The Power of Pink: Diagnosis & Treatment of Breast Disease. Tony L. Weaver, D.O.
|
|
|
- Jennifer Kelly
- 5 years ago
- Views:
Transcription

1 The Power of Pink: Diagnosis & Treatment of Breast Disease Tony L. Weaver, D.O.

2 Objectives Review Anatomy & Physiology Discuss: Diagnosis Management Treatment of benign & Malignant Breast Disease It is about YOU!
 Progesterone Lobular development Prolactin synergizes estrogen and")
3 ANATOMY AND PHYSIOLOGY Breast development Breast formed from ectoderm milk streak Estrogen duct development (double layer of columnar cells) Progesterone Lobular development Prolactin synergizes estrogen and progesterone
4 Hormones and Cyclic changes Estrogen breast swelling, growth of glandular tissue Progesterone maturation of glandular tissue; withdrawal causes menses FSH, LH surge cause ovum release After menopause, lack of estrogen and progesterone results in atrophy of breast tissue

5 Lymphatic drainage 97% is to the axillary nodes 2% is to the internal mammary nodes Any quadrant can drain to the internal mammary nodes Supraclavicular nodes considered N3 disease Primary axillary adenopathy #1 is lymphoma

6

7 You ve Got a lot of Nerve Medial pectoral nerve pectoralis major and pectoralis minor Lateral pectoral nerve ---> Pectoralis Major only Intercostobrachial Nerve lateral cutaneous branch of the 2nd intercostal nerve

8 Nerve Name that Nerve
9 Long thoracic nerve innervates serratus anterior; injury results in winged scapula Important Nerves Thoracodorsal Nerve innervates latissimus dorsi; injury results in weak arm pullups and adduction

10

11 Vessels Internal thoracic artery Intercostal arteries, Thoracoacromial artery lateral thoracic artery Batson s plexus valveless vein plexus direct hematogenous metastasis to spine Lateral thoracic artery supplies serratus anterior Thoracodorsal artery supplies latissimus dorsi

12 BREAST CANCER Breast CA decreased in economically poor areas Japan has lowest rate of breast CA worldwide U.S. breast CA risk 1 in 8 women (12%); 5% in women with no risk factors Screening decreases mortality by 25% Untreated breast cancer median survival 2 3 years 10% of breast CAs have negative mammogram and negative ultrasound Clinical features of breast CA distortion of normal architecture; skin/nipple distortion or retraction; hard, tethered, indistinct borders
13 Breast Cancer Risk Greatly increased risk (relative risk > 4) BRCA gene in patient with family history of breast CA 2 primary relatives with bilateral or premenopausal breast CA DCIS (ipsilateral breast at risk) and LCIS (both breasts have same high risk) Fibrocystic disease with atypical hyperplasia Moderately increased risk (relative risk 2 4) prior breast cancer, radiation exposure, first-degree relative with breast cancer, age > 35 first birth Lower increased risk (relative risk < 2) early menarche, late menopause, nulliparity, proliferative benign disease, obesity, alcohol use, hormone replacement therapy

14 What s a Mammogram?


15

16
17 Screening Mammogram every 2 3 years after age 40, then yearly after 50 High-risk screening mammogram 10 years before the youngest age of diagnosis of breast CA in first-degree relative No mammography in patients < 40 unless high risk hard to interpret because of dense parenchyma Want to decrease radiation dose in young patients
18 Mammography Has 90% sensitivity/specificity Sensitivity increases with age as the dense parenchymal tissue is replaced with fat Mass needs to be 5 mm to be detected Suggestive of CA irregular borders; spiculated; multiple clustered, small, thin, linear, crushed-like and/or branching calcifications; ductal asymmetry, distortion of architecture

19
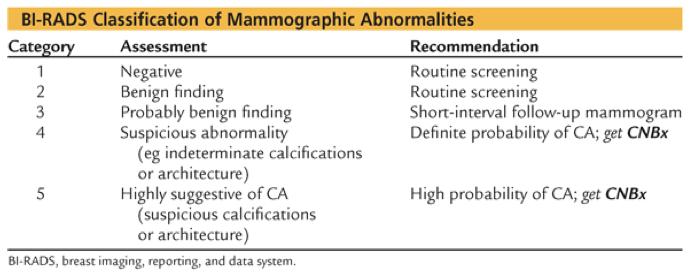
20 What is BIRADS?
21 Nice Negative Breast Benign Please Probably Benign Show Suspicious for Malignancy Me Highly Suspicious for Malignant
22 BiRADS
23 Risk Assessment Tools Gail Model Age, menarche, age of first live birth, previous history of biopsies (benign or atypia), family history of 1 st degree relatives Calculates risk at 5 years and to age 90 of developing breast cancer Gail Pitfalls Underestimates family history (accounts for only disease in first degree relatives), no paternal FH Heavily weighted on biopsy history Not incorporate age at diagnosis Not accepted estimate for need for MRI Other alternatives: Claus tables, BRCAPRO and BOADICEA (genetic counselor) more in depth family assessment

24 Average woman risk of BRCA 1 or 2 mutation: 1/450 to 1/800 Women of Ashkenazi descent risk of BRCA mutation: 1/40 10% of women with breast cancer have a BRCA mutation

25 BRCA 1 Younger age at cancer presentation 30-45yo Premenopausal Lifetime risk for breast cancer 50-80% Risk of contralateral breast cancer 60% Breast cancers tend to be triple negative Ovarian cancer risk 40-60% BRCA2 Same age for development of breast cancer as general population Lifetime risk of BC same as BRCA1 Risk for contralateral BC is same as BRCA1 Breast cancers tend to be ER+ Ovarian cancer risk 16-30% Male breast cancer risk 6% Increased risk for prostate, pancreas, melanoma
 produces an abundance of mucin, more favorable prognosis Scirrhotic worse prognosis Tx: MRM or BCT with postop")
26 85% of all breast CA Ductal Cancer Medullary smooth borders, lymphocytes, bizarre cells, more favorable prognosis Tubular small tubule formations, more favorable prognosis Mucinous (colloid) produces an abundance of mucin, more favorable prognosis Scirrhotic worse prognosis Tx: MRM or BCT with postop XRT
27 Prognostics of Invasive Breast Cancer Good Tubular Papillary Mucinous Adenoid cystic Bad Medullary squamous

28 Considered T4 disease Inflammatory Cancer Very aggressive median survival of 36 months Has dermal lymphatic invasion, which causes peau d orange lymphedema appearance on breast; erythematous and warm Tx: Neoadjuvant chemo, then MRM, then adjuvant chemo-xrt

29 Occult breast CA breast CA that presents as axillary metastases with unknown primary; Tx: MRM (70% are found to have breast CA) Almost all women with recurrence die of disease Increased recurrences and metastases occur with positive nodes, large tumors, negative receptors, unfavorable subtype Metastatic flare pain, swelling, erythema in metastatic areas; XRT can help XRT is good for bone metastases
30 What is the most important prognostic staging factor??
31 Nodes
32 Survival is directly related to the number of positive nodes 0 nodes positive 75% 5-year survival 1 3 nodes positive 60% 5-year survival 4 10 nodes positive 40% 5-year survival
33 What is the MOST COMMON Site of Distal Mets?
34 Bone most common site for distant metastasis (can also go to lung, liver, brain) Takes approximately 5 7 years to go from single malignant cell to 1-cm tumor Central and subareolar tumors have increased risk of multicentricity
35 Invasive BC treatment (all types) Excise to negative margins (no tumor at ink, most aim for >2mm margin) XRT if had successful BCT SLNB +/-ALND in all cases Chemotherapy Hormonal (antiestrogen) Chemotherapy Monoclonal antibody (trastuzumab/herceptin)

36 ALND take level I and II nodes Breast Surgery Basics Complications of MRM infection, flap necrosis, seromas Complications of ALND Infection, lymphedema, lymphangiosarcoma Axillary vein thrombosis sudden, early, postop swelling Lymphatic fibrosis slow swelling over 18 months Intercostal brachiocutaneous nerve injury hyperesthesia of inner arm and lateral chest wall; most commonly injured nerve after mastectomy; no significant sequelae Drains leave in until drainage < 40 cc/day
37 Receptors Positive receptors: better response to hormones, chemotherapy, surgery, and better overall prognosis Receptor-positive tumors are more common in postmenopausal women Progesterone receptor positive tumors have better prognosis than estrogen receptor positive tumors Tumors that are both progesterone receptor & estrogen receptor positive have the best prognosis 10% of breast CA is negative for both receptors
38
39 During SLNB if no radiotracer or dye is found??

