Blood pressure (BP) control. Hypertension
|
|
|
- Conrad Washington
- 5 years ago
- Views:
Transcription
1
")
2 Blood pressure (BP) control

3 Normal heart function
4 Blood pressure (BP) control blood pressure (BP) cardiac output (CO) = total peripheral resistance (TPR) heart rate (HR) filling pressure arteriolar volume contractility blood volume venous tone
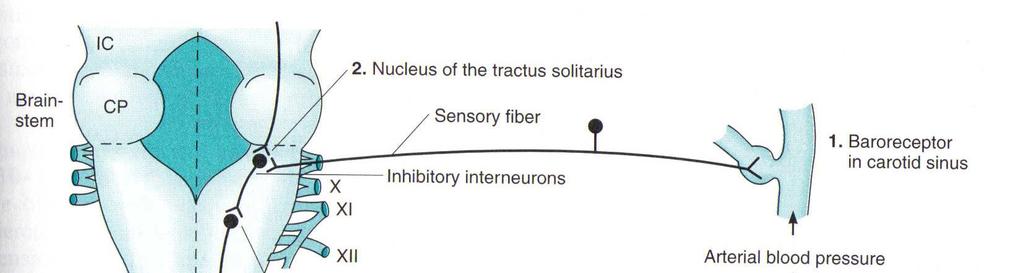
5 Blood pressure (BP) control 1. Baroreceptors aortic arch and carotid sinus kidneys 2. Autonomic control sympathetic (adrenergic) para-sympathetic (cholinergic) 3. Renin-angiotensin-aldosterone system (RAAS) 4. Chemoreceptors 5. CNS control 6. Vasopressin (anti-diuretic hormone)
6 Blood pressure (BP) control 1. Baroreceptors aortic arch and carotid sinus kidneys 2. Autonomic control sympathetic (adrenergic) para-sympathetic (cholinergic) 3. Renin-angiotensin-aldosterone system (RAAS) 4. Chemoreceptors 5. CNS control 6. Vasopressin (Anti-diuretic hormone)
7 Sympathetic control rapid, momentary regulation affects sympathetic and para-sympathetic systems alters vascular constriction and CO
8 Sympathetic control
9 Sympathetic control
10 RAAS control long-term regulation affects angiotensin-ii and aldosterone secretion potent vasoconstrictor affects vascular constriction controls water balance affects blood volume

11 RAAS control
12 Combined control sympathetic activity BLOOD PRESSURE DECREASED renal blood flow cardiac β 1 -adrenoceptors activated smooth muscle α 1 -adrenoceptors activated Sympathetic mediation renin RAAS mediation angiotensin-ii CO TPR BLOOD PRESSURE INCREASED aldosterone Glomerular filtration rate Na +, water retention blood volume
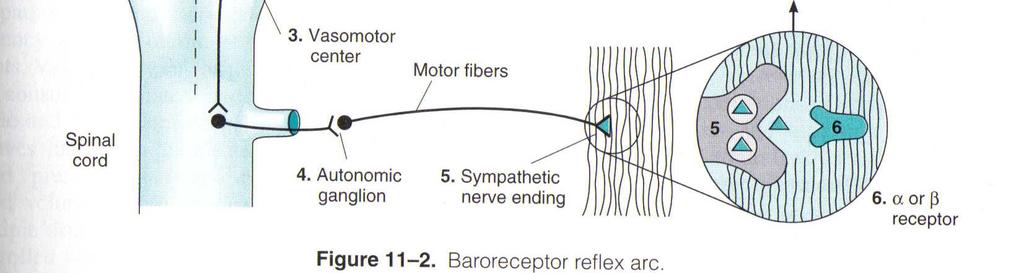
13 (HTN) Classical definition BP > 140/90 NHLBI previous classification Category Normal High Normal Stage 1 (mild HTN) Stage 2 (moderate HTN) Stage 3 (severe HTN) Stage 4 (very severe HTN) Systolic (mm Hg) < Diastolic (mm Hg) <
14 (HTN) Risk assessment Other Risk Factors & Disease History Grade 1 (mild hypertension) SBP or DBP BLOOD PRESSURE (mmhg) Grade 2 (moderate hypertension) SBP or DBP Grade 3 (severe hypertension) SBP 180 or DBP 110 I. no other risk factors LOW RISK MED RISK HIGH RISK II. 1-2 risk factors MED RISK MED RISK VERY HIGH RISK III. 3 or more risk factors or TOD 1 or diabetes HIGH RISK HIGH RISK VERY HIGH RISK IV. ACC 2 VERY HIGH RISK VERY HIGH RISK VERY HIGH RISK 1 - TOD = Target Organ Damage 2 - ACC = Associated Clinical Conditions, including clinical cardiovascular disease and renal disease.

15 JNC-7 guidelines 2003 HTN prevalence - USA: ~ 50 million people

16 JNC-7 guidelines 2003
17 JNC-7 guidelines 2003 Benefits of Lowering BP average % reduction stroke incidence 35 40% myocardial infarction 20 25% heart failure 50% In stage 1 HTN and additional CVD risk factors, achieving a sustained 12 mmhg reduction in SBP over 10 years will prevent 1 death for every 11 patients treated (NNT=11).
18 JNC-7 guidelines 2003 Benefits of Lowering BP the BP relationship to risk of CVD is continuous, consistent, and independent of other risk factors. each increment of 20/10 mmhg doubles the risk of CVD across the entire BP range starting from 115/75 mmhg.
19 JNC-7 guidelines 2003 Benefits of Lowering BP for persons over age 50, SBP is a more important than DBP as CVD risk factor. those with SBP mmhg or DBP mmhg should be considered pre-hypertensive who require health-promoting lifestyle modifications to prevent CVD.
20 JNC-7 guidelines 2003 Goals of antihypertensive therapy reduce CVD and renal morbidity and mortality. treat to BP <140/90 mmhg or BP <130/80 mmhg in patients with diabetes or chronic kidney disease. achieve SBP goal especially in persons >50yo.

