Antihypertensive Agents
|
|
|
- Gordon Lindsey
- 5 years ago
- Views:
Transcription
1 Antihypertensive Agents Öner Süzer Last update: Süzer Farmakoloji 3. Baskı
2 Süzer Farmakoloji 3. Baskı Süzer Farmakoloji 3. Baskı
3 Süzer Farmakoloji 3. Baskı Hypertension Hypertension is a common and usually progressive disease, which if not effectively treated, results in a greatly increased probability of coronary arterial disease, thrombosis, strokes and renal failure. It is the most common cardiovascular disease!!! Keeping the blood pressure below 140/90 mm Hg (systolic/diastolic) reduces morbidity and mortality of these patients significantly. Personally hypertension is the story of tablets. 6 3
4 Diagnosis The diagnosis of hypertension is based on repeated reproducible measurements of elevated blood pressure. A specific cause of hypertension can be established in only 10-15% of patients: renal artery constriction, coarctation of the aorta, pheochromocytoma, Cushing s disease and primary aldosteronism. Patients in whom no specific cause of hypertension can be found are said to have essential hypertension. Elevated blood pressure is usually caused by a combination of several abnormalities (multifactorial): genetic inheritance, psychologic stress environmental and dietary factors (increased salt, perhaps decreased potassium or calcium intake). 7 Regulation of blood pressure BP= cardiac output peripheral vascular resistance In both normal and hypertensive individuals, blood pressure is maintained by moment-to-moment regulation of cardiac output and peripheral vascular resistance. 8 4

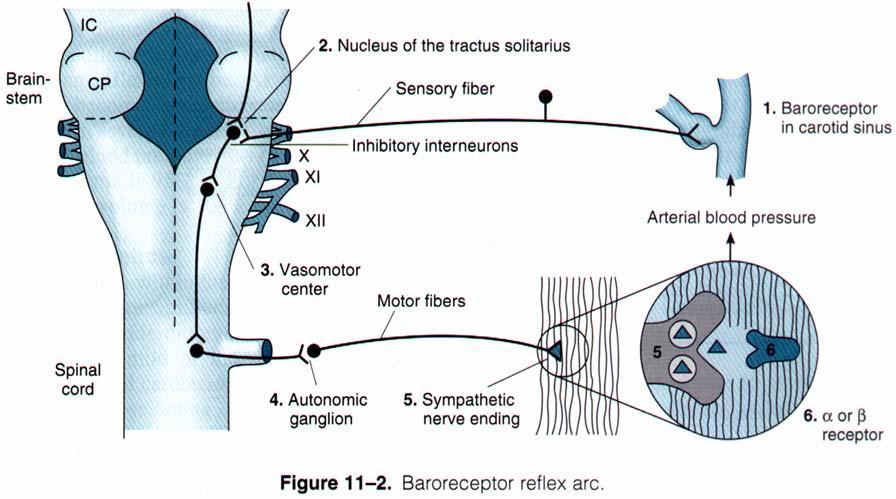
5 Anatomic sites of blood pressure control Arterioles (resistance) Venules (capacitance) Heart (pump output) Kidneys (volume). Baroreflexes that are controlled by autonomic nerve system and humoral mechanisms including renin-angiotensin-aldosteron system coordinate these anatomic sites. The difference between normal and hypertensive patients is that baroreceptors are set to higher levels

6 Basic pharmacology of antihypertensives Diuretics, which lower blood pressure by depleting the body of sodium and reducing blood volume and by vasodilation. Sympathoplegic agents, which lower blood pressure by reducing peripheral vascular resistance, inhibiting cardiac function and increasing venous pooling in capacitance vessels. Direct vasodilators, which reduce blood pressure by relating vascular smooth muscle. Agents that block production or action of angiotensin and thereby reduce peripheral vascular resistance and blood volume
7
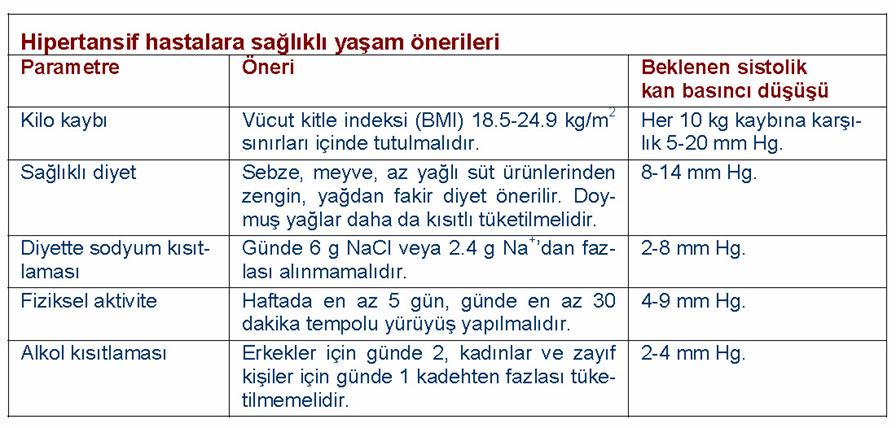
8 First line antihypertensive agents: ABCD Angiotensin antagonists Beta blockers Calcium channel blockers Diuretics 15 Diuretics I Dietary sodium restriction has been known for many years to decrease blood pressure in hypertensive patients. Dietary control of blood pressure is a relatively nontoxic therapeutic measure and may even be preventive. Diuretics lower blood pressure primarily by depleting body sodium stores. Initially they reduce blood pressure by reducing blood volume and cardiac output; peripheral vascular resistance may increase. After 6-8 weeks, cardiac output returns toward normal while peripheric vascular resistance declines. 16 8

9 Rang and dale s Pharmacology 6th Edition Diuretics II Sodium is believed to contribute to vascular resistance due to increases sodium-calcium exchange with a resultant increase in intracellular calcium. Some diuretics like indapamide have direct vasodilator properties. Amiloride inhibits effects of contractile impulses on vascular smooth muscle with a mechanism independent from its natriuretic effect, which is preventing transmembrane and intracellular calcium movements. 18 9
10 Diuretics III Diuretics are effective in lowering blood pressure by mm Hg in most patients and often provide adequate treatment for mild or moderate essential hypertension when used alone. In more severe hypertension diuretics are used in combination with sympathoplegic and vasodilator drugs to control the tendency toward sodium retention caused by these agents. For most patients thiazide diuretics are appropriate when renal and cardiac function is normal. 19 Diuretics IV More powerful diuretics (loop agents) are necessary in severe hypertension, renal insufficiency (GFR< ml/min), and in cardiac failure or cirrhosis where sodium retention is marked. Potassium-sparing diuretics are useful both to avoid excessive potassium depletion, particularly in patients taking digitalis and to enhance the natriuretic effects of other diuretics

11 Adverse effects The most common is potassium depletion, which is especially important in persons taking digitalis, those who have chronic arrhythmias or those with acute myocardial infarction. Restriction of sodium intake may minimize potassium loss. Diuretics may also cause magnesium depletion, impair glucose tolerance and increase serum lipid concentrations. They may increase uric acid concentration and precipitate gout

12 Sympathoplegic agents Centrally acting sympathoplegic agents Methyldopa Clonidine Ganglion blockers Trimethaphan Adrenergic neuron blockers Guanethidine Reserpine Pargyline Adrenergic receptor blockers α-blockers β-blockers
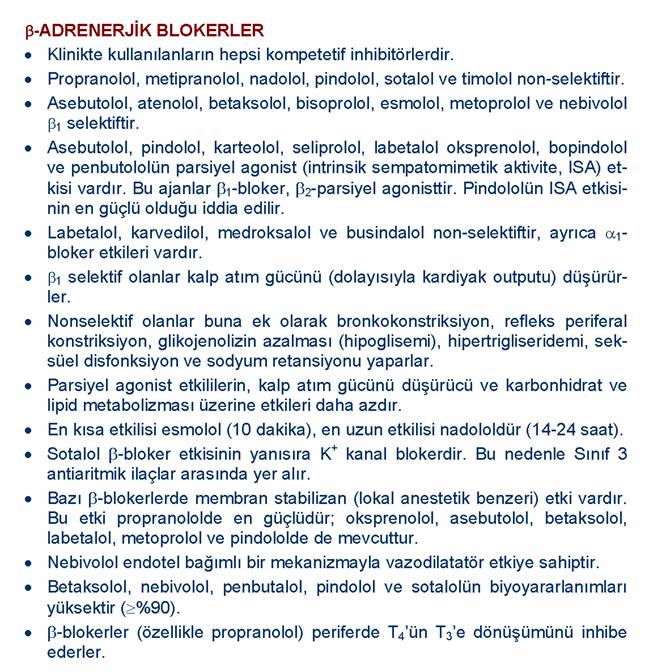
13 25 β-blockers Propranalol: It blocks both β 1 and β 2 receptors. It primarily decreases blood pressure as a result of a decrease in cardiac output. Beta blockade in brain, kidney and peripheral adrenergic neurons has been proposed as contributing to the antihypertensive effect. Propranolol inhibits the stimulation of renin production by catecholamines (β 1 mediated )
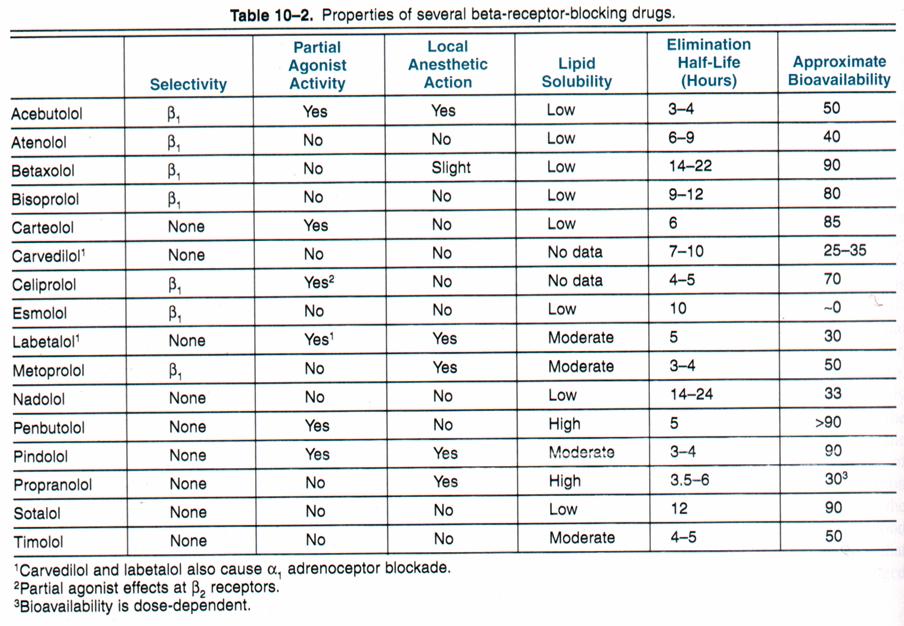
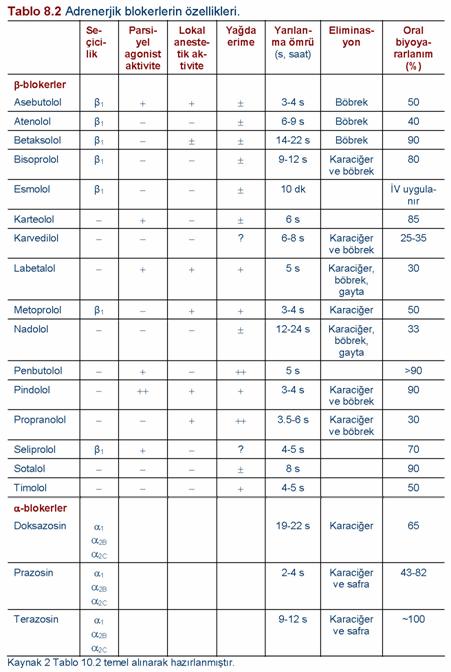
14 Propranolol (continued) It has significant first-pass hepatic inactivation. The principal toxicity occur in patients with reduced myocardial reserve, asthma, peripheral vascular insufficiency and diabetes when discontinued after prolonged use, some patients experience a withdrawal syndrome, manifested by nervousness, tachycardia, increased intensity of angina or increased blood pressure. It may increase plasma triglycerides and reduce HDL. 27 Other β-blocker agents I Metoprolol: It is approximately equipotent to propranolol in inhibiting stimulation of β 1 receptors, but 50 to 100 fold less potent than propranolol in blocking β 2 receptors. This relative cardioselectivity may be advantageous in patients who also suffer from asthma, diabetes or peripheral vascular disease. Nadolol and carteolol are also non-selective. They are not metabolized and are excreted in the urine
15 Other β-blocker agents II Atenolol is β 1 selective and not metabolized. Betaxolol and bisoprolol are β 1 selective, they are metabolized in the liver but their half-life is long. Pindolol, acetobutolol, penbutolol: They are partial agonists (i.e. ISA). Probably they have agonist activity on β 2 receptors rather than antagonism. 29 Other β-blocker agents III Labetalol and carvedilol: Labetalol has 4 stereoisomers. Two of these isomers are inactive, one β blocker and one α blocker. Carvedilol has 2 stereoisomers. S isomer α and β blocker R isomer α blocker. The combined α and β receptor blockade with labetalol makes it useful in pheochromocytoma and hypertensive emergencies. Preliminary studies suggest that carvedilol may be useful in some cases of congestive heart failure

16
17

18