40 Fewer complications than ALND Only for malignant tumors > 1 cm SLNB Patients with clinically positive nodes; Need ALND Accuracy best when primary tumor is present (finds the right lymphatic channels) Lymphazurin blue dye or radiotracer is injected directly into tumor area Risk: Type I hypersensitivity reactions Usually find 1 3 nodes; 95% of the time, the sentinel node is found Contraindications pregnancy, multicentric disease, neoadjuvant therapy, clinically positive nodes, prior axillary surgery, inflammatory or locally advanced disease

41 Lobular Cancer 10% of all breast CAs Does not form calcifications; extensively infiltrative; bilateral, multifocal, and multicentric disease Signet ring cells confer worse prognosis Tx: MRM or BCT with postop XRT
42 Male Breast Cancer < 1% of all breast CAs; usually ductal Poorer prognosis because of late presentation Have pectoral muscle involvement Associated with steroid use, previous XRT, family history, Klinefelter s syndrome Tx: modified radical mastectomy (MRM)


43 Breast Cancer Treatment
44 What is a Name????

45 Surgical Options Lumpectomy/Partial Mastectomy/BCT Mastectomy Survival is equivalent Rates of local recurrence are higher with BCT than with Mastectomy.

 or mastectomy with radiation (hazard ratio, 1.")
46 Compared BCT vs Mastectomy Alone vs Mastectomy w/ Radiation Large Retrospective Study 132,149 pts Breast conservation therapy 70%, Mastectomy alone 27% of patients, Mastectomy with radiation 3% of patients. 5-year breast cancer specific survival rates 97%, 94%, and 90% (P <.001) 10-year breast cancer specific survival rates were 94%, 90%, and 83% (P <.001). Multivariate analysis showed that women undergoing BCT had a higher survival rate than those undergoing mastectomy alone (hazard ratio, 1.31; P <.001) or mastectomy with radiation (hazard ratio, 1.47; P <.001).

47 Breast-Conserving therapy BCT Lumpectomy Quadrectomy + ALND or SLNBcombined with Postop XRT; need 1-cm margin

48 BCT with XRT Need to have negative margins (1 cm) following BCT before starting XRT 10% chance of local recurrence, usually within 2 years of 1st operation, need to re-stage with recurrence Need salvage MRM for local recurrence
49 Radical Mastectomy

50 Radical Mastectomy
51 Modified Radical Mastectomy
52 Modified Radical Modified radical mastectomy Removes all breast tissue, including the nipple areolar complex Includes axillary node dissection level I nodes
53 Simple Mastectomy

54 Simple Mastectomy A simple mastectomy (left) removes the breast tissue, nipple, areola and skin but not all the lymph nodes
55 Subcutaneous Mastectomy

56 Subcutaneous Mastectomy
57 Chemotherapy TAC (taxanes, Adriamycin, and cyclophosphamide) for 6 12 weeks Positive nodes everyone gets chemo except postmenopausal women with positive estrogen receptors they can get hormonal therapy only witharomatase inhibitor (anastrozole) > 1 cm and negative nodes everyone gets chemoexcept patients with positive estrogen receptors they can get hormonal therapy only with tamoxifen if they are premenopausal or aromatase inhibitor (anastrozole) if they are postmenopausal < 1 cm and negative nodes no chemo; hormonal therapy as above if positive estrogen receptors After chemo, patients positive for estrogen receptorsshould receive appropriate hormonal therapy Both chemotherapy and hormonal therapy have been shown to decrease recurrence and improve survival Taxanes docetaxel, paclitaxel Tamoxifen decreases risk of breast CA by 50% 1% risk of blood clots; 0.1% risk of endometrial CA

58 10,253 eligible women enrolled, 1626 women (15.9%) who had a recurrence score of 0 to 10 were assigned to receive endocrine therapy alone without chemotherapy. 5 year Invasive disease free survival was 93.8% Rate of freedom from recurrence of breast cancer at a distant site was 99.3% The rate of freedom from recurrence of breast cancer at a distant or local regional site was 98.7% Rate of overall survival was 98.0% (95% CI, 97.1 to 98.6). Pts with hormone-receptor positive, HER2-negative, axillary node negative breast cancer with tumors that had a favorable gene-expression profile had very low rates of recurrence at 5 years with endocrine therapy alone.
59 Radiotherapy Usually consists of 5,000 rad for BCT and XRT Complications of XRT edema, erythema, rib fractures, pneumonitis, ulceration, sarcoma, contralateral breast CA Contraindications to XRT scleroderma (results in severe fibrosis and necrosis), previous XRT and would exceed recommended dose, SLE (relative), active rheumatoid arthritis (relative) Indications for XRT after mastectomy: > 4 nodes Skin or chest wall involvement Positive margins Tumor > 5 cm (T3) Extracapsular nodal invasion Inflammatory CA Fixed axillary nodes (N2) or internal mammary nodes (N3)
60 Which one of the following represents a contraindication to breast conservation therapy? A. Previous breast irradiation B. Tumors larger than 3 cm diameter C. Unifocal disease D. Ductal carcinoma in situ E. Tumors in large fatty breasts
61 In a female patient with a primary T2N0M0 breast cancer, which one of the following is correct? A. Her overall survival is unaffected whether breast conservation surgery or mastectomy is performed. B. Her risk of local recurrence is unaffected by whether breast conservation surgery or mastectomy is performed. C. Postoperative radiotherapy is required irrespective of whether breast conservation surgery or mastectomy is performed. D. She has a 95% chance of being alive at five years given her disease stage. E. Sentinel lymph node biopsy for this patient has only 65% sensitivity and specificity for breast cancer.

62 Pregnancy & Breast Cancer Tends to present late, leading to worse prognosis Mammography and ultrasound do not work as well during pregnancy Try to use ultrasound to avoid radiation If cyst, drain it and send FNA for cytology If solid, perform core needle biopsy or FNA If core needle and FNA equivocal, need to go to excisional biopsy If breast CA 1st trimester MRM 2nd trimester MRM 3rd trimester MRM or if late can perform lumpectomy with ALND and postpartum XRT No XRT while pregnant; no breastfeeding after delivery
 Can often be large tumors Tx: WLE with negative margins;")
63 Cystosarcoma Phyllodes 10% malignant, based on mitoses per high-power field (> 5 10) No nodal metastases, hematogenous spread if any (rare) Resembles giant fibroadenoma; has stromal and epithelial elements (mesenchymal tissue) Can often be large tumors Tx: WLE with negative margins; no ALND

64 Paget s Disease Scaly skin lesion on nipple; biopsy shows Paget s cells Patients have DCIS or ductal CA in breast Tx: need MRM if cancer present; otherwise simple mastectomy (need to include the nipple-areolar complex with Paget s)

65 Stewart Treves Syndrome Lymphangiosarcoma from chronic lymphedema following axillary dissection Patients present with dark purple nodule or lesion on arm 5 10 years after surgery

66 Nipple Discharge Most nipple discharge is benign All need a history, breast exam, and bilateral mammogram Try to find the trigger point or mass on exam
67 Nipple Discharge Green discharge usually due to fibrocystic disease Tx: if cyclical and nonspontaneous, reassure patient Bloody discharge most commonly intraductal papilloma; occasionally ductal CA Tx: need ductogram and excision of that ductal area Serous discharge worrisome for cancer, especially if coming from only 1 duct or spontaneous Tx: excisional biopsy of that ductal area Spontaneous discharge no matter what the color or consistency is, this is worrisome for CA all these patients need excisional biopsy of duct area causing the discharge Nonspontaneous discharge (occurs only with pressure, tight garments, exercise, etc.) not as worrisome but may still need excisional biopsy (eg if bloody) May have to do a complete subareolar resection if the area above cannot be properly identified (no trigger point or mass felt)
68 Periductal Mastitis (mammary duct ectasia or plasma cellmastitis) Symptoms: noncyclical mastodynia, erythema, nipple retraction, creamy discharge from nipple; can have sterile or infected subareolar abscess Risk factors smoking, nipple piercings Biopsy dilated mammary ducts, inspissated secretions, marked periductal inflammation Tx: if typical creamy discharge is present that is not bloody and not associated with nipple retraction, give antibiotics and reassure; if not or if it recurs, need to rule out inflammatory CA (incisional biopsy including the skin)
69 Mastodynia pain in breast; rarely represents breast CA Dx: H & P, MMG Cyclic mastodynia pain before menstrual period; most commonly from fibrocystic disease Continuous mastodynia continuous pain, most commonly represents acute or subacute infection; continuous mastodynia is more refractory to treatment than cyclic mastodynia enlarge, need excisional biopsy In patients > 40 years old excisional biopsy to ensure diagnosis Tx: Danazol, OCPs, NSAIDs, evening primrose oil, bromocriptine Discontinue caffeine, nicotine, methylxanthines