21 JNC-7 guidelines 2003
22 JNC-7 guidelines 2003 Identifiable causes of HTN sleep apnea drug-induced or related causes chronic kidney disease primary aldosteronism reno-vascular disease chronic steroid therapy and Cushing s syndrome pheochromocytoma coarctation of the aorta thyroid or parathyroid disease

23 JNC-7 guidelines 2003
24 JNC-7 guidelines 2003 HTN-related target organ damage heart left ventricular hypertrophy angina or prior myocardial infarction prior coronary revascularization heart failure brain stroke or transient ischemic attack chronic kidney disease peripheral arterial disease retinopathy
25 JNC-7 guidelines 2003 Lifestyle modifications Modification weight reduction DASH eating plan dietary Na + reduction physical activity alcohol consumption Approximate SBP reduction 5-20 mmhg/10 kg weight loss 8-14 mmhg 2-8 mmhg 4-9 mmhg 2-4 mmhg
26 Therapeutic options: Diuretics β-blockers α 1 -blockers Calcium-channel blockers RAAS modifiers Other
27 Therapeutic options: Diuretics β-blockers α 1 -blockers Calcium-channel blockers RAAS modifiers Other
28 Diuretics (thiazides) currently considered 1 st line (elderly) effective in low oral doses (monotherapy/combination) reduce mortality (stroke, MI, CHF) Hydrochlorothiazide (HCTZ) = Disothiazide
29 Thiazide diuretics most effective diuretics in HTN mechanism: peripheral resistance Na +, H 2 O excretion blood volume blood pressure cardiac output
30 Thiazide diuretics - PK good bioavailability (50-80%) not metabolized HCTZ T 1/2-6-12hr renal excretion HCTZ dosing range mg/d ineffective in moderate-severe renal failure (metolazone/indapamide)
31 Thiazide diuretics - PD HCTZ (mg/d)
32 Thiazide diuretics - ADEs hypokalemia (common) - monitor per risk factors hyperuricemia (common) hyperglycemia (10%) hypomagnesemia
33 Thiazide diuretics - DDIs digoxin (hypokalemia may exacerbate digoxin effect) lithium (thazides reduce lithium renal clearance) other diuretic/hypotensive medications (additive effect)
34 Potassium-sparing diuretics spironolactone (Aldospirone ) reduce K + excretion mild hypotensive effect
35 Loop diuretics furosemide (Fusid ) not used as hypotensives: less effective short T 1/2
36 Therapeutic options: Diuretics β-blockers α 1 -blockers Calcium-channel blockers RAAS modifiers Other
37 β-blockers (BBs)- mechanism β-blocker administration 1 2 cardiac β 1 receptor activation renin release cardiac output angiotensin-ii formation peripheral resistance blood pressure aldosterone secretion Na+, H2O excretion blood volume
38 β-blockers selectivity β 1 vs. β 2 non-selective: propranolol = Deralin, Prolol β 1 -selective: atenolol = Normiten, Normalol metoprolol = Lopressor, Neobloc bisoprolol = Concor, Cardiloc
39 β-blockers - ADEs bradycardia hypotension fatigue insomnia sexual dysfunction altered lipid profile
40 β-blockers - DDIs effect of hypoglycemics effect of digoxin, CCBs, α-blockers, other hypotensives β-blockers precautions and contra-indications might mask hypoglycemic effect of hypoglycemics β 2 -blockade in respiratory disease (propranolol - C/I) severe CHF
41 β-blockers - therapeutic considerations more effective in caucasians than in blacks (as monotherapy) additional benefit in concomitant diseases (CHF, IHD, migraine, post-mi, certain arrhythmias)
42 Therapeutic options: Diuretics β-blockers α 1 -blockers Calcium-channel blockers RAAS modifiers Other
43 α 1 -blockers - mechanism α 1 -blocker administration smooth muscle relaxation arterial venous peripheral resistance blood pressure
44 α-blockers - therapeutic considerations α 1 vs. α 2 α 1 -selective: prazosin (Hypotens ) doxazosin (Cardoral, Cadex, Doxaloc ) terazosin (Hytrin )
45 α 1 -blockers - ADEs postural hypotension (1 st -dose syncope) fatigue headache
46 α 1 -blockers - DDIs other hypotensives effect may be decreased by NSAIDs α 1 -blockers - precautions reflex tachycardia upon initiation (short-term β-blocker)
47 α 1 -blockers - therapeutic considerations reflex tachycardia upon initiation (short-term β-blocker) for mild-moderate HTN usually in combination Tx minimal effect on CO, renal function may improve lipid profile may increase mortality risk in HF patients additional benefit in benign prostate hypertrophy (BPH)
48 Therapeutic options: Diuretics β-blockers α 1 -blockers Calcium-channel blockers RAAS modifiers Other
49 CCBs - subclasses Dihydropyridines HTN-Tx nifedipine (Pressolat, (Osmo)Adalat ) amlodipine (Norvasc, Amlow ) lercanidipine (Vasodip ) felodipine (Logimax )
50 CCBs - subclasses Non-dihydropyridines arrhythmia, IHD verapamil (Ikacor /Ikapress, Veracor /Verapress ) (phenylalkylamine - negative inotropic, minimally vasodilating) diltiazem (Dilatam /Dilapress /Adizam ) (benzothiazepine - intermediate inotrpic/vasodilator) relative affinity to nifedipine diltiazem verapamil cardiac Ca ++ channels vascular Ca ++ channels

51 CCBs - mechanism myocardial and smooth muscle cells dihydropyridine CCB administration artery dilation peripheral resistance intracellular calcium blood pressure muscle contraction
52 CCBs - ADEs hypotension constipation fatigue headache peripheral and pulmonary edema
53 CCBs - DDIs nifedipine - with many drugs: - H 2 blockers, omeprazole - antimicrobials (ciprofloxacin, macrolides, azoles) - levodopa - metoprolol - antieplipetic drugs (phenytoin, valproic acid, phenobarbital) - digoxin less with newer dihydropyridines (amlodipine)
54 CCBs - DDIs diltiazem - with many drugs: - amiodarone - β-blockers - azole antifungals, macrolides, ciprofloxacin - metoprolol - statins - digoxin - antieplipetic drugs (phenytoin, valproic acid, phenobarbital) - grapefruit juice
55 CCBs - DDIs verapamil - with many drugs: - amiodarone - β-blockers - azole antifungals, erythromycin - lithium - statins - digoxin - theophylline - grapefruit juice
56 CCBs - therapeutic considerations intrinsic natriuretic effect (no diuretic required) generally safe in asthma, diabetes, IHD may be effective as monotherapy avoid verapamil in CHF additional benefit: certain arrhythmias
57 Therapeutic options: Diuretics β-blockers α 1 -blockers Calcium-channel blockers RAAS modifiers Other

58 RAAS modifiers
59 RAAS modifiers - ACEIs captopril (Aceril ) enalapril (Convertin, Enaladex ) cilazapril (Vascace, Cilaril ) ramipril (Tritace, Ramitens ) lisinopril (Tensopril ) moexipril (Perdix ) benazepril (Cibacen ) 59 fixed combinations with HCTZ
60 RAAS modifiers - ACEIs 60
61 RAAS modifiers - ACEIs angiotensin-converting enzyme angiotensin-i ACEIs other enzymes vasoconstriction angiotensin-ii aldosterone bradykinin 61 water retention sodium retention vasoconstriction
62 RAAS modifiers - ACEIs angiotensin-converting enzyme angiotensin-i ACEIs other enzymes vasoconstriction angiotensin-ii aldosterone bradykinin 62 water retention sodium retention vasoconstriction
63 RAAS modifiers - ACEIs CO increased: bradykinin, aldosterone, epinephrine water and sodium retention BP vascular resistance 63
64 RAAS modifiers - ACEIs PK: adequate oral absorption (empty stomach) most ACEIs are prodrugs (hepatic activation) PK T 1/2-2-12hr; PD - longer for most ACEIs: renal elimination 64

 dry cough (20%)")
65 RAAS modifiers - ACEIs ADEs: postural hypotn renal impairment angioedema (0.13%) dry cough (20%) bradykinin hyperkalemia 65
66 RAAS modifiers - ACEIs DDIs: potassium-sparing agents, potassium supplements hypoglycemics (improved insulin sensitivity) NSAIDs (vasoconstriction, renal effect) lithium (decreased renal clearance of Li) 66
67 RAAS modifiers - ACEIs additional benefits: HF diabetes post-mi proteinuric chronic renal failure 67
68 RAAS modifiers - ARBs (ATRAs) losartan (Ocsaar, Lotan ) valsartan (Diovan ) candesartan (Atacand ) olmesartan (Olmetec ) fixed combinations with HCTZ 68
69 RAAS modifiers - ARBs (ATRAs) 69

70 RAAS modifiers - ARBs (ATRAs) angiotensin-i angiotensin-converting enzyme other enzymes vasoconstriction angiotensin-ii ARBs aldosterone bradykinin 70 water retention sodium retention vasoconstriction
71 RAAS modifiers - ARBs (ATRAs) advantages over ACEIs: more complete angiotensin-ii blockade no effect on bradykinin 71
