciences of Isfahan university E-Mail: Gholami278@gmail. Com Interpreting
Introduce R. Gholamnezhad Lecturer of school of nursing & midwifery of Iran university Ph.D student tof Immunology, Sh School of medical sciences of Isfahan university E-Mail: Gholami278@gmail. Com Interpreting
Approach to thyroid dysfunction
 Approach to thyroid dysfunction Alice Y.Y. Cheng, MD, FRCPC Twitter: @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or
Approach to thyroid dysfunction Alice Y.Y. Cheng, MD, FRCPC Twitter: @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or
Grave s disease (1 0 )
") THYROID DYSFUNCTION Grave s disease (1 0 ) Autoimmune - activating AB s to TSH receptor High concentrations of circulating thyroid hormones Weight loss, tachycardia, tiredness Diffuse goitre - TSH stimulating
THYROID DYSFUNCTION Grave s disease (1 0 ) Autoimmune - activating AB s to TSH receptor High concentrations of circulating thyroid hormones Weight loss, tachycardia, tiredness Diffuse goitre - TSH stimulating
THYROID HORMONES & THYROID FUNCTION TESTS
 THYROID HORMONES & THYROID FUNCTION TESTS SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES DISCIPLINE OF BIOCHEMISTRY AND MOLECULAR BIOLOGY CLINICAL BIOCHEMISTRY LECTURE BMLS III
THYROID HORMONES & THYROID FUNCTION TESTS SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES DISCIPLINE OF BIOCHEMISTRY AND MOLECULAR BIOLOGY CLINICAL BIOCHEMISTRY LECTURE BMLS III
None. Thyroid Potpourri for the Primary Care Physician. Evaluating Thyroid Function. Disclosures. Learning Objectives
 Thyroid Potpourri for the Primary Care Physician Ramya Vedula DO, MPH, ECNU Endocrinology, Diabetes and Metabolism Princeton Medical Group Assistant Professor of Clinical Medicine Rutgers Robert Wood Johnson
Thyroid Potpourri for the Primary Care Physician Ramya Vedula DO, MPH, ECNU Endocrinology, Diabetes and Metabolism Princeton Medical Group Assistant Professor of Clinical Medicine Rutgers Robert Wood Johnson
Sample Type - Serum Result Reference Range Units. Central Thyroid Regulation Surrey & Activity KT3 4Q. Peripheral Thyroid D Function mark
 Thyroid Plus Sample Type - Serum Result Reference Range Units Central Thyroid Regulation Surrey & Activity KT3 4Q Total Thyroxine (T4)
Thyroid Plus Sample Type - Serum Result Reference Range Units Central Thyroid Regulation Surrey & Activity KT3 4Q Total Thyroxine (T4)
Hyperthyroidism Diagnosis and Treatment. April Janet A. Schlechte, M.D.
 Hyperthyroidism Diagnosis and Treatment Family Practice Refresher Course April 2015 Janet A. Schlechte, M.D. Disclosure of Financial Relationships Janet A. Schlechte, M.D. has no relationships with any
Hyperthyroidism Diagnosis and Treatment Family Practice Refresher Course April 2015 Janet A. Schlechte, M.D. Disclosure of Financial Relationships Janet A. Schlechte, M.D. has no relationships with any
C. Thyrotropin/Thyroid Stimulating Hormone (TSH)
") C. Thyrotropin/Thyroid Stimulating Hormone (TSH) For more than twenty-five years, TSH methods have been able to detect the TSH elevations that are characteristic of primary hypothyroidism. Modern-day TSH
C. Thyrotropin/Thyroid Stimulating Hormone (TSH) For more than twenty-five years, TSH methods have been able to detect the TSH elevations that are characteristic of primary hypothyroidism. Modern-day TSH
Requesting and Management of abnormal TFTs.
 Requesting and Management of abnormal TFTs. At the request of a number of GPs I have produced summary guidelines surrounding thyroid testing. These have been agreed with our Endocrinology leads Dr Bell
Requesting and Management of abnormal TFTs. At the request of a number of GPs I have produced summary guidelines surrounding thyroid testing. These have been agreed with our Endocrinology leads Dr Bell
OUTLINE. Regulation of Thyroid Hormone Production Common Tests to Evaluate the Thyroid Hyperthyroidism - Graves disease, toxic nodules, thyroiditis
 THYROID DISEASE OUTLINE Regulation of Thyroid Hormone Production Common Tests to Evaluate the Thyroid Hyperthyroidism - Graves disease, toxic nodules, thyroiditis OUTLINE Hypothyroidism - Hashimoto s thyroiditis,
THYROID DISEASE OUTLINE Regulation of Thyroid Hormone Production Common Tests to Evaluate the Thyroid Hyperthyroidism - Graves disease, toxic nodules, thyroiditis OUTLINE Hypothyroidism - Hashimoto s thyroiditis,
Thyroid and Antithyroid Drugs. Munir Gharaibeh, MD, PhD, MHPE Faculty of Medicine April 2014
 Thyroid and Antithyroid Drugs Munir Gharaibeh, MD, PhD, MHPE Faculty of Medicine April 2014 Anatomy and histology of the thyroid gland Located in neck adjacent to the 5 th cervical vertebra (C5). Composed
Thyroid and Antithyroid Drugs Munir Gharaibeh, MD, PhD, MHPE Faculty of Medicine April 2014 Anatomy and histology of the thyroid gland Located in neck adjacent to the 5 th cervical vertebra (C5). Composed
Pathophysiology of Thyroid Disorders. PHCL 415 Hadeel Alkofide April 2010
 Pathophysiology of Thyroid Disorders PHCL 415 Hadeel Alkofide April 2010 1 Learning Objectives Understand the pathophysiology of hyperthyroidism & hypothyroidism Describe the signs & symptoms of hyperthyroidism
