Head injuries. Dr.Mohammed altamimi
|
|
|
- Hannah Hunt
- 5 years ago
- Views:
Transcription

1 Head injuries Dr.Mohammed altamimi
2 Pathophysiology Local effects on brain tissue Systemic effects of TBI Management protocols Patient triage and classification mechanism Types of head injuries
3

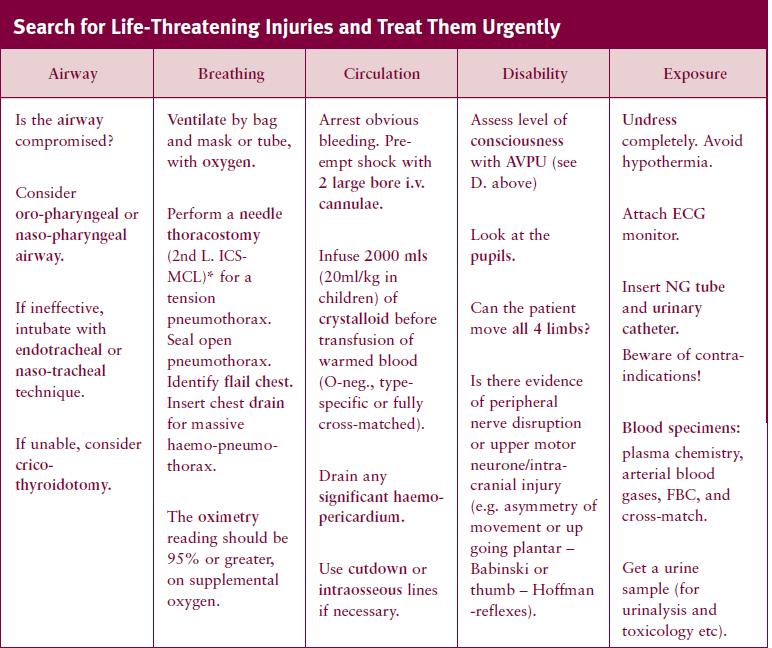
4 The Primary Survey and Resuscitation proceed in parallel A Clear the Airway. Use chin-lift or jaw-thrust. Immobilize the cervical spine with collars, bags and tape until cleared. B Check Ventilation. Administer oxygen at 15 litres per minute with tight-fitting mask with reservoir or use bag, valve and mask. C Check for pulses, skin perfusion and consciousness. Identify obvious sources of blood loss; D Assess the level of consciousness with A.V.P.U.: A (alert); V (responds to verbal communication); P (responds only to pain); U (unconscious); E Expose and examine the patient thoroughly.
5
 M: medication (e.g. a beta-blocker or warfarin) P: previous medical history (e.g. previous surgery or anaesthetic mishap) L: last mealtime (i.")
6 The Secondary Survey Recheck A, B, C and D. Proceed to next stage if the patient is stable and analgesia has been effective. The secondary survey is a headto-toe examination of the patient s body. A.M.P.L.E. - a simple mnemonic for key information A: allergies (e.g. penicillin or aspirin) M: medication (e.g. a beta-blocker or warfarin) P: previous medical history (e.g. previous surgery or anaesthetic mishap) L: last mealtime (i.e. drink versus major meal) E: events surrounding the incident (e.g. fell 5 metres with immediate loss of consciousness)

7
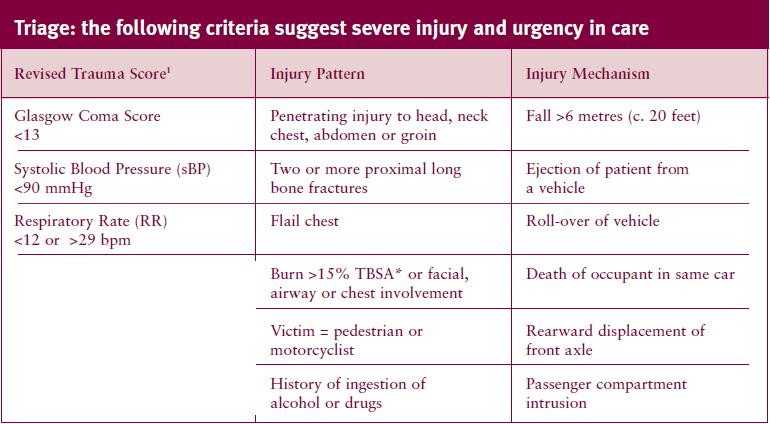
8 INITIAL MANAGEMENT OF SEVERE TRAUMA Most widely accepted system is that recommended in the American College of Surgeons Advanced Trauma Life Support (ATLS) course. The key elements of this approach are the primary survey/resuscitation phase, the secondary survey and the rapid implementation of definitive treatment, which may involve early surgery. The objective is to detect life-threatening conditions as quickly as possible, to stabilise the patient and to start definitive treatment as early as possible, in a prioritised fashion.
9 Intensive management of traumatic brain injury (roles and objectives) The primary focus of intensive management is directed towards patients suffering severe head injury (GCS of 8)following initial resuscitation and to prevent those suffering moderate injuries from deteriorating into unresponsive coma It is universally agreed that a population of neurons is irreversibly damaged at initial impact but neuronal demise continues unchecked until brain resuscitation is initiated It is also agreed that primary brain injury initiates a cascade of metabolic derangement affecting the cerebral vascular system, glial supporting cells, and neurons, which leaves brain vulnerable to secondary injury
10 Hypoxia.Brain stem dysf..ventilation prob.. O2 delivery prob. Head injury Primary impact ischemia.raised ICP.Vasoconstriction.SOL acidosis acidosis Traumatic brain (Secondary injury). Ion pumps dysfunction.deranged autoregulation.oedema(vsogenic,c.toxic)

11 Herniation syndromes

12
13 Systemic effect of T.B.I Cholinergic dysfunction Adrenal hyperactivity Hypothalamic dysfunction Brain stem dysfunction.bradyrrhythmia. hypotension.mi.neurogenic pulmonary edema.di.siadh.csws.hypersecretion of ACTH,GH prolactin.apnoea,.hypoventilation.bradycardia.hypotention.hypertention,.decrease COP.arrhythmias increased secretion of catecholamines and enkephaline, cytokines leading to hypermetabolism, hyperglycemia hypercatabolism and organ dysfunction (lung, liver, heart, gut) through lactic acidosis
14 MECHANISMS OF INJURY inertial or contact mechanisms Inertial injuries are commonly called "acceleration" or "deceleration" injuries Contact injuries are commonly called coup & contercoup injuries.

15
16
17
18

19


20


21
22 Initial management of acute closed head injury at accident site emergency room in the ICU Triage, resuscitation of ABCD (35% incidence of hypoxia (Apnea > 10 min carries high mortality) Controlled ventilation to maintain paco mmhg GCS less than 8 needs intubation and MVA Crystaloid solution infusion and treatment of hypotesion (15% incidence of hypotension ) presence of one episode of shock > 3 min(mostly hypovolemic) increases mortality by up to 50% minimum of syst bp of 100mmhg to maintain adequate cerebral perfusion Systemic approach GCS and B S reflexes Management protocols Immediate intubation and CT brain ilateral cervical xray, Cxr. us abd, pelvic xr. DPL for all severe injured Surgery if CT shows a midline shift(manitol if FND before CT) Ur cath, NG, laboratory tests.cardio-respir. Parameters monitoring.controlled ventilation.peep.hyperventilation.tracheostomy.chest toilet, physiotherapy.neuromuscular paralysis.sedation.b gasses,electrolytes monitoring.antiepileptics.raised intracranial pressure treatment

