Evaluation and Treatment of Dementia
|
|
|
- Winfred Charles
- 5 years ago
- Views:
Transcription
1 Evaluation and Treatment of Dementia Jeffrey M. Burns, MD Edward H. Hashinger Professor of Neurology Co-Director, KU Alzheimer s Disease Center Director, Clinical and Translational Science Unit Disclosures Funding support: NIH, Avid Pharmaceuticals/Lilly Clinical trials with Lilly, Merck, Toyama
2 Memory Clinic Visit 1. History (family) 2. Physical exam 3. Cognitive testing AD8 MOCA Plan Differential Diagnosis Further testing Brain scan Lab tests Other testing: neuropsychology, Treatment plan: medications, lifestyle recommendations
3 The best diagnostic test is a careful history and physical and mental status examination by a physician with a knowledge of and interest in dementia and the dementing diseases. Such an evaluation is time consuming, but nothing can replace it. Differential diagnosis of dementing diseases. NIH Consensus Statement. JAMA 1987; 258:
4 How do we diagnose Alzheimer s? No brain scan or blood test can make the diagnosis. Detailed History Characteristics and pattern of changes Importance of informant / caregiver Physical Examination
5 How do we diagnose Alzheimer s? Rule out other potential causes Blood tests Thyroid hormone Vitamin B12 MRI or CT of the brain Stroke, tumor, other structural problems Depression Medications
6 Clues to Differential Diagnosis Alzheimer s Disease Visual hallucinations + Parkinsonism Vascular dementia Lewy body dementia Frontotemporal dementias
7 Alzheimer s Disease Most common cause of dementia (50 70%) Marked by early memory impairment, executive dysfunction Alzheimer s Facts 5.3 million Americans have AD in 2017 One in ten (10 percent) over 65 have AD Every 66 seconds someone develops AD $259 billion in direct and indirect costs to Medicare, Medicaid, and businesses.


8 Auguste D. Dr. Alois Alzheimer

9
10 What is Dementia? 1. Decline in cognition Memory Executive Function: Planning / Organization Language Orientation 2. Interferes with everyday function
11 Clinical Hallmarks of Dementia Gradual onset Progressive decline Memory loss Other cognitive domains impaired Interferes with function
12 Causes of Dementia Other Vascular Dementia 10% Frontotemporal Dementia: 5% Alzheimer s Disease 50-70% Dementia With Lewy Bodies: 15%

13 Definite Alzheimer s Disease Dementia Syndrome + Plaques and Tangles
14 Probable Alzheimer s Disease Clinical Criteria (1984) 1. Decline in cognition insidious and progressive Memory Executive Function: Planning / Organization Language Orientation Visual and visuospatial 2. Interferes with everyday function 3. Not related to other possible causes (delirium, depression, tumor, etc)
15 Memory Clinic Visit 1. History (family) 2. Physical exam 3. Cognitive testing (15 minutes) MMSE, Logical Memory I and II, Clock drawing, Verbal Fluency, Trailmaking A and B Plan Differential Diagnosis Further testing Brain scan Lab tests Other testing: neuropsychology, Treatment plan: medications, lifestyle recommendations
16 Dementia Detection Informant Trust reliable informant report of memory problem Dementia suggested by: Decline from past level of performance (key feature) Consistency of deficits Interference with usual activities (key feature) Patient Self-reported complaints do not reliably predict dementia Impaired memory performance is key feature
17 Importance of Early Recognition Treatment Evaluate Potential reversible or contributing conditions Family Validates concerns, explains nature of problems Access to services Plan for future Reduce risks, proactive approach to transitions
18 Keys to Early Detection Assumptions ADL impairment Keys Cognitive function is stable with age Decline in performance / less well than before Mistakes / Misconceptions Memory decline is inevitable with age Complete loss of function / relinquish activities History Informant-based Self-report
19 Common Symptoms Memory Loss Forgetfulness (conversations; appointments; medicines; names) Repetition of questions, statements Misplacing items Executive Dysfunction Managing household finances Driving Meal preparation Operating appliances
20 Questions to Ask: Early Recognition Forgetting details of recent events Need help in keeping the calendar? Navigating in unfamiliar places Judgment and problem solving as good as ever? Or, still good but not as good as before? Billpaying / checkbook Cooking / following recipes Fixing stuff around the house
21 Memory Clinic Visit 1. History (family) 2. Physical exam 3. Cognitive testing (15 minutes) MMSE, Logical Memory I and II, Clock drawing, Verbal Fluency, Trailmaking A and B Plan Differential Diagnosis Further testing Brain scan Lab tests Other testing: neuropsychology, Treatment plan: medications, lifestyle recommendations
22 Causes of Dementia Other Vascular Dementia 10% Frontotemporal Dementia: 5% Alzheimer s Disease 50-70% Dementia With Lewy Bodies: 15%
23 Clues to Differential Diagnosis Alzheimer s Disease Visual hallucinations + Parkinsonism Vascular dementia Lewy body dementia Frontotemporal dementias
24 Key Features of Dementing Disorders Key Features Alzheimer s Disease Dementia with Lewy Bodies Frontotemporal Dementia Vascular Dementia Cognition (memory, organization) Motor and Cognition (Parkinsonism, visual hallucinations) Personality, Early Onset (social behavior, language) Vascular (Strokes, MRI vascular changes)
25 Memory Clinic Visit 1. History (family) 2. Physical exam 3. Cognitive testing (15 minutes) MMSE, Logical Memory I and II, Clock drawing, Verbal Fluency, Trailmaking A and B Plan Differential Diagnosis Further testing Brain scan Lab tests Other testing: neuropsychology, Treatment plan: medications, lifestyle recommendations
26 AD-8 Brief informant interview 8 questions Several minutes Good to excellent discrimination of nondemented and early AD. AD-8 Questionnaire Has there been a change in the last several years? Problems with Judgment Reduced interest in hobbies/activities Repeats questions, stories, statements Trouble learning how to use a tool, appliance, or gadget Forgets correct month or year Difficulty handling complicated financial affairs Difficulty remembering appointments Consistent problems with thinking and memory
27 MOCA Widely used 0 30 pts 10 minutes More sensitive but less specific 26 and above is normal
28 Clock Drawing Test Useful in detecting mild dementia Insensitive in detecting the earliest clinical stages of AD.

 Follow-up Time 11 years 12 years 14 years")
29 Follow-up Time 15 years Nondemented (CDR 0) Follow-up Time 0 3 years Very Mild Dementia (CDR 0.5) Follow-up Time 7 years 8 years 10 years 11 years Mild Dementia (CDR 1) Follow-up Time 11 years 12 years 14 years Moderate Dementia (CDR 2)
30 Memory Clinic Visit 1. History (family) 2. Physical exam 3. Cognitive testing (15 minutes) MMSE, Logical Memory I and II, Clock drawing, Verbal Fluency, Trailmaking A and B Plan Differential Diagnosis Further testing Brain scan Lab tests Other testing: neuropsychology, Treatment plan: medications, lifestyle recommendations
31 Differential Diagnosis Low thyroid or B12 Medications Depression Sleep Apnea Medical issues Neurodegenerative dementias
32 Memory Clinic Visit 1. History (family) 2. Physical exam 3. Cognitive testing (15 minutes) MMSE, Logical Memory I and II, Clock drawing, Verbal Fluency, Trailmaking A and B Plan Differential Diagnosis Further testing Brain scan Lab tests Other testing: neuropsychology Treatment plan: medications, lifestyle recommendations
33 Recommended Labs: Clinical Tests TSH, Vitamin B12 Electrolytes, CBC, LFTs Imaging: MRI or CT Optional Neuropsychological testing Sleep apnea testing VERY optional PET Amyloid PET
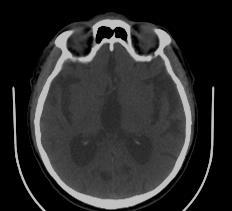
34 What do we learn from Rule things out imaging? Atrophy patterns


35
36 64 year old man with 4 years of behavioral and cognitive decline Onset of behavioral changes at age 60 Withdrew from friends, uninterested Drinking wine on a daily basis Increased interest in sex, inappropriate behavior (slapped her friends on the rear) Apathetic: lounged around in his chair all day Hygiene declined, not shaving or bathing. Language changes: loss of spontaneous speech, only short, simple answers.





