MEDULLARY THYROID CANCER and RELATED MEN SYNDROMES. Irina Kovatch, MD SUNY Downstate Medical Center Grand Rounds January 26 th, 2012
|
|
|
- Ashlee Parks
- 6 years ago
- Views:
Transcription
1 MEDULLARY THYROID CANCER and RELATED MEN SYNDROMES Irina Kovatch, MD SUNY Downstate Medical Center Grand Rounds January 26 th, 2012
2 Thyroid Cancer Comprises 95% of all endocrine malignancies and 1.5% of all cancers Has the greatest annual percentage increase in incidence of any cancers (4% per year) Lifetime risk in US is estimated to be 0.8% for women 0.3% in men Median age of diagnosis is 48 years
3 Categories Follicular cell derived or differentiated thyroid cancer papillary thyroid cancer (PTC) follicular cancer (FC) Hurthle cell cancer (HCC) anaplastic cancer (ATC) Non follicular cell derived variants medullary thyroid cancer (MTC) Lymphoma metastases
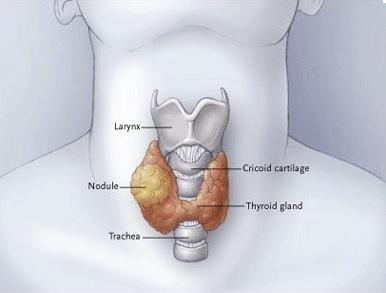
4 Medullary Thyroid Carcinoma Accounts for 5-10% of all thyroid cancers Can occur in a sporadic or hereditary forms (part of MEN 2 syndromes) MEN 2A MEN 2B Familial non-men medullary thyroid carcinoma (FMTC) Originates from the parafollicular cells (C cells) of the thyroid which produce, store, and secrete calcitonin These cells comprise 1% of the total thyroid mass and are dispersed throughout the gland
5 Calcitonin in MTC Basal and stimulated serum calcitonin levels correlate with tumor burden and are always elevated in patients with palpable MTC Calcitonin excess is not associated with hypocalcemia Secretory diarrhea and flushing, most often attributed to elevated calcitonin, are the main paraneoplastic manifestations of advanced MTC MTCs may secrete other hormones, including CEA (>50%) and calcitonin gene-related peptide (CGRP)

6 A solitary mass in a thyroid lobe was removed by total thyroidectomy

7 V Histologically, MTC can be identified by calcitonin staining and by the presence of amyloid in the tumors

8 Clinical Features of Sporadic MTC, MEN 2A, MEN 2B, and FMTC
9 Sporadic vs. Familial MTC Sporadic in 70-80% of cases tumors are usually single and have no familial predisposition multicentric or bilateral disease can be present in 30% Familial in 20-30%, as part of the MEN2A, MEN2B, or isolated familial syndromes all autosomal-dominant inheritance, result from germline mutations in the RET protooncogene
10 MTC Associated with MEN 2 Syndromes Caused by germline mutations in the RET gene on chromosome 10 Gene encodes a transmembrane protein tyrosine kinase The mutations are gain-of-function mutations that cause activation of the protein More than 30 missense mutations have been described
11 Familial Medullary Thyroid Cancer MTC without any other endocrinopathies in >3 affected family members MTC in these patients has a later age of onset and a more indolent clinical course, penetrance is lower Many patients with FMTC are cured by thyroidectomy alone, and those with persistent elevation of calcitonin levels do well for many years The rate of de novo cases is extremely low

12 MEN 2A
13
14 MEN2A MEN2A is the most common hereditary form (66%) presentation in 3 rd -4 th decade of life 90% of gene carriers will develop MTC (multifocal and bilateral) 60% will develop unilateral or bilateral pheochromocytoma 15-30% will develop hyperparathyroidism The aggressiveness of MTC and the probability of developing pheochromocytoma and parathyroid disease are influenced by the specific RET mutation MEN 2A usually has a more favorable long-term outcome than MEN 2B or sporadic MCT

15 MEN 2B
16
17 MEN 2B MEN 2B is the rarest and most aggressive of the hereditary MTC syndromes (presents in infancy) Once MTC presents clinically, it is rarely curable Can be distinguished from MEN2A by the presence of developmental defects and absence of hyperparathyroidism Average age of onset of MTC for patients diagnosed with MEN 2B is 10 years all patients develop MTC all patients have ganglioneuromas and mucosal neuromas 50% develop pheochromocytoma >50% of MEN2B cases occur as a result of de novo germline RET mutations

18 Features of Patients with Hereditary MTC A Bisected thyroid gland from a patient with MEN 2A showing multicentric, bilateral foci of MTC B Adrenalectomy specimen from patient with MEN 2B demonstrating pheochromocytoma C Megacolon in patient with MEN 2B D Tongue of patient with MEN 2B showing characteristic notching 2ry to plexiform neuromas
19 Hereditary MTC Family members of patients with MEN 2 ideally are screened for the RET proto-oncogene Workup includes a detailed family history to inquire about the characteristics of MEN 2 in the patient and family members If MCT is suspected, serum calcium and urinary catecholamines must be determined to evaluate for hyperparathyroidism and possible pheochromocytoma
20 Hereditary MTC Early diagnosis in hereditary MTC is critical because metastases occur in the early stages of disease Lymph node metastases are rarely present in patients in whom genetic testing establishes the diagnosis of MEN 2A or FMTC in childhood and thyroidectomy is performed before the occurrence of a thyroid mass or elevation of calcitonin level
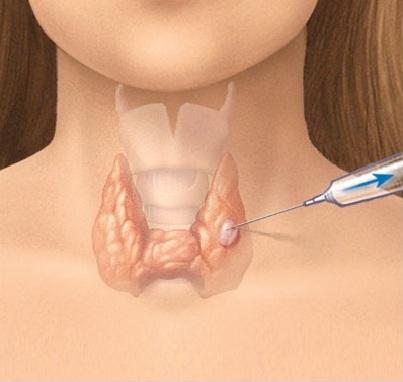
21 Sporadic MTC Most cases of sporadic MTC present as a neck mass detected on physical exam Lymph node metastases are usually present in these patients by the time of diagnosis Diagnosis is made by biopsy (FNA cytology) and measurement of calcitonin levels Germline DNA testing for RET gene mutations is recommended for all patients with MTC regardless of family history ~10% of apparent sporadic MTC will have a de novo mutation in the RET protooncogene
22 MTC Lymphatic Spread Spreads within the central neck compartment Further lymphatic spread can also occur to the lateral neck compartment The outcome of patients with involvement of lower tracheobronchial lymph nodes is equivalent to that of patients with distant metastases The incidence of nodal metastases in palpable, established MTC is 80%
23 Local Invasion of MTC May involve adjacent structures by direct invasion or compression trachea recurrent laryngeal nerve jugular veins and carotid arteries Possible symptoms stridor and upper airway obstruction hoarseness dysphagia bleeding, arterial stenosis or occlusion
24 Metastatic MTC Distant metastases occur in liver, lung, bone and other soft tissues, including breast MTC patients with a palpable mass in the neck have distant metastatic disease in 12-20% of cases Occult remote metastases are the likely cause of persistent hypercalcitoninemia after thyroidectomy and extensive lymph node dissection

25 Spinal metastases from medullary thyroid carcinoma in a patient with MEN 2A

26 Presentation and Diagnosis
27
28 Presentation of MTC Patients with MEN 2A and FMTC have normal appearance diagnosis is made through screening >50% of patients with MEN 2B have a de novo mutation and usually present with a thyroid nodule In patients with palpable MTC >50% have palpable cervical adenopathy up to 80% have histological lymph node metastases 12-20% present with distant metastatasis 13% of patients have respiratory complaints Occasional index cases of MEN 2 present with clinical pheochromocytoma, Hirschsprung's disease, or hyperparathyroidism before the diagnosis of MTC
29
30 Diagnosis of MTC Thyroid nodule FNAB Genetic testing for the relevant mutations in the RET gene is widely available and is very accurate and reliable If positive, need to rule out pheochromocytoma before thyroidectomy Calcitonin is an invaluable serum marker in screening and follow-up settings - correlates with tumor bulk, lymph node metastases, and systemic metastases basal state & after administration of calcium and pentagastrin more useful than CEA, but high CEA levels are associated with a poorer prognosis
31 Preoperative Laboratory Testing
32 Preoperative Laboratory Testing All patients with MTC should be ruled out for MEN2 serum calcium level (to screen for hyperparathyroidism) urine or plasma catecholamines (to r/o pheochromocytoma) A coexisting pheochromocytoma should be treated prior to the thyroidectomy to avoid malignant hypertension on induction

33 Preoperative Imaging Studies
34 Preoperative Imaging Studies Used to determine the extent of local neck disease and the presence of systemic metastases US of the neck is used to evaluate for abnormal lymph nodes in the central and lateral neck in all patients Additional imaging studies are reserved for patients with lymph node metastases or a serum calcitonin level over 400 pg/ml (r/o systemic metastases)
35 Preoperative Imaging Studies CT of the neck, chest, and upper abdomen is useful to evaluate for possible tumor invasion of the upper aerodigestive tract and metastases to the mediastinal lymph nodes, lungs, and liver MRI is the most sensitive imaging modality for detection of liver metastases and is complementary with bone scintigraphy for detection of bone metastases
36 Preoperative Imaging Studies Diagnostic laparoscopy has been advocated prior to initial operation in patients with marked hypercalcitoninemia (>1000 pg/ml) to document the presence of liver disease Staging of MTC is based on tumor size extrathyroidal tumor spread local or regional lymph node metastases systemic metastases