23 GCS Best motor response Obey command Localize the pain Withdrawal to pain Flexion to pain Extention to pain none Verbal response oriented confused Inapprop riate word Incompre hensible sound none Eye opening Spontaneo us To verbal To pain none
24 Low risk group Asymptomatic Head ache Dizziness Scalp hematoma Scalp laceration Absence of moderate or high risk criteria Moderate risk group History of change of consciousness History of progressive headache Alcohol or drug intoxication Unreliable or inadequate history Age less than 2 years Post traumatic seizure or vomiting or amnesia Multiple trauma Serious facial injury Signs of basal fracture Possible skull penetration Depressed fracture Child abuse High risk group Depressed level of consciousnesss not due to drugs or other causes Focal signs Decreasing LOC Penetrating skull injury Palpable depressed fracture Observation alone Observation for high risk signs Consider CT Neurosurgical consultation Consider urgent CT & Neurosurgical consultation& examination
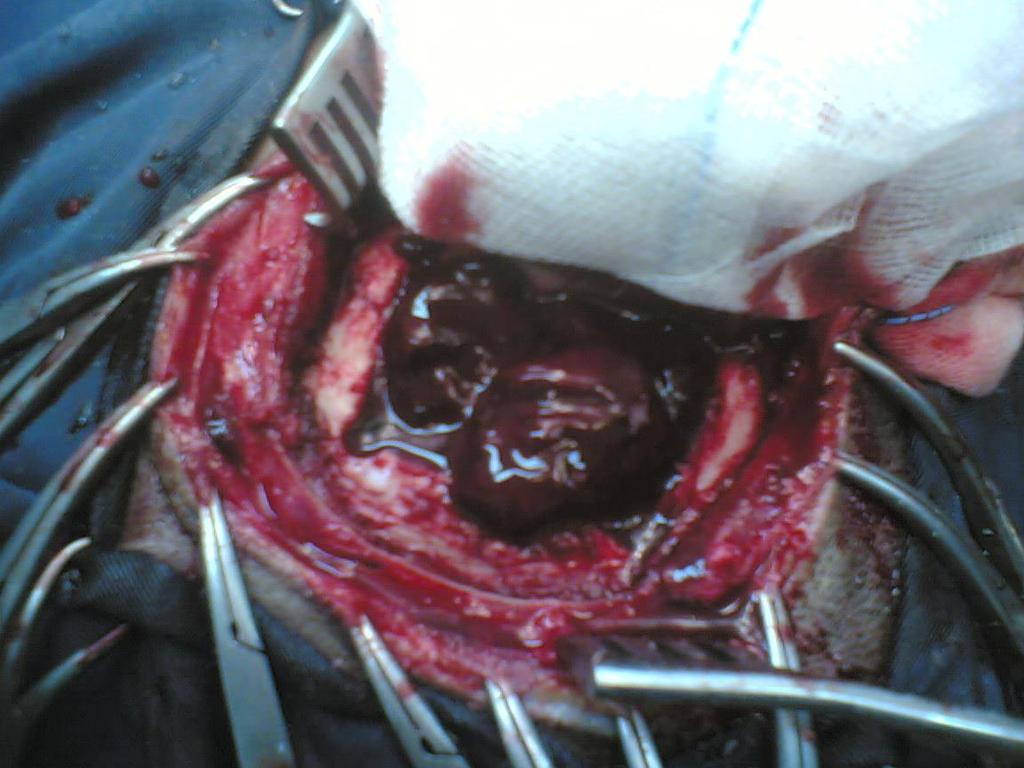
25 Scalp Injuries 1.Injuries severe enough to damage scalp may also damage the underlying skull 2.Acomplete examination of the whole patient is mandatory layers of scalp are S C A L P Skin C.T Aponeurotic (Galia) Areolar tissue Periosteum
26

27 Types Lacerations Avulsions Physical injuries Chemical injuries
28 Scalp Lacerations Small and linear either superficial one (bleeder) or deep one (less beeder) mostly closed under L.A in 2 layers (Galia and skin) Stellated and large either superficial one (bleeder) or deep one (less beeder) mostly closed under G.A especially in children, extensive debridement is unnecessary, all devitalised tissue should be derbided.
29 Reconstruction ladder 1. primary suturing in simple lacerations,sharp, without tissue loss and gross contamination 2. secondary intention in wounds with minimum tissue loss 3. debridement and a split thickness graft in wounds with extensive tissue loss and intact pericranium 4. local flaps in wounds with extensive tissue loss and stripped pericranium and a split thickness graft for donor area (if a defect is left) 5. Pedicular flaps can be used if local flaps are not sufficient especially for occipital areas and small defects 6. Free tissue transplant is used for anterior and large areas

30

31

32

33 Scalp swelling and hematomas 1.Caput succedaneum 2.Cephal hematoma 3.Subglial hematomas
 Comminuted Depressed Linear Diastatic")
34 Skull fractures classification 1.by pattern (according to amount of energy,ratio of impact force to surface area) Comminuted Depressed Linear Diastatic Basal fractures Growing 2.by type Opened Closed 3.by anatomic location Basal convexity
35
36

37

38
39


40

41

42

43

44

45

46
47 Treatment roles Comminuted (replacement as a cranioplasty if not infected with treatment of other associated injuries) Linear fractures (no treatment but observation if closed, debridement if infected and compound) Depressed(replacement as a cranioplasty if not infected, otherwise good debridement and craniectomy) Basilar skull fracture (observation for two days, avoid irrigation of the nose or ear, avoid probing, detailed auditory and vestibular examination is performed at6 weeks interval) Frontal sinus fracture (if in the posterior wall cranialization is necessary)
48 Types of traumatic intracranial leasions Focal(epidural hematoma-subdural hematoma-brain contussion-intracerebral hematomas-focal subarachnoid hematoma) Diffused(subarachnoid hemorhagediffused axonal injury-concussion)

49
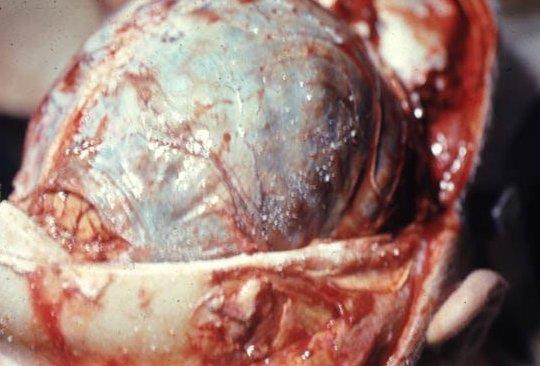
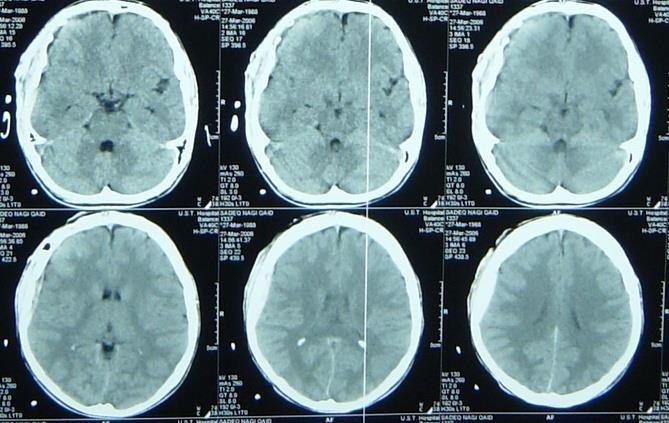
50 Traumatic intracranial hematomas Acute subdural accelerate high speed impact tearing of bridging veins bleeding from cortical vessels, venous sinuses acute brain trauma may coexist altered level of consciousness and focal neurological deficit are common CT and rapid evaluation are necessary If no signs of rapid deterioration or progressive neurological deficit,no mass effect so observation and control of intracranial p. is necessary, otherwise surgery is the role)

51

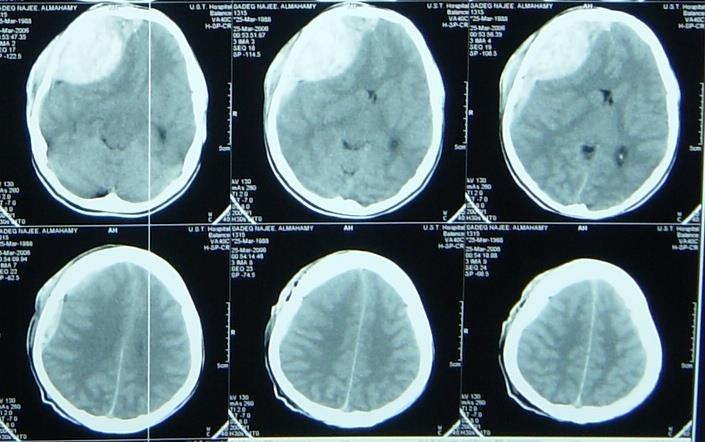
52 Acute Subdural Hematoma Another example of acute subdural hematoma with a midline shift (noncontrast CT)

53 Chronic subdural Mostly in those over 50 years old ½ of patients have got no history of trauma If there is any history of trauma, it is trivial Alcoholism, epilepsy, coagulopathy are common Dementia is common presentation In minimal neuological deficit,medical management is the role If not successful, deterioration of neurological picture so surgery usually by burr hole evacuation.

