Marcin Dada, MD December 03, 2013
|
|
|
- Ashlee Harrison
- 5 years ago
- Views:
Transcription

1 STEMI Imposters Marcin Dada, MD December 03, 2013
2 Marcin Dada, MD Associate Director, Chest Pain Center Hartford Hospital, Hartford, CT Member, AHA Mission Lifeline Steering Committee
3 Outline of Topics STEMI Introduction (challenges) STEMI/ECG STEMI Imposters LBBB with. STEMI vs Pericarditis vs BER Early reciprocal changes in avl
4 Hospitalizations in the U.S. Due to Acute Coronary Syndromes (ACS) Acute Coronary Syndromes* 1.57 Million Hospital Admissions - ACS UA/NSTEMI 1.24 million Admissions per year STEMI.33 million Admissions per year Heart Disease and Stroke Statistics 2007 Update. Circulation 2007; 115: *Primary and secondary diagnoses. About 0.57 million NSTEMI and 0.67 million UA. 4
 Critical Time-dependent")
5 Mortality Reduction (%) 1. Time is Myocardium 2. Infarct Size is Outcome D C 20 0 Extent of Myocardial Salvage B A Time From Symptom Onset to Reperfusion Therapy (h) Critical Time-dependent Period Goal: Myocardial Salvage Time-independent Period Goal: Open Infarct-Related Artery Gersh BJ, et al. JAMA. 2005;293:979.

6 Time To Treatment Goals for Primary PCI 2013 ACCF/AHA guidelines for the management of ST-elevation myocardial infarction: executive summary: a report of the ACC/AHA Task Force on Practice Guidelines. J Am Coll Cardiol 2013;61:

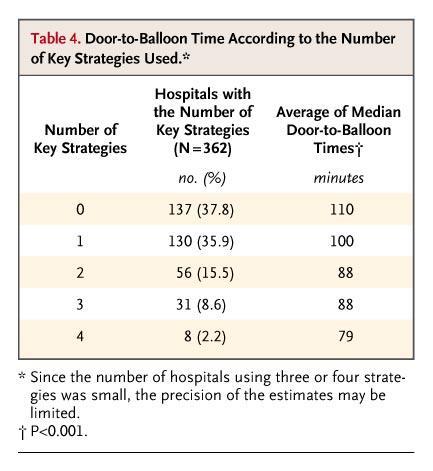
7 Door-to-balloon times down, but inhospital mortality unchanged. 7
8 Total System Delay (First Medical Contact to Device) and Long-Term Mortality Each hour of delay associated with 10% risk of death Terkelsen JAMA. 2010;304(7):
9 Challenges Mean symptom duration is still 2 hours before FMC, and 40% of patients do not contact EMS. An ACC AHA performance measure sets a DIDO goal of 30 minutes for internal quality-improvement purposes, but the metric is not used for public reporting, and the best regional STEMI systems are averaging 45 minutes.
10 Challenges Nearly 70-80% of STEMI patients in the US present to community hospitals without PCI capability For patients requiring interhospital transfer, first-door-to-balloon time is 90 minutes or less in only 33% of cases and 120 minutes or less in only 66%.
11 SUMMARY The primary opportunity for reducing total ischemic time and time to treatment, and for improving outcomes, now lies in the pre-hospital STEMI system of care. Currently: 90% of patients who present directly to PCI-capable hospitals treated within 90 min, median time of approximately 60 minutes

12 Evidence Based Approach
13 Summary By incorporating pre hosp 12L ECGs into routine evaluation of potential of cardiac ischemia, STEMI patients are identified at the point of their earliest interaction with the medical system. By acting on this diagnostic information and using it to trigger an organized, system wide response, STEMI pts achieve reperfusion of the IRA sooner, and thus can expect better outcomes.



14 ECG Expertise The eye does not see what the mind does not know.
15 Systematic approach Step 1: Determine rate and rhythm Step 2: Inspect the 12L for waveform changes (STEMI) Examine one representative complex Step 3: Determine if STEMI is suspected 1 mm in two contiguous leads (if so, find the region) Step 4: Identify additional considerations for STEMI STEP 5: Final interpretation Balance the evidence Decide how compelling is the case for STEMI


16

17 Reciprocal Changes ST depression in leads opposite infarction Strengthen suspicion of AMI Are not necessary to identify STEMI

18 Determination of ST Segment Morphology

19 Computer Anterior STEMI
20 STEMI Imposters LVH BBB (often LBBB) Ventricular Rhythms (often paced) Pericarditis Benign Early Repolarization
21 Ventricular Rhythm/LBBB Ventricles contract sequentially, widening the QRS So, if QRS is prolonged, an imposter is present it could be either. Normal QRS < 0.12sec

22 LVH Does not widen the QRS Instead of increasing the width increases the height Many formulas are available

23 LHV STEP 1: compare V1 and V2, deciding which one has the deepest negative deflection 25mm 27mm

24 LHV STEP 2: compare V5 and V6, deciding which one has the tallest positive deflection 21mm 19mm 27mm
25 LHV STEP 3: add the numbers, and if the sum is 35mm or more, suspect LVH V2 27 mm V5 21mm >35 mm Meets voltage criteria for LHV
26 Important The presence of an imitator does not rule out AMI If you suspect Infarct BEFORE the 12L you must still suspect Infarct AFTER the 12L
27 Question According to the 3 step approach, after comparing V1 and V2, and comparing V5 and V6, and adding the numbers, suspect LVH if the sum is: a) 25mm or less b) less than 35mm c) More than 35mm
28 Top STEMI Imposters LVH BBB (often LBBB) Ventricular Rhythms (often paced) Early Benign Repolarization Pericarditis

29 BER/Pericarditis Very unlikely to see reciprocal changes with either BER or Percarditis Percarditis: Diffuse ST elevation (concave)
30 STEMI/STEMI IMPOSTERS LVH BBB Ventricular paced rhythm Normal QRS QRS >0.12 Early Benign Repolarization Pericarditis Lack of reciprocal changes
31
32 STEMI OR 1) LVH 2) LBBB 3) Ventricular paced rhythm 4) BER 5) Pericarditis

33
34 STEMI OR 1) LVH 2) LBBB 3) Ventricular paced rhythm 4) BER 5) Pericarditis

35 62-year-old female with chest discomfort:
36 STEMI OR 1) LVH 2) LBBB 3) Ventricular paced rhythm 4) BER 5) Pericarditis
37 Systemic analysis STEMI Diagnosis 3 questions 1. ST segment elevation present? 2. QRS complex is normal? 3. ST segment depression is present? If YES to all 3 questions STOP ASKING SO MANY QESTIONS DO SOMETHING!
38 ECG STEMI Not a STEMI Definite Maybe ST elevation in 2 contiguous leads Non of the STEMI imposters Borderline ST elevation Clear ST elevation, but imposter is present No ST elevation in 2 contiguous leads

39 Normal LBBB Rule of appropriate discordance (true for pacemakers)

40 Left Bundle Brunch Block Diagnosis of AMI Sgarbossa criteria
41 LBBB with?
42 LBBB with AMI

43 LBBB with?
44 ECGs and Pericarditis 1. Factors that rule in STEMI 1. STD except in V1 and avr 2. STE in III>II 3. Horizontal and convex upward STE 4.! Waves that you KNOW are NEW 2. Factors that suggest AP 1. Friction rub 2. PR depression in multiple leads (only reliably seen in Viral AP, transient)

45 STEMI or AP

46 STEMI or AP
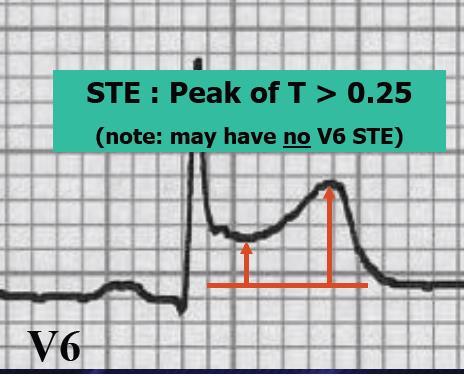
47 AP vs BER Positional changes in pain Fishhook ->BER Height STE:T wave in V6 Old ECGs

