M.C.D. A.A.M.I. A.A.C.D. C.I.N.D. M.C.I. M.N.C.D.
|
|
|
- Susan Patrick
- 5 years ago
- Views:
Transcription
1 M.C.D. A.A.M.I. A.A.C.D. C.I.N.D. M.C.I. M.N.C.D. 1
2 M.C.I. Dr. Gary Sinoff Department of Gerontology University of Haifa, Israel 2
3 3
4 One patient can maintain more AD pathology than another but they appear clinically the same. Clinically Mild Cognitive Impairment may be accompanied by very minimal pathology, or, enough to meet pathologic criteria for AD. 4
5 Definitions 5
6 Benign Senescent Forgetfulness 1958 Limited cognitive disturbance 1982 Mild cognitive decline (MCD) 1982 Questionable dementia 1982 Very mild cognitive decline 1982 Age-associated Memory Impairment (AAMI) 1986 Minimal dementia 1986 Amnestic syndrome 1987 Age-consistent memory impairment 1989 Late Life Forgetfulness 1989 Mild cognitive disorder 1992 Age related cognitive decline (ARCD) 1994 Mild cognitive impairment (MCI) 1994 Cognitive impairment not demented (CIND) 1995 Subclinical cognitive disorder 1996 Borderline dementia 1996 Early onset dementia 2000 Mild Neurocognitive Disorder
7 Mild Cognitive Dysfunction M.C.D. Definition: At least two of the following: - getting lost travelling to unfamiliar location - decline in work performance - word and name deficits apparent - relative little retention of material read - difficulty remembering new names - losing/misplacing objects - concentration deficit upon clinical testing (Reisberg et al., 1982, American Journal of Psychiatry) 7
8 Age Associated Memory Impairment A.A.M.I. Definition:- Complaint of Memory Impairment - Memory function 1SD below young -Age > 50 years - Adequate intellectual functioning - Absence of dementia (MMSE 24) - Absence of memory affecting disease (Crook et al., 1986, Development Neuropsychology) 8
9 Aging-associated Cognitive Decline A.A.C.D. Definition: - Subjective report of declining cognition - Decline in one area of cognition for 6 months - Difficulty in one: Memory and learning Attention and concentration Thinking Language Visuospatial function -1SD below mean by age & education on tests - Exclusion criteria (Levy et al., 1994, International Psychogeriatrics) 9
10 Mild Cognitive Impairment M.C.I. Definition: - Memory complaint by patient, family, or physician - Normal activities of daily living - Normal global cognitive functioning - Objective memory impairment by scores > 1.5SD - CDR (clinical dementia rating) score Not demented - Age between 60 and 89 years Recognize and monitor for cognitive and functional decline due to their increased risk for subsequent dementia 10
11 International Working Group on Mild Cognitive Impairment Winblad B, Palmer K, Kivipelto M, Jelic V, Fratiglioni L, Wahlund LO, Nordberg A, Bäckman L, Albert M, Almkvist O, Arai H, Basun H, Blennow K, de Leon M, DeCarli C, Erkinjuntti T, Giacobini E, Graff C, Hardy J, Jack C, Jorm A, Ritchie K, van Duijn C, Visser P, Petersen RC. Mild cognitive impairment--beyond controversies, towards a consensus: report of the International Working Group on Mild Cognitive Impairment. J. Intern. Med., 2004; 256:
12 International Working Group on Mild Cognitive Impairment - Recommend a clinical, rather than a psychometric definition of MCI - A wide range of cognitive functions appear to decline including memory, attention, language, visuospatial skill, perceptual speed and executive functioning. - Entirely compatible with the original GDS Stage 3 MCI definition. 12
13 Mild Neurocognitive Disorder Definition: - Memory complaint by patient, family, or physician - Normal activities of daily living - Objective memory impairment by scores 1-2 SD - Clinical Judgment with bedside assessments - Not demented - Not related to delirium or other mental disorder Recognize and monitor for cognitive and functional decline 13
14 Mild Neurocognitive Disorder Cognitive domains specified DSM-5: DSM-IV: Complex Memory impairment attention Executive Aphasia function Learning Apraxia & memory Language Agnosia Perceptual-motor Executive dysfunction Social cognition 14
15 Sub-Types of M.C.I. 15




16 16
17 Mild cognitive impairment Amnestic Alzheimer s disease Mild cognitive impairment Multiple domains slightly impaired Alzheimer s disease? Normal aging Mild cognitive impairment Single nonmemory domain Frontotemporal Dementia Lewy Body Dementia Primary Progressive Aphasia Parkinson s Disease Alzheimer s Disease
18 Pathology of M.C.I. 18


19 19
20 20
21 21
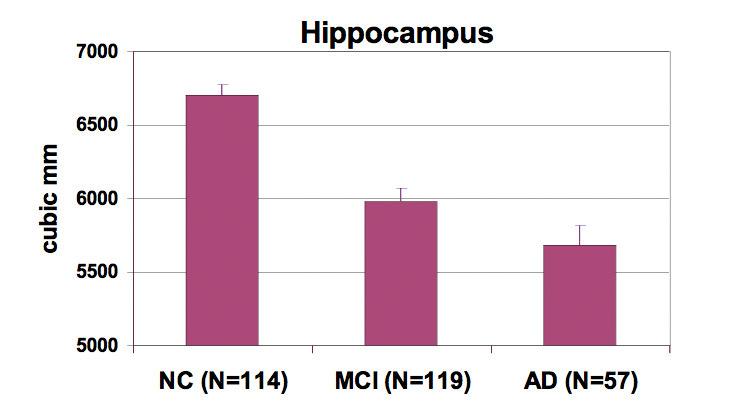
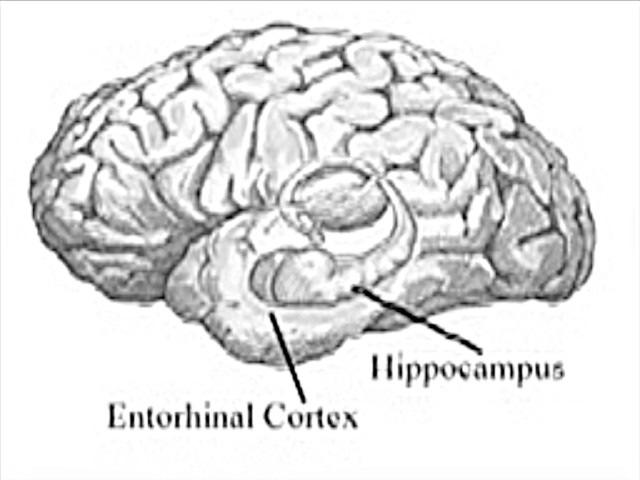
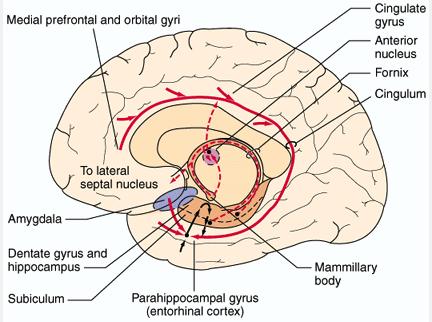
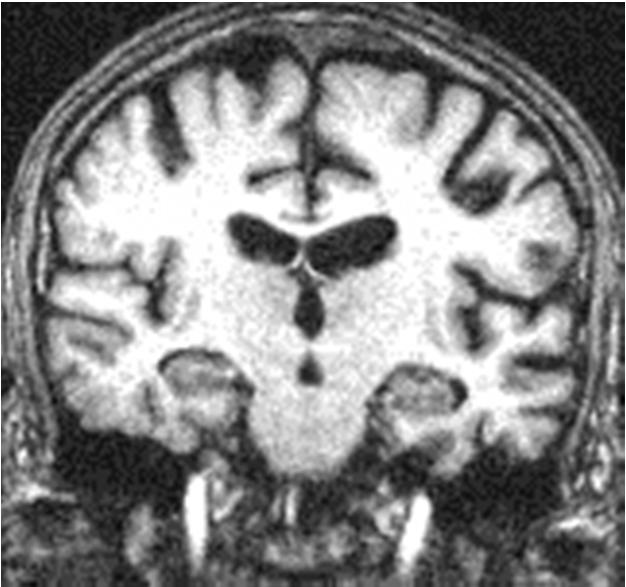
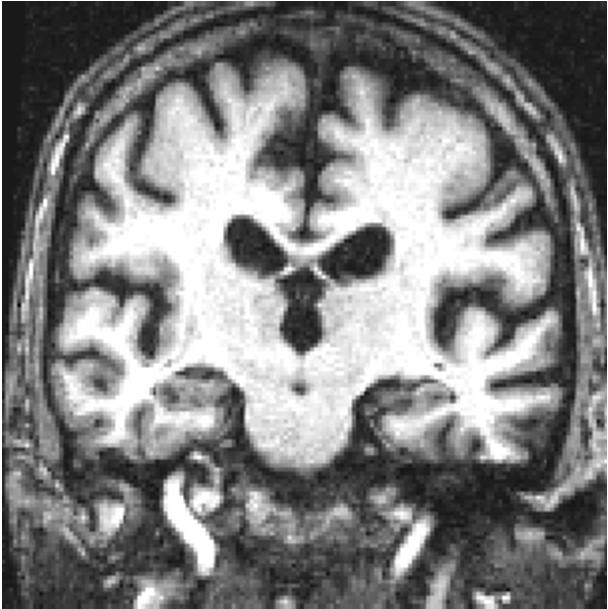
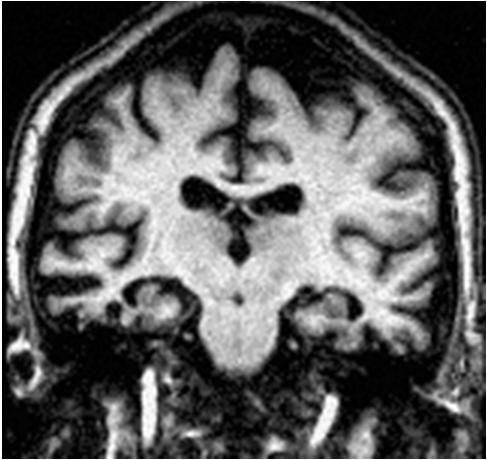
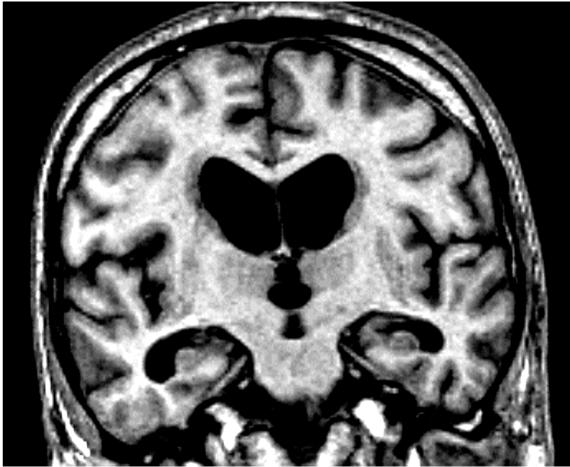
22 Hippocampal atrophy 22
23 Diagnosis 23
24 MARKERS IN AD Biomarkers of Aß deposition * spinal fluid Aßlevels * PET amyloid imaging (Pittsburg Compound B) Biomarkers of neuronal injury * spinal fluid tau levels * MRI looking at hippocampus, temporal lobe or whole brain (high-resolution T2 weighted) * FDG-PET (2-[ 18 fluoro-2-deoxy-d-glucose ) * SPECT(single-photon emission computed tomography) Genes (apolipoprotein E alleles,: others chromosome 14, presenilin-1, chromosome 1, presenilin-2, chromosome 21, APP ) 24
25 BIOMARKERS IN AD Biomarkers of Aß deposition * spinal fluid Aß levels (low) * PET amyloid imaging Biomarkers of neuronal injury * spinal fluid tau levels * MRI looking at hippocampus, temporal lobe or whole brain * FDG-PET * SPECT Genes 25
26 CSF ABeta 42 CSF levels of Total Abeta disappointing as CSF marker ABeta 42 is principal component of plaques Decreased ABeta 42 found in diverse CNS diseases including: MSA ALS CJD 26
27 SPINAL FLUID (CSF) IN AD Aβ42 Tau PTau AD MCI or N or or N Control N N N Phosphorylated tau in tangles Total tau in neuronal axons Aβ 1-42 in senile plaques 27
28 BIOMARKERS IN AD Biomarkers of Aß deposition * spinal fluid Aß levels * PET amyloid imaging (high) Biomarkers of neuronal injury * spinal fluid tau levels * MRI looking at hippocampus, temporal lobe or whole brain * FDG-PET * SPECT Genes 28

29 PIB -ve 29
30 PIB +ve 30
31 BIOMARKERS IN AD Biomarkers of Aß deposition * spinal fluid Aß levels * PET amyloid imaging Biomarkers of neuronal injury * spinal fluid tau levels (high) * MRI looking at hippocampus, temporal lobe or whole brain * FDG-PET * SPECT Genes 31
32 CSF Total-Tau: Elevated in: Head trauma Stroke Encephalitis Guillain-Barre ALS But Normal in: Depression Parkinson s Disease Alcohol overuse Non-specific marker of neuronal destruction 32
33 Phospho-Tau Several Varieties found to be raised in AD? Reflects abnormal phosphorylation in AD and not neuronal damage more generally? P-Tau 18/231, 181, 199, 231, 396/404 Not raised in stroke or Creutzfeldt-Jakob dz ALS, Parkinson s Depression Vascular, frontotemporal, or Lewy Body Dementia 33
