Indication and validity of ultrasonographic evaluation for assessment of vocal fold mobility before and after thyroid surgery
|
|
|
- Derrick Esmond Riley
- 6 years ago
- Views:
Transcription
1 ORIGINAL ARTICLES Indication and validity of ultrasonographic evaluation for assessment of vocal fold mobility before and after thyroid surgery Aya Ebina 1, Iwao Sugitani 2, Yorihisa Orita 3, Soshi Takao 4, Kiyoaki Tukahara 5, Keiko Yamada 6, Kazuyoshi Kawabata 1 1. Division of Head and Neck, Cancer Institute Hospital, Japanese Foundation for Cancer Research, Tokyo, Japan. 2. Division of Endocrine Surgery, Department of Surgery, Nippon Medical School, Tokyo, Japan. 3. Department of Otolaryngology Head and Neck Surgery, Okayama University Graduate School of Medicine, Dentistry and Pharmaceutical Sciences, Okayama, Japan. 4. Department of Epidemiology, Okayama University Graduate School of Medicine, Dentistry and Pharmaceutical Sciences, Okayama, Japan. 5. Department of Otolaryngology Head and Neck Surgery, Tokyo Medical University Hachioji Medical Center, Tokyo, Japan. 6. Division of Ultrasonography, Cancer Institute Hospital, Japanese Foundation for Cancer Research, Tokyo, Japan Correspondence: Aya Ebina. Address: Division of Head and Neck, Cancer Institute Hospital, Ariake, Koto-ku, Tokyo , Japan. aya.ebina@jfcr.or.jp Received: August 23, 2015 Accepted: October 19, 2015 Online Published: October 29, 2015 DOI: /ijdi.v3n1p26 URL: Abstract Background: Evaluating recurrent laryngeal nerve function before and after thyroid surgery is important. Although laryngeal electroendoscope is the most reliable tool for evaluating vocal fold (VF) mobility, ultrasonography (US) may offer a non-invasive alternative. The aim of this study is to evaluate the validity and limitation of US evaluation for the assessment of VF mobility. Methods: This was a study for diagnostic testing of US in a single center. One hundred and one patients who underwent thyroid surgery between February 2011 and August 2011 were enrolled to this study. Observation of the VF mobility using a B-mode US scanner was performed before and after thyroid surgery, through the thyrohyoid membrane, thyroid notch, and cricothyroid membrane. The results of US were compared with those of electroendoscopic examination which was performed on the same day but after the US. Results: First we excluded one case that could not be observed by electroendoscopic examination before surgery. After excluding the cases which the VF mobility was invisible by US, we analyzed 89 out of the 100 patients before thyroid surgery and 89 out of the 101 patients after surgery. The sensitivity and specificity of US were 87.5%, 100% for before and 94.4%, 100% for after surgery, respectively. It was significantly more difficult to assess the VF mobility by US among patients who were men (odds ratio [OR] 24.7, 95% confidence interval [CI] ), 65 years old or more (OR 3.5, 95% CI ), and have past history of thyroid surgery (OR 7.9, 95% CI ). Being obese was also a significant factor (OR 10.5, 95% CI ) among younger patients (less than 65 years). Conclusion: US evaluation can be used for the assessment of recurrent laryngeal nerve function before and after thyroid surgery. This is a safe and non-invasive diagnostic tool which may be performed as a first-line method. Keywords Ultrasonography, Thyroid surgery, Recurrent laryngeal nerve, Vocal fold 26 ISSN E-ISSN
2 1 Introduction Functional evaluation of the recurrent laryngeal nerve before and after thyroid surgery is very important. First, preoperative recurrent laryngeal nerve palsy may indicate extrathyroidal invasion of the tumor which may suggest poor prognosis of the patients [1]. The proper risk definition of the tumor results in appropriate selective approach to patient treatment and postoperative follow-up. Second, if recurrent laryngeal nerve palsy is identified before surgery, the surgeon can be prepared in case that an accidental injury of the contralateral healthy side occurs, and early detection of need for tracheostomy will prevent the patients from suffocation [2-5]. At last, since recurrent laryngeal nerve palsy is frequent complication occurring in thyroid surgery, absence of postoperative recurrent laryngeal nerve palsy can be one of the criteria for proper surgical quality [6, 7]. Laryngeal fiberscope, now electroendoscope is in popular use in Japan, is the most common and reliable instrument for directly checking vocal fold (VF) mobility, but is a little invasive and uncomfortable for patients [2, 8]. In addition, a surgeon who undergoes thyroid surgery is not always proficient in handling a laryngeal fiberscope. Currently, recurrent laryngeal nerve function is also evaluated using the other non-invasive methods such as ultrasonography (US) or electromyography, and especially US could evaluate VF mobility in over 85% of patients with thyroid disease [6, 9, 10]. Now US evaluation is almost indispensable to the patients with thyroid disease, and all we have to do is properly placing the US probe above the thyroid cartilage to observe the VF mobility after routine examination for thyroid and neck lymph nodes [6]. Although US can t detect subtle morphologic abnormalities of the larynx such as laryngeal carcinoma in the first stage of the disease, it may be a useful and cost-effective screening tool for observation of VF mobility. The aim of the present study was to investigate the feasibility and validity of US evaluation for assessment of VF mobility before and after thyroid surgery, and elucidate the factors which make it difficult for US to assess the VF mobility. 2 Matients and methods 2.1 Eligibility criteria for participants Patients who underwent thyroid surgery at Cancer Institute Hospital, tertiary oncology referral center in Japan, between February 2011 and August 2011, were considered as candidates for inclusion in the study. All patients were Japanese and provided written informed consent to participate. All thyroid surgeries were performed by conventional technique with subplatysmal skin flaps, and electocautery was used to make incisions and create skin flaps. Patients who had undergone laryngeal surgery (e.g. partial or total laryngectomy) were not included to the study. All study protocols have been reviewed and approved by the institutional review board. 2.2 Observation of the vocal fold All eligible patients underwent both of the electroendoscopic examination and neck US evaluation on the same days, the days before and after the thyroid surgery. Neck US evaluations (HITACHI-ALOCA, Tokyo, Japan) were performed using 7-18-MHz linear transducer by an experienced radiologist (K.Y), with special regard to VF mobility. During the US examination, the patient was placed in a supine position with the neck slightly extended and a pad under the shoulders to provide optimum exposure of the neck. First we asked all the patients if they had any neck problems like cervical spondylosis, and when they had some neck problems they were positioned at normal supine position. After our routine observation of the thyroid gland and neck lymph nodes, VF evaluation was performed. The US probe was placed transversely along the midline of the neck at the following three points: 1) the thyrohyoid membrane; 2) the thyroid notch; and 3) the cricothyroid membrane (see Figure 1). After the US evaluations, electroendoscopic examinations (OLYMPUS, Tokyo, Japan) via the nasal route were performed while having the patient in a seated position by an experienced otolaryngologist (A. E). Published by Sciedu Press 27
 thyrohyoid membrane; B) thyroid notch; and C) cricothyroid membrane. The black bars indicate the location of the transducer. 2.")


 have never been found by erectroendoscopic examination among the 1011 patients.")

 and 95% confidence intervals (CIs) to examine the association between patients profiles (sex, age, obesity, and prior operation history of thyroid) and")
3 International Journal of Diagnostic Imaging, 2016, Vol. 3, No. 1 The 3 points to place the transducer of ultrasonography to observe the vocal fold. The transducer was placed transversely over three points: A) thyrohyoid membrane; B) thyroid notch; and C) cricothyroid membrane. The black bars indicate the location of the transducer. 2.3 Outcome assessment In the US evaluation, false VFs appear as hyperechoicc structures while true VFs are hypoechoic, andd the vocal ligament (free edge of the true cord) is seen as an echogenic band [11]. Normall recurrent laryngeal nerve function was defined as symmetrically abductivee and adductive motions of the true and false VFs during deep respiration and phonation. Paralyzed recurrent laryngeal nerve was defined as limited motion of those movements or paradoxical movement (see Figure 2). There was one rare case whose VFs were covered by a protruding metastatic retropharyngeal lymph node and could not be fully observed by electroendoscopic examination before Figure 1. The 3 points to place the transducer of ultrasonography to observe the vocal fold thyroid surgery, and wee excluded this case from the analysis. There were no cases whose VFs could not be observed by electroendoscopic examination after surgeries. Any other abnormalities of the larynx than paralysis of recurrent laryngeal nerve (e.g.. laryngeal tumor) have never been found by erectroendoscopic examination among the 1011 patients. We compared the results of US evaluation with those of electroendoscopicc examination among cases of whichh VFs could be visualized by US. Since observation for right and left VF was considered to be essentially independent, we combined these observations. 2.4 Statistical analysis We estimated sensitivity, specificity, positive and negative predictive values to evaluate validity of US evaluation compared with electroendoscopic examination. Then, we calculated crude odds ratios (ORs) and 95% confidence intervals (CIs) to examine the association between patients profiles (sex, age, obesity, and prior operation history of thyroid) and application of US evaluation (NOT being able to visualize vs. being able to visualize) ). Ages were dichotomized into less than 65 years old and 65 years old or more. Obesity was defined by bodyy mass index (BMI) (more than or equal to 25). In addition, we calculated stratum specific ORs with obesity stratified by sex, age, and prior surgical history instead of logistic regression analysis for adjusting those factors at the same time.. The reason why we employed stratified analysis was that the influences of factors except obesity was obvious regardless of other factorss and adjusted ORs did not converge due to small numbers (actually, zero) of some cells. P values of less than 0.05 (two-sided test) were considered statistically significant. All analyses weree performed using STATA 12.1 (StataCorp, College Station, TX, USA) and JMP version 11 (SAS Institute Inc., Cary, NC USA). 3 Results Table 1 describes the characteristics of the study patients of which 75% were women. Mean age at the time of thyroid surgery was 54 years (range, years) ). The age distributions were similar between women and men. Of the 101 patients, 92 (91%) patients had a surgery for papillary thyroid carcinoma, 3 (3%) patients for anaplastic thyroid carcinoma, 2 (2%) patients for medullary thyroid carcinoma, 1 (1%) patient for follicular thyroid carcinoma, and the remaining 3 (3%) patients for benign thyroid tumors. As for surgical procedure, 55 (54%) patients underwent hemithyroidectomy, 30 (30%) patients had total thyroidectomy, and 16 (16%) patients had only neck dissection. All of these 16 patients who underwent only neck dissection had experienced prior thyroid surgeries. 28 ISSN E-ISSN
4 Table 1. Characteristics of the 101 patients who underwent thyroid surgery at Cancer Institute Hospital, Japan, 2011 (n = 101) Characteristics No. of patients (%) Sex Female 76 (75%) Male 25 (25%) Age (years), mean 54 (range, years) Female 53 ± 30 Male 53 ± 25 Obesity BMI (21.8%) BMI < (78.8%) Past history of thyroid surgery Yes 16 (15.8%) No 85 (84.2%) Thyroid pathology Papillary carcinoma 92 (91%) Anaplastic carcinoma 3 (3%) Medullary carcinoma 2 (2%) Follicular carcinoma 1 (1%) Benign tumor 3 (3%) Surgical procedure Hemithyroidectomy + central ND 49 (49%) Total thyroidectomy + central ND 17 (17%) Total thyroidectomy + bilateral ND 8 (8%) Total thyroidectomy + unilateral ND 6 (6%) Hemithyroidectomy + unilateral ND 5 (5%) ND only (secondary operation) 16 (16%) Note. SD: standard deviation, ND: neck dissection, BMI: body mass index. VF mobility could be observed by US evaluation in 89 patients out of the 100 patients whose VFs could be observed by electroendoscopic examination before thyroid surgery. In other words, we had 178 observations of VF mobility combined right and left VFs. After thyroid surgery, 89 out of 101 patients could be observed by US evaluation (178 observations). Sensitivity, specificity, positive and negative predictive values of US evaluation were 87.5%, 100%, 100%, and 99.4% before and 94.4%, 100%, 100%, and 98.6% after the thyroid surgery (see Table 2). Table 2. Assessment of vocal fold movement (right and left results were combined) Paralysis (+) by EE Paralysis (-) by EE Before thyroid surgery Paralysis (+) by US 7 0 Paralysis (-) by US After thyroid surgery Paralysis (+) by US 34 0 Paralysis (-) by US Note. US: ultrasonography; EE: electroendoscopy. Published by Sciedu Press 29




: A")






, 65 years old or more (OR 3.5, 95% CI 1.")
