Clinical evaluation of. Thyroid function tests
|
|
|
- Della Flowers
- 5 years ago
- Views:
Transcription
1 In the name of God Dr.m.omidi Endocrinologist Assistant stant professor of medicine 25 APR 2012
2 Clinical evaluation of Thyroid function tests
3
4
5
6
7
8 Goal of TFT Evaluation of function of thyroid Monitoring of levothyroxine tx(either replacment or suppresive tx) Monitoring i of tx of hyperthyroidism Monitoring of thyroid malignancy(with ith TG and anti tg)
9 Thyroid function test Thyroid function tests included d five parameter 1.assay of HPT axis(with ith TSH) 2.concentration of T3 and T4 in serum 3.anti thyroid anti body 4.Tissue impact of thyroid hormone 5.throid iodine metabolism
10 TSH
11 TSH is a glycoprotein hormone composed of alfa and beta subunit. Alfa subunit similar il to other glycoprotein hormone such as FSH,LH,HCG. But beta subunit is specific for TSH and synthesis of this component is a rate limiting step in the synthesis of TSH.
12 TSH :stimulates synthesis and secretion of (T4) and (T3). Secretion of TSH is stimulated by (TRH), a hypothalamic h tripeptide. id TSH synthesis and release : regulated via a negative feedback mechanism by the level of thyroid hormones. Increased serum levels l of free T4 and T3 depress TSH secretion (hyperthyroidism), while decreased serum levels of free T4 and T3 result in excess TSH secretion (primary hypothyroidism).
13 TSH : no carrier protein TSH : unaffected by changes (such as liver or kidney failure, estrogens, and androgens) in proteins that are known to affect thyroid hormone carrier proteins
14 Average TSH levels l :.4 ± 4.44 mu/l, Alfa subunite similar to FSH,LH and HCG.normal serum level l of alfa is 1_5mic/L Increased in post monuposal,primary hypothyroidism and glycoprotein producing tumors of ant pituitary.
15 First generation immunoassy detected TSH above 1mu/lso can not deffrentiated between hyper and euthyroidism(nl lower limit of for TSH is.4) Second generation assay detected TSH above.1mu/l Third generation assay(chemiluminometric assay)can meassured TSH till.01
16 Second- and third-generation TSH assays can distinguish euthyroid patients from hyperthyroid h patients. 3 rd generation assays 2 nd generation assays 1 st generation assays CV % In nterassay FS = mu/l FS = mu/l Normal range FS = 1-2 mu/l fourth-generation research assays (not yet available for clinical use) to mu/ml TSH mu/l
17 TSH Reference Ranges Serum TSH values : higher in neonates and children. Mean euthyroid TSH values: approximate to 1.5 miu/l, (range 0.3 to 4.0 miu/l in iodinesufficient populations)
18 Some advocated d that t some of pt with TSH level above 2.5 may developed hypothyroidism thus upper limt of normal range shoud be lowerd(those with posstive familial hx,posstive anti thyroid antibody,pregnancy and expouse to drug such as amiodarone,thyroid nodule)
19 But till TSH above 10 to15 no tx needed this recommendation is quistionable.
20 Current guidelines recommend : TSH as the first-line test This is more cost-effective than a panel approach (TSH + FT4 or FT4 + FT3) but necessitates the use of a TSH assay with a functional sensitivity below 0.02 mu/l i.e. (third generation). However, this TSH-first strategy can miss patients, gy p with central hypothyroidism or TSH secreting pituitary tumors who must be assessed by FT4
21 The first tests for assessment of thyroid function are TSH and free T4
22 CLINICAL UTILITY OF THYROID- STIMULATING HORMONE MEASUREMENT
23 3 rd gen. TSH assay elevated Within normal range suppressed below 0.3 mu/l FT4 Anti-TPO FT4 elevated FT4 normal R/o hypothyroidism caused by Hashimoto's thyroiditis R/O THYROTOXICOSIS FT3
24 Clinical situations associated ated with subnormal TSH values
25 Clinical situations associated with subnormal TSH values thyroid hormone excess endogenous hyperthyroidism or excess exogenous thyroid hormone points the activation of the negative feedback loop. Prolonged excessive thyroid hormone physiological "atrophy" of the thyroid stimulatory limb of the hypothalamic-pituitary thyroid axis. Thus several months are usually required for the reestablishment of TSH secretion after the relief of thyrotoxicosis. After excess thyroid hormone treatment after the transient hyperthyroidism associated with subacute or some variants of autoimmune thyroiditis Shorter suppression Severe illness
26 rt3 Hormo one concen ntration FT4 TSH Normal Range TtlT4 Total T4 T3 Mild Moderate severe Recovery Stage of disease TFT during NTI
27 Clinical situations associated with Points subnormal TSH values High-dose glucocorticoids Exogenous dopamine Pharmacological amounts of retinoids Acutely but not chronically In critically ill patients, this effect of dopamine can be superimposed on the suppressive ssi effects of acute illness on thyroid function, reducing T4 production to even lower levels. Dopamine is sufficiently potent to suppress TSH to normal levels in sick patients with primary hypothyroidism. severe central hypothyroidism associated with very low serum TSH concentration has been reported in patients with cutaneous T-cell lymphoma treated with high-dose retinoid X receptor-selective ligand able to suppress TSH secretion.
28 hcg acute psychosis depression agitated psychoses Congenital central hypothyroidism a thyroid stimulator; In normal pregnancy as a slightly subnormal TSH during the first trimester ( mu/l) ; frank, though mild, hyperthyroidism in patients with choriocarcinoma or molar pregnancy. may have high thyroid hormone levels and suppressed or elevated TSH values. Etiology,unkown low serum TSH; may result from mutations affecting TSH alpha gene or the Pit-1 gene
29 In normal pregnancy TSH suppressed in first trimester and return to Nl in second and third trimester. Persistent suppression after first trimester(bellow.1) suggested that hyperthyroidism y due to autonomous thyroid function.
30 Clinical situations associated ated with elevated TSH values
31 Clinical situations associated with elevated TSH values Primary hypothyroidism points The serum free T4 is low normal or reduced but the serum free T3 values remain normal until the level l of thyroid function has markedly deteriorated. Iodine deficiency(the most common cause worldwide) Western Europe, South America, Africa and Asia. during the recovery phase A transient effect ; after a severe illness In such patients a "reawakening" of the hypothalamic-pituitary thyroid axis occurs with the improvement in their clinical state.
32 The remainder of the conditions associated with an elevated TSH are extremely rare : partial or complete TSH resistance inactivating point mutations of the TSH receptor gene. In a patient who has an elevated serum FT4, the presence of TSH at normal or increased levels should lead to a search for either resistance to thyroid hormone or a thyrotroph tumor. Hypothalamic-pituitary dysfunction normal or even modest increases in TSH are explained by the lack of normal TSH glycosylation in the TRH-deficient patient. The diagnosis is generally made by finding a serum free T4 index which is reduced to a greater extent than expected from the coincident serum TSH. Psychiatric illness either elevated or suppressed TSH, but the abnormal values are not usually in the range normally associated with symptomatic thyroid dysfunction
33 Addison's s disease The effect of glucocorticoids to suppress TSH secretion; TSH may be slightly elevated in the absence of primary thyroid disease. the presence of endogenous antimouse gamma globulin antibodies These antibodies, like TSH, can complex the two TSH antibodies resulting in artificially elevated serum TSH assay results in euthyroid patients; forming false bridges between the solid phase and signal antibodies.
34 Total T3 and T4 99/ of these hormone bound to circulating proteins including TBG,albumin and TTR Refrence range for T4(5_11mic/dl) g and T3(70 _190ng/dl)
35 Because high h level l of these hormone are bound to binding proteins,only measurement of total hormone is misleading Most common cause of change in total T3 and T4 is change in protein binding and is not due to thyroid problem. Binding proteins included TBG, albumin and TTR.
36 transport TBG TTR/TBPA Albumin T4 68% 11% 20% 99.97% T3 80% 9% 11% 99.7%
37 Factors that increased TBG 1.estrogen(pregnancy,ocp.HRT,tamoxifen heroin, methadone) 2.acute and chronic hepatitis 3.perphenazine,HIV ph, interferon n, genetic factor Factor that decreased TBG 1.androgens,danazol,glucocorticoid,RGH) g 2.nephrotic syndrome 3.acromegaly 4.Cirrhosis 5.Major systemic illness, Asparaginase
38 For evaluation the effect of binding protein on hormone assay T3Ru should be measured Normal range of T3Ru (27_33/) In condition of binding protein problems, level of T3 and T4 inversely related to T3Ru. T3Ru used for estimation of FT4Ior FT3I FT4i=T3RU total T4


39
40
41 Ru mused for estimation of ft4i
42 1.TBG increased,tt3 and TT4 increased, T3Ru decreased TBG decreased,tt3 and TT4 TBG decreased,tt3 and TT4 decreased,t3ru increased
43 In condition that thyroid pathology present level T3 andt4 related to T3RU(in hypothyroidism h both decreased and in thyrotoxicosis both increased)
44 Effect of various medication on TFT
45 Decreased TSH glucocorticoid Dopamine Octreotide bexarotene
46 Decreased secretion of thyroid hormone Amiodarone Iodine lithium
47 Estrogen Tamoxifen Heroin Methadone HRT Increased TBG
48 decreased TBG Androgens Anabolic steroids glucocorticoids
49 Illness and thyroid Acute illness affected TFT strongly So recommended that TFT dose not evaluated in acute ill patients if thyroid dysfunction is not high suspicious.
