How to use infliximab?
|
|
|
- Gwendoline Barton
- 5 years ago
- Views:
Transcription
1 How to use infliximab? Séverine Vermeire, MD, PhD Division of Gastroenterology University Hospital Gasthuisberg Leuven
2 The how to use infliximab rules Before starting IFX: try optimizing chances for response! Once response: maintain the efficacy! Avoid immunogenicity! When to stop?
3 The how to use infliximab rules Before starting IFX: try optimizing chances for response! Once response: maintain the efficacy! Avoid immunogenicity! When to stop?
4 Optimizing induction of remission 3 Dose Induction vs. Single Dose? 3 dose induction Single dose % pats. Responding P= Weeks Infusions Hanauer S et al; Lancet 2002; 359:
5 Optimizing induction of remission: cotreatment? p< response (%) Luminal CD Fistulising CD imunosuppressives no immunosuppressives Parsi et al; Gastroenterol 2002; 123: Arnott et al; APT. 2003;17:1451-7
6 Optimizing induction of remission: cotreatment? Vermeire S et al, Am J Gastroenterol 2002; 97:
7 Optimizing induction of remission: smoking 100 p< response (%) Luminal CD Fistulising CD Smokers Non smokers Parsi et al; Gastroenterology 2002; 123: Arnott et al; APT. 2003;17:1451-7
8 Conclusion: Predictive factors for response to infliximab Clinical Genetic Other Confirmed Concom immunosuppression Increased CRP Colonic disease Non Smoking Short duration of disease Not confirmed young age LTA haplotype ASCA/pANCA early age at onset FcGR III a-158 Non stricturing FasL-843 TUCAN Cys10* No impact Severity of disease TNF previous therapies NOD2/CARD15 previous resections
9 The how to use infliximab rules Before starting IFX: try optimizing chances for response! Once response: maintain the efficacy! Avoid immunogenicity! When to stop?
10 70 60 Initial Treatment Phase Retreatment Phase Responders at 8 weeks (n=73) % Responding Infliximab (n=37) Placebo (n=36) Week Infusions Most patients will need retreatment! Rutgeerts P, et al. Gastroenterology. 1999; 117:76-69
11
12 ACCENT II
13 which strategy is the best? 1. IFX episodic in monotherapy? 2. IFX episodic + IS? 3. IFX every 8 weeks in monotherapy? 4. IFX every eight weeks + IS? 5. IFX as bridge for IS? Main goal: maintain efficacy and avoid loss of response = optimize not immunize
14 Mouse antibody The problem of immunogenicity Humanized antibody Mouse sequences Chimeric antibody Human sequences

 Mouse")
 CDP870 (PEGylated)")
15 Mouse antibody The problem of immunogenicity Humanized antibody Chimeric antibody Infliximab (Remicade ) Mouse sequences Human sequences CDP571 (Humicade ) CDP870 (PEGylated) Adalimumab (Humira )
16 Antibodies to infliximab (ATI) (formerly HACA) % of Patients Antibody (+) 100% 80% 60% 40% 20% 0% N=125 61% Number of infusions Baert F-Noman M et al NEJM 2003; 348;
17 Duration of Response by ATI Days until subsequent Infusion P<0.001 Negative µg/ml µg/ml > 20 µg/ml [Antibodies to Infliximab] Baert F-Noman M et al NEJM 2003; 348;
18 ATI and Immunosuppressant Tx P<0.01 % of patients antibody (+) 100% 80% 60% 40% 20% 0% 43.0% n= 56 Taking Immunossuppressant 75.0% n= 69 Not taking Immunosuppressants Baert F-Noman M et al NEJM 2003; 348;
19 Infliximab and Immunosuppressant Tx Taking Immunosuppressants Not Taking Immunosuppressants Median serum concentration µg/ml Non-fistula Fistula Non-fistula Fistula Baert F-Noman M et al NEJM 2003; 348;
20 % of patients ATI and MTX or AZA? Does it matter? p = NS neg 73 pos inconcl No IS MTX AZA treatment group Noman M et al DDW 2004
21 ATI Formation and steroid pretreatment Farrell et al, Gastro 2003
22 which strategy is the best? 1. IFX episodic in monotherapy? NO 2. IFX episodic + IS? YES 3. IFX every 8 weeks in monotherapy? 4. IFX every eight weeks + IS? 5. IFX as bridge for IS?
23 which strategy is the best? 1. IFX episodic in monotherapy? NO 2. IFX episodic + IS? YES 3. IFX every 8 weeks in monotherapy? YES 4. IFX every eight weeks + IS? YES 5. IFX as bridge for IS? YES
24 Clinical Response Through Week 54 All Patients Including Episodic Retreatment 80 Proportion of Patients (%) Weeks from the Initial Infusion Single dose (n = 188) 5 mg/kg q 8 wks (n = 192) 10 mg/kg q 8 wks (n = 193) Hanauer S et al; Lancet 2002; 359:
25 Antibodies to Infliximab % of patients Overall No IS IS 0 Episodic Treatment 5 mg/kg q 8wks 10 mg/kg q 8wks Hanauer S et al. Clin Gastroenterol Hepatol. 2004;2: ACCENT I
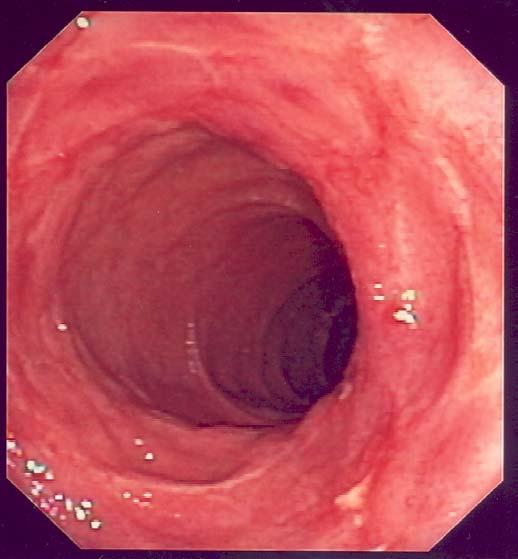
26 ACCENT I Infliximab: Endoscopic Healing Single dose Patients Demonstrating Endoscopic Healing (%) P=0.007 P= % 46% P= % 7% 0/17 10/32 1/14 5/11 8/15 Week 10 Week 54 Combined dose group (5 mg/kg & 10 mg/kg infliximab maintenance) 5 mg/kg infliximab maintenance 10 mg/kg infliximab maintenance Rutgeerts P et al. Gastroenterology. 2002;122(suppl):A-618

27
28
29 Fistulizing CD: time to loss of response at week 54 Patients without loss of response (%) Week 14 responders P<0.001 Induction Maintenance Weeks Episodic (n=99) Infliximab maintenance 5 mg/kg (n=96) Sands B et al; NEJM 2004;350:




30
31 Loss of response over time Step up to 10 mg/kg Shorten interval to less than 8 weeks Consider more humanized antibodies
32 IFX as a bridge for immunosuppressives Infliximab (Week 0, 2, 6) + AZA/MP Steroid dependence > 6 months Stratum 1 ( AZA failure ) AZA 2-3 mg/kg/d (or MP)> 6 mo continued Stratum 2 ( AZA naive ) AZA 2-2,5 mg/kg/d Steroid tapering standardized scheme increase of dose in case of relapse withdrawal if resistance to pred>40 mg/d for 2 wks Placebo (Week 0, 2, 6) + AZA/MP Week 24 End-point Week 52 Follow-up Lemann et al Gut Suppl 2003; 52: A44
33 Remission (CDAI<150) & off steroids 100% 80% 60% 40% 20% 0% P=0.009 P=0.03 P=0.02 P= % 64% 63% 50% 41% 34% 32% 26% Naive Failure Naive Failure Week 12 Week 24 AZA failure (n=56) AZA naive (n=59) Placebo week 0, 2, 6 + AZA/MP Infliximab 5 mg/kg week 0, 2, 6 + AZA/MP Lemann et al Gut 2003; 52: A44
34 Conclusion: optimizing IFX: induction of remission Consider 3-induction regimen (certainly for fistulizing CD) Give/optimize concomitant immunosuppressive therapy Advise patients to stop smoking
35 Conclusion: optimizing IFX: maintenance Eight-weekly IFX preferred over episodic strategy (less immunogenicity, better mucosal healing) Concomitant immunosuppression when episodic strategy is used Eight-weekly IFX for fistulizing CD (long term) Consider pretreatment with hydrocortisone How long to continue immunosuppressives when IFX is given eight-weekly? Consider step up dose to 10 mg/kg if loss of response over time More humanized antibodies for future
36 How long should we continue IFX? No controlled data beyond one year Experience from large centers up to 10 years Try to stop when treatment goal is reached: discontinuation of GCS with maintained remission complete external healing of fistulas continue with immunosuppressives Restart IFX when relapse Placebo-controlled IFX discontinuation study needed
Immunogenicity of Biologic Agents and How to Prevent Sensitization