48 BER vs (MI and Pericarditis) BER MI/Pericarditis
 USUALLY ST SEGMENTS AND T CONCAVE UPWARDS STE II > III (ALMOST ALWAYS) UNLIKELY IN")
49 STEMI vs AP/BER AMI PERICARDITIS, BER STE,STD DIFFUSE OR LOCALIZED STE, FREQUENT RECIPROCAL STD USUALLY DIFFUSE STE, NO RECIPROCAL STD (EXCEPT V1 OR AVR) ST SEGMENT MORPHOLOGY IF STE II AND III EVOLVING CHANGES STRAIGHT, HORIZONTAL, CONVEX OR CONCAVE STE III > II (USUALLY) USUALLY ST SEGMENTS AND T CONCAVE UPWARDS STE II > III (ALMOST ALWAYS) UNLIKELY IN ED

50 Posterior Wall AMI Leads V1-V3 Horizontal ST Depressions Additional features Large R wave Upright T wave Frequently co-existing inferior or lateral
51 Case 56 yo. man presents c/o throat burning, nausea History of HTN, tobacco use, treated with maalox with mild improvement, patient wants to be discharged. 30 minutes later symptoms worsen (now with diaphoresis), ECG is obtained

52 Early Reciprocal Changes in avl (1)

53 Early Reciprocal Changes in avl (2)

54 Early Reciprocal Changes in avl (3)
55 Early Reciprocal Changes in avl The normal ECG lead avl Isoelectric ST-segment Upright T-wave Acute Inferior wall MIs Common reciprocal changes ST-segment down sloping in avl T-wave inversions in avl Reciprocal changes in avl can precede the development of inferior lead abnormalities (Marriott)
56 Class I Recommendation If the ECG is non-diagnostic of STEMI, but the patient remains symptomatic and there is a high clinical suspicion for STEMI, serial ECGs at 5 to 10-minute intervals or continuous 12L ST-segment monitoring should be performed to detect the potential development of ST elevation 2004 ECG Guidelines
57 CONCLUSION Continued efforts are needed to educate patients about STEMI symptoms and about calling 911 to permit EMS triage, treatment, and transport, as STEMI teams shift their focus from in-hospital to prehospital treatment delays.