50 In acute illness conversion of T4 to T3 decreased Binding of thyroid hormone to binding protein is altered. Secretion of TSH decreased Various medication used that affected thyroid function
51 In mild illness such as pneumonia and UTI,TT3 decreased but total and free T4 and TSH is normal(t3 syndrome)
52 As underlying disease progress to moderate degree of severity TSH decreased d but TT4 is normal and RT3 is elevated.
53 In sever disease and in critical ill patients T4 decreased(t4 syndrome) during recovery phase of illness TSH elevated but still T4 and T3 are low(like hypothyroid )
54 About six weeks needed d after complete improvement of underlying disease for normalization of TFT.
55 rt3 Hormo one concen ntration FT4 TSH Normal Range TtlT4 Total T4 T3 Mild Moderate severe Recovery Stage of disease TFT during NTI
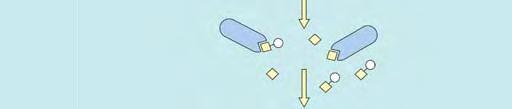
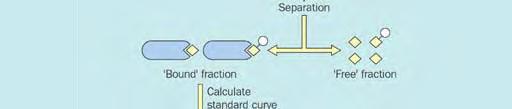
56 Free Hormone Tests (FT4 and FT3) free hormone hypothesis: free fraction of hormone is responsible for the biologic activity of thyroid hormones at the cellular level
57 Free T4 and T3 Measured with dialysate or ultrafiltrate(the accurate method). Only.3 of T3 and.02of T4 are free. In pregnant and ill pt free hormones do not accurate so for pregnancy the normal range of T4 multiplied by 1.5in lieu of a free T4 assay. In severely ill Pt free T4 falsely low and FT4I is better for asses of thyroid function Three method used(1)two step labeled hormone (2)one step (3labeld antibody approach All subject to artifacts from endogenous antibody,abnl binding protein or illness
58 Free Hormone Tests (FT4 and FT3) Index Methods Free T4 Index (FT4I) Free T3 Index (FT3I) Absolute Methods Equilibrium Dialysis Ultrafiltration Gel Filtration/Adsorption ti ti chromatography h Comparative Immunoassays Two-Step labeled Hormone One-step Labeled Hormone Analog Labeled Antibody
59 Index Methods (FT4I and FT3I) require two separate measurements: TT4 or TT3 Thyroid Hormone Binding Ratio (THBR) or "Uptake test Free Hormone Indexes (FT4I and FT3I): simple calculations approximation of the free hormone concentration nt ti n in the presence of abnormal binding proteins estimate free hormone concentrations: 40 y
60 FT4I and FT3I Current THBR tests are usually able to produce normal FT4I and FT3I values when TBG abnormalities are mild (i.e. pregnancy and estrogen therapy) these tests often fail to normalize FT4I and FT3I values in euthyroid patients with grossly abnormal binding proteins (congenital TBG extremes, familial dysalbuminemic hyperthyroxinemia (FDH), thyroid hormone autoantibodies and NTI
61 Clinical Performance Free Hormone Tests The indirect index tests (FT4I) and the direct comparative methods are all protein dependent to some extent These binding protein abnormalities cause discordances d between the total t and free hormone concentrations
62 Summary of a two-step serum free T4 Summary of a two step serum free T4 immunoassay
63 One-Step, Labeled Hormone-Analog FT4 and FT3 Methods hormone-analog n methods were pinipll principally engineered to give normal FT4 values in high TBG states They were found to have poor diagnostic accuracy in the presence of abnormal albumin concentrations secondary to Familial Dysalbuminemic Hyperthyroxinemic (FDH), NTI, high FFA concentrations or thyroid hormone autoantibodies
64 Clinical Performance Free Hormone Tests The only reason to select a free hormone method (FT4 or FT3) in preference to total hormone is to improve the diagnostic accuracy in patients with thyroid hormone binding abnormalities
65 Clinical Performance Free Hormone Tests (continue) No current FT4 method is universally valid in all clinical situations Common conditions that decrease the diagnostic accuracy of current free hormone tests in ambulatory patients include: TBG abnormalities (TBG excess or deficiency) Familial Dysalbuminemic Hyperthyroxinemia T4 and T3 autoantibodies interfering substances such as Rheumatoid Factor and Heterophilic antibodies (HAMA)
66
67 Anomalous Protein Binding of Tracer familial l dysalbuminemic i hyperthyroxinemia (FDH): falsely high free T4 estimate if serum albumin is subnormal, free T4 estimates by analogue tracer methods tend to be low In renal failure; analogue assays: low serum free T4 ( 40% in predialysis samples)
68 FREE T4 IN SPECIAL CIRCUMSTANCES Pregnancy Thyrotoxicosis and Hypothyroidism y Effect of Competitors for Thyroid Hormone Binding The Heparin Artifact Critical Illness
69 Pregnancy Interpretation of measured serum free T4 values during pregnancy is complicated by methodologic differences free T4 and free T3 decrease in the second and third trimesters, with mean levels reduced about 20% to 40% below the normal mean but subnormal levels are uncommon Roti and co-workers compared free T4 by seven different commercial methods in 23 euthyroid women and their infants at term, they found wide method-dependent variations
70 Pregnancy (continue) There is growing concern that the lack of method-specific, trimester- specific reference ranges for current FT4 tests renders these tests unreliable for assessing thyroid status during pregnancy TT4 measurements may be a better option if the reference limits are adjusted d for increased TBG by a factor of 1.5
71 Critical Illness Estimation of thyroid function during critical illness is influenced by multiple medications, such as dopaminergics, furosemide, and glucocorticoids some free T4 methods are vulnerable to the effects of NEFA, which may increase in vitro in heparin-treated patients Lack of specificity of free T4 and TSH results is the basis for recommending against routine testing of thyroid function during critical illness
72 Critical Illness there is a good argument for preferring measurement of total T4, a parameter that is generally free of assay artifact, versus free T4 during critical illness
73 Thyrotoxicosis and Hypothyroidism FT4 and FT3 do not maintain a linear relationship with the total hormone levels in thyrotoxicosis or hypothyroidism. In severe thyrotoxicosis, the total concentration of T4 can be two- to threefold elevated potential rise in free T4 is "buffered" by increased binding to TTR and albumin, there is a disproportionate increase in free T4 as total T4 increases.
74 Effect of Competitors for Thyroid Hormone Binding Numerous medications can displace T4 and T3 from TBG, but it is technically difficult to obtain an accurate reflection of these effects with current methods of measuring free T4
75 PRINCIPAL DRUGS THAT DISPLACE T4 FROM THYROXINE- BINDING GLOBULIN IN NORMAL HUMAN SERUM Drugs Salicylates Acetyl salicylic acid Salicyl salicyclic acid Furosemide Fenclofenac Mefenamic acid Flufenamic acid Diclofenac Difunisali Phenytoin Carbamazepine Mean Percent Increase in Free T4 Fraction 62 >
76 Artifact The effect of heparin in increasing serum free T4 is an important in vitro phenomenon that can lead to spuriously high estimates of circulating free T4
77 3 rd gen. TSH assay elevated Within normal range suppressed below 0.3 mu/l FT4 Anti-TPO FT4 elevated FT4 normal R/o hypothyroidism caused by Hashimoto's thyroiditis R/O THYROTOXICOSIS FT3
78 TSH(low) TSH (high h 5-10) Subclinical hypo T4,ANTI TPO Low T4, NL T4,poss anti tpo Or pregnancy or infertility NL T4,neg anti tpo TX TX f/u 6-12 m
79
80 T3RU and THBR
81
82
83 Effect of amiodarone on TFT Decreased release of T3 and T4 Decreased T4 to T3 conversion Decreased synthesis of thyroid hormone in suspected patients(hypothyroidism)
84 Thyroid inflammation(thyroiditis) or type 2 amiodarone induced thyrotoxicosis(ait) Hyperthyroidism or type 1 AIT
85
86
87
88 Biochemical cal markers of thyroid function 1.Thyrotoxicosis i increased(osteocalcin,alkp,shbg,ferritin,v wf,anf) fa f) Decreased(LDL,Lpa) 2.Hypothyroidism Increased(LDL,LPa,norepinephrine,CK) Decreased(vasopersin)
89 Effect of pregnancy on thyroid 1.Urinary iodine excretion increased so need for iodine increased( mic/day) 2.TBG secretion increased so level of total T4 and T3 increased but free level are nl 3.Autoimmune thyroid diseases during pregnancy ameliorated but after pregnancy may be exacerebrated 4.During first trimester due to HCG effect TSH suppressed and in 2 nd and3th trimester normalized.