.")


 (see Table")

")





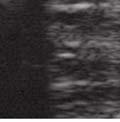
5 International Journal of Diagnostic Imaging, 2016, Vol. 3, No. 1 Figure 2. The images of ultrasonography with transverse view at the level of the thyroid notch. (A): A case with normal mobility of vocal folds. Bilateral false vocal folds show symmetrical abduction and adduction movements; (B): A paralysis case.. The left false vocal fold shows limited abduction movement. Note. The images of ultrasonography with transverse view at the levell of the thyroid notch. The left panel of these pictures shows closing glottis at the time of expiration, and the t right panel shows opening glottis at the time of inspiration. Comparing clinical profiles between patients with visible and invisible VF mobility on US (see Table 3), strong significant differences were observed for men (OR 24.7, 95% CI ), 65 years old or more (OR 3.5, 95% CI ), and have past history of thyroid surgery (OR 7.9, 95% CI ). Although obesity was not a significant factor, stratified analysis identified obesity was an independent predictorr (OR 10.5, 95% CI ) of invisible on US only among younger patients (less than 65 years old) (see Table 4). In preoperativee examination, the case that could not be visualized by EE was excluded (n = 1). US could visualize the vocal fold (VF) mobility in 89 of 100 patients. Sensitivity = 87.5%, specificity = 100% %, positive predictive value = 100%, and negative predictive value = 99.4%. In postoperative examination, VF mobility could be visualized by EE inn all of the 101 cases. US could visualize the VF mobility in 89 of 101 patients. Sensitivity = 94.4%, specificity = 100% %, positive predictive value = 100%, and negative predictive value = 98.6%. Table 3. Crude Odds ratios for NOT being able to visualize vocal foldd mobility by ultrasonographic evaluation before thyroid surgery Odds ratio 95% CI Age (65 vs. 65 <) Sex (men vs. women) Obesity (BMI 25 vs. BMI < 25) Prior operation (+ vs. -) Note. OR: odds ratio; 95%CI: 95% confidence interval. 30 ISSN E-ISSN
6 Table 4. Stratum specific Odds Ratios with obesity for NOT being able to visualize vocal fold mobility by ultrasonographic evaluation before thyroid surgery stratified by sex, age, and prior operation history Stratified by sex Odds ratio 95% CI Men Women N/A N/A Stratified by age Age Age < 65 N/A N/A Stratified by prior operation yes No Note. 95% CI: 95% confidence interval; N/A: not applicable. 4 Discussion The present study found that US could correctly assess recurrent laryngeal nerve function both before and after thyroid surgery, and the sensitivity and specificity were considerably high. However, it could not be available in all of the cases (almost 90% of the study patients). There were four factors that made it difficult for US to observe VF mobility; men, older age (65 years old or more), past history of thyroid surgery, and obesity among the patients younger than 65 years. First, the difficulty to assess the VF mobility by US in men compared with in women may mainly be due to anatomical differences of the larynx between men and women. In the case of adults, the external angle between the blades of the thyroid cartilage is more acute in men than in women and the distance from the thyroid notch to the anterior commissure is greater in men than in women [12]. In other words, it is difficult to appropriately place the flat transducer on the acute angular thyroid cartilage of men, and the distance from the surface of the transducer to the VF tends to be greater in men than in women. Second, the difficulty to assess the VF mobility by US in older patients may mainly be due to increasing thyroid cartilage ossification with advancing age, which processes more extensive in men than in women [13]. Third, past history of thyroid surgery may cause postoperative scaring or fibrosis which may make it more difficult for US to observe VF mobility. At last, the neck subcutaneous fat thickness of the patients with obesity may affect the accuracy of US evaluation for VF mobility. The reason why high BMI was not a significant factor among older age group may be due to the fact that BMI is originally an indicator to assess abdominal obesity and obesity will progress with aging mainly at lower parts of the trunk such as the waist and infragluteal region [14]. Wang et al. also found that US evaluation of VF mobility was significantly more difficult in men than in women, and in older patients than younger patients, which were compatible with the present study [6]. The use of electrocautery during surgery may cause flap edema and greatly thicken the flap [15]. Actually, in the present study, the thickness of the flap measured by the minimum distance from the surface of the neck skin to the thyroid cartilage came to be significantly greater after surgery (4.9 ± 0.3 mm, mean, standard error) than before surgery (3.3 ± 0.2 mm, p <.001, n = 82, data not shown), and actually in one case of which the VFs could have been observed by US before surgery, the VFs came to be invisible by US after the surgery because of severe flap edema. However, validity of US evaluation for VF mobility did not change essentially between before and after surgery. The thyroid cartilage will provide the best window for US imaging of the VF, and VF will also be well visible through the cricothyroid membrane, while the probability to visualize VF through thyrohyoid membrane is 71% [16]. Observation from all of 3 points (thyroid membrane, thyroid notch, and cricothyroid membrane) may a little improve the accuracy of US evaluation for VF, and in one rare case that electroendoscopic examination could not confirm the exact VF mobility due to Published by Sciedu Press 31
7 a protruding metastatic retropharyngeal lymph node over the larynx, the VF mobility could be observed by US. Thus US may also be useful for observation of VF mobility in the case that laryngeal fiber scope is ineffective for observation of the VF. In Japan, since the charge for laryngeal fiberscopic examination is much more expensive than simple thyroid ultrasonography, repeating both of US and laryngeal fiberscopic examination may be too heavy a burden for the patients. Considering the cost performance and the fact that US evaluation is indispensable to examine thyroid diseases and many patients with thyroid cancer are non-smoking elderly women, laryngeal fiberscopic examination may be able to be omitted from the routine pre- and postoperative examination of thyroid surgery, when US evaluation can properly detect the VF mobility and tumor invasion to the larynx or trachea is not suspected. However, up to 30% of patients with normal VF mobility after thyroid surgery complain of subjective voice changes of which exact cause remains unclear [17, 18]. In such patients with postoperative symptoms, fiberscopic examination should be performed to protect the surgeon from subsequent litigation [19] or not to overlook any other abnormalities in the larynx, even when VF mobility can be observed by US. In the present study, there was one limitation that since only one experienced radiologist performed US, general reproducibility and interobserver variability were uncertain, although the technique to handle US for observation of the VF is not difficult. 5 Conclusion The present study suggests that US evaluation can be used for the assessment of recurrent laryngeal nerve function before and after thyroid surgery. This is a safe and non-invasive diagnostic tool which may be performed as a first-line method. Laryngeal fiberscopic examination should be performed only when US evaluation is ineffective or the patient is symptomatic. Or at least, repeated laryngeal fiberscopic examination may be unnecessary when VF mobility can be evaluated by US. References [1] Sugitani I, Kasai N, Fujimoto Y, et al. A novel classification system for patients with PTC: Addition of the new variables of large (3 cm or greater) nodal metastases and reclassification during the follow-up period. Surgery. 