 Immunogenicity of Biologic Agents and How to Prevent Sensitization William J. Sandborn, MD Professor and Chief, Division of Gastroenterology Director, UCSD IBD Center La Jolla, California, USA Learning
Immunogenicity of Biologic Agents and How to Prevent Sensitization William J. Sandborn, MD Professor and Chief, Division of Gastroenterology Director, UCSD IBD Center La Jolla, California, USA Learning
Indications for use of Infliximab
 Indications for use of Infliximab Moscow, June 10 th 2006 Prof. Dr. Dr. Gerhard Rogler Klinik und Poliklinik für Innere Medizin I Universität Regensburg Case report 1989: Diagnosis of Crohn s disease of
Indications for use of Infliximab Moscow, June 10 th 2006 Prof. Dr. Dr. Gerhard Rogler Klinik und Poliklinik für Innere Medizin I Universität Regensburg Case report 1989: Diagnosis of Crohn s disease of
Mucosal Healing in Crohn s Disease. Geert D Haens MD, PhD University Hospital Gasthuisberg University of Leuven Leuven, Belgium
 Mucosal Healing in Crohn s Disease Geert D Haens MD, PhD University Hospital Gasthuisberg University of Leuven Leuven, Belgium Mucosal Lesions in CD: General Features CD can affect the entire GI tract
Mucosal Healing in Crohn s Disease Geert D Haens MD, PhD University Hospital Gasthuisberg University of Leuven Leuven, Belgium Mucosal Lesions in CD: General Features CD can affect the entire GI tract
Position of Biologics in IBD Circa 2006: Top Down vs. Step Up Therapy
 Position of Biologics in IBD Circa 2006: Top Down vs. Step Up Therapy Stephen B. Hanauer, MD University of Chicago Potential Conflicts: Centocor/Schering, Abbott, UCB, Elan, Berlex, PDL Goals of Treatment
Position of Biologics in IBD Circa 2006: Top Down vs. Step Up Therapy Stephen B. Hanauer, MD University of Chicago Potential Conflicts: Centocor/Schering, Abbott, UCB, Elan, Berlex, PDL Goals of Treatment
How to Optimize Induction and Maintenance Responses: Definitions and Dosing Advances in Inflammatory Bowel Disease December 6, 2009
 How to Optimize Induction and Maintenance Responses: Definitions and Dosing 2009 Advances in Inflammatory Bowel Disease December 6, 2009 Fernando Velayos MD MPH University of California, San Francisco
How to Optimize Induction and Maintenance Responses: Definitions and Dosing 2009 Advances in Inflammatory Bowel Disease December 6, 2009 Fernando Velayos MD MPH University of California, San Francisco
Mono or Combination Therapy with. Individualized Approach
 Mono Combination Therapy with Biologics i in IBD: Developing an Individualized Approach David T. Rubin, MD, FACG Co-Direct, Inflammaty Bowel Disease Center Fellowship Program Direct University of Chicago
Mono Combination Therapy with Biologics i in IBD: Developing an Individualized Approach David T. Rubin, MD, FACG Co-Direct, Inflammaty Bowel Disease Center Fellowship Program Direct University of Chicago
Ali Keshavarzian MD Rush University Medical Center
 Treatment: Step Up or Top Down? Ali Keshavarzian MD Rush University Medical Center Questions What medication should IBD be treated with? Can we predict which patients with IBD are high risk? Is starting
Treatment: Step Up or Top Down? Ali Keshavarzian MD Rush University Medical Center Questions What medication should IBD be treated with? Can we predict which patients with IBD are high risk? Is starting
September 12, 2015 Millie D. Long MD, MPH, FACG
 Update on Biologic Therapy in 2015 September 12, 2015 Millie D. Long MD, MPH, FACG Assistant Professor of Medicine Inflammatory Bowel Disease Center University of North Carolina-Chapel Hill Outline Crohn
Update on Biologic Therapy in 2015 September 12, 2015 Millie D. Long MD, MPH, FACG Assistant Professor of Medicine Inflammatory Bowel Disease Center University of North Carolina-Chapel Hill Outline Crohn
An Update on the Biologic Treatment for Patients with Inflammatory Bowel Disease. David A. Schwartz, MD
 An Update on the Biologic Treatment for Patients with Inflammatory Bowel Disease David A. Schwartz, MD Director, Inflammatory Bowel Disease Center Associate Professor of Medicine Vanderbilt University
An Update on the Biologic Treatment for Patients with Inflammatory Bowel Disease David A. Schwartz, MD Director, Inflammatory Bowel Disease Center Associate Professor of Medicine Vanderbilt University
Personalized Medicine in IBD: Where Are We in 2013
 Personalized Medicine in IBD: Where Are We in 2013 David A. Schwartz, MD Director, Inflammatory Bowel Disease Center Associate Professor of Medicine Vanderbilt University Medical Center What is Personalized
Personalized Medicine in IBD: Where Are We in 2013 David A. Schwartz, MD Director, Inflammatory Bowel Disease Center Associate Professor of Medicine Vanderbilt University Medical Center What is Personalized
The advent of infliximab (Remicade; Centocor, Optimizing Anti-TNF Treatment in Inflammatory Bowel Disease
 GASTROENTEROLOGY 2004;126:1593 1610 Optimizing Anti-TNF Treatment in Inflammatory Bowel Disease PAUL RUTGEERTS, GERT VAN ASSCHE, and SÉVERINE VERMEIRE Department of Medicine, Division of Gastroenterology,
GASTROENTEROLOGY 2004;126:1593 1610 Optimizing Anti-TNF Treatment in Inflammatory Bowel Disease PAUL RUTGEERTS, GERT VAN ASSCHE, and SÉVERINE VERMEIRE Department of Medicine, Division of Gastroenterology,
Treatment Goals. Current Therapeutic Pyramids Crohn s Disease Ulcerative Colitis 11/14/10
 Current Management of IBD: From Conventional Agents to Biologics Stephen B. Hanauer, M.D. University of Chicago Treatment Goals Induce and maintain response/ remission Prevent complications Improve quality
Current Management of IBD: From Conventional Agents to Biologics Stephen B. Hanauer, M.D. University of Chicago Treatment Goals Induce and maintain response/ remission Prevent complications Improve quality
Azathioprine for Induction and Maintenance of Remission in Crohn s Disease
 Azathioprine for Induction and Maintenance of Remission in Crohn s Disease William J. Sandborn, MD Chief, Division of Gastroenterology Director, UCSD IBD Center Objectives Azathioprine as induction and
Azathioprine for Induction and Maintenance of Remission in Crohn s Disease William J. Sandborn, MD Chief, Division of Gastroenterology Director, UCSD IBD Center Objectives Azathioprine as induction and
Common Questions in Crohn s Disease Therapy. Case
 Common Questions in Crohn s Disease Therapy Jean-Paul Achkar, MD, FACG Kenneth Rainin Chair for IBD Research Cleveland Clinic Case 23 yo male with 1 year history of diarrhea, abdominal pain and 15 pound
Common Questions in Crohn s Disease Therapy Jean-Paul Achkar, MD, FACG Kenneth Rainin Chair for IBD Research Cleveland Clinic Case 23 yo male with 1 year history of diarrhea, abdominal pain and 15 pound
Anne Griffiths MD, FRCPC. SickKids Hospital, University of Toronto. Buenos Aires, August 16, 2014
 Management and Medical Therapies for Crohn disease: strategies to enhance mucosal healing Anne Griffiths MD, FRCPC SickKids Hospital, University of Toronto Buenos Aires, August 16, 2014 New onset Crohn
