(Not so) New Guidelines for Management of Thyroid Nodules and Differentiated Thyroid Cancer Minnesota/Midwest Chapter of AACE
|
|
|
- Melinda Dorsey
- 6 years ago
- Views:
Transcription


1 (Not so) New Guidelines for Management of Thyroid Nodules and Differentiated Thyroid Cancer Minnesota/Midwest Chapter of AACE Bryan R. Haugen, MD University of Colorado, School of Medicine
2 Outline Some statistics New guidelines grading system New/changed guidelines Summary review of the guidelines Disclosures Research support/honoraria from Genzyme Consultant for Eisai
3 Davis MM, JAMA 305:2343, 2011
 All 3.6% 1.1% Distant Mets 2.4% 2.")
4 2017 Thyroid Cancer Annual increase (incidence) Annual increase (mortality) All 3.6% 1.1% Distant Mets 2.4% 2.9%

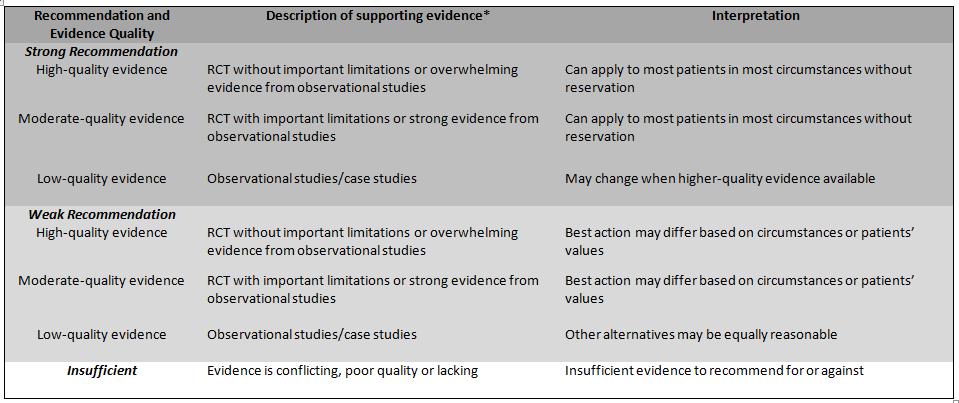
5 Adapted ACP system
6 Are the new guidelines different from the 2009 guidelines? Goal: To be evidence-based and helpful Recommendations Sub-recommendations References Tables 5 17 Figures 5 8 New questions 8 New recommendations 21 Significantly changed recommendations - 21

7 Haugen BR, Cancer 2016
8 Example of Strong Recommendations Based on Low-quality Evidence Recommendation 33A: Preoperative use of cross-sectional imaging studies (CT, MRI) with intravenous (IV) contrast is recommended as an adjunct to US for patients with clinical suspicion for advanced disease.
9 Patient #1 48 yo male incidental 8 mm thyroid nodule High suspicion sonographic pattern, no abnormal LN Thyroidectomy, calcitonin, FNA, monitor Risk of PTC? Risk of bad outcome?
10 Sonographic patterns High suspicion [malignancy risk 70-90%]: Solid hypoechoic nodule or solid hypoechoic component of a partially cystic nodule with one or more of the following features: irregular margins, microcalcifications, taller than wide shape. Intermediate suspicion [malignancy risk 10-20%]: Hypoechoic solid nodule without high suspicion features Low suspicion [malignancy risk 5-10%]: Isoechoic or hyperechoic solid nodule, or partially (> 50%) cystic nodule, with eccentric solid area without high suspicion features Very low suspicion [<3%]: Spongiform or partially cystic nodules without high or intermediate suspicion features Benign [<1%]: Purely cystic nodules











11 Risk of malignancy Microcalcifications, microcalcifications, hypoechoic nodule hyperechoic cystic irregular margins taller than wide nodule irregular margins, extrathyroidal extension nodule with irregular margins, suspicious left lateral lymph node High 70-90% > 1 cm hypoechoic solid regular margin hypoechoic solid regular margin Intermediate 10-20% > 1 cm hyperechoic solid regular margin isoechoic solid regular margin partially cystic with eccentric solid area partially cystic with eccentric solid areas Low 5-10% > 1.5 cm spongiform partially cystic no suspicious features partially cystic no suspicious features Very low <3% > 2 cm If at all jugular carotid Benign <1% Biopsy not needed to r/o malignancy Figure 2 cyst

12 J Am College Radiology 2017
 (FNA is not")
13 Patient #1 48 yo male incidental 8 mm thyroid nodule High suspicion sonographic pattern, no abnormal LN Active surveillance (monitor) (FNA is not required )
14 Follow-up for nodules that do not meet FNA criteria RECOMMENDATION 24 (NEW) A) Nodules with high suspicion US pattern: repeat US 6-12 months (Weak recommendation, Low-quality evidence) B) Nodules with sonographic features of low to intermediate suspicion US pattern: consider repeat US at months. (Weak recommendation, Low-quality evidence). C) Nodules with very low suspicion US pattern (including spongiform nodules) and pure cyst: the utility and time interval of surveillance US for risk of malignancy is not known. If US is repeated, it should be at > 24 months (No recommendation, Insufficient evidence) D) Nodules < 1 cm without high suspicion US pattern do not require routine sonographic FU and if repeated, the US should be performed at 24 months or later (Weak recommendation, Low-quality evidence)
15 Patient #2 38 yo female 2.7 cm high suspicion sonographic pattern No abnormal neck LN FNA - PTC Thyroidectomy with central neck dissection Thyroidectomy Thyroidectomy or lobectomy Lobectomy Observation
16 FNA PTC 2.7 cm Thyroidectomy or lobectomy? 2009 Recommendation: Thyroidectomy Bilimoria KY, Ann Surg 2007 Adam M, Ann Surg 2014 Matsuzu K, World J Surg 2014 Barney BM, Head Neck 2011 Nixon IJ, Surgery 2011 Mendelsohn AH, Arch Otolaryn 2010 Haigh PI, Ann Surg Onc 2005 RECOMMENDATION 35 PTC >1 cm and <4 cm No extrathyroidal extension, cn0 (preoperative assessment) NTT/TT or lobectomy (Strong Recommendation, Moderate-quality evidence)
17 Patient #3 56 yo male FNA PTC US no abnormal LN Thyroidectomy and central neck dissection Path report 3.8 cm FVPTC, involved LN Helpful pathology report?
18 Randolph GW, Thyroid 2012 Yamashita H, Cancer 1997 Lango M, Thyroid 2013 Collini P, Histopath 2004 Recommendation 46 (NEW) Pathology reports should include: AJCC/TNM criteria Vascular invasion and number of vessels Number of LN examined and involved Size of the largest metastatic LN focus Extranodal extension (Strong recommendation, Moderate-quality evidence) Variants with more favorable and unfavorable outcomes (Strong recommendation, Low-quality evidence) Variants associated with familial syndromes (Weak recommendation, Low-quality evidence) Cetta F, JCEM 2000 Laury AR, Thyroid 2011 Volante M, Cancer 2004
19 Patient #3 56 yo male FNA PTC US no abnormal LN Thyroidectomy and central neck dissection Path report: 3.8 cm FVPTC Extrathyroid extension, negative margins No vascular invasion 11/12 LN involved, largest 1.2 cm, no ENE T3N1aMX, Stage III, ATA intermediate risk Post-op TSH 0.2, Tg 1.8, Ab <2 No radioiodine Diagnostic WBS mci 131I, consider rhtsh mci 131I only after THW mci 131I after THW
20 System for Estimating Risk of Persistent or Recurrent Disease ATA Guidelines 2009 Low Risk Classic PTC No local or distant mets Complete resection No ETE No vascular invasion If given, no RAI uptake outside TB 78-91% NED 2-7% Structural Incomplete Cooper et al, Thyroid 2009 Tuttle et al, Thyroid 2010 Vaisman at al, Clin Endo 2012 Pitoia et al, Thyroid 2013 Intermediate Risk Microscopic ETE Cervical LN mets Aggressive Histology Vascular invasion 52-63% NED 21-34% Structural Incomplete High Risk Macroscopic gross ETE Incomplete tumor resection Distant Mets Tg elevation 14-31% NED 56-72% Structural Incomplete
21 Risk of Structural Disease Recurrence (In patients without structurally identifiable disease after initial therapy) High Risk Gross extrathyroidal extension, incomplete tumor resection, distant metastases, or lymph node >3 cm Intermediate Risk Aggressive histology, minor extrathyroidal extension, vascular invasion, or > 5 involved lymph nodes (0.2-3 cm) Low Risk Intrathyroidal DTC 5 LN micrometastases (< 0.2 cm) Figure 4 FTC, extensive vascular invasion ( 30-55%) pt4a gross ETE ( 30-40%) pn1 with extranodal extension, >3 LN involved ( 40%) PTC, > 1 cm, TERT mutated ± BRAF mutated* (>40%) pn1, any LN > 3 cm ( 30%) PTC, extrathyroidal, BRAF mutated*( 10-40%) PTC, vascular invasion ( 15-30%) Clinical N1 ( 20%) pn1, > 5 LN involved ( 20%) Intrathyroidal PTC, < 4 cm, BRAF mutated* ( 10%) pt3 minor ETE ( 3-8%) pn1, all LN < 0.2 cm ( 5%) pn1, 5 LN involved ( 5%) Intrathyroidal PTC, 2-4 cm ( 5%) Multifocal PMC ( 4-6%) pn1 without extranodal extension, 3 LN involved (2%) Minimally invasive FTC ( 2-3%) Intrathyroidal, < 4 cm, BRAF wild type* ( 1-2%) Intrathyroidal unifocal PMC, BRAF mutated*, ( 1-2%) Intrathyroidal, encapsulated, FV-PTC ( 1-2%) Unifocal PMC ( 1-2%)