2004; 135: [2] Bisetti MS, Segala F, Zappia F, et al. Non-invasive assessment of benign vocal folds lesions in children by means of ultrasonography. Int J Pediatr Otorhinolaryngol. 2009; 73(8): PMid: [3] Ko HC, Lee LA, Li HY, et al. Etiologic features in patients with unilateral vocal fold paralysis in Taiwan. Chang Gung Med J. 2009; 32(3): PMid: [4] Dedecjus M, Adamczewski Z, Brzeziński J, et al. Real-time, high-resolution ultrasonography of the vocal folds-a prospective pilot study in patients before and after thyroidectomy. Langenbecks Arch Surg. 2010; 395(7): PMid: [5] Sulica L, Blitzer A. Vocal fold paresis: evidence and controversies. Curr Opin Otolaryngol Head Neck Surg. 2007; 15(3): PMid: [6] Wang CP, Chen TC, Yang TL, et al. Transcutaneous ultrasound for evaluation of vocal fold movement in patients with thyroid disease. Eur J Radiol. 2012; 81(3): PMid: [7] Farrag TY, Samlan RA, Lin FR, et al. The utility of evaluating true vocal fold motion before thyroid surgery. Laryngoscope. 2006; 116: PMid: [8] Vats A, Worley GA, de Bruyn R, et al. Laryngeal ultrasound to assess vocal fold paralysis in children. J Laryngeal Otol. 2004; 118(6): ISSN E-ISSN
8 [9] Wang CP, Chen TC, Lou PJ, et al. Neck ultrasonography for the evaluation of the etiology of adult unilateral vocal fold paralysis. Head Neck. 2012; 34(5): PMid: [10] Cheng SP, Lee JJ, Liu TP, et al. Preoperative ultrasonography assessment of vocal cord movement during thyroid and parathyroid surgery. World J Surg. 2012; 36(10): PMid: [11] Ng SK, Yuen HY, van Hasselt CA, et al. Combined ultrasound/endoscopy-assisted vocal fold injection for unilateral vocal cord paralysis: a case series. Eur Radiol. 2012; 22: PMid: [12] Jotz GP, Stefani MA, da Costa Filho OP, et al. A morphometric study of the larynx. J Voice. 2014; 28(6): PMid: [13] Dang-Tran KD, Dedouit F, Joffre F, et al. Thyroid cartilage ossification and multislice computed tomography examination: a useful tool for age assessment? J Forensic Sci. 2010; 55: PMid: [14] Murakami M, Hikima R, Arai S, et al. Short-term longitudinal changes in subcutaneous fat distribution and body size among Japanese women in the third decade of life. Appl Human Sci. 1999; 18: PMid: [15] Uludag M, Yetkin G, Ozel A, et al. Wound complications and clinical results of electrocautery versus a scalpel to create a cutaneous flap in thyroidectomy: A prospective randomized trial. Surg Today. 2011; 41: PMid: [16] Singh M, Chin KJ, Chan VW, et al. Use of sonography for airway assessment: an observational study. J Ultrasound Med. 2010; 29: PMid: [17] de Pedro Netto I, Fae A, Vartanian JG, et al. Voice and vocal self-assessment after thyroidectomy. Head Neck. 2006; 28: PMid: [18] Stojadinovic A, Shaha AR, Orlikoff RF, et al. Prospective functional voice assessment in patients undergoing thyroid surgery. Ann Surg. 2002; 236: PMid: [19] Schlosser K, Zeuner M, Wagner M, et al. Laryngoscopy in thyroid surgery-essential standard or unnecessary routine? Surgery. 2007; 142: PMid: Published by Sciedu Press 33
Randall J. Amis *, Deepak Gupta *, Jayme R. Dowdall **, Abstract. Introduction
 Ultrasound assessment of Vocal Fold Paresis: A Correlation Case Series with Flexible Fiberoptic Laryngoscopy and Adding the Third Dimension (3-D) to Vocal Fold Mobility Assessment Randall J. Amis *, Deepak
Ultrasound assessment of Vocal Fold Paresis: A Correlation Case Series with Flexible Fiberoptic Laryngoscopy and Adding the Third Dimension (3-D) to Vocal Fold Mobility Assessment Randall J. Amis *, Deepak
THYROID CANCER IN CHILDREN. Humberto Lugo-Vicente MD FACS FAAP Professor Pediatric Surgery UPR School of Medicine
 THYROID CANCER IN CHILDREN Humberto Lugo-Vicente MD FACS FAAP Professor Pediatric Surgery UPR School of Medicine Thyroid nodules Rare Female predominance 4-fold as likely to be malignant Hx Radiation exposure?
THYROID CANCER IN CHILDREN Humberto Lugo-Vicente MD FACS FAAP Professor Pediatric Surgery UPR School of Medicine Thyroid nodules Rare Female predominance 4-fold as likely to be malignant Hx Radiation exposure?
Reoperative central neck surgery
 Reoperative central neck surgery R. Pandev, I. Tersiev, M. Belitova, A. Kouizi, D. Damyanov University Clinic of Surgery, Section Endocrine Surgery University Hospital Queen Johanna ISUL Medical University
Reoperative central neck surgery R. Pandev, I. Tersiev, M. Belitova, A. Kouizi, D. Damyanov University Clinic of Surgery, Section Endocrine Surgery University Hospital Queen Johanna ISUL Medical University
Validation of ultrasound as a diagnostic tool to assess vocal cord motion in an animal feasibility study
 Original Article Validation of ultrasound as a diagnostic tool to assess vocal cord motion in an animal feasibility study Karuna Dewan 1, Merry E. Sebelik 2, John D. Boughter 3, Courtney B. Shires 4 1
Original Article Validation of ultrasound as a diagnostic tool to assess vocal cord motion in an animal feasibility study Karuna Dewan 1, Merry E. Sebelik 2, John D. Boughter 3, Courtney B. Shires 4 1
10/24/2008. Surgery for Well-differentiated Thyroid Carcinoma- The Primary
 Surgery for Well-differentiated Thyroid Carcinoma- The Primary Head and Neck Endocrine Surgery Department of Otolaryngology-Head and Neck Surgery, UCSF October 24-25, 2008 Robert A. Sofferman, MD Professor
Surgery for Well-differentiated Thyroid Carcinoma- The Primary Head and Neck Endocrine Surgery Department of Otolaryngology-Head and Neck Surgery, UCSF October 24-25, 2008 Robert A. Sofferman, MD Professor
Thyroid INTRODUCTION ANATOMY SUMMARY OF CHANGES
 AJC 7/14/06 1:19 PM Page 67 Thyroid C73.9 Thyroid gland SUMMARY OF CHANGES Tumor staging (T) has been revised and the categories redefined. T4 is now divided into T4a and T4b. Nodal staging (N) has been
AJC 7/14/06 1:19 PM Page 67 Thyroid C73.9 Thyroid gland SUMMARY OF CHANGES Tumor staging (T) has been revised and the categories redefined. T4 is now divided into T4a and T4b. Nodal staging (N) has been
Persistent & Recurrent Differentiated Thyroid Cancer
 Persistent & Recurrent Differentiated Thyroid Cancer Electron Kebebew University of California, San Francisco Department of Surgery Objectives Risk factors for persistent & recurrent disease Causes of
Persistent & Recurrent Differentiated Thyroid Cancer Electron Kebebew University of California, San Francisco Department of Surgery Objectives Risk factors for persistent & recurrent disease Causes of
New technologies in Endocrine Surgery
 New technologies in Endocrine Surgery 1. Nerve monitoring 2. New technologies in Endocrine Surgery Jessica E. Gosnell MD Post graduate course in General Surgery March 28, 2012 1 2 Recurrent laryngeal nerve
New technologies in Endocrine Surgery 1. Nerve monitoring 2. New technologies in Endocrine Surgery Jessica E. Gosnell MD Post graduate course in General Surgery March 28, 2012 1 2 Recurrent laryngeal nerve
Ultrasound for Pre-operative Evaluation of Well Differentiated Thyroid Cancer
 Ultrasound for Pre-operative Evaluation of Well Differentiated Thyroid Cancer Its Not Just About the Nodes AACE Advances in Medical and Surgical Management of Thyroid Cancer - 2017 Robert A. Levine, MD,
Ultrasound for Pre-operative Evaluation of Well Differentiated Thyroid Cancer Its Not Just About the Nodes AACE Advances in Medical and Surgical Management of Thyroid Cancer - 2017 Robert A. Levine, MD,
safety margin, To leave a functioning i larynx i.e. respiration, phonation & swallowing.