90 So if after 1 st trimester t TSH still suppress autonomus hyperfunctioning of the thyroid gland cause of abnl thyroid TFT Thyroid function test should be normal in hypothyroid h women when planed pregnancy. During pregnancy need for levothyroxine percent increased.
91 Nuclear medicine and thyroid 1.RAIU:done with iodine(125 or 131) and 2 and 24 hr uptake measured. Used for deffrentiation of cause of thyrotoxicosis and dosimetry 2.Thyroid scan:done with Tc99 or I(125 and 131). Used for evaluation of thyroid nodule when TSH is suppressed, f/u of thyroid malignancy and cause of thyrotoxicosis. Nuclear imaging of thyroid contraindicated in pregnancy. 3.Thyroid ablation with I131 for tx of hyperthyroidism and thyroid malignancy.


92
93 THANK YOU
Pitfalls of TFTs Interpretation
 Mohammad Reza Bakhtiari DCLS, PhD Pitfalls of TFTs Interpretation CME July 2006 Vol.24 No.7, http://keck.usc.edu HPT axis physiology Log-linear relationship between TSH and FT4 Patient Specific Set Point
Mohammad Reza Bakhtiari DCLS, PhD Pitfalls of TFTs Interpretation CME July 2006 Vol.24 No.7, http://keck.usc.edu HPT axis physiology Log-linear relationship between TSH and FT4 Patient Specific Set Point
Chapter I.A.1: Thyroid Evaluation Laboratory Testing
 Chapter I.A.1: Thyroid Evaluation Laboratory Testing Jennifer L. Poehls, MD and Rebecca S. Sippel, MD, FACS THYROID FUNCTION TESTS Overview Thyroid-stimulating hormone (TSH) is produced by the anterior
Chapter I.A.1: Thyroid Evaluation Laboratory Testing Jennifer L. Poehls, MD and Rebecca S. Sippel, MD, FACS THYROID FUNCTION TESTS Overview Thyroid-stimulating hormone (TSH) is produced by the anterior
LABORATORY TESTS FOR EVALUATION OF THYROID DISORDERS
 LABORATORY TESTS FOR EVALUATION OF THYROID DISORDERS Maryam Tohidi Anatomical & clinical pathologist Research Institute for Endocrine Sciences THYROID GLAND (15-25 gr), (12-20 gr), 2 lobes connected by
LABORATORY TESTS FOR EVALUATION OF THYROID DISORDERS Maryam Tohidi Anatomical & clinical pathologist Research Institute for Endocrine Sciences THYROID GLAND (15-25 gr), (12-20 gr), 2 lobes connected by
THROID ABNORMALITIES AMIR ZIAEE
 THROID ABNORMALITIES AMIR ZIAEE 1 Thyroid Hormone Synthesis Table 330-2. Characteristics of Circulating T4 and T3 Hormone Property T4 T3 Serum concentrations Total hormone 8 μg/dl 0.14 μg/dl Fraction of
THROID ABNORMALITIES AMIR ZIAEE 1 Thyroid Hormone Synthesis Table 330-2. Characteristics of Circulating T4 and T3 Hormone Property T4 T3 Serum concentrations Total hormone 8 μg/dl 0.14 μg/dl Fraction of
Decoding Your Thyroid Tests and Results
 Decoding Your Thyroid Tests and Results Wondering about your thyroid test results? Learn about each test and what low, optimal, and high results may mean so you can work with your doctor to choose appropriate
Decoding Your Thyroid Tests and Results Wondering about your thyroid test results? Learn about each test and what low, optimal, and high results may mean so you can work with your doctor to choose appropriate
Thyroid Function TSH Analyte Information
 Thyroid Function TSH Analyte Information 1 2013-05-01 Thyroid-stimulating hormone (TSH) Introduction Thyroid-stimulating hormone (thyrotropin, TSH) is a glycoprotein with molecular weight of approximately
Thyroid Function TSH Analyte Information 1 2013-05-01 Thyroid-stimulating hormone (TSH) Introduction Thyroid-stimulating hormone (thyrotropin, TSH) is a glycoprotein with molecular weight of approximately
Sanjay B. Dixit, M.D. BHS Endocrinology Associates November 11, 2017
 Sanjay B. Dixit, M.D. BHS Endocrinology Associates November 11, 2017 I will not be discussing this Outline of discussion Laboratory tests for thyroid function Diagnosis of hypothyroidism Treatment of
Sanjay B. Dixit, M.D. BHS Endocrinology Associates November 11, 2017 I will not be discussing this Outline of discussion Laboratory tests for thyroid function Diagnosis of hypothyroidism Treatment of
Index. Graves disease, 111 thyroid autoantigens, 110 Autoimmune thyroiditis, 11, 58, 180, 181. B Bamforth Lazarus syndrome, 27
 Index A Adrenergic activation, 77 Allan Herndon Dudley syndrome, 31 Ambulatory practice choice of test, 156, 157 screening general population, thyroid dysfunction, 163, 164 targeted population, 164 167
Index A Adrenergic activation, 77 Allan Herndon Dudley syndrome, 31 Ambulatory practice choice of test, 156, 157 screening general population, thyroid dysfunction, 163, 164 targeted population, 164 167
THYROID HORMONES: An Overview
 1 SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES DISCIPLINE OF BIOCHEMISTRY AND MOLECULAR BIOLOGY PBL SEMINAR MBBS III; BMLS & BDS Year 3 What are the Thyroid Hormones? THYROID
1 SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES DISCIPLINE OF BIOCHEMISTRY AND MOLECULAR BIOLOGY PBL SEMINAR MBBS III; BMLS & BDS Year 3 What are the Thyroid Hormones? THYROID
Endocrine part two. Presented by Dr. Mohammad Saadeh The requirements for the Clinical Chemistry Philadelphia University Faculty of pharmacy
 Endocrine part two Presented by Dr. Mohammad Saadeh The requirements for the Clinical Chemistry Philadelphia University Faculty of pharmacy Cushing's disease: increased secretion of adrenocorticotropic
Endocrine part two Presented by Dr. Mohammad Saadeh The requirements for the Clinical Chemistry Philadelphia University Faculty of pharmacy Cushing's disease: increased secretion of adrenocorticotropic
Table 1: Thyroid panel. Result (reference interval) TSH 89.5 miu/l ( ) Total T4 5.2 µg/dl ( ) T3 uptake 39% (22-35)
 TSH 89.5 miu/l ( ) Total T4 5.2 µg/dl ( ) T3 uptake 39% (22-35)") Introduction Thyroid disease is the second most common endocrine disorder (behind diabetes), and its prevalence increases with increasing age. The incidence of newly diagnosed thyroid cancer is increasing
Introduction Thyroid disease is the second most common endocrine disorder (behind diabetes), and its prevalence increases with increasing age. The incidence of newly diagnosed thyroid cancer is increasing
Euthyroid sick syndrome
 Euthyroid sick syndrome Background Euthyroid sick syndrome can be described as abnormal findings on thyroid function tests that occur in the setting of a nonthyroidal illness (NTI) without preexisting
Euthyroid sick syndrome Background Euthyroid sick syndrome can be described as abnormal findings on thyroid function tests that occur in the setting of a nonthyroidal illness (NTI) without preexisting
Thyroid Disease. I have no disclosures. Overview TSH. Matthew Kim, M.D. July, 2012
 Thyroid Disease I have no disclosures Matthew Kim, M.D. July, 2012 Overview Thyroid Function Tests Hyperthyroidism Hypothyroidism Subclinical Thyroid Disease Thyroid Nodules Questions TSH Best single screening
Thyroid Disease I have no disclosures Matthew Kim, M.D. July, 2012 Overview Thyroid Function Tests Hyperthyroidism Hypothyroidism Subclinical Thyroid Disease Thyroid Nodules Questions TSH Best single screening
Understanding Thyroid Labs
 Understanding Thyroid Labs Chris Sadler, MA, PA-C, CDE, DFAAPA Senior Medical Science Liaison CVM Janssen Scientific Affairs Diabetes and Endocrine Associates La Jolla, CA Disclosures Employee of Janssen
Understanding Thyroid Labs Chris Sadler, MA, PA-C, CDE, DFAAPA Senior Medical Science Liaison CVM Janssen Scientific Affairs Diabetes and Endocrine Associates La Jolla, CA Disclosures Employee of Janssen
university sciences of Isfahan university Com
 Introduce R. Gholamnezhad Lecturer of school of nursing & midwifery of Iran university Ph.D student tof Immunology, Sh School of medical sciences of Isfahan university E-Mail: Gholami278@gmail. Com Interpreting
Introduce R. Gholamnezhad Lecturer of school of nursing & midwifery of Iran university Ph.D student tof Immunology, Sh School of medical sciences of Isfahan university E-Mail: Gholami278@gmail. Com Interpreting
THYROID HORMONES & THYROID FUNCTION TESTS
 THYROID HORMONES & THYROID FUNCTION TESTS SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES DISCIPLINE OF BIOCHEMISTRY AND MOLECULAR BIOLOGY CLINICAL BIOCHEMISTRY LECTURE BMLS III
THYROID HORMONES & THYROID FUNCTION TESTS SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES DISCIPLINE OF BIOCHEMISTRY AND MOLECULAR BIOLOGY CLINICAL BIOCHEMISTRY LECTURE BMLS III
B-Resistance to the action of hormones, Hormone resistance characterized by receptor mediated, postreceptor.