22 Risk of Structural Disease Recurrence (In patients without structurally identifiable disease after initial therapy) High Risk Gross extrathyroidal extension, incomplete tumor resection, distant metastases, or lymph node >3 cm Intermediate Risk Aggressive histology, minor extrathyroidal extension, vascular invasion, or > 5 involved lymph nodes (0.2-3 cm) Low Risk Intrathyroidal DTC 5 LN micrometastases (< 0.2 cm) FTC, extensive vascular invasion ( 30-55%) pt4a gross ETE ( 30-40%) pn1 with extranodal extension, >3 LN involved ( 40%) PTC, > 1 cm, TERT mutated ± BRAF mutated* (>40%) pn1, any LN > 3 cm ( 30%) PTC, extrathyroidal, BRAF mutated*( 10-40%) PTC, vascular invasion ( 15-30%) Clinical N1 ( 20%) pn1, > 5 LN involved ( 20%) Intrathyroidal PTC, < 4 cm, BRAF mutated* ( 10%) pt3 minor ETE ( 3-8%) pn1, all LN < 0.2 cm ( 5%) pn1, 5 LN involved ( 5%) Intrathyroidal PTC, 2-4 cm ( 5%) Multifocal PMC ( 4-6%) pn1 without extranodal extension, 3 LN involved (2%) Minimally invasive FTC ( 2-3%) Intrathyroidal, < 4 cm, BRAF wild type* ( 1-2%) Intrathyroidal unifocal PMC, BRAF mutated*, ( 1-2%) Intrathyroidal, encapsulated, FV-PTC ( 1-2%) Unifocal PMC ( 1-2%)


23 JAMA 1946 Dr Saul Hertz treating a hyperthyroid patient January 1941

24 JCEM 2015
25 Radioiodine Remnant Ablation/Adjuvant Therapy/Therapy Recommendation 51 (Table 14) ATA recurrence risk TNM Staging ATA Low Risk T1a/N0,NX/M0,MX ATA Low Risk T1b, T2/N0,NX/M0,MX ATA Low to intermediate risk T3/N0,NX/M0,MX ATA Low to intermediate risk T1-3/N1a/M0,MX ATA Low to intermediate risk AnyT1-3/N1b/M0,MX Description T < 1cm (unifocal or multifocal) T 1-4 cm T > 4cm or microscopic invasion Hippocratic Oath (modern version) ATA I will High apply, riskfor the benefit of the sick, T4/any all measures N/any [that] M are required, ATA High risk M1 (any T, any N) Central compartment LN metastases Lateral compartment LN metastases Gross extrathyroidal extension Distant metastases avoiding those twin traps of overtreatment and therapeutic nihilism. Post-surgical RAI indicated? No (Strong, Mod) Not routine (W,L) Consider Consider (size and number) Consider (size, number,age) Yes Yes
26 Radioiodine Remnant Ablation/Adjuvant Therapy/Therapy Recommendation 51 (Table 14) ATA recurrence risk TNM Staging ATA Low Risk T1a/N0,NX/M0,MX ATA Low Risk T1b, T2/N0,NX/M0,MX ATA Low to intermediate risk T3/N0,NX/M0,MX ATA Low to intermediate risk T1-3/N1a/M0,MX ATA Low to intermediate risk AnyT1-3/N1b/M0,MX ATA High risk T4/any N/any M ATA High risk M1 (any T, any N) Description T < 1cm (unifocal or multifocal) T 1-4 cm T > 4cm or microscopic invasion Central compartment LN metastases Lateral compartment LN metastases Gross extrathyroidal extension Distant metastases Post-surgical RAI indicated? No (S,M) Not routine (W,L) Consider Consider (size and number) Consider (size, number,age) Yes (S,M) Yes (S,M)
27 Radioiodine Remnant Ablation/Adjuvant Therapy/Therapy Recommendation 51 (Table 14) ATA recurrence risk TNM Staging ATA Low Risk T1a/N0,NX/M0,MX ATA Low Risk T1b, T2/N0,NX/M0,MX ATA Low to intermediate risk T3/N0,NX/M0,MX ATA Low to intermediate risk T1-3/N1a/M0,MX ATA Low to intermediate risk AnyT1-3/N1b/M0,MX ATA High risk T4/any N/any M ATA High risk M1 (any T, any N) Description T < 1cm (unifocal or multifocal) T 1-4 cm T > 4cm or microscopic invasion Central compartment LN metastases Lateral compartment LN metastases Gross extrathyroidal extension Distant metastases Post-surgical RAI indicated? No (S,M) Not routine (W,L) Consider (W,L) Consider (W,L) (size and number) Consider (W,L) (size, number,age) Yes (S,M) Yes (S,M)
28 JCEM 98: , RCT patients 4-12 mo FU 2015 Recommendations ATA low risk disease ATA intermediate risk (lower risk features) 30 mci 131 I generally favored over higher doses Strong recommendation, High-quality evidence
29 Radioiodine Remnant Ablation LT4 withdrawal vs rhtsh RECOMMENDATION 54A ATA low and intermediate risk disease Can use rhtsh (Thyrogen) Noninferiority to WD, short-term QOL Long-term outcomes (observations) Strong recommendation, Moderate-quality evidence Pacini F, JCEM, 2006 Lee J, Thyroid, 2010 Mallick U, NEJM 2012 Schlumberger M, NEJM 2012 Molinaro E, JCEM 2013 Tu J, Radiother Oncol 2014
30 Patient #3 56 yo male FNA PTC US no abnormal LN Thyroidectomy and central neck dissection Path report: 3.8 cm FVPTC Extrathyroid extension, negative margins No vascular invasion 11/12 LN involved, largest 1.2 cm, no ENE T3N1aMX, Stage III, ATA intermediate risk Post-op TSH 0.2, Tg 1.8, Ab <2 Above ablation dose mci 131I, consider rhtsh
31 Patient #4 41 yo female PTC Thyroidectomy Path report: 3.5 cm PTC margins Microscopic extrathyroid extension, negative No vascular invasion No LN removed T3N0MX, Stage I, ATA low to intermediate risk 30 mci 131I (rhtsh), WBS TB only, Tg month FU: TSH 0.4, Tg 0.2, neck US negative 1 year FU: TSH 0.3, Tg 0.1, neck US negative Risk of structural recurrence: <5%, 10-20%, 50%, >75%
32 Assessing Response to Therapy Excellent Response Indeterminate (good) Response Incomplete Response Suppressed Tg < 0.2 ng/ml Detectable, but < 1 > 1 ng/ml ng/ml Stimulated Tg < 1 ng/ml < 10 ng/ml > 10 ng/ml Tg Trend Low Declining Stable or rising Tg antibodies Absent Absent or declining Persistent or rising Neck exam Normal Normal Palpable disease Imaging Negative Indeterminate Clinically Insignificant Positive Lower Risk Estimate Stable Risk Estimate Raise Risk Estimate Courtesy of RM Tuttle
33 Application of Dynamic Risk Classification Risk of Persistent/Recurrent Structural Disease % initial excellent indeterminate incomplete Low Intermediate High Tuttle RM, Thyroid 2010
34 Management Approaches Based on Response to Therapy Low to intermediate risk patients Excellent Indeterminate Biochemical Incomplete Structural Incomplete TSH target <0.1 <0.1 Serum Tg yearly yearly 6-12 months 3-6 months Neck US 5 years 1-3 years 6-12 months 3-6 months Stim Tg No maybe consider consider WBS No maybe consider consider Cross-sectional imaging No No consider yes More aggressive monitoring for high risk patients

35 TSH targets based on benefits vs risks Table 17
36 Patient #5 68 yo female presented with back pain, no neuro Sx 2.6 cm L2 lesion, Bx FTC PET/CT 5-6 bone mets, multiple pulm nodules (<1.5 cm) Thyroidectomy 2.3 cm FTC with vascular invasion Post-op Tg 1200 (TSH 0.06) THW diagnostic WBS THW mci 131I EBRT or thermal ablation to L2 prior to RAI Start TKI (lenvatinib, sorafenib) Entry into clinical trial Phone a friend bryan.haugen@ucdenver.edu
37 Patient #5 68 yo female metastatic FTC 2.6 cm L2 lesion [C38] What is the role for directed therapy in advanced thyroid cancer? RECOMMENDATION 93 B) Thermal ablation or stereotactic radiation should be considered prior to initiation of systemic treatment when the individual distant metastases are symptomatic or at high risk of local complications. (Strong recommendation, Moderate-quality evidence) Consider EBRT or thermal ablation to L2 prior to RAI
38 Radioidine-refractory DTC How is radioiodine refractory DTC defined? (new question) RECOMMENDATION 91 (NEW) Radioiodine-refractory structurally-evident DTC is defined in patients with appropriate TSH stimulation and iodine preparation in four basic ways: 1) the malignant/metastatic tissue does not ever concentrate radioiodine 2) the tumor tissue loses the ability to concentrate radioiodine 3) radioiodine is concentrated in some lesions but not in others 4) metastatic disease progresses despite significant concentration of radioiodine. When a patient with DTC is classified as refractory to radioiodine, there is no indication for further radioiodine treatment. (Strong recommendation, Moderate-quality evidence)