 The aim of the horizontal supra-glottic laryngectomy is: To remove the tumour with good safety margin, To leave a functioning i larynx i.e. respiration, phonation & swallowing. Disadvantages of classical
The aim of the horizontal supra-glottic laryngectomy is: To remove the tumour with good safety margin, To leave a functioning i larynx i.e. respiration, phonation & swallowing. Disadvantages of classical
Avi Khafif, MD, Rami Ben-Yosef, MD, Avrum Abergel, MD, Ada Kesler, MD, Roee Landsberg, MD, Dan M. Fliss, MD
 ORIGINAL ARTICLE ELECTIVE PARATRACHEAL NECK DISSECTION FOR LATERAL METASTASES FROM PAPILLARY CARCINOMA OF THE THYROID: IS IT INDICATED? Avi Khafif, MD, Rami Ben-Yosef, MD, Avrum Abergel, MD, Ada Kesler,
ORIGINAL ARTICLE ELECTIVE PARATRACHEAL NECK DISSECTION FOR LATERAL METASTASES FROM PAPILLARY CARCINOMA OF THE THYROID: IS IT INDICATED? Avi Khafif, MD, Rami Ben-Yosef, MD, Avrum Abergel, MD, Ada Kesler,
Case Scenario #1 Larynx
 Case Scenario #1 Larynx 56 year old white female who presented with a 2 month history of hoarseness treated with antibiotics, but with no improvement. In the last 3 weeks, she has had a 15 lb weight loss,
Case Scenario #1 Larynx 56 year old white female who presented with a 2 month history of hoarseness treated with antibiotics, but with no improvement. In the last 3 weeks, she has had a 15 lb weight loss,
Case Scenario 1. Pathology: Specimen type: Incisional biopsy of the glottis Histology: Moderately differentiated squamous cell carcinoma
 Case Scenario 1 History A 52 year old male with a 20 pack year smoking history presented with about a 6 month history of persistent hoarseness. The patient had a squamous cell carcinoma of the lip removed
Case Scenario 1 History A 52 year old male with a 20 pack year smoking history presented with about a 6 month history of persistent hoarseness. The patient had a squamous cell carcinoma of the lip removed
Innervation of the cricothyroid muscle by the recurrent laryngeal nerve
 ORIGINAL ARTICLE Innervation of the cricothyroid muscle by the recurrent laryngeal nerve Hiroo Masuoka, MD, PhD,* Akira Miyauchi, MD, PhD, Tomonori Yabuta, MD, PhD, Mitsuhiro Fukushima, MD, PhD, Akihiro
ORIGINAL ARTICLE Innervation of the cricothyroid muscle by the recurrent laryngeal nerve Hiroo Masuoka, MD, PhD,* Akira Miyauchi, MD, PhD, Tomonori Yabuta, MD, PhD, Mitsuhiro Fukushima, MD, PhD, Akihiro
Clinical Trials of Active Surveillance of Papillary Microcarcinoma of the Thyroid
 World J Surg (2016) 40:516 522 DOI 10.1007/s00268-015-3392-y ORIGINAL SCIENTIFIC REPORT Clinical Trials of Active Surveillance of Papillary Microcarcinoma of the Thyroid Akira Miyauchi 1,2 Published online:
World J Surg (2016) 40:516 522 DOI 10.1007/s00268-015-3392-y ORIGINAL SCIENTIFIC REPORT Clinical Trials of Active Surveillance of Papillary Microcarcinoma of the Thyroid Akira Miyauchi 1,2 Published online:
Wojciech K. Mydlarz, M.D. Pharyngocutaneous Fistulas after Salvage Laryngectomy: Need for Vascularized Tissue
 Wojciech K. Mydlarz, M.D. Pharyngocutaneous Fistulas after Salvage Laryngectomy: Need for Vascularized Tissue Disclosures No Relevant Financial Relationships or Commercial Interests Educational Objectives
Wojciech K. Mydlarz, M.D. Pharyngocutaneous Fistulas after Salvage Laryngectomy: Need for Vascularized Tissue Disclosures No Relevant Financial Relationships or Commercial Interests Educational Objectives
Review Article Thyroidectomy and Lymph Node Dissection in Papillary Thyroid Carcinoma
 SAGE-Hindawi Access to Research Thyroid Research Volume 2011, Article ID 634170, 6 pages doi:10.4061/2011/634170 Review Article Thyroidectomy and Lymph Node Dissection in Papillary Thyroid Carcinoma Yasuhiro
SAGE-Hindawi Access to Research Thyroid Research Volume 2011, Article ID 634170, 6 pages doi:10.4061/2011/634170 Review Article Thyroidectomy and Lymph Node Dissection in Papillary Thyroid Carcinoma Yasuhiro
Autologous Fat Augmentation of the Vocal Folds
 Tokai J Exp Clin Med., Vol. 39, No. 3, pp. 146-150, 2014 Autologous Fat Augmentation of the Vocal Folds Shinya OKADA *1, Etsuyo TAMURA *2 and Masahiro IIDA *3 *1 Department of Otorhinolaryngology, Tokai
Tokai J Exp Clin Med., Vol. 39, No. 3, pp. 146-150, 2014 Autologous Fat Augmentation of the Vocal Folds Shinya OKADA *1, Etsuyo TAMURA *2 and Masahiro IIDA *3 *1 Department of Otorhinolaryngology, Tokai
Objectives. Purpose. Conference Calls 2 hrs. Process 9/7/2013. Clinical Practice Guideline: Improving Voice Outcomes after Thyroid Surgery
 Objectives Clinical Practice Guideline: Improving Voice Outcomes after Thyroid Surgery 37 th Annual Congress & Nursing Symposium Vancouver, BC September 29, 2013 Carolyn Waddington RN MS FNP-C CORLN Explain
Objectives Clinical Practice Guideline: Improving Voice Outcomes after Thyroid Surgery 37 th Annual Congress & Nursing Symposium Vancouver, BC September 29, 2013 Carolyn Waddington RN MS FNP-C CORLN Explain
The importance of sonographic landmarks by transcutaneous laryngeal ultrasonography in post-thyroidectomy vocal cord assessment
 Title The importance of sonographic landmarks by transcutaneous laryngeal ultrasonography in post-thyroidectomy vocal cord assessment Author(s) Wong, KP; Woo, JW; Youn, YK; Chow, FC; Lee, KE; Lang, BHH
Title The importance of sonographic landmarks by transcutaneous laryngeal ultrasonography in post-thyroidectomy vocal cord assessment Author(s) Wong, KP; Woo, JW; Youn, YK; Chow, FC; Lee, KE; Lang, BHH
Long-term Follow-up for Patients with Papillary Thyroid Carcinoma Treated as Benign Nodules
 Long-term Follow-up for Patients with Papillary Thyroid Carcinoma Treated as Benign Nodules YASUHIRO ITO, TAKUYA HIGASHIYAMA, YUUKI TAKAMURA, AKIHIRO MIYA, KAORU KOBAYASHI, FUMIO MATSUZUKA, KANJI KUMA
Long-term Follow-up for Patients with Papillary Thyroid Carcinoma Treated as Benign Nodules YASUHIRO ITO, TAKUYA HIGASHIYAMA, YUUKI TAKAMURA, AKIHIRO MIYA, KAORU KOBAYASHI, FUMIO MATSUZUKA, KANJI KUMA
Head & Neck Clinical Sub Group. Network Agreed Imaging Guidelines for UAT and Thyroid Cancer. Measure Nos: 11-1C-105i & 11-1C-106i
 Greater Manchester, Lancashire & South Cumbria Strategic Clinical Network & Senate Head & Neck Clinical Sub Group Network Agreed Imaging Guidelines for UAT and Thyroid Cancer Measure Nos: 11-1C-105i &
Greater Manchester, Lancashire & South Cumbria Strategic Clinical Network & Senate Head & Neck Clinical Sub Group Network Agreed Imaging Guidelines for UAT and Thyroid Cancer Measure Nos: 11-1C-105i &
Larynx. Rudimentary. Behind the posterior surface : -stylopharyngeus - salpingopharyngeus -platopharyngeus
 Larynx The larynx is an organ that provides a protective sphincter at the inlet of the air passages and is responsible for voice production. It extends from C3-C6: *Posterior: the pharynx *Lateral: the
Larynx The larynx is an organ that provides a protective sphincter at the inlet of the air passages and is responsible for voice production. It extends from C3-C6: *Posterior: the pharynx *Lateral: the
Get The Cancer Staging Manual Pdf Thyroid
 Get The Cancer Staging Manual Pdf Thyroid Most people with thyroid cancer have no known risk factors that they can change, Manual. They are based on the stage of the cancer when the person is first. Staging
Get The Cancer Staging Manual Pdf Thyroid Most people with thyroid cancer have no known risk factors that they can change, Manual. They are based on the stage of the cancer when the person is first. Staging
Thyroid nodules - medical and surgical management. Endocrinology and Endocrine Surgery Manchester Royal Infirmary
 Thyroid nodules - medical and surgical management JRE Davis NR Parrott Endocrinology and Endocrine Surgery Manchester Royal Infirmary Thyroid nodules - prevalence Thyroid nodules common, increase with
Thyroid nodules - medical and surgical management JRE Davis NR Parrott Endocrinology and Endocrine Surgery Manchester Royal Infirmary Thyroid nodules - prevalence Thyroid nodules common, increase with
Title. CitationInternational Cancer Conference Journal, 4(1): Issue Date Doc URL. Rights. Type. File Information
: Issue Date Doc URL. Rights. Type. File Information") Title Lymph node metastasis in the suprasternal space from Homma, Akihiro; Hatakeyama, Hiromitsu; Mizumachi, Ta Author(s) Tomohiro; Fukuda, Satoshi CitationInternational Cancer Conference Journal, 4(1):
Title Lymph node metastasis in the suprasternal space from Homma, Akihiro; Hatakeyama, Hiromitsu; Mizumachi, Ta Author(s) Tomohiro; Fukuda, Satoshi CitationInternational Cancer Conference Journal, 4(1):
Ultrasound Interpretation of Non-Thyroid Neck Pathology
 Ultrasound Interpretation of Non-Thyroid Neck Pathology Kevin T. Brumund, M.D., F.A.C.S. Associate Professor of Surgery Head and Neck Surgery University of California, San Diego Health Sciences VA Medical
Ultrasound Interpretation of Non-Thyroid Neck Pathology Kevin T. Brumund, M.D., F.A.C.S. Associate Professor of Surgery Head and Neck Surgery University of California, San Diego Health Sciences VA Medical
