Statins ARE Enough For The Prevention of CVD! Professor Kausik Ray Imperial College London, UK
|
|
|
- Lora Whitehead
- 5 years ago
- Views:
Transcription
1 1 Disclosures Advisory boards PCSK9- Sanofi/ Regeneron, Amgen, Pfizer, Roche, MSD NLI/ SC member for Odyssey- (Sanofi/ Regeneron), Roche Investigator initiated research grant support (Sanofi/Regeneron/ Pfizer/ Amgen/ MSD) CME lectures at Symposia (Sanofi/ Regeneron, Amgen, Pfizer, AZ, MSD)


2 Statins ARE Enough For The Prevention of CVD! Professor Kausik Ray Imperial College London, UK
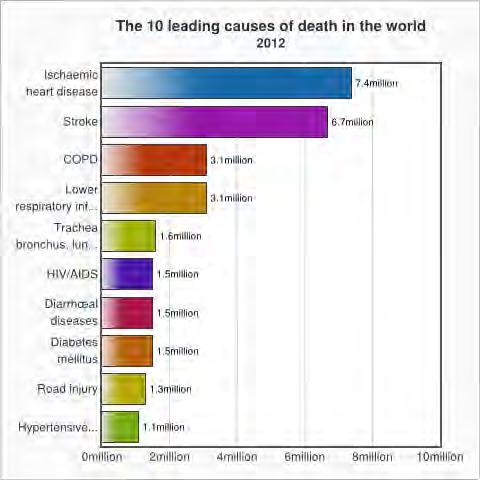
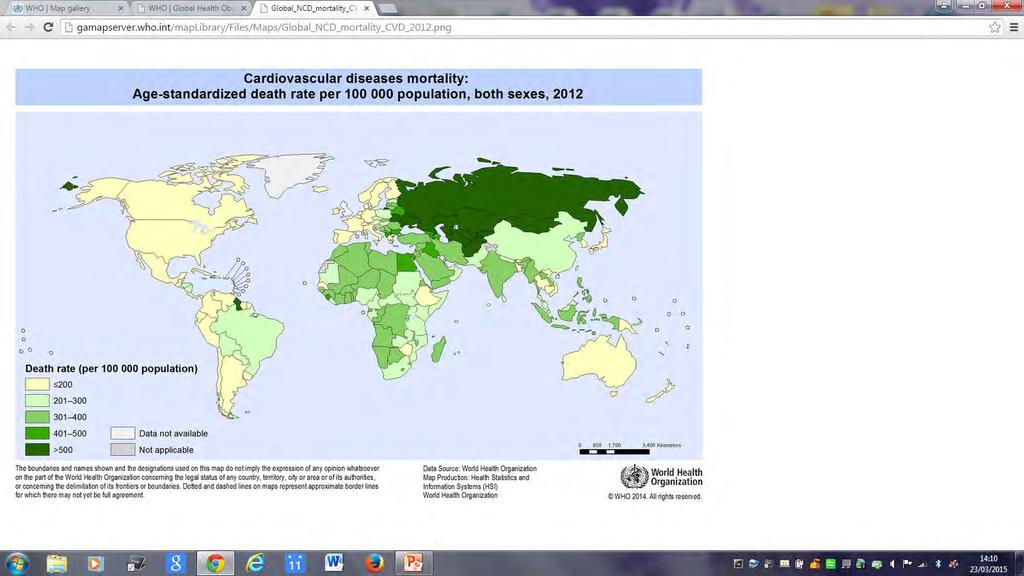
3 Before Considering Whether a Treatment is Enough Consider The Following Is there a problem? Where is the problem/ who is affected? Is there a proven treatment in the majority? Is the treatment easy to administer and take for the patient? Is the treatment safe when you give it to the masses? Is the treatment affordable?
4
5
6
7
8 Statins are the current standard of care in treating dyslipidaemia Statins have been the cornerstone of drug therapy since their introduction in the late 1980s due to their effectiveness in reducing LDL-C by 63% 1 Lowering LDL-C with statin regimens can reduce the 5-year event rate of first major coronary events, revascularisations, and strokes by ~1/4 per 1.0 mmol/l reduction in LDL-C 2 Serious adverse side effects are rare 3,4 A variety of statins with well-established efficacy and safety profiles are available to tailor treatment 1 New formulations may ensure better adherence and more extensive dosing regimens LDL-C, low-density lipoprotein cholesterol 1. Jeger R & Dieterle T. Swiss Med Wkly 2012;142:w13515; 2. Heart Protection Study Collaborative Group. Lancet 2002;360:7 22; 3. Semple SJ. Lipids in Health and Disease 2012;11:40; 4. Naci H et al. Circ Cardiovasc Qual Outcomes 2013;6:
9 Reduction of LDL-C leads to the reduction of major vascular events 50% Major vascular events Proportional reduction in event rate (SE) 40% 30% 20% 10% 0% % Reduction in LDL cholesterol (mmol/l) SE, standard error Baigent C et al. Lancet 2005;366:
10 Effect on major coronary events is independent of baseline prognostic factors Events (%) Groups Treatment Control Rate Ratio (CI) Prior disease Post-MI 1681 (11 7) 2207 (15 4) 0.78 ( ) Other CHD 568 (8 7) 744 (11 4) 0.77 ( ) None 1088 (4 5) 1469 (6 1) 0.72 ( ) Age (years) (6 1) 2344 (8 5) 0.74 ( ) > (9 5) 2076 (11 9) 0.81 ( ) Gender Male 2686 (7 8) 3630 (10 6) 0.76 ( ) Female 651 (6 1) 790 (7 3) 0.82 ( ) Treated hypertension Yes 2038 (8 2) 2596 (10 4) 0.79 ( ) No 1299 (6 4) 1824 (9 1) 0.75 ( ) History of diabetes Yes 776 (8 3) 979 (10 5) 0.78 ( ) No 2561 (7 2) 3441 (9 6) 0.77 ( ) Diastolic blood pressure (mmhg) (7 8) 3590 (10 3) 0.77 ( ) > (6 1) 827 (8 2) 0.76 ( ) Overall 3337 (7 4) 4420 (7 4) 0.77 ( ) MI, myocardial infarction; CHD, coronary heart disease; CI, confidence interval Baigent C et al. Lancet 2005;366: Effect p<0.0001
11 Effect on major coronary events is independent of baseline lipid values Groups (mmol/l) Events (%) Treatment Control Total cholesterol: (6 9) 940 (8 6) > (7 0) 2246 (9 4) > (8 8) 1220 (12 1) LDL cholesterol: (6 8) 1443 (8 7) > (7 3) 1814 (9 6) > (9 3) 1120 (12 9) HDL cholesterol: (9 3) 1538 (12 1) > (7 4) 1270 (10 2) > (6 2) 1595 (8 1) Triglycerides: (7 3) 1521 (9 6) > (7 1) 1304 (9 8) > (7 9) 1564 (10 2) Overall 3337 (7 4) 4420 (9 8) RR & CI (Treatment:Control) Heterogeneity/trend p-value p=0 7 p=0 5 p=0 8 p= ( ) RR, rate ratio, HDL, high-density lipoprotein Baigent C et al. Lancet 2005;366: Treatment Control better better Effect p<0.0001
12 No threshold of baseline LDL-C for benefit from intensive statin therapy Events (% per annum) RR (CI) per 1 mmol/l reduction in LDL-C Trend test Statin/more Control/less More vs less statin <2 mmol/l 704 (4.6%) 795 (5.2%) 0.71 ( ) 2 to <2.5 mmol/l 1189 (4.2%) 1317 (4.8%) 0.77 ( ) 2.5 to <3.0 mmol/l 1065 (4.5%) 1203 (5.0%) 0.81 ( ) χ 2 = to <3.5 mmol/l 517 (4.5%) 633 (5.8%) 0.61 ( ) (p = 0.2) 3.5 mmol/l 303 (5.7%) 398 (7.8%) 0.64 ( ) Total 3837 (4.5%) 4416 (5.3%) 0.72 ( ) 99%; or 95% CI Statin/more better Control/less better Cholesterol Treatment Trialists (CTT) Collaboration. Lancet 2010;376:


13 Guidelines recommend LDL-C targets and the prescription of highest recommended statin doses to reach targets Maximum doses of statins are infrequently prescribed 1 there is room for improvement CVD, cardiovascular disease; a, class of recommendation; b, level of evidence; c, references Tables taken from ESC/EAS Guidelines for the management of dyslipidaemias 2 1. Hermans MP et al. Curr Med Res Opin 2010;26: ; 2. Eur Heart J 2011;32:

14 4 Statin Benefit Groups IA IA IB IA IIaB






15
16 Side effects are not more frequent with high-dose statins Trial ALN 3xULN (%) Higher dose Lower dose CK 10xULN or myopathy (%) Higher dose *Reported as persistent elevation in alanine or aspartate transaminase ALN, alanine transaminase; ULN, upper limit of normal; CK, creatine kinase Armitage J. Lancet 2007;370: Lower dose Rhabdomyolysis (%) Higher dose Lower dose PROVE-IT Phase Z of A to Z trial* TNT* IDEAL SPARCL*