Pathophysiology of Thyroid Disorders PHCL 415 Hadeel Alkofide April 2010 1 Learning Objectives Understand the pathophysiology of hyperthyroidism & hypothyroidism Describe the signs & symptoms of hyperthyroidism
Lecture title. Name Family name Country
 Lecture title Name Family name Country Nguyen Thy Khue, MD, PhD Department of Endocrinology HCMC University of Medicine and Pharmacy, MEDIC Clinic Hochiminh City, Viet Nam Provided no information regarding
Lecture title Name Family name Country Nguyen Thy Khue, MD, PhD Department of Endocrinology HCMC University of Medicine and Pharmacy, MEDIC Clinic Hochiminh City, Viet Nam Provided no information regarding
Thyroid Plus. Central Thyroid Regulation & Activity. Peripheral Thyroid Function. Thyroid Auto Immunity. Key Guide. Patient: DOB: Sex: F MRN:
 Thyroid Plus Patient: DOB: Sex: F MRN: Order Number: Completed: Received: Collected: Sample Type - Serum Result Reference Range Units Central Thyroid Regulation & Activity Total Thyroxine (T4) 127 127
Thyroid Plus Patient: DOB: Sex: F MRN: Order Number: Completed: Received: Collected: Sample Type - Serum Result Reference Range Units Central Thyroid Regulation & Activity Total Thyroxine (T4) 127 127
Laboratory assessment of thyroid function. Nahid Shirazian MD. Internist, Endocrinologist
 Laboratory assessment of thyroid function Nahid Shirazian MD. Internist, Endocrinologist Physiology Thyroid gland produces Thyroxine Converted to active form T3 in tissue Scattered dc cells within ihi
Laboratory assessment of thyroid function Nahid Shirazian MD. Internist, Endocrinologist Physiology Thyroid gland produces Thyroxine Converted to active form T3 in tissue Scattered dc cells within ihi
4) Thyroid Gland Defects - Dr. Tara
 Thyroid Gland Defects - Dr. Tara") 4) Thyroid Gland Defects - Dr. Tara Thyroid Pituitary Axis TRH secreted in the hypothalamus stimulates production and Secretion of TSH TSH stimulates secretion of T3, T4 T4 has negative feedback on secretion
4) Thyroid Gland Defects - Dr. Tara Thyroid Pituitary Axis TRH secreted in the hypothalamus stimulates production and Secretion of TSH TSH stimulates secretion of T3, T4 T4 has negative feedback on secretion
Thyroid gland defects. Dr. Tara Husain
 Thyroid gland defects Dr. Tara Husain Thyroid Pituitary Axis TRH secreted in the hypothalamus stimulates production and Secretion of TSH TSH stimulates secretion of T3,T4 T4 has negative feed back on secretion
Thyroid gland defects Dr. Tara Husain Thyroid Pituitary Axis TRH secreted in the hypothalamus stimulates production and Secretion of TSH TSH stimulates secretion of T3,T4 T4 has negative feed back on secretion
Hyperthyroidism. Objectives. Clinical Manifestations. Slide 1. Slide 2. Slide 3. Implications for Primary Care. hyperthyroidism
 1 Hyperthyroidism Implications for Primary Care Laura A. Ruby, DNP, CRNP Wellspan Endocrinology 2 Objectives! Discuss the clinical manifestations of hyperthyroidism! Review the use of the diagnostic studies!
1 Hyperthyroidism Implications for Primary Care Laura A. Ruby, DNP, CRNP Wellspan Endocrinology 2 Objectives! Discuss the clinical manifestations of hyperthyroidism! Review the use of the diagnostic studies!
Disorders of the Thyroid Gland
 Disorders of the Thyroid Gland István Takács MD., PhD, 1st Department of Medicine, Semmelweis University Connection to the dentistry: close to each other higher operation risk radiating pain macroglossia
Disorders of the Thyroid Gland István Takács MD., PhD, 1st Department of Medicine, Semmelweis University Connection to the dentistry: close to each other higher operation risk radiating pain macroglossia
Thyrotoxicosis in Pregnancy: Diagnose and Management
 Thyrotoxicosis in Pregnancy: Diagnose and Management Yuanita Asri Langi email: meralday@yahoo.co.id Endocrinology & Metabolic Division, Internal Medicine Department, Prof.dr.R.D. Kandou Hospital/ Sam Ratulangi
Thyrotoxicosis in Pregnancy: Diagnose and Management Yuanita Asri Langi email: meralday@yahoo.co.id Endocrinology & Metabolic Division, Internal Medicine Department, Prof.dr.R.D. Kandou Hospital/ Sam Ratulangi
The Number Games and Thyroid Function Arshia Panahloo Consultant Endocrinologist St George s Hospital
 The Number Games and Thyroid Function Arshia Panahloo Consultant Endocrinologist St George s Hospital Presentation Today: Common thyroid problems and treatments Pregnancy related thyroid problems The suppressed
The Number Games and Thyroid Function Arshia Panahloo Consultant Endocrinologist St George s Hospital Presentation Today: Common thyroid problems and treatments Pregnancy related thyroid problems The suppressed
Disorders of Thyroid Function
 Disorders of Thyroid Function Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Thyroid Hormone Axis Hypothalamus TRH
Disorders of Thyroid Function Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Thyroid Hormone Axis Hypothalamus TRH