39 What to do with patients who have RAIrefractory DTC? Monitor (New recommendation 92) Directed Therapy (New recommendation 93) Surgery, EBRT, thermal ablation Clinical trials (New recommendation 95) Clinicaltrials.gov Systemic therapy (New recommendations 96-99) Kinase inhibitors, Bone-directed therapy
40 Management Algorithm for Patients with RAIR DTC (structural disease) Consider directed therapy Few lesions RAIR DTC patient Active surveillance TSH suppression Yes Many lesions Progressive (<12 months) or symptomatic disease? No Consider entry into a clinical trial Consider systemic therapy Consider adding bone-directed therapy for bone metastases FDA-approved therapy Failure of approved therapy Consider off-label therapy Clinical trial not available or appropriate
41 Summary US sonographic risk patterns Don t need to biopsy every nodule > 1 cm Don t have to biopsy any nodule < 1 cm Lobectomy may be reasonable approach More detailed pathology reports Use of selective radioiodine, lower doses Cross-sectional imaging for higher risk disease Stage (AJCC/TNM), ATA recurrence risk, response to therapy Individualize TH therapy and TSH targets Radioiodine refractory DTC Definition, monitoring, directed-therapy, clinical trials and systemic therapy
42 Guidelines Task Force Erik Alexander Keith Bible Jerry Doherty Susan Mandel Yuri Nikiforov Furio Pacini Greg Randolph Anna Sawka Martin Schlumberger Kathryn Schuff Steve Sherman Julie Ann Sosa Dave Steward Mike Tuttle Len Wartofsky Acknowledgements
How Will (Should) the Latest Guidelines Affect the Endocrinologist s Management of Thyroid Cancer? AACE 2017
 the Latest Guidelines Affect the Endocrinologist s Management of Thyroid Cancer? AACE 2017") How Will (Should) the Latest Guidelines Affect the Endocrinologist s Management of Thyroid Cancer? AACE 2017 Bryan R. Haugen, MD University of Colorado, School of Medicine Outline Some statistics New guidelines
How Will (Should) the Latest Guidelines Affect the Endocrinologist s Management of Thyroid Cancer? AACE 2017 Bryan R. Haugen, MD University of Colorado, School of Medicine Outline Some statistics New guidelines
2015 ATA Thyroid Nodule and DTC Guidelines: Perspectives from the Chair What were you thinking????
 2015 ATA Thyroid Nodule and DTC Guidelines: Perspectives from the Chair What were you thinking???? Bryan R. Haugen, MD University of Colorado, School of Medicine Outline Some statistics New guidelines
2015 ATA Thyroid Nodule and DTC Guidelines: Perspectives from the Chair What were you thinking???? Bryan R. Haugen, MD University of Colorado, School of Medicine Outline Some statistics New guidelines
Dynamic Risk Stratification:
 Dynamic Risk Stratification: Using Risk Estimates to Guide Initial Management R Michael Tuttle, MD Clinical Director, Endocrinology Service Memorial Sloan Kettering Cancer Center Professor of Medicine
Dynamic Risk Stratification: Using Risk Estimates to Guide Initial Management R Michael Tuttle, MD Clinical Director, Endocrinology Service Memorial Sloan Kettering Cancer Center Professor of Medicine
Key Topics in Thyroid Cancer Worldwide epidemic What Should the Endocrinologist and Surgeon do?
 Key Topics in Thyroid Cancer Worldwide epidemic What Should the Endocrinologist and Surgeon do? Martin Schlumberger Gustave Presenter Roussy Name and Université Paris Saclay, Villejuif, France 1 Disclosure
Key Topics in Thyroid Cancer Worldwide epidemic What Should the Endocrinologist and Surgeon do? Martin Schlumberger Gustave Presenter Roussy Name and Université Paris Saclay, Villejuif, France 1 Disclosure
Gerard M. Doherty, MD
 Surgical Management of Differentiated Thyroid Cancer: Update on 2015 ATA Guidelines Gerard M. Doherty, MD Chair of Surgery Utley Professor of Surgery and Medicine Boston University Surgeon-in-Chief Boston
Surgical Management of Differentiated Thyroid Cancer: Update on 2015 ATA Guidelines Gerard M. Doherty, MD Chair of Surgery Utley Professor of Surgery and Medicine Boston University Surgeon-in-Chief Boston
I-131 ABLATION AND ADJUVANT THERAPY OF THYROID CANCER
 AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGISTS Advances in Medical and Surgical Management of Thyroid Cancer January 23-24, 2015 I-131 ABLATION AND ADJUVANT THERAPY OF THYROID CANCER 2015 Leonard Wartofsky,
AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGISTS Advances in Medical and Surgical Management of Thyroid Cancer January 23-24, 2015 I-131 ABLATION AND ADJUVANT THERAPY OF THYROID CANCER 2015 Leonard Wartofsky,
Risk Adapted Follow-Up
 Risk Adapted Follow-Up Individualizing Follow- Up Strategies R Michael Tuttle, MD Clinical Director, Endocrinology Service Memorial Sloan Kettering Cancer Center Professor of Medicine Weill Medical College
Risk Adapted Follow-Up Individualizing Follow- Up Strategies R Michael Tuttle, MD Clinical Director, Endocrinology Service Memorial Sloan Kettering Cancer Center Professor of Medicine Weill Medical College
Management of Recurrent Thyroid Cancer
 Management of Recurrent Thyroid Cancer Eric Genden, MD, MHA Isidore Professor and Chairman Department of Otolaryngology- Head and Neck Surgery Senior Associate Dean for Clinical Affairs The Icahn School
Management of Recurrent Thyroid Cancer Eric Genden, MD, MHA Isidore Professor and Chairman Department of Otolaryngology- Head and Neck Surgery Senior Associate Dean for Clinical Affairs The Icahn School
Towards a selective use of postoperative radioiodine in thyroid cancer patients
 Towards a selective use of postoperative radioiodine in thyroid cancer patients Martin Schlumberger Gustave Presenter Roussy Name and Université Paris Saclay, Villejuif, France 1 Disclosure Relevant financial
Towards a selective use of postoperative radioiodine in thyroid cancer patients Martin Schlumberger Gustave Presenter Roussy Name and Université Paris Saclay, Villejuif, France 1 Disclosure Relevant financial
Strategies for detection of recurrent disease in longterm follow-up of differentiated thyroid cancer
 Strategies for detection of recurrent disease in longterm follow-up of differentiated thyroid cancer A rational approach to longterm follow-up based on dynamic risk assessment. World Congress on Thyroid
Strategies for detection of recurrent disease in longterm follow-up of differentiated thyroid cancer A rational approach to longterm follow-up based on dynamic risk assessment. World Congress on Thyroid
Differentiated Thyroid Carcinoma
 Differentiated Thyroid Carcinoma The GOOD cancer? Jennifer Sipos, MD Associate Professor of Medicine Director, Benign Thyroid Program Division of Endocrinology, Diabetes and Metabolism The Ohio State University
Differentiated Thyroid Carcinoma The GOOD cancer? Jennifer Sipos, MD Associate Professor of Medicine Director, Benign Thyroid Program Division of Endocrinology, Diabetes and Metabolism The Ohio State University
Dilemmas in Cytopathology and Histopathology
 Dilemmas in Cytopathology and Histopathology Yuri E. Nikiforov, MD, PhD Division of Molecular & Genomic Pathology University of Pittsburgh Medical Center, USA Objectives Discuss new WHO classification
Dilemmas in Cytopathology and Histopathology Yuri E. Nikiforov, MD, PhD Division of Molecular & Genomic Pathology University of Pittsburgh Medical Center, USA Objectives Discuss new WHO classification
2015 American Thyroid Association Thyroid Nodule and Cancer Guidelines
 2015 American Thyroid Association Thyroid Nodule and Cancer Guidelines Angela M. Leung, MD, MSc, ECNU November 5, 2016 Outline Workup of nontoxic thyroid nodule(s) Ultrasound FNAB Management of FNAB results
2015 American Thyroid Association Thyroid Nodule and Cancer Guidelines Angela M. Leung, MD, MSc, ECNU November 5, 2016 Outline Workup of nontoxic thyroid nodule(s) Ultrasound FNAB Management of FNAB results
WTC 2013 Panel Discussion: Minimal disease