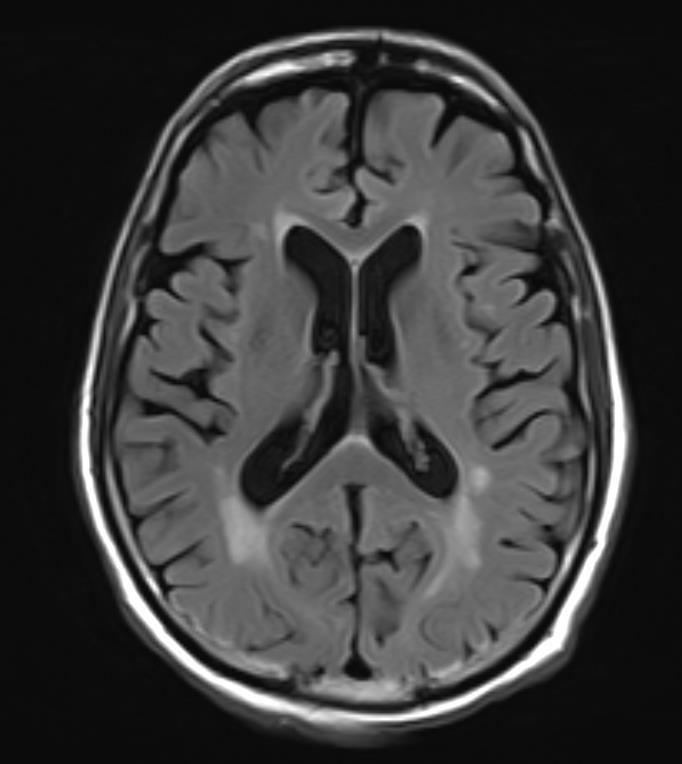
37 Anterior Temporal and Frontal Atrophy
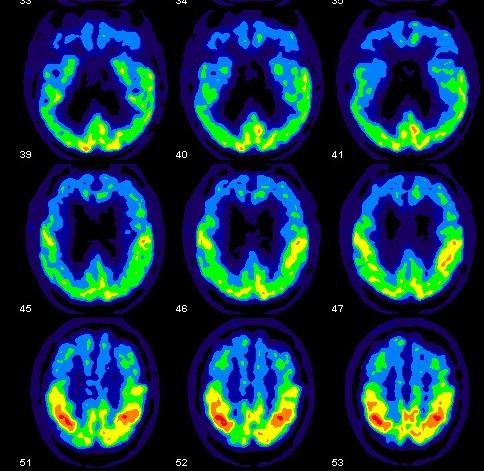

38 Frontal Hypometabolism on PET Axial Sagittal
39 When to Get Further Neuropsychological Testing Corroborates clinical impression Atypical dementia Localize cognitive impairment Mild Cognitive Impairment Value in longitudinal studies
40 Memory Clinic Visit 1. History (family) 2. Physical exam 3. Cognitive testing (15 minutes) MMSE, Logical Memory I and II, Clock drawing, Verbal Fluency, Trailmaking A and B Plan Differential Diagnosis Further testing Brain scan Lab tests Other testing: neuropsychology Treatment plan: medications, lifestyle recommendations
41 Current AD Pharmacologic Therapy Two classes of approved medications Cholinesterase inhibitors increase acetylcholine levels Aricept (donepezil) Exelon (rivastigmine) Razadyne (galantamine) NMDA antagonist Namenda (memantine)
42 Cognitive Abilities Time Effect of Medications on AD Course Initiate Medications Donepezil Galantamine Rivastigmine Cholinesterase inhibitors Namenda
43 Management of Non-Cognitive Symptoms Cholinesterase inhibitors and memantine Depression SSRI antidepressants Agitation atypical neuroleptics anticonvulsants buspirone, trazodone Hallucinations atypical neuroleptics Sleep trazodone, melatonin, neuroleptics
44 Safety Other Recommendations Driving Falls Lifestyle Stay active mentally and physically What s good for the heart is good for the brain Mediterranean Diet Pattern
45 Where are we going? Detect AD changes early or even before the onset of symptoms Halt or reverse the disease process
46 Revised AD Criteria McKhann et al, 2011 Key criteria remain unchanged Identify intra-individual decline in cognition and function as salient clinical features Consider AD biomarkers to enhance confidence in clinical diagnosis
47 80 yo with 2 years of progressive Forgetfulness cognitive decline Geographically challenged Broad but mild cognitive deficits in global cognition, memory, and executive function MMSE 23; LMI 5, LMII 2, Trails 220, Free recall 7,5,2 Enrolled in clinical trial for AD

48 MRI


49 New Age of Molecular Imaging: Plaque and Tangle Imaging Clark, C. M. et al. JAMA 2011;305: Plaques and Tangles


50 Diffuse Amyloid Accumulation

51 Severe Tau Pathology in Limbic and Neocortical Association Areas


52
53 Potential Value of Biomarkers Accurate and early diagnosis Risk assessment Drug Development Measure of disease progression Surrogate endpoints Shorter trials, smaller sample size Enriched samples Identification of preclinical AD
54 Financial Advisor with Cognitive Concerns 70 yo man with complaints of dropping details for the last 5 years FH of dementia in his mother Working as a successful branch manager for investment firm. Wife notes no memory decline, he s never remembered trivial stuff, he does too much Frequent visits to library, avid reader, attends lectures, investment club, involved in local politics
55 Cognitive Testing MMSE 30 out of 30 Logical memory I 20 (norm 14) Logical memory II 22 (norm 13) Trailmaking B 42 (norm 79) SRT recall 13/13/12 (norm 9/10/11)
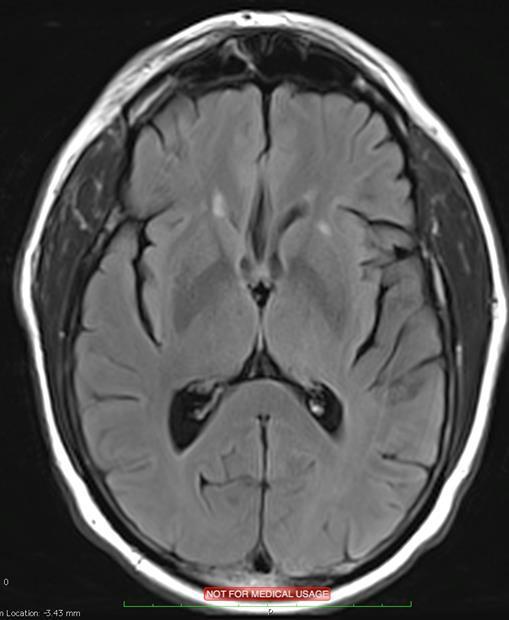

56 MRI


57 Amyloid PET
58 Relevance of Asymptomatic Amyloid 30% of healthy adults have brain amyloid Not a diagnosis of AD Not all develop AD Risk factor for developing AD Magnitude and timing of risk not yet well-defined Likely plays out over 10+ years
59 New Era of Prevention Trials Identifying Alzheimer s changes prior to onset of symptoms may be possible Window of opportunity Foundation for AD prevention trials Exercise Alzheimer s Prevention Through Exercise (APEX) Anti-amyloid strategies Anti-amyloid Treatment in Asymptomatic AD Solanezumab
60 Are We Ready for Presymptomatic Scanning? Not currently justified clinically Clinical significance not well defined May have psychological and behavioral impact Effective interventions not available Research setting Increasingly common for identifying individuals for prevention trials Careful disclosure process: education and monitoring Grill, Johnson, Burns. Neurodegen Dis Manage 2013
61 Biomarker Conclusions Biomarkers are increasingly incorporated into diagnostic algorithms to increase confidence in diagnosis. Field of biomarkers is rapidly evolving in response to Science / clinical studies Reimbursement Treatment options Standardization
62 Why Participate in Research? Help develop new treatment for future generations Regular monitoring Learn about Alzheimer s Improve access to services, support groups, resources
63 KU Alzheimer s Disease Center Mission To improve the lives of patients and families with Alzheimer s disease by eliminating the disease through research into its treatment and prevention
64 KU AD Center Clinical Services: Alzheimer and Memory Clinic 3 physicians, 2 nurse practitioners Research Program 88 members with $13 million annually in federal grants Innovative Programs and Projects Clinical Trials Unit Prestigious national trials and drug development efforts Alzheimer Treatment Program Alzheimer s Prevention Program
65 Anti-Amyloid Treatment Trials: KU ADC Clinical Trial Unit Solanezumab (Eli Lilly) Verubecestat (Merck) Aducanumab (Biogen) Azeliragon (vtv) Neuroprotection TCAD study (Toyama) Bryostatin (Neurotrope) Metabolic Studies (KU led) Metabolic approaches (Diet, Exercise, OAA, S-equol)
66 Prevention is our biggest hope Identify brain changes before symptoms Stop the disease process Drugs anti-amyloid therapies Anti-amyloid for Asymptomatic Amyloidosis (A4) Trial Lifestyle interventions Alzheimer s Prevention thru Exercise (APEX) Trial
67 Accessing Research Opportunities KU Alzheimer s Disease Center Matching services TrialMatch ( ResearchMatch Pioneers ( Alzheimer s Disease Centers ClinicalTrial.gov
Alzheimer s Disease Update: From Treatment to Prevention
 Alzheimer s Disease Update: From Treatment to Prevention Jeffrey M. Burns, MD Edward H. Hashinger Professor of Medicine Co-Director, KU Alzheimer s Disease Center Director, Clinical and Translational Science
Alzheimer s Disease Update: From Treatment to Prevention Jeffrey M. Burns, MD Edward H. Hashinger Professor of Medicine Co-Director, KU Alzheimer s Disease Center Director, Clinical and Translational Science
Dementia is not normal aging!