72 RAAS modifiers - ARBs (ATRAs) PK: good oral absorption long T 1/2, once-daily administration combined renal-fecal elimination 72
73 RAAS modifiers - ARBs (ATRAs) ADEs: generally similar to those of ACEIs cough ( ) angioedema 73
74 RAAS modifiers - ARBs (ATRAs) DDIs - similar to those of ACEIs: potassium-sparing agents, potassium supplements hypoglycemics (improved insulin sensitivity) NSAIDs (vasoconstriction, renal effect) lithium (decreased renal clearance of Li) 74
75 RAAS modifiers - ARBs (ATRAs) additional benefits similar to those of ACEIs: HF diabetes post-mi proteinuric chronic renal failure 75
76 RAAS modifiers - aldosterone antagonist spironolactone (Aldospirone ) potassium-sparing diuretic not as monotherapy for HTN (excessive fluid retention, reflex tachycardia) hyperkalemia, hyponatremia, gynecomastia might decrease effect of digoxin (hyperkalemia) additional benefit - CHF 76
77 Therapeutic options: Diuretics β-blockers α 1 -blockers Calcium-channel blockers RAAS modifiers Other
78 Centrally-acting adrenergic drugs 1. clonidine (Normopressan ) α 2 -agonist inhibition of adrenergic activity BP devoid of renal effect H 2 O, Na + retention: combine with diuretic sedation, nasal dryness gradual tapering-off (rebound)
79 Centrally-acting adrenergic drugs 2. α-methyl dopa (Aldomin ) methylnorepinephrine prodrug, centrally active inhibition of adrenergic activity TPR, BP CO and organ blood supply unchanged devoid of renal effects sedation, drowsiness, dry mouth, impaired LFTs 1 st choice in pregnancy
80 Direct vasodilators smooth muscle relaxation peripheral resistance BP
81 Direct vasodilators 1. hydralazine most active in arteries, peripheral resistance non-teratogenic ADEs: nausea, sweating, lupus-like syndrome (rare) devoid of renal effect H 2 O, Na + retention: combine with diuretic

82 Direct vasodilators 2. minoxidil mainly active in arteries for Tx of refractory HTN ADEs: severe reflex tachycardia, peripheral edema; hair growth
83 Direct vasodilators β-blocker renin activity smooth muscle relaxation peripheral resistance cardiac activity H 2 O, Na + retention BP BP HR, O 2 demand diuretic
84 JNC-7 guidelines 2003

85 JNC-7 guidelines 2003 Widely accepted 1 st line therapy: low-dose HCTZ change drug? goal unmet? increase dose? add 2 nd drug?
86 JNC-7 guidelines 2003 thiazide-type diuretics should be initial drug therapy for most, either alone or combined with other drug classes. certain high-risk conditions are compelling indications for other drug classes. most patients will require two or more antihypertensive drugs to achieve goal BP. if BP is >20/10 mmhg above goal, initiate therapy with two agents, one usually should be a thiazide-type diuretic.
87 JNC-7 guidelines 2003 Lifestyle Modifications Not at Goal Blood Pressure (<140/90 mmhg) (<130/80 mmhg for those with diabetes or chronic kidney disease) Initial Drug Choices Without Compelling Indications With Compelling Indications Stage 1 HTN: (SBP or DBP mmhg): Thiazide-type diuretics for most. May consider ACEI, ARB, BB, CCB, or combination. Stage 2 HTN (SBP >160 or DBP >100 mmhg): 2-drug combination for most (usually thiazide + ACEI/ARB/BB/CCB) Not at Goal Blood Pressure Bi-functional drugs: (diuretics, ACEI, ARB, BB, CCB) as needed. Optimize dosages or add additional drugs until goal blood pressure is achieved. Consider consultation with HTN specialist.

88 JNC-7 guidelines 2003
89 JNC-7 guidelines 2003 Potential favorable effects of HTN-Tx: thiazide-type diuretics useful in slowing demineralization in osteoporosis. BBs useful in the treatment of atrial tachyarrhythmias/fibrillation, migraine, thyrotoxicosis (short-term), essential tremor, or perioperative HTN. CCBs useful in Raynaud s syndrome and certain arrhythmias. α-blockers useful in prostatism.
90 JNC-7 guidelines 2003 Potential unfavorable effects of HTN-Tx: thiazide diuretics should be used cautiously in gout or a history of significant hyponatremia. BBs should be generally avoided in patients with asthma, reactive airways disease, or second- or third-degree heart block. ACEIs and ARBs: C/I in pregnancy ACEIs should not be used with a history of angioedema. aldosterone antagonists and K + -sparing diuretics can cause hyperkalemia.
adherence issues JNC-8")
91 JNC-7 guidelines 2003 (non)adherence issues JNC-8 expected release: 2011
92
93 Current trends Outcomes dependent on achieved BP reduction regardless of therapeutic class beta-blockers less preferred, unless additional indication newer CCBs and RAAS modifiers appealing due to effectiveness, convenience and safety
94 Discontinuation of antihypertensive Tx When to D/C? well-controlled, mild HTN lifestyle modifications importance of patient characteristics
95 Discontinuation of antihypertensive Tx How to D/C? gradual withdrawal preferred abrupt cessation of short-acting β-blockers (propranolol) and α 2 -agonists (clonidine) might cause a fatal withdrawal syndrome these should therefore be tapered-off over weeks
96 - hypertension DRUGS FOR EXAM hydrochlorothiazide spironolactone propranolol metoprolol doxazosin amlodipine diltiazem verapamil enalapril losartan clonidine hydralazine α-methyl-dopa 96
7/7/ CHD/MI LVH and LV dysfunction Dysrrhythmias Stroke PVD Renal insufficiency and failure Retinopathy. Normal <120 Prehypertension
 Prevalence of Hypertension Hypertension: Diagnosis and Management T. Villela, M.D. Program Director University of California, San Francisco-San Francisco General Hospital Family and Community Medicine
Prevalence of Hypertension Hypertension: Diagnosis and Management T. Villela, M.D. Program Director University of California, San Francisco-San Francisco General Hospital Family and Community Medicine
Hypertension (JNC-8)
") Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
Antihypertensive drugs SUMMARY Made by: Lama Shatat
 Antihypertensive drugs SUMMARY Made by: Lama Shatat Diuretic Thiazide diuretics The loop diuretics Potassium-sparing Diuretics *Hydrochlorothiazide *Chlorthalidone *Furosemide *Torsemide *Bumetanide Aldosterone
Antihypertensive drugs SUMMARY Made by: Lama Shatat Diuretic Thiazide diuretics The loop diuretics Potassium-sparing Diuretics *Hydrochlorothiazide *Chlorthalidone *Furosemide *Torsemide *Bumetanide Aldosterone
Antihypertensive Agents Part-2. Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia
 Antihypertensive Agents Part-2 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Agents that block production or action of angiotensin Angiotensin-converting
Antihypertensive Agents Part-2 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Agents that block production or action of angiotensin Angiotensin-converting
Heart failure. Failure? blood supply insufficient for body needs. CHF = congestive heart failure. increased blood volume, interstitial fluid
 Failure? blood supply insufficient for body needs CHF = congestive heart failure increased blood volume, interstitial fluid Underlying causes/risk factors Ischemic heart disease (CAD) 70% hypertension
Failure? blood supply insufficient for body needs CHF = congestive heart failure increased blood volume, interstitial fluid Underlying causes/risk factors Ischemic heart disease (CAD) 70% hypertension
Section 3, Lecture 2
 59-291 Section 3, Lecture 2 Diuretics: -increase in Na + excretion (naturesis) Thiazide and Related diuretics -decreased PVR due to decreases muscle contraction -an economical and effective treatment -protect
59-291 Section 3, Lecture 2 Diuretics: -increase in Na + excretion (naturesis) Thiazide and Related diuretics -decreased PVR due to decreases muscle contraction -an economical and effective treatment -protect
Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs
 Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs Blood Pressure Normal = sys
Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs Blood Pressure Normal = sys
HYPERTENSION: Sustained elevation of arterial blood pressure above normal o Systolic 140 mm Hg and/or o Diastolic 90 mm Hg
 Lecture 39 Anti-Hypertensives B-Rod BLOOD PRESSURE: Systolic / Diastolic NORMAL: 120/80 Systolic = measure of pressure as heart is beating Diastolic = measure of pressure while heart is at rest between