17 No evidence that statins increase the risk of cancer Relative risk of onset of cancer from the Cholesterol Treatment Trialists' (CTT) meta-analysis of statin trials, according to year of onset Year of onset No. with cancer onset in trials Statin (N = 45,054) Control (N = 45,002) Risk Ratio for statin vs control (CI) > > > > All 2810/199,063 person-year (1.4% per year) 2804/197,680 person-year (1.4% per year) Statin better Control better Peto R et al. N Engl J Med 2008;359:
:1011-1012. doi:10.1001/jama.2015.")
18 From: Statin Intolerance: Reconciling Clinical Trials and Clinical Experience JAMA. 2015;313(10): doi: /jama Table Title: Muscle Adverse Events Reported in Randomized, Double-Blind, Placebo-Controlled Cardiovascular Outcome Trials of Statins a Date of download: 5/18/2015 Copyright 2015 American Medical Association. All rights reserved.


19 Patients intolerant to a particular statin are able to tolerate an alternative statin without side effects Due to the different PKs and metabolism of individual statins, patients intolerant to a statin may tolerate another 1 Nearly two-thirds of the statin-intolerant patients were able to tolerate an alternative statin without side effects 1 No evidence so far that add-on LDL-lowering therapies decrease the residual CV risk 2,3 PK pharmacokinetic 1. Nair RK et al. The British Journal of Cardiology. Managing patients with statin intolerance : a retrospective study available at: accessed July 2013; 2. Cimminielo C. Intern Emerg Med 2011;6(suppl 1):53 60; 3. Michos ED et al. J Am Coll Cardiol 2012;59:
20 How well are we doing with statins?
21 Overall rates of secondary prevention medication use for CVD is low worldwide PURE study, 17 countries 100 Antiplatelet Beta-blockers ACEi or ARBs Diuretics % of patients with treatment BP-lowering Ca-channel blockers Statins CHD Stroke CHD or stroke PURE, Prospective Urban Rural Epidemiology; ACEi, angiotensin-converting-enzyme inhibitor; ARB, angiotensin receptor blocker; BP, blood pressure Yusuf S et al. Lancet 2011;378:
22 % of patients at LDL-C goal CEPHEUS: about half of patients achieved LDL-C goals 65 Patients on lipid-lowering drugs for >3 months (stable medication >6 weeks) 41 Europe 1 JETF guidelines Asia 2 NCEP ATP III guidelines* *Patients with 2 cardiovascular risk factors according to NCEP ATP III guidelines; CEPHEUS, CEntralized Pan-European survey on the Under-treatment of hypercholesterolaemia, NCEP ATP, National Cholesterol Educational Program Adult Treatment Panel; JETF, Joint European Task Force 1. Hermans MP et al. Curr Med Res Opin 2010;26: ; 2. Park JE et al. Eur J Prev Cardiol 2012;19:
23 Physicians don t like to switch treatment regimens; patients don t like to be switched Europe (N=15,199) Asia (N=8,064) % of patients Same tablet, same dose Same tablet, dose increased Switched 2 times Switched 3 times About 60% of patients still on same lipid-lowering drug since first prescribed 1,2 Statins could be used better (up-titration, switching) 1. Hermans MP et al. Curr Med Res Opin 2010;26: ; 2. Park JE et al. Eur J Prev Cardiol 2012;19:
24 Nearly half of patients sometimes forget to take their tablets % of patients forgetting to take their tablets Europe (N=15,199) Sometimes Once every 2 weeks 26 Asia (N=8,064) 16 Once every week Europe (N=15,199) Thought that missing their daily tablets at least once a week would not jeopardise their cholesterol levels 32 44% of patients sometimes forgot to take their tablets, up to a quarter forgot once a week 1,2 Up to 40% of the patients thought missing a tablet at least once a week would not affect their cholesterol levels 1,2 % of patients 1. Hermans MP et al. Curr Med Res Opin 2010;26: ; 2. Park JE et al. Eur J Prev Cardiol 2012;19: Asia (N=8,064)
25 Before considering other treatments, increasing persistence may do the job Primary prevention (goal: <130 mg/dl N=87,219) Secondary prevention (goal: <100 mg/dl N=15,139) % of patients reaching LDL-C goal High persistence (PDC 80%) PDC, proportion of days covered Shalev V et al. Pharmacotherapy 2013 doi: /phar.1326 Poor persistence (PDC 33%) Persistence with statins was strongly associated with drug effect of LDL level reduction
26 Screen early, treat early, think about lifetime risk 54.5% relative risk reduction per 1 mm/l (38.7mg/dL) LDL-C lowering 22% relative risk reduction per 1 mmol/l (38.7mg/dL) LDL-C lowering 50% Major vascular events Proportional Risk Reduction (SE) 30% 20% 10% rs rs rs rs rs rs12916 rs rs rs Lower LDL-C (mg/dl) Proportional reduction in event rate (SE) 40% 30% 20% 10% 0% -10% Reduction in LDL cholesterol (mmol/l) Ference BA et al. J Am Coll Cardiol 2012;60: ; Baigent C et al. Lancet 2005;366:
: 9 15% 3 Statins are affordable and available.")