70 Poland s Syndrome 1. Hypoplasia of chest wall & Shoulder, 2. Amastia 3. no pectoralis muscle
 or autoimmune disease (eg SLE) may need to rule out necrotic")
71 Infectious Mastitis most commonly associated with breastfeeding S. aureus most common. nonlactating women think chronic inflammatory diseases (eg actinomyces) or autoimmune disease (eg SLE) may need to rule out necrotic cancer (need incisional biopsy including the skin)

72 Galactorrhea Is often associated with amenorrhea can be caused by prolactin (pituitary prolactinoma) Meds: OCPs, TCAs, phenothiazines, Reglan, alpha-methyl dopa, reserpine Look for source: Prolactin level, Thyroid work up, MRI, medications

73 Gynecomastia 2-cm pinch; MCC idiopathic Assoc. w cimetidine, spironolactone, marijuana Tx: Many regress; may need to resect if cosmetically deforming or causing social problems

74 Intraductal papilloma MCC bloody nipple discharge usually small, nonpalpable, & close to the nipple NOT premalignant contrast ductogram to find papilloma, then needle localization Tx: subareolar resection of the involved duct and papilloma

75 Mondor s Disease superficial vein thrombophlebitis of breast; feels cordlike, can be painful Associated with trauma and strenuous exercise Usually occurs in lower outer quadrant Tx: NSAIDs
, lumpy breast tissue that varies with hormonal cycle Only cancer risk is atypical ductal or lobular hyperplasia need to resect these lesions Do not need to")
76 Fibrocystic Disease Lots of types: papillomatosis, sclerosing adenosis, apocrine metaplasia, duct adenosis, epithelial hyperplasia, ductal hyperplasia, and lobular hyperplasia Symptoms: breast pain, nipple discharge (usually yellow to brown), lumpy breast tissue that varies with hormonal cycle Only cancer risk is atypical ductal or lobular hyperplasia need to resect these lesions Do not need to get negative margins with atypical hyperplasia; just remove all suspicious areas (ie calcifications) that appear on mammogram
 Can have large, coarse calcifications (popcorn lesions) on mammography")
77 Fibroadenoma Most common breast lesion in adolescents and young women; 10% multiple Usually painless, slow growing, well circumscribed, firm, and rubbery Often grows to several cm in size and then stops Can change in size with menstrual cycle and can enlarge in pregnancy Giant fibromas can be > 5 cm (treatment is the same) Can have large, coarse calcifications (popcorn lesions) on mammography from degeneration In patients < 40 years old: 1) Mass needs to feel clinically benign (firm, rubbery, rolls, not fixed) 2) Ultrasound or mammogram needs to be consistent with fibroadenoma 3) Need FNA or core needle biopsy to show fibroadenoma Need all 3 of the above to be able to observe, otherwise need excisional biopsy
Breast Disease: What PCPs Need to Know. Eunice Cho MD FACS
 Breast Disease: What PCPs Need to Know Eunice Cho MD FACS New Breast Cancer Screening Guideline for women with average risk Every other year AGE 40 AGE 45 AGE 55 AGE 55 + Talk with your doctor about when
Breast Disease: What PCPs Need to Know Eunice Cho MD FACS New Breast Cancer Screening Guideline for women with average risk Every other year AGE 40 AGE 45 AGE 55 AGE 55 + Talk with your doctor about when
Lesion Imaging Characteristics Mass, Favoring Benign Circumscribed Margins Intramammary Lymph Node
 Lesion Imaging Characteristics Mass, Favoring Benign Circumscribed Margins Intramammary Lymph Node Oil Cyst Mass, Intermediate Concern Microlobulated Margins Obscured Margins Mass, Favoring Malignant Indistinct
Lesion Imaging Characteristics Mass, Favoring Benign Circumscribed Margins Intramammary Lymph Node Oil Cyst Mass, Intermediate Concern Microlobulated Margins Obscured Margins Mass, Favoring Malignant Indistinct
DISORDERS OF THE BREAST Dated. FIBROADENOSIS Other common names: mastitis, fibrocystic disease, cystic mammary dysplasia.
 DISORDERS OF THE BREAST Dated BENIGN BREAST DISORDERS (Essential Surg 2 nd Ed, pp 540) FIBROADENOSIS Other common names: mastitis, fibrocystic disease, cystic mammary dysplasia. Fibroadenosis is the distortion
DISORDERS OF THE BREAST Dated BENIGN BREAST DISORDERS (Essential Surg 2 nd Ed, pp 540) FIBROADENOSIS Other common names: mastitis, fibrocystic disease, cystic mammary dysplasia. Fibroadenosis is the distortion
BREAST PATHOLOGY. Fibrocystic Changes
 BREAST PATHOLOGY Lesions of the breast are very common, and they present as palpable, sometimes painful, nodules or masses. Most of these lesions are benign. Breast cancer is the 2 nd most common cause
BREAST PATHOLOGY Lesions of the breast are very common, and they present as palpable, sometimes painful, nodules or masses. Most of these lesions are benign. Breast cancer is the 2 nd most common cause
LYMPHATIC DRAINAGE AXILLARY (MOSTLY) INTERNAL MAMMARY SUPRACLAVICULAR
 INTERNAL MAMMARY SUPRACLAVICULAR") BREAST LYMPHATIC DRAINAGE AXILLARY (MOSTLY) INTERNAL MAMMARY SUPRACLAVICULAR HISTOLOGY LOBE: (10 in whole breast) LOBULE: (many per lobe) ACINUS/I, aka ALVEOLUS/I: (many per lobule) DUCT(S): INTRA- or
BREAST LYMPHATIC DRAINAGE AXILLARY (MOSTLY) INTERNAL MAMMARY SUPRACLAVICULAR HISTOLOGY LOBE: (10 in whole breast) LOBULE: (many per lobe) ACINUS/I, aka ALVEOLUS/I: (many per lobule) DUCT(S): INTRA- or
Breast Cancer. Most common cancer among women in the US. 2nd leading cause of death in women. Mortality rates though have declined
 Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women Mortality rates though have declined 1 in 8 women will develop breast cancer Breast Cancer Breast cancer increases
Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women Mortality rates though have declined 1 in 8 women will develop breast cancer Breast Cancer Breast cancer increases
Breast Cancer. Saima Saeed MD
 Breast Cancer Saima Saeed MD Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women 1 in 8 women will develop breast cancer Incidence/mortality rates have declined Breast
Breast Cancer Saima Saeed MD Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women 1 in 8 women will develop breast cancer Incidence/mortality rates have declined Breast
BREAST SURGERY PROGRESS TEST Name:
 General Surgery Residency Program Excellent surgeons BREAST SURGERY PROGRESS TEST Name: Choose the BEST answer for the following questions. 1. All of the following factors are associated with an increased
General Surgery Residency Program Excellent surgeons BREAST SURGERY PROGRESS TEST Name: Choose the BEST answer for the following questions. 1. All of the following factors are associated with an increased
Jose A Torres, MD 1/12/2017
 Jose A Torres, MD 1/12/2017 Background Globally leading cause of cancer related death in women ~249,000 Americans diagnosed with invasive breast cancer ~40,890 will die of their disease Breast cancer risk
Jose A Torres, MD 1/12/2017 Background Globally leading cause of cancer related death in women ~249,000 Americans diagnosed with invasive breast cancer ~40,890 will die of their disease Breast cancer risk
Breast Pathology. Breast Development
 Breast Pathology Lecturer: Hanina Hibshoosh, M.D. Reading: Kumar, Cotran, Robbins, Basic Pathology, 6th Edition, pages 623-635 Breast Development 5th week - thickening of the epidermis - milk line 5th
Breast Pathology Lecturer: Hanina Hibshoosh, M.D. Reading: Kumar, Cotran, Robbins, Basic Pathology, 6th Edition, pages 623-635 Breast Development 5th week - thickening of the epidermis - milk line 5th
Breast Cancer Screening and Surgery. April 26, 2018 Ashley B. Simpson, DO
 Breast Cancer Screening and Surgery April 26, 2018 Ashley B. Simpson, DO Objectives Breast cancer screening Common breast complaints Surgical management of breast cancer Breast Screening Question 1 At
Breast Cancer Screening and Surgery April 26, 2018 Ashley B. Simpson, DO Objectives Breast cancer screening Common breast complaints Surgical management of breast cancer Breast Screening Question 1 At
PRINCIPLES OF BREAST SURGERY & COMPLICATIONS
 PRINCIPLES OF BREAST SURGERY & COMPLICATIONS Adam Cichowitz The Royal Melbourne Hospital ANATOMY Lies in subcutaneous tissue Base: midline to midaxillary line, 2nd to 6th rib Overlies pec major, serratus
PRINCIPLES OF BREAST SURGERY & COMPLICATIONS Adam Cichowitz The Royal Melbourne Hospital ANATOMY Lies in subcutaneous tissue Base: midline to midaxillary line, 2nd to 6th rib Overlies pec major, serratus