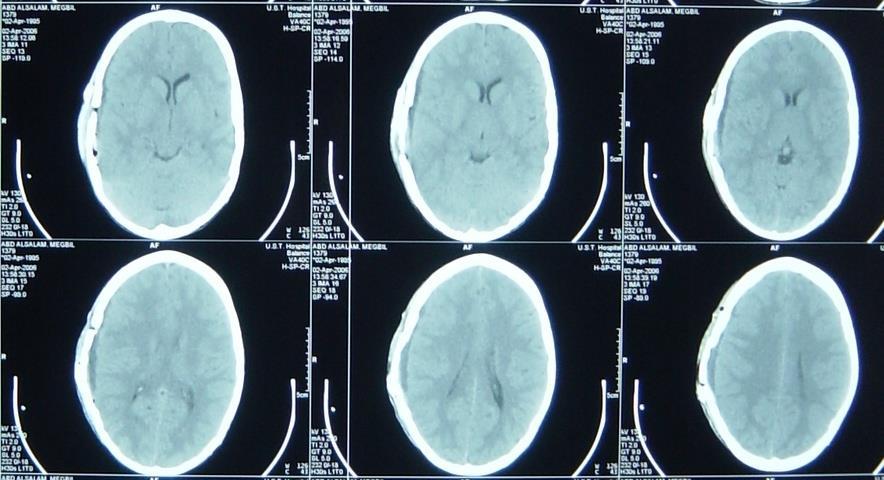
54 Subacute Subdural Hematoma Noncontrast CT note the clot appears less dense in this subacute subdural hematoma.

55

56
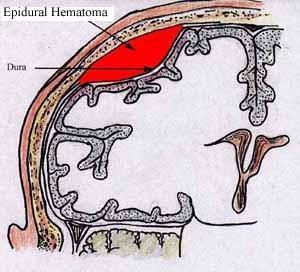
57 Extradural hematomas Mostly resulting from meningial vessel tear (arteries > Veins > sinuses) Fractures are common associated injury Severe associated brain injury is rare Level of consciousness is variable If with mass effect must be evacuated within ½ hour if small follow up is recommended Prognosis depends on level of consciousness at time of presentation
58
59

60
61
62

63
64
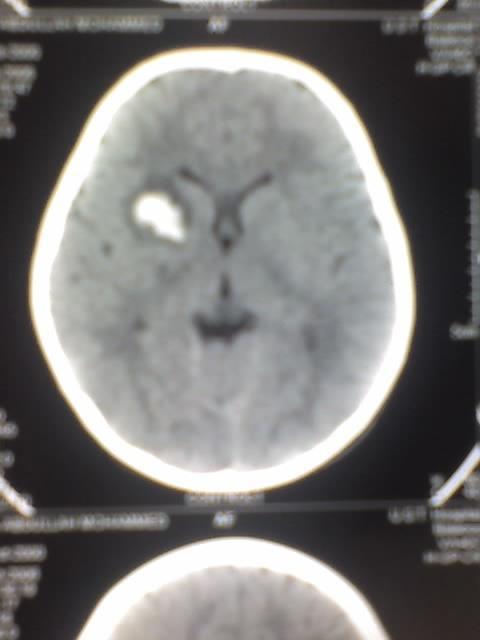
65 Cerebral contusions Small and deep one needs follow up Large and with mass effect needs lobectomy Large one may herniate as late as 9 days post trauma Level of consciousness depends on size of contusion and location

66
67

68

69 SAH more examples Subarachnoid hemorrhage in the right sylvian fissure

70 SAH more examples Blood in the sulci Edema causing a midline shift
71 Posterior fossa hematomas Usually arise from venous sinuses hemorhage Deterioration in level of consciousness is rappid and signs of brain stem and long tract compression are common innitial finding Urgent evacuation is the role
72 Penetrating head injuries Sonic waves and cavitations and decavitation and secondary insults are the injurious mechanisms Infection rates are high Injury far away from site of entrance and exit is common Control of homodynamic state is the initial management Surgical interventions are limited to debridement and removal of mass hematomas and for selected cases Prognosis is usually bad
73