Surgery for Recurrent Thyroid cancer: Considerations and limitations
 Surgery for Recurrent Thyroid cancer: Considerations and limitations 2016 Thyroid Master Class February 13, 2016 Ara A. Chalian MD, FACS Surgical Patient Safety Officer University Of Pennsylvania Health
Surgery for Recurrent Thyroid cancer: Considerations and limitations 2016 Thyroid Master Class February 13, 2016 Ara A. Chalian MD, FACS Surgical Patient Safety Officer University Of Pennsylvania Health
A variation in recurrence patterns of papillary thyroid cancer with disease progression: A long-term follow-up study
 ORIGINAL ARTICLE A variation in recurrence patterns of papillary thyroid cancer with disease progression: A long-term follow-up study Joon-Hyop Lee, MD, Yoo Seung Chung, MD, PhD,* Young Don Lee, MD, PhD
ORIGINAL ARTICLE A variation in recurrence patterns of papillary thyroid cancer with disease progression: A long-term follow-up study Joon-Hyop Lee, MD, Yoo Seung Chung, MD, PhD,* Young Don Lee, MD, PhD
Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer
 Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer AACE - Advances in Medical and Surgical Management of Thyroid Cancer - 2018 Robert A. Levine, MD, FACE, ECNU Thyroid Center of New Hampshire Geisel
Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer AACE - Advances in Medical and Surgical Management of Thyroid Cancer - 2018 Robert A. Levine, MD, FACE, ECNU Thyroid Center of New Hampshire Geisel
Shifting Paradigms and Debates in the Management of Well-differentiated Thyroid Cancer
 DEBATE WJOES Shifting Paradigms and Debates in the Management of Well-differentiated Thyroid Cancer Shifting Paradigms and Debates in the Management of Well-differentiated Thyroid Cancer Ashok R Shaha
DEBATE WJOES Shifting Paradigms and Debates in the Management of Well-differentiated Thyroid Cancer Shifting Paradigms and Debates in the Management of Well-differentiated Thyroid Cancer Ashok R Shaha
Organ preservation in laryngeal cancer
 Organ preservation in laryngeal cancer Wojciech Golusiński Department of Head and Neck Surgery The Great Poland Cancer Centre, Poznan, Poland Poznan University of Medical Sciences, Poznan, Poland Silver
Organ preservation in laryngeal cancer Wojciech Golusiński Department of Head and Neck Surgery The Great Poland Cancer Centre, Poznan, Poland Poznan University of Medical Sciences, Poznan, Poland Silver
How good are we at finding nodules? Thyroid Nodules Thyroid Cancer Epidemiology Initial management Long-term follow up Disease-free status
 New Perspectives in Thyroid Cancer Jennifer Sipos, MD Assistant Professor of Medicine Division of Endocrinology The Ohio State University Outline Thyroid Nodules Thyroid Cancer Epidemiology Initial management
New Perspectives in Thyroid Cancer Jennifer Sipos, MD Assistant Professor of Medicine Division of Endocrinology The Ohio State University Outline Thyroid Nodules Thyroid Cancer Epidemiology Initial management
Laser Cordectomy. Glottic Carcinoma
 Laser Cordectomy in Glottic Carcinoma Department of Otolaryngology gy Head & Neck Surgery Alexandria University Historical Review Endolaryngeal extirpation of vocal cord cancers is a controversial o issue
Laser Cordectomy in Glottic Carcinoma Department of Otolaryngology gy Head & Neck Surgery Alexandria University Historical Review Endolaryngeal extirpation of vocal cord cancers is a controversial o issue
The International Federation of Head and Neck Oncologic Societies. Current Concepts in Head and Neck Surgery and Oncology
 The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
Prediction of ipsilateral and contralateral central lymph node metastasis in unilateral papillary thyroid carcinoma: a retrospective study
 Original Article Prediction of ipsilateral and contralateral central lymph node metastasis in unilateral papillary thyroid carcinoma: a retrospective study Qiang Chen, Xiu-He Zou, Tao Wei, Qiu-Shi Huang,
Original Article Prediction of ipsilateral and contralateral central lymph node metastasis in unilateral papillary thyroid carcinoma: a retrospective study Qiang Chen, Xiu-He Zou, Tao Wei, Qiu-Shi Huang,
PEDIATRIC Ariel Katz MD
 PEDIATRIC Ariel Katz MD Dept. Otolaryngology Head &Neck Surgery Wolfson Medical Center Holon, Israel OBJECTIVES Overview/Background Epidemiology/Etiology Intro to Guidelines Workup Treatment Follow-Up
PEDIATRIC Ariel Katz MD Dept. Otolaryngology Head &Neck Surgery Wolfson Medical Center Holon, Israel OBJECTIVES Overview/Background Epidemiology/Etiology Intro to Guidelines Workup Treatment Follow-Up
A descriptive study on solitary nodular goitre
 Original Research Article A descriptive study on solitary nodular goitre T. Chitra 1*, Dorai D. 1, Aarthy G. 2 1 Associate Professor, 2 Post Graduate Department of General Surgery, Govt. Stanley Medical
Original Research Article A descriptive study on solitary nodular goitre T. Chitra 1*, Dorai D. 1, Aarthy G. 2 1 Associate Professor, 2 Post Graduate Department of General Surgery, Govt. Stanley Medical
Superior Laryngeal Nerve Injury: Diagnosis and Management. Presented by: Nyall London October 10, 2014
 Superior Laryngeal Nerve Injury: Diagnosis and Management Presented by: Nyall London October 10, 2014 1 Case Presentation 49 year old male s/p right side approach anterior cervical discectomy and fusion
Superior Laryngeal Nerve Injury: Diagnosis and Management Presented by: Nyall London October 10, 2014 1 Case Presentation 49 year old male s/p right side approach anterior cervical discectomy and fusion
Evaluation and Treatment of Aerodigestive Tract Invasion by Well-Differentiated Thyroid Carcinoma
 An understanding of the patterns of invasion and the methods of treatment of invasive thyroid carcinoma promotes optimal treatment of invasive thyroid carcinoma. S. Josué. Morning Light, Photo-Realist
An understanding of the patterns of invasion and the methods of treatment of invasive thyroid carcinoma promotes optimal treatment of invasive thyroid carcinoma. S. Josué. Morning Light, Photo-Realist
Preoperative Evaluation
 Preoperative Evaluation Lateral compartment lymph nodes are easier to detect and are amenable to FNA Central compartment lymph nodes are much more difficult to detect and FNA (Tg washout testing is compromised)
Preoperative Evaluation Lateral compartment lymph nodes are easier to detect and are amenable to FNA Central compartment lymph nodes are much more difficult to detect and FNA (Tg washout testing is compromised)
AJCC Staging of Head & Neck Cancer (7 th edition, 2010) -LIP & ORAL CAVITY-
 -LIP & ORAL CAVITY-") TX: primary tumor cannot be assessed T0: no evidence of primary tumor Tis: carcinoma in situ. T1: tumor is 2 cm or smaller AJCC Staging of Head & Neck Cancer (7 th edition, 2010) -LIP & ORAL CAVITY- T2:
TX: primary tumor cannot be assessed T0: no evidence of primary tumor Tis: carcinoma in situ. T1: tumor is 2 cm or smaller AJCC Staging of Head & Neck Cancer (7 th edition, 2010) -LIP & ORAL CAVITY- T2:
4/22/2010. Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey.
 Management of Differentiated Thyroid Cancer: Head Neck Surgeon Perspective Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey Thyroid gland Small endocrine gland:
Management of Differentiated Thyroid Cancer: Head Neck Surgeon Perspective Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey Thyroid gland Small endocrine gland:
Ultrasonography of the Neck as an Adjunct to FNA. Nicole Massoll M.D.
 Ultrasonography of the Neck as an Adjunct to FNA Nicole Massoll M.D. Basic Features of Head and Neck Ultrasound and Anatomy Nicole Massoll M.D. University of Arkansas for Medical Sciences, Little Rock
Ultrasonography of the Neck as an Adjunct to FNA Nicole Massoll M.D. Basic Features of Head and Neck Ultrasound and Anatomy Nicole Massoll M.D. University of Arkansas for Medical Sciences, Little Rock
Initial surgery for differentiated thyroid cancer: What is the appropriate extent and attendant risks and benefits?
 Initial surgery for differentiated thyroid cancer: What is the appropriate extent and attendant risks and benefits? Julie Ann Sosa, MD MA FACS Professor of Surgery and Medicine Chief, Section of Endocrine
Initial surgery for differentiated thyroid cancer: What is the appropriate extent and attendant risks and benefits? Julie Ann Sosa, MD MA FACS Professor of Surgery and Medicine Chief, Section of Endocrine
Surgical Treatment for Papillary Thyroid Carcinoma in Japan: Differences from Other Countries
 REVIEW ARTICLE J Korean Thyroid Assoc Vol. 4, No. 2, November 2011 Surgical Treatment for Papillary Thyroid Carcinoma in Japan: Differences from Other Countries Yasuhiro Ito, MD and Akira Miyauchi, MD
REVIEW ARTICLE J Korean Thyroid Assoc Vol. 4, No. 2, November 2011 Surgical Treatment for Papillary Thyroid Carcinoma in Japan: Differences from Other Countries Yasuhiro Ito, MD and Akira Miyauchi, MD
Please refer back to the slides as these are extra notes only. Slide 2 -The Larynx is a Box of cartilage.