Benign Breast Disease. David Anderson, MD Assistant Professor of Clinical Surgery
 Benign Breast Disease David Anderson, MD Assistant Professor of Clinical Surgery Overview Nipple Discharge Breast infection Breast Pain Gynecomastia Fibroepithelial lesions High Risk Lesions-Papilloma,
Benign Breast Disease David Anderson, MD Assistant Professor of Clinical Surgery Overview Nipple Discharge Breast infection Breast Pain Gynecomastia Fibroepithelial lesions High Risk Lesions-Papilloma,
BREAST PATHOLOGY MCQS
 BREAST PATHOLOGY MCQS 1) :The most important factor in breast enlargement during pregnancy is A. stromal edema B. secretion of chorionic gonadotropin C. glandular hyperplasia D. proliferation of stroma
BREAST PATHOLOGY MCQS 1) :The most important factor in breast enlargement during pregnancy is A. stromal edema B. secretion of chorionic gonadotropin C. glandular hyperplasia D. proliferation of stroma
ABSITE Review. RTC Conference Christina Bailey January 15, 2009
 ABSITE Review RTC Conference Christina Bailey January 15, 2009 How It s Broken Down? 220 questions Junior level (PGY 1 and 2) Exam 60% Basic Science 40% Clinical Management Senior Level (PGY 3-5) exam
ABSITE Review RTC Conference Christina Bailey January 15, 2009 How It s Broken Down? 220 questions Junior level (PGY 1 and 2) Exam 60% Basic Science 40% Clinical Management Senior Level (PGY 3-5) exam
Diseases of the breast (1 of 2)
") Diseases of the breast (1 of 2) Introduction A histology introduction Normal ducts and lobules of the breast are lined by two layers of cells a layer of luminal cells overlying a second layer of myoepithelial
Diseases of the breast (1 of 2) Introduction A histology introduction Normal ducts and lobules of the breast are lined by two layers of cells a layer of luminal cells overlying a second layer of myoepithelial
Maram Abdaljaleel, MD Dermatopathologist and Neuropathologist University of Jordan, School of Medicine
 Maram Abdaljaleel, MD Dermatopathologist and Neuropathologist University of Jordan, School of Medicine The most common non-skin malignancy of women 2 nd most common cause of cancer deaths in women, following
Maram Abdaljaleel, MD Dermatopathologist and Neuropathologist University of Jordan, School of Medicine The most common non-skin malignancy of women 2 nd most common cause of cancer deaths in women, following
Breast Cancer. Dr. Andres Wiernik 2017
 Breast Cancer Dr. Andres Wiernik 2017 Agenda: The Facts! (Epidemiology/Risk Factors) Biological Classification/Phenotypes of Breast Cancer Treatment approach Local Systemic Agenda: The Facts! (Epidemiology/Risk
Breast Cancer Dr. Andres Wiernik 2017 Agenda: The Facts! (Epidemiology/Risk Factors) Biological Classification/Phenotypes of Breast Cancer Treatment approach Local Systemic Agenda: The Facts! (Epidemiology/Risk
Breast Evaluation & Management Guidelines
 Breast Evaluation & Management Guidelines Pamela L. Kurtzhals, M.D. F.A.C.S. Head, Dept. of General Surgery Scripps Clinic, La Jolla Objective Review screening & diagnostic guidelines Focused patient complaints
Breast Evaluation & Management Guidelines Pamela L. Kurtzhals, M.D. F.A.C.S. Head, Dept. of General Surgery Scripps Clinic, La Jolla Objective Review screening & diagnostic guidelines Focused patient complaints
Breast pathology. 2nd Department of Pathology Semmelweis University
 Breast pathology 2nd Department of Pathology Semmelweis University Breast pathology - Summary - Benign lesions - Acute mastitis - Plasma cell mastitis / duct ectasia - Fat necrosis - Fibrocystic change/
Breast pathology 2nd Department of Pathology Semmelweis University Breast pathology - Summary - Benign lesions - Acute mastitis - Plasma cell mastitis / duct ectasia - Fat necrosis - Fibrocystic change/
It is a malignancy originating from breast tissue
 59 Breast cancer 1 It is a malignancy originating from breast tissue including both early stages which are potentially curable, and metastatic breast cancer (MBC) which is usually incurable. Most breast
59 Breast cancer 1 It is a malignancy originating from breast tissue including both early stages which are potentially curable, and metastatic breast cancer (MBC) which is usually incurable. Most breast
Diseases of the breast (2 of 2) Breast cancer
 Breast cancer") Diseases of the breast (2 of 2) Breast cancer Epidemiology & etiology The most common type of cancer & the 2 nd most common cause of cancer death in women 1 of 8 women in USA Affects 7% of women Peak at
Diseases of the breast (2 of 2) Breast cancer Epidemiology & etiology The most common type of cancer & the 2 nd most common cause of cancer death in women 1 of 8 women in USA Affects 7% of women Peak at
Imaging in breast cancer. Mammography and Ultrasound Donya Farrokh.MD Radiologist Mashhad University of Medical Since
 Imaging in breast cancer Mammography and Ultrasound Donya Farrokh.MD Radiologist Mashhad University of Medical Since A mammogram report is a key component of the breast cancer diagnostic process. A mammogram
Imaging in breast cancer Mammography and Ultrasound Donya Farrokh.MD Radiologist Mashhad University of Medical Since A mammogram report is a key component of the breast cancer diagnostic process. A mammogram
Classification System
 Classification System A graduate of the Breast Oncology training program should be able to care for all aspects of disease and/or provide comprehensive management. When referring to a discipline of training
Classification System A graduate of the Breast Oncology training program should be able to care for all aspects of disease and/or provide comprehensive management. When referring to a discipline of training
Vesalius SCALpel : Benign breast disease (see also: breast folios)
") Vesalius SCALpel : Benign breast disease (see also: breast folios) Breast cancer risk Imaging Pain non-proliferative: only fibroadenoma may be associated with a slight risk of cancer proliferative: moderate
Vesalius SCALpel : Benign breast disease (see also: breast folios) Breast cancer risk Imaging Pain non-proliferative: only fibroadenoma may be associated with a slight risk of cancer proliferative: moderate
SIGNIFICANT OTHERS. Miscellaneous Benign Breast Conditions
 SIGNIFICANT OTHERS Miscellaneous Benign Breast Conditions Epworth HealthCare 1 FAT NECROSIS TRAUMATIC Cell rupture Seat-Belt injury Blunt trauma Iatrogenic injury Surgery, Flaps, Radiotherapy Pathology
SIGNIFICANT OTHERS Miscellaneous Benign Breast Conditions Epworth HealthCare 1 FAT NECROSIS TRAUMATIC Cell rupture Seat-Belt injury Blunt trauma Iatrogenic injury Surgery, Flaps, Radiotherapy Pathology
Mousa. Israa Ayed. Abdullah AlZibdeh. 0 P a g e
 1 Mousa Israa Ayed Abdullah AlZibdeh 0 P a g e Breast pathology The basic histological units of the breast are called lobules, which are composed of glandular epithelial cells (luminal cells) resting on
1 Mousa Israa Ayed Abdullah AlZibdeh 0 P a g e Breast pathology The basic histological units of the breast are called lobules, which are composed of glandular epithelial cells (luminal cells) resting on
Excerpts from the American College of Surgeons Educational Courses about Breast Disease:
 1 Excerpts from the American College of Surgeons Educational Courses about Breast Disease: Gynecomastia Gynecomastia is a benign enlargement of the male breast that can be unilateral or bilateral. It typically
1 Excerpts from the American College of Surgeons Educational Courses about Breast Disease: Gynecomastia Gynecomastia is a benign enlargement of the male breast that can be unilateral or bilateral. It typically
Breast Update Therese Cusick MS MD FACS
 Breast Update 2017 Therese Cusick MS MD FACS Conflict of Interest Disclosure Nothing to disclose Sources Adapted from SESAP- Surgical Education and Self-Assessment program American College of Surgeons
Breast Update 2017 Therese Cusick MS MD FACS Conflict of Interest Disclosure Nothing to disclose Sources Adapted from SESAP- Surgical Education and Self-Assessment program American College of Surgeons
Non-mass Enhancement on Breast MRI. Aditi A. Desai, MD Margaret Ann Mays, MD
 Non-mass Enhancement on Breast MRI Aditi A. Desai, MD Margaret Ann Mays, MD Breast MRI Important screening and diagnostic tool, given its high sensitivity for breast cancer detection Breast MRI - Indications
Non-mass Enhancement on Breast MRI Aditi A. Desai, MD Margaret Ann Mays, MD Breast MRI Important screening and diagnostic tool, given its high sensitivity for breast cancer detection Breast MRI - Indications