27 Global access to healthcare is something that needs to be considered Current global population ~7 billion 1 Access to health care ~2 billion 2 No access to health care ~5 billion 2 Worldwide use of statins as secondary preventative medication (PURE study): 9 15% 3 Statins are affordable and available. An increase in global statin exposure will have a greater reduction in population rates of CVD than any new, expensive treatment: 5 billion new patients large ARR vs 2 billion new patients small ARR ARR, absolute risk reduction; WHO, World Health Organisation 1.United States Consensus Bureau. U.S. and World Population Clock. Available at: accessed August 2013; 2. George Institute for Global Health. Available at: accessed August 2013; 3. Yusuf S et al. Lancet 2011;378:
28 What is the real extent of unmet medical need with statins Better access to health care and evidence-based treatment such as statins will have a far greater impact on the global population Further research into optimising the use of statins in the patient population should be undertaken to maximise the benefit of these treatments
29 Why might additional therapies offer very little on top of statins?
30 The lower the baseline LDL-C the less benefit from further LDL-C reduction 1.0 Logit of the Primary Endpoint Atorvastatin 80 mg Pravastatin 40 mg Baseline LDL-C (mg/dl) Giraldez RR et al. J Am Coll Cardiol 2008;52:
31 Increase in NNT as levels of LDL- C fall Low/moderate risk: High risk: Very high risk: <~115 mg/dl <~100 mg/dl <~70 mg/dl (or 50%) LDL cholesterol (mmol/l): Events (%) Treatment Control RR & CI (Treatment:Control) NNT (6.8) 1443 (8.7) 52.6 > (7.3) 1814 (9.6) 43.5 Absolute benefit diminishes at lower baseline LDL-C levels > (9.3) 1120 (12.9) Treatment better Control better NNT, number needed to treat; Guidelines taken from European Guidelines on CVD prevention in clinical practice: Perk J et al. Eur Heart J 2012;33: ; Baigent C et al. Lancet 2005;366:

32 Weighing up the benefit of any treatment to society Statin Absolute Benefit Treatment X Absolute Harm CVD Risk Absolute cost of statins Absolute cost of Treatment X

33 Black hole in your budget with a lot of unknowns!
34 Conclusions Statins are affordable, well-tolerated and effective and have proven effects on outcomes Statins should be used more efficiently Higher dose More potent molecules Biggest population attributable benefit will come from better utilisation of statins and not more expensive, unknown treatments with small absolute gains

35 You might think statins aren t enough and you might think that you are stuck! STATINS

36 But when you find yourself stuck in a situation there is one thing that you should always remember..

37 Not everyone who shows up. PCSK9 CETP inhibitors STATINS Is there to help
Is Lower Better for LDL or is there a Sweet Spot
 Is Lower Better for LDL or is there a Sweet Spot ALAN S BROWN MD, FACC FNLA FAHA FASPC DIRECTOR, DIVISION OF CARDIOLOGY ADVOCATE LUTHERAN GENERAL HOSPITAL, PARK RIDGE, ILLINOIS DIRECTOR OF CARDIOLOGY,
Is Lower Better for LDL or is there a Sweet Spot ALAN S BROWN MD, FACC FNLA FAHA FASPC DIRECTOR, DIVISION OF CARDIOLOGY ADVOCATE LUTHERAN GENERAL HOSPITAL, PARK RIDGE, ILLINOIS DIRECTOR OF CARDIOLOGY,
Macrovascular Residual Risk. What risk remains after LDL-C management and intensive therapy?
 Macrovascular Residual Risk What risk remains after LDL-C management and intensive therapy? Defining Residual Vascular Risk The risk of macrovascular events and microvascular complications which persists
Macrovascular Residual Risk What risk remains after LDL-C management and intensive therapy? Defining Residual Vascular Risk The risk of macrovascular events and microvascular complications which persists
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD
 2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
LDL cholesterol and cardiovascular outcomes?
 LDL cholesterol and cardiovascular outcomes? Prof Kausik Ray, BSc (hons), MBChB, FRCP, MD, MPhil (Cantab), FACC, FESC Professor of Cardiovascular Disease Prevention St Georges University of London Honorary
LDL cholesterol and cardiovascular outcomes? Prof Kausik Ray, BSc (hons), MBChB, FRCP, MD, MPhil (Cantab), FACC, FESC Professor of Cardiovascular Disease Prevention St Georges University of London Honorary
ESC Geoffrey Rose Lecture on Population Sciences Cholesterol and risk: past, present and future
 ESC Geoffrey Rose Lecture on Population Sciences Cholesterol and risk: past, present and future Rory Collins BHF Professor of Medicine & Epidemiology Clinical Trial Service Unit & Epidemiological Studies
ESC Geoffrey Rose Lecture on Population Sciences Cholesterol and risk: past, present and future Rory Collins BHF Professor of Medicine & Epidemiology Clinical Trial Service Unit & Epidemiological Studies
Novel PCSK9 Outcomes. in Perspective: Lessons from FOURIER & ODYSSEY LDL-C. ASCVD Risk. Suboptimal Statin Therapy
 LDL-C Novel PCSK9 Outcomes Suboptimal Statin Therapy ASCVD Risk in Perspective: Lessons from FOURIER & ODYSSEY Jennifer G. Robinson, MD, MPH Professor, Departments of Epidemiology & Medicine Director,
LDL-C Novel PCSK9 Outcomes Suboptimal Statin Therapy ASCVD Risk in Perspective: Lessons from FOURIER & ODYSSEY Jennifer G. Robinson, MD, MPH Professor, Departments of Epidemiology & Medicine Director,
LLL Session - Nutrition support in diabetes and dyslipidemia. Dyslipidemia: targeting the management of cardiovascular risk factors. M.
 ESPEN Congress Leipzig 2013 LLL Session - Nutrition support in diabetes and dyslipidemia Dyslipidemia: targeting the management of cardiovascular risk factors M. Leon Sanz (ES) Dyslipidemia: Targeting
ESPEN Congress Leipzig 2013 LLL Session - Nutrition support in diabetes and dyslipidemia Dyslipidemia: targeting the management of cardiovascular risk factors M. Leon Sanz (ES) Dyslipidemia: Targeting
Preventive Cardiology Scientific evidence
 Preventive Cardiology Scientific evidence Professor David A Wood Garfield Weston Professor of Cardiovascular Medicine International Centre for Circulatory Health Imperial College London Primary prevention
Preventive Cardiology Scientific evidence Professor David A Wood Garfield Weston Professor of Cardiovascular Medicine International Centre for Circulatory Health Imperial College London Primary prevention
Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient
 Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient Steven E. Nissen MD Chairman, Department of Cardiovascular Medicine Cleveland Clinic Disclosure Consulting: Many pharmaceutical
Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient Steven E. Nissen MD Chairman, Department of Cardiovascular Medicine Cleveland Clinic Disclosure Consulting: Many pharmaceutical
What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline?