 [ANATOMY #3] 1 بسم رلاهللا Please refer back to the slides as these are extra notes only. Slide 2 -The Larynx is a Box of cartilage. -The lower border of c6 is the lower border of cricoid cartilage. -The
[ANATOMY #3] 1 بسم رلاهللا Please refer back to the slides as these are extra notes only. Slide 2 -The Larynx is a Box of cartilage. -The lower border of c6 is the lower border of cricoid cartilage. -The
Disclosures Nodal Management in Differentiated Thyroid Carcinoma
 Disclosures Nodal Management in Differentiated Thyroid Carcinoma Nothing to disclose Jonathan George, MD, MPH Assistant Professor UCSF Head and Neck Oncologic & Endocrine Surgery Objectives Overview Describe
Disclosures Nodal Management in Differentiated Thyroid Carcinoma Nothing to disclose Jonathan George, MD, MPH Assistant Professor UCSF Head and Neck Oncologic & Endocrine Surgery Objectives Overview Describe
Differentiated Thyroid Carcinoma
 Differentiated Thyroid Carcinoma The GOOD cancer? Jennifer Sipos, MD Associate Professor of Medicine Director, Benign Thyroid Program Division of Endocrinology, Diabetes and Metabolism The Ohio State University
Differentiated Thyroid Carcinoma The GOOD cancer? Jennifer Sipos, MD Associate Professor of Medicine Director, Benign Thyroid Program Division of Endocrinology, Diabetes and Metabolism The Ohio State University
A Study of Thyroid Swellings and Correlation between FNAC and Histopathology Results
 International Journal of Current Microbiology and Applied Sciences ISSN: 2319-7706 Volume 6 Number 4 (2017) pp. 265-269 Journal homepage: http://www.ijcmas.com Original Research Article https://doi.org/10.20546/ijcmas.2017.604.030
International Journal of Current Microbiology and Applied Sciences ISSN: 2319-7706 Volume 6 Number 4 (2017) pp. 265-269 Journal homepage: http://www.ijcmas.com Original Research Article https://doi.org/10.20546/ijcmas.2017.604.030
C lin ica l research on 2228 ca ses of thyro id gland tum ors WANG J ia2dong, D ENG X ing2cheng, J IN
 20054 40 4 Chin J O torhinolaryngol Head Neck Surg, Ap ril 2005, Vol 40, No1 4 295 2228, 1992 2004 2228 (2072, 156) 2072,4, 011%, 011% ; 55, 216% 156, 8, 3,5 9515% ( 64 /67), Kap lan2meier59810%60 1, 510010%
20054 40 4 Chin J O torhinolaryngol Head Neck Surg, Ap ril 2005, Vol 40, No1 4 295 2228, 1992 2004 2228 (2072, 156) 2072,4, 011%, 011% ; 55, 216% 156, 8, 3,5 9515% ( 64 /67), Kap lan2meier59810%60 1, 510010%
Thyroid Neoplasm. ORL-Head and neck Surgery 2014
 In The Name of God Thyroid Neoplasm ORL-Head and neck Surgery 2014 Malignant Neoplasm By age 90, virtually everyone has nodules Estimates of cancer prevalence at autopsy 4% to 36% Why these lesions are
In The Name of God Thyroid Neoplasm ORL-Head and neck Surgery 2014 Malignant Neoplasm By age 90, virtually everyone has nodules Estimates of cancer prevalence at autopsy 4% to 36% Why these lesions are
Risk factors for postoperative haemorrhage after total thyroidectomy: clinical results based on 2,678 patients
 www.nature.com/scientificreports OPEN Received: 2 February 2017 Accepted: 28 June 2017 Published online: 1 August 2017 Risk factors for postoperative haemorrhage after total thyroidectomy: clinical results
www.nature.com/scientificreports OPEN Received: 2 February 2017 Accepted: 28 June 2017 Published online: 1 August 2017 Risk factors for postoperative haemorrhage after total thyroidectomy: clinical results
Ultrasound-Guided Transcutaneous Needle Biopsy of the Base of the Tongue and Floor of the Mouth From a Submental Approach
 TECHNICAL INNOVATION Ultrasound-Guided Transcutaneous Needle Biopsy of the Base of the Tongue and Floor of the Mouth From a Submental Approach Jason M. Wagner, MD, Rachel D. Conrad, MD, Trinitia Y. Cannon,
TECHNICAL INNOVATION Ultrasound-Guided Transcutaneous Needle Biopsy of the Base of the Tongue and Floor of the Mouth From a Submental Approach Jason M. Wagner, MD, Rachel D. Conrad, MD, Trinitia Y. Cannon,
ELIZABETH CEDARS DR. KOREY HOOD Available September 29
 ELIZABETH CEDARS DR. KOREY HOOD Available September 29 Title and Investigators Optimizing Surgical Management of Thyroid Cancer: Using Surgeon-performed Ultrasound to Predict Extrathyroidal Extension of
ELIZABETH CEDARS DR. KOREY HOOD Available September 29 Title and Investigators Optimizing Surgical Management of Thyroid Cancer: Using Surgeon-performed Ultrasound to Predict Extrathyroidal Extension of
CAP Cancer Protocol and ecc Summary of Changes for August 2014 Thyroid Agile Release
 CAP Cancer Protocol and ecc Summary of Changes for August 2014 Thyroid Agile Release 2 REVISION HISTORY Date Author / Editor Comments 5/19/2014 Jaleh Mirza Created the document 8/12/2014 Samantha Spencer/Jaleh
CAP Cancer Protocol and ecc Summary of Changes for August 2014 Thyroid Agile Release 2 REVISION HISTORY Date Author / Editor Comments 5/19/2014 Jaleh Mirza Created the document 8/12/2014 Samantha Spencer/Jaleh
American Head and Neck Society - Journal Club Volume 22, July 2018
 - Table of Contents click the page number to go to the summary and full article link. Location and Causation of Residual Lymph Node Metastasis After Surgical Treatment of Regionally Advanced Differentiated
- Table of Contents click the page number to go to the summary and full article link. Location and Causation of Residual Lymph Node Metastasis After Surgical Treatment of Regionally Advanced Differentiated
Department of Surgery, Eulji University College of Medicine, Seoul, Republic of Korea 2
 Journal of Oncology Volume 2012, Article ID 734541, 9 pages doi:10.1155/2012/734541 Clinical Study Robotic versus Endoscopic Thyroidectomy for Thyroid Cancers: A Multi-Institutional Analysis of Early Postoperative
Journal of Oncology Volume 2012, Article ID 734541, 9 pages doi:10.1155/2012/734541 Clinical Study Robotic versus Endoscopic Thyroidectomy for Thyroid Cancers: A Multi-Institutional Analysis of Early Postoperative
40 TH EUROPEAN CONGRESS 0F CYTOLOGY LIVERPOOL, UK October 2-5, 2016
 Outcomes from the diagnostic approach of thyroid lesions using US-FNA and LBC in clinical practice Emmanouel Mastorakis MD PhD Cytopathologist Director in Cytopathology Laboratory Regional General Hospital
Outcomes from the diagnostic approach of thyroid lesions using US-FNA and LBC in clinical practice Emmanouel Mastorakis MD PhD Cytopathologist Director in Cytopathology Laboratory Regional General Hospital
Controversies in management of squamous esophageal cancer
 2015.06.12 12.47.48 Page 4(1) IS-1 Controversies in management of squamous esophageal cancer C S Pramesh Thoracic Surgery, Department of Surgical Oncology, Tata Memorial Centre, India In Asia, squamous
2015.06.12 12.47.48 Page 4(1) IS-1 Controversies in management of squamous esophageal cancer C S Pramesh Thoracic Surgery, Department of Surgical Oncology, Tata Memorial Centre, India In Asia, squamous
Parathyroid Imaging: Current Concepts. Maria Gule-Monroe, M.D. Nancy Perrier, M.D.
 Parathyroid Imaging: Current Concepts Maria Gule-Monroe, M.D. Nancy Perrier, M.D. Disclosures None Objectives Ultrasound characteristics of parathyroid adenomas vs. lymph nodes 4D-CT evaluation of hyperparathyroidism
Parathyroid Imaging: Current Concepts Maria Gule-Monroe, M.D. Nancy Perrier, M.D. Disclosures None Objectives Ultrasound characteristics of parathyroid adenomas vs. lymph nodes 4D-CT evaluation of hyperparathyroidism
T1/T2 LARYNX CANCER. Click to edit Master Presentation Date. Thomas J Gernon, MD Otolaryngology-Head and Neck Surgery
 ADVANCES IN TREATMENT OF T1/T2 LARYNX CANCER Click to edit Master Presentation Date Thomas J Gernon, MD Otolaryngology-Head and Neck Surgery I have nothing to disclose CHANGING TRENDS IN HNSCC GLOTTIC
ADVANCES IN TREATMENT OF T1/T2 LARYNX CANCER Click to edit Master Presentation Date Thomas J Gernon, MD Otolaryngology-Head and Neck Surgery I have nothing to disclose CHANGING TRENDS IN HNSCC GLOTTIC
Specialist Referral Service Willows Information Sheets. Laryngeal paralysis
 Specialist Referral Service Willows Information Sheets Laryngeal paralysis Laryngeal paralysis tends to affect middle aged and older animals, especially large breed dogs such as Labrador Retrievers, Golden
Specialist Referral Service Willows Information Sheets Laryngeal paralysis Laryngeal paralysis tends to affect middle aged and older animals, especially large breed dogs such as Labrador Retrievers, Golden
The right middle lobe is the smallest lobe in the lung, and
 ORIGINAL ARTICLE The Impact of Superior Mediastinal Lymph Node Metastases on Prognosis in Non-small Cell Lung Cancer Located in the Right Middle Lobe Yukinori Sakao, MD, PhD,* Sakae Okumura, MD,* Mun Mingyon,
ORIGINAL ARTICLE The Impact of Superior Mediastinal Lymph Node Metastases on Prognosis in Non-small Cell Lung Cancer Located in the Right Middle Lobe Yukinori Sakao, MD, PhD,* Sakae Okumura, MD,* Mun Mingyon,
Operative bed recurrence of thyroid cancer: utility of a preoperative needle localization technique
 Original Article Operative bed recurrence of thyroid cancer: utility of a preoperative needle localization technique Oliver S. Eng 1, Scott B. Grant 2, Jason Weissler 3, Mitchell Simon 4, Sudipta Roychowdhury
Original Article Operative bed recurrence of thyroid cancer: utility of a preoperative needle localization technique Oliver S. Eng 1, Scott B. Grant 2, Jason Weissler 3, Mitchell Simon 4, Sudipta Roychowdhury
