Thyroid Disease: Cameron Ch: Mark Keldahl M.D. Surgery Resident Conference 2/27/08
|
|
|
- Timothy Miller
- 5 years ago
- Views:
Transcription
1 Thyroid Disease: Cameron Ch: Mark Keldahl M.D. Surgery Resident Conference 2/27/08
2 THYROID NODULE
3 Thyroid Nodule United States Prevalence 2-4% History (Malignacy RF) Age (>40) Male gender h/o radiation +FH (MEN 2 A/B) Gardner s, Cowden dz Exam (Malignancy RF) # nodules size Irregular shape Firm Immobile
4 Thyroid Nodule Diagnostic Evaluation FNA GOLD STANDARD U/S Microcalcifications Intranodular vascular markings Irregular bordes Cytology 1948, cytopathologic, not histopathologic NO info re vascular or lymphatic invasion TFT s Majority of patients are euthyroid Thyroid radioisotope scan
5 Thyroid Nodule FNA results Benign (70%) Adenomatoid or hyperplastic Hashimotos Colloid cyst Malignant (5%) Papillary Medullary Anaplastic Lymphoma metastatic Suspicious (10%) follicular neoplasm Hurthle Suspicious for papillary or follicular variant of papillary CA Non diagnostic or Inadequate (15%)
6 Thyroid Nodule Benign: Follow clinically, watch for size, re FNA Approx. 1% convert to malignancy Role of thyroid hormone therapy Malignant Surgery Suspicious Lobectomy w isthmusectomy Total thyroidectomy if clinical suspicion Inadequate
7 NONTOXIC GOITER
8 Nontoxic Goiter Any benign enlargement of the thyroid Etiology: Worldwide endemic #1: Iodine deficiency 12% of world U.S. : non-endemic 3-4% of population Radiation Environmental goitrogens Dyshormonogenesis Thyroid growth factors Most common type: Multinodular goiter Female > M Nodules outgrow blood supply, necrosis, fibrosis
9 Goiter Diagnosis: Painless enlargement Less common: pressure, phlegm, dysphagia, pain radiate to ear, voice change Rare: dyspnea, orthopnea, hoarseness, stridor Rapid growth, firm: suspicious for CA Non OP TX Suppressive therapy Not for functioning nodules Radioactive Iodine Dependent on functioning thyroid tissue Some say suboptimal for multinodular goiter Good for poor surgical candidates
10 Goiter Evaluation Thyroid function tests Majority euthyroid If hyper/hypo: check thyroidantibodies FNA 70% are benign (1% false neg rate) 4% malignant (1% false + rate) 20% indeterminant U/S Solid vs cystic CXR, CT, MRI Radioactive iodine scan Hot: 99% benign Cold: 20% malignant
11 Goiter: Operative Indications Symptomatic: airway, esophagus, SVC Enlargement despite non op RX BX proven or suspicious for malignancy Tracheal deviation or compression on imaging Substernal goiter Cosmetic deformity/patient preference
12 Goiter: Operative options Lobectomy & isthmusectomy Near total thyroidectomy Leave approx 5 g tissue Bilateral subtotal High recurrence Avoid thyroid supplement
13 THYROID CANCER
14 Thyroid Cancer 1.5% of all CA in U.S. 95% of all endocrine CA in U.S. 74% are in women 90% are differentiated type favorable prognosis <10% of thyroid nodules are malignant
15 Presentation of Thyroid CA Most asymptomatic with thyroid nodule Less common Hoarseness Dysphagia Dyspnea Cough Choking spells Cervical lymphadenopathy
16 Physical Exam Fixed or mobile Other nodules? Hoarseness Laryngoscopy cord paralysiis FNA
17 Thyroid Nodule - FNA Benign: Follow clinically, watch for size, re FNA Approx. 1% convert to malignancy Role of thyroid hormone therapy Malignant Surgery Suspicious Lobectomy w isthmusectomy Total thyroidectomy if clinical suspicion Inadequate
18 Classification of Thyroid CA Tumors of follicular cell origin Differentiated Papillary 75% Follicular 10% Hurthle Cell 5% Undifferentiated Anaplastic 5% Parafollicular or C-cell origin Medullary 5% Other Lymphoma <1%
19 Papillary CA Most common malignant thyroid tumor Types: Pure papillary Follicular Tall-cell Columnar cell Oxyphylic Difuse sclerosinig Encapsulated histologic variants 90% of radiation induced thyroid CA
20 Histology Psammoma bodies Intranuclear grooves Cytoplasmic inclusions Multicentric 30-50% Lymphatic Spread Lung and bone common mets
21 Operation some debate Lobectomy w isthmusectomy <1 cm size No systemic or lymphatic mets Low risk for recurrence Recurrence 5% Death rate 0.1% Benefits risk recurrent laryngeal N injury risk hypoparathyroidism <5% of recurrences occur in thyroid bed >50% recurrences can be treated surgically
22 Operations Total thyroidectomy risk of local and regional recurrence Post op radioiodine (131) remnant ablation, improved survival 6-8 wks post op: radioiodine body scan If <1% uptake, ok Otherwise need full radioactive iodine inpatient treatment dose for remnant ablation Eliminates 1% anaplastic transformation
23 Lymph node dissection Papillary CA Prophylactic LN dissection not warranted 30-40% incidence of cervical LN mets Remove enlarged LN n central or lateral neck Frozen section If frozen positive in: Central: central neck dissection Between carotids, hyoid, brachiocephalic vessels Lateral: ipsilateral modified radical neck Anterior and posterolateral to IJV Mastoid superiorly to subclavian vessels inferior Laterally to spinal accessory N (neck levels 2-5)
24 Follicular CA 10% of all thyroid CA 3:1 female 50 years mean age Multicentric and LN mets less common than papillary 10% have spread to LN FNA not able to differentiate adenoma from carcinoma Spread HEMATOGENOUSLY Lung and bone most common
25 Operation Follicular neoplasm on FNA Lobectomy w isthmusectomy Intra-operative Frozen section Convert to total thyroidectomy if capsular or vascular invasion Otherwise wait for permanent If carcinoma, take back for Total thyroidectomy Post op Radioactive iodine RX
26 Hurthle Cell Cancer Similar clinicopathologic pathway as Follicular However <10% take up radioactive iodine >tendency to spread to cervical LN incidence of distant mets
27 Post operative Thyroid replacement, TSH Post op radioiodine RX If>1% uptake on body scan Check TSH post op, >30 ideal Papillary CA >1.5cm +LN mets Invasive follicular/hurthle cell carcinoma 30mCi I 131 for low risk 100mCi I 131 for higher risk Role of synthetic scan (avoid stopping thyroid) Thyroglobulin (glycoprotein) Monitor serum for recurrence If, rule out thyroglobulin antibodies (cause of f+) Follow up whole body scans
28 Medullary Thyroid Cancer (MTC) Malignant transformation of neuroectodermally derived parafollicular cells 5% of thyroid CA 25% hereditary FNA Immunostaining for calcitonin MEN II Careful pheos RET protooncogene Spread Hematogenous
29 MEN II MEN IIA MTC (100%) calcitonin Pheochromocytoma (33%) Urine/serum metanephrines, MIBG RESECT BEFORE THYROID Parathyroid Hyperplasia (50%) 3.5 gland resection MEN IIB MTC (85%) More aggressive than MEN II A Pheo (50%) Mucosal neuromas (100%)