74
75 Questions What are the types of skull fractures What are the parameters of GCS Enumerate the types of traumatic scalp swellings Enumerate the signs and symptoms of raised intracranisl pressure What are the types of traumatic intracranial hemorrhages Right about types of mechanisms of head injury What is the pathophysiology of head injury
76 THANK YOU
10/6/2017. Notice. Traumatic Brain Injury & Head Trauma
 Notice All EMS Live@Nite presentations will be recorded (both audio and video) and available for public viewing online. By participating in EMS Live@Nite, you consent to audio and video recording and its/their
Notice All EMS Live@Nite presentations will be recorded (both audio and video) and available for public viewing online. By participating in EMS Live@Nite, you consent to audio and video recording and its/their
Pre-hospital Response to Trauma and Brain Injury. Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center
 Pre-hospital Response to Trauma and Brain Injury Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center Traumatic Brain Injury is Common 235,000 Americans hospitalized for non-fatal TBI
Pre-hospital Response to Trauma and Brain Injury Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center Traumatic Brain Injury is Common 235,000 Americans hospitalized for non-fatal TBI
8/29/2011. Brain Injury Incidence: 200/100,000. Prehospital Brain Injury Mortality Incidence: 20/100,000
 Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
HEAD INJURY. Dept Neurosurgery
 HEAD INJURY Dept Neurosurgery INTRODUCTION PATHOPHYSIOLOGY CLINICAL CLASSIFICATION MANAGEMENT - INVESTIGATIONS - TREATMENT INTRODUCTION Most head injuries are due to an impact between the head and another
HEAD INJURY Dept Neurosurgery INTRODUCTION PATHOPHYSIOLOGY CLINICAL CLASSIFICATION MANAGEMENT - INVESTIGATIONS - TREATMENT INTRODUCTION Most head injuries are due to an impact between the head and another
V. CENTRAL NERVOUS SYSTEM TRAUMA
 V. CENTRAL NERVOUS SYSTEM TRAUMA I. Concussion - Is a clinical syndrome of altered consiousness secondary to head injury - Brought by a change in the momentum of the head when a moving head suddenly arrested
V. CENTRAL NERVOUS SYSTEM TRAUMA I. Concussion - Is a clinical syndrome of altered consiousness secondary to head injury - Brought by a change in the momentum of the head when a moving head suddenly arrested
Neuropathology Of Head Trauma. Mary E. Case, M.D. Professor of Pathology St. Louis University Health Sciences Center
 Neuropathology Of Head Trauma Mary E. Case, M.D. Professor of Pathology St. Louis University Health Sciences Center Nothing to disclose Disclosure Introduction 500,000 cases/year of serious head injury
Neuropathology Of Head Trauma Mary E. Case, M.D. Professor of Pathology St. Louis University Health Sciences Center Nothing to disclose Disclosure Introduction 500,000 cases/year of serious head injury
Brain Injuries. Presented By Dr. Said Said Elshama
 Brain Injuries Presented By Dr. Said Said Elshama Types of head injuries 1- Scalp injuries 2- Skull injuries 3- Intra Cranial injuries ( Brain ) Anatomical structure of meninges Intra- Cranial Injuries
Brain Injuries Presented By Dr. Said Said Elshama Types of head injuries 1- Scalp injuries 2- Skull injuries 3- Intra Cranial injuries ( Brain ) Anatomical structure of meninges Intra- Cranial Injuries
PRACTICE GUIDELINE. DEFINITIONS: Mild head injury: Glasgow Coma Scale* (GCS) score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8
 score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8") PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
TBI are twice as common in males High potential for poor outcome Deaths occur at three points in time after injury
 Head Injury Any trauma to (closed vs. open) Skull Scalp Brain Traumatic brain injury (TBI) High incidence Most common causes Falls Motor vehicle accidents Other causes Firearm- related injuries Assaults
Head Injury Any trauma to (closed vs. open) Skull Scalp Brain Traumatic brain injury (TBI) High incidence Most common causes Falls Motor vehicle accidents Other causes Firearm- related injuries Assaults
Traumatic Brain Injuries
 Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
Traumatic brain injuries are caused by external mechanical forces such as: - Falls - Transport-related accidents - Assault
 PP2231 Brain injury Cerebrum consists of frontal, parietal, occipital and temporal lobes Diencephalon consists of thalamus, hypothalamus Cerbellum Brain stem consists of midbrain, pons, medulla Central
PP2231 Brain injury Cerebrum consists of frontal, parietal, occipital and temporal lobes Diencephalon consists of thalamus, hypothalamus Cerbellum Brain stem consists of midbrain, pons, medulla Central
Head CT Scan Interpretation: A Five-Step Approach to Seeing Inside the Head Lawrence B. Stack, MD
 Head CT Scan Interpretation: A Five-Step Approach to Seeing Inside the Head Lawrence B. Stack, MD Five Step Approach 1. Adequate study 2. Bone windows 3. Ventricles 4. Quadrigeminal cistern 5. Parenchyma
Head CT Scan Interpretation: A Five-Step Approach to Seeing Inside the Head Lawrence B. Stack, MD Five Step Approach 1. Adequate study 2. Bone windows 3. Ventricles 4. Quadrigeminal cistern 5. Parenchyma
Management of Severe Traumatic Brain Injury
 Guideline for North Bristol Trust Management of Severe Traumatic Brain Injury This guideline describes the following: Initial assessment and management of the patient with head injury Indications for CT
Guideline for North Bristol Trust Management of Severe Traumatic Brain Injury This guideline describes the following: Initial assessment and management of the patient with head injury Indications for CT
Classical CNS Disease Patterns
 Classical CNS Disease Patterns Inflammatory Traumatic In response to the trauma of having his head bashed in GM would have experienced some of these features. NOT TWO LITTLE PEENY WEENY I CM LACERATIONS.
Classical CNS Disease Patterns Inflammatory Traumatic In response to the trauma of having his head bashed in GM would have experienced some of these features. NOT TWO LITTLE PEENY WEENY I CM LACERATIONS.
8th Annual NKY TBI Conference 3/28/2014
 Closed Head Injury: Headache to Herniation A N T H O N Y T. K R A M E R U N I V E R S I T Y O F C I N C I N N A T I B L U E A S H E M S T E C H N O L O G Y P R O G R A M Objectives Describe the pathological
Closed Head Injury: Headache to Herniation A N T H O N Y T. K R A M E R U N I V E R S I T Y O F C I N C I N N A T I B L U E A S H E M S T E C H N O L O G Y P R O G R A M Objectives Describe the pathological
Head injuries. Severity of head injuries
 Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
Mild Traumatic Brain Injury
 Mild Traumatic Brain Injury Concussions This presentation is for information purposes only, not for any commercial purpose, and may not be sold or redistributed. David Wesley, M.D. Outline Epidemiology
Mild Traumatic Brain Injury Concussions This presentation is for information purposes only, not for any commercial purpose, and may not be sold or redistributed. David Wesley, M.D. Outline Epidemiology
Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth. Objectives 11/7/2017
 Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth Objectives 1. Be able to discuss brain anatomy and physiology as it applies to
Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth Objectives 1. Be able to discuss brain anatomy and physiology as it applies to
Introduction to Neurosurgical Subspecialties:
 Introduction to Neurosurgical Subspecialties: Trauma and Critical Care Neurosurgery Brian L. Hoh, MD 1, Gregory J. Zipfel, MD 2 and Stacey Q. Wolfe, MD 3 1 University of Florida, 2 Washington University,
Introduction to Neurosurgical Subspecialties: Trauma and Critical Care Neurosurgery Brian L. Hoh, MD 1, Gregory J. Zipfel, MD 2 and Stacey Q. Wolfe, MD 3 1 University of Florida, 2 Washington University,
Traumatic Brain Injury TBI Presented by Bill Masten
 1 2 Cerebrum two hemispheres and four lobes. Cerebellum (little brain) coordinates the back and forth ballet of motion. It judges the timing of every movement precisely. Brainstem coordinates the bodies
1 2 Cerebrum two hemispheres and four lobes. Cerebellum (little brain) coordinates the back and forth ballet of motion. It judges the timing of every movement precisely. Brainstem coordinates the bodies
European Resuscitation Council
 European Resuscitation Council Incidence of Trauma in Childhood Leading cause of death and disability in children older than one year all over the world Structured approach Primary survey and resuscitation
European Resuscitation Council Incidence of Trauma in Childhood Leading cause of death and disability in children older than one year all over the world Structured approach Primary survey and resuscitation
BATLS Battlefield Advanced Trauma Life Support
 J R Army Med Corps 2002; 148: 151-158 BATLS Battlefield Advanced Trauma Life Support CHAPTER 8 HEAD INJURIES Aim 0801. On successfully completing this topic you will be able to: Discuss general management