58 Discussion Please ask questions and share your thoughts Thank you
All About STEMIs. Presented By: Brittney Urvand, RN, BSN, CCCC. Essentia Health Fargo Cardiovascular Program Manager.
 All About STEMIs Presented By: Brittney Urvand, RN, BSN, CCCC Essentia Health Fargo Cardiovascular Program Manager Updated 10/2/2018 None Disclosures Objectives Identify signs and symptoms of a heart attack
All About STEMIs Presented By: Brittney Urvand, RN, BSN, CCCC Essentia Health Fargo Cardiovascular Program Manager Updated 10/2/2018 None Disclosures Objectives Identify signs and symptoms of a heart attack
Disclosures. STEMI:To Call or Not to Call. Disclosures 9/18/2017. Alternate Title: Hey Doc, If you re not doing anything Saturday Night
 STEMI:To Call or Not to Call Disclosures No financial disclosures September, 2017 Frederick James Trip Meine III MD, FACC, FSCAI Cape Fear Heart Associates, Wilmington, NC Disclosures Alternate Title:
STEMI:To Call or Not to Call Disclosures No financial disclosures September, 2017 Frederick James Trip Meine III MD, FACC, FSCAI Cape Fear Heart Associates, Wilmington, NC Disclosures Alternate Title:
Electrocardiography for Healthcare Professionals. Chapter 14 Basic 12-Lead ECG Interpretation
 Electrocardiography for Healthcare Professionals Chapter 14 Basic 12-Lead ECG Interpretation 2012 The Companies, Inc. All rights reserved. Learning Outcomes 14.1 Discuss the anatomic views seen on a 12-lead
Electrocardiography for Healthcare Professionals Chapter 14 Basic 12-Lead ECG Interpretation 2012 The Companies, Inc. All rights reserved. Learning Outcomes 14.1 Discuss the anatomic views seen on a 12-lead
Acute Coronary Syndromes Unstable Angina Non ST segment Elevation MI (NSTEMI) ST segment Elevation MI (STEMI)
 ST segment Elevation MI (STEMI)") Leanna R. Miller, RN, MN, CCRN-CSC, PCCN-CMC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Evaluate common abnormalities that mimic myocardial infarction. Identify
Leanna R. Miller, RN, MN, CCRN-CSC, PCCN-CMC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Evaluate common abnormalities that mimic myocardial infarction. Identify
Goals: Widen Your Understanding of the Wide QRS!
 Goals: Widen Your Understanding of the Wide QRS! 1. Describe an approach to diagnosis of LBBB 2. Describe the predictive value of New LBBB 3. Describe the ST segment changes that are diagnostic of AMI
Goals: Widen Your Understanding of the Wide QRS! 1. Describe an approach to diagnosis of LBBB 2. Describe the predictive value of New LBBB 3. Describe the ST segment changes that are diagnostic of AMI
Foundations EKG I - Unit 1 Summary
 Foundations EKG I - Unit 1 Summary The accurate diagnosis of ST elevation myocardial infarction (STEMI) is one of the most time critical duties in the practice of EM. Diagnosis is not always easy so guidelines
Foundations EKG I - Unit 1 Summary The accurate diagnosis of ST elevation myocardial infarction (STEMI) is one of the most time critical duties in the practice of EM. Diagnosis is not always easy so guidelines
A few new tools for better detection and understanding of STEMIs in the field.
 A few new tools for better detection and understanding of STEMIs in the field. Let s talk, prep and placement. Try to shoot for quality, consistency and no artifact! (looking sometimes for 1 or 2 mm changes)
A few new tools for better detection and understanding of STEMIs in the field. Let s talk, prep and placement. Try to shoot for quality, consistency and no artifact! (looking sometimes for 1 or 2 mm changes)
Myocardial Infarction. Reading Assignment (p66-78 in Outline )
") Myocardial Infarction Reading Assignment (p66-78 in Outline ) Objectives 1. Why do ST segments go up or down in ischemia? 2. STEMI locations and culprit vessels 3. Why 15-lead ECGs? 4. What s up with avr?
Myocardial Infarction Reading Assignment (p66-78 in Outline ) Objectives 1. Why do ST segments go up or down in ischemia? 2. STEMI locations and culprit vessels 3. Why 15-lead ECGs? 4. What s up with avr?
12 Lead ECG. Presented by Rebecca Sevigny BSN, RN Professional Practice & Development Dept.
 12 Lead ECG Presented by Rebecca Sevigny BSN, RN Professional Practice & Development Dept. Two Main Coronary Arteries RCA LCA which branches into Left Anterior Descending Circumflex Artery Two Main Coronary
12 Lead ECG Presented by Rebecca Sevigny BSN, RN Professional Practice & Development Dept. Two Main Coronary Arteries RCA LCA which branches into Left Anterior Descending Circumflex Artery Two Main Coronary
Masqueraders of STEMI
 Masqueraders of STEMI Steven M. Costa, M.D. Assistant Professor Department of Medicine Division of Cardiology Scott & White Memorial Hospital and Clinic Texas A&M University Health Science Center Disclosures
Masqueraders of STEMI Steven M. Costa, M.D. Assistant Professor Department of Medicine Division of Cardiology Scott & White Memorial Hospital and Clinic Texas A&M University Health Science Center Disclosures
12 LEAD EKG BASICS. By: Steven Jones, NREMT P CLEMC
 12 LEAD EKG BASICS By: Steven Jones, NREMT P CLEMC ECG Review Waves and Intervals P wave: the sequential activation (depolarization) of the right and left atria QRS complex: right and left ventricular
12 LEAD EKG BASICS By: Steven Jones, NREMT P CLEMC ECG Review Waves and Intervals P wave: the sequential activation (depolarization) of the right and left atria QRS complex: right and left ventricular
12 Lead Acquisition and Interpretation APRIL 23 11:00 AM
 12 Lead Acquisition and Interpretation APRIL 23 11:00 AM Presented by : Jennifer Robson, Prehospital Care Specialist Dr. Don Eby, Local Medical Director Objectives Upon completion of this webinar, you
12 Lead Acquisition and Interpretation APRIL 23 11:00 AM Presented by : Jennifer Robson, Prehospital Care Specialist Dr. Don Eby, Local Medical Director Objectives Upon completion of this webinar, you
3/4/2018. March Martina Frost, PA C Desert Cardiology. Electricity moving towards/away from electrode create downward/upward directions of waves
 March 2018 Martina Frost, PA C Desert Cardiology Electricity moving towards/away from electrode create downward/upward directions of waves Frontal view Limb leads: I, II, III, avl, avf, (avr) Horizontal
March 2018 Martina Frost, PA C Desert Cardiology Electricity moving towards/away from electrode create downward/upward directions of waves Frontal view Limb leads: I, II, III, avl, avf, (avr) Horizontal
Cardiac Ischemia ECG Workshop
 Cardiac Ischemia ECG Workshop Classic, Confusing, and Confounding Patterns Amal Mattu, MD, NE Professor and Vice Chair Department of Emergency Medicine University of Maryland School of Medicine amalmattu@comcast.net
Cardiac Ischemia ECG Workshop Classic, Confusing, and Confounding Patterns Amal Mattu, MD, NE Professor and Vice Chair Department of Emergency Medicine University of Maryland School of Medicine amalmattu@comcast.net
Section V. Objectives
 Section V Landscape of an MI Objectives At the conclusion of this presentation the participant will be able to Outline a systematic approach to 12 lead ECG interpretation Demonstrate the process for determining
Section V Landscape of an MI Objectives At the conclusion of this presentation the participant will be able to Outline a systematic approach to 12 lead ECG interpretation Demonstrate the process for determining
Hot Topics in Cardiac Arrest. Should the patient go To the Cath Lab?
 Hot Topics in Cardiac Arrest Should the patient go To the Cath Lab? Tim Russert 1950-2008 Host of NBC s Meet the Press Sudden Cardiac Arrest : Autopsy showed plaque rupture in his LAD ( per LA Times,
Hot Topics in Cardiac Arrest Should the patient go To the Cath Lab? Tim Russert 1950-2008 Host of NBC s Meet the Press Sudden Cardiac Arrest : Autopsy showed plaque rupture in his LAD ( per LA Times,
Diagnosis of Myocardial Infarction/Ischemia with Bundle Branch Blocks
 Diagnosis of Myocardial Infarction/Ischemia with Bundle Branch Blocks Mark I. Langdorf, MD, MHPE, FACEP, FAAEM, RDMS Professor and Chair Associate Residency Director Department of Emergency Medicine University