37 American Joint Committee on Cancer TNM Classification

38 American Joint Committee on Cancer TNM Classification
39 Stage Groupings for MTC
40 MTC Treatment
41 MTC Treatment Considerations Clinical course of MTC is usually more aggressive than that of differentiated thyroid cancer, with higher recurrence and mortality rates MTC cells do not take up radioactive iodine, and radiation therapy and chemotherapy are ineffective MTC is multicentric in 90% of patients with the hereditary forms of the disease MTC spreads to the lymph nodes in the central neck in 50% of patients with sporadic and hereditary MTC Presence of lymph node metastases in the central neck is a risk factor for lateral node involvement
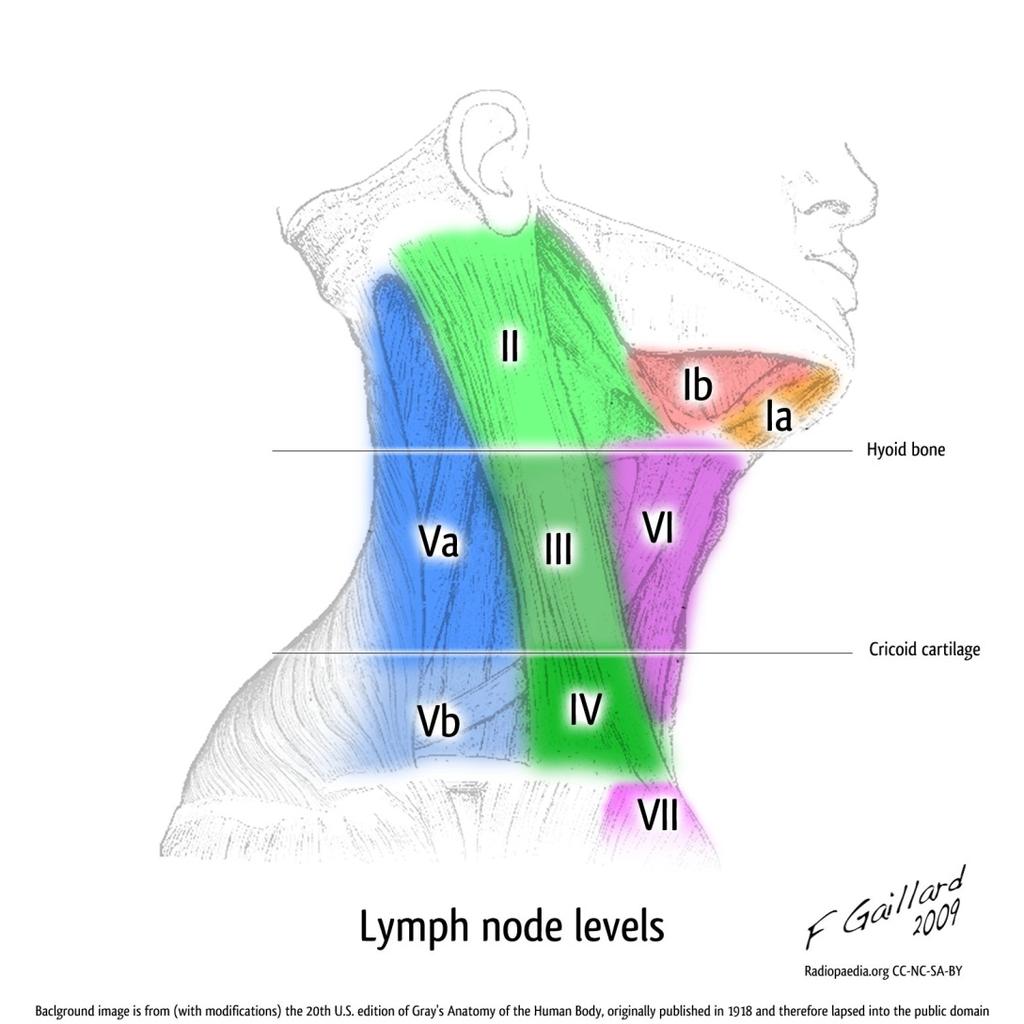
42 MTC Treatment The mainstay of treatment of MTC is surgical For sporadic MTC - at least total thyroidectomy with or without central lymph node dissection search for multicentricity allows appropriate staging A modified neck dissection is indicated in patients with metastatic lymph nodes in the central or lateral neck (removing lymph nodes from levels II-V) Patients with regional lymph node metastases are rarely biochemically cured, even with aggressive bilateral neck dissection
43
44 Preventive Surgery Best chance of cure in familial MTC is provided by complete surgical resection before malignant transformation or before spread beyond the thyroid gland Preventive thyroidectomy is the goal in patients who are identified by genetic testing to have hereditary MTC but who do not yet display clinical evidence of disease It obviates the need for a central compartment lymph node dissection and its risk of hypoparathyroidism
45 Preventive Surgery Patients with MEN 2B (highest risk) should have a total thyroidectomy performed as early as possible, before 6 months of age There is an extremely low likelihood of nodal metastases in patients younger than 8 years with MEN 2A or FMTC and in patients with a normal calcitonin level Patients with mutations with MEN 2A should have thyroidectomy before 5 to 6 years of age Management of patients with FMTC is more controversial (indolent disease course) thyroidectomy before 5 to 10 years of age or based on calcitonin levels
46 Positioning Patient is placed in a supine position with the arms tucked at the sides and a shoulder roll placed lengthwise to extend the neck
47 Incision Transverse collar incision is made two fingerbreadths above the sternal notch along a skin crease

48 Raising Flaps Subcutaneous tissue and the platysma are divided Skin flaps are raised to the level of thyroid cartilage superiorly sternal notch inferiorly sternocleidomastoid muscles laterally

49 Thyroid Gland Exposure Strap muscles are separated in the midline along the median raphe from the prominence of the thyroid cartilage to the sternal notch
50 Middle Thyroid Vein The middle thyroid vein is divided, and the lobe of thyroid is mobilized anteromedially

51 Superior Thyroid Vessels The superior pole vessels are identified by exerting downward traction on the upper pole of the thyroid gland and individually ligated close to the thyroid gland to avoid injury to the external branch of the superior laryngeal nerve

52 Antero-medial Mobilization Areolar tissue between the common carotid artery and the thyroid lobe is dissected using a combination of blunt and sharp techniques, facilitating the anterior and medial rotation of the thyroid lobe
53 Thyroidectomy Inferior thyroid artery is delineated Recurrent laryngeal nerve is identified, traced through its entire course and preserved Routine exposure of the recurrent laryngeal nerve has been shown to reduce the rate of nerve injury Intraoperative nerve monitoring is not necessary and should not be used in lieu of routine exposure of the recurrent laryngeal nerve

54 Division of Inferior Thyroid Vessels Inferior pole of the thyroid gland is mobilized by ligating the tertiary branches of the arteries and veins close to the thyroid gland to preserve the blood supply to the inferior parathyroid gland

55 Clearing the Trachea Remaining thyroid lobe and ligament of Berry are separated from the recurrent laryngeal nerve, preserving the blood supply to the superior parathyroid gland

56 Excision of the Lobe Remaining thyroid lobe and ligament of Berry are separated from the recurrent laryngeal nerve, preserving the blood supply to the superior parathyroid gland
57 Thyroidectomy Contralateral lobe of the thyroid gland is removed in an identical fashion Sternohyoid muscles are re-approximated in the midline, leaving the inferior aspect open (3-4cm) to allow blood to decompress into the subcutaneous space if bleeding develops A drain is not used
58 Parathyroidectomy Leave the parathyroid glands in situ if possible If devascularised autotransplantation Send a small piece for frozen-section (for confirmation) the gland is sliced and autotransplanted into the sternocleidomastoid muscle in patients with sporadic MTC, MTC of MEN2B, and FMTC In patients with MEN2A and a RET mutation, parathyroid gland should be autotransplanted into the brachioradialis muscle of the nondominant forearm (associated with a high risk of hyperparathyroidism)
59 Parathyroidectomy Patients are maintained on calcium and vitamin D supplementation for 4-8 weeks postop Parathyroidectomy with autotransplantation is done in all patients with gross parathyroid enlargement or biochemical evidence of parathyroid disease at the time of operation for MTC
60 Surgery for Palpable Disease Risk for more extensive nodal metastatic disease is increased Total thyroidectomy, parathyroidectomy with autotransplantation, central neck dissection, and ipsilateral level II to V node dissection (maybe bilateral) Persistent disease, evidenced by elevation of calcitonin levels, is present in more than 50% of patients after surgery for palpable MTC A successful operation with a good prognosis is predicted for patients with smaller masses and in whom calcitonin levels are undetectable after surgery
61 Persistent or Recurrent Disease Patients who present with palpable MTC often have elevated calcitonin levels following primary surgery, indicating residual or recurrent MTC Currently, there is no defined role for chemotherapy or radiation therapy in these patients Reoperation for patients with recurrent disease can be done with curative or palliative intent Evidence of distant metastases is a contraindication to surgery unless some palliative benefit can be identified prevent invasion or compression of the airway debulk large tumors that cause profuse, intractable diarrhea secondary to hormone secretion

62 Postoperative Care
63 Postoperative Care Postoperatively, patients are started on a replacement dose of thyroid hormone No need to treat with TSH-suppressive doses of thyroid hormone or radioiodine, because the C cells are not responsive to TSH and don t concentrate radioiodine Subsequent follow-up consists of periodic physical examination and measurement of serum calcitonin and CEA levels to detect recurrent disease
64 Follow-up Yearly screenings for MTC recurrences and other manifestations of the syndrome must be conducted In patients with a calcitonin level less than 150 pg/ml, an US of the neck is sufficient for further evaluation If serum calcitonin levels remain persistently high, further imaging is necessary to locate other potential sites of metastases Recommended imaging studies include CT of the chest, MRI of the liver, and bone scintigraphy Unfortunately, documentation of recurrent MCT by biochemical means is often associated with unresectable recurrence in distant metastatic locations
65 Follow-up For MEN 2 syndromes, routine yearly plasma or 24-hour urine screens must be performed to rule out a pheochromocytoma If catecholamines or metanephrines become elevated, MRI or CT are repeated to localize the tumor MEN 2A patients must have lifelong screening for evidence of hyperparathyroidism Graft-dependant hyperparathyroidism may occur in patients with parathyroid autografts -> debulking
66 Prognosis Prognosis is related to disease stage 10 year survival is ~75%, but decreases to 45% in patients with lymph node involvement Before the use of screening techniques, average life expectancy was 50 years for patients with MEN 2A and 30 years for patients with MEN 2B MTC in the MEN 2 syndromes is usually indolent and slow-growing, but it is lethal in many patients with distant metastases Patients with MEN 2A and FMTC have a better long-term outcome than patients with MEN 2B or sporadic tumors
67 External Beam Radiation Therapy Is an option for grossly positive or microscopically positive margins following surgery and for high-volume disease involving the central and lateral compartments of the neck Not endorsed by the ATA as a substitute for surgery or as a general adjuvant therapy for patients with elevated calcitonin postoperatively
68 Pheochromocytoma Occurs in 40-60% of MEN 2A and MEN 2B patients Arise in adrenal medullary cells that synthesize, store, and secrete catecholamines In MEN 2, pheochromocytomas are often multifocal, with bilateral tumors As opposed to the sporadic form of the disease, malignant and extra-adrenal pheochromocytomas are very rare within MEN 2 populations Pheochromocytomas rarely precede the development of C-cell abnormalities in MEN 2 syndrome
69 Pheochromocytoma Classic signs and symptoms hypertension, headache, heart palpitations, anxiety, and tremulousness Complications of unrecognized disease malignant hypertension, stroke, myocardial infarction, cardiac arrhythmias, and sudden death during unrelated surgical procedures, biopsies, or childbirth Pheochromocytomas may be clinically silent in up to 60% of MEN 2 cases, where they are detected by biochemical testing
70 Diagnosis of Pheochromocytoma Biochemical screening is done by measurement of plasma or 24-hour urine catecholamines and metanephrines If the test is positive or borderline, imaging is needed to determine whether a pheochromocytoma is present Most MEN 2A and MEN 2B patients have some degree of adrenal medullary hyperplasia Adrenal CT or MRI can detect tumors 1 cm or larger MRI may distinguish a pheochromocytoma from an adrenal adenoma, which occurs in up to 9% of normal patients