 The Future of Alzheimer s Disease Treatment Adam L. Boxer, MD, PhD Director, Alzheimer s Disease Clinical Trials Program Memory and Aging Center Assistant Professor of Neurology University of California,
The Future of Alzheimer s Disease Treatment Adam L. Boxer, MD, PhD Director, Alzheimer s Disease Clinical Trials Program Memory and Aging Center Assistant Professor of Neurology University of California,
Understanding Dementia
 Understanding Dementia Dr. Dallas Seitz MD FRCPC Assistant Professor, Department of Psychiatry, Queen s University, Kingston, Ontario, Canada What s Next Information about Dementia, Elder Care and Supports
Understanding Dementia Dr. Dallas Seitz MD FRCPC Assistant Professor, Department of Psychiatry, Queen s University, Kingston, Ontario, Canada What s Next Information about Dementia, Elder Care and Supports
Diagnosis and Treatment of Alzhiemer s Disease
 Diagnosis and Treatment of Alzhiemer s Disease Roy Yaari, MD, MAS Director, Memory Disorders Clinic, Banner Alzheimer s Institute 602-839-6900 Outline Introduction Alzheimer s disease (AD)Guidelines -revised
Diagnosis and Treatment of Alzhiemer s Disease Roy Yaari, MD, MAS Director, Memory Disorders Clinic, Banner Alzheimer s Institute 602-839-6900 Outline Introduction Alzheimer s disease (AD)Guidelines -revised
The ABCs of Dementia Diagnosis
 The ABCs of Dementia Diagnosis Dr. Robin Heinrichs, Ph.D., ABPP Board Certified Clinical Neuropsychologist Associate Professor, Psychiatry & Behavioral Sciences Director of Neuropsychology Training What
The ABCs of Dementia Diagnosis Dr. Robin Heinrichs, Ph.D., ABPP Board Certified Clinical Neuropsychologist Associate Professor, Psychiatry & Behavioral Sciences Director of Neuropsychology Training What
Memory Loss, Dementia and Alzheimer's Disease: The Basics
 Memory Loss, Dementia and Alzheimer's Disease: The Basics What is memory loss? What is age-related memory loss? Typical changes Typical age-related changes involve: Making a bad decision once in a while
Memory Loss, Dementia and Alzheimer's Disease: The Basics What is memory loss? What is age-related memory loss? Typical changes Typical age-related changes involve: Making a bad decision once in a while
WHAT IS DEMENTIA? An acquired syndrome of decline in memory and other cognitive functions sufficient to affect daily life in an alert patient
 DEMENTIA WHAT IS DEMENTIA? An acquired syndrome of decline in memory and other cognitive functions sufficient to affect daily life in an alert patient Progressive and disabling Not an inherent aspect of
DEMENTIA WHAT IS DEMENTIA? An acquired syndrome of decline in memory and other cognitive functions sufficient to affect daily life in an alert patient Progressive and disabling Not an inherent aspect of
Overview. Case #1 4/20/2012. Neuropsychological assessment of older adults: what, when and why?
 Neuropsychological assessment of older adults: what, when and why? Benjamin Mast, Ph.D. Associate Professor & Vice Chair, Psychological & Brain Sciences Associate Clinical Professor, Family & Geriatric
Neuropsychological assessment of older adults: what, when and why? Benjamin Mast, Ph.D. Associate Professor & Vice Chair, Psychological & Brain Sciences Associate Clinical Professor, Family & Geriatric
Assessing and Managing the Patient with Cognitive Decline
 Assessing and Managing the Patient with Cognitive Decline Center of Excellence For Alzheimer s Disease for State of NY Capital Region Alzheimer s Center of Albany Medical Center Earl A. Zimmerman, MD Professor
Assessing and Managing the Patient with Cognitive Decline Center of Excellence For Alzheimer s Disease for State of NY Capital Region Alzheimer s Center of Albany Medical Center Earl A. Zimmerman, MD Professor
Dementia Basics. Welcome! What to expect and how to handle a dementia diagnosis. In partnership with Scripps Health.
 Dementia Basics What to expect and how to handle a dementia diagnosis March 18, 2017 In partnership with Scripps Health Welcome! 1 Welcome Kristin Gaspar San Diego County Supervisor District 3 2 Our Mission:
Dementia Basics What to expect and how to handle a dementia diagnosis March 18, 2017 In partnership with Scripps Health Welcome! 1 Welcome Kristin Gaspar San Diego County Supervisor District 3 2 Our Mission:
Dementia. Aetiology, pathophysiology and the role of neuropsychological testing. Dr Sheng Ling Low Geriatrician
 Dementia Aetiology, pathophysiology and the role of neuropsychological testing Dr Sheng Ling Low Geriatrician Topics to cover Why is dementia important What is dementia Differentiate between dementia,
Dementia Aetiology, pathophysiology and the role of neuropsychological testing Dr Sheng Ling Low Geriatrician Topics to cover Why is dementia important What is dementia Differentiate between dementia,
Alzheimer s disease dementia: a neuropsychological approach
 Alzheimer s disease dementia: a neuropsychological approach Dr. Roberta Biundo, PhD Neuropsychology Coordinator at Parkinson s disease and movement disorders unit of San Camillo rehabilitation hospital
Alzheimer s disease dementia: a neuropsychological approach Dr. Roberta Biundo, PhD Neuropsychology Coordinator at Parkinson s disease and movement disorders unit of San Camillo rehabilitation hospital
The Basics of Alzheimer s Disease
 2017 Memory Loss Conference The Basics of Alzheimer s Disease Tom Ala, MD Center for Alzheimer s Disease and Related Disorders Southern Illinois University School of Medicine Springfield, Illinois SIU
2017 Memory Loss Conference The Basics of Alzheimer s Disease Tom Ala, MD Center for Alzheimer s Disease and Related Disorders Southern Illinois University School of Medicine Springfield, Illinois SIU
4/11/2017. The impact of Alzheimer s disease. Typical changes. The impact of Alzheimer s disease. Problematic changes. Problematic changes
 The impact of Alzheimer s disease Ron Petersen, MD, PhD, is Director of the Mayo Alzheimer's Disease Research Center. 2 The impact of Alzheimer s disease Typical changes Typical age-related changes involve:
The impact of Alzheimer s disease Ron Petersen, MD, PhD, is Director of the Mayo Alzheimer's Disease Research Center. 2 The impact of Alzheimer s disease Typical changes Typical age-related changes involve:
Understanding Symptoms, Causes, and Risks for Alzheimer s Disease
 Understanding Symptoms, Causes, and Risks for Alzheimer s Disease Gene E. Alexander, Ph.D., Professor of Psychology, Neuroscience, and Physiological Sciences; Director, Brain Imaging, Behavior & Aging
Understanding Symptoms, Causes, and Risks for Alzheimer s Disease Gene E. Alexander, Ph.D., Professor of Psychology, Neuroscience, and Physiological Sciences; Director, Brain Imaging, Behavior & Aging
Memory Matters: Learning Objectives: Synapses, Age, and Health. Neuronal Synapses DISCLOSURE DECLARATION. Cognition and Normal Aging
 Standard Deviations from Mean Memory Matters: Preventing and Treating Late-Life, Cognitive Decline Daniel L. Murman, MD, MS Director, Behavioral and Geriatric Neurology Program Professor & Vice Chair,
Standard Deviations from Mean Memory Matters: Preventing and Treating Late-Life, Cognitive Decline Daniel L. Murman, MD, MS Director, Behavioral and Geriatric Neurology Program Professor & Vice Chair,
Alzheimer s Disease without Dementia
 Alzheimer s Disease without Dementia Dr Emer MacSweeney CEO & Consultant Neuroradiologist Re:Cognition Health London Osteopathic Society 13 September 2016 Early diagnosis of Alzheimer s Disease How and
Alzheimer s Disease without Dementia Dr Emer MacSweeney CEO & Consultant Neuroradiologist Re:Cognition Health London Osteopathic Society 13 September 2016 Early diagnosis of Alzheimer s Disease How and
DISCLOSURES. Objectives. THE EPIDEMIC of 21 st Century. Clinical Assessment of Cognition: New & Emerging Tools for Diagnosing Dementia NONE TO REPORT
 Clinical Assessment of Cognition: New & Emerging Tools for Diagnosing Dementia DISCLOSURES NONE TO REPORT Freddi Segal Gidan, PA, PhD USC Keck School of Medicine Rancho/USC California Alzheimers Disease
Clinical Assessment of Cognition: New & Emerging Tools for Diagnosing Dementia DISCLOSURES NONE TO REPORT Freddi Segal Gidan, PA, PhD USC Keck School of Medicine Rancho/USC California Alzheimers Disease