19 α 1 blockers I Prazosin, terazosin, doxazosin: They are α 1 selective blockers. α 2 receptors are intact thus feedback mechanisms for noradrenalin remains intact and less reflex tachycardia is observed than nonselective α-blockers. They produce their antihypertensive effects by blocking α 1 receptors in arterioles and venules. The drugs are more effective when used in combination with other agents, such as a beta-blocker and a diuretic than when use alone. 37 α 1 blockers I Treatment should be initiated with a low dose to prevent postural hypotension and syncope administered at bedtime. Unlike diuretics and beta-blockers, the α 1 -blockers do not adversely and may even beneficially affect plasma lipid profiles. Other selective α 1 -blockers for antihypertensive use are: alfuzosin, tamsulosin, indoramin, and urapidil (it is also a weak α 2 -agonist, 5- HT 1A -agonist and weak β 1 antagonist)
20 Non-selective α-blockers Phentolamine and phenoxybenzamine are non-selective α-blockers. They are useful in diagnosis and treatment of pheochromocytoma and in other clinical situations associated with exaggerated release of catecholamines (eg. in clonidine withdrawal syndrome combined with propranolol). 39 Centrally acting sympathoplegic drugs I Methyldopa: It is an analog of L-dopa and is converted to α- methyldopamine and α-methylnorepinephrine, which are false transmitters. Methyldopa s antihypertensive action appears to be due to stimulation of central α 2 receptors. It may result in postural hypotension one of its advantage is that it decreases renal vascular resistance. Methyldopa is a pregnancy category B drug
21 Centrally acting sympathoplegic drugs II Clonidine is an α 2 and imidazoline receptor agonist. Its antihypertensive action is due to decrease in heart rate, and decrease in cardiac output because of relaxation of capacitance vessels. Renal vascular resistance also decreases. After clonidine application circulating catecholamine levels decrease (chemical sympatectomy). Guanabenz and guanfacine are centrally active antihypertensive agents that share the central alpha-adrenoceptor- stimulating effects of clonidine. 41 Ganglion-blocking agents They act by inhibiting the stimulating action of acetylcholine on postganglionic autonomic neurons. Trimethaphan: It is used intravenously in hypertensive crisis, acute aorta dissection and controlled hypotension in neurosurgery. It has rapid and short action
22 Adrenergic neuron blockers I These drugs decrease blood pressure by inhibiting the release of noradrenaline from sympathetic neurons. Guanethidine, bethanidine, debrisoquin: They are transported across membrane by uptake-1. They are concentrated in transmitter vesicles and cause gradual depletion of norepinephrine. Uptake-1 inhibitors such as cocaine, amphetamine, tricyclic antidepressants decrease their effects. They increase sensitivity to the hypertensive effects of exogenously administered sympathomimetic amines
23 Adrenergic neuron blockers II Reserpine: It blocks the ability of aminergic transmitter vesicles to take up and store biogenic amines. It was widely used previously. It may result in depression. It has no indication in modern antihypertensive therapy but found in the prescriptions of old doctors. Pargyline: It is a MAO inhibitor and is believed to increase the concentration of an ineffective false transmitter. It has no modern use. 45 Direct vasodilators Calcium channel blockers Hydralazine Minoxidil Sodium nitroprusside Diazoxide 46 23
24
25 Calcium channel blockers I They are blockers of L-type calcium channels. Verapamil: It is cardioselective. Dihydropyridines (amlodipine, felodipine, isradipine, nicardipine, nisoldipine): They are vascular smooth muscle selective. Diltiazem: Intermediate 49 Calcium channel blockers II Verapamil may decrease heart rate and cardiac output Dihydropyridines are minimally cardiodepressive with reflex sympathetic activations and mild tachycardia, cardiac output is preserved or even slightly increased. With the use of short acting nifedipine, there is an increase in MI and mortality. In the treatment of hypertension sustained release nifedipine preparations and drugs with long plasma half-life control blood pressure safely
26 Other direct vasodilators I Hydralazine: It relaxes arterioles but not veins. When used alone tachyphlaxis to hypertensive effects develops rapidly. With combination therapy it may be used particularly in severe hypertension. Its bioavailability is low. There is genetic variability for its metabolism. Dosage should be regulated according to individual responses. 51 Other direct vasodilators II Minoxidil: It is a very efficacious orally active vasodilator. Its effect results from the opening of potassium channels in smooth muscle membrane. It dilates arterioles like hydralazine. Clinical responses are better than hydralazine and particularly in renal failure it should be preferred. Topical minoxidil (Rogaine) is used as a stimulant to hair growth for correction of baldness. If it is not combined with a beta-blocker and a loop diuretic, sympathetic stimulation, angina, sodium and fluid retention may occur
27 Other direct vasodilators III Diazoxide: It is an effective and relatively long-acting parenterally administered arteriolar dilator. It opens potassium channels like minoxidil. Its antihypertensive effect initiates within 5 min. and lasts for 4-12 hours. It inhibits insulin release from pancreas and causes renal salt and water retention. 53 Other direct vasodilators IV Sodium nitroprusside: It is a powerful parenterally administered vasodilator that is used in treating hypertensive emergencies as well as severe cardiac failure. It dilates both arterioles and venules. The action occurs as a result of activation of guanylyl cyclase. The result is increased intracellular cgmp, which relates vascular smooth muscle
28 Sodium nitroprusside (continued) In the absence of cardiac failure, blood pressure decreases, owing to decreased vascular resistance, while cardiac output changes slightly. In patients with cardiac failure, cardiac output increases owing to afterload reduction. It is a complex of iron, cyanide groups. With infusions more than 10 μg/kg/min, cyanide toxicity occurs. metabolic acidosis, arrhythmia, hypotension, dead. Aqueus solution is sensitive to light. 55 Inhibitors of angiotensin Angiotensin converting enzyme (ACE) inhibitors Captopril and other drugs in this class inhibit the converting enzyme that hydrolyzes angiotensin I to angiotensin II. The same enzyme inactivates bradykinin a potent vasodilator that works at least in part by stimulating release of nitric oxide and prostacyclin. Angiotensin II is vasoconstrictor and has salt and water retaining activity via aldosteron secretion
29 57 ACE inhibitors I Captopril and lisinopril are orally active agents. Enapril is a prodrog and is converted to active form enaprilat in liver. Enaprilat is only available in IV form for hypertensive emergencies. Benazepril, fosinopril, moexepril, quinapril and ramipril are all prodrugs and hydrolyzed in liver to active forms
30 ACE inhibitors II ACE inhibitors decrease blood pressure by decreasing peripheral vascular resistance. Cardiac output and heart rate do not change significantly. As they do not cause reflex sympathetic activation, they are safe in patients with ischemic heart disease. The absence of reflex tachycardia may be due to downward resetting of the baroreceptors or to enhanced parasympathetic activity. 59 ACE inhibitors III They are particularly useful in treating patients with diabetic nephropathy, diminishing proteinuria and stabilizing renal function. They are also useful in congestive heart failure and after MI. All ACE inhibitors are excreted via kidneys except fosinopril and moexipril. In hypervolemic patients (due to diuretics, salt restriction, GI fluid loss), first doses may result in severe hypotension. Other adverse effects include acute renal failure, hyperkalemia, dry cough, sometimes wheezing and angioedema (dry cough and angioedema due to increased effects of bradykinin)