34 SPINAL FLUID (CSF) IN AD Aβ42 Tau PTau AD MCI or N or or N Control N N N Phosphorylated tau in tangles Total tau in neuronal axons Aβ 1-42 in senile plaques 34
35 BIOMARKERS IN AD Biomarkers of Aß deposition * spinal fluid Aß levels * PET amyloid imaging Biomarkers of neuronal injury * spinal fluid tau levels * MRI looking at hippocampus, temporal lobe or whole brain (smaller) * FDG-PET * SPECT Genes 35


36 Hippocampal volume in Alzheimer s disease AD Normal tmtlwidth = 2.6 mm tmtlwidth = 14.6 mm Dark lines cross the thinnest width of the hippocampus and arrowheads indicate hippocampal boundaries. 36

37 MRI IN AD
38 BIOMARKERS IN AD Biomarkers of Aß deposition * spinal fluid Aß levels * PET amyloid imaging Biomarkers of neuronal injury * spinal fluid tau levels * MRI looking at hippocampus, temporal lobe or whole brain * FDG-PET (areas of reduced metabolism) * SPECT Genes 38
![[18F]FDG](/docs-images/95/126262975/images/39-0.jpg "normal vs")
39 [18F]FDG normal vs AD 39
40 BIOMARKERS IN AD Biomarkers of Aß deposition * spinal fluid Aß levels * PET amyloid imaging Biomarkers of neuronal injury * spinal fluid tau levels * MRI looking at hippocampus, temporal lobe or whole brain * FDG-PET * SPECT (areas of reduced blood flow) Genes 40


41 SPECT scan of normal control vs AD Normal Control Alzheimer s Disease 41
42 MARKERS IN AD Biomarkers of Aß deposition * spinal fluid Aß levels * PET amyloid imaging Biomarkers of neuronal injury * spinal fluid tau levels * MRI looking at hippocampus, temporal lobe or whole brain * FDG-PET * SPECT Genes 42
43 Genes and Alzheimer s disease (60% -80 % of causation) (all known genes relate to βamyloid) Familial AD (onset < 60 y/o) (<5%) Presenilin I, II (ch 14, 1) APP (ch 21) Non-familial (late onset) APOE Clinical studies suggest 40 50% due to ε4 If ε2 is considered, may be 95% of causation Population studies suggest 10 20% cause Evolution over last 300,000 to 200,000 years At least 20 other genes 43
44 Conversion to Dementia APOE 4 noncarrier % APOE 4 carrier Years 44
45 AD Progression Abnormal FDG-PET MRI hippocampal volume Amyloid imaging CSF Aβ 42 Cognitive performance Function (ADL) CSF Tau Normal Presymptomatic emci LMCI Dementia Time Aisen PS, Petersen RC, Donohue MC, et al. Alzheimers Dement. 2010;6:
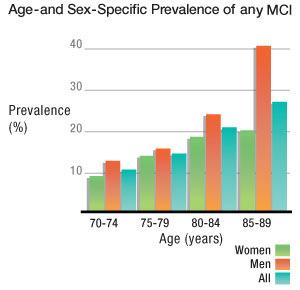
46 Prevalence of M.C.I. 46
47 MCI Prevalence Baseline MCI prevalence 34.8% Amnestic MCI 10.5% Amnestic multi-domain MCI 8.8% Nonamnestic MCI 12.8% Nonamnestic multi-domain MCI 2.7% Sachdev et al. (2010). International Psychogeriatrics, 22:8,
48 48
49 Progression of M.C.I. 49
50 50
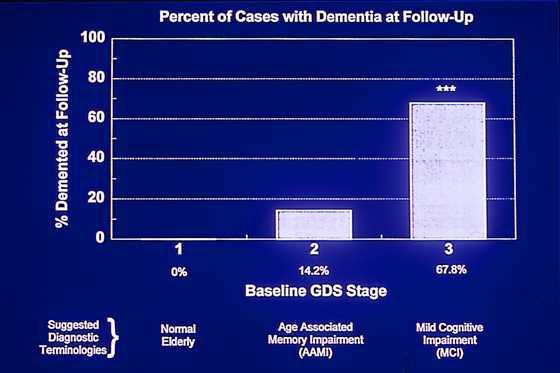
51 Mild Cognitive Impairment MCI AD 12%/yr Control AD 1-2%/yr Initial exam Months 50 Initial exam Months MCI AD Controls AD Petersen RC et al: Arch Neurol 56: ,
52 Progression to Dementia Progression MCI to dementia = 12.8% 1 Progression No Cognitive Impairment (NCI) to dementia = 1.8% % 4,5,6 of those with MCI at baseline reverted to NCI at follow-up Multidomainsubtypes more likely to progress to dementia (vs. NCI) than single domain 52


 Baseline")
53 MCI stability: Published norms Participants (%) Baseline classification 53

54 Importance of MCI as a prodromalsyndrome MCI annual conversion rate to dementia approx 12% Normal controls: 1%-2% develop MCI/Dementia BUT not everyone progresses.. 54



55 55
56 Mild Cognitive Impairment Normal MCI AD CDR GDS
57 CDR CLINICAL DEMENTIA RATE CDR 3 CDR 2 CDR-1 CDR-0.5 שכחה קלה קבועה, היזכרות חלקית שיכחה בינונית בעיקר טווח קצר מפריע בתפקוד יום- יומי שכחהקשה איןיכולתלמידה. שיכחה קשה שאריותשלקטעי זיכרון זיכרון- MEMORY מלאה התמצאות- בזמן-לקוייה מקום ואנשים תקינה בדר"כלקויה, יתכן במקוםתקינה. רק בבני אדם ORIENTATION שיפוט בעיות פתרון הפרעהקלהבפתרון בעיות (דמיון,הבדלים) פתרון בעיות לקוי, שיפוט חברתי שמור פתרון בעיות-לקוי יתכן שיפוט תקין לסירוגין לא קיים תפקוד חברתי תקין עד הפרעה קלה לקוי- למתבונןמקרי יכוללהיראותתקין אין, איןגם העמדתפנים. לא קיים שמור תפקוד בבית הפרעה ברורה תפקידים פשוטים, התענינות מוגבלת אין יזימה לתפקוד כלשהוא / תפקוד מלא זקוק לדרבון עזרהבלבוש היגיינהעצמאי עזרהקלה עזרה רבה בטפול עצמי,בד"כ אי שליטה ADL
58 The Global Deterioration Scale (GDS) 58
59 59
60 60
61 61
62 Global Deterioration Scale Stage Diagnosis and Nl Nl MCI Mild Mod Mod-Severe Severity without with AD AD AD SCI SCI 62
63 GDS Stage 1 Healthy older persons Free of subjective complaints of cognitive impairment Free of objective evidence of cognitive impairment 63
64 GDS Stage 2 Subjective complaints of memory deficit. e.g., forgetting names one formerly knew well Forgetting where one has placed familiar objects. No objective evidence of memory deficit on clinical interview No objective deficit in employment or social situations 64
65 SCI vs NCI: Prediction of Dementia Geerlings, et al., Am J. Psychiatry, year F/U (MMSE 26) x3 risk for SCI van Oijen, et al., Alzheimer s and Dementia, year F/U (MMSE =29 or 30 ) x3 risk in high education group St. John and Montgomery Int J Geriatr Psychiatry, After adjusting for age, gender, and depressive symptoms, SCI predicted dementia. 15% developed dementia in 5 yrs. 65
66 Mean Time to Decline NCI SCI (GDS Stage 1) (GDS Stage 2) 8.8 years 5.3 years SCI persons have a ~ 4.5 x greater risk of decline to MCI or dementia than same gender, similarly aged and educated, non- SCI persons Reisberg, Shulman, Torossian et al., Outcome over seven years of healthy adults with and without subjective cognitive impairment, Alzheimer s & Dementia, 6; 11-24,
67 Survival Analysis: Kaplan-Meier Method 67
68 Top Ten Warning Signs Alzheimer Association 1. Recent memory loss affecting job 2. Difficulty performing familiar tasks 3. Problems with language 4. Disorientation to time or place 5. Poor or decreased judgment 6. Problems with abstract thinking 7. Misplacing things 8. Changes in mood or behavior 9. Changes in personality 10. Loss of initiative 68
69 Implications for Dementia Prevention We are now in a position to address the prevention of AD in persons with complaints beginning >20 years before dementia develops 69
M.C.D. A.A.M.I. A.A.C.D. C.I.N.D. M.C.I. M.N.C.D.
 M.C.D. A.A.M.I. A.A.C.D. C.I.N.D. M.C.I. M.N.C.D. 1 M.C.I. Dr. Gary Sinoff Department of Gerontology University of Haifa, Israel 2 One patient can maintain more AD pathology than another but they appear
M.C.D. A.A.M.I. A.A.C.D. C.I.N.D. M.C.I. M.N.C.D. 1 M.C.I. Dr. Gary Sinoff Department of Gerontology University of Haifa, Israel 2 One patient can maintain more AD pathology than another but they appear
Mild Cognitive Impairment (MCI)
") October 19, 2018 Mild Cognitive Impairment (MCI) Yonas E. Geda, MD, MSc Professor of Neurology and Psychiatry Consultant, Departments of Psychiatry & Psychology, and Neurology Mayo Clinic College of Medicine