Lecture 39 Anti-Hypertensives B-Rod BLOOD PRESSURE: Systolic / Diastolic NORMAL: 120/80 Systolic = measure of pressure as heart is beating Diastolic = measure of pressure while heart is at rest between
Management of Hypertension
 Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Antihypertensives. Antihypertensive Classes. RAAS Inhibitors. Renin-Angiotensin Cascade. Angiotensin Receptors. Approaches to Hypertension Treatment
 Approaches to Hypertension Treatment Antihypertensives Inhibit Sympathetic impulses Inhibit contractility Inhibit heart rate Inhibit vasoconstriction Inhibit smooth muscle function Inhibit RAAS Inhibit
Approaches to Hypertension Treatment Antihypertensives Inhibit Sympathetic impulses Inhibit contractility Inhibit heart rate Inhibit vasoconstriction Inhibit smooth muscle function Inhibit RAAS Inhibit
Hypertension Update. Objectives 4/28/2015. Beverly J. Mathis, D.O. OOA May 2015
 Hypertension Update Beverly J. Mathis, D.O. OOA May 2015 Objectives Learn new recommendations for BP treatment goals Approach to hypertension in the office Use of hypertensive drugs, and how to tailor
Hypertension Update Beverly J. Mathis, D.O. OOA May 2015 Objectives Learn new recommendations for BP treatment goals Approach to hypertension in the office Use of hypertensive drugs, and how to tailor
sympatholytics sympatholytics sympatholytics
 sympatholytics sympatholytics sympatholytics CNS-ACTING SYMPATHOPLEGICS Sympathetic brain signals Doesn t affect baroreceptor reflex (no orthostatic hypotension) Methyldopa α-methylne crosses BBB (+) α-adrenoreceptors
sympatholytics sympatholytics sympatholytics CNS-ACTING SYMPATHOPLEGICS Sympathetic brain signals Doesn t affect baroreceptor reflex (no orthostatic hypotension) Methyldopa α-methylne crosses BBB (+) α-adrenoreceptors
Chapter 23. Media Directory. Cardiovascular Disease (CVD) Hypertension: Classified into Three Categories
 Hypertension: Classified into Three Categories") Chapter 23 Drugs for Hypertension Slide 37 Slide 41 Media Directory Nifedipine Animation Doxazosin Animation Upper Saddle River, New Jersey 07458 All rights reserved. Cardiovascular Disease (CVD) Includes
Chapter 23 Drugs for Hypertension Slide 37 Slide 41 Media Directory Nifedipine Animation Doxazosin Animation Upper Saddle River, New Jersey 07458 All rights reserved. Cardiovascular Disease (CVD) Includes
Introduction. Factors affecting blood pressure: 1-COP = HR X SV mainly affect SBP. 2-TPR = diameter of arterioles X viscosity of blood affect DBP
 Introduction Hypertension is a persistent elevation of blood pressure above 140 / 90 mmhg for more than three sitting. (0ptimal level
Introduction Hypertension is a persistent elevation of blood pressure above 140 / 90 mmhg for more than three sitting. (0ptimal level
Hypertension Update. Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy
 Hypertension Update Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy Introduction 1/3 of US adults have HTN More prevalent in non-hispanic
Hypertension Update Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy Introduction 1/3 of US adults have HTN More prevalent in non-hispanic
Towards a Greater Understanding of Cardiac Medications Foundational Cardiac Concepts That Must Be Understood:
 Towards a Greater Understanding of Cardiac Medications Foundational Cardiac Concepts That Must Be Understood: Cardiac Output (CO) CO=SVxHR (stroke volume x heart rate) Cardiac output: The amount of blood
Towards a Greater Understanding of Cardiac Medications Foundational Cardiac Concepts That Must Be Understood: Cardiac Output (CO) CO=SVxHR (stroke volume x heart rate) Cardiac output: The amount of blood
What in the World is Functional Medicine?
 What in the World is Functional Medicine? An Introduction to a Systems Based Approach of Chronic Disease Meneah R Haworth, FNP-C Disclosure v I am a student of the Institute for Functional Medicine. They
What in the World is Functional Medicine? An Introduction to a Systems Based Approach of Chronic Disease Meneah R Haworth, FNP-C Disclosure v I am a student of the Institute for Functional Medicine. They
Heart Failure (HF) Treatment
 Treatment") Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
HypertensionTreatment Guidelines. Michaelene Urban APRN, MSN, ACNS-BC, ANP-BC
 HypertensionTreatment Guidelines Michaelene Urban APRN, MSN, ACNS-BC, ANP-BC Objectives: Review the definition of the different stages of HTN. Review the current guidelines for treatment of HTN. Provided
HypertensionTreatment Guidelines Michaelene Urban APRN, MSN, ACNS-BC, ANP-BC Objectives: Review the definition of the different stages of HTN. Review the current guidelines for treatment of HTN. Provided
Antihypertensives. Diagnostic category
 Measurement of blood pressure At first assessment, take both arms then choose the one with the higher reading. Beware of orthostatic hypotension. Measure BP in sitting position, and repeat after patient
Measurement of blood pressure At first assessment, take both arms then choose the one with the higher reading. Beware of orthostatic hypotension. Measure BP in sitting position, and repeat after patient
Chapter 10 Worksheet Blood Pressure and Antithrombotic Agents
 Complete the following. 1. A layer of cells lines each vessel in the vascular system. This layer is a passive barrier that keeps cells and proteins from going into tissues; it also contains substances
Complete the following. 1. A layer of cells lines each vessel in the vascular system. This layer is a passive barrier that keeps cells and proteins from going into tissues; it also contains substances
Hypertension. Penny Mosley MRPharmS
 Hypertension Penny Mosley MRPharmS Outline of presentation Introduction to hypertension Physiological control of arterial blood pressure What determines our bp? What determines the heart rate? What determines
Hypertension Penny Mosley MRPharmS Outline of presentation Introduction to hypertension Physiological control of arterial blood pressure What determines our bp? What determines the heart rate? What determines
Heart Failure Clinician Guide JANUARY 2018
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Hypertension CHAPTER-I CARDIOVASCULAR SYSTEM. Dr. K T NAIK Pharm.D Associate Professor Department of Pharm.D Krishna Teja Pharmacy College, Tirupati
 CHAPTER-I CARDIOVASCULAR SYSTEM Hypertension SUB: PHARMACOTHERAPEUTICS-I CODE:T0820006 Dr. K T NAIK Pharm.D Associate Professor Department of Pharm.D Krishna Teja Pharmacy College, Tirupati Hypertension
CHAPTER-I CARDIOVASCULAR SYSTEM Hypertension SUB: PHARMACOTHERAPEUTICS-I CODE:T0820006 Dr. K T NAIK Pharm.D Associate Professor Department of Pharm.D Krishna Teja Pharmacy College, Tirupati Hypertension
Hypertension Update Warwick Jaffe Interventional Cardiologist Ascot Hospital
 Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
Byvalson. (nebivolol, valsartan) New Product Slideshow
 New Product Slideshow") Byvalson (nebivolol, valsartan) New Product Slideshow Introduction Brand name: Byvalson Generic name: Nebivolol, valsartan Pharmacological class: Beta-blocker + angiotensin II receptor blocker (ARB) Strength
Byvalson (nebivolol, valsartan) New Product Slideshow Introduction Brand name: Byvalson Generic name: Nebivolol, valsartan Pharmacological class: Beta-blocker + angiotensin II receptor blocker (ARB) Strength
Beta 1 Beta blockers A - Propranolol,
 Pharma Lecture 3 Beta blockers that we are most interested in are the ones that target Beta 1 receptors. Beta blockers A - Propranolol, it s a non-selective competitive antagonist of beta 1 and beta 2
Pharma Lecture 3 Beta blockers that we are most interested in are the ones that target Beta 1 receptors. Beta blockers A - Propranolol, it s a non-selective competitive antagonist of beta 1 and beta 2
1. Antihypertensive agents 2. Vasodilators & treatment of angina 3. Drugs used in heart failure 4. Drugs used in arrhythmias