31 ACE inhibitors IV ACE inhibitors are contraindicated during the second and third trimesters of pregnancy because of the risk of fetal hypotension, anuria and renal failure, sometimes associated with fetal malformations or death. Potassium supplements or potassium sparing diuretics can result in hyperkalemia. NSAI drugs may impair hypotensive effects by blocking bradykininmediated vasodilation which is at least in part PG mediated. 61 Angiotensin receptor blockers (ARB) Losartan and valsartan are AT 1 receptor blockers. Adverse effects are the same as ACE inhibitors except cough and angioedema, which are not observed. They may be more effective in decreasing the effects of angiotensin because there are other enzymes that produce angiotensin II. Both drugs can be administered orally. Now many sartans are available. Saralasin is also a similar drug which is IV administered. It is out of marked because its vascular effects elated to dose-response cannot be predicted
32 Hypertensive emergency I It is a rare but life threatening situation. In patients with no complication, a diastolic blood pressure more than 150 mm Hg (systolic >210 mm Hg) is an emergency. In patients with encephalopathy, cerebral hemorrhagia, left ventricular failure, aorta stenosis, diastolic blood pressure the emergency limit is >130 mm Hg. Aim is to decrease diastolic pressure to mm Hg. 63 Hypertensive emergency II Sodium nitroprusside and diazoxide are the drugs most commonly used. Other effective IV drugs include nitroglycerin, labetalol, calcium channel blockers, hydralazine, reserpine and methyldopa. Nonparenteral therapy with oral nifedipine, captopril, prazosin or clonidin has also been shown to be useful
33 Thank you
Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs
 Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs Blood Pressure Normal = sys
Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs Blood Pressure Normal = sys
Antihypertensive Agents Part-2. Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia
 Antihypertensive Agents Part-2 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Agents that block production or action of angiotensin Angiotensin-converting
Antihypertensive Agents Part-2 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Agents that block production or action of angiotensin Angiotensin-converting
HYPERTENSION: Sustained elevation of arterial blood pressure above normal o Systolic 140 mm Hg and/or o Diastolic 90 mm Hg
 Lecture 39 Anti-Hypertensives B-Rod BLOOD PRESSURE: Systolic / Diastolic NORMAL: 120/80 Systolic = measure of pressure as heart is beating Diastolic = measure of pressure while heart is at rest between
Lecture 39 Anti-Hypertensives B-Rod BLOOD PRESSURE: Systolic / Diastolic NORMAL: 120/80 Systolic = measure of pressure as heart is beating Diastolic = measure of pressure while heart is at rest between
Antihypertensive drugs SUMMARY Made by: Lama Shatat
 Antihypertensive drugs SUMMARY Made by: Lama Shatat Diuretic Thiazide diuretics The loop diuretics Potassium-sparing Diuretics *Hydrochlorothiazide *Chlorthalidone *Furosemide *Torsemide *Bumetanide Aldosterone
Antihypertensive drugs SUMMARY Made by: Lama Shatat Diuretic Thiazide diuretics The loop diuretics Potassium-sparing Diuretics *Hydrochlorothiazide *Chlorthalidone *Furosemide *Torsemide *Bumetanide Aldosterone
sympatholytics sympatholytics sympatholytics
 sympatholytics sympatholytics sympatholytics CNS-ACTING SYMPATHOPLEGICS Sympathetic brain signals Doesn t affect baroreceptor reflex (no orthostatic hypotension) Methyldopa α-methylne crosses BBB (+) α-adrenoreceptors
sympatholytics sympatholytics sympatholytics CNS-ACTING SYMPATHOPLEGICS Sympathetic brain signals Doesn t affect baroreceptor reflex (no orthostatic hypotension) Methyldopa α-methylne crosses BBB (+) α-adrenoreceptors
Antihypertensives. Antihypertensive Classes. RAAS Inhibitors. Renin-Angiotensin Cascade. Angiotensin Receptors. Approaches to Hypertension Treatment
 Approaches to Hypertension Treatment Antihypertensives Inhibit Sympathetic impulses Inhibit contractility Inhibit heart rate Inhibit vasoconstriction Inhibit smooth muscle function Inhibit RAAS Inhibit
Approaches to Hypertension Treatment Antihypertensives Inhibit Sympathetic impulses Inhibit contractility Inhibit heart rate Inhibit vasoconstriction Inhibit smooth muscle function Inhibit RAAS Inhibit
Antihypertensive Agents
 Antihypertensive Agents Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 7, 08, presented by Ezra Levy, Pharm.D! Usual Dose,
Antihypertensive Agents Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 7, 08, presented by Ezra Levy, Pharm.D! Usual Dose,
Beta 1 Beta blockers A - Propranolol,
 Pharma Lecture 3 Beta blockers that we are most interested in are the ones that target Beta 1 receptors. Beta blockers A - Propranolol, it s a non-selective competitive antagonist of beta 1 and beta 2
Pharma Lecture 3 Beta blockers that we are most interested in are the ones that target Beta 1 receptors. Beta blockers A - Propranolol, it s a non-selective competitive antagonist of beta 1 and beta 2
Section 3, Lecture 2
 59-291 Section 3, Lecture 2 Diuretics: -increase in Na + excretion (naturesis) Thiazide and Related diuretics -decreased PVR due to decreases muscle contraction -an economical and effective treatment -protect
59-291 Section 3, Lecture 2 Diuretics: -increase in Na + excretion (naturesis) Thiazide and Related diuretics -decreased PVR due to decreases muscle contraction -an economical and effective treatment -protect
7/7/ CHD/MI LVH and LV dysfunction Dysrrhythmias Stroke PVD Renal insufficiency and failure Retinopathy. Normal <120 Prehypertension
 Prevalence of Hypertension Hypertension: Diagnosis and Management T. Villela, M.D. Program Director University of California, San Francisco-San Francisco General Hospital Family and Community Medicine
Prevalence of Hypertension Hypertension: Diagnosis and Management T. Villela, M.D. Program Director University of California, San Francisco-San Francisco General Hospital Family and Community Medicine
1. Antihypertensive agents 2. Vasodilators & treatment of angina 3. Drugs used in heart failure 4. Drugs used in arrhythmias
 1. Antihypertensive agents 2. Vasodilators & treatment of angina 3. Drugs used in heart failure 4. Drugs used in arrhythmias Only need to know drugs discussed in class At the end of this section you should
1. Antihypertensive agents 2. Vasodilators & treatment of angina 3. Drugs used in heart failure 4. Drugs used in arrhythmias Only need to know drugs discussed in class At the end of this section you should
DRUGS USED TO TREAT HYPERTENSION BY ALI ALALAWI
 DRUGS USED TO TREAT HYPERTENSION BY ALI ALALAWI 3. Vasodilators Drugs which dilate blood vessels ( decrease peripheral vascular resistance) by acting on smooth muscle cells through non-autonomic mechanisms:
DRUGS USED TO TREAT HYPERTENSION BY ALI ALALAWI 3. Vasodilators Drugs which dilate blood vessels ( decrease peripheral vascular resistance) by acting on smooth muscle cells through non-autonomic mechanisms:
Hypertension (JNC-8)
") Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
Management of Hypertension
 Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Antihypertensive Agents
 1. Blood Pressure Regulation Antihypertensive Agents - 2007 Edward JN Ishac. Ph.D. Associate Professor, Dept. Pharmacology & Toxicology Office: Smith 742; Tel: 828 2127 eishac@hsc.vcu.edu Frank's formula,