October 19, 2018 Mild Cognitive Impairment (MCI) Yonas E. Geda, MD, MSc Professor of Neurology and Psychiatry Consultant, Departments of Psychiatry & Psychology, and Neurology Mayo Clinic College of Medicine
Mild cognitive impairment beyond controversies, towards a consensus: report of the International Working Group on Mild Cognitive Impairment
 Journal of Internal Medicine 2004; 256: 240 246 KEY SYMPOSIUM Mild cognitive impairment beyond controversies, towards a consensus: report of the International Working Group on Mild Cognitive Impairment
Journal of Internal Medicine 2004; 256: 240 246 KEY SYMPOSIUM Mild cognitive impairment beyond controversies, towards a consensus: report of the International Working Group on Mild Cognitive Impairment
Mild Cognitive Impairment
 Mild Cognitive Impairment Victor W. Henderson, MD, MS Departments of Health Research & Policy (Epidemiology) and of Neurology & Neurological Sciences Stanford University Director, Stanford Alzheimer s
Mild Cognitive Impairment Victor W. Henderson, MD, MS Departments of Health Research & Policy (Epidemiology) and of Neurology & Neurological Sciences Stanford University Director, Stanford Alzheimer s
#CHAIR2015. Miami, Florida. September 24 26, JW Marriott Miami. Sponsored by
 #CHAIR2015 September 24 26, 2015 JW Marriott Miami Miami, Florida Sponsored by Case Challenge Workshop Alzheimer s Disease Anand Kumar, MD University of Illinois at Chicago, College of Medicine Chicago,
#CHAIR2015 September 24 26, 2015 JW Marriott Miami Miami, Florida Sponsored by Case Challenge Workshop Alzheimer s Disease Anand Kumar, MD University of Illinois at Chicago, College of Medicine Chicago,
Form D1: Clinician Diagnosis
 Initial Visit Packet Form D: Clinician Diagnosis NACC Uniform Data Set (UDS) ADC name: Subject ID: Form date: / / Visit #: Examiner s initials: INSTRUCTIONS: This form is to be completed by the clinician.
Initial Visit Packet Form D: Clinician Diagnosis NACC Uniform Data Set (UDS) ADC name: Subject ID: Form date: / / Visit #: Examiner s initials: INSTRUCTIONS: This form is to be completed by the clinician.
DEMENTIA? 45 Million. What is. WHAT IS DEMENTIA Dementia is a disturbance in a group of mental processes including: 70% Dementia is not a disease
 What is PRESENTS DEMENTIA? WHAT IS DEMENTIA Dementia is a disturbance in a group of mental processes including: Memory Reasoning Planning Learning Attention Language Perception Behavior AS OF 2013 There
What is PRESENTS DEMENTIA? WHAT IS DEMENTIA Dementia is a disturbance in a group of mental processes including: Memory Reasoning Planning Learning Attention Language Perception Behavior AS OF 2013 There
DISCLOSURES. Objectives. THE EPIDEMIC of 21 st Century. Clinical Assessment of Cognition: New & Emerging Tools for Diagnosing Dementia NONE TO REPORT
 Clinical Assessment of Cognition: New & Emerging Tools for Diagnosing Dementia DISCLOSURES NONE TO REPORT Freddi Segal Gidan, PA, PhD USC Keck School of Medicine Rancho/USC California Alzheimers Disease
Clinical Assessment of Cognition: New & Emerging Tools for Diagnosing Dementia DISCLOSURES NONE TO REPORT Freddi Segal Gidan, PA, PhD USC Keck School of Medicine Rancho/USC California Alzheimers Disease
AT RISK, SCI, EMCI: THE ALPHABET SOUP OF PRECLINICAL AND PRODROMAL ALZHEIMER DISEASE
 AT RISK, SCI, EMCI: THE ALPHABET SOUP OF PRECLINICAL AND PRODROMAL ALZHEIMER DISEASE Mary Ellen Quiceno, MD, FAAN Associate Professor of Neurology Mary Quiceno, MD discloses she has received honoraria
AT RISK, SCI, EMCI: THE ALPHABET SOUP OF PRECLINICAL AND PRODROMAL ALZHEIMER DISEASE Mary Ellen Quiceno, MD, FAAN Associate Professor of Neurology Mary Quiceno, MD discloses she has received honoraria
Outline. Facts and figures Action plans Early / correct diagnosis Conclusions
 Outline Facts and figures Action plans Early / correct diagnosis Conclusions Dementia: the greatest chalenge. Time to act now Philip Scheltens Professor of Neurology VU University Medical Center Amsterdam
Outline Facts and figures Action plans Early / correct diagnosis Conclusions Dementia: the greatest chalenge. Time to act now Philip Scheltens Professor of Neurology VU University Medical Center Amsterdam
Erin Cullnan Research Assistant, University of Illinois at Chicago
 Dr. Moises Gaviria Distinguished Professor of Psychiatry, University of Illinois at Chicago Director of Consultation Liaison Service, Advocate Christ Medical Center Director of the Older Adult Program,
Dr. Moises Gaviria Distinguished Professor of Psychiatry, University of Illinois at Chicago Director of Consultation Liaison Service, Advocate Christ Medical Center Director of the Older Adult Program,
Alzheimer s disease dementia: a neuropsychological approach
 Alzheimer s disease dementia: a neuropsychological approach Dr. Roberta Biundo, PhD Neuropsychology Coordinator at Parkinson s disease and movement disorders unit of San Camillo rehabilitation hospital
Alzheimer s disease dementia: a neuropsychological approach Dr. Roberta Biundo, PhD Neuropsychology Coordinator at Parkinson s disease and movement disorders unit of San Camillo rehabilitation hospital
WHAT IS DEMENTIA? An acquired syndrome of decline in memory and other cognitive functions sufficient to affect daily life in an alert patient
 DEMENTIA WHAT IS DEMENTIA? An acquired syndrome of decline in memory and other cognitive functions sufficient to affect daily life in an alert patient Progressive and disabling Not an inherent aspect of
DEMENTIA WHAT IS DEMENTIA? An acquired syndrome of decline in memory and other cognitive functions sufficient to affect daily life in an alert patient Progressive and disabling Not an inherent aspect of
Dementia. Assessing Brain Damage. Mental Status Examination
 Dementia Assessing Brain Damage Mental status examination Information about current behavior and thought including orientation to reality, memory, and ability to follow instructions Neuropsychological
Dementia Assessing Brain Damage Mental status examination Information about current behavior and thought including orientation to reality, memory, and ability to follow instructions Neuropsychological
Moving Targets: An Update on Diagnosing Dementia in the Clinic
 Moving Targets: An Update on Diagnosing Dementia in the Clinic Eric McDade DO Department of Neurology School of Medicine Alzheimer Disease Research Center Disclosures No relevant financial disclosures
Moving Targets: An Update on Diagnosing Dementia in the Clinic Eric McDade DO Department of Neurology School of Medicine Alzheimer Disease Research Center Disclosures No relevant financial disclosures
Dementia and Healthy Ageing : is the pathology any different?