 Disorders of the endocrine system 38 Disorders of endocrine system mainly are caused by: A-Deficiency or an excess of a single hormone or several hormones: - deficiency :can be congenital or acquired.
Disorders of the endocrine system 38 Disorders of endocrine system mainly are caused by: A-Deficiency or an excess of a single hormone or several hormones: - deficiency :can be congenital or acquired.
Hypothalamo-Pituitary-Thyroid Axis
 SMGr up Hypothalamo-Pituitary-Thyroid Axis Orluwene Chituru Godwill 1 * and Ohiri John U 1 1 Chemical Pathology Department, University of Port Harcourt Teaching Hospital, Nigeria *Corresponding author:
SMGr up Hypothalamo-Pituitary-Thyroid Axis Orluwene Chituru Godwill 1 * and Ohiri John U 1 1 Chemical Pathology Department, University of Port Harcourt Teaching Hospital, Nigeria *Corresponding author:
Lecture title. Name Family name Country
 Lecture title Name Family name Country Nguyen Thy Khue, MD, PhD Department of Endocrinology HCMC University of Medicine and Pharmacy, MEDIC Clinic Hochiminh City, Viet Nam Provided no information regarding
Lecture title Name Family name Country Nguyen Thy Khue, MD, PhD Department of Endocrinology HCMC University of Medicine and Pharmacy, MEDIC Clinic Hochiminh City, Viet Nam Provided no information regarding
Sample Type - Serum Result Reference Range Units. Central Thyroid Regulation Surrey & Activity KT3 4Q. Peripheral Thyroid D Function mark
 Thyroid Plus Sample Type - Serum Result Reference Range Units Central Thyroid Regulation Surrey & Activity KT3 4Q Total Thyroxine (T4)
Thyroid Plus Sample Type - Serum Result Reference Range Units Central Thyroid Regulation Surrey & Activity KT3 4Q Total Thyroxine (T4)
Understanding thyroid function tests. Dr. Colette George
 Understanding thyroid function tests Dr. Colette George Disclosures No financial disclosure I will present fictitious cases and thyroid function tests (TFTs) that are based on scenarios I commonly encounter.
Understanding thyroid function tests Dr. Colette George Disclosures No financial disclosure I will present fictitious cases and thyroid function tests (TFTs) that are based on scenarios I commonly encounter.
Free hormone estimates. Never ending story.
 Free hormone estimates Never ending story. Roger Ekins (1926-2016) - saturation analysis - comp. immunoassay - microarray - RIA (T4, B12) - Free T4 (never really succeeded) Free hormone hypothesis Law
Free hormone estimates Never ending story. Roger Ekins (1926-2016) - saturation analysis - comp. immunoassay - microarray - RIA (T4, B12) - Free T4 (never really succeeded) Free hormone hypothesis Law
Hypothyroidism. Definition:
 Definition: Hypothyroidism Primary hypothyroidism is characterized biochemically by a high serum thyroidstimulating hormone (TSH) concentration and a low serum free thyroxine (T4) concentration. Subclinical
Definition: Hypothyroidism Primary hypothyroidism is characterized biochemically by a high serum thyroidstimulating hormone (TSH) concentration and a low serum free thyroxine (T4) concentration. Subclinical
Thyroid and Antithyroid Drugs
 Thyroid and Antithyroid Drugs Dr. Yunita Sari Pane, MSi Department of Pharmacology HYPOTHALAMIC PITUITARY THYROID AXIS T3 and T4 are synthesized in the thyroid gland. Inorganic iodine is trapped with great
Thyroid and Antithyroid Drugs Dr. Yunita Sari Pane, MSi Department of Pharmacology HYPOTHALAMIC PITUITARY THYROID AXIS T3 and T4 are synthesized in the thyroid gland. Inorganic iodine is trapped with great
Update on Gestational Thyroid Disease. Aidan McElduff The Discipline of Medicine, The University of Sydney
 IADPSG 2016 Update on Gestational Thyroid Disease Aidan McElduff The Discipline of Medicine, The University of Sydney IADPSG 2016 DISCLOSURES and AIM Nil to disclose Aim: to provide an overview 2017 Guidelines
IADPSG 2016 Update on Gestational Thyroid Disease Aidan McElduff The Discipline of Medicine, The University of Sydney IADPSG 2016 DISCLOSURES and AIM Nil to disclose Aim: to provide an overview 2017 Guidelines
Thyroid disorder for Resident
 Thyroid disorder for Resident Chaicharn Deerochanawong M.D. Diabetes and Endocrinology Unit Department of Medicine Rajavithi Hospital, Ministry of Public Health Topics Abnormal thyroid function test Euthyroid
Thyroid disorder for Resident Chaicharn Deerochanawong M.D. Diabetes and Endocrinology Unit Department of Medicine Rajavithi Hospital, Ministry of Public Health Topics Abnormal thyroid function test Euthyroid
Approach to thyroid dysfunction
 Approach to thyroid dysfunction Alice Y.Y. Cheng, MD, FRCPC Twitter: @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or
Approach to thyroid dysfunction Alice Y.Y. Cheng, MD, FRCPC Twitter: @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or
Thyroid Plus. Central Thyroid Regulation & Activity. Peripheral Thyroid Function. Thyroid Auto Immunity. Key Guide. Patient: DOB: Sex: F MRN:
 Thyroid Plus Patient: DOB: Sex: F MRN: Order Number: Completed: Received: Collected: Sample Type - Serum Result Reference Range Units Central Thyroid Regulation & Activity Total Thyroxine (T4) 127 127
Thyroid Plus Patient: DOB: Sex: F MRN: Order Number: Completed: Received: Collected: Sample Type - Serum Result Reference Range Units Central Thyroid Regulation & Activity Total Thyroxine (T4) 127 127
Requesting and Management of abnormal TFTs.