30 Operation MTC Total thyroidectomy w central node dissection 75% with involved nodes NOT amenable to post op radioiodine Serum calcitonin U/S
31 Anaplastic Carcinoma Rare, 2-4 % of all thyroid CA Rapid expanding mass Elderly Tumor necrosis Common: invasion to adjacent structures FNA 5 year survival: 3% No good RX Surgery, radiotherapy, chemo recurencec survival if complete resection (rare to perform) Surgery for tracheal compression for relief
32 Lymphoma <1% Non-Hodgkins, B cell type Often w Hashimotos thyroiditis Female>Male Painless enlarging neck mass FNA Surgical BX may be required Resection rarely needed Radiation PLUS chemo 5 year survival 50-70% Poor prognosis >10cm, dysphagia, mediastinum involved
33 HYPERTHYROIDISM
34 Hyperthyroidism Excess thyroid hormone Medical treatment Thionamide inhibition Radioiodine ablation Surgical treatment Graves (10% Surgically treated) Toxic multinodular goiter Toxic solitary nodule
35 Hyperthyroidism Symptoms Fatigue Wt loss Diaphoresis Palpitations Heat intolerance Muscle weakness Insomnia Diplopia Inc appetite Dyspnea nervousness Irritability Hair loss Diarrhea Irregular menses Emotional lability
36 Hyperthyroidism Physical Findings Goiter, firm, diffuse Tachycardia Tremor Stare, lid lag Proptosis Exophthalmos Keratitis/conjunctivitis Chemosis Periorbital edema ophthalmoplegia Hyperreflexia Hyperpyrexia Flow murmur Gynecomastia Splenomegaly Thin skin/dermopathy Leg sweling Pretibial edema
37 Hyperthyroidism Potential Complications Thyroid storm Cachexia Psychosis/delirium Arrhythmias CHF Jaundice Osteoporosis Infertility/spontaneous abortion
38 Differential diagnosis Hyperthyroidism Graves Toxic multinodular goiter (plummers dz) Toxic adenoma Metastatic thyroid CA Painful, subacute thyroiditis Silent thyroiditis Iodine induced Ectopic thyroid from struma ovarii Excessive pituitary TSH Pituitary resistance to thyroid hormone Excessive trophoblastic TSH Excess hcg from hydatidiform mole/choriocarcinoma Factitious
39 Advantages of surgery Graves Resolution Robust cure Tissue diagnosis Compliance Concern for radioactivity Pregnancy Youth Salvage Cosmesis Cost Thyroid Storm Amiodarone induced Ophthalmopathy
40 Disadvantages of Surgery Graves Nerve injury Parathyroid compromise Bleeding, infection Hypothyroidism Anesthesia Scar Cost
41 Preoperative preparation Graves Inhibit organification of I & coupling of iodthyronine Propylthiouracil (PTU) Methimazole (Tapazole) Carbimazole BHCG (pregnancy) Calcium (concurrent hyperpara) Wait for Euthyroid (3-4 wks) T3 (triiodothyroxine) T4 (thyroxine) TSH (need not normalize) Beta blockade for symptoms Propranolol also inhibit T4 to T3 Iopanoic Acid Inhibit T4 to T3 Iodine (SSKI or Lugol s) Inhibits release of T4 and T3, wait til euthyroid
42 Operation: Graves Total thyroidectomy Hypothyroid post op Almost no recurrence Bilateral subtotal Recurrence up to 70% Nerve & parathyroid injury Unilateral total and contralateral subtotal Leave about 4 grams of tissue
43 Toxic Multinodular Goiter (TMG) Same medical options as in Graves Thyroxine suppression of TSH not favored Radioiodine Poor surgical candidates Elderly Surgery Mainly role for toxic and hot nodules Same options as in Graves Less chance of recurrence if tissue left
44 Toxic Solitary Nodule (TSN) Most are follicular, <1% carcinoma Debate about suppression Ideal for TSH >1 Thyroid levels must be normal or low FNA: inconclusive treat as CA If continues to grow (>3cm) or becomes worrisome: Lobectomy w Frozen Role of radioiodine Poor surgical candidates Not worried about CA Relapse common, up to 50% Surgery or Radioiodine preferred over inhibition Nodulectomy NOT RECOMMENDED
45 Recurrent Hyperthyroidism Up to 12% nerve injury in re op Lateral approach Strap muscle mobilized away from SCM Early identification of RLN
46 THYROIDITIS
47 Thyroiditis Inflamation of thyroid gland Chronic Lymphocytic (Hashimotos) Subacute Granulomatous (de Quervain s) Subacute lymphocytic (painless/postpartum) Acute supporative (acute bacterial) Invasive fibrous (Riedel s)
48 Chronic Lymphocytic: Hashimotos Most common thyroiditis and hypothyroid in U.S. Associated w other autoimmune disorders RA, SLE, Sjogrens 95% Female Most asymptomatic 5% early thyrotoxicosis Lymphoma risk Diagnosis Diffuse, enlarged, firm Thyroglobulin thyroid microsomal antigen thyrotropin receptor TX: non surgical Surgery for nodules or goiter as discussed previously
49 Subacute Granulomatous: dequervain s Giant cell thyroiditis Painful Antibodies not elevated Viral etiology Hyperthyroid symptoms Most return to euthyroid 6 m ESR, RAIU, T4 and T3, low to no TSH BX rarely needed Beta blocker, levothyroxine 3-6m, NSAIDs, rare use of steroids for thyroid and neck pain
50 Subacute Lymphocytic Thyroiditis Postpartum vs Silent Autoimmune etiology invoked Symptoms similar to dequervain s But pain unusual ESR normal Beta blockers, thyroxine
51 Acute thyroiditis Infectious, bacterial Rare 90% w pyriform sinus fistula (L>R) Prone to repeated infection Pain, tender, fever Staph, Strep ABX fungal/mycobacterium/parasite/aids
52 Invasive Fibrous Thyroidits: Riedel s Rare Unclear etiology Extrathyroidal fibrosis seen F>M Firm, fixed, woody mass Compressive symptoms Biopsy: rule out CA Steroids first, surgery to help symptoms Surgery rarely helps Tamoxifen

53 Thyroid Vascular Anatomy

54 Thyroid Surgery

55 Strap Muscles

56 Thyroid: Lateral dissection

57 Thyroid: Rec. laryngeal N.
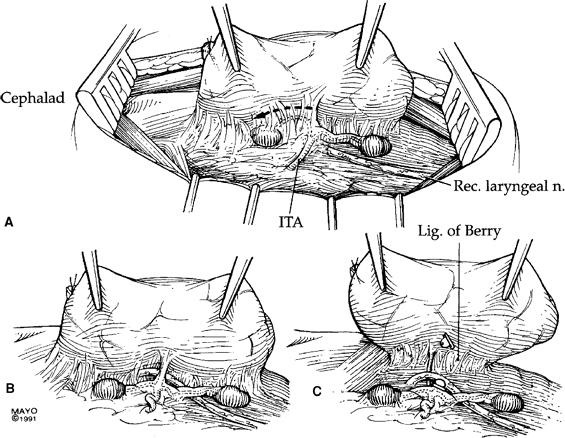
58

59 Superior thyroid Artery

60 Parathyroid Autotransplant
61 THE END
OUTLINE. Regulation of Thyroid Hormone Production Common Tests to Evaluate the Thyroid Hyperthyroidism - Graves disease, toxic nodules, thyroiditis
 THYROID DISEASE OUTLINE Regulation of Thyroid Hormone Production Common Tests to Evaluate the Thyroid Hyperthyroidism - Graves disease, toxic nodules, thyroiditis OUTLINE Hypothyroidism - Hashimoto s thyroiditis,
THYROID DISEASE OUTLINE Regulation of Thyroid Hormone Production Common Tests to Evaluate the Thyroid Hyperthyroidism - Graves disease, toxic nodules, thyroiditis OUTLINE Hypothyroidism - Hashimoto s thyroiditis,
Grave s autoimmune Graves and Hashimotos: antithyroglobulin and antimicrosomal antibodies T3 X 10d should decrease TSH 50%
 Vesalius SCALpel : Thyroid (see also: head and neck folios) Anatomic lingual thyroid most common ectopic location normal thyroid tissue patients may have no thyroid in neck manifest as teenager, may enlarge
Vesalius SCALpel : Thyroid (see also: head and neck folios) Anatomic lingual thyroid most common ectopic location normal thyroid tissue patients may have no thyroid in neck manifest as teenager, may enlarge
Thyroid Nodule. Disclosure. Learning Objectives P A P A P A 3/18/2014. Nothing to disclose.