 Dementia and Healthy Ageing : is the pathology any different? Professor David Mann, Professor of Neuropathology, University of Manchester, Hope Hospital, Salford DEMENTIA Loss of connectivity within association
Dementia and Healthy Ageing : is the pathology any different? Professor David Mann, Professor of Neuropathology, University of Manchester, Hope Hospital, Salford DEMENTIA Loss of connectivity within association
Comments to this discussion are invited on the Alzforum Webinar page. Who Should Use the New Diagnostic Guidelines? The Debate Continues
 Comments to this discussion are invited on the Alzforum Webinar page. Who Should Use the New Diagnostic s? The Debate Continues Ever since new criteria came out for a research diagnosis of prodromal/preclinical
Comments to this discussion are invited on the Alzforum Webinar page. Who Should Use the New Diagnostic s? The Debate Continues Ever since new criteria came out for a research diagnosis of prodromal/preclinical
Dementia. Stephen S. Flitman, MD Medical Director 21st Century Neurology
 Dementia Stephen S. Flitman, MD Medical Director 21st Century Neurology www.neurozone.org Dementia is a syndrome Progressive memory loss, plus Progressive loss of one or more cognitive functions: Language
Dementia Stephen S. Flitman, MD Medical Director 21st Century Neurology www.neurozone.org Dementia is a syndrome Progressive memory loss, plus Progressive loss of one or more cognitive functions: Language
Dementia Update. Daniel Drubach, M.D. Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota
 Dementia Update Daniel Drubach, M.D. Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota Nothing to disclose Dementia Progressive deterioration in mental function
Dementia Update Daniel Drubach, M.D. Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota Nothing to disclose Dementia Progressive deterioration in mental function
Mild cognitive impairment: historical development and summary of research
 City University of New York (CUNY) CUNY Academic Works Publications and Research Lehman College December 2004 Mild cognitive impairment: historical development and summary of research James Golomb New
City University of New York (CUNY) CUNY Academic Works Publications and Research Lehman College December 2004 Mild cognitive impairment: historical development and summary of research James Golomb New
Diagnosis and Treatment of Alzhiemer s Disease
 Diagnosis and Treatment of Alzhiemer s Disease Roy Yaari, MD, MAS Director, Memory Disorders Clinic, Banner Alzheimer s Institute 602-839-6900 Outline Introduction Alzheimer s disease (AD)Guidelines -revised
Diagnosis and Treatment of Alzhiemer s Disease Roy Yaari, MD, MAS Director, Memory Disorders Clinic, Banner Alzheimer s Institute 602-839-6900 Outline Introduction Alzheimer s disease (AD)Guidelines -revised
Assessing and Managing the Patient with Cognitive Decline
 Assessing and Managing the Patient with Cognitive Decline Center of Excellence For Alzheimer s Disease for State of NY Capital Region Alzheimer s Center of Albany Medical Center Earl A. Zimmerman, MD Professor
Assessing and Managing the Patient with Cognitive Decline Center of Excellence For Alzheimer s Disease for State of NY Capital Region Alzheimer s Center of Albany Medical Center Earl A. Zimmerman, MD Professor
Imaging of Alzheimer s Disease: State of the Art
 July 2015 Imaging of Alzheimer s Disease: State of the Art Neir Eshel, Harvard Medical School Year IV Outline Our patient Definition of dementia Alzheimer s disease Epidemiology Diagnosis Stages of progression
July 2015 Imaging of Alzheimer s Disease: State of the Art Neir Eshel, Harvard Medical School Year IV Outline Our patient Definition of dementia Alzheimer s disease Epidemiology Diagnosis Stages of progression
Yin-Hui Siow MD, FRCPC Director of Nuclear Medicine Southlake Regional Health Centre
 Yin-Hui Siow MD, FRCPC Director of Nuclear Medicine Southlake Regional Health Centre Today Introduction to CT Introduction to MRI Introduction to nuclear medicine Imaging the dementias The Brain ~ 1.5
Yin-Hui Siow MD, FRCPC Director of Nuclear Medicine Southlake Regional Health Centre Today Introduction to CT Introduction to MRI Introduction to nuclear medicine Imaging the dementias The Brain ~ 1.5
Personal Reflections on the Design and Delivery of Services to Those with Cognitive Disorders
 Personal Reflections on the Design and Delivery of Services to Those with Cognitive Disorders Dr. David B. Hogan Brenda Strafford Foundation Chair in Geriatric Medicine University of Calgary None to declare
Personal Reflections on the Design and Delivery of Services to Those with Cognitive Disorders Dr. David B. Hogan Brenda Strafford Foundation Chair in Geriatric Medicine University of Calgary None to declare
New diagnostic criteria for Alzheimer s disease and mild cognitive impairment for the practical neurologist
 New diagnostic criteria for Alzheimer s disease and mild cognitive impairment for the practical neurologist Andrew E Budson, 1,2 Paul R Solomon 2,3 1 Center for Translational Cognitive Neuroscience, VA
New diagnostic criteria for Alzheimer s disease and mild cognitive impairment for the practical neurologist Andrew E Budson, 1,2 Paul R Solomon 2,3 1 Center for Translational Cognitive Neuroscience, VA
Brain Health and Risk Factors for Dementia
 Welcome To Brain Health and Risk Factors for Dementia Presented by Kamal Masaki, MD Professor and Chair Department of Geriatric Medicine John A. Burns School of Medicine, UH Manoa April 4, 2018 10:00 11:00
Welcome To Brain Health and Risk Factors for Dementia Presented by Kamal Masaki, MD Professor and Chair Department of Geriatric Medicine John A. Burns School of Medicine, UH Manoa April 4, 2018 10:00 11:00
Dementia Update. October 1, 2013 Dylan Wint, M.D. Cleveland Clinic Lou Ruvo Center for Brain Health Las Vegas, Nevada
 Dementia Update October 1, 2013 Dylan Wint, M.D. Cleveland Clinic Lou Ruvo Center for Brain Health Las Vegas, Nevada Outline New concepts in Alzheimer disease Biomarkers and in vivo diagnosis Future trends
Dementia Update October 1, 2013 Dylan Wint, M.D. Cleveland Clinic Lou Ruvo Center for Brain Health Las Vegas, Nevada Outline New concepts in Alzheimer disease Biomarkers and in vivo diagnosis Future trends
Mild Cognitive Impairment or Mild Neurocognitive Disorder: Implications for Clinical Practice. Hypothesized Key Players in the Pathogenesis of AD
 AD is a Neurodegenerative Disease as Seen in the PET Scan and is Characterized by Amyloid Plaques and Neurofibrillary Tangles Mild Cognitive Impairment or Mild Neurocognitive Disorder: Implications for
AD is a Neurodegenerative Disease as Seen in the PET Scan and is Characterized by Amyloid Plaques and Neurofibrillary Tangles Mild Cognitive Impairment or Mild Neurocognitive Disorder: Implications for
USE OF LABORATORY AND IMAGING INVESTIGATIONS IN DEMENTIA
 USE OF LABORATORY AND IMAGING INVESTIGATIONS IN DEMENTIA c CLINICAL See end of article for authors affiliations Correspondence to: W M van der Flier, Department of Neurology and Alzheimer Center, Vrije
USE OF LABORATORY AND IMAGING INVESTIGATIONS IN DEMENTIA c CLINICAL See end of article for authors affiliations Correspondence to: W M van der Flier, Department of Neurology and Alzheimer Center, Vrije
Overview. Case #1 4/20/2012. Neuropsychological assessment of older adults: what, when and why?