Management and Medical Therapies for Crohn disease: strategies to enhance mucosal healing Anne Griffiths MD, FRCPC SickKids Hospital, University of Toronto Buenos Aires, August 16, 2014 New onset Crohn
The Best of IBD at UEGW (Crohn s)
") The Best of IBD at UEGW (Crohn s) Iyad Issa MD Head of Gastroenterology, Rafik Hariri Univ Hosp Adjunct Faculty, School of Medicine, Leb Univ Founding Faculty, School Of Medicine, Leb Am Univ 1 The Best
The Best of IBD at UEGW (Crohn s) Iyad Issa MD Head of Gastroenterology, Rafik Hariri Univ Hosp Adjunct Faculty, School of Medicine, Leb Univ Founding Faculty, School Of Medicine, Leb Am Univ 1 The Best
Crohn's Disease. The What, When, and Why of Treatment
 Crohn's Disease The What, When, and Why of Treatment Brian Feagan, MD, FACG Professor of Medicine and Epidemiology and Biostatistics Director, Robarts Clinical Trials Robarts Research Institute University
Crohn's Disease The What, When, and Why of Treatment Brian Feagan, MD, FACG Professor of Medicine and Epidemiology and Biostatistics Director, Robarts Clinical Trials Robarts Research Institute University
Association Between Plasma Concentrations of Certolizumab Pegol and Endoscopic Outcomes of Patients With Crohn's Disease
 Association Between Plasma Concentrations of Certolizumab Pegol and Endoscopic Outcomes of Patients With Crohn's Disease Jean Frédéric Colombel, William J. Sandborn, Matthieu Allez, Jean Louis Dupas, Olivier
Association Between Plasma Concentrations of Certolizumab Pegol and Endoscopic Outcomes of Patients With Crohn's Disease Jean Frédéric Colombel, William J. Sandborn, Matthieu Allez, Jean Louis Dupas, Olivier
IBD Updates. Themes in IBD IBD management journey. New tools for therapeutic monitoring. First-line treatment in IBD
 IBD Updates Maria T. Abreu, MD University of Miami Miller School of Medicine Miami, Florida Themes in IBD 213 First-line treatment in IBD New tools for therapeutic monitoring Biologic therapy for CD and
IBD Updates Maria T. Abreu, MD University of Miami Miller School of Medicine Miami, Florida Themes in IBD 213 First-line treatment in IBD New tools for therapeutic monitoring Biologic therapy for CD and
CROHN'S DISEASE/ULCERATIVE COLITIS TREATMENT ALGORITHM
 CROHN'S DISEASE/ULCERATIVE COLITIS TREATMENT ALGORITHM Crohn's Disease Ulcerative Colitis Steroids x 2 No prior AZA/6-MP Biologic Agent AZA/6-MP STEP-UP MANAGEMENT APPROACH Advantages Patients attain remission
CROHN'S DISEASE/ULCERATIVE COLITIS TREATMENT ALGORITHM Crohn's Disease Ulcerative Colitis Steroids x 2 No prior AZA/6-MP Biologic Agent AZA/6-MP STEP-UP MANAGEMENT APPROACH Advantages Patients attain remission
Beyond Anti TNFs: positioning of other biologics for Crohn s disease. Christina Ha, MD Cedars Sinai Inflammatory Bowel Disease Center
 Beyond Anti TNFs: positioning of other biologics for Crohn s disease Christina Ha, MD Cedars Sinai Inflammatory Bowel Disease Center Objectives: To define high and low risk patient and disease features
Beyond Anti TNFs: positioning of other biologics for Crohn s disease Christina Ha, MD Cedars Sinai Inflammatory Bowel Disease Center Objectives: To define high and low risk patient and disease features
Update on Biologics in Ulcerative Colitis. Scott Plevy, MD University of North Carolina Chapel Hill, NC
 Update on Biologics in Ulcerative Colitis Scott Plevy, MD University of North Carolina Chapel Hill, NC Objectives Discuss the latest advances in the pharmacologic management of ulcerative colitis Describe
Update on Biologics in Ulcerative Colitis Scott Plevy, MD University of North Carolina Chapel Hill, NC Objectives Discuss the latest advances in the pharmacologic management of ulcerative colitis Describe
Positioning Biologics in Ulcerative Colitis
 Positioning Biologics in Ulcerative Colitis Bruce E. Sands, MD, MS Acting Chief, Gastrointestinal Unit Massachusetts General Hospital Associate Professor of Medicine Harvard Medical School Sequential Therapies
Positioning Biologics in Ulcerative Colitis Bruce E. Sands, MD, MS Acting Chief, Gastrointestinal Unit Massachusetts General Hospital Associate Professor of Medicine Harvard Medical School Sequential Therapies
John F. Valentine, MD Inflammatory Bowel Disease Program University of Utah
 John F. Valentine, MD Inflammatory Bowel Disease Program University of Utah Hawaii 1/20/2017 DISCLOSURES Research Support: NIH, Pfizer, Celgene, AbbVie, Roche/Genentech, Takeda, CCFA OBJECTIVES Review
John F. Valentine, MD Inflammatory Bowel Disease Program University of Utah Hawaii 1/20/2017 DISCLOSURES Research Support: NIH, Pfizer, Celgene, AbbVie, Roche/Genentech, Takeda, CCFA OBJECTIVES Review
INFLIXIMAB FOR PREVENTION OF POST-OPERATIVE CROHN S DISEASE RECURRENCE: THE PREVENT TRIAL
 INFLIXIMAB FOR PREVENTION OF POST-OPERATIVE CROHN S DISEASE RECURRENCE: THE PREVENT TRIAL A. Hillary Steinhart, MD MSc FRCP(C) Medical Lead, Mount Sinai Hospital IBD Centre Professor of Medicine University
INFLIXIMAB FOR PREVENTION OF POST-OPERATIVE CROHN S DISEASE RECURRENCE: THE PREVENT TRIAL A. Hillary Steinhart, MD MSc FRCP(C) Medical Lead, Mount Sinai Hospital IBD Centre Professor of Medicine University
Il ruolo degli anticorpi anti farmaco nella pratica clinica
 Il ruolo degli anticorpi anti farmaco nella pratica clinica Daniela Pugliese, MD IBD Unit Complesso Integrato Columbus Gemelli Hospital Catholic University Foundation, Rome - Italy Therapeutic Drug monitoring
Il ruolo degli anticorpi anti farmaco nella pratica clinica Daniela Pugliese, MD IBD Unit Complesso Integrato Columbus Gemelli Hospital Catholic University Foundation, Rome - Italy Therapeutic Drug monitoring
Therapy for Inflammatory Bowel Disease
 Therapy for Inflammatory Bowel Disease Jonathan P. Terdiman, MD Professor of Clinical Medicine Clinical Director, Center for Colitis and Crohn s Disease University of California San Francisco, CA UC: Current
Therapy for Inflammatory Bowel Disease Jonathan P. Terdiman, MD Professor of Clinical Medicine Clinical Director, Center for Colitis and Crohn s Disease University of California San Francisco, CA UC: Current
CCFA. Crohns Disease vs UC: What is the best treatment for me? November
 CCFA Crohns Disease vs UC: What is the best treatment for me? November 8 2009 Ellen J. Scherl,, MD, FACP,AGAF Roberts Inflammatory Bowel Disease Center Weill Medical College Cornell University New York
CCFA Crohns Disease vs UC: What is the best treatment for me? November 8 2009 Ellen J. Scherl,, MD, FACP,AGAF Roberts Inflammatory Bowel Disease Center Weill Medical College Cornell University New York
Initiation of Maintenance Treatment in Moderate to Severe New Onset Crohn s Disease
 Initiation of Maintenance Treatment in Moderate to Severe New Onset Crohn s Disease The Case for Starting with Anti-TNFα Agents Maria Oliva-Hemker, M.D. Chief, Division of Pediatric Gastroenterology &