HYPERTHYROIDISM. Hypothalamus. Thyrotropin-releasing hormone (TRH) Anterior pituitary gland. Thyroid-stimulating hormone (TSH) Thyroid gland T4, T3
 Anterior pituitary gland. Thyroid-stimulating hormone (TSH) Thyroid gland T4, T3") HYPERTHYROIDISM Hypothalamus Thyrotropin-releasing hormone (TRH) Anterior pituitary gland Thyroid-stimulating hormone (TSH) Thyroid gland T4, T3 In hyperthyroidism, there is an increased production of
HYPERTHYROIDISM Hypothalamus Thyrotropin-releasing hormone (TRH) Anterior pituitary gland Thyroid-stimulating hormone (TSH) Thyroid gland T4, T3 In hyperthyroidism, there is an increased production of
Hypothyroidism. Definition:
 Definition: Hypothyroidism Primary hypothyroidism is characterized biochemically by a high serum thyroidstimulating hormone (TSH) concentration and a low serum free thyroxine (T4) concentration. Subclinical
Definition: Hypothyroidism Primary hypothyroidism is characterized biochemically by a high serum thyroidstimulating hormone (TSH) concentration and a low serum free thyroxine (T4) concentration. Subclinical
Alvin C. Powers, M.D. 1/27/06
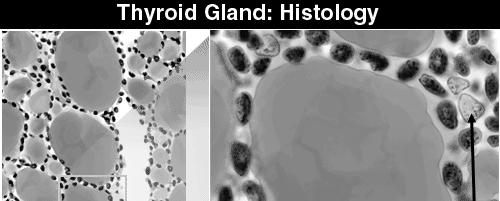
 Thyroid Histology Follicular Cells ECF side Apical lumen Thyroid Follicles -200-400 um Parafollicular or C-cells Colloid Photos from University of Manchester and tutorial created by Dr. James Crimando,
Thyroid Histology Follicular Cells ECF side Apical lumen Thyroid Follicles -200-400 um Parafollicular or C-cells Colloid Photos from University of Manchester and tutorial created by Dr. James Crimando,
Thyroid disorders. Dr Enas Abusalim
 Thyroid disorders Dr Enas Abusalim Thyroid physiology The hypothalamic pituitary thyroid axis And peripheral conversion of T4 to T3, WHERE, AND BY WHAT ENZYME?? Only relatively small concentrations of
Thyroid disorders Dr Enas Abusalim Thyroid physiology The hypothalamic pituitary thyroid axis And peripheral conversion of T4 to T3, WHERE, AND BY WHAT ENZYME?? Only relatively small concentrations of
Euthyroid sick syndrome
 Euthyroid sick syndrome Background Euthyroid sick syndrome can be described as abnormal findings on thyroid function tests that occur in the setting of a nonthyroidal illness (NTI) without preexisting
Euthyroid sick syndrome Background Euthyroid sick syndrome can be described as abnormal findings on thyroid function tests that occur in the setting of a nonthyroidal illness (NTI) without preexisting
TANJA KEMP INTERNAL MEDICINE: ENDOCRINOLOGY
 ENDOCRINE DISORDERS IN THE ELDERLY (part 2) TANJA KEMP INTERNAL MEDICINE: ENDOCRINOLOGY Pituitary axis Target organs of the pituitary gland Negative feedback Hypothalamus-Pituitary-Thyroid axis Thyroid
ENDOCRINE DISORDERS IN THE ELDERLY (part 2) TANJA KEMP INTERNAL MEDICINE: ENDOCRINOLOGY Pituitary axis Target organs of the pituitary gland Negative feedback Hypothalamus-Pituitary-Thyroid axis Thyroid
Thyroid Disorders Towards a Healthy Endocrine System
 Thyroid Disorders Towards a Healthy Endocrine System What are Thyroid Disorders? The thyroid is a butterfly-shaped gland in the middle of the lower neck. Through the release of hormones, the thyroid regulates
Thyroid Disorders Towards a Healthy Endocrine System What are Thyroid Disorders? The thyroid is a butterfly-shaped gland in the middle of the lower neck. Through the release of hormones, the thyroid regulates
03-Dec-17. Thyroid Disorders GOITRE. Grossly enlarged thyroid - in hypothyroidism in hyperthyroidism - production of anatomical symptoms
 Thyroid Disorders GOITRE Grossly enlarged thyroid - in hypothyroidism in hyperthyroidism - production of anatomical symptoms 1 Physiological Goiter load on thyroid supply of I - limited stress due to:
Thyroid Disorders GOITRE Grossly enlarged thyroid - in hypothyroidism in hyperthyroidism - production of anatomical symptoms 1 Physiological Goiter load on thyroid supply of I - limited stress due to:
California Association for Medical Laboratory Technology
 California Association for Medical Laboratory Technology Distance Learning Program Thyroid Hormones and Thyroid Diseases Course # DL-967 by Helen Sowers, M.A., CLS Dept. of Biological Science (retired)
California Association for Medical Laboratory Technology Distance Learning Program Thyroid Hormones and Thyroid Diseases Course # DL-967 by Helen Sowers, M.A., CLS Dept. of Biological Science (retired)
Challenging TFTs (Definition)
") Thyroid Function Tests (Interpretation Challenges) Mohammad Reza Bakhtiari, DCLS, PhD 1/80 Challenging TFTs (Definition) Discordant Results vs. Clinical Picture Inharmonious Results 2/80 1 Challenging
Thyroid Function Tests (Interpretation Challenges) Mohammad Reza Bakhtiari, DCLS, PhD 1/80 Challenging TFTs (Definition) Discordant Results vs. Clinical Picture Inharmonious Results 2/80 1 Challenging
Thyroid Function. Thyroid Antibodies. Analyte Information
 Thyroid Function Thyroid Antibodies Analyte Information - 1-2013-04-30 Thyroid Antibodies Determination of thyroid autoantibodies are, besides TSH and FT4, one of the most important diagnostic parameters.