 Thyroid Nodule Evaluating the patient with a thyroid nodule and some management options. Miguel V. Valdez PA C Disclosure Nothing to disclose. Learning Objectives Examination of thyroid gland Options for
Thyroid Nodule Evaluating the patient with a thyroid nodule and some management options. Miguel V. Valdez PA C Disclosure Nothing to disclose. Learning Objectives Examination of thyroid gland Options for
Diseases of thyroid & parathyroid glands (1 of 2)
") Diseases of thyroid & parathyroid glands (1 of 2) Thyroid diseases Thyrotoxicosis Hypothyroidism Thyroiditis Graves disease Goiters Neoplasms Chronic Lymphocytic (Hashimoto) Thyroiditis Subacute Granulomatous
Diseases of thyroid & parathyroid glands (1 of 2) Thyroid diseases Thyrotoxicosis Hypothyroidism Thyroiditis Graves disease Goiters Neoplasms Chronic Lymphocytic (Hashimoto) Thyroiditis Subacute Granulomatous
- RET/PTC rearrangement: 20% papillary thyroid cancer - RET: medullary thyroid cancer
 Thyroid Cancer UpToDate: Introduction: Risk Factors: Biology: Symptoms: Diagnosis: 1. Lenvina is the first line therapy with powerful durable response and superior PFS in pts with RAI-refractory disease.
Thyroid Cancer UpToDate: Introduction: Risk Factors: Biology: Symptoms: Diagnosis: 1. Lenvina is the first line therapy with powerful durable response and superior PFS in pts with RAI-refractory disease.
THYROID CANCER IN CHILDREN. Humberto Lugo-Vicente MD FACS FAAP Professor Pediatric Surgery UPR School of Medicine
 THYROID CANCER IN CHILDREN Humberto Lugo-Vicente MD FACS FAAP Professor Pediatric Surgery UPR School of Medicine Thyroid nodules Rare Female predominance 4-fold as likely to be malignant Hx Radiation exposure?
THYROID CANCER IN CHILDREN Humberto Lugo-Vicente MD FACS FAAP Professor Pediatric Surgery UPR School of Medicine Thyroid nodules Rare Female predominance 4-fold as likely to be malignant Hx Radiation exposure?
Thyroid nodules. Most thyroid nodules are benign
 Thyroid nodules Postgraduate Course in General Surgery Jessica E. Gosnell MD Assistant Professor March 22, 2011 Most thyroid nodules are benign thyroid nodules occur in 77% of the world s population palpable
Thyroid nodules Postgraduate Course in General Surgery Jessica E. Gosnell MD Assistant Professor March 22, 2011 Most thyroid nodules are benign thyroid nodules occur in 77% of the world s population palpable
Thyroid nodules - medical and surgical management. Endocrinology and Endocrine Surgery Manchester Royal Infirmary
 Thyroid nodules - medical and surgical management JRE Davis NR Parrott Endocrinology and Endocrine Surgery Manchester Royal Infirmary Thyroid nodules - prevalence Thyroid nodules common, increase with
Thyroid nodules - medical and surgical management JRE Davis NR Parrott Endocrinology and Endocrine Surgery Manchester Royal Infirmary Thyroid nodules - prevalence Thyroid nodules common, increase with
Thyroid nodules 3/22/2011. Most thyroid nodules are benign. Thyroid nodules: differential diagnosis
 Most thyroid nodules are benign Thyroid nodules Postgraduate Course in General Surgery thyroid nodules occur in 77% of the world s population palpable thyroid nodules occur in about 5% of women and 1%
Most thyroid nodules are benign Thyroid nodules Postgraduate Course in General Surgery thyroid nodules occur in 77% of the world s population palpable thyroid nodules occur in about 5% of women and 1%
Approach to Thyroid Nodules
 Approach to Thyroid Nodules Alice Y.Y. Cheng, MD, FRCPC Twitter: @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
Approach to Thyroid Nodules Alice Y.Y. Cheng, MD, FRCPC Twitter: @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
Hyperthyroidism Diagnosis and Treatment. April Janet A. Schlechte, M.D.
 Hyperthyroidism Diagnosis and Treatment Family Practice Refresher Course April 2015 Janet A. Schlechte, M.D. Disclosure of Financial Relationships Janet A. Schlechte, M.D. has no relationships with any
Hyperthyroidism Diagnosis and Treatment Family Practice Refresher Course April 2015 Janet A. Schlechte, M.D. Disclosure of Financial Relationships Janet A. Schlechte, M.D. has no relationships with any
5/18/2013. Most thyroid nodules are benign. Thyroid nodules: new techniques in evaluation
 Most thyroid nodules are benign Thyroid nodules: new techniques in evaluation Incidence Etiology Risk factors Diagnosis Gene classification system Treatment Postgraduate Course in General Surgery Jessica
Most thyroid nodules are benign Thyroid nodules: new techniques in evaluation Incidence Etiology Risk factors Diagnosis Gene classification system Treatment Postgraduate Course in General Surgery Jessica
THYROID DISEASE IN CHILDREN
 THYROID DISEASE IN CHILDREN Michelle Schweiger, D.O. Center for Pediatric and Adolescent Endocrinology Cleveland Clinic Foundation Neither I nor any immediate family members have any financial interests
THYROID DISEASE IN CHILDREN Michelle Schweiger, D.O. Center for Pediatric and Adolescent Endocrinology Cleveland Clinic Foundation Neither I nor any immediate family members have any financial interests
Evaluation and Management of Thyroid Nodules. Nick Vernetti, MD, FACE Palm Medical Group Las Vegas, Nevada
 Evaluation and Management of Thyroid Nodules Nick Vernetti, MD, FACE Palm Medical Group Las Vegas, Nevada Disclosure Consulting Amgen Speaking Amgen Objectives Understand the significance of incidental
Evaluation and Management of Thyroid Nodules Nick Vernetti, MD, FACE Palm Medical Group Las Vegas, Nevada Disclosure Consulting Amgen Speaking Amgen Objectives Understand the significance of incidental
42 yr old male with h/o Graves disease and prior I 131 treatment presents with hyperthyroidism and undetectable TSH. 2 hr uptake 20%, 24 hr uptake 50%
 Pinhole images of the neck are acquired in multiple projections, 24hrs after the oral administration of approximately 200 µci of I123. Usually, 24hr uptake value if also calculated (normal 24 hr uptake
Pinhole images of the neck are acquired in multiple projections, 24hrs after the oral administration of approximately 200 µci of I123. Usually, 24hr uptake value if also calculated (normal 24 hr uptake
Toxic MNG Thyroiditis 5-15
 Hyperthyroidism Facts Prevalence 0.5-1.0%, more common in women Thyrotoxicosis is excess thyroid hormones from endogenous or exogenous sources Hyperthyroidism is excess thyroid hormones from thyroid gland
Hyperthyroidism Facts Prevalence 0.5-1.0%, more common in women Thyrotoxicosis is excess thyroid hormones from endogenous or exogenous sources Hyperthyroidism is excess thyroid hormones from thyroid gland
Lectures presented. 3 rd year
 Lectures presented 3 rd year-2016-2017 The metabolic response to trauma Basic concepts: Homeostasis is a mechanism by which the internal environment of the human being is driven constant. It involves a
Lectures presented 3 rd year-2016-2017 The metabolic response to trauma Basic concepts: Homeostasis is a mechanism by which the internal environment of the human being is driven constant. It involves a
Hyperthyroidism, Inflammatory Disorders
 Hyperthyroidism, Inflammatory Disorders free T4 Howard J. Sachs, MD www.12daysinmarch.com Hyperthyroidism, Inflammatory Disorders The total T4 may be elevated in pregnancy and with OCP use Graves I 123
Hyperthyroidism, Inflammatory Disorders free T4 Howard J. Sachs, MD www.12daysinmarch.com Hyperthyroidism, Inflammatory Disorders The total T4 may be elevated in pregnancy and with OCP use Graves I 123
Effect of thyroid hormones of metabolism Thyroid Diseases
 Effect of thyroid hormones of metabolism Thyroid Diseases Medical Perspective Aspects That Will Be Addressed Regulation of thyroid hormone secretion Basic physiology Hyperthyroidism Hypothyroidism Thyroiditis
Effect of thyroid hormones of metabolism Thyroid Diseases Medical Perspective Aspects That Will Be Addressed Regulation of thyroid hormone secretion Basic physiology Hyperthyroidism Hypothyroidism Thyroiditis
John Sutton, DO, FACOI, FACE, CCD. Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989
 John Sutton, DO, FACOI, FACE, CCD Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989 No Disclosures Disease Of the Thyroid Iodide Metabolism/Synthesis of Thyroid Hormone Trap Oxidation Organification(catalyzed
John Sutton, DO, FACOI, FACE, CCD Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989 No Disclosures Disease Of the Thyroid Iodide Metabolism/Synthesis of Thyroid Hormone Trap Oxidation Organification(catalyzed
4/22/2010. Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey.