1. Blood Pressure Regulation Antihypertensive Agents - 2007 Edward JN Ishac. Ph.D. Associate Professor, Dept. Pharmacology & Toxicology Office: Smith 742; Tel: 828 2127 eishac@hsc.vcu.edu Frank's formula,
Introduction. Factors affecting blood pressure: 1-COP = HR X SV mainly affect SBP. 2-TPR = diameter of arterioles X viscosity of blood affect DBP
 Introduction Hypertension is a persistent elevation of blood pressure above 140 / 90 mmhg for more than three sitting. (0ptimal level
Introduction Hypertension is a persistent elevation of blood pressure above 140 / 90 mmhg for more than three sitting. (0ptimal level
ANTIHYPERTENSIVE DRUGS
 ANTIHYPERTENSIVE DRUGS Course: Integrated Therapeutics 1 Lecturer: Dr. E. Konorev Date: September 28, 2010 Materials on: Exam #3 Required reading: Katzung, Chapter 11 1 1 in 3 adults HYPERTENSION 64% of
ANTIHYPERTENSIVE DRUGS Course: Integrated Therapeutics 1 Lecturer: Dr. E. Konorev Date: September 28, 2010 Materials on: Exam #3 Required reading: Katzung, Chapter 11 1 1 in 3 adults HYPERTENSION 64% of
HYPERTENSION IN EMERGENCY MEDICINE Michael Jay Bresler, M.D., FACEP
 HYPERTENSION IN EMERGENCY MEDICINE Michael Jay Bresler, M.D., FACEP What is normal blood pressure? Prehypertension 130-139/80-90 Compared with normal BP Double the risk for developing hypertension. Lifestyle
HYPERTENSION IN EMERGENCY MEDICINE Michael Jay Bresler, M.D., FACEP What is normal blood pressure? Prehypertension 130-139/80-90 Compared with normal BP Double the risk for developing hypertension. Lifestyle
Antihypertensive Drugs. Munir Gharaibeh, MD, PhD, MHPE Faculty of Medicine, The University of Jordan November, 2014
 Antihypertensive Drugs Munir Gharaibeh, MD, PhD, MHPE Faculty of Medicine, The University of Jordan November, 2014 Antihypertensive Drugs What is Hypertension: A common, incurable, persistent, but usually
Antihypertensive Drugs Munir Gharaibeh, MD, PhD, MHPE Faculty of Medicine, The University of Jordan November, 2014 Antihypertensive Drugs What is Hypertension: A common, incurable, persistent, but usually
Treatment of Essential Hypertension
 2016 edition by Mark A. Simmons, PhD Department of Pharmaceutical Sciences School of Pharmacy University of Maryland Eastern Shore Originally developed by Hugh J. Burford, PhD, FCP Department of Pharmacology
2016 edition by Mark A. Simmons, PhD Department of Pharmaceutical Sciences School of Pharmacy University of Maryland Eastern Shore Originally developed by Hugh J. Burford, PhD, FCP Department of Pharmacology
ANTIHYPERTENSIVE AGENTS AND VASODILATORS. Lecture 5
 ANTIHYPERTENSIVE AGENTS AND VASODILATORS Lecture 5 Hypertension Blood pressure BP = CO x PVR n Interaction between autonomic nervous system, cardiovascular system and renal system Normal: 110/70 Prehypertension
ANTIHYPERTENSIVE AGENTS AND VASODILATORS Lecture 5 Hypertension Blood pressure BP = CO x PVR n Interaction between autonomic nervous system, cardiovascular system and renal system Normal: 110/70 Prehypertension
Antihypertensive Drugs. Munir Gharaibeh, MD, PhD, MHPE School of Medicine, The University of Jordan October, 2017
 Antihypertensive Drugs Munir Gharaibeh, MD, PhD, MHPE School of Medicine, The University of Jordan October, 2017 Antihypertensive Drugs What is Hypertension? A common, incurable, persistent, but usually
Antihypertensive Drugs Munir Gharaibeh, MD, PhD, MHPE School of Medicine, The University of Jordan October, 2017 Antihypertensive Drugs What is Hypertension? A common, incurable, persistent, but usually
Antihypertensive drugs: I. Thiazide and other diuretics:
 Clinical assessment of hypertensive patient: You have to take history regarding the presence of other risk factors for CAb like diabetes mellitus, smoking, etc. Take history whether the patient takes medications
Clinical assessment of hypertensive patient: You have to take history regarding the presence of other risk factors for CAb like diabetes mellitus, smoking, etc. Take history whether the patient takes medications
Categories of HTN. Overview of Hypertension. Types of Hypertension
 Categories of HTN Overview of Hypertension Normal SBP 100 Quick review of the Basics: What is
Categories of HTN Overview of Hypertension Normal SBP 100 Quick review of the Basics: What is
Chapter 23. Media Directory. Cardiovascular Disease (CVD) Hypertension: Classified into Three Categories
 Hypertension: Classified into Three Categories") Chapter 23 Drugs for Hypertension Slide 37 Slide 41 Media Directory Nifedipine Animation Doxazosin Animation Upper Saddle River, New Jersey 07458 All rights reserved. Cardiovascular Disease (CVD) Includes
Chapter 23 Drugs for Hypertension Slide 37 Slide 41 Media Directory Nifedipine Animation Doxazosin Animation Upper Saddle River, New Jersey 07458 All rights reserved. Cardiovascular Disease (CVD) Includes
Prof dr Aleksandar Raskovic DIRECT VASODILATORS
 Prof dr Aleksandar Raskovic DIRECT VASODILATORS Direct vasodilators Minoxidil (one of the most powerful peripheral arterial dilators) Opening of KATP channels, efflux of K, lose of Ca and smooth muscle
Prof dr Aleksandar Raskovic DIRECT VASODILATORS Direct vasodilators Minoxidil (one of the most powerful peripheral arterial dilators) Opening of KATP channels, efflux of K, lose of Ca and smooth muscle
Hypertension Update. Objectives 4/28/2015. Beverly J. Mathis, D.O. OOA May 2015
 Hypertension Update Beverly J. Mathis, D.O. OOA May 2015 Objectives Learn new recommendations for BP treatment goals Approach to hypertension in the office Use of hypertensive drugs, and how to tailor
Hypertension Update Beverly J. Mathis, D.O. OOA May 2015 Objectives Learn new recommendations for BP treatment goals Approach to hypertension in the office Use of hypertensive drugs, and how to tailor
New classification of HT Systolic Diastolic Normal <120 <80 Prehypertension Stage1HT Stage 2 HT >160 or >100
 Hypertension 1 Definition Hypertension can be defined as a condition where blood pressure is elevated to an extent that clinical benefit is obtained from blood pressure lowering. it is an important risk
Hypertension 1 Definition Hypertension can be defined as a condition where blood pressure is elevated to an extent that clinical benefit is obtained from blood pressure lowering. it is an important risk
Antihypertensives. Diagnostic category
 Measurement of blood pressure At first assessment, take both arms then choose the one with the higher reading. Beware of orthostatic hypotension. Measure BP in sitting position, and repeat after patient
Measurement of blood pressure At first assessment, take both arms then choose the one with the higher reading. Beware of orthostatic hypotension. Measure BP in sitting position, and repeat after patient
Hypertension. Penny Mosley MRPharmS
 Hypertension Penny Mosley MRPharmS Outline of presentation Introduction to hypertension Physiological control of arterial blood pressure What determines our bp? What determines the heart rate? What determines
Hypertension Penny Mosley MRPharmS Outline of presentation Introduction to hypertension Physiological control of arterial blood pressure What determines our bp? What determines the heart rate? What determines
Treatment of Essential Hypertension
 2016 edition by Mark A. Simmons, PhD Department of Pharmaceutical Sciences School of Pharmacy University of Maryland Eastern Shore Originally developed by Hugh J. Burford, PhD, FCP Department of Pharmacology
2016 edition by Mark A. Simmons, PhD Department of Pharmaceutical Sciences School of Pharmacy University of Maryland Eastern Shore Originally developed by Hugh J. Burford, PhD, FCP Department of Pharmacology
Angina pectoris due to coronary atherosclerosis : Atenolol is indicated for the long term management of patients with angina pectoris.