J R Army Med Corps 2002; 148: 151-158 BATLS Battlefield Advanced Trauma Life Support CHAPTER 8 HEAD INJURIES Aim 0801. On successfully completing this topic you will be able to: Discuss general management
Traumatic Brain Injury
 Traumatic Brain Injury Mark J. Harris M.D. Associate Professor University of Utah Salt Lake City USA Overview In US HI responsible for 33% trauma deaths. Closed HI 80% Missile / Penetrating HI 20% Glasgow
Traumatic Brain Injury Mark J. Harris M.D. Associate Professor University of Utah Salt Lake City USA Overview In US HI responsible for 33% trauma deaths. Closed HI 80% Missile / Penetrating HI 20% Glasgow
LOSS OF CONSCIOUSNESS & ASSESSMENT. Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT
 LOSS OF CONSCIOUSNESS & ASSESSMENT Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT OUTLINE Causes Head Injury Clinical Features Complications Rapid Assessment Glasgow Coma Scale Classification
LOSS OF CONSCIOUSNESS & ASSESSMENT Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT OUTLINE Causes Head Injury Clinical Features Complications Rapid Assessment Glasgow Coma Scale Classification
Pediatric Head Trauma August 2016
 PEDIATRIC HEAD TRAUMA AUGUST 2016 Pediatric Head Trauma August 2016 EDUCATION COMMITTEE PEER EDUCATION Quick Review of Pathophysiology of TBI Nuggets of knowledge to keep in mind with TBI Intracranial
PEDIATRIC HEAD TRAUMA AUGUST 2016 Pediatric Head Trauma August 2016 EDUCATION COMMITTEE PEER EDUCATION Quick Review of Pathophysiology of TBI Nuggets of knowledge to keep in mind with TBI Intracranial
Chapter 26 Head and Spine Trauma The Nervous System The nervous system controls virtually all of our body activities including reflex, voluntary and
 1 2 3 4 5 Chapter 26 Head and Spine Trauma The Nervous System The nervous system controls virtually all of our body activities including reflex, voluntary and involuntary activities Voluntary activities
1 2 3 4 5 Chapter 26 Head and Spine Trauma The Nervous System The nervous system controls virtually all of our body activities including reflex, voluntary and involuntary activities Voluntary activities
Virtual Mentor American Medical Association Journal of Ethics August 2008, Volume 10, Number 8:
 Virtual Mentor American Medical Association Journal of Ethics August 2008, Volume 10, Number 8: 516-520. CLINICAL PEARL The Hazards of Stopping a Brain in Motion: Evaluation and Classification of Traumatic
Virtual Mentor American Medical Association Journal of Ethics August 2008, Volume 10, Number 8: 516-520. CLINICAL PEARL The Hazards of Stopping a Brain in Motion: Evaluation and Classification of Traumatic
Head Trauma Inservice (October)
") John Tramell - Head Trauma Inservice, October 2005.doc Page 1 Head Trauma Inservice (October) Head trauma is the leading cause of death in trauma patients. Having a basic understanding of the anatomy and
John Tramell - Head Trauma Inservice, October 2005.doc Page 1 Head Trauma Inservice (October) Head trauma is the leading cause of death in trauma patients. Having a basic understanding of the anatomy and
Most hypertensive: headache, vomiting, seizures, changes in mental status, fever, changes EKG
 Wk 2. Management of Clients with Stroke 1. Stroke neurologic changes by interruption in blood supply to brain 1) Etiology Ischemia: thrombosis or embolism thrombotic strokes > embolic strokes (1) Thrombosis
Wk 2. Management of Clients with Stroke 1. Stroke neurologic changes by interruption in blood supply to brain 1) Etiology Ischemia: thrombosis or embolism thrombotic strokes > embolic strokes (1) Thrombosis
USASOC Neurocognitive Testing and Post Injury Evaluation and Treatment Clinical Practice Guideline (CPG)
") USASOC Neurocognitive Testing and Post Injury Evaluation and Treatment Clinical Practice Guideline (CPG) Note: The intent of this CPG is to serve as general guidance for medics and medical officers. It
USASOC Neurocognitive Testing and Post Injury Evaluation and Treatment Clinical Practice Guideline (CPG) Note: The intent of this CPG is to serve as general guidance for medics and medical officers. It
Chapter 31. Objectives. Objectives 01/09/2013. Head Trauma
 Chapter 31 Head Trauma Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1. Define key terms introduced
Chapter 31 Head Trauma Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1. Define key terms introduced
Surgical Care at the District Hospital. EMERGENCY & ESSENTIAL SURGICAL CARE
 Surgical Care at the District Hospital 1 17 Orthopedic Techniques Key Points 2 17.1 Traction Use an appropriate method of traction to treat fractures of the extremities and cervical spine Apply extremity
Surgical Care at the District Hospital 1 17 Orthopedic Techniques Key Points 2 17.1 Traction Use an appropriate method of traction to treat fractures of the extremities and cervical spine Apply extremity
3. D Objective: Chapter 4, Objective 4 Page: 79 Rationale: A carbon dioxide level below 35 mmhg indicates hyperventilation.
 1. A Objective: Chapter 1, Objective 3 Page: 14 Rationale: The sudden increase in acceleration produces posterior displacement of the occupants and possible hyperextension of the cervical spine if the
1. A Objective: Chapter 1, Objective 3 Page: 14 Rationale: The sudden increase in acceleration produces posterior displacement of the occupants and possible hyperextension of the cervical spine if the
Standardize comprehensive care of the patient with severe traumatic brain injury
 Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Management Strategies for Communited Fractures of Frontal Skull Base: An Institutional Experience
 80 Original Article THIEME Management Strategies for Communited Fractures of Frontal Skull Base: An Institutional Experience V. Velho 1 Hrushikesh U. Kharosekar 1 Jasmeet S. Thukral 1 Shonali Valsangkar
80 Original Article THIEME Management Strategies for Communited Fractures of Frontal Skull Base: An Institutional Experience V. Velho 1 Hrushikesh U. Kharosekar 1 Jasmeet S. Thukral 1 Shonali Valsangkar
Pediatric Advanced Life Support
 Pediatric Advanced Life Support Pediatric Chain of Survival Berg M D et al. Circulation 2010;122:S862-S875 Prevention Early cardiopulmonary resuscitation (CPR) Prompt access to the emergency response system
Pediatric Advanced Life Support Pediatric Chain of Survival Berg M D et al. Circulation 2010;122:S862-S875 Prevention Early cardiopulmonary resuscitation (CPR) Prompt access to the emergency response system
10. Severe traumatic brain injury also see flow chart Appendix 5
 10. Severe traumatic brain injury also see flow chart Appendix 5 Introduction Severe traumatic brain injury (TBI) is the leading cause of death in children in the UK, accounting for 15% of deaths in 1-15
10. Severe traumatic brain injury also see flow chart Appendix 5 Introduction Severe traumatic brain injury (TBI) is the leading cause of death in children in the UK, accounting for 15% of deaths in 1-15
TRAUMATIC BRAIN INJURY. Moderate and Severe Brain Injury
 TRAUMATIC BRAIN INJURY Moderate and Severe Brain Injury Disclosures Funded research: 1. NIH: RO1 Physiology of concussion 2016-2021, Co-PI, $2,000,000 2. American Medical Society of Sports Medicine: RCT
TRAUMATIC BRAIN INJURY Moderate and Severe Brain Injury Disclosures Funded research: 1. NIH: RO1 Physiology of concussion 2016-2021, Co-PI, $2,000,000 2. American Medical Society of Sports Medicine: RCT
Injuries to the head and spine
 Injuries to the head and spine Aaron J. Katz, AEMT-P, CIC www.es26medic.net 2013 Nervous System Two sub-systems Central Nervous System ( CNS ) Brain and spinal cord Peripheral Nervous System 12 cranial
Injuries to the head and spine Aaron J. Katz, AEMT-P, CIC www.es26medic.net 2013 Nervous System Two sub-systems Central Nervous System ( CNS ) Brain and spinal cord Peripheral Nervous System 12 cranial
Index. Note: Page numbers of article titles are in bold face type.
 Neurosurg Clin N Am 13 (2002) 259 264 Index Note: Page numbers of article titles are in bold face type. A Abdominal injuries, in child abuse, 150, 159 Abrasions, in child abuse, 157 Abuse, child. See Child
Neurosurg Clin N Am 13 (2002) 259 264 Index Note: Page numbers of article titles are in bold face type. A Abdominal injuries, in child abuse, 150, 159 Abrasions, in child abuse, 157 Abuse, child. See Child
Pediatric Abusive Head Trauma
 Pediatric Abusive Head Trauma Rebecca Girardet Associate Professor of Pediatrics Director, Division of Child Protection Pediatrics McGovern Medical School at The University of Texas Health Science Center
Pediatric Abusive Head Trauma Rebecca Girardet Associate Professor of Pediatrics Director, Division of Child Protection Pediatrics McGovern Medical School at The University of Texas Health Science Center
Head injuries in children. Dr Jason Hort Paediatrician Paediatric Emergency Physician, June 2017 Children s Hospital Westmead
 Head injuries in children Dr Jason Hort Paediatrician Paediatric Emergency Physician, June 2017 Children s Hospital Westmead Objectives Approach to minor head injury Child protection issues Concussion
