Follow-up of Abnormal Breast Findings. E.J. Siegl RN, OCN, MA, CBCN BCCCP Nurse Consultant January 2012
|
|
|
- Joan Wilkins
- 5 years ago
- Views:
Transcription
1 Follow-up of Abnormal Breast Findings E.J. Siegl RN, OCN, MA, CBCN BCCCP Nurse Consultant January 2012
2 Abnormal Breast Findings include the following: CBE results of: Nipple discharge, no palpable mass Asymmetric thickening/nodularity Skin Changes (Peau d orange, Erythema, Nipple Excoriation, Scaling/Eczema) Dominant Mass? Unilateral Breast Pain Mammogram results of ACR 0 Assessment Incomplete ACR 4 Suspicious Abnormality, ACR 5 Highly Suggestive of Malignancy
3 Abnormal CBE Results Nipple Discharge Third most common breast complaint by women seeking medical attention after lumps and breast pain During breast self exam, fluid may be expressed from the breasts of 50% to 60% of Caucasian and African-American women and 40% of Asian-American women
4 Nipple Discharge cont. Palpation of the nipple in a woman who does not have a history of persistent spontaneous nipple discharge - not recommended Rationale: Non-spontaneous nipple discharge is a normal physiological phenomenon and of no clinical consequence Infections (E.g. abscess) should be treated with incision and drainage or repeated aspiration if needed (consider antibiotics)
5 Nipple Discharge is of Concern if it is: Blood stained, serosanguinous, serous (watery) with a red, pink, or brown color, or clear 90% of bloody discharges are intraductal papillomas; 10% are breast cancers) appears spontaneously without squeezing the nipple persistent on one side only (unilateral) a fluid other than breast milk
 should be referred for diagnostic breast")
6 Nipple Discharge cont. Non-lactating women who present with a unilateral, spontaneous nipple discharge (whether clear, serous or bloody) should be referred for diagnostic breast imaging and surgical evaluation Diagnostic mammograms in these instances may be negative, but should never delay further diagnostic evaluation
7 Types of Nipple Discharge Discharge Color Milky involves more than one duct Clear, watery or yellowish involving one duct Clear, watery or yellowish involving multiple ducts or bilateral Risk galactorrhea due to medicines or anovulation breast cancer or fibrocystic breast condition fibrocystic breast condition Pink, rusty or bloody involving one or more ducts Greenish black or brown, sticky, tarry involving one duct Greenish black or brown, sticky, tarry involving more than one duct Creamy, pus-like (purulent)- involving any duct intraductal papilloma, in situ or invasive breast cancer mammary duct ectasia, breast cancer mammary duct ectasia infection, abscess, mastitis
8 Nipple Discharge Follow-up CBE: Identify color/consistency of discharge Mammogram: If a suspicious mass together with nipple discharge present refer for additional imaging? and surgical consult Further Diagnostic Tests: --Ductogram/Galactogram not a reimbursable BCCCP code. --Contact NC may map procedure to a BCCCP CPT code. Evaluated on a case by case basis.

9 Nipple Discharge Evaluation A 50-year-old woman with serous discharge from her right nipple. Galactography reveals contrastagent filling defect approximately 4 cm from her nipple. Cytology of the smears from her nipple discharge revealed normal epithelial cells. Histopathology after surgery revealed a solitary intraductal papilloma in a cystic lesion.

10 Nipple Discharge Evaluation A 42-year-old woman with serous discharge from her left nipple. Galactography revealed contrast-agent filling defects approximately 1.5 cm from her nipple. Cytology of smears of secreted fluid revealed malignant epithelial cells. Histopathology after surgery revealed intraductal carcinoma.
11 Based on NCCN Breast Cancer Screening and Diagnosis Clinical Practice Guidelines v BCCCP Medical Protocol Follow-up of Abnormal CBE Results NIPPLE DISCHARGE Unilateral NIPPLE DISCHARGE Revised June 2010 Non-Spontaneous: Multiduct Persistent and reproducible on Exam Spontaneous, unilateral, single duct and clear or colorless, serous, sanguineous or serosanguineous 1. Refer for Diagnostic Mammogram 2. Educate to stop compression of breast and report any spontaneous discharge Refer for: Diagnostic Mammogram +/- Ultrasound Breast Consult Mammogram result determines if breast consult and additional f/u required (See Diagnostic Mammogram Follow-up Evaluation) Further diagnostic follow-up** per surgeon recommendation ** Diagnostic follow-up may include tissue biopsy or recommendation for ductogram (NOTE: Ductogram not reimbursed by BCCCPmay be mapped for reimbursement)
12 Abnormal CBE Findings Asymmetrical Thickening vs. Breast Mass Despite widespread use of screening mammography, breast cancer presents as a palpable mass in the majority of cases 4:1 prevalence of benign breast mass compared to malignant Variation in breast tissue nodularity among pre and post menopausal women is considerable
13 Asymmetrical Thickening or Lump Challenge to clinicians: Is the area of concern part of the normal physiologic nodularity of the breast or is it a dominant mass? Physiologic nodularity is often referred to as fibrocystic disease - designation is incorrect Such nodularity is, in fact, physiologic. - the issue is not one of treatment but of follow-up monitoring Breast consult to decide if immediate or shortterm follow-up required.
14 Asymmetrical Thickening or Lump Providers need to decide how to best follow patients with dense and nodular breast tissue so as to maintain high sensitivity without sacrificing specificity in the clinical breast examination Reassuring women about what they are finding on their own may alleviate some of the anxiety For patients with normal breast cancer risk, annual examination by a health care provider is recommended
15 Based on NCCN Breast Cancer Screening and Diagnosis Clinical Practice Guidelines v BCCCP Medical Protocol Follow-up of Abnormal CBE Results ASYMMETRIC THICKENING/NODULARITY Revised June 2010 Refer for 1. Diagnostic Mammogram 2. Ultrasound 3. Breast Consult Mammogram/US Results ACR 1,2, 3 Mammogram/US Results ACR 4,5 Per Surgeon: Clinically assessed as benign Per Surgeon: Clinically suspicious Tissue Biopsy** Breast consult for Physical Exam at 3-6 mos Further f/u based on surgeon s recommendations Benign Atypical Hyperplasia Malignant ** Tissue biopsy can include any of the following:(incisional, Core Needle, US Guided, Stereotactic, Excisional) Dx Mammogram/ US in 6-12 mos for 1-2 years Possible Excisional Biopsy per surgeon/radiologist recommendation Enroll in BCCCP MTA if eligible
16 Abnormal CBE Results Skin Changes (Red Flags) Nipple retraction Cancer until proven otherwise! Suggests retroareolar mass Peau d'orange Breast skin dotted like the skin of an orange Very ominous sign carcinoma when present over a lump; suggests lymph node involvement
17 Skin Changes (Red Flags) Paget s Disease of the Nipple Skin Retraction Skin Dimpling/Puckering (skin pulled in by an underlying carcinoma) Breast Erythema In non-lactating women: Ominous if persistent mastitis greater than 2 weeks; suggests inflammatory carcinoma In elderly women: erythema with ulceration may suggest neglected carcinoma Visible lump May be due to cysts, giant fibroadenoma, carcinoma

18 Enlarged right breast with nipple retraction

19 Peau d' orange on underside of breast not visible in previous photo

20 Paget s Disease of the Nipple
21 Breast Erythema: Inflammatory Carcinoma
22 Skin Changes Follow-Up Diagnostic work-up for any unilateral breast skin changes or nipple retraction An inflammatory appearance of the breast in any woman older than 40 should be considered inflammatory breast cancer until proven otherwise Bilateral diagnostic mammography is the first line of investigation - should be followed by a surgical consultation and a biopsy of the breast and skin.