Criteria of Malignancy. Evaluation Score
 30 5 Diagnostic Criteria Criteria of Malignancy Table 5.2 lists criteria in contrast-enhancing MR mammography that strongly indicate the presence of malignancy or are unspecific. Unifactorial evaluation
30 5 Diagnostic Criteria Criteria of Malignancy Table 5.2 lists criteria in contrast-enhancing MR mammography that strongly indicate the presence of malignancy or are unspecific. Unifactorial evaluation
CLINICAL SIGNIFICANCE OF BENIGN EPITHELIAL CHANGES
 Papillomas. Papillomas are composed of multiple branching fibrovascular cores, each having a connective tissue axis lined by luminal and myoepithelial cells ( Fig. 23-11 ). Growth occurs within a dilated
Papillomas. Papillomas are composed of multiple branching fibrovascular cores, each having a connective tissue axis lined by luminal and myoepithelial cells ( Fig. 23-11 ). Growth occurs within a dilated
For more information about how to cite these materials visit
 Author: Vincent M. Cimmino, M.D., 2011 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Share Alike 3.0 License: http://creativecommons.org/licenses/by-sa/3.0/
Author: Vincent M. Cimmino, M.D., 2011 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Share Alike 3.0 License: http://creativecommons.org/licenses/by-sa/3.0/
Case Scenario 1: This case has been slightly modified from the case presented during the live session to add clarity.
 Case Scenario 1: This case has been slightly modified from the case presented during the live session to add clarity. Background: 46 year old married premenopausal female with dense breasts has noticed
Case Scenario 1: This case has been slightly modified from the case presented during the live session to add clarity. Background: 46 year old married premenopausal female with dense breasts has noticed
CPC 4 Breast Cancer. Rochelle Harwood, a 35 year old sales assistant, presents to her GP because she has noticed a painless lump in her left breast.
 CPC 4 Breast Cancer Rochelle Harwood, a 35 year old sales assistant, presents to her GP because she has noticed a painless lump in her left breast. 1. What are the most likely diagnoses of this lump? Fibroadenoma
CPC 4 Breast Cancer Rochelle Harwood, a 35 year old sales assistant, presents to her GP because she has noticed a painless lump in her left breast. 1. What are the most likely diagnoses of this lump? Fibroadenoma
Case Scenario 1: This case has been slightly modified from the case presented during the live session to add clarity.
 Case Scenario 1: This case has been slightly modified from the case presented during the live session to add clarity. Background: 46 year old married premenopausal female with dense breasts has noticed
Case Scenario 1: This case has been slightly modified from the case presented during the live session to add clarity. Background: 46 year old married premenopausal female with dense breasts has noticed
Timby/Smith: Introductory Medical-Surgical Nursing, 9/e
 Timby/Smith: Introductory Medical-Surgical Nursing, 9/e Chapter 60: Caring for Clients With Breast Disorders Slide 1 Infectious and Inflammatory Breast Disorders: Mastitis Pathophysiology and Etiology
Timby/Smith: Introductory Medical-Surgical Nursing, 9/e Chapter 60: Caring for Clients With Breast Disorders Slide 1 Infectious and Inflammatory Breast Disorders: Mastitis Pathophysiology and Etiology
Breast Cancer Update 2018 The Latest in Diagnosis and Treatment SARATH K, PALAKODETI, DO, FAACS GENERAL, BREAST, AND COSMETIC SURGEON TOLEDO CLINIC
 Breast Cancer Update 2018 The Latest in Diagnosis and Treatment SARATH K, PALAKODETI, DO, FAACS GENERAL, BREAST, AND COSMETIC SURGEON TOLEDO CLINIC Objectives Identify breast lesions and masses, and know
Breast Cancer Update 2018 The Latest in Diagnosis and Treatment SARATH K, PALAKODETI, DO, FAACS GENERAL, BREAST, AND COSMETIC SURGEON TOLEDO CLINIC Objectives Identify breast lesions and masses, and know
Breast Cancer. Excess Estrogen Exposure. Alcohol use + Pytoestrogens? Abortion. Infertility treatment?
 Breast Cancer Breast Cancer Excess Estrogen Exposure Nulliparity or late pregnancy + Early menarche + Late menopause + Cystic ovarian disease + External estrogens exposure + Breast Cancer Excess Estrogen
Breast Cancer Breast Cancer Excess Estrogen Exposure Nulliparity or late pregnancy + Early menarche + Late menopause + Cystic ovarian disease + External estrogens exposure + Breast Cancer Excess Estrogen
Case 1. BREAST CANCER From Diagnosis to Treatment: The Role of Primary Care
 BREAST CANCER From Diagnosis to Treatment: The Role of Primary Care Leah Karliner, MD MAS University of California San Francisco Primary Care Medicine Update 2009 April 2009 Case 1 AR, a 60 year old African
BREAST CANCER From Diagnosis to Treatment: The Role of Primary Care Leah Karliner, MD MAS University of California San Francisco Primary Care Medicine Update 2009 April 2009 Case 1 AR, a 60 year old African
University of Washington Radiology Review Course: Strange and Specific Diagnoses. Case #1
 University of Washington Radiology Review Course: Strange and Specific Diagnoses Katherine E. Dee, MD Seattle Breast Center Via Radiology 2014 Case #1 37 year old presents with bilateral palpable lumps.
University of Washington Radiology Review Course: Strange and Specific Diagnoses Katherine E. Dee, MD Seattle Breast Center Via Radiology 2014 Case #1 37 year old presents with bilateral palpable lumps.
Case #1: 75 y/o Male (treated and followed by prostate cancer oncology specialist ).
.") SOLID TUMORS WORKSHOP Cases for review Prostate Cancer Case #1: 75 y/o Male (treated and followed by prostate cancer oncology specialist ). January 2009 PSA 4.4, 20% free; August 2009 PSA 5.2; Sept 2009
SOLID TUMORS WORKSHOP Cases for review Prostate Cancer Case #1: 75 y/o Male (treated and followed by prostate cancer oncology specialist ). January 2009 PSA 4.4, 20% free; August 2009 PSA 5.2; Sept 2009
Breast Cancer: Selected Topics for the Primary Care Clinician
 Breast Cancer: Selected Topics for the Primary Care Clinician Leah Karliner, MD MAS October 2009 Primary Care Medicine: Principles and Practice OUTLINE Incidence and Mortality Risk Factors and Risk Reduction/Prevention
Breast Cancer: Selected Topics for the Primary Care Clinician Leah Karliner, MD MAS October 2009 Primary Care Medicine: Principles and Practice OUTLINE Incidence and Mortality Risk Factors and Risk Reduction/Prevention
Armed Forces Institute of Pathology.
 Armed Forces Institute of Pathology www.radpath.com Armed Forces Institute of Pathology Breast Disease www.radpath.org Armed Forces Institute of Pathology Interpretation of Breast MRI Leonard M. Glassman
Armed Forces Institute of Pathology www.radpath.com Armed Forces Institute of Pathology Breast Disease www.radpath.org Armed Forces Institute of Pathology Interpretation of Breast MRI Leonard M. Glassman
Disclaimer no conflict of interest
 Disclaimer no conflict of interest Benign Breast Disease Alison Hayes FRACS Content Clinical assessment of the breast Triple assessment Focal nodularity Breast pain Cysts Infection Nipple discharge Gynaecomastia
Disclaimer no conflict of interest Benign Breast Disease Alison Hayes FRACS Content Clinical assessment of the breast Triple assessment Focal nodularity Breast pain Cysts Infection Nipple discharge Gynaecomastia
Treatment options for the precancerous Atypical Breast lesions. Prof. YOUNG-JIN SUH The Catholic University of Korea
 Treatment options for the precancerous Atypical Breast lesions Prof. YOUNG-JIN SUH The Catholic University of Korea Not so benign lesions? Imaging abnormalities(10% recall) lead to diagnostic evaluation,
Treatment options for the precancerous Atypical Breast lesions Prof. YOUNG-JIN SUH The Catholic University of Korea Not so benign lesions? Imaging abnormalities(10% recall) lead to diagnostic evaluation,
Breast Imaging: Multidisciplinary Approach. Madelene Lewis, MD Assistant Professor Associate Program Director Medical University of South Carolina
 Breast Imaging: Multidisciplinary Approach Madelene Lewis, MD Assistant Professor Associate Program Director Medical University of South Carolina No Disclosures Objectives Discuss a multidisciplinary breast
Breast Imaging: Multidisciplinary Approach Madelene Lewis, MD Assistant Professor Associate Program Director Medical University of South Carolina No Disclosures Objectives Discuss a multidisciplinary breast