 Neuropsychological assessment of older adults: what, when and why? Benjamin Mast, Ph.D. Associate Professor & Vice Chair, Psychological & Brain Sciences Associate Clinical Professor, Family & Geriatric
Neuropsychological assessment of older adults: what, when and why? Benjamin Mast, Ph.D. Associate Professor & Vice Chair, Psychological & Brain Sciences Associate Clinical Professor, Family & Geriatric
Dementia is not normal aging!
 The Future of Alzheimer s Disease Treatment Adam L. Boxer, MD, PhD Director, Alzheimer s Disease Clinical Trials Program Memory and Aging Center Assistant Professor of Neurology University of California,
The Future of Alzheimer s Disease Treatment Adam L. Boxer, MD, PhD Director, Alzheimer s Disease Clinical Trials Program Memory and Aging Center Assistant Professor of Neurology University of California,
Cognitive Screening in Risk Assessment. Geoffrey Tremont, Ph.D. Rhode Island Hospital & Alpert Medical School of Brown University.
 Cognitive Screening in Risk Assessment Geoffrey Tremont, Ph.D. Rhode Island Hospital & Alpert Medical School of Brown University Outline of Talk Definition of Dementia and MCI Incidence and Prevalence
Cognitive Screening in Risk Assessment Geoffrey Tremont, Ph.D. Rhode Island Hospital & Alpert Medical School of Brown University Outline of Talk Definition of Dementia and MCI Incidence and Prevalence
DEMENTIA, THE BRAIN AND HOW IT WORKS AND WHY YOU MATTER
 OVERCOMING THE CHALLENGES OF MANAGING CHRONIC DISEASES IN PERSONS WITH DEMENTIA DEMENTIA, THE BRAIN AND HOW IT WORKS AND WHY YOU MATTER LEARNING OBJECTIVES Be familiar with the diagnostic criteria for
OVERCOMING THE CHALLENGES OF MANAGING CHRONIC DISEASES IN PERSONS WITH DEMENTIA DEMENTIA, THE BRAIN AND HOW IT WORKS AND WHY YOU MATTER LEARNING OBJECTIVES Be familiar with the diagnostic criteria for
A Fresh View of Cognitive Disorders in Older Adults: New Classification and Screening Strategies
 A Fresh View of Cognitive Disorders in Older Adults: New Classification and Screening Strategies Lynda Mackin, PhD, AGPCNP-BC, CNS University of California San Francisco School of Nursing 1 Alzheimer s
A Fresh View of Cognitive Disorders in Older Adults: New Classification and Screening Strategies Lynda Mackin, PhD, AGPCNP-BC, CNS University of California San Francisco School of Nursing 1 Alzheimer s
Dementia. Aetiology, pathophysiology and the role of neuropsychological testing. Dr Sheng Ling Low Geriatrician
 Dementia Aetiology, pathophysiology and the role of neuropsychological testing Dr Sheng Ling Low Geriatrician Topics to cover Why is dementia important What is dementia Differentiate between dementia,
Dementia Aetiology, pathophysiology and the role of neuropsychological testing Dr Sheng Ling Low Geriatrician Topics to cover Why is dementia important What is dementia Differentiate between dementia,
Dementia and Alzheimer s disease
 Since 1960 Medicine Korat โรงพยาบาลมหาราชนครราชส มา Dementia and Alzheimer s disease Concise Reviews PAWUT MEKAWICHAI MD DEPARTMENT of MEDICINE MAHARAT NAKHON RATCHASIMA HOSPITAL 1 Prevalence Increase
Since 1960 Medicine Korat โรงพยาบาลมหาราชนครราชส มา Dementia and Alzheimer s disease Concise Reviews PAWUT MEKAWICHAI MD DEPARTMENT of MEDICINE MAHARAT NAKHON RATCHASIMA HOSPITAL 1 Prevalence Increase
The Person: Dementia Basics
 The Person: Dementia Basics Objectives 1. Discuss how expected age related changes in the brain might affect an individual's cognition and functioning 2. Discuss how changes in the brain due to Alzheimer
The Person: Dementia Basics Objectives 1. Discuss how expected age related changes in the brain might affect an individual's cognition and functioning 2. Discuss how changes in the brain due to Alzheimer
Dementia: A Comprehensive Update Neuroimaging, CSF, and genetic biomarkers in dementia
 Dementia: A Comprehensive Update 2016 Neuroimaging, CSF, and genetic biomarkers in dementia Bradford C. Dickerson, M.D. Associate Professor of Neurology, Harvard Medical School Departments of Neurology
Dementia: A Comprehensive Update 2016 Neuroimaging, CSF, and genetic biomarkers in dementia Bradford C. Dickerson, M.D. Associate Professor of Neurology, Harvard Medical School Departments of Neurology
DEMENTIA 101: WHAT IS HAPPENING IN THE BRAIN? Philip L. Rambo, PhD
 DEMENTIA 101: WHAT IS HAPPENING IN THE BRAIN? Philip L. Rambo, PhD OBJECTIVES Terminology/Dementia Basics Most Common Types Defining features Neuro-anatomical/pathological underpinnings Neuro-cognitive
DEMENTIA 101: WHAT IS HAPPENING IN THE BRAIN? Philip L. Rambo, PhD OBJECTIVES Terminology/Dementia Basics Most Common Types Defining features Neuro-anatomical/pathological underpinnings Neuro-cognitive
ALZHEIMER S DISEASE. Mary-Letitia Timiras M.D. Overlook Hospital Summit, New Jersey
 ALZHEIMER S DISEASE Mary-Letitia Timiras M.D. Overlook Hospital Summit, New Jersey Topics Covered Demography Clinical manifestations Pathophysiology Diagnosis Treatment Future trends Prevalence and Impact
ALZHEIMER S DISEASE Mary-Letitia Timiras M.D. Overlook Hospital Summit, New Jersey Topics Covered Demography Clinical manifestations Pathophysiology Diagnosis Treatment Future trends Prevalence and Impact
Anxiety, Depression, and Dementia/Alzheimer Disease: What are the Links?
 The 2016 Annual Public Educational Forum Anxiety, Depression, and Dementia/Alzheimer Disease: What are the Links? Mary Ganguli MD MPH Professor of Psychiatry, Neurology, and Epidemiology, University of
The 2016 Annual Public Educational Forum Anxiety, Depression, and Dementia/Alzheimer Disease: What are the Links? Mary Ganguli MD MPH Professor of Psychiatry, Neurology, and Epidemiology, University of
Mild Cognitive Impairment in the General Population: Occurrence and progression to Alzheimer s disease
 Mild Cognitive Impairment in the General Population: Occurrence and progression to Alzheimer s disease, Marie Curie Fellow- EU Aging Research Center Department of Neurobiology, Care Sciences and Society
Mild Cognitive Impairment in the General Population: Occurrence and progression to Alzheimer s disease, Marie Curie Fellow- EU Aging Research Center Department of Neurobiology, Care Sciences and Society
Dementia and Delirium: A Neurologist s Approach to Altered Mental Status. Case 1 4/7/11. Which of the following evaluations is your next step?
 Dementia and Delirium: A Neurologist s Approach to Altered Mental Status S. Andrew Josephson, MD Director, Neurohospitalist Program Medical Director, Inpatient Neurology University of California San Francisco
Dementia and Delirium: A Neurologist s Approach to Altered Mental Status S. Andrew Josephson, MD Director, Neurohospitalist Program Medical Director, Inpatient Neurology University of California San Francisco
DISCLAIMER: ECHO Nevada emphasizes patient privacy and asks participants to not share ANY Protected Health Information during ECHO clinics.
 DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
Regulatory Challenges across Dementia Subtypes European View
 Regulatory Challenges across Dementia Subtypes European View Population definition including Early disease at risk Endpoints in POC studies Endpoints in pivotal trials 1 Disclaimer No CoI The opinions
Regulatory Challenges across Dementia Subtypes European View Population definition including Early disease at risk Endpoints in POC studies Endpoints in pivotal trials 1 Disclaimer No CoI The opinions
Clinical Diagnosis. Step 1: Dementia or not? Diagnostic criteria for dementia (DSM-IV)
") Step 1: Dementia or not? Diagnostic criteria for dementia (DSM-IV) A. The development of multiple cognitive deficits manifested by both 1 and 2 1 1. Memory impairment 2. One (or more) of the following
Step 1: Dementia or not? Diagnostic criteria for dementia (DSM-IV) A. The development of multiple cognitive deficits manifested by both 1 and 2 1 1. Memory impairment 2. One (or more) of the following
HOW TO PREVENT COGNITIVE DECLINE.AT MCI STAGE?