ALZHEIMER S DISEASE. Mary-Letitia Timiras M.D. Overlook Hospital Summit, New Jersey
 ALZHEIMER S DISEASE Mary-Letitia Timiras M.D. Overlook Hospital Summit, New Jersey Topics Covered Demography Clinical manifestations Pathophysiology Diagnosis Treatment Future trends Prevalence and Impact
ALZHEIMER S DISEASE Mary-Letitia Timiras M.D. Overlook Hospital Summit, New Jersey Topics Covered Demography Clinical manifestations Pathophysiology Diagnosis Treatment Future trends Prevalence and Impact
A BRIEF LOOK AT DEMENTIA
 Dementia A BRIEF LOOK AT DEMENTIA David Kaufman, MD Neurology Consultants of Bellin Health November 2, 2017 Defined as a progressive decline in cognitive function that impairs daily activities. Always
Dementia A BRIEF LOOK AT DEMENTIA David Kaufman, MD Neurology Consultants of Bellin Health November 2, 2017 Defined as a progressive decline in cognitive function that impairs daily activities. Always
Alzheimer s Treatment and Prevention: What we know and where we are headed
 Alzheimer s Treatment and Prevention: What we know and where we are headed KU Alzheimer s Disease Center www.kualzheimer.org 913-588-0555 Eric Vidoni, PhD evidoni@kumc.edu Nationally-Designated AD Centers
Alzheimer s Treatment and Prevention: What we know and where we are headed KU Alzheimer s Disease Center www.kualzheimer.org 913-588-0555 Eric Vidoni, PhD evidoni@kumc.edu Nationally-Designated AD Centers
Alzheimer's Disease. Dementia
 Alzheimer's Disease Victor W. Henderson, MD, MS Departments of Health Research & Policy (Epidemiology) and of Neurology & Neurological Sciences Stanford University Director, Stanford Alzheimer s Disease
Alzheimer's Disease Victor W. Henderson, MD, MS Departments of Health Research & Policy (Epidemiology) and of Neurology & Neurological Sciences Stanford University Director, Stanford Alzheimer s Disease
Dementia and Fall Geriatric Interprofessional Training. Wael Hamade, MD, FAAFP
 Dementia and Fall Geriatric Interprofessional Training Wael Hamade, MD, FAAFP Prevalence of Dementia Age range 65-74 5% % affected 75-84 15-25% 85 and older 36-50% 5.4 Million American have AD Dementia
Dementia and Fall Geriatric Interprofessional Training Wael Hamade, MD, FAAFP Prevalence of Dementia Age range 65-74 5% % affected 75-84 15-25% 85 and older 36-50% 5.4 Million American have AD Dementia
DEMENTIA? 45 Million. What is. WHAT IS DEMENTIA Dementia is a disturbance in a group of mental processes including: 70% Dementia is not a disease
 What is PRESENTS DEMENTIA? WHAT IS DEMENTIA Dementia is a disturbance in a group of mental processes including: Memory Reasoning Planning Learning Attention Language Perception Behavior AS OF 2013 There
What is PRESENTS DEMENTIA? WHAT IS DEMENTIA Dementia is a disturbance in a group of mental processes including: Memory Reasoning Planning Learning Attention Language Perception Behavior AS OF 2013 There
What is dementia? What is dementia?
 What is dementia? What is dementia? What is dementia? Dementia is an umbrella term for a range of progressive conditions that affect the brain. It has been identified that there are over 200 subtypes of
What is dementia? What is dementia? What is dementia? Dementia is an umbrella term for a range of progressive conditions that affect the brain. It has been identified that there are over 200 subtypes of
Significance A Busy Clinician's Guide to Seniors with Memory Loss
 Significance A Busy Clinician's Guide to Seniors with Memory Loss Victoria Braund MD FACP CMD Division of Geriatrics. NorthShore University HealthSystem Alzheimer's disease is the sixth leading cause of
Significance A Busy Clinician's Guide to Seniors with Memory Loss Victoria Braund MD FACP CMD Division of Geriatrics. NorthShore University HealthSystem Alzheimer's disease is the sixth leading cause of
Fact Sheet Alzheimer s disease
 What is Alzheimer s disease Fact Sheet Alzheimer s disease Alzheimer s disease, AD, is a progressive brain disorder that gradually destroys a person s memory and ability to learn, reason, make judgements,
What is Alzheimer s disease Fact Sheet Alzheimer s disease Alzheimer s disease, AD, is a progressive brain disorder that gradually destroys a person s memory and ability to learn, reason, make judgements,
Michael A. Lobatz MD The Neurology Center Scripps Rehabilitation Center
 Michael A. Lobatz MD The Neurology Center Scripps Rehabilitation Center Dementia an acquired syndrome consisting of a decline in memory and other cognitive functions Alzheimer s Disease Fronto temporal
Michael A. Lobatz MD The Neurology Center Scripps Rehabilitation Center Dementia an acquired syndrome consisting of a decline in memory and other cognitive functions Alzheimer s Disease Fronto temporal
Comments to this discussion are invited on the Alzforum Webinar page. Who Should Use the New Diagnostic Guidelines? The Debate Continues
 Comments to this discussion are invited on the Alzforum Webinar page. Who Should Use the New Diagnostic s? The Debate Continues Ever since new criteria came out for a research diagnosis of prodromal/preclinical
Comments to this discussion are invited on the Alzforum Webinar page. Who Should Use the New Diagnostic s? The Debate Continues Ever since new criteria came out for a research diagnosis of prodromal/preclinical
ALZHEIMER S DISEASE OVERVIEW. Jeffrey Cummings, MD, ScD Cleveland Clinic Lou Ruvo Center for Brain Health
 ALZHEIMER S DISEASE OVERVIEW Jeffrey Cummings, MD, ScD Cleveland Clinic Lou Ruvo Center for Brain Health Prevalence AD: DEMOGRAPHY AND CLINICAL FEATURES Risk and protective factors Clinical features and
ALZHEIMER S DISEASE OVERVIEW Jeffrey Cummings, MD, ScD Cleveland Clinic Lou Ruvo Center for Brain Health Prevalence AD: DEMOGRAPHY AND CLINICAL FEATURES Risk and protective factors Clinical features and
DEMENTIA ANDREA BERG, MD
 DEMENTIA ANDREA BERG, MD What Is Dementia? Decline in memory, language, problem-solving and other cognitive skills that affects a persons ability to perform everyday activities Progressive and disabling
DEMENTIA ANDREA BERG, MD What Is Dementia? Decline in memory, language, problem-solving and other cognitive skills that affects a persons ability to perform everyday activities Progressive and disabling
Imaging of Alzheimer s Disease: State of the Art
 July 2015 Imaging of Alzheimer s Disease: State of the Art Neir Eshel, Harvard Medical School Year IV Outline Our patient Definition of dementia Alzheimer s disease Epidemiology Diagnosis Stages of progression
July 2015 Imaging of Alzheimer s Disease: State of the Art Neir Eshel, Harvard Medical School Year IV Outline Our patient Definition of dementia Alzheimer s disease Epidemiology Diagnosis Stages of progression
Latest Methods to Early Detection for Alzheimer's: Cognitive Assessments and Diagnostic Tools in Practice
 Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/alzheimers-disease-towards-earlier-detection/latest-methods-earlydetection-alzheimers-cognitive-assessments-and-diagnostic-tools-practice/8321/
Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/alzheimers-disease-towards-earlier-detection/latest-methods-earlydetection-alzheimers-cognitive-assessments-and-diagnostic-tools-practice/8321/
Erin Cullnan Research Assistant, University of Illinois at Chicago
 Dr. Moises Gaviria Distinguished Professor of Psychiatry, University of Illinois at Chicago Director of Consultation Liaison Service, Advocate Christ Medical Center Director of the Older Adult Program,
Dr. Moises Gaviria Distinguished Professor of Psychiatry, University of Illinois at Chicago Director of Consultation Liaison Service, Advocate Christ Medical Center Director of the Older Adult Program,
Dementia and Alzheimer s disease
 Since 1960 Medicine Korat โรงพยาบาลมหาราชนครราชส มา Dementia and Alzheimer s disease Concise Reviews PAWUT MEKAWICHAI MD DEPARTMENT of MEDICINE MAHARAT NAKHON RATCHASIMA HOSPITAL 1 Prevalence Increase
Since 1960 Medicine Korat โรงพยาบาลมหาราชนครราชส มา Dementia and Alzheimer s disease Concise Reviews PAWUT MEKAWICHAI MD DEPARTMENT of MEDICINE MAHARAT NAKHON RATCHASIMA HOSPITAL 1 Prevalence Increase
What is dementia? What is dementia?