 What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline? Salim S. Virani, MD, PhD, FACC, FAHA Associate Professor, Section of Cardiovascular Research Baylor
What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline? Salim S. Virani, MD, PhD, FACC, FAHA Associate Professor, Section of Cardiovascular Research Baylor
Contemporary management of Dyslipidemia
 Contemporary management of Dyslipidemia Todd Anderson Feb 2018 Disclosure Statement Within the past two years: I have not had an affiliation (financial or otherwise) with a commercial organization that
Contemporary management of Dyslipidemia Todd Anderson Feb 2018 Disclosure Statement Within the past two years: I have not had an affiliation (financial or otherwise) with a commercial organization that
Treatment to reduce cardiovascular risk: multifactorial management
 Treatment to reduce cardiovascular risk: multifactorial management Matteo Anselmino, MD PhD Assistant Professor San Giovanni Battista Hospital Division of Cardiology, Department of Internal Medicine University
Treatment to reduce cardiovascular risk: multifactorial management Matteo Anselmino, MD PhD Assistant Professor San Giovanni Battista Hospital Division of Cardiology, Department of Internal Medicine University
Disclosures. Objectives 2/11/2017
 Role of Non-Statin Therapy in CV Risk Reduction James A. Underberg, MD, MS, FACPM, FACP, FASH, FNLA,FASPC Clinical Assistant Professor of Medicine NYU School of Medicine NYU Langone Center for Cardiovascular
Role of Non-Statin Therapy in CV Risk Reduction James A. Underberg, MD, MS, FACPM, FACP, FASH, FNLA,FASPC Clinical Assistant Professor of Medicine NYU School of Medicine NYU Langone Center for Cardiovascular
New Guidelines in Dyslipidemia Management
 The Fourth IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2018 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
The Fourth IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2018 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
Making War on Cholesterol with New Weapons: How Low Can We/Should We Go? Shaun Goodman
 Making War on Cholesterol with New Weapons: How Low Can We/Should We Go? Shaun Goodman Disclosures Research grant support, speaker/consulting honoraria: Sanofi and Regeneron Including ODYSSEY Outcomes
Making War on Cholesterol with New Weapons: How Low Can We/Should We Go? Shaun Goodman Disclosures Research grant support, speaker/consulting honoraria: Sanofi and Regeneron Including ODYSSEY Outcomes
Best Medical Therapy for asymptomatic carotid disease
 Best Medical Therapy for asymptomatic carotid disease Richard Bulbulia Consultant Vascular Surgeon and Co-PI ACST-2 MRC Population Health Research Unit CTSU, Nuffield Department of Population Health University
Best Medical Therapy for asymptomatic carotid disease Richard Bulbulia Consultant Vascular Surgeon and Co-PI ACST-2 MRC Population Health Research Unit CTSU, Nuffield Department of Population Health University
JUPITER NEJM Poll. Panel Discussion: Literature that Should Have an Impact on our Practice: The JUPITER Study
 Panel Discussion: Literature that Should Have an Impact on our Practice: The Study Kaiser COAST 11 th Annual Conference Maui, August 2009 Robert Blumberg, MD, FACC Ralph Brindis, MD, MPH, FACC Primary
Panel Discussion: Literature that Should Have an Impact on our Practice: The Study Kaiser COAST 11 th Annual Conference Maui, August 2009 Robert Blumberg, MD, FACC Ralph Brindis, MD, MPH, FACC Primary
Does High-Intensity Pitavastatin Therapy Further Improve Clinical Outcomes?
 Late Breaking Clinical Trial Session at AHA 2017 Does High-Intensity Pitavastatin Therapy Further Improve Clinical Outcomes? The REAL-CAD Study in 13,054 Patients With Stable Coronary Artery Disease Takeshi
Late Breaking Clinical Trial Session at AHA 2017 Does High-Intensity Pitavastatin Therapy Further Improve Clinical Outcomes? The REAL-CAD Study in 13,054 Patients With Stable Coronary Artery Disease Takeshi
AIM HIGH for SATURN and stay SHARP; COURAGE (v1.5)
") AIM HIGH for SATURN and stay SHARP; COURAGE (v1.5) Jacques Genest MD Cardiovascular Research Laboratory McGill University Health Center Disclosure J. Genest MD 2012 Advisory Board, Speaker s Bureau, Consultant,
AIM HIGH for SATURN and stay SHARP; COURAGE (v1.5) Jacques Genest MD Cardiovascular Research Laboratory McGill University Health Center Disclosure J. Genest MD 2012 Advisory Board, Speaker s Bureau, Consultant,
The Clinical Unmet need in the patient with Diabetes and ACS
 The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
Cardiovascular risk reduction in diabetes Lipids (NICE CG181)
") Cardiovascular risk reduction in diabetes Lipids (NICE CG181) Primary Prevention T1DM Offer Atorvastatin 20mg if >40 years old Diabetes duration >10 years Established nephropathy Other CVS risk factors
Cardiovascular risk reduction in diabetes Lipids (NICE CG181) Primary Prevention T1DM Offer Atorvastatin 20mg if >40 years old Diabetes duration >10 years Established nephropathy Other CVS risk factors
New ACC/AHA Guidelines on Lipids: Are PCSK9 Inhibitors Poised for a Breakthrough?
 New ACC/AHA Guidelines on Lipids: Are PCSK9 Inhibitors Poised for a Breakthrough? Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of North Carolina at Chapel Hill Immediate
New ACC/AHA Guidelines on Lipids: Are PCSK9 Inhibitors Poised for a Breakthrough? Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of North Carolina at Chapel Hill Immediate
FOURIER: Enough Evidence to Justify Widespread Use? Did It fulfill Its Expectations?
 FOURIER: Enough Evidence to Justify Widespread Use? Did It fulfill Its Expectations? CVCT Washington, DC November 3, 2017 Marc S. Sabatine, MD, MPH Chairman, TIMI Study Group Lewis Dexter, MD, Distinguished
FOURIER: Enough Evidence to Justify Widespread Use? Did It fulfill Its Expectations? CVCT Washington, DC November 3, 2017 Marc S. Sabatine, MD, MPH Chairman, TIMI Study Group Lewis Dexter, MD, Distinguished
CVD risk assessment using risk scores in primary and secondary prevention
 CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
Reducing low-density lipoprotein cholesterol treating to target and meeting new European goals
 European Heart Journal Supplements (2004) 6 (Supplement A), A12 A18 Reducing low-density lipoprotein cholesterol treating to target and meeting new European goals University of Sydney, Sydney, NSW, Australia
European Heart Journal Supplements (2004) 6 (Supplement A), A12 A18 Reducing low-density lipoprotein cholesterol treating to target and meeting new European goals University of Sydney, Sydney, NSW, Australia
NICE QIPP about Lipitor. Robert Trotter. Clinical Effectiveness Consultant
 NICE QIPP about Lipitor Robert Trotter Clinical Effectiveness Consultant LIP2894c Date of preparation: April 2009 Prescribing information for atorvastatin is available on the last slide Roadmap Background
NICE QIPP about Lipitor Robert Trotter Clinical Effectiveness Consultant LIP2894c Date of preparation: April 2009 Prescribing information for atorvastatin is available on the last slide Roadmap Background
2013 Cholesterol Guidelines. Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc.
 2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009
 The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009 Learning Objectives 1. Understand the role of statin therapy in the primary and secondary prevention of stroke 2. Explain
The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009 Learning Objectives 1. Understand the role of statin therapy in the primary and secondary prevention of stroke 2. Explain
Safety of Anacetrapib in Patients with or
 Safety of Anacetrapib in Patients with or at Risk for Coronary Heart Disease Christopher P. Cannon, MD, Sukrut Shah, PhD, RPh, Hayes M. Dansky, MD, Michael Davidson, MD, Eliot A. Brinton, MD, Antonio M.
Safety of Anacetrapib in Patients with or at Risk for Coronary Heart Disease Christopher P. Cannon, MD, Sukrut Shah, PhD, RPh, Hayes M. Dansky, MD, Michael Davidson, MD, Eliot A. Brinton, MD, Antonio M.