 EAMA CORE CURRICULUM HOW TO PREVENT COGNITIVE DECLINE.AT MCI STAGE? Sofia Duque Orthogeriatric Unit São Francisco Xavier Hospital Occidental Lisbon Hospital Center University Geriatric Unit, Faculty of
EAMA CORE CURRICULUM HOW TO PREVENT COGNITIVE DECLINE.AT MCI STAGE? Sofia Duque Orthogeriatric Unit São Francisco Xavier Hospital Occidental Lisbon Hospital Center University Geriatric Unit, Faculty of
8/14/2018. The Evolving Concept of Alzheimer s Disease. Epochs of AD Research. Diagnostic schemes have evolved with the research
 The Evolving Concept of Alzheimer s Disease David S. Geldmacher, MD, FACP Warren Family Endowed Chair in Neurology Department of Neurology UAB School of Medicine Epochs of AD Research Epoch Years Key Event
The Evolving Concept of Alzheimer s Disease David S. Geldmacher, MD, FACP Warren Family Endowed Chair in Neurology Department of Neurology UAB School of Medicine Epochs of AD Research Epoch Years Key Event
Fact Sheet Alzheimer s disease
 What is Alzheimer s disease Fact Sheet Alzheimer s disease Alzheimer s disease, AD, is a progressive brain disorder that gradually destroys a person s memory and ability to learn, reason, make judgements,
What is Alzheimer s disease Fact Sheet Alzheimer s disease Alzheimer s disease, AD, is a progressive brain disorder that gradually destroys a person s memory and ability to learn, reason, make judgements,
The ABCs of Dementia Diagnosis
 The ABCs of Dementia Diagnosis Dr. Robin Heinrichs, Ph.D., ABPP Board Certified Clinical Neuropsychologist Associate Professor, Psychiatry & Behavioral Sciences Director of Neuropsychology Training What
The ABCs of Dementia Diagnosis Dr. Robin Heinrichs, Ph.D., ABPP Board Certified Clinical Neuropsychologist Associate Professor, Psychiatry & Behavioral Sciences Director of Neuropsychology Training What
Alzheimer s Disease without Dementia
 Alzheimer s Disease without Dementia Dr Emer MacSweeney CEO & Consultant Neuroradiologist Re:Cognition Health London Osteopathic Society 13 September 2016 Early diagnosis of Alzheimer s Disease How and
Alzheimer s Disease without Dementia Dr Emer MacSweeney CEO & Consultant Neuroradiologist Re:Cognition Health London Osteopathic Society 13 September 2016 Early diagnosis of Alzheimer s Disease How and
Dementia. Understanding 9/20/2010. Jan Robson Coordinator of the Alzheimer Society's Dementia Helpline
 Understanding Dementia Jan Robson Coordinator of the Alzheimer Society's Dementia Helpline Marc Labrecque Provincial Coordinator of Programs and Services 1 Understanding Dementia What is dementia Alzheimer
Understanding Dementia Jan Robson Coordinator of the Alzheimer Society's Dementia Helpline Marc Labrecque Provincial Coordinator of Programs and Services 1 Understanding Dementia What is dementia Alzheimer
The Australian Imaging, Biomarkers and Lifestyle Flagship Study of Ageing an example of Australian research on Alzheimer s disease
 The Australian Imaging, Biomarkers and Lifestyle Flagship Study of Ageing an example of Australian research on Alzheimer s disease AIBL: Two site collaborative study Study is conducted at two sites: Perth
The Australian Imaging, Biomarkers and Lifestyle Flagship Study of Ageing an example of Australian research on Alzheimer s disease AIBL: Two site collaborative study Study is conducted at two sites: Perth
Brain imaging for the diagnosis of people with suspected dementia
 Why do we undertake brain imaging in dementia? Brain imaging for the diagnosis of people with suspected dementia Not just because guidelines tell us to! Exclude other causes for dementia Help confirm diagnosis
Why do we undertake brain imaging in dementia? Brain imaging for the diagnosis of people with suspected dementia Not just because guidelines tell us to! Exclude other causes for dementia Help confirm diagnosis
Recommendations for the Diagnosis and Treatment of Dementia 2012
 Recommendations for the Diagnosis and Treatment of Dementia 2012 Based on the Canadian Consensus Conference on the Diagnosis and Treatment of Dementia (4 th CCCDTD) 2012 Gauthier S, Patterson C, Chertkow
Recommendations for the Diagnosis and Treatment of Dementia 2012 Based on the Canadian Consensus Conference on the Diagnosis and Treatment of Dementia (4 th CCCDTD) 2012 Gauthier S, Patterson C, Chertkow
SHARED CARE OF MCI/EARLY DEMENTIA
 SHARED CARE OF MCI/EARLY DEMENTIA BY DR. OLUFEMI BANJO MD, DTM, DCP, DIPA&DS, DHM, M.Med.Sc, FRCP(C) GERIATRIC PSYCHIATRIST. ASSISTANT MEDICAL DIRECTOR, ADULT MENTAL HEALTH AND ADDICTION, GRAND RIVER HOSPITAL
SHARED CARE OF MCI/EARLY DEMENTIA BY DR. OLUFEMI BANJO MD, DTM, DCP, DIPA&DS, DHM, M.Med.Sc, FRCP(C) GERIATRIC PSYCHIATRIST. ASSISTANT MEDICAL DIRECTOR, ADULT MENTAL HEALTH AND ADDICTION, GRAND RIVER HOSPITAL
Diagnosing Dementia: Signs & symptoms, differential diagnosis of common dementias, and non-degenerative memory loss
 Diagnosing Dementia: Signs & symptoms, differential diagnosis of common dementias, and non-degenerative memory loss Incidence of Common Neurological Diseases Incidence New Cases Disease (per 100,000) (per
Diagnosing Dementia: Signs & symptoms, differential diagnosis of common dementias, and non-degenerative memory loss Incidence of Common Neurological Diseases Incidence New Cases Disease (per 100,000) (per
Overview of neurological changes in Alzheimer s disease. Eric Karran
 Overview of neurological changes in Alzheimer s disease Eric Karran Alzheimer s disease Alois Alzheimer 1864-1915 Auguste D. 1850-1906 Case presented November 26 th 1906 Guildford Talk.ppt 20 th March,
Overview of neurological changes in Alzheimer s disease Eric Karran Alzheimer s disease Alois Alzheimer 1864-1915 Auguste D. 1850-1906 Case presented November 26 th 1906 Guildford Talk.ppt 20 th March,
DSM-5 MAJOR AND MILD NEUROCOGNITIVE DISORDERS (PAGE 602)
") SUPPLEMENT 2 RELEVANT EXTRACTS FROM DSM-5 The following summarizes the neurocognitive disorders in DSM-5. For the complete DSM-5 see Diagnostic and Statistical Manualof Mental Disorders, 5th edn. 2013,
SUPPLEMENT 2 RELEVANT EXTRACTS FROM DSM-5 The following summarizes the neurocognitive disorders in DSM-5. For the complete DSM-5 see Diagnostic and Statistical Manualof Mental Disorders, 5th edn. 2013,
ORIGINAL ARTICLE. Prevalence of Neuropsychiatric Symptoms in Mild Cognitive Impairment and Normal Cognitive Aging. normal cognitive aging
 ORIGINAL ARTICLE Prevalence of Neuropsychiatric Symptoms in Mild Cognitive Impairment and Normal Cognitive Aging Population-Based Study Yonas E. Geda, MD, MSc; Rosebud O. Roberts, MB, ChB, MS; David S.
ORIGINAL ARTICLE Prevalence of Neuropsychiatric Symptoms in Mild Cognitive Impairment and Normal Cognitive Aging Population-Based Study Yonas E. Geda, MD, MSc; Rosebud O. Roberts, MB, ChB, MS; David S.
Round table: Moderator; Fereshteh Sedaghat, MD, PhD Brain Mapping in Dementias and Non-invasive Neurostimulation
 Round table: Moderator; Fereshteh Sedaghat, MD, PhD Brain Mapping in Dementias and Non-invasive Neurostimulation 1. Reflection of Mild Cognitive Impairment (MCI) and Dementias by Molecular Imaging, PET
Round table: Moderator; Fereshteh Sedaghat, MD, PhD Brain Mapping in Dementias and Non-invasive Neurostimulation 1. Reflection of Mild Cognitive Impairment (MCI) and Dementias by Molecular Imaging, PET
Response Ratio Female % Male % No Response(s) 1 <1 % Totals %
 1 <1 % Totals %") Constant Contact Survey Results Survey Name: Survey Questions for Researchers Status: Completed Filter: None Dec 03, 2008 1:30:39 PM What is your gender? Female 87 35.3 % Male 158 64.2 % No 1
Constant Contact Survey Results Survey Name: Survey Questions for Researchers Status: Completed Filter: None Dec 03, 2008 1:30:39 PM What is your gender? Female 87 35.3 % Male 158 64.2 % No 1
What APS Workers Need to Know about Frontotemporal, Lewy Body and Vascular Dementias
 What APS Workers Need to Know about Frontotemporal, Lewy Body and Vascular Dementias Presenter: Kim Bailey, MS Gerontology, Program & Education Specialist, Alzheimer s Orange County 1 1 Facts About Our
What APS Workers Need to Know about Frontotemporal, Lewy Body and Vascular Dementias Presenter: Kim Bailey, MS Gerontology, Program & Education Specialist, Alzheimer s Orange County 1 1 Facts About Our
Improving diagnosis of Alzheimer s disease and lewy body dementia. Brain TLC October 2018
 Improving diagnosis of Alzheimer s disease and lewy body dementia Brain TLC October 2018 Plan for this discussion: Introduction to AD and LBD Why do we need to improve diagnosis? What progress has been
Improving diagnosis of Alzheimer s disease and lewy body dementia Brain TLC October 2018 Plan for this discussion: Introduction to AD and LBD Why do we need to improve diagnosis? What progress has been
Memory Loss, Dementia and Alzheimer's Disease: The Basics
 Memory Loss, Dementia and Alzheimer's Disease: The Basics What is memory loss? What is age-related memory loss? Typical changes Typical age-related changes involve: Making a bad decision once in a while
Memory Loss, Dementia and Alzheimer's Disease: The Basics What is memory loss? What is age-related memory loss? Typical changes Typical age-related changes involve: Making a bad decision once in a while
ASSESSMENT MILD COGNITIVE IMPAIRMENT. (i) Is the forgetfulness or confusion acute or chronic?