Thyroid Function Thyroid Antibodies Analyte Information - 1-2013-04-30 Thyroid Antibodies Determination of thyroid autoantibodies are, besides TSH and FT4, one of the most important diagnostic parameters.
DISORDERS OF THE THYROID GLAND SIGNS, SYMPTOMS, & TREATMENT ENDOCRINE SYSTEM AT A GLANCE OBJECTIVES ANATOMY OF THE THYROID
 OBJECTIVES DISORDERS OF THE THYROID GLAND SIGNS, SYMPTOMS, & TREATMENT Stephanie Blackburn, MHS, MLS(ASCP) CM LSU Health Shreveport Clinical Laboratory Science Program Discuss the synthesis and action
OBJECTIVES DISORDERS OF THE THYROID GLAND SIGNS, SYMPTOMS, & TREATMENT Stephanie Blackburn, MHS, MLS(ASCP) CM LSU Health Shreveport Clinical Laboratory Science Program Discuss the synthesis and action
Thyroid Screen (Serum)
") Thyroid Screen (Serum) Patient: DOB: Sex: F MRN: Order Number: Completed: Received: Collected: Sample Type - Serum Result Reference Range Units Central Thyroid Regulation & Activity Total Thyroxine (T4)
Thyroid Screen (Serum) Patient: DOB: Sex: F MRN: Order Number: Completed: Received: Collected: Sample Type - Serum Result Reference Range Units Central Thyroid Regulation & Activity Total Thyroxine (T4)
Quality Control and Interpretation of Laboratory. Nursing and Midwifery. Dr. M. Navidhamidi
 Quality Control and Interpretation of Laboratory Tests of Thyroid Hormones for Nursing and Midwifery Dr. M. Navidhamidi Tehran University of Medical Sciences ١ Physiopathology of Thyroid Gland ٢ Thyroid
Quality Control and Interpretation of Laboratory Tests of Thyroid Hormones for Nursing and Midwifery Dr. M. Navidhamidi Tehran University of Medical Sciences ١ Physiopathology of Thyroid Gland ٢ Thyroid
Icd 10 low tsh level. Icd 10 low tsh level. Search
 Search Icd 10 low tsh level Icd 10 low tsh level 1-10-2012 The 2012 updates to the Current Procedural Terminology 4th Edition (CPT-4) and Healthcare Common Procedure Coding System (HCPCS) National Level
Search Icd 10 low tsh level Icd 10 low tsh level 1-10-2012 The 2012 updates to the Current Procedural Terminology 4th Edition (CPT-4) and Healthcare Common Procedure Coding System (HCPCS) National Level
Mastering Thyroid Disorders. Douglas C. Bauer, MD UCSF Division of General Internal Medicine
 Mastering Thyroid Disorders Douglas C. Bauer, MD UCSF Division of General Internal Medicine Cases 68 yr old female with new atrial fibrillation and no other findings except TSH=0.04, normal free T4 79
Mastering Thyroid Disorders Douglas C. Bauer, MD UCSF Division of General Internal Medicine Cases 68 yr old female with new atrial fibrillation and no other findings except TSH=0.04, normal free T4 79
Icd 10 low tsh level. Cari untuk: Cari Cari
 Cari untuk: Cari Cari Icd 10 low tsh level AMMONIUM PERCHLORATE is a white, crystalline solid or powder. Classified as a division 1.1 explosive if powdered into particles smaller than 15 microns in diameter
Cari untuk: Cari Cari Icd 10 low tsh level AMMONIUM PERCHLORATE is a white, crystalline solid or powder. Classified as a division 1.1 explosive if powdered into particles smaller than 15 microns in diameter
Dharma Lindarto Div. Endokrin-Metabolisme dan Diabetes. Dep Ilmu Penyakit Dalam FK USU / RSUP HAM Medan
 HYPERTHYROIDISM Dharma Lindarto Div. Endokrin-Metabolisme dan Diabetes. Dep Ilmu Penyakit Dalam FK USU / RSUP HAM Medan Anatomy of the Thyroid Gland Tiroid Disease Multi N Aspect fungtion morphology eutiroid,
HYPERTHYROIDISM Dharma Lindarto Div. Endokrin-Metabolisme dan Diabetes. Dep Ilmu Penyakit Dalam FK USU / RSUP HAM Medan Anatomy of the Thyroid Gland Tiroid Disease Multi N Aspect fungtion morphology eutiroid,
Thyroid and Antithyroid Drugs. Dr. Alia Shatanawi Feb,
 Thyroid and Antithyroid Drugs Dr. Alia Shatanawi Feb, 24 2014 Anatomy and histology of the thyroid gland Located in neck adjacent to the 5 th cervical vertebra (C5). Composed of epithelial cells which
Thyroid and Antithyroid Drugs Dr. Alia Shatanawi Feb, 24 2014 Anatomy and histology of the thyroid gland Located in neck adjacent to the 5 th cervical vertebra (C5). Composed of epithelial cells which
Understanding thyroid function tests. Dr. Colette George
 Understanding thyroid function tests Dr. Colette George Disclosures No financial disclosure I will present fictitious cases and thyroid function tests (TFTs) that are based on scenarios I commonly encounter.