71 A, CT scan of the neck in a patient with MEN 2A and untreated medullary thyroid carcinoma (arrow) with adenopathy B, Abdominal computed tomography scan of the same patient showing cystic left pheochromocytoma (arrow)
72 Treatment of Pheochromocytoma Partial or complete adrenalectomy is recommended in patients with MEN 2A and MEN 2B who are found to have a pheochromocytoma It is important to medically stabilize the patient before surgery to avoid any perioperative events due to excessive catechol secretion Preoperative α-blockade is achieved by administration of phenoxybenzamine ( mg/day) for 5 days to 2 weeks before surgery The dose is titrated to the lowest blood pressure tolerated and a β-blocker is added to the treatment regimen if tachycardia or cardiac arrhythmia present
73 Treatment of Pheochromocytoma During operation, it may be necessary to control paroxysmal hypertension with short-acting antihypertensives (sodium nitroprusside or phentolamine) Patients with MEN 2A and MEN 2B are ideally suited to laparoscopic adrenalectomy because the pheochromocytomas arising in these syndromes are rarely malignant and almost never extra-adrenal Contraindications to the laparoscopic approach include large tumors (>8-10 cm), malignant pheochromocytomas, and existing contraindications to laparoscopy
74 Parathyroid Disease in MEN 2A Hyperparathyroidism occurs in 10-35% of patients It is rarely the initial presenting problem It is characterized by multiglandular hyperplasia (<1/5 patients has a single parathyroid adenoma) Parathyroid hyperplasia, in the absence of hyperparathyroidism, is common in MEN 2A Parathyroid hyperplasia is not found in patients with sporadic MTC or in patients with MTC in MEN 2B syndrome
75 Diagnosis of Parathyroid Disease All known MEN 2A carriers need to be screened annually for the presence of hyperparathyroidism by serum calcium measurements PTH levels are measured if the serum calcium is high or borderline
76 Treatment of Parathyroid Disease The need for isolated parathyroidectomy in MEN 2A patients is rare Routine total parathyroidectomy with autotransplantation at the time of thyroidectomy is usually performed regardless of gross appearance of the parathyroid glands Should hyperparathyroidism occur at a later time in these patients with forearm grafts, surgical removal of all or a portion of the graft can be done
77 Question With regard to medullary thyroid carcinoma, which of the following statements is/are correct? A. It is derived from a dedifferentiated variant of the same cell that produces papillary and follicular carcinomas B. It s pattern of metastatic spread is almost exclusively to distant sites C. The serum calcitonin level is useful for diagnosis and management D. The prognosis is approximately the same as that of papillary carcinoma
78 Answer With regard to medullary thyroid carcinoma, which of the following statements is/are correct? A. It is derived from a dedifferentiated variant of the same cell that produces papillary and follicular carcinomas B. It s pattern of metastatic spread is almost exclusively to distant sites C. The serum calcitonin level is useful for diagnosis and management D. The prognosis is approximately the same as that of papillary carcinoma
79 Question Are the following characteristics of medullary thyroid carcinoma associated with its sporadic form, its hereditary form, or both? A. Contains parafollicular cells that secrete calcitonin B. Multifocal and bilateral C. Associated with MEN-IIA and MEN-IIB D. Worse prognosis E. Treatment consists of total thyroidectomy with central node dissection
80 Answers Are the following characteristics of medullary thyroid carcinoma associated with its sporadic form, its hereditary form, or both? A. Contains parafollicular cells that secrete calcitonin - Both B. Multifocal and bilateral C. Associated with MEN-IIA and MEN-IIB D. Worse prognosis E. Treatment consists of total thyroidectomy with central node dissection
81 Answers Are the following characteristics of medullary thyroid carcinoma associated with its sporadic form, its hereditary form, or both? A. Contains parafollicular cells that secrete calcitonin - Both B. Multifocal and bilateral Hereditary MTC C. Associated with MEN-IIA and MEN-IIB D. Worse prognosis E. Treatment consists of total thyroidectomy with central node dissection
82 Answers Are the following characteristics of medullary thyroid carcinoma associated with its sporadic form, its hereditary form, or both? A. Contains parafollicular cells that secrete calcitonin - Both B. Multifocal and bilateral Hereditary MTC C. Associated with MEN-IIA and MEN-IIB Hereditary MTC D. Worse prognosis E. Treatment consists of total thyroidectomy with central node dissection
83 Answers Are the following characteristics of medullary thyroid carcinoma associated with its sporadic form, its hereditary form, or both? A. Contains parafollicular cells that secrete calcitonin - Both B. Multifocal and bilateral Hereditary MTC C. Associated with MEN-IIA and MEN-IIB Hereditary MTC D. Worse prognosis Hereditary MTC E. Treatment consists of total thyroidectomy with central node dissection
84 Answers Are the following characteristics of medullary thyroid carcinoma associated with its sporadic form, its hereditary form, or both? A. Contains parafollicular cells that secrete calcitonin - Both B. Multifocal and bilateral Hereditary MTC C. Associated with MEN-IIA and MEN-IIB Hereditary MTC D. Worse prognosis Hereditary MTC E. Treatment consists of total thyroidectomy with central node dissection - Both
85 Question With regard to the management of a patient with MTC, which of the following statements is/are correct? A. The patient should be screened for hyperparathyroidism and pheochromocytoma B. Total thyroidectomy is the procedure of choice C. If cervical lymph node metastasis are present and no distant metastasis are evident, neck dissection results in little benefit with regard to long-term survival D. If pheochromocytoma is found, adrenal surgery should precede the thyroid surgery E. If hyperparathyroidism is found, it may be surgically managed at the time of thyroidectomy by removing the two largest parathyroid glands
86 Answer With regard to the management of a patient with MTC, which of the following statements is/are correct? A. The patient should be screened for hyperparathyroidism and pheochromocytoma B. Total thyroidectomy is the procedure of choice C. If cervical lymph node metastasis are present and no distant metastasis are evident, neck dissection results in little benefit with regard to long-term survival D. If pheochromocytoma is found, adrenal surgery should precede the thyroid surgery E. If hyperparathyroidism is found, it may be surgically managed at the time of thyroidectomy by removing the two largest parathyroid glands
87 Question With regard to genetic analysis in patients with thyroid cancer, which of the following is/are true about the ret proto-oncogene? A. Is associated with anaplastic thyroid cancer B. Is located on chromosome 10 C. Is associated with familial MTC D. Is associated with MEN-IIA and MEN-IIB E. Is associated with follicular cancer of the thyroid
88 Answer With regard to genetic analysis in patients with thyroid cancer, which of the following is/are true about the ret proto-oncogene? A. Is associated with anaplastic thyroid cancer B. Is located on chromosome 10 C. Is associated with familial MTC D. Is associated with MEN-IIA and MEN-IIB E. Is associated with follicular cancer of the thyroid
89 References Cameron: Current Surgical Therapy, 10th ed. Management of Thyroid Cancer. Christopher R. McHenry, MD, Judy Jin, MD. Copyright 2010 Churchill Livingstone, An Imprint of Elsevier Review of Surgery Rush University Medical Center, 4th ed. Thyroid. Roderick M. Quiros, MD, Richard A Prinz, MD Saunders, An Imprint of Elsevier. Zollinger's Atlas of Surgical Operations, 9 th ed. Thyroidectomy, Subtotal. Robert M. Zollinger, Jr. and E. Christopher Ellison. Copyright 2011 by The McGraw-Hill Companies, Inc.
Calcitonin. 1
 Calcitonin Medullary thyroid carcinoma (MTC) is characterized by a high concentration of serum calcitonin. Routine measurement of serum calcitonin concentration has been advocated for detection of MTC
Calcitonin Medullary thyroid carcinoma (MTC) is characterized by a high concentration of serum calcitonin. Routine measurement of serum calcitonin concentration has been advocated for detection of MTC
THYROID CANCER IN CHILDREN. Humberto Lugo-Vicente MD FACS FAAP Professor Pediatric Surgery UPR School of Medicine
 THYROID CANCER IN CHILDREN Humberto Lugo-Vicente MD FACS FAAP Professor Pediatric Surgery UPR School of Medicine Thyroid nodules Rare Female predominance 4-fold as likely to be malignant Hx Radiation exposure?
THYROID CANCER IN CHILDREN Humberto Lugo-Vicente MD FACS FAAP Professor Pediatric Surgery UPR School of Medicine Thyroid nodules Rare Female predominance 4-fold as likely to be malignant Hx Radiation exposure?
B. Environmental Factors. a. The major risk factor to papillary thyroid cancer is exposure to ionizing radiation, during the first 2 decades of life.