23 ? Possible infection vs. cancer Subtle skin changes (rash, scaliness) Refer to surgeon (unless NP can prescribe antibiotics) Re-evaluate after antibiotics completed If not resolved, refer for diagnostic work-up to rule out cancer
24 Based on NCCN Breast Cancer Screening and Diagnosis Clinical Practice Guidelines v BCCCP Medical Protocol Follow-up of Abnormal CBE Results SKIN CHANGES Revised June 2010 CLINICAL FINDING: 1. Clinically suspicious of inflammatory breast cancer: Peau d orange or Erythema OR 2. Clinically suspicious of Paget s Disease: Nipple Excoriation, scaling, or eczema Refer for: 1. Mammogram +/- Ultrasound 2. Breast Consult Tissue Biopsy (Core Needle, Excisional, Nipple Biopsy or Punch biopsy of Skin (Skin biopsy not reimbursed by BCCCP - contact MDCH Nurse Consultant) Biopsy Results: Benign Biopsy Results: Malignant 1. Reassess clinical/pathology correlation 2. Consider Breast MRI (not reimbursed by BCCCP) 3. Consider Repeat Biopsy Enroll in BCCCP MTA if eligible
25 Abnormal CBE Findings Breast Mass Characteristics of Malignant CBE Findings True masses are generally: asymmetrical in relation to the other breast distinct from the surrounding tissues are three dimensional Cancerous mass: may be firm have attachments to skin or deep fascia with dimpling or nipple retraction
26 Benign CBE Findings Characteristics of Benign Lesions Have discrete, well defined margins Are generally mobile NOTE: DO NOT rely on palpation alone to determine a malignant from benign mass Full diagnostic work-up is required to confirm malignant from bengn mass
27 Abnormal CBE Findings Cysts vs. solid masses Cysts can be difficult to distinguish by palpation from solid masses Studies show equivocal results -- In one study, 58% of 66 palpable cysts were correctly identified by physical examination -- In a second study, 4 surgeons performed physical exams independently they agreed on the need for biopsy in 73% of 15 masses subsequently proven malignant An imaging evaluation is necessary in almost all cases to characterize the type of lesion
28 Drawbacks of Imaging for Breast Abnormalities Not all palpable breast masses will be visualized with conventional imaging techniques Breast Cancer Detection Demonstration Project (BCDDP), which began in 1970, found 9% of cancers by CBE alone this % is now less due to improvements in imaging technology A NEGATIVE MAMMOGRAM SHOULD NEVER OVERRULE A STRONGLY SUSPICIOUS FINDING ON PHYSICAL EXAM FURTHER FOLLOW-UP IS REQUIRED BEYOND THE MAMMOGRAM
29 Abnormal CBE Findings Clinical management of breast mass Breast cancers present clinically in varied ways When a mass is found consider the following: Patient age, menstrual cycle (and whether the change in symptoms are associated with the cycle), hormone use, trauma, durations, changes over time, individual risk factors, & presence of mass in one breast or both breasts
30 Based on NCCN Breast Cancer Screening and Diagnosis Clinical Practice Guidelines v BCCCP Medical Protocol Follow-up of Abnormal CBE Results DOMINANT MASS (formerly lump/mass) Revised June 2010 No Abnormality (Bi-Rads 1) (Immed F/U) Breast Consult AND Tissue biopsy OR (STF) Dx. Mamm/US q 6 mos x 1-2 years to assess stability per surgeon recomm. Solid Mass? (Immed F/U) Breast consult AND possible Tissue Biopsy* per surgeon recommendation BI-Rads Results ACR 1, 2, or 3 Perform Ultrasound Simple Cyst (No F/U) Resume annual screening Diagnostic Mammogram Complex Cyst Breast Consult AND any/all of the following per surgeon s recommendation: 1. STF - CBE, Mammogram, US q 6-12 mos for 1-2 years to assess stability OR 2. (Immed F/U) Fine Needle Aspiration OR 3. (Immed F/U) Tissue Biopsy* Benign Dx Mammogram/ US in 6-12 mos for 1-2 years Bi-Rads Results ACR 4 or 5 Breast Consult AND Tissue Biopsy* Biopsy Result Atypical Hyperplasia Possible Excisional Biopsy per surgeon/radiologist recommendation ** Tissue biopsy can include any of the following:(incisional, Core Needle, US Guided, Stereotactic, Excisional) Malignant Enroll in BCCCP MTA if eligible
31 Based on NCCN Breast Cancer Screening and Diagnosis Clinical Practice Guidelines v BCCCP Medical Protocol Follow-up of Abnormal CBE Results DOMINANT MASS Revised June 2010 Diagnostic Mammogram No Abnormality (Bi-Rads 1, 2, 3) (Immed F/U) Breast Consult AND Tissue biopsy OR (STF) Dx. Mamm/US q 6 mos x 1-2 years to assess stability per surgeon recomm. Solid Mass? (Immed F/U) Breast consult AND possible Tissue Biopsy* per surgeon recommendation BI-Rads Results ACR 1, 2, or 3 Perform Ultrasound Simple Cyst (No F/U) Resume annual screening Complex Cyst Breast Consult AND any/all of the following per surgeon s recommendation: 1. STF - CBE, Mammogram, US q 6-12 mos for 1-2 years to assess stability OR 2. (Immed F/U) Fine Needle Aspiration OR 3. (Immed F/U) Tissue Biopsy* NOTE: Surgical Consult can be ordered per clinician/client request ** Tissue biopsy can include any of the following: Incisional, Core Needle, US Guided, Excisional or Stereotactic, (NOTE: Surgical Consults are NOT required prior to stereotactic biopsies ordered by radiologist
32 CBE Result: Dominant Mass (Coded as Abnormality/Rule Out Cancer) IF the Mammogram AND Ultrasound Results are ANY combination of ACR 1, 2, OR 3 Refer for Follow-up Surgical Consult AND Possible Tissue Biopsy (per surgeon s recommendation) OR 6 month follow-up Diagnostic Mammogram* and/or Ultrasound* along with Surgical Consult* *BCCCP will reimburse
33 CBE Result: Dominant Mass (Coded as Abnormality/Rule Out Cancer) IF the Mammogram Result is ACR 1, 2, OR 3 AND Ultrasound Result shows SOLID mass Refer for Follow-up Surgical Consult AND/OR Tissue Biopsy (per radiologist s OR surgeon s recommendation)
34 CBE Result: Dominant Mass (Coded as Abnormality/Rule Out Cancer) IF the Mammogram Result is ACR 1, 2, OR 3 AND Ultrasound Result shows SIMPLE CYST No Follow-up Required NOTE: If cyst painful may refer to surgeon to perform FNA Post FNA mammogram/us will be reimbursed to determine if cyst refilled
35 CBE Result: Dominant Mass (Coded as Abnormality/Rule Out Cancer) IF the Mammogram Result is ACR 1, 2, OR 3 AND Ultrasound Result shows COMPLEX CYST Refer for Follow-up Surgical Consult AND any/all of the following per surgeon s recommendation: Fine Needle Aspiration* AND/OR Tissue Biopsy* OR CBE, and/or Mammogram, and/or Ultrasound in 6 months to assess stability OR NOTE: *BCCCP will reimburse consult post aspiration/ biopsy to assess stability of cyst
36 Based on NCCN Breast Cancer Screening and Diagnosis Clinical Practice Guidelines v BCCCP Medical Protocol Follow-up of Abnormal CBE Results DOMINANT MASS Revised June 2010 Diagnostic Mammogram Benign Dx Mammogram/ US in 6-12 mos for 1-2 years Bi-Rads Results ACR 4 or 5 Breast Consult AND Tissue Biopsy* Biopsy Result Atypical Hyperplasia Possible Excisional Biopsy per surgeon/radiologist recommendation No approval needed for Excisional Biopsy Malignant Enroll in BCCCP MTA if eligible ** Tissue biopsy can include any of the following: Incisional, Core Needle, US Guided, Excisional or Stereotactic, (NOTE: Surgical Consults are NOT required prior to stereotactic biopsies ordered by radiologist
37 Pre/post Biopsy Questions (Contact NC for guidance) Abscess post biopsy (Will reimburse for surgeon s f/u visits; cannot reimburse for I & D or antibiotics) Lymph node biopsy (If to r/o breast cancer, can map lymph node biopsy to BCCCP code; cannot reimburse if to r/o anything unrelated to breast cancer) Atypical hyperplasia (Can reimburse for Excisional biopsy and 6 month f/u mammogram/surgical consult; cannot reimburse for oncology referral or chemoprevention therapy)
38 Follow-up of Breast Pain Most common breast complaint Etiology is unclear most commonly occurs 1 week prior to menses and in some women on HRT Causes worry and anxiety about breast cancer (Among women with breast pain who have a normal CBE and radiologic studies, cancer will be found in about 0.5% upon f/u)
39 Breast Pain Follow-up cont. HCP should determine the cause of pain Location and duration of the pain Unilateral or bilateral Patient ranked discomfort (scale 1-10) Whether the pain is cyclic, changes with menstrual cycle or related to HRT Whether the pain has altered patient s lifestyle (interfered with exercise, hugs, sexual activity, sleep)
40 Common cause of pain Fibrocystic Breast Condition Occurs from changes in the glandular and stromal tissues of the breast Changes are related to a woman s menstrual cycle and the hormones, estrogen and progesterone Women with fibrocystic breasts often have bilateral cyclic breast pain or tenderness that coincides with their menstrual cycles
41 Fibrocystic Breast Condition cont. Most fibrocystic breast lumps are found in the upper, outer quadrant of the breasts (near the axilla, armpit, region), although these lumps can occur anywhere in the breasts Fibrocystic breast lumps tend to be smooth, rounded, and mobile (not attached to other breast tissue), though some fibrocystic tissue may have a thickened, irregular feel Fibrocystic lumps or irregularities are often tender to touch and may increase or decrease in size during the menstrual cycle
42 Fibrocystic Breast Condition Symptoms of fibrocystic breasts include: cysts, fibrosis, lumpiness, areas of thickening, tenderness, and pain Fibrocystic breasts are not risk factors for breast cancer, but it can make breast cancer more difficult to detect Screening mammograms may be more difficult to perform because the breast density associated with fibrocystic breasts may eclipse breast cancer on the mammogram Additional imaging, biopsy, cyst aspiration may be needed

43 Fibrocystic Breast Tissue on a Mammogram Mammogram shows thickenings which are typical of fibrocystic disease
44 Breast Pain: Is a referral needed? Ask the client the following questions: Unilateral vs. bilateral? Cyclic vs non-cyclic? Constant vs. intermittent? Persists daily for more than a couple of weeks Localized to one specific area of breast (not related to injury) Getting worse over time Interferes with daily activities If Breast Pain meets above criteria - refer for breast consult
45 Follow-up of Breast Pain unrelated to cancer dx Inform the woman that mastalgia is very common Interventions to use: substituting a more supportive bra, lowering/changing estrogen dose, decreasing caffeine intake,? Drug intervention I.e. evening primrose oil, danazol, bromocriptine, vitamin therapy I.e. Vitamin E (800u), Vitamin B6 or niacin Cyclic pain is more responsive than non-cyclic pain
46 Mammogram Results Requiring Short-term or Immediate Follow-up Short-term Follow-up ACR 3: Probably Benign Immediate Follow-up ACR 0: Assessment Incomplete ACR 4: Suspicious Abnormality ACR 5: Highly Suggestive of Malignancy
47 Mammogram Result ACR 3: Probably Benign Finding Finding has < 2% risk of malignancy; not expected to change over f/u interval but radiologist wants to establish its stability 3 findings classified as probably benign: -- non-calcified mass -- focal asymmetry -- cluster of round calcifications Majority of findings can be managed through initial STF (6 mos) up to 2 years (monitor closely as f/u often coincides with annual screening

48 Probably Benign Calcifications Importance of close monitoring The odds for invasive carcinoma versus DCIS are statistically significantly higher among patients with increasing or new microcalcifications. Courtesy Radiology Assistant L image Patient with a few heterogeneous coarse calcifications - BIRADS 3. R image Six month follow up showed calcifications had increased in number; DCIS was found at biopsy.