Understanding thyroid function tests Dr. Colette George Disclosures No financial disclosure I will present fictitious cases and thyroid function tests (TFTs) that are based on scenarios I commonly encounter.
An Approach to: Thyroid Function Tests. Rinkoo Dalan Consultant Department of Endocrinology Tan Tock Seng Hospital
 An Approach to: Thyroid Function Tests Rinkoo Dalan Consultant Department of Endocrinology Tan Tock Seng Hospital Regulation of Thyroid axis Hypothalamus TRH T3,T4 ---- TRH Median Eminence (base of brain)
An Approach to: Thyroid Function Tests Rinkoo Dalan Consultant Department of Endocrinology Tan Tock Seng Hospital Regulation of Thyroid axis Hypothalamus TRH T3,T4 ---- TRH Median Eminence (base of brain)
LABORATORY MEDICINE PRACTICE GUIDELINES Laboratory Support for the Diagnosis and Monitoring of Thyroid Disease
 Table of Contents LABORATORY MEDICINE PRACTICE GUIDELINES Laboratory Support for the Diagnosis and Monitoring of Thyroid Disease Section I. Forward and Introduction Section 2. Pre-analytic factors Section
Table of Contents LABORATORY MEDICINE PRACTICE GUIDELINES Laboratory Support for the Diagnosis and Monitoring of Thyroid Disease Section I. Forward and Introduction Section 2. Pre-analytic factors Section
Hypothyroidism. Causes. Diagnosis. Christopher Theberge
 Hypothyroidism Pronunciations: (Hypothyroidism) Hypothyroidism (under active thyroid) is a condition where the thyroid gland fails to secrete enough of the thyroid hormones thyroxine (T4) and triiodothyronine
Hypothyroidism Pronunciations: (Hypothyroidism) Hypothyroidism (under active thyroid) is a condition where the thyroid gland fails to secrete enough of the thyroid hormones thyroxine (T4) and triiodothyronine
BELIEVE MIDWIFERY SERVICES
 TITLE: THYROID DISEASE IN PREGNANCY EFFECTIVE DATE: July, 2013 POLICY STATEMENT: Pregnancy changes significantly the values influenced by the serum thyroid binding hormone level (i.e., total thyroxine,
TITLE: THYROID DISEASE IN PREGNANCY EFFECTIVE DATE: July, 2013 POLICY STATEMENT: Pregnancy changes significantly the values influenced by the serum thyroid binding hormone level (i.e., total thyroxine,
Pregnancy & Thyroid. Zohreh Moosavi Associate professor of Endocriology Imam Reza General Hospital Mashad University. Imam Reza weeky Conferance
 Pregnancy & Thyroid Zohreh Moosavi Associate professor of Endocriology Imam Reza General Hospital Mashad University Imam Reza weeky Conferance Objectives Thyroid Disorders & Pregnancy Normal thyroid phsyiology
Pregnancy & Thyroid Zohreh Moosavi Associate professor of Endocriology Imam Reza General Hospital Mashad University Imam Reza weeky Conferance Objectives Thyroid Disorders & Pregnancy Normal thyroid phsyiology
Update In Hyperthyroidism
 Update In Hyperthyroidism CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi Copyright
Update In Hyperthyroidism CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi Copyright
HYPOTHYROIDISM IN CHILDREN. IAP UG Teaching slides
 HYPOTHYROIDISM IN CHILDREN 1 OBJECTIVES Introduction Congenital hypothyroidism Etiology, clinical features, diagnosis, approach, treatment and prognosis Acquired hypothyroidism Etiology, clinical features,
HYPOTHYROIDISM IN CHILDREN 1 OBJECTIVES Introduction Congenital hypothyroidism Etiology, clinical features, diagnosis, approach, treatment and prognosis Acquired hypothyroidism Etiology, clinical features,
Management of Common Thyroid Disorders
 Cases Management of Common Thyroid Disorders Douglas C. Bauer, MD UCSF Division of General Internal Medicine No Disclosures 68 yr old female with new atrial fibrillation and no other findings except TSH=0.04,
Cases Management of Common Thyroid Disorders Douglas C. Bauer, MD UCSF Division of General Internal Medicine No Disclosures 68 yr old female with new atrial fibrillation and no other findings except TSH=0.04,
Effect of thyroid hormones of metabolism Thyroid Diseases
 Effect of thyroid hormones of metabolism Thyroid Diseases Medical Perspective Aspects That Will Be Addressed Regulation of thyroid hormone secretion Basic physiology Hyperthyroidism Hypothyroidism Thyroiditis
Effect of thyroid hormones of metabolism Thyroid Diseases Medical Perspective Aspects That Will Be Addressed Regulation of thyroid hormone secretion Basic physiology Hyperthyroidism Hypothyroidism Thyroiditis
Update on Gestational Thyroid Disease. Aidan McElduff The Discipline of Medicine, The University of Sydney
 IADPSG 2016 Update on Gestational Thyroid Disease Aidan McElduff The Discipline of Medicine, The University of Sydney IADPSG 2016 DISCLOSURES and AIM Nil to disclose Aim: to provide an overview 2017 Guidelines