Initiation of Maintenance Treatment in Moderate to Severe New Onset Crohn s Disease The Case for Starting with Anti-TNFα Agents Maria Oliva-Hemker, M.D. Chief, Division of Pediatric Gastroenterology &
Optimizing the effectiveness of anti-tnf therapy in paediatric IBD
 Optimizing the effectiveness of anti-tnf therapy in paediatric IBD Anne Griffiths MD, FRCPC Co-Lead, Inflammatory Bowel Disease Center Northbridge Chair in IBD Hospital for Sick Children, Professor of
Optimizing the effectiveness of anti-tnf therapy in paediatric IBD Anne Griffiths MD, FRCPC Co-Lead, Inflammatory Bowel Disease Center Northbridge Chair in IBD Hospital for Sick Children, Professor of
Levels of C-reactive Protein Are Associated With Response to Infliximab Therapy in Patients With Crohn s Disease
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2011;9:421 427 Levels of C-reactive Protein Are Associated With Response to Infliximab Therapy in Patients With Crohn s Disease MATTHIAS JÜRGENS,* JESTINAH M. MAHACHIE
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2011;9:421 427 Levels of C-reactive Protein Are Associated With Response to Infliximab Therapy in Patients With Crohn s Disease MATTHIAS JÜRGENS,* JESTINAH M. MAHACHIE
Crohn's Disease. The What, When, and Why of Treatment
 Crohn's Disease The What, When, and Why of Treatment Gary R. Lichtenstein, MD, FACG Professor of Medicine Director, Inflammatory Bowel Disease Program University of Pennsylvania Philadelphia, PA In my
Crohn's Disease The What, When, and Why of Treatment Gary R. Lichtenstein, MD, FACG Professor of Medicine Director, Inflammatory Bowel Disease Program University of Pennsylvania Philadelphia, PA In my
Selection and use of the non-anti- TNF biological therapies: Who? When? How?
 Selection and use of the non-anti- TNF biological therapies: Who? When? How? Asher Kornbluth, MD Clinical Professor of Medicine The Henry D. Janowitz Division of Gastroenterology The Icahn School of Medicine
Selection and use of the non-anti- TNF biological therapies: Who? When? How? Asher Kornbluth, MD Clinical Professor of Medicine The Henry D. Janowitz Division of Gastroenterology The Icahn School of Medicine
Withdrawal of drug therapy in patients with quiescent Crohn s disease
 Withdrawal of drug therapy in patients with quiescent Crohn s disease DR. JEAN-FRÉDÉRIC COLOMBEL DIRECTOR OF THE IBD CENTER, ICAHN SCHOOL OF MEDICINE AT MOUNT SINAI, NEW YORK, USA Withdrawal of drug therapy
Withdrawal of drug therapy in patients with quiescent Crohn s disease DR. JEAN-FRÉDÉRIC COLOMBEL DIRECTOR OF THE IBD CENTER, ICAHN SCHOOL OF MEDICINE AT MOUNT SINAI, NEW YORK, USA Withdrawal of drug therapy
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION. 3 October 2012
 The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 3 October 2012 REMICADE 100 mg, powder for concentrate for solution for infusion B/1 vial (CIP code: 562 070-1) Applicant:
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 3 October 2012 REMICADE 100 mg, powder for concentrate for solution for infusion B/1 vial (CIP code: 562 070-1) Applicant:
Personalized Medicine in IBD
 Personalized Medicine in IBD Anita Afzali MD, MPH Assistant Professor of Medicine Director, Inflammatory Bowel Diseases Program University of Washington Harborview Medical Center CCFA April 2 nd, 2016
Personalized Medicine in IBD Anita Afzali MD, MPH Assistant Professor of Medicine Director, Inflammatory Bowel Diseases Program University of Washington Harborview Medical Center CCFA April 2 nd, 2016
Tumor necrosis factor-alpha antibody for maintenace of remission in Crohn s disease (Review)
") Tumor necrosis factor-alpha antibody for maintenace of remission in Crohn s disease (Review) Behm BW, Bickston SJ This is a reprint of a Cochrane review, prepared and maintained by The Cochrane Collaboration
Tumor necrosis factor-alpha antibody for maintenace of remission in Crohn s disease (Review) Behm BW, Bickston SJ This is a reprint of a Cochrane review, prepared and maintained by The Cochrane Collaboration
Mucosal healing: does it really matter?
 Oxford Inflammatory Bowel Disease MasterClass Mucosal healing: does it really matter? Professor Jean-Frédéric Colombel, New York, USA Oxford Inflammatory Bowel Disease MasterClass Mucosal healing: does
Oxford Inflammatory Bowel Disease MasterClass Mucosal healing: does it really matter? Professor Jean-Frédéric Colombel, New York, USA Oxford Inflammatory Bowel Disease MasterClass Mucosal healing: does
Predicting the natural history of IBD. Séverine Vermeire, MD, PhD Department of Gastroenterology University Hospital Leuven Belgium
 Predicting the natural history of IBD Séverine Vermeire, MD, PhD Department of Gastroenterology University Hospital Leuven Belgium Patient 1 Patient 2 Age 22 Frequent cramps and diarrhea for 6 months Weight
Predicting the natural history of IBD Séverine Vermeire, MD, PhD Department of Gastroenterology University Hospital Leuven Belgium Patient 1 Patient 2 Age 22 Frequent cramps and diarrhea for 6 months Weight
Fistulizing Crohn s Disease: The Aggressive Approach
 Fistulizing Crohn s Disease: The Aggressive Approach Bruce E. Sands, MD, MS MGH Crohn s and Colitis Center and Gastrointestinal Unit Massachusetts General Hospital Boston, USA Case Presentation: Summary
Fistulizing Crohn s Disease: The Aggressive Approach Bruce E. Sands, MD, MS MGH Crohn s and Colitis Center and Gastrointestinal Unit Massachusetts General Hospital Boston, USA Case Presentation: Summary
Severe IBD: What to Do When Anti- TNFs Don t Work?
 Severe IBD: What to Do When Anti- TNFs Don t Work? David T. Rubin, MD, FACG Professor of Medicine Co-Director, Inflammatory Bowel Disease Center Interim Chief, Section of Gastroenterology, Hepatology and
Severe IBD: What to Do When Anti- TNFs Don t Work? David T. Rubin, MD, FACG Professor of Medicine Co-Director, Inflammatory Bowel Disease Center Interim Chief, Section of Gastroenterology, Hepatology and
Highlights of DDW 2015: Crohn s disease
 Highlights of DDW 2015: Crohn s disease Mark S. Silverberg, MD, PhD, FRCPC Associate Professor of Medicine, University of Toronto Staff Gastroenterologist, Mount Sinai Hospital Senior Investigator, Lunenfeld-Tanenbaum
Highlights of DDW 2015: Crohn s disease Mark S. Silverberg, MD, PhD, FRCPC Associate Professor of Medicine, University of Toronto Staff Gastroenterologist, Mount Sinai Hospital Senior Investigator, Lunenfeld-Tanenbaum
Drug Level Monitoring in IBD. Objectives
 Drug Level Monitoring in IBD Corey A. Siegel, MD, MS Director, Dartmouth-Hitchcock IBD Center Associate Professor of Medicine, Geisel School of Medicine at Dartmouth Objectives Review non-biologic drug
Drug Level Monitoring in IBD Corey A. Siegel, MD, MS Director, Dartmouth-Hitchcock IBD Center Associate Professor of Medicine, Geisel School of Medicine at Dartmouth Objectives Review non-biologic drug
Latest Treatment Updates for Crohn s Disease: Tailoring Therapy David G. Binion, M.D.