 B. Environmental Factors. a. The major risk factor to papillary thyroid cancer is exposure to ionizing radiation, during the first 2 decades of life. b. Deficiency of dietary iodine: - Is linked with a
B. Environmental Factors. a. The major risk factor to papillary thyroid cancer is exposure to ionizing radiation, during the first 2 decades of life. b. Deficiency of dietary iodine: - Is linked with a
- RET/PTC rearrangement: 20% papillary thyroid cancer - RET: medullary thyroid cancer
 Thyroid Cancer UpToDate: Introduction: Risk Factors: Biology: Symptoms: Diagnosis: 1. Lenvina is the first line therapy with powerful durable response and superior PFS in pts with RAI-refractory disease.
Thyroid Cancer UpToDate: Introduction: Risk Factors: Biology: Symptoms: Diagnosis: 1. Lenvina is the first line therapy with powerful durable response and superior PFS in pts with RAI-refractory disease.
4/22/2010. Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey.
 Management of Differentiated Thyroid Cancer: Head Neck Surgeon Perspective Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey Thyroid gland Small endocrine gland:
Management of Differentiated Thyroid Cancer: Head Neck Surgeon Perspective Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey Thyroid gland Small endocrine gland:
INDEX. Note: Page numbers of issue and article titles are in boldface type. cell carcinoma. ENDOCRINE SURGERY
 ENDOCRINE SURGERY INDEX Note: Page numbers of issue and article titles are in boldface type. Adenylate cyclase, in signal transduction 425-426 Adrenal incidentalomas, 499-509 imaging of, 502-504 in patients
ENDOCRINE SURGERY INDEX Note: Page numbers of issue and article titles are in boldface type. Adenylate cyclase, in signal transduction 425-426 Adrenal incidentalomas, 499-509 imaging of, 502-504 in patients
ABSITE Review. RTC Conference Christina Bailey January 15, 2009
 ABSITE Review RTC Conference Christina Bailey January 15, 2009 How It s Broken Down? 220 questions Junior level (PGY 1 and 2) Exam 60% Basic Science 40% Clinical Management Senior Level (PGY 3-5) exam
ABSITE Review RTC Conference Christina Bailey January 15, 2009 How It s Broken Down? 220 questions Junior level (PGY 1 and 2) Exam 60% Basic Science 40% Clinical Management Senior Level (PGY 3-5) exam
The International Federation of Head and Neck Oncologic Societies. Current Concepts in Head and Neck Surgery and Oncology
 The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
Case Scenario 1: Thyroid
 Case Scenario 1: Thyroid History and Physical Patient is an otherwise healthy 80 year old female with the complaint of a neck mass first noticed two weeks ago. The mass has increased in size and is palpable.
Case Scenario 1: Thyroid History and Physical Patient is an otherwise healthy 80 year old female with the complaint of a neck mass first noticed two weeks ago. The mass has increased in size and is palpable.
Thyroid nodules - medical and surgical management. Endocrinology and Endocrine Surgery Manchester Royal Infirmary
 Thyroid nodules - medical and surgical management JRE Davis NR Parrott Endocrinology and Endocrine Surgery Manchester Royal Infirmary Thyroid nodules - prevalence Thyroid nodules common, increase with
Thyroid nodules - medical and surgical management JRE Davis NR Parrott Endocrinology and Endocrine Surgery Manchester Royal Infirmary Thyroid nodules - prevalence Thyroid nodules common, increase with
Thyroid and Adrenal Gland
 Thyroid and Adrenal Gland NAACCR 2011 2012 Webinar Series 12/1/11 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
Thyroid and Adrenal Gland NAACCR 2011 2012 Webinar Series 12/1/11 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
Medullary Thyroid Cancer: Medullary Thyroid Cancer
 Review & Update Nothing to disclose. Jessica E. Gosnell MD Assistant Professor in Residence Department of Surgery November 9, 2012 Medullary Thyroid Cancer MTC has distinct embryology, genetic association
Review & Update Nothing to disclose. Jessica E. Gosnell MD Assistant Professor in Residence Department of Surgery November 9, 2012 Medullary Thyroid Cancer MTC has distinct embryology, genetic association
Thyroid INTRODUCTION ANATOMY SUMMARY OF CHANGES
 AJC 7/14/06 1:19 PM Page 67 Thyroid C73.9 Thyroid gland SUMMARY OF CHANGES Tumor staging (T) has been revised and the categories redefined. T4 is now divided into T4a and T4b. Nodal staging (N) has been
AJC 7/14/06 1:19 PM Page 67 Thyroid C73.9 Thyroid gland SUMMARY OF CHANGES Tumor staging (T) has been revised and the categories redefined. T4 is now divided into T4a and T4b. Nodal staging (N) has been
Persistent & Recurrent Differentiated Thyroid Cancer
 Persistent & Recurrent Differentiated Thyroid Cancer Electron Kebebew University of California, San Francisco Department of Surgery Objectives Risk factors for persistent & recurrent disease Causes of
Persistent & Recurrent Differentiated Thyroid Cancer Electron Kebebew University of California, San Francisco Department of Surgery Objectives Risk factors for persistent & recurrent disease Causes of
 To the Patient and Family This booklet has been written for people who have received a diagnosis of thyroid cancer or who are being tested for this illness. If you have questions that are not answered
To the Patient and Family This booklet has been written for people who have received a diagnosis of thyroid cancer or who are being tested for this illness. If you have questions that are not answered
Thyroid Nodule. Disclosure. Learning Objectives P A P A P A 3/18/2014. Nothing to disclose.
 Thyroid Nodule Evaluating the patient with a thyroid nodule and some management options. Miguel V. Valdez PA C Disclosure Nothing to disclose. Learning Objectives Examination of thyroid gland Options for
Thyroid Nodule Evaluating the patient with a thyroid nodule and some management options. Miguel V. Valdez PA C Disclosure Nothing to disclose. Learning Objectives Examination of thyroid gland Options for
Reoperative central neck surgery
 Reoperative central neck surgery R. Pandev, I. Tersiev, M. Belitova, A. Kouizi, D. Damyanov University Clinic of Surgery, Section Endocrine Surgery University Hospital Queen Johanna ISUL Medical University
Reoperative central neck surgery R. Pandev, I. Tersiev, M. Belitova, A. Kouizi, D. Damyanov University Clinic of Surgery, Section Endocrine Surgery University Hospital Queen Johanna ISUL Medical University
Thyroid nodules 3/22/2011. Most thyroid nodules are benign. Thyroid nodules: differential diagnosis
 Most thyroid nodules are benign Thyroid nodules Postgraduate Course in General Surgery thyroid nodules occur in 77% of the world s population palpable thyroid nodules occur in about 5% of women and 1%
Most thyroid nodules are benign Thyroid nodules Postgraduate Course in General Surgery thyroid nodules occur in 77% of the world s population palpable thyroid nodules occur in about 5% of women and 1%
10/24/2008. Surgery for Well-differentiated Thyroid Carcinoma- The Primary
 Surgery for Well-differentiated Thyroid Carcinoma- The Primary Head and Neck Endocrine Surgery Department of Otolaryngology-Head and Neck Surgery, UCSF October 24-25, 2008 Robert A. Sofferman, MD Professor
Surgery for Well-differentiated Thyroid Carcinoma- The Primary Head and Neck Endocrine Surgery Department of Otolaryngology-Head and Neck Surgery, UCSF October 24-25, 2008 Robert A. Sofferman, MD Professor
Chapter 14: Thyroid Cancer
 The American Academy of Otolaryngology Head and Neck Surgery Foundation (AAO-HNSF) Presents... Chapter 14: Thyroid Cancer Daiichi Pharmaceutical Corporation, marketers and distributors of FLOXIN Otic (ofloxacin
The American Academy of Otolaryngology Head and Neck Surgery Foundation (AAO-HNSF) Presents... Chapter 14: Thyroid Cancer Daiichi Pharmaceutical Corporation, marketers and distributors of FLOXIN Otic (ofloxacin
Ultrasound for Pre-operative Evaluation of Well Differentiated Thyroid Cancer
 Ultrasound for Pre-operative Evaluation of Well Differentiated Thyroid Cancer Its Not Just About the Nodes AACE Advances in Medical and Surgical Management of Thyroid Cancer - 2017 Robert A. Levine, MD,
Ultrasound for Pre-operative Evaluation of Well Differentiated Thyroid Cancer Its Not Just About the Nodes AACE Advances in Medical and Surgical Management of Thyroid Cancer - 2017 Robert A. Levine, MD,
ATA Guidelines for Medullary Thyroid Cancer: approach to initial management of sporadic and inherited disease
 ATA Guidelines for Medullary Thyroid Cancer: approach to initial management of sporadic and inherited disease Richard T. Kloos, M.D. The Ohio State University Divisions of Endocrinology and Nuclear Medicine
ATA Guidelines for Medullary Thyroid Cancer: approach to initial management of sporadic and inherited disease Richard T. Kloos, M.D. The Ohio State University Divisions of Endocrinology and Nuclear Medicine
Differentiated Thyroid Cancer: Initial Management
 Page 1 ATA HOME GIVE ONLINE ABOUT THE ATA JOIN THE ATA MEMBER SIGN-IN INFORMATION FOR PATIENTS FIND A THYROID SPECIALIST Home Management Guidelines for Patients with Thyroid Nodules and Differentiated
Page 1 ATA HOME GIVE ONLINE ABOUT THE ATA JOIN THE ATA MEMBER SIGN-IN INFORMATION FOR PATIENTS FIND A THYROID SPECIALIST Home Management Guidelines for Patients with Thyroid Nodules and Differentiated
Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer
 Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer AACE - Advances in Medical and Surgical Management of Thyroid Cancer - 2018 Robert A. Levine, MD, FACE, ECNU Thyroid Center of New Hampshire Geisel
Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer AACE - Advances in Medical and Surgical Management of Thyroid Cancer - 2018 Robert A. Levine, MD, FACE, ECNU Thyroid Center of New Hampshire Geisel
PEDIATRIC Ariel Katz MD
 PEDIATRIC Ariel Katz MD Dept. Otolaryngology Head &Neck Surgery Wolfson Medical Center Holon, Israel OBJECTIVES Overview/Background Epidemiology/Etiology Intro to Guidelines Workup Treatment Follow-Up
PEDIATRIC Ariel Katz MD Dept. Otolaryngology Head &Neck Surgery Wolfson Medical Center Holon, Israel OBJECTIVES Overview/Background Epidemiology/Etiology Intro to Guidelines Workup Treatment Follow-Up
NEOPLASMS OF THE THYROID PATHOLOGY OF PARATHYROID GLANDS. BY: Shifaa Qa qa
 NEOPLASMS OF THE THYROID PATHOLOGY OF PARATHYROID GLANDS BY: Shifaa Qa qa Neoplasmas of the thyroid thyroid nodules Neoplastic ---- benign, malignant Non neoplastic Solitary nodules ----- neoplastic Nodules
NEOPLASMS OF THE THYROID PATHOLOGY OF PARATHYROID GLANDS BY: Shifaa Qa qa Neoplasmas of the thyroid thyroid nodules Neoplastic ---- benign, malignant Non neoplastic Solitary nodules ----- neoplastic Nodules
CAP Cancer Protocol and ecc Summary of Changes for August 2014 Thyroid Agile Release
 CAP Cancer Protocol and ecc Summary of Changes for August 2014 Thyroid Agile Release 2 REVISION HISTORY Date Author / Editor Comments 5/19/2014 Jaleh Mirza Created the document 8/12/2014 Samantha Spencer/Jaleh
CAP Cancer Protocol and ecc Summary of Changes for August 2014 Thyroid Agile Release 2 REVISION HISTORY Date Author / Editor Comments 5/19/2014 Jaleh Mirza Created the document 8/12/2014 Samantha Spencer/Jaleh
Health Sciences Centre, Team A, Dr. L. Bohacek (Endocrine Surgery) Medical Expert
 Medical Expert") Health Sciences Centre, Team A, Dr. L. Bohacek (Endocrine Surgery) Introduction Medical Expert This is a three month PGY 1-5 rotation in which residents gain exposure in the care and management of patients
Health Sciences Centre, Team A, Dr. L. Bohacek (Endocrine Surgery) Introduction Medical Expert This is a three month PGY 1-5 rotation in which residents gain exposure in the care and management of patients
3/29/2012. Thyroid cancer- what s new. Thyroid Cancer. Thyroid cancer is now the most rapidly increasing cancer in women
 Thyroid cancer- what s new Thyroid Cancer Changing epidemiology Molecular markers Lymph node dissection Technical advances rhtsh Genetic testing and prophylactic surgery Vandetanib What s new? Jessica
Thyroid cancer- what s new Thyroid Cancer Changing epidemiology Molecular markers Lymph node dissection Technical advances rhtsh Genetic testing and prophylactic surgery Vandetanib What s new? Jessica
THE FACTS YOU NEED TO KNOW
 PHEOCHROMOCYTOMA THE FACTS YOU NEED TO KNOW Pheochromocytoma is a part of the pheochromocytoma and paraganglioma group of syndromes. A pheochromocytoma is a tumor arising in the adrenal gland medulla.
PHEOCHROMOCYTOMA THE FACTS YOU NEED TO KNOW Pheochromocytoma is a part of the pheochromocytoma and paraganglioma group of syndromes. A pheochromocytoma is a tumor arising in the adrenal gland medulla.
Adjuvant therapy for thyroid cancer
 Carcinoma of the thyroid Adjuvant therapy for thyroid cancer John Hay Department of Radiation Oncology Vancouver Cancer Centre Department of Surgery UBC 1% of all new malignancies 0.5% in men 1.5% in women
Carcinoma of the thyroid Adjuvant therapy for thyroid cancer John Hay Department of Radiation Oncology Vancouver Cancer Centre Department of Surgery UBC 1% of all new malignancies 0.5% in men 1.5% in women
Grave s autoimmune Graves and Hashimotos: antithyroglobulin and antimicrosomal antibodies T3 X 10d should decrease TSH 50%
 Vesalius SCALpel : Thyroid (see also: head and neck folios) Anatomic lingual thyroid most common ectopic location normal thyroid tissue patients may have no thyroid in neck manifest as teenager, may enlarge
Vesalius SCALpel : Thyroid (see also: head and neck folios) Anatomic lingual thyroid most common ectopic location normal thyroid tissue patients may have no thyroid in neck manifest as teenager, may enlarge
Case Scenario #1 Larynx
 Case Scenario #1 Larynx 56 year old white female who presented with a 2 month history of hoarseness treated with antibiotics, but with no improvement. In the last 3 weeks, she has had a 15 lb weight loss,
Case Scenario #1 Larynx 56 year old white female who presented with a 2 month history of hoarseness treated with antibiotics, but with no improvement. In the last 3 weeks, she has had a 15 lb weight loss,
Ovid: Oxford Textbook of Endocrinology & Diabetes
 Página 1 de 6 Copyright 2002 Oxford University Press Wass, John A.H., Shalet, Stephen M., Gale, Edwin, Amiel, Stephanie A. Oxford Textbook of Endocrinology & Diabetes, 1st Edition Surgical procedure Part
Página 1 de 6 Copyright 2002 Oxford University Press Wass, John A.H., Shalet, Stephen M., Gale, Edwin, Amiel, Stephanie A. Oxford Textbook of Endocrinology & Diabetes, 1st Edition Surgical procedure Part
What is Thyroid Cancer? Here are four types of thyroid cancer:
 What is Thyroid Cancer? Thyroid cancer is a group of malignant tumors that originate from the thyroid gland. The thyroid is a gland in the front of the neck. The thyroid gland absorbs iodine from the bloodstream
What is Thyroid Cancer? Thyroid cancer is a group of malignant tumors that originate from the thyroid gland. The thyroid is a gland in the front of the neck. The thyroid gland absorbs iodine from the bloodstream
Thyroid Gland. Protocol applies to all malignant tumors of the thyroid gland, except lymphomas.
 Thyroid Gland Protocol applies to all malignant tumors of the thyroid gland, except lymphomas. Procedures Cytology (No Accompanying Checklist) Partial Thyroidectomy Total Thyroidectomy With/Without Lymph
Thyroid Gland Protocol applies to all malignant tumors of the thyroid gland, except lymphomas. Procedures Cytology (No Accompanying Checklist) Partial Thyroidectomy Total Thyroidectomy With/Without Lymph
2015 American Thyroid Association Thyroid Nodule and Cancer Guidelines
 2015 American Thyroid Association Thyroid Nodule and Cancer Guidelines Angela M. Leung, MD, MSc, ECNU November 5, 2016 Outline Workup of nontoxic thyroid nodule(s) Ultrasound FNAB Management of FNAB results
2015 American Thyroid Association Thyroid Nodule and Cancer Guidelines Angela M. Leung, MD, MSc, ECNU November 5, 2016 Outline Workup of nontoxic thyroid nodule(s) Ultrasound FNAB Management of FNAB results
A KINDRED WITH a RET CODON Y791F MUTATION PRESENTING WITH HIRSCHSPRUNG S S DISEASE.
 A KINDRED WITH a RET CODON Y791F MUTATION PRESENTING WITH HIRSCHSPRUNG S S DISEASE. ד"ר מרב פרנ קל ד גנית ברק גרוס דיויד פרופסור השרות לאנדוקרינ ולוגיה ומטבוליזם ירושלים ה דסה עין כר םם, Case Report 36
A KINDRED WITH a RET CODON Y791F MUTATION PRESENTING WITH HIRSCHSPRUNG S S DISEASE. ד"ר מרב פרנ קל ד גנית ברק גרוס דיויד פרופסור השרות לאנדוקרינ ולוגיה ומטבוליזם ירושלים ה דסה עין כר םם, Case Report 36
Thyroid nodules. Most thyroid nodules are benign
 Thyroid nodules Postgraduate Course in General Surgery Jessica E. Gosnell MD Assistant Professor March 22, 2011 Most thyroid nodules are benign thyroid nodules occur in 77% of the world s population palpable
Thyroid nodules Postgraduate Course in General Surgery Jessica E. Gosnell MD Assistant Professor March 22, 2011 Most thyroid nodules are benign thyroid nodules occur in 77% of the world s population palpable
General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons
 General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons MODULE TITLE: ENDOCRINE 5-May-2013 DEVELOPED BY: Jonathan Serpell
General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons MODULE TITLE: ENDOCRINE 5-May-2013 DEVELOPED BY: Jonathan Serpell
Thyroid Nodules. Dr. HAKIMI, SpAK Dr. MELDA DELIANA, SpAK Dr. SISKA MAYASARI LUBIS, SpA
 Thyroid Nodules ENDOCRINOLOGY DIVISION ENDOCRINOLOGY DIVISION Dr. HAKIMI, SpAK Dr. MELDA DELIANA, SpAK Dr. SISKA MAYASARI LUBIS, SpA Anatomical Considerations The Thyroid Nodule Congenital anomalies Thyroglossal
Thyroid Nodules ENDOCRINOLOGY DIVISION ENDOCRINOLOGY DIVISION Dr. HAKIMI, SpAK Dr. MELDA DELIANA, SpAK Dr. SISKA MAYASARI LUBIS, SpA Anatomical Considerations The Thyroid Nodule Congenital anomalies Thyroglossal
Biopsy needle, thyroid gland, 74 technique, Bone hunger syndrome, 23
 The following figures were reproduced by permission, courtesy of the Mayo Clinic: Figures 2-7, 2-l4a, 2-l5a, 2-l5c, 2-l6a, 2-l8a, 3-l5a, 3-21a The following figure was slightly modified and reproduced
The following figures were reproduced by permission, courtesy of the Mayo Clinic: Figures 2-7, 2-l4a, 2-l5a, 2-l5c, 2-l6a, 2-l8a, 3-l5a, 3-21a The following figure was slightly modified and reproduced
Management guideline for patients with differentiated thyroid cancer. Teeraporn Ratanaanekchai ENT, KKU 17 October 2007