 1. Antihypertensive agents 2. Vasodilators & treatment of angina 3. Drugs used in heart failure 4. Drugs used in arrhythmias Only need to know drugs discussed in class At the end of this section you should
1. Antihypertensive agents 2. Vasodilators & treatment of angina 3. Drugs used in heart failure 4. Drugs used in arrhythmias Only need to know drugs discussed in class At the end of this section you should
Antihypertensive drugs: I. Thiazide and other diuretics:
 Clinical assessment of hypertensive patient: You have to take history regarding the presence of other risk factors for CAb like diabetes mellitus, smoking, etc. Take history whether the patient takes medications
Clinical assessment of hypertensive patient: You have to take history regarding the presence of other risk factors for CAb like diabetes mellitus, smoking, etc. Take history whether the patient takes medications
Antihypertensive Agents
 Antihypertensive Agents Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 7, 08, presented by Ezra Levy, Pharm.D! Usual Dose,
Antihypertensive Agents Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 7, 08, presented by Ezra Levy, Pharm.D! Usual Dose,
Hypertension Management - Summary
 Who should have blood pressure assessed? Hypertension Management - Summary All patients over the age of 40 years, every 1-3 years in order to determine their cardiovascular risk (ie. Framingham Risk Score)
Who should have blood pressure assessed? Hypertension Management - Summary All patients over the age of 40 years, every 1-3 years in order to determine their cardiovascular risk (ie. Framingham Risk Score)
Managing Hypertension in Diabetes Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park.
 Managing Hypertension in Diabetes 2015 Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park Case Scenario Mike M is a 59 year old man with type 2 diabetes managed
Managing Hypertension in Diabetes 2015 Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park Case Scenario Mike M is a 59 year old man with type 2 diabetes managed
Heart Failure Clinician Guide JANUARY 2016
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Management of Hypertension. M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine
 Division of Nephrology University of Missouri School of Medicine") Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
By Prof. Khaled El-Rabat
 What is The Optimum? By Prof. Khaled El-Rabat Professor of Cardiology - Benha Faculty of Medicine HT. Introduction Despite major worldwide efforts over recent decades directed at diagnosing and treating
What is The Optimum? By Prof. Khaled El-Rabat Professor of Cardiology - Benha Faculty of Medicine HT. Introduction Despite major worldwide efforts over recent decades directed at diagnosing and treating
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005
 VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
Difficult to Treat Hypertension
 Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Treatment of Essential Hypertension
 2016 edition by Mark A. Simmons, PhD Department of Pharmaceutical Sciences School of Pharmacy University of Maryland Eastern Shore Originally developed by Hugh J. Burford, PhD, FCP Department of Pharmacology
2016 edition by Mark A. Simmons, PhD Department of Pharmaceutical Sciences School of Pharmacy University of Maryland Eastern Shore Originally developed by Hugh J. Burford, PhD, FCP Department of Pharmacology
Managing Hypertension in 2016
 Managing Hypertension in 2016: Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
Managing Hypertension in 2016: Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
HYPERTENSION IN EMERGENCY MEDICINE Michael Jay Bresler, M.D., FACEP
 HYPERTENSION IN EMERGENCY MEDICINE Michael Jay Bresler, M.D., FACEP What is normal blood pressure? Prehypertension 130-139/80-90 Compared with normal BP Double the risk for developing hypertension. Lifestyle
HYPERTENSION IN EMERGENCY MEDICINE Michael Jay Bresler, M.D., FACEP What is normal blood pressure? Prehypertension 130-139/80-90 Compared with normal BP Double the risk for developing hypertension. Lifestyle
8/20/2018. Objectives. What is hypertension? cont. What is hypertension? Epidemiology cont. Epidemiology
 Objectives Hypertension (high blood pressure): Clinical Pearls for the Pharmacy Technician Tanya Schmidt PharmD, RPh Director of Central Operations at Thrifty White Pharmacy North Dakota Board of Pharmacy
Objectives Hypertension (high blood pressure): Clinical Pearls for the Pharmacy Technician Tanya Schmidt PharmD, RPh Director of Central Operations at Thrifty White Pharmacy North Dakota Board of Pharmacy
Treatment of Essential Hypertension
 2016 edition by Mark A. Simmons, PhD Department of Pharmaceutical Sciences School of Pharmacy University of Maryland Eastern Shore Originally developed by Hugh J. Burford, PhD, FCP Department of Pharmacology
2016 edition by Mark A. Simmons, PhD Department of Pharmaceutical Sciences School of Pharmacy University of Maryland Eastern Shore Originally developed by Hugh J. Burford, PhD, FCP Department of Pharmacology
Antihypertensive Agents
 Antihypertensive Agents Öner Süzer www.onersuzer.com osuzer@istanbul.edu.tr Last update: 13.11.2009 1 Süzer Farmakoloji 3. Baskı 2005 2 1 Süzer Farmakoloji 3. Baskı 2005 3 Süzer Farmakoloji 3. Baskı 2005
Antihypertensive Agents Öner Süzer www.onersuzer.com osuzer@istanbul.edu.tr Last update: 13.11.2009 1 Süzer Farmakoloji 3. Baskı 2005 2 1 Süzer Farmakoloji 3. Baskı 2005 3 Süzer Farmakoloji 3. Baskı 2005
Pharmacologic Management of Hypertension
 Current Concepts In Management of Fernando Vega, MD Secondary - Definition Renovascular Disease (The kidney doesn t get impressed by blood pressure) Renovascular stenosis Renal artery stenosis Fibromuscular
Current Concepts In Management of Fernando Vega, MD Secondary - Definition Renovascular Disease (The kidney doesn t get impressed by blood pressure) Renovascular stenosis Renal artery stenosis Fibromuscular
Dr Narender Goel MD (Internal Medicine and Nephrology) Financial Disclosure: None, Conflict of Interest: None
 Financial Disclosure: None, Conflict of Interest: None") Dr Narender Goel MD (Internal Medicine and Nephrology) drnarendergoel@gmail.com Financial Disclosure: None, Conflict of Interest: None 12 th December 2013, New York Visit us at: http://kidneyscience.info/
Dr Narender Goel MD (Internal Medicine and Nephrology) drnarendergoel@gmail.com Financial Disclosure: None, Conflict of Interest: None 12 th December 2013, New York Visit us at: http://kidneyscience.info/
MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure. No relevant financial relationships. Blood Pressure and Risk
 MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
HEART FAILURE PHARMACOLOGY. University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D
 HEART FAILURE PHARMACOLOGY University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 1 LEARNING OBJECTIVES Understand the effects of heart failure in the body
HEART FAILURE PHARMACOLOGY University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 1 LEARNING OBJECTIVES Understand the effects of heart failure in the body
Categories of HTN. Overview of Hypertension. Types of Hypertension
 Categories of HTN Overview of Hypertension Normal SBP 100 Quick review of the Basics: What is
Categories of HTN Overview of Hypertension Normal SBP 100 Quick review of the Basics: What is
University of Al Qadisiyah College of Pharmacy Dr. Bassim I Mohammad, MBChB, MSc, Ph.D
 University of Al Qadisiyah College of Pharmacy Dr. Bassim I Mohammad, MBChB, MSc, Ph.D Cardiovascular Pharmacology 1. Antihypertensives 2. Antianginal 3. Drugs for HF 4. Antiarrythemics 5. Drugs for Hyperlipoproteniemia
University of Al Qadisiyah College of Pharmacy Dr. Bassim I Mohammad, MBChB, MSc, Ph.D Cardiovascular Pharmacology 1. Antihypertensives 2. Antianginal 3. Drugs for HF 4. Antiarrythemics 5. Drugs for Hyperlipoproteniemia
Hypertension Pharmacotherapy: A Practical Approach
 Hypertension Pharmacotherapy: A Practical Approach Ronald Victor, MD Burns & Allen Chair in Cardiology Director, The Hypertension Center Associate Director, The Heart Institute Hypertension Center 1. 2.