 Latest Treatment Updates for Crohn s Disease: Tailoring Therapy David G. Binion, M.D. Co-Director, IBD Center Director, Nutrition Support Service UPMC Presbyterian Hospital Division of Gastroenterology,
Latest Treatment Updates for Crohn s Disease: Tailoring Therapy David G. Binion, M.D. Co-Director, IBD Center Director, Nutrition Support Service UPMC Presbyterian Hospital Division of Gastroenterology,
Recent Advances in the Management of Refractory IBD
 Recent Advances in the Management of Refractory IBD Raina Shivashankar, M.D. Assistant Professor of Medicine Division of Gastroenterology and Hepatology Thomas Jefferson University Philadelphia, PA Outline
Recent Advances in the Management of Refractory IBD Raina Shivashankar, M.D. Assistant Professor of Medicine Division of Gastroenterology and Hepatology Thomas Jefferson University Philadelphia, PA Outline
Efficacy and Safety of Treatment for Pediatric IBD
 Efficacy and Safety of Treatment for Pediatric IBD Andrew B. Grossman MD Co-Director, Center for Pediatric Inflammatory Bowel Disease Assistant Professor of Clinical Pediatrics Division of Gastroenterology,
Efficacy and Safety of Treatment for Pediatric IBD Andrew B. Grossman MD Co-Director, Center for Pediatric Inflammatory Bowel Disease Assistant Professor of Clinical Pediatrics Division of Gastroenterology,
Endpoints for Stopping Treatment in UC
 Endpoints for Stopping Treatment in UC Jana G. Hashash, MD Assistant Professor of Medicine Inflammatory Bowel Disease Center Division of Gastroenterology, Hepatology, and Nutrition University of Pittsburgh
Endpoints for Stopping Treatment in UC Jana G. Hashash, MD Assistant Professor of Medicine Inflammatory Bowel Disease Center Division of Gastroenterology, Hepatology, and Nutrition University of Pittsburgh
Disclosures. What Do I Do When Anti-TNF Therapy Is Not Working Anymore? Fadi Hamid, M.D. Saint Luke s GI Specialists
 What Do I Do When Anti-TNF Therapy Is Not Working Anymore? Fadi Hamid, M.D. Saint Luke s GI Specialists Disclosures No financial relationships to disclose. 1 Learning Objectives Case 24M with ileocolonic
What Do I Do When Anti-TNF Therapy Is Not Working Anymore? Fadi Hamid, M.D. Saint Luke s GI Specialists Disclosures No financial relationships to disclose. 1 Learning Objectives Case 24M with ileocolonic
Risk = probability x consequence
 Explaining Risks of IBD Therapy to Parents and Patients December 4, 2009 CCFA Advances in IBD Hollywood, FL Corey A. Siegel Assistant Professor of Medicine, Dartmouth Medical School Director, Dartmouth-Hitchcock
Explaining Risks of IBD Therapy to Parents and Patients December 4, 2009 CCFA Advances in IBD Hollywood, FL Corey A. Siegel Assistant Professor of Medicine, Dartmouth Medical School Director, Dartmouth-Hitchcock
5/2/2018 SHOULD DEEP REMISSION BE A TREATMENT GOAL? YES! Disclosures: R. Balfour Sartor, MD
 5/2/218 SHOULD DEEP REMISSION BE A TREATMENT GOAL? YES! Disclosures: R. Balfour Sartor, MD Grant support for preclinical studies: Janssen, Gusto Global, Vedanta, Artizan BALFOUR SARTOR, MD DISTINGUISHED
5/2/218 SHOULD DEEP REMISSION BE A TREATMENT GOAL? YES! Disclosures: R. Balfour Sartor, MD Grant support for preclinical studies: Janssen, Gusto Global, Vedanta, Artizan BALFOUR SARTOR, MD DISTINGUISHED
Biologics in IBD. Brian P. Bosworth, MD, NYSGEF Associate Professor of Medicine Weill Cornell Medical College
 Biologics in IBD Brian P. Bosworth, MD, NYSGEF Associate Professor of Medicine Weill Cornell Medical College Case 30 year old man diagnosed with ulcerative proctitis diagnosed in 2003 Had been maintained
Biologics in IBD Brian P. Bosworth, MD, NYSGEF Associate Professor of Medicine Weill Cornell Medical College Case 30 year old man diagnosed with ulcerative proctitis diagnosed in 2003 Had been maintained
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only.
 The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
Biologic agents, such as monoclonal antibodies
 PREDICTING, MEASURING, AND MAINTAINING RESPONSE TO TNF-α ANTAGONISTS IN INFLAMMATORY BOWEL DISEASE Stephen B. Hanauer, MD * ABSTRACT Tumor necrosis factor (TNF) antagonists have substantially improved
PREDICTING, MEASURING, AND MAINTAINING RESPONSE TO TNF-α ANTAGONISTS IN INFLAMMATORY BOWEL DISEASE Stephen B. Hanauer, MD * ABSTRACT Tumor necrosis factor (TNF) antagonists have substantially improved
Perianal and Fistulizing Crohn s Disease: Tough Management Decisions. Jean-Paul Achkar, M.D. Kenneth Rainin Chair for IBD Research Cleveland Clinic
 Perianal and Fistulizing Crohn s Disease: Tough Management Decisions Jean-Paul Achkar, M.D. Kenneth Rainin Chair for IBD Research Cleveland Clinic Talk Overview Background Assessment and Classification
Perianal and Fistulizing Crohn s Disease: Tough Management Decisions Jean-Paul Achkar, M.D. Kenneth Rainin Chair for IBD Research Cleveland Clinic Talk Overview Background Assessment and Classification
Scottish Medicines Consortium
 Scottish Medicines Consortium infliximab 100mg powder for intravenous infusion (Remicade ) No. (364/07) Schering-Plough UK Ltd 6 April 2007 The Scottish Medicines Consortium (SMC) has completed its assessment
Scottish Medicines Consortium infliximab 100mg powder for intravenous infusion (Remicade ) No. (364/07) Schering-Plough UK Ltd 6 April 2007 The Scottish Medicines Consortium (SMC) has completed its assessment
Influence of Immunogenicity on the Long-Term Efficacy of Infliximab in Crohn s Disease
 The new england journal of medicine original article Influence of Immunogenicity on the Long-Term Efficacy of Infliximab in Crohn s Disease Filip Baert, M.D., Maja Noman, M.D., Severine Vermeire, M.D.,
The new england journal of medicine original article Influence of Immunogenicity on the Long-Term Efficacy of Infliximab in Crohn s Disease Filip Baert, M.D., Maja Noman, M.D., Severine Vermeire, M.D.,
Efficacy and Safety of Treatment for Pediatric IBD
 Efficacy and Safety of Treatment for Pediatric IBD Andrew B. Grossman MD Co-Director, Center for Pediatric Inflammatory Bowel Disease Associate Professor of Clinical Pediatrics Division of Gastroenterology,
Efficacy and Safety of Treatment for Pediatric IBD Andrew B. Grossman MD Co-Director, Center for Pediatric Inflammatory Bowel Disease Associate Professor of Clinical Pediatrics Division of Gastroenterology,
Personalized Medicine. Selecting the Right First-line Biologic Agent. Gene Expression Profiles Crohn s Disease. The Right Treatment
 Personalized Medicine Selecting the Right First-line Biologic Agent William Tremaine, M.D. Maxine and Jack Zarrow Professor Mayo Clinic Rochester, MN, USA The Right Treatment Pretreatment Genomic Analysis
Personalized Medicine Selecting the Right First-line Biologic Agent William Tremaine, M.D. Maxine and Jack Zarrow Professor Mayo Clinic Rochester, MN, USA The Right Treatment Pretreatment Genomic Analysis
Lessons to learn from Crohn's disease clinical trials: implications for ulcerative colitis
 Lessons to learn from Crohn's disease clinical trials: implications for ulcerative colitis Aránzazu Jáuregui Amézaga, Elena Ricart, Julián Panés Department of Gastroenterology, Hospital Clínic de Barcelona,
Lessons to learn from Crohn's disease clinical trials: implications for ulcerative colitis Aránzazu Jáuregui Amézaga, Elena Ricart, Julián Panés Department of Gastroenterology, Hospital Clínic de Barcelona,
Join the conversation at #GIFORUMCCFA
 1 Join the conversation at #GIFORUMCCFA 2 Disclosures In accordance with the ACCME Standards for Commercial Support of CME, the speakers for this course have been asked to disclose to participants the
1 Join the conversation at #GIFORUMCCFA 2 Disclosures In accordance with the ACCME Standards for Commercial Support of CME, the speakers for this course have been asked to disclose to participants the
Are Biologicals Safe Enough?