 Is the forgetfulness or confusion acute or chronic?") The main pathological hallmarks of AD are the Betaamyloid plaques and neurofibrillary tangles. The risk factors for the development of this pathology include advanced age, family history, vascular risk
The main pathological hallmarks of AD are the Betaamyloid plaques and neurofibrillary tangles. The risk factors for the development of this pathology include advanced age, family history, vascular risk
Stephen Salloway, M.D., M.S. Disclosure of Interest
 Challenges in the Early Diagnosis of Alzheimer s Disease Stephen Salloway, MD, MS Professor of Neurology and Psychiatry Alpert Medical School, Brown University 2 nd Annual Early Alzheimer s Educational
Challenges in the Early Diagnosis of Alzheimer s Disease Stephen Salloway, MD, MS Professor of Neurology and Psychiatry Alpert Medical School, Brown University 2 nd Annual Early Alzheimer s Educational
7/3/2013 ABNORMAL PSYCHOLOGY SEVENTH EDITION CHAPTER FOURTEEN CHAPTER OUTLINE. Dementia, Delirium, and Amnestic Disorders. Oltmanns and Emery
 ABNORMAL PSYCHOLOGY SEVENTH EDITION Oltmanns and Emery PowerPoint Presentations Prepared by: Ashlea R. Smith, Ph.D. This multimedia and its contents are protected under copyright law. The following are
ABNORMAL PSYCHOLOGY SEVENTH EDITION Oltmanns and Emery PowerPoint Presentations Prepared by: Ashlea R. Smith, Ph.D. This multimedia and its contents are protected under copyright law. The following are
Alzheimer s Disease. Clinical characteristics of late-onset Alzheimer s disease (LOAD) A/Prof David Darby
 A/Prof David Darby") Alzheimer s Disease Clinical characteristics of late-onset Alzheimer s disease (LOAD) A/Prof David Darby Florey Institute of Neuroscience and Mental Health 28-6-2013 The burden of late-onset Alzheimer
Alzheimer s Disease Clinical characteristics of late-onset Alzheimer s disease (LOAD) A/Prof David Darby Florey Institute of Neuroscience and Mental Health 28-6-2013 The burden of late-onset Alzheimer
Evaluation and Treatment of Dementia
 Evaluation and Treatment of Dementia Jeffrey M. Burns, MD Edward H. Hashinger Professor of Neurology Co-Director, KU Alzheimer s Disease Center Director, Clinical and Translational Science Unit Disclosures
Evaluation and Treatment of Dementia Jeffrey M. Burns, MD Edward H. Hashinger Professor of Neurology Co-Director, KU Alzheimer s Disease Center Director, Clinical and Translational Science Unit Disclosures
FRONTOTEMPORAL DEGENERATION: OVERVIEW, TRENDS AND DEVELOPMENTS
 FRONTOTEMPORAL DEGENERATION: OVERVIEW, TRENDS AND DEVELOPMENTS Norman L. Foster, M.D. Director, Center for Alzheimer s Care, Imaging and Research Chief, Division of Cognitive Neurology, Department of Neurology
FRONTOTEMPORAL DEGENERATION: OVERVIEW, TRENDS AND DEVELOPMENTS Norman L. Foster, M.D. Director, Center for Alzheimer s Care, Imaging and Research Chief, Division of Cognitive Neurology, Department of Neurology
review of existing studies on ASL in dementia Marion Smits, MD PhD
 review of existing studies on ASL in dementia Marion Smits, MD PhD Associate Professor of Neuroradiology Department of Radiology, Erasmus MC, Rotterdam (NL) Alzheimer Centre South-West Netherlands, Rotterdam
review of existing studies on ASL in dementia Marion Smits, MD PhD Associate Professor of Neuroradiology Department of Radiology, Erasmus MC, Rotterdam (NL) Alzheimer Centre South-West Netherlands, Rotterdam
Alzheimer's Disease Brain Failure, Stopping the Momentum. Katherine E. Galluzzi, DO, CMD, FACOFP dist.
 AOA/ACOFP 113th Annual Convention and Scientific Seminar Las Vegas, Nevada Alzheimer's Disease Brain Failure, Stopping the Momentum Katherine E. Galluzzi, DO, CMD, FACOFP dist. Monday, October 27, 2008
AOA/ACOFP 113th Annual Convention and Scientific Seminar Las Vegas, Nevada Alzheimer's Disease Brain Failure, Stopping the Momentum Katherine E. Galluzzi, DO, CMD, FACOFP dist. Monday, October 27, 2008
Unequal Burden and Unparalleled Opportunities: Minorities in Alzheimer s Disease Research
 Unequal Burden and Unparalleled Opportunities: Minorities in Alzheimer s Disease Research J Taylor Harden, PhD, RN Executive Director National Hartford Centers of Gerontological Nursing Excellence Agenda
Unequal Burden and Unparalleled Opportunities: Minorities in Alzheimer s Disease Research J Taylor Harden, PhD, RN Executive Director National Hartford Centers of Gerontological Nursing Excellence Agenda
An estimated half a million
 Darcy Cox, PsyD, RPsych, ABPP The role of neuropsychological testing in the care of older adults The standardized administration of cognitive tests and the individualized interpretation of results can
Darcy Cox, PsyD, RPsych, ABPP The role of neuropsychological testing in the care of older adults The standardized administration of cognitive tests and the individualized interpretation of results can
BHIVA Best Practice Management Session
 BHIVA Best Practice Management Session CNS (The brain) - I keep forgetting things DEMENTIA DIAGNOSIS, CLASSIFICATION AND INVESTIGATIONS Paul Holmes Consultant Neurologist Guy s and St Thomas Hospitals
BHIVA Best Practice Management Session CNS (The brain) - I keep forgetting things DEMENTIA DIAGNOSIS, CLASSIFICATION AND INVESTIGATIONS Paul Holmes Consultant Neurologist Guy s and St Thomas Hospitals
Part 2: Early detection, assessment and treatment in relation to the new guidelines. Christopher Patterson McMaster University
 Part 2: Early detection, assessment and treatment in relation to the new guidelines Christopher Patterson McMaster University C. Patterson MD, FRCPC Division of Geriatric Medicine, McMaster University
Part 2: Early detection, assessment and treatment in relation to the new guidelines Christopher Patterson McMaster University C. Patterson MD, FRCPC Division of Geriatric Medicine, McMaster University
Latest Methods to Early Detection for Alzheimer's: Cognitive Assessments and Diagnostic Tools in Practice
 Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/alzheimers-disease-towards-earlier-detection/latest-methods-earlydetection-alzheimers-cognitive-assessments-and-diagnostic-tools-practice/8321/
Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/alzheimers-disease-towards-earlier-detection/latest-methods-earlydetection-alzheimers-cognitive-assessments-and-diagnostic-tools-practice/8321/
Alzheimer's disease (AD), also known as Senile Dementia of the Alzheimer Type (SDAT) or simply Alzheimer s is the most common form of dementia.