 Requesting and Management of abnormal TFTs. At the request of a number of GPs I have produced summary guidelines surrounding thyroid testing. These have been agreed with our Endocrinology leads Dr Bell
Requesting and Management of abnormal TFTs. At the request of a number of GPs I have produced summary guidelines surrounding thyroid testing. These have been agreed with our Endocrinology leads Dr Bell
Thyroid and Antithyroid Drugs. Munir Gharaibeh, MD, PhD, MHPE Faculty of Medicine April 2014
 Thyroid and Antithyroid Drugs Munir Gharaibeh, MD, PhD, MHPE Faculty of Medicine April 2014 Anatomy and histology of the thyroid gland Located in neck adjacent to the 5 th cervical vertebra (C5). Composed
Thyroid and Antithyroid Drugs Munir Gharaibeh, MD, PhD, MHPE Faculty of Medicine April 2014 Anatomy and histology of the thyroid gland Located in neck adjacent to the 5 th cervical vertebra (C5). Composed
LABORATORY MEDICINE PRACTICE GUIDELINES Laboratory Support for the Diagnosis and Monitoring of Thyroid Disease
 Table of Contents LABORATORY MEDICINE PRACTICE GUIDELINES Laboratory Support for the Diagnosis and Monitoring of Thyroid Disease Section I. Forward and Introduction Section 2. Pre-analytic factors Section
Table of Contents LABORATORY MEDICINE PRACTICE GUIDELINES Laboratory Support for the Diagnosis and Monitoring of Thyroid Disease Section I. Forward and Introduction Section 2. Pre-analytic factors Section
An Approach to: Thyroid Function Tests. Rinkoo Dalan Consultant Department of Endocrinology Tan Tock Seng Hospital
 An Approach to: Thyroid Function Tests Rinkoo Dalan Consultant Department of Endocrinology Tan Tock Seng Hospital Regulation of Thyroid axis Hypothalamus TRH T3,T4 ---- TRH Median Eminence (base of brain)
An Approach to: Thyroid Function Tests Rinkoo Dalan Consultant Department of Endocrinology Tan Tock Seng Hospital Regulation of Thyroid axis Hypothalamus TRH T3,T4 ---- TRH Median Eminence (base of brain)
Challenging TFTs (Definition)
") Thyroid Function Tests (Interpretation Challenges) Mohammad Reza Bakhtiari, DCLS, PhD 1/80 Challenging TFTs (Definition) Discordant Results vs. Clinical Picture Inharmonious Results 2/80 1 Challenging
Thyroid Function Tests (Interpretation Challenges) Mohammad Reza Bakhtiari, DCLS, PhD 1/80 Challenging TFTs (Definition) Discordant Results vs. Clinical Picture Inharmonious Results 2/80 1 Challenging
Limits of Liability/Disclaimer of Warranty
 Page 0 of 8 Limits of Liability/Disclaimer of Warranty The author, Brad Shook has made their best effort to produce a high quality and informative reference. The author makes no representation or warranties
Page 0 of 8 Limits of Liability/Disclaimer of Warranty The author, Brad Shook has made their best effort to produce a high quality and informative reference. The author makes no representation or warranties
Thyroid Screen (Serum)
") Thyroid Screen (Serum) Patient: DOB: Sex: F MRN: Order Number: Completed: Received: Collected: Sample Type - Serum Result Reference Range Units Central Thyroid Regulation & Activity Total Thyroxine (T4)
Thyroid Screen (Serum) Patient: DOB: Sex: F MRN: Order Number: Completed: Received: Collected: Sample Type - Serum Result Reference Range Units Central Thyroid Regulation & Activity Total Thyroxine (T4)
Thyrotoxicosis in Pregnancy: Diagnose and Management
 Thyrotoxicosis in Pregnancy: Diagnose and Management Yuanita Asri Langi email: meralday@yahoo.co.id Endocrinology & Metabolic Division, Internal Medicine Department, Prof.dr.R.D. Kandou Hospital/ Sam Ratulangi
Thyrotoxicosis in Pregnancy: Diagnose and Management Yuanita Asri Langi email: meralday@yahoo.co.id Endocrinology & Metabolic Division, Internal Medicine Department, Prof.dr.R.D. Kandou Hospital/ Sam Ratulangi
Page 1. Understanding Common Thyroid Disorders. Cases. Topics Covered
 Cases Understanding Common Thyroid Disorders Douglas C. Bauer, MD UCSF Division of General Internal Medicine No Disclosures 66 yr old female with 1 yr of fatigue and lassitude and no findings except TSH=8.2,
Cases Understanding Common Thyroid Disorders Douglas C. Bauer, MD UCSF Division of General Internal Medicine No Disclosures 66 yr old female with 1 yr of fatigue and lassitude and no findings except TSH=8.2,
Laboratory assessment of thyroid function. Nahid Shirazian MD. Internist, Endocrinologist
 Laboratory assessment of thyroid function Nahid Shirazian MD. Internist, Endocrinologist Physiology Thyroid gland produces Thyroxine Converted to active form T3 in tissue Scattered dc cells within ihi
Laboratory assessment of thyroid function Nahid Shirazian MD. Internist, Endocrinologist Physiology Thyroid gland produces Thyroxine Converted to active form T3 in tissue Scattered dc cells within ihi
Mastering Thyroid Disorders. Douglas C. Bauer, MD UCSF Division of General Internal Medicine
 Mastering Thyroid Disorders Douglas C. Bauer, MD UCSF Division of General Internal Medicine Cases 68 yr old female with new atrial fibrillation and no other findings except TSH=0.04, normal free T4 79
Mastering Thyroid Disorders Douglas C. Bauer, MD UCSF Division of General Internal Medicine Cases 68 yr old female with new atrial fibrillation and no other findings except TSH=0.04, normal free T4 79
Back to the Basics: Thyroid Gland Structure, Function and Pathology
 Back to the Basics: Thyroid Gland Structure, Function and Pathology JANELLE M. CHIASERA LEARNING OBJECTIVES 1. Explain the HPT feedback system involving the thyroid gland. Include the hormone produced
Back to the Basics: Thyroid Gland Structure, Function and Pathology JANELLE M. CHIASERA LEARNING OBJECTIVES 1. Explain the HPT feedback system involving the thyroid gland. Include the hormone produced
None. Thyroid Potpourri for the Primary Care Physician. Evaluating Thyroid Function. Disclosures. Learning Objectives
 Thyroid Potpourri for the Primary Care Physician Ramya Vedula DO, MPH, ECNU Endocrinology, Diabetes and Metabolism Princeton Medical Group Assistant Professor of Clinical Medicine Rutgers Robert Wood Johnson
Thyroid Potpourri for the Primary Care Physician Ramya Vedula DO, MPH, ECNU Endocrinology, Diabetes and Metabolism Princeton Medical Group Assistant Professor of Clinical Medicine Rutgers Robert Wood Johnson
The interpretation and management of thyroid disorders
 Journal of Endocrinology, Metabolism and Diabetes of South Africa 2015 ; 20(2) http://dx.doi.org/10.1080/16089677.2015.1056468 Open Access article distributed under the terms of the Creative Commons License
Journal of Endocrinology, Metabolism and Diabetes of South Africa 2015 ; 20(2) http://dx.doi.org/10.1080/16089677.2015.1056468 Open Access article distributed under the terms of the Creative Commons License
Pearls and Pitfalls of Thyroid Diagnosis. Todd W. Frieze, MD, FACP, FACE, ECNU, CCD Endocrine Care, Hattiesburg Clinic Biloxi MS
 Pearls and Pitfalls of Thyroid Diagnosis Todd W. Frieze, MD, FACP, FACE, ECNU, CCD Endocrine Care, Hattiesburg Clinic Biloxi MS Thyroid Anatomy Isthmus of gland located 1 fingerbreadth below cricoid cartilage
Pearls and Pitfalls of Thyroid Diagnosis Todd W. Frieze, MD, FACP, FACE, ECNU, CCD Endocrine Care, Hattiesburg Clinic Biloxi MS Thyroid Anatomy Isthmus of gland located 1 fingerbreadth below cricoid cartilage
Thyroid Patterns. 1. Hypothyroidism
 Thyroid Patterns We can simplify altered thyroid metabolism into seven patterns. These patterns include expression of altered thyroid metabolism from primary thyroid deficits and alterations in thyroid
Thyroid Patterns We can simplify altered thyroid metabolism into seven patterns. These patterns include expression of altered thyroid metabolism from primary thyroid deficits and alterations in thyroid
C. Thyrotropin/Thyroid Stimulating Hormone (TSH)
") C. Thyrotropin/Thyroid Stimulating Hormone (TSH) For more than twenty-five years, TSH methods have been able to detect the TSH elevations that are characteristic of primary hypothyroidism. Modern-day TSH
C. Thyrotropin/Thyroid Stimulating Hormone (TSH) For more than twenty-five years, TSH methods have been able to detect the TSH elevations that are characteristic of primary hypothyroidism. Modern-day TSH
Disorders of Thyroid Function
 Disorders of Thyroid Function Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Thyroid Hormone Axis Hypothalamus TRH
Disorders of Thyroid Function Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Thyroid Hormone Axis Hypothalamus TRH
The Number Games and Thyroid Function Arshia Panahloo Consultant Endocrinologist St George s Hospital
 The Number Games and Thyroid Function Arshia Panahloo Consultant Endocrinologist St George s Hospital Presentation Today: Common thyroid problems and treatments Pregnancy related thyroid problems The suppressed
The Number Games and Thyroid Function Arshia Panahloo Consultant Endocrinologist St George s Hospital Presentation Today: Common thyroid problems and treatments Pregnancy related thyroid problems The suppressed
DISORDERS OF THE THYROID GLAND SIGNS, SYMPTOMS, & TREATMENT ENDOCRINE SYSTEM AT A GLANCE OBJECTIVES ANATOMY OF THE THYROID