 Are Biologicals Safe Enough? Dr Anne Duggan Director of Gastroenterology, John Hunter Hospital, Hunter New England Area Health Service (HNEAHS) Conjoint A/Professor, University of Newcastle, Australia
Are Biologicals Safe Enough? Dr Anne Duggan Director of Gastroenterology, John Hunter Hospital, Hunter New England Area Health Service (HNEAHS) Conjoint A/Professor, University of Newcastle, Australia
Percent Cumulative. Probability. Penetrating. Inflammatory. Stricturing. Months Patients at risk N =
 Fistulizing Crohn s Disease Edward V. Loftus, Jr., M.D. Professor of Medicine Division of Gastroenterology & Hepatology Mayo Clinic Rochester, Minnesota, USA Outline Fistulizing Crohn s Etiology Incidence
Fistulizing Crohn s Disease Edward V. Loftus, Jr., M.D. Professor of Medicine Division of Gastroenterology & Hepatology Mayo Clinic Rochester, Minnesota, USA Outline Fistulizing Crohn s Etiology Incidence
Optimizing Immunomodulators and
 Optimizing Immunomodulators and Biologics i in Inflammatory Bowel Disease Sunanda Kane, MD, MSPH, FACG Professor of Medicine Division of Gastroenterology and Hepatology Mayo Clinic Rochester, Minnesota,
Optimizing Immunomodulators and Biologics i in Inflammatory Bowel Disease Sunanda Kane, MD, MSPH, FACG Professor of Medicine Division of Gastroenterology and Hepatology Mayo Clinic Rochester, Minnesota,
Optimizing the treatment of IBD through use of therapeutic drug monitoring
 Optimizing the treatment of IBD through use of therapeutic drug monitoring Adam S. Cheifetz Director, Center for Inflammatory Bowel Disease, Beth Israel Deaconess Medical Center Associate Professor of
Optimizing the treatment of IBD through use of therapeutic drug monitoring Adam S. Cheifetz Director, Center for Inflammatory Bowel Disease, Beth Israel Deaconess Medical Center Associate Professor of
The Refractory Crohn s Disease
 The Refractory Crohn s Disease Patient David T. Rubin, MD, FACG Professor of Medicine Co-Director, Inflammatory Bowel Disease Center Interim Chief, Section of Gastroenterology, Hepatology and Nutrition
The Refractory Crohn s Disease Patient David T. Rubin, MD, FACG Professor of Medicine Co-Director, Inflammatory Bowel Disease Center Interim Chief, Section of Gastroenterology, Hepatology and Nutrition
Review article: infliximab therapy for inflammatory bowel disease seven years on
 Alimentary Pharmacology & Therapeutics Review article: infliximab therapy for inflammatory bowel disease seven years on P. RUTGEERTS, G. VAN ASSCHE & S. VERMEIRE Department of Medicine, Division of Gastroenterology,
Alimentary Pharmacology & Therapeutics Review article: infliximab therapy for inflammatory bowel disease seven years on P. RUTGEERTS, G. VAN ASSCHE & S. VERMEIRE Department of Medicine, Division of Gastroenterology,
Intravenous Hydrocortisone Premedication Reduces Antibodies to Infliximab in Crohn s Disease: A Randomized Controlled Trial
 GASTROENTEROLOGY 2003;124:917 924 Intravenous Hydrocortisone Premedication Reduces Antibodies to Infliximab in Crohn s Disease: A Randomized Controlled Trial RICHARD J. FARRELL, MAZEN ALSAHLI, YOON TAE
GASTROENTEROLOGY 2003;124:917 924 Intravenous Hydrocortisone Premedication Reduces Antibodies to Infliximab in Crohn s Disease: A Randomized Controlled Trial RICHARD J. FARRELL, MAZEN ALSAHLI, YOON TAE
Anti-TNF and cyclosporine are identical choices for severe ulcerative colitis refractory to steroid therapy CON Peter Laszlo LAKATOS Semmelweis
 Anti-TNF and cyclosporine are identical choices for severe ulcerative colitis refractory to steroid therapy CON Peter Laszlo LAKATOS Semmelweis University, 1st Department of Medicine Budapest June 13-15,
Anti-TNF and cyclosporine are identical choices for severe ulcerative colitis refractory to steroid therapy CON Peter Laszlo LAKATOS Semmelweis University, 1st Department of Medicine Budapest June 13-15,
Medical Management of Inflammatory Bowel Disease
 Medical Management of Inflammatory Bowel Disease John K. Marshall MD MSc FRCPC AGAF Division of Gastroenterology McMaster University John K. Marshall: Conflicts of Interest Speaker: AbbVie, Allergan, Ferring,
Medical Management of Inflammatory Bowel Disease John K. Marshall MD MSc FRCPC AGAF Division of Gastroenterology McMaster University John K. Marshall: Conflicts of Interest Speaker: AbbVie, Allergan, Ferring,
Definitions. Clinical remission: Resolution of symptoms (stool frequency 3/day, no bleeding and no urgency)
") CROHN S DISEASE Definitions Clinical remission: Resolution of symptoms (stool frequency 3/day, no bleeding and no urgency) Recurrence: The reappearance of lesions after surgical resection Endoscopic remission:
CROHN S DISEASE Definitions Clinical remission: Resolution of symptoms (stool frequency 3/day, no bleeding and no urgency) Recurrence: The reappearance of lesions after surgical resection Endoscopic remission:
Agenda. Predictive markers in IBD. Management of ulcerative colitis. Management of Crohn s disease
 Agenda Predictive markers in IBD Management of ulcerative colitis Management of Crohn s disease 2 Patients With UC (%) Distribution of UC Disease Severity at Presentation 1 Fulminant disease (9%) 8 6 4
Agenda Predictive markers in IBD Management of ulcerative colitis Management of Crohn s disease 2 Patients With UC (%) Distribution of UC Disease Severity at Presentation 1 Fulminant disease (9%) 8 6 4
IBD Understanding Your Medications. Thomas V. Aguirre, MD Santa Barbara GI Consultants
 IBD Understanding Your Medications Thomas V. Aguirre, MD Santa Barbara GI Consultants IBD Understanding Your Medications (& Your Doctor) Thomas V. Aguirre, MD Santa Barbara GI Consultants Disclosure I
IBD Understanding Your Medications Thomas V. Aguirre, MD Santa Barbara GI Consultants IBD Understanding Your Medications (& Your Doctor) Thomas V. Aguirre, MD Santa Barbara GI Consultants Disclosure I
Emerging Therapies in IBD 2006
 Overview Emerging Therapies in IBD 26 David T. Rubin, MD Assistant Professor of Medicine Inflammatory Bowel Disease Center University of Chicago Describe the unmet needs of therapy in IBD Emerging biologic
Overview Emerging Therapies in IBD 26 David T. Rubin, MD Assistant Professor of Medicine Inflammatory Bowel Disease Center University of Chicago Describe the unmet needs of therapy in IBD Emerging biologic
Predicting response to anti - integrin therapy: long term efficacy and roles for optimisation with vedolizumab.