Hypertension Pharmacotherapy: A Practical Approach Ronald Victor, MD Burns & Allen Chair in Cardiology Director, The Hypertension Center Associate Director, The Heart Institute Hypertension Center 1. 2.
STANDARD treatment algorithm mmHg
 STANDARD treatment algorithm 130-140mmHg (i) At BASELINE, If AVERAGE SBP 1 > 140mmHg If on no antihypertensive drugs: Start 1 drug: If >55 years old / Afro-Caribbean: Calcium channel blocker (CCB) 2 If
STANDARD treatment algorithm 130-140mmHg (i) At BASELINE, If AVERAGE SBP 1 > 140mmHg If on no antihypertensive drugs: Start 1 drug: If >55 years old / Afro-Caribbean: Calcium channel blocker (CCB) 2 If
TREATMENT OF HYPERTENSION
 TREATMENT OF HYPERTENSION Aim of treatment BP Goals Main items of treatment Lifestyle modification When to start drug Rx Pharmacological therapy 1. Relief of symptoms 2. Prevention of complications and
TREATMENT OF HYPERTENSION Aim of treatment BP Goals Main items of treatment Lifestyle modification When to start drug Rx Pharmacological therapy 1. Relief of symptoms 2. Prevention of complications and
Preventing and Treating High Blood Pressure
 Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
Combination Therapy for Hypertension
 Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
LESSON ASSIGNMENT. After completing this lesson you will be able to:
 LESSON ASSIGNMENT SUBCOURSE MD0806 LESSON 7 Therapeutics III. Antihypertensive Agents. LESSON ASSIGNMENT Paragraphs 7-1--7-12. LESSON OBJECTIVES After completing this lesson you will be able to: 7-1. From
LESSON ASSIGNMENT SUBCOURSE MD0806 LESSON 7 Therapeutics III. Antihypertensive Agents. LESSON ASSIGNMENT Paragraphs 7-1--7-12. LESSON OBJECTIVES After completing this lesson you will be able to: 7-1. From
DRUGS USED TO TREAT HYPERTENSION BY ALI ALALAWI
 DRUGS USED TO TREAT HYPERTENSION BY ALI ALALAWI 3. Vasodilators Drugs which dilate blood vessels ( decrease peripheral vascular resistance) by acting on smooth muscle cells through non-autonomic mechanisms:
DRUGS USED TO TREAT HYPERTENSION BY ALI ALALAWI 3. Vasodilators Drugs which dilate blood vessels ( decrease peripheral vascular resistance) by acting on smooth muscle cells through non-autonomic mechanisms:
ANTI- HYPERTENSIVE AGENTS
 CLINICAL ANTI- HYPERTENSIVE AGENTS Jacqueline van Schoor, MPharm, BSc (Hons) Amayeza Info Centre Hypertension represents a major public health concern. It affects about a billion people worldwide and is
CLINICAL ANTI- HYPERTENSIVE AGENTS Jacqueline van Schoor, MPharm, BSc (Hons) Amayeza Info Centre Hypertension represents a major public health concern. It affects about a billion people worldwide and is
DRUG CLASSES BETA-ADRENOCEPTOR ANTAGONISTS (BETA-BLOCKERS)
") DRUG CLASSES BETA-ADRENOCEPTOR ANTAGONISTS (BETA-BLOCKERS) Beta-blockers have been widely used in the management of angina, certain tachyarrhythmias and heart failure, as well as in hypertension. Examples
DRUG CLASSES BETA-ADRENOCEPTOR ANTAGONISTS (BETA-BLOCKERS) Beta-blockers have been widely used in the management of angina, certain tachyarrhythmias and heart failure, as well as in hypertension. Examples
Adult Blood Pressure Clinician Guide June 2018
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Adult Blood Pressure Clinician Guide June 2018 Adult Blood Pressure Clinician Guide June 2018 Introduction This Clinician Guide is based on the 2018
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Adult Blood Pressure Clinician Guide June 2018 Adult Blood Pressure Clinician Guide June 2018 Introduction This Clinician Guide is based on the 2018
Combining Antihypertensives in People with Diabetes
 Combining ntihypertensives in People with Diabetes The majority of people with diabetes will develop hypertension and this subsequently increases the risk of microvascular and macrovascular complications.
Combining ntihypertensives in People with Diabetes The majority of people with diabetes will develop hypertension and this subsequently increases the risk of microvascular and macrovascular complications.
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Top 200 Section 4. Cardiovascular Drugs
 Top 200 Section 4 Cardiovascular Drugs Objectives After finishing this presentation the audience should be able to: Describe conditions/disease states that would make a person a candidate for drug therapy.
Top 200 Section 4 Cardiovascular Drugs Objectives After finishing this presentation the audience should be able to: Describe conditions/disease states that would make a person a candidate for drug therapy.
ANTIHYPERTENSIVES. Assoc. Prof. Bilgen Başgut
 ANTIHYPERTENSIVES Assoc. Prof. Bilgen Başgut Hypertension Hypertension is a condition in which the blood pressure is persistently higher than normal Hypertension > 140 mmhg > 90 mmhg Systolic Blood Pressure
ANTIHYPERTENSIVES Assoc. Prof. Bilgen Başgut Hypertension Hypertension is a condition in which the blood pressure is persistently higher than normal Hypertension > 140 mmhg > 90 mmhg Systolic Blood Pressure
Chapter (9) Calcium Antagonists
 Calcium Antagonists") Chapter (9) Calcium Antagonists (CALCIUM CHANNEL BLOCKERS) Classification Mechanism of Anti-ischemic Actions Indications Drug Interaction with Verapamil Contraindications Adverse Effects Treatment of Drug
Chapter (9) Calcium Antagonists (CALCIUM CHANNEL BLOCKERS) Classification Mechanism of Anti-ischemic Actions Indications Drug Interaction with Verapamil Contraindications Adverse Effects Treatment of Drug
Hypertension. Risk of cardiovascular disease beginning at 115/75 mmhg doubles with every 20/10mm Hg increase. (Grade B)
") Practice Guidelines and Principles: Guidelines and principles are intended to be flexible. They serve as reference points or recommendations, not rigid criteria. Guidelines and principles should be followed
Practice Guidelines and Principles: Guidelines and principles are intended to be flexible. They serve as reference points or recommendations, not rigid criteria. Guidelines and principles should be followed
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Younger adults with a family history of premature artherosclerotic disease should have their cardiovascular risk factors measured.