Laryngeal electromyography findings of vocal fold immobility in patients after radiotherapy for nasopharyngeal carcinoma
 ORIGINAL ARTICLE Laryngeal electromyography findings of vocal fold immobility in patients after radiotherapy for nasopharyngeal carcinoma Yi-Ling Hsieh, MD, 1 Ming-Hong Chang, MD, 2 Chen-Chi Wang, MD 1,3,4*
ORIGINAL ARTICLE Laryngeal electromyography findings of vocal fold immobility in patients after radiotherapy for nasopharyngeal carcinoma Yi-Ling Hsieh, MD, 1 Ming-Hong Chang, MD, 2 Chen-Chi Wang, MD 1,3,4*
Causes of recurrent laryngeal nerve paralysis
 Auris Nasus Larynx 29 (2002) 41 45 www.elsevier.com/locate/anl Causes of recurrent laryngeal nerve paralysis Eiji Yumoto a, *, Ryosei Minoda a, Masamitsu Hyodo b, Takahiko Yamagata b a Department of Otolaryngology-Head
Auris Nasus Larynx 29 (2002) 41 45 www.elsevier.com/locate/anl Causes of recurrent laryngeal nerve paralysis Eiji Yumoto a, *, Ryosei Minoda a, Masamitsu Hyodo b, Takahiko Yamagata b a Department of Otolaryngology-Head
Papillary Thyroid Microcarcinoma Presenting as Horner s Syndrome: A Novel Clinical Presentation
 Case Report American Journal of Cancer Case Reports http://ivyunion.org/index.php/ajccr/ Page 1 of 6 Papillary Thyroid Microcarcinoma Presenting as Horner s Syndrome: A Novel Clinical Presentation Ammara
Case Report American Journal of Cancer Case Reports http://ivyunion.org/index.php/ajccr/ Page 1 of 6 Papillary Thyroid Microcarcinoma Presenting as Horner s Syndrome: A Novel Clinical Presentation Ammara
Prognostic value of the 8 th tumor-node-metastasis classification for follicular carcinoma and poorly differentiated carcinoma of the thyroid in Japan
 2018, 65 (6), 621-627 ORIGINAL Prognostic value of the 8 th tumor-node-metastasis classification for follicular carcinoma and poorly differentiated carcinoma of the thyroid in Japan Yasuhiro Ito 1), Akira
2018, 65 (6), 621-627 ORIGINAL Prognostic value of the 8 th tumor-node-metastasis classification for follicular carcinoma and poorly differentiated carcinoma of the thyroid in Japan Yasuhiro Ito 1), Akira
Karoline Nowillo, MD. February 1, 2008
 Case Presentation Karoline Nowillo, MD SUNY Downstate t February 1, 2008 Case Presentation Chief complaint enlarging goiter x 8 months History of present illness shortness of breath, heaviness in chest
Case Presentation Karoline Nowillo, MD SUNY Downstate t February 1, 2008 Case Presentation Chief complaint enlarging goiter x 8 months History of present illness shortness of breath, heaviness in chest
Volume 2 Issue ISSN
 Volume 2 Issue 3 2012 ISSN 2250-0359 Correlation of fine needle aspiration and final histopathology in thyroid disease: a series of 702 patients managed in an endocrine surgical unit *Chandrasekaran Maharajan
Volume 2 Issue 3 2012 ISSN 2250-0359 Correlation of fine needle aspiration and final histopathology in thyroid disease: a series of 702 patients managed in an endocrine surgical unit *Chandrasekaran Maharajan
 To the Patient and Family This booklet has been written for people who have received a diagnosis of thyroid cancer or who are being tested for this illness. If you have questions that are not answered
To the Patient and Family This booklet has been written for people who have received a diagnosis of thyroid cancer or who are being tested for this illness. If you have questions that are not answered
Clinical Study Comparison of Conventional Open Thyroidectomy and Endoscopic Thyroidectomy via Breast Approach for Papillary Thyroid Carcinoma
 International Endocrinology Volume 2015, Article ID 239610, 5 pages http://dx.doi.org/10.1155/2015/239610 Clinical Study Comparison of Conventional Open Thyroidectomy and Endoscopic Thyroidectomy via Breast
International Endocrinology Volume 2015, Article ID 239610, 5 pages http://dx.doi.org/10.1155/2015/239610 Clinical Study Comparison of Conventional Open Thyroidectomy and Endoscopic Thyroidectomy via Breast
ORIGINAL ARTICLE. Incidental Parathyroidectomy During Thyroid Surgery Does Not Cause Transient Symptomatic Hypocalcemia
 ORIGINAL ARTICLE Incidental Parathyroidectomy During Thyroid Surgery Does Not Cause Transient Symptomatic Hypocalcemia Aaron R. Sasson, MD; James F. Pingpank, Jr, MD; R. Wesley Wetherington, MD; Alexandra
ORIGINAL ARTICLE Incidental Parathyroidectomy During Thyroid Surgery Does Not Cause Transient Symptomatic Hypocalcemia Aaron R. Sasson, MD; James F. Pingpank, Jr, MD; R. Wesley Wetherington, MD; Alexandra
Thyroid Gland. Protocol applies to all malignant tumors of the thyroid gland, except lymphomas.
 Thyroid Gland Protocol applies to all malignant tumors of the thyroid gland, except lymphomas. Procedures Cytology (No Accompanying Checklist) Partial Thyroidectomy Total Thyroidectomy With/Without Lymph
Thyroid Gland Protocol applies to all malignant tumors of the thyroid gland, except lymphomas. Procedures Cytology (No Accompanying Checklist) Partial Thyroidectomy Total Thyroidectomy With/Without Lymph
Intermittent intraoperative nerve monitoring in thyroid reoperations: Preliminary results of a randomized, single-surgeon study
 ORIGINAL ARTICLE Intermittent intraoperative nerve monitoring in thyroid reoperations: Preliminary results of a randomized, single-surgeon study Hu Hei, MD, 1 Bin Zhou, MD, 1 Jianwu Qin, MD, 1 Yongping
ORIGINAL ARTICLE Intermittent intraoperative nerve monitoring in thyroid reoperations: Preliminary results of a randomized, single-surgeon study Hu Hei, MD, 1 Bin Zhou, MD, 1 Jianwu Qin, MD, 1 Yongping
Gerard M. Doherty, MD
 Surgical Management of Differentiated Thyroid Cancer: Update on 2015 ATA Guidelines Gerard M. Doherty, MD Chair of Surgery Utley Professor of Surgery and Medicine Boston University Surgeon-in-Chief Boston
Surgical Management of Differentiated Thyroid Cancer: Update on 2015 ATA Guidelines Gerard M. Doherty, MD Chair of Surgery Utley Professor of Surgery and Medicine Boston University Surgeon-in-Chief Boston
Sternotomy in Thyroid Carcinoma: Experience of Loma Linda University Medical Center
 Sternotomy in Thyroid Carcinoma: Experience of Loma Linda University Medical Center Benjamin Bradford 1, Pedro A De Andrade Filho 1, Alfred Simental 1, Hannah Copeland 2, Allen Murga 2, Tracy Bailey 2,
Sternotomy in Thyroid Carcinoma: Experience of Loma Linda University Medical Center Benjamin Bradford 1, Pedro A De Andrade Filho 1, Alfred Simental 1, Hannah Copeland 2, Allen Murga 2, Tracy Bailey 2,
Introduction. Materials and methods Y-N XU 1,2, J-D WANG 1,2
 1 di 5 11/04/2016 17:54 G Chir Vol. 31 - n. 5 - pp. 205-209 Maggio 2010 Y-N XU 1,2, J-D WANG 1,2 Introduction The World Health Organization (WHO) defined papillary thyroid microcarcinomas (PTMC) as tumors
1 di 5 11/04/2016 17:54 G Chir Vol. 31 - n. 5 - pp. 205-209 Maggio 2010 Y-N XU 1,2, J-D WANG 1,2 Introduction The World Health Organization (WHO) defined papillary thyroid microcarcinomas (PTMC) as tumors
Compartmentalization of the larynx Sites and subsites Supraglottis Glottis subglottis Spaces Pre-epiglottic epiglottic space Para-glottic space
 Stroboscopy Rounds February 8, 2008 C. Matt Stewart, M.D.,Ph.D. Compartmentalization of the larynx Sites and subsites Supraglottis Glottis subglottis Spaces Pre-epiglottic epiglottic space Para-glottic
Stroboscopy Rounds February 8, 2008 C. Matt Stewart, M.D.,Ph.D. Compartmentalization of the larynx Sites and subsites Supraglottis Glottis subglottis Spaces Pre-epiglottic epiglottic space Para-glottic
Research Article A Study on Central Lymph Node Metastasis in 543 cn0 Papillary Thyroid Carcinoma Patients
 International Endocrinology Volume 2016, Article ID 1878194, 5 pages http://dx.doi.org/10.1155/2016/1878194 Research Article A Study on Central Lymph Node Metastasis in 543 cn0 Papillary Thyroid Carcinoma
International Endocrinology Volume 2016, Article ID 1878194, 5 pages http://dx.doi.org/10.1155/2016/1878194 Research Article A Study on Central Lymph Node Metastasis in 543 cn0 Papillary Thyroid Carcinoma
Management of Recurrent Thyroid Cancer
 Management of Recurrent Thyroid Cancer Eric Genden, MD, MHA Isidore Professor and Chairman Department of Otolaryngology- Head and Neck Surgery Senior Associate Dean for Clinical Affairs The Icahn School
Management of Recurrent Thyroid Cancer Eric Genden, MD, MHA Isidore Professor and Chairman Department of Otolaryngology- Head and Neck Surgery Senior Associate Dean for Clinical Affairs The Icahn School
Department of Otolaryngology, Kurume University School of Medicine, Kurume, Japan
 THE KURUME MEDICAL JOURNAL Vol. 16, No. 3, 1969 PATHOLOGICAL STUDIES RELATING TO NEOPLASMS OF THE HYPOPHARYNX AND THE CERVICAL ESOPHAGUS IKUICHIRO HIROTO, YASUSHI NOMURA, KUSUO SUEYOSHI, SHIGENOBU MITSUHASHI,
THE KURUME MEDICAL JOURNAL Vol. 16, No. 3, 1969 PATHOLOGICAL STUDIES RELATING TO NEOPLASMS OF THE HYPOPHARYNX AND THE CERVICAL ESOPHAGUS IKUICHIRO HIROTO, YASUSHI NOMURA, KUSUO SUEYOSHI, SHIGENOBU MITSUHASHI,
A Clicking Larynx: Diagnostic and Therapeutic Challenges
 The Laryngoscope VC 2017 The American Laryngological, Rhinological and Otological Society, Inc. Case Report A Clicking Larynx: Diagnostic and Therapeutic Challenges Derrek A. Heuveling, MD, PhD ; Maarten
The Laryngoscope VC 2017 The American Laryngological, Rhinological and Otological Society, Inc. Case Report A Clicking Larynx: Diagnostic and Therapeutic Challenges Derrek A. Heuveling, MD, PhD ; Maarten
Thyroid Surgery: Lobectomy, total thyroidectomy, LN biopsies or only watchful waiting?