 Management of Differentiated Thyroid Cancer: Head Neck Surgeon Perspective Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey Thyroid gland Small endocrine gland:
Management of Differentiated Thyroid Cancer: Head Neck Surgeon Perspective Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey Thyroid gland Small endocrine gland:
Management guideline for patients with differentiated thyroid cancer. Teeraporn Ratanaanekchai ENT, KKU 17 October 2007
 Management guideline for patients with differentiated thyroid Teeraporn Ratanaanekchai ENT, KKU 17 October 2007 Incidence (Srinagarind Hospital, 2005, both sex) Site (all) cases % 1. Liver 1178 27 2. Lung
Management guideline for patients with differentiated thyroid Teeraporn Ratanaanekchai ENT, KKU 17 October 2007 Incidence (Srinagarind Hospital, 2005, both sex) Site (all) cases % 1. Liver 1178 27 2. Lung
Thyroid disorders. Dr Enas Abusalim
 Thyroid disorders Dr Enas Abusalim Thyroid physiology The hypothalamic pituitary thyroid axis And peripheral conversion of T4 to T3, WHERE, AND BY WHAT ENZYME?? Only relatively small concentrations of
Thyroid disorders Dr Enas Abusalim Thyroid physiology The hypothalamic pituitary thyroid axis And peripheral conversion of T4 to T3, WHERE, AND BY WHAT ENZYME?? Only relatively small concentrations of
The Thyroid: No mystery. Just need all the pieces to the puzzle.
 The Thyroid: No mystery. Just need all the pieces to the puzzle. Todd Chennell, MS, RN ANP-C Endocrine surgery University of Rochester 2018 1 According to the American Thyroid Association, 12 percent of
The Thyroid: No mystery. Just need all the pieces to the puzzle. Todd Chennell, MS, RN ANP-C Endocrine surgery University of Rochester 2018 1 According to the American Thyroid Association, 12 percent of
CHAPTER-II Thyroid Diseases. by: j. jayasutha lecturer department of Pharmacy practice Srm college of pharmacy srm university
 CHAPTER-II Thyroid Diseases by: j. jayasutha lecturer department of Pharmacy practice Srm college of pharmacy srm university Aspects That Will Be Addressed Hyperthyroidism Hypothyroidism Thyroiditis Hyperthyroidism
CHAPTER-II Thyroid Diseases by: j. jayasutha lecturer department of Pharmacy practice Srm college of pharmacy srm university Aspects That Will Be Addressed Hyperthyroidism Hypothyroidism Thyroiditis Hyperthyroidism
Disclosures. Learning objectives. Case 1A. Autoimmune Thyroid Disease: Medical and Surgical Issues. I have nothing to disclose.
 Disclosures Autoimmune Thyroid Disease: Medical and Surgical Issues I have nothing to disclose. Chrysoula Dosiou, MD, MS Clinical Assistant Professor Division of Endocrinology Stanford University School
Disclosures Autoimmune Thyroid Disease: Medical and Surgical Issues I have nothing to disclose. Chrysoula Dosiou, MD, MS Clinical Assistant Professor Division of Endocrinology Stanford University School
Well-differentiated Thyroid Cancer. Anton Sharapov, R4
 Well-differentiated Thyroid Cancer Anton Sharapov, R4 Outline Types of DTC Diagnosis of DTC Treatment options Extent of surgery Follow up cases A bit of history Theodore Kocher, Bern, Switzerland 1872,
Well-differentiated Thyroid Cancer Anton Sharapov, R4 Outline Types of DTC Diagnosis of DTC Treatment options Extent of surgery Follow up cases A bit of history Theodore Kocher, Bern, Switzerland 1872,
Endocrine system pathology
 Endocrine system pathology Central endocrine system peripheral endocrine system: thyroid gland parathyroid gland pancreas adrenal glands Thyroid gland. the weight of normal thyroid gland is about 15 grams.
Endocrine system pathology Central endocrine system peripheral endocrine system: thyroid gland parathyroid gland pancreas adrenal glands Thyroid gland. the weight of normal thyroid gland is about 15 grams.
PEDIATRIC THYROID MALIGNACY
 PEDIATRIC THYROID MALIGNACY Anthony Sheyn MD Assistant Professor of Otolaryngology Head and Neck Surgery University of Tennessee Health Science Center Thyroid nodules 20 per 1000 children nodules in children
PEDIATRIC THYROID MALIGNACY Anthony Sheyn MD Assistant Professor of Otolaryngology Head and Neck Surgery University of Tennessee Health Science Center Thyroid nodules 20 per 1000 children nodules in children
Women s Health in General Practice Symposium 2015 Thyroid & Parathyroid Cases
 Women s Health in General Practice Symposium 2015 Thyroid & Parathyroid Cases Bill Fleming Epworth Freemasons Hospital 1 Common Endocrine Presentations anatomical problems thyroid nodule / goitre embryological
Women s Health in General Practice Symposium 2015 Thyroid & Parathyroid Cases Bill Fleming Epworth Freemasons Hospital 1 Common Endocrine Presentations anatomical problems thyroid nodule / goitre embryological
Disorders of the Thyroid Gland
 Disorders of the Thyroid Gland István Takács MD., PhD, 1st Department of Medicine, Semmelweis University Connection to the dentistry: close to each other higher operation risk radiating pain macroglossia
Disorders of the Thyroid Gland István Takács MD., PhD, 1st Department of Medicine, Semmelweis University Connection to the dentistry: close to each other higher operation risk radiating pain macroglossia
Objectives. 1)To recall thyroid nodule ultrasound characteristics that increase the risk of malignancy
To recall thyroid nodule ultrasound characteristics that increase the risk of malignancy") Evaluation and Management of Thyroid Nodules in Primary Care Chris Sadler, MA, PA C, CDE, DFAAPA Medical Science Outcomes Liaison Intarcia Diabetes and Endocrine Associates La Jolla, CA Past President
Evaluation and Management of Thyroid Nodules in Primary Care Chris Sadler, MA, PA C, CDE, DFAAPA Medical Science Outcomes Liaison Intarcia Diabetes and Endocrine Associates La Jolla, CA Past President
Hyperthyroidism. Objectives. Clinical Manifestations. Slide 1. Slide 2. Slide 3. Implications for Primary Care. hyperthyroidism
 1 Hyperthyroidism Implications for Primary Care Laura A. Ruby, DNP, CRNP Wellspan Endocrinology 2 Objectives! Discuss the clinical manifestations of hyperthyroidism! Review the use of the diagnostic studies!
1 Hyperthyroidism Implications for Primary Care Laura A. Ruby, DNP, CRNP Wellspan Endocrinology 2 Objectives! Discuss the clinical manifestations of hyperthyroidism! Review the use of the diagnostic studies!