 Management guideline for patients with differentiated thyroid Teeraporn Ratanaanekchai ENT, KKU 17 October 2007 Incidence (Srinagarind Hospital, 2005, both sex) Site (all) cases % 1. Liver 1178 27 2. Lung
Management guideline for patients with differentiated thyroid Teeraporn Ratanaanekchai ENT, KKU 17 October 2007 Incidence (Srinagarind Hospital, 2005, both sex) Site (all) cases % 1. Liver 1178 27 2. Lung
Thyroid Cancer. With 51 Figures and 30 Tables. Springer
 H.-J. Biersack F. Griinwald (Eds.) Thyroid Cancer With 51 Figures and 30 Tables Springer PART 1 Basics 1 The Changing Epidemiology of Thyroid Cancer 3 R. GORGES 1.1 Basic Epidemiological Problems in Thyroid
H.-J. Biersack F. Griinwald (Eds.) Thyroid Cancer With 51 Figures and 30 Tables Springer PART 1 Basics 1 The Changing Epidemiology of Thyroid Cancer 3 R. GORGES 1.1 Basic Epidemiological Problems in Thyroid
Timing of Early Preventative Thyroidectomy in Children with MEN 2
 Timing of Early Preventative Thyroidectomy in Children with MEN 2 Terry C. Lairmore, M.D. Professor of Surgery Director, Division of Surgical Oncology Texas Chapter of AACE Texas Endocrine Surgical Symposium
Timing of Early Preventative Thyroidectomy in Children with MEN 2 Terry C. Lairmore, M.D. Professor of Surgery Director, Division of Surgical Oncology Texas Chapter of AACE Texas Endocrine Surgical Symposium
B Berry, J. 25 see also suspensory ligament of Berry biopsy see fine-needle aspiration biopsy (FNAB); open wedge biopsy
; open wedge biopsy") 174 Index Index Page numbers in italics refer to illustrations A abscess 80, 137 adenoma 61 parathyroid 18, 18 19, 62, 84 differential diagnosis 84, 84, 85, 85 thyroid 63 follicular 62, 63, 64 macrofollicular
174 Index Index Page numbers in italics refer to illustrations A abscess 80, 137 adenoma 61 parathyroid 18, 18 19, 62, 84 differential diagnosis 84, 84, 85, 85 thyroid 63 follicular 62, 63, 64 macrofollicular
Wilms Tumor and Neuroblastoma
 Wilms Tumor and Neuroblastoma Wilm s Tumor AKA: Nephroblastoma the most common intra-abdominal cancer in children. peak incidence is 2 to 3 years of age Biology somatic mutations restricted to tumor tissue
Wilms Tumor and Neuroblastoma Wilm s Tumor AKA: Nephroblastoma the most common intra-abdominal cancer in children. peak incidence is 2 to 3 years of age Biology somatic mutations restricted to tumor tissue
WTC 2013 Panel Discussion: Minimal disease
 WTC 2013 Panel Discussion: Minimal disease Susan J. Mandel MD MPH Panelists Ken Ain Yasuhiro Ito Stephanie Lee Erich Sturgis Mark Urken Faculty/Presenter Disclosure Relationships with commercial interests
WTC 2013 Panel Discussion: Minimal disease Susan J. Mandel MD MPH Panelists Ken Ain Yasuhiro Ito Stephanie Lee Erich Sturgis Mark Urken Faculty/Presenter Disclosure Relationships with commercial interests
Result Navigator. Positive Test Result: RET. After a positive test result, there can be many questions about what to do next. Navigate Your Results
 Result Navigator Positive Test Result: RET Positive test results identify a change, or misspelling, of DNA that is known or predicted to cause an increased risk for cancer. DNA is the blueprint of life
Result Navigator Positive Test Result: RET Positive test results identify a change, or misspelling, of DNA that is known or predicted to cause an increased risk for cancer. DNA is the blueprint of life
Thyroidectomy. Siu Kwan Ng. Modified Radical Neck Dissection Type II 47
 06 Thyroidectomy Siu Kwan Ng Modified Radical Neck Dissection Type II 47 Thyroidectomy STEP 1. EXPOSING THE THYROID GLAND The collar incision Figure 1 (curvilinear skin crease incision) is made at 1.5-2
06 Thyroidectomy Siu Kwan Ng Modified Radical Neck Dissection Type II 47 Thyroidectomy STEP 1. EXPOSING THE THYROID GLAND The collar incision Figure 1 (curvilinear skin crease incision) is made at 1.5-2
How good are we at finding nodules? Thyroid Nodules Thyroid Cancer Epidemiology Initial management Long-term follow up Disease-free status
 New Perspectives in Thyroid Cancer Jennifer Sipos, MD Assistant Professor of Medicine Division of Endocrinology The Ohio State University Outline Thyroid Nodules Thyroid Cancer Epidemiology Initial management
New Perspectives in Thyroid Cancer Jennifer Sipos, MD Assistant Professor of Medicine Division of Endocrinology The Ohio State University Outline Thyroid Nodules Thyroid Cancer Epidemiology Initial management
Index. Surg Oncol Clin N Am 15 (2006) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Surg Oncol Clin N Am 15 (2006) 681 685 Index Note: Page numbers of article titles are in boldface type. A Ablative therapy, for liver metastases in patients with neuroendocrine tumors, 517 with radioiodine
Surg Oncol Clin N Am 15 (2006) 681 685 Index Note: Page numbers of article titles are in boldface type. A Ablative therapy, for liver metastases in patients with neuroendocrine tumors, 517 with radioiodine
Thyroid and Parathyroid Surgery
 Med 5 Surgery Refresher Course 2013 2014 Thyroid and Parathyroid Surgery Dr Shirley Liu Resident Specialist Honorary Clinical Assistant Professor Team 2 Surgery Prince of Wales Hospital Case scenario:
Med 5 Surgery Refresher Course 2013 2014 Thyroid and Parathyroid Surgery Dr Shirley Liu Resident Specialist Honorary Clinical Assistant Professor Team 2 Surgery Prince of Wales Hospital Case scenario:
Exercise 15: CSv2 Data Item Coding Instructions ANSWERS
 Exercise 15: CSv2 Data Item Coding Instructions ANSWERS CS Tumor Size Tumor size is the diameter of the tumor, not the depth or thickness of the tumor. Chest x-ray shows 3.5 cm mass; the pathology report
Exercise 15: CSv2 Data Item Coding Instructions ANSWERS CS Tumor Size Tumor size is the diameter of the tumor, not the depth or thickness of the tumor. Chest x-ray shows 3.5 cm mass; the pathology report
Disclosures Nodal Management in Differentiated Thyroid Carcinoma
 Disclosures Nodal Management in Differentiated Thyroid Carcinoma Nothing to disclose Jonathan George, MD, MPH Assistant Professor UCSF Head and Neck Oncologic & Endocrine Surgery Objectives Overview Describe
Disclosures Nodal Management in Differentiated Thyroid Carcinoma Nothing to disclose Jonathan George, MD, MPH Assistant Professor UCSF Head and Neck Oncologic & Endocrine Surgery Objectives Overview Describe
40 TH EUROPEAN CONGRESS 0F CYTOLOGY LIVERPOOL, UK October 2-5, 2016
 Outcomes from the diagnostic approach of thyroid lesions using US-FNA and LBC in clinical practice Emmanouel Mastorakis MD PhD Cytopathologist Director in Cytopathology Laboratory Regional General Hospital
Outcomes from the diagnostic approach of thyroid lesions using US-FNA and LBC in clinical practice Emmanouel Mastorakis MD PhD Cytopathologist Director in Cytopathology Laboratory Regional General Hospital
PEDIATRIC THYROID MALIGNACY
 PEDIATRIC THYROID MALIGNACY Anthony Sheyn MD Assistant Professor of Otolaryngology Head and Neck Surgery University of Tennessee Health Science Center Thyroid nodules 20 per 1000 children nodules in children
PEDIATRIC THYROID MALIGNACY Anthony Sheyn MD Assistant Professor of Otolaryngology Head and Neck Surgery University of Tennessee Health Science Center Thyroid nodules 20 per 1000 children nodules in children
Failure to Recognize Multiple Endocrine Neoplasia 2B: More Common Than We Think?
 Annals of Surgical Oncology 15(1):293 301 DOI: 10.1245/s10434-007-9665-4 Failure to Recognize Multiple Endocrine Neoplasia 2B: More Common Than We Think? Curtis J. Wray, 1 Thereasa A. Rich, 1 Steven G.
Annals of Surgical Oncology 15(1):293 301 DOI: 10.1245/s10434-007-9665-4 Failure to Recognize Multiple Endocrine Neoplasia 2B: More Common Than We Think? Curtis J. Wray, 1 Thereasa A. Rich, 1 Steven G.
Read the following article and answer the questions that follow. Refer to the Keys section to check your answers.
 ENGLISH 183 READING PRACTICE - Pheochromocytoma Read the following article and answer the questions that follow. Refer to the Keys section to check your answers. Pheochromocytoma is a tumor on the medulla
ENGLISH 183 READING PRACTICE - Pheochromocytoma Read the following article and answer the questions that follow. Refer to the Keys section to check your answers. Pheochromocytoma is a tumor on the medulla
Karoline Nowillo, MD. February 1, 2008
 Case Presentation Karoline Nowillo, MD SUNY Downstate t February 1, 2008 Case Presentation Chief complaint enlarging goiter x 8 months History of present illness shortness of breath, heaviness in chest
Case Presentation Karoline Nowillo, MD SUNY Downstate t February 1, 2008 Case Presentation Chief complaint enlarging goiter x 8 months History of present illness shortness of breath, heaviness in chest
AACE Thyroid Cancer Tumor board 25 years of the Endocrine and Surgery collaboration
 AACE Thyroid Cancer Tumor board 25 years of the Endocrine and Surgery collaboration Dr. Peter Singer, Endocrinology Dr. Peter Sadow, Pathology Moderator Dr. Greg Randolph, Otolaryngology Relevant Financial
AACE Thyroid Cancer Tumor board 25 years of the Endocrine and Surgery collaboration Dr. Peter Singer, Endocrinology Dr. Peter Sadow, Pathology Moderator Dr. Greg Randolph, Otolaryngology Relevant Financial
Long-term Follow-up for Patients with Papillary Thyroid Carcinoma Treated as Benign Nodules