 What is dementia? What is dementia? What is dementia? Dementia is an umbrella term for a range of progressive conditions that affect the brain. There are over 200 subtypes of dementia, but the five most
What is dementia? What is dementia? What is dementia? Dementia is an umbrella term for a range of progressive conditions that affect the brain. There are over 200 subtypes of dementia, but the five most
FRONTOTEMPORAL DEGENERATION: OVERVIEW, TRENDS AND DEVELOPMENTS
 FRONTOTEMPORAL DEGENERATION: OVERVIEW, TRENDS AND DEVELOPMENTS Norman L. Foster, M.D. Director, Center for Alzheimer s Care, Imaging and Research Chief, Division of Cognitive Neurology, Department of Neurology
FRONTOTEMPORAL DEGENERATION: OVERVIEW, TRENDS AND DEVELOPMENTS Norman L. Foster, M.D. Director, Center for Alzheimer s Care, Imaging and Research Chief, Division of Cognitive Neurology, Department of Neurology
Mild Cognitive Impairment (MCI)
") October 19, 2018 Mild Cognitive Impairment (MCI) Yonas E. Geda, MD, MSc Professor of Neurology and Psychiatry Consultant, Departments of Psychiatry & Psychology, and Neurology Mayo Clinic College of Medicine
October 19, 2018 Mild Cognitive Impairment (MCI) Yonas E. Geda, MD, MSc Professor of Neurology and Psychiatry Consultant, Departments of Psychiatry & Psychology, and Neurology Mayo Clinic College of Medicine
Forgetfulness: Knowing When to Ask for Help
 National Institute on Aging AgePage Forgetfulness: Knowing When to Ask for Help Maria has been a teacher for 35 years. Teaching fills her life and gives her a sense of accomplishment, but recently she
National Institute on Aging AgePage Forgetfulness: Knowing When to Ask for Help Maria has been a teacher for 35 years. Teaching fills her life and gives her a sense of accomplishment, but recently she
Objectives Gain a better understanding of Alzheimer s disease and other dementias. Enhance ability to detect signs and symptoms of dementia and learn
 Dementia Training provided through a Minnesota Department of Human Services Community Service Development Grant Project Catherine Johnson PsyD LP 1 Objectives Gain a better understanding of Alzheimer s
Dementia Training provided through a Minnesota Department of Human Services Community Service Development Grant Project Catherine Johnson PsyD LP 1 Objectives Gain a better understanding of Alzheimer s
3/6/2019 DIAGNOSIS OF DEMENTIA IN THE OUTPATIENT SETTING FINANCIAL DISCLOSURES LEARNING OBJECTIVES
 DIAGNOSIS OF DEMENTIA IN THE OUTPATIENT SETTING MILTA LITTLE, DO, CMD DUKE UNIVERSITY SCHOOL OF MEDICINE FINANCIAL DISCLOSURES Dr. Little has no relevant financial disclosures to report Dr. Little will
DIAGNOSIS OF DEMENTIA IN THE OUTPATIENT SETTING MILTA LITTLE, DO, CMD DUKE UNIVERSITY SCHOOL OF MEDICINE FINANCIAL DISCLOSURES Dr. Little has no relevant financial disclosures to report Dr. Little will
Safety of Disclosing Amyloid Status in Cognitively Normal Older Adults
 Safety of Disclosing Amyloid Status in Cognitively Normal Older Adults Jeffrey M. Burns, MD, MS University of Kansas Alzheimer s Disease Center Disclosures: Research funding from NIH, Avid Radiopharmaceuticals
Safety of Disclosing Amyloid Status in Cognitively Normal Older Adults Jeffrey M. Burns, MD, MS University of Kansas Alzheimer s Disease Center Disclosures: Research funding from NIH, Avid Radiopharmaceuticals
PROJECTION: Worlds dementia population is expected to triple by 2050
 DEMENTIA C L I S K C O N S U LTA N T P H Y S I C I A N I N A C U T E M E D I C I N E A N D G E R I AT R I C M E D I C I N E, B A R N E T H O S P I TA L, R O YA L F R E E N H S F O U N D AT I O N T R U
DEMENTIA C L I S K C O N S U LTA N T P H Y S I C I A N I N A C U T E M E D I C I N E A N D G E R I AT R I C M E D I C I N E, B A R N E T H O S P I TA L, R O YA L F R E E N H S F O U N D AT I O N T R U
DEMENTIA, THE BRAIN AND HOW IT WORKS AND WHY YOU MATTER
 OVERCOMING THE CHALLENGES OF MANAGING CHRONIC DISEASES IN PERSONS WITH DEMENTIA DEMENTIA, THE BRAIN AND HOW IT WORKS AND WHY YOU MATTER LEARNING OBJECTIVES Be familiar with the diagnostic criteria for
OVERCOMING THE CHALLENGES OF MANAGING CHRONIC DISEASES IN PERSONS WITH DEMENTIA DEMENTIA, THE BRAIN AND HOW IT WORKS AND WHY YOU MATTER LEARNING OBJECTIVES Be familiar with the diagnostic criteria for
DEMENTIA Dementia is NOT a normal part of aging Symptoms of dementia can be caused by different diseases Some symptoms of dementia may include:
 DEMENTIA Dementia is NOT a normal part of aging Symptoms of dementia can be caused by different diseases Some symptoms of dementia may include: 1. Memory loss The individual may repeat questions or statements,
DEMENTIA Dementia is NOT a normal part of aging Symptoms of dementia can be caused by different diseases Some symptoms of dementia may include: 1. Memory loss The individual may repeat questions or statements,
MOVEMENT DISORDERS AND DEMENTIA
 MOVEMENT DISORDERS AND DEMENTIA FOCUS ON DEMENTIA WITH LEWY BODIES MADHAVI THOMAS MD NORTH TEXAS MOVEMENT DISORDERS INSTITUTE, INC DEMENTIA de men tia dəˈmen(t)sh(ē)ə/ nounmedicine noun: dementia a chronic
MOVEMENT DISORDERS AND DEMENTIA FOCUS ON DEMENTIA WITH LEWY BODIES MADHAVI THOMAS MD NORTH TEXAS MOVEMENT DISORDERS INSTITUTE, INC DEMENTIA de men tia dəˈmen(t)sh(ē)ə/ nounmedicine noun: dementia a chronic
Managing Patients with Dementia using a Collaborative and Strength-based Approach
 Managing Patients with Dementia using a Collaborative and Strength-based Approach Therapy Network Seminars, Inc. Nicole Dawson, PT, PhD, GCS Learning Objectives The Participant will be able to: Identify
Managing Patients with Dementia using a Collaborative and Strength-based Approach Therapy Network Seminars, Inc. Nicole Dawson, PT, PhD, GCS Learning Objectives The Participant will be able to: Identify
Caring Sheet #11: Alzheimer s Disease:
 CARING SHEETS: Caring Sheet #11: Alzheimer s Disease: A Summary of Information and Intervention Suggestions with an Emphasis on Cognition By Shelly E. Weaverdyck, PhD Introduction This caring sheet focuses
CARING SHEETS: Caring Sheet #11: Alzheimer s Disease: A Summary of Information and Intervention Suggestions with an Emphasis on Cognition By Shelly E. Weaverdyck, PhD Introduction This caring sheet focuses
Dementia and Delirium: A Neurologist s Approach to Altered Mental Status. Case 1 4/7/11. Which of the following evaluations is your next step?