 OBJECTIVES DISORDERS OF THE THYROID GLAND SIGNS, SYMPTOMS, & TREATMENT Stephanie Blackburn, MHS, MLS(ASCP) CM LSU Health Shreveport Clinical Laboratory Science Program Discuss the synthesis and action
OBJECTIVES DISORDERS OF THE THYROID GLAND SIGNS, SYMPTOMS, & TREATMENT Stephanie Blackburn, MHS, MLS(ASCP) CM LSU Health Shreveport Clinical Laboratory Science Program Discuss the synthesis and action
Management of Common Thyroid Disorders
 Cases Management of Common Thyroid Disorders Douglas C. Bauer, MD UCSF Division of General Internal Medicine No Disclosures 68 yr old female with new atrial fibrillation and no other findings except TSH=0.04,
Cases Management of Common Thyroid Disorders Douglas C. Bauer, MD UCSF Division of General Internal Medicine No Disclosures 68 yr old female with new atrial fibrillation and no other findings except TSH=0.04,
Alvin C. Powers, M.D. 1/27/06
 Thyroid Histology Follicular Cells ECF side Apical lumen Thyroid Follicles -200-400 um Parafollicular or C-cells Colloid Photos from University of Manchester and tutorial created by Dr. James Crimando,
Thyroid Histology Follicular Cells ECF side Apical lumen Thyroid Follicles -200-400 um Parafollicular or C-cells Colloid Photos from University of Manchester and tutorial created by Dr. James Crimando,
Invecchiamento e Tiroide
 Simposio La patologia Tiroidea nell Anziano Invecchiamento e Tiroide Fabio Monzani Sezione Geriatria, Dipartimento di Medicina Clinica & Sperimentale, Università di Pisa THE EFFECT OF AGING ON THYROID
Simposio La patologia Tiroidea nell Anziano Invecchiamento e Tiroide Fabio Monzani Sezione Geriatria, Dipartimento di Medicina Clinica & Sperimentale, Università di Pisa THE EFFECT OF AGING ON THYROID
Guidance for Thyroid Function Testing in Primary Care in Lothian
 Guidance for Thyroid Function Testing in Primary Care in Lothian In July 2006 following a lengthy consultation process, a joint working group comprising representatives from the Association of Clinical
Guidance for Thyroid Function Testing in Primary Care in Lothian In July 2006 following a lengthy consultation process, a joint working group comprising representatives from the Association of Clinical
Management of Common Thyroid Disorders
 Management of Common Thyroid Disorders Douglas C. Bauer, MD UCSF Division of General Internal Medicine No Disclosures Cases 68 yr old woman with new atrial fibrillation and no other findings except TSH=0.04,
Management of Common Thyroid Disorders Douglas C. Bauer, MD UCSF Division of General Internal Medicine No Disclosures Cases 68 yr old woman with new atrial fibrillation and no other findings except TSH=0.04,
Thyroid and Antithyroid Drugs. Dr. Alia Shatanawi Feb,
 Thyroid and Antithyroid Drugs Dr. Alia Shatanawi Feb, 24 2014 Anatomy and histology of the thyroid gland Located in neck adjacent to the 5 th cervical vertebra (C5). Composed of epithelial cells which
Thyroid and Antithyroid Drugs Dr. Alia Shatanawi Feb, 24 2014 Anatomy and histology of the thyroid gland Located in neck adjacent to the 5 th cervical vertebra (C5). Composed of epithelial cells which
Endocrine part one. Presented by Dr. Mohammad Saadeh The requirements for the Clinical Chemistry Philadelphia University Faculty of pharmacy
 Endocrine part one Presented by Dr. Mohammad Saadeh The requirements for the Clinical Chemistry Philadelphia University Faculty of pharmacy HORMONES Hormones are chemicals released by a cell or a gland
Endocrine part one Presented by Dr. Mohammad Saadeh The requirements for the Clinical Chemistry Philadelphia University Faculty of pharmacy HORMONES Hormones are chemicals released by a cell or a gland
Thyroid disorders. Dr Enas Abusalim
 Thyroid disorders Dr Enas Abusalim Thyroid physiology The hypothalamic pituitary thyroid axis And peripheral conversion of T4 to T3, WHERE, AND BY WHAT ENZYME?? Only relatively small concentrations of
Thyroid disorders Dr Enas Abusalim Thyroid physiology The hypothalamic pituitary thyroid axis And peripheral conversion of T4 to T3, WHERE, AND BY WHAT ENZYME?? Only relatively small concentrations of
Hyperthyroidism Diagnosis and Treatment. April Janet A. Schlechte, M.D.
 Hyperthyroidism Diagnosis and Treatment Family Practice Refresher Course April 2015 Janet A. Schlechte, M.D. Disclosure of Financial Relationships Janet A. Schlechte, M.D. has no relationships with any
Hyperthyroidism Diagnosis and Treatment Family Practice Refresher Course April 2015 Janet A. Schlechte, M.D. Disclosure of Financial Relationships Janet A. Schlechte, M.D. has no relationships with any
Timothy Bilash MD MS OBG Northern Inyo Hospital, Bishop, CA October 20, :30 PM
 Thyroxine Deficiency in Pregnancy Timothy Bilash MD MS OBG Northern Inyo Hospital, Bishop, CA October 20, 2006 1:30 PM WHI Estrogen recap In http://courses.washington.edu/bonephys/opestrogen.html. from:
Thyroxine Deficiency in Pregnancy Timothy Bilash MD MS OBG Northern Inyo Hospital, Bishop, CA October 20, 2006 1:30 PM WHI Estrogen recap In http://courses.washington.edu/bonephys/opestrogen.html. from:
Thyroid Disease. Scott D. Isaacs, MD, FACP, FACE HRT Symposium Savannah GA July 14 16, All Rights Reserved. 1
 Thyroid Disease Scott D. Isaacs, MD, FACP, FACE HRT Symposium Savannah GA July 14 16, 2016 2016. All Rights Reserved. 1 Disclosure Scott D. Isaacs, MD, FACP, FACE, is the Medical Director at Atlanta Center
Thyroid Disease Scott D. Isaacs, MD, FACP, FACE HRT Symposium Savannah GA July 14 16, 2016 2016. All Rights Reserved. 1 Disclosure Scott D. Isaacs, MD, FACP, FACE, is the Medical Director at Atlanta Center
Southern Derbyshire Shared Care Pathology Guidelines. Hypothyroidism
 Southern Derbyshire Shared Care Pathology Guidelines Hypothyroidism Purpose of Guideline The management and referral criteria of patients with newly diagnosed hypothyroidism in adults. Background Hypothyroidism
Southern Derbyshire Shared Care Pathology Guidelines Hypothyroidism Purpose of Guideline The management and referral criteria of patients with newly diagnosed hypothyroidism in adults. Background Hypothyroidism
Thyroid function testing in pregnancy: 2017 ATA guidelines update. Dr Simon Forehan
 Thyroid function testing in pregnancy: 2017 ATA guidelines update Dr Simon Forehan Several factors are known to tax gravid thyroid economy: Increased plasma volume TBG pool increased Renal clearance Feto-placental
Thyroid function testing in pregnancy: 2017 ATA guidelines update Dr Simon Forehan Several factors are known to tax gravid thyroid economy: Increased plasma volume TBG pool increased Renal clearance Feto-placental
Pregnancy & Thyroid. Zohreh Moosavi Associate professor of Endocriology Imam Reza General Hospital Mashad University. Imam Reza weeky Conferance
 Pregnancy & Thyroid Zohreh Moosavi Associate professor of Endocriology Imam Reza General Hospital Mashad University Imam Reza weeky Conferance Objectives Thyroid Disorders & Pregnancy Normal thyroid phsyiology
Pregnancy & Thyroid Zohreh Moosavi Associate professor of Endocriology Imam Reza General Hospital Mashad University Imam Reza weeky Conferance Objectives Thyroid Disorders & Pregnancy Normal thyroid phsyiology
Pathophysiology of Thyroid Disorders. PHCL 415 Hadeel Alkofide April 2010
 Pathophysiology of Thyroid Disorders PHCL 415 Hadeel Alkofide April 2010 1 Learning Objectives Understand the pathophysiology of hyperthyroidism & hypothyroidism Describe the signs & symptoms of hyperthyroidism
Pathophysiology of Thyroid Disorders PHCL 415 Hadeel Alkofide April 2010 1 Learning Objectives Understand the pathophysiology of hyperthyroidism & hypothyroidism Describe the signs & symptoms of hyperthyroidism
GOITER and Shortness of Breath. Case A: GOITER. Learning Objectives. Common Thyroid Disorders for
 2:25 3:05pm Diagnosing and Treating Thyroid Disorders SPEAKER John Tayek, MD Presenter Disclosure Information The following relationships exist related to this presentation: John Tayek, MD, serves on the
2:25 3:05pm Diagnosing and Treating Thyroid Disorders SPEAKER John Tayek, MD Presenter Disclosure Information The following relationships exist related to this presentation: John Tayek, MD, serves on the
Diseases of thyroid & parathyroid glands (1 of 2)
") Diseases of thyroid & parathyroid glands (1 of 2) Thyroid diseases Thyrotoxicosis Hypothyroidism Thyroiditis Graves disease Goiters Neoplasms Chronic Lymphocytic (Hashimoto) Thyroiditis Subacute Granulomatous
Diseases of thyroid & parathyroid glands (1 of 2) Thyroid diseases Thyrotoxicosis Hypothyroidism Thyroiditis Graves disease Goiters Neoplasms Chronic Lymphocytic (Hashimoto) Thyroiditis Subacute Granulomatous
John Sutton, DO, FACOI, FACE, CCD. Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989
 John Sutton, DO, FACOI, FACE, CCD Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989 No Disclosures Disease Of the Thyroid Iodide Metabolism/Synthesis of Thyroid Hormone Trap Oxidation Organification(catalyzed
John Sutton, DO, FACOI, FACE, CCD Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989 No Disclosures Disease Of the Thyroid Iodide Metabolism/Synthesis of Thyroid Hormone Trap Oxidation Organification(catalyzed
NIH Public Access Author Manuscript Ther Drug Monit. Author manuscript; available in PMC 2013 April 14.