IADPSG 2016 Update on Gestational Thyroid Disease Aidan McElduff The Discipline of Medicine, The University of Sydney IADPSG 2016 DISCLOSURES and AIM Nil to disclose Aim: to provide an overview 2017 Guidelines
THYROID DISEASE IN CHILDREN
 THYROID DISEASE IN CHILDREN Michelle Schweiger, D.O. Center for Pediatric and Adolescent Endocrinology Cleveland Clinic Foundation Neither I nor any immediate family members have any financial interests
THYROID DISEASE IN CHILDREN Michelle Schweiger, D.O. Center for Pediatric and Adolescent Endocrinology Cleveland Clinic Foundation Neither I nor any immediate family members have any financial interests
Toxic MNG Thyroiditis 5-15
 Hyperthyroidism Facts Prevalence 0.5-1.0%, more common in women Thyrotoxicosis is excess thyroid hormones from endogenous or exogenous sources Hyperthyroidism is excess thyroid hormones from thyroid gland
Hyperthyroidism Facts Prevalence 0.5-1.0%, more common in women Thyrotoxicosis is excess thyroid hormones from endogenous or exogenous sources Hyperthyroidism is excess thyroid hormones from thyroid gland
Slide notes: This presentation provides information on Graves disease, a systemic autoimmune disease. Epidemiology, pathology, complications,
 1 This presentation provides information on Graves disease, a systemic autoimmune disease. Epidemiology, pathology, complications, including ophthalmic complications, treatments (both permanent solutions
1 This presentation provides information on Graves disease, a systemic autoimmune disease. Epidemiology, pathology, complications, including ophthalmic complications, treatments (both permanent solutions
Thyroid hormone. Functional anatomy of thyroid gland
 Thyroid hormone ส ว ฒณ ค ปต ว ฒ ต กจ ฑาธ ช ห อง 101 Aims Functional anatomy of thyroid gland Synthesis, secretion and metabolism of the thyroid hormones The mechanism of thyroid hormone action Role of
Thyroid hormone ส ว ฒณ ค ปต ว ฒ ต กจ ฑาธ ช ห อง 101 Aims Functional anatomy of thyroid gland Synthesis, secretion and metabolism of the thyroid hormones The mechanism of thyroid hormone action Role of
Thyroid Function. Thyroglobulin Analyte Information
 Thyroid Function Thyroglobulin Analyte Information - 1-2011-01-11 Thyroglobulin Introduction Thyroglobulin (Tg) is a big dimeric protein consisting of two identical subunits. It has 2,748 amino acids in
Thyroid Function Thyroglobulin Analyte Information - 1-2011-01-11 Thyroglobulin Introduction Thyroglobulin (Tg) is a big dimeric protein consisting of two identical subunits. It has 2,748 amino acids in
How to manage hypothyroid disease in pregnancy
 For mass reproduction, content licensing and permissions contact Dowden Health Media. FIRST OF 2 PARTS How to manage hypothyroid disease in pregnancy Pregnancy complicated by hypothyroidism puts mother
For mass reproduction, content licensing and permissions contact Dowden Health Media. FIRST OF 2 PARTS How to manage hypothyroid disease in pregnancy Pregnancy complicated by hypothyroidism puts mother
Thyroid Hormones (T 4 & T 3 )
") 1 Thyroid Hormones (T 4 & T 3 ) Normalize growth and development, body temperature, and energy levels. Used as thyroid replacement therapy in hypothyroidism. Thyroxine (T 4 ) is peripherally metabolized
1 Thyroid Hormones (T 4 & T 3 ) Normalize growth and development, body temperature, and energy levels. Used as thyroid replacement therapy in hypothyroidism. Thyroxine (T 4 ) is peripherally metabolized
DRUGS. 4- Two molecules of DIT combine within the thyroglobulinto form L-thyroxine (T4)' One molecule of MIT & one molecule of DIT combine to form T3
' One molecule of MIT & one molecule of DIT combine to form T3") THYROID HORMONEs & ANTITHYROID The thyroid secretes 2 types of hormones: DRUGS 1- Iodine containing amino acids (are important for growth, development and metabolism) and these are: triodothyronine, tetraiodothyronine,(
THYROID HORMONEs & ANTITHYROID The thyroid secretes 2 types of hormones: DRUGS 1- Iodine containing amino acids (are important for growth, development and metabolism) and these are: triodothyronine, tetraiodothyronine,(
HYPOTHYROIDISM AND HYPERTHYROIDISM
 HYPOTHYROIDISM AND HYPERTHYROIDISM SHAHIDA PERVEEN, AMBREEN Post RN BSCN Semester II FACULTY SIR RAJA April 13, 016 Objectives: State the functions of thyroid hormone. Understand the pathologic mechanism
HYPOTHYROIDISM AND HYPERTHYROIDISM SHAHIDA PERVEEN, AMBREEN Post RN BSCN Semester II FACULTY SIR RAJA April 13, 016 Objectives: State the functions of thyroid hormone. Understand the pathologic mechanism
Common Issues in Management of Hypothyroidism
 Common Issues in Management of Hypothyroidism Family Medicine Refresher Course April 5, 2018 Janet A. Schlechte, M.D. Disclosure of Financial Relationships Janet A. Schlechte, M.D. has no relationships