 Dementia and Delirium: A Neurologist s Approach to Altered Mental Status S. Andrew Josephson, MD Director, Neurohospitalist Program Medical Director, Inpatient Neurology University of California San Francisco
Dementia and Delirium: A Neurologist s Approach to Altered Mental Status S. Andrew Josephson, MD Director, Neurohospitalist Program Medical Director, Inpatient Neurology University of California San Francisco
Alzheimer s disease is an
 Alzheimer s Disease FACT SHEET Alzheimer s disease is an irreversible, progressive brain disease that slowly destroys memory and thinking skills, and eventually even the ability to carry out the simplest
Alzheimer s Disease FACT SHEET Alzheimer s disease is an irreversible, progressive brain disease that slowly destroys memory and thinking skills, and eventually even the ability to carry out the simplest
UNDERSTANDING ALZHEIMER S AND DEMENTIA
 UNDERSTANDING ALZHEIMER S AND DEMENTIA Geri T., living with Alzheimer's, and her husband and care partner, Jim T. THE IMPACT OF ALZHEIMER S AND DEMENTIA Currently, an estimated 50 million people worldwide
UNDERSTANDING ALZHEIMER S AND DEMENTIA Geri T., living with Alzheimer's, and her husband and care partner, Jim T. THE IMPACT OF ALZHEIMER S AND DEMENTIA Currently, an estimated 50 million people worldwide
Dementia and cognitive decline
 Dementia and cognitive decline Expert Briefing Su Ray and Dr Susan Davidson Research Department Together, we can help everyone to love later life 01 Brain basics Normal ageing, cognitive impairment and
Dementia and cognitive decline Expert Briefing Su Ray and Dr Susan Davidson Research Department Together, we can help everyone to love later life 01 Brain basics Normal ageing, cognitive impairment and
Dementia. Memory Evaluation Center Neurology
 Dementia Memory Evaluation Center Neurology Topics Overview of dementia Stages Medications Advanced planning What is Dementia? Dementia = significant global decline in cognitive function not due to medicine
Dementia Memory Evaluation Center Neurology Topics Overview of dementia Stages Medications Advanced planning What is Dementia? Dementia = significant global decline in cognitive function not due to medicine
Evaluations. Alzheimer s Disease A Public Health Response. Viewer Call-In. July 19, Guest Speakers. Thanks to our Sponsors:
 Alzheimer s Disease A Public Health Response July 19, 2007 1 2 Guest Speakers Thanks to our Sponsors: Earl A. Zimmerman, M.D. Bender Endowed Chair of Neurology and Director of the Alzheimer s Center at
Alzheimer s Disease A Public Health Response July 19, 2007 1 2 Guest Speakers Thanks to our Sponsors: Earl A. Zimmerman, M.D. Bender Endowed Chair of Neurology and Director of the Alzheimer s Center at
Dementia Update. October 1, 2013 Dylan Wint, M.D. Cleveland Clinic Lou Ruvo Center for Brain Health Las Vegas, Nevada
 Dementia Update October 1, 2013 Dylan Wint, M.D. Cleveland Clinic Lou Ruvo Center for Brain Health Las Vegas, Nevada Outline New concepts in Alzheimer disease Biomarkers and in vivo diagnosis Future trends
Dementia Update October 1, 2013 Dylan Wint, M.D. Cleveland Clinic Lou Ruvo Center for Brain Health Las Vegas, Nevada Outline New concepts in Alzheimer disease Biomarkers and in vivo diagnosis Future trends
Understanding Alzheimer s Disease
 Understanding Alzheimer s Disease Alzheimer s disease is an irreversible, progressive brain disorder that slowly impacts memory, thinking, skills and, eventually, the ability to carry out the simplest
Understanding Alzheimer s Disease Alzheimer s disease is an irreversible, progressive brain disorder that slowly impacts memory, thinking, skills and, eventually, the ability to carry out the simplest
WEBINAR SERIES: AGING IN INDIVIDUALS WITH INTELLECTUAL AND DEVELOPMENTAL DISABILITIES
 WEBINAR SERIES: AGING IN INDIVIDUALS WITH INTELLECTUAL AND DEVELOPMENTAL DISABILITIES 1 CMS Medicare-Medicaid Coordination Office (MMCO) Established by Section 2602 of the Affordable Care Act Purpose:
WEBINAR SERIES: AGING IN INDIVIDUALS WITH INTELLECTUAL AND DEVELOPMENTAL DISABILITIES 1 CMS Medicare-Medicaid Coordination Office (MMCO) Established by Section 2602 of the Affordable Care Act Purpose:
What if it s not Alzheimer s? Update on Lewy body dementia and frontotemporal dementia
 What if it s not Alzheimer s? Update on Lewy body dementia and frontotemporal dementia Dementia: broad term for any acquired brain condition impairing mental function such that ADLs are impaired. Includes:
What if it s not Alzheimer s? Update on Lewy body dementia and frontotemporal dementia Dementia: broad term for any acquired brain condition impairing mental function such that ADLs are impaired. Includes:
Mild Cognitive Impairment
 Mild Cognitive Impairment Victor W. Henderson, MD, MS Departments of Health Research & Policy (Epidemiology) and of Neurology & Neurological Sciences Stanford University Director, Stanford Alzheimer s
Mild Cognitive Impairment Victor W. Henderson, MD, MS Departments of Health Research & Policy (Epidemiology) and of Neurology & Neurological Sciences Stanford University Director, Stanford Alzheimer s
Getting Help for Patients with Dementia and their Caregivers. Erica Salamida Associate Director of Programs and Services Alzheimer s Association-NENY
 Getting Help for Patients with Dementia and their Caregivers Erica Salamida Associate Director of Programs and Services Alzheimer s Association-NENY In this session you will learn about: Symptoms of dementia,
Getting Help for Patients with Dementia and their Caregivers Erica Salamida Associate Director of Programs and Services Alzheimer s Association-NENY In this session you will learn about: Symptoms of dementia,
Dementia ALI ABBAS ASGHAR-ALI, MD STAFF PSYCHIATRIST MICHAEL E. DEBAKEY VA MEDICAL CENTER ASSOCIATE PROFESSOR BAYLOR COLLEGE OF MEDICINE
 Dementia ALI ABBAS ASGHAR-ALI, MD STAFF PSYCHIATRIST MICHAEL E. DEBAKEY VA MEDICAL CENTER ASSOCIATE PROFESSOR BAYLOR COLLEGE OF MEDICINE Objectives At the conclusion of the session, participants will be
Dementia ALI ABBAS ASGHAR-ALI, MD STAFF PSYCHIATRIST MICHAEL E. DEBAKEY VA MEDICAL CENTER ASSOCIATE PROFESSOR BAYLOR COLLEGE OF MEDICINE Objectives At the conclusion of the session, participants will be
DEMENTIA NEWSLETTER for PHYSICIANS
 DEMENTIA NEWSLETTER for PHYSICIANS Vol. 6, No. 4 OTTAWA AND RENFREW COUNTY Winter 2008 In This Issue... Mild Cognitive Impairment Monitoring Patient Response to Cognitive Enhancers CDN Diagnostic Assessment
DEMENTIA NEWSLETTER for PHYSICIANS Vol. 6, No. 4 OTTAWA AND RENFREW COUNTY Winter 2008 In This Issue... Mild Cognitive Impairment Monitoring Patient Response to Cognitive Enhancers CDN Diagnostic Assessment
Alzheimer s disease. The facts in brief
 Alzheimer s disease Dementia is an umbrella term used to describe various conditions which damage brain cells and lead to a loss of brain function over time. Dementia causes a progressive decline in a
Alzheimer s disease Dementia is an umbrella term used to describe various conditions which damage brain cells and lead to a loss of brain function over time. Dementia causes a progressive decline in a
Drug Update. Treatments for Cognitive Impairment in the Older Adult. William Solan, M.D. Karen Sanders, Ph.D. Northwest Hospital Seattle
 Drug Update Treatments for Cognitive Impairment in the Older Adult William Solan, M.D. Karen Sanders, Ph.D. Northwest Hospital Seattle Current Drug Treatments for Alzheimer s Disease Cholinesterase Inhibitors:
Drug Update Treatments for Cognitive Impairment in the Older Adult William Solan, M.D. Karen Sanders, Ph.D. Northwest Hospital Seattle Current Drug Treatments for Alzheimer s Disease Cholinesterase Inhibitors:
I have no relevant financial disclosures
 1 ADVANCED INSIGHTS INTO THE PREVENTION, TREATMENT AND MANAGEMENT OF ALZHEIMER S DISEASE Naushira Pandya, MD, CMD, FACP Professor and Chair, Department of Geriatrics Director, Geriatrics Education Center
1 ADVANCED INSIGHTS INTO THE PREVENTION, TREATMENT AND MANAGEMENT OF ALZHEIMER S DISEASE Naushira Pandya, MD, CMD, FACP Professor and Chair, Department of Geriatrics Director, Geriatrics Education Center
Cal MediConnect Dementia Awareness CMC Annual Training
 Cal MediConnect 2017 Dementia Awareness 2017 CMC Annual Training Definition Overview of Dementia Training Diagnosis of Dementia Signs and Symptoms Risk Factors Stages of Dementia Types of Dementia: Reversible/Irreversible
Cal MediConnect 2017 Dementia Awareness 2017 CMC Annual Training Definition Overview of Dementia Training Diagnosis of Dementia Signs and Symptoms Risk Factors Stages of Dementia Types of Dementia: Reversible/Irreversible
Custom Intelligence. Alzheimer s Disease Landscape Summary
 Custom Intelligence Alzheimer s Disease Landscape Summary Prepared August 21 Alzheimer s Disease Landscape: Executive Summary Current standard of care in Alzheimer s Disease (AD) consists of symptomatic
Custom Intelligence Alzheimer s Disease Landscape Summary Prepared August 21 Alzheimer s Disease Landscape: Executive Summary Current standard of care in Alzheimer s Disease (AD) consists of symptomatic
Form D1: Clinician Diagnosis
 Initial Visit Packet Form D: Clinician Diagnosis NACC Uniform Data Set (UDS) ADC name: Subject ID: Form date: / / Visit #: Examiner s initials: INSTRUCTIONS: This form is to be completed by the clinician.