COMMON BENIGN DISORDERS AND DISEASES OF THE BREAST
 COMMON BENIGN DISORDERS AND DISEASES OF THE BREAST Aberrations of Normal Development and Involution (ANDI). The basic principles underlying the aberrations of normal development and involution (ANDI) classification
COMMON BENIGN DISORDERS AND DISEASES OF THE BREAST Aberrations of Normal Development and Involution (ANDI). The basic principles underlying the aberrations of normal development and involution (ANDI) classification
Mammographic imaging of nonpalpable breast lesions. Malai Muttarak, MD Department of Radiology Chiang Mai University Chiang Mai, Thailand
 Mammographic imaging of nonpalpable breast lesions Malai Muttarak, MD Department of Radiology Chiang Mai University Chiang Mai, Thailand Introduction Contents Mammographic signs of nonpalpable breast cancer
Mammographic imaging of nonpalpable breast lesions Malai Muttarak, MD Department of Radiology Chiang Mai University Chiang Mai, Thailand Introduction Contents Mammographic signs of nonpalpable breast cancer
Breast Health. Learning Objectives. Breast Anatomy. Poll Question. Breast Anatomy
 Learning Objectives Describe breast anatomy to a patient Breast Health Answer questions about causes of breast pain and masses Explain breast cancer screening/diagnostic modalities Appropriately triage
Learning Objectives Describe breast anatomy to a patient Breast Health Answer questions about causes of breast pain and masses Explain breast cancer screening/diagnostic modalities Appropriately triage
Case Scenario 1 History and Physical 3/15/13 Imaging Pathology
 Case Scenario 1 History and Physical 3/15/13 The patient is an 84 year old white female who presented with an abnormal mammogram. The patient has a five year history of refractory anemia with ringed sideroblasts
Case Scenario 1 History and Physical 3/15/13 The patient is an 84 year old white female who presented with an abnormal mammogram. The patient has a five year history of refractory anemia with ringed sideroblasts
ACRIN 6666 Therapeutic Surgery Form
 S1 ACRIN 6666 Therapeutic Surgery Form 6666 Instructions: Complete a separate S1 form for each separate area of each breast excised with the intent to treat a cancer (e.g. each lumpectomy or mastectomy).
S1 ACRIN 6666 Therapeutic Surgery Form 6666 Instructions: Complete a separate S1 form for each separate area of each breast excised with the intent to treat a cancer (e.g. each lumpectomy or mastectomy).
BREAST CANCER SURGERY. Dr. John H. Donohue
 Dr. John H. Donohue HISTORY References to breast surgery in ancient Egypt (ca 3000 BCE) Mastectomy described in numerous medieval texts Petit formulated organized approach in 18 th Century Improvements
Dr. John H. Donohue HISTORY References to breast surgery in ancient Egypt (ca 3000 BCE) Mastectomy described in numerous medieval texts Petit formulated organized approach in 18 th Century Improvements
Malignant Breast disorders
 Malignant Breast disorders RISK FACTORS FOR BREAST CANCER Family Hx.: first- and second-degree relatives with breast cancer and their age at diagnosis. RISK FACTORS FOR BREAST CANCER (cont.) Hormonal Risk
Malignant Breast disorders RISK FACTORS FOR BREAST CANCER Family Hx.: first- and second-degree relatives with breast cancer and their age at diagnosis. RISK FACTORS FOR BREAST CANCER (cont.) Hormonal Risk
Breast Cancer Diagnosis, Treatment and Follow-up
 Breast Cancer Diagnosis, Treatment and Follow-up What is breast cancer? Each of the body s organs, including the breast, is made up of many types of cells. Normally, healthy cells grow and divide to produce
Breast Cancer Diagnosis, Treatment and Follow-up What is breast cancer? Each of the body s organs, including the breast, is made up of many types of cells. Normally, healthy cells grow and divide to produce
Practice of Axilla Surgery
 Summer School of Breast Disease 2016 Practice of Axilla Surgery Axillary Lymph Node Dissection & Sentinel Lymph Node Biopsy 연세의대외과 박세호 Contents Anatomy of the axilla Axillary lymph node dissection (ALND)
Summer School of Breast Disease 2016 Practice of Axilla Surgery Axillary Lymph Node Dissection & Sentinel Lymph Node Biopsy 연세의대외과 박세호 Contents Anatomy of the axilla Axillary lymph node dissection (ALND)
Breast Cancer Update. Jeff Falk MD, FACS Surgical Oncology, St. John/ Providence Ascension Michigan Health System
 Breast Cancer Update Jeff Falk MD, FACS Surgical Oncology, St. John/ Providence Ascension Michigan Health System Breast Cancer The leading cause of malignancy related death among American women 15 to 54
Breast Cancer Update Jeff Falk MD, FACS Surgical Oncology, St. John/ Providence Ascension Michigan Health System Breast Cancer The leading cause of malignancy related death among American women 15 to 54
Breast Cancer Basics. Clinical Oncology for Public Health Professionals. Ben Ho Park, MD, PhD
 This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike License. Your use of this material constitutes acceptance of that license and the conditions of use of materials on this
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike License. Your use of this material constitutes acceptance of that license and the conditions of use of materials on this
Follow-up of Abnormal Breast Findings. E.J. Siegl RN, OCN, MA, CBCN BCCCP Nurse Consultant January 2012
 Follow-up of Abnormal Breast Findings E.J. Siegl RN, OCN, MA, CBCN BCCCP Nurse Consultant January 2012 Abnormal Breast Findings include the following: CBE results of: Nipple discharge, no palpable mass
Follow-up of Abnormal Breast Findings E.J. Siegl RN, OCN, MA, CBCN BCCCP Nurse Consultant January 2012 Abnormal Breast Findings include the following: CBE results of: Nipple discharge, no palpable mass
Debate Axillary dissection - con. Prof. Dr. Rodica Anghel Institute of Oncology Bucharest
 Debate Axillary dissection - con Prof. Dr. Rodica Anghel Institute of Oncology Bucharest Summer School of Oncology, third edition Updated Oncology 2015: State of the Art News & Challenging Topics Bucharest,
Debate Axillary dissection - con Prof. Dr. Rodica Anghel Institute of Oncology Bucharest Summer School of Oncology, third edition Updated Oncology 2015: State of the Art News & Challenging Topics Bucharest,
Imaging the Symptomatic Patient. Avice M.O Connell MD,FACR,FSBI Professor of Imaging Sciences Director, Women s Imaging University of Rochester
 Imaging the Symptomatic Patient Avice M.O Connell MD,FACR,FSBI Professor of Imaging Sciences Director, Women s Imaging University of Rochester The four most common symptoms Mass Pain Discharge Infection
Imaging the Symptomatic Patient Avice M.O Connell MD,FACR,FSBI Professor of Imaging Sciences Director, Women s Imaging University of Rochester The four most common symptoms Mass Pain Discharge Infection
Benign Breast Conditions. Dr. Kim Kelly, CCFP, FCFP Breast Expert, CBCP February, 2015
 Benign Breast Conditions Dr. Kim Kelly, CCFP, FCFP Breast Expert, CBCP February, 2015 Kim Kelly M.D. U of A Family Medicine 1996 2011 Special Interest in Breast Medicine designation, CP&S 2012 15, Breast
Benign Breast Conditions Dr. Kim Kelly, CCFP, FCFP Breast Expert, CBCP February, 2015 Kim Kelly M.D. U of A Family Medicine 1996 2011 Special Interest in Breast Medicine designation, CP&S 2012 15, Breast
Breast Cancer FAQ. How does Breast Cancer spread? Breast cancer spreads by invading into
 FAQ Breast Cancer What is Breast Cancer? Breast Cancer is the second leading cause of cancer deaths in women today (second to lung cancer) and is the most common cancer among women excluding non-melanoma
FAQ Breast Cancer What is Breast Cancer? Breast Cancer is the second leading cause of cancer deaths in women today (second to lung cancer) and is the most common cancer among women excluding non-melanoma
Basement membrane in lobule.
 Bahram Memar, MD Basement membrane in lobule. Normal lobule-luteal phase Normal lobule-follicular phase Lactating breast Greater than 95% are adenocarcinomas in situ carcinomas and invasive carcinomas.
Bahram Memar, MD Basement membrane in lobule. Normal lobule-luteal phase Normal lobule-follicular phase Lactating breast Greater than 95% are adenocarcinomas in situ carcinomas and invasive carcinomas.
Jordan University Faculty Of Medicine. Breast. Dr. Ahmed Salman. Assistant professor of anatomy & embryology