 WTC 2013 Panel Discussion: Minimal disease Susan J. Mandel MD MPH Panelists Ken Ain Yasuhiro Ito Stephanie Lee Erich Sturgis Mark Urken Faculty/Presenter Disclosure Relationships with commercial interests
WTC 2013 Panel Discussion: Minimal disease Susan J. Mandel MD MPH Panelists Ken Ain Yasuhiro Ito Stephanie Lee Erich Sturgis Mark Urken Faculty/Presenter Disclosure Relationships with commercial interests
Approach to Thyroid Nodules
 Approach to Thyroid Nodules Alice Y.Y. Cheng, MD, FRCPC Twitter: @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
Approach to Thyroid Nodules Alice Y.Y. Cheng, MD, FRCPC Twitter: @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
Preoperative Evaluation
 Preoperative Evaluation Lateral compartment lymph nodes are easier to detect and are amenable to FNA Central compartment lymph nodes are much more difficult to detect and FNA (Tg washout testing is compromised)
Preoperative Evaluation Lateral compartment lymph nodes are easier to detect and are amenable to FNA Central compartment lymph nodes are much more difficult to detect and FNA (Tg washout testing is compromised)
I treatment for differentiated thyroid carcinoma Current guidelines
 131 I treatment for differentiated thyroid carcinoma Current guidelines François Jamar, UCL Brussels francois.jamar@uclouvain.be IAEA-Belnuc Theranostics course Brussels, October 5 th, 2017 131 I treatment
131 I treatment for differentiated thyroid carcinoma Current guidelines François Jamar, UCL Brussels francois.jamar@uclouvain.be IAEA-Belnuc Theranostics course Brussels, October 5 th, 2017 131 I treatment
Ultrasound for Pre-operative Evaluation of Well Differentiated Thyroid Cancer
 Ultrasound for Pre-operative Evaluation of Well Differentiated Thyroid Cancer Its Not Just About the Nodes AACE Advances in Medical and Surgical Management of Thyroid Cancer - 2017 Robert A. Levine, MD,
Ultrasound for Pre-operative Evaluation of Well Differentiated Thyroid Cancer Its Not Just About the Nodes AACE Advances in Medical and Surgical Management of Thyroid Cancer - 2017 Robert A. Levine, MD,
What s an NIFTP? Keeping Up To Date in Thyroid 2018
 What s an NIFTP? Keeping Up To Date in Thyroid 2018 Kathleen Hands, MD, FACE, ECNU Director, Thyroid Center of South Texas Assistant Clinical Professor UTHSCSA DrHands@Thyroid-Center.com 210-844-6163 text
What s an NIFTP? Keeping Up To Date in Thyroid 2018 Kathleen Hands, MD, FACE, ECNU Director, Thyroid Center of South Texas Assistant Clinical Professor UTHSCSA DrHands@Thyroid-Center.com 210-844-6163 text
Surgical Management of Thyroid Disease. Tom Shi Connally, MD, FACS
 Surgical Management of Thyroid Disease Tom Shi Connally, MD, FACS Disclosures Speaker Bureau: Veracyte Castle Diagnostics Objectives Understand the role of ultrasound and FNA in managing thyroid cancer
Surgical Management of Thyroid Disease Tom Shi Connally, MD, FACS Disclosures Speaker Bureau: Veracyte Castle Diagnostics Objectives Understand the role of ultrasound and FNA in managing thyroid cancer
Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer
 Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer AACE - Advances in Medical and Surgical Management of Thyroid Cancer - 2018 Robert A. Levine, MD, FACE, ECNU Thyroid Center of New Hampshire Geisel
Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer AACE - Advances in Medical and Surgical Management of Thyroid Cancer - 2018 Robert A. Levine, MD, FACE, ECNU Thyroid Center of New Hampshire Geisel
PRACTICE GUIDELINES: Thyroid Nodules and Cancer 2017 ESEO Alexandria
 PRACTICE GUIDELINES: Thyroid Nodules and Cancer 2017 ESEO Alexandria James V. Hennessey MD Associate Professor of Medicine Harvard Medical School Case 1 28 year old woman sees OB for routine visit ROS:
PRACTICE GUIDELINES: Thyroid Nodules and Cancer 2017 ESEO Alexandria James V. Hennessey MD Associate Professor of Medicine Harvard Medical School Case 1 28 year old woman sees OB for routine visit ROS:
Thyroid Cancer: When to Treat? MEGAN R. HAYMART, MD
 Thyroid Cancer: When to Treat? MEGAN R. HAYMART, MD ASSOCIATE PROFESSOR OF MEDICINE UNIVERSITY OF MICHIGAN MICHIGAN AACE 2018 ANNUAL MEETING Thyroid Cancer: When Not to Treat? FOCUS WILL BE ON LOW-RISK
Thyroid Cancer: When to Treat? MEGAN R. HAYMART, MD ASSOCIATE PROFESSOR OF MEDICINE UNIVERSITY OF MICHIGAN MICHIGAN AACE 2018 ANNUAL MEETING Thyroid Cancer: When Not to Treat? FOCUS WILL BE ON LOW-RISK
Sonographic Features of Thyroid Nodules & Guidelines for Management
 Sonographic Features of Thyroid Nodules & Guidelines for Management Mark A. Lupo, MD, FACE, ECNU Thyroid & Endocrine Center of Florida Assistant Clinical Professor of Medicine Florida State University,
Sonographic Features of Thyroid Nodules & Guidelines for Management Mark A. Lupo, MD, FACE, ECNU Thyroid & Endocrine Center of Florida Assistant Clinical Professor of Medicine Florida State University,
- RET/PTC rearrangement: 20% papillary thyroid cancer - RET: medullary thyroid cancer
 Thyroid Cancer UpToDate: Introduction: Risk Factors: Biology: Symptoms: Diagnosis: 1. Lenvina is the first line therapy with powerful durable response and superior PFS in pts with RAI-refractory disease.
Thyroid Cancer UpToDate: Introduction: Risk Factors: Biology: Symptoms: Diagnosis: 1. Lenvina is the first line therapy with powerful durable response and superior PFS in pts with RAI-refractory disease.
PEDIATRIC Ariel Katz MD
 PEDIATRIC Ariel Katz MD Dept. Otolaryngology Head &Neck Surgery Wolfson Medical Center Holon, Israel OBJECTIVES Overview/Background Epidemiology/Etiology Intro to Guidelines Workup Treatment Follow-Up
PEDIATRIC Ariel Katz MD Dept. Otolaryngology Head &Neck Surgery Wolfson Medical Center Holon, Israel OBJECTIVES Overview/Background Epidemiology/Etiology Intro to Guidelines Workup Treatment Follow-Up
Case-Based Discussion of Thyroid Cancer Therapy
 Case-Based Discussion of Thyroid Cancer Therapy Matthew D. Ringel, MD Ralph W. Kurtz Chair and Professor of Medicine Director, Division of Endocrinology The Ohio State University Co-Leader, Molecular Biology
Case-Based Discussion of Thyroid Cancer Therapy Matthew D. Ringel, MD Ralph W. Kurtz Chair and Professor of Medicine Director, Division of Endocrinology The Ohio State University Co-Leader, Molecular Biology
Thyroid Surgery: Lobectomy, total thyroidectomy, LN biopsies or only watchful waiting?
 Thyroid Surgery: Lobectomy, total thyroidectomy, LN biopsies or only watchful waiting? Jacob Moalem, MD, FACS Associate Professor Endocrine Surgery and Endocrinology URMC Agenda 1. When is lobectomy alone
Thyroid Surgery: Lobectomy, total thyroidectomy, LN biopsies or only watchful waiting? Jacob Moalem, MD, FACS Associate Professor Endocrine Surgery and Endocrinology URMC Agenda 1. When is lobectomy alone
CLINICAL GUIDELINES. Introductory notes:
 CLINICAL GUIDELINES Thyroid Ultrasound Reporting Guideline Recommendations Thomas Gilbert, M.D., M.P.P., Robert Kanterman, M.D., Erik Rockswold, MHA Updated June, 2017 Introductory notes: Thyroid nodules
CLINICAL GUIDELINES Thyroid Ultrasound Reporting Guideline Recommendations Thomas Gilbert, M.D., M.P.P., Robert Kanterman, M.D., Erik Rockswold, MHA Updated June, 2017 Introductory notes: Thyroid nodules
Anca M. Avram, M.D. Professor of Radiology
 Thyroid Cancer Theranostics: the case for pre-treatment diagnostic staging 131-I scans for 131-I therapy planning Anca M. Avram, M.D. Professor of Radiology Department of Nuclear Medicine University of
Thyroid Cancer Theranostics: the case for pre-treatment diagnostic staging 131-I scans for 131-I therapy planning Anca M. Avram, M.D. Professor of Radiology Department of Nuclear Medicine University of
4/22/2010. Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey.