 Appendix 2A - Guidance on Management of Hypertension Measurement of blood pressure All adults from 40 years should have blood pressure measured as part of opportunistic cardiovascular risk assessment.
Appendix 2A - Guidance on Management of Hypertension Measurement of blood pressure All adults from 40 years should have blood pressure measured as part of opportunistic cardiovascular risk assessment.
Hypertension and the Challenge of Adherence. Geneva Clark Briggs, Pharm.D., BCPS
 Hypertension and the Challenge of Adherence Geneva Clark Briggs, Pharm.D., BCPS Outline Brief overview of HTN and pharmacologic therapies Role of pharmacists in collaboration with patients and physicians
Hypertension and the Challenge of Adherence Geneva Clark Briggs, Pharm.D., BCPS Outline Brief overview of HTN and pharmacologic therapies Role of pharmacists in collaboration with patients and physicians
Management of Hypertension. Ahmed El Hawary MD Suez Canal University
 Management of Hypertension Ahmed El Hawary MD Suez Canal University Minimal vs. Optimal Care Resources more than science affect type of care and level of management. what is possible (minimal care) and
Management of Hypertension Ahmed El Hawary MD Suez Canal University Minimal vs. Optimal Care Resources more than science affect type of care and level of management. what is possible (minimal care) and
M2 TEACHING UNDERSTANDING PHARMACOLOGY
 M2 TEACHING UNDERSTANDING PHARMACOLOGY USING CVS SYSTEM AS AN EXAMPLE NIGEL FONG 2 JAN 2014 TODAY S OBJECTIVE Pharmacology often seems like an endless list of mechanisms and side effects to memorize. To
M2 TEACHING UNDERSTANDING PHARMACOLOGY USING CVS SYSTEM AS AN EXAMPLE NIGEL FONG 2 JAN 2014 TODAY S OBJECTIVE Pharmacology often seems like an endless list of mechanisms and side effects to memorize. To
Heart Failure. Subjective SOB (shortness of breath) Peripheral edema. Orthopnea (2-3 pillows) PND (paroxysmal nocturnal dyspnea)
 Peripheral edema. Orthopnea (2-3 pillows) PND (paroxysmal nocturnal dyspnea)") Pharmacology I. Definitions A. Heart Failure (HF) Heart Failure Ezra Levy, Pharm.D. HF Results when one or both ventricles are unable to pump sufficient blood to meet the body s needs There are 2 types
Pharmacology I. Definitions A. Heart Failure (HF) Heart Failure Ezra Levy, Pharm.D. HF Results when one or both ventricles are unable to pump sufficient blood to meet the body s needs There are 2 types
Hypertension Management Controversies in the Elderly Patient
 Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Modern Management of Hypertension: Where Do We Draw the Line?
 Modern Management of Hypertension: Where Do We Draw the Line? Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Blood Pressure
Modern Management of Hypertension: Where Do We Draw the Line? Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Blood Pressure
Network Hypertension Algorithm
 Network Hypertension Algorithm Content Review and Approval: This document is subject to review, revision, and (re)approval by the Clinical Integration and Oversight Committee (CIOC) annually and following
Network Hypertension Algorithm Content Review and Approval: This document is subject to review, revision, and (re)approval by the Clinical Integration and Oversight Committee (CIOC) annually and following
Hypertension Update 2009
 Hypertension Update 2009 New Drugs, New Goals, New Approaches, New Lessons from Clinical Trials Timothy C Fagan, MD, FACP Professor Emeritus University of Arizona New Drugs Direct Renin Inhibitors Endothelin
Hypertension Update 2009 New Drugs, New Goals, New Approaches, New Lessons from Clinical Trials Timothy C Fagan, MD, FACP Professor Emeritus University of Arizona New Drugs Direct Renin Inhibitors Endothelin
Heart Failure. Dr. Alia Shatanawi
 Heart Failure Dr. Alia Shatanawi Left systolic dysfunction secondary to coronary artery disease is the most common cause, account to 70% of all cases. Heart Failure Heart is unable to pump sufficient blood
Heart Failure Dr. Alia Shatanawi Left systolic dysfunction secondary to coronary artery disease is the most common cause, account to 70% of all cases. Heart Failure Heart is unable to pump sufficient blood
Lab Period: Name: Physiology Chapter 14 Blood Flow and Blood Pressure, Plus Fun Review Study Guide
 Lab Period: Name: Physiology Chapter 14 Blood Flow and Blood Pressure, Plus Fun Review Study Guide Main Idea: The function of the circulatory system is to maintain adequate blood flow to all tissues. Clinical
Lab Period: Name: Physiology Chapter 14 Blood Flow and Blood Pressure, Plus Fun Review Study Guide Main Idea: The function of the circulatory system is to maintain adequate blood flow to all tissues. Clinical
Modern Management of Hypertension
 Modern Management of Hypertension Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Hypertension Prevalence
Modern Management of Hypertension Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Hypertension Prevalence
4/3/2018 PHARMACOLOGICAL MANAGEMENT OF HYPERTENSION IN THE PATIENT WITH CKD TONI A. HARPS, APRN-CNS, MSN NEPHROLOGY WHY THIS TOPIC/OBJECTIVES
 PHARMACOLOGICAL MANAGEMENT OF HYPERTENSION IN THE PATIENT WITH CKD TONI A. HARPS, APRN-CNS, MSN NEPHROLOGY WHY THIS TOPIC/OBJECTIVES To identify Blood pressure (BP) medications which are used to manage
PHARMACOLOGICAL MANAGEMENT OF HYPERTENSION IN THE PATIENT WITH CKD TONI A. HARPS, APRN-CNS, MSN NEPHROLOGY WHY THIS TOPIC/OBJECTIVES To identify Blood pressure (BP) medications which are used to manage
2014 HYPERTENSION GUIDELINES
 2014 HYPERTENSION GUIDELINES Eileen M. Twomey, Pharm.D., BCPS 1 Learning Objectives Describe specific blood pressure thresholds at which antihypertensive therapy should be initiated and blood pressure
2014 HYPERTENSION GUIDELINES Eileen M. Twomey, Pharm.D., BCPS 1 Learning Objectives Describe specific blood pressure thresholds at which antihypertensive therapy should be initiated and blood pressure
Antihypertensive Drugs. Nafrialdi
 Antihypertensive Drugs Nafrialdi 1 Mechanisms of Blood Pressure Regulation Blood Presure Cardiac Output Peripheral Resistance Heart Rate Stroke volume Vascular tone Vessel elasticity Myocardial contractility
Antihypertensive Drugs Nafrialdi 1 Mechanisms of Blood Pressure Regulation Blood Presure Cardiac Output Peripheral Resistance Heart Rate Stroke volume Vascular tone Vessel elasticity Myocardial contractility
Prof dr Aleksandar Raskovic DIRECT VASODILATORS
 Prof dr Aleksandar Raskovic DIRECT VASODILATORS Direct vasodilators Minoxidil (one of the most powerful peripheral arterial dilators) Opening of KATP channels, efflux of K, lose of Ca and smooth muscle
Prof dr Aleksandar Raskovic DIRECT VASODILATORS Direct vasodilators Minoxidil (one of the most powerful peripheral arterial dilators) Opening of KATP channels, efflux of K, lose of Ca and smooth muscle
Jared Moore, MD, FACP
 Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Hypertension: Update
 Hypertension: Update Meenakshi A Bhalla MD,FACC Associate Professor of Medicine Director Preventive Cardiology Advanced Heart Failure and Transplant Cardiology University of Kentucky Faculty Disclosure
Hypertension: Update Meenakshi A Bhalla MD,FACC Associate Professor of Medicine Director Preventive Cardiology Advanced Heart Failure and Transplant Cardiology University of Kentucky Faculty Disclosure
Cardiovascular Clinical Practice Guideline Pilot Implementation
 Cardiovascular Clinical Practice Guideline Pilot Implementation Pharmacologic Management of Chronic Heart Failure Sept 15, 2004 Angela Allerman, PharmD, BCPS DoD Pharmacoeconomic Center Promoting high
Cardiovascular Clinical Practice Guideline Pilot Implementation Pharmacologic Management of Chronic Heart Failure Sept 15, 2004 Angela Allerman, PharmD, BCPS DoD Pharmacoeconomic Center Promoting high
Cardiovascular Pharmacotherapy
 Cardiovascular Pharmacotherapy Overview Mechanism of cardiovascular drugs Indications and clinical use in cardiology Renin-Angiotensin Inhibitors: Angiotensin-Converting Enzyme Inhibitors, Angiotensin
Cardiovascular Pharmacotherapy Overview Mechanism of cardiovascular drugs Indications and clinical use in cardiology Renin-Angiotensin Inhibitors: Angiotensin-Converting Enzyme Inhibitors, Angiotensin
Circulation. Blood Pressure and Antihypertensive Medications. Venous Return. Arterial flow. Regulation of Cardiac Output.