Common Issues in Management of Hypothyroidism Family Medicine Refresher Course April 5, 2018 Janet A. Schlechte, M.D. Disclosure of Financial Relationships Janet A. Schlechte, M.D. has no relationships
Management of Common Thyroid Disorders
 Management of Common Thyroid Disorders Douglas C. Bauer, MD UCSF Division of General Internal Medicine No Disclosures Cases 68 yr old woman with new atrial fibrillation and no other findings except TSH=0.04,
Management of Common Thyroid Disorders Douglas C. Bauer, MD UCSF Division of General Internal Medicine No Disclosures Cases 68 yr old woman with new atrial fibrillation and no other findings except TSH=0.04,
Back to the Basics: Thyroid Gland Structure, Function and Pathology
 Back to the Basics: Thyroid Gland Structure, Function and Pathology JANELLE M. CHIASERA LEARNING OBJECTIVES 1. Explain the HPT feedback system involving the thyroid gland. Include the hormone produced
Back to the Basics: Thyroid Gland Structure, Function and Pathology JANELLE M. CHIASERA LEARNING OBJECTIVES 1. Explain the HPT feedback system involving the thyroid gland. Include the hormone produced
Page 1. Understanding Common Thyroid Disorders. Cases. Topics Covered
 Cases Understanding Common Thyroid Disorders Douglas C. Bauer, MD UCSF Division of General Internal Medicine No Disclosures 66 yr old female with 1 yr of fatigue and lassitude and no findings except TSH=8.2,
Cases Understanding Common Thyroid Disorders Douglas C. Bauer, MD UCSF Division of General Internal Medicine No Disclosures 66 yr old female with 1 yr of fatigue and lassitude and no findings except TSH=8.2,
Pearls and Pitfalls of Thyroid Diagnosis. Todd W. Frieze, MD, FACP, FACE, ECNU, CCD Endocrine Care, Hattiesburg Clinic Biloxi MS
 Pearls and Pitfalls of Thyroid Diagnosis Todd W. Frieze, MD, FACP, FACE, ECNU, CCD Endocrine Care, Hattiesburg Clinic Biloxi MS Thyroid Anatomy Isthmus of gland located 1 fingerbreadth below cricoid cartilage
Pearls and Pitfalls of Thyroid Diagnosis Todd W. Frieze, MD, FACP, FACE, ECNU, CCD Endocrine Care, Hattiesburg Clinic Biloxi MS Thyroid Anatomy Isthmus of gland located 1 fingerbreadth below cricoid cartilage
Thyroid and Antithyroid Drugs
 Thyroid and Antithyroid Drugs Dr. Yunita Sari Pane, MSi Department of Pharmacology HYPOTHALAMIC PITUITARY THYROID AXIS T3 and T4 are synthesized in the thyroid gland. Inorganic iodine is trapped with great
Thyroid and Antithyroid Drugs Dr. Yunita Sari Pane, MSi Department of Pharmacology HYPOTHALAMIC PITUITARY THYROID AXIS T3 and T4 are synthesized in the thyroid gland. Inorganic iodine is trapped with great
Southern Derbyshire Shared Care Pathology Guidelines. Hyperthyroidism
 Southern Derbyshire Shared Care Pathology Guidelines Hyperthyroidism Purpose of Guideline The management and referral criteria of patients with newly diagnosed hyperthyroidism. Background Hyperthyroidism
Southern Derbyshire Shared Care Pathology Guidelines Hyperthyroidism Purpose of Guideline The management and referral criteria of patients with newly diagnosed hyperthyroidism. Background Hyperthyroidism
Underactive Thyroid. Diagnosis, Treatment & Controversies
 Underactive Thyroid Diagnosis, Treatment & Controversies Dr. Asif Malik Humayun Consultant Endocrinologist Milton Keynes University Hospital NHS Foundation Trust Thyroid Hormone Control of metabolism
Underactive Thyroid Diagnosis, Treatment & Controversies Dr. Asif Malik Humayun Consultant Endocrinologist Milton Keynes University Hospital NHS Foundation Trust Thyroid Hormone Control of metabolism
19th Century Thyroidology
 1 19th Century Thyroidology Dr. Kinnicutt s patient (1893) A cold, tired, constipated middle aged woman Slow pulse rate Low body temperature From physiology it was likely patient needed thyroid replacement
1 19th Century Thyroidology Dr. Kinnicutt s patient (1893) A cold, tired, constipated middle aged woman Slow pulse rate Low body temperature From physiology it was likely patient needed thyroid replacement
The department of Endocrinology and metabolism Huashan Hospital, Fudan University Dr. Hongying Ye
 The department of Endocrinology and metabolism Huashan Hospital, Fudan University Dr. Hongying Ye dryehongying@hotmail.com Main contents Basic knowledge of thyroid Overview of thyroid diseases Hyperthyroidism/Graves
The department of Endocrinology and metabolism Huashan Hospital, Fudan University Dr. Hongying Ye dryehongying@hotmail.com Main contents Basic knowledge of thyroid Overview of thyroid diseases Hyperthyroidism/Graves
NIH Public Access Author Manuscript Ther Drug Monit. Author manuscript; available in PMC 2013 April 14.