 Management of Differentiated Thyroid Cancer: Head Neck Surgeon Perspective Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey Thyroid gland Small endocrine gland:
Management of Differentiated Thyroid Cancer: Head Neck Surgeon Perspective Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey Thyroid gland Small endocrine gland:
Minimalistic Initial Therapy Options For Low Risk Papillary Thyroid Cancer
 Minimalistic Initial Therapy Options For Low Risk Papillary Thyroid Cancer An emphasis on proper patient selection R Michael Tuttle, MD Clinical Director, Endocrinology Service Memorial Sloan Kettering
Minimalistic Initial Therapy Options For Low Risk Papillary Thyroid Cancer An emphasis on proper patient selection R Michael Tuttle, MD Clinical Director, Endocrinology Service Memorial Sloan Kettering
The use of Radioactive Iodine (RAI) for Differentiated Thyroid Cancer
 for Differentiated Thyroid Cancer") The use of Radioactive Iodine (RAI) for Differentiated Thyroid Cancer Wendy Sacks, M.D. Cedars Sinai Medical Center California Chapter Annual Meeting, AACE Nov 5, 2016 Increasing Incidence of Thyroid Cancer
The use of Radioactive Iodine (RAI) for Differentiated Thyroid Cancer Wendy Sacks, M.D. Cedars Sinai Medical Center California Chapter Annual Meeting, AACE Nov 5, 2016 Increasing Incidence of Thyroid Cancer
How good are we at finding nodules? Thyroid Nodules Thyroid Cancer Epidemiology Initial management Long-term follow up Disease-free status
 New Perspectives in Thyroid Cancer Jennifer Sipos, MD Assistant Professor of Medicine Division of Endocrinology The Ohio State University Outline Thyroid Nodules Thyroid Cancer Epidemiology Initial management
New Perspectives in Thyroid Cancer Jennifer Sipos, MD Assistant Professor of Medicine Division of Endocrinology The Ohio State University Outline Thyroid Nodules Thyroid Cancer Epidemiology Initial management
Management of Thyroid Nodules. February 2 nd, 2018 Sarah Hopkins
 Management of Thyroid Nodules February 2 nd, 2018 Sarah Hopkins No disclosures Goals: Review Initial Evaluation of Thyroid Nodules Review Indications for Biopsy Approach to Multinodular Goiter Review Management
Management of Thyroid Nodules February 2 nd, 2018 Sarah Hopkins No disclosures Goals: Review Initial Evaluation of Thyroid Nodules Review Indications for Biopsy Approach to Multinodular Goiter Review Management
Initial surgery for differentiated thyroid cancer: What is the appropriate extent and attendant risks and benefits?
 Initial surgery for differentiated thyroid cancer: What is the appropriate extent and attendant risks and benefits? Julie Ann Sosa, MD MA FACS Professor of Surgery and Medicine Chief, Section of Endocrine
Initial surgery for differentiated thyroid cancer: What is the appropriate extent and attendant risks and benefits? Julie Ann Sosa, MD MA FACS Professor of Surgery and Medicine Chief, Section of Endocrine
3/29/2012. Thyroid cancer- what s new. Thyroid Cancer. Thyroid cancer is now the most rapidly increasing cancer in women
 Thyroid cancer- what s new Thyroid Cancer Changing epidemiology Molecular markers Lymph node dissection Technical advances rhtsh Genetic testing and prophylactic surgery Vandetanib What s new? Jessica
Thyroid cancer- what s new Thyroid Cancer Changing epidemiology Molecular markers Lymph node dissection Technical advances rhtsh Genetic testing and prophylactic surgery Vandetanib What s new? Jessica
Objectives. How to Investigate Thyroid Nodules like A Pro
 How to Investigate Thyroid Nodules like A Pro Chris Sadler, MA, PA C, CDE, DFAAPA Medical Science Outcomes Liaison Intarcia Diabetes and Endocrine Associates La Jolla, CA Past President ASEPA Disclosures
How to Investigate Thyroid Nodules like A Pro Chris Sadler, MA, PA C, CDE, DFAAPA Medical Science Outcomes Liaison Intarcia Diabetes and Endocrine Associates La Jolla, CA Past President ASEPA Disclosures
131-I Therapy Planning in Thyroid Cancer: The role of diagnostic radioiodine scans
 131-I Therapy Planning in Thyroid Cancer: The role of diagnostic radioiodine scans Anca M. Avram, M.D. Associate Professor of Radiology Department of Nuclear Medicine University of Michigan Ann Arbor,
131-I Therapy Planning in Thyroid Cancer: The role of diagnostic radioiodine scans Anca M. Avram, M.D. Associate Professor of Radiology Department of Nuclear Medicine University of Michigan Ann Arbor,
Persistent & Recurrent Differentiated Thyroid Cancer
 Persistent & Recurrent Differentiated Thyroid Cancer Electron Kebebew University of California, San Francisco Department of Surgery Objectives Risk factors for persistent & recurrent disease Causes of
Persistent & Recurrent Differentiated Thyroid Cancer Electron Kebebew University of California, San Francisco Department of Surgery Objectives Risk factors for persistent & recurrent disease Causes of
Objectives. 1)To recall thyroid nodule ultrasound characteristics that increase the risk of malignancy
To recall thyroid nodule ultrasound characteristics that increase the risk of malignancy") Evaluation and Management of Thyroid Nodules in Primary Care Chris Sadler, MA, PA C, CDE, DFAAPA Medical Science Outcomes Liaison Intarcia Diabetes and Endocrine Associates La Jolla, CA Past President
Evaluation and Management of Thyroid Nodules in Primary Care Chris Sadler, MA, PA C, CDE, DFAAPA Medical Science Outcomes Liaison Intarcia Diabetes and Endocrine Associates La Jolla, CA Past President
Differentiated Thyroid Cancer: Initial Management
 Page 1 ATA HOME GIVE ONLINE ABOUT THE ATA JOIN THE ATA MEMBER SIGN-IN INFORMATION FOR PATIENTS FIND A THYROID SPECIALIST Home Management Guidelines for Patients with Thyroid Nodules and Differentiated
Page 1 ATA HOME GIVE ONLINE ABOUT THE ATA JOIN THE ATA MEMBER SIGN-IN INFORMATION FOR PATIENTS FIND A THYROID SPECIALIST Home Management Guidelines for Patients with Thyroid Nodules and Differentiated
Pediatric Thyroid Cancer Lung Metastases. Liora Lazar MD
 Pediatric Thyroid Cancer Lung Metastases Liora Lazar MD Differentiated thyroid cancer (DTC) The 3rd most common solid tumor in childhood and adolescence Accounting for 1.5%-3% of all childhood cancers
Pediatric Thyroid Cancer Lung Metastases Liora Lazar MD Differentiated thyroid cancer (DTC) The 3rd most common solid tumor in childhood and adolescence Accounting for 1.5%-3% of all childhood cancers
Markers in Thyroid Nodule Evaluation. Yuri E. Nikiforov, MD, PhD Division of Molecular & Genomic Pathology University of Pittsburgh Medical Center
 Markers in Thyroid Nodule Evaluation Yuri E. Nikiforov, MD, PhD Division of Molecular & Genomic Pathology University of Pittsburgh Medical Center Disclosures Quest Diagnostics (consultant) UPMC/CBLPath
Markers in Thyroid Nodule Evaluation Yuri E. Nikiforov, MD, PhD Division of Molecular & Genomic Pathology University of Pittsburgh Medical Center Disclosures Quest Diagnostics (consultant) UPMC/CBLPath
Thyroid Nodule Management
 Thyroid Nodule Management Shane O. LeBeau, MD Clinical Associate Professor of Medicine Clinical Lead, Endocrine Thyroid Unit Division of Endocrinology, Diabetes and Metabolism University of Pittsburgh
Thyroid Nodule Management Shane O. LeBeau, MD Clinical Associate Professor of Medicine Clinical Lead, Endocrine Thyroid Unit Division of Endocrinology, Diabetes and Metabolism University of Pittsburgh
New York, the nation s thyroid gland. Christopher Morley ( ), "Shore Leave"
, Shore Leave") New York, the nation s thyroid gland Christopher Morley (1890-1957), "Shore Leave" Thyroid Literature Medline Thyroid disease 136,053 Thyroid tumors 33,554 New Paper on Thyroid Disease Every 3 Hours New
New York, the nation s thyroid gland Christopher Morley (1890-1957), "Shore Leave" Thyroid Literature Medline Thyroid disease 136,053 Thyroid tumors 33,554 New Paper on Thyroid Disease Every 3 Hours New
Clinical and Molecular Approach to Using Thyroid Needle Biopsy for Nodular Disease
 Clinical and Molecular Approach to Using Thyroid Needle Biopsy for Nodular Disease Robert L. Ferris, MD, PhD Department of Otolaryngology/Head and Neck Surgery and Yuri E. Nikiforov, MD, PhD Division of
Clinical and Molecular Approach to Using Thyroid Needle Biopsy for Nodular Disease Robert L. Ferris, MD, PhD Department of Otolaryngology/Head and Neck Surgery and Yuri E. Nikiforov, MD, PhD Division of
Current Issues in Thyroid Cancer Surgery in 2017
 Current Issues in Thyroid Cancer Surgery in 2017 Dr. David Goldstein MD Msc FRCSC FACS Associate Professor, Department Otolaryngology Head & Neck Surgery, U of T Department of Surgical Oncology, Princess
Current Issues in Thyroid Cancer Surgery in 2017 Dr. David Goldstein MD Msc FRCSC FACS Associate Professor, Department Otolaryngology Head & Neck Surgery, U of T Department of Surgical Oncology, Princess
Ini7al Staging of Follicular Cell-derived Thyroid Cancers: the ATA 2015 IRS and AJCC 8th Ed. Cancer Staging Systems
 12/25/17 9th Annual AACE Advances in Thyroid Cancer Course Tempe, Arizona January 12-13, 2018. Ini7al Staging of Follicular Cell-derived Thyroid Cancers: the ATA 2015 IRS and AJCC 8th Ed. Cancer Staging
12/25/17 9th Annual AACE Advances in Thyroid Cancer Course Tempe, Arizona January 12-13, 2018. Ini7al Staging of Follicular Cell-derived Thyroid Cancers: the ATA 2015 IRS and AJCC 8th Ed. Cancer Staging
A Review of Differentiated Thyroid Cancer
 A Review of Differentiated Thyroid Cancer April 21 st, 2016 FPON Webcast Jonn Wu BMSc MD FRCPC Radiation Oncologist, Vancouver Centre Chair, Provincial H&N Tumour Group, BCCA Clinical Associate Professor,
A Review of Differentiated Thyroid Cancer April 21 st, 2016 FPON Webcast Jonn Wu BMSc MD FRCPC Radiation Oncologist, Vancouver Centre Chair, Provincial H&N Tumour Group, BCCA Clinical Associate Professor,
Long Term Follow-Up for Differentiated Thyroid Cancer: The Mayo Experience
 Long Term Follow-Up for Differentiated Thyroid Cancer: The Mayo Experience Geoffrey B. Thompson, MD Professor of Surgery College of Medicine, Mayo Clinic Differentiated Thyroid Cancer Objectives Overview
Long Term Follow-Up for Differentiated Thyroid Cancer: The Mayo Experience Geoffrey B. Thompson, MD Professor of Surgery College of Medicine, Mayo Clinic Differentiated Thyroid Cancer Objectives Overview
1. Protocol Summary Summary of Trial Design. IoN
 1. Protocol Summary 1.1. Summary of Trial Design Title: Short Title/acronym: IoN Is ablative radioiodine Necessary for low risk differentiated thyroid cancer patients IoN EUDRACT no: 2011-000144-21 Sponsor
1. Protocol Summary 1.1. Summary of Trial Design Title: Short Title/acronym: IoN Is ablative radioiodine Necessary for low risk differentiated thyroid cancer patients IoN EUDRACT no: 2011-000144-21 Sponsor
Thyroid Cancer & rhtsh: When and How?