Evaluation and Management of Thyroid Nodules. Overview of Thyroid Nodules and Their Management. Thyroid Nodule detection: U/S versus Exam
 Overview of Thyroid Nodules and Their Management Matthew D. Ringel, M.D. Professor of Medicine Divisions of Endocrinology and Oncology, The Ohio State University Co-Director, Thyroid Cancer Unit Arthur
Overview of Thyroid Nodules and Their Management Matthew D. Ringel, M.D. Professor of Medicine Divisions of Endocrinology and Oncology, The Ohio State University Co-Director, Thyroid Cancer Unit Arthur
Thyroid Nodule. N. Rojanapithayakorn P. Prasarttong-Osoth
 Thyroid Nodule N. Rojanapithayakorn P. Prasarttong-Osoth A Brief History of the Thyroid A Brief History of the Thyroid Fabricius Wharton Von Haller A Brief History of the Thyroid Kendall Enrico Fermi A
Thyroid Nodule N. Rojanapithayakorn P. Prasarttong-Osoth A Brief History of the Thyroid A Brief History of the Thyroid Fabricius Wharton Von Haller A Brief History of the Thyroid Kendall Enrico Fermi A
HYPERTHYROIDISM. Hypothalamus. Thyrotropin-releasing hormone (TRH) Anterior pituitary gland. Thyroid-stimulating hormone (TSH) Thyroid gland T4, T3
 Anterior pituitary gland. Thyroid-stimulating hormone (TSH) Thyroid gland T4, T3") HYPERTHYROIDISM Hypothalamus Thyrotropin-releasing hormone (TRH) Anterior pituitary gland Thyroid-stimulating hormone (TSH) Thyroid gland T4, T3 In hyperthyroidism, there is an increased production of
HYPERTHYROIDISM Hypothalamus Thyrotropin-releasing hormone (TRH) Anterior pituitary gland Thyroid-stimulating hormone (TSH) Thyroid gland T4, T3 In hyperthyroidism, there is an increased production of
Thyroid and Parathyroid Surgery
 Med 5 Surgery Refresher Course 2013 2014 Thyroid and Parathyroid Surgery Dr Shirley Liu Resident Specialist Honorary Clinical Assistant Professor Team 2 Surgery Prince of Wales Hospital Case scenario:
Med 5 Surgery Refresher Course 2013 2014 Thyroid and Parathyroid Surgery Dr Shirley Liu Resident Specialist Honorary Clinical Assistant Professor Team 2 Surgery Prince of Wales Hospital Case scenario:
2015 American Thyroid Association Thyroid Nodule and Cancer Guidelines
 2015 American Thyroid Association Thyroid Nodule and Cancer Guidelines Angela M. Leung, MD, MSc, ECNU November 5, 2016 Outline Workup of nontoxic thyroid nodule(s) Ultrasound FNAB Management of FNAB results
2015 American Thyroid Association Thyroid Nodule and Cancer Guidelines Angela M. Leung, MD, MSc, ECNU November 5, 2016 Outline Workup of nontoxic thyroid nodule(s) Ultrasound FNAB Management of FNAB results
Objectives. How to Investigate Thyroid Nodules like A Pro
 How to Investigate Thyroid Nodules like A Pro Chris Sadler, MA, PA C, CDE, DFAAPA Medical Science Outcomes Liaison Intarcia Diabetes and Endocrine Associates La Jolla, CA Past President ASEPA Disclosures
How to Investigate Thyroid Nodules like A Pro Chris Sadler, MA, PA C, CDE, DFAAPA Medical Science Outcomes Liaison Intarcia Diabetes and Endocrine Associates La Jolla, CA Past President ASEPA Disclosures
THYROID FUNCTION TEST and RADIONUCLIDE THERAPY
 THYROID FUNCTION TEST and RADIONUCLIDE THERAPY Ajalaya Teyateeti, M.D. Division of Nuclear Medicine Department of Radiology I. Thyroid function test OUTLINE Application and interpretation of in vitro TFT
THYROID FUNCTION TEST and RADIONUCLIDE THERAPY Ajalaya Teyateeti, M.D. Division of Nuclear Medicine Department of Radiology I. Thyroid function test OUTLINE Application and interpretation of in vitro TFT
Approach to thyroid dysfunction
 Approach to thyroid dysfunction Alice Y.Y. Cheng, MD, FRCPC Twitter: @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or
Approach to thyroid dysfunction Alice Y.Y. Cheng, MD, FRCPC Twitter: @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or
Thyroid Neoplasm. ORL-Head and neck Surgery 2014
 In The Name of God Thyroid Neoplasm ORL-Head and neck Surgery 2014 Malignant Neoplasm By age 90, virtually everyone has nodules Estimates of cancer prevalence at autopsy 4% to 36% Why these lesions are
In The Name of God Thyroid Neoplasm ORL-Head and neck Surgery 2014 Malignant Neoplasm By age 90, virtually everyone has nodules Estimates of cancer prevalence at autopsy 4% to 36% Why these lesions are
THYROTOXICOSIS DR.J.BALA KUMAR 2 ND YR SURGERY PG
 THYROTOXICOSIS DR.J.BALA KUMAR 2 ND YR SURGERY PG What is the difference between thyrotoxicosis and hyperthyroidism Thyrotoxicosis Thyrotoxicosis is defined as the state of thyroid hormone excess and is
THYROTOXICOSIS DR.J.BALA KUMAR 2 ND YR SURGERY PG What is the difference between thyrotoxicosis and hyperthyroidism Thyrotoxicosis Thyrotoxicosis is defined as the state of thyroid hormone excess and is
5/3/2017. Ahn et al N Engl J Med 2014; 371
 Alan Failor, M.D. Clinical Professor of Medicine Division of Metabolism, Endocrinology and Nutrition University of Washington April 20, 2017 No disclosures to report 1. Appropriately evaluate s in adult
Alan Failor, M.D. Clinical Professor of Medicine Division of Metabolism, Endocrinology and Nutrition University of Washington April 20, 2017 No disclosures to report 1. Appropriately evaluate s in adult
Thyroid Nodules. Dr. HAKIMI, SpAK Dr. MELDA DELIANA, SpAK Dr. SISKA MAYASARI LUBIS, SpA
 Thyroid Nodules ENDOCRINOLOGY DIVISION ENDOCRINOLOGY DIVISION Dr. HAKIMI, SpAK Dr. MELDA DELIANA, SpAK Dr. SISKA MAYASARI LUBIS, SpA Anatomical Considerations The Thyroid Nodule Congenital anomalies Thyroglossal
Thyroid Nodules ENDOCRINOLOGY DIVISION ENDOCRINOLOGY DIVISION Dr. HAKIMI, SpAK Dr. MELDA DELIANA, SpAK Dr. SISKA MAYASARI LUBIS, SpA Anatomical Considerations The Thyroid Nodule Congenital anomalies Thyroglossal
Differentiated Thyroid Cancer: Initial Management
 Page 1 ATA HOME GIVE ONLINE ABOUT THE ATA JOIN THE ATA MEMBER SIGN-IN INFORMATION FOR PATIENTS FIND A THYROID SPECIALIST Home Management Guidelines for Patients with Thyroid Nodules and Differentiated
Page 1 ATA HOME GIVE ONLINE ABOUT THE ATA JOIN THE ATA MEMBER SIGN-IN INFORMATION FOR PATIENTS FIND A THYROID SPECIALIST Home Management Guidelines for Patients with Thyroid Nodules and Differentiated
Imaging in Pediatric Thyroid disorders: US and Radionuclide imaging. Deepa R Biyyam, MD Attending Pediatric Radiologist
 Imaging in Pediatric Thyroid disorders: US and Radionuclide imaging Deepa R Biyyam, MD Attending Pediatric Radiologist Imaging in Pediatric Thyroid disorders: Imaging modalities Outline ACR-SNM-SPR guidelines
Imaging in Pediatric Thyroid disorders: US and Radionuclide imaging Deepa R Biyyam, MD Attending Pediatric Radiologist Imaging in Pediatric Thyroid disorders: Imaging modalities Outline ACR-SNM-SPR guidelines
The Thyroid Gland. Chaitan K. Narsule, M.D.