 Long-term Follow-up for Patients with Papillary Thyroid Carcinoma Treated as Benign Nodules YASUHIRO ITO, TAKUYA HIGASHIYAMA, YUUKI TAKAMURA, AKIHIRO MIYA, KAORU KOBAYASHI, FUMIO MATSUZUKA, KANJI KUMA
Long-term Follow-up for Patients with Papillary Thyroid Carcinoma Treated as Benign Nodules YASUHIRO ITO, TAKUYA HIGASHIYAMA, YUUKI TAKAMURA, AKIHIRO MIYA, KAORU KOBAYASHI, FUMIO MATSUZUKA, KANJI KUMA
Women s Health in General Practice Symposium 2015 Thyroid & Parathyroid Cases
 Women s Health in General Practice Symposium 2015 Thyroid & Parathyroid Cases Bill Fleming Epworth Freemasons Hospital 1 Common Endocrine Presentations anatomical problems thyroid nodule / goitre embryological
Women s Health in General Practice Symposium 2015 Thyroid & Parathyroid Cases Bill Fleming Epworth Freemasons Hospital 1 Common Endocrine Presentations anatomical problems thyroid nodule / goitre embryological
5/18/2013. Most thyroid nodules are benign. Thyroid nodules: new techniques in evaluation
 Most thyroid nodules are benign Thyroid nodules: new techniques in evaluation Incidence Etiology Risk factors Diagnosis Gene classification system Treatment Postgraduate Course in General Surgery Jessica
Most thyroid nodules are benign Thyroid nodules: new techniques in evaluation Incidence Etiology Risk factors Diagnosis Gene classification system Treatment Postgraduate Course in General Surgery Jessica
1/25/13 Right partial nephrectomy followed by completion right radical nephrectomy.
 History and Physical Case Scenario 1 45 year old white male presents with complaints of nausea, weight loss, and back pain. A CT of the chest, abdomen and pelvis was done on 12/8/12 that revealed a 12
History and Physical Case Scenario 1 45 year old white male presents with complaints of nausea, weight loss, and back pain. A CT of the chest, abdomen and pelvis was done on 12/8/12 that revealed a 12
Review Article Management of thyroid carcinoma Alauddin M, Joarder AH
 Management of thyroid carcinoma Alauddin M, Joarder AH The ORION Medical Journal 2004 May;18:163-166 Overview The two most common forms of thyroid cancer, papillaryand follicular thyroid cancer, together
Management of thyroid carcinoma Alauddin M, Joarder AH The ORION Medical Journal 2004 May;18:163-166 Overview The two most common forms of thyroid cancer, papillaryand follicular thyroid cancer, together
Head & Neck Clinical Sub Group. Network Agreed Imaging Guidelines for UAT and Thyroid Cancer. Measure Nos: 11-1C-105i & 11-1C-106i
 Greater Manchester, Lancashire & South Cumbria Strategic Clinical Network & Senate Head & Neck Clinical Sub Group Network Agreed Imaging Guidelines for UAT and Thyroid Cancer Measure Nos: 11-1C-105i &
Greater Manchester, Lancashire & South Cumbria Strategic Clinical Network & Senate Head & Neck Clinical Sub Group Network Agreed Imaging Guidelines for UAT and Thyroid Cancer Measure Nos: 11-1C-105i &
Thyroid Surgery: Lobectomy, total thyroidectomy, LN biopsies or only watchful waiting?
 Thyroid Surgery: Lobectomy, total thyroidectomy, LN biopsies or only watchful waiting? Jacob Moalem, MD, FACS Associate Professor Endocrine Surgery and Endocrinology URMC Agenda 1. When is lobectomy alone
Thyroid Surgery: Lobectomy, total thyroidectomy, LN biopsies or only watchful waiting? Jacob Moalem, MD, FACS Associate Professor Endocrine Surgery and Endocrinology URMC Agenda 1. When is lobectomy alone
Pheochromocytoma AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGY ILLINOIS CHAPTER OCTOBER 13, 2018
 Pheochromocytoma AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGY ILLINOIS CHAPTER OCTOBER 13, 2018 Steven A. De Jong, M.D., FACS, FACE Professor and Vice Chair of Surgery Chief, Division of General Surgery
Pheochromocytoma AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGY ILLINOIS CHAPTER OCTOBER 13, 2018 Steven A. De Jong, M.D., FACS, FACE Professor and Vice Chair of Surgery Chief, Division of General Surgery
Management of Recurrent Thyroid Cancer
 Management of Recurrent Thyroid Cancer Eric Genden, MD, MHA Isidore Professor and Chairman Department of Otolaryngology- Head and Neck Surgery Senior Associate Dean for Clinical Affairs The Icahn School
Management of Recurrent Thyroid Cancer Eric Genden, MD, MHA Isidore Professor and Chairman Department of Otolaryngology- Head and Neck Surgery Senior Associate Dean for Clinical Affairs The Icahn School
Thyroid Cancer (Carcinoma)
") Information for Patients Thyroid Cancer (Carcinoma) Prepared by the American Association of Clinical Endocrinologists (AACE), a not-for-profit national organization of highly qualified specialists in hormonal
Information for Patients Thyroid Cancer (Carcinoma) Prepared by the American Association of Clinical Endocrinologists (AACE), a not-for-profit national organization of highly qualified specialists in hormonal
Normal thyroid tissue
 Thyroid Pathology Overview Normal thyroid tissue Normal thyroid tissue with follicles filled with colloid. Thyroid cells form follicles, spheres of epithelial cells (always single layered in health, usually
Thyroid Pathology Overview Normal thyroid tissue Normal thyroid tissue with follicles filled with colloid. Thyroid cells form follicles, spheres of epithelial cells (always single layered in health, usually
Thyroid Tumors in Dogs A Big Gland in the Neck
 Thyroid Tumors in Dogs A Big Gland in the Neck This week I had the privilege of meeting a wonderful patient referred to me for evaluation of a thyroid tumor. After consulting with the family, I visited
Thyroid Tumors in Dogs A Big Gland in the Neck This week I had the privilege of meeting a wonderful patient referred to me for evaluation of a thyroid tumor. After consulting with the family, I visited
PARATHYROID IMAGING. James Lee, MD Chief, Endocrine Surgery Co-Director NY Thyroid-Parathyroid Center Columbia University Medical Center
 PARATHYROID IMAGING James Lee, MD Chief, Endocrine Surgery Co-Director NY Thyroid-Parathyroid Center Columbia University Medical Center NO DISCLOSURES Overview The hallmarks of the ideal test Benefits
PARATHYROID IMAGING James Lee, MD Chief, Endocrine Surgery Co-Director NY Thyroid-Parathyroid Center Columbia University Medical Center NO DISCLOSURES Overview The hallmarks of the ideal test Benefits
Gerard M. Doherty, MD
 Surgical Management of Differentiated Thyroid Cancer: Update on 2015 ATA Guidelines Gerard M. Doherty, MD Chair of Surgery Utley Professor of Surgery and Medicine Boston University Surgeon-in-Chief Boston
Surgical Management of Differentiated Thyroid Cancer: Update on 2015 ATA Guidelines Gerard M. Doherty, MD Chair of Surgery Utley Professor of Surgery and Medicine Boston University Surgeon-in-Chief Boston
CANCERS OF THE ENDOCRINE ORGANS RARE THYROID CANCERS PREFERRED MODEL OF CARE AND CRITERIA FOR REFERENCE CENTRES
 CANCERS OF THE ENDOCRINE ORGANS RARE THYROID CANCERS PREFERRED MODEL OF CARE AND CRITERIA FOR REFERENCE CENTRES Coordinator: Giuseppe COSTANTE (Endocrinology, Institut Jules Bordet), Ahmad AWADA (Medical
CANCERS OF THE ENDOCRINE ORGANS RARE THYROID CANCERS PREFERRED MODEL OF CARE AND CRITERIA FOR REFERENCE CENTRES Coordinator: Giuseppe COSTANTE (Endocrinology, Institut Jules Bordet), Ahmad AWADA (Medical
Parathyroid Imaging: Current Concepts. Maria Gule-Monroe, M.D. Nancy Perrier, M.D.
 Parathyroid Imaging: Current Concepts Maria Gule-Monroe, M.D. Nancy Perrier, M.D. Disclosures None Objectives Ultrasound characteristics of parathyroid adenomas vs. lymph nodes 4D-CT evaluation of hyperparathyroidism
Parathyroid Imaging: Current Concepts Maria Gule-Monroe, M.D. Nancy Perrier, M.D. Disclosures None Objectives Ultrasound characteristics of parathyroid adenomas vs. lymph nodes 4D-CT evaluation of hyperparathyroidism
Dr J K Jekel Dept. Surgery University of Pretoria
 Dr J K Jekel Dept. Surgery University of Pretoria No Maybe ( T`s and C`s apply ) 1. Total thyroidectomy 2. Neck dissection only if nodes are involved 3. Ablative dose or doses of Radioactive Iodine 4.
Dr J K Jekel Dept. Surgery University of Pretoria No Maybe ( T`s and C`s apply ) 1. Total thyroidectomy 2. Neck dissection only if nodes are involved 3. Ablative dose or doses of Radioactive Iodine 4.
42 yr old male with h/o Graves disease and prior I 131 treatment presents with hyperthyroidism and undetectable TSH. 2 hr uptake 20%, 24 hr uptake 50%
 Pinhole images of the neck are acquired in multiple projections, 24hrs after the oral administration of approximately 200 µci of I123. Usually, 24hr uptake value if also calculated (normal 24 hr uptake
Pinhole images of the neck are acquired in multiple projections, 24hrs after the oral administration of approximately 200 µci of I123. Usually, 24hr uptake value if also calculated (normal 24 hr uptake
Thyroid Neoplasm. ORL-Head and neck Surgery 2014
 In The Name of God Thyroid Neoplasm ORL-Head and neck Surgery 2014 Malignant Neoplasm By age 90, virtually everyone has nodules Estimates of cancer prevalence at autopsy 4% to 36% Why these lesions are
In The Name of God Thyroid Neoplasm ORL-Head and neck Surgery 2014 Malignant Neoplasm By age 90, virtually everyone has nodules Estimates of cancer prevalence at autopsy 4% to 36% Why these lesions are
Management of Neck Metastasis from Unknown Primary