 Lonet Tablet Description Lonet contains Atenolol, a synthetic β1 selective (cardioselective) adrenoreceptor blocking agent without membrane stabilising or intrinsic sympathomimetic (partial agonist) activity.
Lonet Tablet Description Lonet contains Atenolol, a synthetic β1 selective (cardioselective) adrenoreceptor blocking agent without membrane stabilising or intrinsic sympathomimetic (partial agonist) activity.
Heart Failure (HF) Treatment
 Treatment") Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
What in the World is Functional Medicine?
 What in the World is Functional Medicine? An Introduction to a Systems Based Approach of Chronic Disease Meneah R Haworth, FNP-C Disclosure v I am a student of the Institute for Functional Medicine. They
What in the World is Functional Medicine? An Introduction to a Systems Based Approach of Chronic Disease Meneah R Haworth, FNP-C Disclosure v I am a student of the Institute for Functional Medicine. They
ANTIHYPERTENSIVES. Assoc. Prof. Bilgen Başgut
 ANTIHYPERTENSIVES Assoc. Prof. Bilgen Başgut Hypertension Hypertension is a condition in which the blood pressure is persistently higher than normal Hypertension > 140 mmhg > 90 mmhg Systolic Blood Pressure
ANTIHYPERTENSIVES Assoc. Prof. Bilgen Başgut Hypertension Hypertension is a condition in which the blood pressure is persistently higher than normal Hypertension > 140 mmhg > 90 mmhg Systolic Blood Pressure
HypertensionTreatment Guidelines. Michaelene Urban APRN, MSN, ACNS-BC, ANP-BC
 HypertensionTreatment Guidelines Michaelene Urban APRN, MSN, ACNS-BC, ANP-BC Objectives: Review the definition of the different stages of HTN. Review the current guidelines for treatment of HTN. Provided
HypertensionTreatment Guidelines Michaelene Urban APRN, MSN, ACNS-BC, ANP-BC Objectives: Review the definition of the different stages of HTN. Review the current guidelines for treatment of HTN. Provided
Byvalson. (nebivolol, valsartan) New Product Slideshow
 New Product Slideshow") Byvalson (nebivolol, valsartan) New Product Slideshow Introduction Brand name: Byvalson Generic name: Nebivolol, valsartan Pharmacological class: Beta-blocker + angiotensin II receptor blocker (ARB) Strength
Byvalson (nebivolol, valsartan) New Product Slideshow Introduction Brand name: Byvalson Generic name: Nebivolol, valsartan Pharmacological class: Beta-blocker + angiotensin II receptor blocker (ARB) Strength
 Hypertension Epidemiology 6% of deaths worldwide Defined as any of the following: systolic blood pressure 140 mmhg, diastolic blood pressure 90 mmhg, taking antihypertensive medications Pulse pressure=
Hypertension Epidemiology 6% of deaths worldwide Defined as any of the following: systolic blood pressure 140 mmhg, diastolic blood pressure 90 mmhg, taking antihypertensive medications Pulse pressure=
Pharmacology of the Sympathetic Nervous System II
 Pharmacology of the Sympathetic Nervous System II Edward JN Ishac, Ph.D. Professor Smith Building, Room 742 eishac@vcu.edu 828-2127 Department of Pharmacology and Toxicology Medical College of Virginia
Pharmacology of the Sympathetic Nervous System II Edward JN Ishac, Ph.D. Professor Smith Building, Room 742 eishac@vcu.edu 828-2127 Department of Pharmacology and Toxicology Medical College of Virginia
β adrenergic blockade, a renal perspective Prof S O McLigeyo
 β adrenergic blockade, a renal perspective Prof S O McLigeyo Carvedilol Third generation β blocker (both β 1 and β 2 ) Possesses α 1 adrenergic blocking properties. β: α blocking ratio 7:1 to 3:1 Antioxidant
β adrenergic blockade, a renal perspective Prof S O McLigeyo Carvedilol Third generation β blocker (both β 1 and β 2 ) Possesses α 1 adrenergic blocking properties. β: α blocking ratio 7:1 to 3:1 Antioxidant
DRUG CLASSES BETA-ADRENOCEPTOR ANTAGONISTS (BETA-BLOCKERS)
") DRUG CLASSES BETA-ADRENOCEPTOR ANTAGONISTS (BETA-BLOCKERS) Beta-blockers have been widely used in the management of angina, certain tachyarrhythmias and heart failure, as well as in hypertension. Examples
DRUG CLASSES BETA-ADRENOCEPTOR ANTAGONISTS (BETA-BLOCKERS) Beta-blockers have been widely used in the management of angina, certain tachyarrhythmias and heart failure, as well as in hypertension. Examples
Hypertensives Emergency and Urgency
 Hypertensives Emergency and Urgency Budi Yuli Setianto Cardiology Divisision Department of Internal Medicine Faculty of Medicine UGM Sardjito Hospital Yogyakarta Background USA: Hypertension is 30% of
Hypertensives Emergency and Urgency Budi Yuli Setianto Cardiology Divisision Department of Internal Medicine Faculty of Medicine UGM Sardjito Hospital Yogyakarta Background USA: Hypertension is 30% of
University of Al Qadisiyah College of Pharmacy Dr. Bassim I Mohammad, MBChB, MSc, Ph.D
 University of Al Qadisiyah College of Pharmacy Dr. Bassim I Mohammad, MBChB, MSc, Ph.D Cardiovascular Pharmacology 1. Antihypertensives 2. Antianginal 3. Drugs for HF 4. Antiarrythemics 5. Drugs for Hyperlipoproteniemia
University of Al Qadisiyah College of Pharmacy Dr. Bassim I Mohammad, MBChB, MSc, Ph.D Cardiovascular Pharmacology 1. Antihypertensives 2. Antianginal 3. Drugs for HF 4. Antiarrythemics 5. Drugs for Hyperlipoproteniemia
Dr. Vishaal Bhat. anti-adrenergic drugs
 Dr. Vishaal Bhat anti-adrenergic drugs Divisions of human nervous system Human Nervous system Central Nervous System Peripheral Nervous System Autonomic Nervous System Nervous system Includes neurons and
Dr. Vishaal Bhat anti-adrenergic drugs Divisions of human nervous system Human Nervous system Central Nervous System Peripheral Nervous System Autonomic Nervous System Nervous system Includes neurons and
Cardiac Drugs: Chapter 9 Worksheet Cardiac Agents. 1. drugs affect the rate of the heart and can either increase its rate or decrease its rate.
 Complete the following. 1. drugs affect the rate of the heart and can either increase its rate or decrease its rate. 2. drugs affect the force of contraction and can be either positive or negative. 3.
Complete the following. 1. drugs affect the rate of the heart and can either increase its rate or decrease its rate. 2. drugs affect the force of contraction and can be either positive or negative. 3.