 The Thyroid Gland Chaitan K. Narsule, M.D. The Thyroid Gland Thyreoides = shield shaped Goiter well-described in literature in 19th century Seaweed was medical treatment (iodine rich) The Thyroid Gland
The Thyroid Gland Chaitan K. Narsule, M.D. The Thyroid Gland Thyreoides = shield shaped Goiter well-described in literature in 19th century Seaweed was medical treatment (iodine rich) The Thyroid Gland
Thyroid and Adrenal Gland
 Thyroid and Adrenal Gland NAACCR 2011 2012 Webinar Series 12/1/11 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
Thyroid and Adrenal Gland NAACCR 2011 2012 Webinar Series 12/1/11 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
Management of Thyroid Nodules
 Management of Thyroid Nodules 38 y/o female with solid 1.5 cm right Thyroid nodule. TSH=0.68 Vincent J. Reid, MD., FACS Thyroid Cancer Incidence & Mortality 1974 to 2004 Overall Women Men Mortality 1 Cancer
Management of Thyroid Nodules 38 y/o female with solid 1.5 cm right Thyroid nodule. TSH=0.68 Vincent J. Reid, MD., FACS Thyroid Cancer Incidence & Mortality 1974 to 2004 Overall Women Men Mortality 1 Cancer
3/29/2012. Thyroid cancer- what s new. Thyroid Cancer. Thyroid cancer is now the most rapidly increasing cancer in women
 Thyroid cancer- what s new Thyroid Cancer Changing epidemiology Molecular markers Lymph node dissection Technical advances rhtsh Genetic testing and prophylactic surgery Vandetanib What s new? Jessica
Thyroid cancer- what s new Thyroid Cancer Changing epidemiology Molecular markers Lymph node dissection Technical advances rhtsh Genetic testing and prophylactic surgery Vandetanib What s new? Jessica
OPEN ACCESS TEXTBOOK OF GENERAL SURGERY
 OPEN ACCESS TEXTBOOK OF GENERAL SURGERY THE THYROID GLAND DM Dent INTRODUCTION Thyroid problems are commonly encountered in general practice. In most instances they will be minor ones of physiological
OPEN ACCESS TEXTBOOK OF GENERAL SURGERY THE THYROID GLAND DM Dent INTRODUCTION Thyroid problems are commonly encountered in general practice. In most instances they will be minor ones of physiological
TBSRTC 1- Probabilistic approach and Relationship to Clinical Algorithms
 The Benefits of a Uniform Reporting System for Thyroid Cytopathology BETHESDA REPORTING SYSTEM Prof. Fernando Schmitt Department of Pathology and Oncology, Medical Faculty of Porto University Head of Molecular
The Benefits of a Uniform Reporting System for Thyroid Cytopathology BETHESDA REPORTING SYSTEM Prof. Fernando Schmitt Department of Pathology and Oncology, Medical Faculty of Porto University Head of Molecular
DEVELOPMENT & STRUCTURE OF THYROID GLAND DR TATHEER ZAHRA ASSISTANT PROFESSOR ANATOMY
 DEVELOPMENT & STRUCTURE OF THYROID GLAND DR TATHEER ZAHRA ASSISTANT PROFESSOR ANATOMY DEVELOPMENT OF THYROID Concept of pharyngeal arch 3 rd week 4 th week Adults 7 th week HISTOGENESIS OF THYROID GLAND
DEVELOPMENT & STRUCTURE OF THYROID GLAND DR TATHEER ZAHRA ASSISTANT PROFESSOR ANATOMY DEVELOPMENT OF THYROID Concept of pharyngeal arch 3 rd week 4 th week Adults 7 th week HISTOGENESIS OF THYROID GLAND
Goiter, Nodules and Tumors
 Goiter, Nodules and Tumors Howard J. Sachs, MD www.12daysinmarch.com Thyroid Cancer Anaplastic Medullary Thyroid Cancer Anaplastic Medullary Thyroid Cancer Anaplastic Medullary Anaplastic Medullary MEN
Goiter, Nodules and Tumors Howard J. Sachs, MD www.12daysinmarch.com Thyroid Cancer Anaplastic Medullary Thyroid Cancer Anaplastic Medullary Thyroid Cancer Anaplastic Medullary Anaplastic Medullary MEN
Dharma Lindarto Div. Endokrin-Metabolisme dan Diabetes. Dep Ilmu Penyakit Dalam FK USU / RSUP HAM Medan
 HYPERTHYROIDISM Dharma Lindarto Div. Endokrin-Metabolisme dan Diabetes. Dep Ilmu Penyakit Dalam FK USU / RSUP HAM Medan Anatomy of the Thyroid Gland Tiroid Disease Multi N Aspect fungtion morphology eutiroid,
HYPERTHYROIDISM Dharma Lindarto Div. Endokrin-Metabolisme dan Diabetes. Dep Ilmu Penyakit Dalam FK USU / RSUP HAM Medan Anatomy of the Thyroid Gland Tiroid Disease Multi N Aspect fungtion morphology eutiroid,
Adjuvant therapy for thyroid cancer
 Carcinoma of the thyroid Adjuvant therapy for thyroid cancer John Hay Department of Radiation Oncology Vancouver Cancer Centre Department of Surgery UBC 1% of all new malignancies 0.5% in men 1.5% in women
Carcinoma of the thyroid Adjuvant therapy for thyroid cancer John Hay Department of Radiation Oncology Vancouver Cancer Centre Department of Surgery UBC 1% of all new malignancies 0.5% in men 1.5% in women
AACE 2018 Advanced Endocrine Neck Ultrasound and UGFNA Course
 AACE 2018 Advanced Endocrine Neck Ultrasound and UGFNA Course Describe the sonographic appearance of diffuse thyroid diseases: autoimmune thyroid disease Review non thyroidal findings that can be encountered
AACE 2018 Advanced Endocrine Neck Ultrasound and UGFNA Course Describe the sonographic appearance of diffuse thyroid diseases: autoimmune thyroid disease Review non thyroidal findings that can be encountered
Index. radiologic.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A ACC. See Adrenal cortical carcinoma. Acromegaly and the pituitary gland, 551 Acute suppurative thyroiditis, 405, 406 Addison, Thomas and
Index Note: Page numbers of article titles are in boldface type. A ACC. See Adrenal cortical carcinoma. Acromegaly and the pituitary gland, 551 Acute suppurative thyroiditis, 405, 406 Addison, Thomas and
DISORDERS OF THE THYROID GLAND SIGNS, SYMPTOMS, & TREATMENT ENDOCRINE SYSTEM AT A GLANCE OBJECTIVES ANATOMY OF THE THYROID
 OBJECTIVES DISORDERS OF THE THYROID GLAND SIGNS, SYMPTOMS, & TREATMENT Stephanie Blackburn, MHS, MLS(ASCP) CM LSU Health Shreveport Clinical Laboratory Science Program Discuss the synthesis and action
OBJECTIVES DISORDERS OF THE THYROID GLAND SIGNS, SYMPTOMS, & TREATMENT Stephanie Blackburn, MHS, MLS(ASCP) CM LSU Health Shreveport Clinical Laboratory Science Program Discuss the synthesis and action
Thyroid Surgery: Lobectomy, total thyroidectomy, LN biopsies or only watchful waiting?
 Thyroid Surgery: Lobectomy, total thyroidectomy, LN biopsies or only watchful waiting? Jacob Moalem, MD, FACS Associate Professor Endocrine Surgery and Endocrinology URMC Agenda 1. When is lobectomy alone
Thyroid Surgery: Lobectomy, total thyroidectomy, LN biopsies or only watchful waiting? Jacob Moalem, MD, FACS Associate Professor Endocrine Surgery and Endocrinology URMC Agenda 1. When is lobectomy alone
Common Causes of Hypothyroidism
 Common Causes of Hypothyroidism Autoimmune thyroidi4s Surgical removal of thyroid gland Medica4on Therapy Iodine and iodine containing medica4ons Neck radia4on Post Partum thyroidi4s Prevalence of Hypothyroidism
Common Causes of Hypothyroidism Autoimmune thyroidi4s Surgical removal of thyroid gland Medica4on Therapy Iodine and iodine containing medica4ons Neck radia4on Post Partum thyroidi4s Prevalence of Hypothyroidism
NEOPLASMS OF THE THYROID PATHOLOGY OF PARATHYROID GLANDS. BY: Shifaa Qa qa
 NEOPLASMS OF THE THYROID PATHOLOGY OF PARATHYROID GLANDS BY: Shifaa Qa qa Neoplasmas of the thyroid thyroid nodules Neoplastic ---- benign, malignant Non neoplastic Solitary nodules ----- neoplastic Nodules
NEOPLASMS OF THE THYROID PATHOLOGY OF PARATHYROID GLANDS BY: Shifaa Qa qa Neoplasmas of the thyroid thyroid nodules Neoplastic ---- benign, malignant Non neoplastic Solitary nodules ----- neoplastic Nodules
Chapter 14: Thyroid Cancer
 The American Academy of Otolaryngology Head and Neck Surgery Foundation (AAO-HNSF) Presents... Chapter 14: Thyroid Cancer Daiichi Pharmaceutical Corporation, marketers and distributors of FLOXIN Otic (ofloxacin