Diagnosis of Myocardial Infarction/Ischemia with Bundle Branch Blocks Mark I. Langdorf, MD, MHPE, FACEP, FAAEM, RDMS Professor and Chair Associate Residency Director Department of Emergency Medicine University
Family Medicine for English language students of Medical University of Lodz ECG. Jakub Dorożyński
 Family Medicine for English language students of Medical University of Lodz ECG Jakub Dorożyński Parts of an ECG The standard ECG has 12 leads: six of them are considered limb leads because they are placed
Family Medicine for English language students of Medical University of Lodz ECG Jakub Dorożyński Parts of an ECG The standard ECG has 12 leads: six of them are considered limb leads because they are placed
12 Lead Interpretation
 12 Lead Interpretation Objectives Ischemia, injury and infarction ECG complex review J point ST segment STEMI recognition Ischemia to Infarct Infarction is an evolving process As the infarct evolves ECG
12 Lead Interpretation Objectives Ischemia, injury and infarction ECG complex review J point ST segment STEMI recognition Ischemia to Infarct Infarction is an evolving process As the infarct evolves ECG
Pennsylvania Academy of Family Physicians Foundation & UPMC 43rd Refresher Course in Family Medicine CME Conference March 10-13, 2016
 Pennsylvania Academy of Family Physicians Foundation & UPMC 43rd Refresher Course in Family Medicine CME Conference March 10-13, 2016 Disclosures: EKG Workshop Louis Mancano, MD Speaker has no disclosures
Pennsylvania Academy of Family Physicians Foundation & UPMC 43rd Refresher Course in Family Medicine CME Conference March 10-13, 2016 Disclosures: EKG Workshop Louis Mancano, MD Speaker has no disclosures
also aid the clinician in recognizing both the obvious and subtle abnormalities that may help guide therapy.
 Karen Lieberman, MS, CRNP f the many diagnostic tools used to screen for and evaluate cardiac abnormalities, the 12-lead electrocardiogram (ECG) is among the most basic. This inexpensive and noninvasive
Karen Lieberman, MS, CRNP f the many diagnostic tools used to screen for and evaluate cardiac abnormalities, the 12-lead electrocardiogram (ECG) is among the most basic. This inexpensive and noninvasive
Acute Coronary Syndromes. Disclosures
 Acute Coronary Syndromes Disclosures I work for Virginia Garcia Memorial Health Center, Beaverton, OR. Jon Tardiff, BS, PA-C OHSU Clinical Assistant Professor And I am a medical editor for Jones & Bartlett
Acute Coronary Syndromes Disclosures I work for Virginia Garcia Memorial Health Center, Beaverton, OR. Jon Tardiff, BS, PA-C OHSU Clinical Assistant Professor And I am a medical editor for Jones & Bartlett
The Fundamentals of 12 Lead EKG. ECG Recording. J Point. Reviewing the Cardiac Conductive System. Dr. E. Joe Sasin, MD Rusty Powers, NRP
 The Fundamentals of 12 Lead EKG Dr. E. Joe Sasin, MD Rusty Powers, NRP SA Node Intranodal Pathways AV Junction AV Fibers Bundle of His Septum Bundle Branches Purkinje System Reviewing the Cardiac Conductive
The Fundamentals of 12 Lead EKG Dr. E. Joe Sasin, MD Rusty Powers, NRP SA Node Intranodal Pathways AV Junction AV Fibers Bundle of His Septum Bundle Branches Purkinje System Reviewing the Cardiac Conductive
DR QAZI IMTIAZ RASOOL OBJECTIVES
 PRACTICAL ELECTROCARDIOGRAPHY DR QAZI IMTIAZ RASOOL OBJECTIVES Recording of electrical events in heart Established electrode pattern results in specific tracing pattern Health of heart i. e. Anatomical
PRACTICAL ELECTROCARDIOGRAPHY DR QAZI IMTIAZ RASOOL OBJECTIVES Recording of electrical events in heart Established electrode pattern results in specific tracing pattern Health of heart i. e. Anatomical
INTERPRETAZIONE ECG NEL PAZIENTE CON SOSPETTO STEMI
 INTERPRETAZIONE ECG NEL PAZIENTE CON SOSPETTO STEMI Giacomo Veronese Scuola di Specializzazione Medicina d Emergenza e Urgenza Università Milano-Bicocca Siete d accordo se vi propongo per una relazione..
INTERPRETAZIONE ECG NEL PAZIENTE CON SOSPETTO STEMI Giacomo Veronese Scuola di Specializzazione Medicina d Emergenza e Urgenza Università Milano-Bicocca Siete d accordo se vi propongo per una relazione..
By the end of this lecture, you will be able to: Understand the 12 lead ECG in relation to the coronary circulation and myocardium Perform an ECG
 By the end of this lecture, you will be able to: Understand the 12 lead ECG in relation to the coronary circulation and myocardium Perform an ECG recording Identify the ECG changes that occur in the presence
By the end of this lecture, you will be able to: Understand the 12 lead ECG in relation to the coronary circulation and myocardium Perform an ECG recording Identify the ECG changes that occur in the presence
12 Lead EKG. The Basics
 12 Lead EKG The Basics Objectives Demonstrate proper 12 EKG lead placement Determine electrical axis Identify ST and T wave changes as they relate to myocardial ischemia Describe possible complications
12 Lead EKG The Basics Objectives Demonstrate proper 12 EKG lead placement Determine electrical axis Identify ST and T wave changes as they relate to myocardial ischemia Describe possible complications
ECG in coronary artery disease. By Sura Boonrat Central Chest Institute
 ECG in coronary artery disease By Sura Boonrat Central Chest Institute EKG P wave = Atrium activation PR interval QRS = Ventricle activation T wave= repolarization J-point EKG QT interval Abnormal repolarization
ECG in coronary artery disease By Sura Boonrat Central Chest Institute EKG P wave = Atrium activation PR interval QRS = Ventricle activation T wave= repolarization J-point EKG QT interval Abnormal repolarization
STAT 12 Lead ECG Workshop: Basics & ACS
 STAT 12 Lead ECG Workshop: Basics & ACS Part 2: Acute Coronary Syndrome WAYNE W RUPPERT, CVT, CCCC, NREMT-P Cardiovascular Coordinator Bayfront Health Seven Rivers Crystal River, Florida Interventional
STAT 12 Lead ECG Workshop: Basics & ACS Part 2: Acute Coronary Syndrome WAYNE W RUPPERT, CVT, CCCC, NREMT-P Cardiovascular Coordinator Bayfront Health Seven Rivers Crystal River, Florida Interventional
10 ECGs No Practitioner Can Afford to Miss. Objectives
 10 ECGs No Practitioner Can Afford to Miss Mary L. Dohrmann, MD Professor of Clinical Medicine Division of Cardiovascular Medicine University of Missouri School of Medicine No disclosures Objectives 1.
10 ECGs No Practitioner Can Afford to Miss Mary L. Dohrmann, MD Professor of Clinical Medicine Division of Cardiovascular Medicine University of Missouri School of Medicine No disclosures Objectives 1.
Preface: Wang s Viewpoints
 AHA/ACCF/HRS Recommendations for the Standardization and Interpretation of the Electrocardiogram: Part IV, Ischemia and Infarction Presented by: WANG, TZONG LUEN, MD, PhD, JM, FACC, FESC, FCAPSC Professor,
AHA/ACCF/HRS Recommendations for the Standardization and Interpretation of the Electrocardiogram: Part IV, Ischemia and Infarction Presented by: WANG, TZONG LUEN, MD, PhD, JM, FACC, FESC, FCAPSC Professor,
REtrive. REpeat. RElearn Design by. Test-Enhanced Learning based ECG practice E-book
 Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning based ECG practice E-book REtrive REpeat RElearn Design by S I T T I N U N T H A N G J U I P E E R I Y A W A
Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning based ECG practice E-book REtrive REpeat RElearn Design by S I T T I N U N T H A N G J U I P E E R I Y A W A
Chapter 76 Acute Coronary Syndromes Part A
 Chapter 76 Acute Coronary Syndromes Part A Episode Overview: 1. Define Stable Angina, UA, AMI 2. Describe the pathophysiology of AMI 3. What are the components of prehospital management of AMI 4. List
Chapter 76 Acute Coronary Syndromes Part A Episode Overview: 1. Define Stable Angina, UA, AMI 2. Describe the pathophysiology of AMI 3. What are the components of prehospital management of AMI 4. List
NEBRASKA STEMI CONFERENCE 2015 Dr. Doug Kosmicki. 2013, American Heart Association