 Thyroid Cancer & rhtsh: When and How? 8 th Postgraduate Course in Endocrine Surgery Capsis Beach, Crete, September 21, 2006 Quan-Yang Duh, Professor of Surgery, UCSF Increasing Incidence of Thyroid Cancer
Thyroid Cancer & rhtsh: When and How? 8 th Postgraduate Course in Endocrine Surgery Capsis Beach, Crete, September 21, 2006 Quan-Yang Duh, Professor of Surgery, UCSF Increasing Incidence of Thyroid Cancer
Adina Alazraki, MD, FAAP Assistant Professor Radiology and Pediatrics Emory University and Children s Healthcare of Atlanta
 Adina Alazraki, MD, FAAP Assistant Professor Radiology and Pediatrics Emory University and Children s Healthcare of Atlanta Review recently published pediatric guidelines for management of thyroid nodules
Adina Alazraki, MD, FAAP Assistant Professor Radiology and Pediatrics Emory University and Children s Healthcare of Atlanta Review recently published pediatric guidelines for management of thyroid nodules
Correspondence should be addressed to Stan H. M. Van Uum;
 Oncology Volume 2016, Article ID 6496750, 6 pages http://dx.doi.org/10.1155/2016/6496750 Research Article Recombinant Human Thyroid Stimulating Hormone versus Thyroid Hormone Withdrawal for Radioactive
Oncology Volume 2016, Article ID 6496750, 6 pages http://dx.doi.org/10.1155/2016/6496750 Research Article Recombinant Human Thyroid Stimulating Hormone versus Thyroid Hormone Withdrawal for Radioactive
Carcinoma tiroideo differenziato: gestione della persistenza biochimica di malattia
 Carcinoma tiroideo differenziato: gestione della persistenza biochimica di malattia Massimo Torlontano U.O. Endocrinologia IRCCS Casa Sollievo della Sofferenza Thyroid cancer Incidence 1975-2009 (USA)
Carcinoma tiroideo differenziato: gestione della persistenza biochimica di malattia Massimo Torlontano U.O. Endocrinologia IRCCS Casa Sollievo della Sofferenza Thyroid cancer Incidence 1975-2009 (USA)
40 TH EUROPEAN CONGRESS 0F CYTOLOGY LIVERPOOL, UK October 2-5, 2016
 Outcomes from the diagnostic approach of thyroid lesions using US-FNA and LBC in clinical practice Emmanouel Mastorakis MD PhD Cytopathologist Director in Cytopathology Laboratory Regional General Hospital
Outcomes from the diagnostic approach of thyroid lesions using US-FNA and LBC in clinical practice Emmanouel Mastorakis MD PhD Cytopathologist Director in Cytopathology Laboratory Regional General Hospital
Metastatic lymph node characteristics as predictors of recurrence/persistence in the neck and distant metastases in differentiated thyroid cancer
 original article Metastatic lymph node characteristics as predictors of recurrence/persistence in the neck and distant metastases in differentiated thyroid cancer 1 Departamento de Endocrinologia, Universidade
original article Metastatic lymph node characteristics as predictors of recurrence/persistence in the neck and distant metastases in differentiated thyroid cancer 1 Departamento de Endocrinologia, Universidade
MTP: Thyroid Nodules
 Canadian Endocrine Update MTP: Thyroid Nodules Deric Morrison MD, FRCP, ECNU Assistant Professor, Division of Endocrinology and Metabolism, Western University April 2014 Faculty/Presenter Disclosure Faculty:
Canadian Endocrine Update MTP: Thyroid Nodules Deric Morrison MD, FRCP, ECNU Assistant Professor, Division of Endocrinology and Metabolism, Western University April 2014 Faculty/Presenter Disclosure Faculty:
Thyroid Nodules. No conflicts. Overview 5/16/2017. UCSF Internal Medicine Updates May 22, 2017 Elizabeth Murphy, MD, DPhil
 Thyroid Nodules UCSF Internal Medicine Updates May 22, 2017 Elizabeth Murphy, MD, DPhil No conflicts Overview Thyroid nodule and cancer review Ultrasound FNA cytology Nodule follow up Putting it all together
Thyroid Nodules UCSF Internal Medicine Updates May 22, 2017 Elizabeth Murphy, MD, DPhil No conflicts Overview Thyroid nodule and cancer review Ultrasound FNA cytology Nodule follow up Putting it all together
Prophylactic Central Compartment Neck Dissection(CCND) for Papillary Thyroid Cancer: Con
 for Papillary Thyroid Cancer: Con") Prophylactic Central Compartment Neck Dissection(CCND) for Papillary Thyroid Cancer: Con Christopher R. McHenry, M.D. Vice Chairman Department of Surgery MetroHealth Medical Center Professor of Surgery
Prophylactic Central Compartment Neck Dissection(CCND) for Papillary Thyroid Cancer: Con Christopher R. McHenry, M.D. Vice Chairman Department of Surgery MetroHealth Medical Center Professor of Surgery
Evaluation and Management of Thyroid Nodules. Nick Vernetti, MD, FACE Palm Medical Group Las Vegas, Nevada
 Evaluation and Management of Thyroid Nodules Nick Vernetti, MD, FACE Palm Medical Group Las Vegas, Nevada Disclosure Consulting Amgen Speaking Amgen Objectives Understand the significance of incidental
Evaluation and Management of Thyroid Nodules Nick Vernetti, MD, FACE Palm Medical Group Las Vegas, Nevada Disclosure Consulting Amgen Speaking Amgen Objectives Understand the significance of incidental
Thyroid US. Background: Thyroid/Neck US. Use of Office Ultrasound in the Thyroid Surgery Practice
 2010 UCSF Head and Neck Endocrine Surgery Course Use of Office Ultrasound in the Thyroid Surgery Practice Lisa A. Orloff, MD FACS Dept of Otolaryngology-Head and Neck Surgery University of California,
2010 UCSF Head and Neck Endocrine Surgery Course Use of Office Ultrasound in the Thyroid Surgery Practice Lisa A. Orloff, MD FACS Dept of Otolaryngology-Head and Neck Surgery University of California,
Thyroid Nodule. Disclosure. Learning Objectives P A P A P A 3/18/2014. Nothing to disclose.