Management of LDL as a Risk Factor. Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil
 Management of LDL as a Risk Factor Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Consulting for: Merck, Astra Zeneca, ISIS- Genzyme, Novo-Nordisk, BMS, Pfizer,
Management of LDL as a Risk Factor Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Consulting for: Merck, Astra Zeneca, ISIS- Genzyme, Novo-Nordisk, BMS, Pfizer,
Review of guidelines for management of dyslipidemia in diabetic patients
 2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
Goal Achievement after Utilizing an Anti-PCSK9 Antibody in Statin-Intolerant Subjects (GAUSS): Results from a
: Results from a") Goal Achievement after Utilizing an Anti-PCSK9 Antibody in Statin-Intolerant Subjects (GAUSS): Results from a Randomized, d Double-blind, bli Placebo- Controlled Study Evan A. Stein 1, David Sullivan 2,
Goal Achievement after Utilizing an Anti-PCSK9 Antibody in Statin-Intolerant Subjects (GAUSS): Results from a Randomized, d Double-blind, bli Placebo- Controlled Study Evan A. Stein 1, David Sullivan 2,
Effective Treatment Options With Add-on or Combination Therapy. Christie Ballantyne (USA)
") Effective Treatment Options With Add-on or Combination Therapy Christie Ballantyne (USA) Effective treatment options with add-on or combination therapy Christie M. Ballantyne, MD Center for Cardiovascular
Effective Treatment Options With Add-on or Combination Therapy Christie Ballantyne (USA) Effective treatment options with add-on or combination therapy Christie M. Ballantyne, MD Center for Cardiovascular
Reducing CVD globally through combination approaches to prevention: the polypill. Salim Yusuf
 Reducing CVD globally through combination approaches to prevention: the polypill. Salim Yusuf Disclosure None Polypill & CVD Prevention 1. Why do we need a polypill? 2. What components in the polypill?
Reducing CVD globally through combination approaches to prevention: the polypill. Salim Yusuf Disclosure None Polypill & CVD Prevention 1. Why do we need a polypill? 2. What components in the polypill?
Managing Dyslipidemia in Disclosures. Learning Objectives 03/05/2018. Speaker Disclosures
 Managing Dyslipidemia in 2018 Glen J. Pearson, BSc, BScPhm, PharmD, FCSHP, FCCS Professor of Medicine (Cardiology) Co-Director, Cardiac Transplant Clinic; Associate Chair, Health Research Ethics Boards;
Managing Dyslipidemia in 2018 Glen J. Pearson, BSc, BScPhm, PharmD, FCSHP, FCCS Professor of Medicine (Cardiology) Co-Director, Cardiac Transplant Clinic; Associate Chair, Health Research Ethics Boards;
THE ESC/EAS LIPID GUIDELINES IN THE ELDERLY
 THE ESC/EAS LIPID GUIDELINES IN THE ELDERLY Alberico L. Catapano alberico.catapano@unimi.it Alberico L. Catapano Potential Conflict Of Interest Prof. Catapano has received honoraria, lecture fees, or research
THE ESC/EAS LIPID GUIDELINES IN THE ELDERLY Alberico L. Catapano alberico.catapano@unimi.it Alberico L. Catapano Potential Conflict Of Interest Prof. Catapano has received honoraria, lecture fees, or research
Weigh the benefit of statin treatment: LDL & Beyond
 Weigh the benefit of statin treatment: LDL & Beyond Duk-Woo Park, MD, PhD Heart Institute, University of Ulsan College of Medicine, Asan Medical, Seoul, Korea FOURIER Further cardiovascular OUtcomes Research
Weigh the benefit of statin treatment: LDL & Beyond Duk-Woo Park, MD, PhD Heart Institute, University of Ulsan College of Medicine, Asan Medical, Seoul, Korea FOURIER Further cardiovascular OUtcomes Research
New Guidelines in Dyslipidemia Management
 The Third IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2017 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
The Third IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2017 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
2016 ESC/EAS Guideline in Dyslipidemias: Impact on Treatment& Clinical Practice
 2016 ESC/EAS Guideline in Dyslipidemias: Impact on Treatment& Clinical Practice Nattawut Wongpraparut, MD, FACP, FACC, FSCAI Associate Professor of Medicine, Division of Cardiology, Department of Medicine
2016 ESC/EAS Guideline in Dyslipidemias: Impact on Treatment& Clinical Practice Nattawut Wongpraparut, MD, FACP, FACC, FSCAI Associate Professor of Medicine, Division of Cardiology, Department of Medicine
An update on lipidology and cardiovascular risk management. Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine
 An update on lipidology and cardiovascular risk management Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine National and international lipid modification guidelines: A critical appraisal
An update on lipidology and cardiovascular risk management Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine National and international lipid modification guidelines: A critical appraisal
ATP IV: Predicting Guideline Updates
 Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
Prevention of Heart Disease: The New Guidelines
 Prevention of Heart Disease: The New Guidelines Nisha I. Parikh MD MPH Assistant Professor of Medicine Division of Cardiology Department of Medicine University of California San Francisco May 18 th 2015
Prevention of Heart Disease: The New Guidelines Nisha I. Parikh MD MPH Assistant Professor of Medicine Division of Cardiology Department of Medicine University of California San Francisco May 18 th 2015
Dyslipidemia: Lots of Good Evidence, Less Good Interpretation.
 Dyslipidemia: Lots of Good Evidence, Less Good Interpretation. G Michael Allan Evidence & CPD Program, ACFP Associate Professor, Dept of Family, U of A. CFPC CoI Templates: Slide 1 Faculty/Presenter Disclosure
Dyslipidemia: Lots of Good Evidence, Less Good Interpretation. G Michael Allan Evidence & CPD Program, ACFP Associate Professor, Dept of Family, U of A. CFPC CoI Templates: Slide 1 Faculty/Presenter Disclosure
Introduction. Objective. Critical Questions Addressed
 Introduction Objective To provide a strong evidence-based foundation for the treatment of cholesterol for the primary and secondary prevention of ASCVD in women and men Critical Questions Addressed CQ1:
Introduction Objective To provide a strong evidence-based foundation for the treatment of cholesterol for the primary and secondary prevention of ASCVD in women and men Critical Questions Addressed CQ1:
Management of Lipid Disorders and Hypertension: Implications of the New Guidelines
 Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Lipid Management: The Next Level How Will the New ACC/AHA Guidelines Change My Practice
 Lipid Management: The Next Level How Will the New ACC/AHA Guidelines Change My Practice Vera Bittner, MD, MSPH Professor of Medicine Section Head, Preventive Cardiology Medical Director, Cardiac Rehabilitation
Lipid Management: The Next Level How Will the New ACC/AHA Guidelines Change My Practice Vera Bittner, MD, MSPH Professor of Medicine Section Head, Preventive Cardiology Medical Director, Cardiac Rehabilitation
Protecting the heart and kidney: implications from the SHARP trial
 Cardiology Update, Davos, 2013: Satellite Symposium Protecting the heart and kidney: implications from the SHARP trial Colin Baigent Professor of Epidemiology CTSU, University of Oxford S1 First CTT cycle:
Cardiology Update, Davos, 2013: Satellite Symposium Protecting the heart and kidney: implications from the SHARP trial Colin Baigent Professor of Epidemiology CTSU, University of Oxford S1 First CTT cycle:
Dyslipidemia in women: Who should be treated and how?