 NEBRASKA STEMI CONFERENCE 2015 Dr. Doug Kosmicki 2013, American Heart Association 1 Dr. Doug Kosmicki Reperfusion Strategies Disclosure Information Report any disclosure information of conflicts of interest.
NEBRASKA STEMI CONFERENCE 2015 Dr. Doug Kosmicki 2013, American Heart Association 1 Dr. Doug Kosmicki Reperfusion Strategies Disclosure Information Report any disclosure information of conflicts of interest.
Angina Luis Tulloch, MD 03/27/2012
 Angina Luis Tulloch, MD 03/27/2012 Acute coronary syndromes ACS STE > 1 mm, new LBBB* Increased cardiac enzymes STEMI Yes Yes NSTEMI No Yes UA No No *Recognize Wellen s sign/syndrome, posterior wall MI,
Angina Luis Tulloch, MD 03/27/2012 Acute coronary syndromes ACS STE > 1 mm, new LBBB* Increased cardiac enzymes STEMI Yes Yes NSTEMI No Yes UA No No *Recognize Wellen s sign/syndrome, posterior wall MI,
12 Lead Electrocardiogram (ECG) PFN: SOMACL17. Terminal Learning Objective. References
 PFN: SOMACL17. Terminal Learning Objective. References") 12 Lead Electrocardiogram (ECG) PFN: SOMACL17 Slide 1 Terminal Learning Objective Action: Communicate knowledge of 12 Lead Electrocardiogram (ECG) Condition: Given a lecture in a classroom environment
12 Lead Electrocardiogram (ECG) PFN: SOMACL17 Slide 1 Terminal Learning Objective Action: Communicate knowledge of 12 Lead Electrocardiogram (ECG) Condition: Given a lecture in a classroom environment
12 Lead ECG Interpretation: Color Coding for MI s
 12 Lead ECG Interpretation: Color Coding for MI s Anna E. Story, RN, MS Director, Continuing Professional Education Critical Care Nurse Online Instructional Designer 2004 Anna Story 1 Objectives review
12 Lead ECG Interpretation: Color Coding for MI s Anna E. Story, RN, MS Director, Continuing Professional Education Critical Care Nurse Online Instructional Designer 2004 Anna Story 1 Objectives review
TOPICS IN EMERGENCY MEDICINE SEMI-FINAL
 RISK ASSESSMENT IN PATIENTS WITH CHEST PAIN Nora Goldschlager, M.D. FACP, FACC, FAHA, FHRS Cardiology - San Francisco General Hospital UCSF Disclosures: None 1 CHEST PAIN NOT DUE TO MYOCARDIAL ISCHEMIA
RISK ASSESSMENT IN PATIENTS WITH CHEST PAIN Nora Goldschlager, M.D. FACP, FACC, FAHA, FHRS Cardiology - San Francisco General Hospital UCSF Disclosures: None 1 CHEST PAIN NOT DUE TO MYOCARDIAL ISCHEMIA
Preface: Wang s Viewpoints
 AHA/ACCF/HRS Recommendations for the Standardization and Interpretation of the Electrocardiogram: Ischemia and Infarction 103.10.07 Presented by: WANG, TZONG LUEN, MD, PhD, JM, FACC, FESC, FCAPSC Professor,
AHA/ACCF/HRS Recommendations for the Standardization and Interpretation of the Electrocardiogram: Ischemia and Infarction 103.10.07 Presented by: WANG, TZONG LUEN, MD, PhD, JM, FACC, FESC, FCAPSC Professor,
Bundle Branch & Fascicular Blocks. Reading Assignment (p53-58 in Outline )
") Bundle Branch & Fascicular Blocks Reading Assignment (p53-58 in Outline ) Objectives 1. QRS analysis of Right and Left BBB 2. Uncomplicated vs complicated BBB 3. Diagnosis of RBBB with LAFB and LPFB 4.
Bundle Branch & Fascicular Blocks Reading Assignment (p53-58 in Outline ) Objectives 1. QRS analysis of Right and Left BBB 2. Uncomplicated vs complicated BBB 3. Diagnosis of RBBB with LAFB and LPFB 4.
Understanding basics of EKG
 Understanding basics of EKG By Alula A.(R III) www.le.ac.uk Topic for discussion Understanding of cellular electrophysiology Basics Rate Rhythm Axis Intervals P wave QRS ST/T wave Abnormal EKGs Understanding
Understanding basics of EKG By Alula A.(R III) www.le.ac.uk Topic for discussion Understanding of cellular electrophysiology Basics Rate Rhythm Axis Intervals P wave QRS ST/T wave Abnormal EKGs Understanding
Relax and Learn At the Farm 2012
 Relax and Learn At the Farm 2012 Session 2: 12 Lead ECG Fundamentals 101 Cynthia Webner DNP, RN, CCNS, CCRN-CMC, CHFN Though for Today Mastery is not something that strikes in an instant, like a thunderbolt,
Relax and Learn At the Farm 2012 Session 2: 12 Lead ECG Fundamentals 101 Cynthia Webner DNP, RN, CCNS, CCRN-CMC, CHFN Though for Today Mastery is not something that strikes in an instant, like a thunderbolt,
ECG CONVENTIONS AND INTERVALS
 1 ECG Waveforms and Intervals ECG waveforms labeled alphabetically P wave== represents atrial depolarization QRS complex=ventricular depolarization ST-T-U complex (ST segment, T wave, and U wave)== V repolarization.
1 ECG Waveforms and Intervals ECG waveforms labeled alphabetically P wave== represents atrial depolarization QRS complex=ventricular depolarization ST-T-U complex (ST segment, T wave, and U wave)== V repolarization.
REFERRAL HOSPITAL. The Importance of Door In Door Out Time DIDO
 REFERRAL HOSPITAL The Importance of Door In Door Out Time DIDO Jean Skonhovd,RN,BSN,MSAS Emergency Department Director Avera Heart Hospital of South Dakota Time to Treatment is critical for STEMI patients
REFERRAL HOSPITAL The Importance of Door In Door Out Time DIDO Jean Skonhovd,RN,BSN,MSAS Emergency Department Director Avera Heart Hospital of South Dakota Time to Treatment is critical for STEMI patients
ECG Basics Sonia Samtani 7/2017 UCI Resident Lecture Series
 ECG Basics Sonia Samtani 7/2017 UCI Resident Lecture Series Agenda I. Introduction II.The Conduction System III.ECG Basics IV.Cardiac Emergencies V.Summary The Conduction System Lead Placement avf Precordial
ECG Basics Sonia Samtani 7/2017 UCI Resident Lecture Series Agenda I. Introduction II.The Conduction System III.ECG Basics IV.Cardiac Emergencies V.Summary The Conduction System Lead Placement avf Precordial
ECG Workshop. Nezar Amir
 ECG Workshop Nezar Amir Myocardial Ischemia ECG Infarct ECG in STEMI is dynamic & evolving Common causes of ST shift Infarct Localisation Left main artery occlusion: o diffuse ST-depression with ST elevation
ECG Workshop Nezar Amir Myocardial Ischemia ECG Infarct ECG in STEMI is dynamic & evolving Common causes of ST shift Infarct Localisation Left main artery occlusion: o diffuse ST-depression with ST elevation
12 Lead ECG Skills: Building Confidence for Clinical Practice. Presented By: Cynthia Webner, BSN, RN, CCRN-CMC. Karen Marzlin, BSN, RN,CCRN-CMC
 12 Lead ECG Skills: Building Confidence for Clinical Practice NTI 2009 Preconference Session 803 Presented By: Karen Marzlin, BSN, RN,CCRN-CMC 1 12 Lead ECG Fundamentals: The Starting Place for Linking
12 Lead ECG Skills: Building Confidence for Clinical Practice NTI 2009 Preconference Session 803 Presented By: Karen Marzlin, BSN, RN,CCRN-CMC 1 12 Lead ECG Fundamentals: The Starting Place for Linking
12 Lead EKG Chapter 4 Worksheet
 Match the following using the word bank. 1. A form of arteriosclerosis in which the thickening and hardening of the vessels walls are caused by an accumulation of fatty deposits in the innermost lining
Match the following using the word bank. 1. A form of arteriosclerosis in which the thickening and hardening of the vessels walls are caused by an accumulation of fatty deposits in the innermost lining
15 th Sukaman Memorial Lecture ST Segment Elevation: New Electrocardiographic Insights in 2014
 DOI 10.7603/s40602-016-0006-3 ASEAN Heart Journal http://www.globalsciencejournals.com/journal/40602 Vol. 24, no.1, 98 105 (2016) ISSN: 2315-4551 15 th Sukaman Memorial Lecture ST Segment Elevation: New
DOI 10.7603/s40602-016-0006-3 ASEAN Heart Journal http://www.globalsciencejournals.com/journal/40602 Vol. 24, no.1, 98 105 (2016) ISSN: 2315-4551 15 th Sukaman Memorial Lecture ST Segment Elevation: New
THE emergency physician (EP), frequently the
, frequently the") 1256 ST-SEGMENT ELEVATION Brady et al. INTERPRETATION OF ST-SEGMENT ELEVATION Errors in Emergency Physician Interpretation of ST-segment Elevation in Emergency Department Chest Pain Patients WILLIAM J.
1256 ST-SEGMENT ELEVATION Brady et al. INTERPRETATION OF ST-SEGMENT ELEVATION Errors in Emergency Physician Interpretation of ST-segment Elevation in Emergency Department Chest Pain Patients WILLIAM J.
Acute chest pain and ECG need for immediate coronary angiography?
 Acute chest pain and ECG need for immediate coronary angiography? Kjell Nikus, MD, PhD Heart Center, Tampere University Hospital, Finland and Samuel Sclarovsky, MD, PhD Tel Aviv University, Israel There