49 Mammogram Result: ACR 0: Assessment Incomplete- Need Additional Imaging Evaluation Additional imaging evaluation may include: spot compression, magnification, special magnification views, and/or ultrasound Further follow-up beyond second imaging depends on final mammogram results
50 Mammogram Result: ACR 4: Suspicious Abnormality Reserved for findings that do not have classic appearance of malignancy but have a wide probability of malignancy > than ACR 3 findings Follow-up recommended based on appearance/characteristics of findings Surgeon may choose to monitor as shortterm follow-up
 and are associated with extra cell activity in breast tissue Scattered microcalcifications are usually a sign of benign breast")
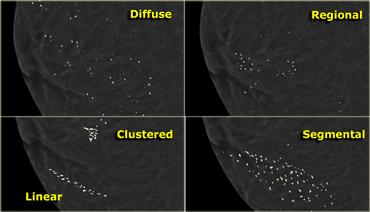
51 Breast Calcifications Microcalcifications shown on mammogram; calcifications are present through ductal Microcalcifications are tiny bits patterns. of calcium that may show up in clusters or in patterns (like circles) and are associated with extra cell activity in breast tissue Scattered microcalcifications are usually a sign of benign breast tissue Probably benign calcifications have < 2% risk of breast cancer (monitored q 6 months x 1 year) Suspicious calcifications (tight clusters) can indicate early breast cancer

52 Microcalcifications are found in ~ half of women > age 50, and 1/10 women < age 50 Benign macrocalcifications are larger and randomly spread throughout the breast. No followup care is usually needed. Microcalcifications are small, appear clustered and have irregular shapes. Suspicious for cancer. Refer for biopsy.
53 Types of Calcifications
54 Mammogram Abnormality ACR 5: Highly Suggestive of Malignancy High probability (> 95%) of being cancer Type of biopsy performed depends on lesion identified More than one biopsy may be performed and/or combined with sentinel node imaging or delayed after neoadjuvant chemotherapy
55 Based on NCCN Breast Cancer Screening and Diagnosis Clinical Practice Guidelines v BCCCP Medical Protocol Follow-up of DIAGNOSTIC Mammogram Results Revised June 2010 ACR 0 - Assessment Incomplete - Work-Up Required Diagnostic work-up includes any or all of the following: 1. Comparison to Prior Films 2. Diagnostic Mammogram 3. Ultrasound as indicated Diagnostic Mammogram Follow-up ACR 1 - Negative ACR 2 - Benign Finding ACR 3 - Probably Benign Routine Screening: Annual CBE/Mammogram/ Breast Awareness EXCEPTION: IF CBE Abnormal - additional work-up required to include any or all of the following: Ultrasound, Breast Consult, Tissue Biopsy) Diagnostic Mammogram at 6 months then every 6-12 months x 1-2 years If return visit uncertain or client very anxious consider consult and possible biopsy Benign Dx Mammogram/US in 6-12 mos for 1-2 years ACR 4- Suspicious Abnormality ACR 5 - Highly Suggestive of Malignancy Breast consult Referral for Tissue Biopsy** Atypical Hyperplasia Possible Excisional Biopsy per surgeon/ radiologist recommendation Malignant Enroll in BCCCP MTA if eligible
56 Case Study # 1 CBE Result: Probably Benign Screening Mammogram Result ACR 0 Diagnostic Mammogram Result ACR 0 Ultrasound confirms complex cyst. Next steps?
57 Based on NCCN Breast Cancer Screening and Diagnosis Clinical Practice Guidelines v BCCCP Medical Protocol Follow-up of Abnormal CBE Results DOMINANT MASS Revised June 2010 Diagnostic Mammogram No Abnormality (Bi-Rads 1, 2, 3) (Immed F/U) Breast Consult AND Tissue biopsy OR (STF) Dx. Mamm/US q 6 mos x 1-2 years to assess stability per surgeon recomm. Solid Mass? (Immed F/U) Breast consult AND possible Tissue Biopsy* per surgeon recommendation BI-Rads Results ACR 1, 2, or 3 Perform Ultrasound Simple Cyst (No F/U) Resume annual screening Complex Cyst Breast Consult AND any/all of the following per surgeon s recommendation: 1. STF - CBE, Mammogram, US q 6-12 mos for 1-2 years to assess stability OR 2. (Immed F/U) Fine Needle Aspiration OR 3. (Immed F/U) Tissue Biopsy* NOTE: Surgical Consult can be ordered per clinician/client request ** Tissue biopsy can include any of the following: Incisional, Core Needle, US Guided, Excisional or Stereotactic, (NOTE: Surgical Consults are NOT required prior to stereotactic biopsies ordered by radiologist
58 Case Study # 2 CBE not performed Mammogram performed at Screening Fair; Result: ACR 0 Referred to BCCCP Diagnostic Mammogram Result: - L breast ACR 2 - simple or complicated cysts without suspicious masses - R breast ACR 4 - solid nodule 10 o clock appears suspicious Next Steps
59 Based on NCCN Breast Cancer Screening and Diagnosis Clinical Practice Guidelines v BCCCP Medical Protocol Follow-up of Abnormal CBE Results DOMINANT MASS Revised June 2010 Diagnostic Mammogram Benign Dx Mammogram/ US in 6-12 mos for 1-2 years Bi-Rads Results ACR 4 or 5 Breast Consult AND Tissue Biopsy* Biopsy Result Atypical Hyperplasia Possible Excisional Biopsy per surgeon/radiologist recommendation No approval needed for Excisional Biopsy Malignant Enroll in BCCCP MTA if eligible ** Tissue biopsy can include any of the following: Incisional, Core Needle, US Guided, Excisional or Stereotactic, (NOTE: Surgical Consults are NOT required prior to stereotactic biopsies ordered by radiologist
60 Oncology Nursing: My Career, my Choice, my Passion E.J. Siegl, RN, OCN, MA, CBCN BCCCP Nurse Consultant
Imaging in breast cancer. Mammography and Ultrasound Donya Farrokh.MD Radiologist Mashhad University of Medical Since
 Imaging in breast cancer Mammography and Ultrasound Donya Farrokh.MD Radiologist Mashhad University of Medical Since A mammogram report is a key component of the breast cancer diagnostic process. A mammogram
Imaging in breast cancer Mammography and Ultrasound Donya Farrokh.MD Radiologist Mashhad University of Medical Since A mammogram report is a key component of the breast cancer diagnostic process. A mammogram
Imaging the Symptomatic Patient. Avice M.O Connell MD,FACR,FSBI Professor of Imaging Sciences Director, Women s Imaging University of Rochester
 Imaging the Symptomatic Patient Avice M.O Connell MD,FACR,FSBI Professor of Imaging Sciences Director, Women s Imaging University of Rochester The four most common symptoms Mass Pain Discharge Infection
Imaging the Symptomatic Patient Avice M.O Connell MD,FACR,FSBI Professor of Imaging Sciences Director, Women s Imaging University of Rochester The four most common symptoms Mass Pain Discharge Infection
Disclaimer no conflict of interest
 Disclaimer no conflict of interest Benign Breast Disease Alison Hayes FRACS Content Clinical assessment of the breast Triple assessment Focal nodularity Breast pain Cysts Infection Nipple discharge Gynaecomastia
Disclaimer no conflict of interest Benign Breast Disease Alison Hayes FRACS Content Clinical assessment of the breast Triple assessment Focal nodularity Breast pain Cysts Infection Nipple discharge Gynaecomastia
Breast Health. Learning Objectives. Breast Anatomy. Poll Question. Breast Anatomy
 Learning Objectives Describe breast anatomy to a patient Breast Health Answer questions about causes of breast pain and masses Explain breast cancer screening/diagnostic modalities Appropriately triage
Learning Objectives Describe breast anatomy to a patient Breast Health Answer questions about causes of breast pain and masses Explain breast cancer screening/diagnostic modalities Appropriately triage
Breast Evaluation & Management Guidelines
 Breast Evaluation & Management Guidelines Pamela L. Kurtzhals, M.D. F.A.C.S. Head, Dept. of General Surgery Scripps Clinic, La Jolla Objective Review screening & diagnostic guidelines Focused patient complaints
Breast Evaluation & Management Guidelines Pamela L. Kurtzhals, M.D. F.A.C.S. Head, Dept. of General Surgery Scripps Clinic, La Jolla Objective Review screening & diagnostic guidelines Focused patient complaints
DISORDERS OF THE BREAST Dated. FIBROADENOSIS Other common names: mastitis, fibrocystic disease, cystic mammary dysplasia.