Initial Visit Packet Form D: Clinician Diagnosis NACC Uniform Data Set (UDS) ADC name: Subject ID: Form date: / / Visit #: Examiner s initials: INSTRUCTIONS: This form is to be completed by the clinician.
Cognitive Screening in Risk Assessment. Geoffrey Tremont, Ph.D. Rhode Island Hospital & Alpert Medical School of Brown University.
 Cognitive Screening in Risk Assessment Geoffrey Tremont, Ph.D. Rhode Island Hospital & Alpert Medical School of Brown University Outline of Talk Definition of Dementia and MCI Incidence and Prevalence
Cognitive Screening in Risk Assessment Geoffrey Tremont, Ph.D. Rhode Island Hospital & Alpert Medical School of Brown University Outline of Talk Definition of Dementia and MCI Incidence and Prevalence
Assessment Toolkits for Lewy Body Dementia
 Study : Assessment Toolkits for Lewy Body Dementia There are two toolkits, depending on whether the patient is presenting with a primary cognitive problem or with cognitive decline in the context of established
Study : Assessment Toolkits for Lewy Body Dementia There are two toolkits, depending on whether the patient is presenting with a primary cognitive problem or with cognitive decline in the context of established
Our rapidly aging population means that more and more people will be diagnosed with Alzheimer s and other dementias in the next 20 years.
 Only 1% of people aged 65 years old have Alzheimer s. 10% of people aged 75 years old have Alzheimer s. 20% of people aged 85 years old have Alzheimer s. Our rapidly aging population means that more and
Only 1% of people aged 65 years old have Alzheimer s. 10% of people aged 75 years old have Alzheimer s. 20% of people aged 85 years old have Alzheimer s. Our rapidly aging population means that more and
Neuropsychological Evaluation of
 Neuropsychological Evaluation of Alzheimer s Disease Joanne M. Hamilton, Ph.D. Shiley-Marcos Alzheimer s Disease Research Center Department of Neurosciences University of California, San Diego Establish
Neuropsychological Evaluation of Alzheimer s Disease Joanne M. Hamilton, Ph.D. Shiley-Marcos Alzheimer s Disease Research Center Department of Neurosciences University of California, San Diego Establish
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017.
 DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
Can aspirin slow cognitive decline and the onset of dementia? The ASPREE study. Mark Nelson on behalf of ASPREE Investigators
 Can aspirin slow cognitive decline and the onset of dementia? The ASPREE study. Mark Nelson on behalf of ASPREE Investigators ASPREE Randomized, double-blind, placebo-controlled trial for extending healthy
Can aspirin slow cognitive decline and the onset of dementia? The ASPREE study. Mark Nelson on behalf of ASPREE Investigators ASPREE Randomized, double-blind, placebo-controlled trial for extending healthy
Stephen Salloway, M.D., M.S. Disclosure of Interest
 Challenges in the Early Diagnosis of Alzheimer s Disease Stephen Salloway, MD, MS Professor of Neurology and Psychiatry Alpert Medical School, Brown University 2 nd Annual Early Alzheimer s Educational
Challenges in the Early Diagnosis of Alzheimer s Disease Stephen Salloway, MD, MS Professor of Neurology and Psychiatry Alpert Medical School, Brown University 2 nd Annual Early Alzheimer s Educational
Alzheimer Disease and Related Dementias. Alzheimer Society of Manitoba Dr. David Strang
 Alzheimer Disease and Related Dementias Alzheimer Society of Manitoba Dr. David Strang What is Dementia? Dementia is a syndrome symptoms include loss of memory, judgment and reasoning, and changes in mood
Alzheimer Disease and Related Dementias Alzheimer Society of Manitoba Dr. David Strang What is Dementia? Dementia is a syndrome symptoms include loss of memory, judgment and reasoning, and changes in mood
PD ExpertBriefing: Cognition and PD: What You ve Always Wanted to Know But Were Too Afraid to Ask. Presented By: Tuesday, March 22, 2011 at 1:00 PM ET
 PD ExpertBriefing: Cognition and PD: What You ve Always Wanted to Know But Were Too Afraid to Ask Presented By: Alexander I. Tröster, PhD, ABPP University of North Carolina, Chapel Hill, NC Tuesday, March
PD ExpertBriefing: Cognition and PD: What You ve Always Wanted to Know But Were Too Afraid to Ask Presented By: Alexander I. Tröster, PhD, ABPP University of North Carolina, Chapel Hill, NC Tuesday, March
Diagnosis and management of non-alzheimer dementias. Melissa Yu, M.D. Department of Neurology
 Diagnosis and management of non-alzheimer dementias Melissa Yu, M.D. Department of Neurology AGENDA Introduction When to think of alternate diagnoses Other forms of dementia Other reasons for confusion
Diagnosis and management of non-alzheimer dementias Melissa Yu, M.D. Department of Neurology AGENDA Introduction When to think of alternate diagnoses Other forms of dementia Other reasons for confusion
7/3/2013 ABNORMAL PSYCHOLOGY SEVENTH EDITION CHAPTER FOURTEEN CHAPTER OUTLINE. Dementia, Delirium, and Amnestic Disorders. Oltmanns and Emery
 ABNORMAL PSYCHOLOGY SEVENTH EDITION Oltmanns and Emery PowerPoint Presentations Prepared by: Ashlea R. Smith, Ph.D. This multimedia and its contents are protected under copyright law. The following are
ABNORMAL PSYCHOLOGY SEVENTH EDITION Oltmanns and Emery PowerPoint Presentations Prepared by: Ashlea R. Smith, Ph.D. This multimedia and its contents are protected under copyright law. The following are
DEMENTIA (Major Neurocognitive Disorder) SUSAN BEHNAWA, M.D. DIVISION OF GERIATRIC MEDICINE AND GERONTOLOGY UC IRVINE HEALTH SCHOOL OF MEDICINE
 SUSAN BEHNAWA, M.D. DIVISION OF GERIATRIC MEDICINE AND GERONTOLOGY UC IRVINE HEALTH SCHOOL OF MEDICINE") DEMENTIA (Major Neurocognitive Disorder) SUSAN BEHNAWA, M.D. DIVISION OF GERIATRIC MEDICINE AND GERONTOLOGY UC IRVINE HEALTH SCHOOL OF MEDICINE Objectives Review the epidemiology and social impact of Dementia
DEMENTIA (Major Neurocognitive Disorder) SUSAN BEHNAWA, M.D. DIVISION OF GERIATRIC MEDICINE AND GERONTOLOGY UC IRVINE HEALTH SCHOOL OF MEDICINE Objectives Review the epidemiology and social impact of Dementia
Community Information Forum September 20, 2014
 Community Information Forum September 20, 2014 Dr. David B. Hogan Brenda Strafford Foundation Chair in Geriatrics Medicine University of Calgary Important to note: The slides used during Dr. Hogan's presentation
Community Information Forum September 20, 2014 Dr. David B. Hogan Brenda Strafford Foundation Chair in Geriatrics Medicine University of Calgary Important to note: The slides used during Dr. Hogan's presentation
What APS Workers Need to Know about Frontotemporal, Lewy Body and Vascular Dementias
 What APS Workers Need to Know about Frontotemporal, Lewy Body and Vascular Dementias Presenter: Kim Bailey, MS Gerontology, Program & Education Specialist, Alzheimer s Orange County 1 1 Facts About Our
What APS Workers Need to Know about Frontotemporal, Lewy Body and Vascular Dementias Presenter: Kim Bailey, MS Gerontology, Program & Education Specialist, Alzheimer s Orange County 1 1 Facts About Our
Common Forms of Dementia Handout Package
 Common Forms of Dementia Handout Package Common Forms of Dementia 1 Learning Objectives As a result of working through this module, you should be better able to: 1. Describe clinical features of 4 major
Common Forms of Dementia Handout Package Common Forms of Dementia 1 Learning Objectives As a result of working through this module, you should be better able to: 1. Describe clinical features of 4 major
Dementia Chronic Brain Failure The forgotten cardiovascular disease Clare Hawley 2015
 Dementia Chronic Brain Failure The forgotten cardiovascular disease Clare Hawley 2015 MB ChB, MRCGP, PG Dip Cardiol, PG Cert Med Ed Associate Specialist Cardiology Chesterfield Royal Hospital GPwSI Refractory