Acute chest pain and ECG need for immediate coronary angiography? Kjell Nikus, MD, PhD Heart Center, Tampere University Hospital, Finland and Samuel Sclarovsky, MD, PhD Tel Aviv University, Israel There
ECG pre-reading manual. Created for the North West Regional EMET training program
 ECG pre-reading manual Created for the North West Regional EMET training program Author:- Dr Juan Carlos Ascencio-Lane juan.ascencio-lane@ths.tas.gov.au 1 Disclaimer This handbook has been created for
ECG pre-reading manual Created for the North West Regional EMET training program Author:- Dr Juan Carlos Ascencio-Lane juan.ascencio-lane@ths.tas.gov.au 1 Disclaimer This handbook has been created for
Acute Coronary Syndrome. Emergency Department Updated Jan. 2017
 Acute Coronary Syndrome Emergency Department Updated Jan. 2017 Goals and Objectives To reduce mortality and morbidity for people who have cardiovascular disease, with a focus on those who experience an
Acute Coronary Syndrome Emergency Department Updated Jan. 2017 Goals and Objectives To reduce mortality and morbidity for people who have cardiovascular disease, with a focus on those who experience an
Part One Objectives. Don t Worry About It. All done for you Paper Speed 25 mm/sec Calibration 1 mv charge over 20 ms = 10 mm tall Lincoln Hat
 12-lead and ACS Review North Lyon Refresher Part One Objectives 12 lead ECG Basics Anatomy and Physiology STEMI Diagnosis Types of MI ACS Review STEMI System and Interventional Cardiology Review The Value
12-lead and ACS Review North Lyon Refresher Part One Objectives 12 lead ECG Basics Anatomy and Physiology STEMI Diagnosis Types of MI ACS Review STEMI System and Interventional Cardiology Review The Value
Ekg pra pr c a tice D.HAMMOUDI.MD
 Ekg practice D.HAMMOUDI.MD Anatomy Revisited RCA (Right Coronary Artery) Right ventricle Inferior wall of LV Posterior wall of LV (75%) SA Node (60%) AV Node (>80%) LCA (Left Coronary Artery) Septal wall
Ekg practice D.HAMMOUDI.MD Anatomy Revisited RCA (Right Coronary Artery) Right ventricle Inferior wall of LV Posterior wall of LV (75%) SA Node (60%) AV Node (>80%) LCA (Left Coronary Artery) Septal wall
2/7/ LEAD ECG CASE STUDIES Lisa Riggs MSN, RN, ACNS-BC, CCRN-K CASE #1 WHAT ELSE WOULD YOU ASSESS? WHAT S YOUR DIAGNOSIS?
 12 LEAD ECG CASE STUDIES Lisa Riggs MSN, RN, ACNS-BC, CCRN-K CASE #1 31 y/o male is a direct admit from the physician s office with c/o chest pain and SOA WHAT ELSE WOULD YOU ASSESS? WHAT S YOUR DIAGNOSIS?
12 LEAD ECG CASE STUDIES Lisa Riggs MSN, RN, ACNS-BC, CCRN-K CASE #1 31 y/o male is a direct admit from the physician s office with c/o chest pain and SOA WHAT ELSE WOULD YOU ASSESS? WHAT S YOUR DIAGNOSIS?
2010 ACLS Guidelines. Primary goals of therapy for patients
 2010 ACLS Guidelines Part 10: Acute Coronary Syndrome Present : 內科 R1 鍾伯欣 Supervisor: F1 吳亮廷 991110 Primary goals of therapy for patients of ACS Reduce the amount of myocardial necrosis that occurs in
2010 ACLS Guidelines Part 10: Acute Coronary Syndrome Present : 內科 R1 鍾伯欣 Supervisor: F1 吳亮廷 991110 Primary goals of therapy for patients of ACS Reduce the amount of myocardial necrosis that occurs in
Chapter 3 for 12 Lead Training -Precourse-
 ONTARIO BASE HOSPITAL GROUP Chapter 3 for 12 Lead Training -Precourse- Ontario Base Hospital Group Education Subcommittee 2008 TIME IS MUSCLE ONTARIO BASE HOSPITAL GROUP Introduction and Purpose Introduction
ONTARIO BASE HOSPITAL GROUP Chapter 3 for 12 Lead Training -Precourse- Ontario Base Hospital Group Education Subcommittee 2008 TIME IS MUSCLE ONTARIO BASE HOSPITAL GROUP Introduction and Purpose Introduction
Mission: Lifeline EMS Recognition : FMC to Device < 90 Minutes Worksheet
 Mission: Lifeline EMS Recognition : FMC to Device < 90 Minutes Worksheet Did Pt. Receive PCI FMC to PCI < 90 Minutes Exclusions Documented Delay after hospital arrival (Refer to Page 4 in EMS Recognition
Mission: Lifeline EMS Recognition : FMC to Device < 90 Minutes Worksheet Did Pt. Receive PCI FMC to PCI < 90 Minutes Exclusions Documented Delay after hospital arrival (Refer to Page 4 in EMS Recognition
12 Lead ECGs: Ischemia, Injury & Infarction. Kevin Handke NRP, FP-C, CCP, CMTE STEMI Coordinator Flight Paramedic
 12 Lead ECGs: Ischemia, Injury & Infarction Kevin Handke NRP, FP-C, CCP, CMTE STEMI Coordinator Flight Paramedic None Disclosures Objectives Upon completion of this program the learner will be able to
12 Lead ECGs: Ischemia, Injury & Infarction Kevin Handke NRP, FP-C, CCP, CMTE STEMI Coordinator Flight Paramedic None Disclosures Objectives Upon completion of this program the learner will be able to
Office ECG Interpretation
 Office ECG Interpretation Jason Evanchan, DO Assistant Professor of Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical Center Outline of topics High risk ischemia T wave
Office ECG Interpretation Jason Evanchan, DO Assistant Professor of Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical Center Outline of topics High risk ischemia T wave
12-Lead ECG Interpretation. Kathy Kuznar, RN, ANP
 12-Lead ECG Interpretation Kathy Kuznar, RN, ANP The 12-Lead ECG Objectives Identify the normal morphology and features of the 12- lead ECG. Perform systematic analysis of the 12-lead ECG. Recognize abnormalities
12-Lead ECG Interpretation Kathy Kuznar, RN, ANP The 12-Lead ECG Objectives Identify the normal morphology and features of the 12- lead ECG. Perform systematic analysis of the 12-lead ECG. Recognize abnormalities
Observation Medicine ECG Instructor Workshop session 2 Serial 12 Lead ECG Interpretation
 American College of Cardiology 20 th Congress 2017 Observation Medicine ECG Instructor Workshop session 2 Serial 12 Lead ECG Interpretation Part 1 By: Wayne W Ruppert, CVT, CCCC, NREMT-P This curriculum
American College of Cardiology 20 th Congress 2017 Observation Medicine ECG Instructor Workshop session 2 Serial 12 Lead ECG Interpretation Part 1 By: Wayne W Ruppert, CVT, CCCC, NREMT-P This curriculum
ECG (MCQs) In the fundamental rules of the ECG all the following are right EXCEP:
 In the fundamental rules of the ECG all the following are right EXCEP:") ECG (MCQs) 2010 1- In the fundamental rules of the ECG all the following are right EXCEP: a- It is a biphasic record of myocardial action potential fluctuations. b- Deflection record occurs only during
ECG (MCQs) 2010 1- In the fundamental rules of the ECG all the following are right EXCEP: a- It is a biphasic record of myocardial action potential fluctuations. b- Deflection record occurs only during
ECG ABNORMALITIES D R. T AM A R A AL Q U D AH
 ECG ABNORMALITIES D R. T AM A R A AL Q U D AH When we interpret an ECG we compare it instantaneously with the normal ECG and normal variants stored in our memory; these memories are stored visually in
ECG ABNORMALITIES D R. T AM A R A AL Q U D AH When we interpret an ECG we compare it instantaneously with the normal ECG and normal variants stored in our memory; these memories are stored visually in
MICS OF MYOCARDIAL ISCHEMIA AND INFARCTION REVISED FOR LAS VEGAS
 ECG MIMICS OF MYOCARDIAL ISCHEMIA AND INFARCTION 102.06.05 Tzong-Luen Wang MD, PhD, JM, FESC, FACC Professor. Medical School, Fu-Jen Catholic University Chief, Emergency Department, Shin-Kong Wu Ho-Su
ECG MIMICS OF MYOCARDIAL ISCHEMIA AND INFARCTION 102.06.05 Tzong-Luen Wang MD, PhD, JM, FESC, FACC Professor. Medical School, Fu-Jen Catholic University Chief, Emergency Department, Shin-Kong Wu Ho-Su
Considerations about the polemic J point location
 Considerations about the polemic J point location V) The J-point of the electrocardiogram Approximate point of convergence between the end of QRS complex and the onset of ST segment. It is considered the
Considerations about the polemic J point location V) The J-point of the electrocardiogram Approximate point of convergence between the end of QRS complex and the onset of ST segment. It is considered the
Disclosures 1/25/2018. Mission: Quality Can Mission Lifeline Help Your Performance Improvement Program? None