Head injuries in children Dr Jason Hort Paediatrician Paediatric Emergency Physician, June 2017 Children s Hospital Westmead Objectives Approach to minor head injury Child protection issues Concussion
Head & Brain Trauma. Presented By: Steven Jones, NREMT-P
 Head & Brain Trauma Presented By: Steven Jones, NREMT-P Head & Brain Trauma ~ 4 million head injuries in US per year ~ 450,000 require hospitalization Most are minor injuries Major head injury most common
Head & Brain Trauma Presented By: Steven Jones, NREMT-P Head & Brain Trauma ~ 4 million head injuries in US per year ~ 450,000 require hospitalization Most are minor injuries Major head injury most common
Introduction to Emergency Medical Care 1
 Introduction to Emergency Medical Care 1 OBJECTIVES 31.1 Define key terms introduced in this chapter. Slides 13 15, 17, 19, 28 31.2 Describe the components and function of the nervous system and the anatomy
Introduction to Emergency Medical Care 1 OBJECTIVES 31.1 Define key terms introduced in this chapter. Slides 13 15, 17, 19, 28 31.2 Describe the components and function of the nervous system and the anatomy
UHSM ED Pathway ELDERLY FALL / COLLAPSE
 UHSM ED Pathway ELDERLY FALL / COLLAPSE Patient name / Pathway for patients who require assessment in ED after a fall or collapse Note: - It can be used if the patient has also sustained a minor head injury
UHSM ED Pathway ELDERLY FALL / COLLAPSE Patient name / Pathway for patients who require assessment in ED after a fall or collapse Note: - It can be used if the patient has also sustained a minor head injury
ATLS: Initial Assessment and Management. SAUSHEC Medical Student Lecture Series
 ATLS: Initial Assessment and Management SAUSHEC Medical Student Lecture Series Objectives Identify sequence of priorities in assessing the multiply injured patient Apply principles outlined in primary
ATLS: Initial Assessment and Management SAUSHEC Medical Student Lecture Series Objectives Identify sequence of priorities in assessing the multiply injured patient Apply principles outlined in primary
THE ESSENTIAL BRAIN INJURY GUIDE
 THE ESSENTIAL BRAIN INJURY GUIDE Neuroanatomy & Neuroplasticity Section 2 Contributors Erin D. Bigler, PhD Michael R. Hoane, PhD Stephanie Kolakowsky-Hayner, PhD, CBIST, FACRM Dorothy A. Kozlowski, PhD
THE ESSENTIAL BRAIN INJURY GUIDE Neuroanatomy & Neuroplasticity Section 2 Contributors Erin D. Bigler, PhD Michael R. Hoane, PhD Stephanie Kolakowsky-Hayner, PhD, CBIST, FACRM Dorothy A. Kozlowski, PhD
INTRACRANIAL PRESSURE -!!
 INTRACRANIAL PRESSURE - Significance raised ICP main cause of death in severe head injury main cause of morbidity in moderate and mild head injury main target and prognostic indicator in the ITU setting
INTRACRANIAL PRESSURE - Significance raised ICP main cause of death in severe head injury main cause of morbidity in moderate and mild head injury main target and prognostic indicator in the ITU setting
NEURO IMAGING 2. Dr. Said Huwaijah Chairman of radiology Dep, Damascus Univercity
 NEURO IMAGING 2 Dr. Said Huwaijah Chairman of radiology Dep, Damascus Univercity I. EPIDURAL HEMATOMA (EDH) LOCATION Seventy to seventy-five percent occur in temporoparietal region. CAUSE Most likely caused
NEURO IMAGING 2 Dr. Said Huwaijah Chairman of radiology Dep, Damascus Univercity I. EPIDURAL HEMATOMA (EDH) LOCATION Seventy to seventy-five percent occur in temporoparietal region. CAUSE Most likely caused
Acute Neurosurgical Emergency Transfer [see also CATS SOP neurosurgical]
![Acute Neurosurgical Emergency Transfer [see also CATS SOP neurosurgical]](/thumbs/87/96512765.jpg "Acute Neurosurgical Emergency Transfer [see also CATS SOP neurosurgical]") Children s Acute Transport Service Clinical Guidelines Acute Neurosurgical Emergency Transfer [see also CATS SOP neurosurgical] Document Control Information Author D Lutman Author Position Head of Clinical
Children s Acute Transport Service Clinical Guidelines Acute Neurosurgical Emergency Transfer [see also CATS SOP neurosurgical] Document Control Information Author D Lutman Author Position Head of Clinical
Trauma Life Support Pre-Hospital (TLS-P) Preparatory Materials
 Preparatory Materials") Trauma Life Support Pre-Hospital (TLS-P) Preparatory Materials 1 1. A high-risk bodily fluid for spreading infection is blood. 2. Items that can reduce the spread of infection include masks, gloves, and
Trauma Life Support Pre-Hospital (TLS-P) Preparatory Materials 1 1. A high-risk bodily fluid for spreading infection is blood. 2. Items that can reduce the spread of infection include masks, gloves, and
Pediatric Trauma Initial Evaluation and management
 Pediatric Trauma Initial Evaluation and management Head Injury Closed head injury Penetrating head injury Closed Head Injury without Fractures Head injury is the most common cause of death and disability
Pediatric Trauma Initial Evaluation and management Head Injury Closed head injury Penetrating head injury Closed Head Injury without Fractures Head injury is the most common cause of death and disability
1. In a rear-impact motor vehicle crash, which area of the spine is most susceptible to injury? A. Cervical B. Thoracic C. Lumbar D.
 1. In a rear-impact motor vehicle crash, which area of the spine is most susceptible to injury? A. Cervical B. Thoracic C. Lumbar D. Sacral-coccygeal 2. A 36-year-old male sustains blunt force thoracic
1. In a rear-impact motor vehicle crash, which area of the spine is most susceptible to injury? A. Cervical B. Thoracic C. Lumbar D. Sacral-coccygeal 2. A 36-year-old male sustains blunt force thoracic
68W COMBAT MEDIC POCKET GUIDE
 GTA 08-05-058 68W COMBAT MEDIC POCKET GUIDE PART I: TRAUMA TREATMENT This publication contains technical information that is for official Government use only. Distribution is limited to U.S. Government
GTA 08-05-058 68W COMBAT MEDIC POCKET GUIDE PART I: TRAUMA TREATMENT This publication contains technical information that is for official Government use only. Distribution is limited to U.S. Government
Time Equals Neurons - Spinal Cord Injury Management in the first 4 Hours
 Time Equals Neurons - Spinal Cord Injury Management in the first 4 Hours William D. Whetstone M.D. Clinical Professor UCSF Department of Emergency Medicine SFGH ED Center for Neuro-Critical Emergencies
Time Equals Neurons - Spinal Cord Injury Management in the first 4 Hours William D. Whetstone M.D. Clinical Professor UCSF Department of Emergency Medicine SFGH ED Center for Neuro-Critical Emergencies
Head Injury כל הזכויות שמורות למד"א מרחב ירושלים. Dan Drory, EMT-P, Instructor
 Head Injury Dan Drory, EMT-P, Instructor Anatomy on a fingertip The brain is a soft and gentle tissue. The brain is the most important organ. כל הזכויות שמורות למד"א מרחב ירושלים Protective layers of the
Head Injury Dan Drory, EMT-P, Instructor Anatomy on a fingertip The brain is a soft and gentle tissue. The brain is the most important organ. כל הזכויות שמורות למד"א מרחב ירושלים Protective layers of the
The dura is sensitive to stretching, which produces the sensation of headache.
 Dural Nerve Supply Branches of the trigeminal, vagus, and first three cervical nerves and branches from the sympathetic system pass to the dura. Numerous sensory endings are in the dura. The dura is sensitive
Dural Nerve Supply Branches of the trigeminal, vagus, and first three cervical nerves and branches from the sympathetic system pass to the dura. Numerous sensory endings are in the dura. The dura is sensitive
Case 1. Case 5/30/2013. Traumatic Brain Injury : Review, Update, and Controversies
 Case 1 Traumatic Brain Injury : Review, Update, and Controversies Shirley I. Stiver MD, PhD 32 year old male s/p high speed MVA Difficult extrication Intubated at scene Case BP 75 systolic / palp GCS 3
Case 1 Traumatic Brain Injury : Review, Update, and Controversies Shirley I. Stiver MD, PhD 32 year old male s/p high speed MVA Difficult extrication Intubated at scene Case BP 75 systolic / palp GCS 3
Traumatic Head Injury
 Traumatic Head Injury Liu Yi, MD. PhD, associate professor Dept. Neurosurgery Conception Any injury to the skull, or brain, caused by external physical forces, in stead of degenerative or congenital nature
Traumatic Head Injury Liu Yi, MD. PhD, associate professor Dept. Neurosurgery Conception Any injury to the skull, or brain, caused by external physical forces, in stead of degenerative or congenital nature
Brief Clinical Report: Recognizing Subdural Hemorrhage in Older Adults
 Research Brief Clinical Report: Recognizing Subdural Hemorrhage in Older Adults Mark T. Pfefer, RN, MS, DC *1 ; Richard Strunk MS, DC 2 Address: 1 Professor and Director of Research, Cleveland Chiropractic
Research Brief Clinical Report: Recognizing Subdural Hemorrhage in Older Adults Mark T. Pfefer, RN, MS, DC *1 ; Richard Strunk MS, DC 2 Address: 1 Professor and Director of Research, Cleveland Chiropractic
Neurotrauma. Béla Faludi Dept.. of Neurology University of PécsP
 Neurotrauma Béla Faludi Dept.. of Neurology University of PécsP Emergency!!! Why here? Opened cranial injury visible: neurosurgery Closed injuries sometimes diagnosed by neurologist Masking situation:
Neurotrauma Béla Faludi Dept.. of Neurology University of PécsP Emergency!!! Why here? Opened cranial injury visible: neurosurgery Closed injuries sometimes diagnosed by neurologist Masking situation:
:: Closed Head Injury in Adults
 ADULT TRAUMA CLINICAL PRACTICE GUIDELINES Initial Management of :: Closed Head Injury in Adults Suggested citation: Dr Duncan Reed 2007, Adult Trauma Clinical Practice Guidelines, Initial Management of
ADULT TRAUMA CLINICAL PRACTICE GUIDELINES Initial Management of :: Closed Head Injury in Adults Suggested citation: Dr Duncan Reed 2007, Adult Trauma Clinical Practice Guidelines, Initial Management of
ITLS Advanced Pre-Test Annotated Key 8 th Edition
 1. A Objective: Chapter 1, Objective 3 Page: 14 Rationale: The sudden increase in acceleration produces posterior displacement of the occupants and possible hyperextension of the cervical spine if the
1. A Objective: Chapter 1, Objective 3 Page: 14 Rationale: The sudden increase in acceleration produces posterior displacement of the occupants and possible hyperextension of the cervical spine if the
Emergency Room Resuscitation of the Unstable Trauma Patient
 Emergency Room Resuscitation of the Unstable Trauma Patient Goals of trauma resuscitation Maintain: Systemic oxygenation Systemic perfusion Neurologic function Approach to unstable trauma patient Primary
Emergency Room Resuscitation of the Unstable Trauma Patient Goals of trauma resuscitation Maintain: Systemic oxygenation Systemic perfusion Neurologic function Approach to unstable trauma patient Primary
PTA 106 Unit 1 Lecture 3
 PTA 106 Unit 1 Lecture 3 The Basics Arteries: Carry blood away from the heart toward tissues. They typically have thicker vessels walls to handle increased pressure. Contain internal and external elastic
PTA 106 Unit 1 Lecture 3 The Basics Arteries: Carry blood away from the heart toward tissues. They typically have thicker vessels walls to handle increased pressure. Contain internal and external elastic
Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University
 Dr Mubarak Abdelrahman Assistant Professor Jazan University") Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University SHOCK Definition: Shock is a syndrome = inability to provide sufficient oxygenated blood to tissues. Oxygen
Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University SHOCK Definition: Shock is a syndrome = inability to provide sufficient oxygenated blood to tissues. Oxygen
North Oaks Trauma Symposium Friday, November 3, 2017
 Traumatic Intracranial Hemorrhage Aaron C. Sigler, DO, MS Neurosurgery Tulane Neurosciences None Disclosures Overview Anatomy Epidural hematoma Subdural hematoma Cerebral contusions Outline Traumatic ICH
Traumatic Intracranial Hemorrhage Aaron C. Sigler, DO, MS Neurosurgery Tulane Neurosciences None Disclosures Overview Anatomy Epidural hematoma Subdural hematoma Cerebral contusions Outline Traumatic ICH
For Emergency Doctors. Dr Suzanne Smallbane November 2011
 For Emergency Doctors Dr Suzanne Smallbane November 2011 A: Orbit B: Sphenoid Sinus C: Temporal Lobe D: EAC E: Mastoid air cells F: Cerebellar hemisphere A: Frontal lobe B: Frontal bone C: Dorsum sellae
For Emergency Doctors Dr Suzanne Smallbane November 2011 A: Orbit B: Sphenoid Sinus C: Temporal Lobe D: EAC E: Mastoid air cells F: Cerebellar hemisphere A: Frontal lobe B: Frontal bone C: Dorsum sellae
Shenandoah Co. Fire & Rescue. Injuries to. and Spine. December EMS Training Bill Streett Training Section Chief
 Shenandoah Co. Fire & Rescue Injuries to the Head and Spine December EMS Training Bill Streett Training Section Chief C.E. Card Information BLS Providers 2 Cards / Provider Category 1 Course # Blank Topic#
Shenandoah Co. Fire & Rescue Injuries to the Head and Spine December EMS Training Bill Streett Training Section Chief C.E. Card Information BLS Providers 2 Cards / Provider Category 1 Course # Blank Topic#
Disclosure Statement. Dr. Kadish has no relevant financial relationships with any commercial interests mentioned in this talk.
 Disclosure Statement Dr. Kadish has no relevant financial relationships with any commercial interests mentioned in this talk. Head Trauma Evaluation Primary and secondary injury Disposition Sports related
Disclosure Statement Dr. Kadish has no relevant financial relationships with any commercial interests mentioned in this talk. Head Trauma Evaluation Primary and secondary injury Disposition Sports related
Traumatic Brain Injury (1.2.3) Management of severe TBI ( ) Learning Objectives
 Management of severe TBI ( ) Learning Objectives") Traumatic Brain Injury (1.2.3) 1.2.3.1 Management of severe TBI 1.2.3.2 Management of concussions 1.2.3.3 Sideline management for team medics/physicians 1.4.2.3.10 Controlled hyperventilation for management
Traumatic Brain Injury (1.2.3) 1.2.3.1 Management of severe TBI 1.2.3.2 Management of concussions 1.2.3.3 Sideline management for team medics/physicians 1.4.2.3.10 Controlled hyperventilation for management
Supplementary Table 1. ICD-9/-10 codes used to identify cycling injury hospitalizations. Railway accidents injured pedal cyclist
 Supplementary Table 1. ICD-9/-10 codes used to identify cycling injury hospitalizations. ICD Code ICD-9 E800-E807(.3) E810-E816, E818-E819(.6) E820-E825(.6) E826-E829(.1) ICD-10-CA V10-V19 (including all
Supplementary Table 1. ICD-9/-10 codes used to identify cycling injury hospitalizations. ICD Code ICD-9 E800-E807(.3) E810-E816, E818-E819(.6) E820-E825(.6) E826-E829(.1) ICD-10-CA V10-V19 (including all
Chapter 16 - Depressed consciousness and coma
 Chapter 16 - Depressed consciousness and coma Episode overview: 1) List a broad differential diagnosis for coma 2) List GCS / Pediatric GCS 3) Describe the oculocephalic and oculovestibular reflex Wise
Chapter 16 - Depressed consciousness and coma Episode overview: 1) List a broad differential diagnosis for coma 2) List GCS / Pediatric GCS 3) Describe the oculocephalic and oculovestibular reflex Wise
Traumatic Brain Injury
 General Information Traumatic Brain Injury What you need to know Complicated condition with high variability in etiology, severity, distribution of injury, and pattern of functional impairment (Klyce,
General Information Traumatic Brain Injury What you need to know Complicated condition with high variability in etiology, severity, distribution of injury, and pattern of functional impairment (Klyce,
Cerebro-vascular stroke
 Cerebro-vascular stroke CT Terminology Hypodense lesion = lesion of lower density than the normal brain tissue Hyperdense lesion = lesion of higher density than normal brain tissue Isodense lesion = lesion
Cerebro-vascular stroke CT Terminology Hypodense lesion = lesion of lower density than the normal brain tissue Hyperdense lesion = lesion of higher density than normal brain tissue Isodense lesion = lesion
McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #3 Penetrating Neck Trauma
 McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #3 Penetrating Neck Trauma Penetrating neck injury (PNI) comprises 5 to 10 percent of traumatic injuries
McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #3 Penetrating Neck Trauma Penetrating neck injury (PNI) comprises 5 to 10 percent of traumatic injuries
Clinical Outcome of Borderline Subdural Hematoma with 5-9 mm Thickness and/or Midline Shift 2-5 mm
 Original Article Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2017/300 Clinical Outcome of Borderline Subdural Hematoma with 5-9 mm Thickness and/or Midline Shift 2-5 mm Raja S Vignesh
Original Article Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2017/300 Clinical Outcome of Borderline Subdural Hematoma with 5-9 mm Thickness and/or Midline Shift 2-5 mm Raja S Vignesh
BRAIN TRAUMA THERAPEUTIC RECOMMENDATIONS
 1 BRAIN TRAUMA THERAPEUTIC RECOMMENDATIONS Richard A. LeCouteur, BVSc, PhD, Dip ACVIM (Neurology), Dip ECVN Professor Emeritus, University of California, Davis, California, USA Definitions Hemorrhage:
1 BRAIN TRAUMA THERAPEUTIC RECOMMENDATIONS Richard A. LeCouteur, BVSc, PhD, Dip ACVIM (Neurology), Dip ECVN Professor Emeritus, University of California, Davis, California, USA Definitions Hemorrhage:
Best-evidence Review of Acute Care for Moderate to Severe Traumatic Brain Injury
 Pragmatic Evidence-based Review Best-evidence Review of Acute Care for Moderate to Severe Traumatic Brain Injury Reviewer Mark Ayson MBChB DPH Date Report Completed August 2011 Important Note: It is not
Pragmatic Evidence-based Review Best-evidence Review of Acute Care for Moderate to Severe Traumatic Brain Injury Reviewer Mark Ayson MBChB DPH Date Report Completed August 2011 Important Note: It is not
SUBJECT: Clinical Practice Guideline for the Management of Severe Traumatic Brain Injury
 ASPIRUS WAUSAU HOSPITAL, INC. Passion for excellence. Compassion for people. Effective Date: December 1, 2005 Proposed By: Samuel Picone III, MD, Trauma Medical Director Approval and Dates: Dr. Bunch,
ASPIRUS WAUSAU HOSPITAL, INC. Passion for excellence. Compassion for people. Effective Date: December 1, 2005 Proposed By: Samuel Picone III, MD, Trauma Medical Director Approval and Dates: Dr. Bunch,