 DISORDERS OF THE BREAST Dated BENIGN BREAST DISORDERS (Essential Surg 2 nd Ed, pp 540) FIBROADENOSIS Other common names: mastitis, fibrocystic disease, cystic mammary dysplasia. Fibroadenosis is the distortion
DISORDERS OF THE BREAST Dated BENIGN BREAST DISORDERS (Essential Surg 2 nd Ed, pp 540) FIBROADENOSIS Other common names: mastitis, fibrocystic disease, cystic mammary dysplasia. Fibroadenosis is the distortion
Breast Cancer Screening and Surgery. April 26, 2018 Ashley B. Simpson, DO
 Breast Cancer Screening and Surgery April 26, 2018 Ashley B. Simpson, DO Objectives Breast cancer screening Common breast complaints Surgical management of breast cancer Breast Screening Question 1 At
Breast Cancer Screening and Surgery April 26, 2018 Ashley B. Simpson, DO Objectives Breast cancer screening Common breast complaints Surgical management of breast cancer Breast Screening Question 1 At
Mary Smania, DNP, FNP-BC Clinical Practice Champion Assistant Professor Michigan State University College of Nursing
 Mary Smania, DNP, FNP-BC Clinical Practice Champion Assistant Professor Michigan State University College of Nursing Identify evidence based routine screening guidelines for women of all ages Identify
Mary Smania, DNP, FNP-BC Clinical Practice Champion Assistant Professor Michigan State University College of Nursing Identify evidence based routine screening guidelines for women of all ages Identify
Case Scenario 1 History and Physical 3/15/13 Imaging Pathology
 Case Scenario 1 History and Physical 3/15/13 The patient is an 84 year old white female who presented with an abnormal mammogram. The patient has a five year history of refractory anemia with ringed sideroblasts
Case Scenario 1 History and Physical 3/15/13 The patient is an 84 year old white female who presented with an abnormal mammogram. The patient has a five year history of refractory anemia with ringed sideroblasts
Benign Breast Disease. David Anderson, MD Assistant Professor of Clinical Surgery
 Benign Breast Disease David Anderson, MD Assistant Professor of Clinical Surgery Overview Nipple Discharge Breast infection Breast Pain Gynecomastia Fibroepithelial lesions High Risk Lesions-Papilloma,
Benign Breast Disease David Anderson, MD Assistant Professor of Clinical Surgery Overview Nipple Discharge Breast infection Breast Pain Gynecomastia Fibroepithelial lesions High Risk Lesions-Papilloma,
ACRIN 6666 IM Additional Evaluation: Additional Views/Targeted US
 Additional Evaluation: Additional Views/Targeted US For revised or corrected form check box and fax to 215-717-0936. Instructions: The form is completed based on recommendations (from ID form) for additional
Additional Evaluation: Additional Views/Targeted US For revised or corrected form check box and fax to 215-717-0936. Instructions: The form is completed based on recommendations (from ID form) for additional
Common Breast Problems: Breast Pain
 Common Breast Problems: Breast Pain Breast pain is the most common symptom that brings women to their physician. In general, there are two common presentations of breast pain: cyclic and noncyclic. Breast
Common Breast Problems: Breast Pain Breast pain is the most common symptom that brings women to their physician. In general, there are two common presentations of breast pain: cyclic and noncyclic. Breast
Plan. Lumps, Bumps, Leaking and Pain. Breast Cancer. Management of Breast Conditions. Palpable breast mass. Non-Palpable breast mass
 Lumps, Bumps, Leaking and Pain Management of Breast Conditions Rebecca A. Jackson, MD Obstetrics, Gynecology & Reproductive Sciences Epidemiology & Biostatistics University of California, San Francisco
Lumps, Bumps, Leaking and Pain Management of Breast Conditions Rebecca A. Jackson, MD Obstetrics, Gynecology & Reproductive Sciences Epidemiology & Biostatistics University of California, San Francisco
Breast lumps to refer or not to refer? Simon Cawthorn Breast Specialist
 Breast lumps to refer or not to refer? Simon Cawthorn Breast Specialist Learning objectives Know the indications to refer urgently Who to reassure and review How to reassure patients with non-urgent symptoms
Breast lumps to refer or not to refer? Simon Cawthorn Breast Specialist Learning objectives Know the indications to refer urgently Who to reassure and review How to reassure patients with non-urgent symptoms
Common Problem of the Breast
 Common Problem of the Breast Breast Lumps, Nipple Discharge, and Pain 本講義表格資料取自 Dains, J.E., Baumann, L.C., & Scheibel, P. (2007). Advanced assessment and clinical diagnosis in primary care. (3rd ed).
Common Problem of the Breast Breast Lumps, Nipple Discharge, and Pain 本講義表格資料取自 Dains, J.E., Baumann, L.C., & Scheibel, P. (2007). Advanced assessment and clinical diagnosis in primary care. (3rd ed).
Amammography report is a key component of the breast
 Review Article Writing a Mammography Report Amammography report is a key component of the breast cancer diagnostic process. Although mammographic findings were not clearly differentiated between benign
Review Article Writing a Mammography Report Amammography report is a key component of the breast cancer diagnostic process. Although mammographic findings were not clearly differentiated between benign
Lumps, Bumps, Leaking and Pain. Plan. Management of Breast Conditions. Palpable breast mass. Non-Palpable breast mass. Perceived. Actual.
 Lumps, Bumps, Leaking and Pain Management of Breast Conditions Rebecca A. Jackson, MD Professor & Chief Department of Obstetrics, Gynecology and Reproductive Sciences San Francisco General Hospital University
Lumps, Bumps, Leaking and Pain Management of Breast Conditions Rebecca A. Jackson, MD Professor & Chief Department of Obstetrics, Gynecology and Reproductive Sciences San Francisco General Hospital University
Timby/Smith: Introductory Medical-Surgical Nursing, 9/e
 Timby/Smith: Introductory Medical-Surgical Nursing, 9/e Chapter 60: Caring for Clients With Breast Disorders Slide 1 Infectious and Inflammatory Breast Disorders: Mastitis Pathophysiology and Etiology
Timby/Smith: Introductory Medical-Surgical Nursing, 9/e Chapter 60: Caring for Clients With Breast Disorders Slide 1 Infectious and Inflammatory Breast Disorders: Mastitis Pathophysiology and Etiology
Benign Breast Conditions. Dr. Kim Kelly, CCFP, FCFP Breast Expert, CBCP February, 2015
 Benign Breast Conditions Dr. Kim Kelly, CCFP, FCFP Breast Expert, CBCP February, 2015 Kim Kelly M.D. U of A Family Medicine 1996 2011 Special Interest in Breast Medicine designation, CP&S 2012 15, Breast
Benign Breast Conditions Dr. Kim Kelly, CCFP, FCFP Breast Expert, CBCP February, 2015 Kim Kelly M.D. U of A Family Medicine 1996 2011 Special Interest in Breast Medicine designation, CP&S 2012 15, Breast
Diseases of the breast (1 of 2)
") Diseases of the breast (1 of 2) Introduction A histology introduction Normal ducts and lobules of the breast are lined by two layers of cells a layer of luminal cells overlying a second layer of myoepithelial
Diseases of the breast (1 of 2) Introduction A histology introduction Normal ducts and lobules of the breast are lined by two layers of cells a layer of luminal cells overlying a second layer of myoepithelial
BREAST PATHOLOGY. Fibrocystic Changes
 BREAST PATHOLOGY Lesions of the breast are very common, and they present as palpable, sometimes painful, nodules or masses. Most of these lesions are benign. Breast cancer is the 2 nd most common cause
BREAST PATHOLOGY Lesions of the breast are very common, and they present as palpable, sometimes painful, nodules or masses. Most of these lesions are benign. Breast cancer is the 2 nd most common cause
Diagnostic Breast Evaluation: When to Refer and What the Results Really Mean. Julie Dreadin RN, MS, WHNP-BC. Peggy Mancuso PhD, CNM, RN
 Diagnostic Breast Evaluation 1 Running head: DIAGNOSTIC BREAST EVALUATION Diagnostic Breast Evaluation: When to Refer and What the Results Really Mean Julie Dreadin RN, MS, WHNP-BC Peggy Mancuso PhD, CNM,
Diagnostic Breast Evaluation 1 Running head: DIAGNOSTIC BREAST EVALUATION Diagnostic Breast Evaluation: When to Refer and What the Results Really Mean Julie Dreadin RN, MS, WHNP-BC Peggy Mancuso PhD, CNM,
Lumps, Bumps, Leaking and Pain
 Lumps, Bumps, Leaking and Pain Management of Breast Conditions Rebecca A. Jackson, MD Professor & Chief Department of Obstetrics, Gynecology and Reproductive Sciences San Francisco General Hospital University
Lumps, Bumps, Leaking and Pain Management of Breast Conditions Rebecca A. Jackson, MD Professor & Chief Department of Obstetrics, Gynecology and Reproductive Sciences San Francisco General Hospital University
Imaging Guidelines for Breast Cancer Screening
 Imaging Guidelines for Breast Cancer Screening Sarah Colwick, MD Dr. Sarah Colwick was born and raised in Sikeston, MO. She attended college and medical school at the University of Missouri-Kansas City
Imaging Guidelines for Breast Cancer Screening Sarah Colwick, MD Dr. Sarah Colwick was born and raised in Sikeston, MO. She attended college and medical school at the University of Missouri-Kansas City
Breast Cancer. Common kinds of breast cancer are
 Breast Cancer A breast is made up of three main parts: glands, ducts, and connective tissue. The glands produce milk. The ducts are passages that carry milk to the nipple. The connective tissue (which
Breast Cancer A breast is made up of three main parts: glands, ducts, and connective tissue. The glands produce milk. The ducts are passages that carry milk to the nipple. The connective tissue (which