The American Academy of Otolaryngology Head and Neck Surgery Foundation (AAO-HNSF) Presents... Chapter 14: Thyroid Cancer Daiichi Pharmaceutical Corporation, marketers and distributors of FLOXIN Otic (ofloxacin
Thyroid Gland. Patient Information
 Thyroid Gland Patient Information Contact details for Endocrine and Thyroid Clinics Hawke s Bay Fallen Soldiers Memorial Hospital Villa 16 Phone: 06 8788109 ext 5891 Text: 0274 102 559 Email: endoclinic@hbdhb.govt.nz
Thyroid Gland Patient Information Contact details for Endocrine and Thyroid Clinics Hawke s Bay Fallen Soldiers Memorial Hospital Villa 16 Phone: 06 8788109 ext 5891 Text: 0274 102 559 Email: endoclinic@hbdhb.govt.nz
MTP: Thyroid Nodules
 Canadian Endocrine Update MTP: Thyroid Nodules Deric Morrison MD, FRCP, ECNU Assistant Professor, Division of Endocrinology and Metabolism, Western University April 2014 Faculty/Presenter Disclosure Faculty:
Canadian Endocrine Update MTP: Thyroid Nodules Deric Morrison MD, FRCP, ECNU Assistant Professor, Division of Endocrinology and Metabolism, Western University April 2014 Faculty/Presenter Disclosure Faculty:
CAP Cancer Protocol and ecc Summary of Changes for August 2014 Thyroid Agile Release
 CAP Cancer Protocol and ecc Summary of Changes for August 2014 Thyroid Agile Release 2 REVISION HISTORY Date Author / Editor Comments 5/19/2014 Jaleh Mirza Created the document 8/12/2014 Samantha Spencer/Jaleh
CAP Cancer Protocol and ecc Summary of Changes for August 2014 Thyroid Agile Release 2 REVISION HISTORY Date Author / Editor Comments 5/19/2014 Jaleh Mirza Created the document 8/12/2014 Samantha Spencer/Jaleh
B Berry, J. 25 see also suspensory ligament of Berry biopsy see fine-needle aspiration biopsy (FNAB); open wedge biopsy
; open wedge biopsy") 174 Index Index Page numbers in italics refer to illustrations A abscess 80, 137 adenoma 61 parathyroid 18, 18 19, 62, 84 differential diagnosis 84, 84, 85, 85 thyroid 63 follicular 62, 63, 64 macrofollicular
174 Index Index Page numbers in italics refer to illustrations A abscess 80, 137 adenoma 61 parathyroid 18, 18 19, 62, 84 differential diagnosis 84, 84, 85, 85 thyroid 63 follicular 62, 63, 64 macrofollicular
Persistent & Recurrent Differentiated Thyroid Cancer
 Persistent & Recurrent Differentiated Thyroid Cancer Electron Kebebew University of California, San Francisco Department of Surgery Objectives Risk factors for persistent & recurrent disease Causes of
Persistent & Recurrent Differentiated Thyroid Cancer Electron Kebebew University of California, San Francisco Department of Surgery Objectives Risk factors for persistent & recurrent disease Causes of
Differentiated Thyroid Carcinoma
 Differentiated Thyroid Carcinoma The GOOD cancer? Jennifer Sipos, MD Associate Professor of Medicine Director, Benign Thyroid Program Division of Endocrinology, Diabetes and Metabolism The Ohio State University
Differentiated Thyroid Carcinoma The GOOD cancer? Jennifer Sipos, MD Associate Professor of Medicine Director, Benign Thyroid Program Division of Endocrinology, Diabetes and Metabolism The Ohio State University
Laura Trask, MD FACP Central Maine Endocrinology Lewiston, ME
 Laura Trask, MD FACP Central Maine Endocrinology Lewiston, ME 795-7520 traskla@cmhc.org No disclosures Objectives To have an understanding of hyperthyroidism To have an understanding of the management
Laura Trask, MD FACP Central Maine Endocrinology Lewiston, ME 795-7520 traskla@cmhc.org No disclosures Objectives To have an understanding of hyperthyroidism To have an understanding of the management
Thyroid Diseases. Dr Rodney Itaki Lecturer Anatomical Pathology Discipline
 Thyroid Diseases Dr Rodney Itaki Lecturer Anatomical Pathology Discipline University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology This is the normal appearance of thethyroid
Thyroid Diseases Dr Rodney Itaki Lecturer Anatomical Pathology Discipline University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology This is the normal appearance of thethyroid
The Number Games and Thyroid Function Arshia Panahloo Consultant Endocrinologist St George s Hospital
 The Number Games and Thyroid Function Arshia Panahloo Consultant Endocrinologist St George s Hospital Presentation Today: Common thyroid problems and treatments Pregnancy related thyroid problems The suppressed
The Number Games and Thyroid Function Arshia Panahloo Consultant Endocrinologist St George s Hospital Presentation Today: Common thyroid problems and treatments Pregnancy related thyroid problems The suppressed
Thyroid Ultrasonography: clinical and radiological correlations
 Thyroid Ultrasonography: clinical and radiological correlations Dr.M.Thijs Radiology Anatomy Inflammatory Thyroid Disease Benign lesions Thyroid tumors Thyroglossal duct cyst Anatomy Transverse Longitudinal
Thyroid Ultrasonography: clinical and radiological correlations Dr.M.Thijs Radiology Anatomy Inflammatory Thyroid Disease Benign lesions Thyroid tumors Thyroglossal duct cyst Anatomy Transverse Longitudinal
Pathology. Hyperthyroidism (Overactive Thyroid), Graves Disease (Basedow Disease) and more. Definitions. See online here
, Graves Disease (Basedow Disease) and more. Definitions. See online here") Pathology Hyperthyroidism (Overactive Thyroid), Graves Disease (Basedow Disease) and more See online here Hyperthyroidism is caused by the excess of thyroid hormones T3 and T4. Graves disease is the most
Pathology Hyperthyroidism (Overactive Thyroid), Graves Disease (Basedow Disease) and more See online here Hyperthyroidism is caused by the excess of thyroid hormones T3 and T4. Graves disease is the most
Disorders of Thyroid Function
 Disorders of Thyroid Function Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Thyroid Hormone Axis Hypothalamus TRH
Disorders of Thyroid Function Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Thyroid Hormone Axis Hypothalamus TRH
Review Article Management of thyroid carcinoma Alauddin M, Joarder AH
 Management of thyroid carcinoma Alauddin M, Joarder AH The ORION Medical Journal 2004 May;18:163-166 Overview The two most common forms of thyroid cancer, papillaryand follicular thyroid cancer, together
Management of thyroid carcinoma Alauddin M, Joarder AH The ORION Medical Journal 2004 May;18:163-166 Overview The two most common forms of thyroid cancer, papillaryand follicular thyroid cancer, together
A rare case of solitary toxic nodule in a 3yr old female child a case report
 Volume 3 Issue 1 2013 ISSN: 2250-0359 A rare case of solitary toxic nodule in a 3yr old female child a case report *Chandrasekaran Maharajan * Poongkodi Karunakaran *Madras Medical College ABSTRACT A three
Volume 3 Issue 1 2013 ISSN: 2250-0359 A rare case of solitary toxic nodule in a 3yr old female child a case report *Chandrasekaran Maharajan * Poongkodi Karunakaran *Madras Medical College ABSTRACT A three
Oh, I get it, the TSH goes up and down
 Evaluation and Management of the Thyroid Nodule Oh, I get it, the TSH goes up and down UCSF Head and Neck Conference October 24, 2008 Peter A. Singer, M.D. Professor and Chief Clinical Endocrinology University
Evaluation and Management of the Thyroid Nodule Oh, I get it, the TSH goes up and down UCSF Head and Neck Conference October 24, 2008 Peter A. Singer, M.D. Professor and Chief Clinical Endocrinology University
Thyroid carcinoma. Assoc. prof. V. Marković, MD, PhD Assoc. prof. A. Punda, MD, PhD D. Brdar, MD, nucl. med. spec.