 NIH Public Access Author Manuscript Published in final edited form as: Ther Drug Monit. 2006 February ; 28(1): 8 11. Thyroid Function Testing in Pregnancy and Thyroid Disease: Trimester-specific Reference
NIH Public Access Author Manuscript Published in final edited form as: Ther Drug Monit. 2006 February ; 28(1): 8 11. Thyroid Function Testing in Pregnancy and Thyroid Disease: Trimester-specific Reference
BELIEVE MIDWIFERY SERVICES
 TITLE: THYROID DISEASE IN PREGNANCY EFFECTIVE DATE: July, 2013 POLICY STATEMENT: Pregnancy changes significantly the values influenced by the serum thyroid binding hormone level (i.e., total thyroxine,
TITLE: THYROID DISEASE IN PREGNANCY EFFECTIVE DATE: July, 2013 POLICY STATEMENT: Pregnancy changes significantly the values influenced by the serum thyroid binding hormone level (i.e., total thyroxine,
Hyperthyroidism. Objectives. Clinical Manifestations. Slide 1. Slide 2. Slide 3. Implications for Primary Care. hyperthyroidism
 1 Hyperthyroidism Implications for Primary Care Laura A. Ruby, DNP, CRNP Wellspan Endocrinology 2 Objectives! Discuss the clinical manifestations of hyperthyroidism! Review the use of the diagnostic studies!
1 Hyperthyroidism Implications for Primary Care Laura A. Ruby, DNP, CRNP Wellspan Endocrinology 2 Objectives! Discuss the clinical manifestations of hyperthyroidism! Review the use of the diagnostic studies!
Jim Paoletti BS Pharmacy, FAARM, FIACP, Director of Education, P2P
 presents A Pioneering Functional Technologies Approach For to Hypothyroidism Lifestyle Based Medicine Part 3 of 3 with Jim Paoletti BS Pharmacy, FAARM, FIACP, Director of Education, P2P Clinical Consultant
presents A Pioneering Functional Technologies Approach For to Hypothyroidism Lifestyle Based Medicine Part 3 of 3 with Jim Paoletti BS Pharmacy, FAARM, FIACP, Director of Education, P2P Clinical Consultant
Checking the Right Box at the Right Age: the Art of Pediatric Endocrine Testing
 Checking the Right Box at the Right Age: the Art of Pediatric Endocrine Testing Jean-Pierre Chanoine, MD Endocrinology and Diabetes Unit British Columbia s Children s Hospital Objectives 1. Interpret the
Checking the Right Box at the Right Age: the Art of Pediatric Endocrine Testing Jean-Pierre Chanoine, MD Endocrinology and Diabetes Unit British Columbia s Children s Hospital Objectives 1. Interpret the
Lothian Guidance for Diagnosis and Management of Thyroid Dysfunction in Pregnancy
 Lothian Guidance for Diagnosis and Management of Thyroid Dysfunction in Pregnancy Early diagnosis and good management of maternal thyroid dysfunction are essential to ensure minimal adverse effects on
Lothian Guidance for Diagnosis and Management of Thyroid Dysfunction in Pregnancy Early diagnosis and good management of maternal thyroid dysfunction are essential to ensure minimal adverse effects on
Southern Derbyshire Shared Care Pathology Guidelines. Hyperthyroidism
 Southern Derbyshire Shared Care Pathology Guidelines Hyperthyroidism Purpose of Guideline The management and referral criteria of patients with newly diagnosed hyperthyroidism. Background Hyperthyroidism
Southern Derbyshire Shared Care Pathology Guidelines Hyperthyroidism Purpose of Guideline The management and referral criteria of patients with newly diagnosed hyperthyroidism. Background Hyperthyroidism
Grave s disease (1 0 )
") THYROID DYSFUNCTION Grave s disease (1 0 ) Autoimmune - activating AB s to TSH receptor High concentrations of circulating thyroid hormones Weight loss, tachycardia, tiredness Diffuse goitre - TSH stimulating
THYROID DYSFUNCTION Grave s disease (1 0 ) Autoimmune - activating AB s to TSH receptor High concentrations of circulating thyroid hormones Weight loss, tachycardia, tiredness Diffuse goitre - TSH stimulating
THYROID FUNCTION EVALUATION IN PATIENTS WITH INCREASED OR DECREASED THYROXINE-BINDING PROTEIN
 THE AMEBICAN JOURNAL OF CLINICAL PATHOLOGY Vol. 50, No. 3 Copyright 1968 by The Williams & Wilkins Co. Printed in U.S.A. THYROID FUNCTION EVALUATION IN PATIENTS WITH INCREASED OR DECREASED THYROXINE-BINDING
THE AMEBICAN JOURNAL OF CLINICAL PATHOLOGY Vol. 50, No. 3 Copyright 1968 by The Williams & Wilkins Co. Printed in U.S.A. THYROID FUNCTION EVALUATION IN PATIENTS WITH INCREASED OR DECREASED THYROXINE-BINDING
Thyroid hormones derived from two iodinated tyrosine molecules
 Thyroid Hormones OBJECTIVES Chemical nature of the thyroid hormones How different enzymes play a role in thyroid hormone formation? And what drugs affect them? Describe Function & Metabolism of thyroid
Thyroid Hormones OBJECTIVES Chemical nature of the thyroid hormones How different enzymes play a role in thyroid hormone formation? And what drugs affect them? Describe Function & Metabolism of thyroid
Hormones. Introduction to Endocrine Disorders. Hormone actions. Modulation of hormone levels. Modulation of hormone levels
 Introduction to Endocrine Disorders Hormones Self-regulating system (homeostasis) Affect: Growth Metabolism Reproduction Fluid and electrolyte balance Hormone actions Endocrine gland Hormone synthesis
Introduction to Endocrine Disorders Hormones Self-regulating system (homeostasis) Affect: Growth Metabolism Reproduction Fluid and electrolyte balance Hormone actions Endocrine gland Hormone synthesis
Thyroid Management. Evolving Controversy - Science, Dogma, Opinion. The Ogden Surgical Medical Society May 2016
 Thyroid Management Evolving Controversy - Science, Dogma, Opinion The Ogden Surgical Medical Society May 2016 Published Guidelines AACE and ATA - Clinical Practice Guidelines in 2012 Guidelines are neither
Thyroid Management Evolving Controversy - Science, Dogma, Opinion The Ogden Surgical Medical Society May 2016 Published Guidelines AACE and ATA - Clinical Practice Guidelines in 2012 Guidelines are neither
Underactive Thyroid. Diagnosis, Treatment & Controversies
 Underactive Thyroid Diagnosis, Treatment & Controversies Dr. Asif Malik Humayun Consultant Endocrinologist Milton Keynes University Hospital NHS Foundation Trust Thyroid Hormone Control of metabolism
Underactive Thyroid Diagnosis, Treatment & Controversies Dr. Asif Malik Humayun Consultant Endocrinologist Milton Keynes University Hospital NHS Foundation Trust Thyroid Hormone Control of metabolism
Pathophysiology of the th E d n ocr i ne S S t ys em B. Marinov, MD, PhD Endocrine system Central: Hypothalamus
 Pathophysiology of the Endocrine System B. Marinov, MD, PhD Pathophysiology Department Medical University of Plovdiv Endocrine system Central: Hypothalamus Pituitary Pineal Peripheral Thymus Thyroid Parathyroid
Pathophysiology of the Endocrine System B. Marinov, MD, PhD Pathophysiology Department Medical University of Plovdiv Endocrine system Central: Hypothalamus Pituitary Pineal Peripheral Thymus Thyroid Parathyroid
Disorders of the Thyroid Gland
 Disorders of the Thyroid Gland István Takács MD., PhD, 1st Department of Medicine, Semmelweis University Connection to the dentistry: close to each other higher operation risk radiating pain macroglossia
Disorders of the Thyroid Gland István Takács MD., PhD, 1st Department of Medicine, Semmelweis University Connection to the dentistry: close to each other higher operation risk radiating pain macroglossia
California Association for Medical Laboratory Technology
 California Association for Medical Laboratory Technology Distance Learning Program Thyroid Hormones and Thyroid Diseases Course # DL-967 by Helen Sowers, M.A., CLS Dept. of Biological Science (retired)
California Association for Medical Laboratory Technology Distance Learning Program Thyroid Hormones and Thyroid Diseases Course # DL-967 by Helen Sowers, M.A., CLS Dept. of Biological Science (retired)
Thyroid. Dr Jessica Triay November 2018
 Thyroid Dr Jessica Triay November 2018 Hypothyroidism in Pregnancy Clinical update: Hypothyroidism in Pregnancy Take home messages Additional evidence supportive for more relaxed TSH targets for those
Thyroid Dr Jessica Triay November 2018 Hypothyroidism in Pregnancy Clinical update: Hypothyroidism in Pregnancy Take home messages Additional evidence supportive for more relaxed TSH targets for those
Critical illness and endocrinology. ICU Fellowship Training Radboudumc
 Critical illness and endocrinology ICU Fellowship Training Radboudumc Critical illness Ultimate form of severe physical stress Generates an orchestrated endocrine response to provide the energy for fight
Critical illness and endocrinology ICU Fellowship Training Radboudumc Critical illness Ultimate form of severe physical stress Generates an orchestrated endocrine response to provide the energy for fight
Reference Intervals for Children and Adults
 for Children and Adults TSH, FT4, FT3, T4, T3, T-Uptake, FT4-index, Anti-TPO, Anti-Tg, Tg Elecsys systems /20 MODULAR ANALYTICS E70 cobas e 4 and cobas e 60 analysers Contents Page Introduction 4 2 Summary
for Children and Adults TSH, FT4, FT3, T4, T3, T-Uptake, FT4-index, Anti-TPO, Anti-Tg, Tg Elecsys systems /20 MODULAR ANALYTICS E70 cobas e 4 and cobas e 60 analysers Contents Page Introduction 4 2 Summary
Neonatal Thyrotoxicosis Management of babies born to mothers with a history of hyperthyroidism (Grave s Disease)
") MCN for Neonatology West of Scotland Neonatal Guideline Neonatal Thyrotoxicosis Management of babies born to mothers with a history of hyperthyroidism (Grave s Disease) This document is applicable to all
MCN for Neonatology West of Scotland Neonatal Guideline Neonatal Thyrotoxicosis Management of babies born to mothers with a history of hyperthyroidism (Grave s Disease) This document is applicable to all
Common Issues in Management of Hypothyroidism
 Common Issues in Management of Hypothyroidism Family Medicine Refresher Course April 5, 2018 Janet A. Schlechte, M.D. Disclosure of Financial Relationships Janet A. Schlechte, M.D. has no relationships
Common Issues in Management of Hypothyroidism Family Medicine Refresher Course April 5, 2018 Janet A. Schlechte, M.D. Disclosure of Financial Relationships Janet A. Schlechte, M.D. has no relationships
The Thyroid and Pregnancy OUTLINE OF DISCUSSION 3/19/10. Francis S. Greenspan March 19, Normal Physiology. 2.