 Predicting response to anti - integrin therapy: long term efficacy and roles for optimisation with vedolizumab. Dr Peter Irving Guy s and St Thomas Hospital, London King s College London Response to vedolizumab
Predicting response to anti - integrin therapy: long term efficacy and roles for optimisation with vedolizumab. Dr Peter Irving Guy s and St Thomas Hospital, London King s College London Response to vedolizumab
COPYRIGHT. Inflammatory Bowel Disease What Every Clinician Needs to Know. Adam S. Cheifetz, MD. Director, Center for Inflammatory Bowel Disease
 Inflammatory Bowel Disease What Every Clinician Needs to Know Adam S. Cheifetz, MD Director, Center for Inflammatory Bowel Disease Beth Israel Deaconess Medical Center Associate Professor of Medicine Harvard
Inflammatory Bowel Disease What Every Clinician Needs to Know Adam S. Cheifetz, MD Director, Center for Inflammatory Bowel Disease Beth Israel Deaconess Medical Center Associate Professor of Medicine Harvard
Biologic Therapy for Inflammatory. Is Top-Down Too Top-Heavy? S. Devi Rampertab, MD, FACG, AGAF Associate Professor of Medicine University of Florida
 Biologic Therapy for Inflammatory Bowel Disease: Is Top-Down Too Top-Heavy? S. Devi Rampertab, MD, FACG, AGAF Associate Professor of Medicine University of Florida Learning Objectives Evaluate evidence
Biologic Therapy for Inflammatory Bowel Disease: Is Top-Down Too Top-Heavy? S. Devi Rampertab, MD, FACG, AGAF Associate Professor of Medicine University of Florida Learning Objectives Evaluate evidence
Long-term outcome after infliximab for refractory ulcerative colitis
 Journal of Crohn's and Colitis (2008) 2, 219 225 available at www.sciencedirect.com Long-term outcome after infliximab for refractory ulcerative colitis Marc Ferrante a, Séverine Vermeire a, Herma Fidder
Journal of Crohn's and Colitis (2008) 2, 219 225 available at www.sciencedirect.com Long-term outcome after infliximab for refractory ulcerative colitis Marc Ferrante a, Séverine Vermeire a, Herma Fidder
WHY HAVE WE NOT FINALLY FIGURED OUT COMBINATION THERAPY?
 WHY HAVE WE NOT FINALLY FIGURED OUT COMBINATION THERAPY? Siew Ng, Professor MBBS, FRCP, (Lon, Edin), PhD (Lond), AGAF, FHKCP, FHKAM (medicine) Department of Medicine and Therapeutics Chinese University
WHY HAVE WE NOT FINALLY FIGURED OUT COMBINATION THERAPY? Siew Ng, Professor MBBS, FRCP, (Lon, Edin), PhD (Lond), AGAF, FHKCP, FHKAM (medicine) Department of Medicine and Therapeutics Chinese University
Communicating with the IBD Patient: How to convey risks and benefits
 Communicating with the IBD Patient: How to convey risks and benefits October 30, 2011 ACG Postgraduate Course National Harbor, Maryland Corey A. Siegel, MD Assistant Professor of Medicine Dartmouth Medical
Communicating with the IBD Patient: How to convey risks and benefits October 30, 2011 ACG Postgraduate Course National Harbor, Maryland Corey A. Siegel, MD Assistant Professor of Medicine Dartmouth Medical
The Effect of Medical Treatment on Patients with Fistulizing Crohn s Disease: A Retrospective Study
 ORIGINAL ARTICLE The Effect of Medical Treatment on Patients with Fistulizing Crohn s Disease: A Retrospective Study Norimitsu Uza, Hiroshi Nakase, Satoru Ueno, Satoko Inoue, Sakae Mikami, Hiroyuki Tamaki,
ORIGINAL ARTICLE The Effect of Medical Treatment on Patients with Fistulizing Crohn s Disease: A Retrospective Study Norimitsu Uza, Hiroshi Nakase, Satoru Ueno, Satoko Inoue, Sakae Mikami, Hiroyuki Tamaki,
Clinical Use of Measuring Trough Levels and Antibodies against Infliximab in Patients with Pediatric Inflammatory Bowel Disease
 Gut and Liver, Published online September 9, 2016 ORiginal Article Clinical Use of Measuring Trough Levels and Antibodies against Infliximab in Patients with Pediatric Inflammatory Bowel Disease So Yoon
Gut and Liver, Published online September 9, 2016 ORiginal Article Clinical Use of Measuring Trough Levels and Antibodies against Infliximab in Patients with Pediatric Inflammatory Bowel Disease So Yoon
Achieving Success in Ulcerative Colitis: the Role of Infliximab
 Achieving Success in Ulcerative Colitis: the Role of Infliximab Dr Gill Watermeyer IBD clinic Groote Schuur Hospital 17 th August 2012 Inflammatory Bowel Disease Crohn s disease and ulcerative colitis
Achieving Success in Ulcerative Colitis: the Role of Infliximab Dr Gill Watermeyer IBD clinic Groote Schuur Hospital 17 th August 2012 Inflammatory Bowel Disease Crohn s disease and ulcerative colitis
Medical Management of Small bowel Crohn s Disease: An evidence-based approach
 Medical Management of Small bowel Crohn s Disease: An evidence-based approach E. Jan Irvine, M.D., F.R.C.P.(C)., M.Sc. Professor of Medicine, University of Toronto, Head, Division of Gastroenterology,
Medical Management of Small bowel Crohn s Disease: An evidence-based approach E. Jan Irvine, M.D., F.R.C.P.(C)., M.Sc. Professor of Medicine, University of Toronto, Head, Division of Gastroenterology,
Association of Trough Serum Infliximab to Clinical Outcome After Scheduled Maintenance Treatment for Crohn s Disease
 CLINICL GSTROENTEROLOGY ND HEPTOLOGY 26;4:1248 1254 ssociation of Trough Serum Infliximab to Clinical Outcome fter Scheduled Maintenance Treatment for Crohn s Disease ELN. MSER, RENT VILLEL, MRK S. SILVERERG,
CLINICL GSTROENTEROLOGY ND HEPTOLOGY 26;4:1248 1254 ssociation of Trough Serum Infliximab to Clinical Outcome fter Scheduled Maintenance Treatment for Crohn s Disease ELN. MSER, RENT VILLEL, MRK S. SILVERERG,
Selective leucocyte trafficking inhibitors for treatment of IBD
 Selective leucocyte trafficking inhibitors for treatment of IBD Séverine Vermeire MD, PhD Department of Gastroenterology University Hospitals Leuven Belgium Migration of Leucocytes plays a key role in
Selective leucocyte trafficking inhibitors for treatment of IBD Séverine Vermeire MD, PhD Department of Gastroenterology University Hospitals Leuven Belgium Migration of Leucocytes plays a key role in
TNF Inhibitors: Lessons From Immunogenicity
 TNF Inhibitors: Lessons From Immunogenicity Edward Keystone, MD, FRCP(C) Professor of Medicine University of Toronto Toronto, Canada Edward Keystone, MD FRCP(C) Disclosures Sources of Funding for Research:
TNF Inhibitors: Lessons From Immunogenicity Edward Keystone, MD, FRCP(C) Professor of Medicine University of Toronto Toronto, Canada Edward Keystone, MD FRCP(C) Disclosures Sources of Funding for Research:
Optimal Use of Immunomodulators and Biologics
 3/17/214 Optimal Use of Immunomodulators and Biologics Edward V. Loftus, Jr., M.D. Professor of Medicine Division of Gastroenterology and Hepatology Mayo Clinic Rochester, Minnesota, U.S.A. Loftus Disclosures