 Jordan University Faculty Of Medicine Breast Dr. Ahmed Salman Assistant professor of anatomy & embryology The breasts are specialized accessory glands of the skin that secretes milk. They are situated
Jordan University Faculty Of Medicine Breast Dr. Ahmed Salman Assistant professor of anatomy & embryology The breasts are specialized accessory glands of the skin that secretes milk. They are situated
Imaging Guidelines for Breast Cancer Screening
 Imaging Guidelines for Breast Cancer Screening Sarah Colwick, MD Dr. Sarah Colwick was born and raised in Sikeston, MO. She attended college and medical school at the University of Missouri-Kansas City
Imaging Guidelines for Breast Cancer Screening Sarah Colwick, MD Dr. Sarah Colwick was born and raised in Sikeston, MO. She attended college and medical school at the University of Missouri-Kansas City
Breast Cancer Screening and Treatment Mrs Belinda Scott Breast Surgeon Breast Associates Auckland
 Breast Cancer Screening and Treatment 2009 Mrs Belinda Scott Breast Surgeon Breast Associates Auckland BREAST CANCER THE PROBLEM 1.1 million women per year 410,000 deaths each year Increasing incidence
Breast Cancer Screening and Treatment 2009 Mrs Belinda Scott Breast Surgeon Breast Associates Auckland BREAST CANCER THE PROBLEM 1.1 million women per year 410,000 deaths each year Increasing incidence
Common Problem of the Breast
 Common Problem of the Breast Breast Lumps, Nipple Discharge, and Pain 本講義表格資料取自 Dains, J.E., Baumann, L.C., & Scheibel, P. (2007). Advanced assessment and clinical diagnosis in primary care. (3rd ed).
Common Problem of the Breast Breast Lumps, Nipple Discharge, and Pain 本講義表格資料取自 Dains, J.E., Baumann, L.C., & Scheibel, P. (2007). Advanced assessment and clinical diagnosis in primary care. (3rd ed).
Breast Cancer. Dr Rodney Itaki Anatomical Pathology Discipline Division of Pathology
 Breast Cancer Dr Rodney Itaki Anatomical Pathology Discipline Division of Pathology Muscles Muscles underneath the breasts separating them from the ribs Breast has no muscle tissue 2 Female Breast Anatomy
Breast Cancer Dr Rodney Itaki Anatomical Pathology Discipline Division of Pathology Muscles Muscles underneath the breasts separating them from the ribs Breast has no muscle tissue 2 Female Breast Anatomy
BREAST SURGERY - SYLLABUS 2014
 UNION EUROPÉENNE DES MÉDECINS SPÉCIALISTES Association internationale sans but lucratif International non-profit organisation AVENUE DE LA COURONNE, 20 T +32 2 649 51 64 BREAST SURGERY - SYLLABUS 2014
UNION EUROPÉENNE DES MÉDECINS SPÉCIALISTES Association internationale sans but lucratif International non-profit organisation AVENUE DE LA COURONNE, 20 T +32 2 649 51 64 BREAST SURGERY - SYLLABUS 2014
General Information Key Points
 The content of this booklet was adapted from content originally published by the National Cancer Institute. Male Breast Cancer Treatment (PDQ ) Patient Version. Updated September 29,2017. https://www.cancer.gov/types/breast/patient/male-breast-treatment-pdq
The content of this booklet was adapted from content originally published by the National Cancer Institute. Male Breast Cancer Treatment (PDQ ) Patient Version. Updated September 29,2017. https://www.cancer.gov/types/breast/patient/male-breast-treatment-pdq
Ultrasound of the Breast BASICS FOR THE ORDERING CLINICIAN
 Ultrasound of the Breast BASICS FOR THE ORDERING CLINICIAN Breast Ultrasound Anatomy Skin Breast Parenchyma Pectoralis Fascia Pectoralis Breast Ultrasound Anatomy Indications for Breast Ultrasound Palpable
Ultrasound of the Breast BASICS FOR THE ORDERING CLINICIAN Breast Ultrasound Anatomy Skin Breast Parenchyma Pectoralis Fascia Pectoralis Breast Ultrasound Anatomy Indications for Breast Ultrasound Palpable
Recent advances in breast cancers
 Recent advances in breast cancers Breast cancer is a hetrogenous disease due to distinct genetic alterations. Similar morphological subtypes show variation in clinical behaviour especially in response
Recent advances in breast cancers Breast cancer is a hetrogenous disease due to distinct genetic alterations. Similar morphological subtypes show variation in clinical behaviour especially in response
Case Scenario 1. 2/15/2011 The patient received IMRT 45 Gy at 1.8 Gy per fraction for 25 fractions.
 Case Scenario 1 1/3/11 A 57 year old white female presents for her annual mammogram and is found to have a suspicious area of calcification, spread out over at least 4 centimeters. She is scheduled to
Case Scenario 1 1/3/11 A 57 year old white female presents for her annual mammogram and is found to have a suspicious area of calcification, spread out over at least 4 centimeters. She is scheduled to
Benign, Reactive and Inflammatory Lesions of the Breast
 Benign, Reactive and Inflammatory Lesions of the Breast Marilin Rosa, MD Associate Member Section Head of Breast Pathology Department of Anatomic Pathology Program Director, Breast Pathology Fellowship
Benign, Reactive and Inflammatory Lesions of the Breast Marilin Rosa, MD Associate Member Section Head of Breast Pathology Department of Anatomic Pathology Program Director, Breast Pathology Fellowship
Breast Cancer Task Force of the Greater Miami Valley A collaborative effort of health care professionals and breast cancer survivors in the Greater
 Breast Cancer Task Force of the Greater Miami Valley A collaborative effort of health care professionals and breast cancer survivors in the Greater Dayton Area Last Updated Fall 2014 TABLE OF CONTENTS
Breast Cancer Task Force of the Greater Miami Valley A collaborative effort of health care professionals and breast cancer survivors in the Greater Dayton Area Last Updated Fall 2014 TABLE OF CONTENTS
ANNEX 1 OBJECTIVES. At the completion of the training period, the fellow should be able to:
 1 ANNEX 1 OBJECTIVES At the completion of the training period, the fellow should be able to: 1. Breast Surgery Evaluate and manage common benign and malignant breast conditions. Assess the indications
1 ANNEX 1 OBJECTIVES At the completion of the training period, the fellow should be able to: 1. Breast Surgery Evaluate and manage common benign and malignant breast conditions. Assess the indications
Evolving Practices in Breast Cancer Management
 Evolving Practices in Breast Cancer Management The Georgia Tumor Registrars Association 2016 Priscilla R. Strom, MD, FACS Objectives 1. understand newer indications for neoadjuvant treatment 2. understand
Evolving Practices in Breast Cancer Management The Georgia Tumor Registrars Association 2016 Priscilla R. Strom, MD, FACS Objectives 1. understand newer indications for neoadjuvant treatment 2. understand
Case study 1. Rie Horii, M.D., Ph.D. Division of Pathology Cancer Institute Hospital, Japanese Foundation for Cancer Research
 NCCN/JCCNB Seminar in Japan April 15, 2012 Case study 1 Rie Horii, M.D., Ph.D. Division of Pathology Cancer Institute Hospital, Japanese Foundation for Cancer Research Present illness: A 50y.o.premenopausal
NCCN/JCCNB Seminar in Japan April 15, 2012 Case study 1 Rie Horii, M.D., Ph.D. Division of Pathology Cancer Institute Hospital, Japanese Foundation for Cancer Research Present illness: A 50y.o.premenopausal
Breast Health Programme at S.G.P.G.I.
 Breast Health Programme at S.G.P.G.I. The first decade Department of Endocrine Surgery Br.H.P.: Components Breast Clinic Surgery Resident training Research Community Education/ Awareness Br.H.P.: Clinical
Breast Health Programme at S.G.P.G.I. The first decade Department of Endocrine Surgery Br.H.P.: Components Breast Clinic Surgery Resident training Research Community Education/ Awareness Br.H.P.: Clinical
Common Breast Problems: Breast Pain
 Common Breast Problems: Breast Pain Breast pain is the most common symptom that brings women to their physician. In general, there are two common presentations of breast pain: cyclic and noncyclic. Breast
Common Breast Problems: Breast Pain Breast pain is the most common symptom that brings women to their physician. In general, there are two common presentations of breast pain: cyclic and noncyclic. Breast
Breast Cancer Risk Assessment and Prevention
 Breast Cancer Risk Assessment and Prevention Katherine B. Lee, MD, FACP October 4, 2017 STATISTICS More than 252,000 cases of breast cancer will be diagnosed this year alone. About 40,000 women will die
Breast Cancer Risk Assessment and Prevention Katherine B. Lee, MD, FACP October 4, 2017 STATISTICS More than 252,000 cases of breast cancer will be diagnosed this year alone. About 40,000 women will die