 Thyroid Nodule Evaluating the patient with a thyroid nodule and some management options. Miguel V. Valdez PA C Disclosure Nothing to disclose. Learning Objectives Examination of thyroid gland Options for
Thyroid Nodule Evaluating the patient with a thyroid nodule and some management options. Miguel V. Valdez PA C Disclosure Nothing to disclose. Learning Objectives Examination of thyroid gland Options for
Thyroid Cancer I 131 Dosing and Treatment: An update on risk stratification, RAI therapy optimization and radiation risk reduction
 Thyroid Cancer I 131 Dosing and Treatment: An update on risk stratification, RAI therapy optimization and radiation risk reduction 2017 AACE Advances in Medical & Surgical Management of Thyroid Cancer,
Thyroid Cancer I 131 Dosing and Treatment: An update on risk stratification, RAI therapy optimization and radiation risk reduction 2017 AACE Advances in Medical & Surgical Management of Thyroid Cancer,
Oh, I get it, the TSH goes up and down
 Evaluation and Management of the Thyroid Nodule Oh, I get it, the TSH goes up and down UCSF Head and Neck Conference October 24, 2008 Peter A. Singer, M.D. Professor and Chief Clinical Endocrinology University
Evaluation and Management of the Thyroid Nodule Oh, I get it, the TSH goes up and down UCSF Head and Neck Conference October 24, 2008 Peter A. Singer, M.D. Professor and Chief Clinical Endocrinology University
Tania Gallant MD, FRCPC Internal Medicine Update April
 Tania Gallant MD, FRCPC Internal Medicine Update April 28 2017 Disclosures Honoraria/Ad board: Sanofi-Aventis, Janssen, Merck Frosst, Eli-Lilly, Astra Zeneca, Boehringer-Ingelheim Objectives By the end
Tania Gallant MD, FRCPC Internal Medicine Update April 28 2017 Disclosures Honoraria/Ad board: Sanofi-Aventis, Janssen, Merck Frosst, Eli-Lilly, Astra Zeneca, Boehringer-Ingelheim Objectives By the end
THYROID CANCER IN CHILDREN. Humberto Lugo-Vicente MD FACS FAAP Professor Pediatric Surgery UPR School of Medicine
 THYROID CANCER IN CHILDREN Humberto Lugo-Vicente MD FACS FAAP Professor Pediatric Surgery UPR School of Medicine Thyroid nodules Rare Female predominance 4-fold as likely to be malignant Hx Radiation exposure?
THYROID CANCER IN CHILDREN Humberto Lugo-Vicente MD FACS FAAP Professor Pediatric Surgery UPR School of Medicine Thyroid nodules Rare Female predominance 4-fold as likely to be malignant Hx Radiation exposure?
Reference No: Author(s) Approval date: October committee. September Operational Date: Review:
 Approval date: October committee. September Operational Date: Review:") Reference No: Title: Author(s) Systemic Anti-Cancer Therapy (SACT) guidelines for Thyroid cancer Dr Fionnuala Houghton Consultant Clinical Oncologist & Dr Lois Mulholland Consultant Clinical Oncologist
Reference No: Title: Author(s) Systemic Anti-Cancer Therapy (SACT) guidelines for Thyroid cancer Dr Fionnuala Houghton Consultant Clinical Oncologist & Dr Lois Mulholland Consultant Clinical Oncologist
Thyroid Carcinoma. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) Version NCCN.org. Continue
 Version NCCN.org. Continue") + NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) Version 1.2016 NCCN.org Continue Version 1.2016, 07/08/2016 National Comprehensive Cancer Network, Inc. 2016, All rights reserved. The
+ NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) Version 1.2016 NCCN.org Continue Version 1.2016, 07/08/2016 National Comprehensive Cancer Network, Inc. 2016, All rights reserved. The
Improving the Long Term Management of Benign Thyroid Nodules
 25 th Annual Scientific AACE Clinical Congress Improving the Long Term Management of Benign Thyroid Nodules Stephanie L. Lee, MD, PhD Director, Thyroid Health Center Section of Endocrinology, Diabetes
25 th Annual Scientific AACE Clinical Congress Improving the Long Term Management of Benign Thyroid Nodules Stephanie L. Lee, MD, PhD Director, Thyroid Health Center Section of Endocrinology, Diabetes
Disclosures Nodal Management in Differentiated Thyroid Carcinoma
 Disclosures Nodal Management in Differentiated Thyroid Carcinoma Nothing to disclose Jonathan George, MD, MPH Assistant Professor UCSF Head and Neck Oncologic & Endocrine Surgery Objectives Overview Describe
Disclosures Nodal Management in Differentiated Thyroid Carcinoma Nothing to disclose Jonathan George, MD, MPH Assistant Professor UCSF Head and Neck Oncologic & Endocrine Surgery Objectives Overview Describe
Management Guidelines for Patients with Thyroid Nodules and Differentiated Thyroid Cancer
 THYROID Volume 16, Number 2, 2006 American Thyroid Association Management Guidelines for Patients with Thyroid Nodules and Differentiated Thyroid Cancer The American Thyroid Association Guidelines Taskforce*
THYROID Volume 16, Number 2, 2006 American Thyroid Association Management Guidelines for Patients with Thyroid Nodules and Differentiated Thyroid Cancer The American Thyroid Association Guidelines Taskforce*
Thyroid Nodules. Hossein Gharib, MD, MACP, MACE
 Thyroid Nodules Hossein Gharib, MD, MACP, MACE Professor of Medicine Mayo Clinic College of Medicine President Elect, American College of Endocrinology University Course January 2008 CP1294362-1 Thyroid
Thyroid Nodules Hossein Gharib, MD, MACP, MACE Professor of Medicine Mayo Clinic College of Medicine President Elect, American College of Endocrinology University Course January 2008 CP1294362-1 Thyroid
Noninvasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP)
") Page of Accepted Preprint first posted on September 0 as Manuscript ERC--0 Noninvasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP) Pedro Weslley Rosario, M.D.; Gabriela Franco
Page of Accepted Preprint first posted on September 0 as Manuscript ERC--0 Noninvasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP) Pedro Weslley Rosario, M.D.; Gabriela Franco
5/3/2017. Ahn et al N Engl J Med 2014; 371
 Alan Failor, M.D. Clinical Professor of Medicine Division of Metabolism, Endocrinology and Nutrition University of Washington April 20, 2017 No disclosures to report 1. Appropriately evaluate s in adult
Alan Failor, M.D. Clinical Professor of Medicine Division of Metabolism, Endocrinology and Nutrition University of Washington April 20, 2017 No disclosures to report 1. Appropriately evaluate s in adult
Imaging in Thyroid Cancer
 Imaging in Thyroid Cancer Susan J. Mandel MD MPH University of Pennsylvania School of Medicine Philadelphia, PA I-123 Ultrasound Background Radioiodine ablation of thyroid remnants after surgery is a generally
Imaging in Thyroid Cancer Susan J. Mandel MD MPH University of Pennsylvania School of Medicine Philadelphia, PA I-123 Ultrasound Background Radioiodine ablation of thyroid remnants after surgery is a generally
34 year-old Female with Thyroid Cancer
 34 year-old Female with Thyroid Cancer KATIE O SULLIVAN, MD FELLOW, ADULT/PEDIATRIC ENDOCRINOLOGY UNIVERSITY OF CHICAGO ENDORAMA THURSDAY, SEPTEMBER 15 TH, 2016 Disclosures: I do not have any relevant
34 year-old Female with Thyroid Cancer KATIE O SULLIVAN, MD FELLOW, ADULT/PEDIATRIC ENDOCRINOLOGY UNIVERSITY OF CHICAGO ENDORAMA THURSDAY, SEPTEMBER 15 TH, 2016 Disclosures: I do not have any relevant
Follicular Derived Thyroid Tumors
 Follicular Derived Thyroid Tumors Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for Medical Sciences
Follicular Derived Thyroid Tumors Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for Medical Sciences
YCN Thyroid NSSG. *** VALID ON DATE OF PRINTING ONLY - all guidelines available at *** page 1 of 8 version number: 1.