 The Thyroid and Pregnancy Francis S. Greenspan March 19, 2010 OUTLINE OF DISCUSSION 1. Normal Physiology 2. Hypothyroidism 3. Hyperthyroidism 4. Thyroid Nodules and Cancer NORMAL PHYSIOLOGY Iodine Requirements:
The Thyroid and Pregnancy Francis S. Greenspan March 19, 2010 OUTLINE OF DISCUSSION 1. Normal Physiology 2. Hypothyroidism 3. Hyperthyroidism 4. Thyroid Nodules and Cancer NORMAL PHYSIOLOGY Iodine Requirements:
Icd 10 low tsh level. Icd 10 low tsh level. Search
 Search Icd 10 low tsh level Icd 10 low tsh level 1-10-2012 The 2012 updates to the Current Procedural Terminology 4th Edition (CPT-4) and Healthcare Common Procedure Coding System (HCPCS) National Level
Search Icd 10 low tsh level Icd 10 low tsh level 1-10-2012 The 2012 updates to the Current Procedural Terminology 4th Edition (CPT-4) and Healthcare Common Procedure Coding System (HCPCS) National Level
OUTLINE. Regulation of Thyroid Hormone Production Common Tests to Evaluate the Thyroid Hyperthyroidism - Graves disease, toxic nodules, thyroiditis
 THYROID DISEASE OUTLINE Regulation of Thyroid Hormone Production Common Tests to Evaluate the Thyroid Hyperthyroidism - Graves disease, toxic nodules, thyroiditis OUTLINE Hypothyroidism - Hashimoto s thyroiditis,
THYROID DISEASE OUTLINE Regulation of Thyroid Hormone Production Common Tests to Evaluate the Thyroid Hyperthyroidism - Graves disease, toxic nodules, thyroiditis OUTLINE Hypothyroidism - Hashimoto s thyroiditis,
Laura Trask, MD FACP Central Maine Endocrinology Lewiston, ME
 Laura Trask, MD FACP Central Maine Endocrinology Lewiston, ME 795-7520 traskla@cmhc.org No disclosures Objectives To have an understanding of hyperthyroidism To have an understanding of the management
Laura Trask, MD FACP Central Maine Endocrinology Lewiston, ME 795-7520 traskla@cmhc.org No disclosures Objectives To have an understanding of hyperthyroidism To have an understanding of the management
Icd 10 low tsh level. Cari untuk: Cari Cari
 Cari untuk: Cari Cari Icd 10 low tsh level AMMONIUM PERCHLORATE is a white, crystalline solid or powder. Classified as a division 1.1 explosive if powdered into particles smaller than 15 microns in diameter
Cari untuk: Cari Cari Icd 10 low tsh level AMMONIUM PERCHLORATE is a white, crystalline solid or powder. Classified as a division 1.1 explosive if powdered into particles smaller than 15 microns in diameter
Canadian Endocrine Review Course 2014
 Canadian Endocrine Review Course 2014 Amiodarone & Thyrotoxicosis Iodine, A Catch 22 Ally P.H. Prebtani Associate Professor of Medicine Internal Medicine, Endocrinology & Metabolism McMaster University
Canadian Endocrine Review Course 2014 Amiodarone & Thyrotoxicosis Iodine, A Catch 22 Ally P.H. Prebtani Associate Professor of Medicine Internal Medicine, Endocrinology & Metabolism McMaster University
Thyroid Disorders Towards a Healthy Endocrine System
 Thyroid Disorders Towards a Healthy Endocrine System What are Thyroid Disorders? The thyroid is a butterfly-shaped gland in the middle of the lower neck. Through the release of hormones, the thyroid regulates
Thyroid Disorders Towards a Healthy Endocrine System What are Thyroid Disorders? The thyroid is a butterfly-shaped gland in the middle of the lower neck. Through the release of hormones, the thyroid regulates
Reference intervals are derived from the statistical distribution of values in the general healthy population.
 Position Statement Subject: Thyroid Function Testing for Adult Diagnosis and Monitoring Approval Date: July 2017 Review Date: July 2019 Review By: Chemical AC, Board of Directors Number: 1/2017 Introduction:
Position Statement Subject: Thyroid Function Testing for Adult Diagnosis and Monitoring Approval Date: July 2017 Review Date: July 2019 Review By: Chemical AC, Board of Directors Number: 1/2017 Introduction:
DRUGS. 4- Two molecules of DIT combine within the thyroglobulinto form L-thyroxine (T4)' One molecule of MIT & one molecule of DIT combine to form T3
' One molecule of MIT & one molecule of DIT combine to form T3") THYROID HORMONEs & ANTITHYROID The thyroid secretes 2 types of hormones: DRUGS 1- Iodine containing amino acids (are important for growth, development and metabolism) and these are: triodothyronine, tetraiodothyronine,(
THYROID HORMONEs & ANTITHYROID The thyroid secretes 2 types of hormones: DRUGS 1- Iodine containing amino acids (are important for growth, development and metabolism) and these are: triodothyronine, tetraiodothyronine,(
Interferences. with Endocrine Tests
 American Association of Clinical Endocrinologists 8/4/18 Interferences with Endocrine Tests Carole Spencer MTC, Ph.D, FACB Professor of Research Medicine Department of Medicine University of Southern California
American Association of Clinical Endocrinologists 8/4/18 Interferences with Endocrine Tests Carole Spencer MTC, Ph.D, FACB Professor of Research Medicine Department of Medicine University of Southern California
HAEMATOLOGY. Test Name Status Result Unit Reference Interval HbA1c (Glycated Haemoglobin) 5.4 % Method : HPLC Sample Type : Whole Blood EDTA
 5.4 % Method : HPLC Sample Type : Whole Blood EDTA") Institution Report Date 25-Dec-2016 05:59 PM HAEMATOLOGY HbA1c (Glycated Haemoglobin) 5.4 % 4.5-6.0 Method : HPLC Sample Type : Whole Blood EDTA REMARKS In vitro quantitative determination of HbA1c in
Institution Report Date 25-Dec-2016 05:59 PM HAEMATOLOGY HbA1c (Glycated Haemoglobin) 5.4 % 4.5-6.0 Method : HPLC Sample Type : Whole Blood EDTA REMARKS In vitro quantitative determination of HbA1c in
Occurrence and management of an aberrant free T4 in combination with a normal TSH
 ORIGINAL ARTICLE Occurrence and management of an aberrant free T4 in combination with a normal TSH K.M. van Veggel 1 *, J.M. Rondeel 2, S. Anten 3 1 Department of Internal Medicine, Isala Hospital (previously
ORIGINAL ARTICLE Occurrence and management of an aberrant free T4 in combination with a normal TSH K.M. van Veggel 1 *, J.M. Rondeel 2, S. Anten 3 1 Department of Internal Medicine, Isala Hospital (previously
HYPERTHYROIDISM. Hypothalamus. Thyrotropin-releasing hormone (TRH) Anterior pituitary gland. Thyroid-stimulating hormone (TSH) Thyroid gland T4, T3
 Anterior pituitary gland. Thyroid-stimulating hormone (TSH) Thyroid gland T4, T3") HYPERTHYROIDISM Hypothalamus Thyrotropin-releasing hormone (TRH) Anterior pituitary gland Thyroid-stimulating hormone (TSH) Thyroid gland T4, T3 In hyperthyroidism, there is an increased production of
HYPERTHYROIDISM Hypothalamus Thyrotropin-releasing hormone (TRH) Anterior pituitary gland Thyroid-stimulating hormone (TSH) Thyroid gland T4, T3 In hyperthyroidism, there is an increased production of