 Mission: Quality Can Mission Lifeline Help Your Performance Improvement Program? Jeremy T Cushman, MD MS EMT-P FACEP FAEMS Associate Professor of Emergency Medicine and Public Health Sciences Chief, Division
Mission: Quality Can Mission Lifeline Help Your Performance Improvement Program? Jeremy T Cushman, MD MS EMT-P FACEP FAEMS Associate Professor of Emergency Medicine and Public Health Sciences Chief, Division
Electrocardiography for Healthcare Professionals
 Electrocardiography for Healthcare Professionals Kathryn A. Booth Thomas O Brien Chapter 10: Pacemaker Rhythms and Bundle Branch Block Learning Outcomes 10.1 Describe the various pacemaker rhythms. 10.2
Electrocardiography for Healthcare Professionals Kathryn A. Booth Thomas O Brien Chapter 10: Pacemaker Rhythms and Bundle Branch Block Learning Outcomes 10.1 Describe the various pacemaker rhythms. 10.2
Παύλος Στουγιάννος. Καρδιολόγος ΓΝΑ «Η ΕΛΠΙΣ»
 Επεμβατική Καρδιολογία. STEMI. Σύγχρονη θεώρηση Παύλος Στουγιάννος Καρδιολόγος ΓΝΑ «Η ΕΛΠΙΣ» Criteria for acute myocardial infarction Thygesen K, et al. Third universal definition of myocardial infarction.
Επεμβατική Καρδιολογία. STEMI. Σύγχρονη θεώρηση Παύλος Στουγιάννος Καρδιολόγος ΓΝΑ «Η ΕΛΠΙΣ» Criteria for acute myocardial infarction Thygesen K, et al. Third universal definition of myocardial infarction.
Electrocardiography. Hilal Al Saffar College of Medicine,Baghdad University
 Electrocardiography Hilal Al Saffar College of Medicine,Baghdad University Which of the following is True 1. PR interval, represent the time taken for the impulse to travel from SA node to AV nose. 2.
Electrocardiography Hilal Al Saffar College of Medicine,Baghdad University Which of the following is True 1. PR interval, represent the time taken for the impulse to travel from SA node to AV nose. 2.
Comments or Questions? me:
 Comments or Questions? Email me: amalmattu@comcast.net Interested in short video tutorials on electrocardiography? Check out www.ecgweekly.com Subscription fee < cost of a cup of coffee/week Covers every
Comments or Questions? Email me: amalmattu@comcast.net Interested in short video tutorials on electrocardiography? Check out www.ecgweekly.com Subscription fee < cost of a cup of coffee/week Covers every
Please check your answers with correct statements in answer pages after the ECG cases.
 ECG Cases ECG Case 1 Springer International Publishing AG, part of Springer Nature 2018 S. Okutucu, A. Oto, Interpreting ECGs in Clinical Practice, In Clinical Practice, https://doi.org/10.1007/978-3-319-90557-0
ECG Cases ECG Case 1 Springer International Publishing AG, part of Springer Nature 2018 S. Okutucu, A. Oto, Interpreting ECGs in Clinical Practice, In Clinical Practice, https://doi.org/10.1007/978-3-319-90557-0
General Introduction to ECG. Reading Assignment (p2-16 in PDF Outline )
") General Introduction to ECG Reading Assignment (p2-16 in PDF Outline ) Objectives 1. Practice the 5-step Method 2. Differential Diagnosis: R & L axis deviation 3. Differential Diagnosis: Poor R-wave progression
General Introduction to ECG Reading Assignment (p2-16 in PDF Outline ) Objectives 1. Practice the 5-step Method 2. Differential Diagnosis: R & L axis deviation 3. Differential Diagnosis: Poor R-wave progression
ACUTE CORONARY SYNDROME
 12 LEAD ECG INTERPRETATION in ACUTE CORONARY SYNDROME WAYNE W RUPPERT, CVT, CCCC, NREMT-P Cardiovascular Clinical Coordinator Bayfront Health Seven Rivers Crystal River, FL Education Specialist St. Joseph
12 LEAD ECG INTERPRETATION in ACUTE CORONARY SYNDROME WAYNE W RUPPERT, CVT, CCCC, NREMT-P Cardiovascular Clinical Coordinator Bayfront Health Seven Rivers Crystal River, FL Education Specialist St. Joseph
FLB s What Are Those Funny-Looking Beats?
 FLB s What Are Those Funny-Looking Beats? Reading Assignment (pages 27-45 in Outline ) The 5-Step Method ECG #: Mearurements: Rhythm (s): Conduction: Waveform: Interpretation: A= V= PR= QRS= QT= Axis=
FLB s What Are Those Funny-Looking Beats? Reading Assignment (pages 27-45 in Outline ) The 5-Step Method ECG #: Mearurements: Rhythm (s): Conduction: Waveform: Interpretation: A= V= PR= QRS= QT= Axis=
Basic electrocardiography reading. R3 lee wei-chieh
 Basic electrocardiography reading R3 lee wei-chieh The Normal Conduction System Lead Placement avf Limb Leads Precordial Leads Interpretation Rate Rhythm Interval Axis Chamber abnormality QRST change What
Basic electrocardiography reading R3 lee wei-chieh The Normal Conduction System Lead Placement avf Limb Leads Precordial Leads Interpretation Rate Rhythm Interval Axis Chamber abnormality QRST change What
Electrocardiogram ECG. Hilal Al Saffar FRCP FACC College of medicine,baghdad University
 Electrocardiogram ECG Hilal Al Saffar FRCP FACC College of medicine,baghdad University Tuesday 29 October 2013 ECG introduction Wednesday 30 October 2013 Abnormal ECG ( ischemia, chamber hypertrophy, heart
Electrocardiogram ECG Hilal Al Saffar FRCP FACC College of medicine,baghdad University Tuesday 29 October 2013 ECG introduction Wednesday 30 October 2013 Abnormal ECG ( ischemia, chamber hypertrophy, heart
The Electrocardiogram part II. Dr. Adelina Vlad, MD PhD
 The Electrocardiogram part II Dr. Adelina Vlad, MD PhD Basic Interpretation of the ECG 1) Evaluate calibration 2) Calculate rate 3) Determine rhythm 4) Determine QRS axis 5) Measure intervals 6) Analyze
The Electrocardiogram part II Dr. Adelina Vlad, MD PhD Basic Interpretation of the ECG 1) Evaluate calibration 2) Calculate rate 3) Determine rhythm 4) Determine QRS axis 5) Measure intervals 6) Analyze
The Window for Fibrinolysis. Frans Van de Werf, MD, PhD Leuven, Belgium
 The Window for Fibrinolysis Frans Van de Werf, MD, PhD Leuven, Belgium ESC STEMI Guidelines : December 2008 Reperfusion Therapy: Fibrinolytic Therapy Recommendations Class LOE In the absence of contraindications
The Window for Fibrinolysis Frans Van de Werf, MD, PhD Leuven, Belgium ESC STEMI Guidelines : December 2008 Reperfusion Therapy: Fibrinolytic Therapy Recommendations Class LOE In the absence of contraindications
12 Lead ECG Interpretation: The Basics and Beyond
 12 Lead ECG Interpretation: The Basics and Beyond Cindy Weston, DNP, RN, CCRN, CNS-CC, FNP-BC Assistant Professor Texas A&M University College of Nursing cweston@tamhsc.edu Objectives Review the basics
12 Lead ECG Interpretation: The Basics and Beyond Cindy Weston, DNP, RN, CCRN, CNS-CC, FNP-BC Assistant Professor Texas A&M University College of Nursing cweston@tamhsc.edu Objectives Review the basics
2017 EKG Workshop Advanced. Family Medicine Review Course Lou Mancano, MD, FAAFP Reading Health System Family and Community Medicine Reading, PA
 2017 EKG Workshop Advanced Family Medicine Review Course Lou Mancano, MD, FAAFP Reading Health System Family and Community Medicine Reading, PA Part II - Objective Describe a useful approach to interpreting
2017 EKG Workshop Advanced Family Medicine Review Course Lou Mancano, MD, FAAFP Reading Health System Family and Community Medicine Reading, PA Part II - Objective Describe a useful approach to interpreting
Paediatric ECG Interpretation
 Paediatric ECG Interpretation Dr Sanj Fernando (thanks to http://lifeinthefastlane.com/ecg-library/paediatric-ecginterpretation/) 3 yo boy complaining of abdominal pain and chest pain Child ECG vs Adult
Paediatric ECG Interpretation Dr Sanj Fernando (thanks to http://lifeinthefastlane.com/ecg-library/paediatric-ecginterpretation/) 3 yo boy complaining of abdominal pain and chest pain Child ECG vs Adult
Acute Coronary Syndromes
 Overview Acute Coronary Syndromes Rabeea Aboufakher, MD, FACC, FSCAI Section Chief of Cardiology Altru Health System Grand Forks, ND Epidemiology Pathophysiology Clinical features and diagnosis STEMI management
Overview Acute Coronary Syndromes Rabeea Aboufakher, MD, FACC, FSCAI Section Chief of Cardiology Altru Health System Grand Forks, ND Epidemiology Pathophysiology Clinical features and diagnosis STEMI management