, also known as Senile Dementia of the Alzheimer Type (SDAT) or simply Alzheimer s is the most common form of dementia.") CHAPTER 3 Alzheimer's disease (AD), also known as Senile Dementia of the Alzheimer Type (SDAT) or simply Alzheimer s is the most common form of dementia. This incurable, degenerative, terminal disease
CHAPTER 3 Alzheimer's disease (AD), also known as Senile Dementia of the Alzheimer Type (SDAT) or simply Alzheimer s is the most common form of dementia. This incurable, degenerative, terminal disease
USE OF BIOMARKERS TO DISTINGUISH SUBTYPES OF DEMENTIA. SGEC Webinar Handouts 1/18/2013
 Please visit our website for more information http://sgec.stanford.edu/ SGEC Webinar Handouts 1/18/2013 2013 WEBINAR SERIES STATE OF THE SCIENCE: DEMENTIA EVALUATION AND MANAGEMENT AMONG DIVERSE OLDER
Please visit our website for more information http://sgec.stanford.edu/ SGEC Webinar Handouts 1/18/2013 2013 WEBINAR SERIES STATE OF THE SCIENCE: DEMENTIA EVALUATION AND MANAGEMENT AMONG DIVERSE OLDER
NACC Minimum Data Set (MDS) Public Data Element Dictionary
 Public Data Element Dictionary") Department of Epidemiology, School of Public Health and Community Medicine, University of Washington 4311 11 th Avenue NE #300 Seattle, WA 98105 phone: (206) 543-8637; fax: (206) 616-5927 e-mail: naccmail@u.washington.edu
Department of Epidemiology, School of Public Health and Community Medicine, University of Washington 4311 11 th Avenue NE #300 Seattle, WA 98105 phone: (206) 543-8637; fax: (206) 616-5927 e-mail: naccmail@u.washington.edu
Mild Cognitive Impairment
 Mild Cognitive Impairment The Role of the Family Physicians McGill Refresher Course December 2018 Fadi Massoud MD FRCPC, Internist-Geriatrician Centre Hospitalier Charles LeMoyne & Institut Universitaire
Mild Cognitive Impairment The Role of the Family Physicians McGill Refresher Course December 2018 Fadi Massoud MD FRCPC, Internist-Geriatrician Centre Hospitalier Charles LeMoyne & Institut Universitaire
The current state of healthcare for Normal Aging, Mild Cognitive Impairment, & Alzheimer s Disease
 The current state of healthcare for Normal Aging, g, Mild Cognitive Impairment, & Alzheimer s Disease William Rodman Shankle, MS MD FACP Director, Alzheimer s Program, Hoag Neurosciences Institute Neurologist,
The current state of healthcare for Normal Aging, g, Mild Cognitive Impairment, & Alzheimer s Disease William Rodman Shankle, MS MD FACP Director, Alzheimer s Program, Hoag Neurosciences Institute Neurologist,
The Aging Brain The Aging Brain
 The Aging Brain The Aging Brain R. Scott Turner, MD, PhD Director, Memory Disorders Program Professor, Department of Neurology Georgetown University Washington, DC memory.georgetown.edu rst36@georgetown.edu
The Aging Brain The Aging Brain R. Scott Turner, MD, PhD Director, Memory Disorders Program Professor, Department of Neurology Georgetown University Washington, DC memory.georgetown.edu rst36@georgetown.edu
ALZHEIMER S DISEASE OVERVIEW. Jeffrey Cummings, MD, ScD Cleveland Clinic Lou Ruvo Center for Brain Health
 ALZHEIMER S DISEASE OVERVIEW Jeffrey Cummings, MD, ScD Cleveland Clinic Lou Ruvo Center for Brain Health Prevalence AD: DEMOGRAPHY AND CLINICAL FEATURES Risk and protective factors Clinical features and
ALZHEIMER S DISEASE OVERVIEW Jeffrey Cummings, MD, ScD Cleveland Clinic Lou Ruvo Center for Brain Health Prevalence AD: DEMOGRAPHY AND CLINICAL FEATURES Risk and protective factors Clinical features and
Roger E. Kelley, M.D. Professor and Chairman Department of Neurology Tulane University School of Medicine New Orleans, Louisiana
 Roger E. Kelley, M.D. Professor and Chairman Department of Neurology Tulane University School of Medicine New Orleans, Louisiana FINANCIAL DISCLOSURE No potential conflict of interest to disclose. OBJECTIVES
Roger E. Kelley, M.D. Professor and Chairman Department of Neurology Tulane University School of Medicine New Orleans, Louisiana FINANCIAL DISCLOSURE No potential conflict of interest to disclose. OBJECTIVES
The added value of the IWG-2 diagnostic criteria for Alzheimer s disease
 The added value of the IWG-2 diagnostic criteria for Alzheimer s disease Miami, January 2016 Bruno Dubois Head of the Dementia Research Center (IMMA) Director of INSERM Research Unit (ICM) Salpêtrière
The added value of the IWG-2 diagnostic criteria for Alzheimer s disease Miami, January 2016 Bruno Dubois Head of the Dementia Research Center (IMMA) Director of INSERM Research Unit (ICM) Salpêtrière
Understanding Symptoms, Causes, and Risks for Alzheimer s Disease
 Understanding Symptoms, Causes, and Risks for Alzheimer s Disease Gene E. Alexander, Ph.D., Professor of Psychology, Neuroscience, and Physiological Sciences; Director, Brain Imaging, Behavior & Aging
Understanding Symptoms, Causes, and Risks for Alzheimer s Disease Gene E. Alexander, Ph.D., Professor of Psychology, Neuroscience, and Physiological Sciences; Director, Brain Imaging, Behavior & Aging
Mild Cognitive Impairment: An Overview
 CME 3 Review Article Mild Cognitive Impairment: An Overview By Ronald C. Petersen, MD, PhD, and Selamawit Negash, PhD ABSTRACT Mild cognitive impairment (MCI) refers to the transitional state between the
CME 3 Review Article Mild Cognitive Impairment: An Overview By Ronald C. Petersen, MD, PhD, and Selamawit Negash, PhD ABSTRACT Mild cognitive impairment (MCI) refers to the transitional state between the
Dementia Past, Present and Future
 Dementia Past, Present and Future Morris Freedman MD, FRCPC Division of Neurology Baycrest and University of Toronto Rotman Research Institute, Baycrest CNSF 2015 Objectives By the end of this presentation,
Dementia Past, Present and Future Morris Freedman MD, FRCPC Division of Neurology Baycrest and University of Toronto Rotman Research Institute, Baycrest CNSF 2015 Objectives By the end of this presentation,
ABCs of Dementia & Caregiving
 ABCs of Dementia & Caregiving Understanding the Symptoms and Behaviors of Dementia & How to Help Teepa Snow, Positive Approach, LLC to be reused only with permission. PET and Aging PET Scan of 20-Year-Old
ABCs of Dementia & Caregiving Understanding the Symptoms and Behaviors of Dementia & How to Help Teepa Snow, Positive Approach, LLC to be reused only with permission. PET and Aging PET Scan of 20-Year-Old
212 Index C-SB-13,
 Index A Acetylcholinesterase inhibitor, treatment, 15 Age-associated memory impairment (AAMI), 5 Alzheimer s disease (AD), 40, 95 96 apolipoprotein E genotype and risk for, 58 cellular neurodegeneration
Index A Acetylcholinesterase inhibitor, treatment, 15 Age-associated memory impairment (AAMI), 5 Alzheimer s disease (AD), 40, 95 96 apolipoprotein E genotype and risk for, 58 cellular neurodegeneration
Form A3: Subject Family History
 Initial Visit Packet NACC Uniform Data Set (UDS) Form A: Subject Family History ADC name: Subject ID: Form date: / / Visit #: Examiner s initials: INSTRUCTIONS: This form is to be completed by a clinician
Initial Visit Packet NACC Uniform Data Set (UDS) Form A: Subject Family History ADC name: Subject ID: Form date: / / Visit #: Examiner s initials: INSTRUCTIONS: This form is to be completed by a clinician
Minnesota Cognitive Acuity Screen (MCAS) Cognitive screening for mortality risk assessment
 Cognitive screening for mortality risk assessment") Minnesota Cognitive Acuity Screen (MCAS) Cognitive screening for mortality risk assessment Stephen K Holland, MD Chief Medical Officer LTCG stephen.holland@ltcg.com 7/18/14 1 Agenda! Cognitive impairment
Minnesota Cognitive Acuity Screen (MCAS) Cognitive screening for mortality risk assessment Stephen K Holland, MD Chief Medical Officer LTCG stephen.holland@ltcg.com 7/18/14 1 Agenda! Cognitive impairment
Mild Cognitive Impairment Symposium January 19 and 20, 2013
 Highlights of Biomarker and Clinical Outcomes in Recent AD Treatment Trials Stephen Salloway, MD, MS Professor of Neurology and Psychiatry Alpert Medical School, Brown University Mild Cognitive Impairment
Highlights of Biomarker and Clinical Outcomes in Recent AD Treatment Trials Stephen Salloway, MD, MS Professor of Neurology and Psychiatry Alpert Medical School, Brown University Mild Cognitive Impairment
Changing diagnostic criteria for AD - Impact on Clinical trials
 Changing diagnostic criteria for AD - Impact on Clinical trials London, November 2014 Bruno Dubois Head of the Dementia Research Center (IMMA) Director of INSERM Research Unit (ICM) Salpêtrière Hospital
Changing diagnostic criteria for AD - Impact on Clinical trials London, November 2014 Bruno Dubois Head of the Dementia Research Center (IMMA) Director of INSERM Research Unit (ICM) Salpêtrière Hospital
Dementia Prepared by: Joanne Leung Psychiatry Resident, University of Toronto
 Dementia Prepared by: Joanne Leung Psychiatry Resident, University of Toronto Dementias are acquired neurodegenerative disorders involving a syndrome of cognitive impairment accompanied with social and
Dementia Prepared by: Joanne Leung Psychiatry Resident, University of Toronto Dementias are acquired neurodegenerative disorders involving a syndrome of cognitive impairment accompanied with social and
3/6/2019 DIAGNOSIS OF DEMENTIA IN THE OUTPATIENT SETTING FINANCIAL DISCLOSURES LEARNING OBJECTIVES
 DIAGNOSIS OF DEMENTIA IN THE OUTPATIENT SETTING MILTA LITTLE, DO, CMD DUKE UNIVERSITY SCHOOL OF MEDICINE FINANCIAL DISCLOSURES Dr. Little has no relevant financial disclosures to report Dr. Little will
DIAGNOSIS OF DEMENTIA IN THE OUTPATIENT SETTING MILTA LITTLE, DO, CMD DUKE UNIVERSITY SCHOOL OF MEDICINE FINANCIAL DISCLOSURES Dr. Little has no relevant financial disclosures to report Dr. Little will
Neuro degenerative PET image from FDG, amyloid to Tau
 Neuro degenerative PET image from FDG, amyloid to Tau Kun Ju Lin ( ) MD, Ph.D Department of Nuclear Medicine and Molecular Imaging Center, Chang Gung Memorial Hospital ( ) Department of Medical Imaging
Neuro degenerative PET image from FDG, amyloid to Tau Kun Ju Lin ( ) MD, Ph.D Department of Nuclear Medicine and Molecular Imaging Center, Chang Gung Memorial Hospital ( ) Department of Medical Imaging