 Dyslipidemia in women: Who should be treated and how? Lale Tokgozoglu, MD, FACC, FESC Professor of Cardiology Hacettepe University Faculty of Medicine Ankara, Turkey. Cause of Death in Women: European
Dyslipidemia in women: Who should be treated and how? Lale Tokgozoglu, MD, FACC, FESC Professor of Cardiology Hacettepe University Faculty of Medicine Ankara, Turkey. Cause of Death in Women: European
Alirocumab Treatment Effect Did Not Differ Between Patients With and Without Low HDL-C or High Triglyceride Levels in Phase 3 trials
 Alirocumab Treatment Effect Did Not Differ Between Patients With and Without Low HDL-C or High Triglyceride Levels in Phase 3 trials G. Kees Hovingh, 1 Richard Ceska, 2 Michael Louie, 3 Pascal Minini,
Alirocumab Treatment Effect Did Not Differ Between Patients With and Without Low HDL-C or High Triglyceride Levels in Phase 3 trials G. Kees Hovingh, 1 Richard Ceska, 2 Michael Louie, 3 Pascal Minini,
Supplementary appendix
 Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Cholesterol Treatment Trialists (CTT) Collaborators.
Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Cholesterol Treatment Trialists (CTT) Collaborators.
New Lipid Guidelines. PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids.
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
4 th and Goal To Go How Low Should We Go? :
 4 th and Goal To Go How Low Should We Go? : Evaluating New Lipid Lowering Therapies Catherine Bourg Rebitch, PharmD, BCACP Clinical Associate Professor Disclosure The presenter has nothing to disclose
4 th and Goal To Go How Low Should We Go? : Evaluating New Lipid Lowering Therapies Catherine Bourg Rebitch, PharmD, BCACP Clinical Associate Professor Disclosure The presenter has nothing to disclose
Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension
 Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension Prof. Massimo Volpe, MD, FAHA, FESC, Chair of Cardiology, Department of Clinical and Molecular Medicine
Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension Prof. Massimo Volpe, MD, FAHA, FESC, Chair of Cardiology, Department of Clinical and Molecular Medicine
Disclosures. Prevention of Heart Disease: The New Guidelines. Summary of Talk. Four guidelines. No relevant disclosures.
 Disclosures Prevention of Heart Disease: The New Guidelines No relevant disclosures Nisha I. Parikh MD MPH Assistant Professor of Medicine Division of Cardiology Department of Medicine University of California
Disclosures Prevention of Heart Disease: The New Guidelines No relevant disclosures Nisha I. Parikh MD MPH Assistant Professor of Medicine Division of Cardiology Department of Medicine University of California
Evan A. Stein 1, David Sullivan 2, Anders G. Olsson 3, Rob Scott 4, Jae B. Kim 4, Allen Xue 4, Thomas Liu 4, Scott M. Wasserman 4
 Goal Achievement after Utilizing an Anti-PCSK9 Antibody in Statin-Intolerant Subjects (GAUSS): Results from a Randomized, Double-blind, Placebo and Ezetimibe Controlled Study Evan A. Stein 1, David Sullivan
Goal Achievement after Utilizing an Anti-PCSK9 Antibody in Statin-Intolerant Subjects (GAUSS): Results from a Randomized, Double-blind, Placebo and Ezetimibe Controlled Study Evan A. Stein 1, David Sullivan
2/10/2016. Is it Time to Return to Cholesterol Goals for Optimal Patient Management? CON. Disclosures. Stipulations
 Is it Time to Return to Cholesterol Goals for Optimal Patient Management? CON Donald M. Lloyd-Jones MD ScMFACC FAHA Eileen M. FoellProfessor Chair, Dept. of Preventive Medicine Senior Associate Dean Director,
Is it Time to Return to Cholesterol Goals for Optimal Patient Management? CON Donald M. Lloyd-Jones MD ScMFACC FAHA Eileen M. FoellProfessor Chair, Dept. of Preventive Medicine Senior Associate Dean Director,
John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam
 Latest Insights from the JUPITER Study John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam Inflammation, hscrp, and Vascular Prevention
Latest Insights from the JUPITER Study John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam Inflammation, hscrp, and Vascular Prevention
Inhibition of PCSK9: The Birth of a New Therapy
 Inhibition of PCSK9: The Birth of a New Therapy Prof. John J.P. Kastelein, MD PhD FESC Dept. of Vascular Medicine Academic Medical Center / University of Amsterdam The Netherlands Disclosures Dr. Kastelein
Inhibition of PCSK9: The Birth of a New Therapy Prof. John J.P. Kastelein, MD PhD FESC Dept. of Vascular Medicine Academic Medical Center / University of Amsterdam The Netherlands Disclosures Dr. Kastelein
Lipid Panel Management Refresher Course for the Family Physician
 Lipid Panel Management Refresher Course for the Family Physician Objectives Understand the evidence that was evaluated to develop the 2013 ACC/AHA guidelines Discuss the utility and accuracy of the new
Lipid Panel Management Refresher Course for the Family Physician Objectives Understand the evidence that was evaluated to develop the 2013 ACC/AHA guidelines Discuss the utility and accuracy of the new
Hyperlipidemia. Intern Immersion Block 2015
 Hyperlipidemia Intern Immersion Block 2015 Christopher Wong, MD Division of General Internal Medicine University of Washington cjwong@u.washington.edu Welcome! Disclosures: royalties from book sales (not
Hyperlipidemia Intern Immersion Block 2015 Christopher Wong, MD Division of General Internal Medicine University of Washington cjwong@u.washington.edu Welcome! Disclosures: royalties from book sales (not
However, if instead, CHD risk is plotted on a doubling scale (as in slide 2) then there is a
 then there is a") Slides 1 and 2: These two illustrative slides (based on notionaldata) were used in my presentation to Dr Godlee at our meeting on 2 December 2013 to show that, if the risk of coronary disease (CHD) is
Slides 1 and 2: These two illustrative slides (based on notionaldata) were used in my presentation to Dr Godlee at our meeting on 2 December 2013 to show that, if the risk of coronary disease (CHD) is
PCSK9 Inhibitors and Modulators
 PCSK9 Inhibitors and Modulators Pam R. Taub MD, FACC Director of Step Family Cardiac Rehabilitation and Wellness Center Associate Professor of Medicine UC San Diego Health System Disclosures Speaker s
PCSK9 Inhibitors and Modulators Pam R. Taub MD, FACC Director of Step Family Cardiac Rehabilitation and Wellness Center Associate Professor of Medicine UC San Diego Health System Disclosures Speaker s
Should we treat everybody over 60 years with a statin? Comprehensive primary prevention in practice
 Should we treat everybody over 60 years with a statin? Comprehensive primary prevention in practice Pathogenesis of atherosclerosis A decades-long disease course Inflammation Selectins ICAM IL M-CSF CRP
Should we treat everybody over 60 years with a statin? Comprehensive primary prevention in practice Pathogenesis of atherosclerosis A decades-long disease course Inflammation Selectins ICAM IL M-CSF CRP
2013 Cholesterol Guidelines. Anna Broz MSN, RN, CNP, AACC Cer=fied Adult Nurse Prac==oner North Ohio Heart, Inc.
 2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Cer=fied Adult Nurse Prac==oner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Cer=fied Adult Nurse Prac==oner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
Placebo-Controlled Statin Trials
 PREVENTION OF CHD WITH LIPID MANAGEMENT AND ASPIRIN: MATCHING TREATMENT TO RISK Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of
PREVENTION OF CHD WITH LIPID MANAGEMENT AND ASPIRIN: MATCHING TREATMENT TO RISK Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of
Decline in CV-Mortality
 Lipids id 2013 What s Changed? Christopher Granger, MD Disclosure Research contracts: AstraZeneca, GSK, Merck, Sanofi- Aventis, BMS, Pfizer, The Medicines Company, Medtronic Foundation, and Boehringer
Lipids id 2013 What s Changed? Christopher Granger, MD Disclosure Research contracts: AstraZeneca, GSK, Merck, Sanofi- Aventis, BMS, Pfizer, The Medicines Company, Medtronic Foundation, and Boehringer
The TNT Trial Is It Time to Shift Our Goals in Clinical
 The TNT Trial Is It Time to Shift Our Goals in Clinical Angioplasty Summit Luncheon Symposium Korea Assoc Prof David Colquhoun 29 April 2005 University of Queensland, Wesley Hospital, Brisbane, Australia
The TNT Trial Is It Time to Shift Our Goals in Clinical Angioplasty Summit Luncheon Symposium Korea Assoc Prof David Colquhoun 29 April 2005 University of Queensland, Wesley Hospital, Brisbane, Australia
Disclosures No relationships (not even to an employer) No off-label uses. Cholesterol Lowering Guidelines: What now?