 Thyroid Surgery: Lobectomy, total thyroidectomy, LN biopsies or only watchful waiting? Jacob Moalem, MD, FACS Associate Professor Endocrine Surgery and Endocrinology URMC Agenda 1. When is lobectomy alone
Thyroid Surgery: Lobectomy, total thyroidectomy, LN biopsies or only watchful waiting? Jacob Moalem, MD, FACS Associate Professor Endocrine Surgery and Endocrinology URMC Agenda 1. When is lobectomy alone
Study of validity of ultrasonographic diagnosis in relation to Fine Needle Aspiration Cytology (FNAC) diagnosis
 diagnosis") Original article: Study of validity of ultrasonographic diagnosis in relation to Fine Needle Aspiration Cytology (FNAC) diagnosis *Dr Rajvi Matalia, ** Dr Y.P.Sachdev, ***Dr D.S.Kulkarni *Junior Resident,
Original article: Study of validity of ultrasonographic diagnosis in relation to Fine Needle Aspiration Cytology (FNAC) diagnosis *Dr Rajvi Matalia, ** Dr Y.P.Sachdev, ***Dr D.S.Kulkarni *Junior Resident,
Evaluation of thyroid isthmusectomy as a potential treatment for papillary thyroid carcinoma limited to the isthmus: A clinical study of 73 patients
 ORIGINAL ARTICLE Evaluation of thyroid isthmusectomy as a potential treatment for papillary thyroid carcinoma limited to the isthmus: A clinical study of 73 patients Jianbiao Wang, MM, 1 Haili Sun, BM,
ORIGINAL ARTICLE Evaluation of thyroid isthmusectomy as a potential treatment for papillary thyroid carcinoma limited to the isthmus: A clinical study of 73 patients Jianbiao Wang, MM, 1 Haili Sun, BM,
Management guideline for patients with differentiated thyroid cancer. Teeraporn Ratanaanekchai ENT, KKU 17 October 2007
 Management guideline for patients with differentiated thyroid Teeraporn Ratanaanekchai ENT, KKU 17 October 2007 Incidence (Srinagarind Hospital, 2005, both sex) Site (all) cases % 1. Liver 1178 27 2. Lung
Management guideline for patients with differentiated thyroid Teeraporn Ratanaanekchai ENT, KKU 17 October 2007 Incidence (Srinagarind Hospital, 2005, both sex) Site (all) cases % 1. Liver 1178 27 2. Lung
Contents. Part A Clinical Evaluation of Laryngeal Disorders. 3 Videostroboscopy and Dynamic Voice Evaluation with Flexible Laryngoscopy...
 Contents Part A Clinical Evaluation of Laryngeal Disorders 1 Anatomy and Physiology of the Larynx....... 3 1.1 Anatomy.................................. 3 1.1.1 Laryngeal Cartilages........................
Contents Part A Clinical Evaluation of Laryngeal Disorders 1 Anatomy and Physiology of the Larynx....... 3 1.1 Anatomy.................................. 3 1.1.1 Laryngeal Cartilages........................
LESSON ASSIGNMENT. After completing this lesson, you should be able to:
 LESSON ASSIGNMENT LESSON 3 Cricothyroidotomy LESSON ASSIGNMENT Paragraphs 3-1 through 3-7. LESSON OBJECTIVES After completing this lesson, you should be able to: 3-1. Define cricothyroidotomy. 3-2. Identify
LESSON ASSIGNMENT LESSON 3 Cricothyroidotomy LESSON ASSIGNMENT Paragraphs 3-1 through 3-7. LESSON OBJECTIVES After completing this lesson, you should be able to: 3-1. Define cricothyroidotomy. 3-2. Identify
Treatment for Supraglottic Ca History: : Total Laryngectomy y was routine until early 50 s, when XRT was developed Ogura and Som developed the one-sta
 Role of Laser Therapy in Laryngeal Cancer Khalid Hussain AL-Qahtani MD,MSc,FRCS(c) MSc Assistant Professor Consultant of Otolaryngology Advance Head & Neck Oncology, Thyroid & Parathyroid,Microvascular
Role of Laser Therapy in Laryngeal Cancer Khalid Hussain AL-Qahtani MD,MSc,FRCS(c) MSc Assistant Professor Consultant of Otolaryngology Advance Head & Neck Oncology, Thyroid & Parathyroid,Microvascular
Endoscopic Posterior Cricoid Split with Costal Cartilage Graft: A Fifteen Year Experience
 1 Endoscopic Posterior Cricoid Split with Costal Cartilage Graft: A Fifteen Year Experience John P. Dahl, MD, PhD, MBA 1,2, *, Patricia L. Purcell, MD 1, MPH, Sanjay R. Parikh, MD, FACS 1, and Andrew F.
1 Endoscopic Posterior Cricoid Split with Costal Cartilage Graft: A Fifteen Year Experience John P. Dahl, MD, PhD, MBA 1,2, *, Patricia L. Purcell, MD 1, MPH, Sanjay R. Parikh, MD, FACS 1, and Andrew F.
Nonrecurrent inferior laryngeal nerves and anatomical findings during thyroid surgery: report of three cases
 Kato et al. Surgical Case Reports (2016) 2:44 DOI 10.1186/s40792-016-0170-5 CASE REPORT Nonrecurrent inferior laryngeal nerves and anatomical findings during thyroid surgery: report of three cases Kumiko
Kato et al. Surgical Case Reports (2016) 2:44 DOI 10.1186/s40792-016-0170-5 CASE REPORT Nonrecurrent inferior laryngeal nerves and anatomical findings during thyroid surgery: report of three cases Kumiko
Thyroid Nodule. Disclosure. Learning Objectives P A P A P A 3/18/2014. Nothing to disclose.
 Thyroid Nodule Evaluating the patient with a thyroid nodule and some management options. Miguel V. Valdez PA C Disclosure Nothing to disclose. Learning Objectives Examination of thyroid gland Options for
Thyroid Nodule Evaluating the patient with a thyroid nodule and some management options. Miguel V. Valdez PA C Disclosure Nothing to disclose. Learning Objectives Examination of thyroid gland Options for
Citation Auris, nasus, larynx (2011), 38(3):
, 38(3):") TitleManagement of metastasis to the thy Author(s) Ishikawa, Masaaki; Hirano, Shigeru; Citation Auris, nasus, larynx (2011), 38(3): Issue Date 2011-06 URL http://hdl.handle.net/2433/139807 Right 2010 Elsevier
TitleManagement of metastasis to the thy Author(s) Ishikawa, Masaaki; Hirano, Shigeru; Citation Auris, nasus, larynx (2011), 38(3): Issue Date 2011-06 URL http://hdl.handle.net/2433/139807 Right 2010 Elsevier
An Unexpected Cause of Hypoglycemia
 An Unexpected Cause of Hypoglycemia Stacey A. Milan, MD FACS Surgical Oncology Nothing to disclose Disclosures Objectives Identify indications for workup of hypoglycemia Define work up for hypoglycemic
An Unexpected Cause of Hypoglycemia Stacey A. Milan, MD FACS Surgical Oncology Nothing to disclose Disclosures Objectives Identify indications for workup of hypoglycemia Define work up for hypoglycemic
FLEXIBLE FIBREOPTIC LARYNGOSCOPY VERSUS SIMPLE VOICE ASSESSMENT IN A ROUTINE CLINICAL SETTING TO PREDICT VOCAL CORD PARALYSIS AFTER THYROID SURGERY
 ISSN: 2250-0359 VOLUME 4 ISSUE 3 2014 FLEXIBLE FIBREOPTIC LARYNGOSCOPY VERSUS SIMPLE VOICE ASSESSMENT IN A ROUTINE CLINICAL SETTING TO PREDICT VOCAL CORD PARALYSIS AFTER THYROID SURGERY Sah BP, Bhandary
ISSN: 2250-0359 VOLUME 4 ISSUE 3 2014 FLEXIBLE FIBREOPTIC LARYNGOSCOPY VERSUS SIMPLE VOICE ASSESSMENT IN A ROUTINE CLINICAL SETTING TO PREDICT VOCAL CORD PARALYSIS AFTER THYROID SURGERY Sah BP, Bhandary
Biomedical Research 2017; 28 (21): ISSN X
: ISSN X") Biomedical Research 2017; 28 (21): 9497-9501 ISSN 0970-938X www.biomedres.info Analysis of relevant risk factor and recurrence prediction model construction of thyroid cancer after surgery. Shuai Lin 1#,
Biomedical Research 2017; 28 (21): 9497-9501 ISSN 0970-938X www.biomedres.info Analysis of relevant risk factor and recurrence prediction model construction of thyroid cancer after surgery. Shuai Lin 1#,
Current Issues in Thyroid Cancer Surgery in 2017
 Current Issues in Thyroid Cancer Surgery in 2017 Dr. David Goldstein MD Msc FRCSC FACS Associate Professor, Department Otolaryngology Head & Neck Surgery, U of T Department of Surgical Oncology, Princess
Current Issues in Thyroid Cancer Surgery in 2017 Dr. David Goldstein MD Msc FRCSC FACS Associate Professor, Department Otolaryngology Head & Neck Surgery, U of T Department of Surgical Oncology, Princess
Work Up & Evaluation of Thyroid Nodules In 2013: State of The Art
 Work Up & Evaluation of Thyroid Nodules In 2013: State of The Art BC Surgical Oncology Network, Fall Update Todd McMullen MD PhD FRCSC FACS Endocrine Surgeon Divisions of General Surgery and Oncology Director,
Work Up & Evaluation of Thyroid Nodules In 2013: State of The Art BC Surgical Oncology Network, Fall Update Todd McMullen MD PhD FRCSC FACS Endocrine Surgeon Divisions of General Surgery and Oncology Director,