Vesalius SCALpel : Benign breast disease (see also: breast folios)
") Vesalius SCALpel : Benign breast disease (see also: breast folios) Breast cancer risk Imaging Pain non-proliferative: only fibroadenoma may be associated with a slight risk of cancer proliferative: moderate
Vesalius SCALpel : Benign breast disease (see also: breast folios) Breast cancer risk Imaging Pain non-proliferative: only fibroadenoma may be associated with a slight risk of cancer proliferative: moderate
Breast Cancer Screening and Diagnosis
 Breast Cancer Screening and Diagnosis Priya Thomas, MD Assistant Professor Clinical Cancer Prevention and Breast Medical Oncology University of Texas MD Anderson Cancer Center Disclosures Dr. Thomas has
Breast Cancer Screening and Diagnosis Priya Thomas, MD Assistant Professor Clinical Cancer Prevention and Breast Medical Oncology University of Texas MD Anderson Cancer Center Disclosures Dr. Thomas has
Office Management of Common Breast Complaints
 Annual Review of Family Medicine UCSF Mission Bay December 7, 2017 Office Management of Common Breast Complaints Michael Policar, MD, MPH Clinical Professor of Ob, Gyn, and Repro Sciences UCSF School of
Annual Review of Family Medicine UCSF Mission Bay December 7, 2017 Office Management of Common Breast Complaints Michael Policar, MD, MPH Clinical Professor of Ob, Gyn, and Repro Sciences UCSF School of
AMSER Case of the Month: September 2018
 AMSER Case of the Month: September 2018 60-year-old woman with a left breast mass noted on screening mammography. Catherine McNulty, MS4 Tulane University School of Medicine Dr. Robin Sobolewski Breast
AMSER Case of the Month: September 2018 60-year-old woman with a left breast mass noted on screening mammography. Catherine McNulty, MS4 Tulane University School of Medicine Dr. Robin Sobolewski Breast
BREAST PATHOLOGY MCQS
 BREAST PATHOLOGY MCQS 1) :The most important factor in breast enlargement during pregnancy is A. stromal edema B. secretion of chorionic gonadotropin C. glandular hyperplasia D. proliferation of stroma
BREAST PATHOLOGY MCQS 1) :The most important factor in breast enlargement during pregnancy is A. stromal edema B. secretion of chorionic gonadotropin C. glandular hyperplasia D. proliferation of stroma
Benign, Reactive and Inflammatory Lesions of the Breast
 Benign, Reactive and Inflammatory Lesions of the Breast Marilin Rosa, MD Associate Member Section Head of Breast Pathology Department of Anatomic Pathology Program Director, Breast Pathology Fellowship
Benign, Reactive and Inflammatory Lesions of the Breast Marilin Rosa, MD Associate Member Section Head of Breast Pathology Department of Anatomic Pathology Program Director, Breast Pathology Fellowship
A study on the usefulness of triple assessment in lumpy breasts in peri-menopausal women
 International Surgery Journal http://www.ijsurgery.com pissn 2349-3305 eissn 2349-2902 Research Article DOI: http://dx.doi.org/10.18203/2349-2902.isj20151249 A study on the usefulness of triple assessment
International Surgery Journal http://www.ijsurgery.com pissn 2349-3305 eissn 2349-2902 Research Article DOI: http://dx.doi.org/10.18203/2349-2902.isj20151249 A study on the usefulness of triple assessment
Your Breasts. Common Questions and Answers
 Your Breasts Common Questions and Answers Your Breasts What do I need to know about my breasts? Your breasts go through many changes over your lifetime. They change in your early teens as you go through
Your Breasts Common Questions and Answers Your Breasts What do I need to know about my breasts? Your breasts go through many changes over your lifetime. They change in your early teens as you go through
Lesion Imaging Characteristics Mass, Favoring Benign Circumscribed Margins Intramammary Lymph Node
 Lesion Imaging Characteristics Mass, Favoring Benign Circumscribed Margins Intramammary Lymph Node Oil Cyst Mass, Intermediate Concern Microlobulated Margins Obscured Margins Mass, Favoring Malignant Indistinct
Lesion Imaging Characteristics Mass, Favoring Benign Circumscribed Margins Intramammary Lymph Node Oil Cyst Mass, Intermediate Concern Microlobulated Margins Obscured Margins Mass, Favoring Malignant Indistinct
Benign Breast Disease & Breast Screening. Leah Kelley, MD OPSC Conference Monterey, CA September, 2018
 Benign Breast Disease & Breast Screening Leah Kelley, MD OPSC Conference Monterey, CA September, 2018 Why this matters to YOU Breast symptoms constitute 3% of all visits by female patients (29.7 per 1,000)
Benign Breast Disease & Breast Screening Leah Kelley, MD OPSC Conference Monterey, CA September, 2018 Why this matters to YOU Breast symptoms constitute 3% of all visits by female patients (29.7 per 1,000)
University of Washington Radiology Review Course: Strange and Specific Diagnoses. Case #1
 University of Washington Radiology Review Course: Strange and Specific Diagnoses Katherine E. Dee, MD Seattle Breast Center Via Radiology 2014 Case #1 37 year old presents with bilateral palpable lumps.
University of Washington Radiology Review Course: Strange and Specific Diagnoses Katherine E. Dee, MD Seattle Breast Center Via Radiology 2014 Case #1 37 year old presents with bilateral palpable lumps.
Breast Disease: What PCPs Need to Know. Eunice Cho MD FACS
 Breast Disease: What PCPs Need to Know Eunice Cho MD FACS New Breast Cancer Screening Guideline for women with average risk Every other year AGE 40 AGE 45 AGE 55 AGE 55 + Talk with your doctor about when
Breast Disease: What PCPs Need to Know Eunice Cho MD FACS New Breast Cancer Screening Guideline for women with average risk Every other year AGE 40 AGE 45 AGE 55 AGE 55 + Talk with your doctor about when
November 23, Dear Maryland Breast and Cervical Cancer Program Provider:
 STATE OF MARYLAND DHMH Maryland Department of Health and Mental Hygiene 201 W. Preston Street Baltimore, Maryland 21201 Martin O Malley, Governor Anthony G. Brown, Lt. Governor John M. Colmers, Secretary
STATE OF MARYLAND DHMH Maryland Department of Health and Mental Hygiene 201 W. Preston Street Baltimore, Maryland 21201 Martin O Malley, Governor Anthony G. Brown, Lt. Governor John M. Colmers, Secretary
Leonard M. Glassman MD
 BI-RADS The New BI-RADS Leonard M. Glassman MD FACR Former Chief of Breast Imaging American Institute for Radiologic Pathology Washington Radiology Associates, PC Breast Imaging Reporting and Data System
BI-RADS The New BI-RADS Leonard M. Glassman MD FACR Former Chief of Breast Imaging American Institute for Radiologic Pathology Washington Radiology Associates, PC Breast Imaging Reporting and Data System
A GP S APPROACH TO BREAST LUMPS AND SYMPTOMS DR KK CHEUNG GPGC WORKSHOP
 A GP S APPROACH TO BREAST LUMPS AND SYMPTOMS DR KK CHEUNG GPGC WORKSHOP 18.08.18 HAVE A SYSTEM HISTORY EXAMINATION INVESTIGATION FOLLOW UP BREAST SYMPTOMS HISTORY DON T FORGET SKIN CHANGES AND NIPPLE CHANGES
A GP S APPROACH TO BREAST LUMPS AND SYMPTOMS DR KK CHEUNG GPGC WORKSHOP 18.08.18 HAVE A SYSTEM HISTORY EXAMINATION INVESTIGATION FOLLOW UP BREAST SYMPTOMS HISTORY DON T FORGET SKIN CHANGES AND NIPPLE CHANGES
COMMON BENIGN DISORDERS AND DISEASES OF THE BREAST
 COMMON BENIGN DISORDERS AND DISEASES OF THE BREAST Aberrations of Normal Development and Involution (ANDI). The basic principles underlying the aberrations of normal development and involution (ANDI) classification
COMMON BENIGN DISORDERS AND DISEASES OF THE BREAST Aberrations of Normal Development and Involution (ANDI). The basic principles underlying the aberrations of normal development and involution (ANDI) classification
Breast Update Therese Cusick MS MD FACS
 Breast Update 2017 Therese Cusick MS MD FACS Conflict of Interest Disclosure Nothing to disclose Sources Adapted from SESAP- Surgical Education and Self-Assessment program American College of Surgeons
Breast Update 2017 Therese Cusick MS MD FACS Conflict of Interest Disclosure Nothing to disclose Sources Adapted from SESAP- Surgical Education and Self-Assessment program American College of Surgeons
BI-RADS Update. Martha B. Mainiero, MD, FACR, FSBI Brown University Rhode Island Hospital
 BI-RADS Update Martha B. Mainiero, MD, FACR, FSBI Brown University Rhode Island Hospital No Disclosures BI-RADS History 1980s Quality Issues ACR Accreditation BI-RADS 1994 2003 4 th Edition MRI, US January
BI-RADS Update Martha B. Mainiero, MD, FACR, FSBI Brown University Rhode Island Hospital No Disclosures BI-RADS History 1980s Quality Issues ACR Accreditation BI-RADS 1994 2003 4 th Edition MRI, US January
Diagnostic Dilemmas of Breast Imaging
 Diagnostic Dilemmas of Breast Imaging Common Causes of Error in Breast Cancer Detection By: Jason Cord, M.D. Mammography: Initial Imaging The standard for detection of breast cancer Screening mammography
Diagnostic Dilemmas of Breast Imaging Common Causes of Error in Breast Cancer Detection By: Jason Cord, M.D. Mammography: Initial Imaging The standard for detection of breast cancer Screening mammography
Pitfalls and Limitations of Breast MRI. Susan Orel Roth, MD Professor of Radiology University of Pennsylvania
 Pitfalls and Limitations of Breast MRI Susan Orel Roth, MD Professor of Radiology University of Pennsylvania Objectives Review the etiologies of false negative breast MRI examinations Discuss the limitations
Pitfalls and Limitations of Breast MRI Susan Orel Roth, MD Professor of Radiology University of Pennsylvania Objectives Review the etiologies of false negative breast MRI examinations Discuss the limitations
Overview. Who Gets Breast Cancer? Breast cancer can strike anyone, although it does tend to follow particular trends.