 Management of Neck Metastasis from Unknown Primary.. Definition Histologic evidence of malignancy in the cervical lymph node (s) with no apparent primary site of original tumour Diagnosis after a thorough
Management of Neck Metastasis from Unknown Primary.. Definition Histologic evidence of malignancy in the cervical lymph node (s) with no apparent primary site of original tumour Diagnosis after a thorough
What is Thyroid Cancer?
 Thyroid Cancer What is Thyroid Cancer? The thyroid is a gland at the base of the throat near the trachea (windpipe). It is shaped like a butterfly, with a right lobe and a left lobe. The isthmus, a thin
Thyroid Cancer What is Thyroid Cancer? The thyroid is a gland at the base of the throat near the trachea (windpipe). It is shaped like a butterfly, with a right lobe and a left lobe. The isthmus, a thin
Thyroid Nodules. Family Medicine Refresher Course Geeta Lal MD, FACS April 2, No financial disclosures
 Thyroid Nodules Family Medicine Refresher Course Geeta Lal MD, FACS April 2, 2014 No financial disclosures Objectives Review epidemiology Work up of Thyroid nodules Indications for FNAB Evolving role of
Thyroid Nodules Family Medicine Refresher Course Geeta Lal MD, FACS April 2, 2014 No financial disclosures Objectives Review epidemiology Work up of Thyroid nodules Indications for FNAB Evolving role of
Evaluation and Management of Thyroid Nodules. Nick Vernetti, MD, FACE Palm Medical Group Las Vegas, Nevada
 Evaluation and Management of Thyroid Nodules Nick Vernetti, MD, FACE Palm Medical Group Las Vegas, Nevada Disclosure Consulting Amgen Speaking Amgen Objectives Understand the significance of incidental
Evaluation and Management of Thyroid Nodules Nick Vernetti, MD, FACE Palm Medical Group Las Vegas, Nevada Disclosure Consulting Amgen Speaking Amgen Objectives Understand the significance of incidental
Papillary Thyroid Microcarcinoma Presenting as Horner s Syndrome: A Novel Clinical Presentation
 Case Report American Journal of Cancer Case Reports http://ivyunion.org/index.php/ajccr/ Page 1 of 6 Papillary Thyroid Microcarcinoma Presenting as Horner s Syndrome: A Novel Clinical Presentation Ammara
Case Report American Journal of Cancer Case Reports http://ivyunion.org/index.php/ajccr/ Page 1 of 6 Papillary Thyroid Microcarcinoma Presenting as Horner s Syndrome: A Novel Clinical Presentation Ammara
Kidney Case 1 SURGICAL PATHOLOGY REPORT
 Kidney Case 1 Surgical Pathology Report February 9, 2007 Clinical History: This 45 year old woman was found to have a left renal mass. CT urography with reconstruction revealed a 2 cm medial mass which
Kidney Case 1 Surgical Pathology Report February 9, 2007 Clinical History: This 45 year old woman was found to have a left renal mass. CT urography with reconstruction revealed a 2 cm medial mass which
Evaluation of Thyroid Nodules
 Evaluation of Thyroid Nodules Stephan Kowalyk, MD January 25 28, 2018 1 Primary goal Exclude malignancy Incidental thyroid nodules If found on CT, MRI, PET scan, carotid Doppler ULTRASOUND!! January 25
Evaluation of Thyroid Nodules Stephan Kowalyk, MD January 25 28, 2018 1 Primary goal Exclude malignancy Incidental thyroid nodules If found on CT, MRI, PET scan, carotid Doppler ULTRASOUND!! January 25
What you need to know about Thyroid Cancer
 What you need to know about Thyroid Cancer This booklet has been designed to help you to learn more about your thyroid cancer. It covers the most important areas and answers some of the frequently asked
What you need to know about Thyroid Cancer This booklet has been designed to help you to learn more about your thyroid cancer. It covers the most important areas and answers some of the frequently asked
MTP: Thyroid Nodules
 Canadian Endocrine Update MTP: Thyroid Nodules Deric Morrison MD, FRCP, ECNU Assistant Professor, Division of Endocrinology and Metabolism, Western University April 2014 Faculty/Presenter Disclosure Faculty:
Canadian Endocrine Update MTP: Thyroid Nodules Deric Morrison MD, FRCP, ECNU Assistant Professor, Division of Endocrinology and Metabolism, Western University April 2014 Faculty/Presenter Disclosure Faculty:
Multiple endocrine neoplasia type 2B in a Chinese patient. Citation Hong Kong Medical Journal, 2004, v. 10 n. 3, p
 Title Multiple endocrine neoplasia type 2B in a Chinese patient Author(s) Chang, A; Chan, WF; Lo, CY; Lam, KSL Citation Hong Kong Medical Journal, 2004, v. 10 n. 3, p. 206-209 Issued Date 2004 URL http://hdl.handle.net/10722/45152
Title Multiple endocrine neoplasia type 2B in a Chinese patient Author(s) Chang, A; Chan, WF; Lo, CY; Lam, KSL Citation Hong Kong Medical Journal, 2004, v. 10 n. 3, p. 206-209 Issued Date 2004 URL http://hdl.handle.net/10722/45152
RECURRENT ADRENAL DISEASE. Megan Applewhite Endorama 2/19/2015 SR , SC
 RECURRENT ADRENAL DISEASE Megan Applewhite Endorama 2/19/2015 SR 2412318, SC 3421561 Category: Adrenal Attendings: Angelos & Grogan PATIENT #1 36yo woman with a hx of Cushing s Syndrome and right adrenalectomy
RECURRENT ADRENAL DISEASE Megan Applewhite Endorama 2/19/2015 SR 2412318, SC 3421561 Category: Adrenal Attendings: Angelos & Grogan PATIENT #1 36yo woman with a hx of Cushing s Syndrome and right adrenalectomy
Avi Khafif, MD, Rami Ben-Yosef, MD, Avrum Abergel, MD, Ada Kesler, MD, Roee Landsberg, MD, Dan M. Fliss, MD
 ORIGINAL ARTICLE ELECTIVE PARATRACHEAL NECK DISSECTION FOR LATERAL METASTASES FROM PAPILLARY CARCINOMA OF THE THYROID: IS IT INDICATED? Avi Khafif, MD, Rami Ben-Yosef, MD, Avrum Abergel, MD, Ada Kesler,
ORIGINAL ARTICLE ELECTIVE PARATRACHEAL NECK DISSECTION FOR LATERAL METASTASES FROM PAPILLARY CARCINOMA OF THE THYROID: IS IT INDICATED? Avi Khafif, MD, Rami Ben-Yosef, MD, Avrum Abergel, MD, Ada Kesler,
Clinical Study Comparison of Conventional Open Thyroidectomy and Endoscopic Thyroidectomy via Breast Approach for Papillary Thyroid Carcinoma
 International Endocrinology Volume 2015, Article ID 239610, 5 pages http://dx.doi.org/10.1155/2015/239610 Clinical Study Comparison of Conventional Open Thyroidectomy and Endoscopic Thyroidectomy via Breast
International Endocrinology Volume 2015, Article ID 239610, 5 pages http://dx.doi.org/10.1155/2015/239610 Clinical Study Comparison of Conventional Open Thyroidectomy and Endoscopic Thyroidectomy via Breast
performed to help sway the clinician in what the appropriate diagnosis is, which can substantially alter the treatment of management.
 Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Case Scenario. 7/13/12 Anterior floor of mouth biopsy: Infiltrating squamous cell carcinoma, not completely excised.
 Case Scenario 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of alcohol.
Case Scenario 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of alcohol.
Cabozantinib for medullary thyroid cancer. February 2012
 Cabozantinib for medullary thyroid cancer February 2012 This technology summary is based on information available at the time of research and a limited literature search. It is not intended to be a definitive
Cabozantinib for medullary thyroid cancer February 2012 This technology summary is based on information available at the time of research and a limited literature search. It is not intended to be a definitive
Karim Said. 41 year old farmer. Referred from the Uro-surgery Department because of uncontrolled hypertension prior to Lt. partial nephrectomy
 Case Presentation Karim Said Cardiology Departement Cairo University 41 year old farmer Referred from the Uro-surgery Department because of uncontrolled hypertension prior to Lt. partial nephrectomy ١
Case Presentation Karim Said Cardiology Departement Cairo University 41 year old farmer Referred from the Uro-surgery Department because of uncontrolled hypertension prior to Lt. partial nephrectomy ١
Shifting Paradigms and Debates in the Management of Well-differentiated Thyroid Cancer
 DEBATE WJOES Shifting Paradigms and Debates in the Management of Well-differentiated Thyroid Cancer Shifting Paradigms and Debates in the Management of Well-differentiated Thyroid Cancer Ashok R Shaha
DEBATE WJOES Shifting Paradigms and Debates in the Management of Well-differentiated Thyroid Cancer Shifting Paradigms and Debates in the Management of Well-differentiated Thyroid Cancer Ashok R Shaha
Dynamic Risk Stratification:
 Dynamic Risk Stratification: Using Risk Estimates to Guide Initial Management R Michael Tuttle, MD Clinical Director, Endocrinology Service Memorial Sloan Kettering Cancer Center Professor of Medicine
Dynamic Risk Stratification: Using Risk Estimates to Guide Initial Management R Michael Tuttle, MD Clinical Director, Endocrinology Service Memorial Sloan Kettering Cancer Center Professor of Medicine
Thyroid and Parathyroid Disease. RTC Conference Christina Edwards Bailey Faculty: Dr. Carmen Solorzano April 2, 2010
 Thyroid and Parathyroid Disease RTC Conference Christina Edwards Bailey Faculty: Dr. Carmen Solorzano April 2, 2010 Case Presentation # 1 CC: Neck Mass HPI: 51f found to have a neck mass on routine PE.
Thyroid and Parathyroid Disease RTC Conference Christina Edwards Bailey Faculty: Dr. Carmen Solorzano April 2, 2010 Case Presentation # 1 CC: Neck Mass HPI: 51f found to have a neck mass on routine PE.