 No off-label uses. Cholesterol Lowering Guidelines: What now?") Disclosures No relationships (not even to an employer) No off-label uses Cholesterol Lowering Guidelines: What now?, FACP 1 2 65-year-old white woman Total cholesterol 175mg/dL HDL 54 mg/dl LDL 96 mg/dl
Disclosures No relationships (not even to an employer) No off-label uses Cholesterol Lowering Guidelines: What now?, FACP 1 2 65-year-old white woman Total cholesterol 175mg/dL HDL 54 mg/dl LDL 96 mg/dl
Should we prescribe aspirin and statins to all subjects over 65? (Or even all over 55?) Terje R.Pedersen Oslo University Hospital Oslo, Norway
 Terje R.Pedersen Oslo University Hospital Oslo, Norway") Should we prescribe aspirin and statins to all subjects over 65? (Or even all over 55?) Terje R.Pedersen Oslo University Hospital Oslo, Norway The Polypill A strategy to reduce cardiovascular disease by
Should we prescribe aspirin and statins to all subjects over 65? (Or even all over 55?) Terje R.Pedersen Oslo University Hospital Oslo, Norway The Polypill A strategy to reduce cardiovascular disease by
Case Presentation. Rafael Bitzur The Bert W Strassburger Lipid Center Sheba Medical Center Tel Hashomer
 Case Presentation Rafael Bitzur The Bert W Strassburger Lipid Center Sheba Medical Center Tel Hashomer Case Presentation 50 YO man NSTEMI treated with PCI 1 month ago Medical History: Obesity: BMI 32,
Case Presentation Rafael Bitzur The Bert W Strassburger Lipid Center Sheba Medical Center Tel Hashomer Case Presentation 50 YO man NSTEMI treated with PCI 1 month ago Medical History: Obesity: BMI 32,
Statins and PCSK9 inhibitors for stroke prevention
 Statins and PCSK9 inhibitors for stroke prevention Haralampos Milionis Professor of Internal Medicine School of Medicine, University of Ioannina Ioannina, Greece Reduction in CV events (%) Every 1 mmol/l
Statins and PCSK9 inhibitors for stroke prevention Haralampos Milionis Professor of Internal Medicine School of Medicine, University of Ioannina Ioannina, Greece Reduction in CV events (%) Every 1 mmol/l
Is there a mechanism of interaction between hypertension and dyslipidaemia?
 Is there a mechanism of interaction between hypertension and dyslipidaemia? Neil R Poulter International Centre for Circulatory Health NHLI, Imperial College London Daegu, Korea April 2005 Observational
Is there a mechanism of interaction between hypertension and dyslipidaemia? Neil R Poulter International Centre for Circulatory Health NHLI, Imperial College London Daegu, Korea April 2005 Observational
Considerations and Controversies in the Management of Dyslipidemia for ASCVD Risk Reduction
 Considerations and Controversies in the Management of Dyslipidemia for ASCVD Risk Reduction Pamela B. Morris, MD, FACC, FAHA, FASCP, FNLA Chair, ACC Prevention of Cardiovascular Disease Council The Medical
Considerations and Controversies in the Management of Dyslipidemia for ASCVD Risk Reduction Pamela B. Morris, MD, FACC, FAHA, FASCP, FNLA Chair, ACC Prevention of Cardiovascular Disease Council The Medical
Nicole Ciffone, MS, ANP-C, AACC Clinical Lipid Specialist
 1 Nicole Ciffone, MS, ANP-C, AACC Clinical Lipid Specialist New Cardiovascular Horizons Multidisciplinary Strategies for Optimal Cardiovascular Care February 7, 2015 2 Objectives After participating in
1 Nicole Ciffone, MS, ANP-C, AACC Clinical Lipid Specialist New Cardiovascular Horizons Multidisciplinary Strategies for Optimal Cardiovascular Care February 7, 2015 2 Objectives After participating in
Cholesteryl ester transfer protein inhibitors - what have we learnt? Philip Barter The Heart Research Institute Sydney, Australia
 Cholesteryl ester transfer protein inhibitors - what have we learnt? Philip Barter The Heart Research Institute Sydney, Australia Philip Barter Disclosures Received honorariums for lectures, consultancies
Cholesteryl ester transfer protein inhibitors - what have we learnt? Philip Barter The Heart Research Institute Sydney, Australia Philip Barter Disclosures Received honorariums for lectures, consultancies
Guidelines on cardiovascular risk assessment and management
 European Heart Journal Supplements (2005) 7 (Supplement L), L5 L10 doi:10.1093/eurheartj/sui079 Guidelines on cardiovascular risk assessment and management David A. Wood 1,2 * 1 Cardiovascular Medicine
European Heart Journal Supplements (2005) 7 (Supplement L), L5 L10 doi:10.1093/eurheartj/sui079 Guidelines on cardiovascular risk assessment and management David A. Wood 1,2 * 1 Cardiovascular Medicine
Hypertension. Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute
 Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
No relevant financial relationships
 MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
Accumulating Clinical data on PCSK9 Inhibition: Key Lessons and Challenges
 ESC 2015 London Accumulating Clinical data on PCSK9 Inhibition: Key Lessons and Challenges Paul M Ridker, MD, MPH Eugene Braunwald Professor of Medicine Harvard Medical School Director, Center for Cardiovascular
ESC 2015 London Accumulating Clinical data on PCSK9 Inhibition: Key Lessons and Challenges Paul M Ridker, MD, MPH Eugene Braunwald Professor of Medicine Harvard Medical School Director, Center for Cardiovascular
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
STATIN THERAPY IN THE ELDERLY: THERE ARE MILES TO GO BEFORE WE SLEEP
 STATIN THERAPY IN THE ELDERLY: THERE ARE MILES TO GO BEFORE WE SLEEP Peter P. Toth, MD, PhD, FAAFP, FICA, FNLA, FCCP, FAHA, FACC Director of Preventative Cardiology CGH Medical Center, Sterling, Illinois
STATIN THERAPY IN THE ELDERLY: THERE ARE MILES TO GO BEFORE WE SLEEP Peter P. Toth, MD, PhD, FAAFP, FICA, FNLA, FCCP, FAHA, FACC Director of Preventative Cardiology CGH Medical Center, Sterling, Illinois
Clinical Efficacy and Safety of Achieving Very Low LDL-C Levels With the PCSK9 Inhibitor Evolocumab in the FOURIER Outcomes Trial
 Clinical Efficacy and Safety of Achieving Very Low LDL-C Levels With the PCSK9 Inhibitor Evolocumab in the FOURIER Outcomes Trial RP Giugliano, TR Pedersen, AC Keech, PS Sever, JG Park, and MS Sabatine,
Clinical Efficacy and Safety of Achieving Very Low LDL-C Levels With the PCSK9 Inhibitor Evolocumab in the FOURIER Outcomes Trial RP Giugliano, TR Pedersen, AC Keech, PS Sever, JG Park, and MS Sabatine,
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
Zürcher Herzkurs, New drugs and interactions. LDL - what else?