 Overview Often women fail to pay attention to breast health unless they are forced to while breast feeding a newborn or when a serious condition like breast cancer occurs. Like most bodily processes, the
Overview Often women fail to pay attention to breast health unless they are forced to while breast feeding a newborn or when a serious condition like breast cancer occurs. Like most bodily processes, the
Ana Sofia Preto 19/06/2013
 Ana Sofia Preto 19/06/2013 Understanding the underlying pathophysiologic processes leading to the various types of calcifications Description and illustration of the several types of calcifications, according
Ana Sofia Preto 19/06/2013 Understanding the underlying pathophysiologic processes leading to the various types of calcifications Description and illustration of the several types of calcifications, according
Current issues and controversies in breast imaging. Kate Brown, South GP CME 2015
 Current issues and controversies in breast imaging Kate Brown, South GP CME 2015 JUDICIOUS USE OF RESOURCES IN REFERRALS FOR BREAST IMAGING THE DILEMMA How do target referrals for breast imaging? Want
Current issues and controversies in breast imaging Kate Brown, South GP CME 2015 JUDICIOUS USE OF RESOURCES IN REFERRALS FOR BREAST IMAGING THE DILEMMA How do target referrals for breast imaging? Want
BREAST AND CERVICAL CANCER CONTROL NAVIGATION PROGRAM MEDICAL PROTOCOL OCTOBER 2018
 1 TABLE OF CONTENTS I. Introduction page 2 II. BCCCNP Clinical Services Provided to Eligible Clients - page 3 III. BCCCNP Age and Insurance Eligibility to Receive Breast and Cervical Cancer Screening and/or
1 TABLE OF CONTENTS I. Introduction page 2 II. BCCCNP Clinical Services Provided to Eligible Clients - page 3 III. BCCCNP Age and Insurance Eligibility to Receive Breast and Cervical Cancer Screening and/or
Breast Health. Knowledge and self-awareness are powerful tools. Understanding and utilizing these tools starts with
 k Breast Health Knowledge and self-awareness are powerful tools. Understanding and utilizing these tools starts with Lake Charles Memorial s Breast Health Program. Developing a sense of what the everyday
k Breast Health Knowledge and self-awareness are powerful tools. Understanding and utilizing these tools starts with Lake Charles Memorial s Breast Health Program. Developing a sense of what the everyday
SAMPLE. Do Not Reproduce. Breast Lumps & Breast Cancer. Breast Lumps. Breast Cancer. Treatment. Signs, Symptoms, and Causes. Signs and Symptoms
 Breast Lumps & Breast Cancer Feeling a lump in a breast can be scary. For a lot of women, the first thought is cancer. The good news is that 80% to 90% of breast lumps are not cancer. If you feel a lump
Breast Lumps & Breast Cancer Feeling a lump in a breast can be scary. For a lot of women, the first thought is cancer. The good news is that 80% to 90% of breast lumps are not cancer. If you feel a lump
Mammography and Other Screening Tests. for Breast Problems
 301.681.3400 OBGYNCWC.COM Mammography and Other Screening Tests What is a screening test? for Breast Problems A screening test is used to find diseases, such as cancer, in people who do not have signs
301.681.3400 OBGYNCWC.COM Mammography and Other Screening Tests What is a screening test? for Breast Problems A screening test is used to find diseases, such as cancer, in people who do not have signs
Non-mass Enhancement on Breast MRI. Aditi A. Desai, MD Margaret Ann Mays, MD
 Non-mass Enhancement on Breast MRI Aditi A. Desai, MD Margaret Ann Mays, MD Breast MRI Important screening and diagnostic tool, given its high sensitivity for breast cancer detection Breast MRI - Indications
Non-mass Enhancement on Breast MRI Aditi A. Desai, MD Margaret Ann Mays, MD Breast MRI Important screening and diagnostic tool, given its high sensitivity for breast cancer detection Breast MRI - Indications
MEDICAL IMAGING AND BREAST DISEASE HOW CAN WE HELP YOU?
 MEDICAL IMAGING AND BREAST DISEASE HOW CAN WE HELP YOU? Barbara M. Preston, M.D. SCREENING MAMMOGRAPHY AVERAGE RISK PATIENTS KAISER RECOMMENDATION: ALL WOMEN (INCLUDING TRANSGENDER FEMALES) Every 1-21
MEDICAL IMAGING AND BREAST DISEASE HOW CAN WE HELP YOU? Barbara M. Preston, M.D. SCREENING MAMMOGRAPHY AVERAGE RISK PATIENTS KAISER RECOMMENDATION: ALL WOMEN (INCLUDING TRANSGENDER FEMALES) Every 1-21
Breast Imaging & You
 Breast Imaging & You What s Inside: Breast Imaging... 2 Digital Breast Tomosynthesis (DBT) mammograms... 4 Breast cancer screening... 6 Dense breast tissue... 8 Automated Breast Ultrasound (ABUS)... 9
Breast Imaging & You What s Inside: Breast Imaging... 2 Digital Breast Tomosynthesis (DBT) mammograms... 4 Breast cancer screening... 6 Dense breast tissue... 8 Automated Breast Ultrasound (ABUS)... 9
Breast Cancer Diagnosis, Treatment and Follow-up
 Breast Cancer Diagnosis, Treatment and Follow-up What is breast cancer? Each of the body s organs, including the breast, is made up of many types of cells. Normally, healthy cells grow and divide to produce
Breast Cancer Diagnosis, Treatment and Follow-up What is breast cancer? Each of the body s organs, including the breast, is made up of many types of cells. Normally, healthy cells grow and divide to produce
PATIENT INFORMATION. about BREAST CANCER
 PATIENT INFORMATION about BREAST CANCER What is Breast Cancer? The female breast is made up mainly of: Lobules (milk-producing glands) Ducts (tiny tubes that carry the milk from the lobules to the nipple)
PATIENT INFORMATION about BREAST CANCER What is Breast Cancer? The female breast is made up mainly of: Lobules (milk-producing glands) Ducts (tiny tubes that carry the milk from the lobules to the nipple)
Breast Cancer Screening and Treatment Mrs Belinda Scott Breast Surgeon Breast Associates Auckland
 Breast Cancer Screening and Treatment 2009 Mrs Belinda Scott Breast Surgeon Breast Associates Auckland BREAST CANCER THE PROBLEM 1.1 million women per year 410,000 deaths each year Increasing incidence
Breast Cancer Screening and Treatment 2009 Mrs Belinda Scott Breast Surgeon Breast Associates Auckland BREAST CANCER THE PROBLEM 1.1 million women per year 410,000 deaths each year Increasing incidence
CPC 4 Breast Cancer. Rochelle Harwood, a 35 year old sales assistant, presents to her GP because she has noticed a painless lump in her left breast.
 CPC 4 Breast Cancer Rochelle Harwood, a 35 year old sales assistant, presents to her GP because she has noticed a painless lump in her left breast. 1. What are the most likely diagnoses of this lump? Fibroadenoma
CPC 4 Breast Cancer Rochelle Harwood, a 35 year old sales assistant, presents to her GP because she has noticed a painless lump in her left breast. 1. What are the most likely diagnoses of this lump? Fibroadenoma
Radiologic and pathologic correlation of non-mass like breast lesions on US and MRI: Benign, high risk, versus malignant
 Radiologic and pathologic correlation of non-mass like breast lesions on US and MRI: Benign, high risk, versus malignant Poster No.: C-1161 Congress: ECR 2013 Type: Educational Exhibit Authors: J. Kwak,
Radiologic and pathologic correlation of non-mass like breast lesions on US and MRI: Benign, high risk, versus malignant Poster No.: C-1161 Congress: ECR 2013 Type: Educational Exhibit Authors: J. Kwak,
Radiologic and pathologic correlation of non-mass like breast lesions on US and MRI: Benign, high risk, versus malignant
 Radiologic and pathologic correlation of non-mass like breast lesions on US and MRI: Benign, high risk, versus malignant Poster No.: C-1161 Congress: ECR 2013 Type: Educational Exhibit Authors: J. Kwak,
Radiologic and pathologic correlation of non-mass like breast lesions on US and MRI: Benign, high risk, versus malignant Poster No.: C-1161 Congress: ECR 2013 Type: Educational Exhibit Authors: J. Kwak,
Breast Imaging Update: Old Dog New Tricks
 Breast Imaging Update: Old Dog New Tricks Claire McKay, DO M&S Imaging Assoc. San Antonio, TX cmckayhart@juno.com Goals Describe modalities available, old and new Provide understanding of pros and cons
Breast Imaging Update: Old Dog New Tricks Claire McKay, DO M&S Imaging Assoc. San Antonio, TX cmckayhart@juno.com Goals Describe modalities available, old and new Provide understanding of pros and cons
Breast Imaging & You
 Breast Imaging & You What s Inside: Breast Imaging... 2 Digital Breast Tomosynthesis (DBT) mammograms... 4 Breast cancer screening... 6 Dense breast tissue... 8 Automated breast ultrasound (ABUS)... 9
Breast Imaging & You What s Inside: Breast Imaging... 2 Digital Breast Tomosynthesis (DBT) mammograms... 4 Breast cancer screening... 6 Dense breast tissue... 8 Automated breast ultrasound (ABUS)... 9
FY16 BCCS Reimbursement Rates and Billing Guidelines Appendix B 2
 FY16 BCCS Reimbursement Rates and Billing Guidelines Appendix B 2 77053 Mammary ductogram or galactogram, single duct, Global Fee $59.05 May be billed with 77055, G0206, 77056, G0204, 76641, 76642 Billable
FY16 BCCS Reimbursement Rates and Billing Guidelines Appendix B 2 77053 Mammary ductogram or galactogram, single duct, Global Fee $59.05 May be billed with 77055, G0206, 77056, G0204, 76641, 76642 Billable
Case Scenario 1: This case has been slightly modified from the case presented during the live session to add clarity.