2017 AHA/ACC Clinical Performance and Quality Measures for Adults With ST-Elevation and Non ST-Elevation Myocardial Infarction
 2017 AHA/ACC Clinical Performance and Quality Measures for Adults With ST-Elevation and Non ST-Elevation Myocardial Infarction Ramzi Khalil MD FACC Assistant Professor Allegheny Gen.Hospital AHN Speakers
2017 AHA/ACC Clinical Performance and Quality Measures for Adults With ST-Elevation and Non ST-Elevation Myocardial Infarction Ramzi Khalil MD FACC Assistant Professor Allegheny Gen.Hospital AHN Speakers
January 2019 Tracings
 Tracings Tracing 1 Tracing 4 Tracing 1 Answer Tracing 4 Answer Tracing 2 Tracing 5 Tracing 2 Answer Tracing 5 Answer Tracing 3 Tracing 6 Tracing 3 Answer Tracing 6 Answer Questions? Contact Dr. Nelson
Tracings Tracing 1 Tracing 4 Tracing 1 Answer Tracing 4 Answer Tracing 2 Tracing 5 Tracing 2 Answer Tracing 5 Answer Tracing 3 Tracing 6 Tracing 3 Answer Tracing 6 Answer Questions? Contact Dr. Nelson
ECG anatomy. V1- V4 principally cover the anteroseptum LAD infarct frequently involves V5 & V6
 Anterior STEMI Aims Recognise anterior STEMI and 3me infarcts Differen3ate from NSTEMI Understand successful reperfusion and need for rescue PCI Be aware of the various ECGs that mimic anterior infarc3on
Anterior STEMI Aims Recognise anterior STEMI and 3me infarcts Differen3ate from NSTEMI Understand successful reperfusion and need for rescue PCI Be aware of the various ECGs that mimic anterior infarc3on
12-Lead EKG Interpretation for the Primary Care Provider
 21 st Annual Southwestern Regional Nurse Practitioner Symposium July 26, 2009 12-Lead EKG Interpretation for the Primary Care Provider Fran Stier MSN, ANP-BC, ACNP-BC Heart Health Care LLC Show Low, AZ
21 st Annual Southwestern Regional Nurse Practitioner Symposium July 26, 2009 12-Lead EKG Interpretation for the Primary Care Provider Fran Stier MSN, ANP-BC, ACNP-BC Heart Health Care LLC Show Low, AZ
12 Lead ECG Interpretation
 12 Lead ECG Interpretation Julie Zimmerman, MSN, RN, CNS, CCRN Significant increase in mortality for every 15 minutes of delay! N Engl J Med 2007;357:1631-1638 Who should get a 12-lead ECG? Also include
12 Lead ECG Interpretation Julie Zimmerman, MSN, RN, CNS, CCRN Significant increase in mortality for every 15 minutes of delay! N Engl J Med 2007;357:1631-1638 Who should get a 12-lead ECG? Also include
Medical Management of Acute Coronary Syndrome: The roles of a noncardiologist. Norbert Lingling D. Uy, MD Professor of Medicine UERMMMCI
 Medical Management of Acute Coronary Syndrome: The roles of a noncardiologist physician Norbert Lingling D. Uy, MD Professor of Medicine UERMMMCI Outcome objectives of the discussion: At the end of the
Medical Management of Acute Coronary Syndrome: The roles of a noncardiologist physician Norbert Lingling D. Uy, MD Professor of Medicine UERMMMCI Outcome objectives of the discussion: At the end of the
Topic. Updates on Definition of Myocardial Infarction
 Topic Updates on Definition of Myocardial Infarction In the past, general consensus for MI? Definition of MI by WHO - Combination of 2 of 3 characteristics - 1. Typical Symptoms 2. Enzyme Rise 3. Typical
Topic Updates on Definition of Myocardial Infarction In the past, general consensus for MI? Definition of MI by WHO - Combination of 2 of 3 characteristics - 1. Typical Symptoms 2. Enzyme Rise 3. Typical
P atients presenting to the emergency department
 129 ORIGINAL ARTICLE The electrocardiographic differential diagnosis of ST segment depression T Pollehn, W J Brady, A D Perron, F Morris... The importance of the electrocardiographic differential diagnosis
129 ORIGINAL ARTICLE The electrocardiographic differential diagnosis of ST segment depression T Pollehn, W J Brady, A D Perron, F Morris... The importance of the electrocardiographic differential diagnosis
Objectives. Acute Coronary Syndromes; The Nuts and Bolts. Overview. Quick quiz.. How dose the plaque start?
 Objectives Acute Coronary Syndromes; The Nuts and Bolts Michael P. Gulseth, Pharm. D., BCPS Pharmacotherapy II Spring 2006 Compare and contrast pathophysiology of unstable angina (UA), non-st segment elevation
Objectives Acute Coronary Syndromes; The Nuts and Bolts Michael P. Gulseth, Pharm. D., BCPS Pharmacotherapy II Spring 2006 Compare and contrast pathophysiology of unstable angina (UA), non-st segment elevation
CASE 10. What would the ST segment of this ECG look like? On which leads would you see this ST segment change? What does the T wave represent?
 CASE 10 A 57-year-old man presents to the emergency center with complaints of chest pain with radiation to the left arm and jaw. He reports feeling anxious, diaphoretic, and short of breath. His past history
CASE 10 A 57-year-old man presents to the emergency center with complaints of chest pain with radiation to the left arm and jaw. He reports feeling anxious, diaphoretic, and short of breath. His past history
ECG Cases and Questions. Ashish Sadhu, MD, FHRS, FACC Electrophysiology/Cardiology
 ECG Cases and Questions Ashish Sadhu, MD, FHRS, FACC Electrophysiology/Cardiology 32 yo female Life Insurance Physical 56 yo male with chest pain Terminology Injury ST elevation Ischemia T wave inversion
ECG Cases and Questions Ashish Sadhu, MD, FHRS, FACC Electrophysiology/Cardiology 32 yo female Life Insurance Physical 56 yo male with chest pain Terminology Injury ST elevation Ischemia T wave inversion
A case of post myocardial infarction ventricular septal rupture CHRISTOFOROS KOBOROZOS, MD
 A case of post myocardial infarction ventricular septal rupture CHRISTOFOROS KOBOROZOS, MD NAVAL HOSPITAL OF ATHENS case presentation Female, 81yo Hx: diabetes mellitus, hypertension, chronic anaemia presented
A case of post myocardial infarction ventricular septal rupture CHRISTOFOROS KOBOROZOS, MD NAVAL HOSPITAL OF ATHENS case presentation Female, 81yo Hx: diabetes mellitus, hypertension, chronic anaemia presented
Name Authentication Date (Position or Committee) Quality & Patient Safety Steering. Meeting Minutes & 08/14 Committee
 Quality & Patient Safety Steering. Meeting Minutes & 08/14 Committee") Title: Document Number: Document Type: Affected Departments: Review Bodies: Revision/(Review) Dates: (Dates that included only a review, but no content 07/14 revision, are in parentheses) Effective Date:
Title: Document Number: Document Type: Affected Departments: Review Bodies: Revision/(Review) Dates: (Dates that included only a review, but no content 07/14 revision, are in parentheses) Effective Date:
Acute Coronary Syndrome
 Acute Coronary Syndrome Clinical Manifestation of CAD Silent Ischemia/asymptomatic Stable Angina Acute Coronary Syndrome (Non- STEMI/UA and STEMI) Arrhythmias Heart Failure Sudden Death Pain patterns with
Acute Coronary Syndrome Clinical Manifestation of CAD Silent Ischemia/asymptomatic Stable Angina Acute Coronary Syndrome (Non- STEMI/UA and STEMI) Arrhythmias Heart Failure Sudden Death Pain patterns with
Transfer in D2B. Scott D Friedman, MD FACC Medical Director, Cardiology Services Shore Health System of Maryland. The Problem
 Transfer in D2B Scott D Friedman, MD FACC Medical Director, Cardiology Services Shore Health System of Maryland The Problem NRMI-5: North Carolina, July 2003- June 2004 NC Nation Guidelines N 2,738 79,927
Transfer in D2B Scott D Friedman, MD FACC Medical Director, Cardiology Services Shore Health System of Maryland The Problem NRMI-5: North Carolina, July 2003- June 2004 NC Nation Guidelines N 2,738 79,927
UPDATE ON THE MANAGEMENTACUTE CORONARY SYNDROME. DR JULES KABAHIZI, Psc (Rwa) Lt Col CHIEF CONSULTANT RMH/KFH 28 JUNE18
 Lt Col CHIEF CONSULTANT RMH/KFH 28 JUNE18") UPDATE ON THE MANAGEMENTACUTE CORONARY SYNDROME DR JULES KABAHIZI, Psc (Rwa) Lt Col CHIEF CONSULTANT RMH/KFH 28 JUNE18 INTRODUCTION The clinical entities that comprise acute coronary syndromes (ACS)-ST-segment
UPDATE ON THE MANAGEMENTACUTE CORONARY SYNDROME DR JULES KABAHIZI, Psc (Rwa) Lt Col CHIEF CONSULTANT RMH/KFH 28 JUNE18 INTRODUCTION The clinical entities that comprise acute coronary syndromes (ACS)-ST-segment