 NIH Public Access Author Manuscript Published in final edited form as: Ther Drug Monit. 2006 February ; 28(1): 8 11. Thyroid Function Testing in Pregnancy and Thyroid Disease: Trimester-specific Reference
NIH Public Access Author Manuscript Published in final edited form as: Ther Drug Monit. 2006 February ; 28(1): 8 11. Thyroid Function Testing in Pregnancy and Thyroid Disease: Trimester-specific Reference
Pathophysiology of the th E d n ocr i ne S S t ys em B. Marinov, MD, PhD Endocrine system Central: Hypothalamus
 Pathophysiology of the Endocrine System B. Marinov, MD, PhD Pathophysiology Department Medical University of Plovdiv Endocrine system Central: Hypothalamus Pituitary Pineal Peripheral Thymus Thyroid Parathyroid
Pathophysiology of the Endocrine System B. Marinov, MD, PhD Pathophysiology Department Medical University of Plovdiv Endocrine system Central: Hypothalamus Pituitary Pineal Peripheral Thymus Thyroid Parathyroid
Thyroid Disease. Scott D. Isaacs, MD, FACP, FACE HRT Symposium Savannah GA July 14 16, All Rights Reserved. 1
 Thyroid Disease Scott D. Isaacs, MD, FACP, FACE HRT Symposium Savannah GA July 14 16, 2016 2016. All Rights Reserved. 1 Disclosure Scott D. Isaacs, MD, FACP, FACE, is the Medical Director at Atlanta Center
Thyroid Disease Scott D. Isaacs, MD, FACP, FACE HRT Symposium Savannah GA July 14 16, 2016 2016. All Rights Reserved. 1 Disclosure Scott D. Isaacs, MD, FACP, FACE, is the Medical Director at Atlanta Center
Hyperthyroidism, Inflammatory Disorders
 Hyperthyroidism, Inflammatory Disorders free T4 Howard J. Sachs, MD www.12daysinmarch.com Hyperthyroidism, Inflammatory Disorders The total T4 may be elevated in pregnancy and with OCP use Graves I 123
Hyperthyroidism, Inflammatory Disorders free T4 Howard J. Sachs, MD www.12daysinmarch.com Hyperthyroidism, Inflammatory Disorders The total T4 may be elevated in pregnancy and with OCP use Graves I 123
Pathology. Hyperthyroidism (Overactive Thyroid), Graves Disease (Basedow Disease) and more. Definitions. See online here
, Graves Disease (Basedow Disease) and more. Definitions. See online here") Pathology Hyperthyroidism (Overactive Thyroid), Graves Disease (Basedow Disease) and more See online here Hyperthyroidism is caused by the excess of thyroid hormones T3 and T4. Graves disease is the most
Pathology Hyperthyroidism (Overactive Thyroid), Graves Disease (Basedow Disease) and more See online here Hyperthyroidism is caused by the excess of thyroid hormones T3 and T4. Graves disease is the most
Thyroid disorder for Resident
 Thyroid disorder for Resident Chaicharn Deerochanawong M.D. Diabetes and Endocrinology Unit Department of Medicine Rajavithi Hospital, Ministry of Public Health Topics Abnormal thyroid function test Euthyroid
Thyroid disorder for Resident Chaicharn Deerochanawong M.D. Diabetes and Endocrinology Unit Department of Medicine Rajavithi Hospital, Ministry of Public Health Topics Abnormal thyroid function test Euthyroid
Disclosures. Learning objectives. Case 1A. Autoimmune Thyroid Disease: Medical and Surgical Issues. I have nothing to disclose.
 Disclosures Autoimmune Thyroid Disease: Medical and Surgical Issues I have nothing to disclose. Chrysoula Dosiou, MD, MS Clinical Assistant Professor Division of Endocrinology Stanford University School
Disclosures Autoimmune Thyroid Disease: Medical and Surgical Issues I have nothing to disclose. Chrysoula Dosiou, MD, MS Clinical Assistant Professor Division of Endocrinology Stanford University School
Thyroid function testing in pregnancy: 2017 ATA guidelines update. Dr Simon Forehan
 Thyroid function testing in pregnancy: 2017 ATA guidelines update Dr Simon Forehan Several factors are known to tax gravid thyroid economy: Increased plasma volume TBG pool increased Renal clearance Feto-placental
Thyroid function testing in pregnancy: 2017 ATA guidelines update Dr Simon Forehan Several factors are known to tax gravid thyroid economy: Increased plasma volume TBG pool increased Renal clearance Feto-placental
Thyroid. Dr Jessica Triay November 2018
 Thyroid Dr Jessica Triay November 2018 Hypothyroidism in Pregnancy Clinical update: Hypothyroidism in Pregnancy Take home messages Additional evidence supportive for more relaxed TSH targets for those
Thyroid Dr Jessica Triay November 2018 Hypothyroidism in Pregnancy Clinical update: Hypothyroidism in Pregnancy Take home messages Additional evidence supportive for more relaxed TSH targets for those
Thyroid Nodule. Disclosure. Learning Objectives P A P A P A 3/18/2014. Nothing to disclose.
 Thyroid Nodule Evaluating the patient with a thyroid nodule and some management options. Miguel V. Valdez PA C Disclosure Nothing to disclose. Learning Objectives Examination of thyroid gland Options for
Thyroid Nodule Evaluating the patient with a thyroid nodule and some management options. Miguel V. Valdez PA C Disclosure Nothing to disclose. Learning Objectives Examination of thyroid gland Options for
John Sutton, DO, FACOI, FACE, CCD. Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989
 John Sutton, DO, FACOI, FACE, CCD Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989 No Disclosures Disease Of the Thyroid Iodide Metabolism/Synthesis of Thyroid Hormone Trap Oxidation Organification(catalyzed
John Sutton, DO, FACOI, FACE, CCD Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989 No Disclosures Disease Of the Thyroid Iodide Metabolism/Synthesis of Thyroid Hormone Trap Oxidation Organification(catalyzed
Hormones. Introduction to Endocrine Disorders. Hormone actions. Modulation of hormone levels. Modulation of hormone levels
 Introduction to Endocrine Disorders Hormones Self-regulating system (homeostasis) Affect: Growth Metabolism Reproduction Fluid and electrolyte balance Hormone actions Endocrine gland Hormone synthesis
Introduction to Endocrine Disorders Hormones Self-regulating system (homeostasis) Affect: Growth Metabolism Reproduction Fluid and electrolyte balance Hormone actions Endocrine gland Hormone synthesis