 Zürcher Herzkurs, 29.09.2017 New drugs and interactions LDL - what else? Heinz Drexel, MD, FESC, FAHA, FRCP (Ed.) VIVIT Institut am Akademischen Lehrkrankenhaus Feldkirch, A Private Universität im Fürstentum
Zürcher Herzkurs, 29.09.2017 New drugs and interactions LDL - what else? Heinz Drexel, MD, FESC, FAHA, FRCP (Ed.) VIVIT Institut am Akademischen Lehrkrankenhaus Feldkirch, A Private Universität im Fürstentum
2014/10/20. Management of Lipid Disorders Eric Klug Sunninghill, Sunward Park and CM JHB Academic Hospitals
 Management of Lipid Disorders Eric Klug Sunninghill, Sunward Park and CM JHB Academic Hospitals Sudden and unexpected deaths in an adult population, Cape Town, South Africa, 2001-2005 1 Sudden and unexpected
Management of Lipid Disorders Eric Klug Sunninghill, Sunward Park and CM JHB Academic Hospitals Sudden and unexpected deaths in an adult population, Cape Town, South Africa, 2001-2005 1 Sudden and unexpected
Use of Subgroups to Rescue a Trial or Improve Benefit-Risk
 1 Use of Subgroups to Rescue a Trial or Improve Benefit-Risk Martin King, Ph.D. Director, Statistics Global Pharmaceutical R&D, Abbott Abbott Park, IL USA 2 Disclaimer The opinions in this presentation
1 Use of Subgroups to Rescue a Trial or Improve Benefit-Risk Martin King, Ph.D. Director, Statistics Global Pharmaceutical R&D, Abbott Abbott Park, IL USA 2 Disclaimer The opinions in this presentation
Update on Current Trends in Hypertension Management
 Friday General Session Update on Current Trends in Hypertension Management Shawna Nesbitt, MD Associate Dean, Minority Student Affairs Associate Professor, Department of Internal Medicine Office of Student
Friday General Session Update on Current Trends in Hypertension Management Shawna Nesbitt, MD Associate Dean, Minority Student Affairs Associate Professor, Department of Internal Medicine Office of Student
Welcome! Mark May 14, Sat!
 Welcome! Mark May 14, Sat! Do We Have All Answers with Statins In Treating Patients with Hyperlipidemia? Kwang Kon Koh, MD, PhD, FACC, FAHA Cardiology, Gil Heart Center, Gachon Medical School, Incheon,
Welcome! Mark May 14, Sat! Do We Have All Answers with Statins In Treating Patients with Hyperlipidemia? Kwang Kon Koh, MD, PhD, FACC, FAHA Cardiology, Gil Heart Center, Gachon Medical School, Incheon,
Nephrologisches Zentrum Göttingen GbR Priv. Doz. Dr. med. V. Schettler
 Therapeutic algorithm for Patients with severe Hypercholesterolemia or isolated Lipoprotein(a)-Hyperlipoproteinemia with progressive cardiovascular disease: PCSK9- Inhibitors, Lipoprotein Apheresis or
Therapeutic algorithm for Patients with severe Hypercholesterolemia or isolated Lipoprotein(a)-Hyperlipoproteinemia with progressive cardiovascular disease: PCSK9- Inhibitors, Lipoprotein Apheresis or
Drug Class Monograph
 Drug Class Monograph Class: Proprotein Convertase Subtilisin/Kexin Type 9 (PCSK9) Inhibitor Drugs: Praluent (alirocumab), Repatha (evolocumab) Line of Business: Medi-Cal Effective Date: February 17, 2016
Drug Class Monograph Class: Proprotein Convertase Subtilisin/Kexin Type 9 (PCSK9) Inhibitor Drugs: Praluent (alirocumab), Repatha (evolocumab) Line of Business: Medi-Cal Effective Date: February 17, 2016
Cardiovascular Controversies: Emerging Therapies for Lowering Cardiovascular Risk
 Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Placebo-Controlled Statin Trials MANAGEMENT OF HIGH BLOOD CHOLESTEROL MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
Long-Term Complications of Diabetes Mellitus Macrovascular Complication
 Long-Term Complications of Diabetes Mellitus Macrovascular Complication Sung Hee Choi MD, PhD Professor, Seoul National University College of Medicine, SNUBH, Bundang Hospital Diabetes = CVD equivalent
Long-Term Complications of Diabetes Mellitus Macrovascular Complication Sung Hee Choi MD, PhD Professor, Seoul National University College of Medicine, SNUBH, Bundang Hospital Diabetes = CVD equivalent
PCSK9 Agents Drug Class Prior Authorization Protocol
 PCSK9 Agents Drug Class Prior Authorization Protocol Line of Business: Medicaid P & T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review of medical
PCSK9 Agents Drug Class Prior Authorization Protocol Line of Business: Medicaid P & T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review of medical
Environmental. Vascular / Tissue. Metabolics
 Global Risk Reduction--WINS Picking Mom and Dad-2016 Environmental Vascular / Tissue Metabolics Stop smoking-1b Physical activity-1b Weight control-1b Chelation therapy-3c Influenza vaccination-1b Blood
Global Risk Reduction--WINS Picking Mom and Dad-2016 Environmental Vascular / Tissue Metabolics Stop smoking-1b Physical activity-1b Weight control-1b Chelation therapy-3c Influenza vaccination-1b Blood
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
Does IMPROVE-IT & FOURIER Confirm or Refute the LDL Hypothesis?
 Does IMPROVE-IT & FOURIER Confirm or Refute the LDL Hypothesis? Controversies and Advances in the Treatment of Cardiovascular Disease The Seventeenth in the Series Beverly Hills, November 16, 2017 Sanjay
Does IMPROVE-IT & FOURIER Confirm or Refute the LDL Hypothesis? Controversies and Advances in the Treatment of Cardiovascular Disease The Seventeenth in the Series Beverly Hills, November 16, 2017 Sanjay
2/10/2016. Perspectives on the 2013 ACC/AHA Cholesterol Guidelines. Disclosures. ATP-III Update 2004
 Perspectives on the 2013 ACC/AHA Cholesterol Guidelines Donald M. Lloyd-Jones, MD ScM Senior Associate Dean Chair and Professor of Preventive Medicine Northwestern Feinberg School of Medicine Disclosures
Perspectives on the 2013 ACC/AHA Cholesterol Guidelines Donald M. Lloyd-Jones, MD ScM Senior Associate Dean Chair and Professor of Preventive Medicine Northwestern Feinberg School of Medicine Disclosures
How would you manage Ms. Gold
 How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
Lifetime clinical and economic benefits of statin-based LDL lowering in the 20-year Followup of the West of Scotland Coronary Prevention Study
 Lifetime clinical and economic benefits of statin-based LDL lowering in the 20-year Followup of the West of Scotland Coronary Prevention Study Harvey White Green Lane Cardiovascular Service and Cardiovascular
Lifetime clinical and economic benefits of statin-based LDL lowering in the 20-year Followup of the West of Scotland Coronary Prevention Study Harvey White Green Lane Cardiovascular Service and Cardiovascular