 YCN Thyroid NSSG Guidelines on Indications for Thyroid Surgery, Prophylactic Level 6 and Radioiodine plus follow-up of low risk differentiated thyroid cancer page 1 of 8 i Document Control Title Author(s)
YCN Thyroid NSSG Guidelines on Indications for Thyroid Surgery, Prophylactic Level 6 and Radioiodine plus follow-up of low risk differentiated thyroid cancer page 1 of 8 i Document Control Title Author(s)
The International Federation of Head and Neck Oncologic Societies. Current Concepts in Head and Neck Surgery and Oncology
 The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
Thyroid Nodules. Family Medicine Refresher Course Geeta Lal MD, FACS April 2, No financial disclosures
 Thyroid Nodules Family Medicine Refresher Course Geeta Lal MD, FACS April 2, 2014 No financial disclosures Objectives Review epidemiology Work up of Thyroid nodules Indications for FNAB Evolving role of
Thyroid Nodules Family Medicine Refresher Course Geeta Lal MD, FACS April 2, 2014 No financial disclosures Objectives Review epidemiology Work up of Thyroid nodules Indications for FNAB Evolving role of
Thyroid Nodules. Dr. HAKIMI, SpAK Dr. MELDA DELIANA, SpAK Dr. SISKA MAYASARI LUBIS, SpA
 Thyroid Nodules ENDOCRINOLOGY DIVISION ENDOCRINOLOGY DIVISION Dr. HAKIMI, SpAK Dr. MELDA DELIANA, SpAK Dr. SISKA MAYASARI LUBIS, SpA Anatomical Considerations The Thyroid Nodule Congenital anomalies Thyroglossal
Thyroid Nodules ENDOCRINOLOGY DIVISION ENDOCRINOLOGY DIVISION Dr. HAKIMI, SpAK Dr. MELDA DELIANA, SpAK Dr. SISKA MAYASARI LUBIS, SpA Anatomical Considerations The Thyroid Nodule Congenital anomalies Thyroglossal
original article INTRODUCTION According to the American Thyroid Association ABSTRACT
 original article Recombinant human TSH versus thyroid hormone withdrawal in adjuvant therapy with radioactive iodine of patients with papillary thyroid carcinoma and clinically apparent lymph node metastases
original article Recombinant human TSH versus thyroid hormone withdrawal in adjuvant therapy with radioactive iodine of patients with papillary thyroid carcinoma and clinically apparent lymph node metastases
AACE-AME 2016 Thyroid Nodule Update
 AACE-AME 2016 Thyroid Nodule Update 26 th Annual AACE Meeting & Clinical Congress Austin May 1-5, 2017 Hossein Gharib, MD, MACP, MACE Professor, Mayo Clinic College of Medicine Past President, American
AACE-AME 2016 Thyroid Nodule Update 26 th Annual AACE Meeting & Clinical Congress Austin May 1-5, 2017 Hossein Gharib, MD, MACP, MACE Professor, Mayo Clinic College of Medicine Past President, American
THYROID CANCER IN CHILDREN
 THYROID CANCER IN CHILDREN Isabel ROCA, Montserrat NEGRE Joan CASTELL HU VALL HEBRON BARCELONA EPIDEMIOLOGY ADULTS males 1,2-2,6 cases /100.000 females 2,0-3,8 cases /100.000 0,02-0,3 / 100.000 children
THYROID CANCER IN CHILDREN Isabel ROCA, Montserrat NEGRE Joan CASTELL HU VALL HEBRON BARCELONA EPIDEMIOLOGY ADULTS males 1,2-2,6 cases /100.000 females 2,0-3,8 cases /100.000 0,02-0,3 / 100.000 children
AACE Thyroid Cancer Tumor board 25 years of the Endocrine and Surgery collaboration
 AACE Thyroid Cancer Tumor board 25 years of the Endocrine and Surgery collaboration Dr. Peter Singer, Endocrinology Dr. Peter Sadow, Pathology Moderator Dr. Greg Randolph, Otolaryngology Relevant Financial
AACE Thyroid Cancer Tumor board 25 years of the Endocrine and Surgery collaboration Dr. Peter Singer, Endocrinology Dr. Peter Sadow, Pathology Moderator Dr. Greg Randolph, Otolaryngology Relevant Financial
Megan R. Haymart, MD 83 rd Annual Meeting of the ATA October 16, 2013
 Megan R. Haymart, MD 83 rd Annual Meeting of the ATA October 16, 2013 Disclosure: Nothing to Disclose Learning Objectives Thyroid cancer - diagnosis - prognosis - treatment - follow-up Thyroid function
Megan R. Haymart, MD 83 rd Annual Meeting of the ATA October 16, 2013 Disclosure: Nothing to Disclose Learning Objectives Thyroid cancer - diagnosis - prognosis - treatment - follow-up Thyroid function
A Risk-Adapted Approach to the Use of Radioactive Iodine and External Beam Radiation in the Treatment of Well-Differentiated Thyroid Cancer
 Both radioactive iodine and external beam radiation can play roles in well-differentiated thyroid cancer. Rebecca Kinkead. Hula No. 3 (detail), 2010. Oil on canvas, 45 37. A Risk-Adapted Approach to the
Both radioactive iodine and external beam radiation can play roles in well-differentiated thyroid cancer. Rebecca Kinkead. Hula No. 3 (detail), 2010. Oil on canvas, 45 37. A Risk-Adapted Approach to the
Thyroid Pathology: It starts and ends with the gross. Causes of Thyrophobia. Agenda. Diagnostic ambiguity. Treatment/prognosis disconnect
 Thyroid Pathology: It starts and ends with the gross Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for
Thyroid Pathology: It starts and ends with the gross Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for
1. Eur J Surg Oncol Jun 22. pii: S (17) doi: /j.ejso [Epub ahead of print]
![1. Eur J Surg Oncol Jun 22. pii: S (17) doi: /j.ejso [Epub ahead of print]](/thumbs/89/99582482.jpg "1. Eur J Surg Oncol Jun 22. pii: S (17) doi: /j.ejso [Epub ahead of print]") 1. Eur J Surg Oncol. 2017 Jun 22. pii: S0748-7983(17)30544-9. doi: 10.1016/j.ejso.2017.06.004. [Epub ahead of print] Management of the lateral neck in well differentiated thyroid cancer. Cracchiolo JR
1. Eur J Surg Oncol. 2017 Jun 22. pii: S0748-7983(17)30544-9. doi: 10.1016/j.ejso.2017.06.004. [Epub ahead of print] Management of the lateral neck in well differentiated thyroid cancer. Cracchiolo JR
Integrating Guidelines, Experience, and Clinical Judgment in the Management of Thyroid Cancer AACE Annual Meeting May 5, 2016
 Integrating Guidelines, Experience, and Clinical Judgment in the Management of Thyroid Cancer AACE Annual Meeting May 5, 2016 Bryan Haugen, M.D. Julie Ann Sosa, M.D. Mike Tuttle, M.D. Peter A. Singer,
Integrating Guidelines, Experience, and Clinical Judgment in the Management of Thyroid Cancer AACE Annual Meeting May 5, 2016 Bryan Haugen, M.D. Julie Ann Sosa, M.D. Mike Tuttle, M.D. Peter A. Singer,
Work Up & Evaluation of Thyroid Nodules In 2013: State of The Art
 Work Up & Evaluation of Thyroid Nodules In 2013: State of The Art BC Surgical Oncology Network, Fall Update Todd McMullen MD PhD FRCSC FACS Endocrine Surgeon Divisions of General Surgery and Oncology Director,
Work Up & Evaluation of Thyroid Nodules In 2013: State of The Art BC Surgical Oncology Network, Fall Update Todd McMullen MD PhD FRCSC FACS Endocrine Surgeon Divisions of General Surgery and Oncology Director,
Thyroid Gland. Protocol applies to all malignant tumors of the thyroid gland, except lymphomas.
 Thyroid Gland Protocol applies to all malignant tumors of the thyroid gland, except lymphomas. Procedures Cytology (No Accompanying Checklist) Partial Thyroidectomy Total Thyroidectomy With/Without Lymph
Thyroid Gland Protocol applies to all malignant tumors of the thyroid gland, except lymphomas. Procedures Cytology (No Accompanying Checklist) Partial Thyroidectomy Total Thyroidectomy With/Without Lymph
Thyroid Nodules: US Risk Stratification. Alex Tessnow, MD, FACE, ECNU University of Texas Southwestern Associate Professor of Medicine Dallas, Texas
 Thyroid Nodules: US Risk Stratification Alex Tessnow, MD, FACE, ECNU University of Texas Southwestern Associate Professor of Medicine Dallas, Texas Which of the following is true? A. All echogenic foci
Thyroid Nodules: US Risk Stratification Alex Tessnow, MD, FACE, ECNU University of Texas Southwestern Associate Professor of Medicine Dallas, Texas Which of the following is true? A. All echogenic foci
Thyroid Nodules: What to do next?
 Thyroid Nodules: What to do next? Ally P. H. Prebtani Professor of Medicine Internal Medicine, Endocrinology & Metabolism McMaster University Canada Copyright 2017 by Sea Courses Inc. All rights reserved.
Thyroid Nodules: What to do next? Ally P. H. Prebtani Professor of Medicine Internal Medicine, Endocrinology & Metabolism McMaster University Canada Copyright 2017 by Sea Courses Inc. All rights reserved.
Thyroid nodules. Most thyroid nodules are benign
 Thyroid nodules Postgraduate Course in General Surgery Jessica E. Gosnell MD Assistant Professor March 22, 2011 Most thyroid nodules are benign thyroid nodules occur in 77% of the world s population palpable
Thyroid nodules Postgraduate Course in General Surgery Jessica E. Gosnell MD Assistant Professor March 22, 2011 Most thyroid nodules are benign thyroid nodules occur in 77% of the world s population palpable
AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS
 AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS PAPILLARY THYROID CARCINOMA Clinical Any age Microscopic to large Female: Male= 2-4:1 Radiation history Lymph nodes Prognosis
AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS PAPILLARY THYROID CARCINOMA Clinical Any age Microscopic to large Female: Male= 2-4:1 Radiation history Lymph nodes Prognosis
Evaluation and Management of Thyroid Nodules. Overview of Thyroid Nodules and Their Management. Thyroid Nodule detection: U/S versus Exam
 Overview of Thyroid Nodules and Their Management Matthew D. Ringel, M.D. Professor of Medicine Divisions of Endocrinology and Oncology, The Ohio State University Co-Director, Thyroid Cancer Unit Arthur
Overview of Thyroid Nodules and Their Management Matthew D. Ringel, M.D. Professor of Medicine Divisions of Endocrinology and Oncology, The Ohio State University Co-Director, Thyroid Cancer Unit Arthur
ATA Guidelines for Medullary Thyroid Cancer: approach to initial management of sporadic and inherited disease
 ATA Guidelines for Medullary Thyroid Cancer: approach to initial management of sporadic and inherited disease Richard T. Kloos, M.D. The Ohio State University Divisions of Endocrinology and Nuclear Medicine
ATA Guidelines for Medullary Thyroid Cancer: approach to initial management of sporadic and inherited disease Richard T. Kloos, M.D. The Ohio State University Divisions of Endocrinology and Nuclear Medicine