 Thyroid carcinoma Assoc. prof. V. Marković, MD, PhD Assoc. prof. A. Punda, MD, PhD D. Brdar, MD, nucl. med. spec. Thyroid tumors PRIMARY TUMORS Tumors of the follicular epithelium : - Tumors of the follicular
Thyroid carcinoma Assoc. prof. V. Marković, MD, PhD Assoc. prof. A. Punda, MD, PhD D. Brdar, MD, nucl. med. spec. Thyroid tumors PRIMARY TUMORS Tumors of the follicular epithelium : - Tumors of the follicular
Normal thyroid tissue
 Thyroid Pathology Overview Normal thyroid tissue Normal thyroid tissue with follicles filled with colloid. Thyroid cells form follicles, spheres of epithelial cells (always single layered in health, usually
Thyroid Pathology Overview Normal thyroid tissue Normal thyroid tissue with follicles filled with colloid. Thyroid cells form follicles, spheres of epithelial cells (always single layered in health, usually
Approach to Thyroid Dysfunction in the Elderly
 Approach to Thyroid Dysfunction in the Elderly Fernando Melaragno Endocrinology Objective The objective of this lecture is to review the epidemiology, clinical presentation, risks and complications, and
Approach to Thyroid Dysfunction in the Elderly Fernando Melaragno Endocrinology Objective The objective of this lecture is to review the epidemiology, clinical presentation, risks and complications, and
10/24/2008. Surgery for Well-differentiated Thyroid Carcinoma- The Primary
 Surgery for Well-differentiated Thyroid Carcinoma- The Primary Head and Neck Endocrine Surgery Department of Otolaryngology-Head and Neck Surgery, UCSF October 24-25, 2008 Robert A. Sofferman, MD Professor
Surgery for Well-differentiated Thyroid Carcinoma- The Primary Head and Neck Endocrine Surgery Department of Otolaryngology-Head and Neck Surgery, UCSF October 24-25, 2008 Robert A. Sofferman, MD Professor
Background to the Thyroid Nodule
 William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital THYROID FNA: PART I Background to the
William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital THYROID FNA: PART I Background to the
 To the Patient and Family This booklet has been written for people who have received a diagnosis of thyroid cancer or who are being tested for this illness. If you have questions that are not answered
To the Patient and Family This booklet has been written for people who have received a diagnosis of thyroid cancer or who are being tested for this illness. If you have questions that are not answered
How good are we at finding nodules? Thyroid Nodules Thyroid Cancer Epidemiology Initial management Long-term follow up Disease-free status
 New Perspectives in Thyroid Cancer Jennifer Sipos, MD Assistant Professor of Medicine Division of Endocrinology The Ohio State University Outline Thyroid Nodules Thyroid Cancer Epidemiology Initial management
New Perspectives in Thyroid Cancer Jennifer Sipos, MD Assistant Professor of Medicine Division of Endocrinology The Ohio State University Outline Thyroid Nodules Thyroid Cancer Epidemiology Initial management
Thyroiditis Diagnosis and Management issues. Prof. Md. Enamul Karim Professor of Medicine Dhaka Medical College
 Thyroiditis Diagnosis and Management issues Prof. Md. Enamul Karim Professor of Medicine Dhaka Medical College Definition Thyroiditis is a general term that refers to inflammation of the thyroid gland.
Thyroiditis Diagnosis and Management issues Prof. Md. Enamul Karim Professor of Medicine Dhaka Medical College Definition Thyroiditis is a general term that refers to inflammation of the thyroid gland.
B. Environmental Factors. a. The major risk factor to papillary thyroid cancer is exposure to ionizing radiation, during the first 2 decades of life.
 B. Environmental Factors. a. The major risk factor to papillary thyroid cancer is exposure to ionizing radiation, during the first 2 decades of life. b. Deficiency of dietary iodine: - Is linked with a
B. Environmental Factors. a. The major risk factor to papillary thyroid cancer is exposure to ionizing radiation, during the first 2 decades of life. b. Deficiency of dietary iodine: - Is linked with a
What you need to know about Thyroid Cancer
 What you need to know about Thyroid Cancer This booklet has been designed to help you to learn more about your thyroid cancer. It covers the most important areas and answers some of the frequently asked
What you need to know about Thyroid Cancer This booklet has been designed to help you to learn more about your thyroid cancer. It covers the most important areas and answers some of the frequently asked
THE THYROID BOOK. Medical and Surgical Treatment of Thyroid Problems
 THE THYROID BOOK Medical and Surgical Treatment of Thyroid Problems Trouble with Your Thyroid Gland The thyroid is a small gland in your neck that plays a big role in how your body functions. It impacts
THE THYROID BOOK Medical and Surgical Treatment of Thyroid Problems Trouble with Your Thyroid Gland The thyroid is a small gland in your neck that plays a big role in how your body functions. It impacts
General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons
 General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons MODULE TITLE: ENDOCRINE 5-May-2013 DEVELOPED BY: Jonathan Serpell
General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons MODULE TITLE: ENDOCRINE 5-May-2013 DEVELOPED BY: Jonathan Serpell
ABSITE Review. RTC Conference Christina Bailey January 15, 2009
 ABSITE Review RTC Conference Christina Bailey January 15, 2009 How It s Broken Down? 220 questions Junior level (PGY 1 and 2) Exam 60% Basic Science 40% Clinical Management Senior Level (PGY 3-5) exam
ABSITE Review RTC Conference Christina Bailey January 15, 2009 How It s Broken Down? 220 questions Junior level (PGY 1 and 2) Exam 60% Basic Science 40% Clinical Management Senior Level (PGY 3-5) exam
B-Resistance to the action of hormones, Hormone resistance characterized by receptor mediated, postreceptor.
 Disorders of the endocrine system 38 Disorders of endocrine system mainly are caused by: A-Deficiency or an excess of a single hormone or several hormones: - deficiency :can be congenital or acquired.
Disorders of the endocrine system 38 Disorders of endocrine system mainly are caused by: A-Deficiency or an excess of a single hormone or several hormones: - deficiency :can be congenital or acquired.
Iodine 131 thyroid Therapy. Sara G. Johnson, MBA, CNMT, NCT President SNMMI-TS VA Healthcare System San Diego
 Iodine 131 thyroid Therapy Sara G. Johnson, MBA, CNMT, NCT President SNMMI-TS VA Healthcare System San Diego OBJECTIVES Describe the basics of thyroid gland anatomy and physiology Outline the disease process
Iodine 131 thyroid Therapy Sara G. Johnson, MBA, CNMT, NCT President SNMMI-TS VA Healthcare System San Diego OBJECTIVES Describe the basics of thyroid gland anatomy and physiology Outline the disease process
Update In Hyperthyroidism
 Update In Hyperthyroidism CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi Copyright
Update In Hyperthyroidism CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi Copyright
Calcitonin. 1
 Calcitonin Medullary thyroid carcinoma (MTC) is characterized by a high concentration of serum calcitonin. Routine measurement of serum calcitonin concentration has been advocated for detection of MTC
Calcitonin Medullary thyroid carcinoma (MTC) is characterized by a high concentration of serum calcitonin. Routine measurement of serum calcitonin concentration has been advocated for detection of MTC
Alvin C. Powers, M.D. 1/27/06
 Thyroid Histology Follicular Cells ECF side Apical lumen Thyroid Follicles -200-400 um Parafollicular or C-cells Colloid Photos from University of Manchester and tutorial created by Dr. James Crimando,
Thyroid Histology Follicular Cells ECF side Apical lumen Thyroid Follicles -200-400 um Parafollicular or C-cells Colloid Photos from University of Manchester and tutorial created by Dr. James Crimando,
Thyroid Nodules. No conflicts. Overview 5/16/2017. UCSF Internal Medicine Updates May 22, 2017 Elizabeth Murphy, MD, DPhil
 Thyroid Nodules UCSF Internal Medicine Updates May 22, 2017 Elizabeth Murphy, MD, DPhil No conflicts Overview Thyroid nodule and cancer review Ultrasound FNA cytology Nodule follow up Putting it all together
Thyroid Nodules UCSF Internal Medicine Updates May 22, 2017 Elizabeth Murphy, MD, DPhil No conflicts Overview Thyroid nodule and cancer review Ultrasound FNA cytology Nodule follow up Putting it all together
Thyroid Pathology: It starts and ends with the gross. Causes of Thyrophobia. Agenda. Diagnostic ambiguity. Treatment/prognosis disconnect
 Thyroid Pathology: It starts and ends with the gross Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for
Thyroid Pathology: It starts and ends with the gross Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for
Chapter I.A.1: Thyroid Evaluation Laboratory Testing
 Chapter I.A.1: Thyroid Evaluation Laboratory Testing Jennifer L. Poehls, MD and Rebecca S. Sippel, MD, FACS THYROID FUNCTION TESTS Overview Thyroid-stimulating hormone (TSH) is produced by the anterior
Chapter I.A.1: Thyroid Evaluation Laboratory Testing Jennifer L. Poehls, MD and Rebecca S. Sippel, MD, FACS THYROID FUNCTION TESTS Overview Thyroid-stimulating hormone (TSH) is produced by the anterior