3/17/214 Optimal Use of Immunomodulators and Biologics Edward V. Loftus, Jr., M.D. Professor of Medicine Division of Gastroenterology and Hepatology Mayo Clinic Rochester, Minnesota, U.S.A. Loftus Disclosures
U of Cape Town, South Africa, 10 U of Washington, Seattle, WA,USA, 11 CHRU de Lille, Hôpital Claude Huriez, Lille, France, 12
 A Multicenter, Double-blind, Placebo-controlled Phase 3 Study of Ustekinumab, a Human IL-12/23p40 Monoclonal Antibody, in Moderate-severe Crohn s Disease Refractory to Anti-TNFα: UNITI-1 WJ Sandborn 1,
A Multicenter, Double-blind, Placebo-controlled Phase 3 Study of Ustekinumab, a Human IL-12/23p40 Monoclonal Antibody, in Moderate-severe Crohn s Disease Refractory to Anti-TNFα: UNITI-1 WJ Sandborn 1,
Emerging g therapies for IBD: A practical approach to positioning. Sequential Therapies for IBD
 Emerging g therapies for IBD: A practical approach to positioning Stephen B. Hanauer, MD Sequential Therapies for IBD Disease Severity at Presentation Severe Anti-TNF +/IS Cyclosporine (UC) Colectomy (UC)
Emerging g therapies for IBD: A practical approach to positioning Stephen B. Hanauer, MD Sequential Therapies for IBD Disease Severity at Presentation Severe Anti-TNF +/IS Cyclosporine (UC) Colectomy (UC)
New and Future Adhesion Molecule Based Therapies in IBD
 New and Future Adhesion Molecule Based Therapies in IBD Brian G. Feagan Professor of Medicine, Epidemiology and Biostatistics University of Western Ontario Robarts Clinical Trials London, Ontario, Canada
New and Future Adhesion Molecule Based Therapies in IBD Brian G. Feagan Professor of Medicine, Epidemiology and Biostatistics University of Western Ontario Robarts Clinical Trials London, Ontario, Canada
Available Data on Pediatric Exposure Response a Clinician s Perspective
 Available Data on Pediatric Exposure Response a Clinician s Perspective Marla Dubinsky, MD Professor of Pediatrics and Medicine Chief Pediatric GI and Nutrition Co-Director Susan and Leonard Feinstein
Available Data on Pediatric Exposure Response a Clinician s Perspective Marla Dubinsky, MD Professor of Pediatrics and Medicine Chief Pediatric GI and Nutrition Co-Director Susan and Leonard Feinstein
Biologics, Novel Therapeutic Approaches in Inflammatory Bowel Diseases
 Biologics, Novel Therapeutic Approaches in Inflammatory Bowel Diseases Walter Reinisch Univ-Klinik für Innere Medizin III Abt. Gastroenterologie & Hepatologie AKH Wien The Biologic s evolution From availabilitydriven
Biologics, Novel Therapeutic Approaches in Inflammatory Bowel Diseases Walter Reinisch Univ-Klinik für Innere Medizin III Abt. Gastroenterologie & Hepatologie AKH Wien The Biologic s evolution From availabilitydriven
Infliximab Therapy in Pediatric Patients 7 Years of Age and Younger
 ORIGINAL ARTICLE: GASTROENTEROLOGY Infliximab Therapy in Pediatric Patients 7 Years of Age and Younger Judith R. Kelsen, Andrew B. Grossman, Helen Pauly-Hubbard, Kernika Gupta, Robert N. Baldassano, and
ORIGINAL ARTICLE: GASTROENTEROLOGY Infliximab Therapy in Pediatric Patients 7 Years of Age and Younger Judith R. Kelsen, Andrew B. Grossman, Helen Pauly-Hubbard, Kernika Gupta, Robert N. Baldassano, and
STELARA (ustekinumab) Clinical Study Report CNTO1275CRD3001
 Clinical Study Report CNTO1275CRD3001") SYNOPSIS Name of Sponsor/Company Janssen Research & Development* Name of Investigational Product STELARA (ustekinumab) * Janssen Research & Development is a global organization that operates through different
SYNOPSIS Name of Sponsor/Company Janssen Research & Development* Name of Investigational Product STELARA (ustekinumab) * Janssen Research & Development is a global organization that operates through different
Latest Meds Approved for IBD: What are they and how do they work?
 Latest Meds Approved for IBD: What are they and how do they work? JAMES LORD, MD PHD BENAROYA RESEARCH INSTITUTE AT VIRGINIA MASON MEDICAL CENTER SEPT 30, 2018 Brief history of IBD Dr. Burrill Crohn JAMA
Latest Meds Approved for IBD: What are they and how do they work? JAMES LORD, MD PHD BENAROYA RESEARCH INSTITUTE AT VIRGINIA MASON MEDICAL CENTER SEPT 30, 2018 Brief history of IBD Dr. Burrill Crohn JAMA
Submitted by xxxxxxxxxxxxxxxxx, xxxxxxxxx RCP and co-ordinated by xxxxxxxxxxxx, xxxxxxxxxxxxxxxxxxxxxxxxxxxxx, Royal Liverpool University Hospital.
 Royal College of Physicians statement on the appraisal of use of tumour necrosis factor alpha (TNF-α) inhibitors (adalimumab, certolizumab pegol and infliximab) and natalizumab for Crohn's disease Submitted
Royal College of Physicians statement on the appraisal of use of tumour necrosis factor alpha (TNF-α) inhibitors (adalimumab, certolizumab pegol and infliximab) and natalizumab for Crohn's disease Submitted
Preventing post-operative recurrence
 Oxford Inflammatory Bowel Disease MasterClass Preventing post-operative recurrence Dr Oliver Brain Oxford Disclosures Presented at IEE, Oxford 2013 AbbVie sponsored meeting Talk Outline Risk factors for
Oxford Inflammatory Bowel Disease MasterClass Preventing post-operative recurrence Dr Oliver Brain Oxford Disclosures Presented at IEE, Oxford 2013 AbbVie sponsored meeting Talk Outline Risk factors for
IBD Case Studies. David Rowbotham. Clinical Director & Consultant Gastroenterologist Dept of Gastroenterology & Hepatology Auckland City Hospital
 IBD Case Studies David Rowbotham Clinical Director & Consultant Gastroenterologist Dept of Gastroenterology & Hepatology Auckland City Hospital Dr David Rowbotham The Leeds Teaching Hospitals NHS Trust
IBD Case Studies David Rowbotham Clinical Director & Consultant Gastroenterologist Dept of Gastroenterology & Hepatology Auckland City Hospital Dr David Rowbotham The Leeds Teaching Hospitals NHS Trust
Special Authorization Drug Products with
 Effective August 1, 2008 Summary Special Authorization Drug Products with Changes to Criteria Special Authorization Drug Products with Changes to Criteria Alberta Blue Cross has been advised by Alberta
Effective August 1, 2008 Summary Special Authorization Drug Products with Changes to Criteria Special Authorization Drug Products with Changes to Criteria Alberta Blue Cross has been advised by Alberta
Doncaster & Bassetlaw Medicines Formulary
 Doncaster & Bassetlaw Medicines Formulary Section 1.5 Chronic Bowel Disorders (including IBD) Aminosalicylates: Mesalazine 400mg and 800mg MR Tablets (Octasa) Mesalazine 1.2g MR Tablets (Mezavant XL) Mesalazine
Doncaster & Bassetlaw Medicines Formulary Section 1.5 Chronic Bowel Disorders (including IBD) Aminosalicylates: Mesalazine 400mg and 800mg MR Tablets (Octasa) Mesalazine 1.2g MR Tablets (Mezavant XL) Mesalazine