 Circulation Blood Pressure and Antihypertensive Medications Two systems Pulmonary (low pressure) Systemic (high pressure) Aorta 120 mmhg Large arteries 110 mmhg Arterioles 40 mmhg Arteriolar capillaries
Circulation Blood Pressure and Antihypertensive Medications Two systems Pulmonary (low pressure) Systemic (high pressure) Aorta 120 mmhg Large arteries 110 mmhg Arterioles 40 mmhg Arteriolar capillaries
Layered Approaches to Studying Drug Responses
 Layered Approaches to Studying Drug Responses Brian B Hoffman, MD Chief of Medicine VA Boston Health Care System Professor of Medicine Harvard Medical School Conflict of Interest: US Federal Grant Funding
Layered Approaches to Studying Drug Responses Brian B Hoffman, MD Chief of Medicine VA Boston Health Care System Professor of Medicine Harvard Medical School Conflict of Interest: US Federal Grant Funding
Pharmacology of the Sympathetic Nervous System II
 Pharmacology of the Sympathetic Nervous System II Edward JN Ishac, Ph.D. Professor Smith Building, Room 742 eishac@vcu.edu 828-2127 Department of Pharmacology and Toxicology Medical College of Virginia
Pharmacology of the Sympathetic Nervous System II Edward JN Ishac, Ph.D. Professor Smith Building, Room 742 eishac@vcu.edu 828-2127 Department of Pharmacology and Toxicology Medical College of Virginia
Update in Hypertension
 Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
LXIV: DRUGS: 4. RAS BLOCKADE
 LXIV: DRUGS: 4. RAS BLOCKADE ACE Inhibitors Components of RAS Actions of Angiotensin i II Indications for ACEIs Contraindications RAS blockade in hypertension RAS blockade in CAD RAS blockade in HF Limitations
LXIV: DRUGS: 4. RAS BLOCKADE ACE Inhibitors Components of RAS Actions of Angiotensin i II Indications for ACEIs Contraindications RAS blockade in hypertension RAS blockade in CAD RAS blockade in HF Limitations
Hypertension diagnosis (see detail document) Diabetic. Target less than 130/80mmHg
 Diabetic. Target less than 130/80mmHg") Hypertension diagnosis (see detail document) Non-diabetic Diabetic Very elderly (older than 80 years) Target less than 140/90mmHg Target less than 130/80mmHg Consider SBP target less than 150mmHg Non-diabetic
Hypertension diagnosis (see detail document) Non-diabetic Diabetic Very elderly (older than 80 years) Target less than 140/90mmHg Target less than 130/80mmHg Consider SBP target less than 150mmHg Non-diabetic
Hypertension: JNC-7. Southern California University of Health Sciences Physician Assistant Program
 Hypertension: JNC-7 Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! Reference Card
Hypertension: JNC-7 Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! Reference Card
Angina pectoris due to coronary atherosclerosis : Atenolol is indicated for the long term management of patients with angina pectoris.
 Lonet Tablet Description Lonet contains Atenolol, a synthetic β1 selective (cardioselective) adrenoreceptor blocking agent without membrane stabilising or intrinsic sympathomimetic (partial agonist) activity.
Lonet Tablet Description Lonet contains Atenolol, a synthetic β1 selective (cardioselective) adrenoreceptor blocking agent without membrane stabilising or intrinsic sympathomimetic (partial agonist) activity.
HYPERTENSION IN CKD. LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL
 HYPERTENSION IN CKD LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL Stages in Progression of Chronic Kidney Disease and Therapeutic Strategies Complications Normal Increased risk Damage GFR
HYPERTENSION IN CKD LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL Stages in Progression of Chronic Kidney Disease and Therapeutic Strategies Complications Normal Increased risk Damage GFR
Explore the Rationale for the Dual Mechanism CCB/ARB Approach in Hypertension Management
 Explore the Rationale for the Dual Mechanism CCB/ARB Approach in Hypertension Management Jeong Bae Park, MD,PhD Dept of Med/Cardiology, Cheil General Hospital, Kwandong University College of Medicine Apr
Explore the Rationale for the Dual Mechanism CCB/ARB Approach in Hypertension Management Jeong Bae Park, MD,PhD Dept of Med/Cardiology, Cheil General Hospital, Kwandong University College of Medicine Apr
New classification of HT Systolic Diastolic Normal <120 <80 Prehypertension Stage1HT Stage 2 HT >160 or >100
 Hypertension 1 Definition Hypertension can be defined as a condition where blood pressure is elevated to an extent that clinical benefit is obtained from blood pressure lowering. it is an important risk
Hypertension 1 Definition Hypertension can be defined as a condition where blood pressure is elevated to an extent that clinical benefit is obtained from blood pressure lowering. it is an important risk
Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, Financial Disclosures
 Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, 2015 William C. Cushman, MD Professor, Preventive Medicine, Medicine, and Physiology University
Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, 2015 William C. Cushman, MD Professor, Preventive Medicine, Medicine, and Physiology University
1/4/18. Heart Failure Guideline Review and Update. Disclosure. Pharmacist Objectives. Pharmacy Technician Objectives. What is Heart Failure?
 Disclosure Heart Failure Guideline Review and Update I have had no financial relationship over the past 12 months with any commercial sponsor with a vested interest in this presentation. Natalie Beiter,
Disclosure Heart Failure Guideline Review and Update I have had no financial relationship over the past 12 months with any commercial sponsor with a vested interest in this presentation. Natalie Beiter,