 Case Scenario 1: This case has been slightly modified from the case presented during the live session to add clarity. Background: 46 year old married premenopausal female with dense breasts has noticed
Case Scenario 1: This case has been slightly modified from the case presented during the live session to add clarity. Background: 46 year old married premenopausal female with dense breasts has noticed
For more information about how to cite these materials visit
 Author: Vincent M. Cimmino, M.D., 2011 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Share Alike 3.0 License: http://creativecommons.org/licenses/by-sa/3.0/
Author: Vincent M. Cimmino, M.D., 2011 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Share Alike 3.0 License: http://creativecommons.org/licenses/by-sa/3.0/
Breast Health and Imaging Glossary
 Contact: Lorna Vaughan HerSpace Breast Imaging & Biopsy Associates 300 State Route 35 South W. Long Branch, NJ 07764 732-571-9100, ext. 104 lorna@breast-imaging.com Breast Health and Imaging Glossary Women
Contact: Lorna Vaughan HerSpace Breast Imaging & Biopsy Associates 300 State Route 35 South W. Long Branch, NJ 07764 732-571-9100, ext. 104 lorna@breast-imaging.com Breast Health and Imaging Glossary Women
The radiologic workup of a palpable breast mass
 Imaging in Practice CME CREDIT EDUCTIONL OJECTIVE: The reader will consider which breast masses require further workup and which imaging study is most appropriate Lauren Stein, MD Imaging Institute, Cleveland
Imaging in Practice CME CREDIT EDUCTIONL OJECTIVE: The reader will consider which breast masses require further workup and which imaging study is most appropriate Lauren Stein, MD Imaging Institute, Cleveland
ORIGINAL ARTICLE EVALUATION OF BREAST LESIONS USING X-RAY MAMMOGRAM WITH HISTOPATHOLOGICAL CORRELATION
 Available online at www.journalijmrr.com INTERNATIONAL JOURNAL OF MODERN RESEARCH AND REVIEWS IJMRR ISSN: 2347-8314 Int. J. Modn. Res. Revs. Volume 3, Issue 10, pp 807-814, October, 2015 ORIGINAL ARTICLE
Available online at www.journalijmrr.com INTERNATIONAL JOURNAL OF MODERN RESEARCH AND REVIEWS IJMRR ISSN: 2347-8314 Int. J. Modn. Res. Revs. Volume 3, Issue 10, pp 807-814, October, 2015 ORIGINAL ARTICLE
Breast Cancer. Most common cancer among women in the US. 2nd leading cause of death in women. Mortality rates though have declined
 Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women Mortality rates though have declined 1 in 8 women will develop breast cancer Breast Cancer Breast cancer increases
Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women Mortality rates though have declined 1 in 8 women will develop breast cancer Breast Cancer Breast cancer increases
Melissa Hartman, DO Women s Health Orlando VA Medical Center
 Melissa Hartman, DO Women s Health Orlando VA Medical Center Most common non-skin cancer and Second deadliest cancer in women Majority are diagnosed by abnormal screening study An approach to breast cancer
Melissa Hartman, DO Women s Health Orlando VA Medical Center Most common non-skin cancer and Second deadliest cancer in women Majority are diagnosed by abnormal screening study An approach to breast cancer
Breast pathology. 2nd Department of Pathology Semmelweis University
 Breast pathology 2nd Department of Pathology Semmelweis University Breast pathology - Summary - Benign lesions - Acute mastitis - Plasma cell mastitis / duct ectasia - Fat necrosis - Fibrocystic change/
Breast pathology 2nd Department of Pathology Semmelweis University Breast pathology - Summary - Benign lesions - Acute mastitis - Plasma cell mastitis / duct ectasia - Fat necrosis - Fibrocystic change/
Karen degenevieve MSN, FNP, BC
 Karen degenevieve MSN, FNP, BC Become more comfortable treating common breast complaints. Discuss recent controversial screening recommendations. Discuss oral medications used in breast cancer prevention
Karen degenevieve MSN, FNP, BC Become more comfortable treating common breast complaints. Discuss recent controversial screening recommendations. Discuss oral medications used in breast cancer prevention
Breast Cancer. Saima Saeed MD
 Breast Cancer Saima Saeed MD Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women 1 in 8 women will develop breast cancer Incidence/mortality rates have declined Breast
Breast Cancer Saima Saeed MD Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women 1 in 8 women will develop breast cancer Incidence/mortality rates have declined Breast
PRINCIPLES OF BREAST SURGERY & COMPLICATIONS
 PRINCIPLES OF BREAST SURGERY & COMPLICATIONS Adam Cichowitz The Royal Melbourne Hospital ANATOMY Lies in subcutaneous tissue Base: midline to midaxillary line, 2nd to 6th rib Overlies pec major, serratus
PRINCIPLES OF BREAST SURGERY & COMPLICATIONS Adam Cichowitz The Royal Melbourne Hospital ANATOMY Lies in subcutaneous tissue Base: midline to midaxillary line, 2nd to 6th rib Overlies pec major, serratus
Mousa. Israa Ayed. Abdullah AlZibdeh. 0 P a g e
 1 Mousa Israa Ayed Abdullah AlZibdeh 0 P a g e Breast pathology The basic histological units of the breast are called lobules, which are composed of glandular epithelial cells (luminal cells) resting on
1 Mousa Israa Ayed Abdullah AlZibdeh 0 P a g e Breast pathology The basic histological units of the breast are called lobules, which are composed of glandular epithelial cells (luminal cells) resting on
Breast Imaging Lexicon
 9//201 200 BI RADS th Edition 201 BI RADS th Edition Breast Imaging Lexicon Mammographic Pathology and Assessment Categories Deborah Thames, R.T.(R)(M)(QM) The Advanced Health Education Center Nonmember:
9//201 200 BI RADS th Edition 201 BI RADS th Edition Breast Imaging Lexicon Mammographic Pathology and Assessment Categories Deborah Thames, R.T.(R)(M)(QM) The Advanced Health Education Center Nonmember:
Epworth Healthcare Benign Breast Disease Symposium. Sat Nov 12 th 2016
 Epworth Healthcare Benign Breast Disease Symposium Breast cancer is common Sat Nov 12 th 2016 Benign breast disease is commoner, and anxiety about breast disease commoner still Breast Care Campaign UK
Epworth Healthcare Benign Breast Disease Symposium Breast cancer is common Sat Nov 12 th 2016 Benign breast disease is commoner, and anxiety about breast disease commoner still Breast Care Campaign UK
Detecting and Treating Breast Problems
 WOMENCARE A Healthy Woman is a Powerful Woman (407) 898-1500 Detecting and Treating Breast Problems A woman's breasts are always changing. They change during the menstrual cycle, pregnancy, breastfeeding,
WOMENCARE A Healthy Woman is a Powerful Woman (407) 898-1500 Detecting and Treating Breast Problems A woman's breasts are always changing. They change during the menstrual cycle, pregnancy, breastfeeding,
Case Scenario 1: This case has been slightly modified from the case presented during the live session to add clarity.