Dementia Chronic Brain Failure The forgotten cardiovascular disease Clare Hawley 2015 MB ChB, MRCGP, PG Dip Cardiol, PG Cert Med Ed Associate Specialist Cardiology Chesterfield Royal Hospital GPwSI Refractory
NEUROPSYCHOMETRIC TESTS
 NEUROPSYCHOMETRIC TESTS CAMCOG It is the Cognitive section of Cambridge Examination for Mental Disorders of the Elderly (CAMDEX) The measure assesses orientation, language, memory, praxis, attention, abstract
NEUROPSYCHOMETRIC TESTS CAMCOG It is the Cognitive section of Cambridge Examination for Mental Disorders of the Elderly (CAMDEX) The measure assesses orientation, language, memory, praxis, attention, abstract
Information Gathering Obtaining history is the most critical first step Patient-provided history may not be reliable Need info from relatives, friends
 ASSESSING COMPETENCE Michael A Hill MD UNC Psychiatry 2008 Information Gathering Obtaining history is the most critical first step Patient-provided history may not be reliable Need info from relatives,
ASSESSING COMPETENCE Michael A Hill MD UNC Psychiatry 2008 Information Gathering Obtaining history is the most critical first step Patient-provided history may not be reliable Need info from relatives,
INSTRUCTIONS FOR THE AD8 DEMENTIA SCREENING INTERVIEW (10/22/2015) (ADS, VERSION 1, 4/29/2015)
 (ADS, VERSION 1, 4/29/2015)") INSTRUCTIONS FOR THE AD8 DEMENTIA SCREENING INTERVIEW (10/22/2015) (ADS, VERSION 1, 4/29/2015) I. General Instructions The AD8 Dementia Screening Interview (ADS) is a measure used to detect dementia. The
INSTRUCTIONS FOR THE AD8 DEMENTIA SCREENING INTERVIEW (10/22/2015) (ADS, VERSION 1, 4/29/2015) I. General Instructions The AD8 Dementia Screening Interview (ADS) is a measure used to detect dementia. The
A PATIENT S GUIDE FOR PERSONS WITH DEMENTIA OR ALZHEIMER S DISEASE
 A PATIENT S GUIDE FOR PERSONS WITH DEMENTIA OR ALZHEIMER S DISEASE 1. WHAT IF I THINK I HAVE ALZHEIMER S DISEASE OR MY DOCTOR TELLS ME I HAVE DEMENTIA? 1.1. Understanding How My Memory Works Memory problems
A PATIENT S GUIDE FOR PERSONS WITH DEMENTIA OR ALZHEIMER S DISEASE 1. WHAT IF I THINK I HAVE ALZHEIMER S DISEASE OR MY DOCTOR TELLS ME I HAVE DEMENTIA? 1.1. Understanding How My Memory Works Memory problems
The current state of healthcare for Normal Aging, Mild Cognitive Impairment, & Alzheimer s Disease
 The current state of healthcare for Normal Aging, g, Mild Cognitive Impairment, & Alzheimer s Disease William Rodman Shankle, MS MD FACP Director, Alzheimer s Program, Hoag Neurosciences Institute Neurologist,
The current state of healthcare for Normal Aging, g, Mild Cognitive Impairment, & Alzheimer s Disease William Rodman Shankle, MS MD FACP Director, Alzheimer s Program, Hoag Neurosciences Institute Neurologist,
Dr. Michael Lobatz Dr. Michael Jackson Dr. James Brewer Dr. Paul Aisen. Dr. Michael Plopper. Dr. Guerry Peavy
 1 Anne State 2 3 Dr. Michael Lobatz Dr. Michael Jackson Dr. James Brewer Dr. Paul Aisen Dr. Michael Plopper Dr. Guerry Peavy 4 Michael Lobatz, MD Medical Director, Neurosciences Medical Director, Rehabilitation
1 Anne State 2 3 Dr. Michael Lobatz Dr. Michael Jackson Dr. James Brewer Dr. Paul Aisen Dr. Michael Plopper Dr. Guerry Peavy 4 Michael Lobatz, MD Medical Director, Neurosciences Medical Director, Rehabilitation
Alzheimer s Disease. Fact Sheet. Fact Sheet. Fact Sheet. What Causes AD?
 2 Alzheimer s Disease Dementia is a brain disorder that seriously affects a person s ability to carry out daily activities. The most common form of dementia among older people is Alzheimer s disease (AD),
2 Alzheimer s Disease Dementia is a brain disorder that seriously affects a person s ability to carry out daily activities. The most common form of dementia among older people is Alzheimer s disease (AD),
Raj C. Shah, MD Associate Professor in Family Medicine Rush Alzheimer s Disease Center Rush University Medical Center
 Raj C. Shah, MD Associate Professor in Family Medicine Rush Alzheimer s Disease Center Rush University Medical Center Raj_C_Shah@rush.edu From Legal Practice to What s Next: The Boomer-Lawyer s Guide to
Raj C. Shah, MD Associate Professor in Family Medicine Rush Alzheimer s Disease Center Rush University Medical Center Raj_C_Shah@rush.edu From Legal Practice to What s Next: The Boomer-Lawyer s Guide to
Understanding Dementia
 Dementia Handbook for Carers Essex Understanding Dementia What is dementia? 1 Summary of dementia symptoms 4 Medication and treatment 5 1 Dementia is the name for several conditions that lead to the progressive
Dementia Handbook for Carers Essex Understanding Dementia What is dementia? 1 Summary of dementia symptoms 4 Medication and treatment 5 1 Dementia is the name for several conditions that lead to the progressive
Alzheimer s Disease - Dementia
 - Dementia Neurocognitive disorder with dysfunction or loss of " Memory " Orientation " Attention " Language " Judgment " Reasoning Other characteristics that can manifest " Personality changes " Behavioral
- Dementia Neurocognitive disorder with dysfunction or loss of " Memory " Orientation " Attention " Language " Judgment " Reasoning Other characteristics that can manifest " Personality changes " Behavioral
What is dementia? Symptoms of dementia. Memory problems
 What is dementia? What is dementia? What is dementia? Dementia is an umbrella term for a range of progressive conditions that affect the brain. The brain is made up of nerve cells (neurones) that communicate
What is dementia? What is dementia? What is dementia? Dementia is an umbrella term for a range of progressive conditions that affect the brain. The brain is made up of nerve cells (neurones) that communicate
CHAPTER 5 NEUROPSYCHOLOGICAL PROFILE OF ALZHEIMER S DISEASE
 CHAPTER 5 NEUROPSYCHOLOGICAL PROFILE OF ALZHEIMER S DISEASE 5.1 GENERAL BACKGROUND Neuropsychological assessment plays a crucial role in the assessment of cognitive decline in older age. In India, there
CHAPTER 5 NEUROPSYCHOLOGICAL PROFILE OF ALZHEIMER S DISEASE 5.1 GENERAL BACKGROUND Neuropsychological assessment plays a crucial role in the assessment of cognitive decline in older age. In India, there
P20.2. Characteristics of different types of dementia and challenges for the clinician
 P20.2. Characteristics of different types of dementia and challenges for the clinician, professor Danish Dementia Research Center Rigshospitalet, University of Copenhagen (Denmark) This project has received
P20.2. Characteristics of different types of dementia and challenges for the clinician, professor Danish Dementia Research Center Rigshospitalet, University of Copenhagen (Denmark) This project has received
Brain Health. UW Medicine SCHOOL OF MEDICINE
 UW Medicine SCHOOL OF MEDICINE Brain Health PAMELA M. DEAN, PH.D., ABPP BOARD CERTIFIED IN CLINICAL NEUROPSYCHOLOGY VA PUGET SOUND HEALTHCARE SYSTEM, SEATTLE ACTING ASSISTANT PROFESSOR DEPARTMENT OF PSYCHIATRY
UW Medicine SCHOOL OF MEDICINE Brain Health PAMELA M. DEAN, PH.D., ABPP BOARD CERTIFIED IN CLINICAL NEUROPSYCHOLOGY VA PUGET SOUND HEALTHCARE SYSTEM, SEATTLE ACTING ASSISTANT PROFESSOR DEPARTMENT OF PSYCHIATRY
Delirium & Dementia. Nicholas J. Silvestri, MD
 Delirium & Dementia Nicholas J. Silvestri, MD Outline Delirium vs. Dementia Neural pathways relating to consciousness Encephalopathy Stupor Coma Dementia Delirium vs. Dementia Delirium Abrupt onset Lasts
Delirium & Dementia Nicholas J. Silvestri, MD Outline Delirium vs. Dementia Neural pathways relating to consciousness Encephalopathy Stupor Coma Dementia Delirium vs. Dementia Delirium Abrupt onset Lasts
GERIATRIC MENTAL HEALTH AND MEDICATION TREATMENT
 Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences GERIATRIC MENTAL HEALTH AND MEDICATION TREATMENT RUTH KOHEN ASSOCIATE PROFESSOR UW DEPARTMENT OF PSYCHIATRY 5-4-2017
Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences GERIATRIC MENTAL HEALTH AND MEDICATION TREATMENT RUTH KOHEN ASSOCIATE PROFESSOR UW DEPARTMENT OF PSYCHIATRY 5-4-2017