Advances in Localized Breast Cancer
 Advances in Localized Breast Cancer Melissa Camp, MD, MPH and Fariba Asrari, MD June 18, 2018 Moderated by Elissa Bantug 1 Advances in Surgery for Breast Cancer Melissa Camp, MD June 18, 2018 2 Historical
Advances in Localized Breast Cancer Melissa Camp, MD, MPH and Fariba Asrari, MD June 18, 2018 Moderated by Elissa Bantug 1 Advances in Surgery for Breast Cancer Melissa Camp, MD June 18, 2018 2 Historical
Index. C Calcifications fat necrosis 1, 61 fat necrosis 4, 69 nipple/peri-areolar involvement 1, 165
 A ADH. See Atypical ductal hyperplasia (ADH) American College of Radiology (ACR), BI-RADS background parenchymal enhancement, 8, 9, 81, 82 fibroglandular tissue guidelines, 6 American Joint Committee on
A ADH. See Atypical ductal hyperplasia (ADH) American College of Radiology (ACR), BI-RADS background parenchymal enhancement, 8, 9, 81, 82 fibroglandular tissue guidelines, 6 American Joint Committee on
ROLE OF MRI IN SCREENING, DIAGNOSIS AND MANAGEMENT OF BREAST CANCER. B.Zandi Professor of Radiology
 ROLE OF MRI IN SCREENING, DIAGNOSIS AND MANAGEMENT OF BREAST CANCER B.Zandi Professor of Radiology Introduction In the USA, Breast Cancer is : The Most Common Non-Skin Cancer The Second Leading cause of
ROLE OF MRI IN SCREENING, DIAGNOSIS AND MANAGEMENT OF BREAST CANCER B.Zandi Professor of Radiology Introduction In the USA, Breast Cancer is : The Most Common Non-Skin Cancer The Second Leading cause of
Abid Irshad, MD Director Breast Imaging. Medical University of South Carolina Charleston
 Abid Irshad, MD Director Breast Imaging Medical University of South Carolina Charleston Cases Financial disclosure: I or my family have no financial interest related to the material discussed in this presentation
Abid Irshad, MD Director Breast Imaging Medical University of South Carolina Charleston Cases Financial disclosure: I or my family have no financial interest related to the material discussed in this presentation
THE MALE BREAST CARCINOMA: EARLY DETECTION HOPE. Author (s) Supreethi Kohli a, Pragya Garg b
 Supreethi Kohli a, Pragya Garg b") Case Report ABSTRACT - Male breast cancer is exceptionally rare and accounts for less than 0.25% of male malignancies and approximately 0.5-1% of all breast cancer (both genders). Mammography of the male
Case Report ABSTRACT - Male breast cancer is exceptionally rare and accounts for less than 0.25% of male malignancies and approximately 0.5-1% of all breast cancer (both genders). Mammography of the male
Q&A. Fabulous Prizes. Collecting Cancer Data: Breast 4/4/13. NAACCR Webinar Series Collecting Cancer Data Breast
 Collecting Cancer Data Breast NAACCR 2012 2013 Webinar Series Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
Collecting Cancer Data Breast NAACCR 2012 2013 Webinar Series Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
Surgery for Breast Cancer
 Surgery for Breast Cancer 1750 Mastectomy - Petit 1894 Radical mastectomy Halsted Extended, Super radical mastectomy 1948 Modified radical mastectomy Patey 1950-60 WLE & RT Baclesse, Mustakallio 1981-85
Surgery for Breast Cancer 1750 Mastectomy - Petit 1894 Radical mastectomy Halsted Extended, Super radical mastectomy 1948 Modified radical mastectomy Patey 1950-60 WLE & RT Baclesse, Mustakallio 1981-85
Patient Guide to Breast Cancer Surgery and Treatment. Mercy Cancer Services. baggotstreet.mercy.net/benefits. Your life is our life s work.
 Patient Guide to Breast Cancer Surgery and Treatment Your life is our life s work. baggotstreet.mercy.net/benefits Mercy Cancer Services Introduction An estimated one out of eight women will develop breast
Patient Guide to Breast Cancer Surgery and Treatment Your life is our life s work. baggotstreet.mercy.net/benefits Mercy Cancer Services Introduction An estimated one out of eight women will develop breast
04/10/2018. Intraductal Papillary Neoplasms Of Breast INTRADUCTAL PAPILLOMA
 Intraductal Papillary Neoplasms Of Breast Savitri Krishnamurthy MD Professor of Pathology Deputy Division Head The University of Texas MD Anderson Cancer Center 25 th Annual Seminar in Pathology Pittsburgh,
Intraductal Papillary Neoplasms Of Breast Savitri Krishnamurthy MD Professor of Pathology Deputy Division Head The University of Texas MD Anderson Cancer Center 25 th Annual Seminar in Pathology Pittsburgh,
What is Cancer? Petra Ketterl, MD Medical Oncology and Functional Medicine
 What is Cancer? Petra Ketterl, MD Medical Oncology and Functional Medicine What is Cancer? Layman s terms: cancer starts when cells grow out of control (in any place in the body) and crowd out normal cells
What is Cancer? Petra Ketterl, MD Medical Oncology and Functional Medicine What is Cancer? Layman s terms: cancer starts when cells grow out of control (in any place in the body) and crowd out normal cells
Overview. Who Gets Breast Cancer? Breast cancer can strike anyone, although it does tend to follow particular trends.
 Overview Often women fail to pay attention to breast health unless they are forced to while breast feeding a newborn or when a serious condition like breast cancer occurs. Like most bodily processes, the
Overview Often women fail to pay attention to breast health unless they are forced to while breast feeding a newborn or when a serious condition like breast cancer occurs. Like most bodily processes, the
STAGE CATEGORY DEFINITIONS
 CLINICAL Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery TX Tis Tis (DCIS) Tis (LCIS) Tis (Paget s) T1 T1mi T1a T1b T1c a b c
CLINICAL Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery TX Tis Tis (DCIS) Tis (LCIS) Tis (Paget s) T1 T1mi T1a T1b T1c a b c
BREAST CANCER BREAST CANCER
 BREAST CANCER George Raptis, M.D., M.B.A Division of Medical Oncology & Hematology College of Physicians & Surgeons Columbia University BREAST CANCER Epidemiology - Commonest cancer in women - About 235,000
BREAST CANCER George Raptis, M.D., M.B.A Division of Medical Oncology & Hematology College of Physicians & Surgeons Columbia University BREAST CANCER Epidemiology - Commonest cancer in women - About 235,000
Benign Breast Disease & Breast Screening. Leah Kelley, MD OPSC Conference Monterey, CA September, 2018
 Benign Breast Disease & Breast Screening Leah Kelley, MD OPSC Conference Monterey, CA September, 2018 Why this matters to YOU Breast symptoms constitute 3% of all visits by female patients (29.7 per 1,000)
Benign Breast Disease & Breast Screening Leah Kelley, MD OPSC Conference Monterey, CA September, 2018 Why this matters to YOU Breast symptoms constitute 3% of all visits by female patients (29.7 per 1,000)
Leonard M. Glassman MD
 BI-RADS The New BI-RADS Leonard M. Glassman MD FACR Former Chief of Breast Imaging American Institute for Radiologic Pathology Washington Radiology Associates, PC Breast Imaging Reporting and Data System
BI-RADS The New BI-RADS Leonard M. Glassman MD FACR Former Chief of Breast Imaging American Institute for Radiologic Pathology Washington Radiology Associates, PC Breast Imaging Reporting and Data System
Breast Imaging Essentials
 Breast Imaging Essentials Module 5 Transcript 2016 ASRT. All rights reserved. Breast Imaging Essentials Module 5 Pathology 1. ASRT Animation 2. Welcome Welcome to Module 5 of Breast Imaging Essentials
Breast Imaging Essentials Module 5 Transcript 2016 ASRT. All rights reserved. Breast Imaging Essentials Module 5 Pathology 1. ASRT Animation 2. Welcome Welcome to Module 5 of Breast Imaging Essentials
Types of Breast Cancer
 IOWA RADIOLOGY 1 Types of Breast Cancer 515-226-9810 Ankeny Clive Downtown Des Moines IOWA RADIOLOGY 1 Table of Contents Introduction... 1 Ductal Carcinoma... 2 Paget s Disease of the Nipple... 8 Lobular
IOWA RADIOLOGY 1 Types of Breast Cancer 515-226-9810 Ankeny Clive Downtown Des Moines IOWA RADIOLOGY 1 Table of Contents Introduction... 1 Ductal Carcinoma... 2 Paget s Disease of the Nipple... 8 Lobular
5.1 Breast, Anatomy. 70
 Chapter 5 Breast 5.1 Breast, Anatomy Breasts, also called Mamma are mammary glands, subcutaneously placed on the ventral side of the trunk in mammalian species, and develop for the sole purpose of secreting
Chapter 5 Breast 5.1 Breast, Anatomy Breasts, also called Mamma are mammary glands, subcutaneously placed on the ventral side of the trunk in mammalian species, and develop for the sole purpose of secreting