 Case Scenario 1: This case has been slightly modified from the case presented during the live session to add clarity. Background: 46 year old married premenopausal female with dense breasts has noticed
Case Scenario 1: This case has been slightly modified from the case presented during the live session to add clarity. Background: 46 year old married premenopausal female with dense breasts has noticed
Understanding. Breast Changes. National Cancer Institute. A Health Guide for Women. National Institutes of Health
 National Cancer Institute Understanding Breast Changes A Health Guide for Women U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES National Institutes of Health It was easier to talk with my doctor after reading
National Cancer Institute Understanding Breast Changes A Health Guide for Women U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES National Institutes of Health It was easier to talk with my doctor after reading
ANNEX 1 OBJECTIVES. At the completion of the training period, the fellow should be able to:
 1 ANNEX 1 OBJECTIVES At the completion of the training period, the fellow should be able to: 1. Breast Surgery Evaluate and manage common benign and malignant breast conditions. Assess the indications
1 ANNEX 1 OBJECTIVES At the completion of the training period, the fellow should be able to: 1. Breast Surgery Evaluate and manage common benign and malignant breast conditions. Assess the indications
Screening Mammograms: Questions and Answers
 CANCER FACTS N a t i o n a l C a n c e r I n s t i t u t e N a t i o n a l I n s t i t u t e s o f H e a l t h D e p a r t m e n t o f H e a l t h a n d H u m a n S e r v i c e s Screening Mammograms:
CANCER FACTS N a t i o n a l C a n c e r I n s t i t u t e N a t i o n a l I n s t i t u t e s o f H e a l t h D e p a r t m e n t o f H e a l t h a n d H u m a n S e r v i c e s Screening Mammograms:
Leonard M. Glassman MD Analysis of Breast Calcifications
 Importance of Calcification Leonard M. Glassman MD FACR American Institute for Radiologic Pathology Washington Radiology Associates, PC Washington DC 45% of all breast cancers present as calcification
Importance of Calcification Leonard M. Glassman MD FACR American Institute for Radiologic Pathology Washington Radiology Associates, PC Washington DC 45% of all breast cancers present as calcification
04/10/2018. Intraductal Papillary Neoplasms Of Breast INTRADUCTAL PAPILLOMA
 Intraductal Papillary Neoplasms Of Breast Savitri Krishnamurthy MD Professor of Pathology Deputy Division Head The University of Texas MD Anderson Cancer Center 25 th Annual Seminar in Pathology Pittsburgh,
Intraductal Papillary Neoplasms Of Breast Savitri Krishnamurthy MD Professor of Pathology Deputy Division Head The University of Texas MD Anderson Cancer Center 25 th Annual Seminar in Pathology Pittsburgh,
Cairo/EG, Khartoum/SD, London/UK Biological effects, Diagnostic procedure, Ultrasound, Mammography, Breast /ecr2015/C-0107
 Role of sono-mammography in the evaluation of clinically palapble breast masses during pregnancy & lactation with differentaition between true patholgical & false physiological lobular hyperlpasia.sudanese
Role of sono-mammography in the evaluation of clinically palapble breast masses during pregnancy & lactation with differentaition between true patholgical & false physiological lobular hyperlpasia.sudanese
Breast Pathology. Breast Development
 Breast Pathology Lecturer: Hanina Hibshoosh, M.D. Reading: Kumar, Cotran, Robbins, Basic Pathology, 6th Edition, pages 623-635 Breast Development 5th week - thickening of the epidermis - milk line 5th
Breast Pathology Lecturer: Hanina Hibshoosh, M.D. Reading: Kumar, Cotran, Robbins, Basic Pathology, 6th Edition, pages 623-635 Breast Development 5th week - thickening of the epidermis - milk line 5th
F r e q u e n t l y A s k e d Q u e s t i o n s. Mammograms
 Mammograms Q: What is a mammogram? A: A mammogram is a safe, low-dose x-ray exam of the breasts to look for changes that are not normal. The results are recorded on x-ray film or directly into a computer
Mammograms Q: What is a mammogram? A: A mammogram is a safe, low-dose x-ray exam of the breasts to look for changes that are not normal. The results are recorded on x-ray film or directly into a computer
Treatment options for the precancerous Atypical Breast lesions. Prof. YOUNG-JIN SUH The Catholic University of Korea
 Treatment options for the precancerous Atypical Breast lesions Prof. YOUNG-JIN SUH The Catholic University of Korea Not so benign lesions? Imaging abnormalities(10% recall) lead to diagnostic evaluation,
Treatment options for the precancerous Atypical Breast lesions Prof. YOUNG-JIN SUH The Catholic University of Korea Not so benign lesions? Imaging abnormalities(10% recall) lead to diagnostic evaluation,
Breast Cancer Task Force of the Greater Miami Valley A collaborative effort of health care professionals and breast cancer survivors in the Greater
 Breast Cancer Task Force of the Greater Miami Valley A collaborative effort of health care professionals and breast cancer survivors in the Greater Dayton Area Last Updated Fall 2014 TABLE OF CONTENTS
Breast Cancer Task Force of the Greater Miami Valley A collaborative effort of health care professionals and breast cancer survivors in the Greater Dayton Area Last Updated Fall 2014 TABLE OF CONTENTS
UW Radiology Review Course Breast Calcifications. BI-RADS 5 th Edition
 UW Radiology Review Course Breast Calcifications Grace Kalish, MD Vantage Radiology BI-RADS 5 th Edition Benign Skin Vascular Large rod like Coarse popcorn Suspicious Amorphous Coarse heterogenous Fine
UW Radiology Review Course Breast Calcifications Grace Kalish, MD Vantage Radiology BI-RADS 5 th Edition Benign Skin Vascular Large rod like Coarse popcorn Suspicious Amorphous Coarse heterogenous Fine
Criteria of Malignancy. Evaluation Score
 30 5 Diagnostic Criteria Criteria of Malignancy Table 5.2 lists criteria in contrast-enhancing MR mammography that strongly indicate the presence of malignancy or are unspecific. Unifactorial evaluation
30 5 Diagnostic Criteria Criteria of Malignancy Table 5.2 lists criteria in contrast-enhancing MR mammography that strongly indicate the presence of malignancy or are unspecific. Unifactorial evaluation
Breast Imaging Essentials
 Breast Imaging Essentials Module 5 Transcript 2016 ASRT. All rights reserved. Breast Imaging Essentials Module 5 Pathology 1. ASRT Animation 2. Welcome Welcome to Module 5 of Breast Imaging Essentials
Breast Imaging Essentials Module 5 Transcript 2016 ASRT. All rights reserved. Breast Imaging Essentials Module 5 Pathology 1. ASRT Animation 2. Welcome Welcome to Module 5 of Breast Imaging Essentials
SIGNIFICANT OTHERS. Miscellaneous Benign Breast Conditions
 SIGNIFICANT OTHERS Miscellaneous Benign Breast Conditions Epworth HealthCare 1 FAT NECROSIS TRAUMATIC Cell rupture Seat-Belt injury Blunt trauma Iatrogenic injury Surgery, Flaps, Radiotherapy Pathology
SIGNIFICANT OTHERS Miscellaneous Benign Breast Conditions Epworth HealthCare 1 FAT NECROSIS TRAUMATIC Cell rupture Seat-Belt injury Blunt trauma Iatrogenic injury Surgery, Flaps, Radiotherapy Pathology
BREAST SURGERY PROGRESS TEST Name:
 General Surgery Residency Program Excellent surgeons BREAST SURGERY PROGRESS TEST Name: Choose the BEST answer for the following questions. 1. All of the following factors are associated with an increased
General Surgery Residency Program Excellent surgeons BREAST SURGERY PROGRESS TEST Name: Choose the BEST answer for the following questions. 1. All of the following factors are associated with an increased
BreastScreen Victoria Annual Statistical Report
 BreastScreen Victoria Annual Statistical Report 005 Produced by: BreastScreen Victoria Coordination Unit Level, Pelham Street, Carlton South Victoria 05 PH 0 9660 6888 FX 0 966 88 EM info@breastscreen.org.au
BreastScreen Victoria Annual Statistical Report 005 Produced by: BreastScreen Victoria Coordination Unit Level, Pelham Street, Carlton South Victoria 05 PH 0 9660 6888 FX 0 966 88 EM info@breastscreen.org.au
Evaluation of Abnormal Screening Mammograms
 342 Evaluation of Abnormal Screening Mammograms Ellen Shaw de Paredes, M.D. The purpose of routine screening mammography is to detect unsuspected cancer that has the potential to be cured. Abnormalities
342 Evaluation of Abnormal Screening Mammograms Ellen Shaw de Paredes, M.D. The purpose of routine screening mammography is to detect unsuspected cancer that has the potential to be cured. Abnormalities
Ultrasound of the Breast BASICS FOR THE ORDERING CLINICIAN
 Ultrasound of the Breast BASICS FOR THE ORDERING CLINICIAN Breast Ultrasound Anatomy Skin Breast Parenchyma Pectoralis Fascia Pectoralis Breast Ultrasound Anatomy Indications for Breast Ultrasound Palpable
Ultrasound of the Breast BASICS FOR THE ORDERING CLINICIAN Breast Ultrasound Anatomy Skin Breast Parenchyma Pectoralis Fascia Pectoralis Breast Ultrasound Anatomy Indications for Breast Ultrasound Palpable
AMSER Case of the Month: November 2018
 AMSER Case of the Month: November 2018 42 year old with right breast mass Rina Kiyota Petek Lake Erie College of Osteopathic Medicine, OMS-III Kossivi Dantey, MD Bibianna Klepchick, MD Matthew Hartman,
AMSER Case of the Month: November 2018 42 year old with right breast mass Rina Kiyota Petek Lake Erie College of Osteopathic Medicine, OMS-III Kossivi Dantey, MD Bibianna Klepchick, MD Matthew Hartman,
PAAF vs Core Biopsy en Lesiones Mamarias Case #1
 5/19/2014 PAAF vs Core Biopsy en Lesiones Mamarias Case #1 Fine Needle Aspiration Cytology of Breast: Correlation with Needle Core Biopsy 64-year-old woman Mass in breast Syed Hoda, MD CD31 Post-Radiation
5/19/2014 PAAF vs Core Biopsy en Lesiones Mamarias Case #1 Fine Needle Aspiration Cytology of Breast: Correlation with Needle Core Biopsy 64-year-old woman Mass in breast Syed Hoda, MD CD31 Post-Radiation