TREATMENT OF HYPERTENSION
 TREATMENT OF HYPERTENSION Aim of treatment BP Goals Main items of treatment Lifestyle modification When to start drug Rx Pharmacological therapy 1. Relief of symptoms 2. Prevention of complications and
TREATMENT OF HYPERTENSION Aim of treatment BP Goals Main items of treatment Lifestyle modification When to start drug Rx Pharmacological therapy 1. Relief of symptoms 2. Prevention of complications and
Chapter 2 ~ Cardiovascular system
 Chapter 2 ~ Cardiovascular System: General Section 1 of 6 Chapter 2 ~ Cardiovascular system 2.1 Positive inotropic drugs 2.1.1 Cardiac glycosides DIGOXIN 2.2 Diuretics Elixir 50micrograms in 1ml Injection
Chapter 2 ~ Cardiovascular System: General Section 1 of 6 Chapter 2 ~ Cardiovascular system 2.1 Positive inotropic drugs 2.1.1 Cardiac glycosides DIGOXIN 2.2 Diuretics Elixir 50micrograms in 1ml Injection
Adrenergic Receptor Antagonists
 Adrenergic Receptor Antagonists α-adrenergic Receptor Antagonists Unlike the β-adrenergic receptor antagonists, which bear clear structural similarities to the adrenergic agonists E, epinephrine, and isoproterenol,
Adrenergic Receptor Antagonists α-adrenergic Receptor Antagonists Unlike the β-adrenergic receptor antagonists, which bear clear structural similarities to the adrenergic agonists E, epinephrine, and isoproterenol,
Circulation. Blood Pressure and Antihypertensive Medications. Venous Return. Arterial flow. Regulation of Cardiac Output.
 Circulation Blood Pressure and Antihypertensive Medications Two systems Pulmonary (low pressure) Systemic (high pressure) Aorta 120 mmhg Large arteries 110 mmhg Arterioles 40 mmhg Arteriolar capillaries
Circulation Blood Pressure and Antihypertensive Medications Two systems Pulmonary (low pressure) Systemic (high pressure) Aorta 120 mmhg Large arteries 110 mmhg Arterioles 40 mmhg Arteriolar capillaries
Cardiovascular drugs
 chapter 13 Cardiovascular drugs Cardiovascular drugs act on the heart or blood vessels to control the cardiovascular system. They are used to treat a variety of conditions from hypertension to chronic
chapter 13 Cardiovascular drugs Cardiovascular drugs act on the heart or blood vessels to control the cardiovascular system. They are used to treat a variety of conditions from hypertension to chronic
M2 TEACHING UNDERSTANDING PHARMACOLOGY
 M2 TEACHING UNDERSTANDING PHARMACOLOGY USING CVS SYSTEM AS AN EXAMPLE NIGEL FONG 2 JAN 2014 TODAY S OBJECTIVE Pharmacology often seems like an endless list of mechanisms and side effects to memorize. To
M2 TEACHING UNDERSTANDING PHARMACOLOGY USING CVS SYSTEM AS AN EXAMPLE NIGEL FONG 2 JAN 2014 TODAY S OBJECTIVE Pharmacology often seems like an endless list of mechanisms and side effects to memorize. To
BIMM118. Autonomic Nervous System
 Autonomic Nervous System Autonomic Nervous System Ganglia close to the innervated organs Myelinated axons Ganglia close to the spinal column Preganglionic axons are myelinated; postganglionic axons are
Autonomic Nervous System Autonomic Nervous System Ganglia close to the innervated organs Myelinated axons Ganglia close to the spinal column Preganglionic axons are myelinated; postganglionic axons are
Autonomic Pharmacology
 Autonomic Pharmacology ADRENERGIC RECEPTOR BLOCKERS Adrenergic-receptor antagonists block the effects of sympathetic stimulation and adrenergic agonists mediated through - and -receptors. Adrenergic receptor
Autonomic Pharmacology ADRENERGIC RECEPTOR BLOCKERS Adrenergic-receptor antagonists block the effects of sympathetic stimulation and adrenergic agonists mediated through - and -receptors. Adrenergic receptor
HYPERTENSION IN CKD. LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL
 HYPERTENSION IN CKD LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL Stages in Progression of Chronic Kidney Disease and Therapeutic Strategies Complications Normal Increased risk Damage GFR
HYPERTENSION IN CKD LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL Stages in Progression of Chronic Kidney Disease and Therapeutic Strategies Complications Normal Increased risk Damage GFR
Dr Narender Goel MD (Internal Medicine and Nephrology) Financial Disclosure: None, Conflict of Interest: None
 Financial Disclosure: None, Conflict of Interest: None") Dr Narender Goel MD (Internal Medicine and Nephrology) drnarendergoel@gmail.com Financial Disclosure: None, Conflict of Interest: None 12 th December 2013, New York Visit us at: http://kidneyscience.info/
Dr Narender Goel MD (Internal Medicine and Nephrology) drnarendergoel@gmail.com Financial Disclosure: None, Conflict of Interest: None 12 th December 2013, New York Visit us at: http://kidneyscience.info/
Hypertension CHAPTER-I CARDIOVASCULAR SYSTEM. Dr. K T NAIK Pharm.D Associate Professor Department of Pharm.D Krishna Teja Pharmacy College, Tirupati
 CHAPTER-I CARDIOVASCULAR SYSTEM Hypertension SUB: PHARMACOTHERAPEUTICS-I CODE:T0820006 Dr. K T NAIK Pharm.D Associate Professor Department of Pharm.D Krishna Teja Pharmacy College, Tirupati Hypertension
CHAPTER-I CARDIOVASCULAR SYSTEM Hypertension SUB: PHARMACOTHERAPEUTICS-I CODE:T0820006 Dr. K T NAIK Pharm.D Associate Professor Department of Pharm.D Krishna Teja Pharmacy College, Tirupati Hypertension
Antihypertensive Drugs. Nafrialdi
 Antihypertensive Drugs Nafrialdi 1 Mechanisms of Blood Pressure Regulation Blood Presure Cardiac Output Peripheral Resistance Heart Rate Stroke volume Vascular tone Vessel elasticity Myocardial contractility
Antihypertensive Drugs Nafrialdi 1 Mechanisms of Blood Pressure Regulation Blood Presure Cardiac Output Peripheral Resistance Heart Rate Stroke volume Vascular tone Vessel elasticity Myocardial contractility
LESSON ASSIGNMENT. After completing this lesson you will be able to:
 LESSON ASSIGNMENT SUBCOURSE MD0806 LESSON 7 Therapeutics III. Antihypertensive Agents. LESSON ASSIGNMENT Paragraphs 7-1--7-12. LESSON OBJECTIVES After completing this lesson you will be able to: 7-1. From
LESSON ASSIGNMENT SUBCOURSE MD0806 LESSON 7 Therapeutics III. Antihypertensive Agents. LESSON ASSIGNMENT Paragraphs 7-1--7-12. LESSON OBJECTIVES After completing this lesson you will be able to: 7-1. From
Chapter 10 Worksheet Blood Pressure and Antithrombotic Agents
 Complete the following. 1. A layer of cells lines each vessel in the vascular system. This layer is a passive barrier that keeps cells and proteins from going into tissues; it also contains substances
Complete the following. 1. A layer of cells lines each vessel in the vascular system. This layer is a passive barrier that keeps cells and proteins from going into tissues; it also contains substances
Lab Period: Name: Physiology Chapter 14 Blood Flow and Blood Pressure, Plus Fun Review Study Guide
 Lab Period: Name: Physiology Chapter 14 Blood Flow and Blood Pressure, Plus Fun Review Study Guide Main Idea: The function of the circulatory system is to maintain adequate blood flow to all tissues. Clinical
Lab Period: Name: Physiology Chapter 14 Blood Flow and Blood Pressure, Plus Fun Review Study Guide Main Idea: The function of the circulatory system is to maintain adequate blood flow to all tissues. Clinical
Drugs Used in Heart Failure. Assistant Prof. Dr. Najlaa Saadi PhD pharmacology Faculty of Pharmacy University of Philadelphia
 Drugs Used in Heart Failure Assistant Prof. Dr. Najlaa Saadi PhD pharmacology Faculty of Pharmacy University of Philadelphia Heart Failure Heart failure (HF), occurs when cardiac output is inadequate to
Drugs Used in Heart Failure Assistant Prof. Dr. Najlaa Saadi PhD pharmacology Faculty of Pharmacy University of Philadelphia Heart Failure Heart failure (HF), occurs when cardiac output is inadequate to
Hypertension Management - Summary
 Who should have blood pressure assessed? Hypertension Management - Summary All patients over the age of 40 years, every 1-3 years in order to determine their cardiovascular risk (ie. Framingham Risk Score)
Who should have blood pressure assessed? Hypertension Management - Summary All patients over the age of 40 years, every 1-3 years in order to determine their cardiovascular risk (ie. Framingham Risk Score)
AUTONOMIC DRUGS: ADRENOCEPTOR AGONISTS AND SYMPATHOMIMETICS. Lecture 4
 AUTONOMIC DRUGS: ADRENOCEPTOR AGONISTS AND SYMPATHOMIMETICS Lecture 4 Introduction (review) 5 key features of neurotransmitter function, which can be targets for pharmacotherapy Synthesis Storage Release
AUTONOMIC DRUGS: ADRENOCEPTOR AGONISTS AND SYMPATHOMIMETICS Lecture 4 Introduction (review) 5 key features of neurotransmitter function, which can be targets for pharmacotherapy Synthesis Storage Release
ANTI- HYPERTENSIVE AGENTS
 CLINICAL ANTI- HYPERTENSIVE AGENTS Jacqueline van Schoor, MPharm, BSc (Hons) Amayeza Info Centre Hypertension represents a major public health concern. It affects about a billion people worldwide and is
CLINICAL ANTI- HYPERTENSIVE AGENTS Jacqueline van Schoor, MPharm, BSc (Hons) Amayeza Info Centre Hypertension represents a major public health concern. It affects about a billion people worldwide and is
b. Describe the pharmacology of centrally acting agents such as clonidine and α methyldopa.