A Guide to the Radiologic Evaluation of Extra-Axial Hemorrhage
 July 2013 A Guide to the Radiologic Evaluation of Extra-Axial Hemorrhage John Dickson, Harvard Medical School Year III Agenda 1. Define extra-axial hemorrhage and introduce its subtypes 2. Review coup
July 2013 A Guide to the Radiologic Evaluation of Extra-Axial Hemorrhage John Dickson, Harvard Medical School Year III Agenda 1. Define extra-axial hemorrhage and introduce its subtypes 2. Review coup
CENTRAL NERVOUS SYSTEM TRAUMA and Subarachnoid Hemorrhage. By: Shifaa AlQa qa
 CENTRAL NERVOUS SYSTEM TRAUMA and Subarachnoid Hemorrhage By: Shifaa AlQa qa Subarachnoid Hemorrhage Causes: Rupture of a saccular (berry) aneurysm Vascular malformation Trauma Hematologic disturbances
CENTRAL NERVOUS SYSTEM TRAUMA and Subarachnoid Hemorrhage By: Shifaa AlQa qa Subarachnoid Hemorrhage Causes: Rupture of a saccular (berry) aneurysm Vascular malformation Trauma Hematologic disturbances
Trauma resuscitation in the Elderlyfrom a physiological perspective
 6 November 2017 Trauma resuscitation in the Elderlyfrom a physiological perspective Joseph Mathew Consultant, Emergency/ 6 November 2017 2 http://www.who.int/ageing/publications/global_health.pdf 6 November
6 November 2017 Trauma resuscitation in the Elderlyfrom a physiological perspective Joseph Mathew Consultant, Emergency/ 6 November 2017 2 http://www.who.int/ageing/publications/global_health.pdf 6 November
CNS pathology Third year medical students. Dr Heyam Awad 2018 Lecture 5: disturbed fluid balance and increased intracranial pressure
 CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 5: disturbed fluid balance and increased intracranial pressure ILOs Understand causes and symptoms of increased intracranial pressure.
CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 5: disturbed fluid balance and increased intracranial pressure ILOs Understand causes and symptoms of increased intracranial pressure.
Referral Criteria for Medical CT Radiation Exposures. Neuro Referrals
 Referral Criteria for Medical CT Radiation Exposures Neuro Referrals CHH & HRI The Ionising Radiation (Medical Exposure) Regulations 2017 Document Control Reference No: 3.2 First published: 2016 Version:
Referral Criteria for Medical CT Radiation Exposures Neuro Referrals CHH & HRI The Ionising Radiation (Medical Exposure) Regulations 2017 Document Control Reference No: 3.2 First published: 2016 Version:
Pathophysiology of stroke
 A practical approach to acute stro ke Dr. Sanjith Aaron, M.D., D.M., Professor, Department of Neurosciences, CMC Vellore Stroke is characterized by an abrupt onset of neurological deficit lasting more
A practical approach to acute stro ke Dr. Sanjith Aaron, M.D., D.M., Professor, Department of Neurosciences, CMC Vellore Stroke is characterized by an abrupt onset of neurological deficit lasting more
Head injury in children
 Head injury in children Michael Kim, MD Department of Emergency Medicine University of Wisconsin- Madison #1 cause of death and disability Bimodal distribution 62,000 hospitalization 564,000 ED visits
Head injury in children Michael Kim, MD Department of Emergency Medicine University of Wisconsin- Madison #1 cause of death and disability Bimodal distribution 62,000 hospitalization 564,000 ED visits
Pre-hospital Trauma Life Support. Rattiya Banjungam Emergency Physician, Khon Kaen Hospital
 Pre-hospital Trauma Life Support Rattiya Banjungam Emergency Physician, Khon Kaen Hospital Golden principles of Prehospital Trauma Care Golden Hour There is a golden hour if you are critically injured,
Pre-hospital Trauma Life Support Rattiya Banjungam Emergency Physician, Khon Kaen Hospital Golden principles of Prehospital Trauma Care Golden Hour There is a golden hour if you are critically injured,
9/19/2011. Damien Beilman, RRT Adult Clinical Specialist Wesley Medical Center. Epidural Hematoma: Lens Shaped.
 Damien Beilman, RRT Adult Clinical Specialist Wesley Medical Center Epidural Hematoma: Lens Shaped. 1 Epidural Hematoma Subdural Hematoma: Crescent-shaped Subdural Hematoma 2 Cerebral Contusion Cause of
Damien Beilman, RRT Adult Clinical Specialist Wesley Medical Center Epidural Hematoma: Lens Shaped. 1 Epidural Hematoma Subdural Hematoma: Crescent-shaped Subdural Hematoma 2 Cerebral Contusion Cause of
North Oaks Trauma Symposium Friday, November 3, 2017
 + Evaluation and Management of Facial Trauma D Antoni Dennis, MD North Oaks ENT an Allergy November 3, 2017 + Financial Disclosure I do not have any conflicts of interest or financial interest to disclose
+ Evaluation and Management of Facial Trauma D Antoni Dennis, MD North Oaks ENT an Allergy November 3, 2017 + Financial Disclosure I do not have any conflicts of interest or financial interest to disclose
Sign up to receive ATOTW weekly
 MANAGEMENT OF PAEDIATRIC TRAUMATIC BRAIN INJURY ANAESTHESIA TUTORIAL OF THE WEEK 127 30 TH MARCH 2009 Kavitha Raghavan, King s College Hospital, London Richard Waddington, Kingston Hospital, Surrey Correspondence
MANAGEMENT OF PAEDIATRIC TRAUMATIC BRAIN INJURY ANAESTHESIA TUTORIAL OF THE WEEK 127 30 TH MARCH 2009 Kavitha Raghavan, King s College Hospital, London Richard Waddington, Kingston Hospital, Surrey Correspondence
CHILD IN NON - TRAUMATIC COMA
 May / 2018 PELC / SLCP 1 CHILD IN NON - TRAUMATIC COMA PELS May / 2018 PELC / SLCP 2 Objectives Recognize depressed mental status Know the causes of depressed mental status in children Assessment and workup
May / 2018 PELC / SLCP 1 CHILD IN NON - TRAUMATIC COMA PELS May / 2018 PELC / SLCP 2 Objectives Recognize depressed mental status Know the causes of depressed mental status in children Assessment and workup
2. Subarachnoid Hemorrhage
 Causes: 2. Subarachnoid Hemorrhage A. Saccular (berry) aneurysm - Is the most frequent cause of clinically significant subarachnoid hemorrhage is rupture of a saccular (berry) aneurysm. B. Vascular malformation
Causes: 2. Subarachnoid Hemorrhage A. Saccular (berry) aneurysm - Is the most frequent cause of clinically significant subarachnoid hemorrhage is rupture of a saccular (berry) aneurysm. B. Vascular malformation
Chapter 8 Trauma Patient Assessment The Patient Assessment Process The Primary Assessment ABCDE s Airway, Breathing, Circulation while securing
 1 2 3 4 5 6 Chapter 8 Trauma Patient Assessment The Patient Assessment Process The Primary Assessment ABCDE s Airway, Breathing, Circulation while securing D-Disability Chief complaint and/or Mechanism
1 2 3 4 5 6 Chapter 8 Trauma Patient Assessment The Patient Assessment Process The Primary Assessment ABCDE s Airway, Breathing, Circulation while securing D-Disability Chief complaint and/or Mechanism
APPROACH TO TRAUMA. Dr E.Memary Anesthesiologist Assistant Professor of SBMU
 APPROACH TO TRAUMA Dr E.Memary Anesthesiologist Assistant Professor of SBMU Objectives Describe the initial approach to the injured patient, including the primary and secondary surveys. Identify the types
APPROACH TO TRAUMA Dr E.Memary Anesthesiologist Assistant Professor of SBMU Objectives Describe the initial approach to the injured patient, including the primary and secondary surveys. Identify the types
Basic Assessment and Treatment of Trauma
 Basic Assessment and Treatment of Trauma Final Exam Version 1 1. In which of the following scenarios would the potential for serious injury or death be the GREATEST? A. 77-kg (170-lb) man who falls 1.2
Basic Assessment and Treatment of Trauma Final Exam Version 1 1. In which of the following scenarios would the potential for serious injury or death be the GREATEST? A. 77-kg (170-lb) man who falls 1.2
NEURORADIOLOGY DIL part 3
 NEURORADIOLOGY DIL part 3 Bleeds and hemorrhages K. Agyem MD, G. Hall MD, D. Palathinkal MD, Alexandre Menard March/April 2015 OVERVIEW Introduction to Neuroimaging - DIL part 1 Basic Brain Anatomy - DIL
NEURORADIOLOGY DIL part 3 Bleeds and hemorrhages K. Agyem MD, G. Hall MD, D. Palathinkal MD, Alexandre Menard March/April 2015 OVERVIEW Introduction to Neuroimaging - DIL part 1 Basic Brain Anatomy - DIL
Patho-physiology of nervous System Talk 2 Syndromes in neurosciences. Petr Maršálek Dept pathological physiology 1.Med. F. CUNI
 Patho-physiology of nervous System Talk 2 Syndromes in neurosciences Petr Maršálek Dept pathological physiology 1.Med. F. CUNI Talks on NS Talk 1 - Pain and Motor disorders Talk 2 - This - Syndromes in
Patho-physiology of nervous System Talk 2 Syndromes in neurosciences Petr Maršálek Dept pathological physiology 1.Med. F. CUNI Talks on NS Talk 1 - Pain and Motor disorders Talk 2 - This - Syndromes in
MODULE IV. Pediatric Trauma
 MODULE IV Pediatric Trauma PRE-HOSPITAL HIGH RISK CRITERIA Blunt injury Significant injury; physiologic compromise Penetrating injuries Thorax, abdomen, head and neck High risk burns: > 10% second degree
MODULE IV Pediatric Trauma PRE-HOSPITAL HIGH RISK CRITERIA Blunt injury Significant injury; physiologic compromise Penetrating injuries Thorax, abdomen, head and neck High risk burns: > 10% second degree