 B. 13 Antihypertensive drugs a. Classify the modes of action of the antihypertensive drugs. central sympathetic tone inhibitors α 2 agonists β antagonists peripheral sympathetic antagonists α blockers
B. 13 Antihypertensive drugs a. Classify the modes of action of the antihypertensive drugs. central sympathetic tone inhibitors α 2 agonists β antagonists peripheral sympathetic antagonists α blockers
Difficult to Treat Hypertension
 Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
MANAGEMENT OF HYPERTENSION IN PREGNANCY, THE ALGORHITHM
 MANAGEMENT OF HYPERTENSION IN PREGNANCY, THE ALGORHITHM Are Particular Anti-hypertensives More Effective or Harmful Than Others in Hypertension in Pregnancy? Existing data is inadequate Methyldopa and
MANAGEMENT OF HYPERTENSION IN PREGNANCY, THE ALGORHITHM Are Particular Anti-hypertensives More Effective or Harmful Than Others in Hypertension in Pregnancy? Existing data is inadequate Methyldopa and
Hypertension: an overview of recommended treatment John Vann Jones PhD, FRCP
 Drug review Hypertension Hypertension: an overview of recommended treatment John Vann Jones PhD, FRCP Skyline Imaging Ltd Professor Vann Jones provides an overview of the wide range of antihypertensive
Drug review Hypertension Hypertension: an overview of recommended treatment John Vann Jones PhD, FRCP Skyline Imaging Ltd Professor Vann Jones provides an overview of the wide range of antihypertensive
By Prof. Khaled El-Rabat
 What is The Optimum? By Prof. Khaled El-Rabat Professor of Cardiology - Benha Faculty of Medicine HT. Introduction Despite major worldwide efforts over recent decades directed at diagnosing and treating
What is The Optimum? By Prof. Khaled El-Rabat Professor of Cardiology - Benha Faculty of Medicine HT. Introduction Despite major worldwide efforts over recent decades directed at diagnosing and treating
HEART FAILURE PHARMACOLOGY. University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D
 HEART FAILURE PHARMACOLOGY University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 1 LEARNING OBJECTIVES Understand the effects of heart failure in the body
HEART FAILURE PHARMACOLOGY University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 1 LEARNING OBJECTIVES Understand the effects of heart failure in the body
Hypertension is also an important risk factor in the development of chronic kidney disease and heart failure.
 Hypertension Hypertension Hypertension is defined as either a sustained systolic blood pressure of greater than 140 mm Hg or a sustained diastolic blood pressure of greater than 90 mm Hg. Hypertension
Hypertension Hypertension Hypertension is defined as either a sustained systolic blood pressure of greater than 140 mm Hg or a sustained diastolic blood pressure of greater than 90 mm Hg. Hypertension
Management of Hypertension. Ahmed El Hawary MD Suez Canal University
 Management of Hypertension Ahmed El Hawary MD Suez Canal University Minimal vs. Optimal Care Resources more than science affect type of care and level of management. what is possible (minimal care) and
Management of Hypertension Ahmed El Hawary MD Suez Canal University Minimal vs. Optimal Care Resources more than science affect type of care and level of management. what is possible (minimal care) and
Angina Pectoris. Edward JN Ishac, Ph.D. Smith Building, Room
 Angina Pectoris Edward JN Ishac, Ph.D. Smith Building, Room 742 eishac@vcu.edu 828-2127 Department of Pharmacology and Toxicology Medical College of Virginia Campus of Virginia Commonwealth University
Angina Pectoris Edward JN Ishac, Ph.D. Smith Building, Room 742 eishac@vcu.edu 828-2127 Department of Pharmacology and Toxicology Medical College of Virginia Campus of Virginia Commonwealth University
Younger adults with a family history of premature artherosclerotic disease should have their cardiovascular risk factors measured.
 Appendix 2A - Guidance on Management of Hypertension Measurement of blood pressure All adults from 40 years should have blood pressure measured as part of opportunistic cardiovascular risk assessment.
Appendix 2A - Guidance on Management of Hypertension Measurement of blood pressure All adults from 40 years should have blood pressure measured as part of opportunistic cardiovascular risk assessment.
Heart failure. Failure? blood supply insufficient for body needs. CHF = congestive heart failure. increased blood volume, interstitial fluid
 Failure? blood supply insufficient for body needs CHF = congestive heart failure increased blood volume, interstitial fluid Underlying causes/risk factors Ischemic heart disease (CAD) 70% hypertension
Failure? blood supply insufficient for body needs CHF = congestive heart failure increased blood volume, interstitial fluid Underlying causes/risk factors Ischemic heart disease (CAD) 70% hypertension
Pharmacology. Drugs affecting the Cardiovascular system (Antianginal Drugs)
") Lecture 7 (year3) Dr Noor Al-Hasani Pharmacology University of Baghdad College of dentistry Drugs affecting the Cardiovascular system (Antianginal Drugs) Atherosclerotic disease of the coronary arteries,
Lecture 7 (year3) Dr Noor Al-Hasani Pharmacology University of Baghdad College of dentistry Drugs affecting the Cardiovascular system (Antianginal Drugs) Atherosclerotic disease of the coronary arteries,
Heart Failure. Subjective SOB (shortness of breath) Peripheral edema. Orthopnea (2-3 pillows) PND (paroxysmal nocturnal dyspnea)
 Peripheral edema. Orthopnea (2-3 pillows) PND (paroxysmal nocturnal dyspnea)") Pharmacology I. Definitions A. Heart Failure (HF) Heart Failure Ezra Levy, Pharm.D. HF Results when one or both ventricles are unable to pump sufficient blood to meet the body s needs There are 2 types
Pharmacology I. Definitions A. Heart Failure (HF) Heart Failure Ezra Levy, Pharm.D. HF Results when one or both ventricles are unable to pump sufficient blood to meet the body s needs There are 2 types
DROGAS PARA HIPERTENSION ARTERIAL JONATHAN POVEDA FERNANDEZ HSJD / 2013 FACC/FSCAI/FESC
 DROGAS PARA HIPERTENSION ARTERIAL JONATHAN POVEDA FERNANDEZ HSJD / 2013 FACC/FSCAI/FESC Pharmacotherapy of HTN Rationale for reducing arterial pressure Reduce cardiac output Reduce heart rate Reduce stroke
DROGAS PARA HIPERTENSION ARTERIAL JONATHAN POVEDA FERNANDEZ HSJD / 2013 FACC/FSCAI/FESC Pharmacotherapy of HTN Rationale for reducing arterial pressure Reduce cardiac output Reduce heart rate Reduce stroke
Hypertension. Antihypertensive Agents
 Hypertension and Antihypertensive Agents Edward JN Ishac, Ph.D. Smith Building, Room 742 eishac@vcu.edu 8-2127 8-2126 Department of Pharmacology and Toxicology Medical College of Virginia Campus of Virginia
Hypertension and Antihypertensive Agents Edward JN Ishac, Ph.D. Smith Building, Room 742 eishac@vcu.edu 8-2127 8-2126 Department of Pharmacology and Toxicology Medical College of Virginia Campus of Virginia
Towards a Greater Understanding of Cardiac Medications Foundational Cardiac Concepts That Must Be Understood:
 Towards a Greater Understanding of Cardiac Medications Foundational Cardiac Concepts That Must Be Understood: Cardiac Output (CO) CO=SVxHR (stroke volume x heart rate) Cardiac output: The amount of blood
Towards a Greater Understanding of Cardiac Medications Foundational Cardiac Concepts That Must Be Understood: Cardiac Output (CO) CO=SVxHR (stroke volume x heart rate) Cardiac output: The amount of blood
Management of Hypertension. M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine
 Division of Nephrology University of Missouri School of Medicine") Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Amlodipine plus Lisinopril Tablets AMLOPRES-L
 Amlodipine plus Lisinopril Tablets AMLOPRES-L COMPOSITION AMLOPRES-L Each uncoated tablet contains: Amlodipine besylate equivalent to Amlodipine 5 mg and Lisinopril USP equivalent to Lisinopril (anhydrous)
Amlodipine plus Lisinopril Tablets AMLOPRES-L COMPOSITION AMLOPRES-L Each uncoated tablet contains: Amlodipine besylate equivalent to Amlodipine 5 mg and Lisinopril USP equivalent to Lisinopril (anhydrous)
Structure and organization of blood vessels
 The cardiovascular system Structure of the heart The cardiac cycle Structure and organization of blood vessels What is the cardiovascular system? The heart is a double pump heart arteries arterioles veins
The cardiovascular system Structure of the heart The cardiac cycle Structure and organization of blood vessels What is the cardiovascular system? The heart is a double pump heart arteries arterioles veins
Hypertension Update Warwick Jaffe Interventional Cardiologist Ascot Hospital
 Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
Pharmacology - Problem Drill 11: Vasoactive Agents
 Pharmacology - Problem Drill 11: Vasoactive Agents Question No. 1 of 10 1. Vascular smooth muscle contraction is triggered by a rise in. Question #01 (A) Luminal calcium (B) Extracellular calcium (C) Intracellular
Pharmacology - Problem Drill 11: Vasoactive Agents Question No. 1 of 10 1. Vascular smooth muscle contraction is triggered by a rise in. Question #01 (A) Luminal calcium (B) Extracellular calcium (C) Intracellular
1. Despite the plethora of new ACE-inhibitors they offer little advantage over the earlier products captopril and enalapril.
 SUMMARY 1. Despite the plethora of new ACE-inhibitors they offer little advantage over the earlier products captopril and enalapril. 2. While diuretics and beta-blockers remain first-line antihypertensive
SUMMARY 1. Despite the plethora of new ACE-inhibitors they offer little advantage over the earlier products captopril and enalapril. 2. While diuretics and beta-blockers remain first-line antihypertensive
Blood pressure (BP) control. Hypertension
 control. Hypertension") Blood pressure (BP) control Normal heart function Blood pressure (BP) control blood pressure (BP) cardiac output (CO) = total peripheral resistance (TPR) heart rate (HR) filling pressure arteriolar volume
Blood pressure (BP) control Normal heart function Blood pressure (BP) control blood pressure (BP) cardiac output (CO) = total peripheral resistance (TPR) heart rate (HR) filling pressure arteriolar volume
HYPERTENSION 4.0 Contact Hours Presented by: CEU Professor
 HYPERTENSION 4.0 Contact Hours Presented by: CEU Professor 7 www.ceuprofessoronline.com Copyright 8 2007 The Magellan Group, LLC All Rights Reserved. Reproduction and distribution of these materials is
HYPERTENSION 4.0 Contact Hours Presented by: CEU Professor 7 www.ceuprofessoronline.com Copyright 8 2007 The Magellan Group, LLC All Rights Reserved. Reproduction and distribution of these materials is
Beta-blockers. Atenolol. Propranolol. Bisoprolol. Metoprolol. Labetalol. Carvedilol.
 Drugs of CVS Beta-blockers Atenolol. Propranolol. Bisoprolol. Metoprolol. Labetalol. Carvedilol. Atenolol.cardioselective Propranolol, nonselective Bisoprolol, cardioselective Metoprolol Carvedilol, alpha
Drugs of CVS Beta-blockers Atenolol. Propranolol. Bisoprolol. Metoprolol. Labetalol. Carvedilol. Atenolol.cardioselective Propranolol, nonselective Bisoprolol, cardioselective Metoprolol Carvedilol, alpha
2017 Guideline for the Prevention, Detection, Evaluation and Management of High Blood Pressure in Adults
 DETAILED SUMMARY FROM THE 2017 Guideline for the Prevention, Detection, Evaluation and Management of High Blood Pressure in Adults A REPORT OF THE American College of Cardiology/ American Heart Association
DETAILED SUMMARY FROM THE 2017 Guideline for the Prevention, Detection, Evaluation and Management of High Blood Pressure in Adults A REPORT OF THE American College of Cardiology/ American Heart Association
Factors Involved in Poor Control of Risk Factors
 Factors Involved in Poor Control of Risk Factors Patient compliance Clinical inertia Health Care System structure 14781 M Limitations of Formal Studies Selection of patients Recruitment and follow-up alter
Factors Involved in Poor Control of Risk Factors Patient compliance Clinical inertia Health Care System structure 14781 M Limitations of Formal Studies Selection of patients Recruitment and follow-up alter
Adrenergic agonists Sympathomimetic drugs. ANS Pharmacology Lecture 4 Dr. Hiwa K. Saaed College of Pharmacy/University of Sulaimani
 Adrenergic agonists Sympathomimetic drugs ANS Pharmacology Lecture 4 Dr. Hiwa K. Saaed College of Pharmacy/University of Sulaimani 2017-2018 Adrenergic agonists The adrenergic drugs affect receptors that
Adrenergic agonists Sympathomimetic drugs ANS Pharmacology Lecture 4 Dr. Hiwa K. Saaed College of Pharmacy/University of Sulaimani 2017-2018 Adrenergic agonists The adrenergic drugs affect receptors that
ANTI - ARRHYTHMIC DRUGS
 ANTI - ARRHYTHMIC DRUGS CARDIAC ACTION POTENTIAL K Out Balance Ca in/k out Na in K Out GENERATION OF ARRHYTHMIAS Four mechanisms of arrhythmia generation; Increased normal automaticity Abnormal automaticity
ANTI - ARRHYTHMIC DRUGS CARDIAC ACTION POTENTIAL K Out Balance Ca in/k out Na in K Out GENERATION OF ARRHYTHMIAS Four mechanisms of arrhythmia generation; Increased normal automaticity Abnormal automaticity
Bisoprolol Fumarate 2.5 mg, 5 mg and 10 mg Tablet
 Bisoprolol Fumarate 2.5 mg, 5 mg and 10 mg Tablet Description Betapro is a preparation of Bisoprolol Fumarate. Bisoprolol is used alone or in combination with other medications to treat high blood pressure.
Bisoprolol Fumarate 2.5 mg, 5 mg and 10 mg Tablet Description Betapro is a preparation of Bisoprolol Fumarate. Bisoprolol is used alone or in combination with other medications to treat high blood pressure.
Chapter / Section / Drug
 2 Cardiovascular System 2.1 Positive inotropic drugs Digoxin Digoxin specific antibody ( DigiFab ) 2.2 Diuretics 2.2.1 Thiazides and related diuretics Indapamide (1 st Line) Bendroflumethiazide Metolazone
2 Cardiovascular System 2.1 Positive inotropic drugs Digoxin Digoxin specific antibody ( DigiFab ) 2.2 Diuretics 2.2.1 Thiazides and related diuretics Indapamide (1 st Line) Bendroflumethiazide Metolazone
Decades of Experience
 JACC Vol. 14. No. 7 December 1989: 1595-608 159s The Evolution of Antihypertensive Decades of Experience Therapy: An Overview of Four GEORGE L. BAKRIS, MD,* EDWARD D. FROHLICH, MD, FACCt New Orlruns. Louisiuna
JACC Vol. 14. No. 7 December 1989: 1595-608 159s The Evolution of Antihypertensive Decades of Experience Therapy: An Overview of Four GEORGE L. BAKRIS, MD,* EDWARD D. FROHLICH, MD, FACCt New Orlruns. Louisiuna
METOTRUST XL-25/50 Metoprolol Succinate Extended-Release Tablets
 METOTRUST XL-25/50 Metoprolol Succinate Extended-Release Tablets COMPOSITION Each film-coated tablet of Metotrust XL-25 contains: Metoprolol Succinate USP 23.75 mg equivalent to Metoprolol Tartrate 25
METOTRUST XL-25/50 Metoprolol Succinate Extended-Release Tablets COMPOSITION Each film-coated tablet of Metotrust XL-25 contains: Metoprolol Succinate USP 23.75 mg equivalent to Metoprolol Tartrate 25
Managing Hypertension in Diabetes Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park.
 Managing Hypertension in Diabetes 2015 Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park Case Scenario Mike M is a 59 year old man with type 2 diabetes managed
Managing Hypertension in Diabetes 2015 Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park Case Scenario Mike M is a 59 year old man with type 2 diabetes managed
Cardiovascular Drugs
 Cardiovascular Drugs Calcium Channel blockers Phenylalkylamine Verapamil Binds to S5-S6 loop and S6 domain.?inactivation/selectivity interference Dihydropyridines Nifedipine i) S5-S6 loop and S6 of domain
Cardiovascular Drugs Calcium Channel blockers Phenylalkylamine Verapamil Binds to S5-S6 loop and S6 domain.?inactivation/selectivity interference Dihydropyridines Nifedipine i) S5-S6 loop and S6 of domain
INDIAN HYPERTENSION GUIDELINES-II
 HYPERTENSION IN SPECIAL SITUATIONS Hypertension with diabetes mellitus Co-existence of hypertension and diabetes is being increasingly recognised. 30-35% of hypertensives are detected to have diabetes.
HYPERTENSION IN SPECIAL SITUATIONS Hypertension with diabetes mellitus Co-existence of hypertension and diabetes is being increasingly recognised. 30-35% of hypertensives are detected to have diabetes.